Optimizing Quality of Life in Aging Population with Chronic Disease: Insights from a Community Oriented Lifestyle Change Program
Nneka Ulu and Susan Rassekh
Department of Medicine, Northwell Health, Manhasset, NY
Background
● Over36millionU.S.adultshavetype2diabetes,withdisproportionatelyhigh morbidity,disability,andhealthcarecostsinagingpopulations.
● Lifestylefactorssuchasdiet,physicalinactivity,andstresssignificantly contributetodiabetesonsetandprogression
● ExistingevidencefromtheCDCNationalDiabetesPreventionProgram(DPP) trialdemonstrateslifestyleinterventionefficacyinreducingdiabetesincidence; however,real-worldtranslation,especiallyinolderadults,requiresfurther evaluationandtailoredimplementation
Hypothesis
Acomprehensive,culturallytailored,CDC-approvedlifestylechangeprogram deliveredover12monthswillleadtoclinicallysignificantimprovementsin glycemiccontrol,sustainedweightloss,enhancedphysicalactivity,andoverall qualityoflifecomparedtostandardcareamongadultsaged60+withtype2 diabetes.
Methods
Design:Prospective,multi-sitepilotinterventionstudywithpreandpost evaluation.
Participants:150adults≥60yearsdiagnosedwithtype2diabetesrecruitedfrom communityandclinicalsettings. Intervention:
● 12-monthCDC-approvedcurriculumadaptedforagingadults,including nutrition,physicalactivity,stressmanagement,copingskills.
● Initialweeklysessionsfor6months,followedbybi-monthlysessions.
● DeliveredbycertifiedLifestyleCoacheswithpeergroupsupport.
● Modalityoptions:face-to-face,virtualsynchronous,orhybrid.
Measures:
● Primaryoutcome:ChangeinHbA1cat6and12months.
● Secondaryoutcomes:Bodyweight,fastingglucose,physicalactivity (accelerometersandself-report),qualityoflife(SF-36),programretention,and self-efficacyscales.
● Datacollectedatbaseline,6months,12months,andviafollow-upsurveysat18 and24monthstoassesssustainedeffect.
Anticipated Results
● ReductioninHbA1cby≥0.5%at12months,aligningwithclinical recommendations.
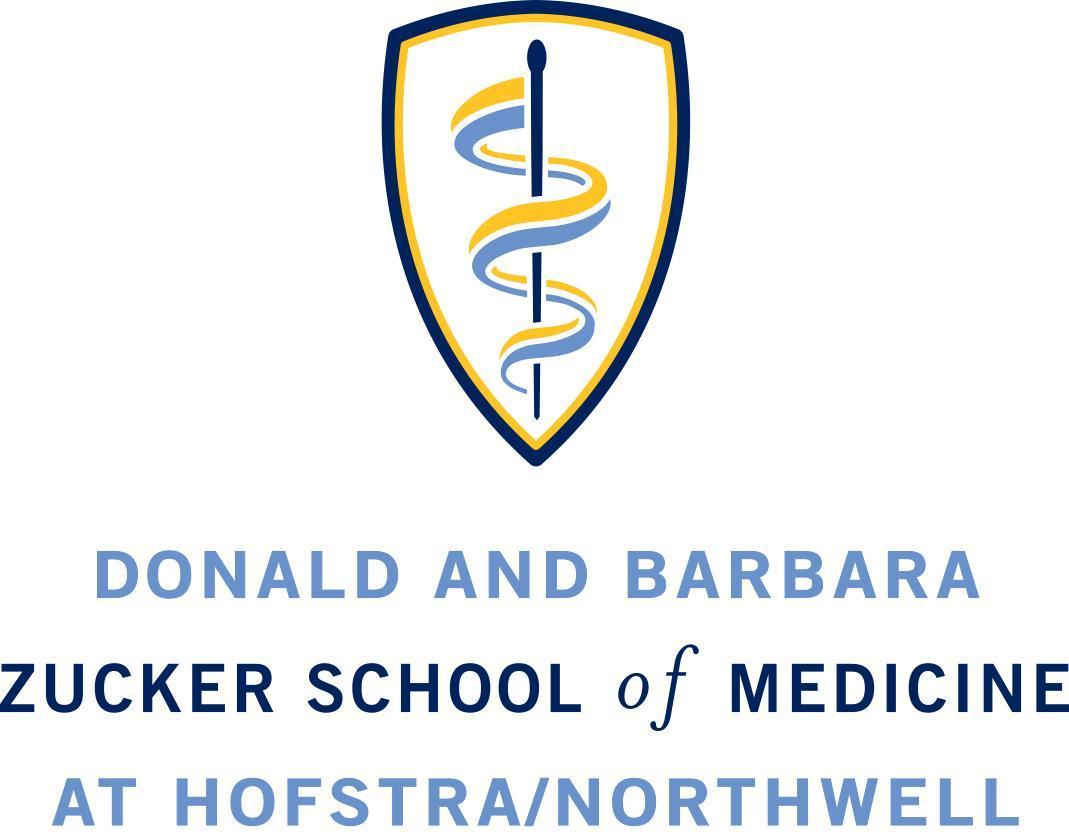
● Meanweightlossof5%orgreatertoreducecomorbidityrisk.
● IncreasedphysicalactivitymeetingCDCguidelinesthroughprogressive engagement.
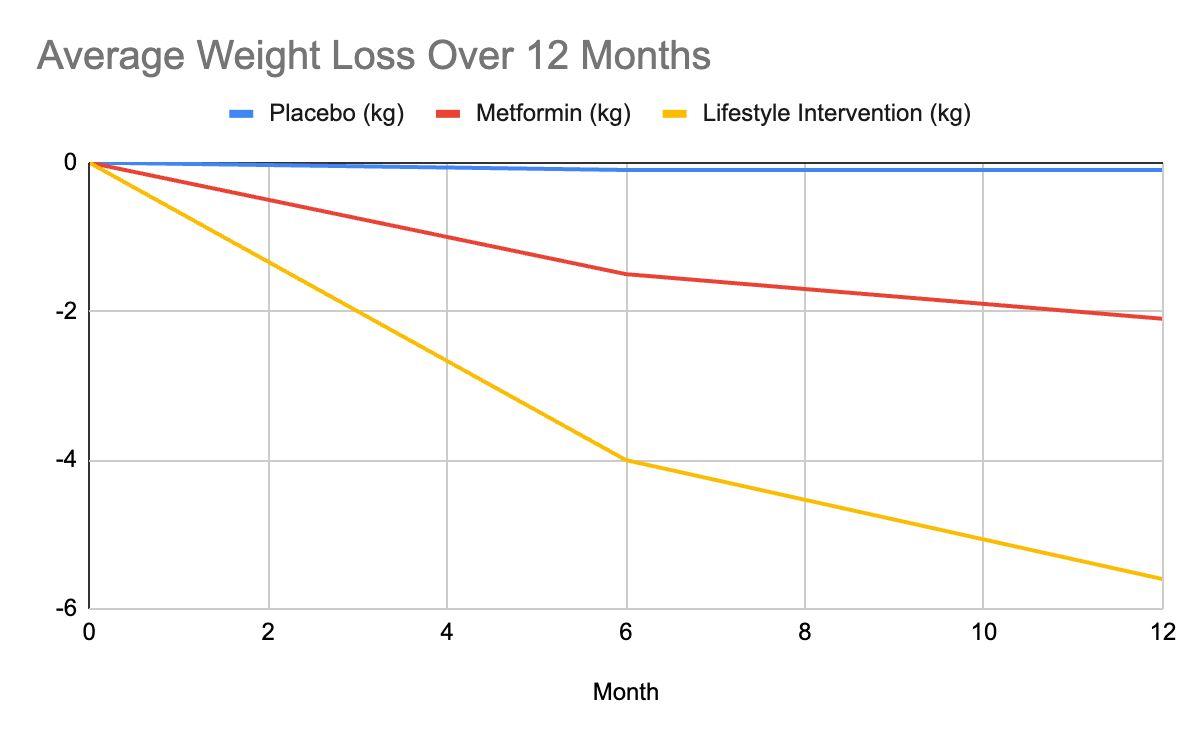
● Highretention(>70%)supportedbycoachingandpeerinteraction.
● Improvedqualityoflifeandpsychosocialwell-beingfrom empowerment-focusedcurriculum.
Conclusions
● TheproposedCDC-approvedlifestylechangeprogramtargetsagingadults withtype2diabetes,apopulationathighriskbutunder-representedin preventionefforts.
● Ourprogramadaptsprovidesatailoredapproachtoolderadults,addressing barrierssuchasmobilityanddigitalaccesswhilefocusingonweightlossand physicalactivity
● Thecombinationofrigorousmethodologicaldesignandflexibledelivery modesaimstoenhanceretentionandadherence,whicharecriticalpredictors ofsuccessinthispopulation.
● Ifeffective,thisprogramcouldsignificantlyreducediabetes-relatedmorbidity andhealthcarecosts,improvingqualityoflifeforagrowingaging demographic.
Future Direction
● IncorporateeHealthtools(apps,wearables)forremotemonitoringand engagement.
● Scaleprogramthroughhealthcareprovidernetworksandemployerwellness initiatives.
● Investigateimpactoncardiovascularevents,frailty,andhealtheconomicsover extendedfollow-up
● Adaptandtesttailoredmodulesforcognitiveimpairmentandethnicminority groups.
Resources
1. KnowlerWC,Barrett-ConnorE,FowlerSE,etal.Reductioninincidenceof type2diabeteswithlifestyleinterventionormetformin.NEnglJMed. 2002;346:393-403
2. AckermannRT.TheU.S.NationalDiabetesPreventionProgramNDPPShows PromiseasaCost-effectiveImplementationStrategy.DiabetesCare. 2025;48:1150-1151
3. MoutonCPetal.LifestyleInterventionStrategytoTreatDiabetesinOlder Adults.DiabetesCare.2022;45:1612-1622
4. FrontiersinClinicalDiabetesandHealthcare.Effectsofdiabetes self-managementforolderadults.2024
5. CDCNationalDPPProgramDetails.