Whats Hot_Immunizations Across the Aging Continuum_2013 Update
Key National Initiatives to Improve Adult Immunization Rates
CDC Healthy Aging Initiative
In 2012, more than 3.5 million Americans reached the age of 65 years. In 20 years, an estimated one of every five Americans will be aged 65 years or older. The Centers for Disease Control and Prevention (CDC) has collaborated with numerous health care and patient advocacy partners to establish tools and resources for adult preventive care. The resulting reports, resources, and interactive tools are available through the CDC Healthy Aging website at http://www.cdc. gov/aging/.
Adults Aged 65 Years and Older
The 2011 report Enhancing Use of Clinical Preventive Services Among Older Adults: Closing the Gap calls attention to the current underutilization of vaccinations, screenings, and other preventive services for adults covered by Medicare.1 Developed collaboratively by CDC, the Administration on Aging, the Agency for Healthcare Research and Quality, and the Centers for Medicare and Medicaid Services (CMS), this report intends to raise awareness of critical gaps among public health and aging service professionals, policy makers, the media, and researchers in order to increase the use
NAVP Workgroup Members
Chairperson
of clinical preventive services, particularly among the underserved.
Eight primary indicators for monitoring the use of clinical preventive services among adults 65 years and older are presented in the report. Two of these indicators target vaccine-preventable illnesses: influenza and pneumococcal disease. The other indicators include counselling for smoking cessation and screenings for various types of cancer, diabetes, cardiovascular disease, and osteoporosis. The shingles (herpes zoster) vaccine is included among a secondary list of recommended preventive services.
Walter A. Orenstein, MD
Professor of Medicine
Associate Director, Emory Vaccine Center
Director, Emory Program for Vaccine Policy and Development
Program Director for Operations Management and Initiatives
Influenza Pathogenesis and Immunology Research Center
Emory University School of Medicine
Atlanta, Georgia
Barbara Resnick, PhD, RN, CRNP, FAAN, FAANP Professor of Nursing
University of Maryland School of Nursing
Adjunct Professor
Department of Epidemiology and Preventive Medicine
University of Maryland School of Medicine
Baltimore, Maryland
William Schaffner, MD
Professor and Chair
Department of Preventive Medicine
Professor of Medicine (Infectious Diseases)
Vanderbilt University School of Medicine
Nashville, Tennessee
Adults Aged 50 to 64 Years
The Healthy Aging initiative provides interactive tools and resources to improve preventive care among adults aged 50 to 64 years. Influenza and pneumococcal vaccines are included among the primary indicators recommended in a comprehensive report developed through collaboration among CDC, AARP, and the American Medical Association.2
Advisory Committee on Immunization Practices
The CDC Advisory Committee on Immunization Practices (ACIP) consists of 15 members external to the federal government with expertise in public health, vaccine safety, efficacy, development, and research, including one individual with consumer perspectives on immunizations. Ex-officio members from 8 federal agencies and 30 additional non-voting representatives from numerous professional societies and liaison organizations add expertise and perspectives. ACIP has statutory authority to provide advice and guidance about vaccines and related agents for control of vaccine-preventable diseases to the Secretary of the Department of Health and Human Services (HHS), the Assistant Secretary for Health, and the Director of CDC.3 ACIP meets three times a year to assess emerging research and trends. The committee develops general recommendations regarding the use and storage of vaccines and annually updates recom-
mended immunization schedules for children, adolescents, and adults. ACIP also establishes and periodically reviews vaccine recommendations for children and adolescents through the Vaccines for Children Program. The committee may add, alter, or withdraw specific vaccine recommendations as new information becomes available or the risk of disease changes. ACIP forms its recommendations on evidence including population-based studies evaluating efficacy, safety, cost, benefits, and riskbenefit analyses.3
ACIP Revision of General Recommendations
The most recent version of ACIP’s General Recommendations on Immunization, released January 2011 and superseding the 2006 version, includes information about vaccine administration, dose, number, and timing; contraindications and precautions; and storage and handling.4 ACIP collaborated with of the American Academy of Pediatrics, the American Academy of Family Physicians, the American Congress of Obstetrics and Gynecology, and the American College of Physicians to develop these recommendations. CDC and HHS reviewed and approved the recommendations, which were published in CDC’s Morbidity and Mortality Weekly Report4 and reprinted in Epidemiology and Prevention of VaccinePreventable Diseases, 12th edition, commonly known as the Pink Book, available at http://www.cdc.gov/vaccines/ pubs/pinkbook/index.html.
Important additions and updates to the 2011 General Recommendations on Immunization include:4
• Conditions commonly misperceived as contraindications to vaccinations (new section).
• Stricter requirements for the storage and handling of immunobiologics.
• Specific guidance on immunobiologics that are out of temperature range.
• Guidance on vaccinations for recipients of hematopoietic cell transplants (HCT).
A key addition to the updated report is a listing of conditions commonly misperceived as contraindications to receiving certain vaccines. Examples of misperceptions regarding contraindications for vaccination include mild acute illness with or without fever; mild-to-moderate local reaction; lack of previous physical examination in a wellappearing person; current antimicrobial therapy; recent exposure to infectious disease; convalescent phase of illness; preterm birth; history of penicillin or other non-vaccine allergies; relatives with allergies; or receiving allergen extract immunotherapy. Presence or history of these conditions is not considered a contraindication to receiving any of the available vaccines.4
In the discussion of the Storage and Handling of Immunobiologics, requirements for storage have become more stringent and specific to maintain vaccine quality and avoid reducing or destroying vaccine potency. For example, vaccines should not be placed inside a new storage location until the unit has maintained a stable and correct temperature over time. Guidance is also provided with regard to the safety of storing clinical specimens and vaccines within the same storage unit. Clinical specimens may be stored within the same unit with vaccines; however, the clinical specimens should be placed on the shelf below the vaccines to prevent contamination of the vaccines. The 2011 update adds guidance on steps to take when vaccines reach an out-of-range temperature. Vaccines stored at an inappropriate temperature should not be administered. Furthermore, if such a vaccine has been administered to a patient, readministration with an appropriately stored vaccine is recommended.4
Updates for vaccinating HCT recipients also are outlined. These recommendations are based on data confirming that antibody titers are reduced following transplantation. HCT recipients of all ages are at increased risk for certain vaccine-preventable diseases, including diseases caused by encapsulated bacteria (i.e., pneumococal, meningococcal, and Haemophilus influenzae type b [Hib]
infections). Regardless of whether the HCT source is autologous or allogeneic, revaccination with inactivated vaccines should be routinely performed 6 months after HCT, instead of waiting 12 months. Influenza vaccine may be administered between 4 and 6 months after HCT, and a second dose should be considered. Pneumococcal revaccination should begin 3 to 6 months after the transplant, with 3 sequential doses of pneumococcal conjugate vaccine, followed by a dose of pneumococcal polysaccharide vaccine. A 3-dose regimen of Hib vaccine should be administered beginning 6 months after HCT, with each dose separated by 1 month—a change from the previous 2006 recommendations. Measles, mumps, rubella (MMR) vaccine should be administered 24 months following transplant for immunocompetent HCT recipients. Finally, the recommendations outline guidance for case-by-case consideration of the risks and benefits of using the varicella vaccine in HCT recipients.4 Barriers and challenges associated with adult immunizations are discussed in the General Recommendations on Immunization, including lack of knowledge about the importance of immunization in adults among both patients
and providers. Cost and lack of insurance or underinsurance also present barriers. In addition, providers whose patients’ vaccination history is unknown are challenged to determine which vaccines to use, when the vaccines should be administered, and how to bring patients’ vaccination status up to date. The report offers guidance to address these situations and challenges.4
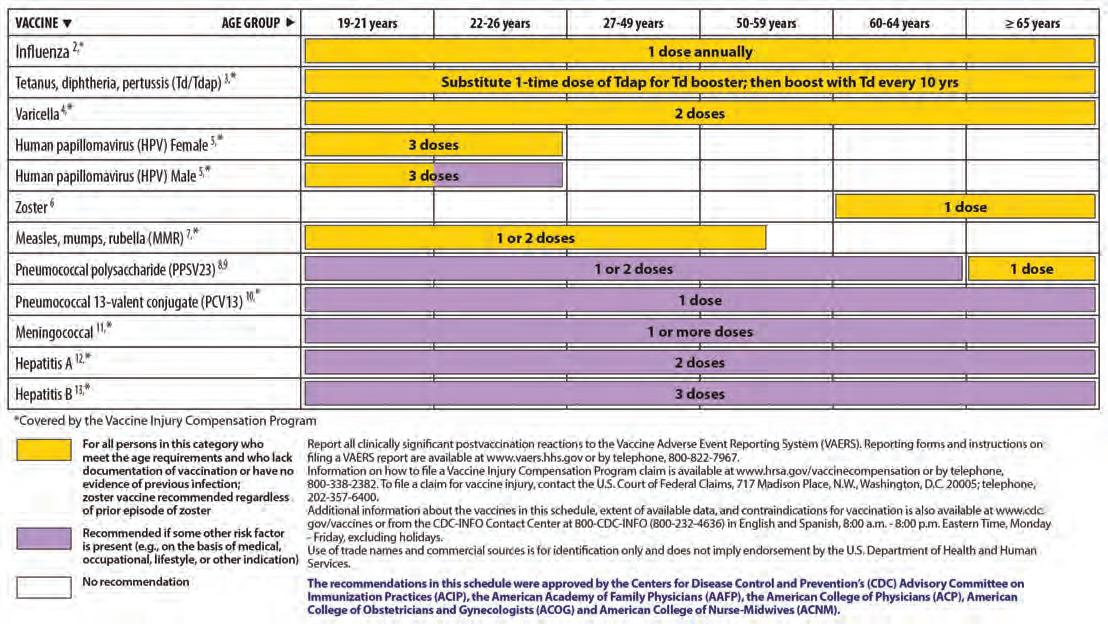
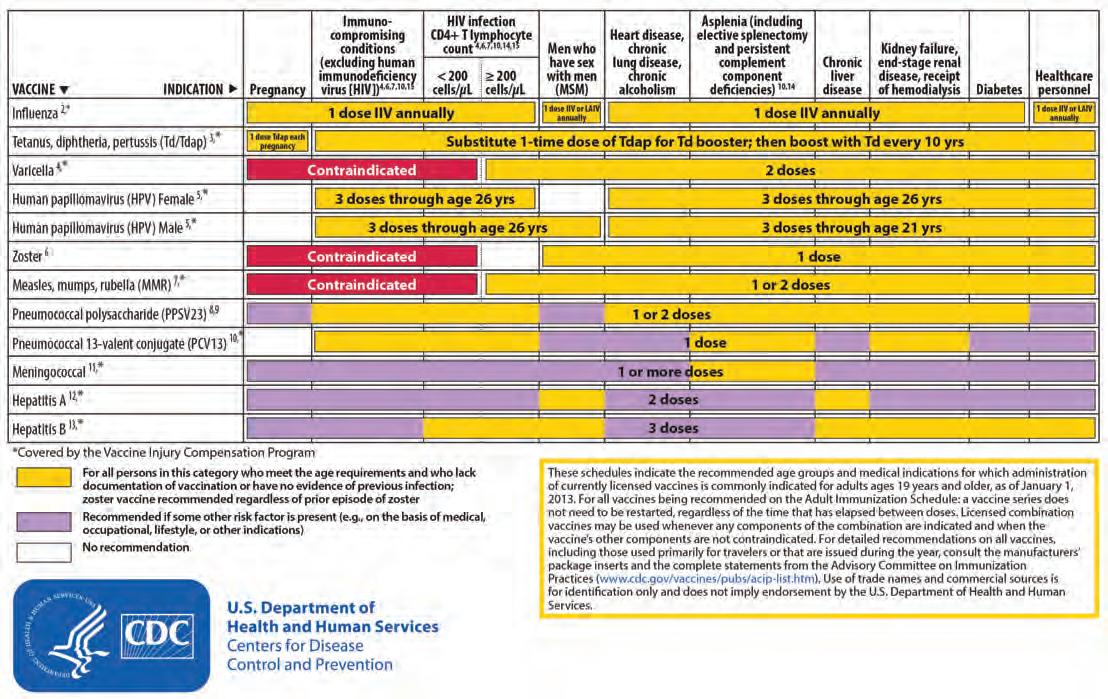
2013 Adult Immunization Schedules
Annual vaccine schedules are published every January in Morbidity and Mortality Weekly Report. Recommendations outline which vaccines should be administered to individuals of specific ages, and state the appropriate route, dose, and frequency of administration of the vaccine as well as any associated immunoglobulin or antimicrobial agent as appropriate. The 2013 Adult Immunization Schedules are shown in Figures 1 and 2. 5
Health Care Personnel
In recognition of the risks of transmitting vaccine-preventable illnesses among those who work in health care settings and patients seeking care, ACIP updated the recommendations for immunizing health care person-
nel in November 2011. Recommended vaccines include hepatitis B; influenza; MMR; varicella; tetanus, diphtheria, and acellular pertussis (Tdap)/tetanus and diphtheria (Td); and meningococcal.6 These recommendations are summarized in Table 1 6,7 Additional resources for immunization and education of health care personnel are available from the Immunization Action Coalition (IAC) at http://www.immunize.org/handouts/ healthcare-worker-vaccination.asp.
Tdap in Adults Aged 65 Years and Older
In February 2012, ACIP voted 14 to 1 to expand recommendations for Tdap to include all adults aged 65 years and older who have not received Tdap. This recommendation is based on increasing incidence of pertussis and evidence of safety and efficacy of Tdap in this population and replaces previous recommendations that limited Tdap to those in contact with infants younger than 12 months.8
Nominations to Serve on ACIP
CDC is slated to begin the next cycle of evaluating potential ACIP candidates in fall 2013 for selection of nominees to replace members whose terms will end on June 30, 2014.
Hepatitis B
Influenza
Measles, mumps, and rubella
Varicella (chickenpox)
Give 3-dose series (dose #1 now, #2 give 1 month later, #3 approximately 5 months after #2). Give IM. Obtain anti-HBs serologic testing 1–2 months after dose #3.
Give 1 dose of influenza vaccine annually. Give inactivated injectable influenza vaccine IM or intradermally, or give live attenuated influenza vaccine intranasally, as indicated.
For HCP born in 1957 or later without serologic evidence of immunity or prior vaccination, give 2 doses of vaccine, 4 weeks apart. For HCP born prior to 1957, see CDC recommendations. Give SC.
For HCP who have no serologic proof of immunity, prior vaccination, or diagnosis/verification (by a health care provider) of a history of varicella disease or herpes zoster, give 2 doses of varicella vaccine, 4 weeks apart. Give SC.
Tetanus, diphtheria, and pertussisGive a one-time dose of Tdap as soon as feasible to all HCP who have not received Tdap previously. Give Td boosters every 10 years thereafter. Give IM.
Meningococcal
Give 1 dose to microbiologists who are routinely exposed to isolates of Neisseria meningitidis. Give IM or SC.
ACIP = Advisory Committee on Immunization Practices; anti-HBs = hepatitis B surface antibody; CDC = Centers for Disease Control and Prevention; HCP = health care personnel; IM = intramuscular; SC = subcutaneous; Td = tetanus and diphtheria; Tdap = tetanus, diphtheria, and acellular pertussis.
Source: Adapted from references 6 and 7.
Table 1. Health Care Personnel Vaccine Recommendations
Figure 1. Recommended Adult Immunization Schedule, by Vaccine and Age Group—United States, 2013
Figure 2. Recommended Vaccinations Indicated for Adults Based on Medical and Other Indications— United States, 2013
Source: Reference 5.
Selection of members is based on candidates’ qualifications to contribute to the accomplishment of ACIP objectives. See the CDC website, http://www. cdc.gov/vaccines/acip/committee/ req-nominate.html, for details. The deadline for receipt of applications is November 15, 2013.
Immunization Action Coalition
IAC works to increase immunization rates and prevent disease by creating and distributing educational materials for health professionals, government health agencies, and the public to enhance effectiveness and delivery of immunization services. IAC collaborates with and receives financial support from CDC to develop practical tools and resources for disseminating ACIP recommendations and other immunization-related data.9
The IAC website, http://www. immunize.org, provides handouts for health professionals on a variety of topics, such as vaccine administration and screening tools, as well as patient handouts. IAC also provides resources for vaccination clinics, including “howto” information about documentation, coding, and billing.
Prevention and Public Health Fund: Program Area 5
The Prevention and Public Health Fund was established to support cooperative agreements that assist grantees in implementing changes under the Affordable Care Act (ACA). Six program areas comprise the fund. Program Area 5 focuses specifically on implementing adult immunization programs and is designed to help awardees prepare for an environment of expanded insurance coverage for adult immunizations.10
In September 2011, cooperative agreements, collectively totaling $5.7 million, were awarded to five states: Arkansas, Connecticut, Massachusetts, Minnesota, and Washington. The award amounts range from $400,000 to $2 million. Awardees are required to collaborate with employers to increase immunizations among employees, and with phar-
macies to improve immunization rates among adult customers. In addition, awardees are engaging in expansion of adult immunization at community health centers, improving rates among health care workers, ensuring ACIPrecommended immunizations are included in preventive benefits by state Medicaid programs, and improving specific immunizations within certain settings (e.g., hepatitis B in health departments and clinics for the treatment of sexually transmitted infections; influenza and pneumococcal vaccine administration at hospital discharge).10
Employer-based efforts include a variety of collaborative and technologyfocused activities. State awardees are working with local business associations to identify and overcome barriers to immunizations, involving occupational nurse groups, local health departments, and community immunizers to staff employer vaccine clinics. They also are developing resource toolkits for employer clinics. Many programs are aimed to expand access to and use of immunization information systems. Some programs target specific groups of employees, including child care workers and state government agency employees.10
Awardees are collaborating with pharmacists and pharmacies in many ways. All grantees are identifying barriers by working with state pharmacist associations and are working to expand the types of vaccines offered, with an emphasis on shingles. Furthermore, they are working to certify and train pharmacists as immunizers, expand pharmacists’ use of immunization information systems, identify payment issues, and coordinate with other providers in states where a prescription is required for vaccine administration.10
CDC WhatWorks! Increasing Adult Vaccination Rates
CDC has compiled a list of low-cost, easy-to-implement tools, strategies, and resources that are demonstrated to improve adult immunization rates. Examples include standing orders,
computerized record reminders, home visits, patient education and reminders, and personal health records. Available in print and interactive formats, each strategy is fully described with a definition, advantages and disadvantages, steps for implementation, and evidence of effectiveness.11
Partnership for Adult Vaccination and Education
The Partnership for Adult Vaccination and Education (PAVE) is a collaborative led by the University of Wisconsin School of Medicine and Public Health, the Physicians’ Institute for Excellence in Medicine, Healthcare Performance Consulting, and CME Enterprise. PAVE aims to increase the rates of ACIPrecommended immunizations for adults and adolescents in the United States through education, outreach, dissemination of immunization resources, and modeling of performance improvement practices. Educational initiatives focus on overcoming barriers, improving communication skills, changing attitudes, enhancing knowledge, and incorporating system-level improvement strategies. Education for clinicians highlights three models of performance improvement. One involves maintenance of certification by the American Board of Internal Medicine; another supports local health care practices in Wisconsin; and the third targets primary care practices in Florida, Georgia, Kentucky, and Oklahoma.12
Self-assessment, curriculum tools, and assessment strategies allow for adaptation of interventions to meet local needs. PAVE has pooled and developed numerous resources for health professionals, including adult immunization recommendations and tools for broad integration, videos, slide presentations, patient fact sheets, and performance improvement activities. Resources are available at http://paveresources.com/. ✻
A Pathway to Leadership for Adult Immunization
The National Vaccine Advisory Committee (NVAC) was established in 1987 through the Public Health Service Act. NVAC advises and makes recommendations on issues related to ensuring adequate supplies of vaccines, identifying research priorities and measures to enhance safety and efficacy of vaccines, and defining priority areas of government and nongovernment collaboration. In 2009, NVAC was charged to develop recommendations for establishing a comprehensive, sustainable, national adult immunization program that would reduce vaccinepreventable diseases by improving adult immunization coverage levels. Over a period of 2 years, NVAC reviewed reports and recommendations that had been generated over the past 20 years to address challenges in adult immunizations. Through this effort, NVAC identified and studied nine categories of barriers to adult immunization, including lack of coordination, public knowledge, provider recommendations, access to and utilization of health care services, and inadequate use of immunization schedule reminder or assessment systems. Other barriers included financial impediments, racial and ethnic disparities, health literacy, and safety concerns. NVAC sought novel ways to overcome persistent unresolved challenges that perpetuate morbidity and mortality from vaccinepreventable illnesses in adults. This analysis led to three broad recommendations and a national strategy described in a white paper approved by the NVAC in June 2011 and published in Public Health Reports in January 2012.13
Recommendation #1: National Leadership for an Adult Immunization Program
Because adult health care is delivered by many different types of providers practicing in a variety of specialty and generalized practices, strong national leadership of adult vaccine efforts is
necessary to achieve widespread sustained improvements in adult immunization rates. NVAC recommends that HHS should develop and adequately support a coordinated and comprehensive National Adult Immunization Program, utilizing an Interagency Working Group that would be accountable for providing annual progress reports to NVAC.13
Recommendation #2: Resources for an Adult Immunization Program and Action Plan Implementation
Financial and infrastructure resources must be allocated to enact the strategic action plan. Resources should include staffing for a CDC National Adult Immunization Program office at levels sufficient to implement the national strategic action plan.13
Recommendation #3: Strategic Plan for Adult Immunization
NVAC called for the recommended Interagency Working Group to develop a National Strategic Plan for Adult Immunizations. This plan should emphasize innovation, align with the National Vaccine Plan, and meet the goals of Healthy People 2020. At a minimum, the plan components would include mechanisms to address the following gaps in adult immunization and the key elements outlined by NVAC in accordance with the National Strategic Plan for Adult Immunizations.13
Improving Infrastructure
NVAC advises working to align immunization recommendations across agencies, and similarly evaluating and harmonizing quality measures for adult vaccination from various sources to the extent feasible, with metrics expanded to include vaccine uptake and barrier identification and mitigation. Other infrastructure recommendations include the addition of immunization require-
ments and funding in federal grant programs and integration of funding for adult immunization coordinators into state and local grants. CDC should establish and expand collaborative partnerships with a variety of organizations to develop and coordinate an infrastructure that supports and facilitates the delivery of adult vaccines through the expanding network of adult vaccinators.
Expanding Access
Barriers that prevent multiple suppliers for each licensed and recommended vaccine should be examined and addressed to ensure a consistent and adequate supply of adult vaccines for the United States. In addition, savings in childhood vaccine spending from Section 317 of the Public Health Service Act—realized through implementation of the ACA—should be redirected to address gaps in adult immunization efforts. Such funds could be used to purchase vaccines for targeted, highrisk adult populations. Other strategies include enhancing existing partnerships between public health and interested stakeholders, and developing new collaborations to encourage and provide adult vaccination services. Access also could be improved through standardizing Medicaid vaccine administration reimbursement rates among all states.
Implementing Provider-Based and System-Based Interventions
Adult immunization networks should be expanded to connect traditional adult immunizers with providers who may not be traditionally or widely involved in adult immunization (e.g., obstetricians/ gynecologists, subspecialists, pharmacists). These providers can be engaged in educating patients, and encouraging and administering vaccines. The creation of adult immunization stations or vaccination clinics in children’s hospitals, in ACA-created exchanges, and in schools could serve adults and their children. Electronic health records (EHRs) should be utilized in forming
connections. Provider education that integrates best practices, standards of care in immunizations, and quality improvement should be developed. Vaccine providers and partners need to be educated about the adult vaccinerelated provisions of the ACA and quality improvement methods; refinement of quality assessment activities among insurers and agencies should be facilitated. Best business-related practices need to be identified and shared in areas such as inventory management, billing, and barrier reduction. Immunization information systems should be improved and expanded to include information for adult vaccination standards as well as childhood immunizations. Systems also should
promote data exchange and interfacing with EHRs to assist providers and generate reminder prompts.
Increasing Community Demand
Ongoing, comprehensive education and widespread outreach should be targeted to the public and providers to increase demand at a grassroots level, from the public, patients, caregivers, and families to their health care providers.
Conducting Research
NVAC identified a comprehensive list of research needs to gather information necessary to achieve and support widespread, sustainable improvements in adult immunizations. The list ranges from evaluating vaccine costs and reim-
State-Based Initiatives
States are at the center of grassroots immunization activities and are crucial partners in implementing immunization programs and services. In an effort to ensure vaccines are administered to patients who need them, states work to determine community immunization needs and capacity for delivering them. Vaccines are frequently delivered through health departments and other clinics and through collaboration between states and primary care practices. State health agencies engage in outreach and education to encourage patients to be vaccinated and to inform and prepare providers. States actively monitor immunization rates, vaccine shortages, and disease outbreaks. The following examples describe some state-level immunization initiatives and programs.
Regional Adult Immunization Seed Grants
In January 2012, the National Business Coalition on Health launched the Adult Immunization Seed Grant Program that provided four state-based coalitions with grants to improve immunizations within the workplace. The four coalitions selected were the HealthCare 21
Business Coalition, the MidAtlantic Business Group on Health, the Nevada Health Care Coalition, and the Virginia Business Coalition on Health.14 HealthCare 21 Business Coalition in Knoxville, Tennessee, is partnering with Lincoln Memorial University to improve immunization rates in rural areas. Together, these groups plan, educate, and provide employers with the necessary tools to increase employee awareness about the importance of receiving vaccinations.
MidAtlantic Business Group on Health, centered in the Baltimore, Maryland/Washington, DC region, has partnered with American University School of Education, Teaching, and Health; Erickson Living; and McCormick & Company. Together, they aim to prevent pertussis through an initiative focused on raising employee awareness on the increasing incidence and risks of pertussis infection, the importance of becoming immunized, and staying current with Tdap vaccinations.
Nevada Health Care Coalition in Reno, Nevada, is working to increase education, awareness, and immunization rates among employees. The 18 partnering employers represent most of the major employers in the Reno, Sparks,
bursement, to uptake data and trends, economic benefits, and reimbursement systems. Research is also needed to evaluate provider education, assess the relative impact of different vaccine providers and venues, and measure changes in public and provider knowledge, attitudes, and practices following implementation of the national strategy. Other research priorities include studying vaccine stocking and administration practices of providers, impact of the anticipated 2013–2014 Medicaid reimbursement modifications, influences of health literacy on health and vaccination disparities, use of social networking, state-level policies and practices, and discovery of innovations in vaccines and delivery systems.13 ✻
and Carson City areas of the state. Their goal is to reduce the burden of vaccinepreventable illness that employees pose not only to their coworkers and customers, but also to their families and their community.
Virginia Business Coalition on Health, located in Virginia Beach, Virginia, focuses their initiative on the importance of educating adults who care for infants and children to ensure they receive immunizations. Emphasis of this program is placed on Tdap vaccinations.
The Maryland Healthcare Personnel Immunization Initiative was launched 7 years ago as a collaboration between the Maryland Department of Health and Mental Hygiene, Maryland Partnership for Prevention, and professional associations across the state. The goal of this initiative is to increase vaccination rates among health care professionals to prevent the spread of vaccine-preventable disease to their patients, their family members, and their community. Participants were provided with grants of up to $1,000 to provide campaign
material throughout their facilities to raise awareness and increase employee immunization rates.15
Virginia Adult Hepatitis B Immunization Initiative
The Virginia Adult Hepatitis B Immunization Initiative, the Immunization Department of the Virginia Department of Health, other local health departments, and community partners in Virginia have joined forces to provide hepatitis B vaccinations free of charge to adults who are identified as high risk for hepatitis B infection. To qualify for the vaccine, patients must be 19 years of age or older and susceptible to hepatitis B through reported lifestyle choices,
health status, medical history, sexual and drug use/abuse history, presenting sexually transmitted infections, or contact with hepatitis B-infected persons. Providers and patients can access the vaccines or obtain more information by contacting their local health department to find participating clinics and dates.16
Adult Immunization Michigan
The Adult Immunization Michigan program works to overcome the challenges and barriers to adult immunization in a state that previously had very low immunization rates. Activities are focused on educating providers and raising public awareness of the importance of vaccines throughout the life span.17
Issues of Access and Cost
Access and cost are significant barriers that prevent many adults from obtaining recommended vaccinations. These factors are strong contributors to the increasing financial and public health burden of vaccinepreventable illness in the United States.
Access to Medicare Part D Vaccinations
In December 2011, the U.S. Government Accountability Office (GAO) released the results of a study on Medicare beneficiary access to routinely recommended vaccinations covered under Part D.19 The report examines:
• The extent to which beneficiaries have received Part D–covered vaccinations.
• Factors affecting access to vaccinations.
• Findings and recommendations of government agencies and other stakeholders to increase access to Part D–covered vaccinations.
More than 19 million beneficiaries aged 65 years and older who were enrolled in Medicare Part D in 2009 did not receive recommended covered vaccinations.19 Only 11% of beneficiaries with Part D coverage received shingles
vaccine and 53% received Td vaccine. Of these, Medicare data from 2007 to 2009 indicate that relatively few beneficiaries actually received these vaccines under their Part D benefit (i.e., 5% for shingles and less than 1% for Td or Tdap), raising questions about access, delivery, and payment.19
Access to routinely recommended Part D–covered vaccinations was affected by a number of factors, including cost, billing challenges, limited supply through physician offices or pharmacies, beneficiary cost-sharing, reimbursement challenges, and inconsistent recommendations by physicians. GAO recommends that CMS continue coverage of vaccines and explore options and take steps to address administrative challenges, such as billing and coverage verification by physicians. HHS concurred with these recommendations.19 The full report can be accessed at http://www.gao.gov/ assets/590/587009.pdf.
Disease Burden and Cost of Influenza
Researchers at CDC estimated age- and risk-specific disease burden along with medical and indirect costs attributable
Rhode Island Immunize for Life
In Rhode Island, efforts have been focused on state distribution of the influenza vaccine. Success has been demonstrated through optimizing costs and achieving influenza immunization rates that rank among the highest percentiles in the nation. The state’s Immunize for Life Program spans all ages, from infants through adults. In addition, the Quality Partners of Rhode Island (now Healthcentric Advisors) developed an engaging CMS-funded campaign and toolkit to improve immunization rates among nursing home residents and staff, accessible at http://www.innovations.ahrq.gov/ content.aspx?id=1684.18 ✻
to annual influenza epidemics in the United States.20 Investigators utilized a probabilistic model and publicly available 2003 epidemiological data to estimate the number of influenza cases leading to outpatient visits, hospitalization, mortality, and time lost from work absenteeism or premature death. Data from health insurance claims and projections of either earnings or statistical life values were used to estimate health care resource utilization associated with influenza cases as well as medical and productivity (indirect) costs.20
Influenza resulted in an estimated average of 610,660 life-years lost (undiscounted), 3.1 million hospitalized days, and 31.4 million outpatient visits annually. The estimated annual burden attributable to direct medical costs was $10.4 billion, and projected lost earnings from illness and loss of life was $16.3 billion annually. The total economic burden of annual influenza epidemics amounted to $87.1 billion. Researchers concluded that hospitalization costs are important contributors to overall costs, with the bulk of the economic burden of influenza attributable to lost productivity from missed work days and premature death.20
Cost-Effectiveness of the 2010 CDC Recommended Adult Immunization Schedule
The health and economic consequences of the 2010 CDC Recommended Adult Immunization Schedule were evaluated by a team of researchers from the Harvard School of Public Health, i3 Innovus, and GlaxoSmithKline; the full report is pending publication.21 Researchers aggregated the results of seven individual cost-effectiveness stud-
ies (published between 2000–2009) involving influenza, pneumococcal, Td/ Tdap, varicella, shingles, and human papillomavirus (HPV) vaccines.22-28 Six of the seven vaccines recommended for all persons in an age category independent of high-risk factors, listed in the complete 2010 CDC Recommended Adult Immunization Schedule, were evaluated. MMR was excluded from this analysis due to a lack of published literature on the cost-effectiveness of MMR
in adults that met inclusion criteria. The main outcome, health-related quality-adjusted life-years (QALYs), conservatively estimates the incremental cost-effectiveness ratio of the immunization schedule including the six vaccines evaluated to be $15,600 per QALY gained. Results were robust to sensitivity analyses.21 ✻
Adult Immunizations in the Transitioning U.S. Health Care System
The ACA expanded preventive care coverage, funding, and reporting within the U.S. health care system. Efforts to improve immunization rates and decrease the burden of vaccinepreventable illnesses are integrated specifically into many aspects of the law and evolving regulations, including elimination of out-of-pocket costs for certain preventive services and an annual wellness visit that includes ACIPrecommended immunizations:29,30
• Influenza vaccine for all adults.
• Pneumococcal vaccination for all adults aged 65 years and older.
• Pneumococcal vaccinations for highrisk adults aged 19 to 64 years.
• HPV vaccination for women aged 19 to 26 years.
• MMR, Td/Tdap, and meningococcal vaccines as indicated.
Co-pay and cost-sharing restrictions apply to plans or policies effective September 23, 2011, and permit a delay of up to 1 year for coverage of newly recommended vaccines.29 The ACA extended coverage for preventive services without cost-sharing to an additional 54 million working Americans with insurance coverage through the ACA.31 Broadly, the ACA established:29,30
• Prevention and Public Health Fund, allocating $500 million in 2010 and $750 million in 2011 for the devel-
opment and expansion of health prevention activities and programs; this amount increases incrementally each year with an original target of $15 billion over 10 years. (However, in 2011, this funding target was reduced through political negotiations to $10 billion.32)
• Clinical Preventive Services Task Force and Community Preventive Services Task Force, coordinating with the U.S. Preventive Services Task Force and ACIP to track and report progress in preventive care, including immunization rates.
• Expansion of Section 317 of the Public Health Service Act allowing states to purchase adult vaccines in addition to those for children with funds allocated through this section.
• Funding of a GAO study to evaluate access and coverage of vaccines under Medicare Part D.
• Development of school-based health centers.
• Educational campaign on using preventive services to be developed by CDC.
• CDC grants for state demonstration projects.
• National Report Card with preventive health indicators for influenza and pneumococcal vaccines administered
through CDC. The interactive tool is available at http://apps.nccd.cdc.gov/ SAHA/Default/NationalReport.aspx.
Within Medicare, all beneficiaries now have access to an annual preventive care visit and the establishment of a personalized prevention plan that includes immunizations. Numerous vaccines are available through Part D (e.g., shingles, Td/Tdap) and others (e.g., influenza, pneumococcal) are covered under Part B.29,30 Administrative, regulatory, and system barriers may interfere with access for some beneficiaries; potential solutions are under investigation.20 Medicare also has increased utilization of quality report cards for hospitals, nursing homes, and others that include immunizationrelated indicators.
Additional information regarding the ACA and immunizations is available at the HHS website http://www. healthcare.gov/news/factsheets/2010/ 09/affordable-care-act-immunization. html. ✻
Facts and Figures
Immunization rates among adults are slowly improving, yet they still fall well short of the Healthy People 2020 targets listed in Table 2. 33 Racial disparities also are evident and may stem in part from financial and access barriers. Current adult immunization rates by age are listed in Tables 3 and 4 34,35
Pharmacists as Immunizers
In every state, Puerto Rico, and the District of Columbia, pharmacists are authorized to administer vaccines against influenza and shingles. Most states also provide authority for pharmacists to administer many other vaccines, although specifics vary as noted
in Figure 3. Pharmacists may immunize against pneumococcus in 51 states and territories (excluding South Dakota). Pharmacists can vaccinate against tetanus, diphtheria, and pertussis in 47 states. In 44 states and territories, pharmacists can administer any vaccine. Student pharmacists under supervision may administer vaccines in 37 states and the District of Columbia.36 Optimizing opportunities for collaboration among members of the health care team can improve immunization rates and address administrative and regulatory barriers. For example, many vaccines are administered in physicians’ offices and clinics; however, physicians cannot verify patient eligibility at the
Table 2. Healthy People 2020 Baseline Data and Goals
Source: Reference 33.
Table 3. Proportion of Adults Receiving Influenza Vaccination, by Age Groupa
point of care for vaccines covered under Medicare Part D. ✻
Noteworthy Numbers
• 16—dollars saved in avoided costs per $1 spent on immunizations.30
• 52—number of states and territories authorizing pharmacists to administer vaccines.36
• 222—number of people in the United States who got measles disease in 2011, 70 of whom required hospitalization.37
• 41,880—number of new cases of pertussis reported in the United States in 2012.38
Table 4. Proportion of Adults Receiving
Tetanus vaccination, past 10 years
(at least 3 doses), ever
Table 4. Proportion of Adults Receiving Selected Vaccinations, by Age Group and High-Risk Status, 2009
(continued)
Herpes zoster (shingles) vaccination, ever
Human papillomavirus vaccination (at least 1 dose), ever
aStatistically significant difference from 2008 at P<0.05.
Source: Reference 35.
Figure 3. Types of Vaccines Pharmacists Are Authorized to Administer, by State, 2013
Influenza, pneumococcal, and zoster vaccine NY, FL
Other combinations MD, NH, OH**, WV**, WY**
*Via Rx for some; **broad list of vaccines.
Source: Reference 36. Adapted and used with permission from the American Pharmacists Association.
Safety and Adverse Effects of Vaccines
In 2009, the Institute of Medicine (IOM) convened a committee of experts in pediatrics, internal medicine, neurology, immunology, immunotoxicology, neurobiology, rheumatology, epidemiology, biostatistics, and law to evaluate and study the evidence regarding immunizations and adverse events.39 This work was commissioned by the Health Resources and Services Administration to determine causality of an association between vaccines and 60 specific adverse events to provide the basis for claims of vaccine injury by the National Vaccine Injury Compensation Program. The vaccines evaluated included varicella; shingles; influenza; hepatitis B; HPV; tetanus toxoid–containing vaccines (other than those containing the whole-cell pertussis component); MMR; hepatitis A; and meningococcal vaccines.39
The IOM committee reviewed over 1,000 research articles and developed causality conclusions for 158 pairs of vaccines and adverse events using epidemiologic and mechanistic evidence. Decisions were based on the strength and weaknesses of the biological, clinical, and epidemiological research and are outlined in the 896-page report. Outcomes focused solely on potential risks and did not examine risk-benefit ratios.39
Each relationship between a vaccine and an adverse health problem was assigned to one of the following four categories of causality conclusion:39
• Evidence convincingly supports a causal relationship (14)
• Evidence favors acceptance of a causal relationship (4)
• Evidence favors rejection of a causal relationship (5)
• Evidence is inadequate to accept or reject a causal relationship (135)
Causality
Evidence convincingly supports causation with possible rare adverse events in association with 14 specific vaccine–adverse event pairs:39
• MMR, varicella, influenza, hepatitis B, meningococcal, and tetanus vaccines: can trigger anaphylaxis.
• MMR vaccine: fever-trigger seizures (usually benign), brain inflammation known as measles inclusion body encephalitis, attributed to individuals with demonstrated severe immune system deficiencies.
• Varicella vaccine: can induce pneumonia, hepatitis, brain swelling, meningitis, shingles, and chickenpox in individuals with immunodeficiencies because of their increased susceptibility to live viruses.
Evidence favors acceptance that certain vaccines can lead to other problems, although the evidence is less convincing than for the events above:39
• MMR vaccine: transient arthralgia (joint pain) in women and children.
• HPV vaccine: anaphylaxis.
• Influenza vaccine: mild, temporary oculorespiratory syndrome with conjunctivitis, mild upper respiratory symptoms, and facial swelling.
Importantly, evidence was strong enough to favor rejection of an association for five vaccine–adverse event pairs (Table 5). The committee found that certain vaccines are not linked to four specific conditions that have contributed historically to concerns about immunization safety: autism, type 1 diabetes, asthma exacerbation, and Bell’s palsy.39
In 135 of the suggested associations evaluated, there is too little evidence or the available evidence is conflicting or otherwise inconclusive. The causality conclusions were defined as inadequate to accept or reject a causal relationship. Findings show that few problems are clearly connected to vaccines. When there are adverse event associations, they occur rarely and sometimes in specific populations. Although risk-benefit ratios were not considered in this analysis, the committee noted that death and disability due to vaccine-preventable infectious diseases have been dramatically reduced over the last century.39 ✻
Table 5. IOM Causality Conclusions Favoring Rejection of an Association Between Vaccines and Adverse Events
Source:
Public Health Burden of Vaccine-Preventable Illness
Vaccine-preventable illnesses place a tremendous burden on public health and health care costs in the United States. Seasonal influenza affects more than 15.2 million adults annually and is associated on average with greater than 23,000 deaths annually. Older adults are disproportionately affected, with 89.5% of deaths occurring
in those over 65 years of age. Younger adults also are at risk for morbidity and mortality associated with influenza, with an average of 2,485 annual deaths attributable to adults 19 to 64 years of age. Pneumococcal illness, independently and as a complication of influenza, also is associated with high morbidity and mortality in adults. Table 6 includes
Table 6. Disease Burden of Vaccine-Preventable Illnesses
a summary of morbidity and mortality drawn from the work of the NVAC, supplemented with data from the CDC.13,37,38,40 The number of lives saved through vaccination in the United States could increase with coordinated outreach and emphasis in adult immunizations.41 ✻
Average of 23,607 annual deaths with underlying respiratory and circulatory causes (including pneumonia and influenza causes) during 1976–2007 (range: 3,349–48,614 deaths)
• Adults aged 19–64 years: average of 2,485 annual deaths (range: 1,927–3,788 deaths)
• Adults ≥65 years of age: average of 21,098 annual deaths (range: 19,832–24,206 deaths)
Pneumococcal disease Morbidity Invasive pneumococcal disease rate in 2009 for adults aged ≥65 years: 38.7 per 100,000 population
Pertussis Morbidity 41,880 cases reported in 2012
• Aged ≥20 years: 8,890 cases Prevalence of pertussis now exceeds number of cases reported in 1960
Hepatitis A Morbidity 2,585 cases reported in 2008
• Aged ≥25 years: 1,840 cases
Accounting for underreporting and asymptomatic infection, estimated 13,000 total cases in 2007
Mortality
Average 74 deaths annually for adults aged ≥20 years 12 reported deaths in 2007
Hepatitis B Morbidity 4,033 cases reported in 2008
• Aged ≥25 years: 3,688 cases
Accounting for underreporting and asymptomatic infection, estimated 25,000 total cases in 2007
Herpes zoster (shingles)
Cervical cancer caused by human papillomavirus
Mortality
Morbidity
Morbidity
Mortality
Measles Morbidity
3,000 deaths annually
• All ages: 5.4 cases per 1,000 person-years
• Aged ≥22 years: 3.6 cases per 1,000 person-years
• Aged 45–64 years: 6.8 cases per 1,000 person-years
• Aged ≥65 years: 11.7 cases per 1,000 person-years
11,978 incident cases of cervical cancer diagnosed in 2005 in adults aged ≥20 years
• Aged 20–44 years: 4,781 cases
• Aged ≥45 years: 7,197 cases
3,923 cervical cancer deaths in 2005 in adults aged ≥20 years
• Aged 20–44 years: 803 deaths
• Aged ≥45 years: 3,120 deaths
71 cases all ages, in 2009
222 cases all ages, in 2011
Tetanus Morbidity During 1990–2001, a total of 534 cases of tetanus in all ages were reported
• Aged 19–64 years: 301 cases
• Aged ≥65 years: 201 cases
Source: Adapted from references 13, 37, 38, and 40.
Research: Adult Immunization in Developed Economies
In recognition of the potential for adult transmission of vaccine-preventable diseases, waning immunity over time, increasing severity of certain diseases in older individuals, and the inherent ability for globalization and travel to contribute to transmission of disease, researchers at the HHS National Vaccine Program Office conducted a study to evaluate adult vaccination policies in developed countries. Investigators surveyed representatives of health ministries in 33 countries with advanced economies across Europe, Asia, North America, and Australia to assess the presence of national recommendations for
16 adult vaccines or vaccine components, available funding mechanisms, and estimates of immunization rates. Of the 31 countries responding, only 12 (38.7%) reported having a comprehensive recommended adult immunization schedule. Survey responses revealed a wide variability in the number and types of vaccines recommended, with seasonal influenza, tetanus, hepatitis B, and pneumococcal vaccines being most prevalent. The vast majority of funding sources are public, with a few reporting private funding or a mix between public and private sources. Researchers concluded that although most countries
with advanced economies reported availability of funding mechanisms, over 60% of countries do not have comprehensive immunization schedules for adults and very few track immunization rates for this population. The essential components of successful childhood immunization programs include stable funding, standard recommendations, and routine assessment of vaccine coverage. Continued growth with regard to these elements in adult immunization could translate proven success in childhood immunizations to the adult population.41 ✻
Summary: Promise and Challenge of Vaccines
The discovery of and advances in immunizations over the twentieth century have had a tremendous effect on improving the health and wellbeing of society by reducing morbidity and mortality from previously common and devastating infectious diseases including smallpox, polio, measles, and pertussis. Vaccines also help to reduce the burden of influenza, pneumococcus, shingles, hepatitis A and B, and other illnesses, yet they remain underutilized.1-3,19,33-35,42 Continued progress in the United States can contribute to worldwide improvements in health and reduction of vaccine-preventable illnesses. As a relatively inexpensive and effective means of improving health and welfare, vaccination has been correlated with poverty reduction and economic development in countries previously encumbered by disease.43
Pockets of success in communities and states around the country provide examples and encouragement. Numerous national, state, and local initiatives are working to define and implement improvements in systems, education, information, provider and public awareness, and steps to increase
access. Federal funding is available to stimulate rapid advances in these areas and to improve information systems, tracking, and reporting. Proven strategies are being documented and disseminated, along with evidence on safety and identification of which populations benefit from vaccination.
Emphasis on vaccination is being challenged by some who believe that funding for vaccine-preventable illnesses should be minimized in favor of focusing on chronic diseases such as diabetes, cardiovascular disease, chronic obstructive pulmonary disease, and unhealthy lifestyle conditions such as obesity and smoking.30 It is essential to help inform policy decision makers in national budget discussions—as they consider continued funding of the Prevention and Public Health Fund and others—regarding how vaccinations contribute to positive outcomes
in patients with chronic diseases. Downward trends in immunization, as seen with the resurgence of measles in western European countries, can quickly reverse decades of progress.38
The most effective approaches will involve systematic implementation of interventions across settings and providers, backed by vaccine accessibility, awareness, and insurance coverage. The challenge remains: how can the United States coordinate public and private efforts and maximize opportunities through expansion in care, funding, and services available through the ACA and evolving regulations to reduce the burden of vaccine-preventable illness by improving vaccination of adults? ✻
1. Centers for Disease Control and Prevention; Administration on Aging; Agency for Healthcare Research and Quality; Centers for Medicare and Medicaid Services. Enhancing Use of Clinical Preventive Services Among Older Adults: Closing the Gap. Washington, DC: AARP; 2011.
2. Centers for Disease Control and Prevention; AARP; American Medical Association. Promoting Preventive Services for Adults 50–64: Community and Clinical Partnerships. Atlanta, GA: National Association of Chronic Disease Directors; 2009.
3. Centers for Disease Control and Prevention. Charter of the Advisory Committee on Immunization Practices. April 1, 2012. Available at: http://www.cdc. gov/vaccines/acip/committee/charter.pdf. Accessed May 31, 2013.
4. Centers for Disease Control and Prevention. General recommendations on immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2011;60 (RR-2):1–61.
5. Centers for Disease Control and Prevention. Advisory Committee on Immunization Practices (ACIP) recommended immunization schedule for adults aged 19 years and older—United States, 2013. MMWR Surveill Summ. 2013;62(suppl 1):9–19.
6. Shefer A, Atkinson W, Friedman C, et al. Immunization of health-care personnel: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2011;60(RR-7):1–45.
7. Immunization Action Coalition. Healthcare personnel vaccination recommendations. Item #P2017. July 2012. Available at: http://www.immunize.org/ catg.d/p2017.pdf. Accessed March 24, 2012.
8. Centers for Disease Control and Prevention. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine in adults aged 65 years and older—Advisory Committee on Immunization Practices (ACIP), 2012. MMWR Morb Mortal Wkly Rep. 2012;61(25);468–470.
9. Immunization Action Coalition. About us. Available at: http://www.immunize.org/aboutus/. Accessed March 3, 2013.
10. Graitcer SB. Prevention and Public Health Fund, Program Area 5: Increasing Adult Immunization. Presented at the Centers for Disease Control and Prevention, November 10, 2011; Atlanta, GA.
11. Centers for Disease Control and Prevention. Strategies for increasing adult vaccination rates: WhatWorks! June 2010. Available at: http://www. cdc.gov/vaccines/recs/rate-strategies/adultstrat. htm#whatworks. Accessed March 20, 2012.
12. Partnership for Adult Vaccination and Education. Adult vaccination: a performance improvement approach. 2010. Available at: http://www.partnersin knowledge.com%2FGSKCenterforMedicalEducation %2Fdownload%2Frow1b.pdf. Accessed February 1, 2012.
13. National Vaccine Advisory Committee. A pathway to leadership for adult immunization: recommendations of the National Vaccine Advisory Committee. Public Health Rep. 2012;127(suppl 1):1–42.
14. Community Coalitions Health Institute. Adult Immunization Seed Grants. 2012. Available at: http://www.nbch.org/Adult-Immunization. Accessed March 28, 2013.
15. Maryland Department of Health and Mental Hygiene. 2012–2013 Maryland Healthcare Personnel Immunization Initiative. Available at: http://phpa. dhmh.maryland.gov/OIDEOR/IMMUN/SitePages/ maryland-healthcare-immunization-initiative.aspx. Accessed March 28, 2013.
16. Virginia Department of Health. Virginia Adult Hepatitis B Immunization Initiative (VAHBII). September 2012. Available at: http://www.vdh.state. va.us/epidemiology/immunization/hbii/index.htm. Accessed March 28, 2013.
17. Alliance for Immunization in Michigan. About AIM. Available at: http://www.aimtoolkit.org/about.php. Accessed February 4, 2012.
18. State of Rhode Island Department of Health. Office of Immunization (Immunize for Life). Available at: http://www.health.ri.gov/programs/immunizeforlife/. Accessed March 26, 2012.
19. U.S. Government Accountability Office. Medicare: many factors, including administrative challenges, affect access to Part D vaccinations. December 15, 2011. Available at: http://www.gao.gov/products/ GAO-12-61. Accessed February 8, 2012.
20. Molinari NA, Ortega-Sanchez IR, Messonnier ML, et al. The annual impact of seasonal influenza in the US: measuring disease burden and costs. Vaccine. 2007;25:5086–5096.
21. Unpublished data. H. Crouch, PharmD, personal communication, February 15, 2012.
22. Elbasha EH, Dasbach EJ, Insinga RP, et al. Agebased programs for vaccination against HPV Health. 2009;12:697–707.
23. Lee GM, Murphy TV, Lett S, et al. Cost-effectiveness of pertussis vaccination in adults. Am J Prev Med. 2007;32:186–193.
24. Smith KJ, Roberts MS. Cost effectiveness of vaccination strategies in adults without a history of chickenpox. Am J Med. 2000;108:723–729.
25. Rothberg MB, Virapongse A, Smith KJ. Costeffectiveness of a vaccine to prevent herpes zoster and post neuralgia in older adults. Clin Infectious Dis. 2007;44:1280–1288.
26. Prosser LA, O’Brien MA, Molinari NA, et al. Non-traditional settings for influenza vaccination of adults: costs and cost effectiveness. Pharmacoeconomics. 2008;26(2):163–178.
27. Maciosek M, Solberg L, Coffield A, et al. Influenza vaccination health impact and cost effectiveness among adults aged 50 to 64 and 65 and older. Am J Prev Med. 2006;31:72–79.
28. Smith KJ, Zimmerman RK, Lin CJ, et al. Alternative strategies for adult pneumococcal polysaccharide vaccination effectiveness analysis. Vaccine. 2008;26:1420–1431.
29. U.S. Department of Health and Human Services. The Affordable Care Act and immunization. Updated January 20, 2012. Available at: http://www. healthcare.gov/news/factsheets/2010/09/affordablecare-act-immunization.html. Accessed May 6, 2013.
30. Wheeler JB. Immunizations and the Affordable Care Act. NCSL Legisbrief. April–May 2011.
31. Sommers BD, Wilson L. Fifty-four million additional Americans are receiving preventive services coverage without cost-sharing under the Affordable Care Act. ASPE Issue Brief. February 15, 2012. Available at: http:// aspe.hhs.gov/health/reports/2012/PreventiveServices/ ib.shtml. Accessed March 22, 2012.
32. Fleming C. Health Policy Brief: The Prevention and Public Health Fund. Health Affairs Blog. March 1, 2012. Available at: http://healthaffairs.org/blog/ 2012/03/01/health-policy-brief-the-prevention-andpublic-health-fund/. Accessed March 22, 2012.
33. Healthy People 2020. Immunization and infectious diseases. Available at: http://www.healthypeople. gov/2020/topicsobjectives2020/objectiveslist. aspx?topicId=23. Accessed March 2, 2012.
34. Centers for Disease Control and Prevention. Early release of selected estimates based on data from the January–September 2011 National Health Interview Survey. Page 26. March 2012. Available at: http:// www.cdc.gov/nchs/nhis/released201203.htm#4. Accessed March 26, 2012.
35. Centers for Disease Control and Prevention. Statistics and surveillance: 2009 adult vaccination coverage, NHIS. Available at: http://www.cdc.gov/ vaccines/stats-surv/nhis/2009-nhis.htm. Accessed March 2, 2012.
36. American Pharmacists Association. Immunization Center: Pharmacist authority to immunize—by type of immunization; other data. 2013. Available at: http://www.pharmacist.com/immunization-center. Accessed May 14, 2013.
37. Centers for Disease Control and Prevention. Measles—United States, 2011. MMWR Morb Mortal Wkly Rep. 2012;61:253–257.
38. Centers for Disease Control and Prevention. 2012 Provisional Pertussis Surveillance Report. 2013. Available at: http://www.cdc.gov/pertussis/ downloads/Provisional-Pertussis-SurveillanceReport.pdf. Accessed March 29, 2013.
39. Institute of Medicine. Adverse Effects of Vaccines: Evidence and Causality. Washington, DC: The National Academies Press; 2011.
40. Kretsinger K, Broder K, Cortese M, et al. Preventing tetanus, diphtheria, and pertussis among adults: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2006;55(RR-17):1–33.
41. Wu LA, Kanitz E, Crumly J, et al. Adult immunization policies in advanced economies: vaccination recommendations, financing, and vaccination coverage. Int J Public Health. 2013. [Epub ahead of print]. Available at: http://link.springer.com/content/ pdf/10.1007%2Fs00038-012-0438-x.pdf. Accessed March 3, 2013.
42. Shires DA, Stange KC, Divine G, et al. Prioritization of evidence-based preventive health services during periodic health examinations. Am J Prev Med. 2012;42(2):164–173.
43. Bloom DE, Canning D, Weston M. The value of vaccination. World Economics. 2005;6(3):15–39.