AI-Powered Chemotherapy Ordering: Unlocking Annual Savings While Enhancing Safety and Accuracy Kirsty Mullin – Operational Excellence, Slade Pharmacy Services Russell Hill – Slade Pharmacy Services and Slade Health Compounding Background Chemotherapy order processing for over 70 outreach oncology clinics involved inconsistent and manual workflows, leading to significant administrative burden, risk of transcription errors, and delays. Slade Pharmacy Services implemented an AI solution to streamline chemotherapy order entry while maintaining critical clinical oversight.
Objective To automate chemotherapy transcription using AI to improve safety, reduce errors, and enhance workforce efficiency in Slade Pharmacy Services.
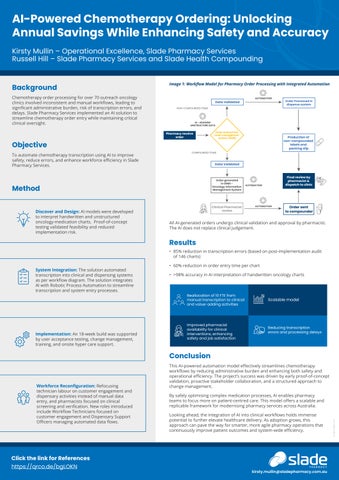
Image 1: Workflow Model for Pharmacy Order Processing with Integrated Automation
Data Validated NON-COMPOUNDED ITEMS
Order Processed in dispense system
AI - READING UNSTRUCTURE DATA
Pharmacy receive order
Order entered into order management system (OSM)
Production of non-compounded labels and packing slip
COMPOUNDED ITEMS
Data Validated
Order generated in OIMS Oncology Information Management System
Method Discover and Design: AI models were developed to interpret handwritten and unstructured oncology-medication charts. Proof-of-concept testing validated feasibility and reduced implementation risk.
AUTOMATION
Clinical Pharmacist review
Final review by pharmacist & dispatch to clinic
AUTOMATION
AUTOMATION
Order sent to compounder
All AI-generated orders undergo clinical validation and approval by pharmacist. The AI does not replace clinical judgement.
Results
• 85% reduction in transcription errors (based on post-implementation audit of 146 charts) System Integration: The solution automated transcription into clinical and dispensing systems as per workflow diagram. The solution integrates AI with Robotic Process Automation to streamline transcription and system entry processes.
Implementation: An 18-week build was supported by user acceptance testing, change management, training, and onsite hyper care support.
• 60% reduction in order entry time per chart • >98% accuracy in AI interpretation of handwritten oncology charts
Reallocation of 10 FTE from manual transcription to clinical and value-adding activities
Scalable model
Improved pharmacist availability for clinical interventions, enhancing safety and job satisfaction
Reducing transcription errors and processing delays
Conclusion
By safely optimising complex medication processes, AI enables pharmacy teams to focus more on patient-centred care. This model offers a scalable and replicable framework for modernising pharmacy services across Australia. Looking ahead, the integration of AI into clinical workflows holds immense potential to further elevate healthcare delivery. As adoption grows, this approach can pave the way for smarter, more agile pharmacy operations that continuously improve patient outcomes and system-wide efficiency.
Click the link for References https://qrco.de/bgLOKN
kirsty.mullin@sladepharmacy.com.au
AU GRP 114039_ 2510
Workforce Reconfiguration: Refocusing technician labour on customer engagement and dispensary activities instead of manual data entry, and pharmacists focused on clinical screening and verification. New roles introduced include Workflow Technicians focused on customer engagement and Dispensary Support Officers managing automated data flows.
This AI-powered automation model effectively streamlines chemotherapy workflows by reducing administrative burden and enhancing both safety and operational efficiency. The project’s success was driven by early proof-of-concept validation, proactive stakeholder collaboration, and a structured approach to change management.