2026 MYELOMA COMMUNITY WORKSHOP
KANSAS CITY, MO

MARCH 28, 2026









MARCH 28, 2026
• Slides from Friday & Saturday Programming
• Evaluations for Friday & Saturday Programming
• SparkCures Search Engine specific for the Florida region
• Ways to Give


The International Myeloma Foundation was founded in 1990, when a myeloma patient, care partner, and their specialist came together to fulfill an unmet need: a trusted resource for the global myeloma community, so no one would feel alone.



1942 - 2025
IMF President & CEO

“I
am humbled to serve alongside so many who are making a difference every day for patients and families affected by myeloma, and I look forward to building on the IMF’s legacy of impact”
The International Myeloma Foundation is the global leader in multiple myeloma
OUR MISSION:
To improve the quality of life of myeloma patients while working toward prevention & a cure

OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease


Together, we are turning hope into action:

one meeting, one conversation, one connection at a time.

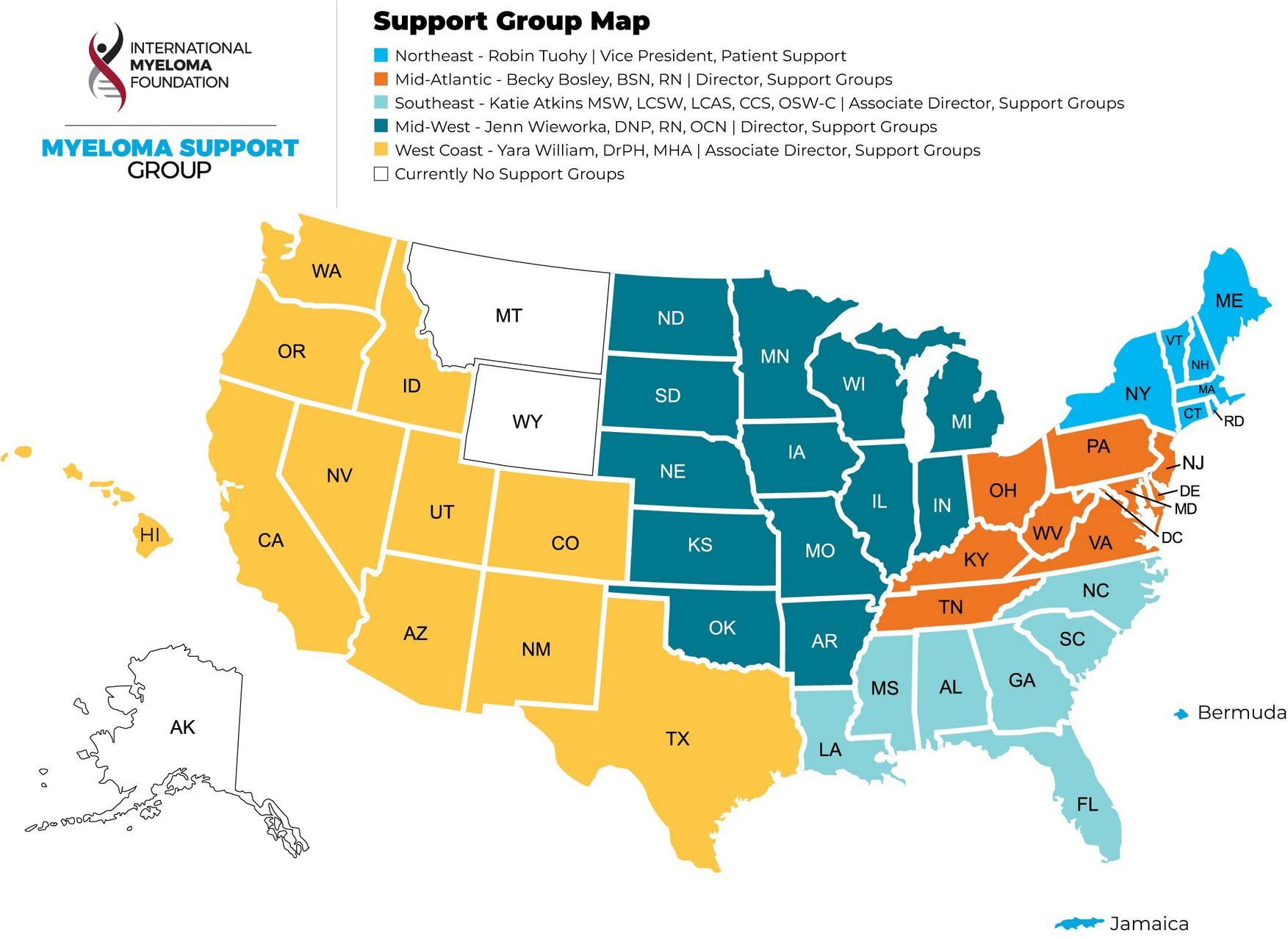
Support Groups empower patients & care partners with information, insight & hope
The IMF provides educational support to a network of over 155 myeloma specific groups


Special interest groups are designed as a supplemental support for specific populations of patients, in addition to their local Support Groups
MM Families
Founded in 2021
For patients & care partners with young children
Las Voces de Mieloma
Founded in 2022
For Spanish speaking patients & care partners
Living Solo & Strong
Founded in 2022
For patients without a care partner
Veterans SIG
Founded in 2025
For those who served our country
MM in the Middle
Founded in 2026
For those diagnosed before age 50
Smolder Bolder
Founded in 2023
For smoldering myeloma patients & care partners
Living with High-Risk Multiple Myeloma
Founded in 2023
For high-risk myeloma patients & care partners
Care Partners Only
Founded in 2024
For myeloma care partners only
Stronger Together: The IMF’s Commitment
The Myeloma Treatment Landscape
Guided Member Roundtable
Myeloma.org website walkthrough
ASH/ASCO Research Updates

Emotional Health: The Unseen Impact of Myeloma
Understanding Clinical Trials

Hope and Healing When the Future Is Uncertain
Palliative Care & Hospice
Emergency Planning





• Boca Raton, FL – March 13 – 14
• Cleveland, OH – May 1 – 2
• Los Angeles, CA – August 14 – 15
• Short Hills, NJ – October 2 – 3

Myeloma Community Workshops
• Kansas City, MO – March 28
• Virtual – April 20 – Newly Diagnosed
• Minneapolis, MN – April 25
• Detroit, MI – June 27
• Salt Lake City, UT – August 1
• Virtual – August 24 - Relapsed • Portland, OR – September 19
San Diego, CA – October 24 • Phoenix, AZ – November 14
Virtual – November 16

This year’s theme, #MoreThanMyeloma, reminds us that every patient is more than their diagnosis. And together, we will make the world take notice by lighting landmarks red across the globe.
Help shine a light on multiple myeloma by asking your city to light up a local landmark in red this March. From bridges and buildings to monuments and city halls, every illuminated landmark sparks curiosity and inspires conversation.


The IMF Advocacy Team collaborates with multiple stakeholders to inform and influence decision-making on the critical healthcare issues that directly impact myeloma patients.

The U.S. Advocacy Team advocates for equitable access to timely diagnosis, innovative treatments and research on Capitol Hill and with key regulatory
The team advocates both alongside of and on behalf of the patient community that we serve.
Advocacy play a critical role to educate policymakers about the issues important to our community and motivate them to act.
Each year, the International Myeloma Foundation brings myeloma patients and caregivers to Capitol Hill to meet with members of Congress. Together, we advocate for:
• Better access to treatment
• Stronger support for cancer research
• Policies that improve the lives of people living with myeloma
No policy experience is needed.
Just a willingness to share your experience.
IMF provides:
• Advocacy training
• Policy briefings
• Guidance every step of the way
Email us to join the IMF Advocacy Master Class and prepare for the next Hill Day.

Videos, Webinars, Podcasts, and







Understanding
Booklets
Tip Cards
Myeloma Minute
Weekly Updates

Myeloma Today
Quarterly News






S. Vincent Rajkumar, MD IMF Board Chair

Sagar Lonial, MD, FACP
Winship Cancer Institute, Emory University

Joseph Mikhael, MD, MEd, FRCPC, FACP IMF Chief Medical Officer

Thomas Martin, MD UCSF, Helen Diller
Family Comprehensive Cancer Center

Wee Joo Chng, MD National University of Singapore

María-Victoria Mateos, MD, PhD University of Salamanca

Vania Hungria, MD, PhD Santa Casa de São Paulo

Philippe Moreau, MD University Hospital of Nantes

Sigurður Yngvi Kristinsson, MD, PhD University of Iceland

NIkhil Munshi, MD Dana-Farber Cancer Institute

Shaji Kumar, MD Mayo Clinic

Jesús San Miguel, MD, PhD University of Navarra

Saad Zafar Usmani, MD, MBA, FACP, FASCO
Memorial Sloan Kettering Cancer Center

Under the guidance of the IMF Scientific Advisory Board, the IMWG identifies critical research needs, collaborations, and funding
• Primary Goal: To improve patient outcomes by identifying the most promising research to prevent and treat myeloma and ultimately, find a cure!

355 Doctors
43 Countries
70 Publications

19th Annual ONS Symposium
4,400+ learners
25,000 MM patients impacted per month!




Tanya Wildes MD, MSCI
Division of Hematology/Oncology

Normal plasma cells MGUS Smoldering myeloma
Multiple myeloma and related cancers
Normal Asymptomatic “pre-cancer” Cancer
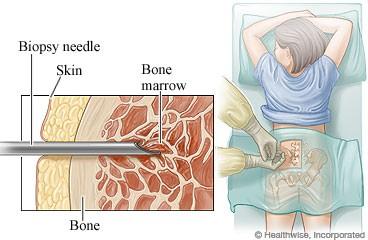
• Blood work:
• Blood counts
• Kidney function
• Calcium levels
• Beta-2 macroglobulin/LDH
• Immunoglobulin levels
• Urine tests:
• 24 hour urine collection

End-organ damage (2005)
Calcium Serum calcium >11 mg/dL (or >1mg/dL above ULN)
Renal Serum creatinine
>2mg/dL (or CrCl <40ml/min)
Anemia
Hgb <10 mg/dL (or <2 mg/dL below LLN)
Biomarkers
(SLiM, 2015) Caveats
Involved:Uninvolved
Free Light Chain ratio
≥100 Only cast nephropathy meets “R” criteria
Sixty percent plasma cells ** Must exclude other causes of anemia **
Bone lesions ≥1 lytic lesion on skeletal imaging (WBCT or PET)
MRI with >1 focal lesions (STIR MRI) Beware skull lucencies
1970
Melphalan 1990s
Autologous Stem
Cell Transplant
Thalidomide
2000s
Bortezomib
Lenalidomide
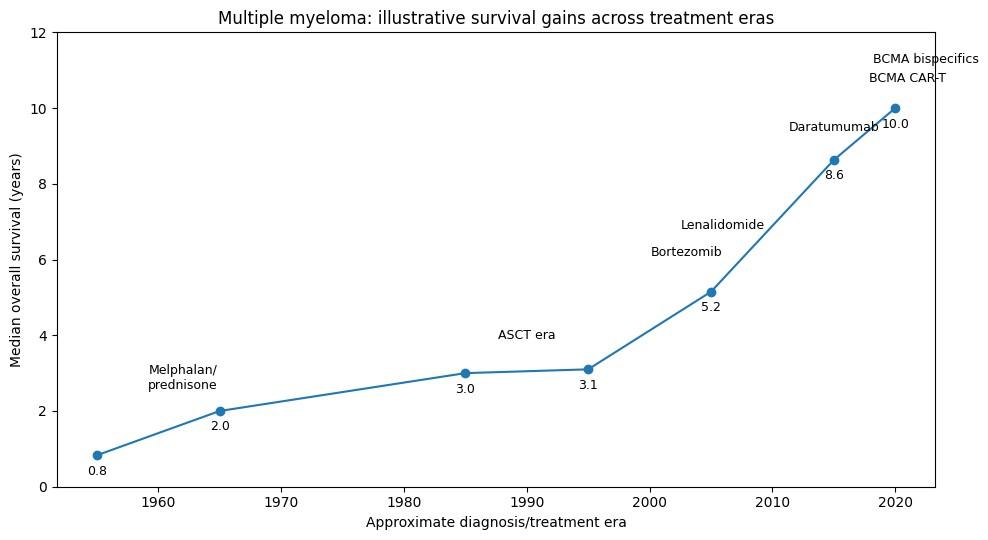
• Still considered incurable, but survival can exceed 10 years
• Trends: newer drugs 1st approved for later lines then move forward.
• Trends toward minimizing steroids
2010s
Pomalidomide
Carfilzomib
Ixazomib
Elotuzumab
Daratumumab
Isatuximab
Selinexor
2020s
Cilta-cel
Ide-cel
Teclistimab
Elranatamab
Talquetamab
Linvoseltamab
Belantamabmafadotin



Complete blood count
Comprehensive metabolic profile
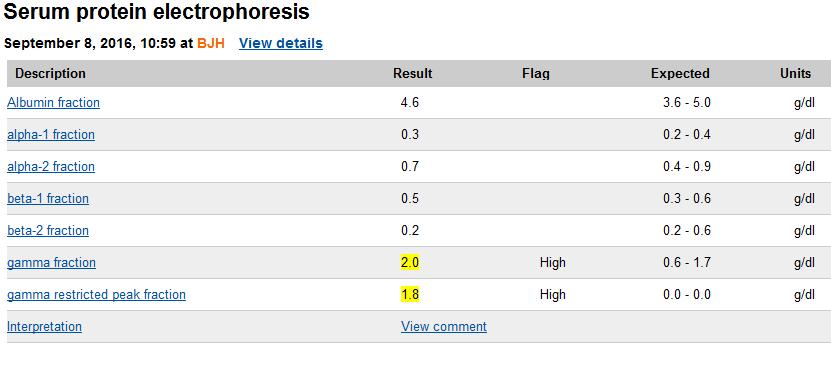
Serum protein electrophoresis +/- Immunotyping
Quantitative immunoglobulins
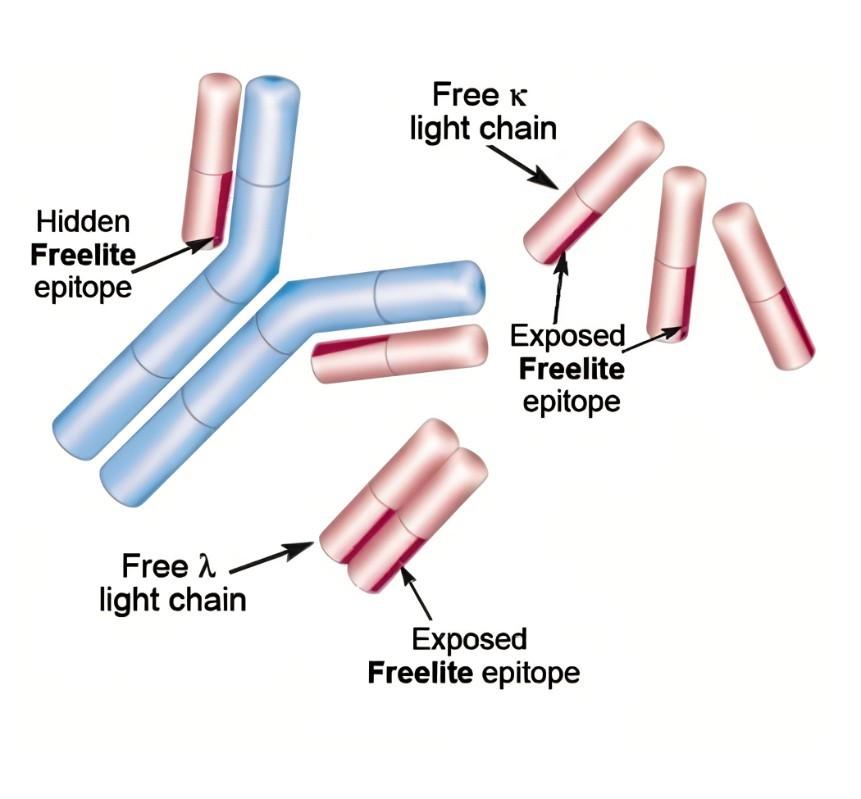
Serum free light chains
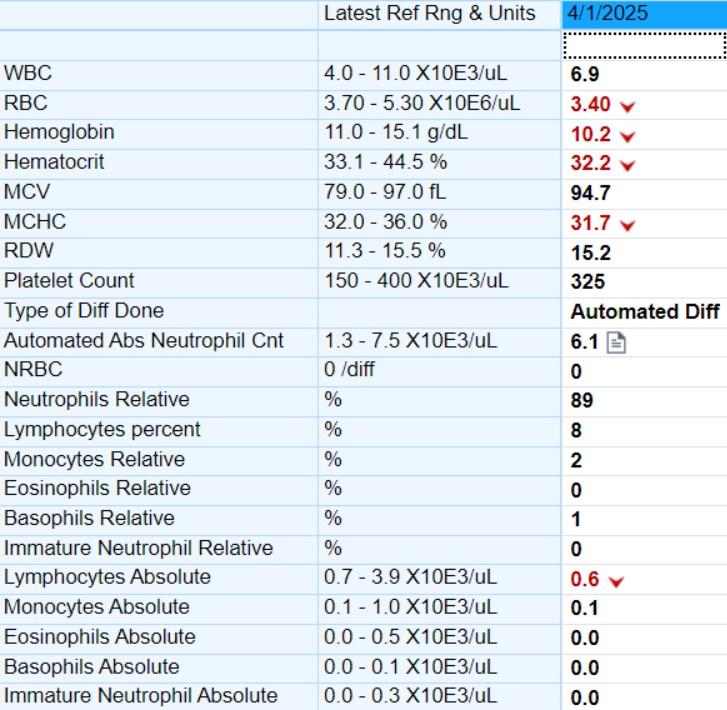
Total white blood cell count = sum of types of white blood cells (absolute neutrophils, lymphocytes, eosinophils, basophils and monocytes)
• MCV – mean corpuscular volume
• MCHC – mean corpuscular hemoglobin concentration
• RDW – red blood cell distribution width
• Usually low due to treatments (lenalidomide, bortezomib)
• Risk of bleeding due to low platelets doesn’t really increase until <30
• In hospital, we don’t transfuse unless <10
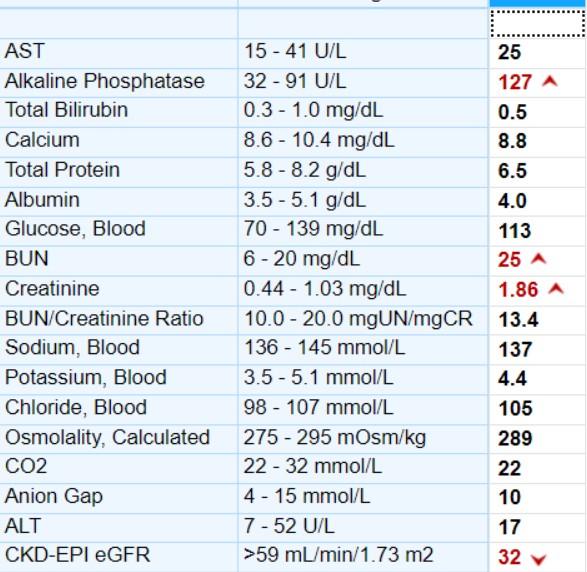
• Creatinine – trend is really important
• Calcium
• BUN/Cr>20 ratio is a marker of dehydration
• Alkaline phosphatase can be a marker of bone healing
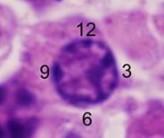
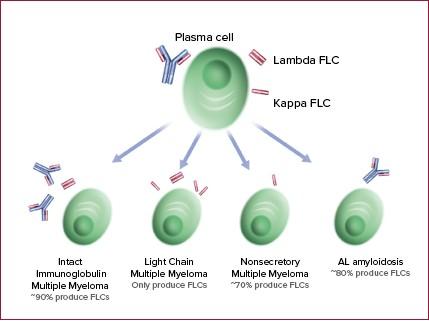
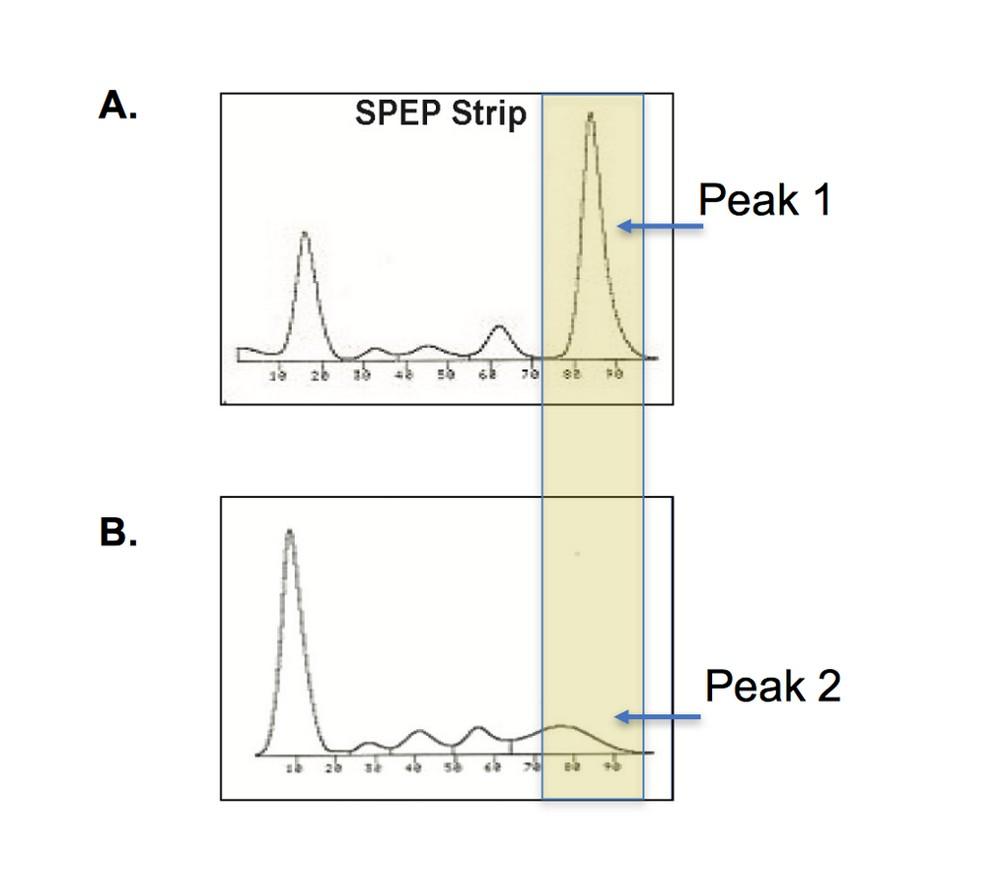
•Myeloma cells = abnormal Plasma cells
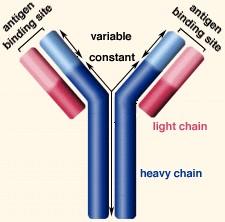
• Produce antibodies
May be an intact immunoglobulin or light chains only
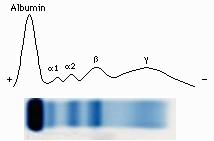
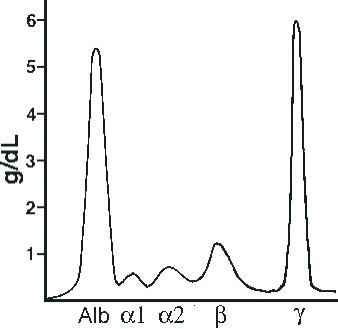
Interchangeable terms for monoclonal protein: paraprotein, monoclonal protein, M-protein, M-spike, restricted peak and more!
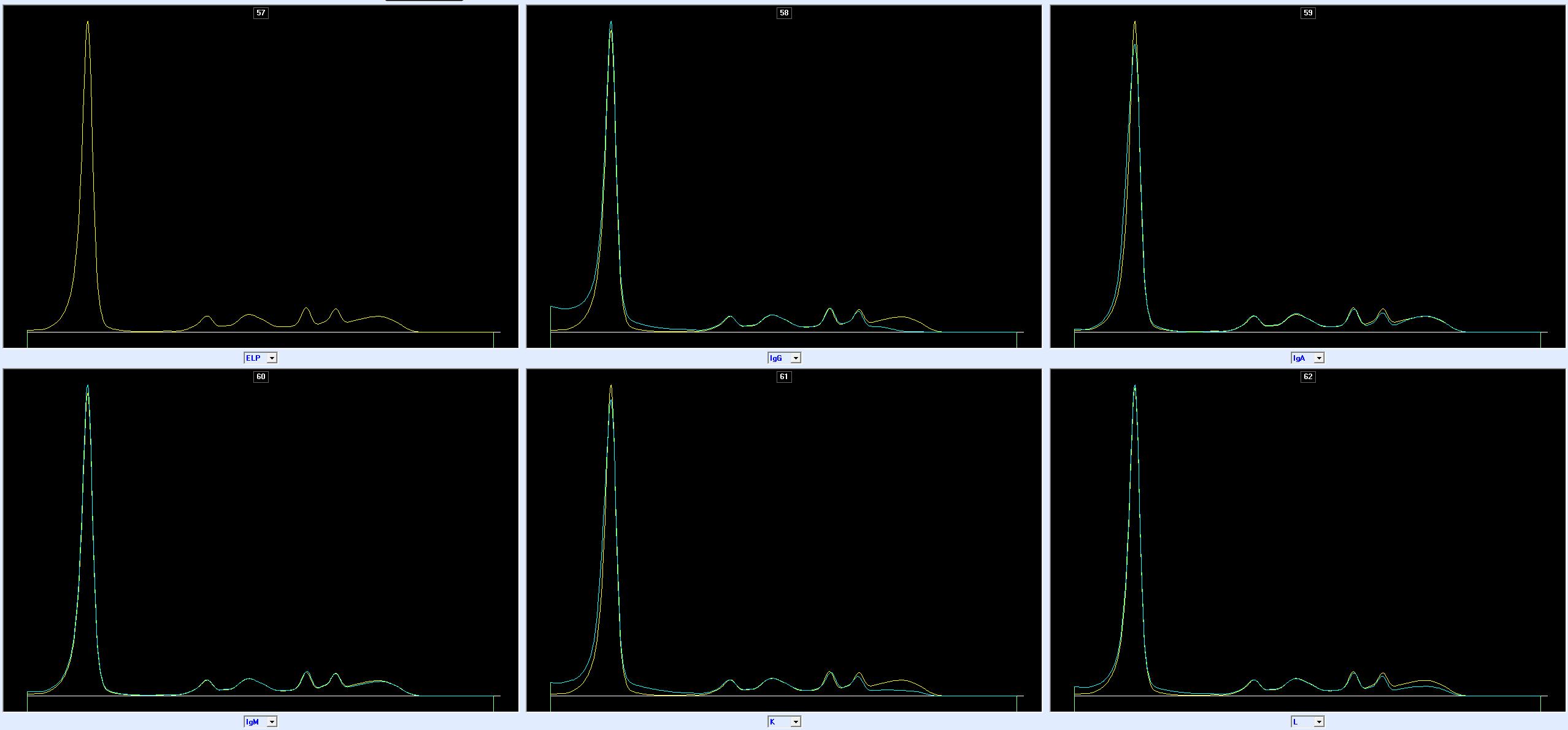
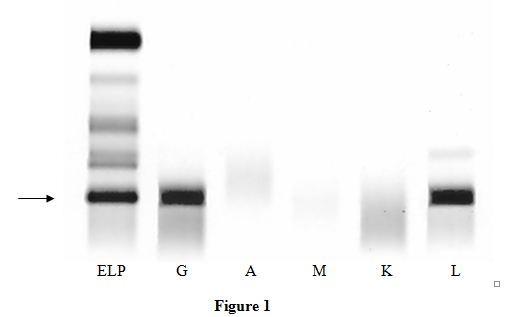
Protein electrophoresis IgG removed IgA removed
IgM removed Kappa removed
Lambda removed
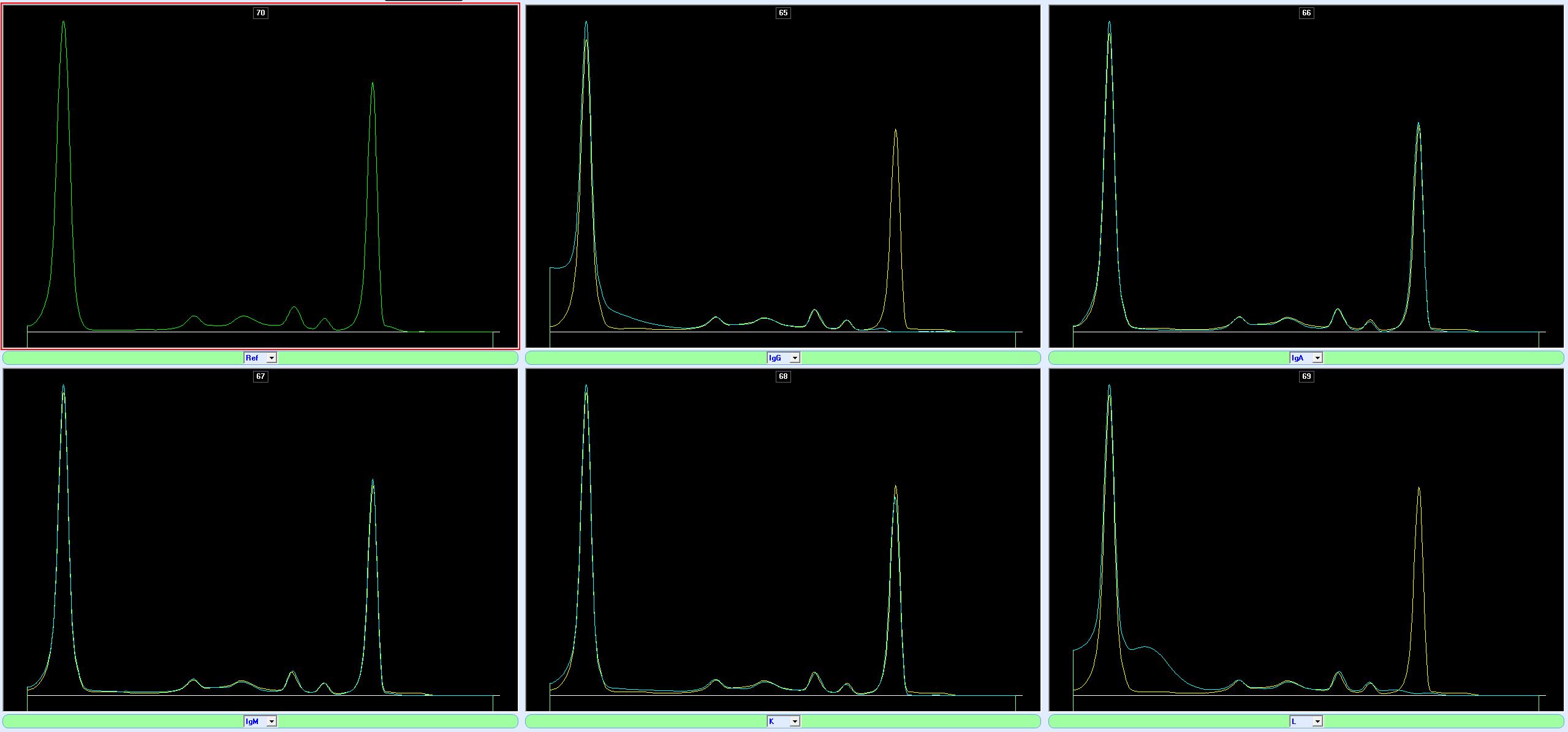
Protein electrophoresis
IgG removed IgA removed
IgM removed Kappa removed
Lambda removed
With thanks to Dr Fyffe-Freil

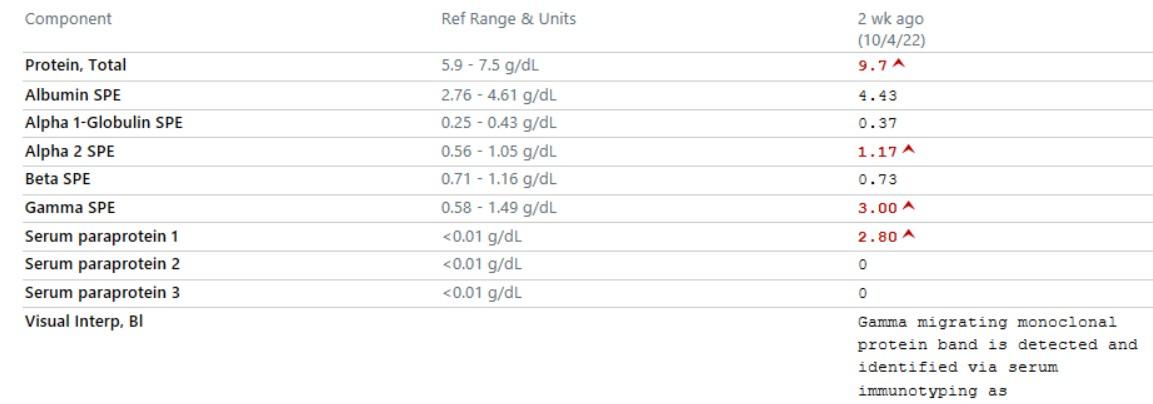
• Note well units: mg/dL or mg/L
• Normal ranges are really too narrow
• Any source of inflammation increase K & L
• Absolute levels and ranges increase with age and renal impairment
• If Green means good, is anything outside of green BAD?
• Must abnormal labs all be fixed for everything to be alright?

• If Green means good, is anything outside of green BAD?
• Must abnormal labs all be fixed for everything to be alright?
• Thankfully, NO
• Distribution based
• Large sample of “healthy people”
• Sometimes stratified by factors like sex
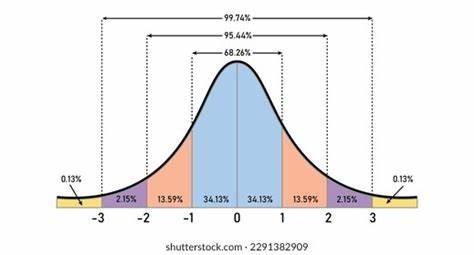
• Physiologic ranges
• Is there a cutoff above or below which there are impact on health/disease risk?
• Example: Cholesterol levels
Why do we have 2 different reference ranges on the same lab test the same day???
References ranges for ferritin are:
1. Different by gender
2. Reflect high prevalence of iron deficiency in women
Men
Women
Pitfall #1: what if “normal” population has a high prevalence of disorder?
-> Need Physiology-based normal

Example: Duffy Null phenotype

CLIA (federal lab standards) has % variation they consider acceptable. Usually ~10% but Can be 30%!!!
In statistics, regression toward the mean (also called regression to the mean, reversion to the mean, and reversion to mediocrity) is the phenomenon where if one sample of a random variable is extreme, the next sampling of the same random variable is likely to be closer to its mean
#5. Abnormal due to chance alone.

JOSEPH MIKHAEL, MD, MED, FRCPC, FACP, FASCO
CHIEF MEDICAL OFFICER, INTERNATIONAL MYELOMA FOUNDATION
Rakesh Gaur MD, MPH, FACP

From poison to less of a poison to pursuit of perfection

I may get what may be the therapy of future
I will know more about my condition
I will make friends and learn from their experience
I will be part of an expert team
I may live longer
I may live life more happily
I may be able to help someone else
I may even get the costs covered
I am a Guinea pig
I don’t trust the system
I will get a sugar-coated pill
I didn’t know a trial existed
I can’t travel that far
I may not be covered by my insurance
I have no suitable trial for me

Over 5000 trials have been conducted in myeloma
Less than 5% of patients are treated on a trial
Minorities such as African Americans comprise 20% of all myeloma. Yet the trials participation is only about 4%
Melphalan + prednisone standard
Median survival 2–3 years
Management of symptoms
Muddy designs
MRD did not exist
IFM 90 Trial: ASCT vs chemotherapy
Improved overall survival up to >8 years
Established transplant as a standard
Younger/fit patient
Subsequent maintenance

SWOG S0777: VRd vs Rd
Bortezomib improved survival >6 years
Lenalidomide expands outpatient therapy
Triplet (PI,Imid,Dex) regimen becomes standard
MAIA Trial: Daratumumab + Rd Vs. Rd for Transplant ineligible
Significant PFS improvement
Anti-CD38 becomes backbone therapy
Deep responses (MRD negativity)
CAR-T (ide-cel, cilta-cel) CARTITUDE, KARMAA
High response rates in refractory MM
Durable remissions >35% beyond 5 years
New kid on the block
Teclistamab (Tecvayli) BCMA x CD3 MajesTEC-1
ORR: 63%; Median PFS: 11.3 mo; mDOR: 18.4 mo
Talquetamab (Talvey) GPRC5D x CD3 MonumenTAL-1
ORR: 71-74% ; mDOR: 9.5 mo
Elranatamab (Elrexfio)
x CD3
ORR: 61%; 15-month PFS rate: 50.9%
•IFM 2005-02 (Maintenance): lenalidomide maintenance after autologous stem cell transplant (ASCT)
•IFM 2009 (VRd + ASCT): Confirmed that the combination of bortezomib, lenalidomide, and dexamethasone (VRd) followed by ASCT leads to longer, deeper remissions than VRd alone.
•CASSIOPEIA (Dara-Velcade Thalidomide Dex): Better PFS in transplant-eligible
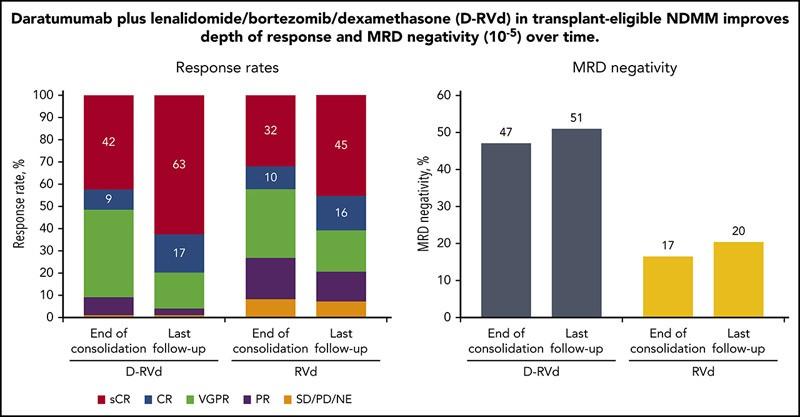
•GRIFFIN (Dara-VRd): Daratumumab with VRd improved stringent complete response rates transplant-eligible.
•MAIA (Dara-Rd): daratumumab with lenalidomide and dexamethasone for transplant-ineligible patients.
•FORTE (KRd + ASCT): carfilzomib, lenalidomide, and dexamethasone (KRd)
Relapsed/Refractory Multiple Myeloma POLLUX (Dara-Len Dex): reduces the risk of progression.
CASTOR (Dara-Velcade Dex): is superior to standard triplet.
ELOQUENT-2 (Elo-Rd): Approval of elotuzumab (antiSLAMF7) PFS and overall survival (OS).
ICARIA-MM (Isa-Pd): Isatuximab anti-CD38 PFS improvement in refractory patients.
KarMMa (Ide-cel): CAR T-cell therapy (idecabtagene vicleucel) targeting BCMA in heavily pretreated.
CARTITUDE-1 (Cilta-cel): Demonstrated deep, durable responses with ciltacabtagene autoleucel in relapsed/refractory patients, leading to earlier approval.
MajesTEC-1 (Teclistamab): 1st BCMA-targeted bispecific antibody-"off-the-shelf" option for triple-class exposed.
Overall Survival Progression-Free Survival →
Quality of life
Patient reported outcomes
MRD negativity
Faster completion and regulatory approvals
Financial toxicity
Biomarker-based
Global collaboration
Real-world evidence
Adaptive Design
Inclusion of frail
Median survival now >10 years
Higher complete remission rates by MRD
Turning into a Chronic disease
Leaping towards cure

Earlier detection and treatment
CAR-T use upfront
Bispecific antibodies in community
Trispecific trials
Better risk assessments
Personalized risk-based sequencing of drugs
Large Learning model-driven trials
All of us need to step up!
https://www.myeloma.org/sparkcures/
RAKESH
Rakesh Gaur, MD, MPH, FACP
Avoid NSAIDS- Over the counter pain medications
Hydrate well
Avoid stress on weight bearing areas if bones affected
Avoid infections
Avoid constipation
Be comfortable with your team. It will be a long journey.
PET scan
NGS- Next generation sequencing
NGF- Next Generation flow
FISH analysis
MRD- Minimal or Measurable residual disease 10-5 = 1/100000 nucleated marrow cells
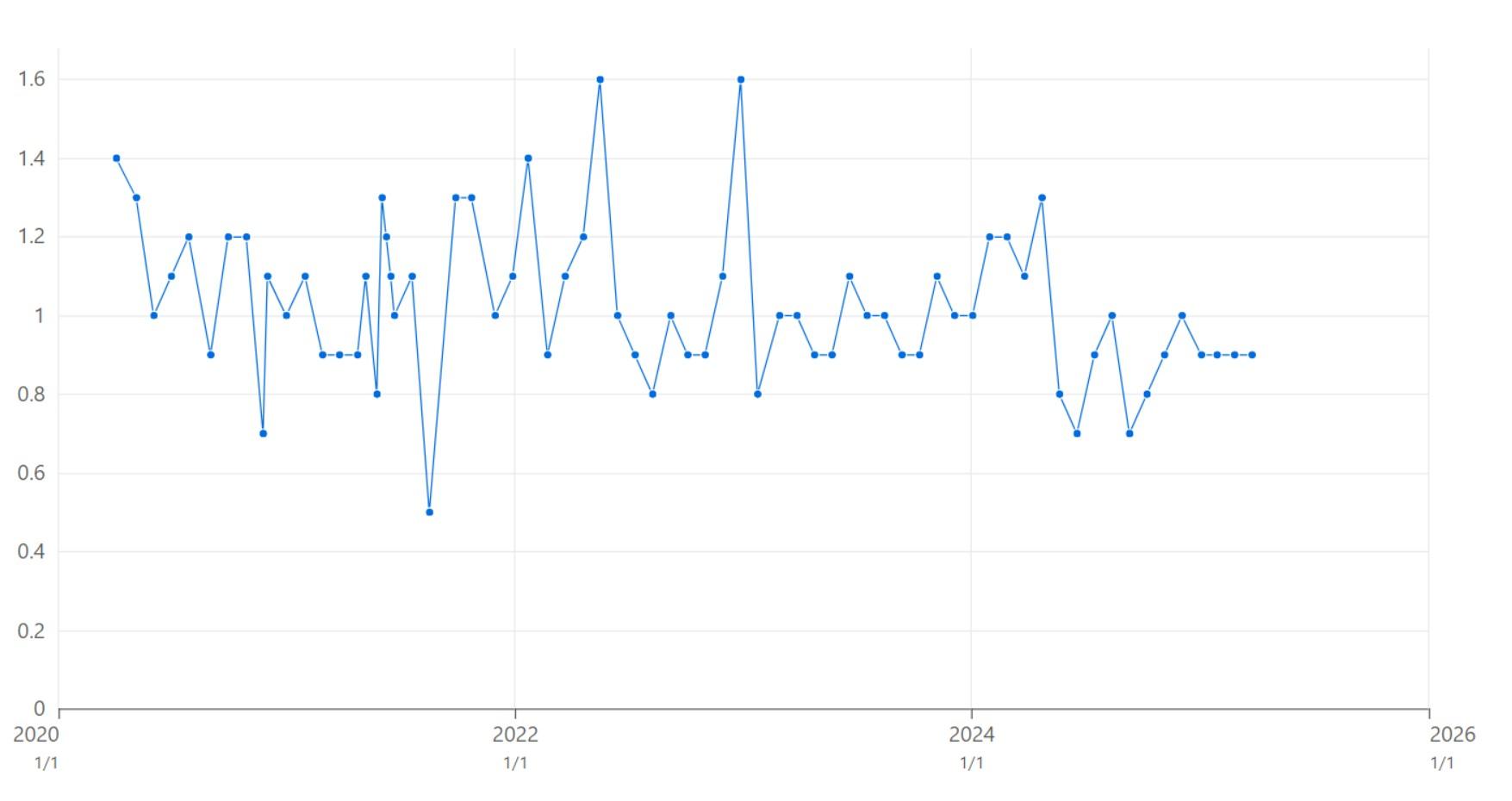
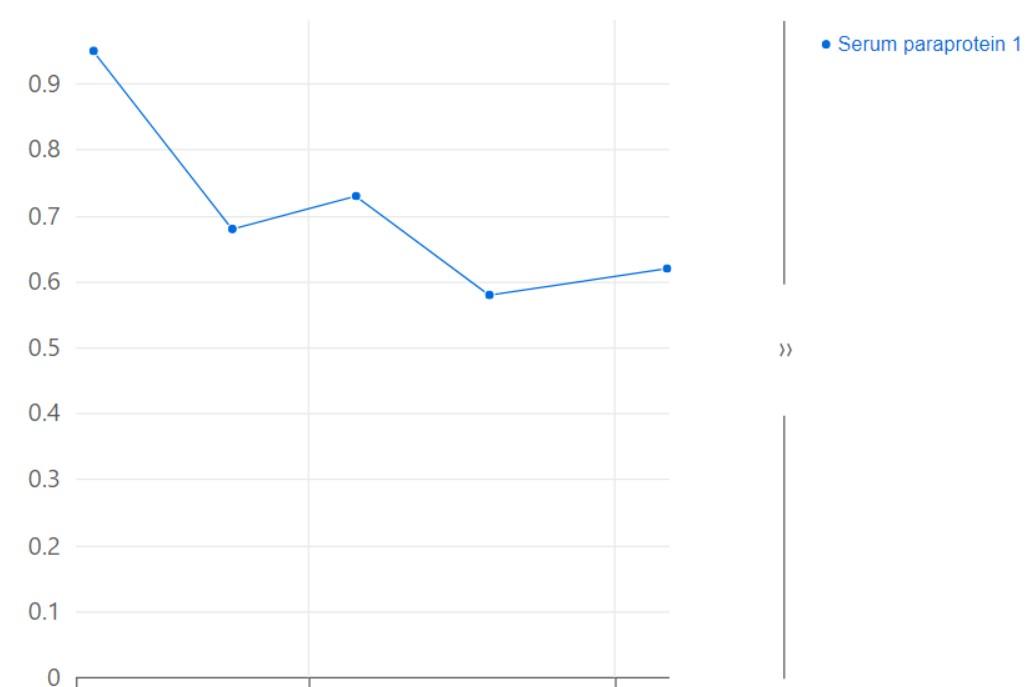
M spike
Free light chains
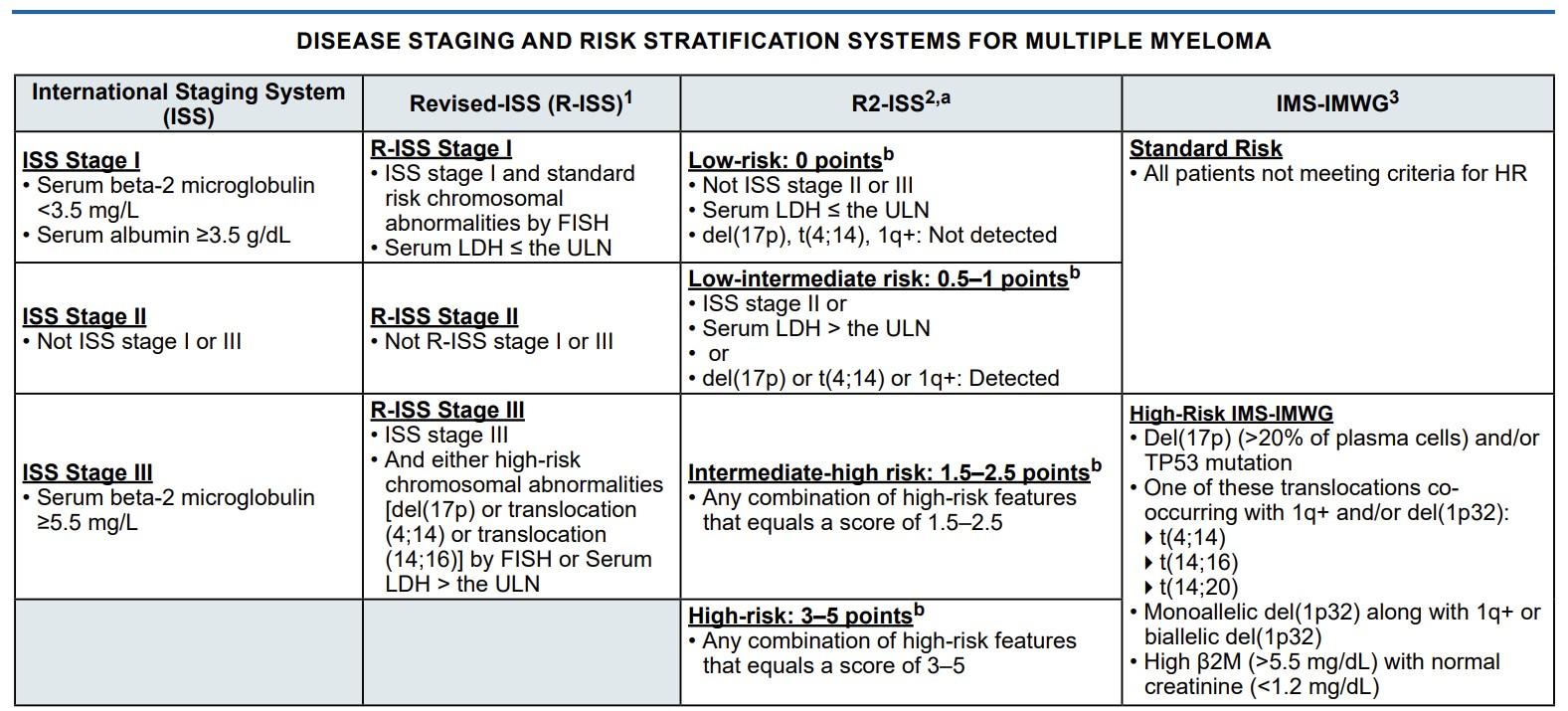
Standard risk= Not High risk
High risk(International Myeloma Working Group 2025)
-del(17p) with a clonal fraction (CCF) of 20% or greater
-Presence of t(4;14), t(14;16), or t(14;20) AND 1q+ or del 1p32
-Gain or amplification of 1q21 [amp(1q21)] or biallelic del(1p32)
-β2 microglobulin >5.5 with normal Creatinine (<1.2)
Eligible= Fit, young, good organ functions
Ineligible= Frail, >65-75, significant co morbidities
Imid- Lenalidomide, Thalidomide
Proteosome inhibitor- Velcade, Kyprolis
Antibody – Anti CD380 Darzalex, Sarclissa
Steroids-Dexamethasone
Chemotherapy- Cytoxan, Melphalan
Induction
Consolidation/transplant
Maintenance
Yes, as of now
It is at least another tool
May not last in future
Toxicities are relevant
New trials will answer
May be for more selective individuals
MASTER trial- standard-risk disease with sustained minimal residual disease (MRD) negativity may safely discontinue therapy
GMMG-CONCEPT and OPTIMUM–excellent outcomes for high-risk disease using intensive post-transplant consolidation and multi-agent maintenance
Confirmed SMM ≤5 years
Bone marrow plasma cells ≥10%
≥1 high-risk feature:
M-protein ≥30 g/L
FLC ratio ≥8 and <100
IgA subtype M protein
Immunoparesis - Decline in 2 other types of Ig
BM plasma cells >50% <60%
40% were considered high risk By Mayo criteria
Bone Marrow Plasma Cells > 20%
Serum M-Protein: > 2 g/dL
Serum Free Light Chain (FLC) Ratio: Involved/uninvolved ratio > 20

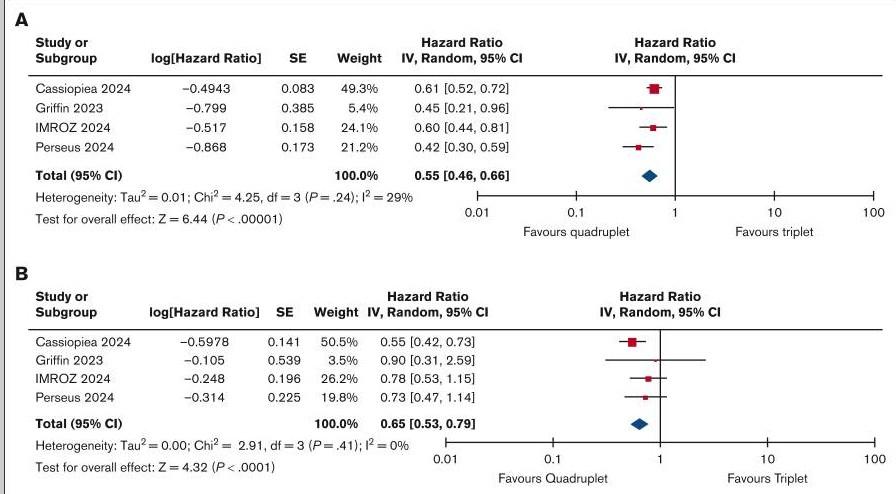
First blow is the best blow
Quadruplets may reduce chance of mutant plasma cells
Quads have a better depth of response
Many may not get a chance for 2nd or 3rd or 4th line of therapy-Attrition
Stem cell mobilization has not been a concern
Appropriate for transplant ineligible
GRIFFIN(Phase 2) - Dara Rev Velcade Dex
IMROZ- Isa Rev Velcade Dex (Transplant Ineligible)
PERSEUS(Phase 3) - Dara Rev Velcade Dex – 84% PFS at 4 years
ADVANCE- Dara Kyprolis Rev Dex – Transplant for MRD positive
IFM studies- improved survival with Lenalidomide
Small risk for secondary Hematologic Malignancies
High risk myeloma may need additional maintenance
Need to carefully monitor for neutropenic toxicities
Length of maintenance not well defined, subject to studies
Bisphosphonates
Denosumab
Anticoagulation- PREVEMM score
Prophylactic Acyclovir/Valacyclovir
Role of Kyphoplasty/Vertebroplasty
Radiation for pain
Monitor for Candidiasis
Bowel regimen with narcotics for pain
IVIG for Bite/CAR-T
Blessed is the physician whose patient trusts him. Thank You!
UNIVERSITY OF NEBRASKA MEDICAL CENTER
Tanya M Wildes, MD, MSCI
Division of Hematology/Oncology

Define relapse
What does “refractory” mean?
Distinguish between biochemical and clinical relapse

Myeloma progresses either while a patient is receiving the treatment or within 6 months of discontinuing it

Generally
we do not reuse a drug which the patient’s myeloma has proven it is refractory to…
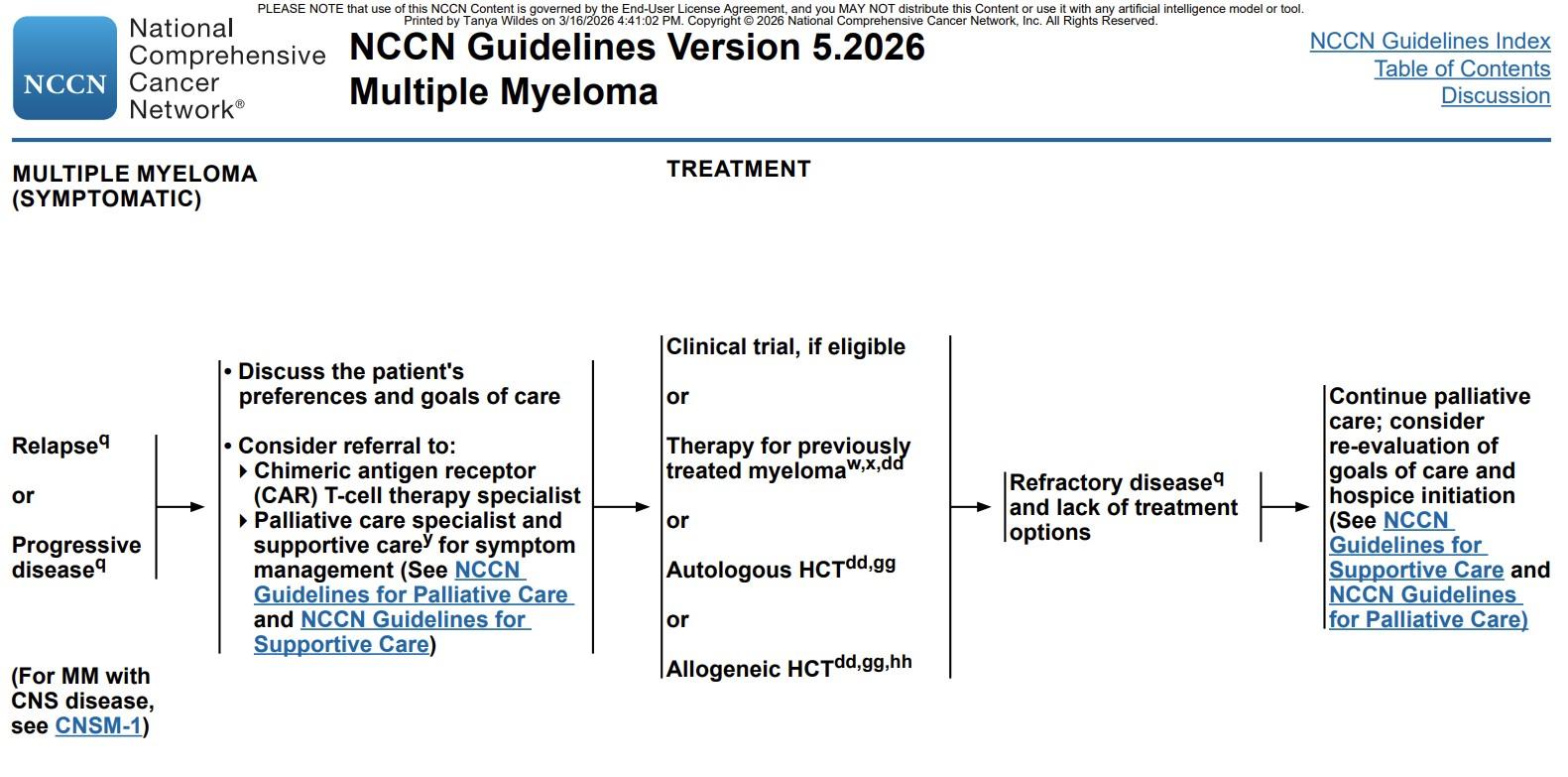
Determine if this is clinical or biochemical relapse
Determine what “Line of Therapy” we are entering
Examine prior treatments and why stopped Consider comorbidities and performance status
Inquire about preferences Any clinical trials? Choose Re-evaluate
• Proteasome inhibitors
• Immunomodulatory agents/ celmods • Monoclonal antibodies
• Chimeric antigen receptor T-cell therapy
• Bispecific T-cell engager • Antibody-drug conjugate • Conventional chemotherapy • Selinxor
Drug Administration Side effects
Bortezomib (Velcade)
Carfilzomib (Kyprolis) Intravenous (IV) Cardiac
Ixazomib (Ninlaro) Pills Diarrhea, neuropathy
Thalidomide Pills
Lenalidomide Pills
Birth defects, blood clots, low blood counts
Birth defects, blood clots, low blood counts
Pomalidomide Pills
Birth defects, blood clots, low blood counts
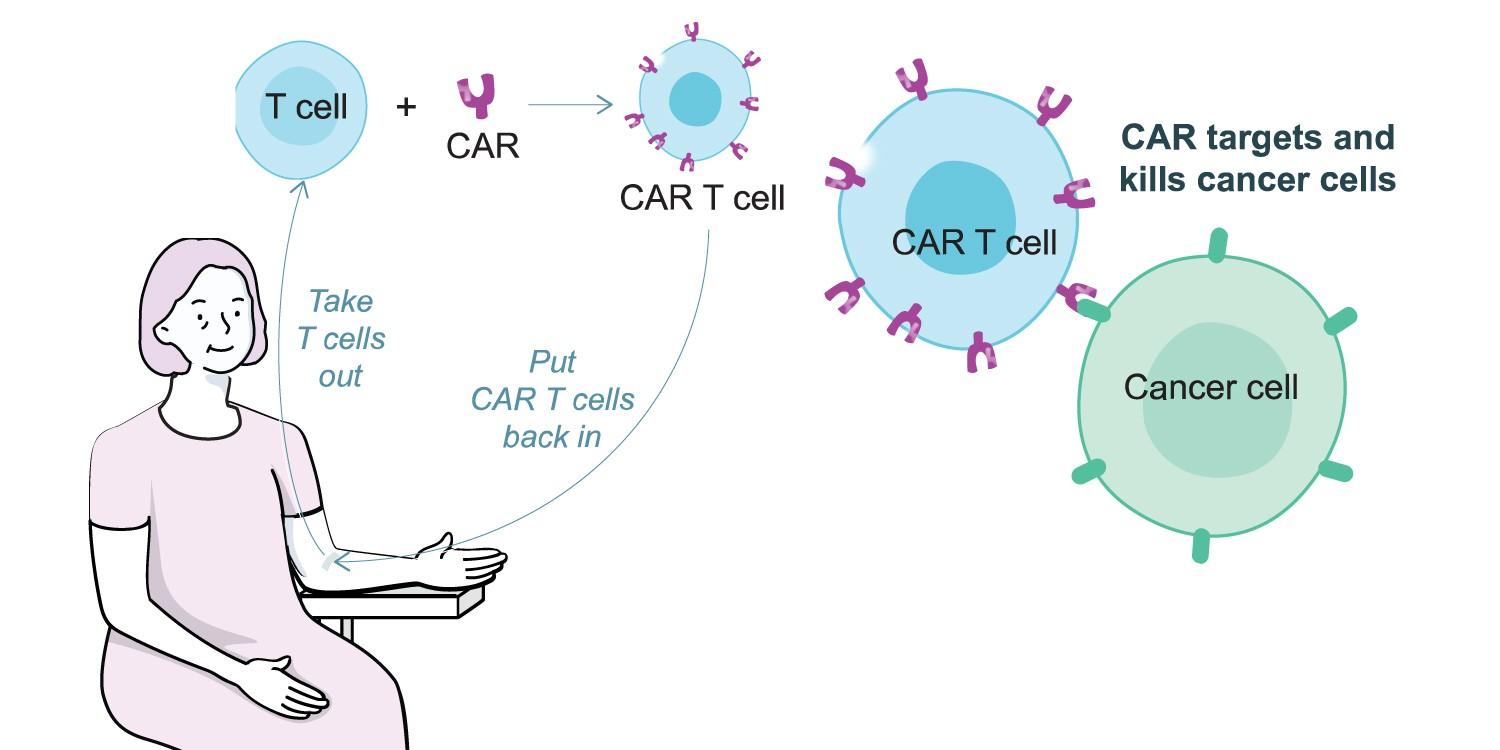
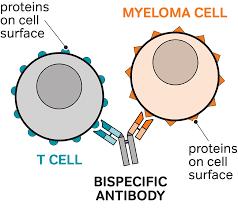
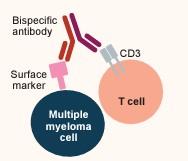
T cells are a type of white blood cell that detect and destroy abnormal cells, like myeloma cells
T cells may not recognize cancerous myeloma cells as harmful, allowing them to spread
Bispecific antibodies help to bring T cells to myeloma cells so they can attack them
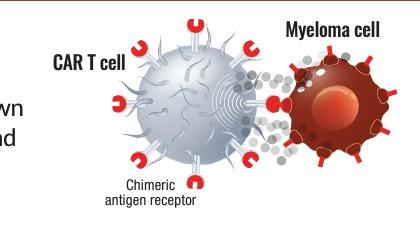
CAR T-cell therapy helps T cells bind directly to myeloma cells so they can attack them


T cell collection
One time only


CAR T cell manufacturing


Bridging therapy (if needed)


Lymphodepleting chemotherapy


CAR T infusion

Monitoring for side effects and observation
Entire process takes several weeks
Hospitalization times vary
Caregiving necessary for at least 4 weeks after treatment
• Off-the-shelf immediate treatment
• No lymphodepletion or other preparation
• Subcutaneous injection

• First two to three doses are administered as step-up doses*
‒ ~3 days apart
‒ Hospitalized ~48 hours after each step-up dose

• Ongoing weekly or biweekly (every 2 weeks) administration until disease progression or unacceptable toxicity
*Smaller doses that gradually increase to the full dose to minimize side effects
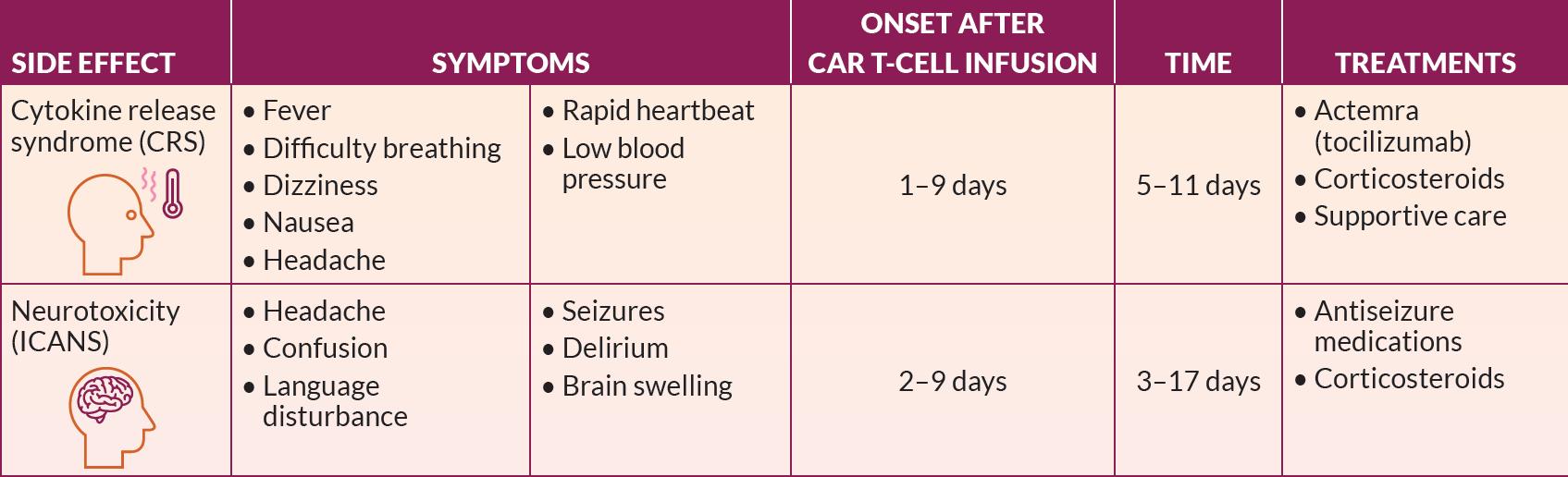
Cytokine release syndrome (CRS)

Neurotoxicity (ICANS)

Low blood counts
ICANS, immune effector cell-associated neurotoxicity syndrome
DURATION
DURATION
*Specific to talquetamab
Cytokine release syndrome (CRS)

Blood counts
Neurotoxicity (ICANS)
Infections
Skin changes/rash
Taste changes (dysgeusia)*
• One-time therapy
• Requires time to manufacture
• Able to tolerate lymphodepletion
• Treatment logistics
• Access to treatment center
• Hospitalization
• Need for a caregiver for 4 to 8 weeks after treatment
• No wait period
• No special treatment centers
• No need for lymphodepletion
• Treatment logistics
• Requires hospitalization for step-up doses
• Requires ongoing administration (weekly or biweekly)
• Caregiver play an essential role in the treatment process
• Provide help with basic day-to-day issues
• Provide emotional support
• Take patient to appointments
• Required because of driving restrictions up to 8 weeks after CAR T-cell therapy
• Note side effects
• Changes in mental state from ICANS
• Signs of CRS (fever, flu-like symptoms)



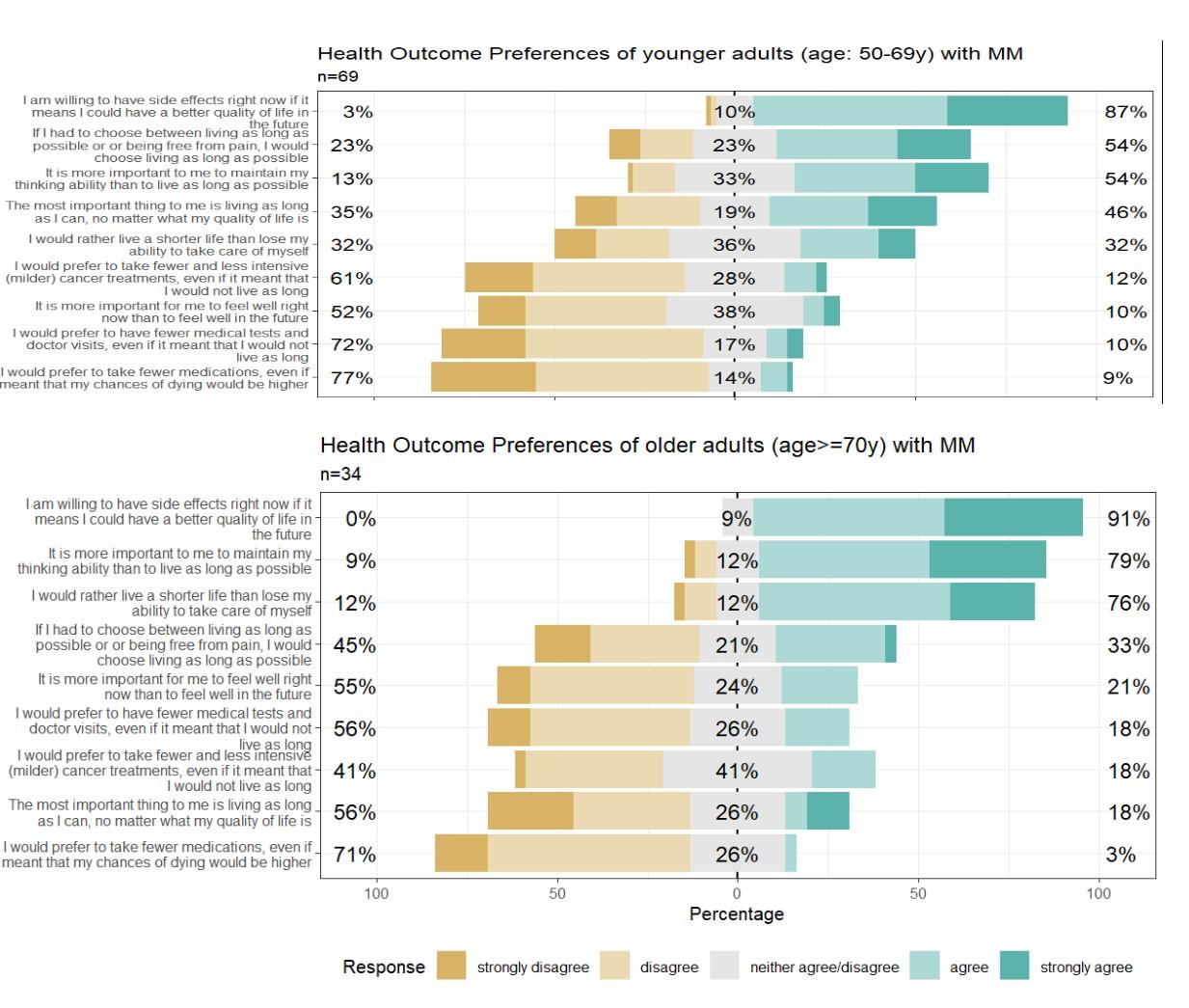
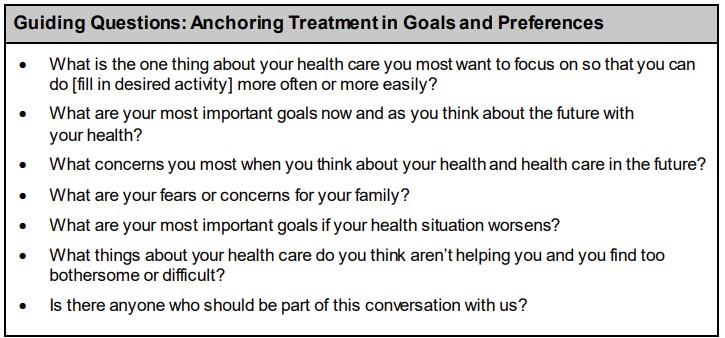
“What Matters to Older Adults? A Toolkit”

Many thanks for the opportunity to participate in this event!
• Slides from Friday & Saturday Programming
• Evaluations for Friday & Saturday Programming
• SparkCures Search Engine specific for the Florida region
• Ways to Give
• Slides from Friday & Saturday Programming
• Evaluations for Friday & Saturday Programming
• SparkCures Search Engine specific for the Florida region
• Ways to Give
March 28, 2026
Teresa S. Miceli
Mayo Clinic – Rochester, MN
Myeloma Basics NDMM Treatment
Living Well
Treatment Managing Symptoms .



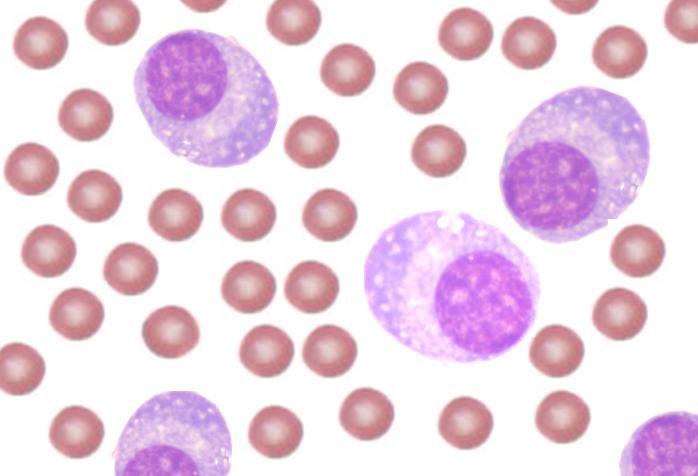
come from white blood cells produced in the bone marrow and make many different antibodies to help fight infection (polyclonal).
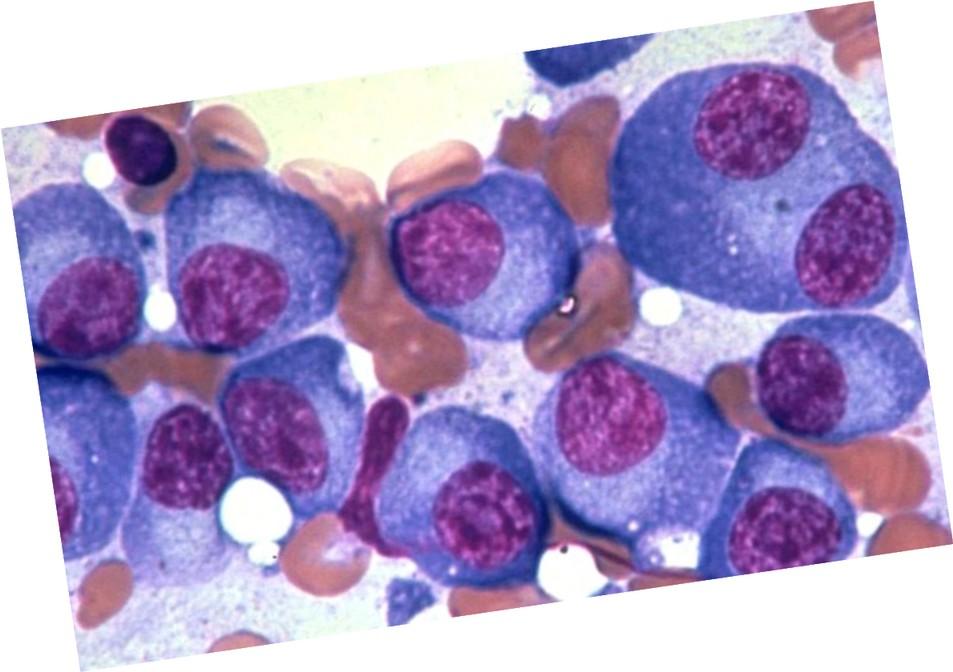
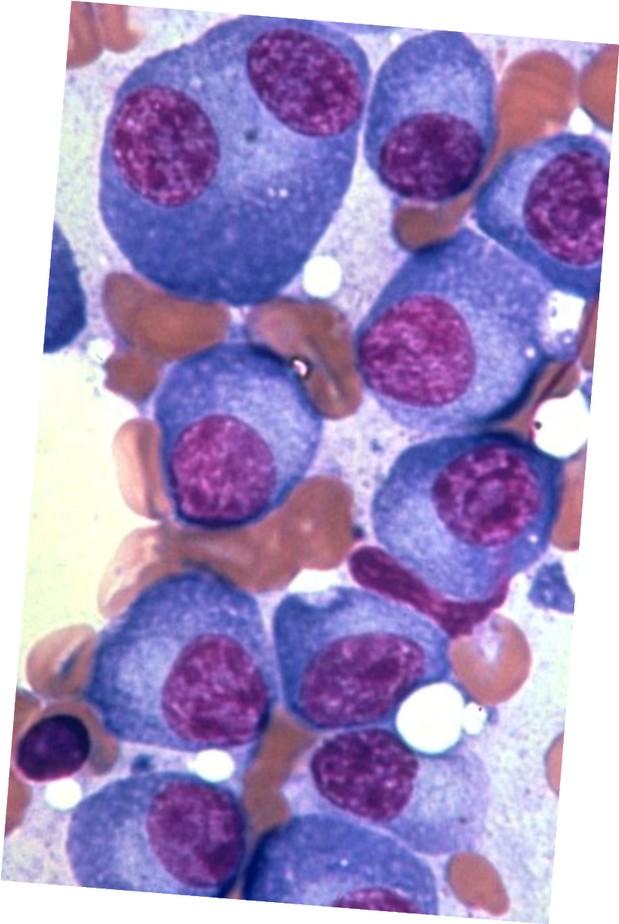
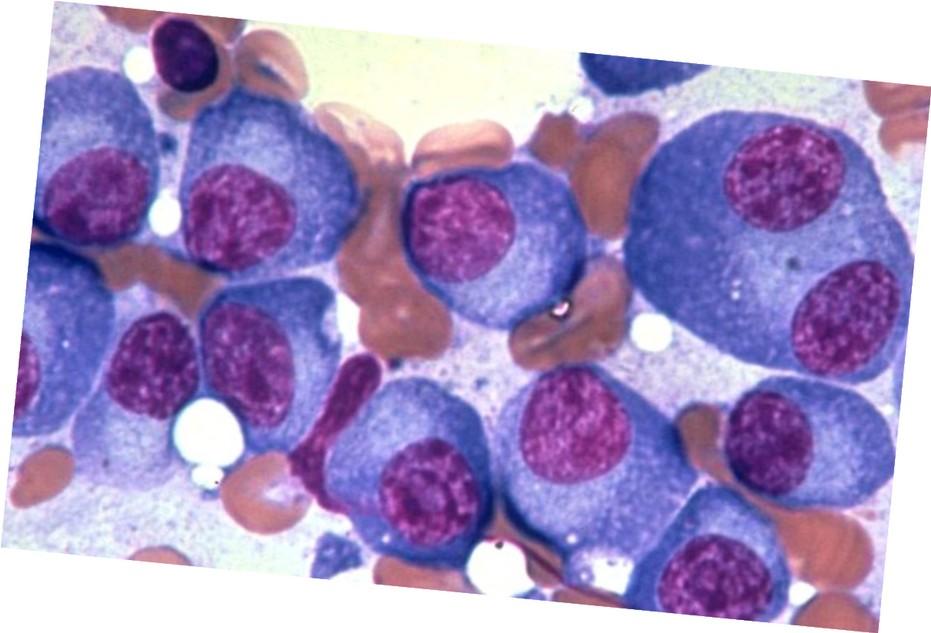
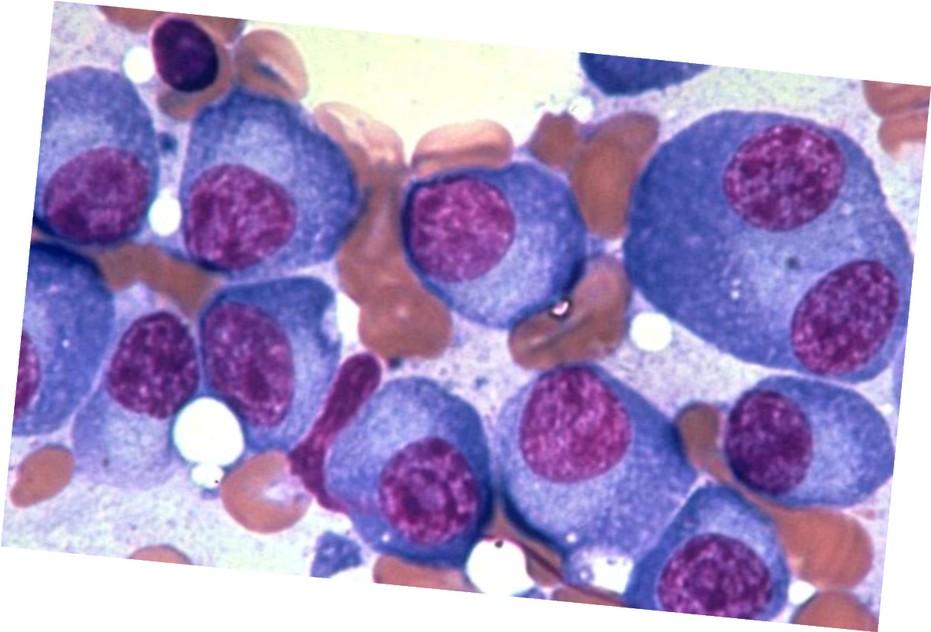
In Multiple Myeloma, one plasma cell mutates, making many identical plasma cells (monoclonal).





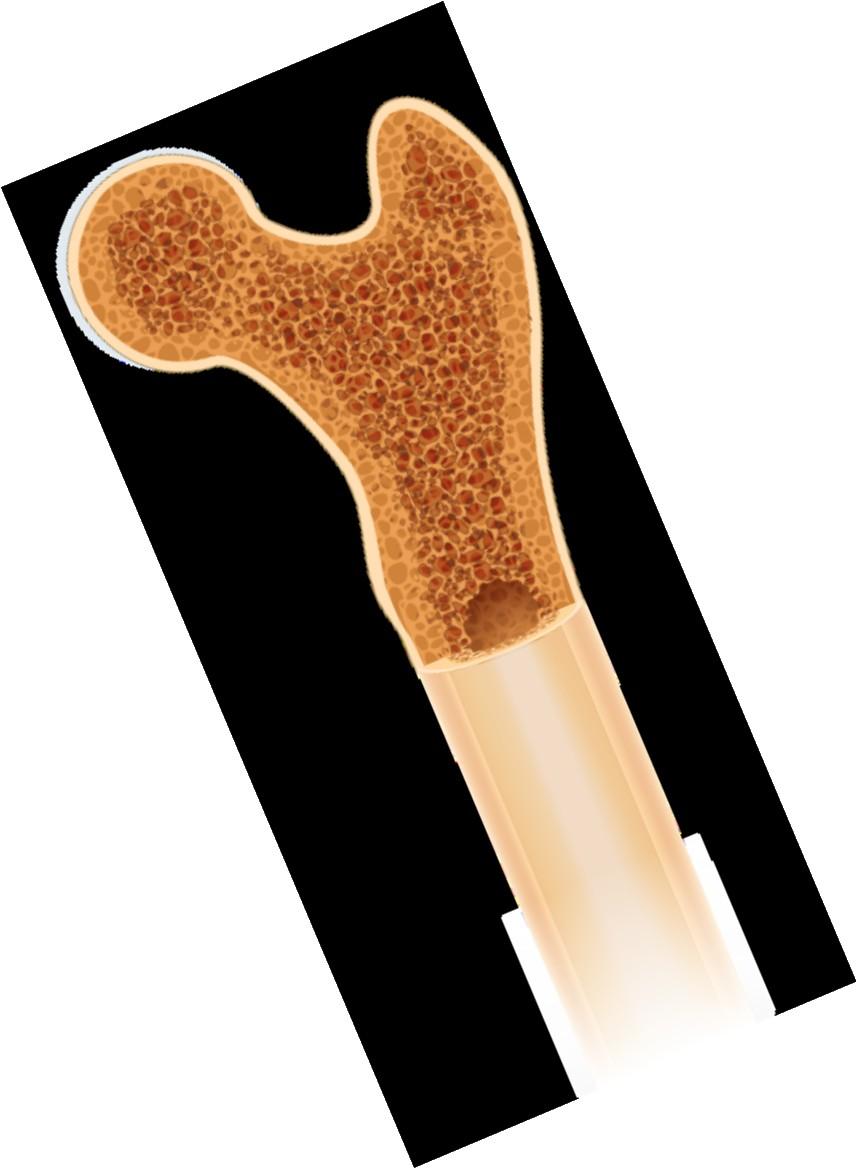
Bone marrow
Anxiety
Stress
Depression

Decreased red blood cells
Decreased white blood cells
Anemia & Fatigue
Immune Dysfunction & Infection
Myeloma protein in blood and urine
Changes in bone remodeling
Clonal myeloma plasma cells can cause many symptoms
• Crowd out normal bone marrow cells
• Produce myeloma protein
• Can cause kidney dysfunction
• Affect bone cells (balance of osteoclasts & osteoblasts)
Renal Dysfunction
Bone Damage


Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Environmental control
(avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
As recommended by your healthcare team:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
IMWG = International Myeloma Working Group; HCP = healthcare provider. Raje NS, et al. Lancet Haematol.2022;9(2):143–161. IMF Nurse Leadership Board ONS Symposia 2024.
Preventative and/or supportive medications

Myeloma Treatment
Stay hydrated--drink water
Avoid certain medications
• IV contrast dyes

• NSAIDs like Advil (ibuprofen), Aleve (naproxen)
Be alert: symptoms of kidney dysfunction
• Fatigue and weakness
• Nausea and vomiting
• Foamy or dark urine
• Swelling in feet, ankles, or face
• Shortness of breath
• Persistent itching
• Loss of appetite
• Muscle cramps
• High blood pressure

• Myeloma Treatment
• Nutrition
• Vitamin D
• Calcium (if approved by doctor)
• Weight-bearing activity (e.g., walking, standing, climbing stairs, stretching, dancing)
• Bone-strengthening agents (prescribed by your healthcare team)
Report any new or worsening bone pain to your healthcare provider
Pain can significantly compromise quality of life and add to distress.
Sources of pain include bone disease, neuropathy and medical procedures.
Prevention
• Decrease fracture risk through myeloma treatment, bone strengthening agents, physical activity, preventative surgery
• Prevent Nerve Damage: prevent shingles, manage diabetes, myeloma medication dosing and route of administration
• Combine scheduled medical procedures, when possible (Ex. blood draw, biopsy), use sedation if available
Interventions depend on source of pain, may include
• Medications, Surgery, Radiation therapy, etc.
• Physical therapy & continued activity, complementary therapies (Mind-body, meditation, yoga, supplements, acupuncture, etc.)
• Scrambler therapy for neuropathy
HR-SMM = high risk smoldering multiple myeloma; M-protein = monoclonal protein; MGUS = monoclonal gammopathy of undetermined significance; misc = miscellaneous (no dominant clone); MM = multiple myeloma; SMM = smoldering multiple myeloma.
Adapted from Durie B. Keats JJ, et al. Blood. 2012;120(5):1067-1076.
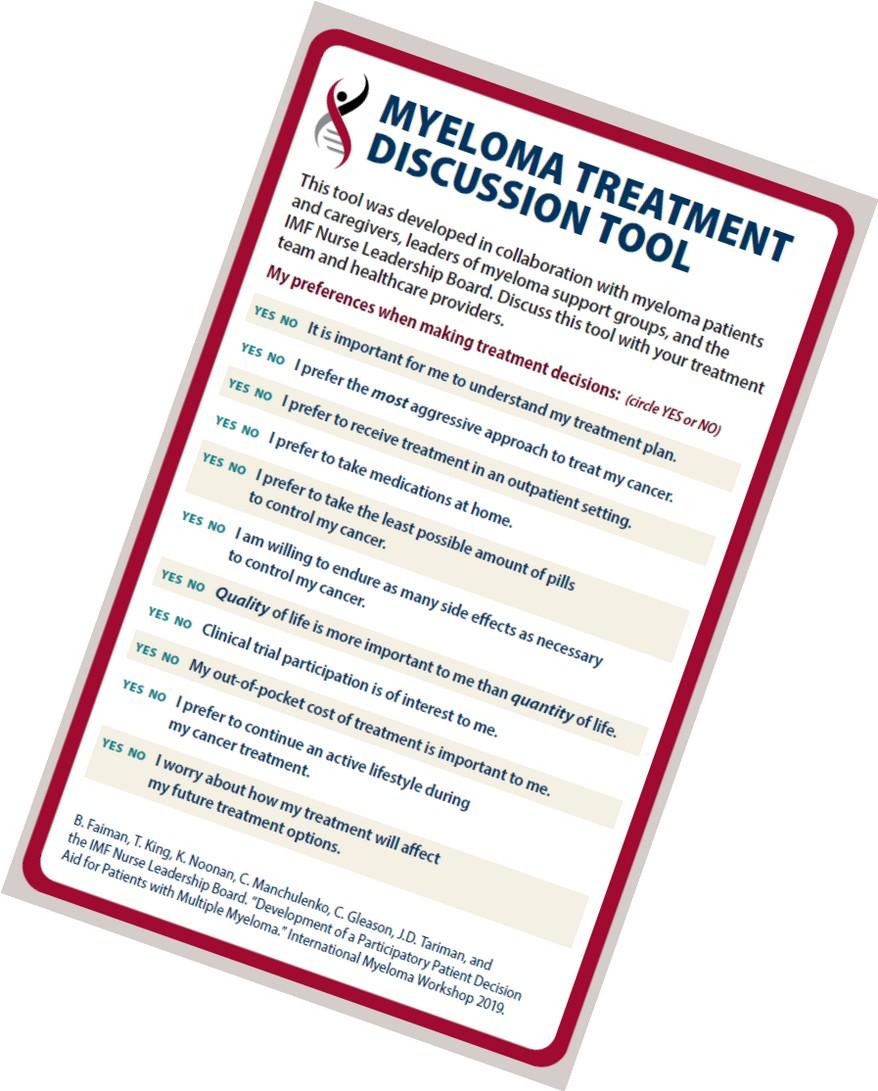
“The
aim of shared decision-making is to ensure that:
- Patients understand their options and the pros and cons of those options.
- Patient's goals and treatment preferences are used to guide decisions.”


The nature of multiple myeloma means patients and their care partners may have multiple points to make decisions about treatment
People with myeloma are living longer; goals, preferences, and values may change over time
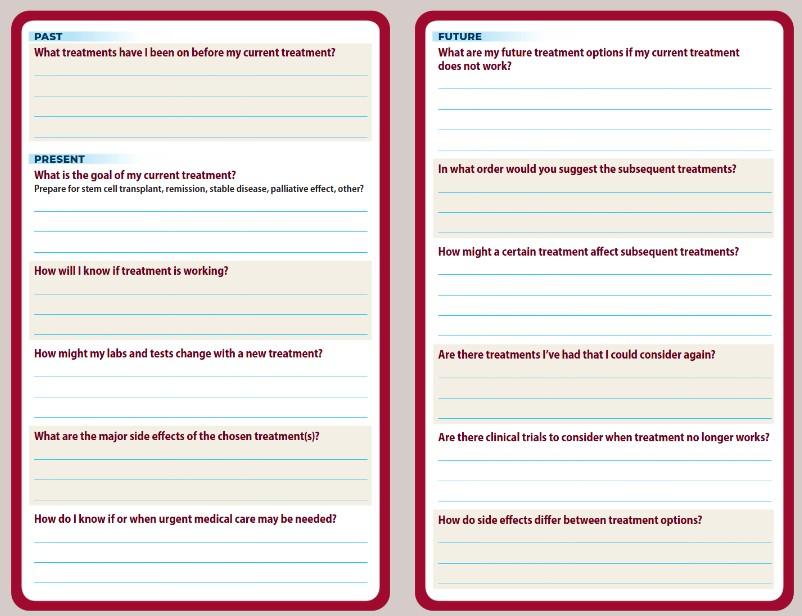
Ask questions (write them down in advance of visit)
• What are my treatment options?
• What are the pros and cons of each option? Efficacy? Side effects? Administration? Insurance nuances?
• Are there treatments that wouldn’t be a good option for me? Why?
Express your desire to participate in the treatment decisions
• I want to make sure the treatment we chose is the best option for me
• I want to be sure we a choosing the best therapy for my husband/wife
Ask for time (if needed/ appropriate)
• There is a lot to think about. Can I/we have some time to consider the options?
• Ask for information you can consider at home
• Note: if medical emergency/high risk, may not be appropriate
Understand options; consider priorities
• Use reliable sources of information like the IMF and Myelo
• Use caution when considering stories of personal experiences
• Consider your goals, values and preferences
Express your goals/values/preferences; create a dialog
Arrive at a treatment decision together; reevaluate over time
• My top priority is [goal/value]; additional [preferences] are also important.
• I think [treatment] may be a good choice given my priorities… What do you think?
• What treatment would you recommend given my goals and priorities?

• Be empowered to be part of decision-making
• Stay informed, understand options
• Use reliable and current sources of information
• Use caution considering stories of personal experiences
• Consider your priorities
• Discuss with your care partner
• Consider your goals/values/preferences
• Be a part of the conversation, create a dialog
• Ask questions & Express your goals/values/preferences
• Ask for time to consider options, if needed
• Arrive at a treatment decision together
• Arrange follow up to review and adjust, if needed
High potential to progress to active MM in 2 years
• M-spike ≥ 2 g/dL
• Free light chain assay (involved/uninvolved ratio ≥ 20)
• Bone marrow ≥ 20% clonal plasma cells
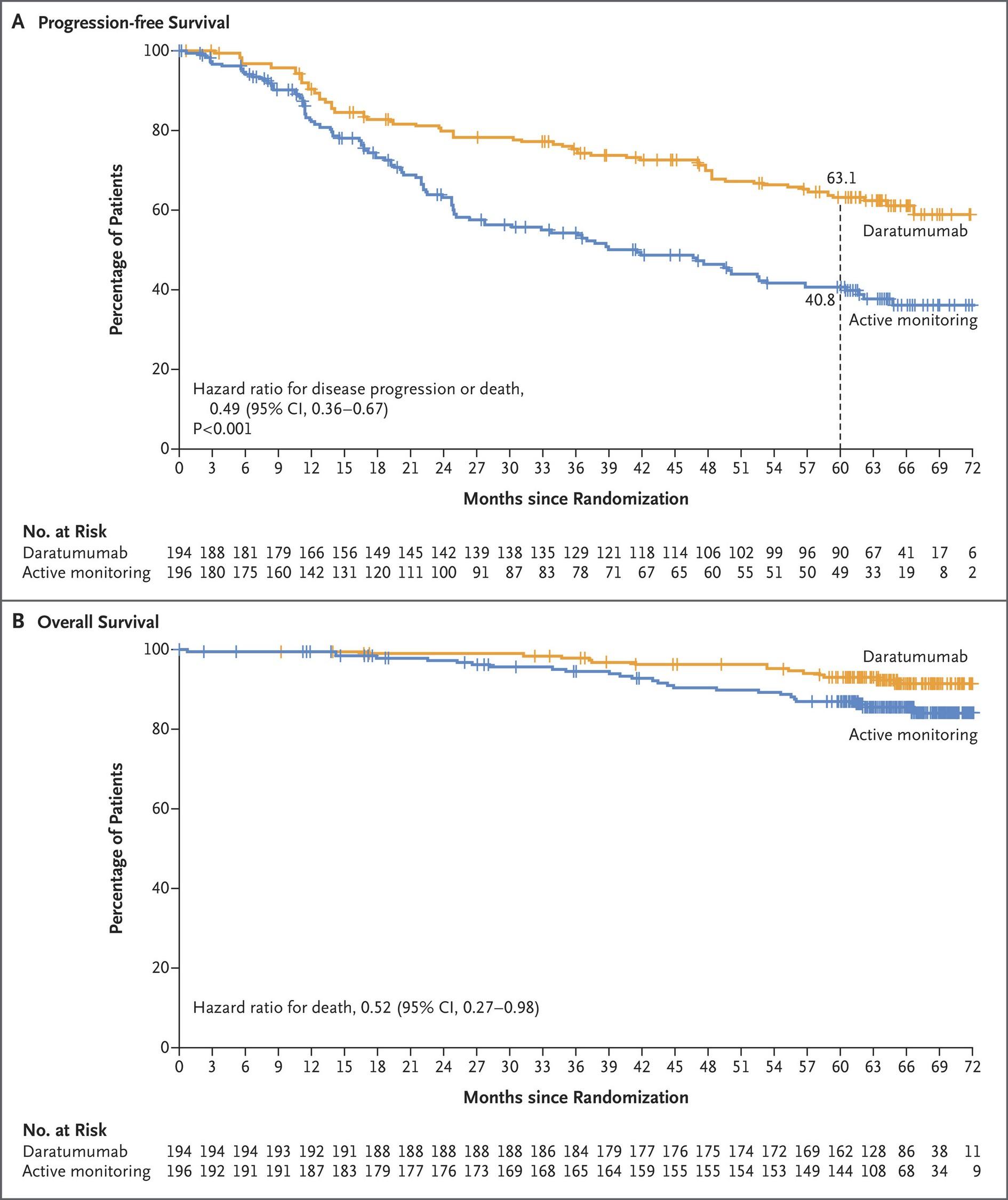
51% Reduction in risk of disease progression or death with Darzalex Faspro® treatment of high-risk SMM (compared with active monitoring)
FDA approved Nov2025
DARZALEX FASPRO® as monotherapy is indicated for the treatment of adult patients with high-risk smoldering multiple myeloma
FDA = US Food and Drug Administration; MM = multiple myeloma; SMM = smoldering multiple myeloma
Dimopoulous MA, et al. N Engl J Med. 2024;394(18):1777-1788. doi: 10.1056/NEJMoa2409029. Mateos, MV, et al. Blood Cancer J. 2020;10:102. (2020). https://doi.org/10.1038/s41408-020-00366-3 Use shared decision-making with your provider to determine if treatment is right for you.
Initial treatments aimed at reducing the amount of myeloma cells
Intensification of treatment to deepen response. Either additional cycles of induction or autologous stem cell transplant (in eligible patients)
Prolonged lower-intensity treatment designed to sustain remission
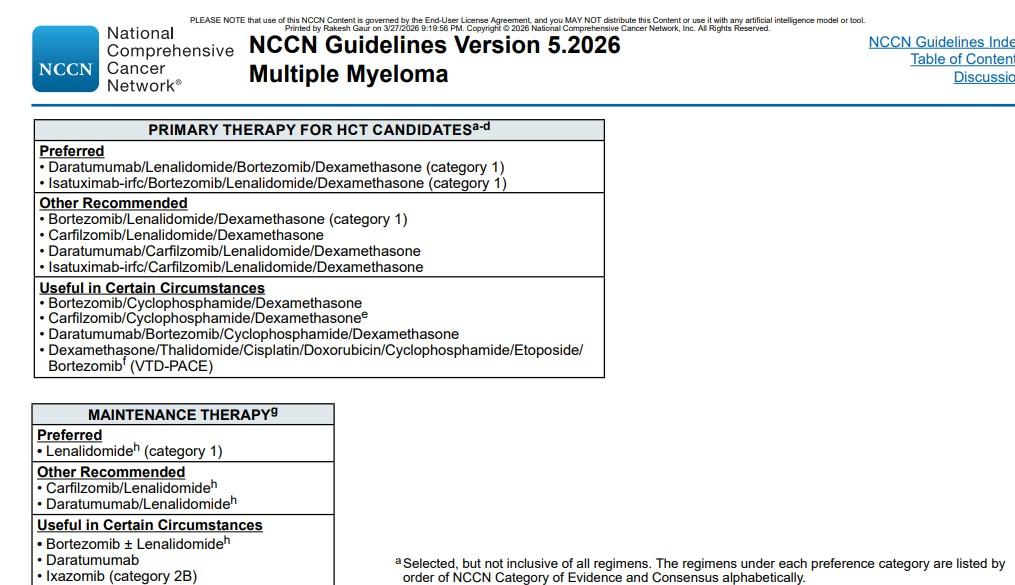
National Comprehensive Cancer Network® (NCCN®) NCCN Clinical Practice Guidelines In Oncology (NCCN Guidelines®) for Multiple Myeloma. Version 4.2026. To view the most recent or complete version of the guideline, go online to NCCN.org; Rajkumar et al, 2014. Rajkumar SV. Am J of hematology. 2022;97(8):1086–1107. https://doi.org/10.1002/ajh.26590; Faiman et al, 2016.

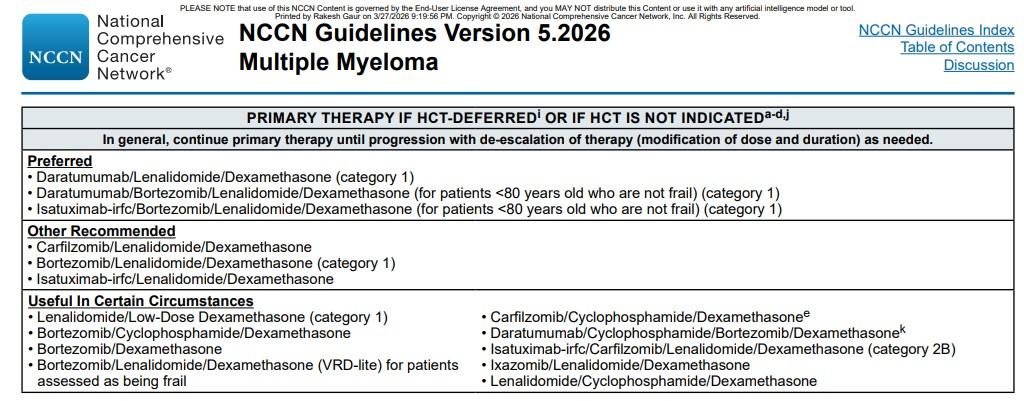
Quadruplet therapy is preferred for nearly all patients with newly diagnosed myeloma
1 2 3 4
Anti-CD38 monoclonal antibody (mAb)
• Darzalex (daratumumab)
• Sarclisa (isatuximab)
Proteosome Inhibitor (PI)
• Velcade (bortezomib)
• Kyprolis (carfilzomib)
At infusion clinic: subcutaneous injection or on body device or infusion
Supportive medication:
Immunomodulatory drug (IMiD)
Revlimid (lenalidomide)
• Pomalyst (pomalidomide)
• Prednisone
Oral medication taken at home
• Antiviral prophylaxis (i.e., acyclovir or valacyclovir) to prevent viral infections, particularly shingles.
• Antibacterial agents (i.e., Bactrim, levofloxacin) to prevent bacterial infections.
• Aspirin or other anticoagulant therapy to reduce the risk of blood clots from IMiDs.
• Bone-strengthening agents (i.e., zoledronic acid, denosumab) to strengthen bones and protect against fractures.
Steroids enhance the effectiveness of other myeloma therapies
Your provider may decrease or discontinue the dose as myeloma responds to therapy. Do not stop or alter your dose of steroids without discussing it with your provider
• Irritability, mood swings, depression
• Difficulty sleeping (insomnia), fatigue
• Blurred vision, cataracts
• Increased risk of infections, heart disease
• Muscle weakness, cramping
• Increased blood pressure, water retention
• Flushing/sweating
• Stomach bloating, hiccups, heartburn, ulcers, or gas
• Weight gain, hair thinning/loss, skin rashes
• Increased blood sugar levels, diabetes
• Consistent schedule (AM vs. PM)
• Take with food
• Stomach discomfort: Overthe-counter or prescription medications
• Medications to prevent shingles, thrush, or other infections
Rajkumar SV, et al. Lancet Oncol 11(1):29–37. King T, Faiman B. Clin J Oncol Nurs. 2017;21(2):240-249. Banerjee,R. et al. Blood 9.25.24
Symptoms:
Numbness
Tingling
Prickling sensations
Sensitivity to touch
Burning and/or cold
sensation
Muscle weakness
Peripheral neuropathy happens when there is damage to nerves in the extremities (hands, feet, limbs). Damage can be the result of myeloma, treatment or unrelated conditions (i.e., diabetes). Nerve
Prevention / management:
Bortezomib once-weekly and/or subcutaneous administration
Massage area with cocoa butter regularly
Neuroprotective Supplements
• i.e., B-complex vitamins (B1, B6, B12)
Safe environment: rugs, furnishings, shoes
If neuropathy worsens, your provider may:
Adjust your treatment plan
Prescribe oral or topical pain medication
Suggest physical therapy
HCPs may manage DVT/PE risk by
• Adjusting medications and schedules
Blood clots can cause swelling, pain, discoloration (DVT), shortness of breath, chest pain, sense of doom (PE). Blood clots are serious and can be life threatening.
• Prescribing blood-thinning medications according to assessed risk (DOAC, aspirin, warfarin, heparin)
• Balancing the risk of DVT and PE with that of bleeding with low platelets

Additional strategies to reduce risk of clots:
• Anti-embolism stockings (elastic stockings)
• Exercise regimen
• Moving frequently when sitting long periods
• Travel precautions (foot/leg exercises, walking, aspirin if not already on blood thinner)
You may be at risk:
• Family History
• Obesity
• Immobility
• Smoking
• Surgery
DOAC = direct oral anticoagulant; HCP = health care provider; DVT=deep vein thrombosis; PE=pulmonary embolism
Rome, S, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105. De Stefano, et al. Hematologica, 2022
ELGIBILITY
Location: Transplant Center P H A S E 1
Measuring treatment response Testing for Eligibility
Insurance authorization Collecting stem cells
Duration: Approximately 2 weeks
P H A S E 2
TRANSPLANT
HD-Melphalan Stem cell infusion Supportive Care
• GI Management
• Transfusions
• Antibiotics
Hair Loss Engraftment
Duration: Approx. 3-4
weeks Location: Transplant Center
Location: HOME P H A S E 3
Restrengthening Appetite recovery
“Day 100” assessment
Begin maintenance therapy
Duration: Approximately 1012 weeks
Stem cell transplant after induction remains the standard of care for eligible patients
Fluid intake can help with both diarrhea and constipation and helps kidney function
Constipation is more common in the induction phase
Opioid pain relievers, antidepressants, heart or blood pressure medications (check with provider, pharmacist)
Supplements: Calcium, Iron, vitamin D (rarely), vitamin B-12 deficiency
Increase fiber
Stay well hydrated
Fruits, vegetables, high fiber whole grain foods
Fiber binding agents – Metamucil® ,
Citrucel®, Benefiber®
Anorexia, the inability to eat, is common during transplant and resolves with time.
• Hydration is most important
• Small, frequent meals with a focus on protein intake
• You will work closely with a dietician to help monitor your calorie intake
Diarrhea is common during transplant and long-term maintenance therapy.
Other medications and supplements can cause GI issues.
Hydration is very important
Electrolyte replacement is common
Good skin care will help prevent irritation
Stool exam may be needed to rule-out infection
If no infection, anti-diarrheal medication may be prescribed
Discuss GI issues with healthcare providers to identify causes and adjust medications and supplements
Smith LC, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105.
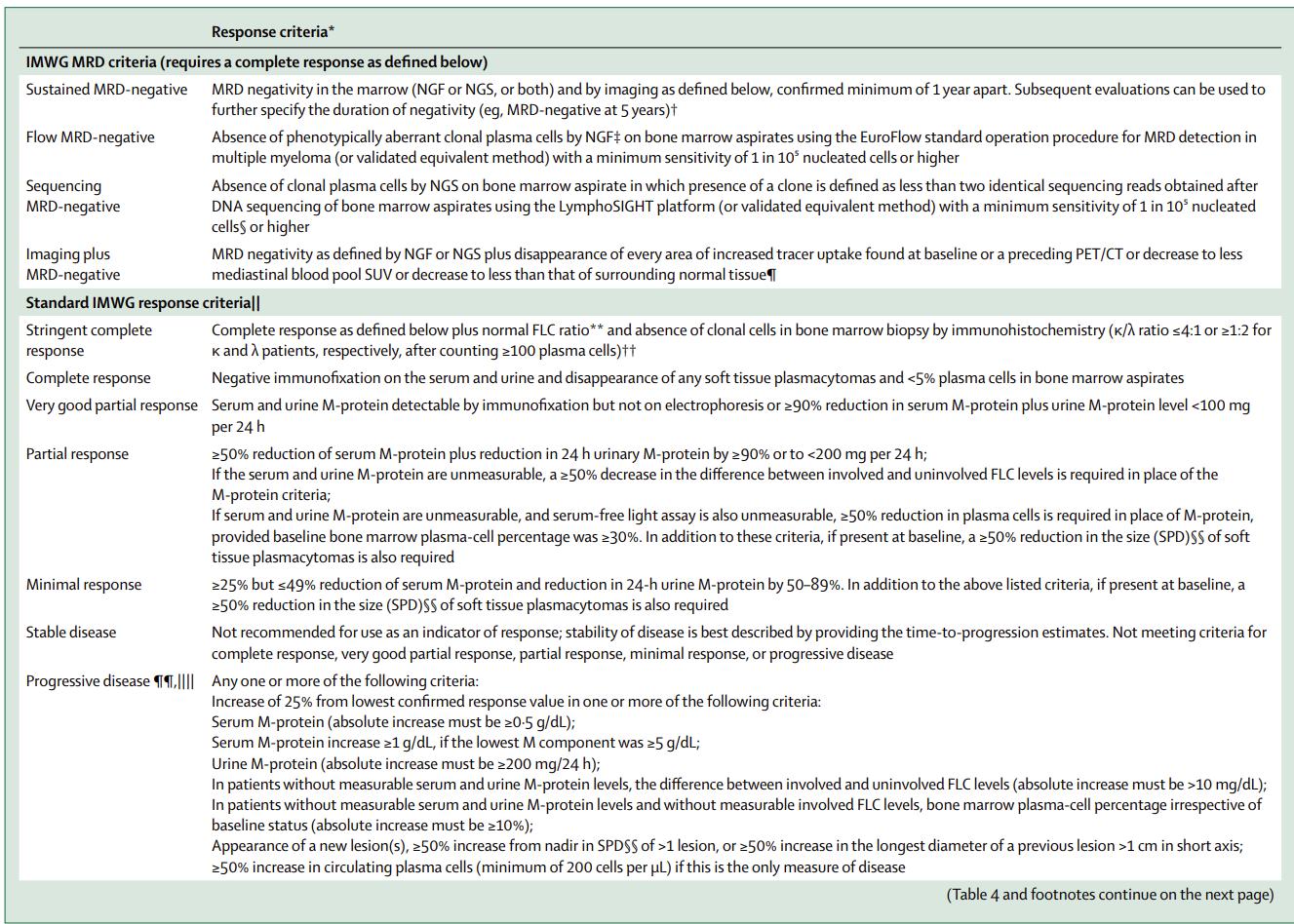
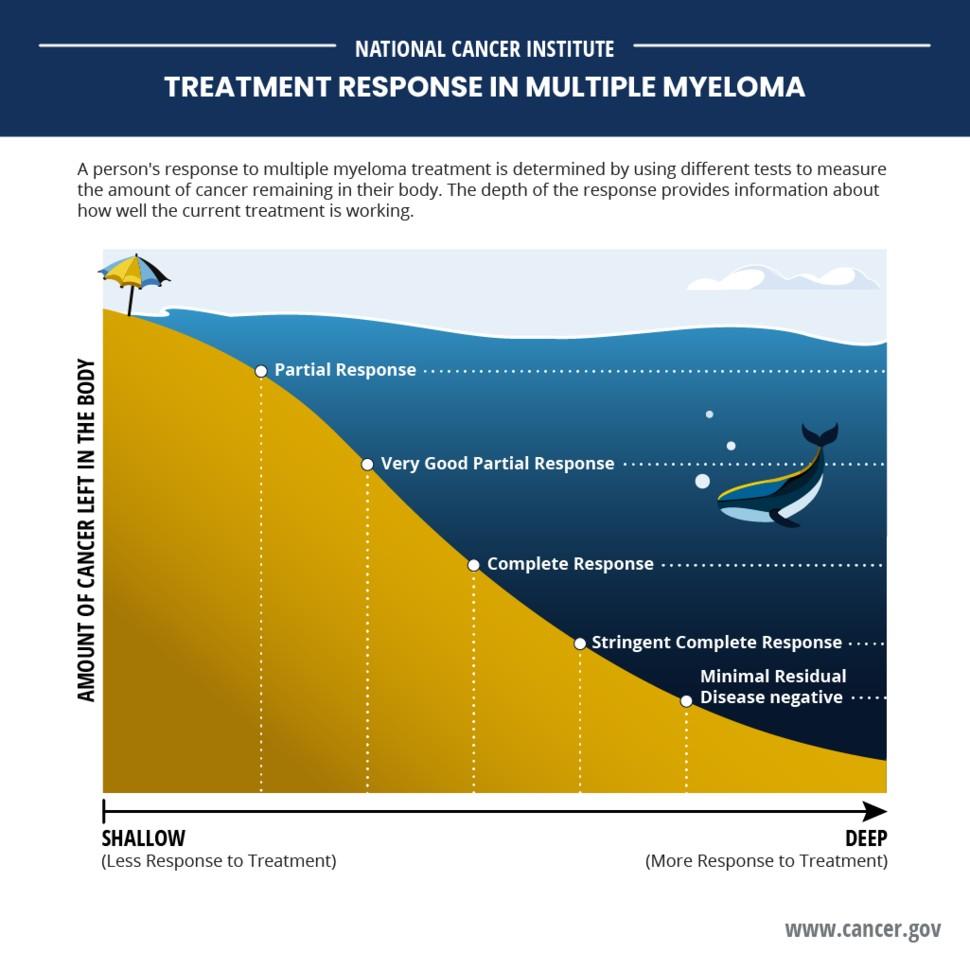
• Can provide information on how well treatment is working
• Is recommended after each treatment stage (e.g., after induction, consolidation, maintenance)
• Should be initiated only at the time of suspected complete response.
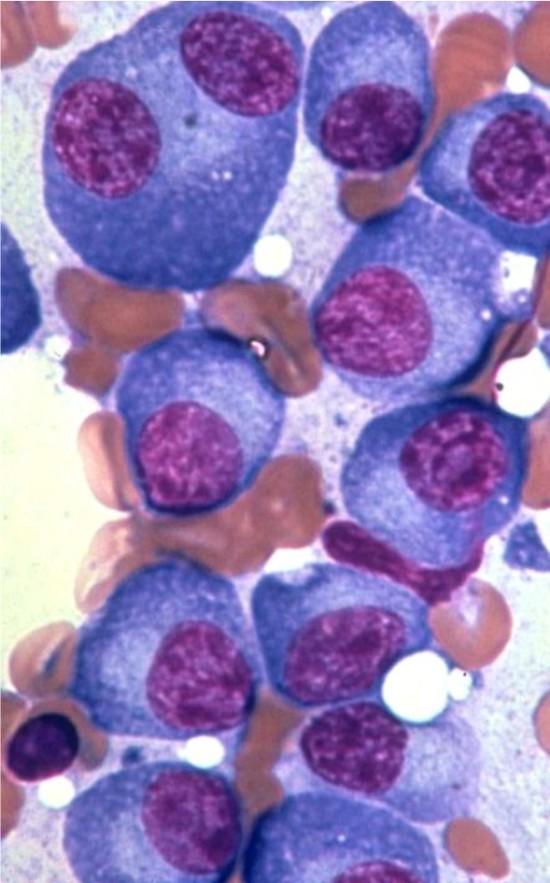
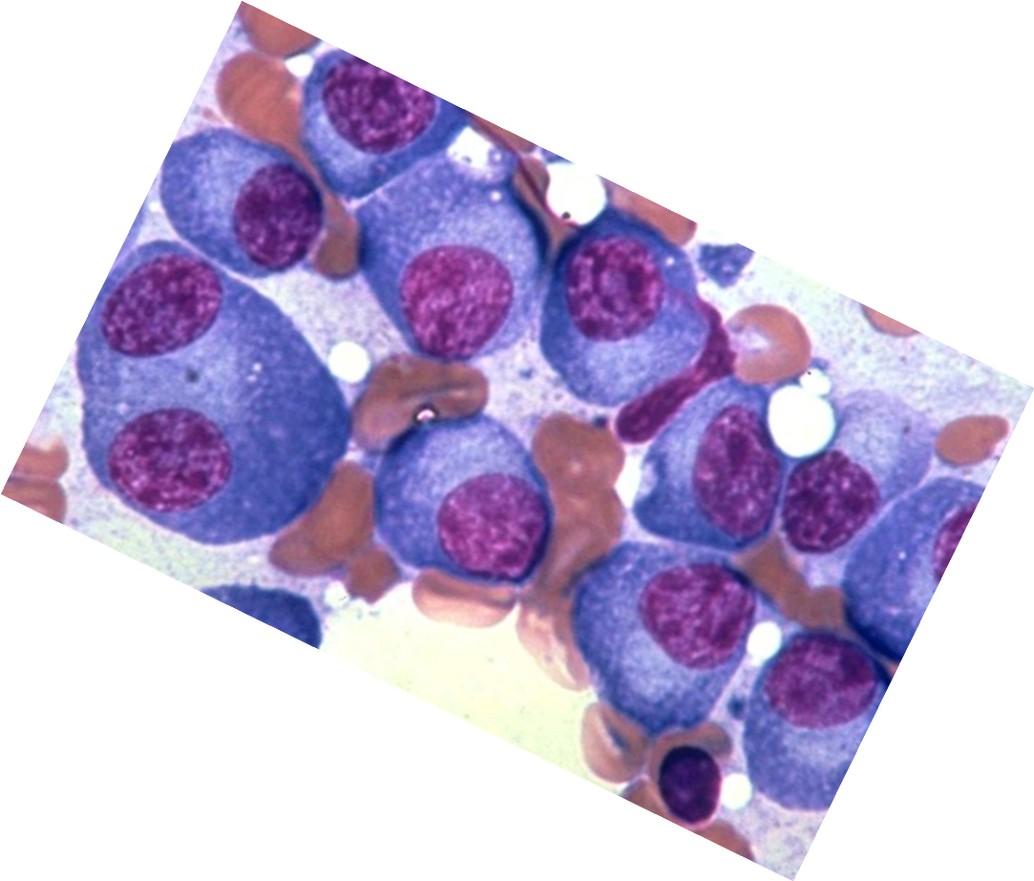
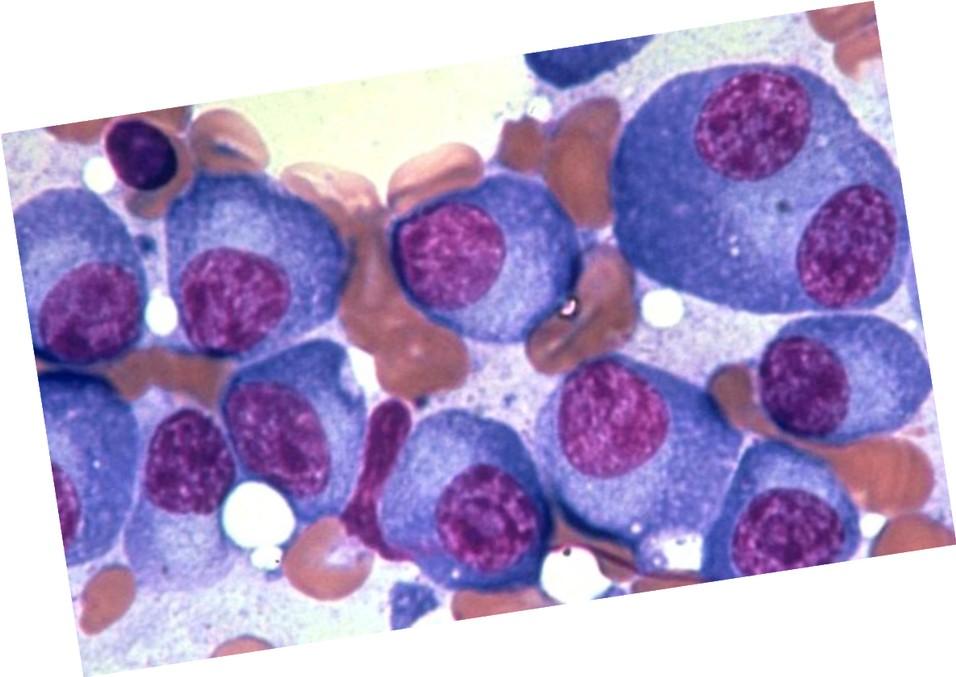
Myeloma cells (purple) crowd out normal bone marrow cells (peach)
No detectable myeloma protein <5% myeloma cells in bone marrow
MRD negative
10-5 = <1 myeloma cell in 100,000 10-6 = <1 myeloma cells in 1,000,000
Myeloma Therapy
Common Combinations or Therapy Names
Belantamab mafodotina BVd, BPd, BKRd
Bortezomib (SQ admin)
Carfilzomib
Car T-cell
Daratumumab
Elotuzumab
VRd, Vd, VCd
KRd, Kd, Dara-Kd, Isa-Kd
Cilta-Cel®, Ide-Cel®
Dara-Rd, Dara-Vd, Dara-Pd, Dara-VMp, Dara-Kd, Dara-Tecvayli®
ERd, EPda
Isatuximab Isa-Pda, Isa-Kd
Ixazomib IRd
Lenalidomide
Many therapy options are in the myeloma toolkit and more are being studied
VRd, Rd, KRd, Dara-Rd, ERd, IRd
Pomalidomidea Pda, Dara-Pd, EPda, PCdc
Selinexor
Xd, XVd, XKdc, Dara-Xdc
T cell Engager (Bispecific)b Elrexfio®, Lynozyfic™, Talvey®, Tecvayli
New agents or regimens in clinical trials may be an option

a2 or more prior therapies. b4 or more prior therapies. cOff-label; not currently FDA-approved.
C = cyclophosphamide; d = dexamethasone; Dara = daratumumab; FDA = US Food and Drug Administration; E = elotuzumab; Isa = isatuximab; I = ixazomib; K = carfilzomib; M = melphalan; p = prednisone; P = pomalidomide;
R = lenalidomide; SQ = subcutaneous; V = bortezomib; X = selinexor.
NCCN Guidelines®. Multiple Myeloma V4.2026. Accessed December 22, 2025.
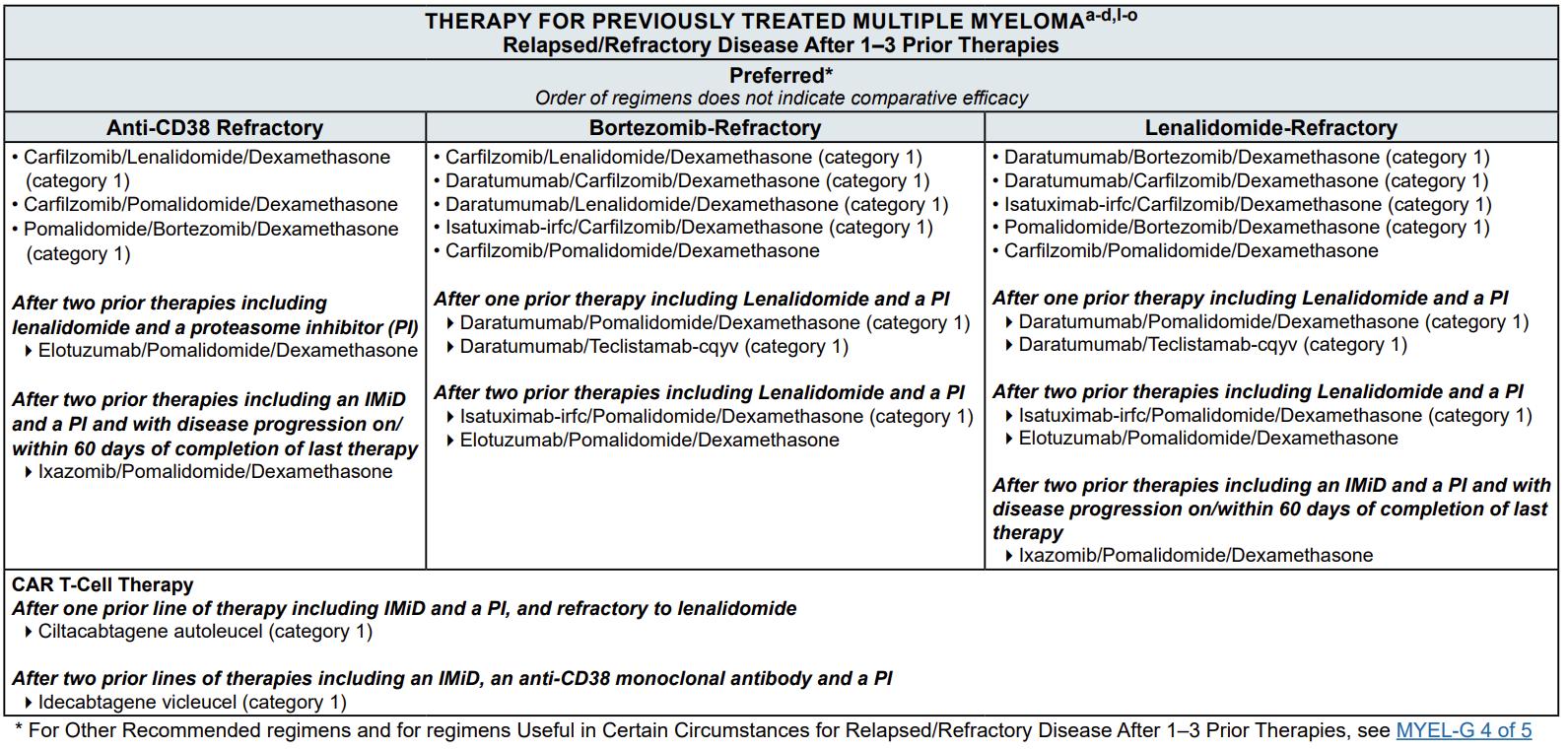
Relapsed MM with 1-2 prior LOT
BCMA target: potential for infection
• Abecma® (ide-cel)
• Carvykti® (cilta-cel)
• (anito-cel – pending FDA approval)
Bridging therapy, if needed; Lymphodepleting therapy when CAR T cells are ready T Cell Infusion Close monitoring and Management of side effects 1 3 4 5 HOME! Apheresis to Collect T Cells T Cell Manufacturing 2a 2b
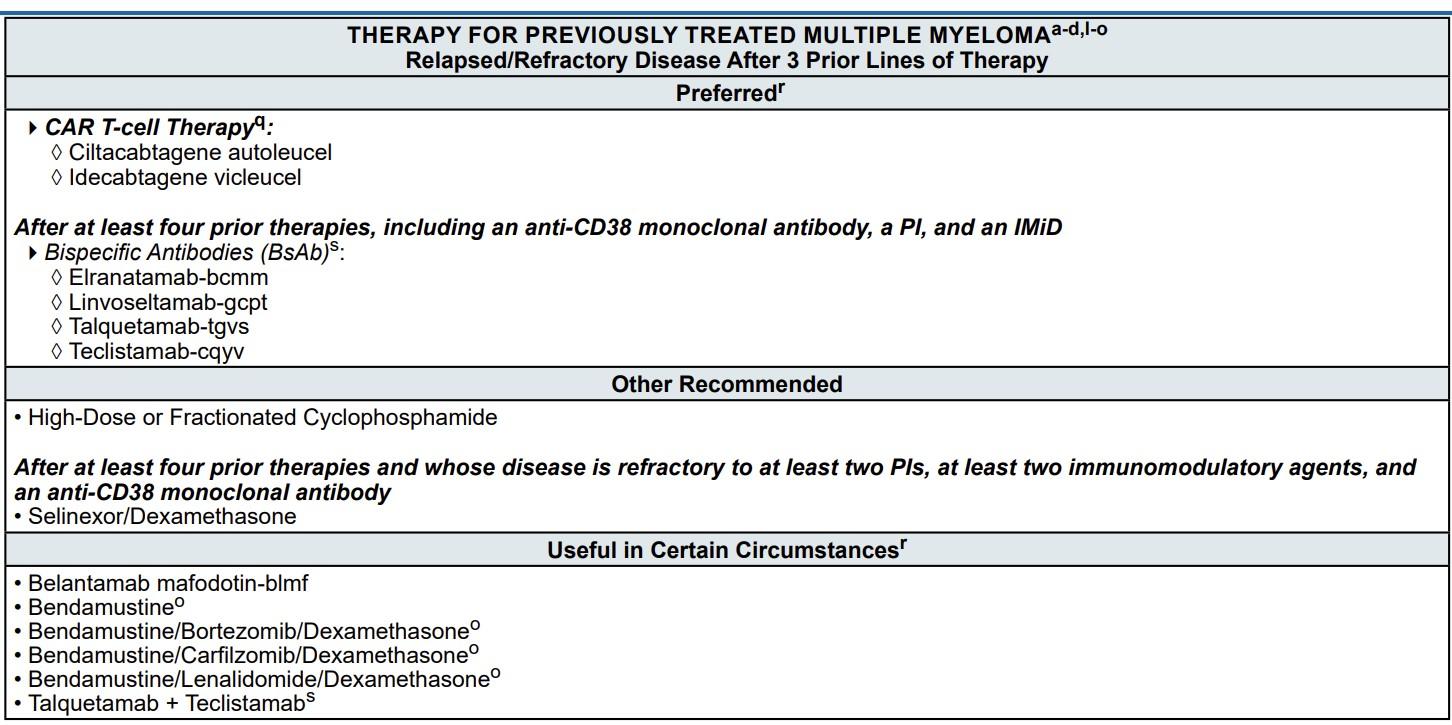
Relapsed MM after 4 prior LOT (or clinical trials)
TCE are innovative immunotherapies used in the treatment of relapsed multiple myeloma. These therapies work by redirecting the patient's own T-cells to recognize and attack myeloma cells.
Bispecific antibodies
• About 7 in 10 patients respond
• Off-the-shelf treatment; no waiting for engineering cells
BCMA target: potential for infection
• Tecvayli® (teclistamab)
• Elrexfio® (elranatamab)
• Lynozyfic™ (linvoseltamab)
Cytotoxic cytokines
Bispecific antibody T cell MM cell
GPRC5D target: potential for skin and nail side effects, GI issues of taste change, anorexia and weight loss
• Talvey® (talquetamab)
FcRH5 target: new myeloma target
• (cevostamab - pending FDA approval)

Target CD3


BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; GPRC5D = G protein–coupled receptor, class C, group 5, member D; CAR = Chimeric Antigen Receptor; LOT = Lines of Therapy; MM = multiple myeloma.
Shah N, et al. Leukemia. 2020;34(4):985-1005.
CYTOKINE RELEASE SYNDROME (CRS) ICANS AND NEUROTOXICITY
• Fever
• Fatigue & Weakness
• Headache
• Nausea/Vomiting/Diarrhea
• Chills
• Low blood pressure
• Rapid heart rate
• Difficulty breathing
CRS is a common but typically mild & manageable side effect
• Headache
• Difficulty concentrating
• Lethargy
• Agitation
• Hallucinations
• Tremors
• Confusion
• Memory loss
Neurotoxicit
PREVENTION AND MANAGEMENT of CRS
• Disease management to reduce tumor burden
• Bispecific Step-up Dosing (SUD)
• Tocilizumab
• Steroids
• Anti-Seizure medications
• Close monitoring
• Aphasia (difficulty with speech, reading, writing, or understanding language)
• Personality change
• Delayed Neurotoxicity can include Parkinsonism, Cranial Nerve Palsies and Peripheral Neuropathy/Guillan Barré syndrome (GBS)
CAR = chimeric antigen receptor. ICANS = Immune Effector Cell-Associated Neurotoxicity Syndrome Brudno JN, Kochenderfer JN. Blood. 2016;127(26):3321-3330. Lee DW, et al. Biol Blood Marrow Transplant. 2019;25:625638. Kumar, et al. Blood (2024) 144 (Supplement 1): 4758.
Type of Infection Risk
Medication Recommendation(s) for Healthcare Team Consideration
Viral: Herpes Simplex (HSV/VZV); CMV Acyclovir prophylaxis
Bacterial: blood, pneumonia, and urinary tract infection
PJP (P. jirovecii pneumonia)
Fungal infections
COVID-19 and Influenza
IgG < 400 mg/dL (general infection risk)
ANC < 1000 cells/μL (general infection risk)
Consider prophylaxis with levofloxacin
Consider prophylaxis with trimethoprim-sulfamethoxazole
Consider prophylaxis with fluconazole
Antiviral therapy if exposed or positive for covid per institution recommendations
IVIg recommended for patients receiving CAR T or TCE therapies
Consider GCSF 2 or 3 times/wk (or as frequently as needed) to maintain ANC > 1000 cells/μL and maintain treatment dose intensity
Some people receiving BCMA-targeting therapies have experienced infections that are less common like CMV, PJP and fungal infections
ANC = absolute neutrophil count; BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; CMV, cytomegalovirus; GCSF = granulocyte colony-stimulating factor; HSV = herpes simplex virus; IVIg = intravenous immunoglobulin;
PJP = Pneumocystis jirovecii pneumonia; VZV = varicella zoster virus.
Raje NS, et al. Lancet Haematol.2022;9(2):143–161.
Xerostomia
OTC dry mouth rinse, gel, spray are recommended. Avoid hot beverages. Anti-fungal therapy for oral thrush.
Dysgeusi a Dexamethasone oral solutions “swish and spit” may provide benefit. Sour citrus or candies before meals are also recommended.
Dysphagia
= Dry Mouth = Difficulty Swallowing = Taste Change
Dietary modifications with small bites, eating upright, and sips with food can help manage symptoms
Weight Monitoring
Some medications lead to weight gain, others to weight loss. Meet with a nutritionist
Consider diet changes, supplements
Dental Care
Attention to oral hygiene. Regular dental cleaning and evaluation. Close monitoring for ONJ, oral cancer and dental caries
Work closely with your entire health care team to manage oral side effects.
ONJ = Osteonecrosis of the Jaw; OTC = Over The Counter
Catamero D, Purcell K, Ray C, et al. Presented at the 20th International Myeloma Society (IMS) Annual Meeting Nurse Symposium; September 27–30, 2023; Athens, Greece.
Possible side effect to some treatments and supportive care medications

Skin Rash
Prevent dry skin; apply lotion
Report changes to your care team
Medication interruption or alternative, as needed
Steroids:
• Topical for grades 1-2,
• Systemic and topical for Grade 3
Antihistamines, as needed


Nail Changes

Keep your nails short and clean.
Watch for “catching and tearing”
Apply a heavy moisturizer like Vaseline or salve. Wear cotton hand coverings to bed
A nail hardener may help with thinning
Tell the team if you have signs of a fungal infection, like thickened or discolored nails
Fatigue is the most reported symptom. Sources include anemia, pain, reduced activity, insomnia, treatment toxicity, bone marrow suppression. Symptoms can improve with continued physical activity.
Symptoms are under-reported:
“I mentioned it before. Nothing can be done.”
“I don’t want to be put on another medication.”

• Mental health / social engagement
• Stress reduction; relaxation
• Sufficient Sleep
• Maintain a healthy weight; eat nutritiously
• Activity / exercise / prevent falls, injury
• Stop smoking
• Sexual health / intimacy
• Complementary or alternative therapy
• Socialize and Connect with others
Have a PCP for general check ups, preventative care, health screenings, vaccinations
Have specialists for dental care, eye exams/screening, skin cancer screening
Recommended Health Screenings
Blood pressure
Cholesterol
Cardiovascular disease Colonoscopy Dental checkups & cleaning
Dermatologic evaluation
Diabetes
Hepatitis
Hearing
Vision
Women specific: mammogram, pap smear
Men specific: prostate
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56.
Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.
Multiple studies demonstrate that strong social ties are associated with
• Increased longevity including people with cancer
• Improved adherence to medical treatment leading to improved health outcomes
• Lower risk of cardiovascular diseases
• Increased sense of purpose & life satisfaction
• Improved mood and happiness
• Reduced stress and anxiety
• Enhanced resilience
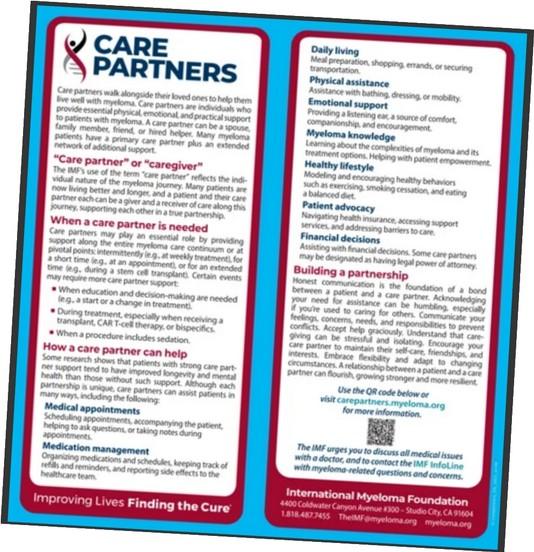
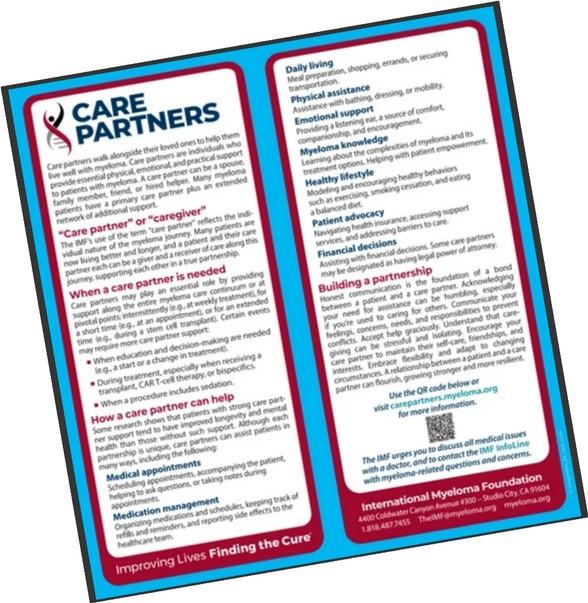
Care partners may help with medical appointments, managing medication, daily living, physical assistance, emotional support, myeloma knowledge, healthy lifestyle, patient advocacy, financial decisions
Caring for the care partner
• Recognize that caregiving is difficult and stressful
• Encourage care partners to maintain their health, interests, and friendships
• The IMF has information and resources to help care partners
Care partners can be a spouse, close relative, a network of people (family, friends, neighbors, church members, etc) IMF Tip Cards


“THANK YOU!”

February 28, 2026
Jim Weber



How did I miss that Putt?
There’s more than Red and White Blood cells?
Free light chains
Immunoglobulins – IGA, IGG, IGM
Immunotherapy
Football Season!
The DEX Rollercoaster Cycle
Physical Plan –
Food/Liquids/Exercise
Mental Plan – or Not
The Caregiver





Relapse Cancer Doesn’t Care about Inspirational Moments or Stories
Relapse was When the Real Marathon Began
Leverage the IMF and Others
Start Over

0.00000%




JENNIFER WIEWORKA, DNP, RN, OCN DIRECTOR, SUPPORT GROUPS, INTERNATIONAL MYELOMA FOUNDATION
IMF Support Group Directors




The International Myeloma Foundation Support Group Team presents this information to support learning and conversations with your healthcare team.
This presentation is for informational purposes only and is not intended to provide medical advice or replace guidance from your medical providers.

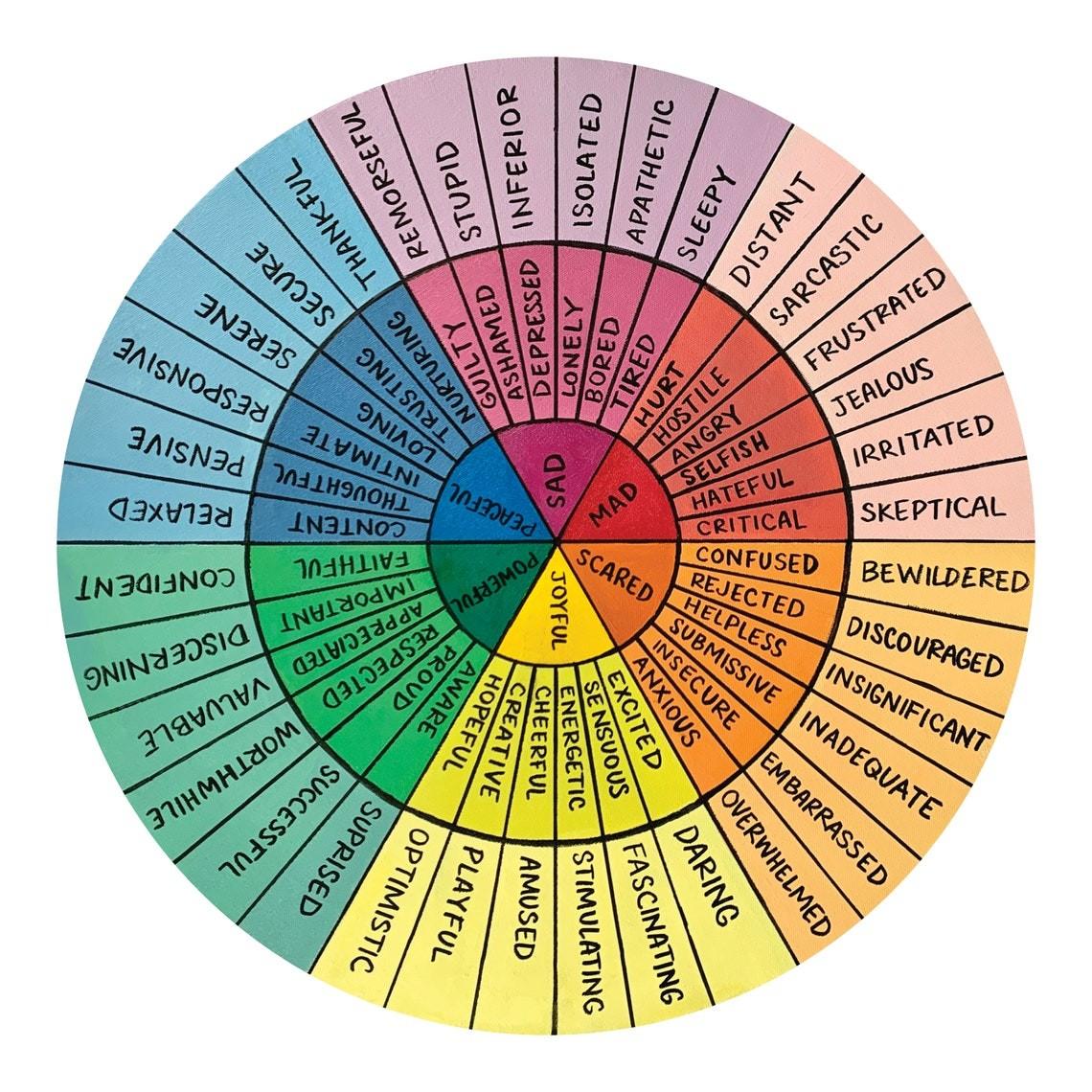
Common Emotional Responses
The Spectrum of Emotions
Coping with your Emotions
Grounding Exercises
When & Where to Seek Help
Wellness Tips & Resources for Support
Questions & Discussion
Myeloma is often seen through the lens of physical symptoms, treatments, and survival rates.


Beneath the surface of this medical battle lies a profound emotional journey that affects not only the person diagnosed but also their loved ones.

Getting a diagnosis of cancer can feel like getting the wind knocked out of you.
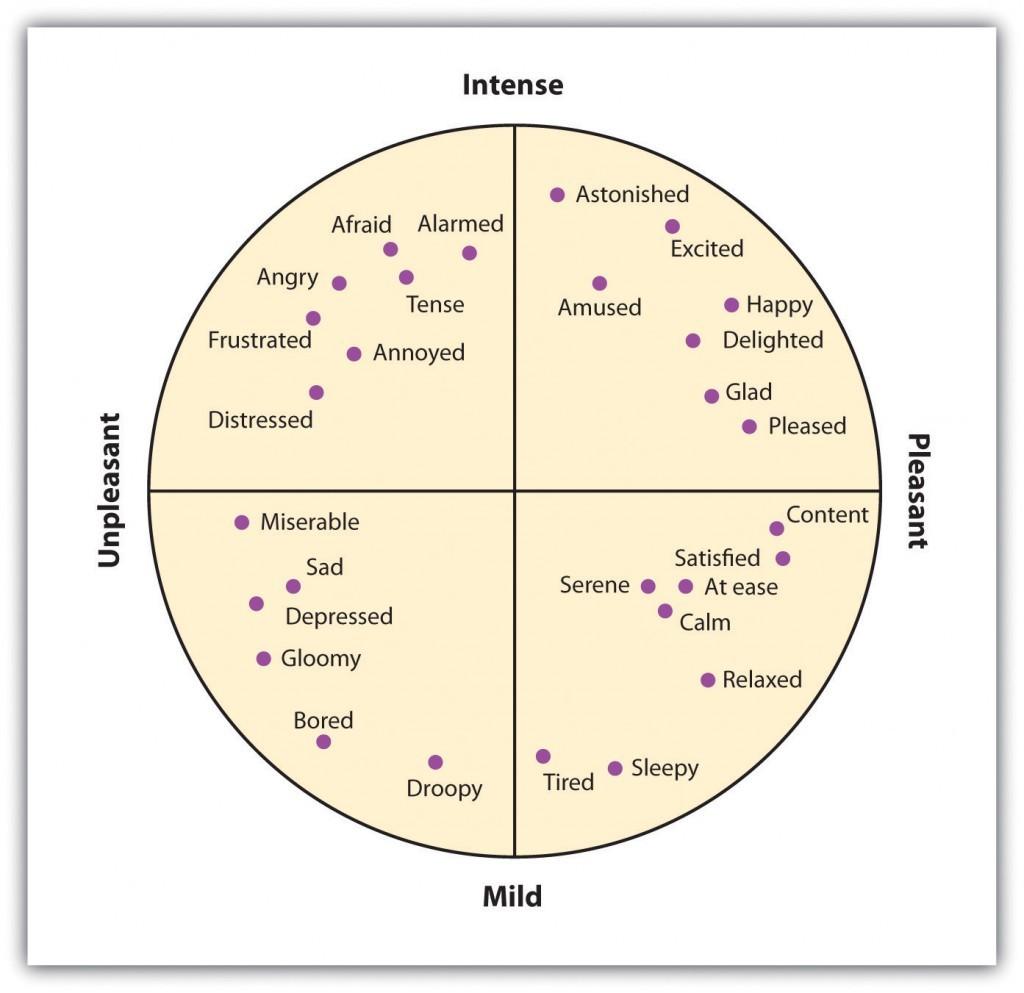
https://opentextbc.ca/introductiontopsychology/chapter/10-1-the-experience-of-emotion/
Some patients describe a feeling of numbness or surrealism after a cancer diagnosis; unable to fully grasp the weight of the news.
• Confusion
• Disconnection
• Denial

It is completely normal to experience anger towards:
• Doctors
• Healthcare team
• Yourself
• God
Patients describe many fears after a myeloma diagnosis, including:
• Fear of death and dying
• Fear of pain or treatment
• Fear of rejection/loneliness
• Fear about the future
• Practical worries (finances, housing, career, etc.)

• Side effects like fatigue, hair loss, nausea, and cognitive changes can strip away one’s sense of normalcy and identity.
• Some people feel isolated as they withdraw from social activities, work, or relationships due to physical limitations or emotional distress.
• The loss of independence and routine can be demoralizing and defeating.
• Cancer can significantly impact relationships with partners, family, friends, and coworkers.
• Some people may not know how to respond or offer support, leading to awkwardness, discomfort, or distance.
• Care partners can also experience emotional exhaustion, guilt, and helplessness as they witness their loved one's suffering.

Symptoms of anxiety include:
• ruminating about a specific fear
• sleep disturbance
• feeling restless or edgy
• irritability
• being easily fatigued or overstimulated
• difficulty concentrating or forgetfulness

Symptoms of depression include:
Sleep disturbance Loss of interest/pleasure in activities that used to feel exciting (anhedonia)
• Feelings of guilt or worthlessness
• Changes in energy or excessive fatigue
• Appetite/weight changes

• Psychomotor disturbance
• Suicidal thoughts
• Depressed mood
• In the US, 23.1% of the general population meet criteria for a diagnosis of a mental health disorder.
• Over 56% of patients living with blood cancers experience anxiety and depression
• This is never about suggesting the illness itself is “good” or that someone should suffer.
• Rather, it’s about recognizing that within extremely difficult or unwanted experiences, people sometimes discover forms of meaning, strength, connection, or clarity.
Research in psycho-oncology shows that post-traumatic growth is surprisingly common. People sometimes describe:
• A greater appreciation for life’s small moments
• New or deepened spiritual beliefs
• A sense of inner strength they didn’t know they had
• Increased empathy or patience

Suffering forces confrontation with vulnerability and uncertainty, and some individuals emerge with a transformed worldview.
• We may not yet have a cure for myeloma, and the reality is our physical bodies are never perfect, but we can experience emotional or spiritual healing in the midst of this journey.
• Consider for yourself what it would mean to engage in “healing.”

Cancer strips away control, but in that loss, people often find a different kind of agency:
• Choosing how to spend meaningful time
• Choosing how to speak about their experience
• Choosing how they meet uncertainty emotionally and spiritually

The struggle becomes a teacher of resilience and presence.
A powerful source of meaning comes from turning personal suffering into support for others:
• Advocating
• Volunteering
• Leading a support group
• Sharing one’s story

• Helping someone newly diagnosed
The idea of “I can use what I’ve been through” gives suffering a sense
of direction.
• Awareness
• Identify
• Accept
• Recognize
• Stay Curious
• Let go
Don’t feel that you have to be “strong.”
If you feel tired, lonely, anxious, depressed, angry, etc., acknowledge your feelings and talk about them. If all you want to do is cry, then go ahead.
“The work of the mature person is to carry grief in one hand and gratitude in the other and to be stretched large by them.
How much sorrow can I hold? That’s how much gratitude I can give. If I carry only grief, I’ll bend toward cynicism and despair. If I have only gratitude, I’ll become saccharine and won’t develop much compassion for other people’s suffering.
Grief keeps the heart fluid and soft, which helps make compassion possible.”

-Francis Ward Weller

5-4-3-2-1 Grounding Exercise
The “Butterfly Hug” or other bilateral stimulation exercises
Mindful Walking
4 Square breathing Categories (i.e. Colors, college football teams, etc.)
Aromatherapy
Hold a piece of ice

Eat a small bite of food with intention and mindfulness
Think about what you need. Lots of people will want to help but don’t know how.
• Practical needs
• Financial help
• Emotional support

Your mental health is as important as your physical health!
Tell your healthcare team or another medical professional if you need support.
Ask if your hematology/oncology clinic employs a clinical social worker or counselor. Emotional support and therapy services are available at many clinics.

• Included
• Welcomed
• Connected
• Accepted
• Involved
• Supported
• Heard
• Valued
• Seen
• Hopeful

Talk to friends and family, and others you trust
Ask for help and be specific about what you need

Join a support group

Get education and information only from reliable/reputable sources
Take time for yourself
Spend time with supportive friends
Celebrate every victory!
Talk with your doctor to determine what plan of action works best for you. Medications could potentially be part of a treatment plan that you and your doctor work on together.
If you think therapy/counseling could be beneficial, ask for a referral or check out websites/platforms such as:
• Headway
• Better Help
• Talkspace
• CaringBridge
• Psychology Today


• Slides from Friday & Saturday Programming
• Evaluations for Friday & Saturday Programming
• SparkCures Search Engine specific for the Florida region
• Ways to Give
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease.


• Slides from Friday & Saturday Programming
• Evaluations for Friday & Saturday Programming
• SparkCures Search Engine specific for the Florida region
• Ways to Give