Influenza virus can result in severe respiratory illness and is a common cause of hospitalisation, particularly among older adults and children under five.1 In 2025, Australia recorded its highest notifications of influenza on record with high inter-seasonal activity, alongside declining vaccination rates.2-4 Needle fear is a significant barrier to vaccination, with the Royal Children’s Hospital (Melbourne) reporting that 27% of children aged four and older have an intense fear of needles, often preventing timely vaccination.2,5
FluMist® is an intranasal live attenuated trivalent influenza vaccine that has been available internationally for over 20 years.1,6-9 It provides a convenient, needle-free alternative that may improve uptake.6 It has demonstrated comparable protection against severe disease compared to injectable formulations and is TGA-approved for use in children aged 2–17 years.1,5,9
FluMist® is delivered by a healthcare professional via a nasal spray into each nostril and is rapidly absorbed, even if the child sneezes after the dose.1,5 Side effects are usually mild and transient, including blocked or runny nose, headache, sore throat, fever and tiredness.1,6 Anaphylaxis is extremely rare.1,6
FluMist® has not been studied in patients with severe asthma or active wheeze and is contraindicated in immunocompromised individuals.9,10
This year several state governments including New South Wales, Queensland, South Australia and Western Australia (as of Feb 2026) have announced
funded FluMist® programs for young children ahead of the influenza season to improve uptake in priority groups (see Table 1).10-14 Potential supply constraints due to high demand and limited shelf life (up to 15 weeks) may influence availability.9
For updated information on FluMist® availability and eligibility for 2026, refer to the National Centre for Immunisation Research and Surveillance (NCIRS)1 and state/territory health department communications as the influenza season approaches.
Scan this QR code for the latest influenza vaccination information from NCIRS.
State/Territory Funded Groups
QLD
NSW
SA
WA
Children aged 2 to 5 years (inclusive)
Children aged 2 to <5 years
Children aged 2 to <12 years
TAS, VIC, NT, ACT Awaiting details
Table 1: State/Territory funded initiatives. Up to date 17/02/202611-14
Refer to the product information for comprehensive details, including contraindications, dosing and administration guidance.9
Scan QR code to view all article references.
Updates on ACE Inhibitor-Induced Angioedema
Meg Maynard, Critical Care Pharmacist - Slade Pharmacy Wesley
Angioedema is localised subcutaneous or submucosal swelling, resulting from extravasation of fluid into interstitial tissues.1 It commonly affects the face, lips, tongue and throat.1 Angioedema can occur as an isolated condition or alongside allergic reactions such as urticaria; however involvement of the upper airways can be life-threatening and requires urgent diagnosis and treatment.1
ACE Inhibitor-Induced Angioedema
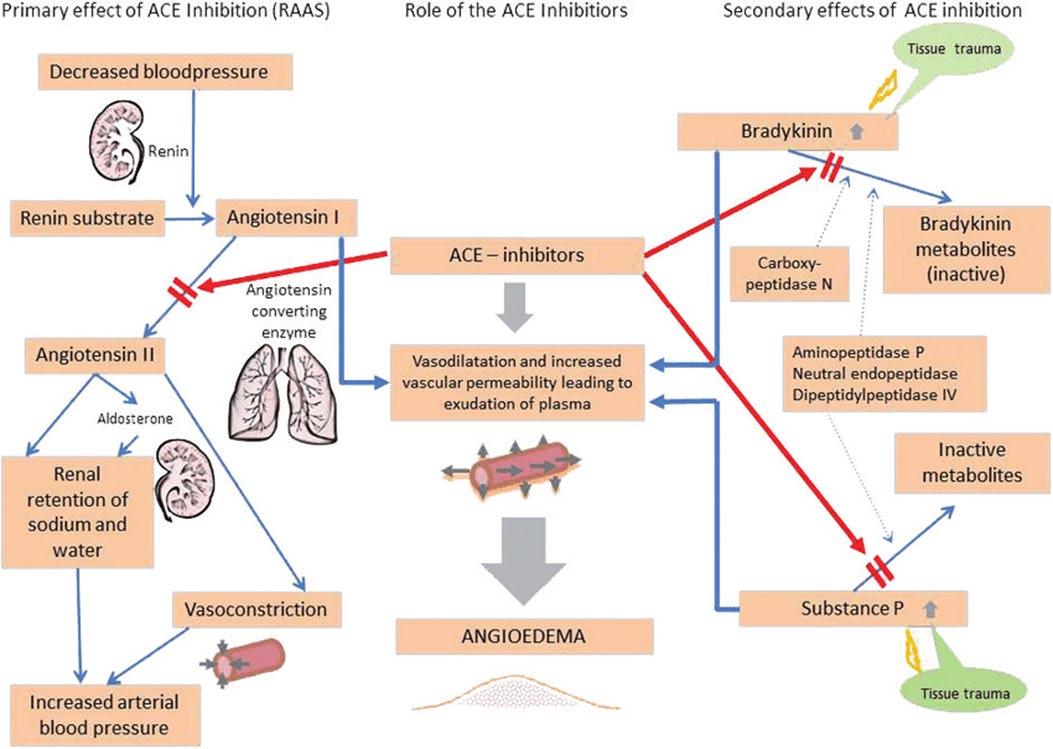
ACE inhibitors block angiotensin-converting enzyme, an important component of the renin–angiotensin system responsible for converting angiotensin I to angiotensin II and degrading bradykinin.1 By inhibiting this enzyme, ACE inhibitors decrease the formation of angiotensin II, a vasoconstrictor, and increase levels of bradykinin, a peptide vasodilator (refer to Figure 1).1 This combination acts synergistically to lower blood pressure and is the primary antihypertensive mechanism of these medications.1 A side effect of increased vasodilation and vascular permeability through excess bradykinin is angioedema.1
Unlike allergic reactions, ACE inhibitor-induced angioedema is not immunoglobulin E (IgE) - mediated; therefore, usual allergy treatments such as adrenaline, steroids and antihistamines are likely to be ineffective.1,2 Angioedema is an idiosyncratic drug reaction that can occur at any time during therapy, even after years of ACE inhibitor use.1
Management
Airway management is the most critical aspect of treatment. In cases of severe angioedema with airway involvement, intubation or a tracheotomy may be necessary.2
STOP the ACE inhibitor. In many cases, symptoms resolve in 48-72 hours after stopping the offending drug, with patients requiring monitoring and supportive care.1,2 However approximately one-third of cases are admitted to intensive care with 10% requiring intubation.2
In severe or refractory cases where airways are threatened, the use of off - label medication may be considered. Most therapies are licenced in Australia for hereditary angioedema (HAE), a disorder that is also bradykinin mediated,3 and may theoretically benefit ACE inhibitor–induced angioedema, however study results are conflicting, and real-world use is limited.2
Refractory treatment options
Icatibant selectively blocks bradykinin B2 receptors, inhibiting the effect of excess bradykinin that has accumulated.4 There is limited evidence available for the use of icatibant in ACE inhibitor-induced angioedema. One study of 27 patients demonstrated time to complete resolution of oedema was significantly shorter with icatibant (2 hours) than combination glucocorticoid and antihistamine therapy (11.7 hours; P=0.03).4 However, in a subsequent larger trial of icatibant vs placebo (121 patients) there was no observable difference in time to resolution between icatibant (2 hours) and placebo (1.6 hours; P = 0.57).5
Figure 1: Angioedema formation due to pharmacological inhibition of angiotensin-converting enzyme1
Fresh frozen plasma (FFP) contains angiotensin-converting enzyme, and the administration of plasma is thought to degrade high levels of bradykinin.6 Case reports have described improvement after FFP administration in refractory cases,6-8 with resolution of angioedema within 2-4 hours.7,8 However, the levels of angiotensin converting enzyme in individual units of plasma can vary significantly.7
Treatment with plasma-derived C1-esterase inhibitor (Berinert®) is thought to decrease the production of bradykinin allowing the excess bradykinin induced by the ACE inhibitor to be degraded to inactive bradykinin metabolites.10 In several case studies, C1-esterase inhibitor was shown to be effective in ACE inhibitor-induced angioedema11,12 however, in a small, randomised trial (25 patients) no significant difference was found.13
Tranexamic acid inhibits the plasmin-dependent formation of bradykinin.14 A review of seven studies (retrospective series or case reports; 98 patients), suggested possible benefit of tranexamic acid in ACE inhibitorinduced angioedema.14 In another study, length of stay in an emergency department was not reduced after administration of tranexamic acid (21 hours) compared to placebo (12 hours) however, the severity of angioedema was greater in the tranexamic acid group which had higher number of intubated patients.
Ecallantide (Kalbitor®) is also indicated in HAE, but it is not currently approved or registered in Australia and carries a high risk of anaphylaxis.16
In the absence of strong evidence, reserve refractory treatment options: icatibant, C1-esterase inhibitor, FFP and tranexamic acid, for patients presenting with severe angioedema, where airways are threatened and actively worsening.16 Best outcomes occur when treatments are given within the first few hours from symptom onset.16
Avoid future ACE inhibitor use
Following ACE inhibitor-induced angioedema patients should be closely monitored until symptoms resolve. Angioedema may reoccur within the first three months following an initial reaction despite discontinuation of the 17 Patients should be provided with clear guidance on recognising early symptoms and instructed on when and how to seek urgent medical care if swelling recurs.
Availability of C1-esterase inhibitor and icatibant varies between hospitals, but FFP and tranexamic acid are widely available in Australia.
ACE Inhibitors should never be reintroduced.
Alternative medications, such as angiotensin receptor blockers (ARBs), which do not inhibit bradykinin breakdown, may be safely used to manage the patient's underlying condition without the risk of inducing angioedema.16
Entresto® is a fixed dose combination medication containing sacubitril, a neprilysin inhibitor, and valsartan, an ARB, used for heart failure. As neprilysin breaks down bradykinin, sacubitril can also cause angioedema by the subsequent bradykinin build up and is therefore also contraindicated in patients with ACE inhibitor-induced angioedema.
References: See front page.
Showcasing Our Innovations
In 2025, our pharmacy team presented several innovative research and service development projects at the Advanced Pharmacy Australia and Clinical Oncology Society of Australia conferences. We’ve highlighted one below. Scan the QR code to explore more of our work.
Enhancing Safety in Cancer Services: A Risk Assessment Framework for Monoclonal Antibody Handling
Enhancing Safety in Cancer Services: A Risk Assessment Framework for Monoclonal Antibody Handling
Enhancing Safety in Cancer Services: A Risk Assessment Framework for Monoclonal Antibody Handling
Margaret Patterson1, Michelle Rantucci1,2
Margaret Patterson1, Michelle Rantucci1,2
1 Slade Pharmacy Quality and Medication Safety Unit
1 Slade Pharmacy Quality and Medication Safety Unit
2 Icon Group Cancer Services
Margaret Patterson1, Michelle Rantucci1,2 1. Slade Pharmacy Quality and Medication Safety Unit, 2. Icon Group Cancer Services
2 Icon Group Cancer Services
Background
Background
Monoclonal antibodies (mABs) are widely used in the treatment of cancer and non-cancer conditions. Unlike traditional cancer treatments, mABs are not cytotoxic (unless conjugated to a cytotoxic molecule) and are usually not considered hazardous.
Monoclonal antibodies (mABs) are widely used in the treatment of cancer and non-cancer conditions. Unlike traditional cancer treatments, mABs are not cytotoxic (unless conjugated to a cytotoxic molecule) and are usually not considered hazardous.
As new mABs are developed, many present novel mechanisms of action, increased compounding complexity, and uncertain compatibility with closed-system transfer devices (CSTDs).
As new mABs are developed, many present novel mechanisms of action, increased compounding complexity, and uncertain compatibility with closed-system transfer devices (CSTDs).
This highlights the need for further evaluation beyond existing general guidelines.
This highlights the need for further evaluation beyond existing general guidelines.
Objective
Objective
To develop a standardised risk assessment tool that:
To develop a standardised risk assessment tool that:
Actions
Actions
• Literature review conducted to identify any existing risk assessment frameworks
• Literature review conducted to identify any existing risk assessment frameworks
• Researched key medication formulation factors that may influence the likelihood of systemic absorption
• Researched key medication formulation factors that may influence the likelihood of systemic absorption
• Risk assessment tool developed
• Risk assessment tool developed
• Refined in collaboration with nursing & pharmacy teams
• Refined in collaboration with nursing & pharmacy teams
• Endorsed by the organisation’s Medication Safety Committee
• Endorsed by the organisation’s Medication Safety Committee
Development of a New Risk Matrix:
Development of a New Risk Matrix:
The organisation’s default risk matrix based on “likelihood” and “impact” (severity of consequence) was not fit for purpose.
The organisation’s default risk matrix based on “likelihood” and “impact” (severity of consequence) was not fit for purpose.
A new risk matrix was created mapping risk ratings against likelihood of exposure/absorption and using hazardous classification as the consequence descriptor.
A new risk matrix was created mapping risk ratings against likelihood of exposure/absorption and using hazardous classification as the consequence descriptor.
Hazardous ratings were categorised to align with existing guidelines (e.g. eviQ):
Hazardous ratings were categorised to align with existing guidelines (e.g. eviQ):
• Non-hazardous
• Non-hazardous
• Hazardous
• Hazardous
• Reproductive and/or developmental risk only
• Reproductive and/or developmental risk only
References: See front page.
Evaluation
Evaluation
Since implementation, the tool has been successfully applied to assess several newly introduced mABs.
Since implementation, the tool has been successfully applied to assess several newly introduced mABs.
Feedback from pharmacists and nursing staff has been positive, reporting increased confidence when compounding and during administration of these medications. This highlights the value of a consistent, structured approach ensuring appropriate controls are in place.
Feedback from pharmacists and nursing staff has been positive, reporting increased confidence when compounding and during administration of these medications. This highlights the value of a consistent, structured approach ensuring appropriate controls are in place.
Discussion
Discussion
QR code for Epcoritamab
While general guidelines exist for the safe handling of mABs, there was no comprehensive tool to assess the safety of individual agents, particularly in relation to compounding and administration requirements.
While general guidelines exist for the safe handling of mABs, there was no comprehensive tool to assess the safety of individual agents, particularly in relation to compounding and administration requirements.
Risk assessment adoption across a national cancer care organisation demonstrates its practical utility and potential for broader implementation.