















Findings
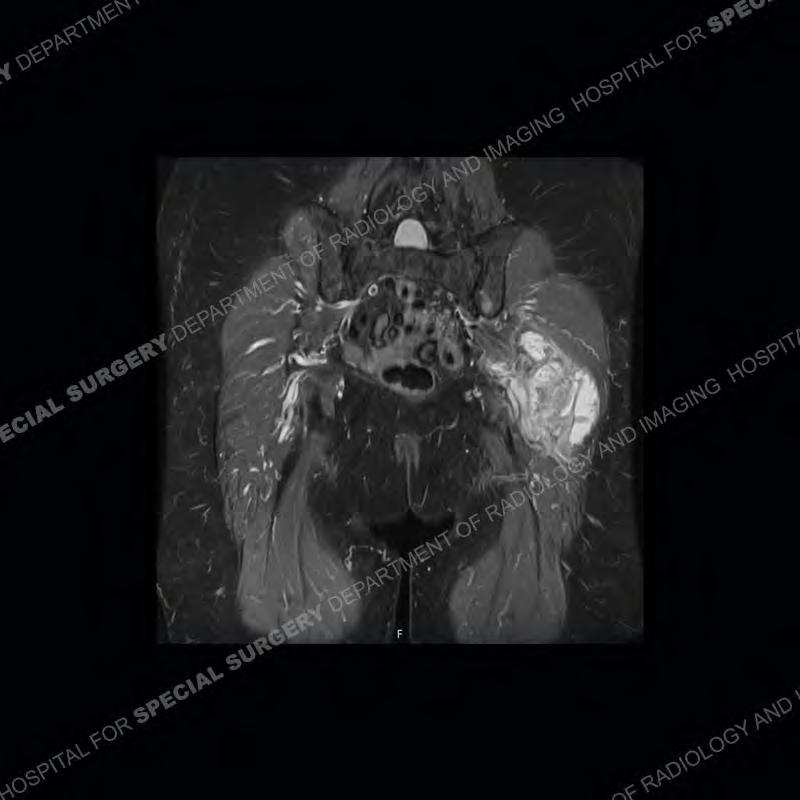
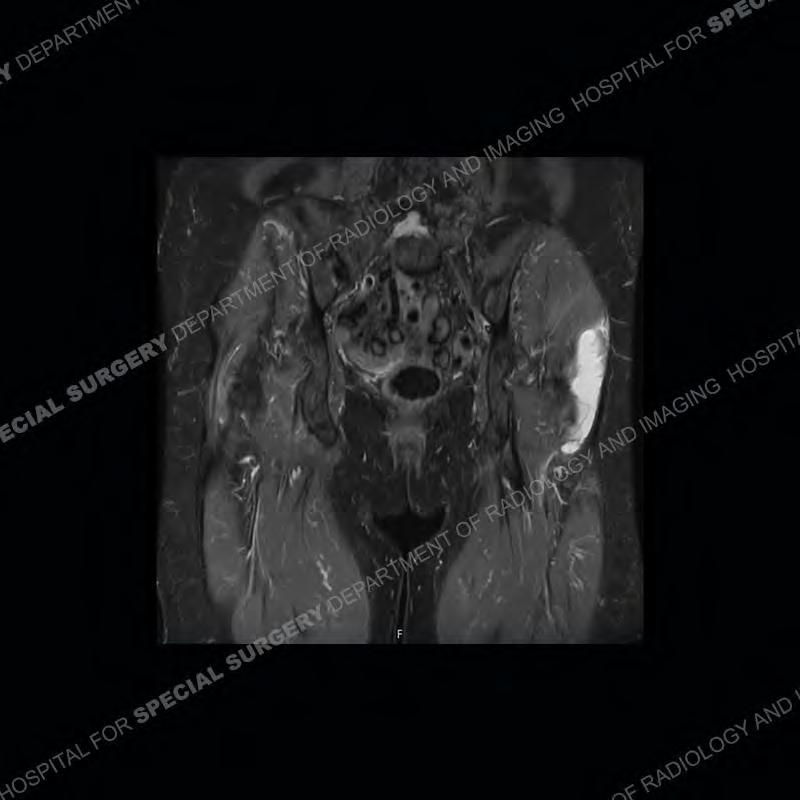
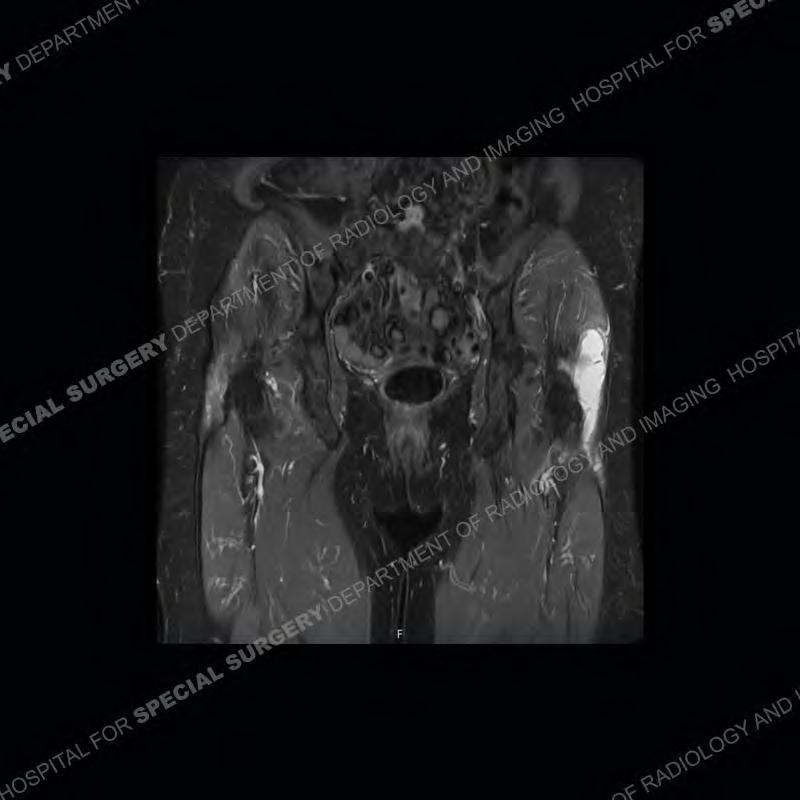
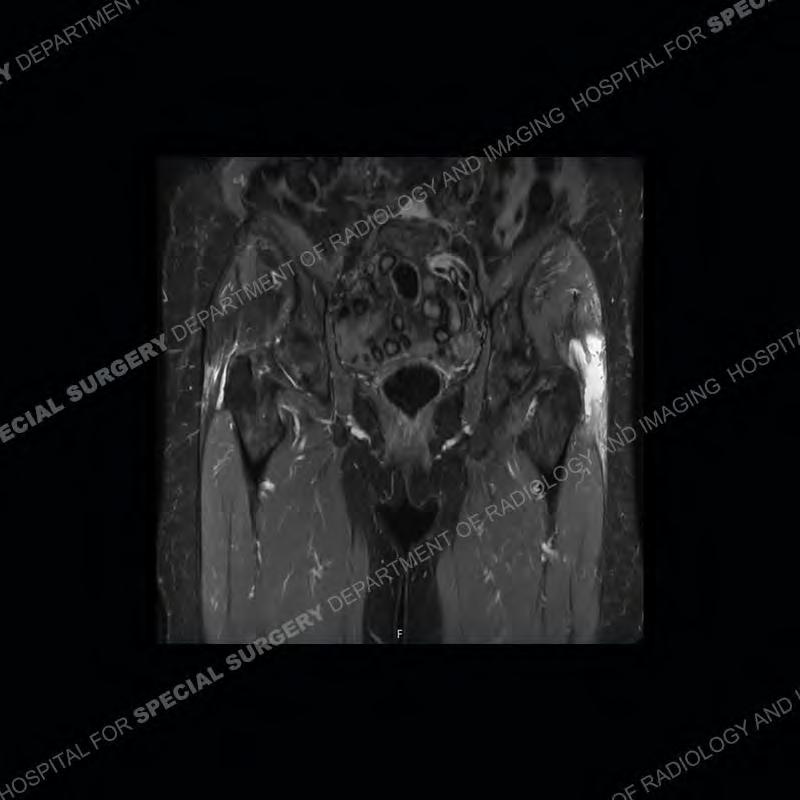
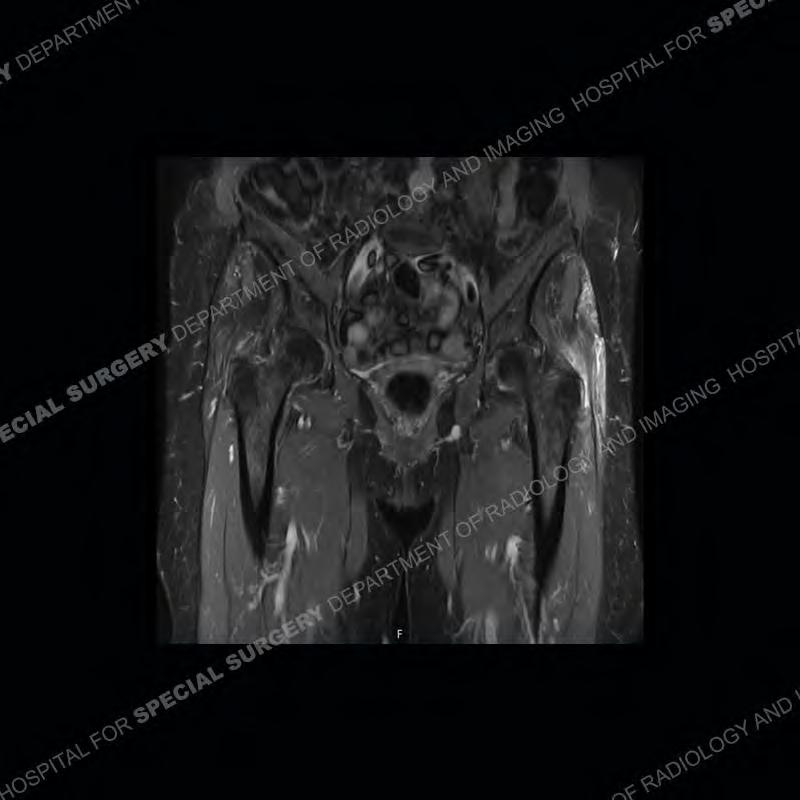
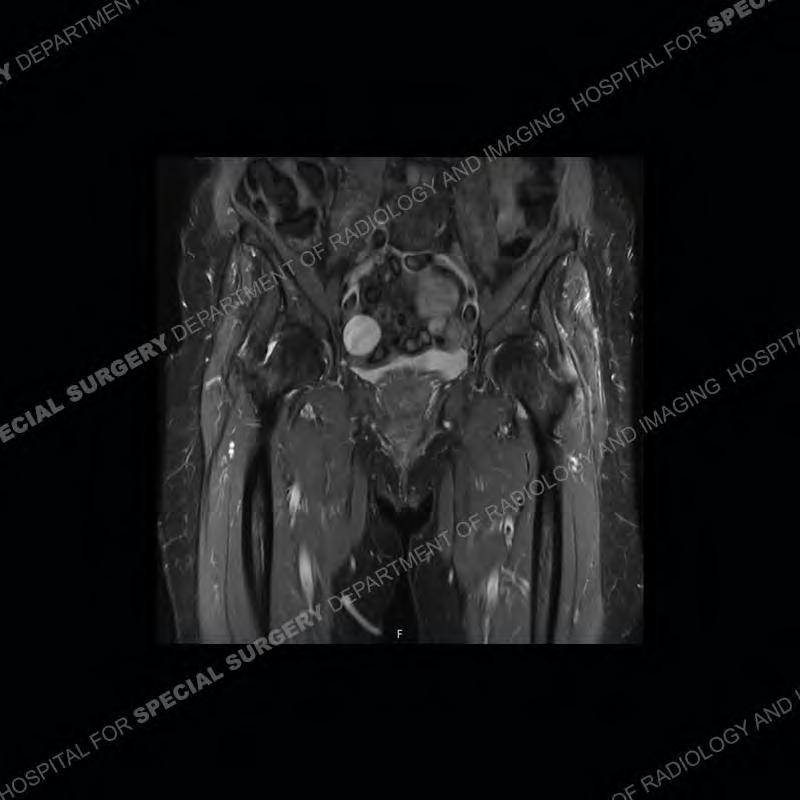
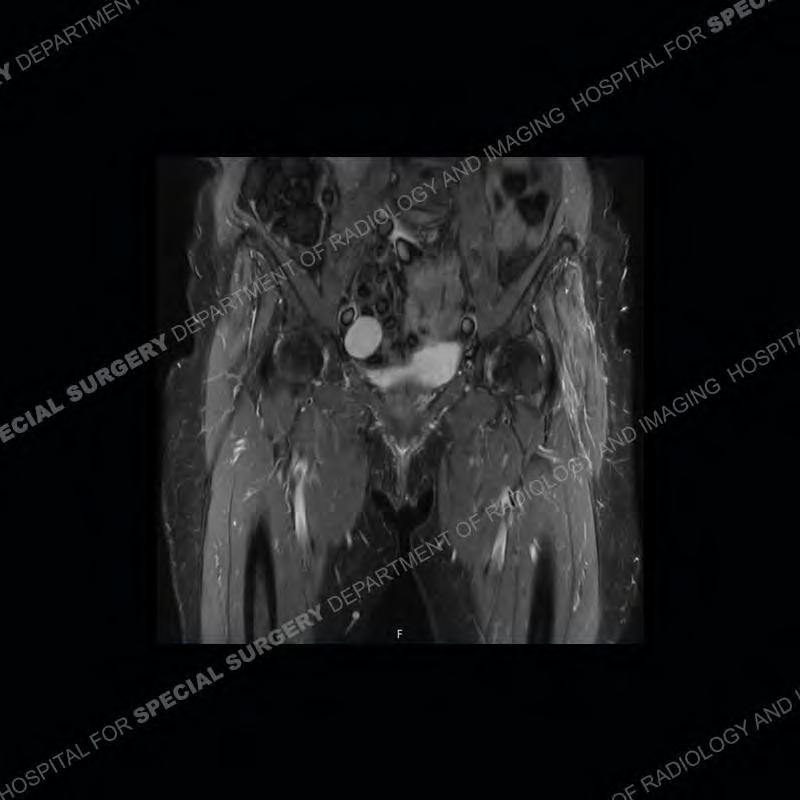
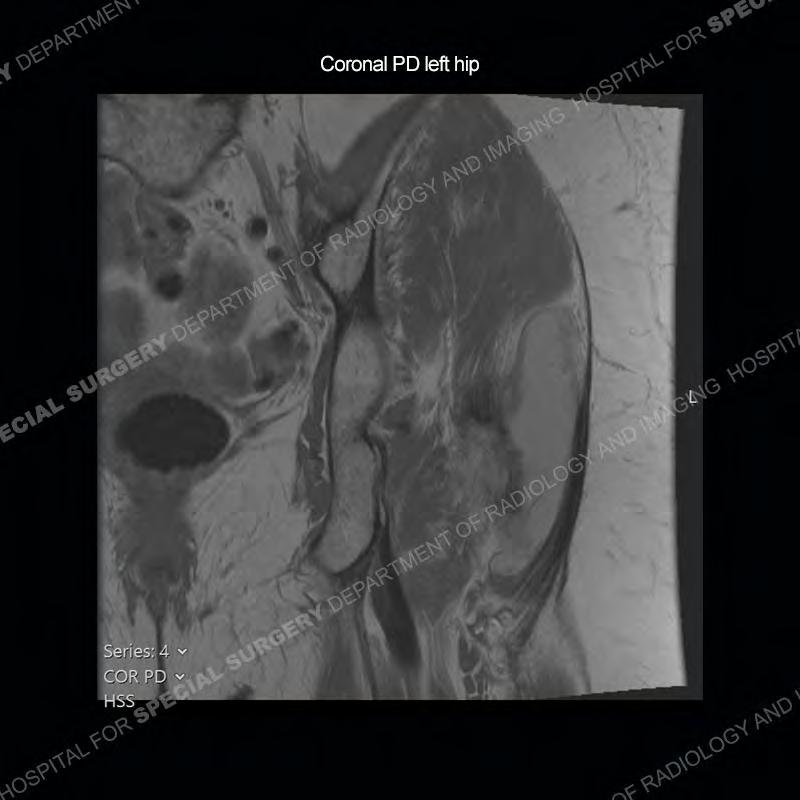
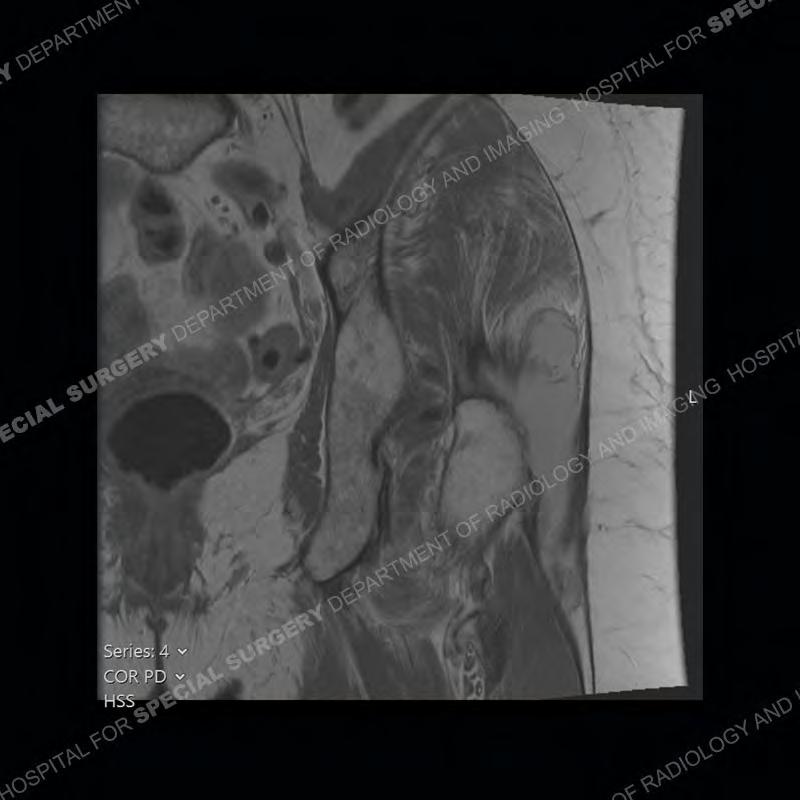
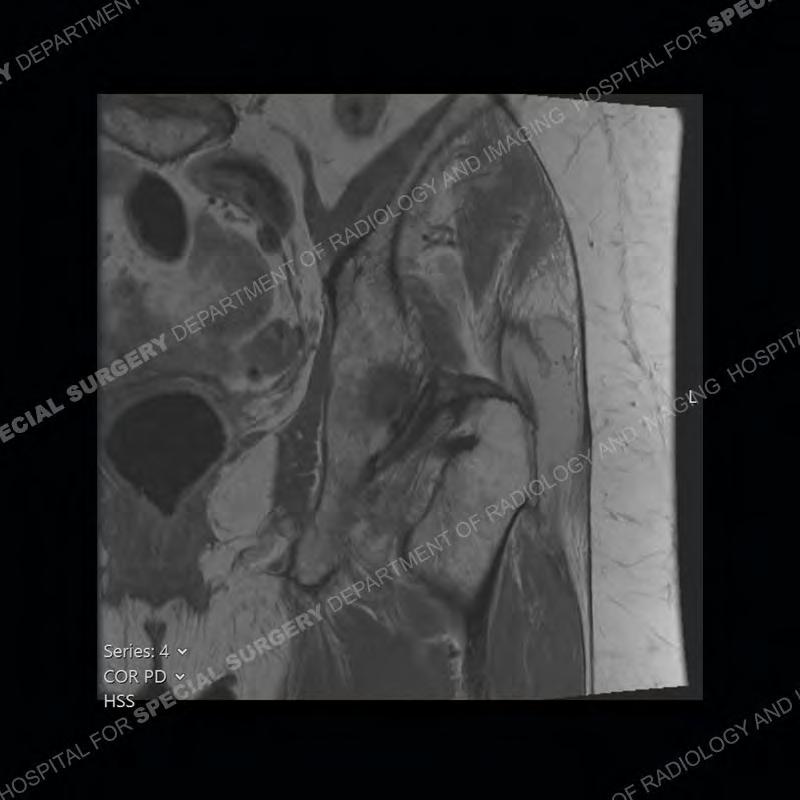
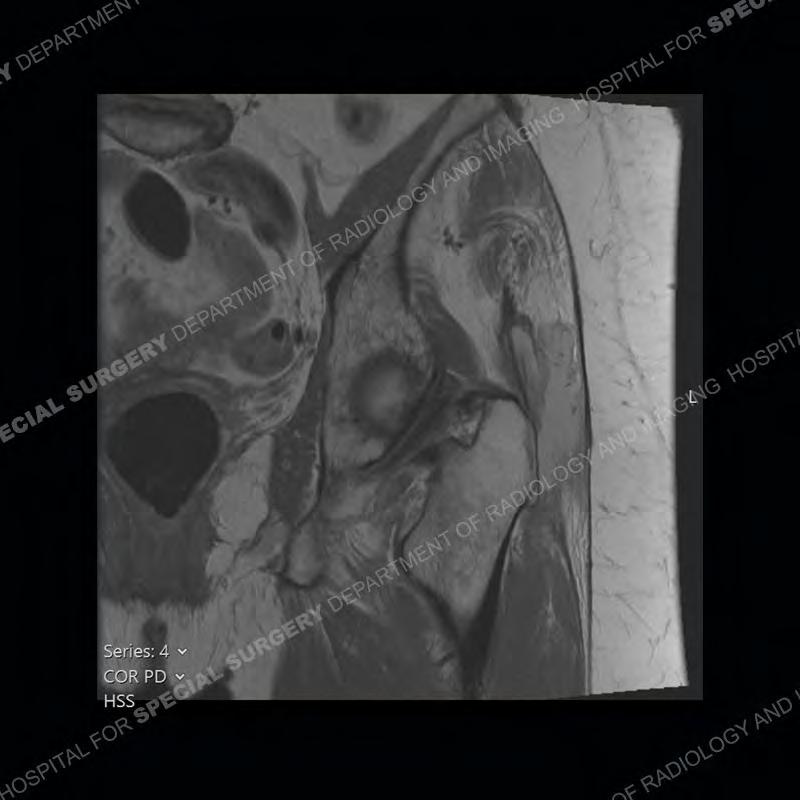
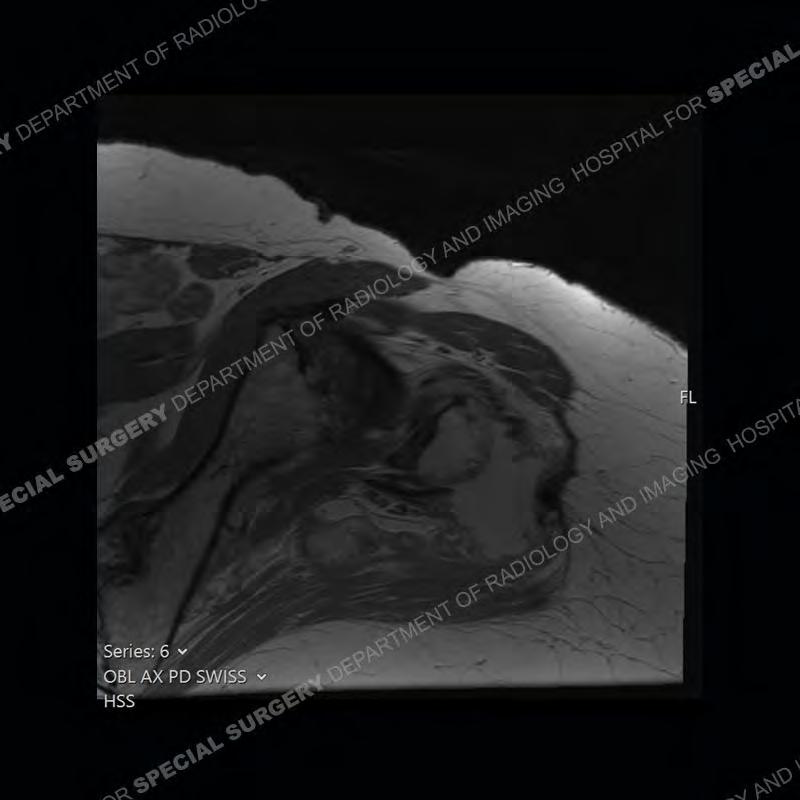
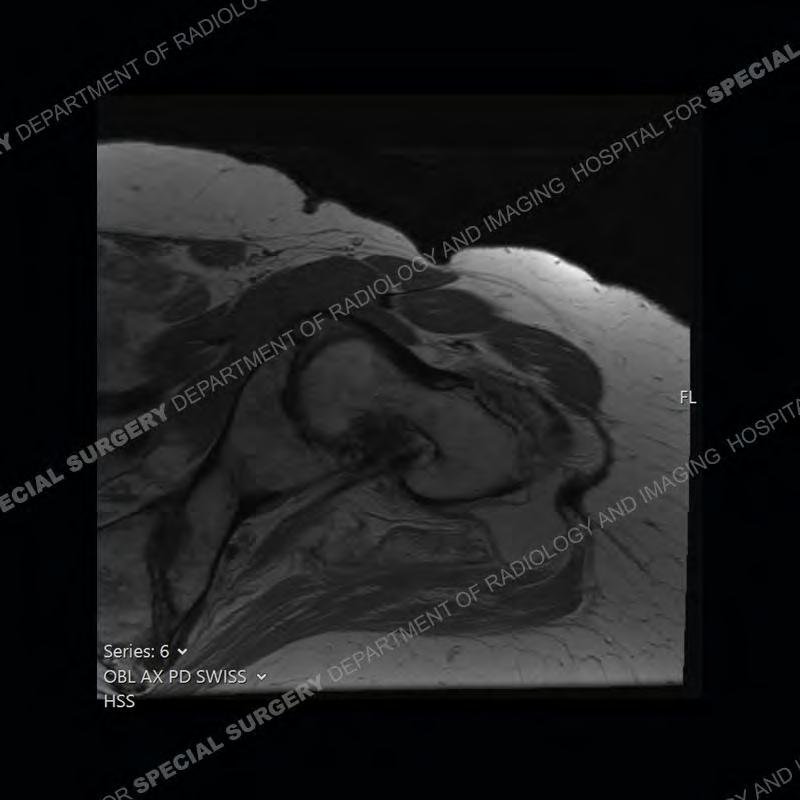
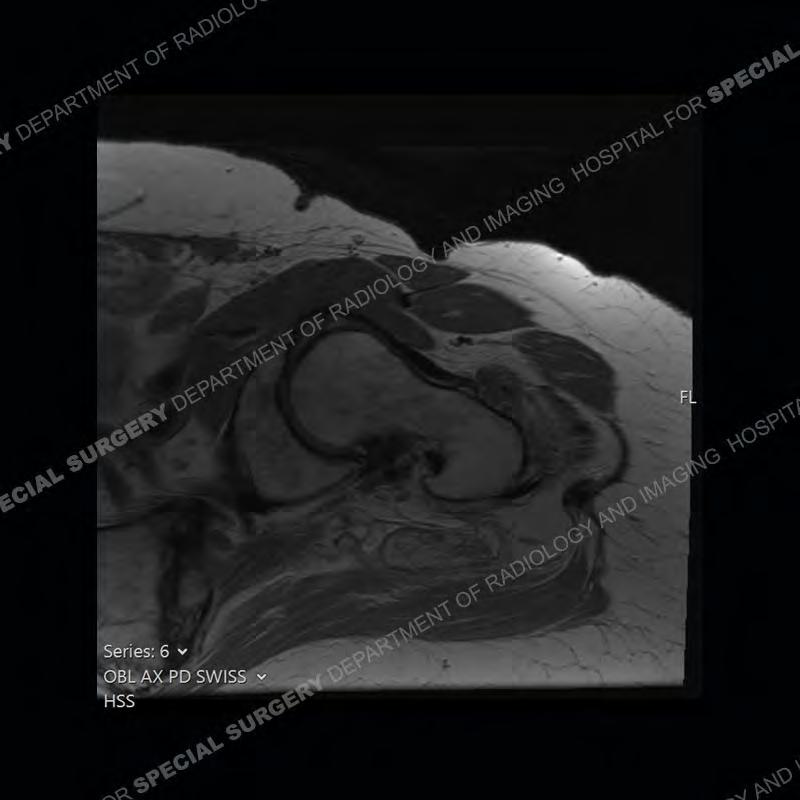
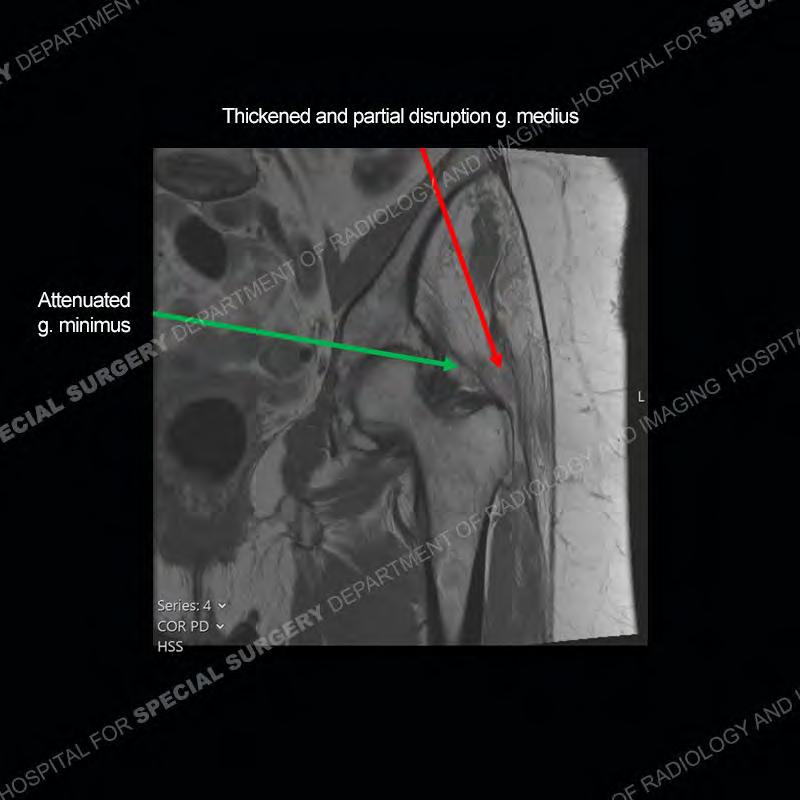
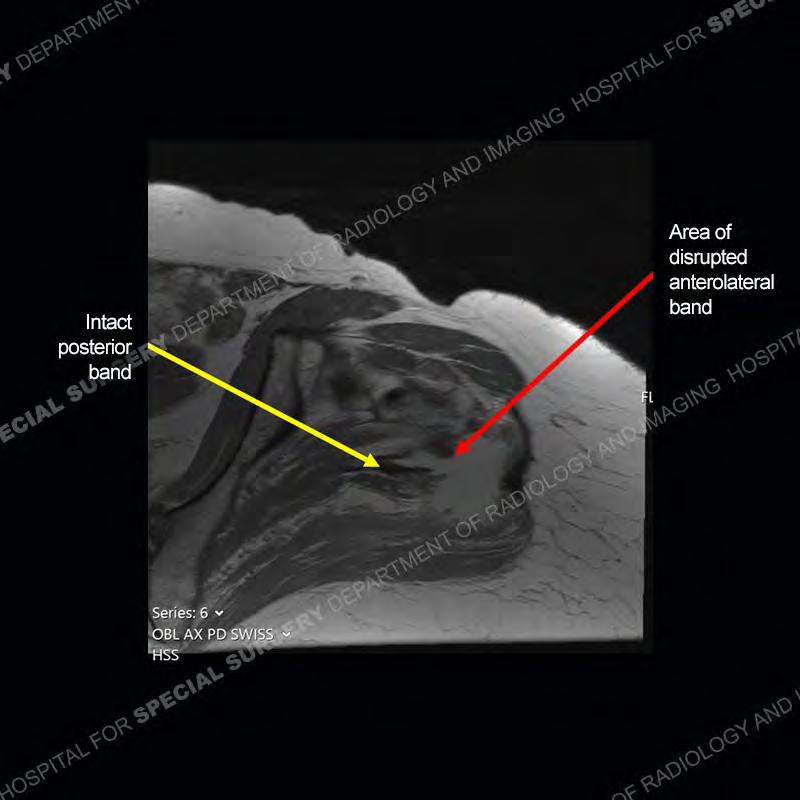
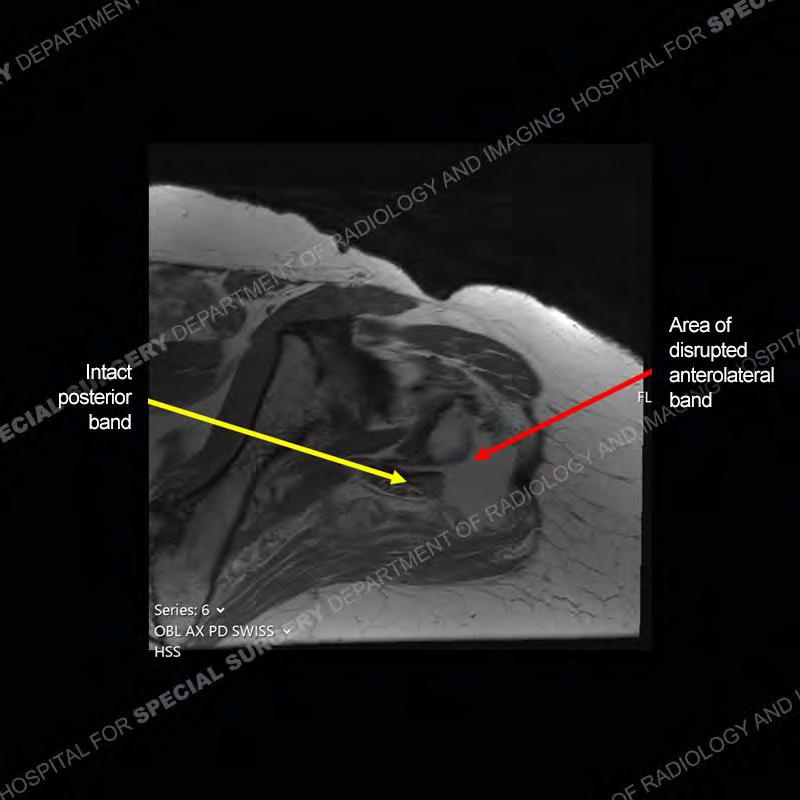
The radiograph is not particularly contributory in this case. The MRI demonstrates markedly abnormal architecture of the gluteus minimus and anterolateral band of the gluteus medius. Portions of the tendons are high signal, portions are highly attenuated, and portions are disrupted. A large, complex fluid collection is present in the adjacent soft tissue.






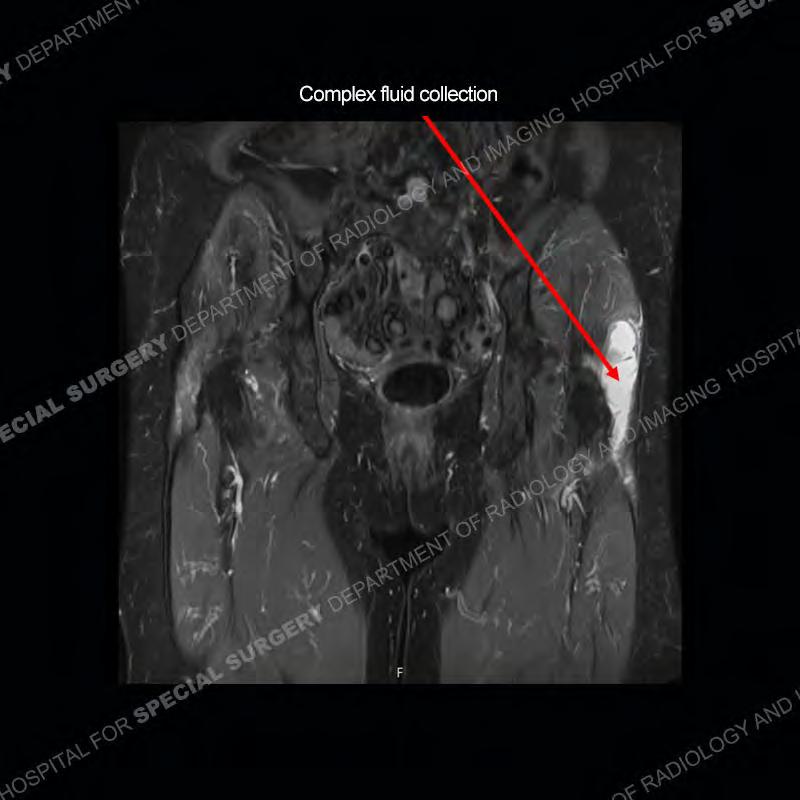









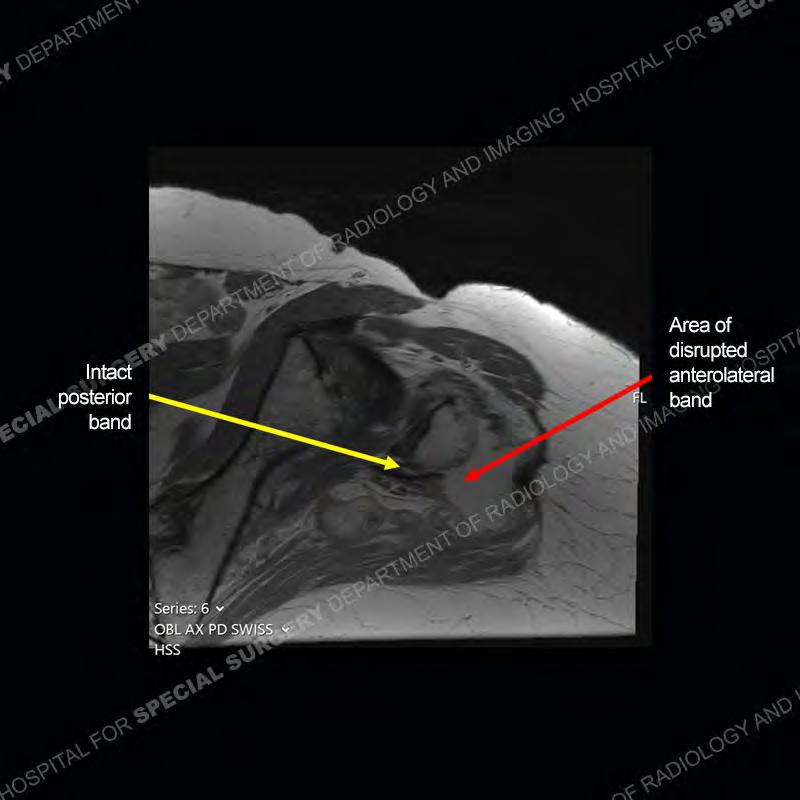
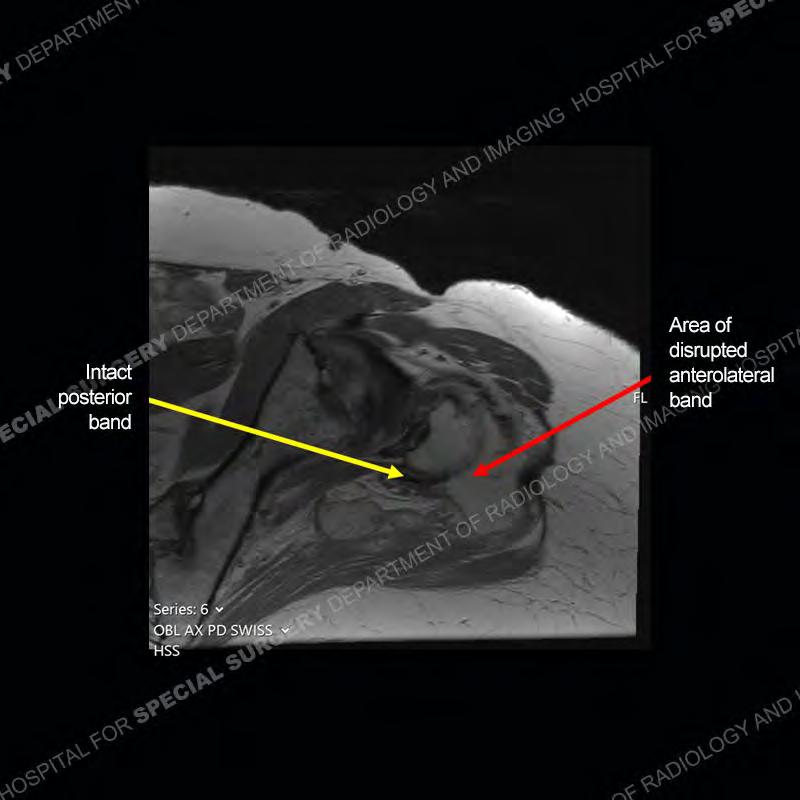


Diagnosis: Gluteal Tendinosis and Disruption with Complex Trochanteric Bursal Collection
Not as much of a diagnostic dilemma as many of the other cases shown but just a nice example of the pathology seen of the gluteal tendons and a cause of trochanteric pain. Although, frequently thought of in isolation, trochanteric bursitis or bursal thickening is much more commonly a reactive change to underlying pathology of the subjacent gluteal tendons. The gluteus medius is divided into a posterior band and an anterolateral band. Tendinosis and partial tearing very commonly will involve the gluteus minimus and especially the more posterior fibers and then propagate into the anterior lateral band of the gluteus medius. Involvement of the posterior band of the medius is much less common and engenders a marked degree of functional impairment.
The bursae about the greater trochanter can be a little bit confusing especially given the terminology. Trochanteric bursitis is implied to mean the subgluteus maximus bursa which is present deep to the maximus and just lateral/superficial to the trochanter. That is the bursa involved in this case. In this case the complexity of the bursa relates to the tendon tearing with inflammatory change and probably hemorrhage accounting for the complexity. Two other, less frequently involved bursa are also present. The subgluteus medius and subgluteus minimus bursa are found just deep to the named tendons. Although pathology does frequently follow the previously described pattern it is possible to have isolated pathology to either the medius or minimus.