GEORGE LALIOTIS Dr.



DearReaders,
Sincerely,

SIMRANKHAN ProjectEditor




























DearReaders,
Sincerely,
SIMRANKHAN ProjectEditor
Fordecades,oncologywasapracticeofeducatedguessing.Wetreatedthe‘average’patient, usingprotocolsbuiltonpopulationstatistics.Butasanydoctorknows,thepersonsittinginthe examroom—anxious,hopeful,andterrified—isnotastatistic.Theyarechemicallyand biologicallyunique.Today,thedarknessofguessworkisfinallyfading.Itismydistincthonor topresent“The10MostInnovativeLeadersinOncology&PrecisionMedicinetoWatch in2026,”acollectionofvisionarieswhoareprovingthatthecureforcancerliesnotjustin newdrugs,butinbetterdata.
Leadingthistransformationisourcoverfeature,Dr.GeorgeLaliotis,FounderandCEOof DiveGenomicsAI.Dr.Laliotisstandsuniquelybetweenthecoldworldofbigdataandthe warmrealityofpatientcare.Aphysician-scientisttrainedfromGreecetoJohnsHopkins,he grewtiredofthe“one-size-fits-all”approach.Hissolutionisthe“DigitalPatientTwin”—a revolutionaryAImodelthatcreatesacomputationalmirrorofapatient.Thistechnology allowsdoctorstosimulatehowaspecifictumorwillrespondtotreatmentbeforeasingledrop ofchemotherapyisadministered.Byactingasa“physician’sco-pilot,”Dr.Laliotisismoving theindustryfrommerelydetectingcancertopredictingandpre-emptingit.
Trueinnovation,however,requiresadiversearmyofthinkers.Thiseditionalsohighlightsthe workofGregoryA.MercurioJr.,SeniorVicePresidentatAmericanSharedHospital Services,andDr.VivekVerma,AssociateDirectorofSurgicalOncologyatMaxSuper SpecialityHospital.WealsoprofileYujiOtsuki,CEOofFerroptoCureInc.,alongside Dr.GeorgeYoo,ChiefMedicalOfficerattheKarmanosCancerInstitute.
Theseleadersunderstandthatwhiletechnologyisthetool,thepatientremainsthepurpose. Theyarebuildingafuturewherewedon’tjustreadthecodeoflife—weunderstandit.
PUBLISHER
EDITOR-IN-CHIEF
MANAGING EDITOR
ARCHANA GHULE
VIKRAM SURYAWANSHI
PANKAJ GHOLAP
PROJECT EDITOR SIMRAN
PROJECT MANAGERS
SATISH WATHORE
YOGESH UJJAINKAR
RAJNISH KUMAR
VISUALIZER
GRAPHIC DESIGNER PRIYANKA
HEAD
HEAD
RESEARCH ANALYSTS
ADVERTISING
JAMES
MARIA




The Architect of the Digital Twin and the End of Guesswork in Oncology
Founder and CEO | Dive Genomics AI


Inthevastrealmofmodernoncology,there
isasignificantdistinctionbetweenhaving dataandhavinganswers.Wearecurrently overwhelmedbytheformer.Everyday, laboratoriessequencegenomes,hospitalsupdate electronichealthrecords,andclinicaltrials generatevastamountsofinformation.Yet,forthe patientsittingintheexamroom,theperson waitingforthedoctortodeliverlife-altering news,thatmountainofdataoftenfeelsdistant, cold,andabstract.Theyarenotconcernedwith populationstatistics;theyarefocusedontheir ownsituation.

Dr.GeorgeLaliotisoccupiesauniqueposition betweentheanxiouspatientandthevast collectionofmedicaldata.Throughouthislife,he hasearnedvariouscredentials(MD,MPH,MHA) notmerelyforthesakeofthetitles,buttodevelop acomprehensiveunderstandingofhealthcareand medicine.Asaphysician-scientist,hegraspsthe intricaciesofcellularbiology;asahealthcare administrator,heunderstandsthecomplexitiesof thehealthcaresystem.Now,astheFounderand CEOofDiveGenomicsAI,heisdedicatedto bridgingthegapbetweenthesetwoworlds.
Foundedin2025inBoston,Massachusetts,the heartofglobalbiotechinnovation,Dive GenomicsAIrepresentstheculminationofa careerspentgrapplingwithasingle,persistent question: Why are we still guessing?
Dr.Laliotisisapersonofquietintensity.Hedoesnotusethe hyperboliclanguageoftenfoundamongtechfounders.When hediscusses“revolutionizing”healthcare,hemeansitinthe literalsenseofshiftingtheperspective,movingawayfromthe “one-size-fits-all”approachofthepasttowardafuturewhere everypatienthasa“DigitalPatientTwin.”Heisdedicatedto provingthattheindividualwhohasbeenlabeledasjust averageis,infact,completelyunique,bothchemicallyand biologically.
TounderstandthearchitectureofDiveGenomics,youmust lookatthearchitectureofDr.Laliotis’smind.Itwasbuiltona foundationofrigorouscuriosity,startingthousandsofmiles awayfromBoston.
“My journey began in Greece at the University of Crete Medical School,” Dr.Laliotissays.Itwasaresearch-intensive environment,thekindofplacethatdoesn’tjustteachyou how totreatapatient,butforcesyoutoask why thediseaseexistsin thefirstplace.Thisinstilledinhimadeepcuriosityforcancer biology.Butmedicinealonewasn’tenough.Hesensedearly onthatbeingagooddoctorrequiredunderstandingthe machineryofhealthcareitself.
So,hepursuedamulti-disciplinarypath.HeearnedaMaster ofPublicHealth(MPH)andaMasterofHealthAdministration (MHA). “I wanted to understand healthcare from both clinical and systemic perspectives,” heexplains.Mostpeople specializetonarrowtheirfocus;Dr.Laliotisspecializedto widenhis.
Thishungerforaholisticviewtookhimfrom GreecetotheUnitedStates,landinghimat someofthepremierinstitutionsintheworld. HeengagedinpostdoctoralworkatJohns HopkinsSchoolofMedicineandOhioState University There,hedidn’tjuststudycancer; hestudiedthemolecularwhispersthatdriveit, specificallyPI3K/AKTsignalingandRNA regulationinsolidtumors.
“I was fascinated from a young age by the potential of science to transform lives on a global scale,” herecalls.Butthetransitionto theU.S.wasnotwithoutitsfriction. “Early in my career in the U.S., I had to navigate the transition from a clinical environment to a highly technical graduate research setting in a new country,” headmits.Hewasstartingfrom scratchinahyper-competitiveenvironment.
Howdidherespond?Notwitharrogance,but withradicalaccountability “I responded by dedicating myself to continuous education......... focusing on radical accountability and collaboration with my peers.” Thisresiliencedidn’tjustgethim throughtheprogram;itforgedtheleadership styleheusestoday.Itallowedhimto eventuallyleadteamsofscientistsandmanage complexclinicalprograms,provingthatthe bestleadersareoftenthemost dedicatedstudents.
Never stop educating yourself. In a field as fastmoving as AI and genomics, your ability to remain a student is your greatest professional asset.” “
BeforefoundingDiveGenomicsAI,Dr.Laliotis stoodatthehelmofOncologyLifecycle ManagementatNatera.Itisavantagepointthat offersabreathtakingviewofthestateofcancercare.
“My tenure..... was incredibly rewarding,” hesays. Hedirectedmedicalstrategiesforaportfolioofover 150studies.Hecontributedtothelaunchof industry-leadinggenomicproducts.Hesawthesheer scaleofwhatwaspossible,dealingwithvast amountsofmultimodaldata,involving“over thousandstumorexomesandmillionsof datapoints.”
Itwashere,amidstthisoceanofinformationthatthe “Why” ofhisnextventurebegantocrystallize.He realizedthatwhiletheindustryhadbecome excellentatdetection,itwasstilllagging inprediction.
“My journey to this point was defined by a realization that while we have entered an era of ‘big data’in oncology, the ability to translate that data into individual patient outcomes remained a significant hurdle,” hesays.Hesawthatwewere collectingmillionsofdatapoints,butforthepatient sittingontheexamtable,thetreatmentplanwas oftenstillbasedongeneralpopulationstatistics.
“The ‘one-size-fits-all' approach is no longer sufficient,” Dr.Laliotisasserts. “I am driven by the belief that every patient’s cancer has a unique molecular signature that can—and should—be decoded.”
ThisconvictionledtothebirthofDiveGenomics AIin2025.Thevisionwastransformative: to bridge the gap between high-dimensional biological data and bedside clinical practice.
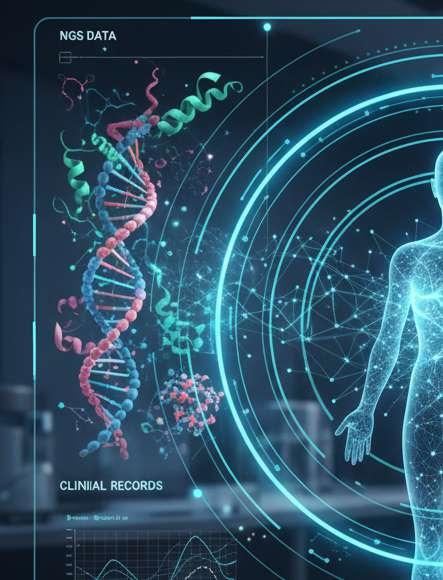
Thecoreofthisvisionisthe“DigitalPatientTwin.” Itsoundslikesciencefiction,butDr.Laliotis explainsitwiththegroundedpracticalityofa clinician. “These digital models allow us to simulate patient responses to specific therapies and predict the risk of disease progression,” hesays.
TheplatformminesNext-GenerationSequencing (NGS)andlongitudinalclinicalrecords.Itcreatesa computationalmirrorimageofthepatient.Byrunning simulationsonthistwin,doctorscanseewhich treatmentsmightfailandwhichmightsucceedbefore asingledropofchemotherapyentersthepatient'svein.
“We are moving toward a future where AI foundation models, trained on hundreds of thousands of tumor exomes and clinical timepoints, can predict therapeutic responses with high statistical confidence,” Dr.Laliotisexplains.
Thisisnotaboutreplacingthedoctor.Dr.Laliotisis adamantaboutthat.HeseesAIasthe “physician’s co-pilot.” Itisatoolthatallowsthehumanproviderto seearoundcorners. “By identifying molecular residual disease (MRD) earlier than traditional imaging, we can intervene when the cancer is most treatable,” henotes.
Dr.Laliotisknowsthatinnovationcannothappenina vacuum.Anewtechnology,nomatterhowbrilliant,is uselessifitdoesn’tfitintotheexistingworkflowof hospitalsandinsurers.
“Our mission relies on ‘Triple-Helix’collaboration between academic medical centers, biotechnology partners, and patient advocacy groups,” hesays.He hasbeenbusy.Inashorttime,hehasestablishedover 20collaborativerelationshipswithleadingcancer centersandkeyopinionleaders(KOLs).
Hisgoalisspecificandstrategic:toensuretheseAI modelsareintegratedintostandard-of-careguidelines likeNCCN(NationalComprehensiveCancer Network)andASCO(AmericanSocietyofClinical Oncology).Heunderstandsthattotrulyservethe patient,youmustconvincethesystem.
ThisiswherehisbackgroundinHealthAdministration (MHA)shines.Heisn’tjustbuildingagadget;heis buildingadossier “Securing Medicare reimbursement dossiers for various solid tumors has ensured that these innovations are accessible to the patients who need them most,” hesays,referencinghispast successes.Heknowsthataccessibilityisthefinal, crucialstepofinnovation.

So,whatdoestheCEOofa companytryingtopredictthe futureactuallydoallday?
“My day-to-day involves high-impact decision-making,” Dr.Laliotissays.Heisdrafting evidencedossiersforclinical guidelines.Heiscollaborating withR&Dandmarketingteams. Heisdesigning investigator-initiatedstudies.
Butthepartthatexciteshim,the thingthatlikelygetshimoutof bedintheBostonmorninggray,is themomentofdiscovery “The moment of ‘clinical utility’..... when a data-driven insight directly changes a patient’s treatment plan for the better,” he says. “I am incredibly excited by the accuracy of sophisticated computational tools and their ability to find ‘signals’in genomic data that the human eye might miss.”
Itisademandingrole.Headmits thathedoesn’tbelievea “scientificmind”evertruly switchesoff.Buthemanagesthe weightofitthroughadedication tolearningthatborderson thespiritual.
“I find balance through continuous learning and reading,” hesays.Heplayssportsandvideo games,butheisjustaslikelytobe foundtinkeringwithstatistical softwarelikeRStudioorreading philosophy.Hecites The Saviors of God byNikosKazantzakisasa favorite,adense,philosophical textaboutthestruggleofthe humanspirit.Itisafittingchoice foramanwrestlingwiththe complexitiesoflifeanddeath.
Dr.Laliotis’svisionforthefutureisclear “I want to build a platform where every patient’s treatment is guided by a personalized AI algorithm that forecasts their specific journey,” hesays. “The bigger vision is a world where we don’t just treat cancer; we predict and preempt it.”
Hehastheresumetobackuptheambition.Hehas BoardCertificationinInternalMedicineandAIin Medicine.Hisresearchonimmunotherapyresponse signatureshasbeenpublishedin Nature Communications and Annals of Surgery
Hehasdesignedover10PhaseII-IIIclinicaltrials. HeunderstandsGoodClinicalPractice(GCP)and EMEAregulations,aswellascode.
Butdespitetheaccolades,thedegrees,andtheCEO title,Dr.Laliotisremainsfundamentallyastudent. Whenaskedforamessagetothenextgenerationof leaders,hedoesnotofferaplatitudeaboutsuccess orgrinding.Heoffersawarningandablessing.
“To the next generation of leaders: never stop educating yourself,” hesays. “In a field as fast-moving as AI and genomics, your ability to remain a student is your greatest professional asset.”
Dr.GeorgeLaliotisisbuildingthefutureof oncology,butheisdoingitwiththehumble, rigorous,andobservantheartofalifelonglearner. Heisservingthepatientbyensuringthatwhenthey facetheunknown,theydon’thavetofaceitalone; theyhaveadigitaltwin,aphysicianco-pilot,and theaccumulatedwisdomofmillionsofdatapoints walkingbesidethem.
Visit Us:
LinkedIn: https://www.linkedin.com/in/georgelaliotis/
X: https://x.com/Geor_Laliot
https://www.georgelaliotis.com/
https://www.dive-genomics-ai.com/team



Rehabilitation Services

Dr.GeorgeYoo’sjourneyinoncologybeganlongbeforehe tookontheroleofChiefMedicalOfficerattheKarmanos CancerInstitutein2008.Overtheyears,Dr Yoohasbuilt areputationforpushingtheboundariesofcancertreatment,focusing onheadandneckcancer,andchampioningapatient-centeredapproach ineveryaspectofhiswork.Hiscareerreflectsahands-oncommitment toadvancingcareandfindingsolutionsthatmattertopatients.
AtKarmanos,Dr.Yooisresponsibleformanagingtheinstitute’s clinicaloperations.Thisincludesoverseeingateamofmorethan300 oncologyspecialistswhotreatover12,000newpatientseachyear Whilehisroledemandsattentiontohigh-levelstrategy,it’sthepatient careandoutcomesthatdrivehisday-to-daydecisions.Whetherit’s ensuringthesafetyofpatientsduringtreatmentorrefiningthequality ofcareprotocols,Dr.Yooisinvolvedineverystepoftheprocess.
WhatsetsDr.Yooapartishisexpertiseinmicrovascular reconstructionforheadandneckcancers.Asanotolaryngologistand surgicaloncologist,hebringsyearsofexperienceintreatingthese complexcases,oftenworkingwithmultidisciplinaryteamstoensure eachpatientreceivesthemostcomprehensivecarepossible.His contributionstothefieldextendtoacademia,whereheholdsatenured professorshipatWayneStateUniversity’sSchoolofMedicine. Throughthisrole,hetrainsandmentorsthenextgenerationofmedical students,residents,andfellows,passingontheknowledgethathas shapedhisdistinguishedcareer
Dr Yoo’simpactoncancerresearchissignificant.Withover$2 millioninNIHfunding,hisworkhascontributedtobreakthroughsin cancertreatment,particularlyinheadandneckoncology.Hehas authoredmorethan70peer-reviewedpublications,sharinghisfindings withthebroadermedicalcommunity.Hisresearchnotonlydrives advancementsatKarmanosbutalsoinfluencescancercarepractices acrossthenation.
TheKarmanosCancerInstituteitselfstandsoutasoneofonly53 NationalCancerInstitute-designatedcomprehensivecancercentersin theU.S.ItscollaborationwithWayneStateUniversityallowsitto remainatthecuttingedgeofresearchandclinicaltrials,offering patientsaccesstothelatesttherapies.
Theinstitutespecializesinseveraltypes ofcancer,includingbreast,lung,and gastrointestinalcancers,alongwithDr Yoo’sspecialty,headandneckcancers.
UnderDr.Yoo’sleadership,Karmanos continuestoevolve.Hedoesn’tseehis roleasstaticbutasanopportunityto innovateandadapttotheever-changing landscapeofcancertreatment.Heworks closelywithhisteamstoexplorenew waystoimprovepatientcareand streamlinethedeliveryoftreatments. Thisforward-thinkingapproachkeeps Karmanosattheforefrontofoncology, ensuringthattheinstituteremainsa beaconofhopeforcancerpatients.
Dr Yoo’sleadershipismorethanjust aboutmanagingpeopleandprocesses. It’saboutfosteringanenvironment whereinnovationthrives,wherepatient carecomesfirst,andwherethenext generationofdoctorscanlearnfromone ofthebest.Inafieldaschallengingas oncology,havingaleaderlikeDr Yoo, whocombinesclinicalexpertisewitha passionforresearchandteaching,makes aworldofdifference.Hisworkisnot onlyshapingthefutureofcancercare butisalsoatestamenttotheimpactone personcanhaveonanentirefield.


Let’stalkabouttherecentpast.
Afewyearsago,aglobalcrisis triggeredafrantic, disorganizedgoldrush.Thegoldwas “telehealth.”Everyhealthsystem,clinic, andentrepreneurscrambledtostakea claim,launchingsimple,standalone applicationsthatdidlittlemorethanbolt avideocameraontoaschedulingtool. Theywerecelebratedasinnovators.
Thatgoldrushisover.Thebattlefieldis nowlitteredwiththecasualties.
Manyofthoseearly,flimsyplatformsare failing.Patientadoptionhasplateaued, clinicianburnouthasworsened,andthe promisedcostsavingshavefailedto materialize.Why?Becausethesewere notstrategicplatforms.Theyweredigital waitingrooms—commoditieswithno defensibility,noloyalty,andnoreal integrationintothecomplexmachinery ofhealthcaredelivery Theywerea panic-drivenreaction,nota forward-thinkingstrategy
Ifyouarealeaderinthisspace,youmust understandthis:continuingtoinvestina simple“telehealthapp”islikearrivingat adepletedgoldminewithashovel.The easygoldisgone.
Theopportunitynowisinfinitelylarger andrequiresmorestrategicdiscipline. Thenextgenerationofwinnerswillnot bebuildingapps.Theywillbebuilding integrated,defensibleVirtualCare DeliveryPlatforms.Thedifference betweenthesetwoisnotsemantic.Itis thedifferencebetweenfleetingsurvival andmarketdominance.
TheAutopsyofaFailedGoldRush: WhyFirst-GenerationTelehealthIs Dying
Towinthefuture,youmustfirstdissect thefailuresofthepast.Thefirstwaveof telehealthappsmadethreefatalerrors.
1.TheyFellintotheCommodityTrap:
Astandalonevideoconsultationapphas zerostrategicmoat.Itisacommodity,no differentfromadozenothers.Ifyour onlyvaluepropositionisavirtualvisit, youarecompetingwitheveryother provider,includingretailgiantsand venture-backedstartupswhocan outspendyouandundercutyouonprice. Patientloyaltytoacommodityiszero. Theywillusewhateverischeapestor mostconvenientinthemoment.You havebuiltadigitalturnstile,notalasting relationship.
2.TheyCreatedaDisconnectedExperience: Mostoftheseappsexistonanisland,completely detachedfromthecoresystemsofcare.The clinicianhastoexittheirEHR,logintoaseparate system,conductthecall,thenreturntotheEHRto documentit.Thepatienthasaseparatelogin,a separateinbox,andaseparateexperiencethatfeels divorcedfromtheiroverallcarejourney.This fragmentationcreatesmoreworkforyourstaffand adisjointed,frustratingexperienceforyour patients.Itsolvesoneproblem(thevisit)by creatingthreemore(documentation,navigation, andfollow-up).
3.TheyWereEmptyWaitingRooms:Themantra was“ifyoubuildit,theywillcome.”Itwasalie. Buildingthetechnologydidnotmagicallyrewire decadesofpatientbehaviororcomplexclinical workflows.Theseappsweresolutionsinsearchofa definedproblem.Theylackedaclearstrategyfor clinicianadoptionbeyondatop-downmandate,and theyhadnoplanforpatientengagementbeyondthe initialnovelty Theywereemptydigitalrooms waitingforpeoplewhonevershowedupin sustainablenumbers.
TheStrategicPivot:From“App”to“Platform”
Thesmartmoneyisnolongerfunding“telehealth apps.”ItisfundingthecreationoftrueVirtualCare DeliveryPlatforms.Aplatformisnotatool;itisa fundamentalre-architectureofhowyoudeliver care.Itisbuiltonthreestrategicpillarsthatcreatea defensible,high-valuesystem.
Pillar1:DeepClinicalWorkflowIntegration (TheEngine)Atrueplatformdoesnotsitontopof theworkflow;itiswovenintoitsveryfabric.Itis theengine,notasidecar.
· YourMandate:Theplatformmusthavedeep, bidirectionalintegrationwithyourEHR(Epic, Cerner,etc.).Itmustpullpatientdatatogivethe cliniciancontext before thevisitandpushvisit data,notes,andordersbackintotheEHR automatically.Itautomatesscheduling,coding, andbilling.Thegoalissimplebutpowerful:the platformmustreducetheclinician’stotal workload,notaddtoit.Thisistheonlywayto achievetrue,enthusiasticadoptionfromyour mostvaluableasset:yourproviders.
Pillar2:ContinuousPatientEngagement(TheMoat) Acommodityappistransactional.Aplatformis relational.Itsjobisnotfinishedwhenthevideocall ends.Itisdesignedtomanagethepatient’sjourney between visits.
· YourMandate:Youmustbuildamoataroundyour patientrelationship.Thismeansintegratingtoolsthat createcontinuousvalue.RemotePatientMonitoring (RPM)forchronicdiseasemanagement,wheredaily vitalsaretrackedautomatically.Secureasynchronous messagingfornon-urgentfollow-upquestions. Personalizededucationalcontentpushedtothepatient basedontheircondition.Integratedprescription managementandadherencetracking.Thisecosystem ofcontinuouscarecreatesimmense“stickiness.”It makesswitchingtoacompetitor’scommodityapp unthinkableforthepatient.
Pillar3:DataasaStrategicAsset(TheFuel)Asimple appgeneratesarecordofatransaction.Aplatform generatesalongitudinaldatastream.Thisisitsfuel.
· YourMandate:Youmusttreatthedatafromyour platformasacorestrategicasset.Byanalyzingpatient engagement,RPMdata,andclinicaloutcomesover time,youcanmovefromreactivesick-careto proactive,predictivehealth.Youcanidentifyat-risk patientsbeforetheydecompensate.Youcanprove yourplatformimprovesoutcomesandlowersthetotal costofcare.Thisdataiswhatyouwilluseto negotiatefavorabletermswithpayersandto demonstrateyourclinicalsuperiorityinthemarket.
TheExecutionMandate:ForgingYourVirtualCare Platform
Buildingatrueplatformrequiresalevelofstrategicrigor absentfromthegoldrush.
1.DefineYourBeachhead,ThenDominate:Donottry tobeeverythingtoeverypatient.Thatisarecipefor failure.Instead,identifyaspecificclinicaloroperational beachheadwhereyoucanestablishdominance.IsIt post-operativeorthopediccare,whereRPMcanreduce readmissions?Isitchronicdiabetesmanagement,where continuousengagementiskey?Isitdermatology,where asynchronouscaremodelscanbehighlyefficient?Pick oneniche.Perfectyourplatform,proveitsclinicaland financialvalue,andthenexpandfromthatpositionof strength.

2.PartnerwithanArchitect,NotaBuilder:Stoplooking fora“telemedicineappdeveloper.”Youarenotbuilding fromagenericfeaturelist.Youneedtopartnerwitha virtualcarearchitect.Thisisateamwhosefirstquestions areaboutyourclinicalworkflows,yourEHRintegration points,andyourbusinessgoals—notyourcolorpalette. Theirdeepexperiencewithhealthcareinteroperability standards(HL7,FHIR)andEHRsystemsisinfinitelymore valuablethantheirabilitytocodeaslickfront-end.Vet themontheirstrategicunderstandingofhealthcaredelivery, notjusttheirtechnicalskill.
3.TheFutureisAsynchronous:Themostsignificant, immediateopportunityforefficiencyandscaleisnotAIor blockchain.Itisasynchronouscare.
Thismeans“store-and-forward”interactionswherepatients andclinicianscommunicateontheirowntime.Apatient sendsasecuremessagewithaphotoofaskincondition. Adermatologistreviewsitbetweenscheduled appointmentsandsendsbackadiagnosisandprescription. Adiabeticpatientuploadstheirglucosereadings,anda nursereviewsthedataandadjuststheircareplanlaterthat day.
Thismodelbreaksthetyrannyoftheone-to-one,real-time appointment.Itallowsonecliniciantomanageamuch largerpanelofpatientswithincredibleefficiency
Yourplatformmustbebuiltfromthegrounduptosupport bothsynchronous(livevideo)andasynchronous workflows.Thisdualcapabilityisamassivecompetitive advantage.
TheChoice:DigitalWaitingRoomorVirtualCare System?
Thefirst,chaoticchapterofremotecareisclosed.The marketismaturing,andthestandardsforsuccessare risingdramatically.Continuingtooperateastandalone, commoditytelehealthappisnolongeraviablestrategy.It isaslow-motionsurrender
Theopportunitybeforeyounowistobuildadurable, strategicasset.Tomovebeyondthedigitalwaitingroom andconstructatruesystemofvirtualcaredelivery—one thatisdeeplyintegrated,continuouslyengaging,and fueledbydata.
Thisistheworkofseriousleaders.Itrequiresinvestment, discipline,andaclear-eyedviewofthecompetitive landscape.
So,thechoiceisyours.Willyoukeeppatchingtheroofof asimpledigitalwaitingroom?Orwillyouarchitectthe integratedvirtualcaresystemthatwilldefinethefutureof yourorganizationandbecometheengineofitsgrowth?
Noparentcanfaceagreaterfearthanthespecter
ofcancerintheirchild.Itcastsalongshadow,a thiefofjoy,aquestionmarkoverthebrightest futures.Fortoolong,childhoodcancerhasbeena relentlessfoe.Butnow,thetideisturning.Bravedoctors andgroundbreakingsciencearedeliveringvictories previouslythoughtimpossible.
Considerthis:thegreatestbattlesarewonwhentheenemy isspottedearly.Incancer,earlydetectionisnotjustan advantage;itisoftenthedecidingfactor Dr.Vivek Verma,AssociateDirectorofSurgicalOncologyatMax SuperSpecialityHospital,Patparganj,understandsthis crucialtruth.Hechampionstheadvancementsthatnow allowdoctorstoseetheunseenenemy–cancer–earlier thaneverbefore.
Imaginetechnologysorefineditcanpinpointtumors whentheyaremerewhispersinthebody Thisisno longeradream.AdvancedimagingtechnologieslikeMRI, PET,andCTscansnowactasvigilantscouts,identifying threatsattheirearlieststages.Buttheinnovationgoes further.
Pictureasimplebloodtestcapableofrevealingcancer’s hiddenpresence.Liquidbiopsies,arevolutionarymethod, achieveexactlythis.TheydetectcirculatingtumorDNA inbloodsamples,uncoveringcancerevenbefore symptomsshouttheirwarning.Earlydetectionmeans timelyactionandtimelyactionmeansimproved chances–abrighterprognosisforchildren.
Moreover,understandingtheenemyatacellularlevelis key.Genetictestingandmolecularprofilingnowdissect tumors,exposingtheiruniquevulnerabilities.Doctorscan identifythespecificmutationsdrivingthedisease.Thisis notguesswork;thisisprecision.Thisknowledgeallows fortreatmentplanstailoredtotheindividualchild, personalizedmedicineatitsmostpotent.Dr.Verma utilizesthesediagnosticadvancementstoensurehis patientsreceivethemosteffectivetreatments,minimizing unnecessaryhardship.

RefinedWeaponsintheArsenal:Treatment ModalitiesEvolved
Letusbeclear:thefightagainstcancerdemandsthe bestweapons.Traditionaltreatments–chemotherapy, surgery,andradiation–remainvital,buttheyareno longerbluntinstruments.Theyarenowrefined,honed forgreaterprecision,anddesignedtodeliver maximumimpactwithminimizedharm.Dr.Verma,a mastersurgeontrainedattheprestigiousTata MemorialCancerCentre,wieldsthesetoolswith expertise,alwaysseekingtoenhancetheir effectivenessandreducesideeffectsforhisyoung patients.Heconstantlyseekstorefinesurgical techniquesandintegratethemwiththelatest advancementsinchemotherapyandradiation protocols.
TheRevolutionaries:TargetedTherapiesand ImmunotherapyArrive
Buttherealrevolutionliesinthearrivaloftargeted therapiesandimmunotherapy.Thesearenotjust improvements;theyaregame-changers.Targeted therapiesarelikeguidedmissiles,programmedto strikecancercellsdirectly,leavinghealthycells untouched.Considerneuroblastoma,leukemia,and braintumors–onceterrifyingdiagnoses,nowmetwith tailoredtherapiesthatattacktheverymolecularroots ofthesediseases.Thesearetreatmentsbornof precision,deliveringgreatereffectivenesswithfewer oftheharshsideeffectsassociatedwitholdermethods.
Then,thereisimmunotherapy.Imagineunleashingthe body'sowndefenseforce–theimmunesystem–to fightcancer.Immunotherapyachievesthis.Immune checkpointinhibitorsactascatalysts,empoweringthe immunesystemtorecognizeanddestroycancercells. Foradultcancers,immunotherapyhasalreadyproven itsmettle. Now,clinicaltrialsrevealitspromisefor pediatriccancerslikelymphoma,leukemia,and neuroblastoma.

Associate Director of Surgical Oncology

CAR-Ttherapy,atrulyinnovativeformofimmunotherapy, representsabeaconofhope.Itisaprocessofreengineeringachild’sownT-cells–theimmunesystem’s soldiers–tobecomecancer-seekingmissiles.Doctors extractT-cells,reprogramthemtoidentifyandeliminate cancercells,andthenreturnthemtothechild’sbody CAR-Ttherapyoffersalifelineforchildrenfacingblood cancersthatonceseemedinsurmountable.Dr Vermaisat theforefrontofapplyingthesegroundbreakingtherapies, offeringnewhopewherelittleexistedbefore.
Thefightagainstcancerisnotonlyaphysicalbattle;itisan emotionalandmentalmarathonforbothchildandfamily Enhancedsupportivecarerecognizesthisprofoundtruth. Gonearethedayswhensideeffectsweresimplyendured. Today,thefocusonqualityoflifeisparamount.Better medicationsnowmanagenausea,pain,andfatigue,easing theburdensoftreatment.Butmedicationisonlypartofthe story
Imagineacircleofsupportsurroundingthechildand family–counseling,therapy,peergroups.Thesearenot luxuries;theyareessentialcomponentsofmodern pediatriconcology.Emotionalandmentalwell-beingare nowrecognizedascriticaltothehealingprocess. Pediatriconcologycentersnowroutinelyofferprograms tohelpfamiliesnavigatetheemotionalstormofcancer Thisholisticapproach,championedbyleaderslikeDr. Verma,ensuresthatchildrenreceivenotonlythebest medicaltreatmentbutalsothecomprehensivesupport neededtothriveduringandaftertheirbattle.
WorldUnitedAgainstChildhoodCancer:Global CollaborationandAwareness
Considerthepowerofaunitedfront.Global collaborationandawarenessareamplifyingthefight againstpediatriccancer.Internationalandnational organizationsarejoiningforces,coordinatingresearch, standardizingtreatments,andsharingvitaldataacross borders.Thisunifiedeffortacceleratesprogressand ensuresthatadvancementsreachchildrenworldwide, regardlessoflocation.Dr Verma’sengagementwith internationalmedicalcommunitieskeepshimatthe cuttingedgeofglobalbestpractices,whichhebrings backtobenefithispatientsinIndia.
Theevidenceisundeniable:pediatriccancercarehas undergoneatransformation.Earlydetectionissharper. Treatmentsaremoretargetedandeffective.Supportive careismorecompassionateandcomprehensive.Global collaborationamplifieseveryeffort.
Dr VivekVermastandsasaleaderinthisrevolution.His dedication,expertise,andembraceofinnovationare drivingforcesinthefightforhealthierfuturesfor children.Whilechallengesremain,thepathforwardis illuminatedbyprogressandhope.Personalizedmedicine andimmunotherapyarenotjustfuturepossibilities;they arepresentrealities,offeringbrighterprospectsfor childrenandfamiliesfacingcancer Thevictoryover childhoodcancer,onceadistantdream,isnow,thanksto pioneerslikeDr Verma,apromisewithinreach.



If You Run an Online Pharmacy, You’re in a Trust Business First—Logistics Second.
Youruserisn’tjustbuyingapill.They’re buyingtimesaved.They’rebuyingprivacy They’rebuyingcertaintythatthemedication theyneedwon’tgetdelayed,lost,orfaked.
Andwhenthatcertaintybreaks—even once—theywalk.
Onlinepharmaciesareexplodinginpopularity, andforgoodreason.Butthegapbetweenwhat customersloveandwhatthey tolerate isstill toowide.Anyonebuildingorrunningan ePharmacytodayneedstounderstandthis: you’renotcompetingonpricealone.You’re competingon predictability
Here’swhatmakescustomersstay—andwhat makesthemneverreturn.
Patientsdon'tvisityourapp.Theyarriveatitoutofnecessity
Chronicpain.Post-surgeryfatigue.Achildwithafever Thesearenot shoppingmoods.Theseare“getthisdonenow”moments.Sowhen yourappallowsuserstouploadaprescription,ordermeds,andmove oninunderfiveminutes,youwin.
Themoreyoucutfriction,themoretrustyouearn. That’swhyconvenienceisn'tjustafeature.It’sthewholeproduct.
Customerslovethattheycanuseonlinepharmaciesat1:43a.m.
There’sno“we’reclosed”sign.NoSundayschedule.That'snotjust convenient—that'sthedifferencebetweengettingsleeporsittingina waitingroomatmidnight.
Anursewithagraveyardshift.Acaregiveruplatewithanaging parent.Aparentpanickingovertheirkid’sfirstallergicrash.Theyall wantthesamething:access now.
Platformsthatprovide24/7ordering,support,andrefillnotifications areremovingbarriersthatbrick-and-mortarstoressimplycan’t.

Noteverymedicalconcernisonepeople wanttodiscussinpublic.Mentalhealth meds.
Contraceptives.GIissues.
Onlinepharmacieseliminatethepharmacy counterawkwardness.Youdon'tneedto explainyourconditiontosomeonebehinda glasspanel.Youclick,confirm,andreceive.
Thismattersmorethanmanyrealize. Anonymityoftendetermineswhethera personseekshelp—oravoidsit.
Inalocalstore,comparingmedicationsfeels awkward.Online?It’sexpected.
Usersnowjumpbetweengenericand brandedmeds,searchcoupons,andapply discountswithouthavingtoaskanyone anything.
Theyappreciateknowingthey’renot overpaying.Evenbetter,theylikeknowing whattheirmeds actually do—thankstoclear descriptions,dosageguidelines,andside effectbreakdownsmanyonlineplatforms provideupfront.
Whenappsdoubledownoninformationand pricecomparisontools,customersrepay themwithrepeatorders.
Runningoutofmedsisstressful.Customers expectsmartreminders,auto-refilloptions, andawaytomanageeverythinginoneplace.
Iftheytakethyroidmedsorinsulin,they can’t affordgapsindelivery.Misseddoses= hospitalvisits.Hospitalvisits=alost customer.
Appsthatbuildtrusthere—bygettingrefills right—don’tjustretainusers.Theyownthe customerrelationshiplong-term.
Manyruralortier-2pharmaciessimplydon’tcarryniche drugs.Onlinepharmaciesdo.
Whetherit’sararehormonetreatment,aspecificallergy formulation,ornon-mainstreamwellnesssupplements,digital shelvesarebroader.
Customerswhooncedrove40minutestofindtheirmedication nowgetitattheirdoorstep.Ifyourplatformsupportsthiskind ofaccess,you'renotjustapharmacy You’reinfrastructure.
7.FastSupport.HumanorBot.Doesn’tMatter.
Whensomethinggoeswrong,customersdon’twantempathy. Theywant fixes.
They’reokaywithchatbotsiftheywork.They’refinewaiting 30secondsonacallifitgetsthemalivepersonwhocan cancelawrongorderorresendamissingone.
Thestandardisnotperfection—it’sresolution.
Appsthatprovidein-appsupport,chat-basedpharmacist access,andno-nonsensereturnswinmoreloyaltythanthe onesthat“care”butdon’trespondfor48hours.
1.DelayedorMissedDeliveries
Youdon’tgetasecondchancewithtime-sensitivemeds.
Customersforgiveaslowshampoodelivery Theydon'tforgiveaweek-lateinsulinshipment.
Whenlogisticsbreakdown,trustbreaksinstantly NoUXtweakorchatbotcanpatchthatdamage.
Fast,reliable,real-timetrackingwithproactivedelay notificationsisn’tabonus—it’sthefoundation.
2.DoubtAboutDrugAuthenticity
Customerscan’tseeyourwarehouse.Theycan’tsmellthe pills.They have totrustyougotitright.
Ifyourapplookssketchy,yourbrandsoundsgeneric,orthe pillslookdifferentfromwhatthey’reusedto,suspicion kicksin.

Certificates,verifiedsources, photosofpackaging,expiry dates—thesebuildtrust.
Getanyofitwrong,andthe customerthinks:“Arethese real?”
Theywon’torderagainto findout.
Ifyourappmakesusersfeel dumb,theywon’tuseitagain.
Confusinginterfaces,broken prescriptionuploads, hard-to-readfonts,12-step checkouts—thesekill transactions.Simpleis profitable.
Olderusersespeciallyneed intuitiveflows.Iftheyneed theirgrandsontouploada prescriptionorfindarefill, youjustlostthesale.
Click-to-chatisn’tenough.
Somemedicationsare complex.Somehaveside effectsusersdon’t understand.Andsome customersaretaking7 differentpillsalreadyand don’tknowwhat’ssafe.
In-personpharmacistssolve thisinstantly
Onlinepharmaciesmust replicatethatimmediacy. In-apppharmacistaccess, clearescalationpaths,and consultbookinglinksarethe baselinenow—notthebonus.
Acustomergetstocheckout.Theirwalletappisn’t supported.Orthere’snocash-on-deliveryoption.That’sit. They’regone.
Everyfailedpaymentflow=realrevenueloss.
Digitalwallets,UPI,bankcards,insurance,EMIon high-costtreatments—itallmatters.Ifyourplatform doesn’tsupportit,you’renotjustinconvenient.You’re irrelevant.
Customerswon’tgiveyousensitivedataiftheythinkyou’ll loseit—orsellit.
Medicalhistory,personalIDs,paymentdata—it’sall high-stakes.
Ifyourplatformdoesn’tleadwithcompliance(HIPAA, GDPR,etc.)andvisibleencryptionpractices,youinvite skepticism.
Andifthere’severaleak,youwon’tgetthemback.
Missedorders.Wrongmeds.Failedrefunds.
Withoutfastanddecisiveservice,you’llpayinchurn.
Customersdon’tjustwantresponses.Theywant resolutions—fast.Refunds.Replacements.Clarifications.
Ifyoursupportticketsfeellikeblackholes,yourbrandwill, too.
Here’stheshortlist:
· Letcustomerstrackdeliveriesinreal-time
· Showdrugauthenticityandsourcedetails
· Supportauto-refillsandcleardosageinstructions
· Addlivepharmacistchatorvideoconsults
· Optimizeforspeed:orderingshouldtake<5minutes
· MakeUIusablebya70-year-oldwithbadvision
· Accepteverycommonpaymentmethod
· Builddataprotectionintotheproductfromdayone
· Addmulti-languagesupportforunderservedgeographies
· Createreliablesystemsforerrorhandlingandrefunds
OneRule:Designforthepersonwho needs themeds—nottheonebrowsingsupplements forfun.
Onlinepharmaciesarenotjustabout medicine.They’reaboutkeepingpromises.
Youdeliveronconvenience,privacy, speed—andtrustfollows.Butonemistake, onedelay,onebadsupportcall,andthattrust disappears.
Inthismarket,thebestpharmacyappwon’tbe theflashiest.It’llbetheonethat never makes customerswonderwhatwentwrong.
Sodon’tchasefeatures.Chasereliability That’showonlinepharmacieswillwin. Quietly.Repeatedly Atscale.

Thenews,whenitcame,feltlikeaverdict.The60% majorityshareholderofthreeradiationoncology centersinRhodeIsland,vitalarteriesinthestate’s cancercareecosystem,wasfilingforbankruptcy Thetwolocal healthsystempartners,eachowning20%,hadnoexperiencein radiationoncologyoperationsandwerenotinterestedin investing.Themajorityshareholderwasplanningtopetitionthe bankruptcycourttoclosethethreefacilities,whichwerecaring for100patientsperday.
Forthehundredsofpatientsinthemiddleoftheirtreatment regimens,thenewswascatastrophic.Cancercareis acontinuum,arelentless,preciselytimedbattle. Aninterruptionisnotaninconvenience;itisapotentialdefeat, alife-threateningdisruptiontoacarefullylaidplan. Thesituationwaspoisedtobecomean “enormous negative impact,” apublichealthcrisisunfoldinginreal-time.
Inthismomentofimpendingchaos,GregoryA.MercurioJr sawnotjustaproblemtobesolved,butapromisetobekept. Thiswashiscommunity Thesewerehisneighbors.Hemoved quickly,notwithpanic,butwiththefocusedcalmofamanwho hasspentalifetimeunderstandinghowtheintricategearsof healthcareactuallyturn. “I compiled the best group of industry professionals to quickly remedy this,” herecalls,thesimplicity ofhisstatementbelyingthecomplexityofthetask.
Aftervettingmanypotentialsuitors,heselected AmericanSharedHospitalServices(ASHS), apubliclytradedcompany,toacquirethe60% interest.ASHSinvested$2.7millioninthe acquisitionandanother$2millionintechnology andinfrastructureimprovements.Hepreserved thepatients’continuumofcare,afeatof businessacumenandsheerwillthatstandsas oneoftheproudestmomentsofhiscareer.
TounderstandhowGregorycouldsteersucha crisistoasafeharbor,youhavetounderstand thepaththatledhimthere—apaththatbegan withacloseddoor
Likemanybright,ambitiousyoungpeople, GregoryMercurio’sinitialambitionswereset onbecomingaphysician.Butafternotgaining admittancetomedicalschool,hefaceda crossroads.Insteadofseeingitasanend,he sawitasaredirection.Hemadeadeliberate choicetofocusonthebusinessofmedicine,to findadifferentwaytomakeanimpacton patientcare.




Thatdecision,hereflectsnow,was“indeed fortuitous.” Gregory’sfirstrole,beginningin1983,wasinthe orthopedicindustry,afieldheremainedinthrough2000. Thispivotawayfromaclinicaltracksethimonacourse throughorthopedics,lasersurgery,andeventually,radiation oncology.Itwasajourneythatallowedhimtotouchthe machineryofhealthcarefromauniquevantagepoint. “Through my career,”hesays, “I have personally been able to impact patient care of many more individuals than if I had become a physician.”
Today,thatimpactiswieldedfrommultipleleadership positions.HeistheSeniorVicePresidentofRadiation OncologyatASHS,theCEOofPrecisionRadiation OncologyofRhodeIsland,andtheCEOofBrachyclip HeisalsotheChiefStrategyOfficerforIylonPrecision Oncology,aworldwidecompanyprovidingcustom chemotherapyprescriptions.
InhisroleatASHS,hehasoversightofthreeradiation therapyfacilitiesinRhodeIsland,driveslocalbusiness partnershipinitiatives,and,asamemberofthesenior managementandexecutivecommittee,isinvolvedinevery criticaldecisionregardingbusinessdevelopmentand radiationfacilitiesonaglobalscale.Itisalongwayfrom thatinitialcloseddoor.
AttheheartofGregory’ssuccessisanuancedanddeeply personalapproachtobusiness. “While I am a highly competitive individual,” headmits, “my approach and style to negotiations is cooperative and collaborative to ensure the result works for all parties.” Inanindustrydefinedby highstakesandcomplexnegotiations,heoperateswitha philosophybuiltontwopillars:deepexpertiseand long-standingrelationships.
Gregorynavigatestheintricateworldofhealthcare partnershipsbyhavinganin-depthunderstandingofthe goalsandobjectivesofeverystakeholderatthetable. However,histruestrategicadvantageissomethingless tangible,aqualityhecalls “a nuance that is often overlooked but invaluable.” Heexplains, “Relationships matter and I have spent my entire life in the communities I have served and serve, professionally and personally, so it is obvious I have a vested interest in the outcomes.” Heis notjustabusinessmanflyinginforadeal;heisa communitymemberwhosereputationiswovenintothe fabricoftheregion.Thisgiveshimaleveloftrustand credibilitythatcannotbemanufactured.
HespecificallychoseASHSasapartnerbecauseof theircommitmenttoinvestinRhodeIslandcancer care,expandaccessinunderservedcommunities (suchasBristol),andintroducecutting-edge technologieslikeProtonTherapy.Equallyimportant, ASHSwasnotashort-terminvestoraimingtoflipthe equityin4–5yearsforquickprofit,butalong-term partnergenuinelyfocusedonimprovingpatient outcomes.Gregoryacknowledgesadeepsenseof gratitudetowardASHSforbelievinginhisvision andinvestingsignificantlyinRhodeIsland’scancer carefuture.
Evenwithsuccessfulpartnerships,Gregoryfacesa pressing,industry-widechallengethatrequires constantcreativity. “Challenges with radiation oncology physician recruitment, as well as all the specialty clinical roles unique to radiation oncology are immense,” hestates.It’sastarkrealityofsupply anddemandwhere “the national demand for these roles far exceeds the current and future available pool of qualified individuals.”
Thisisn’tafleetingissue;Gregoryidentifiesitas “both a short-term and long-term challenge with no quick or easy solutions.” Successinthisenvironment requiresmorethanjustacompetitiveoffer “We have to be creative,” heinsists, “and utilize all our expertise, experience and resources to attract the most qualified and compassionate individuals to serve our patients’ needs.” It’saconstant,high-stakessearchfor theverypeoplewhomakeworld-classcarepossible.
Gregory’sabilitytonavigatebothhumanand regulatorycomplexitiesiscrucialinhisfield.Radiation therapyisahighlyregulatedindustrypreciselybecause itinvolvestheuseofradiation,apowerfuland potentiallydangeroustool.Toensuresafety,about50 percentofstatesmandatethatprovidersobtain CertificatesofNeed(CONs)toacquirenew technology.Heseesthis “government created safeguard” notasabureaucraticobstacle,butasa necessaryprocesstoensureonlythemostcapable providersareapproved.WhilesomeviewtheCON processasarduous,hiscollaborativestylehasmade himexceptionallysuccessfulinsecuringthesevital approvals.

Thisskillhasbeeninstrumentalinpursuing whatGregorycallsthe“pinnacleofradiation therapy”:ProtonTherapy.Heidentifiedthat eachyear,approximately400patientsinthe regionwouldbeidealcandidatesforthis treatmentbutwereforcedtotraveltoBostonor NewYorktoreceiveit.SecuringtheCONfora futureProtonCenterinRhodeIslandisoneof hisproudestaccomplishments,alongside obtainingaCONfortheunderserved communityofBristol,RI.Thenewproton facilitywillbeagame-changer,allowing patientstobetreatedwithatechnologyso precisethatitavoidsunnecessaryradiationto healthytissue,resultinginfewersideeffects.
ThisistheultimateexpressionofGregory’s leadershipphilosophy:apatient-centric principlethatdemands “the right treatment, provided by the most highly qualified physicians, at the right time, with the right technology, in a compassionate manner.”

‘ ‘
All healthcare businesses must be operated in a patient centric, regulatory compliant, manner. - American
Heachievesthisnotbymicromanaging,butby empowering. “By assembling the best team and truly empowering them to work together to best serve patients’ needs,” hesays.Recently,dueto theseaccomplishments,hewashonoredwitha HealthCareHeroesAward,amomenthe celebratedwithhisfamily,friends,and colleagues.
Foramanwhoadmitstobeing “a highly driven individual,” theconceptofaperfectwork-life balanceiselusive.Gregory’sworkdayoften extendsintoeveningsandweekends.
Hefindshisbalanceintimespentwithfamily,in philanthropicworkwithorganizationslikethe Jeffrey Osborne Foundation,andonthegolf course,thoughhe “certainly do not claim to have the perfect work-life balance.” Thedrivetomake animpactistoostrong.
Lookingahead,Gregoryisenergizedandexcited aboutthedaythefirstpatientistreatedatthenew ProtonCenter.Afterthat? “Perhaps retirement,” hemuses,thoughitsoundslesslikeadestination andmorelikeabriefpause. “Of course, if something else comes across the horizon, that I feel I can positively contribute to providing or impacting patient care I will certainly find myself involved in those initiatives.”
Itisthisrelentlessfocusonthepatientthat definesGregory’sentirecareer.Hebelievesall healthcarebusinessesmustbeoperatedina patientcentric,regulatorycompliant,manner
Forhim,thismeansthatincancercareespecially, “patients’ physical, psychological, social and economic needs must be tended to in a high quality, compassionate, cost-effective manner.” It’saholisticviewofcarethatheseesasthe foundationofsustainablesuccess.
“If this path is followed, with patients’ needs first, then business will grow, and profits will be realized,” Gregoryconcludes.Itisasimple, powerfulformulathathasguidedhimfroma closeddooratthestartofhiscareertothe pinnacleofcancercare,buildingalegacyof healinginthecommunityhehasalwayscalled home.

In cancer care especially, patients’ physical, psychological, social and economic needs must be tended to in a high quality, compassionate, cost-effective manner. ‘ ‘
- American Shared Hospital Services



What if the most overlooked solution to healthcare burnout, patient overload, and ballooning costs was already in your system—and answering phones?
Everyhealthexecutivetalksaboutscalingcare.Few aredoingitwithoutdrowningtheirclinicalstaffor inflatinginfrastructure.Butsomehavefound leveragewhereothershaven’tlooked:nurse-first, telehealth-poweredsystemsthatusesomethingas unsexyasthetelephonetodeliverscalable, equitable,andefficientcare.
Let’sgettoit.
Let’sStartwiththeHardTruths
Hospitalsarehemorrhagingstaff—not metaphorically,literally.Nursesleavefasterthan systemscanreplacethem.Emergencydepartments overflowwithpatientswhodon’tbelongthere.And physicians?Burnedout,overextended,andexitingin droves.
Everyoneislookingforrelief.Manyareinvestingin techstacksthatpromiseit.Buthere’stheproblem: toomanyleadersaresolvingforthewrong bottleneck.
Theissueisn’tjustaccess.It’sdecision-makingat themomentofuncertainty.Whenapatientfeels unsure,theydefaulttothemostfamiliarpath:theED.
That’snotatechnologyissue.That’sasystem designissue.

WhyNurse-FirstIsn’tOptionalAnymore
Let’sbreakthisdown.
ImagineaSaturdayafternoon.Afrailpatient—let’scall himArthur—feelsworsethanusual.Hisfamilypanics. Nodoctorpicksup.Nonurseisreachable.Noguidance comesthrough.Sotheydowhatmillionsdo:callan ambulanceandgototheER.
Arthurendsupgettingtestshedoesn’tneed.He’s dischargedhourslater,moreexhausted,moreconfused, andnobetter
Nowscalethatscenario.
That’shappeningacrossthousandsofhealthsystems, everysingleweekend.
Themissinglink?Anurseonthelinein real-time—someonewithclinicalexperiencewhocan evaluate,calm,redirect,andescalateonlywhen necessary.Nothourslater.Notafteracallback.Inthe moment.
That’swhatanurse-first,telehealth-drivenmodel delivers.
Andno,itdoesn’tneedametaverseheadsetor multimillion-dollarapp.
Itneedsanurse,aphone,andaclearprotocol.
ThePhoneIsStilltheMostPowerfulCareToolin Healthcare
Healthcareexecslovetochasedigitaltransformation. Butintheprocess,they’reforgettingthemostubiquitous, accessible,andunderutilizedtechnology:thephone.
Let’sgetreal:
· 98%ofAmericanadultshaveaphoneintheirhand rightnow
· 95%ofteensdotoo.
· Evenunderserved,rural,elderly,ormarginalized populationsmaynothavebroadband—buttheyhavea dialtone.
Whensystemsembednurse-firsttriageprotocols directlyintotelephonicchannels,theymeetpatients wheretheyare.
Thebrillianceofthismodelisn’tinfuturisticUX—it’s initsinclusivity,simplicity,andimmediacy.Anyone, anywhere,canreacharealclinicalprofessionalwho knowswhattodonext.
Noapps.Nowaiting.Noconfusion.
ThisIsn’tJustTriage—It’sCommandandControl forYourEntireFlow
Let’smovepastsymptomchecks.
Centralized,nurse-ledtelehealthsystemscanroute patients,managehigh-acuityflow,optimizebed utilization,andpreventclinicalbottlenecks.
Here’showitworks:
1.Atriagenurseanswersthecall.
2.Theyassessthecaseinrealtime.
3.Theyescalateifneeded,routeifnot,anddocument astheygo.
4.Ifatransferisneeded,theyinitiateit—immediately
Youremovefrictionfromtheprocess.Youstopforcing already-exhaustedphysiciansorfloornursestobroker thelogisticsofcare.Andyouletdata—not drama—drivethehandoffs.
MostHealthSystemsThinkThey’reFast.TheData SaysOtherwise.
Mosthospitalexecsassumetheirtransferortriage timesarereasonable.
Buthere’swhathappenswhenyouactuallytrackby 10-minuteincrements,acrossspecialties,andacross peersystems:
· Neurologytransferstake2+hours.
· Cardiologytransfersdroppedfrom20/monthto0.
· Onebehavioralhealthpatientwaits3daysintheED forplacement.
That’snotaresourceproblem.That’sasystem problem
Whenacentralizednurse-firstteammanagestransfers andtriage,theycanspottheselagsinstantly.Theycan escalate,redirect,andload-balanceacrossfacilities withoutinternalpoliticsslowingthingsdown.


Don’tunderestimatethis.
Executiveswhoseethisdatastarttoact.Theyreallocate resources.Theycourse-correct.Andtheyimproveoutcomes fast.
BurnoutHasaSource.ThisModelCutsItOff.
Here’swhatnoonetellsyou:
Physicianburnoutisn’tjustabouthours.It’sabouthow thosehoursarespent.
Whendoctorsspendnightsfieldingnon-urgentpatient questionsthatatrainednursecouldhandle,theylose capacityforactualclinicalcare.
Nurse-firsttriageflipstheequation:
· Nursesabsorbthefirstwaveofpatientneed.
· Theyhandle80–90%ofinquirieswithoutescalation.
· Physiciansfocusonlyoncasesthattrulyneedtheir expertise.
Yougetmoreresteddoctors.Betterdecision-making. Andfarlessriskofclinicalerrorsdrivenbyfatigue.
It’snotjustaboutefficiency.It’saboutprotectingthe integrityofyourcareteams
ButWhatAboutCost?
Outsourcingthiskindofmodelfeelsexpensive—untilyou compareittothecostofnotdoingit:
· UnnecessaryEDvisitscost$500–$2,000each.
· Poortransferperformanceclogsuphigh-acuitybeds.
· Burned-outphysiciansleadtoturnoverandcostlylocum tenenshires.
· Delayedroutingresultsinworseoutcomes,longerstays, andhigherreadmissionrates.
Meanwhile,acentralized,nurse-ledtelehealthhuboperates atscale,standardizesperformance,andprovides data-driveninsightintoeverycaretransaction.
It'snotoverhead.It’s . anoperationalengine
Anditfreesyouron-siteteamstodowhatonlytheycan do—careforpatientsinperson.
BottomLine:ThisModelWorksBecauseIt’sBoring
There’snoflashydevicehere.NoAIavatarorVR simulation.
Justexperiencednurses.Provenworkflows.Simpletools. Relentlessconsistency
Thismodeldeliversbecauseit , removesdecisionparalysis speedsupcare,protectsyourworkforce,andgivespatients confidence—withoutexpensiveinfrastructureorheavy learningcurves.
Inaworldthatovercomplicatesinnovation,thisishow healthsystemswinquietly.
FinalThoughtforHealthcareLeaders
Ifyou’reaCEO,COO,orCNOlookingforscale,thisis yourleveragepoint.
Stopthrowingpeopleattheproblem.Startbuilding systemsthatthinkahead.
Letnurseslead.
Usethephone.
Tracktherightdata.
Buildamodelthatworksontheground,notjustinyour boardroomslidedeck.
Thesmartesthealthsystemsarealreadydoingthis.Therest willcatchup—butatacost.
●YujiOtsukileadsFerroptoCureindevelopingnewanticancerdrugsusingferroptosis, anovelapproachtargetingseriousillnesses.
●FerroptoCure’sbreakthroughsincludeadvanceddrugsinclinicaltrialsandtheuseof technologieslikenext-generationsequencingandsilicoanalysis.
●YujiiseagertoexpandFerroptoCure’sdrugpipelineandexplorenewtherapies, focusingoninnovationandbetterpatientoutcomes.
“Hopeisthefoundationofthehumanspirit,andit’swhat drivesustofighteventhemostdauntingbattles.”
ThesewordscapturethedriveofYujiOtsuki,CEOof FerroptoCureInc.Ascancerandneurodegenerative diseasesbecomemorecommon,especiallyintheAsiaPacificregionamongthoseover50,theneedfornew treatmentshasneverbeenmoreurgent.
FerroptoCureactivelydevelopsnext-generationanticancer andtherapeuticdrugs,focusingonferroptosis,acuttingedgeapproachtotargetingcancerandotherserious illnesses.UnderYuji’sleadership,thecompanycontinuesto pushtheboundariesofmedicalresearchandpatientcare.
Yuji’sjourneystartedwithamedicaldegreefromHokkaido University,followedbydoctoralstudiesatKeioUniversity, withafocusononcology.Hisexperiencemanagingaclinic gavehimuniqueinsightsintopatientcare,directly informinghowheleadsFerroptoCuretoday
Inarecentconversation,Yujisharedhisthoughtsonthe challengesandbreakthroughsincancertreatment.His commitmenttoadvancingmedicalscienceand improvingpatientoutcomesdrivesFerroptoCure’s missionforward.
GHM:FerroptoCureInc.wasestablishedwitha powerfulmissioninmind.Couldyouelaborateon howthecompany’svaluesandgoalsshapeyour approachtodrugdiscovery?
Yuji:FerroptoCureInc.wasfoundedwithaclear mission:“Treatingdiseasebyferroptosisdrug discovery.”Ourcorevalues—integrity,urgency,anda commitmenttoimprovingpatientlives—guide everythingwedo.Manyofourteammembershave firsthandexperiencewiththechallengesoftreating diseasesinclinicalsettings.Thisdrivesourdesiretofind curesforpatientswhocurrentlyhavelimitedorno treatmentoptions.


Ourgoalistodevelopinnovativetherapiesthatleverage theferroptosismechanism,whichhasshownpromisein addressingvariousdiseases,includingcancerand neurodegenerativedisorders.
GHM:Couldyouexplainthesignificanceof ferroptosisandhowFerroptoCureInc.isutilizingthis mechanismindrugdevelopment?
Yuji:Ferroptosisisanaturalformofcelldeaththatrelies onironandistriggeredbyoxidativestress.Itplaysakey roleinthedevelopmentandprogressionofvarious diseases,includingcancer,neurodegenerativedisorders likeAlzheimer’sandParkinson’s,andliverconditions suchasNASH(non-alcoholicsteatohepatitis).
Recentresearchhashighlightedtheimportanceof controllingferroptosis,particularlyinitsconnectionto canceroccurrence,proliferation,andthedevelopmentof resistancetocertainanticancerdrugs.
AtFerroptoCure,weaimtoharnessthismechanismto developnewanticancertherapieswiththepotentialfor unprecedentedefficacyacrossawiderangeofcancer types.Ourapproachinvolvesadvancedtechnologieslike next-generationsequencing,datainformatics,andin silicoanalysis.
Inaddition,wecollaboratewithleadingresearch institutionsanduniversitiesattheforefrontofferroptosis researchtoacceleratethediscoveryanddevelopmentof thesegroundbreakingtreatments.
GHM:Canyoutellusmoreaboutyourmost impactfulproductsandhowthey’reshapingthe futureofcancertherapy?
Yuji:Ourmostsignificantproductsarenext-generation anticancerdrugsthattriggerferroptosisincancercells. Thisprocesshelpsstopcancerfromprogressing, especiallyincaseswhereconventionaltreatmentshave failed.Wefocusondisruptingtheantioxidant mechanismsofcancercells,particularlythoseinvolving thecystine/glutamatetransporter(xCT)andglutathione peroxidase4(GPX4),whicharecriticalfortheirsurvival.
Todevelopthesetherapies,werelyonadvanced technologieslikenext-generationsequencinganddata informatics.Thesetoolsgiveusdeeperinsightsintothe geneticandmolecularrootsofdiseases,whichallowsus tocreatemorepreciseandeffectivetreatments.
Inaddition,weuseinsilicoanalysis,wherecomputer simulationshelpuspredicthowourdrugswillworkin biologicalsystems.Thisacceleratesthedrugdevelopment processandhelpsidentifypotentialchallengesearlyon.
Wehavealsoseenpromisingresultsinclinicaltrialsusing xCTinhibitors.Whencombinedwithchemotherapy,these inhibitorshaveshownpotentialinprolongingprogressionfreesurvivalinpatientswithadvancedlungcancer Tostay attheforefrontofscientificadvancements,wecollaborate withleadingresearchinstitutes.
Interestingly,weareextendingtheapplicationofour anticancertechnologiestocompanionanimals,aimingto createeffectivetreatmentsforpetssufferingfromcancer. Currently,ourprimarytargetsaretriple-negativebreast cancerandrenalcancer
GHM:Canyousharemoreaboutyourkey responsibilitiesasCEOandhowyoufoster collaborationwithinyourteam?
Yuji:AsCEO,Ifocusonseveralkeyareas—fundraising, strategicplanning,day-to-dayoperations,andguidingour researchefforts.Iworkcloselywithadedicatedteamof researchersandprofessionalstoensureallprojectsstay alignedwithourmissionandvalues.Creatinga collaborativeandinnovativeworkenvironmentisessential, andIfocusonblendingthediverseskills,knowledge,and experiencesofourteammembers,eachofwhombrings uniqueexpertisefromparticularregions.
GHM:InyourjourneyleadingFerroptoCure,what challengeshaveyoufaced,andhowhaveyouovercome them?
Yuji:Throughoutmycareer,I’vefacedsignificant challenges,suchassecuringfundingforourresearchand navigatingcomplexregulatoryhurdles.Totacklethese,I focusedonbuildingstrongnetworks—notjustwithinthe scientificcommunitybutalsowithfinancialandbusiness developmentprofessionals.Formingstrategicpartnerships hasbeencrucialinsupportingourinitiativesandpushing ourmissionforward.
GHM:Canyouhighlightsomeofyourkeyresearch achievementsandsharewhatexcitesyouaboutthe future?
Yuji:Oneofourkeyaccomplishmentsisthesuccessful developmentofourleaddrugcandidate,whichhasentered

Phase1clinicaltrials.Thismarksthefirst clinicaltrialinourregionfocusedon ferroptosis-inducingcancertherapy.Beyond that,ourresearchhassignificantlyadvancedthe understandingofferroptosisincancerbiology, leadingtoinnovativetherapeuticapproaches.
Lookingahead,I’mexcitedaboutour upcomingprojects.Weareexpandingourdrug pipelineandexploringnewtherapeuticareas. Ourgoalistoadvanceourresearchin ferroptosistodeveloptreatmentsforother diseasesbeyondcancer
GHM:Assomeonedeeplyinvolvedin cutting-edgecancerresearch,whatmessage wouldyouliketosharewiththoseaffected bycancerandotherseriousillnesses?
Yuji:Iwanttoencouragereaderstostay hopefulinthefightagainstcancerandother debilitatingdiseases.AtFerroptoCure,weare deeplycommittedtoinnovationandpatient care.Ourongoingresearchandcollaborative effortsdriveusforward,andwefirmlybelieve that,together,wecanmakesignificantstridesin improvinghealthoutcomesforeveryone.
We’re not just developing treatments for cancer; we’re also applying our technologies to improve health outcomes for companion animals, which we call ONE CURE.


SCAN & GET INSPIRED, STAY UPDATED WITH ALL THE BUSINESS WORLD BUZZ WITH GLOBAL HEALTH CARE MAGAZINE

