2026 IMF PATIENT AND FAMILY SEMINAR
BOCA RATON, FL

MARCH 13 & 14, 2026












MARCH 13 & 14, 2026
• Slides from Friday & Saturday Programming
• Evaluations for Friday & Saturday Programming
• SparkCures Search Engine specific for the Florida region
• Ways to Give


The International Myeloma Foundation is the global leader in multiple myeloma

OUR MISSION:
To improve the quality of life of myeloma patients while working toward prevention & a cure

OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease

Together, we are turning hope into action: one meeting, one conversation, one connection at a time.

We are an Empowered, Engaged, and Educated CoMMunity!

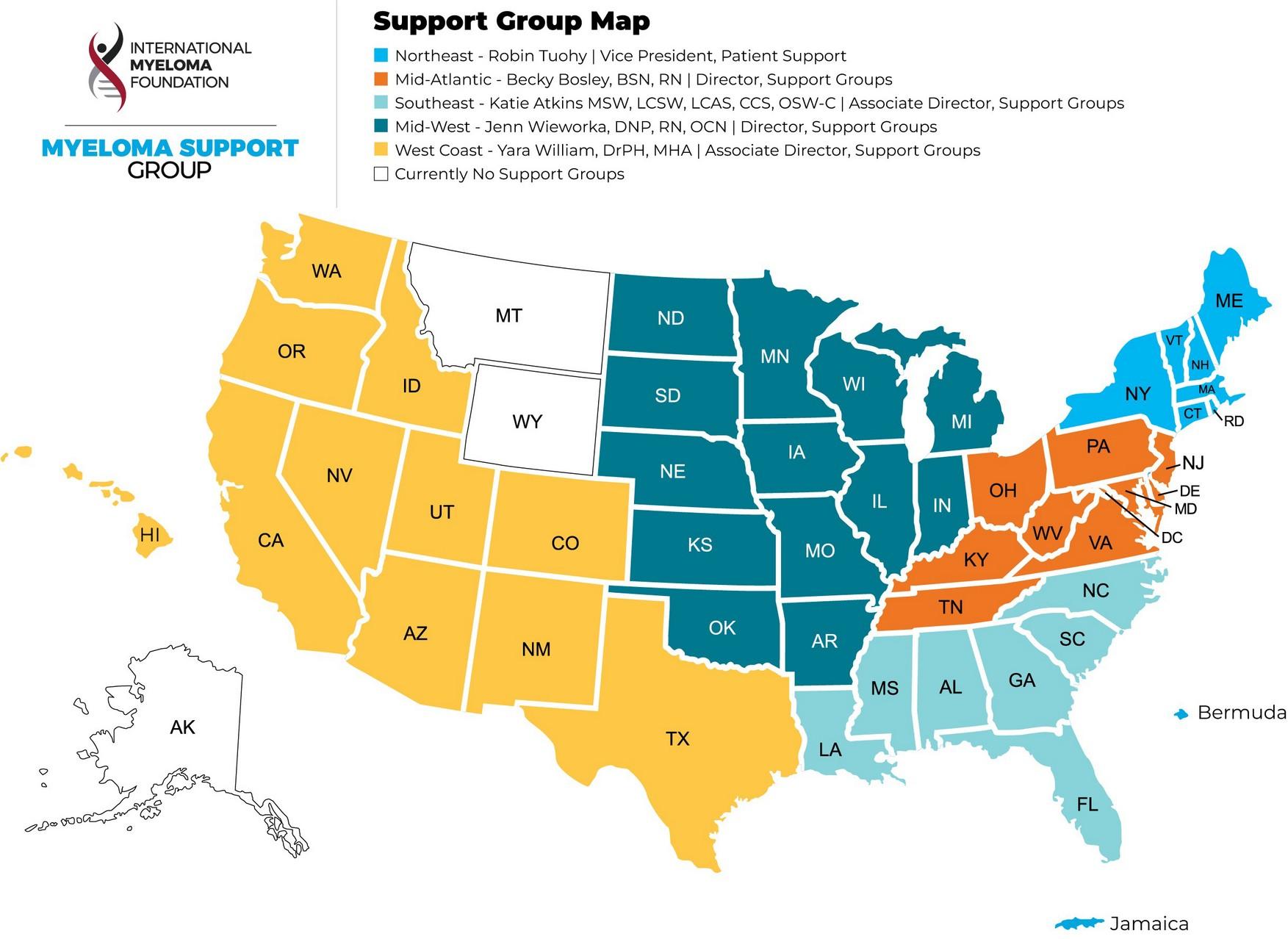
Support Groups empower patients & care partners with information, insight & hope
The IMF provides educational support to a network of over 155 myeloma specific groups


Special interest groups are designed as a supplemental support for specific populations of patients, in addition to their local Support Groups
MM Families
Founded in 2021
For patients & care partners with young children
Las Voces de Mieloma
Founded in 2022
For Spanish speaking patients & care partners
Living Solo & Strong
Founded in 2022
For patients without a care partner
Veterans SIG
Founded in 2025
For those who served our country

MM in the Middle
Founded in 2026
For those diagnosed before age 50
Smolder Bolder
Founded in 2023
For smoldering myeloma patients & care partners
Living with High-Risk Multiple Myeloma
Founded in 2023
For high-risk myeloma patients & care partners
Care Partners Only
Founded in 2024
For myeloma care partners only
Stronger Together: The IMF’s Commitment
The Myeloma Treatment Landscape
Guided Member Roundtable
Myeloma.org website walkthrough
ASH/ASCO Research Updates

Emotional Health: The Unseen Impact of Myeloma
Understanding Clinical Trials
Hope and Healing When the Future Is Uncertain

Palliative Care & Hospice
Emergency Planning




• Boca Raton, FL – March 13 – 14
• Cleveland, OH – May 1 – 2
• Los Angeles, CA – August 14 – 15
• Short Hills, NJ – October 2 – 3

Myeloma Community Workshops
• Kansas City, MO – March 28
• Virtual – April 20 – Newly Diagnosed
• Minneapolis, MN – April 25
• Detroit, MI – June 27
• Salt Lake City, UT – August 1
• Virtual – August 24 - Relapsed • Portland, OR – September 19
San Diego, CA – October 24 • Phoenix, AZ – November 14
Virtual – November 16

This year’s theme, #MoreThanMyeloma, reminds us that every patient is more than their diagnosis. And together, we will make the world take notice by lighting landmarks red across the globe.
Help shine a light on multiple myeloma by asking your city to light up a local landmark in red this March. From bridges and buildings to monuments and city halls, every illuminated landmark sparks curiosity and inspires conversation.


Videos, Webinars, Podcasts,







Understanding Booklets
Tip Cards
Myeloma Minute
Weekly Updates

Myeloma Today
Quarterly News





IMF President & CEO

“I am humbled to serve alongside so many who are making a difference every day for patients and families affected by myeloma, and I look forward to building on the IMF’s legacy of impact”
HEATHER COOPER
PRESIDENT & CEO
Continuing education programs
Clinical updates and consensus guidance
Workshops and global symposia

Tools to improve early recognition across specialties

Collaborative global initiatives accelerating prevention and cure


The Scientific Advisory Board (SAB) provides strategic scientific guidance and identifies emerging research priorities
The SAB helps shape and oversee major IMF research initiatives
The International Myeloma Working Group (IMWG), a global network of more than 300 myeloma researchers, collaborates to develop consensus guidelines, research standards, and landmark publications
The Black Swan Research Initiative (BSRI) drives innovative research aimed at achieving a cure for myeloma
Together, these programs foster global collaboration and accelerate scientific discovery

Result: Coordinated international leadership advancing prevention, better treatments, and a cure for myeloma.

Provide independent scientific guidance to the International Myeloma Foundation
Identify emerging scientific opportunities and research priorities
Advise on strategy for major IMF research initiatives & review and guide research programs and grant funding
Help translate scientific discoveries into improved patient outcomes
Provide scientific leadership for global collaborations including the International Myeloma Working Group and the Black Swan Research Initiative
Through the SAB’s leadership, the IMF accelerates global collaboration and scientific innovation aimed at preventing and curing myeloma.

Global network of leading myeloma investigators
Develops consensus diagnostic criteria and guidelines
Advances understanding of precursor conditions
Shapes international standards of care


IMF’s bold initiative focused on achieving cure
Emphasis on measurable residual disease (MRD)
Precision medicine and immune-based strategies
Multi-institutional collaborative trials


Regional research collaboration across Asia Expands clinical trial access Enhances physician education
Strengthens global data sharing


Regional clinical and research collaboration
Improves access to modern therapies
Supports culturally responsive education Advances equitable care delivery

• Considering ways to expand our education & support programs
• Responding to your needs
• Creation of linguistic & culturally appropriate programs and materials
•
Goal: More ways to help people living with myeloma and their care partners have better quality of life
I want to hear from you!
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease.


Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO Chief Medical Officer, International Myeloma Foundation
Carl Ola Landgren, MD, PhD University of Miami
WHEN YOU RETURN FROM BREAK PLEASE HEAD TO YOUR
SELECTED
BREAKOUT SESSION:
BREAKOUT A: NEWLY DIAGNOSED: FRONTLINE THERAPY
Please move to Royal Palm
BREAKOUT B: MANAGING RELAPSED MYELOMA
Please remain in this room
Melissa Alsina,MD
Moffitt Cancer Center
Tampa, Fl
1Einsele H. Moving CAR-T into first-line therapy in Multiple Myeloma. Physician session #PS08-1. Presented at: 6th European CAR Tcell Meeting; Feb 17, 2024; Valencia, ES.
Residual cells-even in deep remission undetectable cancer cells can remain
Treatment Resistance- over time myeloma cells adapt and become resistant to therapy
High risk genetics- high risk genetic markers can make the disease more aggressive and more likely to return
Immune system dysfunction- a weakened immune system can fail to keep myeloma cells in check
• Listen to your body
• Regular follow up with your
• oncologist/ myeloma doctor
• Know your myeloma
• Be your own advocate!!









Negative by next generation flow (NGF) (minimum sensitivity 1 in 10-5 nucleated cells or higher)*
mCR AND normal Free Light Chain ratio, Bone Marrow negative by flow, 2 measures
CR AND negative PCR
Complete Response: Negative immunofixation (IFE); no more than 5% plasma cells in BM; 2 measures
Very Good Partial Response: 90% reduction in myeloma protein
Partial Response: at least 50% reduction in myeloma protein
Minimal Response
Stable Disease: Not meeting above criteria
Progressive Disease: At least 25% increase in identified myeloma protein from lowest level
MRD = Minimal Residual Disease sCR = Stringent Complete Response; BM = Bone Marrow
Key – when myeloma relapses, it “overcomes” the current therapy being used, so it is necessary to change the approach to the
disease with a new a
mechanism of action
Discuss clinical trials !!-may give you an opportunity to have early access to potential better and or safer treatment
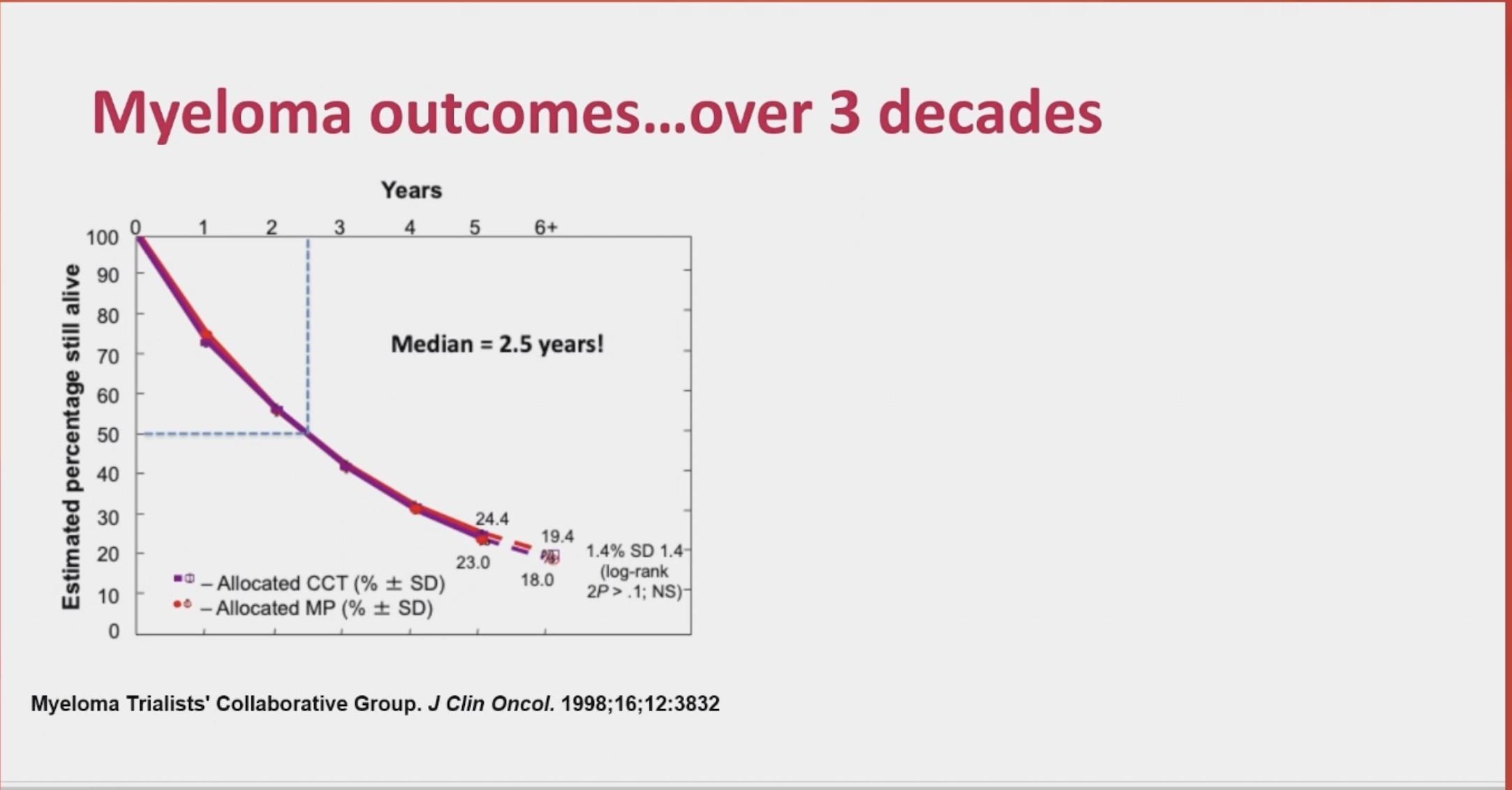
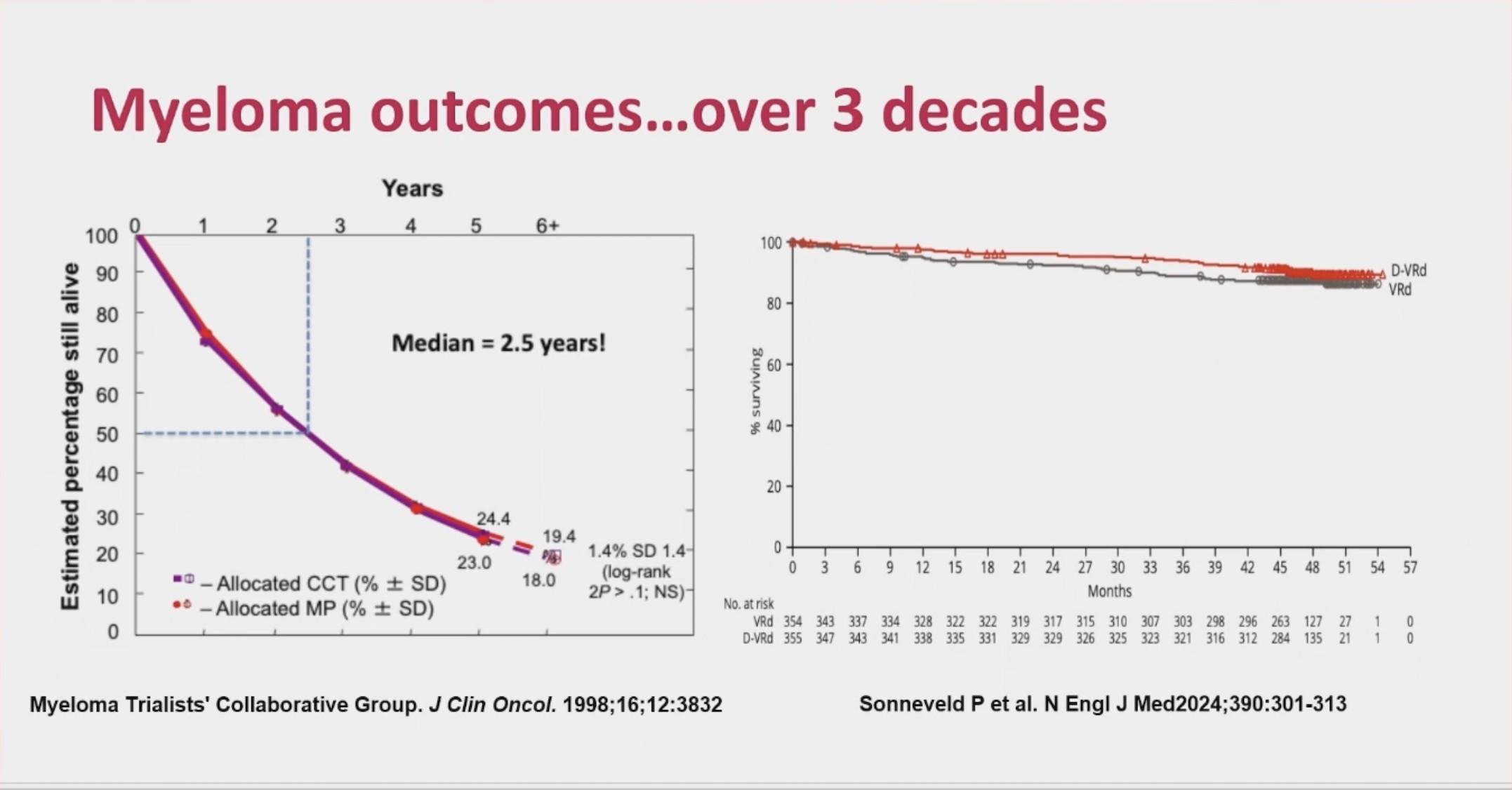
Typically the most durable remissions occur earlier in the disease course
So, we want to use the best possible therapies before the disease becomes more resistant
Therapies tend to have a greater effect earlier in the disease course...
As will be discussed today, options for relapsed myeloma have grown and these three approaches have the best outcomes
This has to be balanced with patient characteristics and preferences – so other options (like doublets) can be considered
NEW – the combination of Teclistamab and Daratumumab was approved in March 2026
• Renal insufficiency
• Hepatic impairment
• Comorbidities
• Preferences
• Social factors
– Support system
– Accessibility to treatment center
– Insurance coverage
• Previous therapies
• Prior treatment-related adverse event(s)
Disease Treatment Patient
• Nature of relapse
– Biochemical vs symptomatic
• Risk stratification
– High-risk chromosomal abnormalities: del(17p), t(4;14), t(14;16)
• Disease burden
• Regimen-related toxicity
• Depth and duration of previous response
MRD refers to the persistence of residual tumor cells after treatment and is responsible for relapse1
Current techniques can detect MRD with a sensitivity of 10-6 for MM cells2
MR→PR→ VGPR→CR →sCR
1. Adapted from Hauwel M, Matthes T. Swiss Med Wkly 2014:144:w13907
2. Biran N, et al. Curr Hematol Malig Rep 2014;9:368–78

We are still learning what is the “optimal” sequence of therapies but it is clear there is no “optimal” sequence as so many variables influence choice
But a few lessons are being learned:
1. In general if a patient is CAR T eligible, it is preferred prior to bispecific antibodies
2. All therapies can be sequenced in any order but it can reduce its efficacy – T cells in particular may need a ”rest”
We do not treat myeloma, but PEOPLE! How it affects your life and your preferences is critical and should be considered...
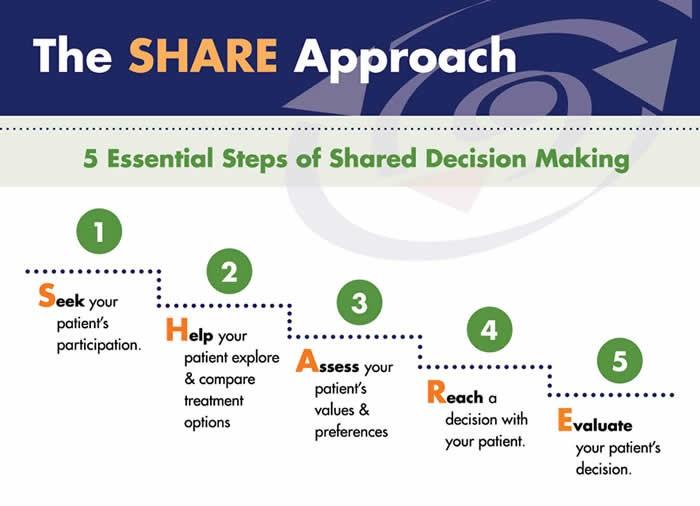
“The aim of shared decision making is to ensure that:
- Patients understand their options and the pros and cons of those options.
- Patient's goals and treatment preferences are used to guide decisions.”


• Slides from Friday & Saturday Programming
• Evaluations for Friday & Saturday Programming
• SparkCures Search Engine specific for the Florida region
• Ways to Give
Kevin Brigle, PhD, ANP
Massey Comprehensive Cancer Center, Virginia Commonwealth University
March 14, 2026
Kevin Brigle, PhD, ANP
Massey Comprehensive Cancer Center
Virginia Commonwealth University


Kevin Brigle, PhD, ANP





Myeloma’ s
Terrain
In Multiple Myeloma, one plasma cell mutates, making many identical plasma cells (monoclonal).
Cells come from white blood cells produced in the bone marrow and make many different antibodies to help fight infection (polyclonal).
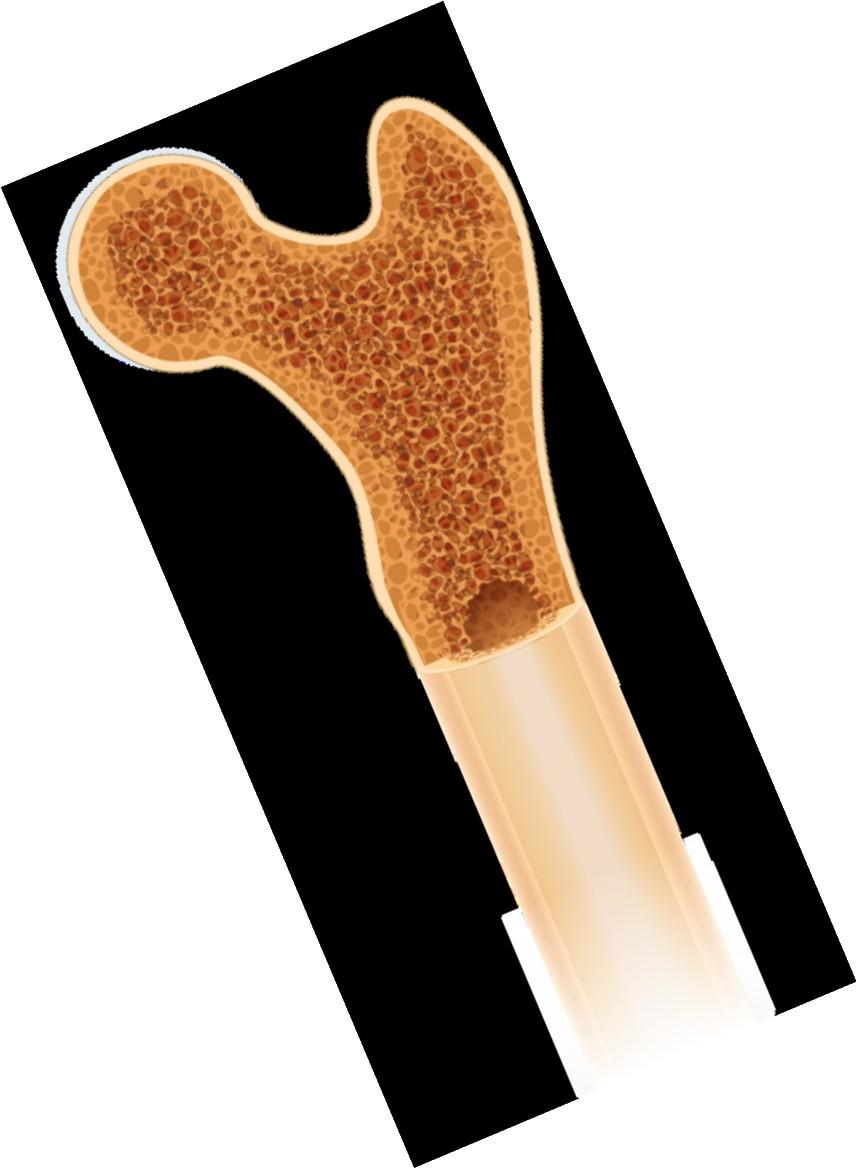





Myeloma’
Terrain
Bone marrow
Anxiety
Stress
Depression

Decreased red blood cells
Decreased white blood cells
Myeloma protein in blood and urine
Changes in bone remodeling
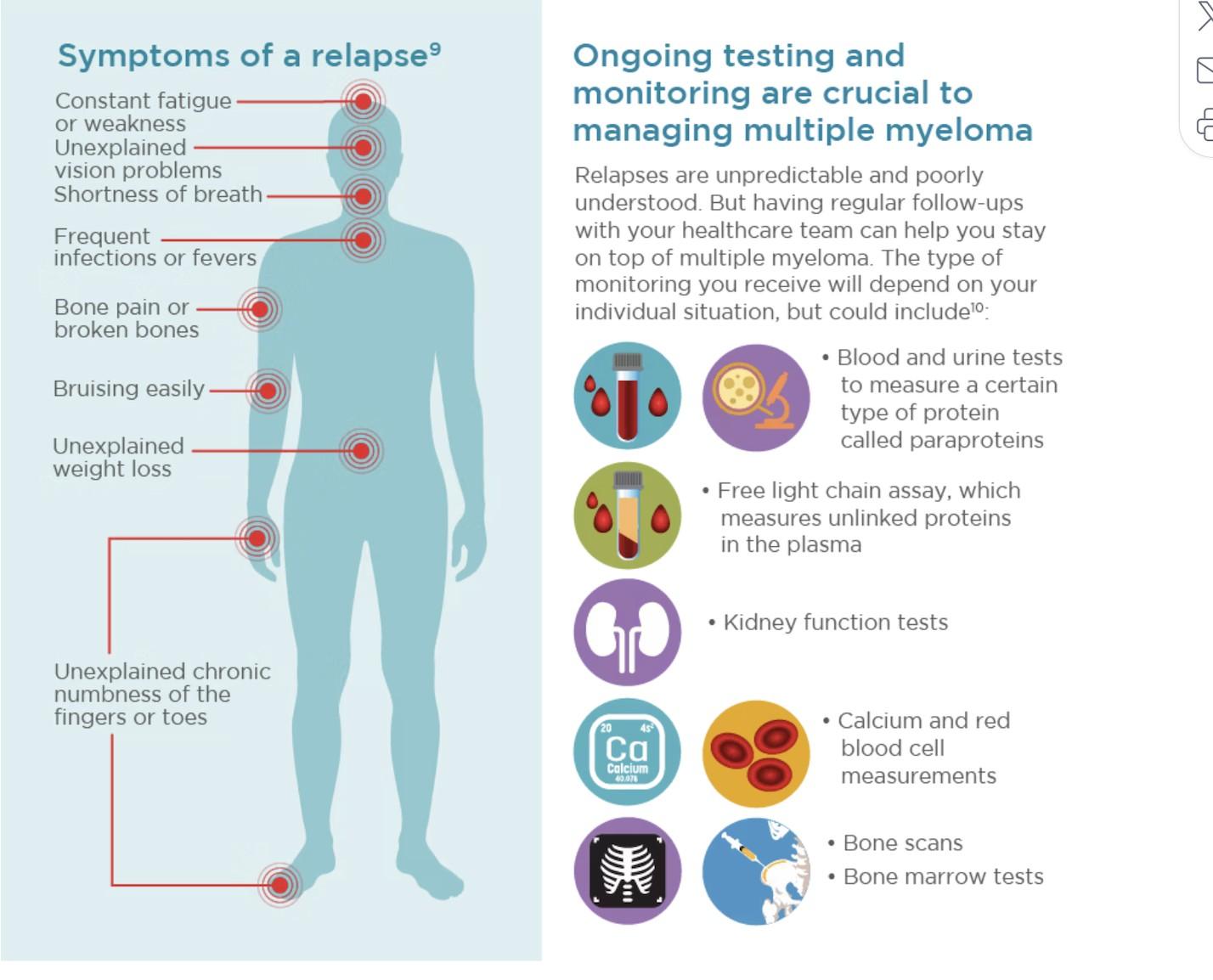
Clonal myeloma plasma cells can cause many symptoms
• Crowd out normal bone marrow cells
• Produce myeloma protein
• Can cause kidney dysfunction
• Affect bone cells (balance of osteoclasts & osteoblasts)
Anemia & Fatigue
Immune Dysfunction & Infection
Renal Dysfunction
Bone Damage

Myeloma’ s Terrain
Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).

Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
As recommended by your healthcare team:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
IMWG = International Myeloma Working Group; HCP = healthcare provider. Raje NS, et al. Lancet Haematol.2022;9(2):143–161. IMF Nurse Leadership Board ONS Symposia 2024.
Preventative and/or supportive medications

Myeloma Treatment
Stay hydrated--drink water
Avoid certain medications
• IV contrast dyes

• NSAIDs like Advil (ibuprofen), Aleve (naproxen)
Be alert: symptoms of kidney dysfunction
• Fatigue and weakness
• Nausea and vomiting
• Foamy or dark urine
• Swelling in feet, ankles, or face
• Shortness of breath
• Persistent itching
• Loss of appetite
• Muscle cramps
• High blood pressure

• Myeloma Treatment
• Nutrition
• Vitamin D
• Calcium (if approved by doctor)
• Weight-bearing activity (e.g., walking, standing, climbing stairs, stretching, dancing)
• Bone-strengthening agents (prescribed by your healthcare team)
to your healthcare provider
Pain can significantly compromise quality of life and add to distress.
Sources of pain include bone disease, neuropathy and medical procedures.
• Decrease fracture risk through myeloma treatment, bone strengthening agents, physical activity, preventative surgery
• Prevent Nerve Damage: prevent shingles, manage diabetes, myeloma medication dosing and route of administration
• Combine scheduled medical procedures, when possible (Ex. blood draw, biopsy), use sedation if available
Interventions depend on source of pain, may include
• Medications, Surgery, Radiation therapy, etc.
• Physical therapy & continued activity, complementary therapies (Mind-body, meditation, yoga, supplements, acupuncture, etc.)
• Scrambler therapy for neuropathy
HR-SMM = high risk smoldering multiple myeloma; M-protein = monoclonal protein; MGUS = monoclonal gammopathy of undetermined significance; misc = miscellaneous (no dominant clone); MM = multiple myeloma; SMM = smoldering multiple myeloma.
Adapted from Durie B. Keats JJ, et al. Blood. 2012;120(5):1067-1076.
High potential to progress to active MM in 2 years
• M-spike ≥ 2 g/dL
• Free light chain assay (involved/uninvolved ratio ≥ 20)
• Bone marrow ≥ 20% clonal plasma cells
FDA approved Nov2025
51% Reduction in risk of disease progression or death with Darzalex Faspro® treatment of high-risk SMM (compared with active monitoring)
DARZALEX FASPRO® as monotherapy is indicated for the treatment of adult patients with high-risk smoldering multiple myeloma
FDA = US Food and Drug Administration; MM = multiple myeloma; SMM = smoldering multiple myeloma

Dimopoulous MA, et al. N Engl J Med. 2024;394(18):1777-1788. doi: 10.1056/NEJMoa2409029. Mateos, MV, et al. Blood Cancer J. 2020;10:102. (2020). https://doi.org/10.1038/s41408-020-00366-3 Use
“The aim of shared decision-making is to ensure that:
- Patients understand their options and the pros and cons of those options.
- Patient's goals and treatment preferences are used to guide decisions.”


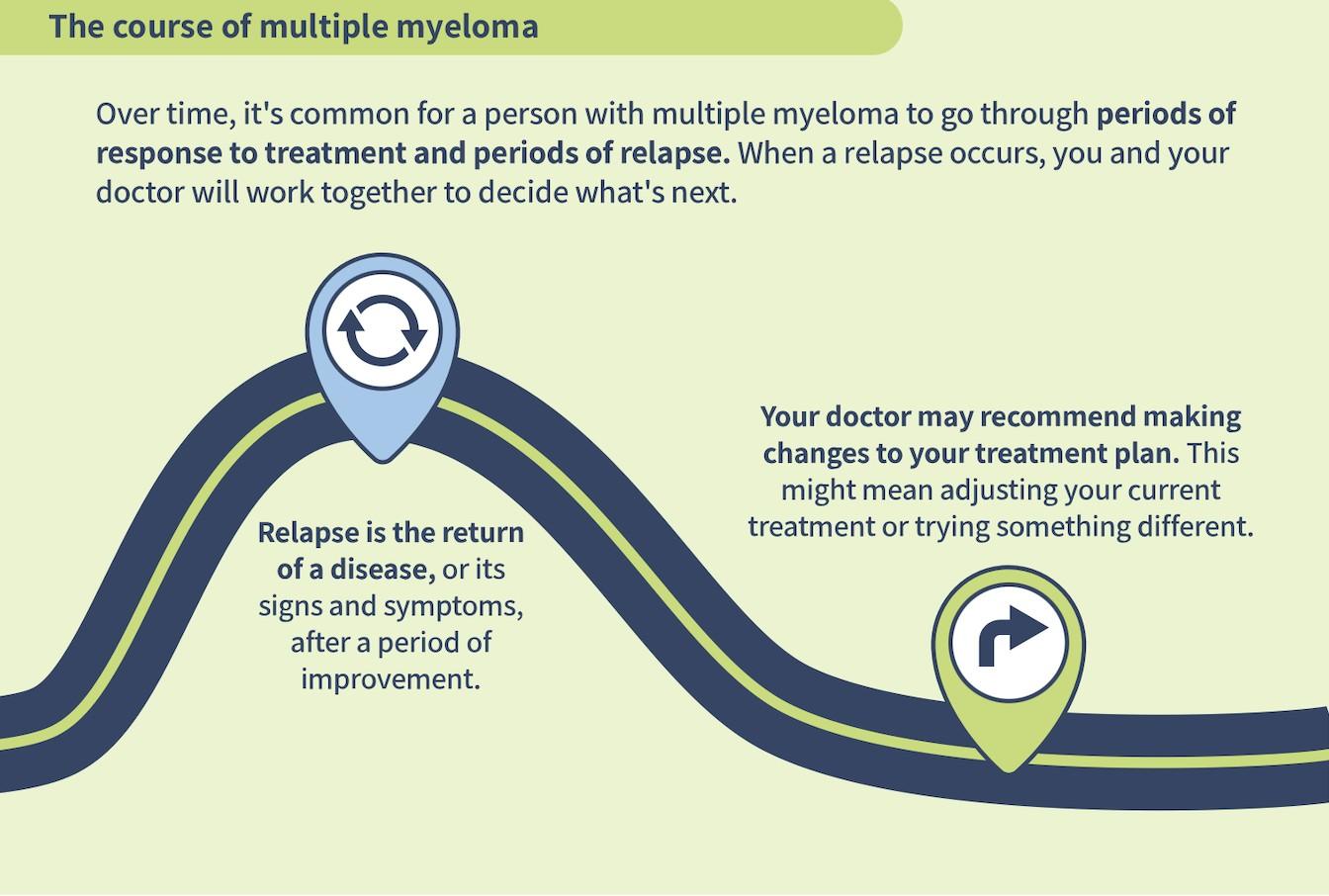
The relapsing nature of multiple myeloma means patients and their care partners may have multiple points to make decisions about treatment
People with myeloma are living longer; goals, preferences, and values may change over time
Ask questions (write them down in advance of visit)
• What are my treatment options?
• What are the pros and cons of each option?
Efficacy? Side effects? Administration? Insurance nuances?
• Are there treatments that wouldn’t be a good option for me? Why?
Express your desire to participate in the treatment decisions
• I want to make sure the treatment we chose is the best option for me
• I want to be sure we a choosing the best therapy for my husband/wife
Ask for time (if needed/ appropriate)
• There is a lot to think about. Can I/we have some time to consider the options?
• Ask for information you can consider at home
• Note: if medical emergency/high risk, may not be appropriate
Starting Your Trek
Understand options; consider priorities
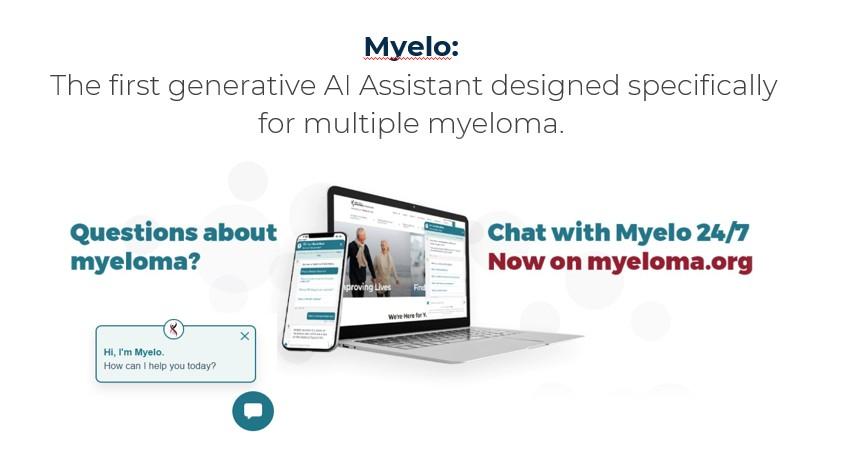
• Use reliable sources of information like the IMF and Myelo
• Use caution when considering stories of personal experiences
• Consider your goals, values and preferences
Express your goals/values/preferences; create a dialog
Arrive at a treatment decision together
• My top priority is [goal/value]; additional [preferences] are also important.
• I think [treatment] may be a good choice given my priorities… What do you think?
• What treatment would you recommend given my goals and priorities?

• Be empowered to be part of decision-making
• Stay informed, understand options
• Use reliable and current sources of information
• Use caution considering stories of personal experiences
• Consider your priorities
• Discuss with your care partner
• Consider your goals/values/preferences
• Be a part of the conversation, create a dialog
• Ask questions & Express your goals/values/preferences
• Ask for time to consider options, if needed
• Arrive at a treatment decision together
• Arrange follow up to review and adjust, if needed
Consolidation
Initial treatments aimed at reducing the amount of myeloma cells
Intensification of treatment to deepen response. Either additional cycles of induction or autologous stem cell transplant (in eligible patients) National Comprehensive Cancer Network® (NCCN®) NCCN Clinical Practice Guidelines In Oncology (NCCN Guidelines®) for Multiple Myeloma. Version 4.2026. To view the most recent or complete version of the guideline, go online to NCCN.org; Rajkumar et al, 2014. Rajkumar SV. Am J of hematology. 2022;97(8):1086–1107. https://doi.org/10.1002/ajh.26590; Faiman et al, 2016.
Prolonged lower-intensity treatment designed to sustain remission Maintenance
Your Trek
Quadruplet therapy is preferred for nearly all patients with newly diagnosed myeloma
1 2 3 4
Anti-CD38 monoclonal antibody (mAb)
• Darzalex (daratumumab)
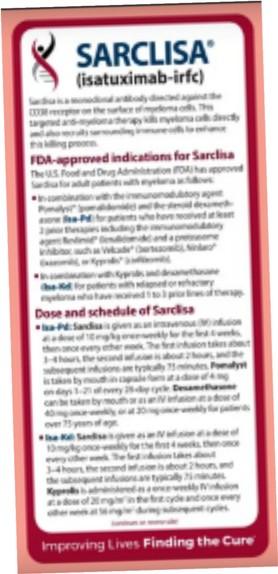
• Sarclisa (isatuximab)
Proteosome Inhibitor (PI)
• Velcade (bortezomib)
• Kyprolis (carfilzomib)
At infusion clinic: subcutaneous injection or on body device or infusion
Supportive medication:
Immunomodulatory drug (IMiD)
Revlimid (lenalidomide)
• Pomalyst (pomalidomide)
• Prednisone
Oral medication taken at home
• Antiviral prophylaxis (i.e., acyclovir or valacyclovir) to prevent viral infections, particularly shingles.
• Antibacterial agents (i.e., Bactrim, levofloxacin) to prevent bacterial infections.
• Aspirin or other anticoagulant therapy to reduce the risk of blood clots from IMiDs.
• Bone-strengthening agents (i.e., zoledronic acid, denosumab) to strengthen bones and protect against fractures.
Starting Your Trek
Steroids enhance the effectiveness of other myeloma therapies
Your provider may decrease or discontinue the dose as myeloma responds to therapy. Do not stop or alter your dose of steroids without discussing it with your provider
• Irritability, mood swings, depression
• Difficulty sleeping (insomnia), fatigue
• Blurred vision, cataracts
• Increased risk of infections, heart disease
• Muscle weakness, cramping
• Increased blood pressure, water retention
• Flushing/sweating
• Stomach bloating, hiccups, heartburn, ulcers, or gas
• Weight gain, hair thinning/loss, skin rashes
• Increased blood sugar levels, diabetes
• Consistent schedule (AM vs. PM)
• Take with food
• Stomach discomfort: Overthe-counter or prescription medications
• Medications to prevent shingles, thrush, or other infections
Rajkumar SV, et al. Lancet Oncol 11(1):29–37. King T, Faiman B. Clin J Oncol Nurs. 2017;21(2):240-249. Banerjee,R. et al. Blood 9.25.24
Peripheral neuropathy happens when there is damage to nerves in the extremities (hands, feet, limbs). Damage can be the result of myeloma, treatment or unrelated conditions (i.e., diabetes).
Symptoms:
Numbness
Tingling
Prickling sensations
Sensitivity to touch
Burning and/or cold
sensation
Muscle weakness
Prevention / management:
Bortezomib once-weekly and/or subcutaneous administration
Massage area with cocoa butter regularly
Neuroprotective Supplements
• i.e., B-complex vitamins (B1, B6, B12)
Safe environment: rugs, furnishings, shoes
If neuropathy worsens, your provider may:
Adjust your treatment plan
Prescribe oral or topical pain medication
Suggest physical therapy
Starting Your Trek
HCPs may manage DVT/PE risk by
• Adjusting medications and schedules
Blood clots can cause swelling, pain, discoloration (DVT), shortness of breath, chest pain, sense of doom (PE). Blood clots are serious and can be life threatening.
• Prescribing blood-thinning medications according to assessed risk (DOAC, aspirin, warfarin, heparin)
• Balancing the risk of DVT and PE with that of bleeding with low platelets

Additional strategies to reduce risk of clots:
• Anti-embolism stockings (elastic stockings)
• Exercise regimen
• Moving frequently when sitting long periods
• Travel precautions (foot/leg exercises, walking, aspirin if not already on blood thinner)
You may be at risk:
• Family History
• Obesity
• Immobility • Smoking
• Surgery
DOAC = direct oral anticoagulant; HCP = health care provider; DVT=deep vein thrombosis; PE=pulmonary embolism
Rome, S, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105. De Stefano, et al. Hematologica, 2022
ELGIBILITY
Location: Transplant Center P H A S E 1
Measuring treatment response Testing for Eligibility
Insurance authorization Collecting stem cells
Duration: Approximately 2 weeks
P H A S E 2
TRANSPLANT
HD-Melphalan Stem cell infusion Supportive Care
• GI Management
• Transfusions
• Antibiotics
Hair Loss Engraftment
Duration: Approx. 3-4 weeks Location: Transplant Center
Location: HOME P H A S E 3
Restrengthening Appetite recovery
“Day 100” assessment
Begin maintenance therapy
Duration: Approximately 1012 weeks
Stem cell transplant after induction remains the standard of care for eligible patients
Fluid intake can help with both diarrhea and constipation and helps kidney function
Constipation is more common in the induction phase
Opioid pain relievers, antidepressants, heart or blood pressure medications (check with provider, pharmacist)
Supplements: Calcium, Iron, vitamin D (rarely), vitamin B-12 deficiency
Increase fiber
Stay well hydrated
Fruits, vegetables, high fiber whole grain foods
Fiber binding agents – Metamucil® ,
Citrucel®, Benefiber®
Anorexia, the inability to eat, is common during transplant and resolves with time.
• Hydration is most important
• Small, frequent meals with a focus on protein intake
• You will work closely with a dietician to help monitor your calorie intake
Diarrhea is common during transplant and long-term maintenance therapy.
Other medications and supplements can cause GI issues.
Hydration is very important
Electrolyte replacement is common
Good skin care will help prevent irritation
Stool exam may be needed to rule-out infection
If no infection, anti-diarrheal medication may be prescribed
Discuss GI issues with healthcare providers to identify causes and adjust medications and supplements
Starting Your Trek
• Can provide information on how well treatment is working
• Is recommended after each treatment stage (e.g., after induction, consolidation, maintenance)
• Should be initiated only at the time of suspected complete response.
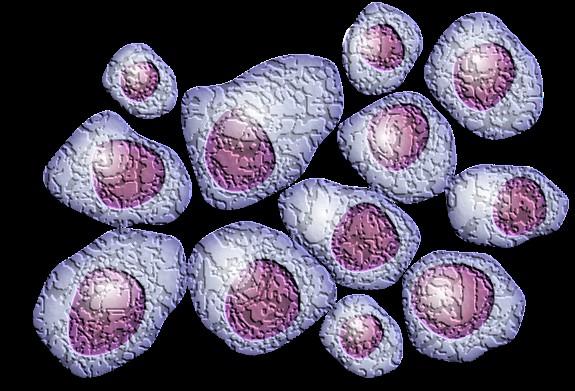
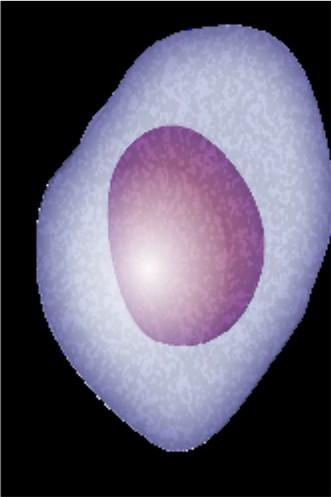
Myeloma cells (purple) crowd out normal bone marrow cells (peach)
No detectable myeloma protein <5% myeloma cells in bone marrow
MRD negative
10-5 = <1 myeloma cell in 100,000
10-6 = <1 myeloma cells in 1,000,000

Myeloma Therapy
Belantamab mafodotina BVd, BPd, BKRd
Bortezomib (SQ admin)
Carfilzomib
Car T-cell
Daratumumab
Elotuzumab
Isatuximab
Ixazomib
Lenalidomide
Common Combinations or Therapy Names
VRd, Vd, VCd
KRd, Kd, Dara-Kd, Isa-Kd
Cilta-Cel®, Ide-Cel®
Dara-Rd, Dara-Vd, Dara-Pd, Dara-VMp, Dara-Kd, Dara-Tecvayli®c
ERd, EPda
Isa-Pda, Isa-Kd
IRd
VRd, Rd, KRd, Dara-Rd, ERd, IRd
Pomalidomidea Pda, Dara-Pd, EPda, PCdc
Selinexor
Xd, XVd, XKdc, Dara-Xdc
T cell Engager (Bispecific)b Elrexfio®, Lynozyfic™, Talvey®, Tecvayli
New agents or regimens in clinical trials may be an option
Many therapy options are in the myeloma toolkit and more are being studied

a2 or more prior therapies. b4 or more prior therapies. cOff-label; not currently FDA-approved.
C = cyclophosphamide; d = dexamethasone; Dara = daratumumab; FDA = US Food and Drug Administration; E = elotuzumab; Isa = isatuximab; I = ixazomib; K = carfilzomib; M = melphalan; p = prednisone; P = pomalidomide;
R = lenalidomide; SQ = subcutaneous; V = bortezomib; X = selinexor.
NCCN Guidelines®. Multiple Myeloma V4.2026. Accessed December 22, 2025.
Relapsed MM with 1-2 prior LOT
BCMA target: potential for infection
• Abecma® (ide-cel)
• Carvykti® (cilta-cel)
• (anito-cel – pending FDA approval)
Bridging therapy, if needed; Lymphodepleting therapy when CAR T cells are ready T Cell Infusion Close monitoring and Management of side effects 1 3 4 5 HOME! Apheresis to Collect T Cells T Cell Manufacturing 2a 2b
Relapsed MM after 4 prior LOT (or clinical trials)
TCE are innovative immunotherapies used in the treatment of relapsed multiple myeloma. These therapies work by redirecting the patient's own T-cells to recognize and attack myeloma cells.
Bispecific antibodies
• About 7 in 10 patients respond
• Off-the-shelf treatment; no waiting for engineering cells
BCMA target: potential for infection
• Tecvayli® (teclistamab)
• Elrexfio® (elranatamab)
• Lynozyfic™ (linvoseltamab)
Cytotoxic cytokines
Bispecific antibody T cell MM cell
GPRC5D target: potential for skin and nail side effects, GI issues of taste change, anorexia and weight loss
• Talvey® (talquetamab)
FcRH5 target: new myeloma target
• (cevostamab - pending FDA approval)

Target CD3


BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; GPRC5D = G protein–coupled receptor, class C, group 5, member D; CAR = Chimeric Antigen Receptor; LOT = Lines of Therapy; MM = multiple myeloma.
J. 2019;doi:10.1038/s41408-018-0164-6. Shah N, et al. Leukemia. 2020;34(4):985-1005.
CYTOKINE RELEASE SYNDROME (CRS) ICANS AND NEUROTOXICITY
• Fever
• Fatigue & Weakness
• Headache
• Nausea/Vomiting/Diarrhea
• Chills
• Low blood pressure
• Rapid heart rate
• Difficulty breathing
CRS is a common but typically mild & manageable side effect
PREVENTION AND MANAGEMENT of CRS
• Disease management to reduce tumor burden
• Bispecific Step-up Dosing (SUD)
• Tocilizumab
• Steroids
• Anti-Seizure medications
• Close monitoring
• Headache
• Difficulty concentrating
• Lethargy
• Agitation
• Hallucinations
• Tremors

• Confusion
• Memory loss
• Aphasia (difficulty with speech, reading, writing, or understanding language)
• Personality change
• Delayed Neurotoxicity can include Parkinsonism, Cranial Nerve Palsies and Peripheral Neuropathy/Guillan Barré syndrome (GBS)
CAR = chimeric antigen receptor. ICANS = Immune Effector Cell-Associated Neurotoxicity Syndrome
Brudno JN, Kochenderfer JN. Blood. 2016;127(26):3321-3330. Lee DW, et al. Biol Blood Marrow Transplant. 2019;25:625-638. Kumar, et al.
Blood (2024) 144 (Supplement 1): 4758.
Type of Infection Risk
Medication Recommendation(s) for Healthcare Team Consideration
Viral: Herpes Simplex (HSV/VZV); CMV Acyclovir prophylaxis
Bacterial: blood, pneumonia, and urinary tract infection
PJP (P. jirovecii pneumonia)
Fungal infections
COVID-19 and Influenza
IgG < 400 mg/dL (general infection risk)
ANC < 1000 cells/μL (general infection risk)
Consider prophylaxis with levofloxacin
Consider prophylaxis with trimethoprim-sulfamethoxazole
Consider prophylaxis with fluconazole
Antiviral therapy if exposed or positive for covid per institution recommendations
IVIg recommended for patients receiving CAR T or TCE therapies
Consider GCSF 2 or 3 times/wk (or as frequently as needed) to maintain ANC > 1000 cells/μL and maintain treatment dose intensity
Some people receiving BCMA-targeting therapies have experienced infections that are less common like CMV, PJP and fungal infections
ANC = absolute neutrophil count; BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; CMV, cytomegalovirus; GCSF = granulocyte colony-stimulating factor; HSV = herpes simplex virus; IVIg = intravenous immunoglobulin;
PJP = Pneumocystis jirovecii pneumonia; VZV = varicella zoster virus.
Raje NS, et al. Lancet Haematol.2022;9(2):143–161.
Changing Course
Xerostomia
OTC dry mouth rinse, gel, spray are recommended. Avoid hot beverages. Anti-fungal therapy for oral thrush.
Dysgeusi a Dexamethasone oral solutions “swish and spit” may provide benefit. Sour citrus or candies before meals are also recommended.
Dysphagia
= Dry Mouth = Difficulty Swallowing = Taste Change
Dietary modifications with small bites, eating upright, and sips with food can help manage symptoms
Weight Monitoring
Some medications lead to weight gain, others to weight loss. Meet with a nutritionist
Consider diet changes, supplements
Dental Care
Attention to oral hygiene. Regular dental cleaning and evaluation. Close monitoring for ONJ, oral cancer and dental caries
ONJ = Osteonecrosis of the Jaw; OTC = Over The Counter
Work closely with your entire health care team to manage oral side effects.
Possible side effect to some treatments and supportive care medications

Skin Rash
Prevent dry skin; apply lotion
Report changes to your care team
Medication interruption or alternative, as needed
Steroids:
• Topical for grades 1-2,
• Systemic and topical for Grade 3
Antihistamines, as needed

Nail Changes

Keep your nails short and clean.
Watch for “catching and tearing”
Apply a heavy moisturizer like Vaseline or salve. Wear cotton hand coverings to bed
A nail hardener may help with thinning
Tell the team if you have signs of a fungal infection, like thickened or discolored nails
Fatigue is the most reported symptom. Sources include anemia, pain, reduced activity, insomnia, treatment toxicity, bone marrow suppression. Symptoms can improve with continued physical activity.
Symptoms are under-reported:
“I mentioned it before. Nothing can be done.”
“I don’t want to be put on another medication.”


• Mental health / social engagement
• Stress reduction; relaxation
• Sufficient Sleep
• Maintain a healthy weight; eat nutritiously
• Activity / exercise / prevent falls, injury
• Stop smoking
• Sexual health / intimacy
• Complementary or alternative therapy
Have a PCP for general check ups, preventative care, health screenings, vaccinations
Have specialists for dental care, eye exams/screening, skin cancer screening
Recommended Health Screenings
Blood pressure
Cholesterol
Cardiovascular disease
Colonoscopy
Dental checkups & cleaning Dermatologic evaluation
Diabetes
Hepatitis
Hearing
Vision
Women specific: mammogram, pap smear
Men specific: prostate
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56.
Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.
Multiple studies demonstrate that strong social ties are associated with
• Increased longevity including people with cancer
• Improved adherence to medical treatment leading to improved health outcomes
• Lower risk of cardiovascular diseases
• Increased sense of purpose & life satisfaction
• Improved mood and happiness
• Reduced stress and anxiety
• Enhanced resilience
Care partners may help with medical appointments, managing medication, daily living, physical assistance, emotional support, myeloma knowledge, healthy lifestyle, patient advocacy, financial decisions
Care partners can be a spouse, close relative, a network of people (family, friends, neighbors, church members, etc)
Caring for the care partner
• Recognize that caregiving is difficult and stressful
• Encourage care partners to maintain their health, interests, and friendships
• The IMF has information and resources to help care partners
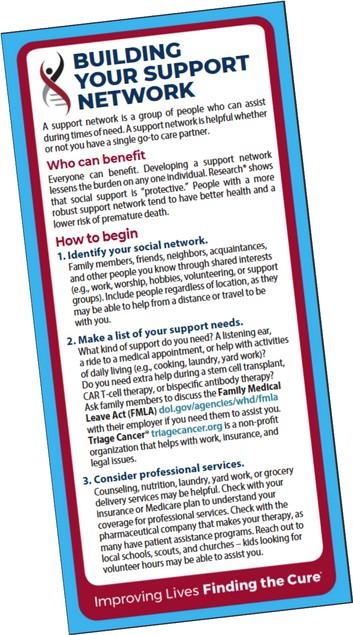
Tip Cards




“THANK YOU!”

Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO Chief Medical Officer, International Myeloma Foundation

Joseph Mikhael MD, MEd, FRCPC, FASCO Chief Medical Officer, International Myeloma Foundation
Professor, Translational Genomics Research Institute, City of Hope Cancer Center
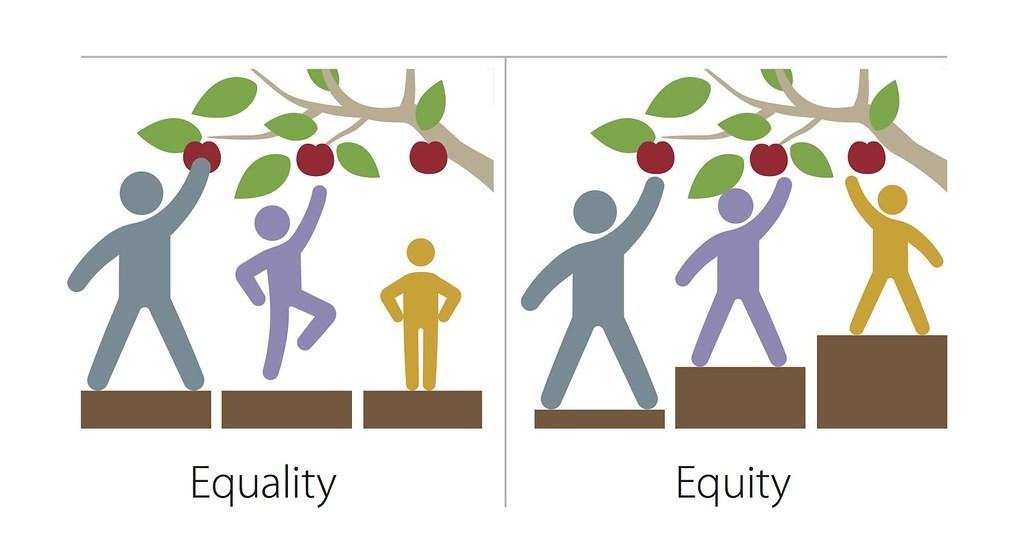
Health disparities are preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations
- Centers for Disease Control (CDC)
Health equity generally refers to individuals achieving their highest level of health through the elimination of disparities in health and health care



The core vision of this initiative is to improve the short- and long-term outcomes for African American patients with myeloma.
We want to empower patients and communities to change the course of myeloma…
Enhance access to optimal care by educating myeloma providers about the disparity and how to reduce it
Engage the community to increase awareness and provide support
Shorten the time to diagnosis by educating primary care providers to recognize the disease and order the right tests










Kyle RA. Mayo Clin Proc. 2003;78:21-33.



Other Physician
Emergency Care
Hematologist
Oncologist
Primary Care/ Internal Medicine
Nephrologist
Orthopedic
Rheumatologi st Neurologist
Typical diagnostic intervals1
Hematology/Oncology: < 3 months
Primary Care: > 6 months
The average patient will see their PCP THREE times with signs and symptoms of MM before the diagnosis is suspected!2
1. Kariyawasan CC, et al. QJM. 2007;100:635-640. 2. Hossain M, et al. An in depth analysis of factors contributing to diagnostic delay in myeloma: a retrospective UK study of patients journey from primary care to specialist secondary care. Blood. 2021;138(suppl 1):3007.
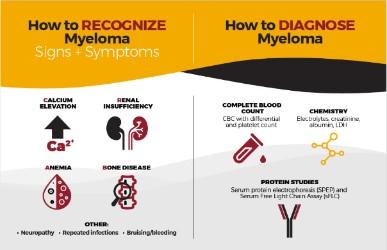
Our goal is to reduce DELAYS in diagnosis among African Americans by educating the primary care community with a focus on:
• Recognizing the signs and symptoms of myeloma
• Discriminating myeloma from other diagnoses such as diabetes
• Capturing an accurate diagnosis through proper use of testing
• Providing referral guidelines for Hematology and Oncology

• Grand Rounds
8,000
• Postcards mailed to 6,000+ PCPs in target cities
• Free PCP CME course “Don’t Miss Myeloma”
• Cobb Institute talk

• Talk at NMA Annual Meeting Dinner Meetings Articles and pending publications


• 11 1st through 3rd year medical students from all over the country met in Chicago on July 21st at the NMA Annual Convention and Scientific Assembly
• Presented posters, they worked on with a multiple myeloma experts immediately following the Jane Cooke Wright Symposium
• 2 students delivered oral presentations at a NMA session






Over 750,000 visits to M-Power site!





Objective: To promote trust and educate patients regarding clinical trials, particularly those from populations underserved by clinical trials, laying the groundwork for potential future trial participation
1.Identify Myeloma Patients who have been on a trial from historically underrepresented groups
2.Diversity in Clinical Trials Academy
• The patients and partners attended an in-person training on the ABCs of Clinical Trials, unconscious bias, reasons for participation in trials, limitations of trials, informed consent, and how to effectively relate their personal stories.
• They were recorded sharing their stories and their interaction with clinical trials

3.Rollout of the program
This will be incorporated into IMF in-person meetings, videos, the IMF website, articles, podcasts, social media campaigns, and support group curricula

• Health disparities are sadly prevalent across all diseases, but particularly in multiple myeloma in the Black community
• KNOW the signs/symptoms of myeloma – Fatigue, Pain and Anemia
• If you know someone with myeloma, we are here for you!
• The IMF’s M-Power is designed to reduce the inequity by ENGAGING the community, EDUCATING primary care providers and ENHANCING the care of patients with myeloma...
•Be more conscious of the topics of health equity
•Evaluate the opportunities in your experience to reduce disparities
•Support the M-Power movement!


PLEASE HEAD TO YOUR SELECTED BREAKOUT SESSION:
BREAKOUT A: PATIENTS ONLY – LESSONS LEARNED
Please remain in this room
BREAKOUT B: CARE PARTNERS ONLY
Please move to Royal Palm
Carl Ola Landgren, MD, PhD
University of Miami
Rafat Abonour, MD
University of Miami
Moffitt Cancer Center
• Slides from Friday & Saturday Programming
• Evaluations for Friday & Saturday Programming
• SparkCures Search Engine specific for the Florida region
• Ways to Give
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease.