Questions each have a theme (i.e. speciality) and a focus (e.g. macroscopy, cut up, governance)
• Likely skin will be a few SBA questions and 1 or 2 EMQs
• Certain topics keep coming up
• Immunobullous disorders
• Lichenoid conditions
Useful resources
• Robbins or similar
Weedon • McKee
• RCPath pathway documents
• DermnetNZ
• St Johns institute website
Inflammatory dermatoses Adnexal neoplasms
Syndromes
Melanocytic lesions
Inflammatory Dermatoses
• A. Tissue reaction patterns
• Spongiotic
• Psoriasiform
• Lichenoid
• Vasculopathic
• Granulomatous
• Vesiculobullous
• B. Patterns of inflammation
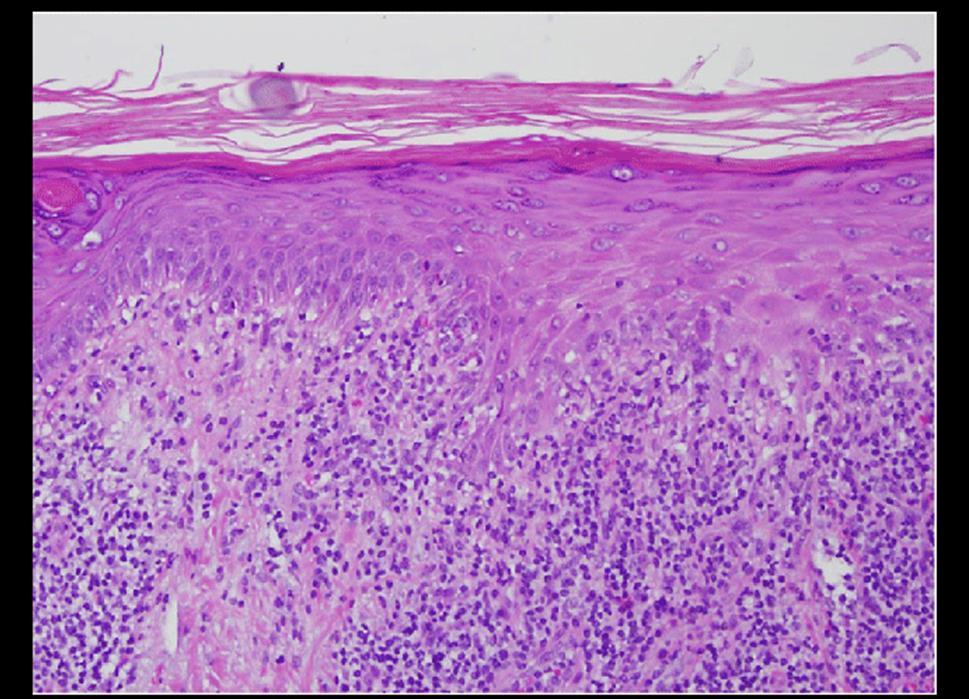
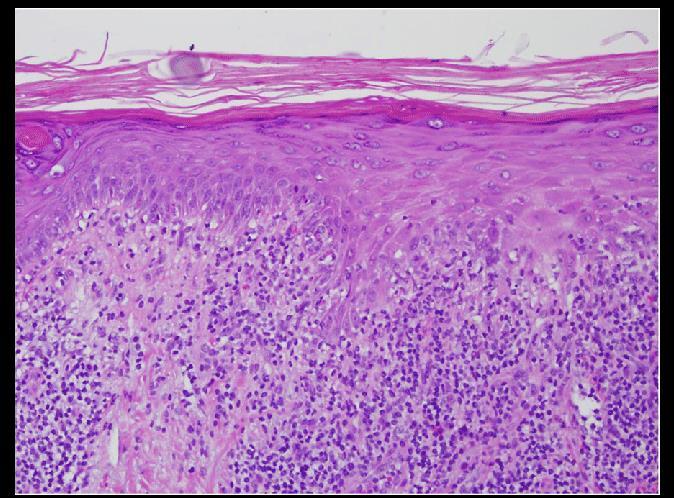
Spongiotic reaction
Eczematous dermatitis
• Early/’typical’ lesions: spongiosis and lymphocyte exocytosis
• Overlying parakeratin, acanthosis
• Late lesions: psoriasiform hyperplasia
• Always perform a fungal stain for dermatophyte infection
• Eosinophilic spongiosis (eosinophils in the epidermis with spongiosis)
• Drug reaction
• Allergic/contact dermatitis
• Insect bite reaction
• Pre-bullous bullous pemphigoid
• Langerhan cell vesicles – allergic/contact
• Underlying vascular changes – stasis dermatitis
• Lipping or separation of keratin (‘teapot sign’) – pityriasis rosea
• Hyphae – dermatophyte infection
MCQ 1
33 year old male printer complained of a 3 month history of hand dermatitis. Patch testing was negative. A biopsy showed spongiosis and lymphocyte exocytosis. No Munro’s microabcesses are seen. Identify the most likely diagnosis.
• A. Prebullous pemiphigoid
• B. Psoriasis vulgaris
• C. Irritant/contact eczematous dermatitis
• D. Mycosis fungoides
• E. Drug reaction
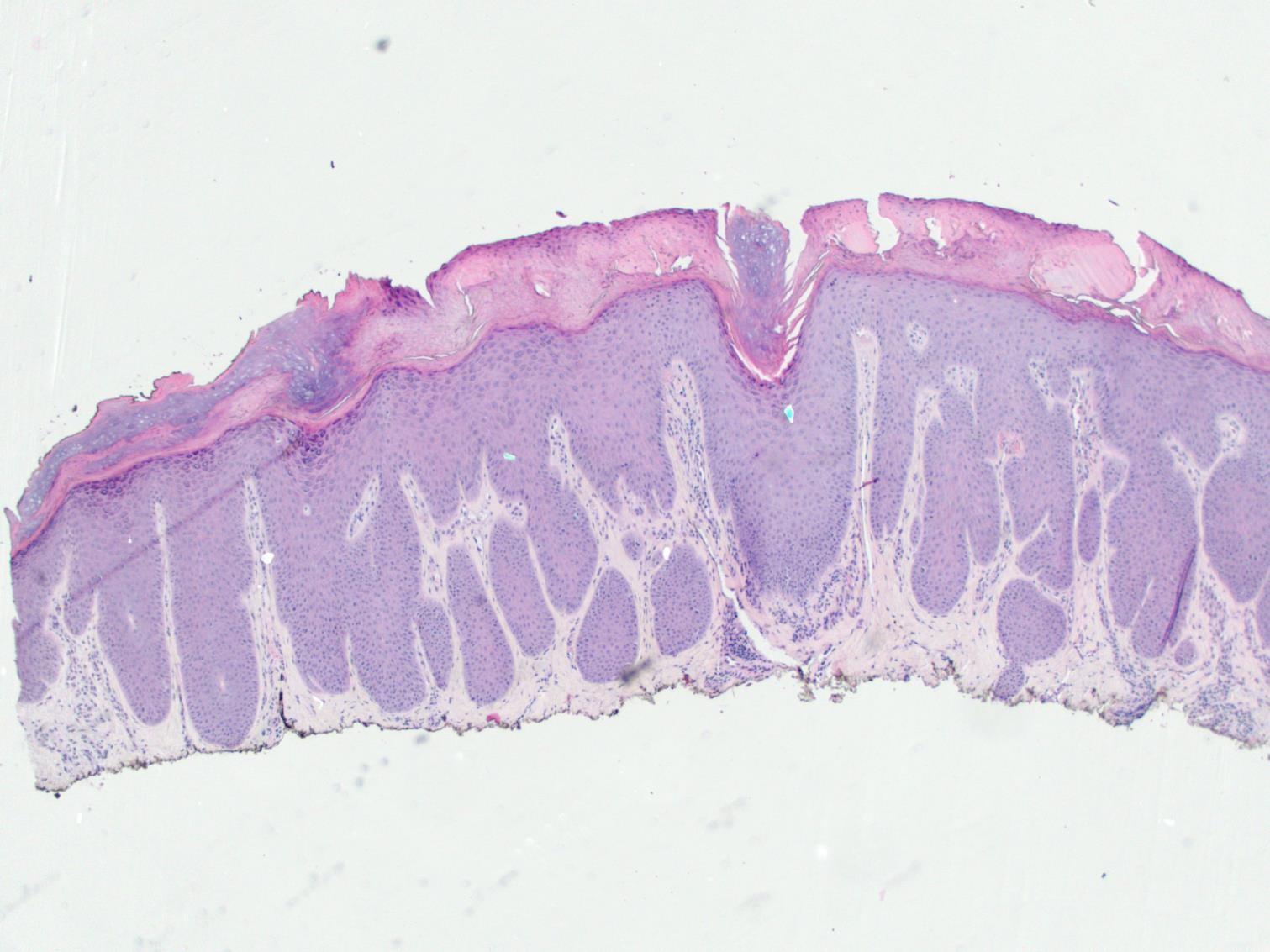
Psoriasiform reaction
• Regular elongation and broadening of rete
•Psoriasis •Lichen simplex chronicus
•Pityriasis rubra pilaris •Psoriasiform changes in eczematous dermatitis
Psoriasis
• Chronic non-infectious inflammatory dermatosis
• Well demarcated erythematous plaques topped with silvery scales
• Variants: Plaque, Palmoplantar, Scalp, Guttate, Flexural, Nail
•Early
• Vascular proliferation in dermal papillae
• Slight spongiosis
•Established lesions
• Regular acanthosis with regular elongation of rete ridges
• Thinning of supra-papillary epidermal plate
Inflammatory dermatoses
• Parakeratosis
• Increased mitotic activity at the base of epidermis
• Reduced/absent granular cell layer
• Neutrophil pustules – Munro microabscesses
Inflammatory dermatoses
MCQ 2a
• Which statement is false.
• Psoriasis:
a. Can result in alopecia
b. Sacrum affected
c. Pustular form exists
d. Histologically shows spongiform pustule of Kogoj
e. Vascular ectasia is seen with margination of neutrophils
• A 34 year old patient presents with multiple silvery skin plaques. A skin biopsy is performed to confirm the diagnosis.
MCQ 2b
• Identify the finding which would not be consistent with a diagnosis of psoriasis.
a. Can result in alopecia
b. Sacrum affected
c. Pustular form exists
d. Histologically shows spongiform pustule of Kogoj
e. Vascular ectasia is seen with margination of neutrophils
• A 34 year old patient presents with multiple silvery skin plaques involving the extensor surface of the limbs, scalp and lower back. The condition is worse after periods of stress and
MCQ 2c
localises to areas of trauma. A skin biopsy is performed to confirm the diagnosis.
• Identify the finding which would not be expected in this condition.
a. Can result in alopecia
b. Sacrum affected
c. Pustular form exists
d. Histologically shows spongiform pustule of Kogoj
e. Vascular ectasia is seen with margination of neutrophils
MCQ 2d
• A 34 year old patient presents with multiple silvery skin plaques involving the extensor surface of the limbs, scalp and lower back. The condition is worse after periods of stress and localises to areas of trauma. A skin biopsy is performed to confirm the diagnosis.
• Identify the finding which would not be expected in this condition.
a. Fibrous replacement of hair follicles
b. Parakeratosis
c. Neutrophilic pustules in the epidermis
d. Vascular ectasia is seen with margination of neutrophils
e. Loss of the granular cell layer
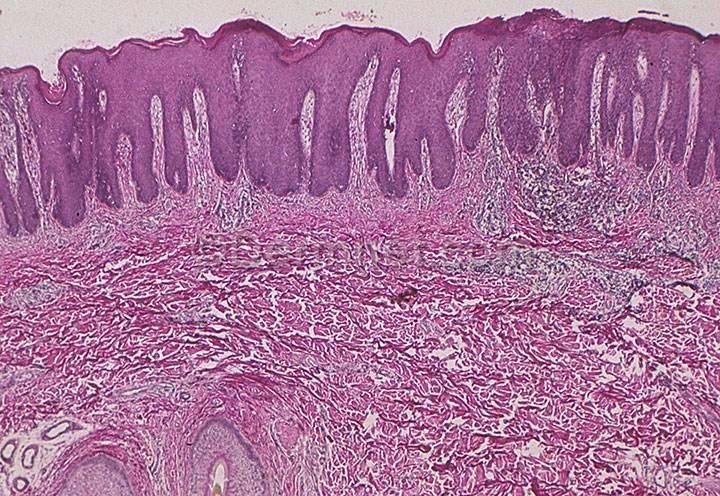
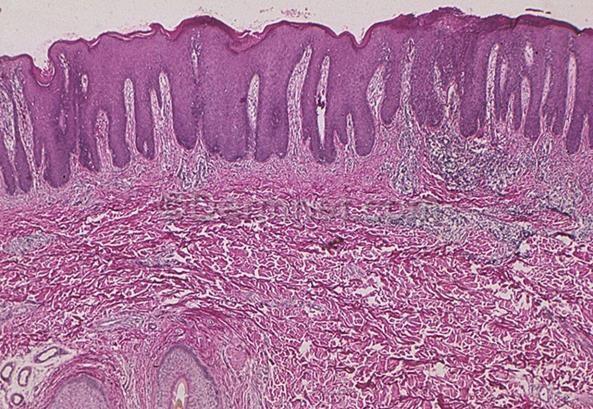
Pityriasis rubrapilaris (PRP)
• Red-orange well demarcated scaling patches
• Islands of sparing
• Can present with erythoderma
• ‘Alternating orthokeratin and parakeratin’ in a checkerboard pattern •
Psoriasiform hyperplasia
Lichen simplex chronicus/nodular prurigo
• Dermatosis related to chronic excoriation without an underlying aetiology
• Common in practice but a difficult exam question to write
• Many biopsies show an element of this with other clues to underlying cause
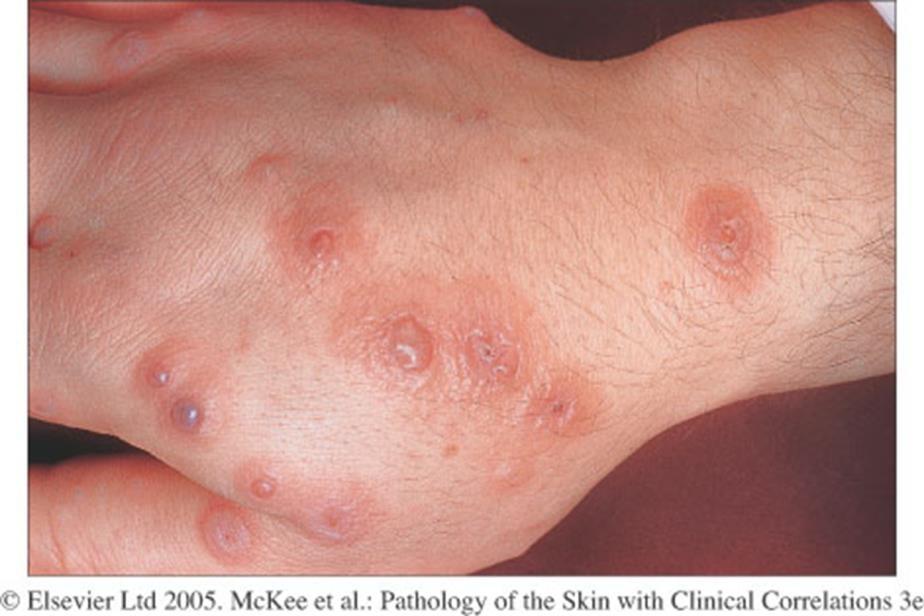
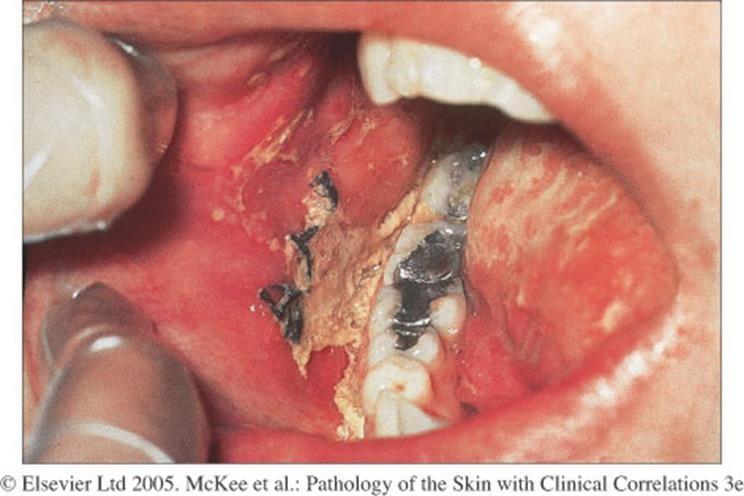
Syphilis
• Secondary syphilis
• Shows a widespread hyperpigmented maculopapular eruption.
• Causes: idiopathic, viral, bacterial, fungal, drugs (antibiotics, NSAIDs), other
• Oral, conjunctival, genital lesions not uncommon
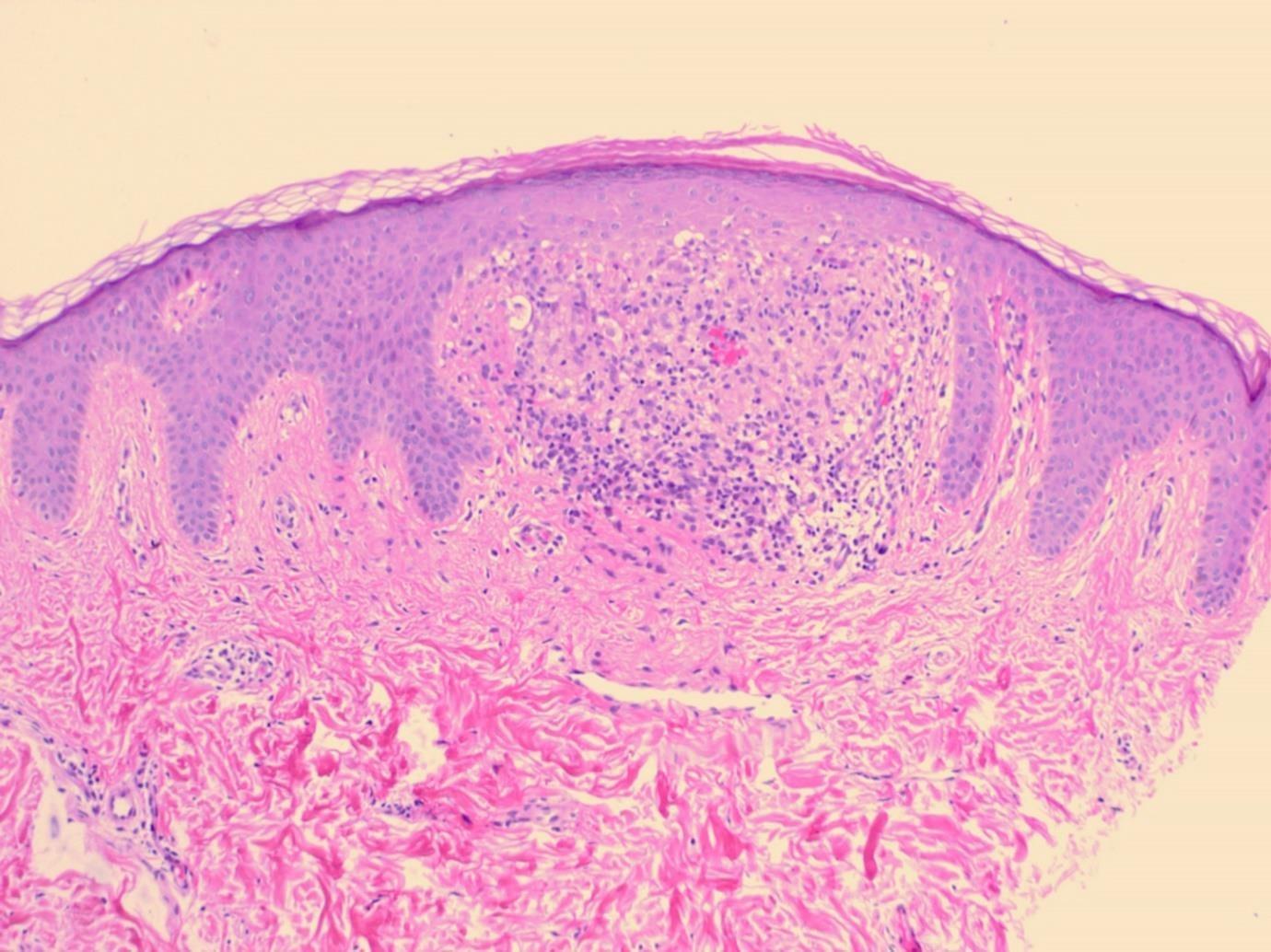
• Interface change >lichenoid infammation
MCQ 3
•A 44 year old taxi-driver presents with an sudden eruption on the trunk and limbs. Target lesions are present on the hands and feet. His skin biopsy shows basal cell damage with apoptotic keratinocytes.
•Identify the most likely diagnosis.
a. Lichen planus
b. Dermatomyositis
c. Erythema multiforme
d. Chronic graft versus host disease
e. Lichen nitidus
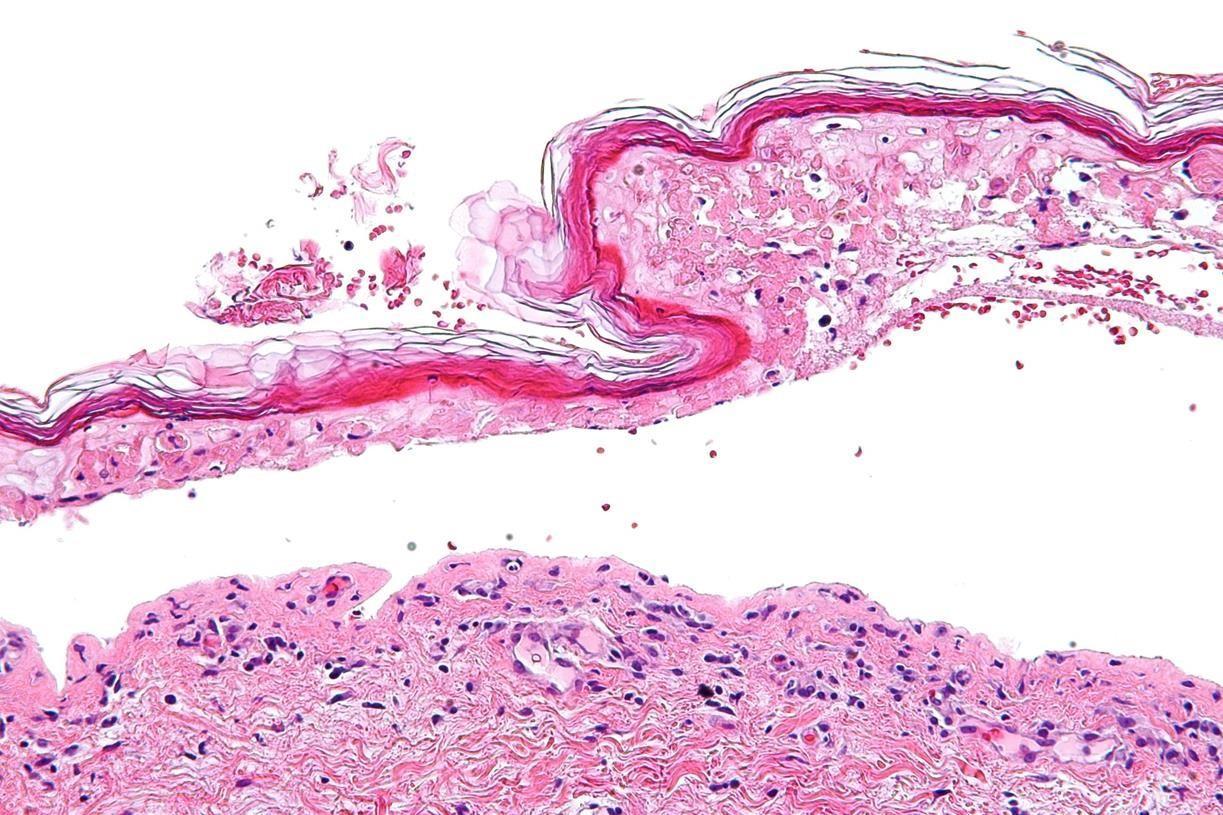
Toxic epidermal necrolysis (TEN)
• Sub-epidermal blisters with necrotic overlying epidermis
• Medical emergency
• Treated as a burns patient
• Main clinical differential – staphylococcal scalded skin
Lupus erythematosus
•Clinically: Sharply demarcated erythematous, scaly patches with follicular plugging.
•Characterised by
1. Interface change +/- lichenoid reaction
2. Superficial and deep perivascular and periadnexal chronic inflammatory cell infiltrate.
3. Hyperkeratosis, follicular plugging and epidermal atrophy.
4. Thickening of basement membrane
5. Increased dermal mucin
Graft versus host disease
• Usually a clinical diagnosis
• Following transplantation the donor's immune cells in the transplant (graft) make antibodies against the patient's tissues (host).
• Organs most often affected include the skin, gastrointestinal (GI) tract and the liver.
• Acute < 100 days
• Chronic > 100 days
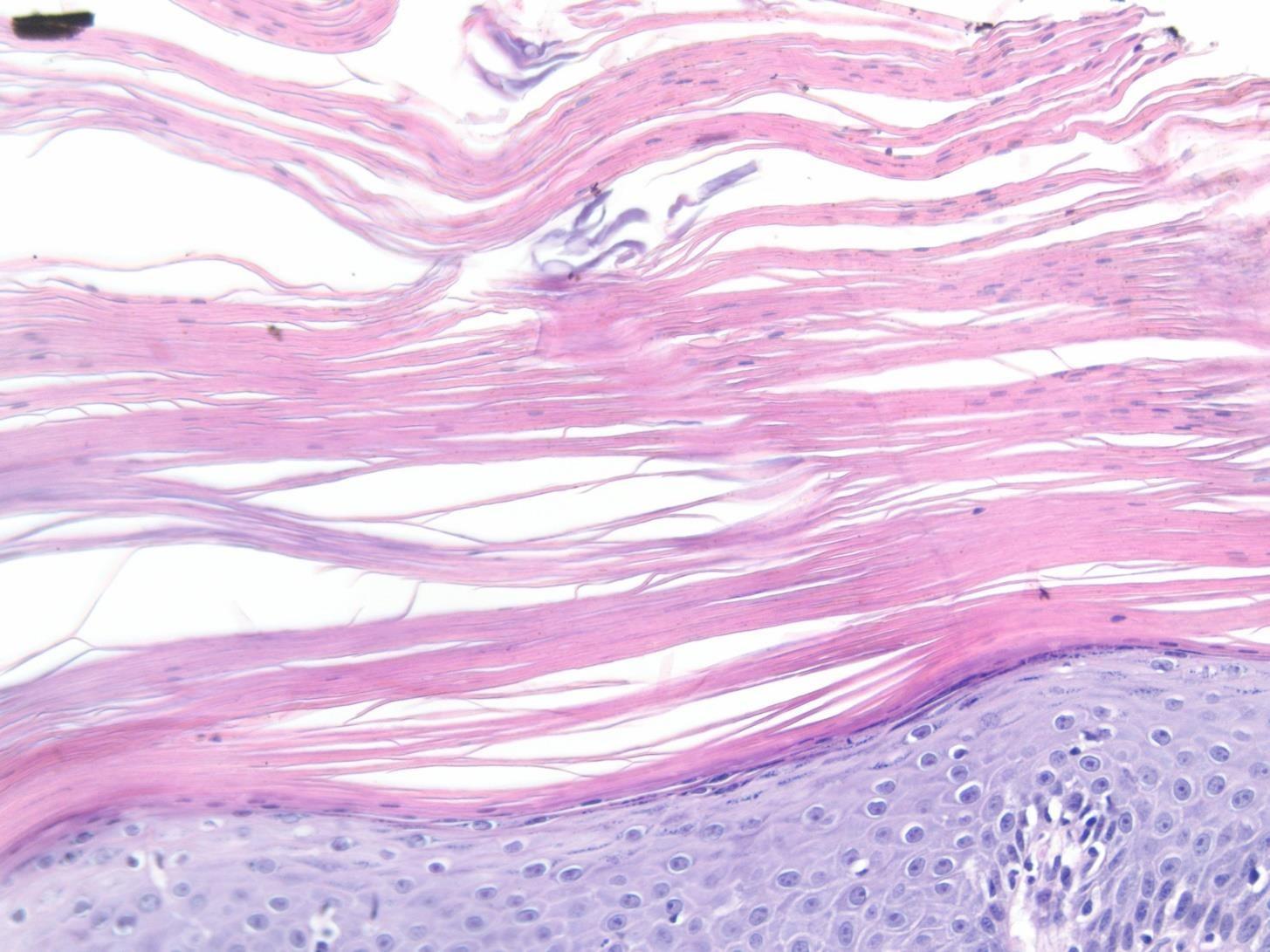
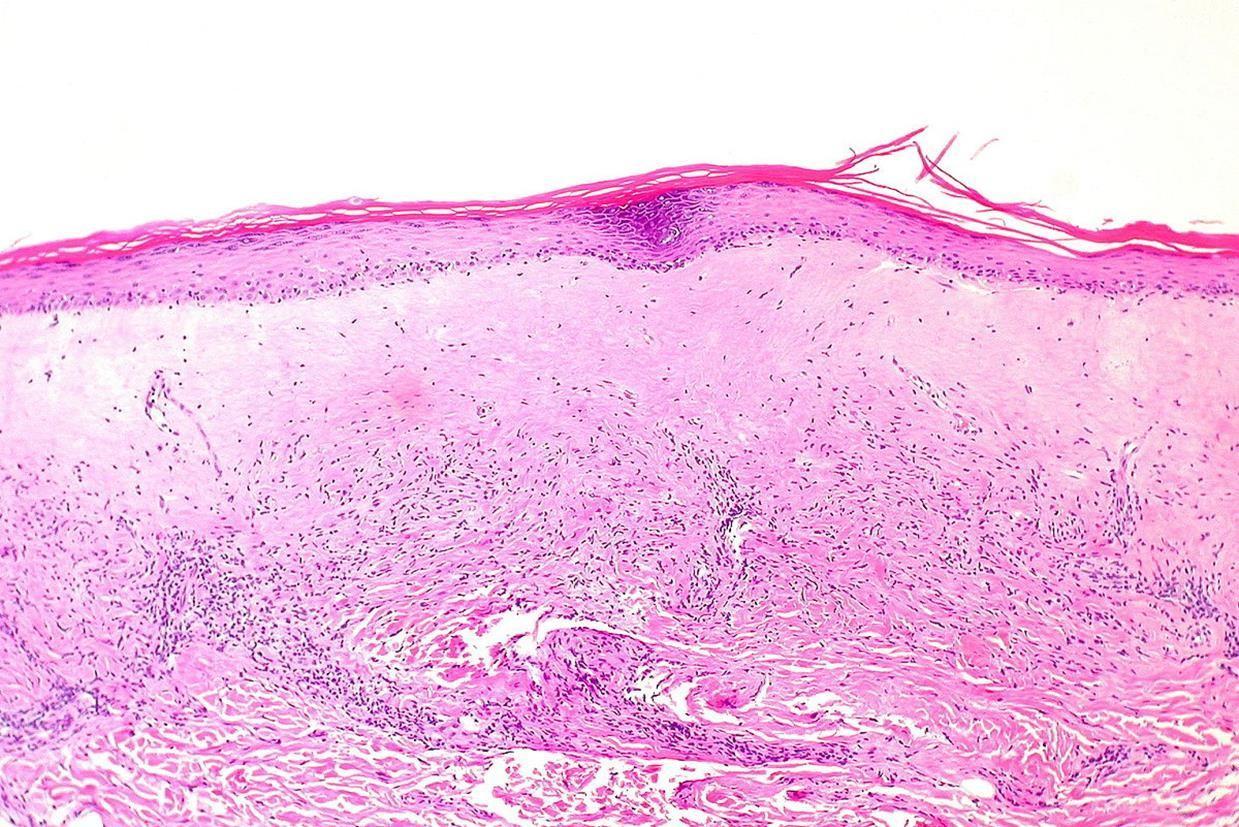
Lichen sclerosus
• Pale atrophic patches
• Clinical DD often morphoea
• Lichenoid reaction (often subtle)
• Homogenisation of dermal collagen
• Thickening of basement membrane
• Ectatic vessels
• Underlying inflammatory infiltrate – often contains eosinophils
Inflammatory dermatoses
Vasculopathic conditions
• Vasculopathic just means it involves the blood vessels.
• Conditions include:
• Inflammation of vessels – vasculitis.
• Changes in the walls – porphyria, amyloid.
• Something in the lumen – thrombosis.
• More widespread changes – stasis dermatitis, arteriopathic changes.
Inflammatory dermatoses
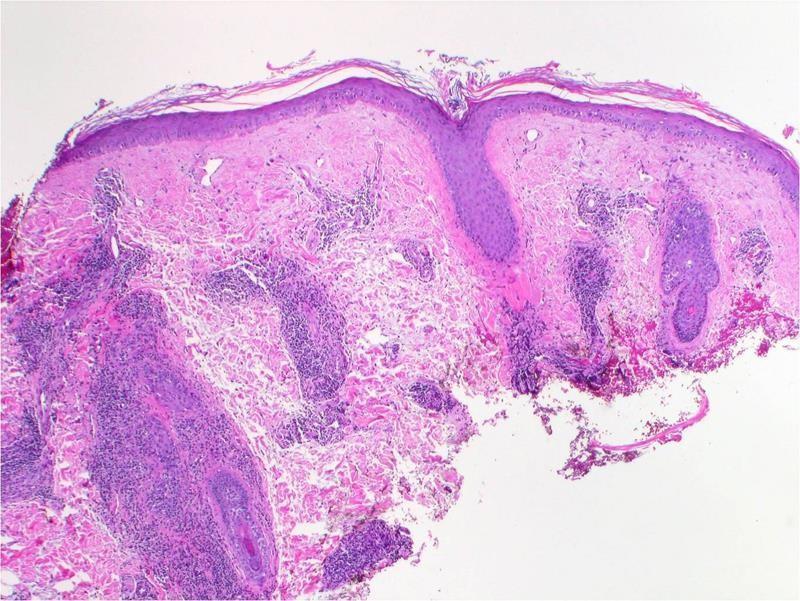
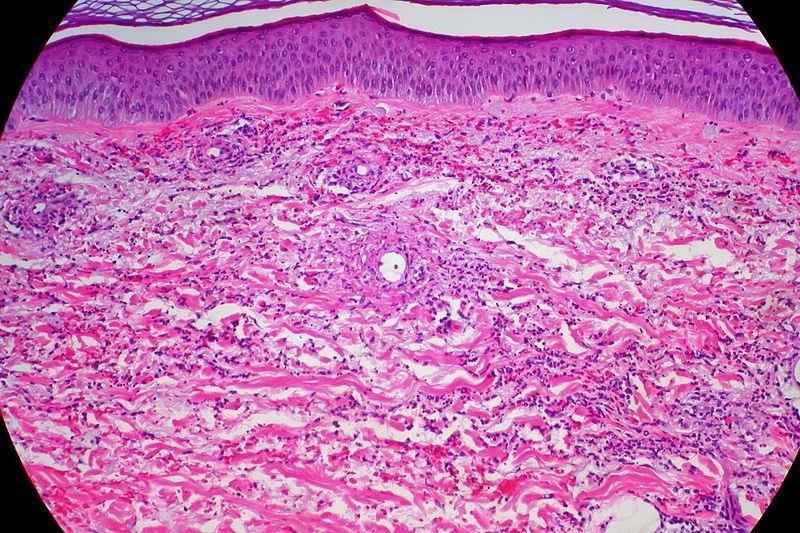
Leukocytoclastic vasculitis
• Tissue reaction pattern which can be idiopathic or have underlying associations including drugs, connective tissue disease, infection and systemic vasculitis.
• Intramural neutrophils
• Red blood cell extravasation
• Fibrinoid necrosis
• Leukocytoclasis
Inflammatory dermatoses
Polyarteritis nodosa (PAN)
• Necrotising vasculitis of medium sized vessels
• Uncommon
• Tender nodules
• May develop hypertension, renal failure and neuropathy
• Similar findings to leukocytoclastic vasculitis but involves deeper vessels (into subcutis)
Wegener’s granulomatosis/Granulomatosis with polyangiitis
• Multiple purpuric macules and papules
• Possible to have ulcerating plaques and nodules.
Inflammatory dermatoses
• Histology
• Leukocytoclastic vasculitis.
• May see ill-defined granulomatous infiltrate surrounding vessels.
• c-ANCA positive
• Respiratory tract (nasal and lung) biopsies show necrosis associated with a granulomatous infiltrate
Inflammatory dermatoses
•Which of the following conditions does not show a leukocytoclastic vasculitis?
A. Erythema nodosum
B. Microscopic polyangiitis
C. Wegeners granulomatosis
D. Polyarteritis nodosa
E. Urticarial vasculitis
• A 42 year old patient presents with purpuric lesions involving both limbs. Inflammatory markers are raised. A skin biopsy is taken and shows features of a leukocytoclastic vasculitis.
• Identify the condition which does not show this feature.
A. Erythema nodosum
B. Eosinophilic granulomatosis with polyangiitis
C. Granulomatosis with polyangiitis
D. Polyarteritis nodosa
E. Urticarial vasculitis
MCQ 4c
• A 42 year old patient presents with purpuric lesions involving both limbs. Inflammatory markers are raised. A skin biopsy is taken and shows fibrinoid necrosis of vessel walls with leukocytoclasis and red blood cell extravasation.
• Identify the condition which would not show these features.
A. Erythema nodosum
B. Eosinophilic granulomatosis with polyangiitis
C. Granulomatosis with polyangiitis
D. Polyarteritis nodosa
E. Urticarial vasculitis
• A 42 year old patient presents with purpuric lesions involving both limbs. Inflammatory markers are raised. A skin biopsy is taken and shows fibrinoid necrosis of vessel walls with leukocytoclasis and red blood cell extravasation.
• Identify the most likely diagnosis.
A. Erythema nodosum
B. Eczematous dermatitis
C. Epidermolysis bullosa acquista
D. Erythema multiforme
E. Polyarteritis nodosa
Granulomatous inflammation/reaction
Types of granulomatous inflammation
•Sarcoidal
Foreign body
Suppurative
Tuberculoid •Necrobiotic
Interstitial
Differential always includes infection in all patterns of granulomatous inflammation
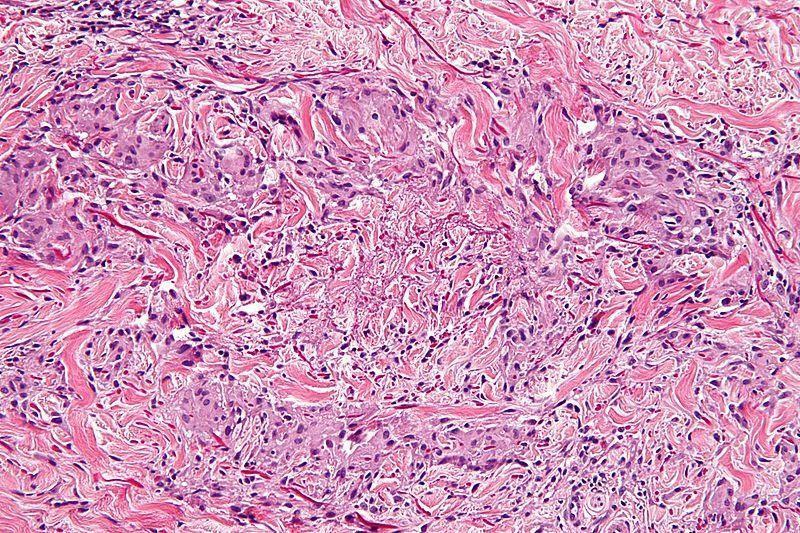
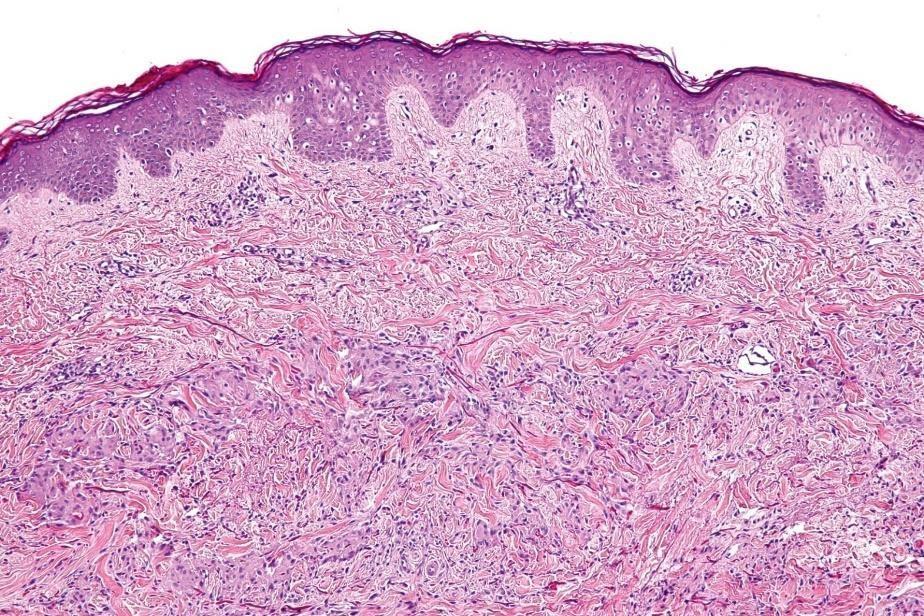
Sarcoidal granulomas
• Sarcoidosis
• Reaction to foreign materials
• Secondary Syphilis • Infection
• Crohn’s disease
Sarcoidosis
• Multisystem disorder
• Skin, liver, spleen, lung, eyes, lymph nodes
• 10-35% patients with systemic sarcoid have cutaneous lesions
• Sarcoidal granulomas are composed of epithelioid cells and giant cells, some containing asteroid bodies or other inclusions.
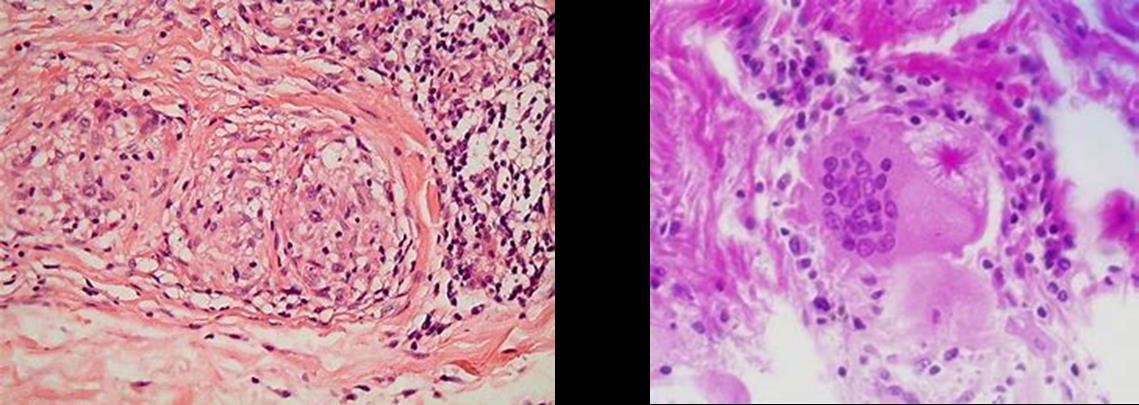
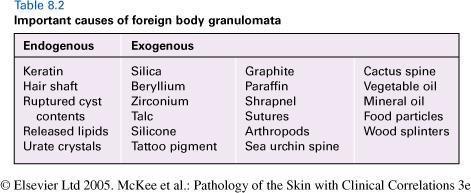
Foreign Body Granulomas
•Seen every day
•Scar/re-excision specimens
•Ruptured epidermoid cysts/follicles
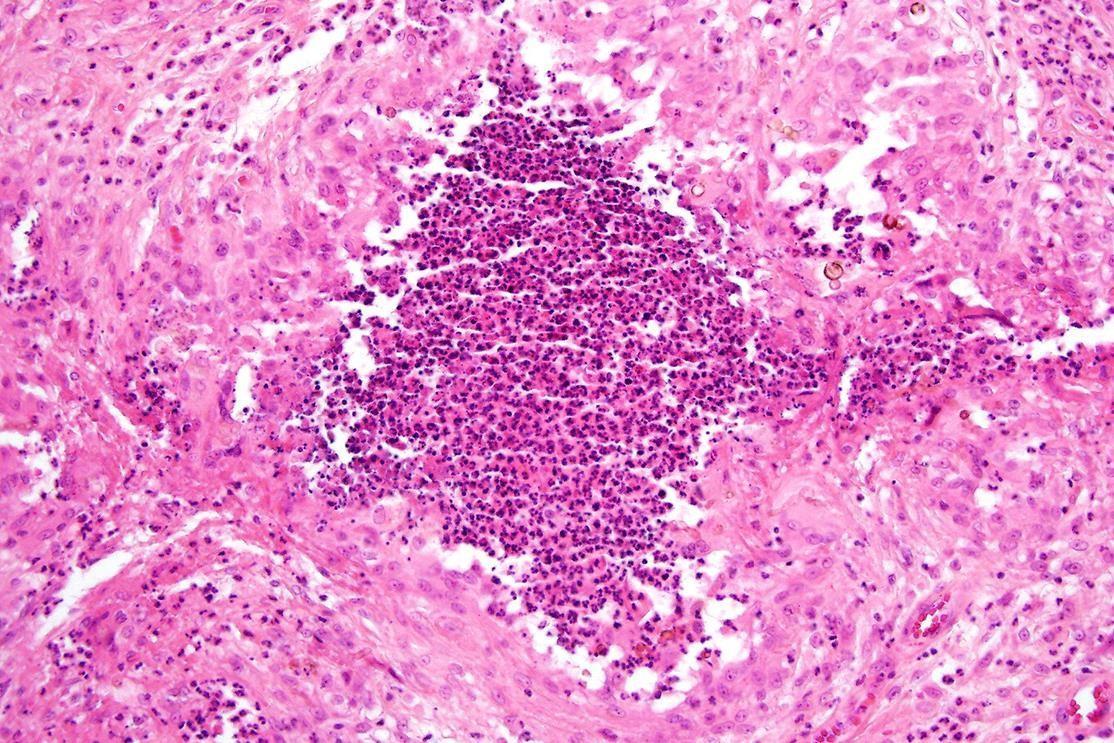
Suppurative Granulomas
• Neutrophils within and sometimes surrounding the granuloma. The granulomatous component is not always well defined.
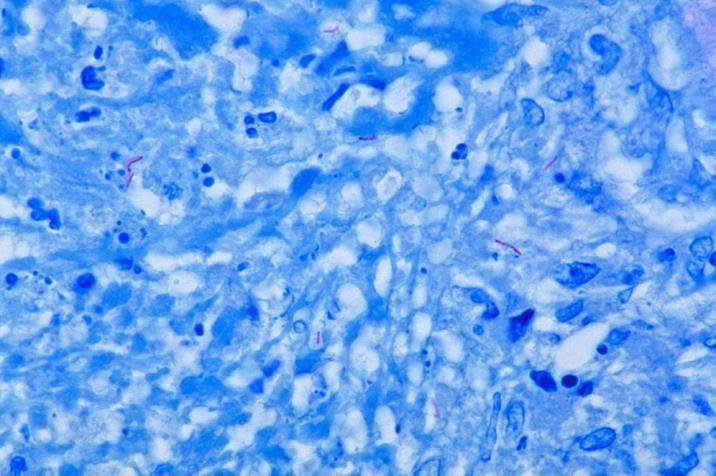
• Infection needs to be excluded – special stains don’t necessarily do this.
• Gram – Bacteria
• PAS and Grocott silver – fungal infection
• Ziehl Neelsen and Wade-Fite –acid fast bacilli
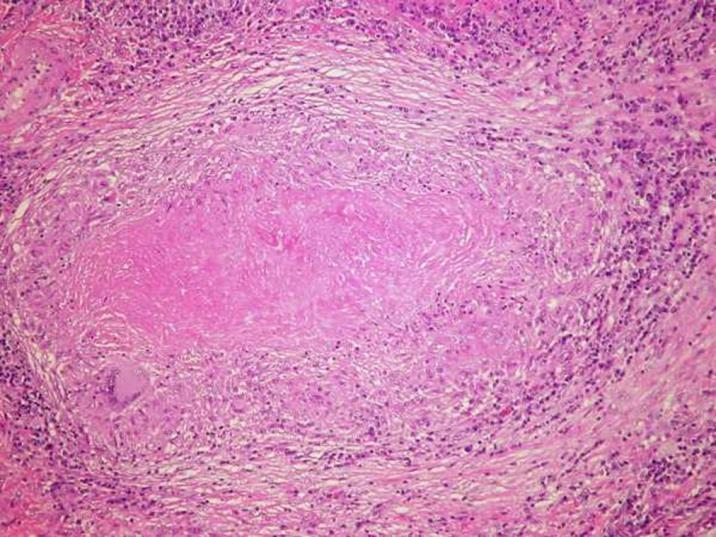
Tuberculosis – Tuberculoid granulomas
• Primary tuberculosis
• Miliary tuberculosis of skin
• Lupus vulgaris
• Scrofuloderma
• Tuberculous gumma
• Tuberculosis cutis orificialis
• Papulonecrotic
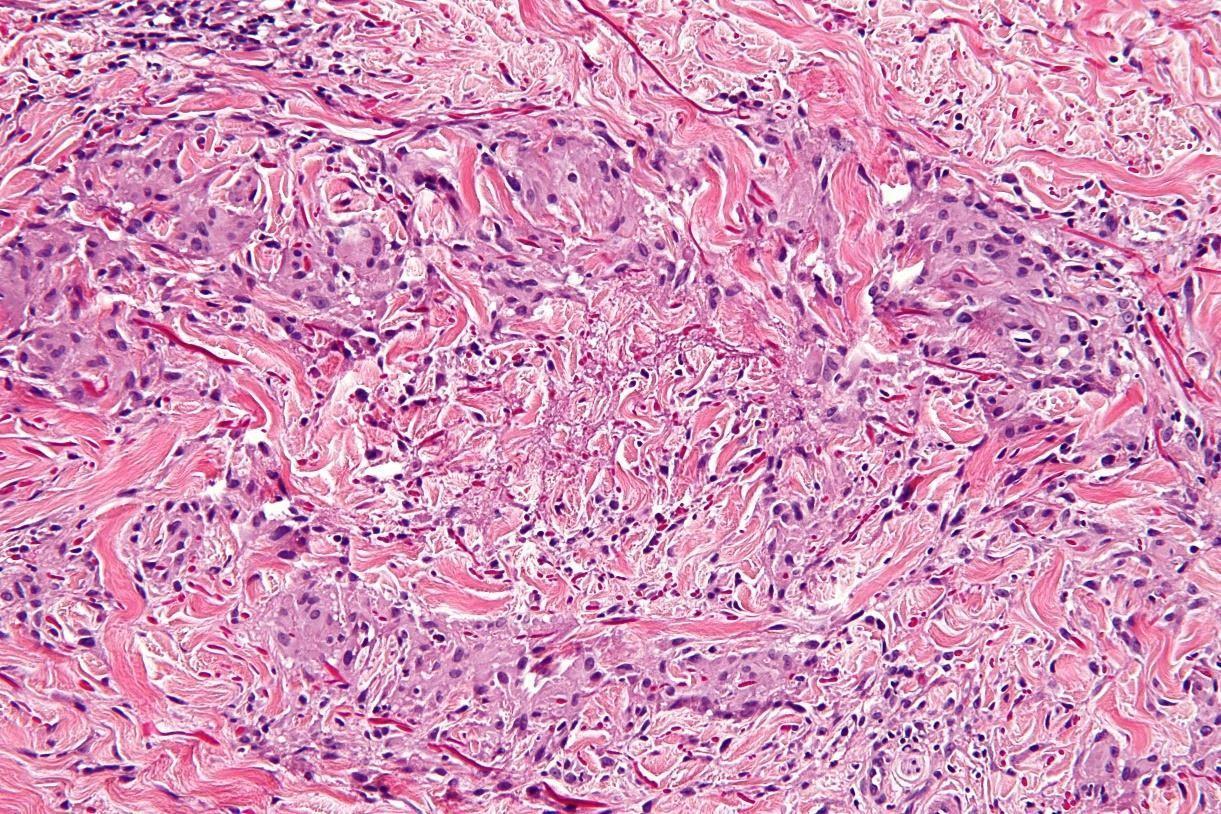
Necrobiotic granulomas
• Palisading of histiocytes around degenerate collagen
Necrobiotic granulomatous dermtoses
•Granuloma Annulare – palpable annular lesions on hands, feet or face
•Necrobiosis lipoidica – shiny atrophic yellowish red plaques on shins (62% in diabetics)
•Rheumatoid nodule - a local swelling or tissue lump, over bony prominences which occurs almost exclusively in association with rheumatoid arthritis
• Granuloma annulare
• Superficial/mid dermis
• Often intersitial (‘incomplete’)
• No plasma cells
• Eosinophils
• Mucin stain
• Necrobiosis lipoidica
• Diabetes
• Mid to deep dermis
• Linear pattern
• Plasma cells
• Rheumatoid nodules
• History
• Over joints
• Deep dermis to subcutis
• Palisading of histiocytes around eosinophilic material
• Fibrin/Trichrome stain
MCQ 5a
• Which of the following conditions is not associated with granulomatous inflammation.
A. Sarcoidosis
B. Granuloma annulare
C. Pemphigus vulgaris
D. Fungal infection
E. Tuberculosis
MCQ 5b
• A 58 year year old woman presents with itchy annular skin lesions. She has a history of Crohn’s disease for which she is on systemic therapy. A skin biopsy show aggregates of histiocytes.
A Grocott silver stain is positive.
• Identify the most likely diagnosis.
A. Sarcoidosis
B. Granuloma annulare
C. Necrobiosis lipoidica
D. Fungal infection
E. Metastatic Crohn’s disease
MCQ 5c
• A 59 year old lady presents with annular lesions over the dorsal surfaces of both hands. A biopsy shows an interstitial infiltrate of histiocytes with mucin deposition and focal necrobioisis. No plasma cells are seen.
• Identify the most likely diagnosis
• Necrobiosis lipoidica
• Sarcoidosis
• Granuloma annulare
• Fungal infection •
Rheumatoid nodules
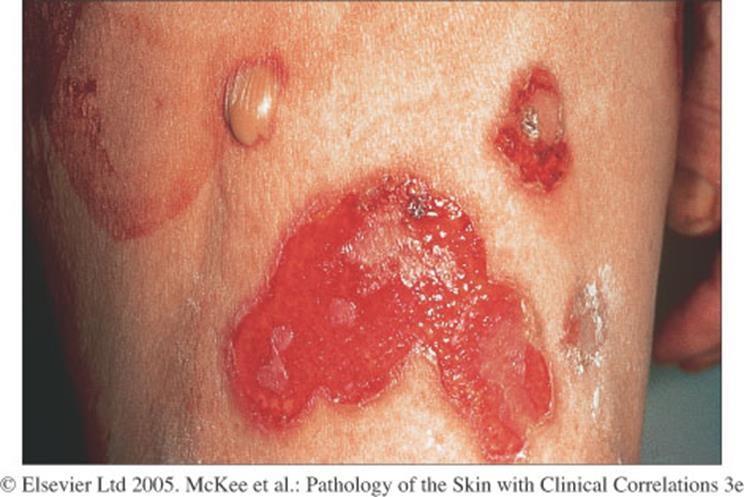
Blistering conditions
1. Anatomical level of split 2. Mechanism
responsible 3. Nature of inflammatory cell infiltrate
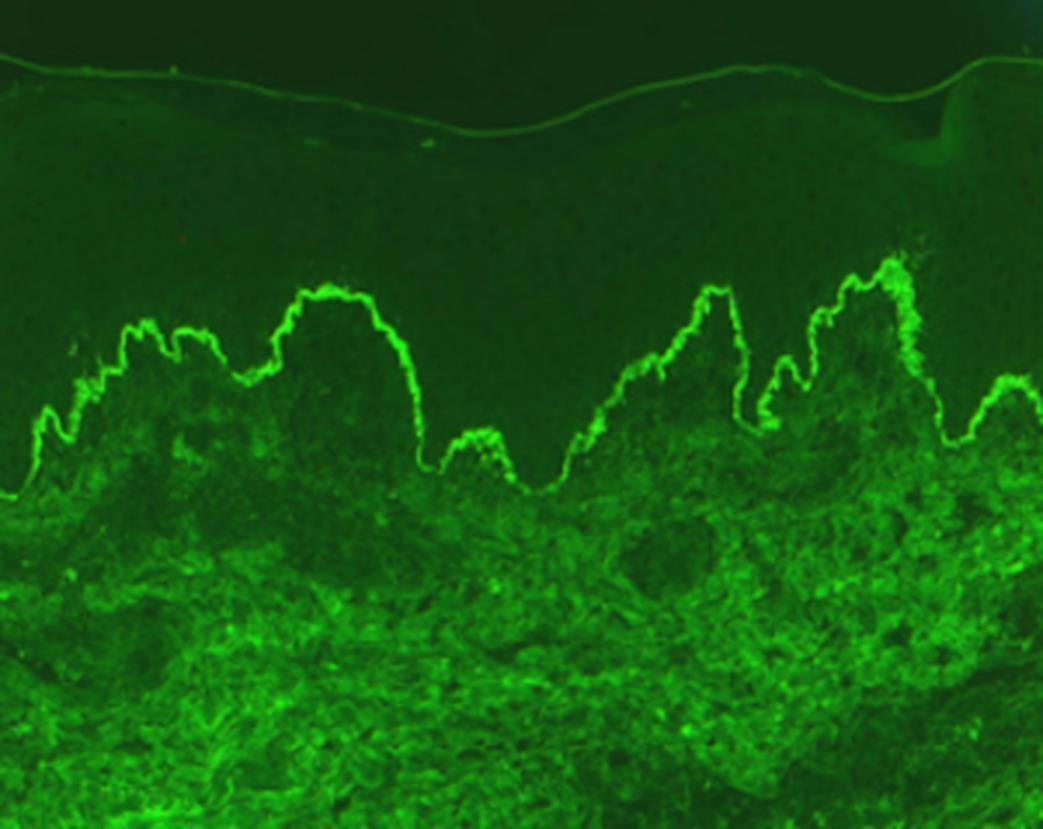
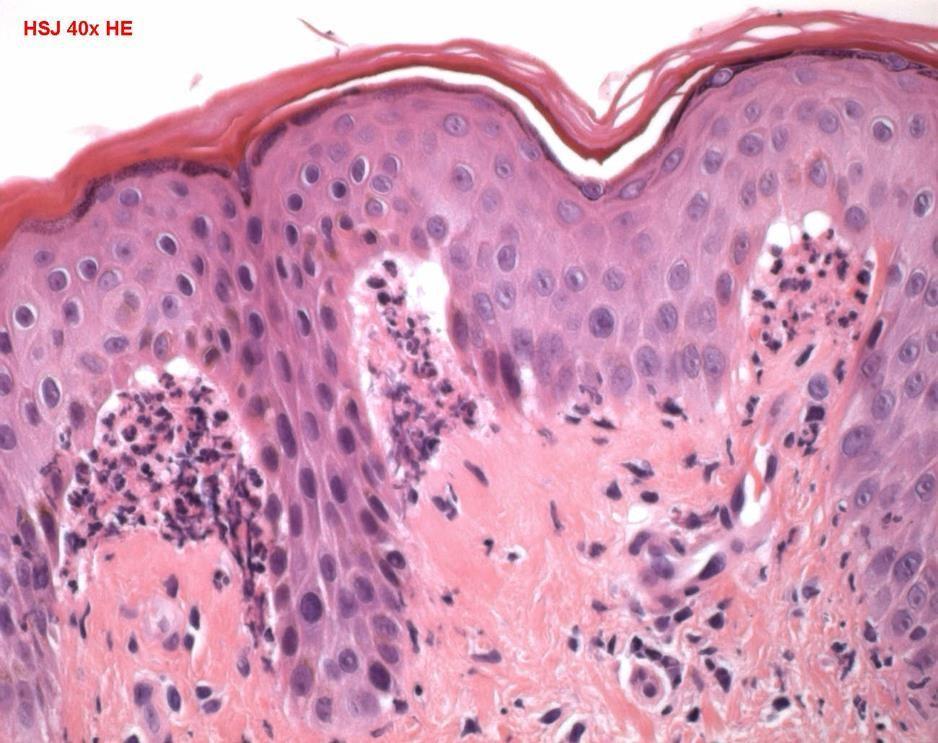
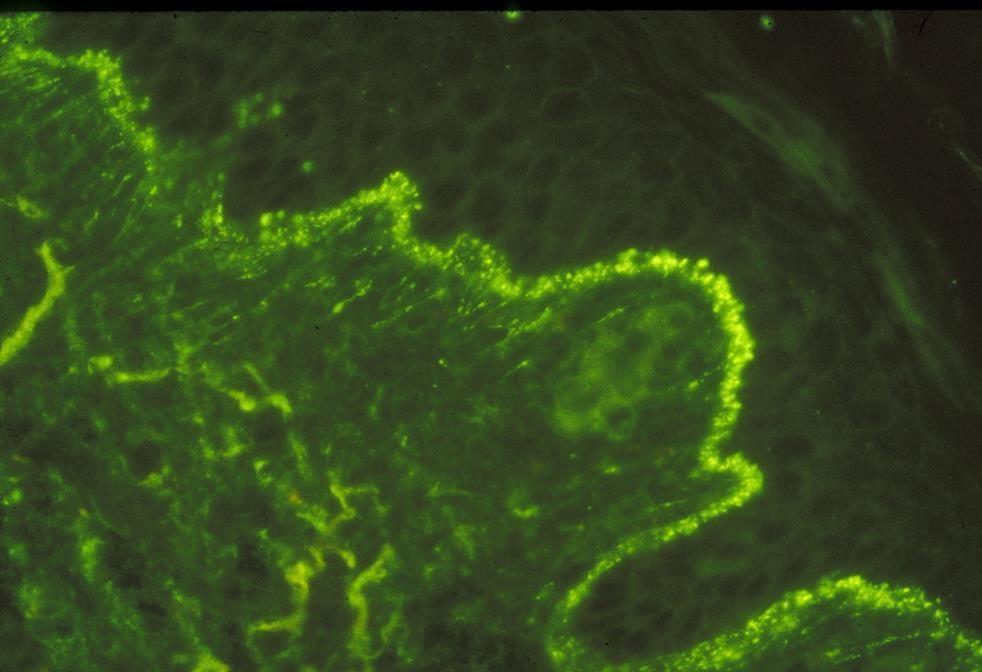
• Granular IgA in the tips of the dermal papillae on direct immunofluorescence.
• Vesiculo-bullous eruption of hepatobiliary disease may also present with dermatitisherpetiformis-likefeatures
• Linear IgA disease (and chronic bullous disease of childhood) show similar morphology
• Older individuals – present with blisters
• Distinguish by immunofluoresence
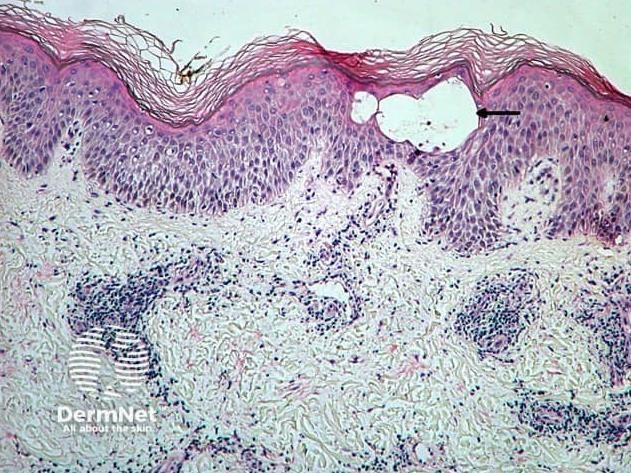
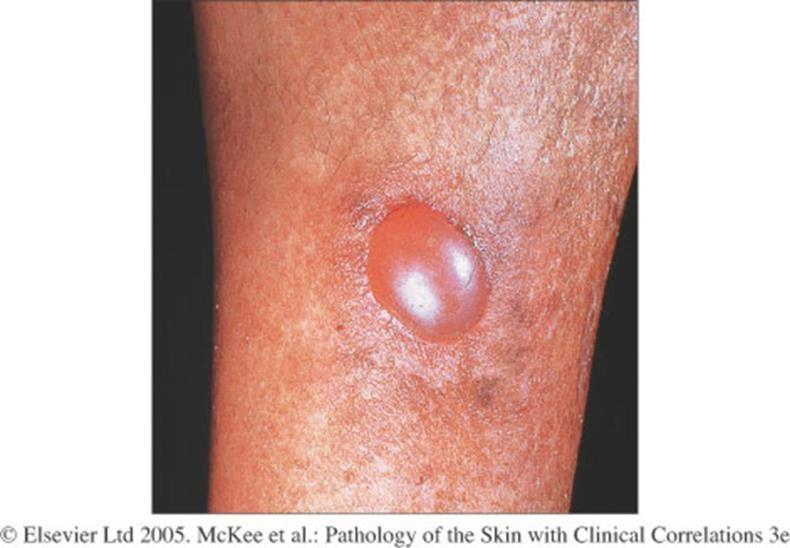
MCQ 6
• A 68 year old female has a 1/52 history of tense large blisters arising on erythematous skin. A skin biopsy shows a subepidermal blister containing eosinophils.
• Identify the most likely diagnosis.
A.Pemphigus vulgaris
B.Pemphigus foliaceus
C.Darier’s disease
D.Bullous pemphigoid
E.Grover’s disease
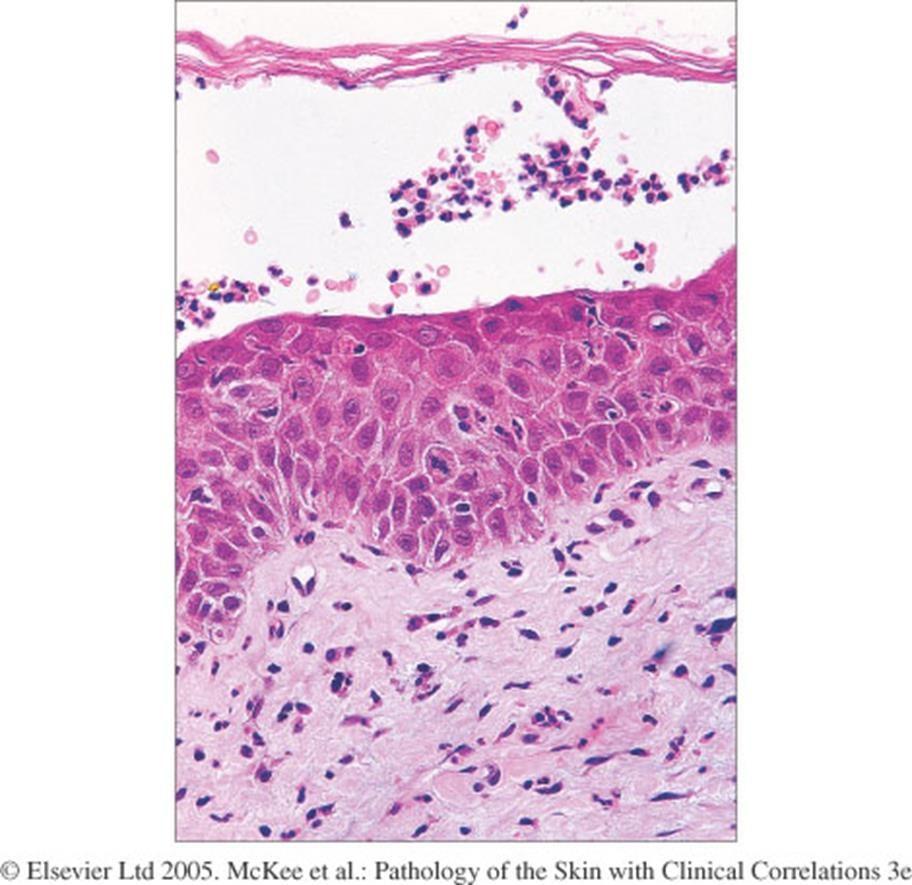
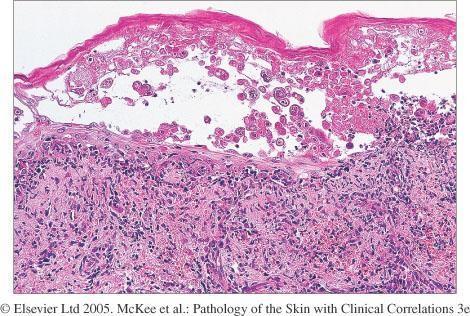
Cell poor subepidermal blisters
• Bullous pemphigoid
• Porphyria cutea tarda
• Burns
• Toxic epidermal necrolysis
• Suction blister
• Drugs
• Bullous amyloid
• Bullous diabeticorum
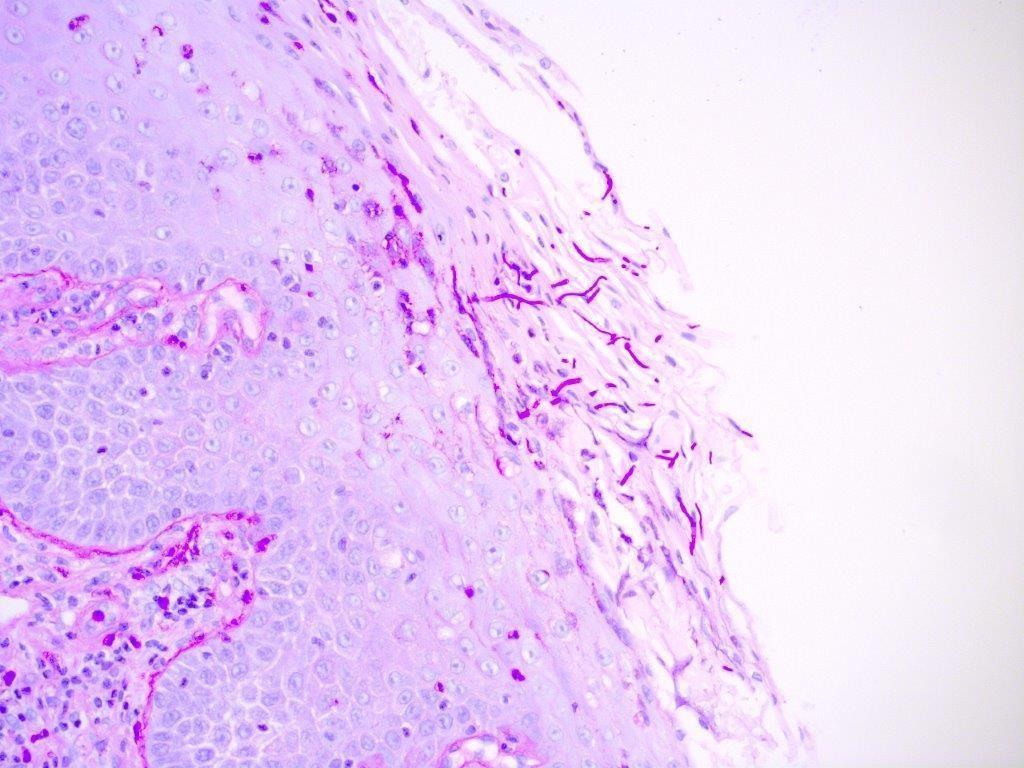
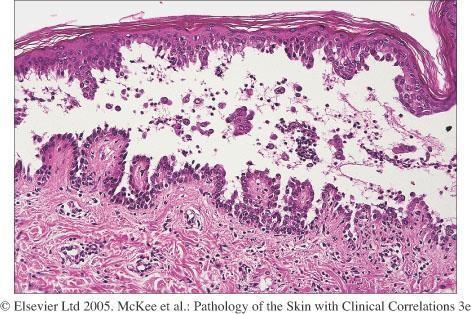
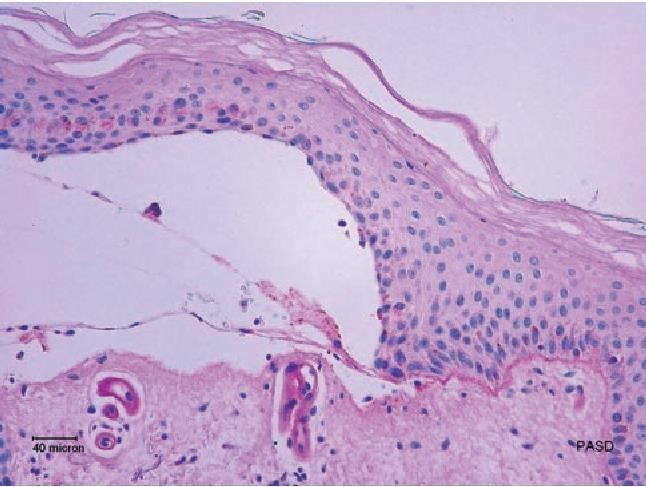
Porphyria cutea tarda
• Increasingly fragile skin hands and feet
• Fluid filled blisters (vesicles and bullae)
• Tiny cysts (milia) arising as the blisters heal
• Increased sensitivity to the sun
• Cell poor sub-epidermal blister
• Deposition of basement membrane material in epidermis – ‘caterpillar bodies’
• Thickening and increased eosinophilic in dermal vessels