Regd.With RNI No.MAHENG/2007/22045.Postal Regd.No.MCS/162/2025 - 27.Printed and Published byVaidehi Thakar on behalf of The Indian Express (P) Limited and Printed at The Indian Express Press,Plot No.EL-208,TTC Industrial Area,Mahape,Navi Mumbai-400710 and Published at Mafatlal Centre,7th floor,Ramnath Goenka Marg,Nariman Point,Mumbai 400021.
Reproduction in anymanner,electronic or otherwise,in whole or in part,without prior written permission is prohibited.
Towards safer paediatric prescriptions
The cough syrup linked-deaths of children in Madhya Pradesh has revived concerns not just of manufacturing norms but also irrational use/abuse of common medications. It's an open secret that medicines from cough syrups to antibiotics can be bought over the counter in India, without a prescription. While the irrational use of antibiotics has given rise to antimicrobial resistance and rendered many patients unresponsive to most antibiotics, the overuse of cough syrups in children is particularly harmful.
An advisory issued by the Directorate General of Health Services (DGHS) on the rational use of cough syrups in paediatric populations highlights that cough and cold medications should not be prescribed or dispensed to children below the age of two years. It also stresses that any use should be after careful clinical evaluation, followed by close supervision, to ensure appropriate dosing and avoiding use of multiple drug combinations. A letter written by the Health Ministry to the Director of Health Services of all States and Union Territories reportedly mentions that most acute cough illnesses in children are self-limiting and often resolve without pharmacological intervention.
Medical professionals agree with this assessment. Dr Sujit Paul, CEO, Zota Healthcare in fact calls the advisory a milestone, marking the ‘New Age of Pediatric Medication Awareness’, highlighting how the conversation is shifting from "what to prescribe" to "whether to prescribe or not." Dr Paul suggests that rather than turning to syrup prescriptions, clinicians can concentrate on educating caregivers, specifying under what conditions drug therapy is appropriate and when it is not. He also makes the point that the message can be used on all paediatric medications, antibiotics to vitamins.
(See Dr Paul’s blog: https://www.expresshealthcare.in/ blogs/ guest-blogs-healthcare/the-new-age-of-pediatric-medication-awareness/451227/)
Public health expert Dr Sameer Bhati explains that while OTC cough medications may be safe in adult measured amounts, they could be poisonous to infants as their developing organs metabolise medications differently. Hence infants are more likely to experience side effects such as drowsiness, fast heart rate, vomiting, and, in the worst instances, shortness of breath. As he analyses, it's not necessarily an issue of unsafe products but of unsafe use, self-diagnosis, estimation of doses at home, and dismissal of age-related medical advice.
His advice to healthcare professionals is that it's time now to bid adieu to symptomatic treatment and move towards root-cause management. Echoing the DGHS advisory, Dr Bhati points out that cough and cold in infants are more frequently than not viral and self-limiting and call for acts of comfort and not drugs. The way
The deaths of children due to a cure which turned harmful should hopefully result in more awareness among doctors, parents/caregive rs and pharmacies/phar macists
forward is to train caregivers to distinguish between viral and bacterial infections, fluid hydration, and home remedies can limit unwarranted drug exposure.
(See Dr Bhati’s blog: https://www.expresshealthcare.in/ blogs/guest-blogs-healthcare/from-syrups-to-safety-shifting-focus-in-child-healthcare/451211/)
But will clinicians stop prescribing cough syrups? Will parents stop buying and giving their babies and toddlers cough syrups? Will pharmacists, both online and offline, stop selling cough and cold medications without a prescription? The doctor/pharmacy knows that if they don't write such prescriptions or give medications without a prescription, caregivers will simply walk over to the next doctor’s clinic or chemist shop.
Zooming out from this harsh reality, report after report highlights that India’s healthcare sector is an investor’s destination, with a wave of investor-driven consolidation underlining the sector’s strong fundamentals and growth potential. For instance, as per Grant Thornton Bharat’s Q3 2025 Pharma and Healthcare Dealtracker, India’s hospital sector recorded 19 deals worth USD 264 million. Multi-specialty consolidation gained pace in western India and NCR, while singlespecialty formats like dialysis, IVF, oncology, and women and child-care drove volumes. The health tech side saw steady volumes and moderate valuations, with investments concentrated in digital health, AI diagnostics, and patient engagement tools. The wellness and preventive care segment saw sustained growth, backed by consumer awareness, nutraceutical innovation, and digital-first health platforms. Deal activity in medical devices saw episodic but strategic M&A, especially in orthopaedic and cardiology devices; outbound deals expanded global access. And diagnostics and homecare saw selective consolidation, favouring scalable, regional, asset-light platforms.
But on the other side of investor confidence and bullish sentiment, are the tragic deaths which triggered the Health Ministry’s advisory on improper prescribing/dispensing of cough syrups. The deaths of children due to a cure which turned harmful should hopefully result in more awareness among doctors, parents/caregivers and pharmacies/pharmacists about the dangers of quick fixes like cough/cold medications and the merits of slow acting but more lasting holistic healing principles.
Abalanced PPPmodel holds transformative potential for India’s healthcare ecosystem
Dr Azad Moopen, Founder and Chairman of Aster DM Healthcare,in an interaction with Kalyani Sharma, shares his insights on the key forces shaping India’s healthcare future,the role of public-private partnerships,digital transformation,workforce development,and Aster’s vision for sustainable and inclusive growth
What, according to you, are the most critical forces shaping the future of healthcare in India, and how do you see the sector contributing to India’s journey towards becoming a $5 trillion economy?
As India advances toward its $5 trillion economic vision, the healthcare sector must be viewed as a powerful catalyst for economic growth. Beyond improving the well-being of citizens, the sector fuels employment, infrastructure expansion, and innovation which forms the key pillars of a thriving economy.
Government initiatives such as Ayushman Bharat and the National Digital Health Mission have made notable strides in expanding access. However, increasing public health expenditure, currently around 2 per cent of GDP and addressing regional disparities remain crucial. A comprehensive approach centered on accessibility, affordability, and sustainability will be vital to ensure equitable healthcare across both urban and rural regions.
Innovation and technology will continue to define the sector’s future. The rapid adoption of telemedicine, digital health solutions, and AI-driven diagnostics is already transforming healthcare delivery. These advancements not only enhance patient outcomes but also contribute significantly to economic momentum by generating employment and strengthening allied industries, including pharmaceuticals, medical devices, and health tourism.
Despite progress, India’s healthcare spending remains at around 2 per cent of GDP. What policy reforms or public-private partnership models do you believe are essential to improve accessibility and affordability of healthcare?
A balanced public-private partnership (PPP) model holds transformative potential for India’s healthcare ecosystem. By combining the government’s expansive reach with the private sector’s agility, innovation, and operational excellence, PPPs can bridge critical gaps in accessibility, particularly between urban and rural areas. While urban centres continue to have a higher concentration of healthcare resources, rural regions— home to a significant share of the population—remain underserved. A strategic PPP
model can address this imbalance by leveraging public infrastructure and integrating private expertise to deliver high-quality care across geographies.
This model also brings financial sustainability to healthcare initiatives. By channeling private investments and corporate social responsibility (CSR) funds into public infrastructure development, the model can address resource constraints.
Moreover, PPPs foster innovation introducing advanced technology, modern management practices, and digital health solutions into the public domain. The collaborative success seen during the COVID-19 pandemic, particularly in testing, treatment, and vaccine deployment, underscores the power of public-private
synergies.
To ensure long-term success, PPPs must be carefully curated with clear roles and responsibilities for both parties. Transparency in operations, competitive bidding processes, and performance-linked incentives are essential for maintaining trust and efficiency within these partnerships. Additionally, policies must focus on scaling these models sustainably while tailoring them to address specific regional healthcare needs.
Additionally, a comprehensive approach that prioritises accessibility, affordability, and sustainability is crucial to achieving equitable healthcare across both urban and rural India. Leveraging innovation and technology will play a pivotal role in making healthcare globally competitive. The swift expansion of telemedicine, digital health platforms, and AI-driven diagnostics is already revolutionising the sector. These innovations enhance patient outcomes while simultaneously driving economic growth by generating jobs and strengthening allied industries such as pharmaceuticals, medical devices, and health tourism.
With technology such as Artificial Intelligence (AI), robotics, and telemedicine transforming care delivery, how do you envision the role of digital health in bridging gaps in quality healthcare across tier 2 and tier 3 cities? Technological innovation is transforming India’s healthcare sector by
enhancing accessibility, efficiency, and patient outcomes. AI is advancing diagnostics, predictive analytics, and personalised treatment plans, while telemedicine is bridging the urban–rural divide by connecting patients in remote areas with medical experts. Wearable devices and remote monitoring enable real-time management of chronic diseases, ensuring timely interventions. Meanwhile, robotic-assisted surgeries and minimally invasive procedures are improving precision and recovery rates. Digital health platforms and electronic medical records are also streamlining data management, fostering better coordination among healthcare providers.
At Aster, our partnership with the Indian Institute of Science led to the establishment of the Aster AI Lab, which developed the AI Carpal Tunnel Syndrome (CTS) diagnostic tool, an innovation by our Neurology Department that is revolutionising nerve ultrasound analysis. Our TeleHealth Services further strengthen accessibility by leveraging technology to deliver comprehensive, highquality care across regions.
We also recently introduced the Aster Health App, designed to make healthcare more convenient and integrated. With a simple tap, users can access essential medical services, and the app will soon expand to include pharmacy, diagnostics, and home care, building a holistic healthcare ecosystem. It also enhances in-hospital
STRATEGY
experiences by streamlining admissions, inpatient services, and payments.
The impact of these initiatives is clearly visible: AIdriven tools have significantly improved diagnostic accuracy, resulting in better clinical outcomes, while telemedicine has extended specialist care to remote areas, lowered consultation costs, and improved healthcare access for underserved communities.
The shortage of skilled healthcare professionals continues to challenge the sector. What steps should India take at a systemic level to ensure a future-ready healthcare workforce?
India continues to grapple with the persistent challenge of bridging the gap in skilled healthcare professionals. Addressing it requires a multipronged strategy beyond encouraging more people to specialise. We also need to focus on continuous upskilling and provide the existing workforce exposure to advanced technologies, along with effective integration of allied health professionals to strengthen the care continuum.
Aster has recognised this growing gap and has taken a proactive approach to address it through its education and training initiatives. The Aster Health Academy is one of our key initiatives to bridge this gap by offering specialised and advanced programs designed to upskill healthcare professionals, including those in primary care.
Additionally, Aster is working directly with medical colleges and hospitals across the country to provide realworld clinical exposure, mentorship, and jobshadowing opportunities for young doctors and medical students. These programs don’t just build technical expertise, they also help prepare professionals for broad, community-focused care.
Aster DM Healthcare is expanding its presence in India with significant investments and an increase
in bed capacity. How does this growth align with your long-term vision for Aster’s role in the Indian healthcare ecosystem?
Aster has laid out a welldefined and ambitious expansion strategy to capitalise on the fast-evolving Indian healthcare landscape.
As part of this plan, the company intends to add over ~2,368 beds across the country over the next few years. A total capital outlay of approximately ~Rs 2300cr has been committed to this growth initiative, of which Rs 350cr already invested in critical projects as of September 2025. Of the ~2,368 planned beds, over 490+ will be added in FY26, 1,050+ in FY27, and the remaining 1080+ beyond FY27. This expansion includes 1439 beds in Bengaluru, 554 in Kerala, and additional capacity across other key regions, reinforcing Aster’s national presence. Key upcoming additions include 2 new hospitals in Bengaluru – a 430 bed and 500-bed facility on Sarjapur Road and Yeshwanthpur and 350 beds at Aster CMI Hospital, reinforcing our leadership position among the top three healthcare providers in the city. In Kerala, we are developing a new greenfield project: a 454-bed Aster Capital Hospital in Trivandrum and adding 100 beds to Aster Medcity and in Hyderabad a state-of-the-art 300-bed Women & Children’s Hospital is being planned and 75 beds at Aster Ramesh, Ongole.
A key milestone in our India growth strategy was the announcement of merger between Aster and Quality Care India Ltd. (QCIL), backed by Blackstone. This merger [subject to regulatory approvals] marks one of the most transformative moves in the Indian healthcare sector, positioning the combined entity ‘Aster DM Quality Care Ltd.’ among the top three hospital chains in India by revenue and bed capacity. Looking ahead, the merged entity will aim to increase bed capacity to around 14,190+ beds over the coming years. Of
the planned,3,820+ bed additions by the merged entity, ~2,368 beds will be added by Aster and the remaining by QCIL.
The merger also paves the way for Aster to expand into new markets beyond its strong existing presence in Kerala and Karnataka, with increased reach into states like Madhya Pradesh, Odisha, Chhattisgarh, and Tamil Nadu.
Aster is also focusing on areas like oncology, cardiology, neurology, and precision medicine. How do you see these specialities and innovations strengthening Aster’s positioning and impact on patient outcomes? Cancer care remains one of our foremost priorities at Aster, where we have made significant investments to build a holistic, technologyenabled ecosystem that supports patients through every stage—from early detection to advanced treatment and recovery. To strengthen our oncology services, we launched the Aster International Institute of Oncology – a state-of-theart multidisciplinary international standard cancer care institute offering an entire range of oncologyrelated services backed by our highly experienced team of doctors, cutting-edge technologies and the latest innovations.
On the diagnostics front, we provide cutting-edge imaging technologies such as 3D mammography for accurate breast cancer detection, Digital PET CT, SPECT CT, Gamma Cameras, and 256-slice CT scanners, all of which enable precise imaging, staging, and monitoring of cancer progression.
Our treatment infrastructure features some of the world’s most advanced systems, including the Elekta Versa HD LINAC and TrueBeam for high-precision radiotherapy, as well as Intraoperative Electron Radiation Therapy (IOERT), which delivers targeted radiation during surgery for improved outcomes. We also
utilise state-of-the-art robotic platforms such as the 4thgeneration Da Vinci Robot and SSI Mantra, enabling complex oncological surgeries with greater accuracy, precision, and minimal invasiveness.
In the last financial year alone, Aster successfully conducted over 1,865 robotic surgeries and 575 transplants, underscoring the growing trust and confidence patients place in our expertise.
Through this integrated, patient-centric approach— powered by advanced technology and compassionate care—we are setting new benchmarks in cancer care across our network.
We have also introduced three pioneering initiatives: Precision Oncology Clinics, the Aster Cancer Grid, and Onco Collect software. These are designed to advance personalised cancer treatment through genomic profiling, ensuring therapies are tailored to each patient for improved efficacy and fewer side effects. The Aster Cancer Grid connects hospitals, researchers, and institutions to promote collaborative research, standardise clinical protocols, and facilitate multicenter clinical trials.
Meanwhile, Onco Collect integrates patient data into a unified digital platform, supporting evidence-based decision-making and real-time outcome tracking.
Beyond treatment, we also focus deeply on patients’ emotional and physical wellbeing. Our Scalp Cooling System, for example, helps reduce hair loss during chemotherapy—a seemingly small intervention that makes a significant difference to a patient’s confidence and comfort during care.
By blending innovation, personalisation, and empathy, Aster continues to redefine the future of cancer care for the communities we serve.
Social responsibility plays a big part in Aster’s philosophy. How has the Aster Volunteers programme helped translate that commitment into realworld change?
Social responsibility has always been deeply embedded in Aster’s philosophy. The idea behind the Aster Volunteers programme was born from a simple yet powerful belief that healthcare should extend beyond the walls of hospitals and reach people where they are, especially those who need it the most. I envisioned Aster Volunteers as a structured platform that could channel the compassion, expertise, and commitment of Aster’s employees, doctors, and partners into meaningful community service. What began as a small initiative to make quality healthcare accessible to the underserved has now evolved into a global movement for good.
The Aster Volunteers programme mobilises employees, doctors, and medical staff to participate in free medical camps, health education drives, disaster relief efforts, and outreach missions in remote areas. Recently, we launched our 66th mobile medical unit that serve remote regions of states such as Jammu & Kashmir, Rajasthan, Assam, Karnataka, Gujarat, and others.
The Aster Volunteers team has also been among the first to respond during calamities such as the 2024 landslides in Wayanad and the train accident in Odisha, providing both relief and essential medical care. Following the devastating Kerala floods in 2018, we constructed and handed over more than 250 homes to families who had lost their shelter.
Over the years, this initiative has touched the lives of over 7.2 million people through various programmes, with more than 85,000 registered volunteers across geographies. From preventive health to emergency response, Aster Volunteers embodies our mission of “We’ll Treat You Well” — translating compassion into action and reaffirming our commitment to building healthier, more resilient communities.
Atul Grover,MD-India and South Asia,Becton,Dickinson (BD) stresses that PPPs are vital to improving TB diagnosis and treatment.Regulatory policies should incentivise private hospitals and diagnostic centres to collaborate with the National TB Elimination Program (NTEP) through structured agreements
India’s ambitious goal of eliminating tuberculosis (TB) by 2025 has gained momentum with the launch of a 100-day campaign in December 2024, targeting 347 highburden districts. This initiative aims to enhance case detection, streamline treatment, and leverage technology to curb TB transmission. While the campaign reflects strong political will and strategic intent, its long-term success depends on regulatory coherence, private sector participation, and systemic reforms.
Strengthening
Public-private partnerships (PPPs) and infrastructure
PPPs are vital to improving TB diagnosis and treatment. Regulatory policies should incentivise private hospitals and diagnostic centres to collaborate with the National TB Elimination Program (NTEP) through structured agreements. Simplifying approval processes, offering financial incentives, and integrating private-sector data into national TB surveillance systems can improve case reporting and treatment adherence. Ad-
ditionally, linking the accreditation of private healthcare facilities to TB detection and treatment success rates can enhance accountability. Infrastructure development is equally crucial. Expanding molecular diagnostic labs, deploying mobile testing units, and leveraging telemedicine solutions can improve access, particularly in remote and tribal areas. Financial support through direct benefit transfer schemes—such as the government’s Rs 3,338 crore allocation—should be broad-
ened to cover nutrition and transportation costs for TB patients, ensuring uninterrupted treatment adherence and better health outcomes.
Social outreach and corporate engagement
Corporate engagement presents a significant opportunity to strengthen TB elimination efforts. Expanding Corporate Social Responsibility (CSR) mandates to include TB-focused healthcare initiatives, awareness campaigns, and infrastructure support can drive
greater impact. Offering tax incentives to companies investing in TB diagnostics, treatment, and mobile health units can further accelerate progress.
Social stigma continues to be a significant barrier to TB elimination. Strengthening regulatory frameworks to promote community-driven awareness programs and encouraging corporate and civil society participation can help combat misinformation. ASHA workers, who have played a key role in rural TB detection,
should receive fair remuneration and enhanced training to bolster their advocacy and patient support efforts.
Integrating TB care with social securitymeasures TB disproportionately affects vulnerable populations, making social security support a crucial element of elimination strategies. Policies should integrate TB care with broader social security measures, including housing assistance, nutritional programs, and employment support for TB-affected individuals. Ensuring financial stability and social protection can reduce treatment dropout rates and prevent reinfection.
Conclusion
India’s 100-day campaign is a bold step towards TB elimination, but sustained regulatory oversight, strong PPPs, and systemic healthcare improvements are essential for longterm success. A multi-pronged approach—incorporating stringent reporting mechanisms, corporate participation, social security integration, and infrastructure enhancements—will be key to achieving this ambitious goal.
Technology is transforming healthcare roles,skills,and systems but keeping the human touch intact remains the sector’s biggest test
By Kalyani Sharma
India’s healthcare sector is at a turning point. Technology integration is becoming integral to clinical decision-making, administrative workflows and patient monitoring. This transformation is crucial but it is as much about people as it is about technology. Technology is transforming healthcare roles, skills, and systems but keeping the human touch intact remains the sector’s biggest test.
Preparing India's healthcare workforce to grow in a digital, data-driven ecosystem without losing the touch of empathy will be a real challenge.
Tech-enabled care
The healthcare job profiles are changing across hospitals, diagnostics centres and even primary care setups. Majority of tasks, once relied heavily on manual effort is now increasingly being done by intelligent systems.
Aryaman Tandon, Managing Partner, Healthcare & Lifesciences, Praxis Global Alliance observes, “Digital technologies are fundamentally reshaping healthcare roles by shifting routine and repetitive tasks toward decision support, data interpretation, and remote care.”
This evolution is not about job replacement but job reimagination. Chris George, CEO and Founder, QubeHealth, points out that digital technologies are shifting healthcare roles from repetitive, manual tasks toward oversight, interpretation, coordination, and human-tech collaboration.
“Overall, job descriptions are evolving: healthcare workers need to interact with, manage, and trust digital tools rather than simply ignore or replace them.”
Healthcare workers today must not only use digital tools but also learn to “interact with, manage, and trust” them.
Automation is streamlining administrative functions, freeing doctors and nurses to focus on patients.
As Shantanu Baruah, Global Head – Life Sciences, Healthcare & Insurance, Hexaware, puts it, “Technology is a colleague that
Digital technologies are fundamentally reshaping healthcare roles by shifting routine and repetitive tasks toward decision support,data interpretation, and remote care
Aryaman Tandon
Managing
Partner, Healthcare & Lifesciences, Praxis Global Alliance
Overall,job descriptions are evolving: healthcare workers need to interact with,manage,and trust digital tools rather than simply ignore or replace them
Chris George
CEO
and Founder,
QubeHealth
Technology is a colleague that removes friction; the human still carries the responsibility
Shantanu Baruah Global Head – Life Sciences, Healthcare & Insurance,Hexaware
While AI can analyse data,compassion and intuition remain uniquely human.A balanced approach is encouraged- one that nurtures emotional intelligence, ethical judgment,and patient communication alongside digital proficiency
Jasdeep Singh Group CEO, SPARSH Group
of Hospitals
removes friction; the human still carries the responsibility.” Hospitals are moving from labourintensive workflows to insightdriven models where clinicians partner with machines rather than compete with them.
Anewskills equation
With new skill requirements emerging across every level of healthcare workforce, traditional medical expertise must now be paired with digital fluency.
According to Jasdeep Singh, Group CEO, SPARSH Group of Hospitals, “Healthcare professionals today must combine clinical acumen with digital literacy. Doctors are learning to interpret algorithmic outputs, validate AIdriven insights, and ensure ethical data use.”
Tandon categorises these competencies into four broad pillars: digital literacy i.e. proficiency in EHRs, telemedicine platforms, and AI-assisted diagnostic tools; data literacy i.e. understanding AI outputs, recognising algorithmic limitations, and maintaining data hygiene and privacy compliance; technical proficiency i.e. operating surgical robots, remote monitoring devices, and point-of-care diagnostic tools and human-centric skills such as empathy and ethics.
Similarly, Arindam Sen, CEO and Director, Heartnet India, underscores the importance of adaptability and cybersecurity awareness. “ Medical workers require new skills beyond clinical training, including areas of IT such as virtual consultations and real-time data management, as well as remote ECG and ICCU monitoring. Key competencies include the successful use of Electronic Health Records (EHR) systems, as well as telehealth platforms for remote consultations, diagnosis, and treatment. Cybersecurity awareness is also important for safeguarding sensitive patient information. Communication skills are evolving for remote consultation, which necessitates clarity and empathy via virtual channels.”
In essence, the future clinician must be as comfortable at
the console as they are at the bedside — a theme echoed by many leaders across the healthcare spectrum.
Continuous learning becomes the newnorm
As digitisation is more deeply integrated into the system, hospitals are realising that training cannot be a one time exercise but must be embedded into the workflow.
Sushant Rabra, Partner and Head-Digital Strategy and Transformation, KPMG in India, notes that, “Forward-looking healthcare organisations are institutionalising digital learning through in-house academies, simulation labs, and collaborations with edtech partners and GCCs. The focus is on ‘learning in flow,’ helping clinicians and administrators gain digital confidence while on the job and seamlessly integrate technology into care workflows. Many organisations are now linking digital competency with career progression, signalling that digital readiness is a core part of healthcare excellence.”
Deepak Sharma, Co-founder
CONTRIBUTOR’S CHECKLIST
● Express Healthcare accepts editorial material for the regular columns and from pre-approved contributors/columnists.
● Express Healthcare has a strict non-tolerance policy towards plagiarism and will blacklist all authors found to have used/referred to previously published material in any form, without giving due credit in the industryaccepted format.
● As per our organisation’s guidelines,we need to keep on record a signed and dated declaration from the author that the article is authored by him/her/them,that it is his/her/their original work,and that all references have been quoted in full where necessary or due acknowledgement has been given.The declaration also needs to state that the article has not been published before and there exist no impediment to our publication.Without this declaration we cannot proceed.
● If the article/column is not an original piece of work,the author/s will bear the onus of taking permission for re-publishing in Express Healthcare.The final decision to carry such republished articles rests with the Editor.
● Express Healthcare’s prime audience is senior
Medical workers require new skills beyond clinical training,including areas of ITsuch as virtual consultations and real-time data management,as well as remote ECG and ICCU monitoring
Arindam Sen CEO and Director, Heartnet India
Forward-looking healthcare organisations are institutionalising digital learning through in-house academies,simulation labs,and collaborations with edtech partners and GCCs
Sushant Rabra Partner and Head-Digital Strategy and Transformation, KPMG in India
management and professionals in the hospital industry.Editorial material addressing this audience would be given preference.
● The articles should cover technology and policy trends and business related discussions.
● Articles by columnists should talk about concepts or trends without being too company or product specific.
● Article length for regular columns: Between 1300 - 1500 words.These should be accompanied by diagrams,illustrations,tables and photographs,wherever relevant.
● We welcome information on new products and services introduced by your organisation for our Products sections.Related photographs and brochures must accompany the information.
● Besides the regular columns,each issue will have a special focus on a specific topic of relevance to the Indian market.You may write to the Editor for more details of the schedule.
● In e-mail communications,avoid large document attachments (above 1MB) as far as possible.
● Articles may be edited for brevity,style, relevance.
● Do specify name,designation,company name,
and CEO, MedLern also highlights that organisations are embedding a culture of continuous learning and using analytics to track competencies, close skill gaps and drive accountability. The shift is clear—training is no longer a one-time exercise, but a strategic lever for improving quality, efficiency and patient outcomes.
As Baruah explains, “the future-ready healthcare workforce will learn continuously, in smaller, faster cycles, embedded within their daily digital environment.”
Expanding reach to underserved India
Technology is also helping bridge the country’s deep workforce and access gaps, particularly in tier 2 and tier 3 cities.
Tandon points out that telemedicine and remote monitoring are “amplifying healthcare reach and productivity in underserved areas.” Digital health IDs, mobile health units, and cloud-based training platforms are allowing specialists to consult, diagnose, and even train staff remotely
department and e-mail address for feedback,in the article.
● We encourage authors to send a short profile of professional achievements and a recent photograph,preferably in colour,high resolution with a good contrast.
Email your contribution to: viveka.r@expressindia.com viveka.roy3@gmail.com Editor, Express Healthcare
cover )
For Sen, “India faces a big healthcare gap as there are more patients in rural areas, while specialists like cardiologists and oncologists mostly work in cities, leaving rural regions with just one doctor for a large population. Technology is the game-changer here. As per the Ministry of Statistics & Programme Implementation, around 86.3 per cent of Indian households have internet access, which means mobile health apps and AI diagnostics are now reaching places doctors physically can’t.”
Masaharu Morita, Founder, NURA-AI Health Screening Centre, agrees that “AI has helped with screening, tele-medicine platforms and remote diagnostics centres which in turn has brought special support to areas with insufficient resources. Moreover, digital up-skilling of frontline staff will help them strengthen their reach and impact. Challenges such as infrastructure, literacy and data governance still exist but with the right combination of tools, training and collaboration eventually we can achieve a more capable and distributed workforce and quality care made available in every corner of the country."
Balancing technologywith empathy
Even as hospitals embrace digital transformation, the soul of healthcare — empathy — must remain intact.
“Technology should amplify not overshadow the human touch in medicine. Hospitals are increasingly training clinicians to use digital tools as supports for empathy and judgment, not substitutes. While AI can analyse data, compassion and intuition remain uniquely human. A balanced approach is encouraged- one that nurtures emotional intelligence, ethical judgment, and patient communication alongside digital proficiency”, says Singh
For Rabra, “Technology should never replace the human connection; it should reinforce it. Human-centered design principles and ethical AI governance ensure that empathy and clinical
judgment remain at the heart of every digital interaction.”
Baruah advocates for a “human-in-the-loop” approach where “AI can draft, summarise, and alert, but clinicians review, add context, and decide”
Dhrubaa Ghosh, Partner, Healthcare, Management Consulting, BDO India, stresses that "High adoption rates of digital health technology are changing how health service delivery is organised. It is paramount that the focus must now shift towards
The shift is clear—training is no longer a one-time exercise,but a strategic lever for improving quality,efficiency and patient outcomes
Deepak Sharma Co-founder and CEO, MedLern
Challenges such as infrastructure, literacy and data governance still exist but with the right combination of tools, training and collaboration eventually we can achieve a more capable and distributed workforce and quality care made available in every corner of the country
Masaharu Morita Founder,NURA-AI Health Screening Centre
Policy-makers need to enable the adoption of technology while maintaining the timeless human element of care-giving in order to shape a sustainable and resilient health systems
Dhrubaa Ghosh Partner,Healthcare,Management Consulting, BDO India
upskilling the health workforce with digital skills, responsible data usage and data-driven decision-making abilities. Fair access to knowledge and skill upgrade opportunities would go a long way towards closing the skill gap, addressing the shortage of manpower and achieving universal health coverage. Policymakers need to enable the adoption of technology while maintaining the timeless human element of care-giving in order to shape a sustainable and re-
silient health systems."
The policyroadmap ahead
As digitalisation accelerates, both workforce management and policy frameworks must evolve in tandem.
Rabra highlights the growing need for new hybrid roles. “As healthcare becomes more digitally integrated, policy frameworks must evolve to recognise new hybrid roles, data stewardship responsibilities, and crossdomain credentialing. There’s a
growing need for frameworks that recognise new job categories such as digital health coordinators and clinical data analysts. The ‘Ayushman Bharat Digital Mission’ has already laid a strong foundation, but scaling this transformation will require ongoing collaboration between policymakers, academia, and industry.”
Similarly, Sharma calls for strong data privacy norms and equitable access, while Baruah stresses the importance of clear regulatory guidance on interoperability and AI accountability.
George explains, “An increasingly digital ecosystem demands major shifts in workforce management: new roles (e.g., digital health specialist, AI-monitoring nurse), continuous reskilling, revised curricula and career paths. Policy implications include data governance, interoperability standards, equitable access and regulatory oversight for AI/automation. The European EIT Health study flagged six domains for action: education/skills, liability/regulation, data quality/governance, funding and reimbursement. In India, policy must also address digital literacy deficits, rural connectivity, and workforce shortages while designing incentives and infrastructure that support tech-enabled care rather than exacerbate disparities.”
Wayforward
India’s healthcare workforce is entering an era where success will depend on how effectively people and technology work together. As Tandon puts it, the clinician’s role is shifting “from task executor to oversight and validation.” In this future, AI will assist, not replace; automation will enable, not alienate; and data will guide, not dictate.
The vision is clear: a digitally competent, empathetic, and adaptive healthcare workforce that uses technology not as a substitute for care, but as a multiplier of its impact.
From cure to prevention: Howdiagnostics is redefining healthcare
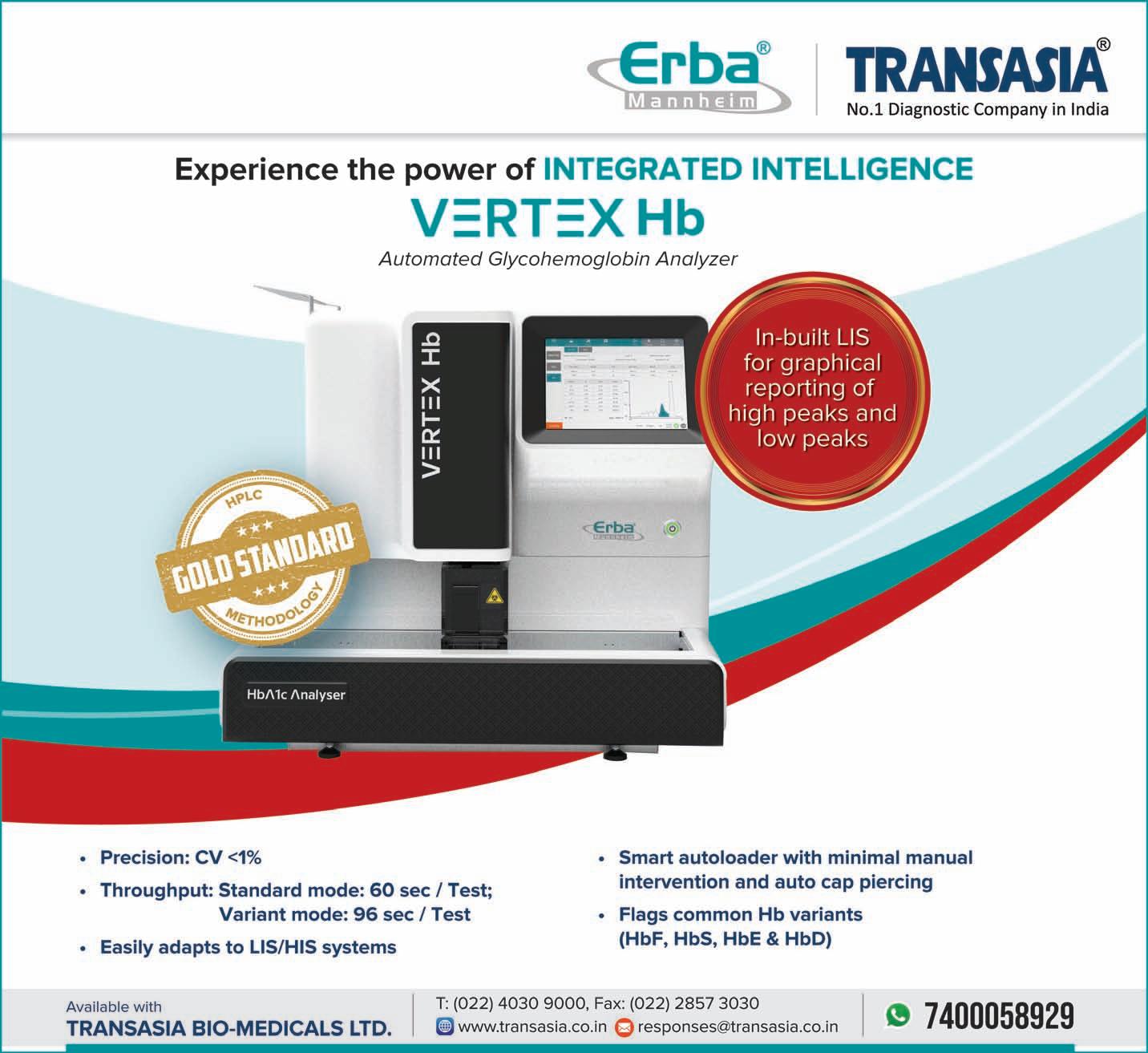
Nishant Saxena, Global CEO,Erba Transasia,explains how scaling screening and early detection can pave the way for a healthier and happier future
The global health landscape is being reshaped by the mounting burden of chronic diseases. According to the International Diabetes Federation, more than 589 million adults currently live with diabetes, a number projected to exceed 850 million by 2050.
Nearly 43 per cent of these individuals remain undiagnosed, silently developing complications that increase the risk of cardiovascular disease, kidney failure, and premature death. Meanwhile, chronic kidney disease (CKD) affects approximately 850 million people worldwide, and cardiovascular diseases (CVDs) continue to claim 17.9 million lives every year, accounting for nearly onethird of global deaths.
Further, hemoglobinopathies such as thalassemia and sickle cell disease, though often overlooked, affect over 300,000 newborns annually, with India representing one of the highest national burdens.
These statistics paint a stark picture: the majority of these diseases develop quietly and are detectable well before symptoms appear. Early testing could p revent millions of avoidable deaths and disabilities each year. Diagnostics, therefore, is not just a clinical tool—it is the foundation of preventive and equitable healthcare.
Diagnostics: The first line of defence Healthcare systems worldwide are shifting from reactive care to proactive health management; prioritising prevention, early detection, and wellness. At the heart of this transformation lies diagnostics. Studies show that nearly 70 per cent of clinical decisions depend on diagnostic insights, yet diagnos-
Healthcare systems worldwide are shifting from reactive care to proactive health management; prioritising prevention,early detection,and wellness.At the heart of this transformation lies diagnostics
tics accounts for less than 5 per cent of total healthcare spending. Strengthening diagnostic access offers a high-impact opportunity to reduce disease burden, healthcare costs, and inequities in care.
Preventive diagnostics allows early identification of risk factors such as elevated glucose, cholesterol, or creatinine levels, well before symptoms appear. It empowers clinicians and individuals to act in time, improving outcomes and quality of life.
Focusing on high-burden diseases
◆ Diabetes and metabolic disorders: Diabetes epitomises the silent progression of disease. Routine glucose and HbA1c testing can identify prediabetes years before complications develop. Incorporating these tests into wellness and community programs helps prevent or delay onset, while reducing healthcare costs—advanced-stage treatment can cost up to ten times more than preventive care.
◆ Hemoglobinopathies: Thalassemia and sickle cell disease remain major public-health challenges, particularly in India. Carrier screening, prenatal
testing, and newborn diagnostics are proven to curb transmission and improve outcomes. School- and community-based screening enables early detection and informed health decisions for families.
◆ Renal health: Chronic kidney disease (CKD) progresses silently until late stages. Simple tests for serum creatinine, eGFR, and urine albumin can detect early dysfunction, enabling timely management and averting costly interventions such as dialysis or transplantation.
◆ Cardiovascular disease: Cardiovascular conditions are the world’s leading cause of death, yet their risks are easily measurable. Lipid profiles, ECGs, and cardiac biomarkers allow identification of high-risk individuals before cardiac events occur. Regular monitoring of blood pressure, glucose, and lipid levels forms the foundation of cardiovascular prevention.
◆ Communicable diseases: While non-communicable diseases dominate global concerns, communicable diseases remain critical. Tuberculosis (TB) continues to affect millions, with India accounting for nearly 28 per cent of global cases. Likewise, sexually transmitted infections such as HIV, syphilis, and hepatitis B and C require regular screening to prevent spread and enable early treatment. Integrating these diagnostics into outreach, antenatal care, and wellness programs ensures a truly comprehensive approach to public health.
From diagnostics to prevention: Asystemic shift
The future of healthcare depends on embedding diagnostics at every level of the system.
Preventive screening must move beyond hospitals into workplaces, schools, and communities. Regular testing should become a habit of wellness—an act of empowerment rather than a reaction to illness.
In India, partnerships between diagnostic providers and government health agencies are already enabling largescale screening for diabetes, anemia, and non-communicable diseases. These collaborations demonstrate how shared responsibility between public health institutions and private partners can bring testing to the last mile, improving outcomes through early detection.
Universal Health Coverage (UHC) in India
India’s commitment to UHC reflects its vision of “Health for All” under the National Health Policy (2017), ensuring equitable access to care without financial hardship. Flagship initiatives like Ayushman Bharat, Health and Wellness Centres (HWCs), and the National Digital Health Mission (NDHM) are transforming primary care through early diagnostics and preventive services.
More than 1.6 lakh HWCs now deliver preventive, promotive, and diagnostic services nationwide—a decisive step toward integrating early detection into public health. The National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases, and Stroke (NPCDCS) has screened over 100 million individuals, making it one of the largest preventive diagnostic initiatives globally. Despite these achievements, challenges remain. Public health expenditure stands at about 2.1 per cent of GDP, while out-of-pocket costs still account
DIAGNOSTICS
for nearly 48 per cent of total spending. Strengthening diagnostic infrastructure, especially in rural and semi-urban regions, is essential to achieving equitable health outcomes. Public–private partnerships (PPPs) are helping bridge these gaps. Collaborations between diagnostic providers and state health departments are expanding affordable testing, enhancing laboratory capacity, and supporting training programs. By integrating preventive diagnostics into national screening efforts, these partnerships are turning UHC’s vision into a practical, scalable reality.
Erba Transasia is aligned with this mission, partnering with governments to build diagnostic capacity, support screening initiatives, and train healthcare workers, thereby creating long-term, sustainable impact across both urban and rural healthcare ecosystems.
From developing the country’s first mobile infectious disease lab (iLAB) during the COVID pandemic to upgrading laboratory networks under the National Health Mission by partnering with public health organisations like Andhra Pradesh Medical Services & Infrastructure Development Corporation (APMSIDC), Assam Medical Services Corporation Ltd., Tamil Nadu Medical Services Corporation Ltd., Telangana State Medical Services & Infrastructure Development Corporation, West Bengal Medical Services Corporation Ltd, Gujarat Medical Services Corporation Limited, besides other bodies and delivered cutting-edge, Made-in-India diagnostic solutions to even the most remote corners of the country.
Emerging trends in preventive diagnostics Laboratory medicine is evolv-
ing rapidly toward automation, data intelligence, and connectivity. Key trends shaping the future include:
◆ Artificial intelligence and predictive analytics, which use large datasets to identify disease risk before symptoms emerge
◆ Point-of-Care Testing (POCT), which brings accurate, rapid diagnostics to primary centers, workplaces, and mobile units
◆ Integrated laboratory networks, linking biochemistry, hematology, and molecular diagnostics for a holistic health view
◆ Digital connectivity, enabling real-time data sharing among clinicians and policymakers for better disease surveillance and targeted interventions
Together, these advances –combined with affordability and accessibility – can make preventive diagnostics a reality for every citizen, not only those
in urban centers.
Conclusion
The future of healthcare will belong to those who diagnose early, act fast, and prevent decisively. By integrating diagnostics into the core of our public health framework and fostering stronger partnerships between government and industry, India can move from reactive care to proactive wellness—turning the vision of Universal Health Coverage into a lived reality for every citizen.
References:
1. International Diabetes Federation. IDF Diabetes Atlas, 10th Edition, 2024
2. World Health Organization. Cardiovascular Diseases (CVDs) Fact Sheet, March 2024
3. International Society of Nephrology. Global Kidney Health Atlas, 3rd Edition, 2023
4. WHO Genetic Disorders Programme. Global Epidemiology of Hemoglobin Disorders, 2023
5. AdvaMedDx / McKinsey & Co. The Value of Diagnostics, 2023
7. Ministry of Health and Family Welfare, Government of India. National Health Policy 2017
8. National Health Authority (NHA)- Ayushman Bharat Digital Mission Dashboard, 2024
9. WHO India. Universal Health Coverage Country Profile: India, 2024
10. Ministry of Health and Family Welfare.National Health Accounts Estimates for India (2024)
11. NPCDCS Progress Report, Directorate General of Health Services, 2024
DIAGNOSTICS
Revolutionising Haematologywith smart automation
Anil
Prabhakaran, Managing Director,Sysmex
India Pvt Ltd,highlights how the XR-1500 is setting new benchmarks in analytical performance,operational efficiency,and patient-centric outcomes for modern laboratories across India
In today’s fast-paced diagnostic landscape, laboratories are seeking intelligent automation that balances speed, accuracy, precision and reliability. Sysmex XR-1500 rises to this challenge representing Sysmex’s latest innovation in haematology automation, engineered to deliver uncompromising analytical performance and workflow excellence.
Driving precision and productivityin modern laboratories
Built on Sysmex’s proven technology Fluorescence Flow Cytometry and enhanced with intelligent workflow automation, Sysmex XR-1500 represents the next generation in haematology automation — designed to deliver faster, smarter, and more reliable results with advanced clinical parameters like reportable NRBC, IG, Ret-He, IPF for laboratories managing high workloads and aiming for precise and accurate results with best TAT.
Smart design,seamless integration
Sysmex XR-1500 is a fully integrated haematology automation system that combines the XR10/20- advanced cell counters with the SP-50 slide maker/stainer for seamless haematology sample processing. It delivers comprehensive CBC and differential analysis with EIP- Extended Inflammatory Parameters and Aged Sample indicator. The analysis profile is extended automatically to include smear-making and staining for desired samples based on the reflex from pre-defined rules based on Cell counter results and or query flags.
Integrated Slide Maker / stainer SP-50 provides Consistent smears with a beautiful cell monolayer that makes further microscopic diagnostics as easy and powerful as possible.
XR-1500’s intelligent workflow automation minimises manual handling and ensures faster turnaround times. With reflex and rerun automation, it enhances laboratory productivity and consistency. The XR-1500 based on modular architecture, allowing laboratories to expand capacity effortlessly as demand grows. Further integrating a digital cell imaging solution, DI-60 with XR-1500, complements and completes the whole CBC analysis by automating microscopy analysis of Peripheral blood smears.
Its intuitive user interface, data integration capabilities, and robust system reliability make it perfect for medium to large laboratories focused on operational efficiency and patient-centric outcomes.
◆ 3D Scattergrams: Improved visualization for better insightful evaluation of results and scattergrams
Aged Sample Identifier
XR-1500’s intelligent workflow automation minimises manual handling and ensures faster turnaround times
(ASI)- Automatically detects aged samples to minimize unnecessary reflex testing and smear reviews. By combining cutting-edge automation with intelligent workflow excellence, XR-1500 enables laboratories to deliver high-quality results faster, supporting better clinical decisions and patient care. XR1500 incorporates intelligent flagging, digital cell imaging connectivity, and automated rerun/reflex testing, significantly reducing manual intervention and turnaround time.
MEDTECH
Over the last three to five years,FUJIFILM India’s healthcare business has delivered strong double-digit growth
Koji Wada, MD,FUJIFILM India Healthcare discusses the company’s growth plans and its vision for inclusive,technology-driven healthcare in India.He shares insights on how AI, localisation and partnerships are reshaping access and innovation across India’s evolving medtech landscape,in an exclusive interview with Lakshmipriya Nair
India’s medtech sector is clearly full of promise. But what do you see as the biggest opportunities and risks on the horizon?
India’s medtech sector is indeed full of promise, and we see tremendous opportunities on the horizon. Domestic manufacturing is at the forefront, with government initiatives like the PLI scheme creating a strong ecosystem for local production of both consumables and advanced diagnostic equipment. This aligns well with our own longterm “Make in India” vision. The integration of digital health and AI-powered diagnostics represents another major opportunity, enabling early detection, improved accuracy, and affordable access, particularly in Tier 2 and Tier 3 cities where FUJIFILM India has already built scale, with over 79,000 imaging systems and strong service support.While there is immense potential of growth, at the same time, the sector must navigate certain challenges. Regulatory frameworks for AI-based healthcare are still evolving, and clarity on data governance and privacy will be critical to ensuring trust. As digital devices proliferate, cybersecurity and supply chain resilience require sustained focus. We see these not as obstacles but as opportunities for closer
collaboration between industry, government, and academia. By strengthening quality standards, enhancing local capabilities, and investing in talent, India can address these challenges and set global benchmarks. For FUJIFILM India, our
commitment remains to bring inn ovative, AI-enabled, and inclusive healthcare solutions that support India’s ambition of becoming a world leader in medtech.
India has a mix of strong homegrown manufacturers
and global players like Fujifilm. How can international companies contribute to shaping the ecosystem here without overshadowing local innovation?
International medtech companies have a critical role to play in strengthening India’s healthcare ecosystem, and this can be achieved in ways that empower, rather than overshadow local innovation. The most effective approach lies in partnership, collaborative R&D, technology transfer, and co-development of products tailored to India’s unique needs. At FUJIFILM India, for example, initiatives like the NURA Global Development Centre in Kozhikode demonstrate how international expertise can combine with local talent to build scalable solutions for preventive healthcare. Such collaborations not only accelerate innovation but also build skills and knowledge pipelines that benefit India and global operations alike.
Equally important is supporting the startup ecosystem through funding, mentoring, and incubation, giving young inn ovators access to advanced technology, regulatory knowhow, and global networks. By localising manufacturing and building Global Capability Centres, international players also create jobs,
expand domestic supply chains, and el evate India’s export potential. Moreover, sharing best practices in compliance, quality, and sustainability helps Indian innovators compete on global standards.
The key is to ensure partnerships are designed to amplify Indian ingenuity, through joint initiatives, reverse innovation, and alignment with 'Make in India' and 'Atmanirbhar Bharat.' This way, international companies contribute global scale and expertise while creating an ecosystem where homegrown innovation thrives alongside global excellence, positioning India as a true medtech leader
AI in imaging is already improving speed and accuracy. But beyond efficiency, what kinds of new care models or possibilities can AI open up for India’s healthcare system?
AI in imaging is already enhancing speed and accuracy, but its true potential lies in reshaping care models and expanding access to quality healthcare across India. One of the most promising avenues is largescale p reventive screening. AI-powered tools are enabling population-level detection of diseases like tuberculosis and cancer, even in rural areas where
radiologists are scarce. This has the potential to shift India’s healthcare system from reactive treatment to proactive prevention, improving outcomes and reducing long-term costs.
AI is also transforming rural telehealth and remote diagnostics. By integrating imaging with telemedicine platforms, scans can now be interpreted by experts hundreds of miles away, bringing specialist-level care to underserved communities and bridging the urban–rural divide. Beyond access, AI’s predictive capabilities are powering population health management, helping identify high-risk patients earlier and reducing avoidable hospital admissions.
Looking ahead, AI can unlock more personalised treatment by combining imaging with genetic and clinical data, tailoring therapies to each individual’s needs. Privacy-preserving models such as federated learning are further enabling collaboration among hospitals while protecting sensitive patient data. Importantly, these technologies also empower the clinical workforce by automating repetitive tasks, allowing scarce medical expertise to focus on complex cases.
For India, this means AI is not just about efficiency, it is about enabling new, inclusive, and patient-centric care models that bring advanced diagnostics and preventive medicine to every corner of the country, reinforcing the vision of equitable healthcare for all.
Advanced diagnostics often don’t reach rural and underserved areas. In your view, what models of decentralised healthcare can make the biggest difference? Can you share some examples?
Decentralised healthcare models are essential to closing the gap between advanced diagnostics and rural populations, where geography and
infrastructure often limit access. Mobile medical units (MMUs) equipped with advanced diagnostic technologies are emerging as a powerful solution. For example, in Himachal Pradesh’s Mandi district, a programme by FUJIFILM India, combines static diagnostic centres with fully equipped mobile van covering nearly 3,950 sq km, bringing critical services such as portable X-rays and on-the-spot clinical chemistry testing directly to communities. This approach enables early detection of
Tier 3 cities is that access challenges can be overcome with the right blend of technology, service, and partnerships. The company’s success has been anchored in building a robust nationwide service and application support network, ensuring high equipment uptime, rapid repairs, and continuous clinician training. This reliability has been critical in regions where infrastructure and expertise are limited. Another key learning is the importance of partnerships: by working closely with state health departments, private
shaping up in areas like CT, MRI, and digital radiography?
Over the last three to five years, FUJIFILM India’s healthcare business has delivered strong double-digit growth, with some segments emerging as clear frontrunners. CT and MRI systems have been among the fastest-growing areas, particularly in tertiary hospitals and advanced diagnostic centres, where their clinical accuracy, compact design, and cost efficiency have driven rapid adoption. Endoscopy has also
One of the biggest lessons from FUJIFILM India’s journey in India’s Tier 2 and Tier 3 cities is that access challenges can be overcome with the right blend of technology,service and partnerships
diseases like tuberculosis and COPD, helping patients access timely care without long and costly travel. The model also integrates tele-radiology and teleconsultation, allowing patients in remote locations to benefit from expert radiology readings and doctor consultations virtually, overcoming the shortage of specialists in rural areas. By blending mobile outreach with fixed facilities, it ensures both sustainability and wide reach. If scaled to other remote and difficult terrains, such technology-driven, community-focused initiatives have the potential to transform rural healthcare delivery, making sophisticated diagnostics more inclusive and accessible across India.
FUJIFILM has built a strong presence in tier-2 and tier-3 cities. What lessons from this journey could be applied to other emerging markets that face similar healthcare access challenges?
One of the biggest lessons from FUJIFILM India’s journey in India’s Tier 2 and
diagnostic chains, and NGOs, FUJIFILM India has been able to decentralise its customer base and expand adoption in underserved regions.
Equally important is tailoring solutions to local needs. CT and MRI systems, portable X-ray units like FDR Xair, and AI-powered platforms have been designed to deliver high clinical accuracy while remaining accessible for smaller hospitals and diagnostic centres. Finally, linking technology with social impact, such as largescale TB and breast cancer screening programmes, has built trust and reinforced the role of advanced diagnostics in public health. These lessons underscore that emerging markets benefit most when global inn ovation is paired with local customisation, robust support infrastructure, and community-driven healthcare models.
Over the last three to five years, which areas of FUJIFILM India’s healthcare business have grown the fastest? And how do you see competition
seen remarkable momentum, recording over 30 per cent year-on-year growth for the last three years and establishing India as one of the fastest-growing global markets for Fujifilm’s endoscopy business. In digital radiography, portable X-ray solutions such as the FDR Xair have gained significant traction in both urban and rural healthcare setups, further strengthening Fujifilm’s leadership in the segment. As competition intensifies in CT, MRI, and radiography, we see it as a positive force that will expand the market, accelerate innovation, and improve access. Fujifilm’s differentiator lies in combining cutting-edge technology with a strong nationwide service network and deep presence in Tier 2 and 3 cities. By focusing on AI-powered solutions, localized support, and partnerships across public and private health systems, we believe we are well positioned not just to maintain leadership, but to expand the role of advanced diagnostics in strengthening India’s healthcare infrastructure
Public health in India is focused heavily on NCDs and infectious diseases. What more can the devices industry do to support those priorities? Where does Fujifilm see its role in that bigger picture?
Non-communicable diseases (NCDs) and infectious diseases remain India’s most pressing public health priorities, and the devices industry can play a vital role in addressing both by enabling early detection, improving access, and supporting large-scale screening. Portable diagnostic tools backed with teleradiology, for example, make it possible to conduct mass screenings for tuberculosis, advanced technology for breast cancer, and cardiovascular diseases, even in Tier 2 and Tier 3 cities where specialist availability is limited. By focusing on solutions that are accurate, and easy to deploy, the industry can help shift the system from reactive care to proactive, preventive healthcare.
Fujifilm sees its role as being an enabler of this transformation. Through innovations such as the FDR Xair portable X-ray, CAD EYE in endoscopy, and Synapse AI platform in radiology, we are supporting programmes that detect TB, cancers, and other highburden diseases at scale. Our partnerships with state health departments, NGOs, and diagnostic chains have allowed us to decentralise care delivery and extend advanced diagnostics to underserved populations. Looking ahead, we aim to build further on these models by expanding preventive healthcare initiatives, strengthening AI-enabled solutions, and aligning with national health missions, so that technology not only supports but accelerates India’s journey towards reducing the burden of NCDs and infectious diseases.
India’s Rising MedTech Export Story: From Reliable Partner to Global Powerhouse
Aaryaman Baid, Lead- International Strategy,Poly Medicure Ltd stresses that while tariffs have created temporary barriers,they have also spurred Indian companies to diversify markets, strengthen competitiveness, and focus on sustainable long-term growth
India’s medical device sector is quietly scripting one of the most promising chapters in the country’s export story. Once viewed largely as a domestic industry serving local healthcare needs, Indian medtech is now emerging as a reliable and competitive partner for global markets. Even in the face of recent tariff challenges including those imposed by the United States the sector continues to demonstrate remarkable resilience, underpinned by innovation, quality manufacturing, and growing global trust.
India’s medical device exports have maintained a steady upward trajectory despite global trade disruptions and protectionist policies. The sector’s resilience lies in its unique ability to blend cost-effectiveness with uncompromised quality, a balance that global buyers increasingly value. From single-use disposables and consumables to high-end diagnostic and therapeutic technologies, Indian manufacturers are today meeting international benchmarks of safety and performance.
While tariffs have created temporary barriers, they have also spurred Indian companies to diversify markets, strengthen competitiveness, and focus on sustainable longterm growth. Value engineering, robust quality management systems, and collaborative partnerships are becoming the new pillars of India’s export strategy.
A significant global realignment is now underway. Europe’s conscious move to reduce dependence on Chinese suppliers including new mandates restricting Chinese medical devices in public procurement above certain value thresholds has opened a rare window of opportunity for India.
Asignificant
global
realignment is now underway.Europe’s conscious move to reduce dependence on Chinese suppliers including new mandates restricting Chinese medical devices in public procurement above certain value thresholds has opened a rare window of opportunity for India
This shift is not just commercial but geopolitical. Global buyers are increasingly seeking partners who offer reliability, transparency, and neutrality.
India fits that profile perfectly. With a strong manufacturing base, skilled technical talent, and a maturing regulatory ecosystem, the country is well
positioned to fill the gap left by China’s waning dominance in the medtech space.
The European market, known for its exacting standards and preference for quality over cost, is now beginning to view India as a credible alternative, a shift that could redefine global medical supply chains over the next decade.
To fully seize this moment, India must strategically integrate diplomacy into its trade narrative. Economic diplomacy through health partnerships, bilateral agreements, and government-to-government collaborations can help unlock new markets across Latin America, Africa, Eastern Europe, and Southeast Asia.
A critical enabler here would be mutual recognition of certifications and standards, which currently remain a significant barrier for small and midsized manufacturers. India’s diplomatic channels, export promotion councils, and trade missions can work in sync to build trust and visibility for Indian medtech globally.
Embassies, too, can serve as brand ambassadors curating exhibitions, buyer-seller meets, and health dialogues that position India not merely as a lowcost producer, but as a partner of choice for quality healthcare technologies.
The “Brand India” narrative in medtech needs to evolve beyond affordability. The focus must now shift to innovation, reliability, and clinical efficacy. Indian companies are already demonstrating global excellence in diverse categories from infusion therapy and renal care to critical care and minimally invasive surgery.
While large international expos such as Arab Health and MEDICA continue to be vital platforms, India’s presence
must expand to key regional exhibitions that bring together focused buyers from Africa, ASEAN, Latin America, and Central Asia. Consistent participation across these forums can reinforce India’s credibility and help forge new partnerships in emerging markets.
Despite India’s strong fundamentals, a barrier for many smaller manufacturers remains the prohibitive cost of international certifications such as CE marking and FDA approvals. A well-structured government incentive or subsidy framework to offset these expenses could be a game-changer enabling more local players to tap into global demand.
Equally important is the need for knowledge-sharing within the ecosystem. Established MedTech Export Champions can mentor emerging manufacturers, guiding them through global regulatory landscapes, market access pathways, and distribution strategies. Such mentorship networks could accelerate capability building and foster a culture of collaboration rather than competition.
India’s evolution from an import-dependent market to a global medtech exporter is a story of persistence, innovation, and purpose. The next phase of this journey will depend on stronger industry-government collaboration focused on policy support, brand building, and global outreach.
As the world seeks to rebalance healthcare supply chains for greater resilience, India stands at a strategic inflection point. With the right mix of diplomatic engagement, targeted incentives, and ecosystem collaboration, the Indian medical device sector can truly emerge as a $10-billion export powerhouse.
MEDTECH
Reimagining medical imaging: HowTruevis is making PET-CTaccessible across India
From Manufacturing excellence to Customer service innovations,Truevis Technologies is driving India’s Medtech innovation and manufacturing infrastructure
Transforming access, empowering care
India’s healthcare landscape is undergoing a pivotal transformation — one that demands not just world-class technology but also localised capability, reliability, and reach. Leading this change from the country’s eastern coast is Truevis Technologies, a MedTech innovator housed within the Andhra Pradesh MedTech Zone (AMTZ) in Visakhapatnam.
Building on its strength in CT and PET-CT manufacturing, Truevis is now redefining the next frontier: making highend imaging accessible, affordable, and sustainable across India.
Milind Deshpande, Joint Managing Director, Truevis Technologies: “Our mission goes beyond machines — it’s about empowering every clinician and hospital to deliver precision care with confidence by making high technology equipment within the reach.”
Empowering people,driving precision
At the core of Truevis’s success lies a team that blends technical mastery with purpose. Engineers, clinical specialists, and service professionals — many with decades of experience in global imaging companies — form the foundation of its innovation ecosystem.
Through structured training programs and technology transfer initiatives with global partner Neusoft Medical Systems, Truevis ensures to bring home global designs and service expertise.
The Truevis Experience & Training Centre at Visakhapatnam takes this further by offering clinicians and biomedical engineers hands-on exposure to PET-CT systems, software platforms, and image analytics — transforming technology
At the core of Truevis’s success lies a team that blends technical mastery with purpose.Engineers, clinical specialists,and service professionals — many with decades of experience in global imaging companies — form the foundation of its innovation ecosystem
adoption into true clinical empowerment.
World-Class manufacturing with qualityand compliance
Truevis facility is planned to ensure that every PET-CT and CT system undergoes rigorous performance, safety, and reliability validation in compliance with the quality standards and regulatory requirements. This includes testing the performances including accuracy and safety requirements. In addition, Truevis aligns its design and testing standards with local and global guidelines, ensuring traceability, risk management, and long-term device
reliability.This robust framework not only ensures global quality parity but also instils confidence among hospitals and regulators alike — a critical foundation for scaling MedTech manufacturing in India.
Service that sustains performance In imaging diagnostics, uptime defines trust. Truevis’s service is modelled to ensure hospitals experience minimal downtime through a proactive, technology-driven approach.
This includes a 24×7 Command and Control Centre monitors installations nationwide, supported by AI-based predictive maintenance that identi-
fies potential issues before they impact operations.
With regional service hubs across India, Truevis guarantees rapid on-site response and continuity of care — creating a new gold standard in MedTech service delivery.
Dharmendra Kumar, Director, Truevis Technologies: “Reliability is our biggest product. Every scan, every patient, every uptime minute counts.”
Expanding PET-CTaccess across India
PET-CT imaging has revolutionised oncology care globally, yet India’s penetration remains limited — concentrated in metro hospitals. Truevis is
bridging that gap through its PET-CT, a system engineered to combine digital imaging precision, operational simplicity, and cost efficiency.
Manufactured and serviced entirely within India, the it enables Tier-2 and Tier-3 hospitals to deploy world-class imaging systems, bringing cancer diagnostics closer to underserved communities.
This initiative directly supports Ayushman Bharat and the Make in India vision, positioning Truevis as a driving force behind India’s MedTech self-reliance.
Engineering the future of imaging
Looking ahead, Truevis is integrating AI-driven image analytics, cloud connectivity, and data-backed maintenance to enhance diagnostic accuracy and service transparency. By merging innovation, skill, and national purpose, Truevis Technologies is reimagining what accessible healthcare truly means — transforming India’s imaging landscape from dependency to self-sufficiency.
Truevis at a Glance
◆ Manufacturing Facility: Andhra Pradesh MedTech Zone (AMTZ), Visakhapatnam
◆ Key Partnership: Neusoft Medical Systems (China)
◆ Focus Areas: Manufacturing, Service Network, AI-enabled Imaging
◆ Vision: “Made in India, Designed for the World”
HEALTHCARE IT
INTERVIEW
AI is going to be a keyenabler in our future roadmap
In an interaction with Express Healthcare, Guruswamy K, CEO,BPLMedical Technologies, shares how the company is balancing its rich legacy of innovation with a future-focused approach driven by R&D,AI integration,and digital health solutions
BPL is a household name in India, especially remembered for introducing the country’s first in-house ECG machine back in 1967. How do you balance this legacy while staying relevant in today’s fast-evolving MedTech landscape?
Introducing India’s first indigenous ECG machine in 1967 was a defining milestone and continues to inspire us. For us at BPL MedTech, legacy is not just about looking back but about building forward. We leverage the trust and credibility built over decades while staying agile and futureready through continuous R&D, new product introductions, and digital health innovations. This balance between heritage and innovation is what keeps us relevant in today’s rapidly evolving MedTech ecosystem.
BPL Medical Technologies just completed 12 years in its current form. What would you highlight as the company’s biggest inflection point in this journey so far? Since 2013, BPL Medical Technologies has grown steadily, but the true inflection point came when we strengthened our R&D and manufacturing base in India. The decision to design and produce “Made in India” solutions at scale was transformative. It positioned us as a credible domestic leader while opening new opportunities in exports and partnerships, helping us accelerate growth.
You’ve doubled down on “Made in India” products at a time when the government is pushing the PLI scheme. Can you share specific areas where BPL has gained a competitive edge through
Since 2013,BPLMedical Technologies has grown steadily, but the true inflection point came when we strengthened our R&D and manufacturing base in India.The decision to design and produce “Made in India” solutions at scale was transformative
local manufacturing?
Our advanced facilities in Bengaluru and Palakkad give us complete control over the value chain, from design to quality testing. By producing locally, we are able to customise devices for Indian demographics, ensure affordability, and reduce dependence on imports. ECG machines, patient monitors, and X-ray systems are great examples of products engineered specifically for Indian conditions, which gives us a clear edge in pricing, usability, and long-term sustainability.
Do you see India truly emerging as a global hub for medtech manufacturing, or are there systemic gaps that still need to be addressed? India has the potential to truly emerge as a global medtech hub, backed by its strong talent base, manufacturing capabilities and government initiatives such as the Production Linked Incentive (PLI) scheme. At the same time, there are systemic challenges that need attention such as harmonising regulations, strengthening the supply chain and sustaining higher levels of R&D investment. Encouragingly, new measures are being introduced including the Promotion of Research and Innovation in Pharma MedTech (PRIP) Scheme, which aims to boost R&D, and the Strengthening of Medical Device Industry (SMDI) Scheme, which supports clinical studies and industry advancements. With this continued policy support and industry focus, India is well positioned to become a key player in the global medtech supply chain.
BPL has hinted at expanding
its R&D focus, including AIenabled medical devices. Could you share what categories or devices we can expect AI integration in first?
AI is going to be a key enabler in our future roadmap. We are initially focusing on diagnostic and monitoring devices where AI can make the most immediate impact. For example, AI-enabled imaging systems such as X-rays are areas where we see significant scope to enhance accuracy, reduce clinician workload, and enable faster clinical decisionmaking.
How does BPL approach balancing affordability and cutting-edge innovation, especially for markets like rural India?
For us, affordability and innovation are not contradictory goals. By designing in India for India, we ensure world-class technology is accessible at price points that work for both urban and rural healthcare providers. Our focus in rural healthcare has been on portable, easy-touse devices that don’t compromise on quality but remain cost-effective, ensuring that advanced medical technology reaches the last mile.
With more medtech companies moving into digital health, where does BPL see itself, are you exploring remote monitoring, connected devices, or telemedicinelinked hardware?
We have already entered the digital health ecosystem with the launch of BPL iCare OT, a state-of-the-art OT charting software application that automates OT documentation process and improves
efficiency. Furthermore, our upcoming digital solutions in radiology and ICU care will extend these benefits across departments, enabling hospitals to seamlessly integrate patient data, enhance clinical decisionmaking, and optimise resource utilisation. These innovations are part of our larger vision to build a fully connected care ecosystem, where technology supports clinicians at every step of the patient journey while driving better outcomes and operational excellence.
Data is becoming as important as devices. Does BPL have plans to create its own digital ecosystem around your hardware, or will you remain primarily a device manufacturer?
Devices will always remain at the core of our business, but we have moved beyond being only a device provider. We are steadily building a digital
health ecosystem that complements our hardware and addresses the evolving needs of hospitals and caregivers. We’ve recently introduced BPL iCare OT, which streamlines operating theatre workflows. Building on this, we are working on other AI-integrated models, which will extend the same benefits of remote monitoring, data integration, and advanced analytics into intensive care and radiology departments. With these solutions, our vision is to ensure that our devices are not standalone units but part of an integrated digital ecosystem that improves clinical outcomes and makes healthcare delivery smarter and more efficient.
The Indian medtech market is growing at nearly 15 per cent annually, and several startups are emerging alongside global players. How does BPL differentiate
itself in such a competitive landscape?
Our differentiation lies in three things; heritage of trust built over five decades, one of the strongest service networks in the country, and a balanced portfolio that caters to both premium hospitals and costsensitive rural markets. This combination of scale, trust, and accessibility is not easy to replicate and sets us apart in a crowded market.
You’ve built one of the largest service networks in the country. Is this an underappreciated advantage when competing with newer medtech entrants?
Yes, it is often an underappreciated advantage. While newer medtech entrants may bring products, building a strong service backbone takes years of commitment and investment. At BPL MedTech, we are not just supplying medical devices,
we act as a reliable partner to hospitals and healthcare providers. If any issue arises post-purchase, our extensive service network, backed by trained engineers and trusted channel partners, ensures quick support. This ability to stand by our customers consistently across the country gives us a distinct edge in the market and reinforces why so many institutions continue to rely on us.
What are the next 2–3 product categories or solutions that will define BPL Medical Technologies in the coming decade?
The next decade for BPL Medical Technologies will be defined by AI-driven diagnostic and monitoring solutions, advanced imaging technologies such as ultrasound and X-ray systems, and connected devices that bring digital health into both
home and hospital care. These categories will shape our future portfolio and growth strategy.
If I were to ask you for one exclusive announcement today, whether it’s an upcoming launch, new partnership, or breakthrough in AI/IoT, what would that be?
BPL MedTech has long been trusted by leading healthcare institutions across India for our reliable medical devices and strong service support. Building on this legacy, we have already introduced BPL iCare OT and are soon extending the ecosystem with digital solutions in radiology and ICU care. With this digital ecosystem, we are confidently moving from being a trusted device provider to delivering an integrated digital health ecosystem, combining our hardware expertise with smart, connected solutions.
START-UPS
India ensuring culturallycontextual AI requires a fundamental shift
Tanisha Sheth and Dr Anirudh Anilkumar, Co-founders and Board Members of the Behtar Healthcare Foundation,in an interaction with Kalyani Sharma talks about their vision to make technology work for every citizen,not just a privileged few.They discuss how their foundation positions AI as public infrastructure,the systemic gaps in India’s digital health landscape,and the need for culturally contextual,open,and equitable digital health frameworks that empower communities rather than merely serve them
What inspired the creation of the Behtar Healthcare Foundation, and can you tell us more about its mission and team?
Tanisha Sheth: The Behtar Healthcare Foundation was created to fix what we kept seeing across India’s healthcare system: powerful technology exists, but it rarely reaches the people who need it most. We were incubated at EkStep Foundation’s People+AI initiative, which is part of Nandan Nilekani’s broader mission to enable societal-scale change through open technology. Nearly 70 per cent of Bharat lives in rural areas, yet less than 30 per cent of doctors serve these regions. Treatment gaps for chronic conditions range between 40–70 per cent. While existing frameworks focus on testing AI against medical benchmarks, new frameworks need to be created around real-world patient care. To this effect, we’re lucky to have a team that bridges a lot of these disparate worlds – Dr Anirudh Anilkumar, who is a physician-scientist with a background in clinical AI research, Luv Singh, who has built AI systems that deliver care in the last mile, across formats and languages, Shashwat Shukla who has grown non-profits from the ground up, Dr Raunaq Pradhan who worked extensively on Ayushman Bharat Digital Mission (ABDM) at the National Health Authority and brings insights into public health ecosystems, and Parul Aggarwal who is a digital health
strategist and has built India’s largest healthcare community. Our collective experience connects us deeply to India’s innovation ecosystem—across IITs, IISc, and national health organisations—allowing us to bridge academic, institutional, and implementation networks.
Behtar positions AI as public infrastructure rather than a proprietary solution. Could you explain how this approach changes the way digital health innovation and impact are measured?
Dr Anirudh Anilkumar: When you treat AI as public infrastructure rather than a proprietary product, you fundamentally shift how impact is measured — and who gets to measure it.
Traditional health-tech metrics focus on control with metrics like MAUs, revenue and data ownership. Public infrastructure metrics focus on ecosystem leverage: How many organisations can build on this foundation? How quickly do solutions spread beyond our direct reach? Do communities gain agency over the technology, or remain dependent on us?
Let me give you a concrete example. When PhysicsWallah needed mental health support for their students, they didn't become "customers" or wait for our capacity. They took our open-source frameworks, customised them, and reached hundreds of thousands of users within weeks. In a traditional business model, that would be
"lost market share." In an infrastructure model, it's proof the system works.
This changes three things:
First, scale is measured differently. Our direct reach through Sukoon might be tens of thousands. But when you count everyone reached through adaptations — PhysicsWallah, VOPA, and organisations we don't even know about yet — the impact becomes exponential. One tool becomes ten solutions.
Second, sustainability is measured differently. A proprietary health app dies when the company shuts down or funding ends. Public infrastructure persists because multiple actors have stakes in maintaining it. If Behtar disappeared tomorrow, the
code would remain, and organisations could continue building.
Third, equity is measured differently. In traditional models, serving "unprofitable" populations (rural, low-income, non-English speakers) is a CSR activity at best. In infrastructure models, designing for those furthest from access becomes the core strategy — because when you design for rural Bihar first, solutions that work everywhere emerge naturally.
One of the challenging things for us is creating good frameworks for measuring infrastructure impact yet. They want to know "How many users does Behtar have?" when the right question is "How many users can the ecosystem serve
TanishaSheth
DrAnirudhAnilkumar
because Behtar exists?" We're still learning how to make that case compellingly.
India’s digital health ecosystem has grown rapidly, but access and usability remain uneven. In your view, what are the systemic gaps preventing equitable digital transformation in healthcare?
Sheth: The gaps preventing equitable digital health in India aren't primarily technical — they're systemic, cultural, and rooted in how power and resources are distributed.
First, the infrastructure divide. We talk about "digital health for all" while assuming stable internet, smartphones, and digital literacy. An ASHA worker managing 1,000 households with a feature phone and intermittent connectivity can't use tools designed for urban clinics. The technology exists, but it's designed for the wrong context.
Second, the trust deficit. Communities have watched tech pilots come and go, extracting data without delivering sustained value. When you've been a research subject multiple times with nothing to show for it, skepticism isn't irrational — it's learned. Digital health tools often feel like surveillance, not service.
Third, the language and cultural gap. Most health tech operates in English, assumes Western clinical models, and ignores the cultural contexts through which Indians navigate healthcare — caste, gender, stigma, traditional medicine. A mental health chatbot that can't understand why someone would consult an astrologer before a psychiatrist isn't contextually intelligent, no matter how sophisticated the AI.
Fourth, fragmentation masquerading as innovation. Every hospital, NGO, startup, and state program builds isolated systems that don't talk to each other. There's no shared infrastructure, so we keep reinventing wheels while patients fall through the cracks between silos.
The systemic gap isn't that India lacks digital health
innovation — it's that innovation serves the 30 per cent who already have access, while ignoring the 70 per cent who need it most.
So the question then becomes what would equitable digital transformation actually require?
◆ One: Invert the design priority. Start with the hardest contexts — low-literacy, lowbandwidth, non-English speakers — and build up, not down. When you design for feature phones in rural Jharkhand, the solution also works for smartphones in Bangalore. The reverse isn't true.
◆ Two: Build shared infrastructure, not competing solutions. India doesn't need fifty different hospital management systems. We need interoperable building blocks that any health actor can use — like UPI did for payments. This requires policy frameworks that incentivise collaboration over competition.
◆ Three: Make data governance participatory, not extractive. Communities should decide how their health data is used, who benefits from AI trained on it, and what value flows back to them. Right now, data flows from villages to venture capitalists with nothing in return.
◆ Four: Invest in the "last mile" — not just the technology, but the change management, training, and trust-building needed for adoption. The most sophisticated AI tool is useless if frontline workers don't understand it, don't trust it, or find it adds burden instead of reducing it.
It is not about "How do we bring digital health to underserved communities?" It's "How do we ensure underserved communities shape, own, and benefit from digital health on their terms?"
AI in healthcare is often criticised for being exclusionary or “imported” in design. How can India ensure that AI tools are culturally contextual, accessible, and ethically deployed?
Dr Anilkumar: India ensuring
culturally contextual AI requires a fundamental shift: communities must move from being data sources to decisionmakers in how AI is built, deployed, and governed.
Three principles matter:
Co-creation from day one. At Behtar, every tool begins with extensive needs assessments with the people we're building for — patients, ASHAs, doctors. When we built Sukoon, students told us WhatsApp felt too public for mental health conversations. We rebuilt for web. That pivot only happened because users had veto power over our assumptions.
Transparent explainability. "This AI is 95 per cent accurate" means nothing to an ASHA worker. What matters is: "This tool asks three questions to help you decide if a patient needs urgent care." Cultural context means explaining why the AI suggests something, in language that respects local health-seeking behaviors.
Open-source as accountability. When our code is public, anyone can verify we're not encoding bias, misusing data, or making clinically unsafe decisions.
Transparency isn't just ethical — it's how you build trust in communities that have been burned by opaque technology before.
The hard truth? Most AI deployed in India today is "imported" not because it's technically foreign, but because it's designed without Indian communities at the table. Until we fund community-led AI development — not just community consultation — we'll keep building tools that work in theory but fail in practice.
What does "culturally contextual" actually look like in practice?
◆ Language is the obvious starting point, but it's not enough. Sukoon works in 12+ Indian languages, but that's table stakes. Cultural context means understanding that a Marathi-speaking widower might describe depression as "mann bhaari aahe" (heavy heart), not medical terminology. It means recognising that someone might seek both a therapist and a temple priest —
and that's not "noncompliance," it's holistic care.
◆ Accessibility means designing for constraints, not ideal conditions. We build for feature phones because that's what most Indians have. We design for low literacy using voice interfaces. We assume intermittent internet and offline functionality. These aren't "nice-to-haves" — they're baseline requirements if you're serious about equity.
Ethical deployment means answering hard questions upfront:
◆ Who owns the data generated by this AI?
◆ Who benefits economically if this AI scales?
◆ What happens when this tool makes a mistake — who is accountable?
◆ Can users opt out without losing access to care?
Here's an example of what happens when you get it wrong: A mental health chatbot deployed in rural Karnataka used direct translation from English. It asked users to rate their mood on a scale of 1-10.
Most users abandoned it within minutes — not because they didn't understand the language, but because the concept of quantifying emotions felt alien. The tool is linguistically translated but culturally tonedeaf.
India ensuring contextual AI requires:
◆ Policy: Mandate that public health AI tools undergo "cultural validation" the same way drugs undergo clinical trials. Does this tool work for the communities it claims to serve?
◆ Funding: Redirect grants toward community-led AI development, not just extraction of community data for AI training.
◆ Governance: Create participatory frameworks where affected communities have decision-making power over AI deployment — not just consultation rights.
The goal isn't "AI with an Indian accent." It's AI shaped by Indian communities' lived realities, owned by them, and accountable to them.
Open-source models are well established in software but
still nascent in healthcare. What are the opportunities and potential risks of applying open-source principles to digital health tools?
Dr Anilkumar: Open source in healthcare turns innovation into a shared public good. The opportunity lies in speed, transparency, and equity—if one team builds a triage algorithm or therapy chatbot, others shouldn’t have to start from scratch. It makes progress compounding.
The risk, of course, is misuse or loss of clinical quality and all the different challenges that come along with working in such a sensitive industry.
◆ Fear of liability. Software bugs are fixable. Healthcare mistakes can kill people. This makes organisations rightfully cautious about opening their code for modification.
◆ Misaligned incentives. In software, open-source thrives because companies make money on services, not licenses (Red Hat, etc.). In healthcare, the revenue model is still "sell the product," so open-sourcing feels like giving away the business.
◆ Regulatory ambiguity. India's medical device regulations weren't written with open-source in mind. It's unclear how liability, approval processes, and quality standards apply when code is collaboratively developed and modified.
The way forward is opensource with governance — a commons, not a free-for-all. India can learn from OpenMRS, DHIS2, and OpenSRP, and newer collaborations like BioPeak or Longevity@IISc, which show how open ecosystems thrive when research, implementation, and policy share stewardship.
India needs more longhorizon consortia — joint university–industry–state initiatives that maintain shared models, datasets, and evaluation frameworks over time. That’s why at Behtar, we publish our work with context— what worked, what failed, and why—so that others can adapt safely, not blindly with a sense of shared responsibility.
START-UPS
Public–private collaboration is critical for building sustainable digital health ecosystems. What kind of partnerships or policy frameworks are needed to make such collaborations effective in India?
Sheth: We believe that effective digital health collaboration must follow the Samaaj–Sarkaar–Bazaar balance — where civil society, state, and market each play their part.
◆ Sarkaar (State): Fund base infrastructure — datasets, APIs, consent frameworks, and open rails. The cost of public infrastructure must be borne publicly.
◆ Samaaj (Civil Society): Act as the ethical steward — shaping governance, protecting inclusion, and building trust.
◆ Bazaar (Private Sector): Build sustainable innovations, business models, and managed
services on top of open rails.
Policy enablers include:
◆ Open-first procurement, mandating APIs and preventing lock-in.
◆ Regulatory sandboxes for faster testing and validation.
◆ A Commons Maintenance Fund to sustain open infrastructure and shared datasets.
The state builds the rails, society keeps them fair, and the market keeps them alive — together making digital health not just scalable, but sustainable.
Behtar’s initiatives like Project Sukoon and the AIfor-Therapists pilot aim to bridge mental health and technology. What early insights or challenges have emerged from deploying these open-source tools in realworld settings?
Sheth: Our biggest learning has
been that technology isn’t the hardest part—trust is.
When we piloted Sukoon, an open-source mental health chatbot for college students, we learned early that usability was more emotional than technical. Students told us WhatsApp— our initial interface—felt too crowded for therapy conversations; many associated it with family or academic groups. They preferred a standalone web app, which gave them emotional distance and a greater sense of privacy. That single design shift dramatically improved engagement.
Over 600 students from IIT Kanpur participated in our early testing phase, offering structured feedback that shaped Sukoon’s tone, flow, and accessibility. The project has since been adapted by the Maharashtra nonprofit VOPA, reaching more than 50,000 users, and by PhysicsWallah,
which built on our evaluation frameworks to support millions of students. These adoptions reaffirmed that open infrastructure multiplies impact—when you build transparently, others build with you. Our second pilot, AI for Therapists, explored how AI personas could help postgraduate psychology students practice therapy safely before engaging with real patients. The results were both encouraging and humbling. Students found AI simulations less intimidating than live clients, using them to rehearse empathy, reflective listening, and conversational pacing. Yet, they also pointed out what AI can’t do—it can teach attentiveness, but not intuition. While technology is necessary it is not sufficient. The real work is building trust, training people, and creating
systems where communities own and shape the tools — not just use them.
However, while open-source accelerates innovation but requires new thinking about sustainability and quality control. The future of digital health in India won't be built by one organisation doing everything. It will be built by a thousand organisations building together on shared infrastructure. And that's not a distant vision—it's already beginning. Every time an organisation adapts our work, every time a community shapes a tool to their reality, every time data flows back to those who generated it, we're proving infrastructure thinking works. The challenge now is making it sustainable, scalable, and standard practice.
Ami Polymer’s Single-Use Bags: The Backbone of Modern Bioprocessing
In the rapidly advancing world of biopharmaceutical manufacturing, the demand for sterile, scalable, and contamination-free fluid management has never been higher. Single-Use Systems (SUS) have rev olutionized how vaccines, monoclonal antibodies, cell therapies, and APIs are produced—offering the flexibility and purity today’s facilities require.
At the forefront of this transformation stands Ami Polymer Pvt. Ltd., a pioneer in silicone and polymer-based solutions with 25 + years of innovation in the life-sciences industry. From concept to commercialization, Ami Polymer delivers custom-engineered Single-Use Bags that ensure process reliability, compliance, and safety at every stage of bioprocessing.
1.The Role of Single-Use Bags in Bioprocessing
Single-Use Bags serve as sterile containment and transfer systems used throughout upstream, downstream, and fillfinish operations. Unlike traditional stainless-steel systems, they eliminate cleaning validation, reduce turnaround time, and mitigate cross-contamination risk— making them indispensable for multiproduct facilities and rapid-response manufactur-
◆ Media and buffer preparation
◆ Cell culture and fermentation
◆ Harvest, clarification, and intermediate storage
◆ Filtration, mixing, and formulation
◆ Aseptic filling and sampling
2.Comprehensive Range of Single-Use Bags
Ami Polymer’s portfolio is built around process versatility and user convenience.
2D Bags
◆ Flat, flexible design for volumes up to 50 L
◆ Ideal for rocking platforms, hanging setups, and smallscale transfers
◆ Commonly used for media preparation, sampling, and buffer storage
3D Bags
◆ Cuboidal structure for > 50
L volumes
◆ Designed for integration with rigid tanks and totes
◆ Enables bulk storage, largescale mixing, and high-volume
fluid transfer
Tank Liners (2D / 3D)
◆ Open-top containment bags compatible with process tanks
◆ Available with or without bottom drain ports
◆ Gusseted and non-gusseted options to maintain structural integrity
Powder Bags
◆ Antistatic films prevent
ing (such as vaccines or cell therapies).
Applications include:
charge buildup during powder handling
◆ Safe for APIs, excipients,
and lyophilized materials
◆ Available with or without blind caps; 5 L . 50 L with 4 / 6 feeding ports
Mixer Bags
◆ Fitted with precision impellers or magnet-driven mixers
◆ Deliver consistent mixing with high burst and tensile strength
◆ Range: 50 L . 1000 L, available with powder addition ports
Filling Bags
◆ Multi-line inlet/outlet designs for aseptic filling and drainage
◆ Gamma-sterilized, leaktested, and customizable
◆ Standard volumes: 5 L, 10 L, 20 L, 50 L
ing
◆ Available from 50 mL . 1 L
3.WhySo Many Variants?
Every bioprocess step presents distinct physical and chemical demands:
◆ 2D vs 3D – Flat storage for compact systems vs volumetric containment for bulk.
◆ Liners – Simplify tank cleaning and product changeover.
◆ Powder Bags – Protect sensitive materials from static and moisture.
◆ Mixer Bags – Achieve homogeneous blending of media and buffers.
◆ Filling Bags – Ensure sterile product transfer to vials or syringes.
◆ Pre-sterilized, ready-to-use systems for contaminationfree sampling
◆ Multiple port configurations for in-process monitor-
out breaching sterility. This breadth allows process engineers to build end-to-end, fully disposable fluid paths with maximum efficiency and minimal risk.
Imaflexell™ Series
HEALTHCARE TRACKER
4.Film Technology: The Core of Performance
Ami Polymer’s Single-Use Bags are built from advanced multilayer films developed to deliver chemical compatibility, mechanical strength, and biocompatibility.
9101 Infuflex Film
◆ 5-layer co-extruded structure: LDPE / TIE / EVOH / TIE / ULDPE
◆ High oxygen and moisture barrier
◆ Low extractables and excellent clarity
◆ Certified to USP <87>, USP <88>, USP <661.1>, and ISO 10993
5.Advantages of Ami Polymer Single-Use Bags
◆ Sterility & Safety – Manufactured in cleanroom environments and supplied gamma-sterilized. Customization – Multiple port sizes, tubing types, and connection interfaces (TC, Luer, CPC, etc.).
Regulatory Compliance –Meets USP, ISO, and EP standards for biocompatibility and chemical resistance. Operational Efficiency – Eliminates cleaning validation, reduces downtime, and accelerates changeover.
◆ Global Compatibility –
Works seamlessly with leading SUS connectors and hardware systems.
6.PVC vs.Non-PVC Films in Bioprocessing
While PVC remains common in traditional medical infusion bags, biopharmaceutical processes increasingly demand non-PVC, multilayer films such as EVA, PE, or polyolefin composites.
7.Quality,Compliance, and Manufacturing Excellence
Every Ami Polymer SingleUse Bag is:
◆ Produced under ISO 13485 and cGMP-aligned systems
◆ 100 % integrity-tested (visual + pressure)
◆ Documented with a Certificate of Analysis (CoA) and Sterility Report
◆ Backed by full traceability
of raw materials and gamma sterilization batches
Ami Polymer’s manufacturing ecosystem supports both standard and customized bag configurations, ensuring scalability from R&D to commercial production.
Conclusion
From sterile media transfer to final product filling, Ami Poly-
mer’s Single-Use Bags enable safe, efficient, and scalable bioprocessing. Backed by decades of polymer expertise, proprietary film technology, and rigorous quality control, these bags form the core infrastructure of modern singleuse manufacturing.
Ami Polymer Pvt. Ltd. continues to empower the biopharma industry with reliable solutions that uphold the three pillars of progress—Purity, Performance, and Precision.
Written by: Atharwa Mishra
Sales
Executive
- Healthcare Division Ami Polymer Private Limited medical@amipolymer.com
HowMedika Business Solution (MBS) is transforming hospital procurement
MBS acts as a one-stop solution,offering hospitals and clinics access to a wide range of consumables,medical equipment and devices,and pharmaceuticals all under one roof
Running a hospital is not just about treating patients it also means ensuring that the right medicines, equipment, and consumables are always available when needed. Unfortunately, procurement is often one of the most stressful parts of hospital operations.
Hospitals and clinics face constant challenges such as:
◆ Stockouts of life-saving medicines, consumables, or devices at critical moments.
◆ Dealing with multiple vendors, each with different timelines, pricing structures, and service levels, which leads to
confusion and inefficiency.
◆ High procurement costs, especially when items are sourced in smaller quantities.
◆ Unpredictable deliveries that disrupt smooth hospital operations.
◆ Limited access to branded products in tier 2 and 3 cities, forcing hospitals to compromise on quality or availability.
◆ Manual inventory tracking, which increases the chances of mismanagement and unnecessary expenses. These hurdles not only affect hospital staff but also impact patient care, making procurement a key area in need of transformation.
This is where MBS steps in as a reliable partner. MBS acts as a one-stop solution, offering hospitals and clinics access to a wide range of consumables, medical equipment and devices, and pharmaceuticals all under one roof. By bringing everything together, MBS eliminates the need to juggle multiple vendors and ensures smoother operations.
WhyMedikabazaar Business Solutions?
◆ Cost savings: Hospitals can save significantly through bulk buying and optimized procurement.
◆ Access to multiple brands: Wide choice across leading, trusted brands to meet diverse needs.
◆ Inventory planning and analytics: Tools that help hospitals forecast demand, plan stock, and prevent shortages.
◆ Hassle-free deliveries: Reliable, timely supply of essential products so hospitals can focus on care.
◆ Flexible payment options: Tailored solutions to ease fi-
nancial pressure and improve cash flow.
Most importantly, MBS extends these benefits to tier 2 and tier 3 cities, where procurement challenges are often even more severe due to limited local suppliers. Hospitals in smaller cities can now enjoy the same access to quality products and brands as those in metro areas, ensuring that patients everywhere receive the care they deserve. By reducing costs, saving time, and guaranteeing availability, MBS is not just simplifying procurement it is strengthening the backbone of healthcare delivery across India.
Property PVC Bags
Ami Polymer’s Infuflex/ Imaflexell Films (Non-PVC)
REGD.WITH RNI NO.MAHENG/2007/22045,POSTAL REGD.NO.MCS/162/2025 – 27,PUBLISHED ON 8TH EVERY MONTH, POSTED ON 14TH,15TH,16TH EVERY MONTH,POSTED AT MUMBAI PATRIKA CHANNEL SORTING OFFICE,MUMBAI – 400001