


Theme: Innovation in Precision Digestive Medicine
Date: September 27th (Sat) ~ 28th (Sun), 2025
Venue: NTUH International Convention Center


Theme: Innovation in Precision Digestive Medicine
Date: September 27th (Sat) ~ 28th (Sun), 2025
Venue: NTUH International Convention Center
Chun-Jen Liu
Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
Viral hepatitis due to chronic hepatitis B virus (HBV) or hepatitis C virus (HCV) infection and metabolic dysfunction-associated fatty liver disease (MAFLD) are common liver diseases worldwide. Therefore, in clinical practice, we may encounter subjects with dual etiology of liver diseases such as co-existing HBV/HCV and MAFLD/HBV. In my presentation, the clinical features and mutual
interactions of HBV with co-existing HCV will be reviewed first. From the experience of these interactions between HBV and HCV, the impact of MAFLD on the clinical presentations of liver diseases and treatment outcomes in patients with chronic viral hepatitis B, and the clinical questions to be addressed regarding dual etiology will be discussed.
Yuko Kitagawa
Department of Surgery, Keio University, School of Medicine, Tokyo, Japan
While non-invasive medical approaches have become mainstream in many areas of gastroenterology, surgery continues to address various challenges as the last resort for the treatment of refractory diseases. Laparoscopic-endoscopic cooperative surgery for early gastrointestinal cancer has become an essential technique for minimally invasive and personalized treatment. A future is approaching where individualized precision surgeries using lymphatic mapping are performed with endoscopic full-thickness resection and intraperitoneal surgery utilizing flexible endoscopes. With the advancement of drug therapies such as immune checkpoint inhibitors and radiation therapy, opportunities for conversion surgery in initially unresectable cases have increased. Liver transplantation as a form of conversion surgery has also begun as advanced medical treatment for hepatocellular carcinoma and cholangiocarcinoma. Looking ahead, future transplant medicine is expected to evolve with organoid technologies, organ generation using chimeric animals, xenotransplantation, and organ regeneration medicine, including esophageal and
liver regeneration research that we have been conducting. Given that fluctuations in the intestinal microbiota are significantly related to the host’s postoperative infection risk and immune responses, approaches such as probiotics, synbiotics and fecal microbiota transplantation are being considered for perioperative management. Elucidating the mechanisms by which the intestinal environment interacts with systemic organs will help establish optimal perioperative management and intensive care. Efforts are also underway to use artificial intelligence (AI) for analyzing genomes and pathologies, predicting prognoses, and selecting optimal treatments by interpreting genetic and pathological data. In pharmaceutical development, AI is expected to facilitate faster drug development by enabling molecular and protein structure analysis and optimizing clinical trials. Furthermore, AI is also essential tool to improve quality of surgery. Through these studies and in collaboration with gastroenterologists and basic researchers, we surgeons aspire to contribute to the innovation in precision digestive medicine and further advancement of gastroenterology.
Ryosuke Tonozuka
Department of Gastroenterology and Hepatology, Tokyo Medical University, Tokyo, Japan
Endoscopic ultrasound (EUS) plays a pivotal role in the diagnosis of pancreatic and biliary diseases, particularly in detecting small pancreatic tumors that often escape conventional imaging modalities. However, diagnostic accuracy is heavily dependent on operator expertise. The integration of artificial intelligence (AI) into EUS—especially through computer-aided diagnosis (CAD) systems—offers the potential to standardize and enhance diagnostic precision across institutions. The first report on EUS-CAD was published by Norton et al. in 2001, who developed a basic neural network model for differentiating chronic pancreatitis from pancreatic malignancy. Since then, although only a limited number of studies using basic AI models have been conducted, reports of deep learning-based CAD models have markedly increased in 2020s. In 2020, our group also reported a single-center model for pancreatic cancer detection, achieving a sensitivity of 92.4%, specificity of 84.1%, and an area under the ROC curve of 0.940. Building on these findings, we subsequently conducted a multicenter collaborative
study of EUS-CAD. In this recent research, we highlight a convolutional neural network trained on over 1,600 EUS cases across six high-volume centers in Japan. This model achieved impressive accuracy in tumor detection (sensitivity 95.5%, specificity 97.0%), binary classification (neoplasm vs. non-neoplasm accuracy: 85.2%), and three-class categorization (PDAC: 74.8%, PNEN: 41.2%, others: 61.3%). While the results for tumor detection were satisfactory, those for differentiation remained insufficient, largely due to the diversity of pancreatic disease imaging features and the limited number of cases in each category. Moving forward, further refinement through large-scale data accumulation and real-world clinical application of CAD systems will be essential. Although challenges remain in generalizability and data diversity, the results underscore the growing maturity of EUS-CAD and its potential for clinical integration. AI is not a distant future—the future of endoscopic diagnosis, augmented by AI, may indeed be right before our eyes.
Man-Fung Yuen
Department of Medicine, School of Clinical Medicine, The University of Hong Kong, Hong Kong
Although disease outcome and the factors associated with the risk of development of disease complications of chronic hepatitis B infection have been largely defined, criteria of treatment are constantly evolving. In the recent years, recommendations and guidelines for treatment indication have become less stringent. The expansion of antiviral treatment for chronic hepatitis B represents a pivotal shift in modern healthcare, offering both unprecedented opportunities and notable challenges. On one hand, broader access to antiviral therapies can significantly reduce the incidence of liver cirrhosis, hepatocellular carcinoma, and related complications, improving patient outcomes and overall public health. Enhanced treatment strategies may also curb the transmission rates of the virus, thereby contributing to long-term disease control at the population level.
However, the widespread implementation of antiviral regimens raises important concerns. Longterm treatment is associated with risks of patient non-compliance, potential long-term side effects
and poor patient acceptability. However, these caveats are not insuperable. Treat-all approach is also a complexed decision as there are multiple factors including local disease epidemiology, health resource availability and socioeconomic factors, all of which are uniquely different among different regions and countries. The economic burden of lifelong treatment for millions of affected individuals also poses serious questions about healthcare resource allocation and sustainability, especially in regions with limited funding. Furthermore, expanding treatment eligibility may require careful consideration of individual patient factors, such as comorbidities, adherence potential, and quality of life impacts.
Ultimately, while the expansion of antiviral treatment holds promise for transforming the landscape of chronic hepatitis B management, it must be balanced by thoughtful policy-making, vigilant clinical oversight, and continued investment in research and education.
Eugene B. Chang
Department of Medicine, University of Chicago, Chicago, IL, USA
The interactions of gut microbiome with host immune and metabolic processes are dynamic, bidirectional and critical for all stages of life including immune development and regulation, energy harvest and metabolism, and modulation of gut mucosal function and homeostasis. On the other hand, perturbations that cause gut dysbiosis and dysfunction in the Gut-Immune-Metabolic Axis can cause and contribute to diseases like inflammatory bowel diseases, obesity/diabetes, fatty liver diseases and colorectal cancer. Currently, most microbiome therapies lack precision and
evidence that support claims of their efficacy. Better tools and technologies are needed that stem from disentangling the intricacies of host-microbe interactions underpinning stages and states of gut microbiome health, stability and resilience and host gene expression and function. This knowledge will inform future strategies for the development of more effective and precision microbiome-based interventions that can maintain, restore or reprogram the Gut-Immune-Metabolic Axis to promote health and prevent or treat digestive diseases.
Sutep Gonlachanvit
Gastrointestinal Motility Ceneter, Bumrungrad International Hospital, Bangkok, Thailand
Patients with refractory gastroesophageal reflux symptoms despite adequate acid-suppressive therapy are frequently encountered in clinical practice. This group includes individuals with functional heartburn, esophageal hypersensitivity with normal distal esophageal acid exposure, and true refractory GERD. The latter refers to patients with objectively confirmed GERD whose symptoms remain uncontrolled despite optimized acid suppression. Traditional management strategies for refractory GERD—lifestyle modifications, optimization of acid suppression, adjunctive pharmacological therapy, and anti-reflux procedures—have been utilized for decades. Nevertheless, a considerable proportion of patients continue to report unsatisfactory outcomes, even following surgical or endoscopic interventions. It has been demonstrated that GERD frequently overlaps with disorders of gut–brain interaction (DGBIs), and that such overlap is associated with poor response to proton pump inhibitor (PPI) therapy. Despite the clinical relevance, the pathophysiological interplay between GERD and DGBIs remains incompletely understood. At my center (CUNM), increasing attention has been directed toward the influence of belching behavior, constipation, abdominal bloating, and gut fermentation on gastroesophageal reflux (GER) and treatment-resistant GERD.
Supra-gastric belching (SGB) has been identified as a major mechanism underlying reflux episodes in patients with both GERD and belching symptoms. A recent study indicated that SGB-associated GER is not explained by abnormal gastro-thoracic pressure gradients but is more likely related to modulation of transient lower esophageal sphincter relaxations (TLESRs) by behavioral or central mechanisms. Indeed, TLESR-related belching frequently precedes
pressure changes induced by belching. These findings suggest that abnormal belching behavior itself contributes to reflux pathogenesis, and that targeted management of SGB may ameliorate GERD symptoms even in the absence of acid-suppressive therapy.
Constipation and colonic stool retention have also been implicated in the modulation of GER. Patients with GERD experience fewer postprandial reflux episodes when the colon is emptied compared to when stool retention is present. Consistent with this, interventions such as psyllium supplementation not only improve constipation but also reduce GERD symptoms and prolong remission compared to PPIs alone. This highlights the therapeutic potential of addressing constipation in GERD patients with coexisting bowel dysfunction.
Abdominal bloating, often linked to intestinal gas production and colonic fermentation, also plays a role in GER. Experimental studies have demonstrated that colonic infusion of short-chain fatty acids, the principal products of fermentation, induces relaxation of the lower esophageal sphincter. Moreover, high-FODMAP meals (e.g., wheat-based) provoke greater postprandial reflux compared with low-FODMAP meals (e.g., rice-based), underscoring the dietary contribution to symptom modulation.
These insights emphasize that comorbid DGBIs—including belching disorders, constipation, bloating, and IBS—not only worsen GERD symptoms but also impair response to conventional therapies. Data from the Center of Excellence in Neurogastroenterology and Motility at Chulalongkorn University (CUNM), presented at the Federation of Neurogastroenterology and Motility (FNM 2024), showed that GERD patients who achieved control of belching or bloating were
significantly more likely to discontinue or reduce PPI therapy. Notably, comorbid DGBIs are observed in approximately 40%–46% of GERD patients in Asia, highlighting their substantial clinical impact.
Conclusion:
GERD overlapping with DGBIs is common, associated with diminished quality of life, and characterized by poor responsiveness to PPI
therapy. Emerging evidence indicates that targeted management of comorbid DGBIs can reduce GERD severity, sustain remission, and decrease reliance on acid-suppressive medication. Integrating the treatment of DGBIs into GERD management frameworks therefore represents an essential step toward optimizing patient outcomes.
Yutaka Saito
Endoscopy Division, National Cancer Center Hospital, Tokyo, Japan
The risk of lymph node metastasis (LNM) in colorectal T1 cancer is primarily evaluated using the Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines.¹ These guidelines recommend surgical resection when submucosal (SM) invasion exceeds 1,000 μm, lymphovascular invasion (Ly/V) is present, tumor budding is grade 2/3, or when poorly differentiated adenocarcinoma is identified.¹
Recent meta-analyses have demonstrated that the LNM risk is extremely low if all other risk factors are absent, even when SM invasion is deep.² However, significant interobserver variability exists in measuring SM invasion depth, and diagnostic concordance for Ly/V remains suboptimal despite immunohistochemical staining.
A large multicenter study by the JSCCR involving 4,673 T1 colorectal cancer cases identified additional LNM risk factors, including SM invasion >2,000 μm, rectal or sigmoid tumor location, female sex, and moderately differentiated histology.³ Notably, rectal cancers are often treated less aggressively due to concerns about postoperative quality of life, yet they exhibit higher metastatic recurrence rates than colon cancers.
Moreover, a recent meta-analysis reported that up to 40% of high-risk T1 cancer patients who develop recurrence without surgery ultimately die from the primary disease.⁴ These findings underscore the urgent need for improved treatment strategies.
Ongoing clinical trials, such as JCOG1612, are currently evaluating adjuvant chemoradiotherapy (CRT) following local resection as a potential
alternative for patients at high risk.⁵ This presentation will summarize the current limitations of endoscopic treatment for colorectal T1 cancer and highlight future directions for additional therapeutic strategies.
1. Hashiguchi Y, Muro K, Saito Y, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int J Clin Oncol. 2020;25(1):1–42.
2. Zwager LW, Bastiaansen BAJ, et al. Deep Submucosal Invasion Is Not an Independent Risk Factor for Lymph Node Metastasis in T1 Colorectal Cancer: A Meta-Analysis. Gastroenterology. 2022;163(1):174–189.
3. Kajiwara Y, Oka S, Tanaka S, et al. Nomogram as a novel predictive tool for lymph node metastasis in T1 colorectal cancer treated with endoscopic resection: a nationwide, multicenter study. Gastrointest Endosc. 2023;97(6):1119–1128.e5.
4. Dang H, Dekkers N, le Cessie S, et al. Risk and Time Pattern of Recurrences After Local Endoscopic Resection of T1 Colorectal Cancer: A Meta-analysis. Clin Gastroenterol Hepatol. 2022;20(12):2817–2828.
5. Noguchi M, Shitara K, Kawazoe A, et al. Shortterm safety of adjuvant chemoradiotherapy after local resection for patients with high-risk submucosal invasive rectal cancer: a singlearm, multicenter phase II trial. Jpn J Clin Oncol. 2021;51(5):707–712
Kyle Farh
Illumina Artificial Intelligence Laboratory, Illumina, Inc., San Diego, CA, USA
Large scale human genetics cohorts, comprising hundreds of thousands of individuals with medical record data, are now at the leading edge of modern drug discovery pipeline. This strategy aims to improve upon the current low rate of success in pivotal clinical trials by demonstrating evidence of efficacy directly in humans, as opposed to the
traditional strategy of testing in mice and other model organisms. Here we demonstrate the use of the latest AI and deep learning technologies to improve interpretation of both protein-coding and noncoding genetic variation in large human genetic cohorts, leading to novel insights for genetic risk prediction and drug target discovery.
of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea
Metabolic dysfunction–associated steatotic liver disease (MASLD) has emerged as the most prevalent chronic liver disease worldwide, with a rapidly increasing burden in both Western and Asian populations. While most patients remain asymptomatic, a substantial proportion progress to advanced fibrosis, cirrhosis, and hepatocellular carcinoma (HCC), and are also at heightened risk for extrahepatic outcomes including cardiovascular disease (CVD) and chronic kidney disease (CKD). Accordingly, accurate risk stratification is essential not only for guiding surveillance and therapeutic interventions, but also for allocating healthcare resources efficiently. Traditionally, liver biopsy has served as the gold standard for fibrosis assessment and prognostic evaluation, but its invasive nature, sampling variability, and limited acceptability have spurred growing reliance on non-invasive tests (NITs).
Over the past decade, NITs—including serumbased indices such as FIB-4, NAFLD fibrosis score, and the enhanced liver fibrosis (ELF) test, as well as imaging modalities such as vibration-controlled transient elastography (VCTE) and magnetic resonance elastography (MRE)—have demonstrated robust diagnostic accuracy in staging fibrosis. More importantly, emerging longitudinal evidence has highlighted their prognostic utility. Elevated liver stiffness measurements by VCTE or MRE independently predict the risk of HCC, hepatic decompensation, and liver-related mortality in MASLD patients. Similarly, higher FIB-4 or ELF scores are consistently associated with adverse outcomes, not only of hepatic origin but also cardiometabolic events, underscoring the systemic implications of fibrotic burden.
Dynamic changes in NITs further enhance prognostication. Recent cohort studies indicate that increases in VCTE-derived liver stiffness or persistent
high-risk Agile scores are closely linked with subsequent clinical events, whereas regression in NIT categories may correlate with improved outcomes. These findings open opportunities for repeated NIT monitoring to track disease trajectory and evaluate therapeutic responses in both clinical practice and clinical trials.
Nevertheless, challenges remain. Cut-off values may differ across populations depending on age, obesity, and diabetes prevalence. The low positive predictive value of simple scores like FIB-4 in younger or community-based cohorts limits their application as stand-alone prognostic tools. Moreover, integration of NITs into real-world clinical pathways remains suboptimal; many primary care physicians are unaware of or do not utilize simple indices such as FIB-4, resulting in missed referrals and underdiagnosis of advanced fibrosis.
Looking ahead, risk stratification in MASLD is expected to evolve into a multimodal approach. Combining NITs with clinical features, genetic and metabolic biomarkers, and artificial intelligence–based modeling will likely improve predictive accuracy and enable precision medicine. Large-scale collaborative cohorts, such as those harmonizing VCTE and MRE data, are now providing critical evidence to refine prognostic thresholds and validate risk models across diverse populations.
In this lecture, I will review the current evidence on the prognostic utility of NITs in MASLD, covering hepatic and extrahepatic outcomes, the role of dynamic monitoring, and integration into care cascades. I will also highlight ongoing efforts to build international NIT-based networks and propose future directions toward optimized prognostication and individualized management of MASLD patients.
Jun Yu
Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Hong Kong
The gut microbiome and its role in carcinogenesis is a rapidly evolving research field. We have revealed the multi-kingdom alterations of gut microbiota in CRC and identified the oncogenic effects of specific CRC-enriched microbes, including P. anaerobius (Gastro 2017b, Nat Microbiol 2019), A. rambellii (Gastro 2022a), P. stomatis (Cell Host Microbe 2024). These microbes promote CRC via director binding to host cell surface protein to activate oncogenic pathways (Nat Microbiol 2024). For clinical translation, we discovered CRC-depleted bacteria (i.e. S. thermophilus, L. gallinarum, C. maltaromaticum) that are capable of producing anti-CRC enzymes or metabolites (Gastro 2021b, Gut 2022b, Cancer Cell 2023). For CRC screening, we pioneered the use of fecal microbes (e.g. Lachnoclostridium sp., F.
nucleatum) or metabolites as non-invasive markers for the detection of colorectal adenoma and cancer (Gut 2017a, Gut 2017b, Clin Cancer Res 2017, Gut 2019, Cancer Cell 2024a). For immunotherapy, we identified R. intestinalis generated butyrate boosts anti-PD-1 efficacy in CRC by activating cytotoxic CD8+ T cells (Gut 2023a) and L. gallinarum boosts anti-PD1 efficacy by inhibiting regulatory T cells through modulating IDO1/Kyn/AHR axis (Gut 2023b). Moreover, F. nucleatum facilitates anti-PD-1 therapy in MSS CRC (Cancer Cell 2024b). These findings collectively provide new insights for the function, mechanism and clinical translation of gut microbiota in cancers (Yu J etc, Nat Rev Gastrolenterol and Hepatol 2019, 2023; Nat Rev Gastroenterol Hepatol, 2023; Cell 2024b).
Masayuki Saruta
Division of Gastroenterology and Hepatology, Department of Internal Medicine, The Jikei University School of Medicine, Tokyo, Japan
Inflammatory bowel disease (IBD), comprising ulcerative colitis (UC) and Crohn’s disease (CD), is previously it was more prevalent in Western countries, especially in North America and Europe, while over the past two decades, the incidence and prevalence of both UC and CD in Asia have risen dramatically. In Japan, the number of UC and CD patients in JAPAN in 2014 was more than 180,000 and 40,000, respectively, recent epidemiological survey revealed that the number of UC and CD patients in JAPAN in 2024 was 316,900 and 95,700, respectively. The clinical characteristics, genetic background, and disease behavior in Asian patients often differ from those seen in Western populations, highlighting the need for region-specific data and treatment strategies. On the other hand, in the
past, advanced treatments for IBD in Asia lagged significantly behind those in Western countries, but in recent years, as Asian countries have increasingly participated in international clinical trials, this drug lag has been steadily diminishing.
This lecture highlights the evolving trends in IBD management in Asia, with a special focus on endoscopic techniques, mucosal healing as a treatment target, and the real-world application of biologics and small molecules. Drawing from our clinical experience and data, we will explore how the integration of endoscopic scoring systems and treatto-target strategies can improve patient outcomes. In addition, I will also focus on disparities in access to advanced therapies and the need for harmonized treatment guidelines across Asian countries.
Joseph Sung
Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore
Despite the proven success of colorectal cancer screening in reducing incidence and mortality of the disease, there are still many gaps in our implementation of the screening program.
Getting people in the door (and back again). Screening uptake still lags targets (especially ages 45–49 and several racial/ethnic groups). Even after a positive stool test, too many people never complete the follow-up colonoscopy, which erases most of the benefit of screening. Capacity and care navigation. Systems struggle to absorb surges in demand (younger start age, more positives from stool/FIT or blood tests), leading to bottlenecks and delayed follow-up. Quality variation in colonoscopy. Adenoma detection rate (ADR), withdrawal time, and bowel-prep quality vary meaningfully—fueling interval cancers (especially right-sided) from missed lesions and inadequate prep. AI-assisted detection helps but isn’t universally implemented.
Equity gaps. Lower screening and follow-
up among some communities (e.g., Black, Asian, Hispanic; lower income; immigrants) persist, with measurable differences in follow-up colonoscopy and ADR. Modality trade-offs aren’t well “operationalized.” Stool DNA and the new bloodbased tests (easier, can lift uptake) still have lower sensitivity for advanced adenomas and require tight recall systems; programs haven’t fully optimized who gets what, how often, and how to ensure positive tests end in colonoscopy. Risk-stratified screening isn’t mainstream. Polygenic risk scores (PRS), clinical calculators, and microbiome signatures show promise, but aren’t yet integrated into routine screening pathways or reimbursement in a way that clearly improves outcomes.
Young-onset CRC (EOCRC) uncertainty. We lowered the start age to 45, but optimal strategies for <45 (based on symptoms, family history, PRS, lifestyle) remain unsettled.
38th Annual Academic Meeting
Seung
Metabolic dysfunction–associated steatotic liver disease (MASLD) has rapidly emerged as the most common cause of chronic liver disease worldwide, with an estimated prevalence of 25–30% among adults and even higher rates in highrisk populations such as those with obesity, type 2 diabetes mellitus (T2DM), and metabolic syndrome. The recent shift from the term “NAFLD” to “MASLD” emphasizes the disease’s metabolic underpinnings and its strong links with extrahepatic conditions, particularly cardiovascular disease (CVD) and chronic kidney disease (CKD). For hepatologists, this epidemiologic shift carries profound implications: MASLD is no longer a niche diagnosis but a central challenge in liver practice that intersects with global public health priorities.
This presentation will highlight why MASLD must be a strategic focus for hepatologists now and in the coming decades. I will first review recent epidemiologic data showing MASLD’s rising contribution to cirrhosis, hepatocellular carcinoma (HCC), and liver transplantation, alongside its role as a driver of non-liver mortality, particularly CVD. I will then discuss how its systemic pathophysiology — including insulin resistance, adipose tissue dysfunction, lipotoxicity, chronic inflammation, and gut–liver axis alterations — links hepatic injury to broader metabolic complications.
A core component of the talk will focus on risk stratification and early detection, with an emphasis on integrating noninvasive tests (NITs) such as FIB-4, vibration-controlled transient elastography (VCTE), and magnetic resonance elastography (MRE) into routine workflows in both primary and specialty care. The evidence supporting fibrosis stage as
the strongest predictor of liver outcomes will be discussed, along with practical strategies for triaging patients efficiently.
I will also cover the therapeutic landscape, beginning with lifestyle interventions — still the first-line therapy — and progressing to emerging pharmacologic options, including GLP-1 receptor agonists, dual/triple incretin agonists, FGF-21 analogues, and THR-β agonists. I will highlight key clinical trial data relevant to hepatologists, including their effects on steatosis, inflammation, fibrosis, and metabolic risk factors. Procedural interventions such as bariatric surgery will also be addressed for appropriate candidates.
Finally, I will address the future of MASLD care from a hepatologist’s perspective. This includes embracing a more multidisciplinary role — collaborating closely with endocrinology, cardiology, nephrology, nutrition, and primary care — and adapting to new models of precision medicine, combination therapy, and long-term monitoring. Challenges such as disease heterogeneity, healthcare system burden, cost of emerging therapies, and the need for long-term outcome data will be critically examined.
By the end of this talk, attendees will have an updated framework for understanding MASLD not just as a liver condition, but as a multisystem disease that demands early detection, individualized treatment, and coordinated care. The goal is to equip hepatologists with the knowledge and strategies necessary to meet this rapidly evolving clinical challenge and to improve both hepatic and systemic outcomes for their patients.
38th Annual Academic Meeting
Yen-Po Yeh
Changhua County Public Health Bureau, Changhua, Taiwan Institute of Epidemiology and Preventive Medicine, College of Public Health & Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan
Preventive health service has gained traction with a transformative approach to public health that integrates traditional evidence-based practices with emerging precision health strategies. In the past two decades, the initiatives in Changhua have demonstrated how the inter-disciplinary collaborative approaches were adopted to pursue such a transformation of preventive health care extending from early detection of screening to primary prevention. This approach has been particularly relevant to gastroenterology, given that more than 40% of cancer-related deaths in Taiwan are attributable to gastrointestinal cancers.
The Changhua Community-based Integrated Screening (CHICS) program was launched in 2005. CHCIS is built on the principles of evidence-based medicine and strives to integrate preventive health services within the community, addressing both neoplastic and non-neoplastic diseases. Screening for hepatitis B and C, liver cirrhosis, liver cancer, colorectal cancer, H. pylori infection for the primary prevention of gastric cancer, as well as metabolic dysfunction-associated steatotic liver disease (MASLD) were included in the program. By combining population-based screening with behavioral risk factor surveillance, CHICS has created a community-oriented platform supported by collaborations between local communities, healthcare providers, and governmental agencies to improve health outcomes at scale.
A key feature of CHICS is its advanced
registration and information system, linked to national health databases. This infrastructure enables organized screening through a call–recall mechanism, on-site outreach activities in accessible community locations, and structured follow-up care. Together, these features support individualized screening implementation and ensure continuity of care. The presentation highlights the program’s impact, detailing significant advancements in gastrointestinal cancer screening and HCV elimination.
The CHICS program has gradually integrated various screening programs tailored for multiple diseases into a unified framework and also extended to incorporate a series of health promotion programs to prevent the occurrence of diseases until so far. Importantly, recent advances highlight the growing need to address multi-system diseases such as cardio–kidney–metabolic (CKM) syndrome and MASLD, which demand multidisciplinary and holistic approaches. The CHICS program exemplifies this perspective by demonstrating a shift from a one-size-fits-all model of evidence-based medicine toward more nuanced, tailored strategies aligned with the principles of precision health. In doing so, it underscores the potential of county-wide, community-based initiatives to drive transformative change in preventive health services and offer transferable insights for other regions confronting similar challenges.
38th Annual Academic Meeting
Most Total Pancreatectomies for Ductal Adenocarcinoma Potentially Can Be Replaced by Whipple over the Splenic
Department of Surgery, National Taiwan University Hospital, Taipei, Taiwan
Department of Surgery, University of California San Diego, La Jolla, CA, USA
Pancreatic ductal adenocarcinoma (PDAC) invading both the gastroduodenal and splenic arteries has traditionally required total pancreatectomy (TP) to achieve oncological clearance (R0 resection). However, TP results in permanent insulin-dependent diabetes and diminished tolerance to subsequent treatments, which negatively impacts quality of life and clinical outcomes. The “Whipple Over the Splenic Artery” (WOTSA) procedure, developed by the NTUH pancreatic surgery team, is an innovative technique that extends the pancreatic transection line beyond the splenic artery, enabling preservation of the pancreatic tail and spleen.
This retrospective before-and-after cohort study analyzed 70 patients with PDAC between 2016 and 2022, comparing outcomes between those who underwent TP (n = 30) and WOTSA (n = 40).
The WOTSA procedure demonstrated a non-inferior R0 resection rate (100%) and comparable lymph node yield without increasing morbidity. Notably, WOTSA was associated with superior postoperative glycemic control (5% insulin dependence vs. 100% in
the TP group), a higher completion rate of adjuvant chemotherapy (73% vs. 47%), and improved median disease-free survival (14 vs. 7.5 months).
Clinical Contribution: This study challenges the traditional reliance on TP for complex PDAC, demonstrating that WOTSA can be safely and effectively applied in selected patients. By preserving pancreatic function, this approach improves postoperative quality of life and reduces the burden of lifelong metabolic management.
Innovation: WOTSA represents a hybrid approach that integrates the principles of anatomical oncologic clearance with organ preservation. It redefines the surgical boundaries in PDAC management, avoiding overtreatment while maintaining oncologic rigor.
Future Perspective: The promising results of WOTSA highlight the need for prospective multicenter trials to validate this technique. In the future, precision surgical strategies like WOTSA may become a standard of care in multidisciplinary PDAC management.
38th Annual Academic Meeting
Shang-Chin Huang
Department of Internal Medicine, National Taiwan University Hospital Bei-Hu Branch, Taipei, Taiwan
Background & aims: Steatotic liver disease (SLD) is prevalent among patients with chronic hepatitis B (CHB). However, the effects of metabolic dysfunction-associated SLD (MASLD) on the longterm survival of such patients remain unknown. Accordingly, this study investigated the mortality risks in patients with CHB and concurrent SLD.
Methods: Consecutive patients with CHB and concurrent SLD were retrospectively recruited at National Taiwan University Hospital. MASLD was defined by the presence of cardiometabolic risk factors. The cumulative incidences of all-cause and cause-specific mortality were compared.
Results: A total of 8,718 patients with CHB and concurrent SLD were included from 2006 to 2021.
At baseline, the MASLD group (n = 6,562) was older and had a lower proportion of HBeAg positivity and lower HBV DNA levels compared with the nonMASLD group (n = 2,156). After a median follow-up period of 9.1 years, the MASLD group exhibited a
higher risk of all-cause mortality compared with the non-MASLD group (adjusted hazard ratio 1.79, 95% CI 1.24–2.58, p = 0.002). Furthermore, cumulative cardiometabolic risk factors dose-dependently elevated the risks of all-cause, liver-related, and cardiovascular mortality (all p < 0.05). During the follow-up period, new-onset diabetes mellitus, hypertension, and significant weight gain further increased the risks of all-cause and liver-related mortality (all p < 0.05). However, patients with SLD had a lower mortality risk than those without SLD after propensity score matching (hazard ratio 0.62, 95% CI 0.53–0.74, p < 0.001).
Conclusions: Among patients with CHB and SLD, metabolic burden dose-dependently increases all-cause, liver-related, and cardiovascular mortality risks. Patients with SLD have a lower mortality risk than those without SLD. Identifying these metabolic dysfunctions is crucial for stratifying the level of risk in daily care.
38th Annual Academic Meeting
Ya-Chin Hou
Institute of Clinical Medicine, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Background and Aims
Oncogenic KRAS mutations are present in approximately 90% of pancreatic ductal adenocarcinoma (PDAC). However, Kras mutation alone is insufficient to transform precancerous cells into metastatic PDAC. This study investigates how KRAS-mutated epithelial cells acquire the capacity to escape senescence or even immune clearance, thereby progressing to advanced PDAC.
Methods
Single-cell RNA sequencing and analysis of primary PDAC tumors were conducted. Genetically engineered pancreas-specific Kras-mutated, dual specificity phosphatase-2 (Dusp2) knockout mouse models were established. Human and mouse primary pancreatic cancer cell lines were used for in vitro assessment of cancer characteristics. Tumor progression was studied via pancreas orthotopic and portal vein injection in the immune-competent mice. Clinical relevance was validated by digital spatial transcriptomic analysis of PDAC tumors.
Results
Kras mutation induces the formation of pancreatic intraepithelial neoplasia (PanIN), these
lesions also exhibit significant apoptotic signals. Single-cell RNA sequencing identified a subset of ERKactiveDUSP2low cells continuing to expand from early to advanced stage PDAC. In vitro and in vivo studies reveal that early infiltrating macrophagederived tissue inhibitor of metallopeptidase 1 (TIMP-1) is the key factor in maintaining the ERKactiveDUSP2low cell population in a CD63dependent manner. The ERKactiveDUSP2low cancer cells further exacerbate macrophage-mediated cancer malignancy, including loss of epithelial trait, increased lymphangiogenesis, and immune escape. Digital spatial profiling analysis of PDAC samples demonstrates the colocalization of TIMP1high macrophages and CD63high cancer cells. The presence of TIMP-1high macrophages and CD63high epithelial cells correlates with poor prognosis in PDAC.
Conclusions
Our study reveals the vicious cycle between early infiltrating macrophages and pancreatic cancer cells, providing a mechanistic insight into the dynamic regulation directing pancreatic cancer progression.
Department of Internal Medicine, National Taiwan University Hospital, College of Medicine, National Taiwan University, Taipei, Taiwan
The human microbiome is increasingly recognized as a source of biomarkers with direct implications for gastrointestinal, hepatic, metabolic, and systemic diseases. In colorectal cancer (CRC), Fusobacterium nucleatum is enriched in tumors and stool, linked to tumorigenesis, chemoresistance, and prognosis, while Peptostreptococcus anaerobius, Parvimonas micra, and enterotoxigenic Bacteroides fragilis contribute to oncogenic inflammation. Microbial panels integrating F. nucleatum with fecal immunochemical testing (FIT) or circulating DNA enhance early CRC detection. In inflammatory bowel disease (IBD), depletion of Faecalibacterium prausnitzii, expansion of adherent-invasive Escherichia coli, enrichment of Ruminococcus gnavus, and reduced diversity correlate with disease activity and therapeutic response.
In hepatocellular carcinoma (HCC) and chronic liver disease, overgrowth of Enterococcus faecalis
and Escherichia/Shigella, loss of butyrate producers (Roseburia, Lachnospiraceae), and secondary bile acid signatures associate with fibrosis progression and carcinogenesis. Metabolic disorders are characterized by reduced Akkermansia muciniphila, enrichment of Prevotella copri, altered Firmicutes/ Bacteroidetes ratios, and loss of short-chain fatty acid producers, linking the microbiome to obesity, insulin resistance, and diabetes. In systemic lupus erythematosus (SLE), enrichment of Ruminococcus gnavus and Bacteroides species, alongside depletion of Lachnospiraceae and Ruminococcaceae, reflects immune dysregulation.
Although promising, these biomarkers remain in discovery or validation stages. Standardized assays are needed before routine clinical adoption, but their integration with existing diagnostic tools offers strong potential for precision medicine.
Deng-Chyang Wu
Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
School of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
Fecal microbiota transplantation (FMT) has transitioned from an experimental intervention to an established therapy, particularly for recurrent Clostridioides difficile infection (CDI), where cure rates exceed 80–90%. This success has led to regulatory approval of standardized microbiotabased products, including RBX2660 (Rebyota) and SER-109 (VOWST). Beyond CDI, rapid advances in microbiome science have broadened the scope of FMT across multiple diseases.
1. Advances in Formulations: Fresh or frozen stool suspensions are being replaced by freeze-dried capsules (e.g., SER-109) and liquid preparations (e.g., RBX2660), offering improved safety, scalability, and patient acceptance.
2. Precision Microbiome Therapy: Integration of metagenomics, metabolomics, and artificial intelligence has enabled the identification of core microbial taxa or metabolites with immunomodulatory and metabolic functions, paving the way for synthetic consortia and targeted microbiome therapeutics.
3. Clinical Applications – Illustrative Examples:
– Ulcerative Colitis (UC): RCTs have shown that approximately 30% of UC patients achieved clinical and endoscopic remission within 8 weeks following FMT, with multi-
donor strategies yielding the best results.
– Hepatic Encephalopathy (HE): Pilot studies demonstrated that FMT reduces hyperammonemia, improves cognitive function, and lowers hospital readmission rates.
– Cancer Immunotherapy: In melanoma patients refractory to immune checkpoint inhibitors, FMT has restored treatment responsiveness in a subset of cases.
– Metabolic Disorders: Preliminary studies suggest that FMT may improve insulin resistance and metabolic profiles in obese individuals, although large-scale validation is still required.
4. Safety and Regulatory Considerations: While FMT demonstrates strong therapeutic promise, concerns remain regarding donor variability, transmission of infectious agents, and longterm safety.
Conclusion: FMT is undergoing a paradigm shift from “empirical medicine” to “precision microbiome medicine.” With standardized formulations, growing clinical evidence, and novel therapeutic indications, FMT is emerging as a cornerstone of microbiomebased healthcare.
Chun-Ying Wu
Institute of Biomedical Informatics,
National Yang Ming Chiao Tung University, Taipei, Taiwan
Division of Translational Research, Taipei Veterans General Hospital, Taipei, Taiwan
National Human Microbiota Core Facility, Taipei, Taiwan
This lecture presents the Asia–Pacific Microbiota Consortium’s consensus framework for developing and evaluating Live Biotherapeutic Products (LBPs) from bench to bedside. We begin by clarifying what LBPs are, and are not, within current regulatory landscapes (e.g., FDA guidance and EU Novel Food context), distinguishing them from “nextgeneration probiotics,” foods, and supplements. We then summarize the APMC consensus process and acceptance criteria, followed by the statement set organized across three development stages. Part A (Rationale) addresses sourcing and selecting candidate organisms, emphasizing diseasespecific mechanisms, quality, and traceability. Part B (Preclinical) details a rigorous laboratory pipeline: species/strain screening and identification, standardized genotyping and phenotyping, bioinformatics protocols, and pharmacology/ toxicology assessments, including vigilance for virulence and antimicrobial-resistance traits. Part C (Clinical Readiness) outlines requirements for strain
cell banking and genetic stability monitoring, dose optimization with pharmacodynamic readouts, formulation and delivery strategies, risk-managed clinical trial design, and post-marketing surveillance. Case-based examples illustrate how this framework applies to gastrointestinal, metabolic, and oncology indications, and how LBPs can be paired with biomarkers and multi-omics to refine targeting and monitoring. Throughout, we discuss statistical and AI tools for harmonizing heterogeneous microbiome data, mitigating bias, and planning robust external validation. The session concludes with a practical checklist for investigators and sponsors, covering documentation, manufacturing controls, safety governance, and efficacy endpoints, and a roadmap of research priorities (mechanismlinked endpoints, real-world evidence, and longterm safety registries). Participants will leave with a concise, end-to-end playbook to design, de-risk, and evaluate LBPs that meet scientific, regulatory, and clinical utility standards.
Cheng-Yen Kao
Institute of Microbiology and Immunology, National Yang Ming Chiao Tung University, Taipei, Taiwan
Advancements in microbiota research have greatly enhanced our understanding of how specific bacterial species/strains correlate with human health and disease. However, translating these associations into functional insights or therapeutic applications often reaches a critical bottleneck at the stage of bacterial cultivation. This challenge, central to the emerging field of culturomics, stems from our limited knowledge of the growth requirements of many novel and health-relevant microbes, as well as the strain-specific genomic and phenotypic traits that complicate their isolation. Strain-level validation is essential not only for confirming microbiota study findings, but also for developing next-generation
probiotics and live biotherapeutic products. To address these challenges, our team at National Yang Ming Chiao Tung University, supported by the National Science and Technology Council, has established a microbiota research platform dedicated to strain isolation and characterization. We have successfully isolated several promising strains from key genera such as Akkermansia, Faecalibacterium, and Bacteroides, and integrated whole-genome sequencing for downstream functional analyses. This presentation will focus on the role of culturomics in microbiota research, highlighting practical workflows and considerations in strain isolation, cultivation, and characterization.
Neurogastroenterology and Motility Symposium: Updates on Clinical Management
Sutep Gonlachanvit
Gastrointestinal Motility Ceneter, Bumrungrad International Hospital, Bangkok, Thailand
Chronic constipation is a prevalent condition encountered in clinical practice. According to the Rome IV criteria, chronic constipation is defined as the presence of symptoms for at least the past 3 months, with symptom onset at least 6 months prior to diagnosis. Diagnostic criteria require the presence of two or more of the following symptoms during more than 25% of defecations: straining, lumpy or hard stools (Bristol Stool Form Scale type 1 or 2), sensation of incomplete evacuation, sensation of anorectal obstruction, and manual maneuvers to facilitate defecation, in addition to fewer than three spontaneous bowel movements per week. Furthermore, loose stools should be rarely present without the use of laxatives, and the diagnostic criteria for irritable bowel syndrome (IBS) must not be fulfilled.
Pelvic floor dysfunction is a recognized consequence in patients with chronic constipation, often resulting from prolonged straining. This dysfunction may contribute to a range of complications, including gynecological and urological problems, as well as rectal intussusception and prolapse. A meta-analysis of defecography studies in patients with evacuation disorders revealed that high-grade rectal intussusception was present in 23.7% of cases, highlighting the common occurrence of anorectal anatomical abnormalities in this patient population. Despite this, most clinical guidelines for the management of chronic constipation do not adequately address pelvic floor abnormalities.
Management strategies for chronic constipation vary across regions, influenced by differences in colorectal cancer prevalence,
availability of pharmacological therapies, and access to specialized diagnostic testing. Standard clinical practice involves the exclusion of secondary causes, followed by lifestyle and dietary modifications, fiber supplementation, and the use of simple or osmotic laxatives. Referral to a gastroenterologist is recommended for patients who are unresponsive to first-line therapies. In such cases, anorectal physiologic evaluation, including anorectal manometry, should be performed to assess for functional disorders such as dyssynergic defecation.
In patients without anorectal dysfunction, or following successful biofeedback therapy for anorectal dysfunction, colonic transit studies are indicated to assess for slow-transit constipation. New pharmacologic agents, effective for both chronic idiopathic constipation and IBS-C, are recommended when patients fail to respond to conventional laxatives. Surgical interventions, such as total colectomy, should be reserved for carefully selected cases and only after thorough preoperative evaluation.
Most clinical guidelines primarily aim to improve constipation symptoms, particularly by increasing spontaneous bowel movements. However, as previously discussed, pelvic floor damage is a significant and often underrecognized consequence of chronic constipation. Inadequate management may contribute to progression of this damage, especially due to chronic straining, which can lead to pelvic organ prolapse. Notably, a recent Japanese guideline highlighted straining as a target symptom, although it did not emphasize its role in the prevention of pelvic floor injury.
In conclusion, the management of chronic
constipation should adopt a comprehensive approach that includes: identification and treatment of secondary causes, implementation of lifestyle and dietary interventions, use of laxatives and newer pharmacologic agents, performance of anorectal and colonic physiologic tests, and evaluation for pelvic floor abnormalities using defecography. Anorectal manometry should be employed in patients unresponsive to first-line
treatments to detect dyssynergic defecation, a treatable condition through biofeedback therapy. Additionally, assessment of pelvic floor damage should be considered in patients with defecatory disorders, and efforts should be made to prevent excessive straining through appropriate therapeutic interventions. Future research should focus on strategies to prevent pelvic floor damage in patients with chronic constipation.
Neurogastroenterology and Motility Symposium: Updates on Clinical Management
Division of Gastroenterology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
The 2025 San Diego Consensus introduced refined definitions for laryngopharyngeal reflux (LPR). Laryngopharyngeal symptoms (LPS) are aerodigestive manifestations potentially induced by gastric reflux, such as cough, voice changes, throat clearing, phlegm, and throat pain. Laryngopharyngeal reflux disease (LPRD) requires both LPS and objective reflux evidence, underscoring that symptoms alone are insufficient. In contrast, the 2024 Dubai Definition emphasized LPR as a disease of the upper aerodigestive tract caused by direct and/or indirect effects of gastric or duodenal reflux, leading to morphological and/or neurological changes.
Pathophysiology
The Dubai Consensus highlighted that upper esophageal sphincter dysfunction and refluxrelated symptoms may differ from gastroesophageal reflux disease (GERD). Patients with combined LPR and typical GERD symptoms show more frequent pharyngeal reflux, suggesting distinct subtypes with different mechanisms. The San Diego Consensus stressed that esophageal hypervigilance and symptom-specific anxiety are critical drivers of symptom severity, potentially outweighing reflux burden, and should be considered therapeutic targets.
The Dubai Consensus proposed hypopharyngeal multichannel intraluminal impedance–pH (HMIIpH) monitoring, with more than one pharyngeal
reflux event in 24 hours deemed abnormal. The ACG guidelines and Lyon Consensus 2.0 recommend HMII-pH testing for suspected isolated LPS before initiating PPIs and suggest incorporating MNBI as a supportive parameter. The San Diego Consensus aligned LPRD diagnostics with GERD criteria (endoscopy, MII-pH, wireless pH monitoring), with wireless pH monitoring particularly useful in patients with esophageal symptoms or when escalating therapy.
The Dubai Consensus recommended a threemonth empirical therapy trial (acid, weak acid, non-acid) when HMII-pH is unavailable, tailoring drug regimens to reflux patterns. The San Diego Consensus advised that patients with concomitant GERD symptoms begin with standard-dose PPI plus alginates and lifestyle measures for three months, with objective testing required if symptoms persist. For isolated LPS, empirical PPI therapy is not recommended. Instead, management should target psychological and sensory contributors, such as laryngeal recalibration therapy (LRT), speech therapy, CBT, and neuromodulators, with reflux testing reserved for refractory cases.
Together, these advances highlight a paradigm shift toward more precise, mechanism-based, and personalized approaches in diagnosing and treating LPR.
Neurogastroenterology and Motility Symposium: Updates on Clinical Management
Ping-Huei Tseng
Endoscopic Division, Department of Integrated Diagnostic & Therapeutics, National Taiwan University Hospital, Taipei, Taiwan
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
The prevalence of gastroesophageal reflux disease (GERD) is increasing rapidly in Taiwan and worldwide as a result of epidemic obesity and metabolic syndrome. Proton pump inhibitor (PPI) remains the mainstay in GERD treatment. However, refractory symptoms are noted in up to 40% of patients despite PPI treatment at standard doses. The underlying pathophysiology involved in refractory GERD or PPI failure is complex. These patients have common psychological characteristics such as anxiety and depression, which may contribute to their hypersensitive perception of trivial luminal stimuli. Actually, the brain-gut axis plays a significant role in mediating esophageal symptoms. Luminal and mucosal injury in the gut can sensitize visceral afferents, leading to allodynia or hyperalgesia. Psychological and cognitive factors, such as hypervigilance, also contribute to
heightened pain perception. Both centrally and peripherally directed treatments can be beneficial in managing these symptoms. Patients with GERD may have concomitant functional gastrointestinal disorders, now known as disorders of gut-brain interaction (DGBI), such as functional dyspepsia and irritable bowel syndrome (IBS), which share some similar clinical characteristics, including female predominance, middle age, and psychological disorders such as depression and anxiety. Increasing studies suggested GERD patients with symptoms refractory to PPIs might have overlapping DGBI. In this speech, we will discuss about the impact of DGBI on the treatment responses of patients with GERD and the importance of a personalized treatment based on a comprehensive evaluation for GERD patients with overlap DGBI.
Neurogastroenterology and Motility Symposium: Updates on Clinical Management
Ming-Wun Wong
Division of Gastroenterology, Department of Medicine, Hualien Tzu Chi Hospital, Hualien, Taiwan
This presentation addresses the evolving understanding and management of belching disorders, particularly supragastric belching (SGB), within the context of gastroesophageal reflux disease (GERD) and disorders of gut-brain interaction (DGBI). Excessive SGB is increasingly recognized as a behavioral phenomenon contributing to PPIrefractory GERD, with marked regional variation in prevalence—reported at 18.5% in Japan and 36.1% in the UK.
A major challenge in managing SGB lies in its diagnosis via 24-hour impedance-pH monitoring, which currently requires time-intensive manual interpretation. Emerging research from the United States and Taiwan supports the development of AIassisted interpretation tools, mirroring advances in the automated detection of reflux episodes. This innovation holds promise for streamlining diagnosis and improving clinical decision-making.
Therapeutic strategies are grounded in patientcentered care. For gastric belching, behavioral
modifications such as slow eating and avoidance of carbonated beverages are recommended. In contrast, supragastric belching benefits from cognitive behavioral therapy (CBT) and speech therapy, particularly diaphragmatic breathing techniques and retraining of abnormal swallowing–respiration patterns. Local data show that up to 75%–83% of SGB patients respond positively to speech therapy alone.
Finally, SGB shows substantial overlap with DGBI phenotypes, including functional dyspepsia, IBS, and globus sensation. Studies indicate that diaphragmatic breathing not only alleviates belching but also improves symptoms across these related disorders, supporting a unified, multidisciplinary treatment model.
By integrating advanced diagnostic approaches, behavioral therapies, and personalized treatment planning, this framework aims to redefine precision care for patients with belching-related disorders.
Wei-Chih Liao
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
Artificial intelligence (AI) is rapidly transforming diagnostics and risk prediction across medicine, particularly in gastrointestinal (GI) disorders. Research shows AI models can match or exceed expert performance in early detection, characterization, and risk stratification.
In colorectal cancer, AI improves adenoma detection and reduces miss rates using endoscopic imaging. In inflammatory bowel disease (IBD), AI automates endoscopic scoring, predicts flares, and guides individualized treatment decisions. For liver disease, noninvasive tools enable fibrosis staging and prediction of hepatocellular carcinoma recurrence through multimodal data integration.
AI also predicts complications, recurrence, and survival in GI malignancies, optimizing treatment allocation in IBD and chronic GI conditions. Deep learning and radiomics demonstrate high accuracy in detecting pancreatic ductal adenocarcinoma (PDAC), distinguishing benign from malignant
lesions, and forecasting outcomes using CT, MRI, and ultrasound. Convolutional and transformerbased models further enhance lesion segmentation, classification, and automated characterization. In pancreatic cystic lesions, AI surpasses conventional clinical and imaging criteria for risk stratification and malignant transformation prediction. Integration of clinical, genetic, and biomarker data enables individualized PDAC risk assessment. Beyond cancer, AI supports noninvasive screening, workflow optimization, and decision-making in pancreatitis and neuroendocrine tumors.
In summary, AI-driven diagnostics and risk prediction hold great promise for precision medicine in GI disorders, offering enhanced accuracy, efficiency, and personalized care. However, robust external validation, prospective trials, and mitigation of bias are essential. Ethical concerns, interpretability, and equitable deployment must also be addressed before widespread adoption.
Amrita Chattopadhyay
Institute of Epidemiology and Preventive Medicine, National Taiwan University, Taipei, Taiwan
Generative Artificial Intelligence (AI) is rapidly emerging as a powerful tool in the diagnosis, prognosis, and management of gastrointestinal (GI) diseases. This talk introduces generative AI models, such as GANs and large language models, in transforming complex imaging and sequencing data into actionable clinical insights. Generative models can simulate high-fidelity endoscopic and histopathologic images, enhancing lesion detection and reducing diagnostic variability. These tools also support clinician training by providing diverse, synthetic visual examples of rare or subtle pathologies. On the sequencing front, generative AI enables deeper analysis of genomic data by
generating realistic patient profiles and predicting disease trajectories. This is particularly valuable in complex disorders like inflammatory bowel disease (IBD) and colorectal cancer, where personalized treatment decisions can benefit from integrating multi-omics data. This presentation will highlight real-world examples of generative AI improving clinical workflows, from automated report generation to synthetic datasets used in model training, while also addressing challenges around validation, ethics, and patient safety, towards a clear understanding of how generative AI can support decision-making, and ultimately enhance care delivery in gastroenterology.
Chun-Ying Wu
Institute of Biomedical Informatics,
National Yang Ming Chiao Tung University, Taipei, Taiwan
Division of Translational Research, Taipei Veterans General Hospital, Taipei, Taiwan
National Human Microbiota Core Facility, Taipei, Taiwan
This lecture surveys how artificial intelligence (AI) reshapes biomedical research and clinical decisionmaking through multi-modal data integration while candidly addressing the limits of both traditional statistics and AI. We begin by clarifying where classical statistical analysis struggles in modern healthcare datasets: stringent model assumptions, the coexistence of structured and unstructured data, high dimensionality, streaming scale from wearables and sensors, and manual feature engineering that can miss interactions or redundancies. We then introduce the core AI paradigms: supervised, unsupervised, and reinforcement learning, mapping each to healthcare use cases: risk stratification and prognosis prediction; patient clustering, cohort discovery, and anomaly detection; and policy optimization for treatment pathways and resource allocation. Building on this foundation, the lecture details how multi-modal learning connects signals across EHR tables, radiology and pathology images, free-text reports, ‘omics profiles, environmental exposures, and continuous sensor data to produce more robust, context-aware models. Participants will see practical patterns for feature and model
selection automation, scalable training on large, evolving datasets, and deployment considerations for latency, throughput, and monitoring.
A dedicated segment contrasts discriminative and generative AI for clinical applications. Discriminative approaches excel at classification and regression tasks that require calibrated probabilities and clear decision boundaries, whereas generative approaches unlock data synthesis, imputation, augmentation, and cross-modal reasoning. We discuss when to prefer one over the other and when hybrid workflows outperform either alone, such as using generative models to curate labels or harmonize heterogeneous inputs before discriminative modeling. Finally, we address the AI’s own limitations and risks. Topics include label noise and dataset shift, spurious correlations and overfitting in high-dimensional regimes, opacity and explainability gaps, fairness and representation bias, reproducibility and governance, cost and carbon considerations, and clinical integration. The session closes with pragmatic take-home points on building translatable AI solutions.
Joseph Sung
Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore
AI is already enabling more personalized therapies for digestive (gastrointestinal) diseases, and its role is expected to grow. By integrating data from genomics, imaging, endoscopy, pathology, electronic health records (EHR), and even microbiome profiles, AI can help tailor treatment strategies to each patient’s unique biology and clinical context. Below is a structured overview with key areas and concrete examples.
1. Personalized Therapy in Inflammatory Bowel Disease (IBD) IBD (Crohn’s disease and ulcerative colitis) is a major area where AI is moving toward precision medicine.
2. Colorectal Cancer (CRC) and Other GI Cancers
AI can identify molecular subtypes and predict drug sensitivity, allowing tailored therapies.
3. Liver Diseases (Hepatitis, NASH, Cirrhosis)
Personalized therapy is crucial in chronic liver disease and hepatocellular carcinoma (HCC).
Fibrosis staging and treatment for MSALD, HCC treatment decision support are clear examples.
4. Functional GI Disorders (IBS, Dyspepsia) These conditions lack clear biomarkers, making personalization challenging — but AI is beginning to help.
5. AI-Driven Clinical Trial Matching AI can rapidly screen molecular profiles and EHR data to match GI patients to precision-therapy clinical trials.
AI can and already does enable personalized therapy for digestive diseases, from predicting drug response in IBD to selecting targeted therapy in colorectal and liver cancer. Integration of multimodal data (genomics, pathology, imaging, microbiome, lifestyle) is the cornerstone of this personalization. Challenges remain in data quality, regulatory approval, explainability, and ensuring equity, but the trajectory is strongly toward AIdriven precision gastroenterology.
Chia-Yen Dai
Division of Hepatology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
Metabolically-dysfunctional-associated steatotic liver disease (MASLD) has become the most common chronic liver disease globally, mirroring the alarming rise of obesity. Obesity is defined as a chronic, multifactorial disease characterized by abnormal or excessive fat accumulation that impairs health, increases the risk of long-term complications, and reduces life expectancy. Traditional reliance on body mass index (BMI) inadequately reflects disease heterogeneity, as individuals with identical BMI values may have vastly different metabolic and inflammatory profiles. The concept of metabolically healthy obesity highlights subgroups with lower visceral fat, better insulin sensitivity, higher cardiorespiratory fitness, and reduced inflammatory burden, although most obese individuals eventually develop metabolic complications.
Epidemiologic data show that MASLD affects approximately 30% of the global adult population, with prevalence exceeding 40% in Latin America and the Middle East. MASH (metabolic dysfunction–associated steatohepatitis), the progressive form, occurs in roughly 5% of the population and is strongly enriched among patients with obesity, diabetes, dyslipidemia, and hypertension. Among obese individuals, MASH prevalence ranges from 35–96%, highlighting the tight coupling between
adiposity and advanced liver disease. The rising prevalence in younger populations and children with obesity raises concerns about early-onset cirrhosis and hepatocellular carcinoma (HCC).
Clinical management requires a comprehensive approach beyond weight loss alone. Lifestyle interventions combining calorie restriction, exercise, and behavioral modification remain the foundation, with weight reduction of ≥7–10% associated with significant histological improvement. Pharmacologic therapies such as GLP-1 receptor agonists and THR-β agonists show promise, producing steatohepatitis resolution and fibrosis regression in clinical trials while achieving substantial weight loss. Bariatric surgery remains the most effective option for selected patients with morbid obesity, leading to sustained MASLD remission and reduced HCC risk.
In summary, obesity should be regarded as a systemic disease requiring early detection and targeted intervention. MASLD, as its hepatic phenotype, offers a window of opportunity for integrated cardiometabolic risk reduction. Preventive strategies at the population and policy levels will be essential to mitigate the long-term health and economic burdens associated with this intertwined disease spectrum.
Multifaceted Association of MASLD and Obesity
Chia-Chi Wang
Department of Gastroenterology, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei, Taiwan School of Medicine, Tzu Chi University, Hualien, Taiwan
Metabolic dysfunction-associated steatotic liver disease (MASLD), the hepatic manifestation of obesity and metabolic syndrome, progresses through a cascade of obesity-driven pathogenic mechanisms. Central to this process are visceral adiposity and insulin resistance, which increase free fatty acid flux to the liver and promote de novo lipogenesis and impaired very-low-density lipoprotein (VLDL) export resulting in hepatic steatosis. Lipotoxicity triggers endoplasmic reticulum stress, oxidative damage, mitochondrial dysfunction, and inflammation, advancing MASLD
to metabolic dysfunction-associated steatohepatitis (MASH). Obesity exacerbates fibrosis via Kupffer cell activation and hepatic stellate cell proliferation through the adipokines such as TNF-α and IL6, while gut dysbiosis further amplifies inflammation. The clinical implications section emphasizes that obesity exacerbates MASLD-related risks, including cardiovascular disease (CVD), type 2 diabetes mellitus (T2DM), and HCC. Finally, it reviews the use of non-invasive diagnostic tools such as FIB-4 and elastography for risk stratification of MASLD.
Ming-Ling Chang
Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital at Linkou, Taoyuan, Taiwan Department of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan
Patients with obesity are at increased risk of metabolic dysfunction-associated steatotic liver disease (MASLD), which is a disease that involves both the liver and adipose tissues. The disease progression is not only facilitated by biochemical signals, but also by mechanical cues such as the increase in stiffness often seen with fibrotic fatty livers. The change in stiffness and accumulation of excess lipid droplets impact the ability of a cell to mechanosense and mechanotranduce, which perpetuates the disease. Moreover, a diet characterized by excessive intake of energy, carbohydrates, fructose, or ultraprocessed foods leads to the formation of MASLD and abdominal obesity by enhancing pathways such as de novo lipid synthesis in the liver, insulin resistance, gut-liver dysfunction, and inflammation. Free fatty acids may mediate excessive lipid deposition and hepatocellular damage through the action of hormones. These pathways to liver damage exacerbate MASLD and progression to metabolic dysfunction-associated steatohepatitis (MASH) and fibrosis. Specifically, macrophages play crucial roles
in immune response and tissue homeostasis, with their functions becoming increasingly complex in obesity-mediated metabolic disorders. In the context of obesity, macrophages respond adaptively to lipid overloads and inflammatory cues in adipose tissue, profoundly influencing insulin resistance and metabolic homeostasis. Finally, the procedures such as lifestyle intervention and bariatric surgery and the drugs acting via weight loss (incretin (co)agonists, sodium-glucose co-transporter 2 inhibitors) potentially treat obesity and MASLD simultaneously, while with the drugs exerting no weight loss (pioglitazone; resmetirom) mainly target MASLD. Whether the former effects better than the latter remains elusive. Taken together, the multifaceted association of MASLD and obesity, will be comprehensively reviewed from the perspectives of the hepatocyte and adipocyte mechanobiology, diet-associated metabolic alterations, macrophagefocusing immunology and the treatments with or without cutting weight.
Seung
Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea
Metabolic dysfunction–associated steatotic liver disease (MASLD) has become the leading cause of chronic liver disease worldwide, paralleling the global epidemic of obesity and type 2 diabetes mellitus (T2DM). The close interplay among hepatic steatosis, insulin resistance, and adipose tissue dysfunction highlights the urgent need for therapies that target both hepatic and systemic metabolic pathways. In this context, incretin-based therapies— particularly glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and the newer dual agonists— have emerged as promising options for managing MASLD in obese and metabolically compromised patients.
Incretin hormones, mainly GLP-1 and glucose-dependent insulinotropic polypeptide (GIP), regulate glucose homeostasis, satiety, and energy expenditure. Pharmacologic GLP-1 RAs have demonstrated significant benefits in weight reduction, glycemic control, and cardiovascular risk mitigation in large clinical trials. More recently, their potential to improve liver histology has attracted substantial attention. Studies such as the LEAN trial and subsequent phase 2b and phase 3 investigations have shown that GLP-1 RAs can achieve NASH resolution in a considerable proportion of patients, often surpassing the efficacy of prior investigational agents. Importantly, reductions in body weight, visceral adiposity, and systemic inflammation appear to mediate much of the hepatic benefit, highlighting the dual utility of incretin therapy in obesity and MASLD.
The recent introduction of dual agonists (GLP1/GIP co-agonists, such as tirzepatide) and triple agonists (GLP-1/GIP/glucagon receptor agonists) has further expanded the therapeutic horizon.
These agents have shown unprecedented weight loss efficacy, often exceeding 20% reduction in body weight, and preliminary evidence suggests favorable effects on hepatic steatosis and fibrosis markers. Given the strong link between weight loss and histological improvement in MASLD, incretinbased therapies may soon represent the backbone of pharmacologic intervention in this population. However, several challenges remain before broad incorporation into MASLD management can be realized. First, MASLD patients are heterogeneous; not all derive equal benefit from weight loss–centered approaches, and residual fibrotic risk may persist even after metabolic improvement. Second, the high cost of incretin therapies poses barriers to long-term adherence, particularly in healthcare systems without reimbursement policies. Third, adverse events such as gastrointestinal intolerance, gallbladder disease, or rare pancreatobiliary complications require careful monitoring. Finally, questions remain regarding optimal treatment duration, durability of hepatic benefits after drug discontinuation, and whether combination strategies with other antifibrotic agents may achieve greater long-term efficacy.
Despite these limitations, incretin therapies represent a paradigm shift for both obesity and MASLD. Unlike most prior drug candidates, they address the root causes of disease— obesity, insulin resistance, and cardiometabolic dysfunction—while simultaneously improving hepatic endpoints. Incorporating these agents into MASLD treatment pathways will require careful patient selection, structured monitoring of NITs and metabolic outcomes, and integration with lifestyle interventions. Future research should also clarify
whether early initiation can prevent progression to cirrhosis and hepatocellular carcinoma, and whether dynamic improvement in non-invasive fibrosis markers during incretin therapy translates into reduced hard clinical outcomes.
This lecture will summarize the current evidence on incretin-based therapies for obesity and MASLD, review key trial data and mechanistic insights, and discuss how these agents may be incorporated into
routine hepatology practice. I will also highlight unmet needs, cost-effectiveness considerations, and the potential for combination regimens that target both fibrotic and metabolic burden. Ultimately, incretin-based strategies hold the promise of transforming the management of MASLD by simultaneously addressing hepatic, metabolic, and cardiovascular outcomes.
Masayuki Saruta
Division of Gastroenterology and Hepatology, Department of Internal Medicine, The Jikei University School of Medicine, Tokyo, Japan
Bowel urgency is one of the most distressing and disruptive symptoms experienced by patients with ulcerative colitis (UC). Although often underrecognized in clinical trials and routine practice, bowel urgency profoundly impacts patients’ quality of life, daily functioning, and emotional well-being. Emerging data from clinical trials and real-world studies suggest that certain advanced therapies—particularly biologics and small molecules—can significantly reduce bowel urgency when used with a treat-to-target approach. In addition, novel endpoints such as “bowel urgency remission” are being proposed in clinical research, further validating its importance as a therapeutic
goal.
I will focus on the integration of bowel urgency assessment into routine care, including the use of patient-reported outcomes (PROs) and symptom-based monitoring tools. By recognizing and addressing bowel urgency proactively, clinicians can help patients transition from flare to freedom—achieving not just clinical remission, but a meaningful recovery in quality of life.
This lecture explores the pathophysiology, clinical relevance, and management strategies for bowel urgency in UC, aiming to shift the focus from disease control to true patient-centered remission.
in IBD:
Chen-Wang Chang
Division of Gastroenterology, Department of Internal Medicine, MacKay Memorial Hospital, Taipei, Taiwan
Inflammatory Bowel Disease (IBD), including Crohn’s disease and ulcerative colitis, is increasingly diagnosed in individuals over 60. Elderly-onset IBD accounts for 10–15% of new cases, with ulcerative colitis being more common. Though often presenting with milder disease activity, elderly patients face unique challenges due to comorbidities, frailty, and age-related immune changes.
A. Diagnostic Challenges
IBD symptoms in older adults may mimic other conditions such as diverticulitis or ischemic colitis, often leading to diagnostic delays. Endoscopic evaluation may be limited by concerns about procedural risk and sedation tolerance.
B. Treatment Considerations
Management requires careful selection of therapies to minimize side effects:
1. 5-ASA agents are generally safe for mild UC.
2. Steroids increase the risk of osteoporosis, diabetes, and infections.
3. Immunomodulators and biologics must be used cautiously due to higher infection and malignancy risks.
4. JAK inhibitors should be reserved for select cases due to cardiovascular and thrombotic concerns.
Polypharmacy is common in older adults, increasing the risk of drug interactions.
C. Surgical and Nutritional Aspects
1. Surgery carries higher risk in the elderly; minimally invasive approaches are preferred.
2. Nutritional assessment is critical, as malnutrition and sarcopenia are prevalent.
D. Psychosocial and Functional Issues
Depression, isolation, and frailty impact quality of life and treatment outcomes. Comprehensive geriatric assessment and caregiver support are essential.
Conclusion
Elderly-onset IBD requires an individualized, multidisciplinary approach that balances efficacy and safety. Early recognition, appropriate therapy, and holistic care can improve outcomes in this growing patient population.
Chia-Jung Kuo
Division of Gastroenterology, Department of Internal Medicine, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
Historically, patients with inflammatory bowel disease (IBD) have been associated with leaner body types, as weight loss and malnutrition were hallmark features of the disease. However, the prevalence of obesity in IBD patients has been increasing. Recent trends show that 15%–40% of IBD patients are now obese, making weight a central component in comprehensive disease management.
Obesity is linked with autoimmunity, elevating the risk of developing inflammatory diseases. The pro-inflammatory cytokines and adipokines secreted by adipose tissue are known to influence immune responses, potentially exacerbating disease activity, outcomes, and treatment efficacy in autoimmune
diseases, including IBD.
Studies have suggested that obesity influences the clinical course and management of IBD, potentially impacting disease activity, outcomes, and treatment responses. Obesity can negatively affect the efficacy of advanced therapies, including biologics, possibly due to altered drug pharmacokinetics and increased inflammatory burden. Some studies suggest increased risk of poor response and adverse outcomes with obesity in IBD.
A multidisciplinary, stepwise approach is recommended for the management of obesity in individuals with IBD.
Hepatic Disease Center, Chuang Shan Medical University Hospital, Taichung, Taiwan
Pregnancy can be a complex and risk-filled event for women with inflammatory bowel disease (IBD), the management of pregnancy in IBD, practical recommendations are provided to transform the care of women with IBD worldwide. The global consensus on pregnancy in inflammatory bowel disease (IBD) was recently established by the PIANO Expert Global Consensus, published in August 2025. This consensus provides standardized, evidencebased guidelines for managing pregnancy in women with IBD to improve maternal and neonatal outcomes.
Very Early-Onset Inflammatory Bowel Disease (VEO-IBD) is a subtype of inflammatory bowel disease that manifests before the age of six. Genetic analysis shows that many cases of VEO-IBD are associated with monogenic defects, where rare gene variants affect immune regulation, intestinal epithelial
barrier function, and inflammatory pathways. Early identification of these genetic abnormalities is possible through whole-exome sequencing and whole-genome typing. Furthermore, a multidisciplinary management approach that integrates drug therapy, nutritional support, and psychosocial interventions is evolving to improve the quality of life for affected children.
Managing Very Early-Onset Inflammatory Bowel Disease (VEO-IBD) requires a specialized, often multidisciplinary approach, focusing on both medical and nutritional therapies. Treatment plans are individualized, as some children may not respond to standard IBD therapies, personalized treatment plans based on the patient’s specific genetic background. Some patients with genetic defects may be cured through allogeneic hematopoietic stem cell transplantation.
Ken Shirabe
Division of Hepatobiliary and Pancreatic Surgery, Department of General Surgical Science, Gunma University, Gunma, Japan
Background: PHLF is sometimes fatal. Functional future remnant liver volume (fFRLV) using EOB-MRI and 3D CT could reflect liver function of remnant liver. Hepatic vein embolization (HVE) added to portal vein embolization (PVE), is reported to stimulate liver regeneration.
Methods and Results: Based on the intensity of the future remnant liver parenchyma measured 20 minutes after EOB-MRI and the postoperative remnant liver volume, we calculated the functional future remnant liver volume (fFRLV) and established our criteria. The most notable finding was that no patients developed PHLF when the fFRLV exceeded our criteria. If the fFRLV exceeded our criteria, hepatectomy, usually right lobectomy was performed. It fell below our criteria, PVE was undertaken. Following PVE, fFRLV was recalculated. Since fFRLV assessed by EOB-MRI reflects segmental hepatic function, this method remained valid even
after PVE.
When the recalculated fFRLV after PVE exceeded our criteria, hepatic resection was carried out as planned. If it remained below our critera, HVE as added, and fFRLV was re-evaluated accordingly.
As a result, PVE was performed in 43 patients whose initial fFRLV was below our criteria. Among them, 29 patients (67.4%) underwent hepatectomy after PVE. Of the 12 patients whose post-PVE, fFRLV still remained below our criteria, 9 achieved a sufficient increase in fFRLV after HVE. Ultimately, hepatectomy was performed in 38 out of 43 patients (resection rate: 88.4%), and none of the patients who underwent hepatectomy developed PHLF.
Conclusion: Our strategy, fFRLV is useful as main axis of indication and makes sequential usage of PVE and HVE, secured the resection rate and was useful for preventing PHLF.
Yan-Shen Shan
Division of General Surgery, Department of Surgery, National Cheng Kung University Hospital, Tainan, Taiwan
Institute of Clinical Medicine, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Pancreatic cancer is a formidable disease with one digital 5-year survival until now. Surgery with postoperative adjuvant therapy is the only curative treatment for resectable disease. However, its median overall survival is around 25%. Though there are several combinational regimens, including mFolfirinox, Gem/Nab-P, and Onivyde with 5-Fu, showing modest benefit in survival for metastatic pancreatic cancer.
Precision medicine has proposed in recent years, and it did show great improvement in those patients who can be treated by druggable target therapy or immunotherapy after receiving genetic
study. Therefore, application of precision medicine may improve survival of pancreatic cancer patients. In NCKUH, from 2020, new pancreatic cancer patients will be divided into four groups of patients based on the image findings (figure 1). Then, patients will sign informed consent for next generation sequence and WES study. Those patients will receive treatment based on our algorithm and clinical studies. Under this precision medicine project, the survival of pancreatic cancer patients in NCKUH was much improved. I will present our achievements to our society and colleagues.
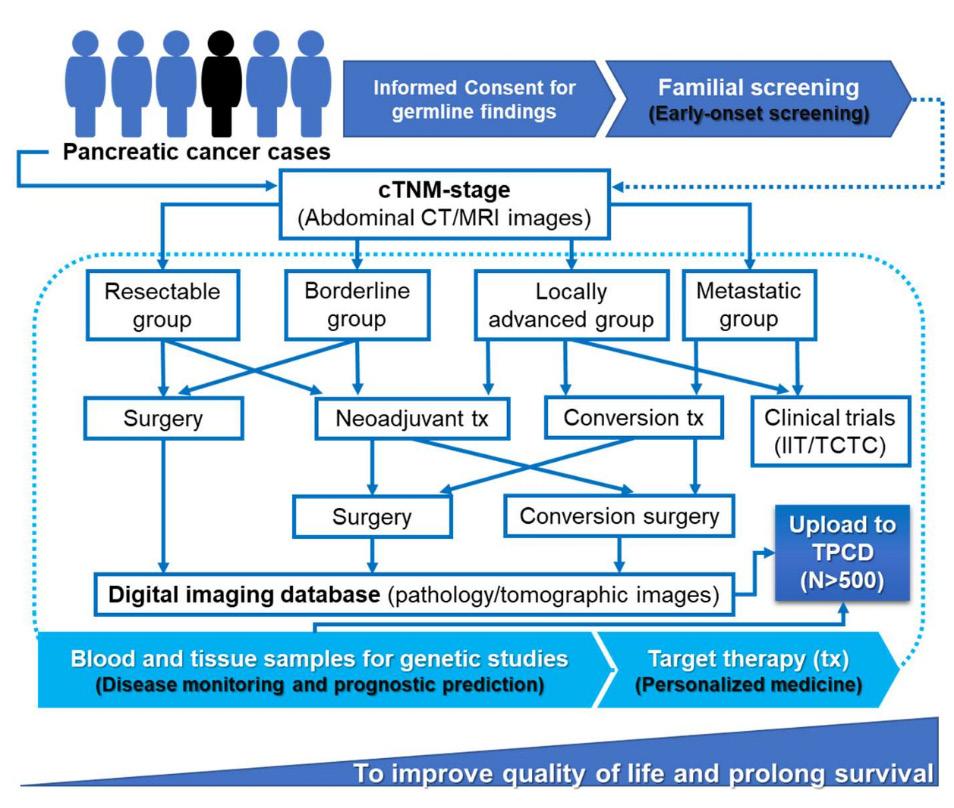
Jaw-Yuan Wang
Department of Surgery, Kaohsiung Medical University Chung-Ho Memorial Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
Colorectal cancer (CRC) continues to be a major global health burden, particularly in its metastatic form (mCRC), where molecular heterogeneity drives variable outcomes and treatment responses. Recent progress in precision oncology has emphasized the role of biomarker-guided therapy, leveraging genomic profiling to refine therapeutic strategies. This presentation provides an updated overview of advances in molecularly targeted therapies, immunotherapy, and surgical innovations in CRC management.
Actionable genomic alterations—including KRAS, NRAS, BRAF, HER2, MSI-H/dMMR, KRAS G12C, and NTRK fusions—have enabled more personalized approaches. BRAF V600E mutations remain a marker of poor prognosis, yet novel regimens such as encorafenib plus cetuximab with chemotherapy (BREAKWATER trial) are improving survival outcomes. Immunotherapy has reshaped treatment of MSI-H/ dMMR CRC, with durable benefit demonstrated in KEYNOTE-177 and CheckMate-8HW. For HER2positive, RAS wild-type CRC, novel antibody-drug conjugates and combinations (e.g., trastuzumab deruxtecan, tucatinib with trastuzumab) are establishing new standards. Meanwhile, KRAS G12C inhibitors (sotorasib, divarasib) in combination with EGFR antibodies offer promising results. In addition,
circulating tumor DNA (ctDNA) is emerging as a critical biomarker for minimal residual disease detection and recurrence risk stratification, guiding escalation or de-escalation of therapy.
Complementing systemic therapy, Robotic Assisted Surgery (RAS) has become an integral component of CRC management. In Taiwan, nationwide adoption of da Vinci systems has demonstrated superior outcomes in rectal resection, including reduced conversion rates, lower anastomotic leakage, and improved organ preservation. Multi-institutional evidence shows that robotic platforms not only expand surgical feasibility in anatomically complex cases but also support quality assurance, structured training, and equitable reimbursement through the National Health Insurance system. Future directions highlight integration of artificial intelligence, enhanced imaging, and next-generation robotic platforms to further elevate surgical precision and patient outcomes.
In summary, the convergence of precision oncology and robotic innovation underscores a new era in CRC management, enabling tailored strategies across both systemic and surgical domains to optimize survival and quality of care.
Wen-Chi Chou
Biliary tract cancers (BTCs), including cholangiocarcinoma, gallbladder cancer, and ampullary carcinoma, are aggressive malignancies with poor prognosis. Most patients present with advanced or unresectable disease, where systemic therapy remains the cornerstone of management.
The therapeutic journey of BTC has progressed significantly over the past three decades. Early studies established chemotherapy as superior to best supportive care, with gemcitabine plus cisplatin (GemCis) confirmed as the first-line standard by the pivotal ABC-02 trial, extending survival to 11.7 months. Alternative regimens, such as gemcitabine with S-1, have provided region-specific options. For second-line therapy, the ABC-06 trial established FOLFOX as a standard, with additional data supporting nanoliposomal irinotecan plus 5FU in selected populations.
A major breakthrough emerged with immunotherapy. The phase III TOPAZ-1 trial demonstrated that adding durvalumab to
GemCis improved overall survival to 12.9 months, establishing chemo-immunotherapy as a new global standard. KEYNOTE-966 confirmed pembrolizumab as another effective partner for GemCis, further supporting checkpoint inhibitor integration.
Concurrently, molecular profiling has ushered BTC into the era of precision oncology. Actionable alterations—including FGFR2 fusions, IDH1 mutations, HER2 amplification, BRAF mutations, NTRK and RET fusions, and MSI-H/dMMR—have led to multiple targeted therapies showing meaningful benefit, including pemigatinib, futibatinib, ivosidenib, zanidatamab, and others. Universal genomic testing is now critical to identify candidates for these therapies.
In conclusion, treatment of metastatic BTC has evolved from empiric chemotherapy toward an immunotherapy- and biomarker-driven paradigm. Ongoing efforts should focus on optimizing sequencing, overcoming resistance, and ensuring broader access to precision strategies.
Yao-Chun Hsu
Department of Medical Research, E-Da Hospital, Kaohsiung, Taiwan
When to start antiviral therapy in chronic hepatitis B (CHB) remains one of the field’s most debated questions. In this lecture, Dr. Hsu will critically appraise the rationale, evidence, and trade - offs of treating earlier versus deferring therapy with close monitoring.
On the pro side, he will examine data linking cumulative HBV viremia exposure to cirrhosis and hepatocellular carcinoma (HCC), the risk of under-recognizing disease when relying on conventional ALT cutoffs, and the potential of early therapy to slow fibrosis progression, prevent HCCs, and reduce transmission. Dr. Hsu will highlight subgroups in whom early therapy may be most compelling: adults > 3-40 years with high HBV DNA regardless ALT levels, individuals with family history of HCC, and those at risk of acute exacerbation. We
will discuss how quantitative biomarkers (qHBsAg, HBcrAg, HBV RNA) and noninvasive measurement of liver fibrosis can refine selection.
On the con side, Dr. Hsu will address the reality that current NA monotherapy rarely achieves HBsAg loss, risking prolonged or indefinite treatment with attendant cost, adherence burden, and potential safety concerns. He will elaborate on the uncertain cost- effectiveness of broad early treatment, potential for overtreatment in truly inactive disease, and the need for robust monitoring whether or not treatment is initiated or deferred.
The session concludes with a practical, risk-adapted framework: who to treat early, who to monitor, how to communicate benefits and harms, and research priorities to resolve remaining uncertainties.
Wen-Juei Jeng
Department of Gastroenterology and Hepatology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
The landscape of chronic hepatitis B management is shifting from indefinite nucleos(t) ide analogue (NUC) therapy to the possibility of treatment discontinuation in carefully selected patients. The key questions remain: who is the right candidate, when should cessation be considered, and how should monitoring and retreatment be guided?
In this session, we will review updated evidence, including clinical trials, on outcomes of NUC
withdrawal in CHB patients, the predictive value and limitations of currently available biomarkers, the role of HBV DNA kinetics in anticipating flare, comparisons between TAF and other NUCs, and the long-term prognosis after discontinuation. By the end, participants will gain a clear framework to integrate the “who, when, and how” of NUC discontinuation into daily clinical practice, moving from empirical decisions toward evidencebased, personalized strategies.
Tung-Hung
Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
Fibrosis is a crucial indicator of liver damage and an important predictor of disease progression. Monitoring fibrosis is essential in the management of chronic hepatitis B (CHB), as advanced fibrosis and cirrhosis are associated with an increased risk of liver-related complications, including liver failure and hepatocellular carcinoma (HCC). Because of the invasive nature of liver biopsy, non-invasive tests (NITs) have transformed the clinical approach to chronic liver diseases, particularly CHB.
NITs include routine blood-based indices (such as APRI and FIB-4), fibrosis-related serological markers (such as M2BPGi and the ELF test), and elastography-based imaging modalities (such as vibration-controlled transient elastography, acoustic radiation force impulse imaging, and magnetic
resonance elastography). Current evidence supports the utility of these tools in measuring liver stiffness, which correlates with the degree of liver fibrosis.
These modalities have been widely used to predict fibrosis stage, cirrhosis, hepatic decompensation, HCC, and mortality in patients without antiviral therapy. In those receiving longterm antiviral treatment, on-treatment NITs provide additional prognostic value by identifying individuals who remain at risk for liver-related complications despite sustained viral suppression.
This lecture will review the current evidence and practical applications of NITs in CHB, highlighting their role in risk prediction models and their integration into precision hepatology for clinical practice.
Man-Fung Yuen
Department of Medicine, School of Clinical Medicine, The University of Hong Kong, Hong Kong
In the last 10 years, treatment for chronic hepatitis B virus (HBV) infection has been fast evolving. In addition to the standard of therapy, mainly long-term viral suppressive agents (nucleoside analogues) and pegylated interferon alpha, innumerable novel agents have been tested for their efficacies and safety in phase I - III studies. They act against nearly all the steps/ intermediates of hepatitis B virus replication. The goal is to reduce high-load antigenemia that consistently weakens host immunity. These agents include small interfering RNAs, anti-sense oligonucleotides, core protein assembly modulators. The former two agents knock down the pregenomic RNA and mRNA transcripts. The latter inhibits capsid encapsidation as well as replenishment of covalently closed circular
DNA.
Acting through immune restoration pathway to control hepatitis B, novel immunomodulators are also being developed. They are monoclonal antibody neutralizing HBsAg (also with vaccinal effects), toll like receptor agonists enhancing innate immunity and therapeutic vaccines enhancing T cell HBV specific responses. Combination of these two groups of novel agents have also been tested with additive responses in term of the rate of functional cure. New and exciting programs using agents modulating epigenetics of HBV through methylation and directly degrading cccDNA and integrated viral DNA have been started. With these innovations, chronic hepatitis B management is rapidly evolving from disease control to the prospect of true eradication.
Yan-Shen Shan
Division of General Surgery, Department of Surgery, National Cheng Kung University Hospital, Tainan, Taiwan
Institute of Clinical Medicine, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Recently, there have been many improvements in fluid biopsy for diagnosis and monitoring of disease, esp application of circulating tumor cells (CTC) and cell free DNA (cfDNA). However, suitable methods with good biomarkers are very important for clinical application. In this presentation, I will present our progress in fluid biopsy for pancreatic cancer. We developed several methods, including combined analysis of glypican 1 (GPC1) mRNA
expression in the exosomes-rich (Exo) EV and GPC1 membrane protein (mProtein) expression in the microvesicles-rich (MV) EV for early detection of pancreatic cancer, cfDNA amount and early retention of Kras in serum by dPCR for detection of distant metastasis of pancreatic cancer during treatment (figure), and monitoring for recurrence of pancreatic cancer after resection (detecting minimal residual cancer, MRD).
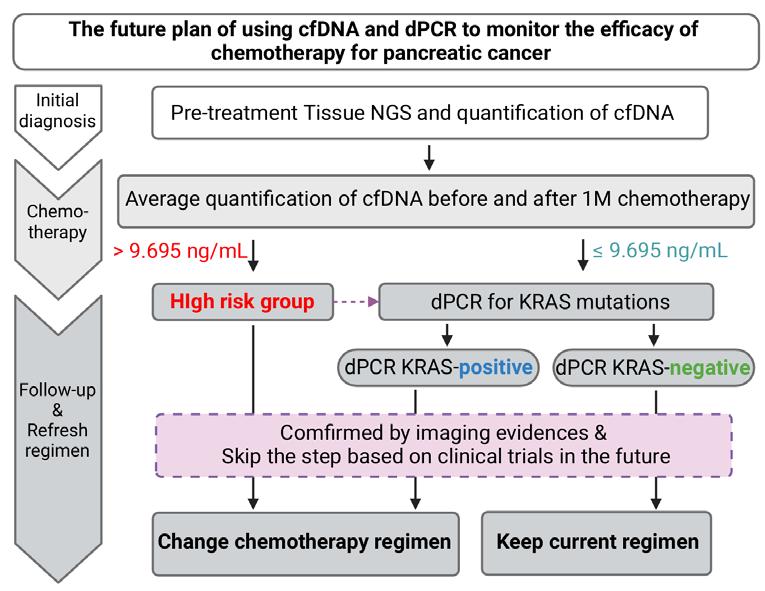
Jun Yu
Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Hong Kong
Immune checkpoint inhibitors (ICIs) have transformed cancer treatment but show limited efficacy in most gastrointestinal cancers. Responses are mainly seen in patients with dMMR, MSI-H and high mutational burden. Recent studies highlight gut microbiota’s key role in modulating ICI response. In colorectal cancer (CRC), we demonstrated that P. anaerobius enriched in CRC modulate the tumour immune microenvironment to facilitate CRC progression (Nat Microbiol 2019). P. anaerobius impairs anti-PD1 therapy in CRC mouse models by inducing MDSC infiltration and immunosuppression, activating integrin α2β1-NF-κB signaling to secrete CXCL1 and recruit CXCR2+ MDSCs, and directly enhancing MDSC activity via lytC_22 binding to Slamf4; targeting integrin α2β1 or Slamf4 offers promising strategies to overcome this resistance (Nat Microbiol 2024). We reported that F. nucleatum, a CRC pathogen, paradoxically facilitates anti-PD-1 therapy in microsatellite-stable (MSS) CRC (Cancer Cell 2024). On the other hand, Roseburia intestinalis-produced butyrate and Lactobacillus gallinarum-derived ICA, both depleted in CRC, enhance anti-PD-1 efficacy by activating cytotoxic CD8+ T cells (Gut 2023a) and suppressing CD4+ Treg differentiation via the IDO1/ Kyn/AHR axis (Gut 2023b). We recently identified that
Clostridium butyricum boosts anti-PD-1 therapy in MSS CRC by activating CD8+ T cells and suppressing macrophages. Its protein secD inhibits GRP78 and the PI3K/Akt-NF-κB pathway, lowering IL-6 to enhance immune response. This was confirmed in humanized mice, and patient organoids, making C. butyricum a promising immunotherapy adjuvant (Cancer Cell, in press). Thus, R. intestinalis, L. gallinarum and C. butyricum are potential adjuvants to augment anti-PD1 efficacy against CRC. In gastric cancer, we revealed that Streptococcus anginosus colonizes the gastric mucosa in mice, triggering gastric tumorigenesis. Its surface protein TMPC interacts with Annexin A2 to activate MAPK/ PI3K signaling, disrupts tight junctions, and alters the immune microenvironment by promoting inflammation, immunosuppressive macrophages, MDSCs, and exhausted CD8+ T cells. Targeting TMPC reverses these effects and restores immune balance (Cell 2024a). Findings of these studies will pave the new way for the clinical development of bacteriabased adjuvant therapy to enhance the therapeutic efficacies of existing ICIs for cancer treatment (Nat Rev Clin Oncol 2023, Nat Rev Gastroenterol Hepatol 2024. Cell 2024b).
Tzu-Chan Hong
Department of Internal Medicine, National Taiwan University Hospital Cancer Center, National Taiwan University College of Medicine, Taipei, Taiwan
The rise of patient-derived organoids (PDOs) has revolutionized gastrointestinal (GI) cancer modeling, enabling the recapitulation of tumorspecific architecture, heterogeneity, and molecular landscapes in a physiologically relevant ex vivo system. In this talk, we will explore the translational impact of PDOs across GI tract malignancies, including colorectal, pancreatic, esophageal, and gastric cancers, highlighting how these 3D cultures bridge the gap between preclinical modeling and precision oncology.
Despite advances in conventional preclinical models such as 2D cell lines and patient-derived xenografts, these systems often fail to preserve the intra- and intertumoral complexity of GI tumors. PDOs, by contrast, retain key histological, genomic, and proteomic features of the original tumor, and enable functional readouts such as individualized drug sensitivity and resistance profiling.
We will examine critical innovations that enhance PDO applicability in translational settings: (1) standardized workflows for tissue dissociation,
cryopreservation, and 3D culture expansion, (2) integrative fidelity assessment via histopathology, single-cell transcriptomics, and proteomics, and (3) high-throughput pharmacotyping for therapeutic decision-making. Co-culture systems with immune or stromal components and secretome/exosome profiling further extend PDO utility for studying tumor–microenvironment and host–pathogen interactions.
However, limitations remain: culture variability across institutions, underrepresentation of rare histotypes, and incomplete modeling of immune responses challenge the full clinical integration of PDO platforms. To address these, we propose harmonized biobanking efforts and co-clinical trials as necessary steps to validate PDOs as predictive tools in the era of precision GI oncology.
In conclusion, PDOs offer a scalable, patient-representative model for functional precision medicine, enabling not only tailored therapy selection but also a deeper mechanistic understanding of GI cancer heterogeneity.
Chu-An Wang
Institute of Basic Medical Sciences, National Cheng Kung University, Tainan, Taiwan Department of Physiology, National Cheng Kung University, Tainan, Taiwan
Pancreatic ductal adenocarcinoma (PDAC) is associated with a poor prognosis, particularly when diagnosed at regional or distant metastatic stages, largely due to the lack of early symptoms and limited treatment options. Extracellular vesicles (EVs), which are secreted by cells, play a vital role in facilitating intercellular communication and have essential functions in tumor biology. Exploring the regulation and properties of tumor-derived EVs may yield valuable insights into their potential applications as diagnostic indicators and drug delivery vehicles.
Over 90% of PDAC cases harbor KRAS mutations, which recruit macrophage infiltration and create a tumor-supportive environment by promoting the metastatic ability and immune invasion of pancreatic cancer cells. Mechanistically, macrophages activate ERK signaling while suppressing dual specificity
phosphatase 2 (DUSP2), resulting in sustained ERK activation in pancreatic cancer cells. The downregulation of DUSP2 enhances the secretion of vascular endothelial growth factor C (VEGF-C) via EVs, promoting lymphangiogenesis and lymphovascular invasion. Bioinformatic analyses have revealed that histone deacetylase (HDAC) inhibitors could be effective in PDAC treatment. Our investigation of the HDAC1/2 inhibitor B390 demonstrated that it restores DUSP2 function, suppresses tumor growth, and increases apoptosis. Additionally, B390 reduced EV-associated VEGF-C expression and inhibited lymphangiogenesis and metastasis in a mouse model of PDAC. Therefore, targeting tumorsecreted EV-VEGFC may mitigate pancreatic cancer metastasis.
Yen-Chen Anne Feng
Institute of Health Data Analytics and Statistics, Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taipei, Taiwan
The genomics era has transformed our understanding of how genetic variation shapes human health, uncovering the widespread polygenicity and pleiotropy that underlie complex diseases. Alongside advances in epidemiological modeling, new methods now harness polygenic architectures to estimate individual disease risk from genetic profiles. In this talk, I will introduce the technologies and bioinformatics behind genomic profiling, highlight our collaborative efforts in developing polygenic risk scores, and discuss their application to risk stratification in digestive health. I will also address the clinical potential—and the challenges—of polygenic risk prediction in the era of large-scale biobank studies.
Hsiang-En
Proteomics, powered by innovations in mass spectrometry, has become a transformative approach for deciphering complex biological systems. Unlike genomics or transcriptomics, which reflect potential or ongoing biological activity, proteomics directly captures the functional molecular landscape−what proteins are actually present, modified, and active. This is particularly valuable in cancer biology, where the progression of disease and the response to treatment are frequently influenced by proteinlevel dynamics. With the ability to quantitatively profile thousands of proteins and post-translational modifications such as phosphorylation from limited surgical samples, cutting-edge proteomic platforms empower the simultaneous analysis of tumor signaling, immune infiltration, and microbial content. In gastrointestinal cancers, this technique has uncovered functionally distinct tumor subtypes, identified non-genetic drivers of progression, and supported more precise patient stratification. In our recent proteomic study of gastric cancer, we analyzed paired tumor and adjacent non-tumor (NAT) tissues from 154 patients, integrating host proteome, phosphoproteome, immune profiles, microbial signatures and valuable clinical data. This multi-dimensional analysis revealed novel
insights into tumor initiation, progression, and molecular heterogeneity. Interestingly, microbial protein profiling identified metabolically active or translocated bacterial components within the tumor microenvironment, revealing patterns not captured by transcriptomic data. Helicobacter pylori was predominantly enriched in NAT, suggesting a spatial shift in microbial niches during tumorigenesis. In contrast, H. pylori-negative tissues exhibited more complex microbial networks and were associated with distinct proteomic and immune signatures, including hypoxia, cytokine signaling, and activation of oncogenic pathways. By combining microbial, immune, and proteomic data, we identified high-risk tumor subgroups associated with poor prognosis, notably those with immune-silent phenotypes. In contrast, another subgroup demonstrated high expression of epithelial barrier proteins, such as CLDN18, appeared less inflamed and potentially less aggressive. These findings demonstrate how proteomics can functionally resolve tumor heterogeneity shaped by microbial ecology and host response, providing a framework for identifying clinically meaningful subtypes and informing therapeutic strategies.
Eugene B. Chang
Department
of Medicine,
University of Chicago, Chicago, IL, USA
The gut microbiome is a vital organ crucial for development, immunity, and overall health. Unlike other organs, it is acquired early in life through maternal transfer and social interactions. Dysbiosis, or microbiome imbalance and dysfunction, is linked to diseases such as inflammatory bowel diseases, cancer, obesity, MASLD, and diabetes. Restoring eubiosis holds promise for prevention and treatment of these conditions, but effective tools to quantitatively assess gut health are lacking leaving the field mired in empiricism. Most existing methods focus on microbial composition rather than function. To address this, we developed a supervised machine-learning approach identifying
20 metabolomic markers consistently present in healthy adults. These markers reflect key functional subsystems of a healthy microbiome. From a cohort of 176 healthy individuals, we established reference ranges and created a composite Z score to distinguish eubiosis from dysbiosis. We validated this panel across multiple groups—including healthy adults, inflammatory bowel disease patients, and clinical cases of recurrent C. difficile and functional bowel disease. This first-of-its-kind clinical tool provides a quantitative measure of gut microbiome function, enabling maintenance of eubiosis, targeted therapies, and the development of effective microbiome-based interventions.
Wei-Kai Wu
Department of Medical Research, National Taiwan University Hospital, Taipei, Taiwan
Xenobiotics—spanning food additives, trace antibiotic residues, and high-dose antimicrobial cocktails—profoundly reshape gut microbial ecology and, in turn, digestive and metabolic health. This presentation integrates recent evidence across three exposure contexts. First, common dietary emulsifiers (e.g., lecithin, sucrose fatty acid esters, carboxymethylcellulose, mono-/diglycerides) can reprogram intestinal communities and disrupt host metabolism, producing hyperglycemia, hyperinsulinemia, and insulin resistance; notably, mono-/diglycerides have been linked to mucus encroachment and elevated circulating LPS, underscoring epithelial barrier dysfunction as a key mechanism. Second, extremely low, food-relevant antibiotic residues (e.g., tylosin at the theoretical maximal daily intake) aggravate diet-induced obesity and insulin resistance via microbiota shifts
that alter bile-acid composition and downstream enterohepatic signaling. Early-life exposure imprints durable metabolic vulnerability that is transferable by fecal microbiota transplantation. Third, refined antibiotic-cocktail regimens for pseudo-germfree models show how tuning depletion protocols can minimize toxicity while enabling causal interrogation of microbiota–host crosstalk; such depletion remodels tumor proteomics and can sensitize pancreatic cancer to chemotherapy, highlighting therapeutic implications of microbiome manipulation. Together, these studies support a framework in which xenobiotic class, dose, and timing—particularly in early life—govern the direction and magnitude of microbiota-mediated effects on epithelial integrity, inflammatory tone, and metabolic control.
Endoscopic Bariatric and Metabolic Therapies (EBMT)
Rationale and Current Evidence of Endoscopic Bariatric and Metabolic Therapies (EBMT)
Sheng-Shih Chen
Division of General Surgery, Department of Surgery & Metabolic and Bariatric Surgical Center, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
Introduction
Obesity is a growing global epidemic. Traditional methods such as diet, exercise, medications, and surgery have their roles. However, not all patients are suited for surgery, and this gap is where endoscopic bariatric and metabolic therapies (EBMTs) come in.
Obesity and Metabolic Disease
Obesity is linked to multiple chronic conditions, including diabetes, hypertension, and fatty liver disease. Hence, there’s a pressing need for effective, safe, and accessible treatments.
What is Endoscopic Therapy?
Endoscopic therapy involves using a flexible endoscope passed through the mouth to reach the GI tract. These procedures do not require incisions and are often performed on an outpatient basis.
Types of Therapies
The main types include:
1. Intragastric Balloons.
2. Endoscopic Sleeve Gastroplasty (ESG).
3. Duodenal Mucosal Resurfacing (DMR).
4. Transpyloric Shuttle. Let’s look at each briefly.
Intragastric Balloons
These are saline- or gas-filled balloons placed in the stomach. They create a sense of fullness and help reduce food intake. They are typically removed after six months.
Endoscopic Sleeve Gastroplasty (ESG)
ESG involves using sutures to reduce stomach volume, mimicking the effect of a surgical sleeve. It’s minimally invasive, repeatable, and reversible.
Duodenal Mucosal Resurfacing (DMR)
DMR ablates the duodenal lining to alter metabolic signaling, especially improving glycemic control. It’s still under active investigation.
Mechanisms of Action
These therapies work via gastric volume restriction, delayed emptying, and hormonal modulation—affecting GLP-1, insulin, and satiety.
Clinical Evidence
Recent data:
– A 2024 study on 404 ESG patients showed 15.8% TBWL maintained for 10 years.
– A 2025 study showed 16.1 kg weight loss at 12 months post-ESG.
– A 2025 review highlighted EBMT’s benefits on HbA1c, liver markers, and metabolic syndrome.
Benefits
EBMTs are minimally invasive, have short recovery periods, and are suitable for patients not eligible for surgery. 2025 reviews show additional benefits in metabolic and liver health.
Limitations
They offer less weight loss compared to
bariatric surgery, and some methods like balloons have temporary effects. Procedures must be done by experienced clinicians.
Future Perspectives
Combining ESG with GLP-1 receptor agonists like semaglutide can yield 25–30% TBWL. DMR systems are being evaluated for sustainable metabolic benefits. AI-assisted patient matching
may further optimize outcomes.
Conclusion
Endoscopic bariatric therapies strike a balance between efficacy and safety. They fill the treatment gap between medication and surgery. Continued innovation and research will further enhance their role.
Chu-Kuang Chou
The landscape of obesity treatment has been transformed by the emergence of highly effective anti-obesity medications (AOMs), particularly incretin-based therapies such as GLP-1 receptor agonists and dual agonists like tirzepatide. These agents have demonstrated unprecedented efficacy in achieving meaningful weight loss and improving cardiometabolic outcomes, reshaping clinical algorithms worldwide. However, their rapid adoption raises critical questions about the role of endoscopic sleeve gastroplasty (ESG) and other endoscopic bariatric procedures in modern obesity care.
This talk explores whether ESG remains relevant in an era dominated by pharmacologic breakthroughs. Drawing from the latest clinical data and real-world experiences, we will examine
the comparative efficacy, durability, safety profiles, and cost considerations of ESG versus AOMs. Importantly, we will highlight how ESG may serve not as a competitor, but as a complementary strategy—particularly for patients who experience medication intolerance, require durable anatomical restriction, or desire non-surgical yet procedurebased interventions.
We will also discuss emerging paradigms that integrate ESG with pharmacotherapy to optimize weight loss, enhance long-term adherence, and individualize treatment strategies. As obesity is a chronic, relapsing disease, a personalized and multidisciplinary approach remains essential. Rather than a binary choice, the future of obesity care lies in strategic combination—leveraging both procedural and medical tools to maximize patient outcomes.
Po-Jen Yang
Bariatric surgery has undergone remarkable evolution since its introduction in the 1950s, progressing from malabsorptive procedures to contemporary operations that primarily reduce gastric volume, often combined with gastrointestinal bypass. The adoption of laparoscopic techniques in the 1990s further improved safety and recovery, establishing metabolic and bariatric surgery (MBS) as the most effective long-term therapy for severe obesity and related comorbidities, including type 2 diabetes. In Taiwan, current National Health Insurance coverage requires a BMI ≥37.5 kg/m², or ≥32.5 kg/m² with major comorbidities, in adults aged 20–65 years who have failed six months of medical therapy. By contrast, the ASMBS and IFSO advocate lower thresholds for Asian populations, recommending bariatric surgery for individuals with BMI ≥27.5 kg/m² in the presence of obesity-related disorders, without strict age restrictions and with appropriateness extended to carefully selected children and adolescents.
Endorsed MBS procedures include sleeve gastrectomy, Roux-en-Y gastric bypass, oneanastomosis gastric bypass, biliopancreatic diversion/duodenal switch, single-anastomosis duodeno-ileal bypass with sleeve, and adjustable gastric banding. Each technique has distinct advantages and limitations in terms of weight reduction and metabolic improvements, as well as specific risks such as bleeding, leakage, malnutrition, anemia, reflux esophagitis, marginal ulceration, dumping syndrome, and bile reflux. As the number of patients undergoing bariatric surgery continues to rise, gastroenterologists are increasingly likely to encounter these individuals in clinical practice. For GI endoscopists, familiarity with surgical anatomy, procedure-specific complications, and long-term outcomes is essential to ensure accurate diagnosis, effective endoscopic management, and optimal multidisciplinary care for this growing patient population.
Endoscopic Bariatric and Metabolic Therapies (EBMT)
Chen-Shuan Chung
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan
Obesity has emerged as one of the most critical global health challenges, contributing to a growing burden of metabolic diseases, cardiovascular disorders, and reduced life expectancy. While lifestyle modification and pharmacological therapy remain first-line treatments, their long-term efficacy is often limited. Bariatric surgery, though effective, is invasive and not suitable for all patients. In response to this treatment gap, endoluminal interventions have gained increasing attention as minimally invasive alternatives that offer meaningful weight loss and metabolic benefits with improved safety profiles.
This presentation will explore the latest advances in endoluminal therapies for obesity, including gastric and intestinal approaching methods. We will
discuss their mechanisms of action, clinical efficacy, durability of outcomes, and safety data based on recent clinical trials.
As technology advances and our understanding of gut-brain metabolic signaling improves, the role of endoluminal therapy is poised to expand beyond weight loss alone, with potential indications in type 2 diabetes, fatty liver disease, and even cardiovascular risk reduction. We will also address the challenges of patient selection, procedure standardization, and integration into multidisciplinary care pathways. This session aims to provide a comprehensive overview of the future directions in endoscopic metabolic interventions and highlight their emerging role in reshaping obesity management strategies worldwide.
Yen-Hsuan Ni
Department of Pediatrics, National Taiwan University Hospital, Taipei, Taiwan
A long-term prospective monitoring on the development of diseases and the evolution of gut microbiota is pivotal to unravel the critical role(s) of the gut microbiota and their metabolites in the disease courses. To induce the phenotype in an appropriate animal model by administering these candidate bacteria are also important to prove their causaleffect relationship. The gut microbiota modulates the disease courses through several different pathways, mainly through neurotransmitters, endocrinological and metabolic factors, and immune cytokines. We have proven an early colonization with R. gnavus in the gut promoted allergic disease in infants. We also demonstrated that Desulfovibrio could induce non-alcoholic liver diseases in obese children. We also demonstrated the antagonism of R. gnavus and A. muciniphila may modulate the clinical course of chronic hepatitis B infection. With the metabolomic
studies, we have established the cause-effect relationship between these microbiomes and their related diseases. The diseases involved, such as metabolic diseases, cancers, immunologic diseases, and neurologic disorders, may be attributed to the dysbiosis in the early life. Based on these findings, we started to look for the responsible gut microbiome and its metabolites or gene products as the therapeutic target(s), which will be the next generation probiotics. Our perspectives on the microbiome-based therapeutics will be diseasespecific medicines. In the meantime, they should undergo clinical trials as the pharmaceuticals. The next generation probiotics and their derivatives, including the fermented cultured medium, engineered probiotic, and exosomes, should be medical-graded products and not just healthpromoting food.
Chi-San Tai
Department of Pediatrics, National Taiwan University Hospital, Taipei, Taiwan
Infantile cholestasis presents a multifaceted diagnostic challenge for pediatric hepatologists, especially when discerning genetically rooted etiologies. Despite advances in genetic medicine, the rarity and diversity of genetic cholestatic diseases, coupled with limited access to early-stage genetic testing, complicate timely diagnosis and resource allocation. This study introduces JADE-B (Jaundice Diagnosis Easy for Baby), a machine-learning-based predictive model aimed at identifying cholestatic infants likely to harbor genetic liver diseases, thereby optimizing the prioritization for genetic diagnostics.
Patient data from the Integrated Medical Database of National Taiwan University Hospital (NTUH) from 2006 to 2018 served as the foundation for analysis. A cohort of 1008 infants under one year of age diagnosed with cholestatic liver disease was selected, and 47 clinical and laboratory parameters were incorporated across various timeframes. The study employed four machine learning classifiers— Logistic Regression, XGBoost, LightGBM, and Random Forest—to construct five predictive models. After feature selection and comparative performance evaluation, Model 5, a Random Forest classifier trained on 20 accessible clinical features within one month of disease onset, was designated
as the JADE-B model. JADE-B achieved an AUROC of 0.836, sensitivity of 0.8421, specificity of 0.8239, and a notably high negative predictive value of 0.9873. SHAP analysis highlighted key predictive features including elevated direct bilirubin levels and persistent liver enzyme abnormalities. External validation using cohorts from Thailand and South Korea confirmed an AUROC of 0.7115, indicating generalizability across populations.
The model enables physicians to stratify infants with cholestasis and efficiently allocate genetic testing resources, especially in contexts with limited availability or financial constraints. Its use of earlystage markers ensures prompt prediction without delaying critical diagnoses, such as biliary atresia. Furthermore, the model’s simplicity enhances its applicability in diverse clinical settings. JADE-B represents a significant step toward precision medicine in neonatal hepatology, offering a scalable tool for prioritizing genetic evaluation. Its integration into diagnostic workflows could expedite personalized care and inform long-term prognosis for affected infants. Future directions include prospective multicenter validation and adaptation for other pediatric liver diseases.
Ni-Chung Lee
Department of Medical Genetics and Pediatrics, National Taiwan University Hospital, Taipei, Taiwan
With the rapid advancement of next-generation sequencing (NGS) technologies, their clinical applications have grown substantially in recent years. However, to maximize diagnostic yield, it’s essential to select the most appropriate molecular testing strategy based on the suspected disease mechanism. Different molecular bases often require distinct analytical approaches—for example, singlegene disorders may benefit from targeted panels, while more complex or atypical presentations may warrant whole exome sequencing (WES) or whole genome sequencing (WGS).
WES and WGS often identify multiple pathogenic or likely pathogenic variants, but not all of these are necessarily causative for the patient’s specific phenotype. Therefore, careful interpretation and a strong focus on genotype–phenotype correlation are critical. Clinicians must evaluate how well a variant explains the observed clinical features, taking into account inheritance patterns, penetrance, and
phenotypic variability.
While some diseases are clearly monogenic, especially those with early onset, many adult-onset or progressive disorders are multifactorial, involving complex interactions between genetic, epigenetic, and environmental factors. As such, a single approach may not be sufficient for comprehensive diagnosis.
In this talk, I will introduce the current molecular diagnostic strategies implemented at our hospital, including our approach to variant interpretation and case discussions that highlight real-world diagnostic challenges. In addition, I will explore how integrating multi-omic data—such as transcriptomics, epigenomics, and proteomics—can enhance diagnostic precision and support timely clinical decision-making. By combining clinical insights with advanced genomic tools, we aim to improve the diagnostic journey for patients with rare and complex genetic conditions.
Gar-Yang Chau
Division
of
General Surgery, Department of Surgery, Taipei Veterans General Hospital, Taipei, Taiwan
Hepatocellular carcinoma (HCC) is a leading cause of cancer-related mortality worldwide, frequently developing in patients with chronic liver disease. Surgical resection remains a cornerstone of curative treatment, and minimally invasive surgery (MIS), including laparoscopic and robotic techniques, has increasingly become the preferred approach in select cases due to its association with reduced morbidity and faster recovery. This lecture aims to provide a focused update on the role and advancements of MIS for HCC, highlighting clinical evidence, patient selection, technological innovations, and outcomes.
The lecture will review the evolution and expanding indications of MIS in HCC management, emphasizing evidence from recent meta-analyses demonstrating comparable oncologic efficacy between MIS and open liver resection, with benefits including less intraoperative blood loss and shorter hospitalization. Particular attention will be given
to the integration of intraoperative tools such as laparoscopic ultrasound and indocyanine green (ICG) fluorescence imaging that enhance tumor visualization and margin assessment.
The lecture will discuss challenges unique to HCC patients, including underlying cirrhosis, tumor location, and size, and how careful preoperative evaluation via advanced imaging can optimize patient selection. The role of MIS in combination with loco-regional and systemic therapies will also be briefly addressed to contextualize surgical options within comprehensive HCC care.
We will present our institution’s experience, sharing outcomes from over 800 patients who underwent minimally invasive liver resections for HCC between 2013-2023. Our data corroborate the safety and effectiveness of MIS in this population, with comparable complication rates and promising long-term survival, underscoring the feasibility of broader MIS adoption in clinical practice.
Yu-Yun Shao
Department of Oncology, National Taiwan University Hospital, Taipei, Taiwan
Despite a decade of clinical experience, immunotherapy for hepatocellular carcinoma (HCC) still faces major hurdles across the disease continuum. In advanced HCC, immune checkpoint blockade must be paired with either targeted agents or a second checkpoint inhibitor to provide survival benefits as first-line therapy; yet even these combinations leave roughly 40% of patients without clinical benefit, and nearly all patients who had stable disease eventually develop resistance. Innovative strategies to circumvent both primary and acquired resistance remain an urgent priority.
Equally pressing is the need to translate the success seen in advanced disease to earlier stages. In the intermediate stage, the optimal sequencing or integration of immune-based regimens with transarterial embolization—and the combination most likely to extend survival—are undefined. At the early stage, no phase III trial has yet demonstrated a clear advantage for adjuvant immunotherapy. Addressing resistance mechanisms, exploring novel targets, and refining combination will be pivotal to unlocking the full potential of immunotherapy for HCC from early through advanced disease.
Chien-Hao Huang
Division of Hepatology, Department of Gastroenterology and Hepatology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
Background and Aims: Hepatocellular carcinoma (HCC) arises within a tolerogenic tumorimmune microenvironment (TIME) characterized by dominant immunosuppression and impaired effector responses. Regulatory T cells (Tregs) are key mediators of this tolerance and correlate with poor outcomes, yet their functional heterogeneity in HCC remains incompletely defined. We aimed to delineate Treg subclusters using single-cell CITE-seq and to validate their clinical/prognostic relevance in patients with HCC.
Method: Single-cell CITE-seq was performed on 51,067 CD4+ T cells from eight HCC patients, analyzing samples from the tumor, non-tumor, and peripheral blood compartments. Validation involved 96 HCC patients and 53 healthy donors through flow cytometry, functional assays, and clinical data integration.
Results: Trajectory and TCR analyses identified a Foxp3high Treg subset in peripheral blood that preferentially migrates to tumor sites, acquiring a terminally differentiated, activated phenotype. Tumor-infiltrating Foxp3high Tregs exhibited elevated LAYN and tissue-resident memory (TRM)
signatures and enhanced Foxp3 expression driven by proinflammatory cytokines in the tumor microenvironment. These proinflammatory cytokines could promote FOXP3, chemokine expression, and Treg activation. The CCL5/CCR5 axis mediated their recruitment from peripheral blood to tumors. A significant correlation was found between peripheral and intratumoral Foxp3high Tregs, supporting their potential as biomarkers. A predictive model using peripheral Foxp3high Tregs/ CD4+ T cells >3.5% was developed, demonstrating robust prognostic performance for overall survival and early recurrence, with AUROCs exceeding 0.753 in both training and validation cohorts. The results were further supported by TCGA-LIHC data.
Conclusion: Peripheral Foxp3high Tregs migrate to tumors via the CCR5-CCL5 axis and mature under proinflammatory cytokines. Their proportion in blood correlates with tumor presence, making them a promising biomarker for predicting HCC outcomes. Targeting intratumoral Treg function may offer a promising adjunctive strategy in future immunebased therapies for HCC.
Chung-Ying Lee
Division of Gastroenterology, Department of Internal Medicine, Shuang Ho Hospital, New Taipei City, Taiwan
Adenoma detection rate (ADR) is widely regarded as the cornerstone quality indicator for colonoscopy, with strong evidence linking higher ADRs to lower risks of post-colonoscopy colorectal cancer (PCCRC). However, recent data suggest a “ceiling effect” beyond which further increases in ADR yield diminishing returns in PCCRC prevention. This underscores the need for more nuanced quality metrics that reflect not only detection but also completeness and thoroughness. Metrics such as adenomas per colonoscopy (APC) and adenomas per positive procedure (APP) provide more granular insight into mucosal inspection and help mitigate the “one-and-done” phenomenon, where additional
lesions may be overlooked once a single adenoma is found. Evidence suggests that lower APC is independently associated with increased PCCRC risk, even among endoscopists with acceptable ADRs. Furthermore, emerging indicators such as proximal serrated polyp detection rate (PSPDR) and incomplete resection rate (IRR) are gaining attention as complementary quality benchmarks. This lecture will review the limitations of ADR, introduce these advanced quality indicators, and discuss their roles in enhancing detection, reducing missed lesions, and ultimately improving patient outcomes in colorectal cancer screening.
Wey-Ran Lin
Department of Gastroenterology and Hepatology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
Post-colonoscopy colorectal cancer (PCCRC) remains a critical quality indicator and ongoing challenge in colorectal cancer prevention. A significant proportion of PCCRC cases are attributed to incomplete polypectomy, highlighting a need for deeper understanding of its root causes and implications for clinical practice. Multifactorial contributors result in incomplete polypectomy, including lesion characteristics (e.g., size, morphology, and location), endoscopist skill and
technique, limitations in detection technologies, and procedural inadequacies. Although technological advancements will improve polyp detection, reduce missed lesions, prevent incomplete resections, and enhance overall procedure quality, the most effective strategy remains regular interval selfassessment with each unit. This talk assesses key performance metrics - such as cecal intubation rate, adenoma detection rate, withdrawal time, PCCRC incidence, and incomplete resections.
Meng-Ying Lin
Department of Internal Medicine, National Cheng Kung University Hospital, Tainan, Taiwan
The integration of quality metrics into gastrointestinal endoscopy has become essential for ensuring patient safety, procedural efficacy, and optimal clinical outcomes. Among the most commonly performed endoscopic procedures— esophagogastroduodenoscopy (EGD), endoscopic retrograde cholangiopancreatography (ERCP), and endoscopic ultrasound (EUS)—each has a distinct profile of indications, technical complexity, and associated risks, necessitating procedure-specific quality indicators.
For EGD, quality metrics focus primarily on appropriate indications, complete mucosal visualization, adequate photodocumentation, and biopsy protocol adherence. Additional benchmarks include duodenal intubation rates, complication rates, and the completeness of procedure reports. These metrics aim to enhance diagnostic yield, particularly in cancer surveillance and evaluation of upper gastrointestinal symptoms.
ERCP, being a predominantly therapeutic and high-risk procedure, requires rigorous quality monitoring. Key metrics include rates of successful biliary and pancreatic duct cannulation, therapeutic
success (e.g., stone extraction or stent placement), and complication rates such as post-ERCP pancreatitis, bleeding, and perforation. Prophylactic measures, including the use of rectal NSAIDs in highrisk patients, and minimizing fluoroscopy time, are also emphasized.
EUS combines high-resolution imaging with fine-needle aspiration or therapeutic interventions, demanding high operator skill. Quality indicators for EUS include appropriate indication, complete examination of target structures, diagnostic yield of EUS-guided tissue acquisition, and complication rates. For therapeutic EUS, technical and clinical success rates are central metrics, along with adequate documentation and follow-up planning.
Across all three procedures, common themes in quality assurance include appropriate patient selection, informed consent, thorough documentation, and post-procedural outcome tracking. As endoscopic technology and techniques evolve, the continuous assessment and refinement of these metrics remain critical for advancing patientcentered care and maintaining high standards in gastrointestinal endoscopy practice.
Han-Mo Chiu
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
Performance-based reimbursement has gained attention as a means to align financial incentives with the delivery of high-quality endoscopy. Colonoscopy provides a prime example, as its effectiveness in colorectal cancer (CRC) prevention depends on the quality of adenoma detection and complete resection rather than procedure volume alone. Traditional fee-for-service models do not capture this variability, whereas linking reimbursement to quality indicators such as adenoma detection rate (ADR), cecal intubation rate, or adherence to surveillance guidelines offers a mechanism to reward qualitydriven practice. Emerging evidence indicates that higher ADR is associated with lower risks of post-
colonoscopy CRC and mortality, supporting the rationale for performance-based payment schemes. However, key challenges remain, including defining appropriate performance thresholds, avoiding unintended behaviors (e.g., excessive polypectomy of diminutive lesions), and accounting for differences in patient case mix and healthcare system resources. This lecture will review the evidence base, highlight experiences from various screening programs, and discuss future directions for performance-based reimbursement in endoscopy, with a focus on its role in improving population-level outcomes in CRC prevention.
I-Chen Wu
Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
PNETs represent a rare but increasingly recognized subgroup of gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs). The diagnosis of PNETs, especially small and functional subtypes, remains challenging due to their nonspecific symptoms and indolent growth. Functional PNETs often present with hormone-related symptoms such as secretory diarrhea or intractable ulcers, depending on the hormone secreted (e.g., VIPomas or gastrinomas). It is important to distinguish these from other gastrointestinal disorders such as irritable bowel syndrome (IBS). A subset of patients may present with multiple endocrine neoplasia type 1 (MEN-1), warranting attention to clinical clues such as multiple tumors, family history, hypercalcemia, and renal dysfunction. Pathologically, PNETs demonstrate characteristic histological and immunohistochemical features. Accurate diagnosis is essential not only for treatment planning but also for predicting behavior and
prognosis.
Endoscopic ultrasound (EUS) plays a pivotal role in the diagnosis and management of small PNETs. EUS with fine-needle biopsy (FNB) offers high diagnostic yield, especially for solid pancreatic lesions. Complementary techniques such as color Doppler and contrast-enhanced harmonic EUS (CEHEUS) improve lesion characterization, particularly when margins are unclear or when vascularity assessment is needed. For selected cases of small, localized, functional PNETs, minimally invasive endoscopic therapies offer a promising alternative to surgical resection. EUS-guided interventions, including ethanol injection or radiofrequency ablation (RFA), have been successfully used for tumor debulking and symptom control. These techniques are particularly valuable for patients who are poor surgical candidates or have multiple small lesions, as in MEN-1.
Ching-Yao
Department of Surgery, National Taiwan University Hospital, and College of Medicine National Taiwan University, Taipei, Taiwan
Pancreatic neuroendocrine tumors (PNETs) are relative uncommon disease. However, the incidence of PNETs is increasing not only in western countries, but also in Taiwan. Currently, PNETs is the second most of pancreatic malignant neoplasms followed by pancreatic ductal adenocarcinoma. Every year, about 220–250 patients were newly diagnosed as PNETs. Surgical resection of PNETs is
the fundamental treatment for this disease. In this talk, we will focus on the major surgical issues about PNETs management, including (1) the importance of lymph nodes dissection (2) the indication and debate about surgery for small PNETs (<2 cm) (3) the role of surgery on metastatic PNETs. Finally, we will share the surgical experience of PNETs in NTUH.
Jia-Hong Chen
Division of Hematology and Oncology, Department of Internal Medicine, Tri-Service General Hospital, Taipei, Taiwan
Drug treatment for pancreatic neuroendocrine tumors (PNETs) includes targeted therapies like everolimus and sunitinib (which block tumor growth and blood vessel formation), chemotherapy agents such as streptozotocin and temozolomide (for more aggressive tumors), somatostatin analogs like octreotide (to manage symptoms and control tumor growth). The specific treatment depends on the tumor’s grade and stage, its genetic factors, and the patient’s symptoms.
• Somatostatin Analogs: These drugs help control symptoms in functional PNETs and can also slow tumor growth.
– Octreotide (Sandostatin): Administered as a short-acting daily injection or a long-acting monthly injection.
Lanreotide (Somatuline Depot): A longacting form given as an injection every four weeks.
• Targeted Drug Therapy: These drugs target specific molecules or proteins that help cancer cells grow and divide.
– Everolimus (Afinitor): Inhibits the mTOR protein, which is crucial for cell growth and division.
– Sunitinib (Sutent): Prevents the formation of new blood vessels that supply the tumor with nutrients.
Cabozantinib (Cabometyx): Blocks several tyrosine kinases that are involved in cancer cell growth and survival.
–
–
Chemotherapy: Chemotherapy is typically used for high-grade tumors or those with a large tumor burden.
Streptozotocin: Often combined with 5-fluorouracil (5-FU), this drug damages DNA and causes cancer cells to die.
Temozolomide: An oral drug that damages cancer cells, often used with capecitabine.
Cisplatin: A chemotherapy agent sometimes combined with etoposide for high-grade PNETs.
Immunotherapy, particularly using immune checkpoint inhibitors (ICIs), shows promise for treating PNETs, but its role is still under investigation and not yet standard treatment. While ICIs have proven effective in other cancers, response rates in PNETs are generally low, though responders often experience durable disease control. Ongoing clinical trials are exploring combination therapies, such as combining ICIs with other treatments or using different immunotherapy strategies, to improve effectiveness. Researchers are also working to identify biomarkers to select patients most likely to benefit from immunotherapy.
Future research will focus on identifying specific patient populations who can benefit from immunotherapy.
Developing novel combinations of conventional therapy, targeted therapy, and immunotherapy will be a key area of development.
Chia-Hsun Hsieh
Division of Oncology, Department of Internal Medicine, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
Pancreatic neuroendocrine tumors (PNETs) are a biologically and clinically heterogeneous group of neoplasms that often present therapeutic challenges, especially in advanced disease. Conventional treatments—including surgery, somatostatin analogs, targeted agents, and peptide receptor radionuclide therapy (PRRT)—have improved outcomes, but many patients eventually experience disease progression.
This 20-minute lecture will provide an overview of emerging therapies that may redefine the treatment landscape for PNET. The talk will highlight novel targeted approaches such as next-
generation tyrosine kinase inhibitors and mTOR pathway modulators, advances in immunotherapy including immune checkpoint blockade and cellular therapies, as well as innovative combinations that integrate systemic agents with PRRT or locoregional strategies. Translational insights from genomic and epigenetic profiling will be discussed to illustrate opportunities for precision medicine and biomarkerdriven treatment.
By bridging current clinical practice with ongoing research, this presentation aims to outline the future directions of PNET therapy and their potential to improve patient outcomes.
Pi-Yi Chang
Interventional Radiology Department, Taichung Veterans General Hospital, Taichung, Taiwan
Percutaneous transhepatic cholangiography and drainage (PTCD) is a well-established imageguided procedure that plays a vital role in the management of biliary obstruction, especially in patients who are not candidates for endoscopic approaches. Originally developed as a palliative treatment for malignant obstruction, PTCD now serves broader indications, including biliary decompression, management of bile leaks, and preoperative drainage.
Our recent retrospective analysis from January 2022 to February 2024 included 98 PTBD procedures categorized by bile duct dilatation status (nondilated, mildly, moderately, and severely dilated). The overall technical success rate was high across all groups, with 90% in nondilated ducts and ≥94% in the remaining groups. Although procedures in patients with nondilated bile ducts required longer fluoroscopy time (average 41.7 min), complication and post-procedural morbidity rates were comparable among all groups.
Advanced techniques such as portal veinoriented puncture and central duct puncture aided
in accessing nondilated ducts, enhancing procedural feasibility and safety. These approaches, particularly valuable in post-transplant or altered anatomy cases, exemplify the adaptability of PTCD in complex clinical scenarios.
Supporting literature also underscores PTCD’s utility in controlling bile leaks, delaying definitive surgery, and improving outcomes in high-risk surgical candidates. Comparative studies indicate PTBD may offer fewer procedure-related complications than endoscopic drainage in select preoperative patients. However, long-term drainage complications, including occlusion and cholangitis, remain a concern, especially in malignant disease or bilateral drainage cases.
In conclusion, PTCD remains a versatile and effective intervention. With tailored techniques and appropriate imaging guidance, even challenging cases such as nondilated ducts can be managed successfully. The continued refinement of access strategies and follow-up protocols will further enhance the safety and efficacy of this crucial procedure.
Image-Guided Hepatobiliary Intervention
Chien-An Liu
Division of Abdominal Imaging, Department of Radiology
Taipei Veterans General Hospital, Taichung, Taiwan
Malignant biliary obstruction from cholangiocarcinoma, pancreatic cancer, or metastatic disease causes jaundice, cholangitis, and impaired quality of life. When endoscopic drainage fails or is not feasible, percutaneous metallic biliary stent placement (PTBS) provides reliable palliation.
PTBS is a robust, minimally invasive option that should be considered when ERCP fails, particularly for hilar or surgically altered anatomy. Technical success rates exceed 95%, with procedure-related mortality under 1%. Self-expanding metallic stents
(SEMS) offer longer patency than plastic stents and fewer re-interventions.
Optimal patient selection, careful tract creation, and familiarity with covered versus uncovered stents are key to maximizing outcomes.
This presentation will review indications, technical approaches, outcomes, and complication management, emphasizing how PTBS can be integrated into multidisciplinary care to improve symptom control and quality of life for patients with advanced biliary obstruction.
Image-Guided Hepatobiliary Intervention
Chih-Kai Chang
Department of Medical Imaging, National Taiwan University Hospital Hsinchu Branch, Hsinchu, Taiwan
Liver biopsy remains a fundamental tool for the diagnosis and staging of liver diseases. While percutaneous liver biopsy is most commonly employed in clinical practice, transjugular liver biopsy (TJLB), introduced in the 1970s, has become an established procedure within interventional radiology. TJLB provides a safe and effective alternative for patients in whom percutaneous biopsy is contraindicated, such as those with ascites or thrombocytopenia. Advances in biopsy devices and angiographic technology have further enhanced the safety, reliability, and diagnostic
yield of this technique. Importantly, TJLB can also be performed in conjunction with hepatic venous pressure gradient (HVPG) measurements, thereby offering both histopathologic and hemodynamic information in the evaluation of unexplained liver dysfunction.
This presentation will provide an overview of the indications, advantages, and limitations of TJLB, supported by illustrative clinical cases, with the aim of improving awareness and fostering greater integration of this procedure into hepatology practice.
Image-Guided Hepatobiliary Intervention
Chiung-Yu Chen
The learning curve for TIPS (transjugular intrahepatic portosystemic shunt) is generally consideredsteep and prolonged, typically requiring 20–50 cases for basic competency and 75–100+ cases fortrue proficiency.
Indications: Our primary indication is refractory ascites as an elective procedure. For acute varicealbleeding and critically ill patients in the ICU, we preferentially perform percutaneous transportalvariceal embolization.
The most challenging aspect of TIPS creation is establishing guidewire access from the jugular veinthrough the liver parenchyma to the splenic or superior mesenteric vein—a step that often determinesprocedural success.
The classic TIPS creation follows an antegrade approach from hepatic vein to the portal system, whichhas an inherently steep learning curve. We
have adopted a retrograde approach, creating TIPS fromthe portal system to the systemic veins using the one-needle-pass technique developed by severalpioneers in the field.
In this presentation, I will share our modified one-needle-pass technique utilizing a portal veinlocalization (PVL) sheath, which significantly simplifies the procedure and flattens the learning curvefor interventional radiologists in training. Our initial experience with this technique demonstrated 100%technical and hemodynamic success rates with no 30-day mortality. The mean fluoroscopic time was45.7 minutes with a mean procedure time of 175.3 minutes. This technical modification has improvedour success rates while reducing procedural complexity, making TIPS more accessible to operatorswith varying levels of experience, especially for young interventional radiologists.
Image-Guided Hepatobiliary Intervention
Chih-Horng Wu
Department of Medical Imaging, National Taiwan University Hospital, Taipei, Taiwan
Histotripsy is an innovative non-invasive therapy that employs short-cycle, high-intensity ultrasound mechanical waves to disintegrate targeted tissues. By inducing controlled cavitation, this technique transforms tissue into acellular debris, which the body naturally clears within one to two months, leaving only minimal scarring.
Key advantages of histotripsy include:
• Non-invasive: No skin incisions are required.
• Radiation-free: Eliminates risks associated with radiation exposure.
• Non-thermal: Prevents heat-related injury, preserving surrounding structures such as blood vessels.
Owing to its high tissue selectivity, histotripsy is particularly well-suited for hepatocellular carcinoma, as it is not restricted by thermal coagulation effects. Real-time ultrasound guidance further ensures precise targeting and treatment.
Beyond direct tumor ablation, histotripsy may also modulate the tumor microenvironment, stimulating immune responses. When combined with immunotherapy, it has the potential to enhance treatment efficacy and patient outcomes, positioning histotripsy as a promising new frontier in cancer therapy.
TDDW–JDDW–KDDW
Upper GI:
National Strategy for Gastric Cancer Control-Perspectives from Taiwan, Japan, and Korea
Yi-Chia Lee
Division of Gastroenterology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
Population-based screening and eradication of Helicobacter pylori infection, a well-established cause of gastric cancer, is emerging as an effective strategy to reduce gastric cancer incidence and mortality. To support systematic implementation at the population level, Taiwan adopted a threetiered foundation that includes: (1) a centralized planning committee; (2) screening service delivery through primary care providers, guided by clinical guidelines established by medical societies; and (3) community engagement to raise awareness of stomach health and promote participation in screen-and-treat programs through social media campaigns. Program execution strictly follows the principles of organized screening, supported by standardized quality indicators, integrated digital tracking systems, structured audit mechanisms, and both effectiveness and cost-effectiveness assessments. Strategies are tailored to local contexts: in the Matsu Islands, mass screening using the ¹³C urea breath test and subsequent eradication treatment led to reductions in H. pylori prevalence and gastric cancer incidence and mortality; in
Changhua County, a pragmatic randomized clinical trial showed that dual screening using H. pylori stool antigen and fecal immunochemical testing improved participation and reduced gastric cancer incidence; and in Indigenous communities, household-based approaches utilizing the ¹³C urea breath test could enhance H. pylori detection rate and reduce the intrafamilial transmission. In addition to the continuous assessment of effectiveness in preventing both gastric cancer and peptic ulcer disease, all these programs consistently maintain high standards of quality and equity, ensuring accessibility for diverse populations with varying socioeconomic positions. Collectively, it demonstrates how robust scientific evaluations, when combined with organized screening principles and systematic performance monitoring, can be effectively translated into sustainable, evidencebased programs for population-wide gastric cancer prevention. In this presentation, we will discuss in detail the dual screening strategy scheduled for nationwide rollout in 2026.
TDDW–JDDW–KDDW
Upper GI: National Strategy for Gastric Cancer Control-Perspectives from Taiwan, Japan, and Korea
Osamu Dohi
Molecular Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine Graduate School of Medical Science, Kyoto, Japan
Although the mortality rate of gastric cancer has been decreasing in Japan, it remains the second most common malignancy in terms of its incidence. As part of the national strategy, radiographic screening for gastric cancer has been implemented for decades and endoscopic screening has recently demonstrated improvements in prognosis.
Helicobacter pylori eradication therapy is a fundamental measure for primary prevention. Since 2013, Japan’s National Health Insurance has covered eradication therapy for all H. pylori-related diseases, effectively initiating a nationwide approach to gastric cancer prevention.
Endoscopic resection has significantly advanced
as a minimally invasive treatment option. Endoscopic submucosal dissection has been widely adopted for early gastric cancer, and clinical trials have confirmed its efficacy and safety. Additionally, image-enhanced endoscopy has improved the detection rate of EGC, contributing to earlier diagnosis and less invasive treatment. It is anticipated that the number of endoscopic resections for gastric cancer will soon exceed that of surgical interventions.
This lecture provides an overview of Japan’s national strategies for gastric cancer control, with a particular focus on the evolving role of endoscopy in prevention, detection, and treatment.
TDDW–JDDW–KDDW
Upper GI:
National Strategy for Gastric Cancer Control-Perspectives from Taiwan, Japan, and Korea
Young-Il Kim
Center for Gastric Cancer, National Cancer Center, Goyang, Korea
Gastric cancer remains a significant global health issue, ranking as the fifth most common cancer and the fifth leading cause of cancer-related deaths worldwide in 2022, with approximately one million new cases and 660,000 deaths annually. The Korea has one of the highest incidence rates globally, with 27.0 cases per 100,000 person-years. Thus, the Korean government established a National Cancer Screening Program for gastric cancer (NCSPGC) to detect gastric cancer at earlier stages and to reduce mortality from the gastric cancer.
The NCSP-GC initiated in 1999 for Medical Aid Program recipients, and expanded to cover all adults aged 40 years or older in 2002, recommending biennial screening. Since 2018, endoscopic screening has become the primary screening method in the NCSP-GC, which proved to be more effective. In 2023, the proportion of endoscopic screening was 93.4%.
The NCSP-GC has contributed to an increase in early detection and a decrease in the gastric cancer mortality. The proportions of gastric cancer with localized and regional stages have increased
and reached about 85% of newly diagnosed gastric cancer. Accordingly, the number of patients who can be treated by minimally invasive treatment including endoscopic resection or laparoscopic gastrectomy has increased. After the implementation of NCSPGC, there was a significant decrease in the gastric cancer mortality. The 5-year relative survival rate for gastric cancer in Korea has dramatically increased, rising from 43.9% in the 1993-1995 period to 78.4% for 2018–2022.
Despite its success, the NCSP-GC faces new challenges. Gastric cancer incidence in Korea has been declining since 2011, partly due to a decrease in H. pylori prevalence and the increased detection and removal of precancerous gastric adenomas. These trends suggest the need to transition from universal screening to a more efficient, risk-stratified model. Future screening strategies will likely be modified based on individual risk factors, primarily H. pylori infection and the presence of premalignant conditions like gastric atrophy and intestinal metaplasia.
TDDW–JDDW–KDDW
Upper GI: National Strategy for Gastric Cancer Control-Perspectives from Taiwan, Japan, and Korea
Multiomic Perspectives on Gastric Carcinogenesis: Modeling Host–Microbe–Environment Interactions
Tzu-Chan Hong
Department of Internal Medicine, National Taiwan University Hospital Cancer Center, National Taiwan University College of Medicine, Taipei, Taiwan
Gastric cancer arises in a complex biological landscape shaped by environmental exposures, microbial communities, and host genomic features. In this talk, I will present a multiomic framework that integrates genomic, transcriptomic, proteomic, phosphoproteomic, and microbiome data to systematically dissect the etiology and heterogeneity of gastric cancer. Leveraging paired tumor and non-malignant adjacent tissues from 154 East Asian patients, our study captures carcinogenic trajectories driven by both exogenous factors, including Helicobacter pylori infection and dietary carcinogens, and endogenous remodeling processes. We delineate spatially resolved tumor subtypes
along anatomical axes of the stomach, and highlight distinct microbial signatures and kinase activity profiles associated with immune and oncogenic pathways. Notably, a simplified proteogenomic risk score incorporating immune subtype and carcinogen exposure provides independent prognostic value beyond clinical staging, offering a precision medicine tool for risk stratification. This integrative approach not only deepens our understanding of gastric tumorigenesis but also illustrates how host–microbe–environment interactions shape cancer evolution, with implications for early detection, classification, and therapy.
TDDW–JDDW–KDDW
Upper GI: National Strategy for Gastric Cancer Control-Perspectives from Taiwan, Japan, and Korea
Fumiaki Ishibashi
Department of Gastroenterology, International University of Health and Welfare Ichikawa Hospital, Chiba, Japan
In Japan, an organized screening program has been implemented to detect gastric cancer (GC) in healthy individuals aged 50 and older. However, the prevalence of Helicobacter pylori (H. pylori, Hp) has changed significantly over the past few decades due to improved hygiene and the widespread use of eradication therapy.
We conducted a systematic review of published studies and applied a meta-regression model to integrate the data. Our analysis of a cohort of 46,490 individuals born between 1930 and 2011 in Japan revealed that the Hp-uninfected rate was 86.1%. By birth year, the uninfected rates were 38.6% for those born in 1950, 72.1% for those born in 1970, and 87.4% for those born in 1990. These findings indicate a rapid decline in Hp prevalence among the generations currently or soon eligible for endoscopic screening.
In such low-infection cohorts, H. pylori-naïve gastric cancers (HpNGCs) may become the primary screening targets. However, our meta-analysis of 248,482 individuals found that the prevalence of HpNGC was only 0.015%, with an incidence of just 1.40 per 1,000 person-years. Furthermore, our large-scale cohort study involving 222,656 Hpnaïve individuals showed that 71.4% of poorly differentiated/signet-ring cell (por/sig) lesions, a biologically aggressive subtype, were already at stage pT1b or deeper at the time of diagnosis, with 57.1% requiring surgical treatment. A central review confirmed that none of these por/sig lesions had been missed in previous endoscopic examinations.
Collectively, these results suggest that periodic endoscopic screening may no longer be effective in detecting GC in Hp low-infection cohorts, prompting a need to reconsider current screening strategies.
TDDW–JDDW–KDDW
Upper GI:
National Strategy for Gastric Cancer Control-Perspectives from Taiwan, Japan, and Korea
Jae Yong Park
Division of Gastroenterology, Department of Internal Medicine, Chung-Ang University College of Medicine, Seoul, Korea
Endoscopic submucosal dissection (ESD) is a widely adopted treatment for gastric neoplasms, but national-level data on how procedural volume affects clinical outcomes have been limited. In this presentation, I will share findings from a large-scale population-based study using Korean National Health Insurance Service data, which examined the impact of hospital volume on the safety and quality of gastric ESD.
We identified over 94,000 ESD procedures for gastric cancer or adenoma performed between 2011 and 2017. Hospitals were categorized into high-, medium-, and low-volume centers based on ESD case thresholds. The study focused on major postprocedural adverse events, including hemorrhage, perforation, pneumonia, and 30-day mortality,
as well as the need for additional resection. To address potential confounding, we applied inverse probability of treatment weighting.
Our findings revealed a significant association between procedural volume and adverse event rates. High- and medium-volume centers showed a significantly lower risk of composite complications compared to low-volume centers. This trend was consistent for individual outcomes such as hemorrhage, perforation, and pneumonia, though not for additional resection rates.
The significant association between the procedural volume and clinical outcomes suggests that the outcomes of gastric ESD should be systemically monitored in a nationwide level to ensure the quality and safety of procedures.
Lower GI: Nationwide Approaches to Optimize Detection and
in Taiwan, Japan, and Korea
Jae Myung Cha
Department of Internal Medicine, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea
Colorectal cancer (CRC) is the second most commonly diagnosed cancer and the third leading cause of cancer-related death in Korea. To address this public health burden, the Korean National Cancer Screening Program (NCSP) has implemented annual fecal immunochemical testing (FIT) for individuals aged ≥50 years since 2004. While FIT is cost-effective and accessible, its limited sensitivity for advanced adenomas and CRC has prompted growing concerns regarding its long-term effectiveness. Consequently, a paradigm shift toward primary colonoscopy screening is under active discussion by national health authorities, supported by international evidence suggesting superior diagnostic yield and potential mortality reduction with colonoscopy. However, transitioning to colonoscopy as the first-line screening modality presents substantial challenges, including limited endoscopic capacity, inter-operator variability, and procedural risks. In this context, artificial intelligence (AI)–assisted colonoscopy—particularly computer-aided detection (CADe) and diagnosis (CADx) systems—
has emerged as a promising solution to enhance adenoma detection rates, reduce miss rates, and improve overall quality assurance in endoscopic practice. Recent studies conducted in both Western and Asian populations have demonstrated that AI tools can significantly augment the performance.
Despite its technological promise, the widespread integration of AI into routine CRC screening is still in its infancy due to lack of reimbursement, uncertainty around costeffectiveness, and concerns regarding explainability and regulatory oversight.
As Korea contemplates a nationwide shift in screening strategy, a comprehensive evaluation of both population-based colonoscopy screening and AI-assisted colonoscopy is urgently needed. This topic aims to provide an updated overview of the current CRC screening practices in Korea, evaluate the feasibility and implications of adopting colonoscopy as a primary tool, and explore the evolving role of AI in shaping the future of population-based CRC prevention.
Lower GI: Nationwide Approaches to Optimize Detection and Treatment of Early-Stage Neoplasms in Taiwan, Japan, and Korea
Hiroaki Ikematsu
Department of Advanced Gastrointestinal Endoscopy, Advanced Clinical Research Center, Institute of Medical Science, The University of Tokyo, Tokyo, Japan
Department of Gastroenterology, IMSUT Hospital, Tokyo, Japan
The standard treatment for colorectal T1 cancer is surgical resection with lymph node dissection, due to an approximately 10% risk of lymph node metastasis (LNM). Based on investigations of LNM risk factors, lesions with an extremely low risk of metastasis are now considered suitable for endoscopic resection.
Accurate diagnosis of high-risk T1 colorectal cancers with potential lymph node metastasis is made possible through advanced endoscopic techniques, including image-enhanced endoscopy with NBI or BLI for JNET classification, and magnifying chromoendoscopy for pit pattern classification. These diagnostic modalities offer high accuracy, enabling appropriate treatment selection. In recent years, detailed evaluations of pathological findings have been undertaken with the aim of further expanding the indications for endoscopic resection. Meanwhile, with the advancement of techniques such as endoscopic submucosal dissection (ESD),
the concept of “total biopsy” has emerged, where the decision to proceed with additional surgery is made based on pathological evaluation after endoscopic resection. However, approximately 20% of T1 colorectal cancers treated endoscopically present with a positive vertical margin. Therefore, endoscopic resection should be avoided as the primary therapeutic approach in such cases.
Surgical resection for rectal cancer is highly invasive, and some patients reject surgical treatment. A clinical trial (JCOG1612) is currently underway to evaluate whether adjuvant chemoradiotherapy following local excision is non-inferior to standard surgical resection. Additionally, new techniques such as per anal endoscopic myectomy and fullthickness resection—both aiming for negative vertical margins—have recently been reported. When combined with adjuvant chemoradiotherapy, these approaches hold promise for avoiding radical rectal surgery in rectal T1 cancer.
GI: Nationwide
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
The widespread adoption of colorectal cancer (CRC) screening in Taiwan has increased the detection of T1 CRC, shifting clinical focus toward balancing effective treatment with quality of life. While endoscopic resection can cure many cases, the risk of lymph node metastasis (LNM) in a subset of patients remains a crucial determinant for subsequent surgical intervention. The challenge lies in optimizing risk stratification to avoid overtreatment—leading to unnecessary surgery and postoperative morbidity—or undertreatment, which may result in missed metastases and cancer recurrence.
This presentation will review current risk stratification models based on histopathological features such as depth of submucosal invasion, lymphovascular invasion, and tumor differentiation will be discussed, with emphasis on their limitations and predictive accuracy for LNM. The clinical and economic burden of overtreatment and undertreatment will then be examined. Overtreatment, often driven by high false-positive
rates of current criteria, contributes to increased healthcare costs and compromises patient quality of life. Conversely, under-treatment carries the risk of recurrence and poor oncological outcomes.
Next, the talk will summarize the current diagnostic modalities for assessing LNM in T1 CRC, including histopathology, and emerging liquid biopsy approaches such as circulating tumor DNA, exosomal RNA, and proteomic signatures. The limitations of conventional methods and the potential role of molecular diagnostics and artificial intelligence in improving predictive accuracy will be addressed.
Finally, the presentation will outline the future roadmap for T1 CRC management in Taiwan, focusing on integrative strategies that combine clinicopathological, and molecular biomarkers to refine risk stratification. Prospects for incorporating machine learning models, real-world data validation, and regional collaboration across Taiwan, Japan, and Korea will be highlighted as essential steps toward individualized treatment and optimized outcomes.
TDDW–JDDW–KDDW
Lower GI: Nationwide Approaches to Optimize Detection and Treatment of Early-Stage Neoplasms in Taiwan, Japan, and Korea
Teppei Akimoto
Division of Research and Development for Minimally Invasive Treatment, Cancer Center, Keio University School of Medicine, Tokyo, Japan
Colorectal endoscopic submucosal dissection (ESD) is a minimally invasive technique that enables high R0 resection rates regardless of lesion size. However, the procedure remains technically demanding, limiting its widespread adoption and prompting the development of various supportive devices and techniques. Among the procedural steps, creation of the mucosal flap is widely recognized as the most technically challenging, and traction is considered a key component in overcoming this difficulty.
Various traction methods and devices have been introduced for colorectal ESD, including dedicated traction devices, the tunneling method, and the pocket-creation method. Recently, innovative approaches utilizing buoyancy and water
jet pressure under saline conditions—collectively referred to as the water pressure method—have attracted increasing attention. Our team initially developed and reported this method to address duodenal tumors, which are among the most technically demanding targets for ESD. We have since expanded and refined the technique for application to other gastrointestinal sites.
In colorectal ESD, the water pressure method has demonstrated notable efficacy by improving endoscopic visualization and potentially reducing procedure time. In this lecture, I will share practical tips and strategies to facilitate safe and effective colorectal ESD, with a focus on traction techniques and device selection.
Lower GI: Nationwide Approaches to Optimize Detection and Treatment
Early-Stage
in Taiwan, Japan, and Korea
Bun Kim
Center for Colorectal Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Korea
Colorectal cancer (CRC) remains one of the most prevalent malignancies worldwide and was the fourth most common cancer in the Republic of Korea in 2019. The mortality rate of CRC has shown a steady increase in recent years, emphasizing the importance of early detection and effective screening programs. Among the available screening modalities, the fecal immunochemical test (FIT) is widely adopted because of its simplicity, noninvasiveness, and cost-effectiveness. However, despite its extensive use, limited data are available on the long-term outcomes of individuals with positive FIT results, particularly in relation to compliance with subsequent screening. To address this gap, we conducted a population-based study using the National Health Insurance Service Big Data database, which allowed comprehensive evaluation of CRC incidence over an extended follow-up period.
In this study, we analyzed 1,737,633 individuals who underwent FIT screening in 2009, identifying 101,143 (5.82%) with positive FIT results. Over a 10year follow-up period, 4,395 of these participants (4.35%) were diagnosed with CRC. Importantly, individuals who participated in a second round of screening demonstrated a markedly lower 5-year cumulative CRC incidence (approximately 1.25%) compared with those who did not (approximately 3.75%). Non-compliance with follow-up screening was associated with a 2.8-fold higher CRC risk. These findings highlight the critical role of followup adherence in reducing CRC incidence among FIT-positive individuals and underscore the need for targeted strategies and public health interventions to enhance compliance with subsequent screening rounds in this high-risk group.
TDDW–JDDW–KDDW
Lower GI: Nationwide Approaches to Optimize Detection and Treatment of Early-Stage Neoplasms in Taiwan, Japan, and Korea
Hsu-Hua Tseng
Division of Gastroenterology & Hepatology, Department of Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
Background and aims: Early-onset colorectal cancer (CRC) is increasing globally. While the United States has lowered the age of initiation of screening to 45 years, other countries still start screening at 50 years of age. In Taiwan, the incidence of CRC has declined in 55- to 74-year-olds after the initiation of screening, but still increased in those 50-54 years of age, potentially due to the rising precancerous lesion incidence in 40- to 49-year-olds. This study aimed to explore the chronological trend of the prevalence of colorectal advanced neoplasms (AN) in the screening population 40–54 years of age.
Methods: We retrospectively analyzed a screening colonoscopy cohort for prevalence of AN in average-risk subjects 40–54 years of age from 2003 to 2019. Logistic regression was used to distinguish cohort effect from time-period effect on the prevalence of AN.
Results: In total, 27,805 subjects (52.1% male)
were enrolled. There were notable increases in prevalence of AN in all 3 age groups during the 17year span, but these were more rapid in those 40–44 years of age (0.99% to 3.22%) and 45–49 years of age (2.50% to 4.19%). Those 50–54 years of age had a higher risk of AN (adjusted odds ratio [aOR], 1.62; 95% confidence interval [CI], 1.19–2.19) in 2003–2008 but not in later periods (2009–2014: aOR, 1.08; 95% CI, 0.83–1.41; 2015–2019: aOR, 0.76; 95% CI, 0.56–1.03) when compared with those 45–49 years of age.
Conclusion: The prevalence of AN in those 40–54 years of age increased in the Taiwanese population, with a later birth cohort having a higher prevalence of AN. However, the prevalence of AN in those 45–49 years of age increased more remarkably and approximated that in those 50–54 years of age, which may justify earlier initiation of CRC screening in those 45 years of age.
TDDW–JDDW–KDDW
Liver:
Hepatocellular Carcinoma Surveillance in Taiwan, Japan and Korea: Unmet Needs and Possible Solutions
Hepatocellular Carcinoma Surveillance in Taiwan: Current Practice and Future Direction
Sheng-Nan Lu
Division of Hepato-Gastroenterology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
Hepatocellular carcinoma (HCC) is currently the fourth most common cancer and the second leading cause of cancer-related deaths. Over the past two decades, there has been a notable shift in the distribution of HCC stages: an increase in earlystage diagnoses, a decrease in intermediate-stage cases, and a stabilization of advanced-stage cases. Approximately one-third of patients continue to be diagnosed at an advanced stage. The median survival for patients diagnosed at BCLC stage 0 is 9.9 years, while those at stage A have a median survival of 6.6 years. In contrast, patients diagnosed at stages C and D have a median survival of less than one year. Therefore, a key objective of HCC surveillance is to prevent patients from being diagnosed at advanced stages.
The primary etiological factors for HCC differ by gender: hepatitis B virus (HBV) is the leading cause in men, while hepatitis C virus (HCV) predominates among women. Approximately 70%–75% of patients are positive for HBsAg and anti-HCV. In 2020, a national screening program for HBV and HCV was launched, targeting individuals born between 1941 and 1980, achieving a screening rate of 70% or more. This year, the screening will be expanded to include all residents born before the universal HBV vaccination in 1986. This initiative effectively
identifies individuals at risk due to viral infections. However, there has not yet been a systematic strategy to identify the remaining one-fourth of patients who belong to non-viral risk groups. Fortunately, the Adult Health Service for individuals aged 30 and older encompasses many risk factors associated with Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD), which should serve as a foundation for a national control program.
HCC surveillance utilizing ultrasonography and alpha-fetoprotein (AFP) testing for high-risk groups has been standard practice for over 30 years, demonstrating significantly better sensitivity than reported in published meta-analyses. PIVKA II testing has also been reimbursed since 2020, although it is currently limited to certain higher-risk patients. There remains room for improvement in screening tools, such as adjusting US parameters to overcome fatty liver backgrounds, lowering the AFP cutoff, and refining the interpretation of false positives for PIVKA II. Enhancing awareness and accessibility of HCC surveillance for high-risk groups should be a central focus of national policy.
In conclusion, a comprehensive, epidemiologybased, and national policy-oriented HCC surveillance program is essential to prevent diagnoses at advanced stages of the disease.
Liver:
Hepatocellular Carcinoma Surveillance in Taiwan, Japan and Korea: Unmet Needs and Possible Solutions
Hepatocellular
Ryosuke Tateishi
Department of Gastroenterology, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan
Japan pioneered organized hepatocellular carcinoma (HCC) surveillance and continues to achieve world-leading early detection rates and outcomes. The current Japan Society of Hepatology guidelines recommend semiannual abdominal ultrasonography combined with three biomarkers—α-fetoprotein (AFP), AFP-L3, and des-γ-carboxy prothrombin (DCP/PIVKA-II)—with 3–4-month intervals for the highest-risk strata. National reimbursement for all three biomarkers has facilitated broad implementation.
However, major shifts in disease etiology are challenging the performance of this program. While viral hepatitis–related HCC is declining due to widespread HCV eradication, non-viral HCC related to metabolic dysfunction–associated steatotic liver disease (MASLD) and alcohol use is rising. Key issues include: (1) a growing proportion of patients outside surveillance programs due to the absence of established workflows for non-viral
liver disease; (2) reduced ultrasound sensitivity in obese populations; and (3) competing health risks in MASLD patients, such as cardiovascular disease and other malignancies, which diminish the overall impact of surveillance.
Potential solutions include implementing riskstratified surveillance pathways that integrate clinical variables with biomarkers, introducing standardized quality assessment for ultrasound adequacy, and adopting abbreviated MRI for patients in whom ultrasound is unsuitable. These priorities align with global recommendations to modernize HCC control through integrated prevention, early detection, and linkage to curative therapies. Comparative discussion with Taiwan and Korea should aim to harmonize risk stratification frameworks, assess biomarker and insurance policies, and design prospective multicenter trials to validate surveillance strategies across prevalent etiologies in East Asia.
TDDW–JDDW–KDDW
Liver:
Hepatocellular Carcinoma Surveillance in Taiwan, Japan and Korea: Unmet Needs and Possible Solutions
Won Sohn
Division of Gastroenterology, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea
Hepatocellular carcinoma (HCC) is indolent and asymptomatic at an early stage, and approximately half of HCC cases are diagnosed at an advanced tumor stage. Thus, it is necessary to determine and monitor the high-risk groups for liver disease-related complications, including HCC, through surveillance programs aimed at reducing liver-related mortality. A meta-analysis revealed that HCC surveillance was beneficial in detecting early-stage tumors, increasing the chance of curative therapy, and improving overall survival in cirrhotic patients. Surveillance is the repeated screening of patients with the at-risk population. An intervention is considered effective if it provides an increase in longevity of about 100 days, i.e., about 3 months. Although the levels were set years ago, and may not be appropriate today, interventions that can be achieved at a cost of less than about $50,000/year of life gained are considered cost-effective. HCC surveillance is recommended based on the cost-effectiveness considering threshold incidence for efficacy of surveillance according to the etiology of chronic liver disease and presence of cirrhosis (below table). Most guidelines recommend HCC surveillance in high-risk groups (cirrhosis of any cause or chronic hepatitis B [CHB]) using ultrasonography and/or serum alphafetoprotein (AFP) every 6 months. However, there is a lack of existing clinical evidence on the effect of HCC surveillance on chronic liver disease prognosis, and
there are only two randomized clinical trials on HCC surveillance in Chinese patients with CHB. Besides, one of those randomized trials used serum AFP only for HCC surveillance and did not show a reduction in mortality in patients who underwent surveillance. In addition, the adherence to HCC surveillance is poor even in high-risk groups.
HCC surveillance is particularly crucial for reducing the disease burden and improving the prognosis of patients with chronic liver disease. In South Korea, HCC is the 5th most common cancer and 2nd highest cause of cancer death. The Korean government has been running the national cancer screening program for the whole population since 1999. The National Liver Cancer Screening Program (NLCSP) for HCC surveillance has been conducted in South Korea since 2003. From 2003 onwards, the NLCSP in Korea began to provide ultrasonography and serum AFP for HCC surveillance of patients aged ≥40 years with CHB, CHC, or liver cirrhosis. Repeat screening for HCC surveillance was recommended every 6 months from 2003–2010, every 12 months from 2011–2015, and every 6 months since 2016. HCC surveillance using the national screening program in patients with chronic viral hepatitis or liver cirrhosis provides better opportunity for curative treatment for HCC and improves overall survival in South Korea.
Hepatitis B virus (HBV) infection is a global health concern that causes acute and chronic infections that can progress to liver cirrhosis, HCC, and liver failure, with eventual death. To increase the early detection of HCC, reduce complications among the patients with CHB, and improve overall survival. HCC surveillance is recommended for CHB patients with high-risk group which consisted of cirrhosis or Asians aged over 40 years. This is because the annual incidence of HCC in Asian patients with CHB irrespective of cirrhosis begins to exceed 0.2% after age 40 when surveillance for HCC is cost-effective.
The risk of HCC in CHB depends on viral activity (HBeAg, HBV DNA), disease activity (ALT level), fibrotic burden, and host factors (age, gender, family history, diabetes, alcohol, and smoking). The prediction of HCC risk in patients with CHB has been stratified using the risk score models based on above-mentioned factors.
Most of risk prediction scores for HCC in untreated patients were derived from Asian cohorts. Host factors (age and gender) were included in all models in untreated patients. Fibrotic burden was also included in all models. However, fibrotic burden was assessed in various method such as presence of cirrhosis, platelet count, albumin level, liver stiffness measurement (LSM), and spleen size. Viral factors (high level of HBV DNA, and HBeAg positivity), and disease activity (high level of ALT) were included in the risk prediction model in untreated patients. The accuracy of prediction for HCC development over 5–10 years ranged between 0.76 and 0.92, which was presented by the area under the receiver operating characteristic curve (AUROC).
Nowadays, use of oral antiviral agents (nucleos(t)ide analogue, NA) has been established as the standard treatment for CHB. The use of antiviral agents suppresses HBV replication and decreases hepatic inflammation. Furthermore, longterm use of antiviral agents can improve advanced fibrosis or cirrhosis in the histologic findings. There is no question about the role of preventive effect of antiviral agents on the reducing risk of HCC in patients with CHB. The use of antiviral agents significantly reduces the risk of HCC in CHB compared to patients with no use of antiviral agents.
There are several prediction models for HCC risk
in CHB patients receiving antiviral agents. Most of them were derived from Asia, but PAGE-B model was made based on Caucasian patients. Host factors (age and gender) and fibrotic burden were included in all models in CHB patients receiving antiviral agents. Some models included However, viral factors (HBV DNA, and HBeAg), and disease activity (ALT) are not included in the models with use of antiviral agents. The AUROC for HCC development over 5–10 years ranged between 0.76 and 0.86.
Recently, a paradigm shift from interferonbased to direct-acting antiviral (DAA) treatments for chronic hepatitis C (CHC) occurred. Recent metaanalyses have shown that DAA therapy reduces the risk of HCC, decompensation, and mortality in patients with CHC. Sustained virological response (SVR) to DAA treatment in cirrhotic patients with CHC improved portal hypertension and reduced the hepatic venous pressure gradient. SVR to DAA treatment decreased the risk of HCC in patients with CHC.
There is no doubt of HCC surveillance in CHC patients with cirrhosis in terms of cost-effectiveness. However, there is a lack of HCC surveillance in noncirrhotic patients achieving SVR. Some studies showed that HCC surveillance might be useful in patients with advanced fibrosis (F3). However, liver biopsy is invasive and not widely used in real practice. It is needed to determine high risk group in non-cirrhotic patients using noninvasive fibrosis marker. A study showed that the post SVR state with FIB-4 index with >3.25 had 2.16% of HCC incidence which had cost-effectiveness for HCC surveillance.
Metabolic dysfunction-associated steatotic liver disease (MASLD) is a chronic liver disease, which is defined as intrahepatic triglyceride content of >5%. It has become widespread with the increasing prevalence of obesity and metabolic syndrome. The spectrum of MASLD includes simple steatosis, metabolic dysfunction-associated steatohepatitis (MASH), fibrosis, and cirrhosis. It’s reasonable to include MASH-cirrhosis as an at-risk population for HCC surveillance. However, HCC can develop
in MASLD without advanced fibrosis or cirrhosis. A study reported that 30% of MASLD-HCC developed in the background of no cirrhosis. Unlike viral hepatitis, the risk factors for HCC development are unclear in patients with MASLD/MASH.
Recent studies showed that genetic polymorphisms (PNPLA3, MBOAT7, TM6SF2, and GCKR) that are associated with hepatic fat content predicted HCC development in patients with MASLD. Polygenic risk score which consists of several genetic polymorphisms was suggested as a prediction model for MASLD-HCC development. However, the diagnostic accuracy is still not high. Further studies are needed to clarify the precise risk factors for MASLD-HCC. It is not difficult to determine an at-risk population for HCC development in patients with non-cirrhotic MASLD.
References:
1. Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005 Nov;42(5):1208–36.
2. Della Corte C, Colombo M. Surveillance for hepatocellular carcinoma. Semin Oncol. 2012 Aug;39(4):384–98.
3. Sohn W, Kang D, Kang M, Guallar E, Cho J, Paik YH. Impact of nationwide hepatocellular carcinoma surveillance on the prognosis in patients with chronic liver disease. Clin Mol Hepatol. 2022 Oct;28(4):851–63.
4. Sohn W, Lee YS, Lee JG, An J, Jang ES, Lee DH, et al. A Survey of Liver Cancer Specialists’ Views on the National Liver Cancer Screening Program in Korea. J Liver Cancer. 2020 Mar;20(1):53-59.
5. Sohn W, Cho JY, Kim JH, Lee JI, Kim HJ, Woo MA,
et al. Risk score model for the development of hepatocellular carcinoma in treatment-naïve patients receiving oral antiviral treatment for chronic hepatitis B. Clin Mol Hepatol. 2017 Jun;23(2):170–8.
6. Chen Q, Ayer T, Adee MG, Wang X, Kanwal F, Chhatwal J. Assessment of Incidence of and Surveillance Burden for Hepatocellular Carcinoma Among Patients With Hepatitis C in the Era of Direct-Acting Antiviral Agents. JAMA Netw Open. 2020 Nov 2;3(11):e2021173.
7. Farhang ZH, Wong WWL, Sander B, Bell CM, Mumtaz K, Kowgier M, et al. Cost Effectiveness of Hepatocellular Carcinoma Surveillance After a Sustained Virologic Response to Therapy in Patients With Hepatitis C Virus Infection and Advanced Fibrosis. Clinical Gastroenterology and Hepatology. 2019 Aug;17(9):1840-1849. e16.
8. Sohn W, Lee HW, Lee S, Lim JH, Lee MW, Park CH, et al. Obesity and the risk of primary liver cancer: A systematic review and meta-analysis. Clin Mol Hepatol. 2021 Jan;27(1):157–74.
9. Bianco C, Jamialahmadi O, Pelusi S, Baselli G, Dongiovanni P, Zanoni I, et al. Non-invasive stratification of hepatocellular carcinoma risk in non-alcoholic fatty liver using polygenic risk scores. Journal of Hepatology. 2021 Apr;74(4):775–82.
10. Sohn W, Lee YS, Kim SS, Kim JH, Jin YJ, Kim GA, et al. KASL clinical practice guidelines for the management of metabolic dysfunctionassociated steatotic liver disease 2025. Clin Mol Hepatol. 2025;31(Suppl):S1-S31.
TDDW–JDDW–KDDW
Liver: Hepatocellular Carcinoma Surveillance in Taiwan, Japan and Korea: Unmet Needs and Possible Solutions
Shang-Chin Huang
Department of Internal Medicine, National Taiwan University Hospital Bei-Hu Branch, Taipei, Taiwan
Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
Chronic hepatitis B (CHB) remains a major global health burden, with outcomes strongly influenced by host metabolic status. In our largescale cohort studies involving thousands of HBeAgpositive and -negative patients, we demonstrated that metabolic dysfunctions such as diabetes and obesity significantly increase the risks of cirrhosis, hepatocellular carcinoma (HCC), and mortality. Paradoxically, the presence of simple hepatic steatosis was consistently associated with favorable outcomes, including accelerated HBsAg loss and reduced incidence of cirrhosis, HCC, liver-related, and all-cause mortality. These findings suggest that steatosis exerts effects distinct from other metabolic comorbidities in CHB. To further dissect underlying
mechanisms, we established an in vitro model by inducing steatosis in HepG2.2.15 cells with oleic acid. Consistent with clinical observations, steatotic hepatocytes showed a marked reduction in HBsAg secretion with a dose-dependent relationship. Preliminary mechanistic exploration revealed that this effect is probably mediated, at least in part, through the inhibition of autophagy, implicating a potential interplay between lipid metabolism and viral protein turnover. Together, these data highlight the paradoxical role of hepatic steatosis in CHB progression. Investigating this complex biology may provide new insights for therapeutic strategies in patients with CHB.
Liver:
Hepatocellular Carcinoma Surveillance in Taiwan, Japan and Korea: Unmet Needs and Possible Solutions
Takuma Nakatsuka
Department of Gastroenterology, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan
Introduction: Steatotic liver disease (SLD) is a growing global health concern, and identifying patients at high risk of developing hepatocellular carcinoma (HCC) remains challenging. While liver fibrosis is a well-established risk factor for HCC, other histopathological features may also contribute to hepatocarcinogenesis. Deep learning (DL) and digital pathology have shown promise in analyzing complex tissue patterns and identifying novel features associated with disease progression. We aimed to develop a DL model based on digital pathology to predict future HCC development in patients with SLD, using non-tumorous liver biopsy specimens obtained prior to HCC onset.
Methods: This study utilized data from the STEAtotic Liver registry for invesTigating clinical outcomes including HCC (STEALTH study), a nationwide, multicenter, biopsy-based cohort of Japanese patients with SLD. A total of 639 patients who remained HCC-free for ≥7 years post-biopsy (non-HCC group) and 46 patients who developed HCC <7 years post-biopsy (HCC group) were included. Paired cases from both groups, matched by biopsy date and institution, were used to train the DL model, while the remaining non-paired cases were used for validation. The DL model, based on convolutional neural networks (CNNs), was trained using 28,000 image tiles cropped from hematoxylin and eosin-stained whole-slide images of the paired cases. Five-fold cross-validation was performed, and
model performance was further evaluated using the non-paired cases. Predictive performance was compared with a logistic regression model using fibrosis stage as a predictor.
Results: In cross-validation with paired cases, the DL model achieved an accuracy of 81.0% and an area under the receiver operating characteristic curve (AUC) of 0.80 for predicting HCC development. Validation using non-paired cases also demonstrated good performance, with an accuracy of 82.3% and an AUC of 0.84. These results were comparable to those of the fibrosis-based logistic regression model, which achieved accuracy of 78.2% and an AUC of 0.81 in non-paired cases. Notably, the DL model successfully identified HCC development in patients with mild fibrosis. Saliency maps derived from explainable artificial intelligence revealed that features such as nuclear atypia, a high nuclear-tocytoplasmic ratio, immune cell infiltration, fibrosis, and lack of large fat droplets were associated with HCC prediction.
Conclusion: This study demonstrates the potential of DL-based histopathological analysis of liver biopsies to predict future HCC development in patients with SLD. The ability of the DL model to capture subtle histological features beyond fibrosis highlights its potential for identifying early signs of hepatocarcinogenesis, even in patients with mild fibrosis.
Liver:
Hepatocellular Carcinoma Surveillance in Taiwan, Japan and Korea: Unmet Needs and Possible Solutions
miR-660-5p and miR-125a-5p
Young Chang
Institute for Digestive Research, Digestive Disease Center, Department of Internal Medicine, Soonchunhyang University College of Medicine, Seoul, Korea
Liver fibrosis is associated with changes in microRNA (miRNA) expression, identifying these miRNAs could provide insights into potential therapeutic targets. This study aims to evaluate the therapeutic potential of specific miRNAs in modulating the progression of liver fibrosis.
Next-generation sequencing (NGS) was employed to analyze circulating miRNAs correlated with liver fibrosis stages in a human cohort from liver biopsies (n = 20). Mice with steatohepatitis were divided into control and treatment groups, each administered specific miRNA modulators. An in vitro cell model using co-cultured Huh7 and LX-2 cells, treated with free fatty acids and LPS to simulate steatohepatitis, supplemented the in vivo experiments.
NGS analysis highlighted significant differences
in the expressions of miR-660-5p and miR-125a5p across different stages of liver fibrosis. In vivo, treatment with miR-660-5p and miR-125a-5p antagonists (3 mg/kg, twice weekly for 12 weeks) significantly reduced liver fibrosis, decreasing markers such as collagen 1A, α-SMA, fibronectin, and TGF-β at the protein level. These findings were supported by liver histologic assessment using Sirius Red and α-SMA immunohistochemistry staining. Similar reductions in fibrosis markers at both protein and mRNA levels were observed in the steatohepatitis cell model, demonstrating the consistent.
This study confirms the potential of miR660-5p and miR-125a-5p antagonists as effective treatments for liver fibrosis, significantly reducing fibrosis markers in both animal and cell models.
TDDW–JDDW–KDDW
Pancreas
Keiji Hanada
Endoscopy Center, JA Onomichi General Hospital, Hiroshima, Japan
Pancreatic cancer remains one of the most lethal malignancies worldwide, largely due to the difficulty of early diagnosis and the lack of standardized, population-based screening programs. In Japan, where the 5-year survival rate has historically been low, significant progress has been made through a series of pioneering initiatives. The publication of the Clinical Practice Guidelines for Pancreatic Cancer by the Japan Pancreas Society in 2006 marked a turning point, identifying key risk factors such as diabetes mellitus, family history, chronic pancreatitis, intraductal papillary mucinous neoplasm (IPMN), and smoking. Building on this foundation, Japan has led the way in developing community-based early detection programs that leverage regional medical networks to target high-risk individuals. These efforts have yielded promising results, including increased rates of early diagnosis, higher resection rates, and
improved long-term survival. Japan’s experience demonstrates the feasibility and effectiveness of a risk factor–based approach to early pancreatic cancer detection. To further accelerate this national effort, several key developments are underway: refinement of diagnostic risk factors; better identification of indirect imaging findings (such as main pancreatic duct dilation, focal pancreatic atrophy, and pancreatic cysts); standardized surveillance protocols for high-risk individuals; advancement in pathological diagnosis using modalities such as endoscopic ultrasound (EUS) and duodenoscopy; development of novel tumor markers; and research into biomarker-based screening kits using duodenal fluid, which may be applicable during routine upper GI endoscopy. Japan’s leadership in this field offers a model for global strategies in tackling one of the most challenging cancers of our time.
TDDW–JDDW–KDDW
Wei-Chih Liao
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
Early detection of pancreatic ductal adenocarcinoma (PDAC) remains a major clinical challenge due to the deep anatomical location of the pancreas, subtle early lesions, and nonspecific symptoms. Up to 40% of pancreatic cancers smaller than 2 cm are missed on CT, and even larger tumors may escape detection because their radiologic features often mimic benign conditions.
Artificial intelligence (AI) has emerged as a transformative tool to enhance imaging-based detection. Convolutional neural networks (CNNs) trained on contrast-enhanced CT scans have demonstrated superior sensitivity compared to radiologists and can detect visually occult earlystage PDAC. A nationwide validation study showed that a CNN-based computer-aided detection system achieved 89.7% sensitivity and 92.8% specificity, with 75% sensitivity for lesions under 2 cm.
Radi_omics provides a complementary approach, converting CT images into quantitative features reflecting tumor texture and morphology. Machine learning models based on radiomic features have consistently achieved AUCs above 0.90 for PDAC discrimination, and real-world validation of a
radiomics-based CAD tool reported 91.8% sensitivity and 82.2% specificity.
AI can also detect pre-diagnostic imaging features. A 3D-CNN model identified visually occult cancers on CT up to 16 months before clinical diagnosis with strong sensitivity and specificity. More recently, CNN-transformer algorithms have shown outstanding performance on unenhanced CT, with 92.9% sensitivity and 99.9% specificity, while also differentiating between subtypes of pancreatic lesions.
Beyond imaging, AI applied to electronic health records (EHRs) enables earlier risk stratification. Transformer-based models analyzing trajectories of over six million patients achieved AUCs of 0.83–0.88 for predicting PDAC up to three years before diagnosis, with good generalizability across populations.
Collectively, these advances highlight the potential of AI as a valuable adjunct to radiologists. By improving sensitivity, standardizing detection across institutions, and enabling earlier intervention, AI may play a pivotal role in shifting PDAC diagnosis to earlier, more treatable stages.
TDDW–JDDW–KDDW
Pancreas & Biliary:
Enhancing Early Detection and Diagnosis for Pancreatic Cancer: Perspectives from Japan, Korea, and Taiwan
Exosomal Proteomics for Malignant Risk Stratification in IPMN: A Minimally
Namyoung Park
Division of Gastroenterology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
Intraductal papillary mucinous neoplasm (IPMN) of the pancreas is a precancerous lesion with the potential to progress to invasive pancreatic cancer.¹-² Although surgical resection remains the only curative modality for malignant IPMN, it is not recommended for all patients to undergo surgery due to the substantial morbidity and mortality associated with pancreatic surgery.³ Therefore, it is clinically essential to accurately identify patients with high-risk lesions to avoid both overtreatment and delayed intervention.
Imaging modalities, including contrastenhanced computed tomography, magnetic resonance imaging, and endoscopic ultrasound (EUS), are important tools for assessing the malignant risk of IPMN. Many international guidelines rely heavily on imaging findings—such as enhancing mural nodules, main pancreatic duct dilation, and cyst size—to estimate malignant potential.⁴-⁷ While these findings provide valuable anatomical information, the supporting levels of evidence are relatively low, and their diagnostic accuracy remains limited.⁸-⁹ Moreover, imaging does not necessarily reflect the biological aggressiveness of the neoplasm.
Serum biomarkers, most notably carbohydrate antigen 19-9 (CA19-9) and carcinoembryonic antigen (CEA), are widely used in clinical practice. However,
these markers demonstrate limited diagnostic performance. CA19-9 demonstrates a sensitivity of approximately 40%–50% and a specificity of less than 85% in distinguishing malignant from benign IPMN, while CEA performs even less reliably in this setting.¹⁰-¹² Accordingly, these biomarkers are insufficient as standalone indicators of invasive IPMN.
Cyst fluid analysis obtained through EUSguided fine needle aspiration (EUS-FNA) provides access to molecular and proteomic data that can help differentiate mucinous from non-mucinous cysts and identify oncogenic mutations associated with malignant transformation. Despite these advantages, EUS-FNA is an invasive procedure associated with risks such as pancreatitis, infection, and, rarely, needle tract seeding, which limits its use for routine or repeated surveillance.¹³-¹⁴ The overall incidence of tract seeding following EUSFNA for pancreatic cystic lesions has been reported to be approximately 0.3%.¹⁵ However, in patients who subsequently undergo surgical resection for IPMN, the incidence of peritoneal dissemination appears higher, reported at 2.3%, with all affected cases pathologically confirmed to have high-grade dysplasia or invasive carcinoma.¹⁶ Nevertheless, this difference was not statistically significant when compared with patients who did not undergo
preoperative EUS-FNA (4.4%, p = 0.403). For these reasons, EUS-FNA is generally reserved for cases in which imaging findings are inconclusive or when cytologic or molecular results are expected to affect clinical decision-making.⁴-⁵
Given these limitations, there is growing interest in noninvasive, biologically informative biomarkers that can accurately predict malignant transformation of IPMN. Exosomes, a class of extracellular vesicles released by virtually all cell types—including neoplastic cells—have emerged as a promising platform for biomarker discovery.¹⁷-¹⁹ These nanosized vesicles carry a diverse cargo of proteins, nucleic acids, and lipids, while maintaining relative stability.²¹ These intracellular cargos play a key role in cell-to-cell communication, and are reflective of the biological state of their cells of origin.21 Exosomes are present in various biofluids including plasma and cyst fluid, offering the possibility of serial, minimally invasive monitoring.²²-²³ Compared to conventional biomarkers, exosomal profiling provides a unique window into tumor biology. Proteomic profiling of exosomes has shown promise in early cancer detection and risk stratification. In pancreatic ductal adenocarcinoma, Melo et al. demonstrated that glypican-1 positive exosomes in serum could distinguish pancreatic cancer patients from healthy individuals and those with benign disease with high specificity, suggesting their utility in early diagnosis.²⁴ Subsequent studies have supported these findings, showing correlations between glypican-1 positive exosome levels and tumor burden, as well as enhanced diagnostic performance when combined with other biomarkers such as CD82 and CA19-9.²⁵-²⁶ More recently, Yang et al. reported that extracellular vesicle–associated MUC5AC in plasma could discriminate malignant IPMN (including those with high-grade dysplasia or invasive carcinoma) from low-risk lesions, with specificity ranging from 97% to 100%. Their results significantly outperformed current imaging-based criteria, highlighting the diagnostic power of exosomal proteomics.²⁷
These findings suggest that exosomal proteomic profiling can complement established diagnostic approaches, increasing specificity in predicting malignant risk and enabling ongoing surveillance through minimally invasive blood sampling.
However, to realize clinical integration, further research is required to validate results across larger, prospective, multicenter cohorts and to standardize exosome isolation and analysis methods. In conclusion, exosomal proteomic analysis offers a biologically informed, minimally invasive strategy for identifying malignant IPMN. It has the potential to refine patient selection for surgery, reduce unnecessary procedures, and support longitudinal monitoring. Future efforts combining exosomal biomarkers with clinical and imaging data may revolutionize the management of IPMN and improve patient outcomes.
References:
1. Valsangkar NP, Morales-Oyarvide V, Thayer SP, et al. 851 resected cystic tumors of the pancreas: a 33-year experience at the Massachusetts General Hospital. Surgery 2012;152(3 Suppl 1):S4-S12. (In eng). DOI: 10.1016/j.surg.2012.05.033.
2. Winter JM, Cameron JL, Lillemoe KD, et al. Periampullary and pancreatic incidentaloma: a single institution’s experience with an increasingly common diagnosis. Ann Surg 2006;243(5):673-683. (In eng). DOI: 10.1097/01. sla.0000216763.27673.97.
3. Hirono S, Yamaue H. Surgical strategy for intraductal papillary mucinous neoplasms of the pancreas. Surg Today 2020;50(1):50-55. (In eng). DOI: 10.1007/s00595-019-01931-5.
4. Ohtsuka T, Fernandez-Del Castillo C, Furukawa T, et al. International evidence-based Kyoto guidelines for the management of intraductal papillary mucinous neoplasm of the pancreas. Pancreatology 2024;24(2):255-270. (In eng). DOI: 10.1016/j.pan.2023.12.009.
5. European evidence-based guidelines on pancreatic cystic neoplasms. Gut 2018;67(5):789804. (In eng). DOI: 10.1136/gutjnl-2018-316027.
6. Elta GH, Enestvedt BK, Sauer BG, Lennon AM. ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts. Am J Gastroenterol 2018;113(4):464-479. (In eng). DOI: 10.1038/ajg.2018.14.
7. Vege SS, Ziring B, Jain R, Moayyedi P. American gastroenterological association institute guideline on the diagnosis and management of asymptomatic neoplastic pancreatic
cysts. Gastroenterology 2015;148(4):81922; quize12-3. (In eng). DOI: 10.1053/j. gastro.2015.01.015.
8. Pulvirenti A, Margonis GA, Morales-Oyarvide V, et al. Intraductal Papillary Mucinous Neoplasms: Have IAP Consensus Guidelines Changed our Approach?: Results from a Multi-institutional Study. Ann Surg 2019 (In eng). DOI: 10.1097/ sla.0000000000003703.
9. Tanaka M, Fernandez-del Castillo C, Adsay V, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012;12(3):183-97. (In eng). DOI: 10.1016/j.pan.2012.04.004.
10. Ciprani D, Morales-Oyarvide V, Qadan M, et al. An elevated CA 19-9 is associated with invasive cancer and worse survival in IPMN. Pancreatology 2020;20(4):729-735. DOI: https:// doi.org/10.1016/j.pan.2020.04.002.
11. Wang W, Zhang L, Chen L, et al. Serum carcinoembryonic antigen and carbohydrate antigen 19-9 for prediction of malignancy and invasiveness in intraductal papillary mucinous neoplasms of the pancreas: A meta-analysis. Biomed Rep 2015;3(1):43-50. DOI: 10.3892/ br.2014.376.
12. Kim JR, Jang J-Y, Kang MJ, et al. Clinical implication of serum carcinoembryonic antigen and carbohydrate antigen 19-9 for the prediction of malignancy in intraductal papillary mucinous neoplasm of pancreas. Journal of HepatoBiliary-Pancreatic Sciences 2015;22(9):699-707. DOI: https://doi.org/10.1002/jhbp.275.
13. Mohan BP, Madhu D, Khan SR, et al. Intracystic Glucose Levels in Differentiating Mucinous From Nonmucinous Pancreatic Cysts: A Systematic Review and Meta-analysis. J Clin Gastroenterol 2022;56(2):e131-e136. (In eng). DOI: 10.1097/ mcg.0000000000001507.
14. Lee LS. Updates in diagnosis and management of pancreatic cysts. World J Gastroenterol 2021;27(34):5700-5714. (In eng). DOI: 10.3748/ wjg.v27.i34.5700.
15. Facciorusso A, Crinò SF, Gkolfakis P, et al. Needle Tract Seeding after Endoscopic Ultrasound Tissue Acquisition of Pancreatic Lesions: A Systematic Review and Meta-Analysis. Diagnostics (Basel) 2022;12(9) (In eng). DOI:
10.3390/diagnostics12092113.
16. Yoon WJ, Daglilar ES, Fernández-del Castillo C, Mino-Kenudson M, Pitman MB, Brugge WR. Peritoneal seeding in intraductal papillary mucinous neoplasm of the pancreas patients who underwent endoscopic ultrasoundguided fine-needle aspiration: the PIPE Study. Endoscopy 2014;46(5):382-7. (In eng). DOI: 10.1055/s-0034-1364937.
17. Thery C, Zitvogel L, Amigorena S. Exosomes: composition, biogenesis and function. Nature reviews Immunology 2002;2(8):569-79. (In eng). DOI: 10.1038/nri855.
18. Raposo G, Stoorvogel W. Extracellular vesicles: exosomes, microvesicles, and friends. The Journal of cell biology 2013;200(4):373-83. (In eng). DOI: 10.1083/jcb.201211138.
19. Kahlert C, Kalluri R. Exosomes in tumor microenvironment influence cancer progression and metastasis. Journal of molecular medicine (Berlin, Germany) 2013;91(4):431-7. (In eng). DOI: 10.1007/s00109-013-1020-6.
20. Armstrong EA, Beal EW, Chakedis J, et al. Exosomes in Pancreatic Cancer: from Early Detection to Treatment. Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract 2018;22(4):737-750. (In eng). DOI: 10.1007/s11605-018-3693-1.
21. Kalluri R, LeBleu VS. The biology, function, and biomedical applications of exosomes. Science 2020;367(6478):eaau6977. DOI: 10.1126/ science.aau6977.
22. Wunsch BH, Smith JT, Gifford SM, et al. Nanoscale lateral displacement arrays for the separation of exosomes and colloids down to 20 nm. Nat Nanotechnol 2016;11(11):936-940. (In eng). DOI: 10.1038/nnano.2016.134.
23. Li Z, Tao Y, Wang X, et al. Tumor-Secreted Exosomal miR-222 Promotes Tumor Progression via Regulating P27 Expression and ReLocalization in Pancreatic Cancer. Cell Physiol Biochem 2018;51(2):610-629. (In eng). DOI: 10.1159/000495281.
24. Melo SA, Luecke LB, Kahlert C, et al. Glypican-1 identifies cancer exosomes and detects early pancreatic cancer. Nature 2015;523(7559):17782. (In eng). DOI: 10.1038/nature14581.
25. Frampton AE, Prado MM, López-Jiménez E, et al.
Glypican-1 is enriched in circulating-exosomes in pancreatic cancer and correlates with tumor burden. Oncotarget 2018;9(27):19006-19013. (In eng). DOI: 10.18632/oncotarget.24873.
26. Xiao D, Dong Z, Zhen L, et al. Combined Exosomal GPC1, CD82, and Serum CA19-9 as Multiplex Targets: A Specific, Sensitive, and Reproducible Detection Panel for the Diagnosis of Pancreatic
Cancer. Mol Cancer Res 2020;18(2):300-310. (In eng). DOI: 10.1158/1541-7786.Mcr-19-0588.
27. Yang KS, Ciprani D, O’Shea A, et al. Extracellular Vesicle Analysis Allows for Identification of Invasive IPMN. Gastroenterology 2021;160(4):1345-1358.e11. (In eng). DOI: 10.1053/j.gastro.2020.11.046.
Pancreas & Biliary: Enhancing Early Detection and Diagnosis for Pancreatic Cancer: Perspectives from Japan, Korea, and Taiwan
Chien-Jui Huang
Section of Digestive disease, Department of Internal medicine, National Cheng Kung University Hospital, Tainan, Taiwan
Pancreatic ductal adenocarcinoma (PDAC) is notoriously poor prognosis after treatments, which may be due to the lack of precise biomarkers. The incidence rate of PDAC in Taiwan was gradually increased, but the patients’ survival rates were still not improved. Surgery is still most effective therapy for PDAC. However, up to 80%–85% patients who presented as unresectable or metastatic disease at initial diagnosis were not suitable for surgery. In the past decades, many developing chemotherapies were amenable to control tumors, but the most challenging issue on the management of treatment responses is that there are still no ideal biomarkers to monitor and predict the prognosis after treatments timely and precisely. A traditional biomarker, carbohydrate antigen 19-9 is not sufficient for timely
checking treatment responses. Besides, the clinical stage, disease status and severity of pancreatic cancer patients by traditional image study are often underestimated due to image limitations. The usage of low-invasive liquid biopsies, e.g. cell-free DNA (cfDNA) from blood, has shown to improve prognostication for several cancers, but not precise for PDAC, especially for predictive prognosis without longitudinal sampling in recent studies. I will present out experience and current ongoing study in the utilization of cfDNA, ctDNA in the prediction of the treatment response in patients with PDAC regardless of the disease status include metastatic or resectable, and also the innovation of the clinical use of dPCR in cfDNA.
TDDW–JDDW–KDDW
Pancreas & Biliary: Enhancing Early Detection and Diagnosis for Pancreatic Cancer: Perspectives from Japan, Korea, and Taiwan
Patient Selection Method, Characteristic Imaging, and Cytopathological Diagnosis in the
Ryota Sagami
Department of Advanced Gastrointestinal Cancer Medicine, Faculty of Medicine, Oita University, Oita, Japan
Early detection of pancreatic cancer (PC) is essential, given its extremely poor prognosis and high mortality rate. Key components in achieving early detection include appropriate patient selection, recognition of characteristic imaging findings, and accurate cytopathological diagnosis. We define early PC as high-grade pancreatic intraepithelial neoplasia and invasive PC measuring ≤10 mm in diameter.
In Western countries, screening for early PC in the general population is typically based solely on familial or genetic risk factors. However, this approach is insufficient, as such factors account for only 3%–10% of all PC cases. Recently developed scoring systems may support more effective patient selection beyond these traditional criteria.
Radiological imaging, including endoscopy, plays a critical role in diagnosing early PC. Indirect imaging findings—such as main pancreatic duct
(MPD) stenosis, dilation, irregular caliber, branch duct dilation, focal parenchymal atrophy, and hypoechoic changes around the MPD—are particularly useful for identifying early PC in the absence of an overt mass. We explore the potential of these findings to be detected by various imaging modalities and endoscopic techniques, including endoscopic ultrasound (EUS) and endoscopic retrograde pancreatography.
Moreover, we review the current role and future potential of endoscopy-based cytological and histological approaches for early PC diagnosis. Special focus is given to EUS-guided tissue acquisition and pancreatic juice cytology via nasopancreatic drainage. The Japanese strategy for early PC detection, supported by emerging evidence, will also be discussed.
TDDW–JDDW–KDDW
Sung Hyun Cho
Department of Gastroenterology, Asan Medical Center, Ulsan University College of Medicine, Seoul, Korea
Pancreatic ductal adenocarcinoma (PDAC) is recognized as one of the most aggressive and fatal malignancies, with a consistently poor prognosis despite recent advances in treatment. In recent years, endoscopic ultrasound (EUS)-guided interventions have evolved beyond diagnostic applications, introducing new therapeutic possibilities. Among them, EUS-guided radiofrequency ablation (EUSRFA) has emerged as a promising local ablative therapy for PDAC, with the potential to enhance the efficacy of systemic therapy and modulate the tumor microenvironment.
EUS-RFA enables targeted ablation of pancreatic tumors under real-time imaging, minimizing damage to surrounding structures. Several observational studies and small-scale trials have demonstrated the technical feasibility and safety of EUS-RFA. In a prospective Korean study, EUS-RFA combined with systemic chemotherapy yielded a median overall survival of 24 months in patients with unresectable PDAC, with an acceptable adverse event profile. Similarly, a recent pilot study comparing EUSRFA combined with chemotherapy versus chemotherapy alone demonstrated significantly greater tumor necrosis and improved pain control in
the combination group.
In theory, EUS-RFA may induce coagulative necrosis and trigger the release of tumor antigens, potentially leading to systemic immunologic responses. Although the immunomodulatory effects of EUS-RFA remain under investigation, its combination with chemotherapy or immunotherapy is being actively explored in current research. Furthermore, EUS-guided intratumoral injection therapy may evolve to support combination approaches such as RFA with intratumoral injections of cytotoxic or immunologic agents.
Despite encouraging preliminary results, EUS-RFA has not yet been fully validated. Current challenges include standardization of ablation protocols, identifying optimal candidates, and validating survival benefits through randomized controlled trials. Nevertheless, EUS-RFA represents a novel and rapidly evolving frontier in the locoregional management of pancreatic cancer.
This lecture will review current evidence on the efficacy, safety, and future directions of EUSRFA in the treatment of pancreatic malignancies, highlighting its role within multidisciplinary therapeutic strategies.
OPTIMAL FECAL IMMUNOCHEMICAL TEST CUTOFF VALUES FOR DETECTING ADVANCED NEOPLASMS IN AVERAGE-RISK INDIVIDUALS
AGED 45–49
Hsu-Hua Tseng1, Mark Pi-Chun Chuang1, Hao-Yu Wu2, Wei-Yuan Chang1, Wen-Feng Hsu1, Li-Chun Chang1, Ming-Shiang Wu1, Han-Mo Chiu1
1Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Department of Internal Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
偵測 45–49 歲一般風險族群大腸進行性 腫瘤之最佳免疫法糞便潛血檢查臨界值
曾旭華1 莊弼鈞1 吳浩宇2 張為淵1 許文峰1 張立群1 吳明賢1 邱瀚模1
1 國立臺灣大學醫學院附設醫院內科部
2 國立臺灣大學醫學院附設醫院癌醫中心分院綜合內 科部
Background: Colorectal cancer (CRC) screening for the average-risk population is now recommended starting at age 45 due to rising incidence in younger populations. The fecal immunochemical test (FIT) is the most widely used non-invasive test for identifying individuals at risk of high-risk neoplasms. A recent study suggests that a non-invasive test with 30% sensitivity for detecting advanced precancerous lesions (APL) could reduce CRC incidence by 45% and mortality by 58% in individuals aged 45 (Ladabaum et al., JNCI 2022). The optimal FIT cutoff values for detecting advanced neoplasms (AN) in individuals aged 45–49, however, remain unclear.
Aims: We aimed to find the optimal FIT cutoff value for detecting AN in average-risk individuals aged 45–49.
Methods: We conducted a retrospective analysis of a screening cohort of average-risk individuals aged 45–74 who underwent concurrent colonoscopy and FIT to determine AN prevalence and FIT positivity. AN was defined as colorectal adenomas ≥10 mm, adenomas with a villous component or high-grade dysplasia, sessile serrated lesions ≥10 mm or with dysplasia, or invasive cancer. Data from 2011–2019 were sourced from a prospectively maintained database. Stool samples were collected prior to colonoscopy and bowel preparation, with FIT
conducted using the OC-SENSOR (Eiken Chemical Co., Ltd., Tokyo, Japan). Quantitative measurements of FIT were collected and stored in the database. Colonoscopy served as the diagnostic reference standard for evaluating FIT performance in AN detection. Receiver operating characteristic (ROC) curves and area under the curve (AUC) were used to assess FIT accuracy, including positivity rate, sensitivity, specificity, and the number needed to scope (NNScope) to detect one AN across different cutoff values.
Results: Among 15,957 average-risk subjects aged 45–74 who received FIT and first-time screening colonoscopy during the study period, 12,246 subjects (50.4% male) were aged 50–74, and 3,711 subjects (50.8% male) were aged 45–49. The NNScope to detect one AN among individuals aged 50–74 with a FIT cutoff of 20 μg/g was 4.4, comparable to individuals aged 45–49 with a FIT cutoff of 40 μg/g (NNScope = 4.5). The quantitative FIT’s AUC for detecting AN in the 45–49 group was 0.70 (95% CI: 0.64–0.76), with an optimal cutoff value of 41.6 μg/g feces. At a higher cutoff, FIT achieved a sensitivity for AN of 30.3% and a specificity of 90.16% in individuals aged 45–49, meeting the Centers for Medicare & Medicaid Services (CMS) performance standards for non-invasive test for CRC screening. Conclusions: Quantitative FIT may be an effective primary screening tool for detecting advanced colorectal neoplasms in individuals aged 45–49. A threshold of 40 μg/g balances colonoscopy resource use with detection efficiency in this age group.
RECLASSIFYING HIGH-RISK COLONOSCOPIC FINDINGS FOR PRECISION SURVEILLANCE – A PROSPECTIVE OBSERVATIONAL STUDY OF A LARGE COLONOSCOPIC POLYPECTOMY TRIAL
Wei-Yuan Chang, Li-Chun Chang, Wen-Feng Hsu, Ming-Shiang Wu, Han-Mo Chiu
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
重新定義高風險大腸鏡發現以進行精準 追蹤:一項大型大腸鏡瘜肉切除試驗的
張為淵 張立群 許文峰 吳明賢 邱瀚模 國立臺灣大學醫學院附設醫院內科部
Background: Colorectal cancer (CRC) is a leading global malignancy, and colonoscopic removal of precursor lesions is key to its prevention. Postpolypectomy surveillance plays a critical role in preventing metachronous advanced colorectal neoplasms (meta-ACRN), particularly among individuals at high risk. However, current risk stratification strategies based on index colonoscopy findings may inadequately capture risk heterogeneity within this high-risk population.
Aims: This study aimed to evaluate real-world surveillance outcomes in high-risk individuals from a large multicenter trial and to explore refined risk stratification of meta-ACRN based on detailed index colonoscopy characteristics.
Methods: We analyzed data from high-risk participants in the Taiwan Cold Snare Polypectomy (TACOS) Trial, a multicenter randomized controlled trial conducted from 2018 to 2020. High-risk individuals (n = 1,385) were prospectively followed, and surveillance outcomes were collected through electronic medical records or structured followup interviews. Participants were stratified into four groups based on index colonoscopy findings: (1) 3–10 low-risk adenomas (LRAs), (2) single high-risk adenoma (HRA), (3) single HRA with synchronous LRA, and (4) multiple HRAs. Meta-ACRN incidence was assessed using Kaplan–Meier methods and Cox proportional hazards regression.
Results: By May 2025, 730 (52.7%) of high-risk individuals underwent surveillance colonoscopy. The overall incidence of meta-ACRN was 45.9 per 1,000
person-years. Individuals with multiple HRAs and those with a single HRA plus synchronous LRA had significantly higher meta-ACRN incidence compared to those with 3–10 LRAs (aHR: 3.18, p < 0.001; aHR: 1.83, p = 0.039, respectively). Among those with HRA, the presence of synchronous neoplasms further increased meta-ACRN risk (aHR: 2.09, p = 0.038).
Based on estimated 3-year cumulative incidence thresholds, proposed surveillance intervals were 1.1, 2.3, and 4.0 years for individuals with multiple HRAs, single HRA with synchronous LRA, and single HRA during index colonoscopy, respectively.
Conclusions: Current surveillance guidelines may benefit from further refinement within highrisk individuals. A more nuanced classification incorporating adenoma multiplicity and synchronous lesions can better inform precision surveillance intervals to optimize CRC prevention.
PROTEOGENOMIC RISK STRATIFICATION PREDICTS
SURVIVAL IN GASTRIC CANCER: A MULTI-OMIC STUDY FROM THE TAIWAN CANCER MOONSHOT PROJECT
Tzu-Chan Hong1,2, Ya-Hsuan Chang3, Hsiang-En Hsu4, Juanilita Waniwan4, Kuen-tyng Lin4, Jyh-Ming Liou1,2, Deng-Chyang Wu5, Hsuan-Yu Chen6, Ming-Shiang Wu1,2, Yu-Ju Chen4
1Department of Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
2Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
3Institute of Molecular and Genomic Medicine, National Health Research Institutes, Miaoli, Taiwan
4Institute of Chemistry, Academia Sinica, Taipei, Taiwan
5Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Chung-Ho Memorial Hospital, Kaohsiung, Taiwan
6Institute of Statistical Science, Academia Sinica, Taipei, Taiwan
以基因體及蛋白質體風險分級預測胃癌 預後:台灣癌症登月計畫的胃癌多體學 研究結果
洪子瞻1,2 張雅媗3 徐祥恩4 Juanilita Waniwan4 林坤廷4 劉志銘1,2 吳登強5 陳璿宇6 吳明賢1,2 陳玉如4
1 台大醫院癌醫分院綜合內科部
2 台大醫院內科部
3 國家衛生研究院分子與基因醫學研究所
4 中央研究院化學研究所
5 高雄醫學大學附設中和紀念醫院胃腸內科
6 中央研究院統計科學研究所
Background: The human stomach, located at the intersection of dietary, microbial, and environmental exposures, offers a unique opportunity to investigate digestive carcinogenesis. While previous studies have advanced molecular subtyping of gastric cancer, the interplay between carcinogen exposure, pathogenic factors, the host proteogenomic landscape, and immune responses remains incompletely understood. Here, we present a comprehensive multi-omic analysis that maps the exposome–pathogen–proteome–
immune axis with its prognostic implications in gastric cancer.
Aims: To develop a simplified proteogenomic risk stratification for predicting overall survival in gastric cancer patients.
Methods: We conducted a prospective cohort study involving 154 patients, collecting paired gastric cancer and adjacent non-cancerous surgical specimens from two tertiary referral centers in Taiwan. Multi-omic integration encompassed genomic, transcriptomic, proteomic, phosphoproteomic and microbial data layers. Genomic profiling included whole-exome sequencing (WES) and RNA-seq, with non-negative matrix factorization (NMF) used to infer carcinogenassociated mutational signatures. Proteomic and phosphoproteomic profiling employed a TMT 11plex–based mass spectrometry platform, while microbiome-associated signals were characterized via RNA-seq and proteomic detection.
Results: Among 154 patients (62% male), 38.3% had diffuse-type and 44.8% intestinal-type tumors; stage distribution ranged from I (25.3%) to IV (20.1%). We identified unique exogenous carcinogen, proteomics and bacterial signatures specific to Taiwanese gastric cancer, absent in TCGA, that drive immune remodeling and oncogenic progression. In a multivariable Cox proportional hazards model incorporating clinical variables including stages and molecular features, both proteomic immune subtype and carcinogen risk classification were independently associated with overall survival (HR = 2.86, p = 0.009; HR = 2.72, p = 0.034, respectively), while age and gender were not significant. Based on these two variables, we developed a composite proteogenomic risk score that effectively stratified overall survival across the entire cohort (log-rank p = 0.0017), and within stage III patients (p = 0.010), with a trend observed in stages II as well. The score also significantly separated survival among patients with intestinal-type histology (p = 0.0055). These findings were consistent in progressionfree survival analyses (overall p = 0.0054; stage III p = 0.0062). Further integration with phosphoproteomic data and pathway enrichment analysis revealed actionable signaling modules, providing mechanistic insights and potential therapeutic targets for future investigation.
Conclusions: Our study demonstrates that a simplified proteogenomic risk score, integrating immune subtype and carcinogen exposure status, provides independent prognostic value beyond traditional clinical factors. These findings not only inform precision prognostics and therapeutics tailored to Asian gastric cancer, but also help resolve the clinical uncertainty regarding the need for intensified treatment in stage III patients.
EARLIER AND MORE SEVERE RELAPSE AFTER NUCLEOS(T)IDE ANALOGUE DISCONTINUATION IN HBEAG-POSITIVE CHRONIC HEPATITIS B PATIENTS
Yen-Chun Liu1,2, Chien-Wei Peng1, Wen-Juei Jeng1,2, Rong-Nan Chien1,2
1Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
2School of Medicine, Chang Gung University, Taoyuan, Taiwan
E 抗原陽性慢性 B 型肝炎患者停用核 苷
復發
劉彥君1,2 彭建維1 鄭文睿1,2 簡榮南1,2
1 林口長庚紀念醫院胃腸肝膽科系
2 長庚大學醫學系
Background: HBeAg-positive and -negative chronic hepatitis B (CHB) represent distinct immunovirological phenotypes. However, many studies of finite nucleos(t)ide analogue (Nuc) therapy have analyzed them together, potentially obscuring the impact of baseline HBeAg status on off-Nuc outcomes.
Aims: This study aimed to compare the incidence, timing, and severity of relapse after finite Nuc therapy between pretherapy HBeAg-positive and -negative patients.
Methods: CHB patients who stopped Nuc therapy per APASL criteria (HBV DNA undetectable ≥1 year; HBeAg loss for ≥1 year) were analyzed. Clinical relapse (CR) was defined as ALT ≥2 times upper limit of normal (xULN) and HBV DNA ≥2000 IU/mL. Severe flare was defined as ALT ≥1000 U/L, total bilirubin ≥3.5 mg/dL or CR with hepatic decompensation (HD: total bilirubin >2 mg/dL and INR ≥1.5). CR incidence, timing, and severity were compared between HBeAg-positive and -negative patients before and after propensity score matching (PSM) by age, sex, pretherapy ALT, HBV DNA, and end-of-treatment (EOT) HBsAg. Cox regression was used to identify predictors of severe flare.
Results: A total of 286 HBeAg-positive and 2355 HBeAg-negative patients were analyzed (median follow-up: 4.6 years). CR occurred in 60% vs. 67%, respectively. HBeAg-positive patients had higher
ALT at CR (345 vs. 244 U/L, p < 0.01), more ALT ≥10× ULN (48% vs. 37%, p < 0.01), higher HBV DNA at CR (7.3 vs. 5.7 log₁₀ IU/mL), earlier relapse (34 vs. 39 weeks, p < 0.01), and higher CR-related mortality (2% vs. 0.3%, p = 0.04). After PSM (n = 265/group), baseline characteristics were balanced. HBeAgpositive patients still had higher peak ALT, (345 vs. 269 U/L), HBV DNA at CR (7.3 vs. 6.4 log₁₀ IU/mL), and HD incidence (3% vs. 0%) (all p < 0.05). The 2-year cumulative incidence of severe flare was higher in HBeAg-positive patients before and after PSM (pre: 11% vs. 8%, p = 0.02; post: 11% vs. 7%, p = 0.12), while CR rates post PSM were comparable (58% vs. 66%, p = 0.20). In multivariate analysis, pretherapy HBeAg positivity (aHR: 1.6), cirrhosis (aHR: 1.8), ALT ≥5× ULN (aHR: 1.8), and non-entecavir use (aHR: 1.7) independently predicted severe flare among offNuc CR patients.
Conclusions: HBeAg-positive CHB patients experience earlier and more severe relapse after finite NUC therapy. Off-therapy outcomes should be stratified by baseline HBeAg status, with intensified monitoring recommended for those with cirrhosis, pretherapy flare, or non-entecavir use.
Jin Ho Choi, Kyung Min Lee, In Rae Cho, Woo Hyun Paik, Ji Kon Ryu, Sang Hyub Lee
Department of Internal Medicine, Seoul
National University Hospital, Seoul National University College of Medicine, Seoul, Republic of Korea
Background: Oxaliplatin (OXA) resistance remains a remarkable challenge in the treatment of pancreatic cancer. Ferroptosis, an iron-dependent form of cell death characterized by lipid peroxidation, has emerged as a promising therapeutic target for overcoming chemotherapy resistance.
Aims: In this study, we used patient-derived pancreatic cancer organoids (PDPCOs) to investigate whether ferroptosis induction could overcome OXA resistance.
Methods: We established 42 patient-derived pancreatic cancer organoids (PDPCOs) and performed integrative molecular profiling including RNA sequencing and drug response characterization. Transcriptomic analysis identified ferroptosisrelated alterations in OXA-resistant PDPCOs. Cell viability assays and synergy analysis evaluated the combination effects of artesunate (ART) and OXA. Mechanistic studies included lipid peroxidation, iron accumulation, and mitochondrial function assessments. Gene expression was analyzed by qRTPCR and Western blotting, with functional validation using siRNA knockdown. In vivo efficacy was evaluated using PDPCO-derived xenograft models. Results: Transcriptomic analysis revealed distinct ferroptosis-related alterations in OXA-resistant PDPCOs, including a negative enrichment of ferroptosis suppressor genes. The ferroptosis inducer artesunate (ART) synergistically enhanced the anticancer effects of OXA in cell lines and PDPCOs.
In vitro mechanistic studies demonstrated that this combination therapy induced ferroptotic cell death by promoting lipid peroxidation, intracellular iron accumulation, and mitochondrial dysfunction. The combination therapy also remarkably inhibited tumor growth in PDPCO-derived xenograft models. ART/OXA treatment upregulated the expressions of iron transport proteins transferrin receptor (TFRC) and divalent metal transporter 1 (DMT1), which contributed to ferroptosis induction.
Overexpression of solute carrier family 7 member 11 (SLC7A11) conferred dual resistance to OXA and ART by suppressing ferroptosis, whereas its knockdown or pharmacological inhibition with erastin sensitized resistant cells to the combination therapy. Notably, the triple combination of ART, OXA, and erastin effectively overcame resistance in the dual-resistant PDPCOs.
Conclusions: These findings justify the use of ferroptosis-based therapeutic strategies for OXAresistant pancreatic cancer and highlight SLC7A11 as a potential predictive biomarker.
CLINICAL INTEGRATION FOR EVALUATING NON-CONTRAST CT IN FOCAL
Pushpanjali Gupta1,2,3, Chun-Ying Wu1,2,3,4,5, Sulagna Mohapatra2, Che-Lun Hung1,2, Yao-Chun Hsu6,7, Yuan-Chia Chu8,9, Chia-Sheng Chu10,11
1Institute of Biomedical Informatics, National Yang Ming Chiao Tung University, Taipei, Taiwan
2Health Innovation Center, National Yang Ming Chiao Tung University, Taipei, Taiwan
3Institute of Public Health, National Yang Ming Chiao Tung University, Taipei, Taiwan
4Division of Translational Research, Taipei Veterans General Hospital, Taipei, Taiwan
5Department of Public Health, China Medical University, Taichung, Taiwan
6Division of Gastroenterology and Hepatology, E-Da Hospital, Kaohsiung, Taiwan
7School of Medicine, I-Shou University, Kaohsiung, Taiwan
8Information Management Office & Big Data Center, Taipei Veterans General Hospital, Taipei, Taiwan
9Department of Information Management, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan
10Division of Gastroenterology and Hepatology, Taipei City Hospital Yang Ming Branch, Taipei, Taiwan
11Program of Interdisciplinary Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
Background: Liver cancer is the sixth most common cancer and the third leading cause of cancer-related deaths worldwide, with only about 10% of patients surviving five years post-diagnosis. While some focal liver lesions may appear similar, their treatment and prognosis differ significantly. Thus, accurate classification during diagnosis is crucial for effective treatment planning and management of liver diseases.
Aims: To explore whether combining explainable AI with non-contrast CT and laboratory data can accurately diagnose focal liver lesions (FLLs) like contrast-enhanced CT.
Methods: This retrospective study (January 2004 to
December 2020) screened 69004 patients, ultimately including 2140 naïve cases with four phases of CT. Of these, 1712 (672 malignant) were used for training and 428 (279 malignant) for testing, covering various lesions such as cysts, hemangiomas, and nodules. We extracted 1143 radiomics features per lesion and employed the SHapley Additive exPlanations method to identify key features and validate the model’s reasoning.
Results: The model achieved an accuracy of 0.89 (95% CI: 0.87, 0.91) and an AUC of 0.93 (95% CI: 0.92, 0.94) with all 1143 features from non-contrast CT. Reducing to the top 9 features-maintained accuracy at 0.89 while increasing AUC to 0.95. Incorporating lab data improved accuracy and sensitivity to 0.95 (95% CI: 0.94, 0.96) and AUC to 0.98 (95% CI: 0.97, 0.99), emphasizing the importance of factors like FIB4. The model remained effective with non-contrast CT alone, achieving an accuracy of 0.95 and an AUC of 0.99 when including arterial phase CT features.
Conclusions: Non-contrast CT and lab data can effectively diagnose FLLs, reducing the need for contrast-enhanced scans. This approach benefits patients by lowering radiation exposure and reduces costs for the healthcare system.
HBCRAG LEVELS STRATIFY RISK OF IMMUNE-ACTIVE TRANSITION IN HBEAG-NEGATIVE PATIENTS WITH INDETERMINATE CHRONIC HEPATITIS B
Hsing-Yu Yeh1, Kuan-Hui Hsin1, Chun-Jen Liu1,2,4, Chun-Ming Hong1,5, Tung-Hung Su1,2, Hung-Chih Yang1,2,4,6, Chen-Hua Liu1,2, Pei-Jer Chen1,2,4, Tai-Chung Tseng1,2,3, Jia-Horng Kao1,2,3,4
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
3Department of Medical Research, National Taiwan University Hospital, Taipei, Taiwan
4Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine
Taipei, Taiwan
5Division of Hospital Medicine, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
6Department of Microbiology, National Taiwan University College of Medicine Taipei, Taiwan
HBcrAg 濃度可分層預測 HBeAg 陰性灰 色地帶患者的免疫活化風險
葉星佑1 辛冠輝1 劉俊人1,2,4 洪俊銘1,5 蘇東弘1,2 楊宏志1,2,4,6 劉振驊1,2 陳培哲1,2,4 曾岱宗1,2,3 高嘉宏1,2,3,4
1 國立臺灣大學醫學院附設醫院胃腸肝膽科
2 國立臺灣大學醫學院附設醫院肝炎研究中心
3 國立臺灣大學醫學院附設醫院醫學研究部
4 國立臺灣大學醫學院臨床醫學研究所
5 國立臺灣大學醫學院附設醫院整合醫學科
6 國立臺灣大學醫學院微生物學科暨研究所
Background: Chronic HBV (CHB) infection with ongoing hepatic inflammation increases the risk of cirrhosis and hepatocellular carcinoma (HCC). Among HBeAg-negative individuals, those in the indeterminate phase exhibit a heterogeneous clinical course, with a subset eventually progressing to immune-active hepatitis.
Aims: This study aimed to investigate whether hepatitis B core-related antigen (HBcrAg), a surrogate marker of intrahepatic cccDNA activity, can predict transition from the indeterminate phase to the immune-active phase in HBeAg-negative patients.
Methods: We analyzed 1,090 HBeAg-negative grey zone patients from the ERADICATE-B cohort (n = 2,666), which excluded inactive CHB patients (HBV DNA <2000 IU/mL + ALT <1x ULN by AASLD definition) and those with ALT >2× ULN. Baseline measurements included HBV-related seromarkers (HBcrAg, HBV DNA, HBsAg) and liver function. The risk of immune-active transition (ALT >2x ULN + HBV DNA >2000 IU/mL), HBV-associated hepatitis (ALT >100 U/L + HBV DNA >2000 IU/mL), HBsAg loss, death and liver-related death were assessed using Kaplan-Meier survival analysis and Cox proportional hazards models.
Results: During 11,674.6 person-years of followup, 619 patients progressed to the immune-active phase, yielding an incidence rate of 5.3 per 100 person-years (95% CI: 4.9–5.7). Higher baseline HBcrAg levels were associated with increased risk of immune-active transition and showed superior predictive performance compared to HBV DNA (P = 0.03). Compared to patients with HBcrAg <10 KU/ mL, those with levels of 10–99 KU/mL and ≥100 KU/ mL were associated with higher risks of immuneactive transition, HBV-associated hepatitis, mortality, liver-related death, and lower probability of HBsAg loss. In multivariable analysis, HBcrAg remained an independent predictor of immune-active transition after adjustment for age, baseline ALT, HBV DNA, and HBsAg levels.
Conclusions: Among HBeAg-negative indeterminate patients, baseline HBcrAg levels are independent predictors of immune-active transition and other adverse outcomes. HBcrAg may serve as a useful biomarker to identify patients who may benefit from closer monitoring or preemptive antiviral therapy.
ENDOSCOPIC APPLICATION OF TRANEXAMIC ACID AND SUCRALFATE IN UPPER GASTROINTESTINAL BLEEDING: A RANDOMIZED CONTROLLED TRIAL
Meng-Hsuan Lu, Po-Jun Chen, Er-Hsiang Yang, Chiung-Yu Chen, Chiao-Hsiung Chuang, Xi-Zhang Lin, Hsueh-Chien Chiang
Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan
經內視鏡投藥以預防上消化道出血復發
呂孟璇 陳柏潤 楊貳翔 陳炯瑜 莊喬雄 林錫璋 姜學謙
國立成功大學醫學院附設醫院內科部
Background: Upper gastrointestinal bleeding (UGIB) is a prevalent and potentially life-threatening condition in clinical practice. Common etiologies for UGIB include peptic ulcer bleeding, variceal bleeding, diffuse mucosal hemorrhage, angiodysplasia, and tumor-related bleeding. Although standard endoscopic hemostatic interventions achieve initial hemostasis in approximately 80%–90% of gastrointestinal bleeding cases, diffuse mucosal hemorrhage and tumor-associated bleeding continue to pose significant therapeutic challenges, with reported rebleeding rates ranging from 10%–50%. Our previous studies have demonstrated that the topical application of tranexamic acid effectively reduces early rebleeding rate for peptic ulcer bleeding, and topical sucralfate has shown efficacy in reducing the incidence rate of delayed polypectomy bleeding.
Aims: This study aims to evaluate the efficacy and safety of combining topical tranexamic acid and sucralfate powder in achieving hemostasis and preventing rebleeding across various types of upper gastrointestinal hemorrhage. Meanwhile, this study will figure out the retaining time of drug powders on the bleeding site.
Methods: This prospective, randomized clinical trial was conducted at National Cheng Kung University Hospital. Patients presenting with non-variceal upper gastrointestinal bleeding were enrolled in the study. After undergoing standard endoscopic hemostatic therapy, the patients were randomly assigned to either the experimental group or the standard group. In the experimental group, an
additional 1g tranexamic acid and 2g sucralfate powder were applied directly to the bleeding site via endoscopic spray. Immediate hemostasis was evaluated 5 minutes after the intervention. All patients will receive a second-look EGD after 48-hour intravenous PPI infusion. Outcome measurement includes early treatment failure rate within the first 4 days and recurrent bleeding with 30 days. Early treatment failure is defined as (1) index bleeder recurrent bleeding; (2) index bleeder requiring repeated endoscopic hemostasis during the second-look EGD; or (3) recurrent bleeding requiring transarterial embolization (TAE) or surgery. All participants will be monitored for 30 days to assess the incidence of rebleeding. To assess the adherence of the applied powders, 1g barium sulfate powder was also administered in the experimental group, and abdominal radiographs were taken 4, 8, and 12 hours after endoscopic treatment.
Results: Between October 2024 and May 2025, a total of 60 patients with upper gastrointestinal bleeding were enrolled and randomized equally into two groups: the intervention group and the standard group, with 30 patients in each arm. Baseline characteristics and bleeding severity were well-matched between the two groups, ensuring comparability for outcome assessment. As a result, the intervention group exhibited a significantly lower rate of early treatment failure compared to the standard group (6.7% vs. 30.0%; P = 0.042). Patients in the intervention group also had a reduced 30-day rebleeding rate (10.0% vs. 36.7%; P = 0.030). The duration of bleeding-free survival was significantly longer in the intervention group (P = .018). Additionally, radiographic assessments showed that the drug powders adhered to the bleeding site for approximately 8–12 hours in both the stomach and duodenum. No severe adverse events related to the use of drug powder were observed.
Conclusions: The precise delivery of topical tranexamic acid and sucralfate alongside standard endoscopic hemostasis significantly reduced both the early treatment failure rate and 30-day rebleeding rate in patients presenting with upper gastrointestinal bleeding.
Section:HBV
DIVERGENT EFFECTS OF GLYCEMIC BURDEN ON HBEAG SEROCLEARANCE AND HCC RISKS IN HBEAG-POSITIVE CHB: A LARGE MULTICENTER COHORT STUDY
Shang-Chin Huang1,2,3,4, Rex Wan-Hin Hui5, Tai-Chung Tseng3,6, Karen Cheuk-Ying Ho5, Lung-Yi Mak5,7, Shih-Jer Hsu2,3, Chun-Ming Hong8, Chen-Hua Liu2,3, Hung-Chih Yang2,3, Chun-Jen Liu2,3,4, Wai-Kay Seto5,7, Tung-Hung Su2,3, Man-Fung Yuen5,7, Jia-Horng Kao2,3,4
1Department of Internal Medicine, National Taiwan University Hospital Bei-Hu Branch, Taipei, Taiwan
2Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
3Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
4Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
5Department of Medicine, The University of Hong Kong, Hong Kong
6Department of Medical Research, National Taiwan University Hospital, Taipei, Taiwan
7State Key Laboratory of Liver Research, The University of Hong Kong, Hong Kong
8Division of Hospital Medicine, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
血糖負荷對 e 抗原清除與肝癌風險之分 歧效應:一項針對 e 抗原陽性 B 型肝炎 患者之大型多中心研究
黃上秦1,2,3,4 許允軒5 曾岱宗3,6 何卓盈5 麥龍兒5,7
徐士哲2,3 洪俊銘8 劉振驊2,3 楊宏志2,3 劉俊人2,3,4
司徒偉基5,7 蘇東弘2,3 袁孟峰5,7 高嘉宏2,3,4
1 國立臺灣大學醫學院附設醫院北護分院胃腸肝膽內 科
2 國立臺灣大學醫學院附設醫院胃腸肝膽科
3 國立臺灣大學醫學院附設醫院肝炎研究中心
4 國立臺灣大學醫學院臨床醫學研究所
5 香港大學內科學系
6 國立臺灣大學醫學院附設醫院醫學研究部
7 香港大學肝病研究國家重點實驗室
8 國立臺灣大學醫學院附設醫院整合醫學科
Background: HBeAg seroclearance marks a critical milestone in the natural course of chronic hepatitis B (CHB). With the rising prevalence of metabolic dysfunction-associated steatotic liver disease (MASLD) and metabolic comorbidities, their impact on HBeAg-positive CHB remains poorly understood, particularly regarding viral clearance and long-term oncologic outcomes.
Aims: To investigate the impact of steatotic liver disease (SLD) and glycemic burden on HBeAg seroclearance and hepatocellular carcinoma (HCC) risk in patients with HBeAg-positive CHB, using large-scale real-world cohorts from Taiwan and Hong Kong.
Methods: HBeAg-positive CHB patients with serial HBeAg measurements were consecutively enrolled from the National Taiwan University Hospital (NTUH, internal cohort). SLD and cardiometabolic risk factors were defined per international guidelines. Cumulative incidences of HBeAg seroclearance and HCC were compared after adjustment for confounding factors. External validation was conducted in an independent cohort from The University of Hong Kong (HKU, external cohort).
Results: This study included 2,531 HBeAg-positive patients in the internal cohort and 866 in the external cohort, with a median follow-up of 8.2 and 14.4 years, respectively. At baseline, the median age was 38.8 and 39.2 years, and the proportion of males was 57.8% and 61.0%, respectively. Nucleos(t) ide analogue therapy had been initiated in 30.6% and 36.6% of patients, while diabetes mellitus (DM) was present in 5.3% and 4.5%. In both cohorts, SLD was not associated with HBeAg seroclearance. Conversely, DM significantly increased the likelihood of HBeAg seroclearance (internal cohort: adjusted hazard ratio [aHR]: 1.38, 95% confidence interval [CI]: 1.07 – 1.77; external cohort: aHR 1.61, 95% CI 1.02 –2.55; both p < 0.05). The glycemic burden consistently demonstrated a dose-dependent association with HBeAg seroclearance (aHR: 1.41 and 1.17 for HbA1c ≥6.5% and 5.9 – 6.4% vs. ≤5.8%; p for trend = 0.006). HbA1c ≥ 6.5% was also independently associated with an increased HCC risk (internal cohort: aHR: 1.92, 95% CI: 1.17 – 3.16; external cohort: aHR 6.58, 95% CI 1.75 – 27.42; both p < 0.05). The sensitivity analyses, including propensity score matching, multiple imputation for missing data, and timedependent covariate analysis for antiviral therapy, confirmed the robustness of results.
Conclusions: The glycemic burden exerts a diverse and paradoxical impact on HBeAg-positive CHB, enhancing HBeAg seroclearance while increasing HCC risks. These findings underscore the importance of routine glycemic monitoring and metabolic control in this special population. The mechanisms behind the virus-host metabolic interplay represent a novel area for future research.
HIGH HBSAG LEVEL IDENTIFIES GENUINE IMMUNE-TOLERANT CHRONIC HEPATITIS B PATIENTS WITH REDUCED RISK OF HEPATOCELLULAR CARCINOMA AND LIVER-RELATED MORTALITY
Kuan-Hui Hsin1, Tai-Chung Tseng1,2,3, Chun-Jen Liu1,2,4, Chien-Jen Chen6, Tung-Hung Su1,2, Hung-Chih Yang1,2,4,5, Chen-Hua Liu1,2, Pei-Jer Chen1,2,3,4,5, Hwai-I Yang6,7,8,9,10, Jia-Horng Kao1,2,3,4
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
3Department of Medical Research, National Taiwan University Hospital, Taipei, Taiwan
4Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine
Taipei, Taiwan
5Department of Microbiology, National Taiwan University College of Medicine Taipei, Taiwan
6Genomics Research Center, Academia Sinica, Taipei, Taiwan
7Institute of Clinical Medicine, National YangMing Chiao Tung University, Taipei, Taiwan
8Graduate Institue of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
9Biomedical Translation Research Center, Academia Sinica, Taipei, Taiwan
10Doctoral Program of Clinical and Experimental Medicine, National Sun Yat-Sen University, Kaohsiung, Taiwan
高 B 型肝炎表面抗原濃度可用來區分真 正免疫耐受型慢性 B 型肝炎患者,顯示 其肝癌與肝病相關死亡風險相對較低 辛冠輝1 曾岱宗1,2,3 劉俊人1,2,4 陳建仁6 蘇東弘1,2 楊宏志1,2,4,5 劉振驊1,2 陳培哲1,2,3,4,5 楊懷壹6,7,8,9,10 高嘉宏 1,2,3,4
1 國立臺灣大學醫學院附設醫院胃腸肝膽科
2 國立臺灣大學醫學院附設醫院肝炎研究中心
3 國立臺灣大學醫學院附設醫院醫學研究部
4 國立臺灣大學臨床醫學研究所
5 國立臺灣大學醫學院微生物學系
6 中央研究院基因體研究中心
7 國立陽明交通大學臨床醫學研究所
8 高雄醫學大學醫學研究所
9 中央研究院生醫轉譯研究中心
10 國立中山大學臨床醫學科學博士學位學程
Background: Although immune-tolerant (IT) chronic hepatitis B (CHB) is considered clinically quiescent, a subset of IT patients still develop liver-related adverse events, reflecting the high variability of ALT and HBV DNA, the core criteria defining the IT phase.
Aims: We explored whether quantitative hepatitis B surface antigen (HBsAg) can help identify genuine IT patients with lower risk of HCC and liver-related mortality on top of 2025 AASLD criteria.
Methods: Among 6,250 treatment-naïve, noncirrhotic Taiwanese adults with CHB, 2,666 from the ERADICATE-B study and 3,584 from the REVEAL-HBV study, 370 met the 2025 AASLD IT criteria (HBeAgpositive, normal ALT levels, and HBV DNA ≥ 10 million IU/mL). HBsAg level of 10,000 IU/mL was adopted to stratify these patients and the Kaplan–Meier curves, Cox proportional hazards models, and Fine-Gray competing risk models were adopted to explore their likelihood of HBeAg seroclearance and liver-related events, including hepatocellular carcinoma (HCC), and liver-related death.
Results: Among the 370 IT patients, a total of 8972.3 person-years of follow-up were accumulated (mean ± SD: 24.25 ± 6.37 years). During follow-up period, 129 patients (2.46%/year) achieved HBeAg seroclearance, 71 (0.93%/year) developed HCC, 58 (0.65%/year) died of liver-related causes, and 95 (1.06%/year) died from any cause. Compared with those with HBsAg < 10,000 IU/mL (n = 55), patients with HBsAg ≥ 10,000 IU/mL (n = 308) had lower likelihoods of HBeAg seroclearance (HR 0.52, 95% CI 0.33–0.81), HCC (HR 0.57, 95% CI 0.33–0.99), and liver-related death (SHR 0.43, 95% CI 0.23–0.80). In contrast, no significant difference was shown in non–liver-related mortality (HR 1.26, 95% CI 0.48–3.29), highlighting the liver-specific discriminative value of HBsAg. The addition of HBsAg ≥10,000 IU/mL to current IT criteria identified patients with lower likelihoods of HBeAg seroclearance and delayed onset of HCC and liver-related death, suggesting an earlier phase of HBV infection.
Conclusions: In our cohorts of 370 IT patients defined by 2025 AASLD guideline, patients with HBsAg level ≥10,000 IU/mL were associated with delayed development of HCC and liver-related death as well as lower chance of HBeAg seroclearance. These findings support HBsAg as a complimentary marker to define genuine IT patients.
IMPACT OF HBV RELAPSE PATTERNS ON HBSAG SEROCLEARANCE AFTER ENTECAVIR OR TDF DISCONTINUATION
Chien-Hung Chen, Yi-Hao Yen, Yuan-Hung Kuo, Jing-Houng Wang, Tsung-Hui Hu, Chao-Hung Hung, Sheng-Nan Lu
Division of Hepato-Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan
B 型肝炎病毒復發模式對停用貝樂克或惠 立妥治療後表面抗原消失的影響 陳建宏 顏毅豪 郭垣宏 王景弘 胡琮輝 洪肇宏 盧勝男 長庚醫療財團法人高雄長庚紀念醫院胃腸肝膽科系 暨長庚大學醫學系
Background: Although discontinuing NAs may result in a high risk of HBV relapse, it also increases the likelihood of HBsAg seroclearance.
Aims: To investigate the association between HBV relapse patterns and HBsAg seroclearance after stopping entecavir or tenofovir disoproxil fumarate (TDF).
Methods: A total of 902 non-cirrhotic patients (617 HBeAg-negative and 285 HBeAg-positive at treatment initiation) who had discontinued entecavir or TDF for at least 12 months were retrospectively analyzed.
Results: HBeAg-negative patients had a significantly higher HBsAg seroclearance rate than HBeAgpositive patients (p = 0.002), despite similar rates of clinical relapse and retreatment. In clinical relapsers, the cumulative rate of HBsAg seroclearance at 10 years in HBeAg-negative patients were 29.7% (no retreatment) and 17.1% (with retreatment) (p < 0.001), while in HBeAg-positive patients they were 25% and 8.7%, respectively (p = 0.631). Among HBeAgnegative patients, those with clinical relapse prior to HBsAg seroclearance had higher HBsAg levels at end-of-treatment (EOT) than those without relapse (p < 0.001). HBeAg-negative patients with HBsAg at EOT <50 IU/mL had a low clinical relapse rate (4.34%) prior to HBsAg seroclearance compared to patients with HBsAg at EOT ≥ 50 IU/mL (42.9%). Lower peak ALT levels and a reduced incidence of ALT >5× ULN were observed in HBeAg-negative patients with
clinical relapse and HBsAg seroclearance, whereas HBeAg-positive patients with seroclearance had higher ALT flares (peak ALT, p = 0.003; ALT >10× ULN, p = 0.039) compared with those with clinical relapse without HBsAg seroclearance. Among 124 patients who received another course of finite therapy, the 6-year cumulative rate of HBsAg seroclearance rate was 21.5%. Eight patients experienced hepatic decompensation upon clinical relapse, with 3 deaths despite timely retreatment.
Conclusions: HBV relapse patterns significantly impact HBsAg seroclearance. Post-treatment monitoring is essential to detect relapse early and prevent severe outcomes like hepatic decompensation.
AIR
Tyng-yuan Jang, Chia-Yen Dai
Division of Hepatobiliary, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
空氣污染與慢性
張庭遠 戴嘉言
高雄醫學大學附設中和紀念醫院肝膽胰內科
Background: Air pollution has been linked to fatty liver disease
Aims: Its effects on fatty liver disease in patients with chronic hepatitis B remain unclear
Methods: This cross-sectional study recruited 80 hepatitis B e antigen (HBeAg)–negative CHB patients who prepared to receive antiviral agents. Fatty liver disease was detected using abdominal ultrasound, and the risk factors associated with the condition were analyzed. The daily estimates of air pollutants (particulate matter ≤2.5 µm in diameter (PM2.5), nitrogen dioxide (NO2), ozone (O3), and benzene) were aggregated to calculate the mean levels for the month prior to the date of recruitment.
Results: A total of 80 patients were recruited for the current study. Overall, 62.5% of the patients were found to have fatty liver disease based on ultrasound results. Compared with patients without fatty liver disease, patients with fatty liver had a higher mean body mass index (BMI) (26.4 kg/m² vs 22.3 kg/m²; P < 0.001), higher serum triglyceride level (108.5 mg/ dL vs 85.1 mg/dL; P = 0.03), higher proportion of diabetes (26.3% vs 3.3%; P = 0.01), and substantially higher PM2.5 (24.1 mg/m³ vs 19.9 mg/m³; P = 0.08).
PM2.5 > 24 ug/m³ had higher ratio of fatty liver than PM2.5 < 24 ug/m³ (78.8% vs 51.5%; P = 0.02). The multivariate logistic regression analysis revealed the factors associated with fatty liver were BMI > 24 kg/ m² (odds ratio (OR), 43.74; 95% confidence intervals (CI), 7.61–251.58; P < 0.001) and PM2.5 > 24 ug/m³ (OR, 5.91; 95% CI, 1.24–28.24; P = 0.03).
Conclusions: Among HBeAg-negative CHB patients with relatively low viral loads, PM2.5 is associated with fatty liver disease in CHB patients.
INCIDENCES OF VIROLOGICAL AND CLINICAL RELAPSES AFTER CESSATION OF TENOFOVIR ALAFENAMIDE, TENOFOVIR DISOPROXIL FUMARATE, OR ENTECAVIR IN PATIENTS WITH HBEAG-NEGATIVE CHRONIC HEPATITIS B
Jan-Bo Tu1, Cheng-Hao Tseng1,2,3, Teng-Yu Lee4,5, Chi-Yi Chen6, Chung-Feng Huang7, Po-Yueh Chen6, Tyng-Yuan Jang7, Tzeng-Huey Yang8, Chia-Ching Wu9, Yao-Chun Hsu1,3,9
1Division of Gastroenterology and Hepatology, E-DA Hospital, Kaohsiung, Taiwan
2Division of Gastroenterology and Hepatology, E-DA Cancer Hospital, Kaohsiung, Taiwan
3School of Medicine, College of Medicine, I-Shou University, Kaohsiung, Taiwan
4School of Medicine, Chung Shan Medical University, Taichung, Taiwan
5Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
6Division of Gastroenterology and Hepatology, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
7Hepatobiliary Division, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
8Department of Internal Medicine, Lotung PohAi Hospital, Yilan, Taiwan
9Graduate Institute of Medicine, I-Shou University, Kaohsiung, Taiwan
在 e 抗原陰性的慢性 B 肝患者中停用核
苷 酸類似物的復發率比較:Tenofovir Alafenamide 、 Tenofovir Disoproxil
Fumarate 及 Entecavir
涂展博1 曾政豪1,2,3 李騰裕4,5 陳啟益6 黃釧峰7 陳柏岳6 張庭遠7 楊增慧8 吳佳錦9 許耀峻1,3,9
1 義大醫院胃腸肝膽科
2 義大癌治療醫院胃腸肝膽科
3 義守大學醫學系
4 中山醫學大學醫學系
5 臺中榮民總醫院胃腸肝膽科
6 嘉義基督教醫院胃腸肝膽科
7 高雄醫學大學附設中和紀念醫院肝膽胰內科
8 羅東博愛醫院內科部
9 義守大學醫學研究所
Background: Recent data indicate a higher rate of HBsAg seroclearance following nucleos(t)ide analogue (NA) cessation compared to continuous treatment. The relapse pattern following the discontinuation of tenofovir alafenamide (TAF) in patients with chronic hepatitis B (CHB) remains unclear.
Aims: This study aimed to compare the two-year incidences of virological and clinical relapses among patients who discontinued Tenofovir Alafenamide (TAF) versus those who discontinued tenofovir disoproxil fumarate (TDF) or entecavir (ETV).
Methods: This multicenter retrospective study enrolled non-cirrhotic hepatitis B e antigen (HBeAg)negative CHB patients who discontinued TAF, TDF, or ETV with undetectable HBV DNA at treatment cessation. For patients who switched from ETV or TDF to TAF, a minimum TAF exposure duration of 12 months was required for inclusion in the off-TAF group. Inverse probability of treatment weighting was employed to adjust for baseline differences.
Results: A total of 162 patients (off-TAF: 37, offTDF: 87, off-ETV: 38) were included in the primary analysis. The two-year cumulative incidence of virological relapse was significantly higher in the offTAF group (85.0%) compared to the off-TDF group (69.5%, P = 0.024) and the off-ETV group (51.5%, P = 0.010). Similarly, the two-year cumulative incidence of clinical relapse was significantly higher in the offTAF group (62.4%) compared to the off-TDF group (39.0%, P = 0.026) and the off-ETV group (22.5%, P = 0.024).
Conclusions: HBeAg-negative patients who discontinue TAF face a higher risk of both virological and clinical relapses compared to those discontinuing TDF or ETV. These findings underscore the need for more intense monitoring in CHB patients after TAF cessation.
EXPANSION OF DYSFUNCTIONAL MEMORY B CELLS IS ASSOCIATED WITH HEPATITIS FLARES AND DISEASE ACTIVITY IN CHRONIC HEPATITIS B
Thi Kim Duyen Nguyen2, Yen-Chun Liu1,2, Hsiang-Wei Huang2, Chia-Wei Lin2, Jian-He Fan2, Wei-Ting Ku2, Cheng-Heng Wu2, Wen-Juei Jeng1,2, Chun-Yen Lin1,2
1Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
2College of Medicine, Chang Gung University, Taoyuan, Taiwan
慢性 B 型肝炎患者功能失調之記憶 B 細
胞增生與肝炎急性發作及疾病活動度之 相關性
阮金緣2 劉彥君1,2 黃祥瑋2 林家緯2 方健合2 古唯鼎2 吳承衡2 鄭文睿1,2 林俊彥1,2
1 林口長庚紀念醫院胃腸肝膽科系
2 長庚大學醫學院
Background: Atypical memory B cells (atMBC) are a functionally impaired subset of B cells with enhanced pro-inflammatory cytokine profile that expand in chronic immune activation, including chronic hepatitis B (CHB). However, the clinical significance of atMBCs in CHB remains poorly understood.
Aims: This study aims to elucidate the role of atMBCs in CHB by examining their relationship with hepatitis flare and virological parameters.
Methods: A total of 42 patients with CHB were prospectively enrolled, including NA-treated (n = 30) and treatment-naïve (n = 12) subjects. Patients represented a spectrum of disease activity and ALT levels. Hepatitis flare was defined as ALT > 5 times the upper limit of normal (ULN). Six subsets of B cells in peripheral blood mononuclear cells were analyzed by flow cytometry. Clinical parameters, including ALT, HBV DNA, and quantitative HBsAg levels were collected at the time of sampling. Linear regression and Spearman correlation analysis were applied when necessary with statistical significance defined as p < 0.05.
Results: The frequencies of atMBCs and activated memory B cells (actMBC) were significantly increased in CHB patients who were experiencing hepatitis
flares compared to normal ALT CHB patients (p = 0.003 and p = 0.0104, respectively). The frequency of atMBCs was not associated with age and gender. AtMBCs and actMBCs were highly correlated with each other (r = 0.7639, p < 0.0001). atMBCs were positively associated with HBV DNA levels (p = 0.0392), but not with HBsAg levels (p = 0.1806). In contrast, actMBCs demonstrated a significant positive correlation with HBsAg levels (p = 0.0182). Classical memory B cells (cMBC) and naïve B cells were reduced in patients with hepatitis flare, although the differences were not statistically significant (p = 0.342 and p = 0.1952, respectively). Interestingly, the ratio of atMBC/actMBC was numerically significantly higher in patients with ALT>5x ULN than patients with normal ALT (median: 4.112 vs. 2.547, p = 0.0811). This observation suggests that a higher grade of inflammation is associated with a stronger tendency toward the development of atMBC.
Conclusions: Hepatitis flare in CHB is associated with an increase in both atypical and activated memory B cells. Moreover, a higher grade of liver inflammation correlates with a stronger tendency toward the development of atypical memory B cells. This implies that functionally exhausted atypical memory B cells might play an important role in patients with high grade of inflammation.
EXTERNAL VALIDATION OF THE CHAMPS SCORE IN TAIWAN FOR PREDICTING IN-HOSPITAL MORTALITY AMONG PATIENTS WITH NON-VARICEAL UPPER GASTROINTESTINAL BLEEDING
Jung-Ching Liao1, Chung-Ying Lee1,2,3, Tsung-Chun Lee1,2,3
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taipei Medical University-Shuang Ho Hospital, New Taipei City, Taiwan
2TMU Research Center for Digestive Medicine, Taipei Medical University, Taipei, Taiwan
3Department of Internal Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan
台灣地區 CHAMPS 評分在非靜脈曲張性
上消化道出血病人住院死亡風險預測之 外部驗證研究
廖容靖1 李宗穎1,2,3 李宗錞1,2,3
1 衛生福利部雙和醫院消化內科
2 臺北醫學大學消化醫學研究中心
3 臺北醫學大學消化內科
Background: Non-variceal upper gastrointestinal bleeding (NVUGIB) remains a critical medical emergency with significant in-hospital mortality despite advances in endoscopic therapeutics. The Charlson comorbidity index–in-hospital onset–albumin–mental status–Eastern Cooperative Oncology Group performance status–steroids (CHAMPS) score, a novel risk stratification model developed in Japan, has shown promise in predicting mortality. However, external validation of the CHAMPS score in Asian populations outside of Japan is limited. This study aimed to explore the validity of the CHAMPS for predicting in-hospital mortality among NVUGIB patients treated at a tertiary-referred medical center in Taiwan. Secondary objectives included prediction of rebleeding and the need for rescue surgical interventions. We also compared the CHAMPS with other established scoring systems.
Aims: To validate the CHAMPS score for predicting in-hospital mortality in a Taiwanese cohort.
Methods: This single-center retrospective study enrolled adult patients (≥18 years) admitted for
NVUGIB who underwent endoscopic hemostasis at Taipei Medical University Shuang-Ho Hospital from January 2023 to December 2023. Patients with variceal bleeding, tumor bleeding, bleeding following endoscopic resection, or incomplete data were excluded. The predictive performance of CHAMPS and other scoring systems was assessed by calculating the area under the receiver operating characteristic curve (AUROC) using the DeLong test. Outcomes included in-hospital mortality (primary) as well as rebleeding and rescue surgical interventions (secondary). The study protocol was reviewed and approved by Research Ethics Committee.
Results: Among 193 patients, 111 met the inclusion/ exclusion criteria. The overall in-hospital mortality rate was 18.0% (20/111 cases). The CHAMPS score demonstrated excellent predictive accuracy for mortality (AUROC = 0.897), outperforming GBS (AUROC = 0.688, p = 0.001) and Rockall score (AUROC = 0.592, p < 0.0001). However, its performance was not significantly different from AIMS65 (AUROC: 0.897 vs. 0.839, p = 0.198) and the ABC score (AUROC: 0.897 vs. 0.818, p = 0.098). For secondary outcomes, CHAMPS showed suboptimal predictive value for rebleeding (22/111 cases) and rescue surgical interventions (9/111 cases) (AUROC = 0.638 and 0.570, respectively), not significant from other models.
Conclusions: Our preliminary study validated the CHAMPS score for predicting in-hospital mortality in a Taiwanese cohort. Further larger case-number studies are warranted to improve the CHAMPS score’s performance in predicting rebleeding and the need for surgical interventions.
Po-Chun Yang, Chu-Kuang Chou, Li-Jen Chang, Chang-Chao Su, Kok-Yean Koh, Shu-Hsien Lin, Tsung-Jung Tsai, Ming-Tse Hsu, Chi-Yi Chen, Po-Yueh Chen
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
精準影像技術助力食道癌早期檢測
楊博鈞 周莒光 張力仁 蘇昶昭 許國衍 林淑賢 蔡崇榮
許銘澤 陳啟益 陳柏岳
戴德森醫療財團法人嘉義基督教醫院胃腸肝膽科
Background: Early detection of esophageal cancer (ECA), particularly at the early stage, is vital for initiating timely treatment and improving patient outcomes. Conventional white light imaging (WLI) and narrow-band imaging (NBI) are widely used in endoscopic diagnosis, but their diagnostic accuracy is limited. Emerging technologies such as hyperspectral imaging (HSI) and artificial intelligence (AI) offer the potential to enhance early cancer detection.
Aims: This study aimed to evaluate the effectiveness of integrating HSI and AI-based object detection models for improved prediction of early-stage ECA and to compare their performance with traditional imaging modalities.
Methods: We collected and categorized 3,984 white light images (WLIs) and 3,666 narrow-band images (NBIs) into RGB-WLI and NBI datasets. The YOLOv5 deep learning model, a state-of-the-art object detection algorithm, was trained separately on four subsets derived from these datasets. Additionally, we developed a model trained with HSI-processed images. Performance metrics—including accuracy, precision, and recall—were calculated for each model.
Results: The model trained with HSI-processed images outperformed the standard NBI-based model, demonstrating an 8% increase in accuracy and a 5%–8% improvement in both precision and recall. Among all datasets, models trained on WLI images showed the most significant performance enhancement when combined with HSI and AI
technologies.
Conclusions: The integration of hyperspectral imaging with AI-based deep learning models significantly enhances the detection of early ECA compared to traditional imaging approaches. These findings support the incorporation of such technologies into clinical endoscopic systems to enhance diagnostic accuracy and efficiency in realworld healthcare settings.
OPTIMIZING GASTRIC CANCER DIAGNOSIS: THE ROLE OF SPECTRUM-AIDED VISUAL ENHANCER (SAVE) IN DEEP LEARNING APPLICATIONS
Kok-Yean Koh, Chu-Kuang Chou, Chang-Chao Su, Li-Jen Chang, Po-Chun Yang, Shu-Hsien Lin, Tsung-Jung Tsai, Ming-Tse Hsu, Chi-Yi Chen, Po-Yueh Chen
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
優化胃癌診斷:光譜輔助視覺增強器 (SAVE)在深度學習應用中的作用
許國衍 周莒光 蘇昶昭 張力仁 楊博鈞 林淑賢 蔡崇榮
許銘澤 陳啟益 陳柏岳
戴德森醫療財團法人嘉義基督教醫院胃腸肝膽科
Background: Early diagnosis is vital for effective GI disease treatment. While capsule endoscopy is more comfortable than traditional methods, it has limitations in navigation control, image resolution, and advanced imaging capabilities. This project integrates capsule endoscopy with HSI, NBI, and AI to develop a smart medical display system that enhances diagnostic precision and improves medical service quality.
Aims: This project aims to enhance GI disease detection by integrating advanced imaging and AI into capsule endoscopy. Key objectives: (1) develop an integration system combining HSI, NBI, and magnetic navigation; (2) improve image interpretability through AI; and (3) increase diagnostic accuracy for SCC and dysplasia, creating a solution that is both clinically effective and economical.
Methods: The project uses Quanyao Medical Electronics’ endoscope system with magnetic control and high-spectral imaging. Images are enhanced through National Chung Cheng University’s backend systems. YOLOv5 and YOLOv9 AI models detect lesions from hyperspectral data. ChengPing Technology’s system provides monitoring, clinical interface, and cloud storage. Chiayi Christian Hospital validates image datasets and diagnostic accuracy.
Results: YOLOv5 with HSI and NBI outperformed
YOLOv8 in identifying SCC and dysplasia. YOLOv5 achieved 85.1% precision (95% CI: 83.2–87.0%; p < 0.01) and 52.5% F1-score (95% CI: 50.1–54.9%; p < 0.01), while YOLOv8 reached 81.7% precision (95% CI: 79.6–83.8%; p < 0.01) and 49.4% F1-score (95% CI: 47.0–51.8%; p < 0.05). Building on these results, the project will integrate additional endoscopy images and implement YOLOv9 to target 90% accuracy for SCC diagnosis.
Conclusions: This project demonstrates the potential of combining capsule endoscopy with advanced imaging and AI for improved GI disease detection. HSI and NBI with YOLOv5 significantly enhanced diagnostic accuracy. With YOLOv9 implementation and further image integration, higher precision in SCC diagnosis is expected. This integrated platform will contribute to smarter, more precise GI diagnostics, enhancing clinical outcomes and healthcare quality.
LUGOL-VOID LESIONS AS POTENTIAL MARKERS OF ALCOHOL-RELATED ESOPHAGEAL RISK IN ALDH2DEFICIENT GENERAL POPULATION
Jyun-Han Lu1, Yu-Ching Huang2, Po-Chen Liang3, Bo-Rong Chen4, Chi-Sheng Yang1, Song-Wei Wang1, Yao-Kuang Wang1,2, I-Chen Wu1,2, Yi-Hsun Chen1,4
1Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
2School of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
3Division of Hepatobiliary, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
4School of Post Baccalaureate Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
以 Lugol 陰性病灶作為 ALDH2 缺乏一般
族群中酒精相關食道風險之潛在標記
盧俊翰1 黃郁清2 梁博程3 陳柏榮4 楊啓昇1 王崧維1
王耀廣1,2 吳宜珍1,2 陳以勳1,4
1 高雄醫學大學附設中和紀念醫院胃腸內科
2 高雄醫學大學醫學系
3 高雄醫學大學附設中和紀念醫院肝膽胰內科
4 高雄醫學大學學士後醫學系
Background: The Aldehyde dehydrogenase 2 (ALDH2) deficiency impairs acetaldehyde metabolism, increasing carcinogenic risk when combined with alcohol consumption. Retrospective studies have linked this interaction to a higher incidence of head and neck cancers. Lugol-voiding lesions (LVLs) are unstained esophageal areas during Lugol chromoendoscopy, associated with squamous cell carcinoma and dysplasia. Other research in patients with esophageal cancer suggests that the prevalence of LVLs is higher among individuals with ALDH2 deficiency and increased alcohol consumption.
Aims: This prospective cohort study investigates the association between LVLs, alcohol consumption, and ALDH2 deficiency in the general population.
Methods: After obtaining written informed consent,
participants completed a questionnaire assessing demographic information and alcohol consumption habits. Lugol chromoendoscopy was performed during the esophagogastroduodenoscopy (EGD) to evaluate the presence of LVLs. LVL grades A and B were classified as low-grade LVLs, while grades C and D were classified as high-grade LVLs. Saliva and blood samples were collected for genotyping of the ALDH2 and ADH1B genes. Data on LVLs, alcohol consumption, and ALDH2 deficiency were analyzed using SPSS statistical software.
Results: During September 2021 to June 2025, a total of 130 subjects were enrolled in the study, and after excluding the participants who did not want to receive lugol chromoendoscopy (N = 42) and few DNA to get the ALDH2 report (N = 7), 81 participants were enrolled to our study which comprising 25 females and 56 males, with a mean age of 51.8 years. Among the enrolled participants, those with highgrade LVLs were associated with higher alcohol consumption (363.8 ± 776.8 g/week vs. 180.7 ± 443.7 g/week, p = 0.363) and a greater prevalence of ALDH2 deficiency (12.5% vs. 4.1%, p = 0.207). Interestingly, individuals with ALDH2 deficiency also reported greater alcohol consumption to those without the deficiency (218.8 ± 632.4 g/week vs. 178.2 ± 333.5 g/week, p = 0.707). However, none of these differences reached statistical significance. Despite this, a trend was observed suggesting an association between high-grade LVLs, increased alcohol consumption, and ALDH2 deficiency. Conclusions: The findings of this study suggest a potential association between high-grade LVLs, increased alcohol consumption, and ALDH2 deficiency. Although statistical significance was not reached, a clear trend was observed. We plan to continue enrolling additional participants to enhance the statistical power of our analysis. In the future, we aim to further investigate whether Lugolvoiding lesions can serve as a feasible screening tool for early esophageal cancer, particularly among individuals with ALDH2 deficiency.
ASSOCIATION OF STREPTOCOCCUS
ANGINOSUS IN GASTRIC JUICE WITH GASTRITIS AND GASTRIC CANCER IN HUMAN
Song-Wei Wang1, Ju-Hui Wu2,3, Chung-Jung Liu1, Yu-Hsuan Yeh1, Bi-Chuang Weng1, Jaw-Yuan Wang4,5, Deng-Chyang Wu1,5, Chao-Hung Kuo1,5
1Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
2Department of Dentistry, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
3Department of Oral Hygiene, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
4Division of Colorectal Surgery, Department of Surgery, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
5School of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
胃液中咽峽炎鏈球菌與人類胃炎、胃癌 的關係
王崧維1 吳如惠2,3 劉忠榮1 葉于瑄1 翁碧娟1 王照元4,5 吳登強1,5 郭昭宏1,5
1 高雄醫學大學附設中和紀念醫院胃腸內科
2 高雄醫學大學附設中和紀念醫院牙科部
3 高雄醫學大學口腔衛生學系
4 高雄醫學大學附設中和紀念醫院大腸直腸外科
5 高雄醫學大學醫學系
Background: Despite the declining prevalence of Helicobacter pylori infections after eradication therapies, gastric cancer remains a significant global health concern. Previous studies have suggested that bacteria other than H. pylori may also contribute directly or indirectly to gastric carcinogenesis. Research in murine models has demonstrated that Streptococcus anginosus can induce gastric inflammation and subsequent gastric cancer.
Aims: Our study aims to investigate the association between the presence of Streptococcus anginosus in human gastric fluid and the occurrence of gastritis and gastric cancer.
Methods: We recruited 231 participants, including patients presenting with upper abdominal discomfort
scheduled for esophagogastroduodenoscopy (EGD), and patients with a history of gastric cancer undergoing surveillance EGD. During the endoscopic procedure, gastric juice samples were collected. These samples were then analyzed using quantitative Polymerase Chain Reaction (qPCR) to detect the presence of Streptococcus anginosus.
Results: Of the 231 participants, 135 (58.4%) were positive for S. anginosus (S.a(+)). A statistically significant association was observed between S. anginosus positivity and gender (p=0.036), with males more prevalent in the S.a(+) group. Gastric juice pH was also significantly higher in S.a(+) patients (mean 4.9 ± 2.0) compared to S.a(-) patients (mean 2.1 ± 1.7) (P<0.001). The percentage of S. anginosus positive cases progressively increased across gastritis without intestinal metaplasia (IM) (45.7%), gastritis with IM+ (58.6%), gastric cancer (GCA) post-treatment (76.9%), and GCA (92.3%).
Conclusions: Our findings indicate a strong association between the presence of Streptococcus anginosus in gastric fluid and the progression of gastric disease, from gastritis to gastric cancer. The higher prevalence of S. anginosus in patients with gastric cancer and those with more severe intestinal metaplasia suggests its potential role as a contributing factor or a significant marker in gastric carcinogenesis
PROGNOSTIC COMPARISON OF ENDOSCOPIC SUBMUCOSAL DISSECTION VERSUS SURGERY FOR UNDIFFERENTIATED EARLY GASTRIC CANCER: A MULTICENTER STUDY IN TAIWAN
Chen-Huan Yu1, Wei-Chen Tai2, Wen-Hung Hsu3, Ming-Yao Chen4, Chung-Ying Lee4, Tze-Yu Shieh5, Chu-Kuang Chou6, Hsu-Heng Yen7, Hsi-yuan Chien8, Sz-Iuan Shiu8, Jui-Wen Kang9, Wei-Chih Su10, Chen-Shuan Chung1
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan
2Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
3Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
4Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taipei Medical University Shuang Ho Hospital Ministry of Health and Welfare, New Taipei City, Taiwan
5Division of Gastroenterology, Department of Internal Medicine, Mackay Memorial Hospital, Taipei, Taiwan
6Division of Gastroenterology and Hepatology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
7Division of Gastroenterology, Changhua Christian Hospital, Changhua, Taiwan
8Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
9Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan
10Department of Gastroenterology, Buddhist Tzu Chi Medical Foundation, Taipei Tzu-Chi Hospital, New Taipei City, Taiwan
內視鏡黏膜下剝離術與外科手術治療未
分化型早期胃癌之預後比較:台灣多中
心研究
余臣桓1 戴維震2 許文鴻3 陳明堯4 李宗頴4 謝子鈺5 周莒光6 顏旭亨7 簡錫淵8 許斯淵8 康瑞文9 蘇偉志10 鍾承軒1
1 亞東紀念醫院肝膽胃腸科
2 高雄長庚紀念醫院胃腸肝膽科
3 高雄醫學大學附設中和紀念醫院胃腸內科
4 衛生福利部雙和醫院胃腸肝膽科
5 馬偕紀念醫院胃腸肝膽科
6 嘉義基督教醫院胃腸肝膽科
7 彰化基督教醫院胃腸肝膽內科
8 台中榮民總醫院胃腸肝膽科
9 國立成功大學醫學院附設醫院內科部
10 台北慈濟醫院肝膽腸胃科
Background: Endoscopic submucosal dissection (ESD) is considered a minimally invasive treatment alternative for early gastric cancer (EGC), yet its role in cases of undifferentiated-type histology is still subject to controversy.
Aims: This study evaluates and compares the clinical outcomes of ESD versus surgical treatment for undifferentiated early gastric cancer (UD-EGC) in Taiwan.
Methods: We conducted a retrospective analysis of data from patients with UD-EGC who were treated with either ESD or surgery at 11 hospitals in Taiwan between September 2007 and January 2025. Patients with UD-EGC who met the expanded indications (intramucosal, ≤20 mm in size, without ulceration or lymphovascular invasion) were included in the study. We collected demographic, endoscopic, and pathological data, and compared long-term outcomes, including recurrence and survival rates, between the two groups.
Results: A total of 37 patients who underwent ESD and 42 patients who had surgery for UD-EGC within expanded indications were analyzed. En bloc resection was successfully achieved in all cases, with R0 resection rates of 86% for ESD and 98% for surgery (P = 0.06). ESD was associated with significantly shorter mean procedure times (84.6 minutes vs. 285.7 minutes, P = 0.04) and shorter hospital stays (6.8 days vs. 17.6 days, P = 0.004) compared to the surgery group. The complication rates were similar (11% for ESD vs. 14% for surgery, P = 0.86). Although the 1-year, 3-year, and 5-year recurrence rates were comparable, survival analysis indicated a higher proportion of recurrence-free patients in the surgery
group (P = 0.017). The five-year overall survival rates were similar (89% for ESD vs. 88% for surgery, P = 0.92). In univariate analysis, ESD (P = 0.05), atrophic gastritis (P = 0.09), and non-margin-free resection (P = 0.05) were linked to an increased risk of recurrence, but none remained significant in multivariate analysis.
Conclusions: ESD provides a minimally invasive alternative to surgery for patients with UD-EGC who meet expanded indications, demonstrating similar short-term outcomes and survival rates. The higher long-term recurrence rate underscores the necessity for meticulous patient selection and diligent postESD monitoring, while the comparable survival rate suggests that ESD is a non-inferior treatment option compared to surgery.
SERUM MAC-2-BINDING PROTEIN GLYCOSYLATION ISOMER LEVEL HELPS TO PREDICT THE LONG-TERM COMPLICATIONS IN UNTREATED CHRONIC HEPATITIS C PATIENTS
Ze-Min Ling3, Tung-Hung Su1,2, Mei-Hsuan Lee4, Chun-Jen Liu1,2, Pei-Jer Chen1,2,5,6,7, Hung-Chih Yang1,2, Chen-Hua Liu1,2, Chi-Ling Chen6, Tai-Chung Tseng1,2,5, Chien-Hung Chen1,8, Hsuan-Shu Lee1, Chien-Jen Chen7, Jia-Horng Kao1,2,5,6
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
3Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
4Institute of Clinical Medicine, National Yang‐Ming Chiao Tung University, Taipei, Taiwan
5Department of Medical Research, National Taiwan University Hospital, Taipei, Taiwan
6Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
7Genomics Research Center, Academia Sinica, Taipei, Taiwan
8Department of Internal Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
血清 MAC-2 結合蛋白醣基化異構體的濃 度有助於預測未經治療的慢性丙型肝炎 患者的長期併發症
凌澤民3 蘇東弘1,2 李美璇4 劉俊人1,2 陳培哲1,2,5,6,7 楊宏志1,2 劉振驊1,2 陳祈玲6 曾岱宗1,2,5 陳健弘1,8 李宣書1 陳建仁7 高嘉宏1,2,5,6
1 國立臺灣大學醫學院附設醫院胃腸肝膽科
2 國立臺灣大學醫學院附設醫院肝炎研究中心
3 國立臺灣大學醫學院附設醫院內科部
4 國立陽明交通大學臨床醫學研究所
5 國立臺灣大學醫學院附設醫院醫學研究部
6 國立臺灣大學臨床醫學研究所
7 中央研究院基因體研究中心
8 國立臺灣大學醫學院附設醫院癌醫中心分院綜合內 科部
Background: The FIB-4 index is a simple way to
assess the risk of cirrhosis, HCC, and death in people with chronic hepatitis C. However, a diagnostic gray zone remains for those with intermediate FIB-4 values.
Aims: To investigate the predictive role of serum Mac2-binding protein glycosylation isomer (M2BPGi) for liver outcomes in HCV patients, particularly those with intermediate FIB-4 level.
Methods: We conducted a retrospective study to include untreated CHC patients who received longitudinal follow-up at National Taiwan University Hospital’s liver clinic from 1986 to 2014. We excluded patients with incomplete medical records, coinfection of hepatitis B or human immunodeficiency virus, or HCC development before the first year, or a followup duration of less than 3 years. The development of cirrhosis, HCC, and death were traced, and multivariable analyses were performed to identify predictors for adverse liver outcomes.
Results: A total of 772 patients from the ERADICATE-C cohort were included in the study. Their mean age was 55 years, 63% were female, and 80 patients had baseline cirrhosis. The median M2BPGi level was 1.2 cut-off index (COI), and the FIB-4 level was 2.1. After a median follow-up of 12 years, 207, 159, and 95 patients newly developed cirrhosis, HCC, and death, respectively. Among patients with intermediate baseline FIB-4 levels, elevated M2BPGi levels were significantly associated with an increased risk of cirrhosis (HR: 1.47; 95% CI: 1.29–1.68) and HCC (HR: 1.48; 95% CI: 1.27–1.72), but not with mortality. The cut-off point of 2.0 COI for M2BPGi was selected to achieve a specificity greater than 80% to further stratify the risk of HCC and cirrhosis. In the subgroup of HCV RNA-negative patients, M2BPGi also helped predict the future risk of hepatocellular carcinoma (HCC) and cirrhosis.
Conclusions: In patients with intermediate FIB-4, M2BPGi can predict the subsequent development of cirrhosis and HCC in untreated CHC patients.
⑭PULMONARY VASCULAR PERMEABILITY AND EXTRAVASCULAR LUNG WATER INDEX VARY WITH INFECTION SITE IN PATIENTS WITH LIVER CIRRHOSIS AND SEPTIC SHOCK
Hsiang-Ting Keng1, Kang-Wei Peng1, Ming-Ling Chang1, Rong-Nan Chien1, Yung-Chang Chen2, Ya-Chung Tian2, Ji-Tseng Fang2, Chih-Wei Yang2, Hui-Chun Huang3,4, Fa-Yauh Lee4, Ming-Hung Tsai1
1Division of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou Medical Center, Chang Gung University, Taoyuan, Taiwan
2Division of Critical Care Nephrology, Kidney Institute, Chang Gung Memorial Hospital, Linkou Medical Center, Chang Gung University, Taoyuan, Taiwan
3Division of Gastroenterology and Hepatology, Department of Medicine, Taipei Veteran General Hospital, Faculty of Medicine, YangMing University School of Medicine, Taipei, Taiwan
4Division of General Medicine, Department of Medicine, Taipei Veteran General Hospital, Faculty of Medicine, Yang-Ming University School of Medicine, Taipei, Taiwan
肝硬化併敗血性休克患者之肺血管通透 性指數與血管外肺水指數隨感染部位變 化
耿祥庭1 彭康維1 張明鈴1 簡榮南1 陳永昌2 田亞中2 方基存2 楊智偉2 黃惠君3,4 李發耀4 蔡銘鴻1
1 林口長庚紀念醫院胃腸肝膽科
2 林口長庚紀念醫院腎臟科
3 臺北榮民總醫院胃腸肝膽科
4 臺北榮民總醫院一般內科
Background: Patients with cirrhosis are susceptible to sepsis and septic shock. Responses to treatment for septic shock may vary significantly depending on the site of infection. While cirrhotic patients with spontaneous bacterial peritonitis (SBP) can benefit from volume expansion with albumin, nonSBP group is not conferred such a benefit. Safety concerns are even raised about lung edema in non-
SBP group treated with albumin infusion. Pneumonia represents one of the most common types of nonSBP infection. Pneumonia group has been shown to carry higher risk of developing lung edema during resuscitation in patients with liver cirrhosis and septic shock. Cirrhotic patients have increased pulmonary capillary permeability. It has been shown that increased pulmonary vascular permeability index (PVPI) and extravascular lung water index (EVLWI) are associated with a poor prognosis in cirrhotic patients with septic shock. It is conceivable that PVPI and EVLWI may differ with different types of infection, impacting the response to resuscitation. We hypothesize that PVPI and EVLWI are higher in the pneumonia group. Phenotyping pneumonia group by PVPI and EVLWI may represent a tool to risk stratify this specific group and help avoid pulmonary complication during volume resuscitation.
Aims: Pulse Indicator Continuous Cardiac Output (PiCCO) is an established tool to measure PVPI and EVLWI. Therefore, we conducted this retrospective study to investigate PVPI and EVLWI of different type of infection in cirrhotic patients with septic shock using PiCCO monitoring, with a special emphasis on pneumonia group.
Methods: We included 138 patients with liver cirrhosis and septic shock. EVLW indexed to actual body weight (aEVLWI), EVLW indexed to predicted body weight (pEVLWI), PVPI, disease severity scores, and other biomarkers were analyzed. We collected the PiCCO data on the first 2 days.
Results: The values of PVPI, aEVLWI, and pEVLWI were significantly higher in non-SBP patients, compared to SBP group. The pneumonia group constituted the most part of non-SBP patients (64.46%). In pneumonia group, the levels of PVPI, aEVLWI, and pEVLWI on day 2 were significantly higher in nonsurvivors. The discriminating power of PVPI on day 2 (PVPID2) to predict 28-day mortality of pneumonia group was tested using the area under a ROC curve. The areas under ROC curves (mean ± SEM) were 0.815 ± 0.051 for PVPID2. Those pneumonia patients with higher PVPID2 (>2.95) had higher SOFA score, CRP and 28-day mortality (80% vs. 26.7%, p < 0.001).
Conclusions: Higher levels of PVPID2 are associated with a higher inflammation state, disease severity and mortality rates in cirrhotic patients with pneumonia and septic shock. The source of infection may impact on response to treatment and clinical trial design.
STREAMLINING THE SCREENING PROCESS FOR HEPATITIS C VIRUS ELIMINATION IN A PRISON SETTING: AN UPDATED REPORT
Chia-Chia Lu1, Po-Han Chen1, Yen-Chun Peng2,3, Teng-Yu Lee2,4
1Division of Gastroenterology, Department of Internal Medicine, Taichung Veterans General Hospital Chiayi Branch, Chiayi, Taiwan
2Division of Gastroenterology & Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
3School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
4School of Medicine, Chung Shan Medical University, Taichung, Taiwan
C 型肝炎根除計畫:篩檢流 程優化後成果更新報告
呂家嘉1 陳柏翰1 彭彥鈞2,3 李騰裕2,4
1 臺中榮民總醫院嘉義分院肝膽腸胃科
2 臺中榮民總醫院胃腸肝膽科
3 國立陽明交通大學醫學系
4 中山醫學大學醫學系
Background: Hepatitis C virus (HCV) elimination is a critical public health priority, particularly among high-risk populations such as incarcerated individuals. Treatment completion in prisons is often hindered by inmate transfers or releases.
Aims: This study aimed to analyze the improvement in overall screening and treatment completion rates following the simplification of the screening process and the enhancement of HCV outpatient treatment support.
Methods: In this retrospectively cohort study, we analyzed data from incarcerated individuals at Chiayi Prison, Taiwan, who were enrolled in a HCV elimination program. The program included financial support, outreach mass screening, on-site clinics, and routine HCV surveillance for new prisoners to provide comprehensive care. Individuals who tested positive for HCV RNA received pangenotypic (directacting antivirals (DAAs). The primary endpoint was achieving a sustained virologic response 12 weeks after treatment completion (SVR12).
Results: From May 2024 to March 2025, a total of 3,707 incarcerated individuals were invited to
undergo anti-HCV screening, with 3,200 (86.3%) participating. Anti-HCV antibodies were detected in 10.7% (342/3,200) of participants, and 50.0% (161/322) of those tested positive for viremia. The treatment rate among viremic patients was 90.7% (146/161). A total of 143 patients completed a DAA treatment course, with 97.9% (143/146) achieving treatment completion. Among 121 patients who completed the SVR12 assessment by the end of June 2025, 95.87% were people who inject drugs (PWID), 18.18% experienced reinfection, and 57.85% had hepatitis B virus co-infection. The median baseline FIB-4 score was 1.12 (IQR: 0.85–1.49). Four patients had Child-Pugh class A cirrhosis, and another two had class B cirrhosis. The median baseline HCV RNA level was 6.43 log10 IU/mL (IQR: 5.75–6.68). The most prevalent genotype (GT) was GT-6 (47.9%), followed by GT-1 (26.5%) and GT-3 (13.2%). The SVR12 rate was 100%.
Conclusions: PWID constitute the majority of HCV-infected individuals in prison settings. With optimized screening and treatment process support, excellent efficacy has been demonstrated.
IMPACT OF HANDHELD ABDOMINAL ULTRASOUND ON TIMELINESS OF DIAGNOSTIC IMAGE AND ACCURACY IN GASTROENTEROLOGY AND HEPATOLOGY CONSULTATIONS: INTERIM ANALYSIS OF A CLUSTERRANDOMIZED CONTROLLED TRIAL
Mark Pi-Chun Chuang, Te-Yao Hsueh, Chun Hsun Liao, Che-Yu Rau, Han-Mo Chiu, Chun-Jen Liu
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
攜帶式腹部超音波輔助住院消化系照會 之影像時效與診斷正確性分析:叢集式 隨機試驗期中分析
莊弼鈞 薛德曜 廖俊勛 饒哲宇 邱瀚模 劉俊人
國立臺灣大學醫學院附設醫院內科部
Background: Handheld ultrasound has emerged as a valuable adjunct in evaluating acute abdominal conditions due to its portability, bedside accessibility, and diagnostic performance comparable to conventional ultrasound in select scenarios. Its incorporation into gastroenterology and hepatology consultations may streamline workflows and facilitate timely clinical decisionmaking during hospitalization.
Aims: To investigate whether integrating handheld abdominal ultrasound into the consultation process can reduce time to diagnostic evaluation without compromising diagnostic accuracy.
Methods: This single-center, prospective, timestratified, cluster-randomized controlled trial aimed to enroll 250 inpatients referred for gastroenterology or hepatology consultation over one year. Between December 2024 and June 19, 2025, 153 patients were enrolled and randomized to an intervention group (handheld ultrasound plus standard consultation) or a control group (standard consultation alone). The primary outcome was the time from consultation request to acquisition of diagnostic imaging. Secondary outcomes included diagnostic concordance with final outcomes and changes in clinical management.
Results: Among the 153 enrolled patients, 76 were assigned to the intervention group and 77 to the control group. The mean time to handheld
ultrasound in the intervention group (309 minutes) was significantly shorter than the mean time to conventional imaging in the control group (689 minutes) (p = 0.027, mean difference: 379.6, CI: 44.1, 715.1). Diagnostic agreement with final outcomes did not differ significantly between groups. Handheld ultrasound led to a change in clinical decision-making in 10 cases, corresponding to a number needed to scan (NNS) of 7.6.
Conclusions: Interim findings suggest that handheld abdominal ultrasound may expedite diagnostic imaging in hospitalized patients undergoing gastroenterology or hepatology consultation without compromising diagnostic accuracy. Pointof-care ultrasound represents a scalable strategy to enhance workflow efficiency and optimize resource use in inpatient settings.
DIFFERENTIAL IMPACT OF INTERFERON-BASED AND DIRECTACTING ANTIVIRAL THERAPIES ON BONE METABOLISM IN CHRONIC HEPATITIS C: INSIGHTS FROM TRANSCRIPTOMIC AND CLINICAL ANALYSES
Jung-Chun Lin1, Yi-Lin Chiu2, Tsai-Yuan Hsieh1, Tien-Yu Huang1, Hsuan-Hwai Lin1, Yu-Lueng Shih1,3
1Division of Gastroenterology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
2Department of Biochemistry, National Defense Medical University, Taipei, Taiwan
3Division of Gastroenterology, Department of Internal Medicine, Taichung Armed Forces General Hospital, Taichung, Taiwan
干擾素基礎療法與直接作用抗病毒藥物 療法對慢性 C 型肝炎骨代謝的差異化影 響:轉錄組學與臨床分析的見解
林榮鈞1 邱奕霖2 謝財源1 黃天祐1 林煊淮1 施宇隆1,3
1 國防醫學大學三軍總醫院胃腸科
2 國防醫學大學生物化學研究所
3 國軍臺中總醫院腸胃內科
Background: Chronic hepatitis C (CHC) is a known risk factor for hepatic osteodystrophy, which increases the likelihood of osteoporosis and fractures. While historical pegylated interferon/ribavirin (PEGIFN/RBV) therapy showed variable effects on bone, the impact of newer direct-acting antivirals (DAAs) on bone metabolism and osteoporosis risk remains less clear.
Aims: This study aimed to compare the effects of these distinct antiviral treatment strategies on bone metabolism in patients with CHC and to investigate the underlying mechanisms of these observed impacts.
Methods: We conducted a clinical study involving seventy-three treatment-naïve CHC patients at TriService General Hospital, Taipei, Taiwan. We assessed longitudinal changes in bone mineral density (BMD) and bone turnover markers (BTMs) after treatment with either PEG-IFN/RBV (n = 63) or DAA regimens (n = 10). To explore mechanistic insights, publicly available peripheral blood mononuclear cell (PBMC)
transcriptomic datasets from CHC patients treated with PEG-IFN/RBV (GSE7123) or sofosbuvir with ribavirin (SOF/RBV) DAA (GSE51699) were analyzed.
Results: Clinically, PEG-IFN/RBV therapy induced a temporary increase in lumbar spine BMD, followed by a post-treatment decline, and modulated BTMs. In contrast, DAA therapy demonstrated minimal effects on BMD or BTMs. PBMC transcriptomic analysis revealed that PEG-IFN/RBV responders experienced downregulation of osteoclast precursor (OCP)related gene sets and a concurrent upregulation of osteoblast-related gene sets (e.g., GO:0045669, BMP signaling). DAAs, however, showed minimal impact on these PBMC pathways.
Conclusions: These findings indicate that PEGIFN/RBV and DAA therapies have distinct effects on bone metabolism. PEG-IFN/RBV significantly modulates PBMC OCP (downregulation) and osteoblast-related (upregulation) gene expression, which contributes to the complex clinical changes observed in BMD. Conversely, DAAs appear bone neutral. This distinction underscores the importance of considering treatment-specific osteoporosis risk and surveillance needs in CHC patients.
CLINICAL AND HISTOPATHOLOGICAL SPECTRUM OF IGG4-ASSOCIATED AUTOIMMUNE HEPATITIS: A SYSTEMATIC REVIEW
Chun-Hsun Liao1, Hsu-Hua Tseng1,3, Ting-An Shen2, Tzu-Chan Hong3,4, Shih-Jer Hsu1,5, Jia-Horng Kao1,4,5, Chun-Jen Liu1,4,5
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Division of Chest, Department of Chest Medicine, National Taiwan University Hospital, Taipei, Taiwan
3Department of Internal Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
4Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
5Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
IgG4 相關自體免疫性肝炎的臨床與病理 特徵:一篇系統性回顧
廖俊勛1 曾旭華1,3 沈庭安2 洪子瞻3,4 徐士哲1,5 高嘉宏1,4,5 劉俊人1,4,5
1 國立臺灣大學醫學院附設醫院胃腸肝膽科
2 國立臺灣大學醫學院附設醫院胸腔科
3 國立臺灣大學醫學院附設醫院癌醫中心分院綜合內 科部
4 國立臺灣大學臨床醫學研究所
5 國立臺灣大學醫學院附設醫院肝炎研究中心
Background: IgG4-associated autoimmune hepatitis (IgG4-AIH) is an increasingly recognized diagnostic entity, characterized by an overlap of features seen in classical autoimmune hepatitis (AIH) and systemic IgG4-related disease (IgG4-RD). Since its initial description in 2007, a growing number of case reports and series have been published. However, this has led to significant heterogeneity, and the true prevalence and clinical significance of IgG4-AIH remain unclear.
Aims: This systematic review aims to synthesize all available published articles to comprehensively delineate the clinical and histopathological landscape of IgG4-AIH. The goal is to provide a clear and integrated overview to aid in the diagnosis and
management of this emerging disease and to guide future research directions.
Methods: Following PRISMA guidelines, a systematic literature search was in PubMed, Embase, and Web of Science up to March 20th, 2025. A rigorous selection process was conducted by paired reviewers, with a third reviewer mediating any disagreements via panel discussion. Summary data were extracted from eligible studies. Risk of bias assessment using the Joanna Briggs Institute (JBI) tools.
Results: A total of 1,289 articles were identified, of which 43 studies (32 case reports and 11 case series) met inclusion criteria. Our analysis revealed that the majority of IgG4-AIH patients were of Asian origin and showed a female predominance. Serologically, the most common autoantibody was anti-nuclear antibody (ANA) (73-78%), while serum IgG4 levels, though highly variable, exceeded the diagnostic threshold of 135 mg/dL in all cases. Histopathologically, high-grade interface hepatitis and plasma cell infiltration were the most frequent features. Notably, advanced fibrosis (Stage 3–4) was observed in approximately half of the patients. The prevalence of concurrent IgG4-RD in other organs was high in case reports (58%) but substantially lower in the aggregated data from case series (8.2%). Regarding treatment response, most patients responded rapidly to glucocorticoid therapy, with over 70% achieving biochemical remission within three months, a timeline significantly faster than the treatment goals for classical AIH.
Conclusions: This systematic review characterizes IgG4-AIH as a distinct clinical entity that bridges classical AIH and systemic IgG4-RD. Future efforts should focus on establishing consensus diagnostic criteria and elucidating its unique pathophysiology and long-term prognosis through large, prospective cohort studies.
HIGH SEMA4B EXPRESSION AND HYPOMETHYLATION: DRIVERS OF PANCREATIC ADENOCARCINOMA (PAAD) PROGRESSION AND IMMUNOSUPPRESSIVE MICROENVIRONMENT
Cheng-Shin Tsai1, Pei-Yi Chu1,3, Hung-Yu Lin1,2
1Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan
2Research Assistant Center, Show Chwan Memorial Hospital, Changhua, Taiwan
3Department of Pathology, Show Chwan Memorial Hospital, Changhua, Taiwan
高表達的 SEMA4B 及其低甲基化:胰腺 腺癌(PAAD)進展與免疫抑制微環境的 驅動因素
蔡承欣1 朱旆億1,3 林宏昱1,2
1 國立中興大學學士後醫學系
2 秀傳紀念醫院研究中心
3 秀傳紀念醫院病理部
Background: Pancreatic adenocarcinoma (PAAD), comprising 80% of pancreatic cancer cases, represents 4.88% of all new cancer diagnoses in Taiwan (Taiwan Ministry of Health and Welfare). Although its incidence is comparatively lower than other malignancies, PAAD is associated with a disproportionately high mortality rate due to its asymptomatic nature in early stages, resulting in delayed diagnosis and poor prognosis. Surgical resection is the most effective treatment but is limited to stages I and II. Neoadjuvant therapy is often required due to the complexity of PAAD. Semaphorins, known to regulate various malignancy-associated processes, have unclear mechanistic roles in PAAD.
Aims: This study investigates the expression and methylation of Semaphorin 4B (SEMA4B) in relation to diagnosis, prognosis, immune microenvironment, mutation burden, and pharmacogenomics in PAAD.
Methods: The correlation between copy number variation (CNV) and expression levels of SEMA4B was analyzed using DriverDB v4. Differential expression and promoter methylation were evaluated via UALCAN. Prognostic significance was assessed using Kaplan-Meier Plotter. Immune infiltration
was analyzed through GSCA and TISIDB. Gene set enrichment analysis (GSEA) was conducted using GENI. Drug sensitivity screening was performed using GSCA and DepMap portals.
Results: SEMA4B expression positively correlated with CNV and was significantly elevated in tumor tissues. Promoter hypomethylation was observed in tumors, particularly in stages I and II. Elevated SEMA4B expression was associated with higher histological grades and poor overall survival. Additionally, SEMA4B expression negatively correlated with anti-tumor immune cells (e.g., NK cells, cytotoxic T cells) and positively correlated with pro-tumor immune cells (e.g., nTregs, Th2), indicating an immunosuppressive microenvironment. GSEA revealed SEMA4B’s association with cell cycle checkpoint pathways. Sensitivity to FDA-approved drugs, including Afatinib, Gefitinib, Lapatinib, Trametinib, and Alectinib, was observed in cells with high SEMA4B expression. SEMA4B also correlated positively with oncogenes (KRAS, ERBB2) and negatively with tumor suppressors (SMAD4).
Conclusions: SEMA4B promoter hypomethylation contributes to its overexpression, with significant diagnostic and prognostic implications. Its role in shaping an immunosuppressive tumor microenvironment and guiding precision medicine warrants further investigation through preclinical and clinical studies.
Hsing-Chien Wu1,4, Chien-Hui Wu2,5, Wei-Chih Liao3,4
1Department of Medicine, National Taiwan University Cancer Center
2Department of Surgery, National Taiwan University Hospital, Taipei, Taiwan
3Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
4Department of Internal Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
5Department of Surgery, National Taiwan University College of Medicine, Taipei, Taiwan
應用三維血液切片技術檢測胰臟癌與胰 臟囊腫患者之周邊血單核細胞:一項前 瞻性初步研究
吳行健1,4 吳健暉2,5 廖偉智3,4
1 國立臺灣大學醫學院附設醫院癌醫中心分院綜合內 科部
2 國立臺灣大學醫學院附設醫院外科部
3 國立臺灣大學醫學院附設醫院胃腸肝膽科
4 國立臺灣大學醫學院內科
5 國立臺灣大學醫學院外科
Background: Pancreatic cancer inherited with a poor prognosis, with a 5-year survival rate of around 10%, making it one of the most lethal malignancies. The lack of obvious symptoms during early-stage results in approximately 85%–90% of cases being diagnosed at advanced stages. Surgical resection for early pancreatic cancer is the most likely management to cure, but effective early diagnostic tools are lacking. Circulating tumor cells (CTCs) can be detected when the tumor of pancreatic ductal adenocarcinoma (PDAC) is small than 1cm using the most advanced technology before tumor being detected by imaging. CTCs and circulating epithelial cells (CECs) together constitute at most approximately 0.09% of all peripheral blood mononuclear cells (PBMCs), which are isolated from whole blood by separating
them from red blood cells, granulocytes, and plasma. PBMCs are mostly B or T lymphocytes (60%–75%), NK cells (5%–15%), monocytes (10%–20%), and dendritic cells (<1%–2%); thus, identification of CTCs or CECs are technically difficult. Pancreatic cancer inherited with a poor prognosis, with a 5-year survival rate of around 10%, making it one of the most lethal malignancies. The lack of obvious symptoms during early-stage results in approximately 85%–90% of cases being diagnosed at advanced stages. Surgical resection for early pancreatic cancer is the most likely management to cure, but effective early diagnostic tools are lacking. Circulating tumor cells (CTCs) can be detected when the tumor of pancreatic ductal adenocarcinoma (PDAC) is small than 1cm using the most advanced technology before tumor being detected by imaging. CTCs and circulating epithelial cells (CECs) together constitute at most approximately 0.09% of all peripheral blood mononuclear cells (PBMCs), which are isolated from whole blood by separating them from red blood cells, granulocytes, and plasma. PBMCs are mostly B or T lymphocytes (60%–75%), NK cells (5%–15%), monocytes (10%–20%), and dendritic cells (<1%–2%); thus, identification of CTCs or CECs are technically difficult. Previous techniques demonstrated suboptimal sensitivity for detecting early-stage PDAC, whereas the novel 3D blood slice technology offers promising potential for accurate early detection.
Aims: We aimed to explore the diagnostic potential of circulating tumor cell methods with 3D blood slice technology.
Methods: From June, 2023 to December, 2023, eligible patients with and without a diagnosis of PDAC were enrolled in National Taiwan University Hospital Cancer Center and National Taiwan University Hospital. Eight milliliters of blood was drawn from each participant and underwent preparation within 8 hours. Following erythrocyte depletion, PBMCs are preserved. PBMC within the are subsequently labeled with immunofluorescent antibodies of DAPI (nucleus), CA19-9 protein, CD4, CD11b, CD163, CD14, CD68, and CD16. The entire cell suspension is then immobilized in a three-dimensional matrix and subjected to rapid volumetric imaging with laser-based fluorescence microscopy (Nebulum Technologies). Receiver operating characteristic (ROC) curves and areas under the curve (AUC) for the diagnosis of PDAC in the population. Using DeLong method, AUC of CA19-9 will be compared to that of
Results: In this pilot study, a total of 29 patients were enrolled, including 9 and 20 patients with and without PDAC, respectively. Patients with PDAC were younger than non-PDAC participants. Among patients with PDAC, 1 (11.1%), 2 (22.2%), 2 (22.2%), and 4 (44.4%) were classified as stage I, II, III, and IV, respectively. Among participants without PDAC, 10 (50.0%) had pancreatic cystic lesions and 1 (5.0%) had chronic pancreatitis. For the microscopic findings of PBMC, the CA19-9+ circulating cells and immune cells were well demonstrated, and unique CA19-9+/immune cell clusters were identified. The average (95% CI) CA19-9+ cell numbers were 4.38 (1.35), 18.48 (8.92), and 146.78 (51.10) in normal, cyst/pancreatitis, and PDAC groups, respectively. The immune cell ratio within cell clusters—calculated by dividing the number of immune cells by the total number of CA19-9+ and immune cells—was 0.79, 0.65, and 0.12 in the normal, cystic/pancreatitis, and PDAC groups, respectively. When used as diagnostic markers for PDAC, the area under the ROC curve (AUC) was 0.98 for CA19-9+ cells, 0.99 for the immune cell ratio, and 0.94 for serum CA19-9. When the sensitivity for diagnosis was 100%, the specificity for CA19-9+ cell (cut-off: 19/8 ml), serum CA19-9 (cutoff: 33.08 U/ml), and immune cluster ratio (cut-off: 0.316) were 84%, 84%, and 95%, respectively.
Conclusions: In a pilot study utilizing 3D blood slice technology for PBMC analysis, the clustering of CA19-9+ cells with immune cells emerged as a unique phenomenon, suggesting its potential as a diagnostic biomarker for PDAC. In addition, CA19-9+ circulating cells were also detected in participants with pancreatic cystic lesions, highlighting the potential utility of this technology for surveillance and diagnosis in this population.
DIAGNOSTIC PERFORMANCE OF ENDOSCOPIC ULTRASOUNDGUIDED TISSUE ACQUISITION FOR MALIGNANT PANCREATIC SOLID TUMORS IN A SOUTHERN MEDICAL CENTER
Jui-Hsiang Li1, Wei-Chih Sun1,4, Tzung-Jiun Tsai1,3, Wen-Chi Chen1,3, Wei-Lun Tsai1,2,3, Feng-Woei Tsay1,3
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
2Division of General Medicine, Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
3School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
4Institute of Biomedical Sciences, National Sun Yat-sen University, Kaohsiung, Taiwan
內視鏡超音波導引組織採樣對於惡性胰 臟固態腫瘤之診斷表現:南部一家醫學 中心之研究
李瑞祥1 孫煒智1,4 蔡騌圳1,3 陳文誌1,3 蔡維倫1,2,3
蔡峯偉1,3
1 高雄榮民總醫院胃腸肝膽科
2 高雄榮民總醫院一般內科
3 國立陽明交通大學醫學系
4 國立中山大學生物醫學研究所
Background: Endoscopic ultrasound-guided tissue acquisition (EUS-TA) is essential for the diagnosis of pancreatic tumors. The ASGE guidelines suggests a diagnostic rate of at least 70% as a key quality indicator for malignancy on EUS-TA of pancreatic mass lesions.
Aims: To identify factors that determined the diagnostic performance of EUS-TA for malignant pancreatic solid tumors.
Methods: A total of 150 patients, who underwent EUS-TA for pancreatic solid tumors between December 2019 and December 2024, were enrolled in this study. At our institute, we embarked EUSTA in 2019, and both rapid on-site evaluation in cytology and routine sedation were unavailable till now. Clinical and procedural factors were analyzed and compared for patients with definitive and inconclusive EUS-TA sampling for the diagnosis of
malignant pancreatic solid tumors.
Results: A total of 156 EUS-TA samples were included, of which 29 cases (18.6%) were inconclusive. Of 24 patients without a definite diagnosis from initial EUS-TA, 9 were proved to have pancreatic cancer by surgery, 7 by clinical progression of malignant behavior, 4 by repeat EUS-TA, 2 by CT-guided biopsy, 1 by trans-papillary biopsy, and 1 by endoscopic biopsy of duodenal tumor invasion. There were 2 (1.3%) adverse events, including mild degree pancreatitis and self-limited immediate bleeding. In univariate analyses, concurrent pancreatitis, concurrent biliary obstruction, pre-procedural biliary drainage, tumor located at the head or uncinate, tumor size smaller than 2cm, trans-duodenal access, and patient intolerance were associated with a higher rate of inconclusive diagnosis. In the multivariate analysis, patient intolerance was the only independent and significant determining factor for the diagnostic performance of EUS-TA for malignant pancreatic solid tumors (OR: 0.031; 95% CI: 0.003 to 0.332; p = 0.004).
Conclusions: Our diagnostic yield of EUS-TA for malignant pancreatic solid tumors was acceptable. When initiating EUS-TA, employing strategies to reduce procedure time and minimize patient discomfort may enhance diagnostic performance.
EARLY NEEDLE-KNIFE PRECUT OVER PANCREATIC STENT VERSUS TRANSPANCREATIC SPHINCTEROTOMY IN DIFFICULT
BILIARY CANNULATION: A PROSPECTIVE RANDOMIZED CONTROLLED TRIAL (ENKPT TRIAL)
Kuan-Fu Huang, Fai-Meng Sou, Yi-Chun Chiu, Lung-Sheng Lu, Cheng-Kun Wu, Chung-Mou Kuo, Pao-Yuan Huang, Chih-Ming Liang
Division of Hepato-Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
困難性膽道插管中兩種技術之比較:針 刀預切合併胰管支架與經胰管括約肌切
開術之前瞻性隨機試驗
黃冠輔 蘇輝明 邱逸群 盧龍生 吳鎮琨 郭仲謀 黃寳源 梁志明
高雄長庚紀念醫院胃腸肝膽科系
Background: Selective bile duct cannulation is essential in therapeutic endoscopic retrograde cholangiopancreatography (ERCP), yet remains unsuccessful in 10–20% of cases despite experienced hands. When standard techniques fail, advanced methods such as needle-knife precut papillotomy (NKPP) and transpancreatic sphincterotomy (TPS) are employed. In the previous RCT trail, “Early” precut is an effective technique and can significantly reduce the incidence of PEP. Repeated biliary cannulation attempts are a real risk factor for this complication. While both techniques have been studied individually, randomized controlled trials comparing early NKPP over a pancreatic stent (NKPSIPS) with TPS in difficult cannulation cases remain limited.
Aims: To compare the efficacy and safety of “Early” NKPP over a pancreatic stent versus TPS in patients with difficult biliary cannulation, with respect to cannulation success rate, procedural time, and adverse events.
Methods: This prospective, randomized controlled trial was conducted at Kaohsiung Chang Gung Memorial Hospital, Taiwan, from November 2021 to May 2025. ERCP-naïve patients aged ≥20 years
undergoing therapeutic ERCP were screened. “Difficult cannulation” was defined as failure to achieve bile duct cannulation within 5 minutes or after ≥3 unintended main pancreatic duct (MPD) cannulations. Patients with ≥3 MPD cannulations were randomized 1:1 into two groups: (1) NKPP following pancreatic stent placement (NKP-SIPS group), and (2) TPS with pancreatic stent placement (TPS group). Patients with complete CBD and MPD cannulation failure received NKPP or fistulotomy based on papillary morphology and were excluded from randomization. The primary endpoint was successful CBD cannulation. Secondary outcomes included adverse events: post-ERCP pancreatitis (PEP), perforation, and bleeding. All ERCPs were performed by a single experienced endoscopist using a side-viewing duodenoscope and standard accessories. In the NKP-SIPS group, a 5-Fr pancreatic stent was placed prior to a limited (<5 mm) freehand needle-knife incision directed at the biliary sphincter. TPS was performed following pancreatic duct cannulation, with a pull-type sphincterotome used to incise the septum between the pancreatic and bile ducts (11–12 o’clock direction). Pancreatic duct stents and prophylactic measures including rectal diclofenac 50mg and aggressive IV hydration were applied as appropriate. Block randomization was conducted using one block with 4 numbers with allocation concealed from the performing endoscopist until after inclusion.
Results: Of the 513 ERCP procedures performed during the study period, 351 involved patients with naïve papillae. Among these, 71 cases (20.2%) met criteria for difficult biliary cannulation requiring sphincterotomy-based intervention. After applying exclusion criteria (prior sphincterotomy, active pancreatitis, coagulopathy, inadequate sedation, periampullary tumor, or refusal of consent), 40 patients consented to randomization: 20 were assigned to the NKP-SIPS group and 20 to the TPS group. The primary endpoint of successful bile duct cannulation was achieved in all 20 patients (100.0%) in the NKP-SIPS group compared to 17 out of 20 (85.0%) in the TPS group (P = 0.072). The mean time to achieve successful cannulation was 18.1 ± 8.2 minutes in the NKP-SIPS group and 16.4 ± 5.2 minutes in the TPS group (P = 0.466). The total procedural duration was also comparable between groups: 28.2 ± 11.0 minutes for NKP-SIPS and 26.7 ± 9.0 minutes for TPS (P = 0.594). Post-ERCP pancreatitis occurred in 2 patients (10.0%) in each group (P =
1.000). Bleeding was observed in 5 patients (25.0%) in the NKP-SIPS group and 3 patients (15.0%) in the TPS group (P = 0.429). All bleeding events were selflimited and resolved spontaneously without the need for endoscopic or surgical intervention. No perforations were observed in either group.
Conclusions: In this prospective randomized controlled trial, both early needle-knife precut papillotomy over a pancreatic stent (NKP-SIPS) and transpancreatic sphincterotomy (TPS) demonstrated high cannulation success and comparable safety profiles in patients with difficult biliary cannulation. Although the NKP-SIPS group achieved a numerically higher cannulation success rate, the difference did not reach statistical significance.
Chia-Tien Hsieh1, Kuo-Kuan Chang1, Gour-Shenq Kao2, Yuan-Chi Mao1, I-I Chen1, Ruey-Chang Lin1
1Department of Hepatogastroenterology, Tainan Municipal Hospital (Managed By Show Chwan Medical Care Corporation), Tainan, Taiwan
2Research Assistance Center, Show Chwan Health Care System, Changhua, Taiwan
BAP1 基因在膽管癌中的表現分析
1 張國寬1 高國勝2 毛元治1 陳一毅1 林瑞昌1
1 台南市立醫院(委託秀傳醫療社團法人經營)腸胃 內科
2 秀傳紀念醫院醫學研究輔佐中心
Background: Cholangiocarcinoma (CCA), a highly lethal cancer of the bile ducts, is a relatively rare but increasingly encountered aggressive malignancy with a dismal prognosis overall. The etiology of cholangiocarcinoma is both multifactorial and not entirely understood.
Aims: This study aimed to identify candidate signaling molecules for potential diagnostic and therapeutic applications.
Methods: Functional genomic characterization robustly elucidated signaling cascade expression profiles in cholangiocarcinoma, derived from the Cancer Genome Atlas (TCGA) dataset. This work highlights a promising therapeutic potential for further study.
Results: The expression of BRCA1-associated protein 1 (BAP1) demonstrates its specificity role (as 4.8:4.0) across cholangiocarcinoma tumor samples (n = 36) paired with normal tissues (n = 9) within the Cancer Genome Atlas (TCGA). The finding potentially undermines its established function as a tumor suppressor. Genomic instability, rather than DNA methylation, facilitates those outcomes, thereby challenging BAP1’s presumed function as a tumor suppressor. Cholangiocarcinoma samples exhibited a 15.7% BAP1 mutation frequency, characterized by frameshift (3.9%), nonsense (3.9%), and missense (7.8%) mutations at varying percentages. Genomic instability alterations are correlated with the process of natural aging. The Kaplan-Meier survival analysis stratified by BAP1 gene expression demonstrated a
marked divergence between cholangiocarcinoma cohorts. Patients with high BAP1 expression experienced a rapid decline, with complete mortality observed by approximately 2000 days. In contrast, those with low BAP1 expression retained a survival rate near 40% by the end of the study period, although this difference did not reach statistical significance. Additionally, race emerged as a significant clinical factor associated with survival outcomes (ANOVA p = 1.2 × 10-²).
Conclusions: Elevated BAP1 gene expression demonstrates a potential correlation with unfavorable prognoses in cholangiocarcinoma, warranting further investigation through expanded studies to validate statistical relevance. Observed racial stratification emphasizes the influence of population-specific variables on clinical outcomes, thereby necessitating consideration of such factors in therapeutic strategies.
㉔CLINICAL UTILITY AND SAFETY OF A NOVEL ULTRA-SLIM CATHETERTYPE PERORAL CHOLANGIOSCOPE/ PANCREATOSCOPE (UCPOCS/ UCPOPS) : A SINGLE-CENTER CASE SERIES
Yosuke Miwa, Hiroyuki Kojima, Takayoshi Tsuchiya, Reina Tanaka, Ryosuke Tonozuka, Shuntaro Mukai, Kazumasa Nagai, Yukitoshi Matsunami, Hirohito Minami, Noriyuki Hirakawa, Kyoko Asano, Kazuki Hama, Takao Itoi
Department of Gastroenterology and Hepatology, Tokyo Medical University Hospital, Tokyo, Japan
Background: Peroral cholangioscopy (POCS) and pancreatoscopy (POPS) are increasingly used to evaluate biliary and pancreatic diseases. However, the relatively large diameter (≈4 mm) of conventional scopes limits their utility in narrow ducts. A newly developed ultra-slim catheter-type peroral cholangioscope/pancreatoscope (UCPOCS/ UCPOPS; DRES Slim Scope, Japan Lifeline, Tokyo) with an outer diameter of 2.3 mm may overcome this limitation.
Aims: To evaluate the clinical utility and safety of UCPOCS/UCPOPS in patients with pancreatobiliary diseases.
Methods: We conducted a retrospective singlecenter observational study of 12 patients who underwent UCPOCS or UCPOPS from November 2022 to August 2024. UCPOCS was used in 8 cases for bile duct stones (n = 3), strictures (n = 3), tumors (n = 1), bleeding (n = 1), and endoscopic nasogallbladder drainage (n = 1). UCPOPS was used in 4 cases: 2 for post-stone removal and 2 for intraductal papillary mucinous neoplasm (IPMN). Antibiotics were used in 6 cases (4 prophylactically, 2 for inflammation).
Results: Biliary observation was achieved in all UCPOCS cases, even in ducts as narrow as 1.8 mm. In one case, bleeding was identified post-hepatectomy using UCPOCS. Another case initially showed no malignancy on UCPOCS but was later diagnosed with adenocarcinoma, indicating the importance of shortterm follow-up. In the UCPOPS group, observation was feasible even after duodenopancreatectomy using balloon-assisted ERCP. One patient developed mild post-ERCP pancreatitis (PEP), which resolved with conservative management. No other adverse
events occurred, and no significant difference in cholangitis incidence was observed with or without antibiotic use.
Conclusions: UCPOCS and UCPOPS were effective and safe in evaluating narrow bile and pancreatic ducts. Their affordability, ease of setup, and minimal complications support their broader application in clinical practice.
THE EFFICACY OF WATER EXCHANGE COLONOSCOPY WITH COMPUTERAIDED DETECTION, LINKED-COLOR IMAGING, AND ENDOCUFF VISION (WE-COMBO) IN INCREASING PROXIMAL SERRATED POLYP DETECTION RATE: A SINGLE-CENTER, OBSERVATIONAL STUDY
Chi-Liang Cheng1, Yen-Lin Kuo1, I-Chia Su1, Yi-Ning Tsui1, Bai-Ping Lee1, Hui-Ting Lin1, Yan-Lun Syu1, Zi-Wei Chen2, Yun-Shien Lee2
1Division of Gastroenterology, Department of Medicine, Evergreen General Hospital, Taoyuan, Taiwan
2Department of Biotechnology, School of Health Technology, Ming Chuan University, Taoyuan, Taiwan
換水法大腸鏡合併使用人工智慧息肉偵 測系統、影像強化內視鏡技術與視野擴 充帽蓋對提高近端大腸鋸齒狀息肉偵測 率的效果評估:一單中心觀察性研究
鄭吉良1 郭彥麟1 蘇怡佳1 崔怡寧1 李百萍1 林慧婷1 許晏綸1 陳子瑋2 李御賢2
1 中壢長榮醫院胃腸科 2 銘傳大學生物科技學系
Background: The proximal serrated polyp detection rate (SPDR) is inversely associated with postcolonoscopy colorectal cancer risk. Water exchange (WE) colonoscopy with computer-aided detection (CADe) assistance (WE-CADe) increased polyp detection compared with WE alone in a recently completed randomized controlled trial (RCT) (WEAID trial [NCT06173258]). Linked-color imaging (LCI) and Endocuff Vision (ECV) separately enhanced the sessile serrated lesion (SSL) detection rate in RCTs.
Aims: We aimed to determine whether the inclusion of LCI and ECV with WE-CADe (WE-COMBO) led to a significantly higher proximal SPDR compared with WE-CADe alone.
Methods: This observational study was conducted at Evergreen Hospital, Taiwan, using the CAD-EYE CADe system (Fujifilm, Tokyo, Japan). Patients aged 45-75 years undergoing WE with routine indications were enrolled. Data for the WE-CADe group were derived from the WEAID trial, conducted between
December 2023 and June 2024. Data for the WECOMBO group were collected prospectively on consecutive patients undergoing CADe-assisted WE between July and November 2024. The proximal colon included colon segments from the cecum to the splenic flexure. Serrated polyps included SSL, traditional serrated adenomas (TSA), and hyperplastic polyps (HP). Non-neoplastic lesions were defined as those with histological diagnoses other than malignancy, conventional adenomas, SSLs, TSAs, HPs measuring ≥ 10 mm anywhere in the colon, or HPs measuring 6-9 mm in the proximal colon. The primary outcome was proximal SPDR. Secondary outcomes included adenoma detection rate (ADR) and SSL detection rate.
Results: A total of 280 patients (men: 52.9%; mean age: 58.0 ± 8.1 years; 140 for each group) were included in the intention-to-treat analysis. Both groups had similar baseline and clinical characteristics, except more patients in the WECOMBO group had screening indications and more patients in the WE-CDAe group had surveillance indications. Proximal SPDR was significantly higher in the WE-COMBO group than in the WE-CADe group (75.7% vs. 62.1%, relative risk [RR] = 1.89, 95% confidence interval [CI] [1.13 3.18], P = 0.020). The WE-COMBO group had a higher SSL detection rate compared with the WE-CADe group, but the difference was not significant (7.1% vs. 4.3%, RR = 1.72, 95% CI [0.61 4.86]). There was no significant difference in overall ADR (59.3% vs. 57.9%, RR = 1.06, 95% CI [0.55 1.71]). Withdrawal times and the nonneoplastic lesion resection rate were comparable between groups.
Conclusions: For CADe-assisted WE colonoscopy, the integration of LCI and ECV significantly increased proximal SPDR without prolonging the withdrawal time or causing a concomitant increased nonneoplastic lesion resection. Whether the inclusion of all polyp optimization techniques will significantly enhance proximal SPDR and overall SSL detection rate warrants further investigation.
EVALUATION OF TOLERABILITY AND GASTROINTESTINAL SYMPTOM IMPROVEMENT WITH A LOWOSMOLARITY REHYDRATION
SOLUTION CONTAINING LACTOBACILLUS RHAMNOSUS GG DURING THE POST-COLONOSCOPY POLYPECTOMY RECOVERY PERIOD
Chien-An Chen
Department of Hepato-Gastroenterology, Da-An Women and Children Hospital, Tainan, Taiwan
液於大腸息肉切除術後恢復期之耐受性 與腸胃症狀改善成效評估 陳建安
大安婦幼醫院胃腸肝膽科
Background: Colorectal polyps, such as tubular adenomas (TA), sessile serrated adenomas/polyps (SSA/P), and traditional serrated adenomas (TSA), are well-established precursors to colorectal cancer. Timely removal through polypectomy is essential for prevention. However, post-polypectomy gastrointestinal symptoms—such as abdominal pain, bloating, diarrhea, and rectal bleeding— may impact patient recovery and adherence to surveillance protocols. Lactobacillus rhamnosus GG (LGG) is a widely studied probiotic known to restore microbiota balance, strengthen the intestinal barrier, and modulate host immunity. Muco-relax LGG+ORS powder drink combines LGG with a low-osmolarity oral rehydration solution to support hydration, electrolyte balance, and gut microbial homeostasis.
Aims: This randomized controlled trial evaluated whether supplementation with this formulation during the recovery period could alleviate gastrointestinal symptoms following colorectal polypectomy.
Methods: Participants: Adults scheduled for colorectal polypectomy for TA, SSA/P or TSA (≥0.5 cm in size) were enrolled. Study Design: Participants were randomized into: (1) Control group: 600 mL/ day bottled water. (2) Experimental group: 600 mL/day Muco-relax LGG + ORS powder drink. (3) The intervention began on Day 0 (surgery day) and continued through Day 6. Outcome Measures:
Participants recorded daily self-assessments of: (1) Rectal bleeding, (2) Abdominal pain, (3) Bloating, (4) Diarrhea, (5) Constipation/difficulty defecating.
Results: A total of 90 participants were enrolled and randomized into the experimental group and control group. Baseline characteristics: There were no statistically significant differences between the two groups in baseline characteristics, including age, sex, height, weight, polyp size, operative time, or incidence of preoperative gastrointestinal symptoms (p > 0.05 for all comparisons). Postoperative gastrointestinal symptom trends: During the 7-day postoperative intervention period, the overall incidence of selfreported gastrointestinal symptoms (rectal bleeding, abdominal pain, abdominal bloating, diarrhea, and constipation) showed a statistically significant trend of reduction over time in both groups. Differences in the incidence of postoperative gastrointestinal symptoms: Compared to the control group, the experimental group reported significantly fewer incidents of rectal bleeding (p = 0.0205) and diarrhea (p = 0.0248), but there were no statistically significant differences in abdominal pain, abdominal bloating, or constipation.
Conclusions: Post-polypectomy supplementation with a low-osmolarity rehydration solution containing LGG significantly reduced rectal bleeding and diarrhea. The formulation was well tolerated and may enhance mucosal healing and microbiota stability. This probiotic-electrolyte solution offers a promising adjunct for gastrointestinal symptom management following colorectal polypectomy.
THE PROGNOSTIC VALUE OF TISSUE BIOENERGETICS IN COLORECTAL CANCERS AND PERIPHERAL
Wei-En Hou1, Wey-Ran Lin1,2,3
1Department of Gastroenterology and Hepatology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
2College of Medicine, Chang Gung University, Taoyuan, Taiwan
3Liver Research Center, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
結直腸癌與鄰近正常黏膜之組織代謝特
侯瑋恩1 林蔚然1,2,3
1 林口長庚紀念醫院胃腸肝膽科系
2 長庚大學醫學院
3 林口長庚紀念醫院肝臟研究中心
Background: Bioenergetic reprogramming is a hallmark of colorectal cancer (CRC), yet its prognostic implications remain unclear. Prior studies have shown decreased oxygen consumption rate (OCR) in CRC compared to adjacent normal mucosae, but the relevance to recurrence risk has not been fully investigated.
Aims: To characterize metabolic alterations in CRC tissues and adjacent mucosae, and evaluate whether OCR, extracellular acidification rate (ECAR), and their ratio (OCR/ECAR, or O/E) can serve as prognostic biomarkers for recurrence risk stratification.
Methods: Paired tumor and adjacent mucosal tissues from 106 CRC patients were collected at Chang Gung Memorial Hospital (2012–2017). Mitochondrial OCR and glycolytic ECAR were quantified using a Seahorse XF Analyzer. Mean follow-up was 64.9 months, and mean time to recurrence was 23.1 months.
Results: CRC tissues exhibited significantly lower OCR (2967.6 ± 119.6 vs. 3593.9 ± 151.4 mMol/ min/mg, P < 0.001) and O/E ratio (6.49 ± 0.24 vs. 8.84 ± 0.45 mMol/mpH, P < 0.001) than adjacent mucosae, indicating a glycolytic shift. High tumor ECAR (>740 mpH/min/mg) was associated with worse recurrence-free survival (RFS) (HR = 5.56, P = 0.002). Tumor O/E >8.45 also predicted poor RFS (HR = 3.69, P = 0.003). In adjacent mucosa, O/E >8.8 was similarly associated with poor RFS (HR = 2.48, P = 0.046), suggesting a metabolic field effect.
Conclusions: High ECAR and O/E ratios in CRC tissues are linked to poorer recurrence outcomes, reflecting aggressive metabolic traits. Elevated O/E in adjacent mucosa suggests a possible field effect. Tissue bioenergetics may serve as a prognostic marker in CRC.
Po-Jung Chen, Ming-Yao Su
Division of Gastroenterology and Hepatology, Department of Internal Medicine, New Taipei Municipal TuCheng Hospital, New Taipei City, Taiwan
人工智能與醫師比較:大腸息肉偵測率 分析比較
蘇銘堯 新北市立土城醫院胃腸肝膽科
Background: Colorectal polyps are precursors to colorectal cancer (CRC), and their early detection is critical for cancer prevention. Artificial intelligence (AI) has shown promise in assisting endoscopists in polyp detection, but its efficacy compared to experienced physicians remains under investigation.
Aims: This study compares the performance of AI with experienced physicians in detecting colorectal polyps and adenomas.
Methods: A prospective study was conducted using real-time endoscopic images from colonoscopy procedures. AI-assisted detection was compared with two groups of physicians: those with ≥10 years of experience and those with <5 years of experience. Detection rates, false-positive rates, false-negative rates, adenoma detection rates (ADR), and polyp size distribution were analyzed.
Results: The AI system detected 1080 polyps with a false-positive rate of 15% and a false-negative rate of 3%. Physicians with ≥10 years of experience detected 1069 polyps, while those with <5 years of experience detected 974 polyps. The ADR was 46% for AI, 46% for experienced physicians, and 40% for less experienced physicians. Analysis of polyp size distribution showed statistically significant differences in detection rates between the groups (p < 0.05).
Conclusions: AI-assisted detection shows promise as a supplementary tool for polyp and adenoma detection in colonoscopy. AI’s detection rate was comparable to experienced physicians, with a slightly higher false-positive rate. Future improvements in AI specificity and its integration into routine practice could enhance early polyp and adenoma detection, ultimately improving CRC prevention.
TO INVESTIGATE THE POSITIVE RATE OF FECAL IMMUNOCHEMICAL TESTS AND THE SUBSEQUENT COLONOSCOPY FINDINGS IN ADULTS UNDER 50
Chi-Chu Lo1, Cheng-Lu Lin1,2, Kuan-Chih Chen1,2
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan
2Health Management Center, Far Eastern Memorial Hospital, New Taipei City, Taiwan
探討 50 歲以下無症狀之年輕成人糞便免 疫化學檢測的陽性率及大腸鏡檢查結果 之探討
羅際竹1 林政錄1,2 陳冠至1,2
1 亞東紀念醫院肝膽胃腸科
2 亞東紀念醫院健康管理中心
Background: The incidence of colorectal cancer (CRC) in adults under 50 has been increasing, potentially due to genetic predispositions, dietary and lifestyle changes, and environmental factors. The fecal immunochemical test (FIT) has proven to be an effective screening tool for CRC in individuals over 50, with positivity rates in Taiwanese adults in this age group ranging from 5.7% to 6.7%. However, little is known about FIT positivity rates and the subsequent colonoscopy findings in asymptomatic younger adults under 50.
Aims: This study aimed to determine the prevalence of positive FIT results and the subsequent colonoscopy findings in asymptomatic adults under 50 years old.
Methods: We conducted a retrospective study at a tertiary hospital, analyzing FIT results and the subsequent colonoscopy findings from asymptomatic individuals under 50 years old between 2011 and 2025. Binary logistic regression was performed for analysis, with statistical significance set at P < 0.05.
Results: A total of 202676 asymptomatic patients from the Far Eastern Memorial Hospital Health Management Center underwent FIT during the study period. Of these, 9466 (4.7%) had positive FIT results, while 193210 had negative results. The relationship between FIT results and patient factors, such as age and gender, was analyzed. The overall
FIT positivity rate was higher in female (4.94% vs. 4.47%, P < 0.001). Notably, a higher FIT positivity rate in males compared to females was observed only in the 45–49 age group (5.17% vs. 4.62%, P = 0.005), and FIT positivity was significantly associated with age. Among 1,973 individuals with positive FIT who underwent subsequent colonoscopy, 141 (7.1%) were found to have advanced neoplasms, with 78.7% of these cases occurring in individuals aged 40 to 49 years. When comparing the 40–44 and 45–49 age groups, the latter exhibited a significantly higher prevalence of advanced neoplasms. Regarding time-period and the potential effects of birth cohort, there was an increasing trend in the detection of advanced neoplasms in the 45–49 age group.
Conclusions: The FIT positivity rate among asymptomatic adults under 50 was comparable to that of individuals aged 50 or older. In the current era, initiating colorectal cancer (CRC) screening at age 45 may be more reasonable. However, given the significant influence of birth cohort effects, it will be important to re-evaluate the future prevalence of advanced neoplasms in adults under 50, particularly in the 40–44 age group.
USING LARGE LANGUAGE MODELS
ANALYSIS OF COLONOSCOPY AND PATHOLOGY REPORTS FOR IMPROVING SURVEILLANCE COLONOSCOPY INTERVAL RECOMMENDATIONS
Hao-Yu Wu1, Wei-Yuan Chang2, Hsuan-Ho Lin3, Chen-Ya Kuo4, Wen-Feng Hsu2, Li-Chun Chang2, Ming-Shiang Wu2, Joyce Tzu-Yu Liu5, Han-Mo Chiu2
1Department of Internal Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
2Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
3Department of Internal Medicine, National Taiwan University Hospital, Hsin-Chu Branch Hsin-Chu Hospital, Hsinchu, Hsinchu, Taiwan
4Division of Gastroenterology and Hepatology, Department of Internal Medicine, Fu Jen Catholic University Hospital, New Taipei City, Taiwan
5Department of Electrical Engineering, National Taiwan University, Taipei, Taiwan
使用大型語言模型結構化分析大腸鏡檢 查和病理報告以優化追蹤大腸鏡檢查間 隔建議
吳浩宇1 張為淵2 林宣合3 郭震亞4 許文峰2 張立群2 吳明賢2 劉子毓5 邱瀚模2
1 台大醫院癌醫中心分院綜合內科部
2 台大醫院內科部
3 台大醫院新竹分院內科部
4 輔仁大學附設醫院胃腸肝膽科
5 國立臺灣大學電機系
Background: Extracting structured data from unstructured health records, such as endoscopic and pathology reports, is a significant challenge in medical research. Traditional Natural Language Processing (NLP) techniques are often resourceintensive and may lack generalizability across diverse clinical environments. Colonoscopy and pathology reports are vital for determining appropriate surveillance intervals for colorectal cancer, but manual interpretation often leads to errors, with adherence to international guidelines below 50%. Although Large Language Models (LLMs) have shown promise in this domain, prior studies have
frequently relied on synthetic datasets, limiting the applicability of their findings in real-world contexts. For example, one study reported an 87% consistency rate with a baseline LLM in a synthetic setting, while another achieved 79% accuracy using a Retrieval-Augmented Generation (RAG) approach; nonetheless, the dependence on synthetic data constrains their generalizability.
Aims: This study aimed to leverage LLMs for the structured extraction and analysis of unstructured colonoscopy and pathology reports to improve the determination of surveillance colonoscopy intervals. The goal was to overcome the data extraction limitations of traditional NLP methods and to enhance the accuracy and consistency of follow-up interval recommendations.
Methods: The research utilized a dataset of 205 patients’ medical records, which included unstructured endoscopy and pathology reports, with a physician-annotated ground truth for comparison. The process involved data cleaning, de-identification, and standardization to prepare the reports for analysis. Colonoscopy Reports: The extraction process consisted of three stages. First, regular expressions were employed for pre-processing to isolate relevant sections, such as Colonoscopic Findings and Endoscopic Diagnosis. Second, key procedural details, including bowel preparation quality and insertion depth, were extracted using regular expressions. Finally, Gemini-1.0-flash and Llama-3-8B-Instruct were deployed to transform the unstructured findings into structured data, using optimized prompts and few-shot learning examples.
Pathology Reports: Three LLMs—Gemini-1.0-flash, ChatGPT-4.0, and Llama-3-70B—were evaluated without task-specific fine-tuning. Detailed prompts defined the required structured fields and extraction rules. Reports containing multiple samples were divided and processed as separate structured units.
Evaluation: For the pathology reports, a random sample of 50 reports was used to assess extraction accuracy by comparing the LLMs’ structured outputs against the ground truth using string matching for each data field.
Results: Colonoscopy Reports: Regular expressions effectively extracted basic information, achieving 98% accuracy. LLMs performed strongly in structuring the main colonoscopic findings, with accuracy exceeding 94% for key fields such as diagnosis and lesion size. Pathology Reports: Llama3-70B generally achieved the highest accuracy
for most fields, particularly Specimen Source and Dysplasia Grade. ChatGPT-4.0 outperformed others for Site Label, Tumor Size, and Invasion Depth. Overall, Gemini’s accuracy was comparatively lower. Notably, Llama frequently produced clinically sound answers that extended beyond predefined response options, reflecting its robust reasoning capabilities but also a tendency to deviate from strict prompt adherence.
Conclusions: This study demonstrates the feasibility of using LLMs to automatically extract structured data from unstructured colonoscopy and pathology reports, offering a more accurate and efficient approach for generating surveillance interval recommendations. The findings show that LLMs can deliver high accuracy in information extraction without extensive domain-specific fine-tuning, providing a clear advantage over conventional NLP techniques. Models such as ChatGPT and Gemini achieved over 90% accuracy for most fields. The study also identified challenges, including the Llama model’s weaker compliance with prompt instructions. Overall, this work underscores the significant potential of LLMs to automate medical report analysis and support clinical decision-making.
PREDICTORS OF AGGRESSIVE RECURRENCE FOLLOWING CURATIVE RESECTION FOR HEPATOCELLULAR CARCINOMA
Kuo-Cheng Wu1,2, I-Cheng Lee1,3, Chi-Ping Tan1, Jiing-Chyuan Luo1,3, Ming-Chih Hou1,3, Yi-Hsiang Huang1,3,4,5
1Division of Gastroenterology and Hepatology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
2Division of Gastroenterology and Hepatology, Department of Medicine, Keelung Hospital, Ministry of Health and Welfare, Keelung, Taiwan
3School of Medicine, College of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
4Institute of Clinical Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
5Department of Medical Research, Taipei Veterans General Hospital, Taipei, Taiwan
肝細胞癌根治性切除後侵襲性復發的預 測因子
胡果正1,2 李懿宬1,3 談啟蘋1 羅景全1,3 侯明志1,3 黃怡翔1,3,4,5
1 臺北榮民總醫院胃腸肝膽科
2 衛生福利部基隆醫院胃腸肝膽科
3 國立陽明交通大學醫學系
4 國立陽明交通大學臨床醫學研究所
5 臺北榮民總醫院醫學研究部
Background: Recurrence patterns and outcomes following curative resection for hepatocellular carcinoma (HCC) are highly heterogeneous. In particular, the predictors of aggressive recurrence remain poorly defined.
Aims: This study aimed to identify the predictors of various aggressive recurrence patterns in patients with HCC after curative resection.
Methods: From 2007 to 2023, 893 of 1,813 patients who experienced recurrence after curative resection for HCC were retrospectively enrolled. Aggressive recurrence patterns analyzed included recurrence beyond the Milan criteria, recurrence with macrovascular invasion, extrahepatic metastasis, and recurrence at an advanced stage (BCLC stage C). Relevant clinicopathological factors were evaluated to identify independent predictors for
each recurrence pattern. Confluent multinodular or infiltrative type HCC were defined as high risk morphology.
Results: Among the 893 patients with recurrent HCC, 350 (39.2%) had recurrence beyond the Milan criteria, 60 (6.7%) had macrovascular invasion, 144 (16.1%) developed extrahepatic metastases, and 191 (21.4%) presented with BCLC stage C disease. Microvascular invasion (odds ratio (OR) = 2.830, p = 0.002), early recurrence (OR = 3.391, p < 0.001), and high risk morphology (OR = 2.942, p < 0.001) were independent predictors of recurrence beyond the Milan criteria. Poor differentiation (OR = 14.941, p < 0.001) and high risk morphology (OR = 2.915, p = 0.025) were associated with macrovascular invasion. Early recurrence (OR = 3.093, p = 0.009), AFP level >400 ng/mL (OR = 3.482, p < 0.001), ALBI grade 2-3 (OR = 0.404, p = 0.014), and high risk morphology (OR = 2.991, p = 0.002) were independent predictors of extrahepatic metastasis. Elevated AFP level >400 ng/mL (OR = 2.917, p = 0.002), poor differentiation (OR = 1.888, p = 0.044), high risk morphology (OR = 2.984, p = 0.001), and early recurrence (OR = 2.746, p = 0.007) predicted recurrence at BCLC stage C.
Conclusions: Aggressive recurrence patterns following curative resection for HCC are significantly associated with distinct tumor characteristics. These findings may inform post-recurrence treatment strategies, particularly in the context of adjuvant immunotherapy or upfront liver transplantation, and support the design of future clinical trials.
THE ETIOLOGY OF HEPATOCELLULAR CARCINOMA DOES NOT AFFECT OUTCOMES IN HCC PATIENTS RECEIVING ATEZOLIZUMAB
Wei-Fan Hsu1,2, Hsueh-Chou Lai1,2, Hung-Wei Wang1,3, Cheng-Kuo Chen4, Shih-Chao Hsu5, Long-Bin Jeng5, Cheng-Yuan Peng1,3
1Center for Digestive Medicine, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan
2School of Chinese Medicine, China Medical University, Taichung, Taiwan
3School of Medicine, China Medical University, Taichung, Taiwan
4Division of Gastroenterology & Hepatology, Department of Internal Medicine, Asia University Hospital, Taichung, Taiwan
5Department of Surgery, China Medical University Hospital, Taichung, Taiwan
肝細胞癌的病因不會影響接受 Atezolizumab 合併 Bevacizumab 治療的 患者預後
許偉帆1,2 賴學洲1,2 王鴻偉1,3 陳政國4 許士超5 鄭隆賓5 彭成元1,3
1 中國醫藥大學附設醫院消化醫學中心
2 中國醫藥大學中醫學系
3 中國醫藥大學醫學系
4 亞洲大學附屬醫院胃腸肝膽科
5 中國醫藥大學附設醫院外科部
Background: Hepatocellular carcinoma (HCC) is a leading cause of cancer-related death and a common malignancy worldwide. Atezolizumab plus bevacizumab (Atezo-Bev) is the first-line systemic therapy against unresectable HCC (uHCC). Besides viral hepatitis, metabolic dysfunction–associated steatotic liver disease (MASLD) is also a growing etiology of HCC. Recent studies revealed that fatty liver-related HCC had a poor response to immunotherapy-based systemic therapy.
Aims: We investigated the impact of different etiologies of HCC on the outcomes in patients with uHCC receiving Atezo-Bev therapy.
Methods: From July 2020 to February 2025, 164 consecutive patients with uHCC received at least one
dose of Atezo-Bev. MASLD was diagnosed based on the presence of fatty liver, as detected by abdominal ultrasonography or computed tomography (CT), and at least one of the following cardiometabolic risk factors: body mass index (BMI)≥23 kg/m², prediabetes or diabetes mellitus, blood pressure ≥130/85 mmHg, or dyslipidemia. Hepatitis B viral (HBV) infection was defined as the presence of serum hepatitis B surface antigen for more than 6 months. Hepatitis C viral (HCV) infection was defined as the presence of detectable HCV RNA. Alcohol consumption was defined as men and women who drank >30 and 20 g/day of alcohol, respectively. Exclusion criteria included no available information on fatty liver, no evaluable follow-up CT, and an overall survival (OS) of less than 3 months. Finally, 140 patients were enrolled in the analysis. Factors associated with progressionfree survival (PFS) and OS at the initiation of AtezoBev were collected. An AFP response was defined as a decline of more than 15% in AFP level within the initial 3 months of Atezo-Bev therapy.
Results: Of the enrolled 140 patients, 111 (79.3%) were male, and the median age was 66.4 (57.2–73.4) years (first–third quartile). In total, 27 (19.3%), 71 (50.7%), 22 (15.7%), and 64 (45.7%) patients drank alcohol, had HBV infection, had HCV infection, and had MASLD, respectively. Patients may have more than one etiology of HCC. There were 3 (2.1%), 21 (15%), and 116 (82.9%) patients belonging to BCLC stages A, B, and C, respectively. The median ALBI score, AFP, and total tumor volume were -2.44 (-2.77 to -2.17), 81.76 (7.25–3845.5) ng/mL, 1641.3 (215.1–7191.8) cm^3. In total, 8 (5.7%), 26 (18.6%), 49 (35.0%), and 55 (39.3%) patients had a complete response (CR), partial response (PR), stable disease, and progressive disease, respectively. The duration of PFS and OS was 5.23 (4.03–6.43) and 23.10 (18.74–27.47) months, respectively. A multivariable Cox regression analysis identified AFP response (hazard ratio [HR]: 0.568, 95% confidence interval [CI]: 0.364–0.886) and objective response (OR = CR + PR, HR: 0.134, 95% CI: 0.063–0.285) as independent predictors of PFS. A multivariable Cox regression analysis identified AFP response (HR: 0.533, 95% CI: 0.288–0.988) and OR (HR: 0.086, 95% CI: 0.020–0.363) as the independent predictors of OS. Alcohol consumption, viral hepatitis (HBV or HCV infection), or MASLD were not predictors of PFS or OS.
Conclusions: The etiology of HCC, including alcohol, viral hepatitis, and MASLD, did not affect PFS or OS in patients receiving Atezo-Bev therapy.
A NEW MODEL BASED ON PREOPERATIVE AFP, PIVKAII, AND TUMOR BURDEN SCORE FOR PREDICTING MICROVASCULAR INVASION IN HCC
Hsin-Yi Tseng1, Chih-Chi Wang2, Yueh-Wei Liu2, Wei-Feng Li2, Ming-Chao Tsai1,3
1School of Medicine, College of Medicine, National Sun Yat-sen University, Kaohsiung, Taiwan
2Division of General Surgery, Department of Surgery, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine Kaohsiung, Taiwan
3Division of Hepato-Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan
使用 AFP、PIVKA-II 與腫瘤負荷分數建立 一個術前的模型預測肝癌的微血管侵犯
曾心怡1 王植熙2 劉約維2 李韋鋒2 蔡明釗1,3
1 國立中山大學學士後醫學系
2 高雄長庚紀念醫院一般外科
3 高雄長庚紀念醫院胃腸肝膽科系
Background: Microscopic vascular invasion (MVI) is a key determinant of recurrence and prognosis in hepatocellular carcinoma (HCC), but non invasive preoperative prediction remains inadequate.
Aims: We aimed to build a novel model to predict MVI in the preoperative setting.
Methods: We conducted a retrospective analysis of 233 patients with BCLC stages 0–C HCC who underwent resection at Kaohsiung Chang Gung Memorial Hospital from January 2020 to July 2023 (training cohort), and validated findings in 93 patients resected between July 2007 and May 2023 (validation cohort). Baseline variables (AFP, PIVKA II, tumor burden score [TBS]) and pathological MVI status were recorded. Multivariate logistic regression identified independent predictors, and model performance was assessed by AUC and calibration error.
Results: In multivariable analysis, AFP ≥20 ng/mL (OR 2.11, 95% CI 1.22–3.65; P = 0.008), PIVKA-II ≥35 ng/mL (OR 3.45, 95% CI 2.02–5.89; P < 0.001) and
TBS ≥6.4 (OR 2.47, 95% CI 1.22–4.99; P = 0.012) were independent predictors of MVI. A nomogram based on the aggregated risk score yielded an AUC of 0.744 (95% CI 0.678–0.805), mean calibration error 0.022 and Hosmer–Lemeshow P = 0.808 in the training cohort, and demonstrated robust discrimination on external validation with an AUC of 0.758 (95% CI 0.668–0.844) and Hosmer–Lemeshow P = 0.719.
Conclusions: This cost-effective and non-invasive model offers accurate preoperative prediction of MVI in patients with HCC, facilitating personalized treatment strategies. To promote clinical utility, a web-based calculator was also implemented.
Makoto Nagashima
Department of Gastroenterology and Hepatology, Tokyo Medical University, Tokyo, Japan
Background: Hepatocellular carcinoma (HCC) is one of the leading causes of mortality among patients with liver disease, and early detection and accurate diagnosis are essential for improving patient prognosis. Currently, imaging plays a central role in the noninvasive diagnosis of HCC, and the Liver Imaging Reporting and Data System (LI-RADS) is widely used as an imaging diagnostic algorithm for hepatic tumors in high-risk patients. Traditionally, LI-RADS using computed tomography (CT) and magnetic resonance imaging (MRI) (CT/MRI LIRADS) has been considered the standard diagnostic method. In recent years, however, contrast-enhanced ultrasound (CEUS) LI-RADS has also been proposed and has attracted attention due to its advantages such as real-time imaging and the safety profile of contrast agents. In particular, the second-generation contrast agent Sonazoid is distinguished from other agents by its ability to evaluate the Kupffer phase, allowing for more detailed differentiation of tumorous lesions. However, CEUS LI-RADS has different imaging features and diagnostic criteria compared to CT/MRI LI-RADS, and the diagnostic performance and concordance between the two modalities have not been fully investigated. Evidence is especially limited regarding the diagnostic accuracy of a modified CEUS LI-RADS that incorporates Kupffer-phase findings as a major feature using Sonazoid, as well as its ability to distinguish non-HCC malignancies. The aim of this study was to compare the diagnostic performance and inter-modality agreement between the modified CEUS LI-RADS using Sonazoid and CT/MRI LI-RADS for liver nodules in high-risk patients for HCC, and to clarify the utility and limitations of each modality. Aims: To compare the diagnostic performance based on the modified CEUS Liver Imaging Reporting and Data System (LI-RADS), which includes Kupfferphase findings as a major imaging feature, with that of CT and MRI (CT/MRI) LI-RADS for liver nodules in patients at high risk of HCC.
Methods: To compare the diagnostic performance based on the modified CEUS Liver Imaging Reporting and Data System (LI-RADS), which includes Kupfferphase findings as a major imaging feature, with that of CT and MRI (CT/MRI) LI-RADS for liver nodules in patients at high risk of HCC.
Results: The inter-modality agreement for the modified CEUS LI-RADS and CT/MRI LI-RADS was slight agreement (kappa = 0.139, p = 0.015). The diagnostic accuracies of HCCs for the modified CEUS LR-5 and CT/MRI LR-5 were 70.0% (95% confidence interval [CI]: 61.0%, 78.0%) versus 70.8% (95% CI: 61.8%, 78.8%) (p = 0.876), respectively. The diagnostic accuracies of non-HCC malignancies for the modified CEUS LR-M and CT/MRI LR-M were 84.2% (95% CI: 76.4%, 90.2%) versus 96.7% (95% CI: 91.7%, 99.1%) (p = 0.002), respectively.
Conclusions: The diagnostic performance for HCCs on the modified CEUS LR-5 and CT/MRI LR-5 are comparable. In contrast, CT/MRI LR-M has better diagnostic performance for non-HCC malignancy than that of the modified CEUS LR-M.
PROGNOSTIC PREDICTORS ASSOCIATED WITH HEPATOCELLULAR CARCINOMA AFTER SURGICAL RESECTION
Hung-En Chen1, Bou-Zenn Lin1, Chih-Lin Lin1, Ting-An Chang2, Chin-Tsung Ting3, Tsung-Jung Lin1
1Department of Gastroenterology, Renai Branch, Taipei City Hospital, Taipei, Taiwan
2Department of Pathology, Renai Branch, Taipei City Hospital, Taipei, Taiwan
3Department of Gastrointestinal Surgery, Renai Branch, Taipei City Hospital, Taipei, Taiwan
影響肝細胞癌手術切除後預後之預測因 子探討
陳弘恩1 林柏任1 林志陵1 張廷安2 丁金聰3 林聰蓉1
1 臺北市立聯合醫院仁愛院區消化內科
2 臺北市立聯合醫院仁愛院區病理科
3 臺北市立聯合醫院仁愛院區消化外科
Background: Although surgical resection remains one of the most effective treatments for HCC, longterm survival varies significantly among patients. Therefore, identifying factors associated with survival is crucial for risk stratification and optimizing postoperative management strategies.
Aims: This study aimed to analyze independent prognostic factors in HCC patients who underwent surgical resection.
Methods: Total 233 patients who underwent surgical resection for HCC were recruited consecutively from the database of Cancer Registries between January 2011 and December 2021 in Taipei City Hospital, Renai Branch. Patients were followed for survival status until December 2022. Total fifteen variables including age, gender, body mass index, alcohol consumption history, tumor size, serum creatinine, total bilirubin, international normalized ratio (INR), Child-Pugh classification, alpha-fetoprotein (AFP) levels, Barcelona Clinic Liver Cancer (BCLC) stage, liver fibrosis, pathological differentiation, lymphovascular invasion and surgical margin status, were selected from Cancer Registries database. The hazard ratios of the factors in the survival outcome were assessed by univariate and multivariate Cox proportional hazard regression analysis.
Results: In univariate Cox regression analysis, the following eight variables were significantly
associated with survival, including age, tumor size, serum creatinine, total bilirubin, ChildPugh classification, AFP levels, BCLC stage and lymphovascular invasion. In multivariate Cox regression analysis, five factors were significantly independent predictors of survival. Age (hazard ratio [HR]: 1.036; 95% confidence interval [CI], 1.011 – 1.061; p = 0.004), serum creatinine (HR: 1.193; 95% CI, 1.007 – 1.413; p = 0.041), total bilirubin levels (HR: 1.937; 95% CI, 1.211 – 3.100; p = 0.006), BCLC stage (HR: 1.971; 95% CI, 1.232 – 3.154; p = 0.005), and lymphovascular invasion (HR: 2.046; 95% CI, 1.189 –3.519; p = 0.010) were significantly associated with poorer survival.
Conclusions: Age, serum creatinine, total bilirubin levels, BCLC stage and lymphovascular invasion were the significant prognostic predictors in HCC patients after surgical resection. These findings may assist clinicians in postoperative risk stratifications to guide individualized surveillance and adjuvant therapies.
HIGH GALAD SCORES PREDICT HEPATOCELLULAR CARCINOMA IN HEPATITIS B-RELATED CIRRHOSIS PATIENTS WHO RECEIVED ANTIVIRAL THERAPY
Hsi-An Chen1, Tung-Hung Su1,2, Chun-Jen Liu1,2, Hung-Chih Yang1,2, Tai-Chung Tseng1,2,3, Shang-Chin Huang1,2,4,5, Shih-Jer Hsu1,2, Chun-Ming Hong1, Chen-Hua Liu1,2, Pei-Jer Chen1,2, Jia-Horng Kao1,2,3,5
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
3Department of Medical Research, National Taiwan University Hospital, Taipei, Taiwan
4Department of Internal Medicine, National Taiwan University Hospital Bei-Hu Branch, Taipei, Taiwan
5Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
GALAD Score 在慢性 B 型肝炎肝硬化病 人中可預測肝癌發生
陳錫安1 蘇東弘1,2 劉俊人1,2 楊宏志1,2 曾岱宗1,2,3
黃上秦1,2,4,5 徐士哲1,2 洪俊銘1 劉振驊1,2 陳培哲1,2
高家宏1,2,3,5
1 台大醫院胃腸肝膽科
2 台大醫院肝炎研究中心
3 台大醫院醫學研究部
4 台大醫院北護分院內科部
5 台大醫學院臨床醫學研究所
Background: In hepatitis B-related cirrhosis patients on long-term antiviral therapy, hepatocellular carcinoma (HCC) risk persists, motivating the need for risk prediction. The GALAD score, encompassing gender, age, alpha-fetoprotein L3, alpha-fetoprotein, and des-gamma carboxyprothrombin (DCP) measurements, is designed for HCC detection. This study investigates the role of the GALAD score in HCC prediction in CHB-related cirrhosis patients on antiviral therapy.
Aims: Assessment of GALAD score in chronic hepatitis B related cirrhotic patients.
Methods: We conducted a retrospective cohort
study to include HBV-related cirrhotic patients undergoing long-term antiviral therapy with regular HCC surveillance. The serum samples were retrieved for alpha-fetoprotein-L3, alpha-fetoprotein, and DCP measurements to calculate the GALAD score. Cox proportional hazard regression analysis identified risk predictors for HCC.
Results: A total of 252 patients were included, with a median follow-up of 6.1 years. HCC developed in 64 patients with an annual incidence of 4%. The GALAD scores were measured before therapy in 213 patients and after a median of 2.6 years of antiviral therapy in 39 patients, with a median GALAD score of -2.84 and -3.76, respectively (p=0.012). Overall, the pretreatment GALAD score classifies the risks of 1-year HCC significantly better than alpha-fetoprotein-L3, alpha-fetoprotein, and DCP, with an AUROC of 0.857. Higher GALAD scores significantly increased the risk of HCC before antiviral therapy (per 1 GALAD score increase, adjusted hazard ratio [aHR] 1.20, 95% confidence interval [CI]: 1.06-1.35), and during antiviral therapy (aHR: 1.72, 95% CI: 1.10-2.70). The pretreatment GALAD score ≥ -1.35 (vs. <-1.35) or ontreatment GALAD score ≥ -3.38 (vs. <-3.38) increased 1.83-folds and 3.85-folds risks of HCC, respectively. Conclusions: High pre-treatment or on-treatment GALAD scores significantly stratified a greater risk of HCC. The GALAD score may be measured during routine HCC surveillance.
DEEP LEARNING-ENHANCED PREDICTION OF SMALL INTESTINAL BLEEDING POINTS USING LONG SHORT-TERM MEMORY NETWORKS
Tsung-Jung Tsai, Po-Chun Yang, Li-Jen Chang, Chang-Chao Su, Chu-Kuang Chou, Chi-Yi Chen, Po-Yueh Chen
Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
使用長短期記憶網路之深度學習技術提 升小腸出血點之預測能力
楊博鈞 張力仁 蘇昶昭 周莒光 陳啟益
戴德森醫療財團法人嘉義基督教醫院內科部
Background: Capsule endoscopy is an essential diagnostic instrument for identifying gastrointestinal (GI) hemorrhaging, linked to numerous GI disorders, such as ulcers, polyps, tumors, and Crohn’s disease. Gastrointestinal bleeding can be classified as active or non-active, happening along the gastrointestinal tract. Capsule endoscopy facilitates thorough viewing of the gastrointestinal tract, enabling early identification and localization of hemorrhagic sources, thereby offering significant therapeutic insights for diagnosis and treatment.
Aims: This study aimed to use a successful development of a deep learning methodology for the detection of gastrointestinal bleeding via wireless capsule endoscopy images.
Methods: This study employed two datasets for automated bleeding detection: one from National Cheng Kung University, consisting of White Light Imaging (WLI) images from 100 patients obtained via PillCam™ SB 3 capsule endoscopy, and the KvasirCapsule Image dataset, which includes 47,238 labeled images across 14 pathological categories. Nineteen continuous picture sequences were recovered, comprising 3,806 bleeding photos and 3,275 non-bleeding images. Data augmentation was implemented, utilizing Convolutional Neural Networks (CNNs) for feature extraction, succeeded by Long Short-Term Memory (LSTM) networks for prediction.
Results: The CNN model attained an accuracy of 98.6% for 10 categories and 96.7% for 2 categories. The total accuracy of LSTM training and testing for the 10-category dataset is 96.2% and 87.1%,
respectively.
Conclusions: This study’s findings showed the efficacy of combining CNN and LSTM models for predicting images of minor intestinal hemorrhage. The capacity of CNN to extract spatial information, coupled with LSTM’s proficiency in capturing temporal relationships, indicates a viable methodology for medical image analysis.
Jian-Liang Chen1, Chen-Shuan Chung1,2,3, Chung-Hsin Chang4, Chia-Jung Kuo3,5,6, Jen-Wei Chou3,7, Tien-Yu Huang3,8, Wen-Hung Hsu3,9, Chen-Wang Chang3,10, Puo-Hsien Le3,5,6
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan
2College of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan
3Taiwan Association for the Study of Intestinal Diseases (TASID)
4Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
5Department of Gastroenterology and Hepatology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
6Inflammatory Bowel Disease Center, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
7Division of Gastroenterology and Hepatology, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan
8Division of Gastroenterology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
9Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
10Division of Gastroenterology and Hepatology, Department of Internal Medicine, Mackay Memorial Hospital, Taipei, Taiwan
Risankizumab
2 輔仁大學醫學系
3 台灣腸道醫學會
4 臺中榮民總醫院胃腸肝膽科
5 林口長庚紀念醫院胃腸肝膽科系
6 林口長庚紀念醫院發炎性腸道疾病中心
7 中國醫藥大學附設醫院消化系內科
8 三軍總醫院胃腸肝膽科
9 高雄醫學大學附設醫院胃腸內科
10 馬偕紀念醫院消化科系
Background: Crohn’s disease (CD) remains a challenging condition, especially in patients with moderate-to-severe disease. Risankizumab, an antiIL-23p19 monoclonal antibody, has shown efficacy in clinical trials. However, real-world data (RWD) in Asian populations are limited.
Aims: This study aims to evaluate the clinical response, improvement, and remission rates of Risankizumab in East Asian patients with moderate to severe Crohn’s disease in Taiwan, along with the assessment of treatment-related adverse events.
Methods: This multicenter cohort study enrolled adult patients with moderate-to-severe CD who received Risankizumab between September 2024 and May 2025 in Taiwan. Efficacy was assessed at weeks 4, 8, and 12 using CD Activity Index (CDAI), Patientreported outcomes-2 (PRO2), and Inflammatory Bowel Disease (IBD)-Disk scores. Safety outcomes and treatment response by prior biologic exposure, including ustekinumab, were evaluated.
Results: Forty-nine patients (mean age 41.5 years, 69.4% male) were included. Clinical response rates were 53.1%, 75.5%, and 91.8% at weeks 4, 8, and 12, respectively; clinical remission was achieved in 12.2%, 22.4%, and 42.9%. PRO2 remission reached 53.5% by week 12. Both CDAI and IBD-Disc score improved at weeks 4, 8 and 12 with statistical significance (P < 0.0001). Transmural healing was observed in 16.3% of patients at weeks 12. Clinical remission at weeks 12 was consistent regardless of prior Ustekinumab exposure (exposed 36.36% vs. naïve 44.74%, P = 0.630) or biologic-naïve status (exposed 36.84% vs. naïve 63.63%, P = 0.119). No severe adverse events were reported but mild events included headache and transient liver enzyme elevation (each 2.04%).
Conclusions: Risankizumab demonstrated significant short-term efficacy and favorable safety in real-world treatment of moderate-to-severe CD in an Asian cohort. Outcomes were consistent with clinical trials, supporting Risankizumab as an effective treatment option across diverse CD populations.
BOWEL URGENCY IN ULCERATIVE COLITIS IS INDEPENDENTLY ASSOCIATED WITH HISTOLOGIC INFLAMMATION AND STOOL FORM DESPITE ENDOSCOPIC REMISSION
Zih-Hao Wei1,2, Cheng-Tang Chiu3,4,5,6,7, Puo-Hsien Le3,4,5,6,7
1School of Medicine, Chang Gung University, Taoyuan, Taiwan
2Department of Medical Education, Taichung Veterans General Hospital, Taichung, Taiwan
3Taiwan Association for the Study of Intestinal Diseases (TASID), Taoyuan, Taiwan
4Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
5Chang Gung Microbiota Therapy Center, Linkou, Taoyuan, Taiwan
6Chang Gung Inflammatory Bowel Disease Center, Linkou, Taoyuan, Taiwan
7College of Medicine, Chang Gung University, Taoyuan, Taiwan
潰瘍性結腸炎患者的排便急迫感,即使 在內視鏡緩解情況下,仍與組織學發炎 與糞便形態獨立相關
魏子豪1,2 邱正堂3,4,5,6,7 李柏賢3,4,5,6,7
1 長庚大學醫學系
2 臺中榮民總醫院教學部
3 台灣腸道醫學會
4 林口長庚紀念醫院胃腸肝膽科
5 林口長庚紀念醫院微菌治療中心
6 林口長庚紀念醫院發炎性腸道疾病中心
7 長庚大學醫學院
Background: Bowel urgency (BU) is a troublesome symptom in ulcerative colitis (UC) patients, yet its associations with disease activity and patientreported outcomes remain unclear.
Aims: This study aims to provide the first comprehensive evaluation of the relationships between clinical, endoscopic, histological activity, stool consistency, and patient-reported disability. Methods: We prospectively enrolled 100 UC patients (Sep 2024–Mar 2025), classifying into two groups based on the Urgency Numeric Rating Scale (NRS): BU-active (BU-A; NRS > 1) and BU-remission (BU-R; NRS ≤ 1). Clinical parameters including the partial
Mayo score, Mayo endoscopic subscore (MES), Nancy Index (NI), Bristol Stool Form Scale (BSFS), and IBD Disk score were evaluated. Logistic regression analyses were performed to identify independent predictors of active BU.
Results: 50 patients were in BU-A, and 50 in BU-R. Endoscopic remission (MES=0) occurred in 14% of BU-A and 34% of BU-R; Histological remission (NI = 0) in 10% and 36%, respectively. Stool consistency was predominantly normal (Bristol types 3–5) in both groups (60% of BU-A, 72% of BU-R); however, type 6–7 stools were more frequent in the BU-A group (32% vs. 6%). BU-A group had significantly higher partial Mayo scores, MES, NI, and total IBD Disk scores (25.3 ± 20.0 vs. 12.0 ± 14.9, P < 0.001).
In multivariate analysis, higher NI (OR: 1.874; 95% CI: 1.277–2.750; P < 0.001) and BSFS score (OR: 1.499; 95% CI: 1.052–2.137; P = 0.025) were independently associated with active BU.
Conclusions: BU may persist despite endoscopic or histological remission and normal stool form, warranting targeted evaluation beyond traditional marker of disease activity.
THE CORRELATION BETWEEN HELICOBACTER PYLORI INFECTION AND IRON DEFICIENCY ANEMIA IN ADULTS WITH INFLAMMATORY BOWEL DISEASE: A RETROSPECTIVE STUDY IN A MEDICAL CENTER IN TAIWAN
Yi-Hua Wu1,2, Jen-Wei Chou1,2, Jye-Lin Hsu2, Cheng-Yuan Peng1,2
1Center for Digestive Disease, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan
2School of Medicine, China Medical University, Taichung, Taiwan
幽門螺旋桿菌感染症與缺鐵性貧血在發 炎性腸道疾病患者的相關性:台灣一間 醫學中心的回顧性研究
吳宜樺1,2 周仁偉1,2 徐婕琳2 彭成元1,2
1 中國醫藥大學附設醫院消化內科
2 中國醫藥大學醫學系
Background: Iron deficiency anemia (IDA) effects around 45% of individuals with inflammatory bowel disease (IBD), encompassing ulcerative colitis (UC) and Crohn’s disease (CD). The pathophysiology of IDA in people with IBD is multifaceted, including intestinal hemorrhage, malabsorption, and insufficient oral intake. In adult populations, Helicobacter pylori (H. pylori) infection (HPI) induced atrophic gastritis is associated with decreased iron absorption owing to reduced stomach acid output, ultimately leading to IDA. Although increasing research in the Europe and United States indicates that people with HPI exhibit a reduced prevalence of IBD, H. pylori may have a protective effect against the onset of IBD; however, no related studies have been conducted in Taiwan so far.
Aims: The objective of this research was to assess the correlation between H. pylori infection and the reduction of iron reserves in individuals with inflammatory bowel disease.
Methods: A population-based research was performed using a random sample of one million beneficiaries from the National Health Insurance program. Individuals diagnosed with inflammatory bowel illness, iron deficiency anemia, and HPI were found from the National Health Insurance Research
Database. The yearly prevalence and incidence of IBD, IDA, and HPI in adults were assessed using International Classification of Diseases, Ninth Revision, Clinical Modification diagnostic codes to identify pertinent cases from 2011 to 2021. Results: This research comprised 5044 IBD patients, including 3724 with UC and 1253 with CD. Male patients constituted the majority of the patient population (62.7%). The mean age at diagnosis was 46.26 ± 16.57 years (CD: 40.26 ± 17.60 years, UC: 48.36 ± 15.68 years). IDA included 14.02% of all IBD patients (14.82% with CD and 13.74% with UC). Trends in HPI prevalence among patients with IDA and IBD in Taiwan, 2011 to 2021 (Figure 1). A predominant proportion of these patients were female (68.13%). HPI represented 9.79% of all IBD patients, including 10.94% with CD and 9.41% with UC. The incidence of HPI in IBD associated with IDA was 2.79% (3.01% in CD and 2.74% in UC). The predominant number of these patients suffer from CD. The mean hemoglobin levels in the H. pylori-positive cohort were significantly lower than those in the H. pylori-negative cohort. Research on logistic regression demonstrated a correlation between female sex and HPI with iron deficiency. The prevalence of H. pylori is now 30% among adults over the age of 20 in Taiwan. The prevalence among children and adolescents is 10%. However, the trend in HPI prevalence increased (Figure 2), but HPI incidence decreased among patients with IBD from 2011 to 2021 in Taiwan (Figure 3).
Conclusions: 1. HP infection may constitute a potential risk factor linked to IDA in IBD. 2. There is a potential risk of reverse causation between H. pylori status and IBD, which could be the consequence of high-dose steroid use or biologic treatment in IBD; however, the association is inadequately comprehended, necessitating more investigation. 3. Regular screening and diagnosis in these people are essential, as they often exhibit a combination of IDA and HP infection, which may be beneficial for individuals with IBD.
Wan-Tai Wu, Jia-Feng Wu
Department of Pediatrics, National Taiwan University Children’s Hospital, Taipei, Taiwan
利用營養狀況預測兒童發炎性腸道疾病 之病程與治療
吳嘉峯
國立臺灣大學醫學院附設醫院兒童醫院小兒腸胃科
Background: Pediatric inflammatory bowel disease (PIBD) is becoming increasingly prevalent in the AsiaPacific region, including Taiwan. Previous studies have highlighted the close association between inflammatory bowel disease (IBD) and nutrition, with recent evidence suggesting that nutritional factors play a significant role in the disease’s etiopathogenesis. Vitamin D levels have been linked to both nutritional status and inflammatory activity, indicating their potential as biomarkers. Other studies have suggested associations with iron parameters, serum folate, and vitamin B12 levels. However, data on the nutritional profiles of pediatric IBD patients in Taiwan remain limited.
Aims: We aimed to use the nutritional status to predict the outcomes and treatment responses of pediatric patients with IBD in Taiwan.
Methods: We conducted a retrospective review of pediatric IBD patients (≤18 years at diagnosis) treated at a single medical center in Taiwan from June 2005 to November 2022. A total of 53 patients were included (32 with Crohn’s disease [CD], 21 with ulcerative colitis [UC]). Nutritional parameters—iron profile, serum folic acid, vitamin B12, and vitamin D—were assessed at early disease stages and after treatment. Disease activity and subsequent use of advanced therapies, including biologic agents, were evaluated.
Results: Among the CD group, no patients exhibited vitamin B12 deficiency and only 9.4% had folate deficiency at the early stage of disease. However, vitamin D and iron deficiencies were present in 62.1% and 58.6%, respectively. After treatment, rates of vitamin D and iron deficiencies declined to 14.3% and 33.3%. Notably, 72.2% of patients with initial
vitamin D deficiency and 82.4% with iron deficiency later required biologic therapy. In the UC group, vitamin B12 and folate deficiencies were absent, while vitamin D and iron deficiencies affected 52.9% and 56.3% of patients, respectively. These rates decreased to 22% each after treatment. Unlike in CD, no significant association was observed between micronutrient deficiencies and subsequent biologic use in UC.
Conclusions: Vitamin B12 and folic acid deficiencies were uncommon in pediatric CD and UC patients while vitamin D and iron deficiencies affected more than half patients at the early stage of the disease. This highlights the importance of adequate supplement and regular monitor of vitamin D and iron profile in pediatric IBD management. Furthermore, deficiencies in vitamin D or iron at the early stage of the disease in pediatric CD patients were associated with a higher possibility of requiring biologic therapy in the future, suggesting their potential role as predictors of treatment escalation.
Risako Osaka, Hironori Tanei, Tadashi Ichimiya, Kumiko Uchida, Masakatsu Fukuzawa, Takao Itoi
Department of Gastroenterology and Hepatology, Tokyo Medical University Hospital, Tokyo, Japan
Background: Mirikizumab, an anti-IL-23p19 monoclonal antibody, represents a novel therapeutic option for patients with moderate-to-severe ulcerative colitis (UC).
Aims: This study aimed to evaluate the clinical outcomes of mirikizumab treatment in UC patients at our institution.
Methods: We retrospectively analyzed 11 UC patients who initiated mirikizumab therapy between June 2023 and November 2024. Clinical disease activity was assessed using the Partial Mayo Score (PMS). Clinical response was defined as a decrease in PMS of ≥2 points, and clinical remission was defined as a PMS ≤1 with a rectal bleeding subscore of 0.
Results: The study included 11 patients (6 males, 5 females; mean age 49.2 ± 9.9 years). Disease extent was pancolitis in 6 patients (55%), left-sided colitis in 3 (27%), and proctitis in 2 (18%). The mean baseline PMS was 5.45 ± 1.23. Prior treatments included prednisolone (n = 2), advanced therapies (n = 8; JAK inhibitors [n = 2], anti-TNFα antibodies [n = 7], anti-IL12/23p40 antibodies [n = 5], anti-α4β7 antibody [n = 1]; with overlap), and budesonide foam (n = 1). At week 8, 5 patients (45%) achieved clinical response and 4 patients (36%) achieved clinical remission; 2 patients (18%) showed no response or worsening. Among the 9 patients who responded to treatment, 7 (78%) had previously experienced secondary loss of response to biologics, while 2 (22%) were biologic-naïve. The 2 patients with no response included 1 biologic-naïve case and 1 primary non-responder to prior biologics. At week 24, all 7 patients who continued mirikizumab maintained clinical remission, and no adverse events were reported.
Conclusions: These findings suggest that mirikizumab is a potentially effective induction therapy, with week 8 response and remission rates of 45% and 36%, respectively. In addition, all patients who achieved remission were able to maintain it through week 24, indicating the potential of mirikizumab as an effective induction and maintenance therapy in UC.
GASTROINTESTINAL SYNDROME AND MICROBIOTA ALTERATIONS WITH MUCOSAL BARRIER ASSESSMENT IN POSTACUTE
COVID-19: A SINGLECENTER RETROSPECTIVE STUDY IN TAIWAN
Yu-Fu Chen1,2, Yu-Jen Chen1,2,3, Tsung-Chieh Yang1,2,3, Hui-Chun Huang1,2,3, Jiing-Chyuan Luo1,3, Ming-Chih Hou1,2,3
1Division of Gastroenterology and Hepatology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
2Therapeutic and Research Center of Liver Cirrhosis and Portal Hypertension, Taipei Veterans General Hospital, Taipei, Taiwan
3School of Medicine, College of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
COVID-19 後急性期症候群患者之腸胃症 候群、腸道菌相變化與黏膜屏障評估: 臺灣單一中心回溯性研究
陳昱甫1,2 陳宥任1,2,3 楊宗杰1,2,3 黃惠君1,2,3 羅景全1,3 侯明志1,2,3
1 臺北榮民總醫院胃腸肝膽科
2 臺北榮民總醫院肝硬化與門脈高壓治療暨研究中心
3 國立陽明交通大學醫學系
Background: This retrospective study investigated the prevalence and characteristics of gastrointestinal (GI) symptoms in post-acute COVID-19 syndrome (PACS) patients. It also assessed microbiota alterations and mucosal barrier function using confocal laser endomicroscopy (CLE) to elucidate underlying mechanisms.
Aims: This retrospective study aims to investigate the prevalence and characteristics of GI symptoms, such as abdominal fullness, constipation, GERD, and diarrhea, in patients with PACS. Additionally, the study assessed microbiota alterations and evaluated mucosal barrier function using confocal laser endomicroscopy (CLE) to elucidate mechanisms underlying GI manifestations in PACS.
Methods: Data from 1,316 PACS patients at Taipei Veteran General Hospital (Jan 2021–Jun 2022) were analyzed. GI symptoms were identified via patient-reported outcomes. Microbiota alterations were assessed using 16S rRNA sequencing at
baseline (Cov1) and three months later (Cov2). CLE was performed on five patients with prominent GI symptoms to assess mucosal barrier integrity. Statistical analyses included descriptive statistics and multivariate regression.
Results: Among 1,316 PACS patients, 282 (21.4%) reported GI symptoms, with constipation (12.8%), gastroesophageal reflux disease (GERD) (10.0%), abdominal fullness (5.4%), and diarrhea (0.8%) being most prevalent. Constipation and abdominal fullness were associated with end-stage renal disease (ESRD) and advanced age ($\ge$75 years). GERD was linked to acute kidney injury (AKI), ESRD, and chronic liver disease. Diarrhea was associated with AKI and chronic liver disease. Microbiota analysis showed decreased Fusobacteria and Erysipelotrichaceae, and increased Bacteroidota and Lachnospiraceae over time. The Firmicutes/Bacteroidota ratio declined (p = 0.015). CLE in five patients revealed fluorescein leakage at intercellular junctions, indicating mucosal barrier dysfunction
Conclusions: This study highlights a substantial prevalence of GI symptoms in PACS and identifies advanced age, ESRD, AKI, and chronic liver disease as key risk factors. Gut microbiota alterations and mucosal barrier impairment suggest potential mechanisms for symptom persistence. These findings enhance understanding of GI PACS pathophysiology and support further investigation into microbiome and barrier-targeted therapies.
COMPARISON OF VONOPRAZANBASED VERSUS LANSOPRAZOLEBASED TRIPLE THERAPY, HIGH DOSE DUAL THERAPY, BISMUTH AND NONBISMUTH QUADRUPLE THERAPY IN THE FIRST-LINE TREATMENT OF HELICOBACTER PYLORI INFECTION –A MULTICENTER, OPEN LABELLED, RANDOMIZED TRIAL
Mei-Jyh Chen1,2, Yu-Jen Fang3, Po-Yueh Chen4, Chieh-Chang Chen1,2, Ming-Shiang Wu1,2, Jyh-Ming Liou1,2,5
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Department of Internal Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
3Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Yun-Lin Branch, Yun-lin, Taiwan
4Department of Internal Medicine, Chia-Yi Christian Hospital, Chiayi, Taiwan
5Department of Internal Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
比較含 Vonoprazan 與 Lansoprazole 的
二合一療法、三合一療法與四合一療法 在幽門桿菌第一線治療的多中心隨機分 派臨床試驗
陳美志1,2 方佑仁3 陳柏岳4 陳介章1,2 吳明賢1,2 劉志銘1,2,5
1 台大醫院消化內科
2 國立臺灣大學醫學院內科
3 台大醫院雲林分院消化內科
4 嘉義基督教醫院內科
5 台大醫院癌醫分院內科
Background: The eradication rates of empirical triple therapy have decreased. Vonoprazan, a potassiumcompetitive acid blocker (PCAB), is known to have a superior effect on inhibiting gastric acid secretion compared to traditional proton pump inhibitors (PPIs).
Aims: We conducted a randomized trial to evaluate the efficacy of 14-day vonoprazan-based therapies
(dual, triple, bismuth quadruple, and hybrid) compared to lansoprazole-based therapies (bismuth quadruple and triple) as first-line treatments.
Methods: Using block randomization (block size 16, 1:1 ratio), 1,200 adults aged 20+ with confirmed H. pylori infection will be assigned to one of eight treatment regimens: 14-day vonoprazan-based triple therapy (T-V14), 7-day vonoprazan-based triple therapy (T-V7), 14-day vonoprazan-based dual therapy (D-V14), 14-day vonoprazan-based highdose dual therapy (HD-V14), 14-day vonoprazanbased bismuth quadruple therapy (BQ-V14), 14-day vonoprazan-based reverse hybrid therapy (RH-V14), 14-day lansoprazole-based bismuth quadruple therapy (BQ-L14), or 14-day lansoprazole-based triple therapy (T-L14). Primary outcomes include eradication rates assessed in ITT and PP analyses. The secondary outcomes are the changes of gut microbiota, antibiotic resistance, and metabolic parameters.
Results: Among 809 patients, 14-day vonoprazanbased bismuth quadruple therapy showed the highest eradication rates: 96.0% (95% CI: 92.1%–99.8%) in ITT and 99.0% (95% CI: 96.9%–100%) in PP, followed by reverse hybrid therapy (96.1%, 95% CI: 92.3%–99.9% in ITT and PP). Other vonoprazan-based regimens also showed strong efficacy, including 14day triple therapy (92.0%, 95% CI: 87.1%–97.4% in ITT and 93.1%, 95% CI: 88.2%–98.0% in PP), dual therapy (92.2%, 95% CI: 83.4%–96.1% in ITT and 93.1%, 95% CI: 84.7%–96.9% in PP), and high-dose dual therapy (93.3, 95% CI: 88.6%–98.1% in ITT and 93.3, 95% CI: 88.5%–98.1% in PP). The 7-day vonoprazan-based triple therapy had an eradication rate of 88.9% (95% CI: 82.7%–95.1%). The lowest eradication rate was in the 14-day lansoprazole-based triple therapy group (87.0%, 95% CI: 80.4%–93.6%). Adverse effect rates ranged from 30.6% to 57.3% with the highest in the lansoprazole-based bismuth quadruple therapy group. A trend of decrease of insulin resistance was observed after eradication therapy (p = 0.018). The transient increase of antibiotic resistance of Escherichia coli at week 2 was restored to basal state at week 8.
Conclusions: Our study demonstrates that vonoprazan-based therapies, particularly the 14-day bismuth quadruple regimen, reverse hybrid therapy, and dual therapy achieve high eradication rates and are better tolerated than lansoprazole-based therapies.
CHOLESTASIS AND LANSOPRAZOLE
ALTER GUT MICROBIAL STRUCTURE BUT NOT RICHNESS IN COMMON BILE DUCT LIGATION RATS MODEL: A PILOT STUDY
Kuan-Pei Lin
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
膽汁淤積與氫離子幫浦抑制劑 (Lansoprazole)改變大鼠腸道菌相結構 但不影響菌相豐富度之先導性研究
林官霈
臺中榮民總醫院胃腸肝膽科
Background: Cholestasis alters bile flow and composition, which can significantly impact the gut microbial ecosystem through modulation of microbial metabolites and host immunity. Lansoprazole, a commonly used proton pump inhibitor (PPI), may further influence intestinal microbiota, especially under cholestatic conditions.
Aims: This study aimed to investigate the effects of common bile duct ligation (CBDL) and lansoprazole treatment on fecal microbiota composition in a rat model, with a particular focus on key genus-level alterations.
Methods: Sprague-Dawley rats (n = 21, sex not stratified) were randomly assigned to four groups: Sham (n = 5), Sham + lansoprazole (n = 5), CBDL (n = 6), and CBDL + lansoprazole (n = 5). Two weeks after surgery, fecal samples were collected for 16S rRNA gene sequencing (V4 region). Taxonomic classification was performed using the SILVA database. Given the non-normal and zero-inflated nature of the data, genus-level comparisons were conducted using Kruskal–Wallis tests followed by Mann–Whitney U post hoc tests with false discovery rate (FDR) correction.
Results: Alpha diversity indices (Shannon, observed OTUs) showed no significant differences among groups, indicating comparable microbial richness and evenness. However, beta diversity analysis based on Bray–Curtis dissimilarity revealed distinct clustering between the CBDL-related groups and the Sham groups, reflecting significant changes in community composition. Notably, Lactobacillus was enriched in CBDL rats, whereas Prevotella
and Ruminococcus were significantly reduced. Lansoprazole further modulated gut microbiota composition, especially in cholestatic animals. Conclusions: CBDL-induced cholestasis and lansoprazole treatment altered the composition— but not the richness—of the gut microbiota. The observed dysregulation of Lactobacillus, Prevotella, and Ruminococcus suggests a microbial shift potentially relevant to mucosal immunity and bile acid metabolism. These findings provide insight into gut microbial changes under bile duct obstruction and support further mechanistic studies of microbiota-targeted interventions in cholestatic liver disease.
Chun-Chia Yang1, Pei-Jui Wu1, Feng-Woei Tsay2, Deng-Chyang Wu3, Jyh-Chin Yang4, Seng-Kee Chuah5, Kuan-Yang Chen6, Chien-Lin Chen7, Chia-Long Lee8, Chih-An Shih9, Yu-Hwa Liu10, Sz-Iuan Shiu11, Wei-Chen Tai5, Chao-Hung Kuo3, Wei-Yi Lei7,
Sung-Shuo Kao12, Tzung-Jiun Tsai2, I-Che Feng1, Ping-I Hsu13, Ming-Jen Sheu1
1Division of Hepatogastroenterology, Department of Internal Medicine, Chi Mei Medical Center, Tainan, Taiwan
2Division of Gastroenterology and Hepatology, Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
3Division of Gastroenterology, Department of Internal Medicine Kaohsiung Medical University Chung-Ho Memorial Hospital, Kaohsiung, Taiwan
4Division of Gastroenterology, Department of Internal Medicine, Hospital and College of Medicine, National Taiwan University, Taipei, Taiwan
5Division of Hepatogastroenterology, Department of Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, and Chang Gung University College of Medicine, Kaohsiung, Taiwan
6Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taipei City Hospital, Renai Branch, Taipei, Taiwan
7Division of Gastroenterology and Hepatology, Department of Internal Medicine, Hualien Tzu Chi Hospital, Hualien, Taiwan
8Division of Gastroenterology and Hepatology, Department of Internal Medicine, Cathay General Hospital, Taipei, Taiwan
9Division of Gastroenterology and Hepatology, Department of Internal Medicine, Antai Medical Care Corporation, Antai Tian-Sheng Memorial Hospital, Pingtung, Taiwan
10Division of Gastroenterology, Department of Internal Medicine Shin Kong Wu Huo-Shih Memorial Hospital, Taipei, Taiwan
11Division of Gastroenterology and Hepatology,
Department of Internal Medicine, Taichung
Veterans General Hospital, Taichung, Taiwan
12Division of Gastroenterology and Hepatology, Department of Internal Medicine, Pingtung
Veterans General Hospital, Pingtung, Taiwan
13Department of Medicine, An Nan Hospital, China Medical University, Tainan, Taiwan
臺灣幽門螺旋桿菌抗生素抗藥性於 2019 至 2024 年間的變化趨勢
楊峻嘉1 吳佩叡1 蔡峯偉2 吳登強3 楊智欽4 蔡成枝5 陳冠仰6 陳健麟7 李嘉龍8 石志安9 劉玉華10 許斯淵11 戴維震5 郭昭宏3 雷尉毅7 高崧碩12 蔡騌圳2 馮意哲1 許秉毅13 許銘仁1
1 奇美醫院胃腸肝膽科
2 高雄榮民總醫院胃腸肝膽科
3 高雄醫學大學附設中和紀念醫院胃腸肝膽科
4 國立臺灣大學醫學院附設醫院胃腸肝膽科
5 高雄長庚紀念醫院胃腸肝膽科
6 臺北市立聯合醫院仁愛院區胃腸肝膽科
7 花蓮慈濟醫院胃腸肝膽科
8 國泰綜合醫院胃腸肝膽科
9 安泰醫院胃腸肝膽科
10 新光吳火獅紀念醫院胃腸肝膽科
11 臺中榮民總醫院胃腸肝膽科
12 屏東榮民總醫院胃腸肝膽科
13 臺南市立安南醫院胃腸肝膽科
Background: Antibiotic resistance significantly impacts the treatment failure rates of Helicobacter pylori (H. pylori) infections.
Aims: This study aimed to assess the trends in primary antibiotic resistance of H. pylori in Taiwan over the past six years and to compare the differences in the frequencies of antibiotic resistance among different regions of Taiwan.
Methods: We conducted a retrospective analysis of H. pylori isolates from Taiwanese who had not undergone previous treatments (n = 1408), collected between January 2019 and December 2024. Susceptibility of these strains to amoxicillin, clarithromycin, levofloxacin, metronidazole, and tetracycline was tested using the Epsilometer test. We analyzed the trends in single and dual antibiotic resistance profiles over the study period, and compared antibiotic resistance across different regions (northern, southern and eastern areas) of Taiwan.
Results: The overall resistance rates for H. pylori
to amoxicillin, clarithromycin, metronidazole, tetracycline, and levofloxacin in Taiwan were 1.3%, 18.0%, 31.0%, 0.8%, and 28.7%, respectively. Tetracycline resistance increased significantly from 0% in 2019 to 3.5% in 2024 (p-value in χ² test for linear trend: <0.001), while metronidazole resistance declined from 35.5% to 13.0% (p-value in χ² test for linear trend: <0.001). No significant changes of amoxicillin, clarithromycin and levofloxacin resistances were observed. The dual antibiotic resistances to clarithromycin plus tetracycline, and metronidazole plus tetracycline both increased significantly from 0% to 1.7% from 2019 to 2024 (p-value in χ² test for linear trend: <0.05). Furthermore, no significant regional differences in resistance frequencies except for levofloxacin were detected.
Conclusions: Primary antibiotic resistance to tetracycline in H. pylori has increased in Taiwan from 2019 to 2024, while resistance to metronidazole have decreased during the same period. The dual resistance to clarithromycin plus tetracycline and metronidazole plus tetracycline both increased significantly.
CLINICAL CHARACTERISTICS OF VONOPRAZAN COMBINED HIGH DOSE AMOXICILLIN DUAL THERAPY FOR HELICOBACTER PYLORI: ANALYSIS OF ADULT PATIENT IN YIN KUI HOSPITAL MACAU
Wai Kit Choi, Choy Yee Tham
Department of Internal Medicine, Macau Yin Kui Hospital, Macau
伏諾拉生聯合高劑量阿莫西林二聯治療 幽門螺旋桿菌
Background: Helicobacter pylori (HP) as primary carcinogen in WHO defined. It relative to multiple gastric disease such as peptic ulcer, gastric carcinoma, gastric lymphoma, chronic gastritis, gastric intestinal metaplasia. Therefore, Helicobacter pylori eradication is an important issue in improving public health. However, Helicobacter pylori eradication rate was not satisfied with many reasons such as antibiotic overused, lack of medication treatment standardization, poor patient compliance due to medication side effects, antibiotic resistance, and patient understanding on the important of the completeness course of medication. International guidelines recommended various regimens. Some cases failure found using typical triple therapy which is proton pump inhibitors (PPI) with two kinds of antibiotic and/or quadruple therapy (PPI, two kinds of antibiotic and bismuth) because they have varying degrees of drug resistance and side effect. In these years, Dual therapy of Vonoprazan combined with amoxicillin found able to reduce the side effects of antibiotics, improve patient compliance, and achieve a satisfactory success rate of Helicobacter pylori eradication, this study analyzed the actual efficacy of the program based on data from a local private hospital in Macau. This report showed a private hospital real data in Macau community.
Aims: Understand the current effectiveness, clinical characteristics, and efficacy of Vonoprazan combined with amoxicillin dual therapy in the Macao population, and provide a basis for clinical treatment.
Methods: Retrospective analysis of the general
situation, effectiveness and clinical characteristics of dual therapy with Vonoprazan combined with highdose amoxicillin in a private hospital in Macau from September 1, 2022, to August 31, 2024.
Results: There were 82 patients in total, with an average age of 44 years old. The male to female ratio in the treatment group was similar, and some of them were secondary treatments after failure of conventional first-line treatment. The program group was given Vonoprazan 40 mg/day + amoxicillin 3 g/ day x 14 days of treatment, and carbon 13 breath test (UBT) was performed after 4–6 weeks. Negative UBT was the criterion for successful eradication, and the eradication success rate was 92%. It is similar to the conventional triple therapy (PPI with two antibiotics) and is better than the guideline’s goal of achieving an eradication rate of 85%.
Conclusions: As a new type of anti-acid drug, Vonoprazan, combined with amoxicillin as a doublecombination method, has similar therapeutic effects to the general triple/quadruple sterilization regimen, but can relatively reduce side effects and further improve patient compliance, which is worthwhile. As a treatment plan for clinical first-line use.
FOURTEEN-DAY VONOPRAZANBASED DUAL THERAPY WITH AMOXICILLIN AS FIRST-LINE HELICOBACTER PYLORI TREATMENT IN COMPARISON WITH EXTENDED SEQUENTIAL THERAPY: A RANDOMIZED CONTROLLED TRIAL IN TAIWAN
Te-Ling Ma1, Yen-Po Liou1,5, Chen-Ya Kuo1,2, Kuang-Yi Sung1,3, Yu-Tse Chiu1,2,3, Po-Rui Wu1, Fu-Jen Lee1,2,4, Kai-Shun Liang1,2, Kuan-Wei Wu1, Yu-Tsung Chen1,2, Chi-Yang Chang1,2
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Fu Jen Catholic University Hospital, New Taipei City, Taiwan
2School of Medicine, College of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan
3Institute of Biomedical Informatics, National Yang Ming Chiao Tung University, Taipei, Taiwan
4Graduate Institute of Public Health, College of Public Health, China Medical University, Taichung, Taiwan
5Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
包含 Vonoprazan 及高劑量 Amoxicillin
的十四天二合一處方作為治療幽門螺旋 桿菌的一線殺菌藥物,對比目前標準的 二週系列性治療 一隨機分派性試驗
馬德齡1 劉彥伯1,5 郭震亞1,2 宋寬益1,3 邱毓澤1,2,3
吳柏叡1 李輔仁1,2,4 梁凱舜1,2 吳冠緯1 陳昱宗1,2 張吉仰1,2
1 天主教輔仁大學附設醫院肝膽腸胃科
2 天主教輔仁大學醫學系
3 國立陽明交通大學生物醫學資訊研究所
4 中國醫藥大學公共衛生學系
5 國立臺灣大學醫學院附設醫院內科部
Background: Helicobacter pylori infection is a well-established risk factor for peptic ulcer disease and gastric cancer. The current standard firstline treatment, extended proton pump inhibitor (PPI)-based sequential therapy, has an eradication rate of 90.7% (95% CI, 87.4%–94.0%). However, its complexity can confuse patients and lead to
treatment failure. The emerging vonoprazan-based dual therapy offers an appealing alternative due to its simplicity and low pill burden.
Aims: This study aimed to compare the efficacy and safety of the current standard first-line regimen, sequential therapy, with vonoprazan-based dual therapy using amoxicillin.
Methods: This was a single-center, prospective, randomized controlled trial with a non-inferiority design. Subjects aged over 20 years with confirmed H. pylori infection were prospectively enrolled from Fu Jen Catholic University Hospital. Participants were randomly assigned to the VA-14 group (vonoprazan 20 mg + amoxicillin 1000 mg twice daily for 14 days) or the S-14 group (lansoprazole 30 mg + amoxicillin 1000 mg twice daily for 7 days, followed by lansoprazole 30 mg + clarithromycin 500 mg + metronidazole 500 mg twice daily for 7 days). At the conclusion of their 14-day antibiotic regimen, each patient was asked to complete selfadministered questionnaires to report any adverse effects. The primary endpoint was the eradication rate for first-line treatment, evaluated using the urea breath test after 4 weeks. Non-inferiority was determined using the Farrington-Manning method. Secondary outcomes included adverse event rates and compliance.
Results: Between December 2023 and December 2024, a total of 337 patients were recruited. The eradication rates by per-protocol (PP) and intentionto-treat (ITT) analyses were 90.9%/83.9% for the VA-14 group and 85.6%/73.9% for the S-14 group, respectively. The VA-14 regimen was non-inferior to S-14 in ITT analysis (Farrington-Manning method, p < 0.0001). The VA-14 group experienced fewer instances of diarrhea, taste distortion, nausea, poor appetite, dizziness, any adverse events and severe adverse events compared to the S-14 group. However, the VA-14 group was more prone to experiencing constipation. Overall, compliance with taking all pills correctly was significantly higher in the VA-14 group (93.8%) compared to the S-14 group (90.0%) (Chi-square test, p = 0.04)
Conclusions: Our findings support the use of vonoprazan-based dual therapy with amoxicillin as a potential standard first-line treatment for H. pylori infection.
STEATOTIC LIVER DISEASE IS ASSOCIATED WITH A REDUCED HCC RISK IN NUCLEOS(T)IDE-TREATED CHRONIC HEPATITIS B: A SUBGROUP HAZARD ANALYSIS
Hung-Wei Wang1,2, Hsueh-Chou Lai1,3, Wei-Fan Hsu1,3, Sheng-Hung Chen1,2, Cheng-Yuan Peng1,2
1Center for Digestive Medicine, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan
2School of Medicine, China Medical University, Taichung, Taiwan
3School of Chinese Medicine, China Medical University, Taichung, Taiwan
脂肪肝病與接受核 苷(酸)類藥物治療 之慢性 B 型肝炎患者的肝細胞癌風險降 低相關:一項亞組風險分析
王鴻偉1,2 賴學洲1,3 許偉帆1,3 陳昇弘1,2 彭成元1,2
1 中國醫藥大學附設醫院消化醫學中心
2 中國醫藥大學醫學系
3 中國醫藥大學中醫學系
Background: Despite antiviral therapy, the risk of hepatocellular carcinoma (HCC) persists in patients with chronic hepatitis B (CHB). Coexisting steatotic liver disease (SLD) may reduce this risk, although the underlying mechanisms remain unclear.
Aims: To investigate how SLD influences HCC risk in nucleos(t)ide analogue-treated CHB patients.
Methods: Subgroup hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated, and forest plots were constructed to evaluate whether SLD affects HCC risk across strata in nucleos(t)ide analogue-treated CHB patients.
Results: A total of 1,012 CHB patients receiving oral antiviral therapy were enrolled: 702 with SLD and 310 without. Seventy-three HCC events occurred. In univariable Cox regression analysis, SLD was associated with an overall HR of 0.467 (95% CI: 0.295–0.739), indicating a 53% reduction in HCC risk. Subgroup analyses revealed significant heterogeneity by age (cut-off: 50 years), cirrhosis status, and cardiometabolic risk factors (CMRFs). Among patients aged ≥50 years, SLD conferred a pronounced protective effect (HR: 0.383; 95% CI: 0.225–0.653), while those aged <50 years exhibited
a non-significant trend toward increased HCC risk (HR: 1.674; 95% CI: 0.484–5.787). In cirrhotic patients, SLD remained protective (HR: 0.566; 95% CI: 0.342–0.935), whereas no clear effect was observed in noncirrhotic patients (HR: 0.946; 95% CI: 0.256–3.503). The effect of SLD also varied by CMRFs: HRs were 0.357 (95% CI: 0.216–0.588) for ≥1 CMRF, 0.262 (95% CI: 0.129–0.529) for ≥2 CMRFs, and 0.514 (95% CI: 0.276–0.957) for <2 CMRFs. Among patients aged ≥50 years, fibrosis severity was consistently lower in the SLD group compared to the non-SLD group at baseline (median FIB-4: 2.45 vs. 4.42; P < 0.001) and at years 1, 3, and 5. Liver stiffness measurements (LSM) were also lower at year 1 (median: 1.20 vs. 1.38 m/s; P = 0.002) and remained lower throughout follow-up. In cirrhotic patients, baseline FIB-4 was markedly lower in those with SLD (median: 2.38 vs. 5.31; P < 0.001), and this difference persisted over time. In patients with ≥1, ≥2, or <2 CMRFs, SLD was consistently associated with significantly lower baseline FIB-4 scores (1.95 vs. 3.89; 2.13 vs. 3.90; and 1.84 vs. 3.00, respectively; all P < 0.001), this pattern maintained throughout follow-up. Similar trends were observed for LSM. However, the majority of percentage changes from baseline in quantitative HBsAg (qHBsAg), HBV DNA, and FIB-4 during treatment did not significantly differ between the SLD and non-SLD groups. Notably, qHBsAg levels at most time points were higher in SLD than in non-SLD group among those aged ≥50 years, with cirrhosis, or with CMRFs.
Conclusions: In nucleos(t)ide analogue-treated CHB patients, SLD was associated with a significantly reduced risk of HCC, particularly in those aged ≥ 50 years, with cirrhosis, or with CMRFs. This protective effect may result from the persistently lower fibrosis status seen in SLD patients, despite their higher qHBsAg levels and comparable antiviral treatment response to their non-SLD counterparts.
GCKR POLYMORPHISMS INCREASE THE RISKS OF LOW BONE MINERAL DENSITY IN YOUNG AND NONOBESE PATIENTS WITH MASLD AND HYPERURICEMIA
Ying-Ying Yang1,2,3, Tzu-Hao Li4,6, Hsiao-Yun Yeh1,3, Chien-Wei Su2,3, Hwai-I Yang5, Ming-Chih Hou2,3, Han-Chieh Lin2
1Department of Medical Education, Taipei
Veterans General Hospital, Taipei, Taiwan
2Division of Gastroenertology and Hepatology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
3School of Medicine, College of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
4Division of Allergy, Immunology, and Rheumatology, Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan
5Genomics Research Center, Academia Sinica, Taipei, Taiwan
6School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan
GCKR 多態性增加患有 MASLD 和高尿酸 血症的年輕非肥胖患者骨密度降低的風 險
楊盈盈1,2,3 黎子豪4,6 葉筱芸1,3 蘇建維2,3 楊懷壹5 侯明志2,3 林漢傑2
1 臺北榮民總醫院教學部
2 臺北榮民總醫院胃腸肝膽科
3 國立陽明交通大學醫學系
4 新光吳火獅紀念醫院過敏免疫風濕科
5 中央研究院基因體中心
6 天主教輔仁大學醫學系
Background: Metabolic-associated steatotic liver disease (MASLD) encompasses common comorbidities including low bone mineral density (BMD) and hyperuricemia (HU), yet relevant genetic analyses are limited.
Aims: This study aimed to investigate the genetic effects of risk single nucleotide polymorphisms (SNPs) on the occurrence of low BMD in patients with MASLD and HU, particularly focusing on relatively young or non-obese populations.
Methods: We conducted a cross-sectional study
utilizing data from the Taiwan Biobank, screening a total of 150,709 participants who were prospectively enrolled over a period of 13 years. The risk SNPs of MASLD were identified. Genotype analyses of HU and its effects on the occurrence of low BMD in the general population were evaluated, with further analyses of common SNPs focusing on patients with MASLD, including subgroup analyses on relatively young and non-obese populations.
Results: A total of 20,496 participants were eligible for analysis, including 7,526 patients with MASLD. Several risk SNPs for MASLD were identified.
Furthermore, MASLD patients carrying the PNPLA3rs738409 C_C, PNPLA3-rs2896019 T_T, GCKRrs780094 T_T, and GCKR-rs1260326 T_T genotypes exhibited an increased risk of comorbidity with HU. Trend analysis revealed that the T alleles in GCKRrs780094 and GCKR-rs1260326 were associated with the occurrence of low BMD in MASLD individuals comorbid with HU, particularly among relatively young or non-obese populations. In relatively young, non-obese patients with MASLD and HU, genetic effects significantly increase the risk of occurrence of low BMD.
Conclusions: Although the risk of BMD loss may seem ostensibly low due to age and anthropometric characteristics, genetic effects are still significant in this subgroup. Therefore, heightened awareness and close follow-up are recommended.
51
INHIBITION OF VISCERAL ADIPOSE TISSUE-DERIVED PATHOGENIC SIGNALS BY ACTIVATION OF ADENOSINE A2AR IMPROVES HEPATIC AND CARDIAC DYSFUNCTION OF NASH MICE
Ying-Ying Yang1,2,3, Hsiao-Yun Yeh1,2, Chien-Wei Su2,3,4, Ming-Chih Hou3, Han-Chieh Lin3
1Department of Medical Education, Taipei Veterans General Hospital, Taipei, Taiwan
2Faculty of Medicine, School of Medicine, National Yang-Ming Chiao Tung University, Taipei, Taiwan
3Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
4Division of General Medicine, Department of Internal Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
透過活化腺 苷 A2AR 抑制內臟脂肪組織 來源的致病訊號可改善 NASH 小鼠的肝 功能和心臟功能障礙
楊盈盈1,2,3 葉筱芸1,2 蘇建維2,3,4 侯明志3 林漢傑3
1 臺北榮民總醫院教學部
2 國立陽明交通大學醫學系
3 臺北榮民總醫院胃腸肝膽科
4 臺北榮民總醫院一般內科
Background: A2AR-disrupted mice is characterized by severe systemic and visceral adipose tissue (VAT) inflammation. Increasing adenosine cyclase (AC), cAMP and protein kinase A (PKA) formation through A2AR activation suppress systemic/VAT inflammation in obese mice.
Aims: This study explores the effects of four-weeks A2AR agonist PSB0777 treatment on the VATdriven pathogenic signals in hepatic and cardiac dysfunction of non-alcoholic steatohepatitis (NASH) obese mice.
Methods: HFD-fed NASH mice were included for measurement of hepatic, visceral adipose tissue (VAT) and cardiac inflammation, injury, steatosis, apoptosis, fibrosis without and with 4 weeks of PSB07777 treatments. Then, body composition, cardiac echogram, various markers in liver, VAT and heart tissues, were measured. The AD2AR-AC-cAMP-
PKA signal pathway, injury, fibrotic, contractile, apoptotic signals were evaluated.
Results: Among NASH mice with cardiac dysfunction, simultaneous decrease in the A2AR, AC, cAMP and PKA levels were observed in VAT, liver, and heart. PSB0777 treatment significantly restores AC, cAMP, PKA, HSL levels, decreased SREBP-1/FASN, MCP-1 and CD68 levels, reduces infiltrated CD11b+F4/80+ cells and adipogenesis in VAT of NASH + PSB0777 mice. The changes in VAT were accompanied by the suppression of hepatic and cardiac lipogenic/ inflammatory/injury/apoptotic/fibrotic markers, the normalization of cardiac contractile [sarco/ endoplasmic reticulum Ca2+ ATPase (SERCA2)] marker, and cardiac dysfunction.
Conclusions: The study revealed that, A2AR agonists are potential agent to inhibit the effects of VAT inflammation-driven pathogenic signals on the hepatic and cardiac lipogenesis, inflammation, injury, apoptosis, fibrosis, hypo-contractility, and subsequently improve hepatic and cardiac dysfunction in NASH mice
52
PROGNOSTIC VALUE OF HEPATIC FIBROSIS IDENTIFIED BY THE FIBROSIS-4 INDEX IN HEART FAILURE WITH PRESERVED EJECTION FRACTION
Kai-Chun Chang1,4, Tung-Hung Su2,3, Kuan-Chih Huang4, Zheng-Wei Chen1, Jen-Fang Cheng1, Ting-Tse Lin1, Lian-Yu Lin1, Cho-Kai Wu1
1Division of Cardiology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
3Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
4Division of Cardiology, Department of Internal Medicine, National Taiwan University Hospital Hsinchu Branch, Hsinchu, Taiwan
肝纖維化指數(Fibrosis-4 Index)在射 出分率正常心衰竭患者中的預後價值
張凱鈞1,4 蘇東弘2,3 黃冠智4 陳政瑋1 鄭人方1 林廷澤1 林亮宇1 吳卓鍇1
1 國立臺灣大學醫學院附設醫院心臟內科
2 國立臺灣大學醫學院附設醫院胃腸肝膽內科
3 國立臺灣大學醫學院附設醫院肝炎研究中心
4 國立臺灣大學醫學院附設醫院新竹臺大分院心臟內 科
Background: Heart failure (HF) is a syndrome with high mortality, often associated with abnormal liver function tests, reflecting heart-liver interactions.
Aims: We investigated the association between hepatic fibrosis identified by the FIB-4 index and mortality in patients with HF with preserved ejection fraction (HFpEF).
Methods: Patients with HFpEF confirmed by diuretics use and echocardiography from 2006 to 2022 were retrospectively included if complete liver profiles were available. The patients were classified according to risk of liver fibrosis assessed by FIB-4. The primary outcome was death, which was further classified into cardiovascular and non-cardiovascular death. Multi-variable analysis was done for adjust for confounding factors and restricted cubic spline analysis was performed.
Results: 3293 patients were included for analysis and 42.5% patients were classified as group 3, the highrisk group according to FIB-4 score. With a median follow-up of 2.6 years, 1918 (58.2%) patients died, and 72.5% were classified as non-cardiovascular death. Compared with FIB-4 < 1.3, there are significantly higher risk of all-cause mortality (adjusted hazard ratio (aHR): 1.27, 95% CI: 1.03-1.57), cardiovasculardeath (aHR: 1.64, 95% CI: 1.02-2.62) in FIB-4 > 2.67. In subgroup analysis for patients below 65-year-old, FIB-4 positively correlated with both cardiovascular death and non-cardiovascular death.
Conclusions: FIB-4 is a simple yet effective predictor of mortality in HFpEF, particularly in patients under 65. Comprehensive liver function assessment is essential for risk stratification in this population.
53
CARDIOMETABOLIC BURDEN INCREASES THE RISK OF KIDNEY FAILURE IN A DOSE-DEPENDENT MANNER AMONG PATIENTS WITH STEATOTIC
Han-Tse Cheng1, Hsin-Yun Wu3, Tung-Hung Su2, Kai-Chun Chang1, Shang-Chin Huang4, Tai-Shuan Lai5, Tai-Chung Tseng2, Chun-Ming Hong2, Chen-Hua Liu2, Hung-Chih Yang2, Chun-Jen Liu2, Jia-Horng Kao2
1Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Division of Gastroenterology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
3Division of Gastroenterology, Department of Internal Medicine, National Taiwan University Hospital, Jinshan Branch, Taipei, Taiwan
4Division of Gastroenterology, Department of Internal Medicine, National Taiwan University Hospital, Bei-Hu Branch, Taipei, Taiwan
5Division of Nephrology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
心血管代謝風險因子的負荷呈劑量依賴 性地增加脂肪性肝病患者發生腎功能衰 竭的風險
鄭翰澤1 吳心耘3 蘇東弘2 張凱鈞1 黃上秦4 賴台軒5 曾岱宗2 洪俊銘2 劉振驊2 楊宏志2 劉俊人2 高嘉宏2
1 台大醫院內科部
2 台大醫院胃腸肝膽科
3 台大醫院金山分院胃腸肝膽科
4 台大醫院北護分院胃腸肝膽科
5 台大醫院腎臟科
Background: Emerging evidence links metabolic dysfunction–associated steatotic liver disease (MASLD) with renal outcomes. However, few studies have assessed how cumulative cardiometabolic risk factors (CMRFs) influence kidney failure in MASLD patients.
Aims: We aimed to examine the impact of metabolic burden on the incidence of kidney failure among individuals with steatotic liver disease (SLD).
Methods: We conducted a retrospective cohort study using the National Taiwan University Hospital
Integrated Medical Database from 2006 to 2019. A total of 14,343 patients with persistent steatosis confirmed by abdominal ultrasound were included. MASLD was defined by hepatic steatosis with at least 1 CMRF, based on the 2023 multisociety consensus. Patients were classified as “MASLD” (n = 12,296), “SLD with later MASLD” (n = 1,442), and “SLD without later MASLD” (n = 605) groups. The primary outcome was kidney failure, defined by chronic kidney disease (CKD) stage 5 or receiving renal replacement therapy. The Fine–Gray subdistribution hazard model was used to adjust for competing mortality.
Results: MASLD patients were older and had more comorbidities than other groups. After adjusting for age, sex, estimated Glomerular filtration rate (eGFR), malignancy, HBV, HCV, cirrhosis, and rheumatologic disease, MASLD was significantly associated with kidney failure (Sub-distribution Hazard Ratio [SHR] 3.415; 95% CI: 1.092–10.678; P = 0.035) compared with the SLD without later MASLD group. There is also a trend of increased kidney failure risks in patients with SLD who later developed MASLD (SHR: 1.270, 95% CI: 0.380–4.244). When analyzing CMRFs separately, there was a significant dose-dependent association with kidney failure risk. Compared to individuals with no CMRFs, the risk for kidney failure increased with each additional risk factor, with the SHR: 2.01 (95% CI: 1.28–3.15, P = 0.002), 1.85 (95% CI: 1.17–2.91, P = 0.008), 2.93 (95% CI: 1.91–4.50, P < 0.0001), 3.85 (95% CI: 2.50–5.93, P < 0.0001), and 5.84 (95% CI: 3.68–9.26, P < 0.0001) in patients with 1, 2, 3, 4 and 5 CMRFs, respectively. Diabetes mellitus and hypertension were the most significant contributors (SHR 2.17 and 1.76, respectively; both P < 0.0001). In contrast, dyslipidemia and BMI ≥23 kg/m² were not associated with kidney failure development.
Conclusions: There is a dose-dependent relationship between metabolic burden and kidney failure risks in patients with SLD. The cumulative number of CMRFs—particularly diabetes and hypertension— strongly predicts kidney failure. These findings highlight the need for early identification and management of metabolic risks in MASLD to prevent kidney-related complications. 54
ASSOCIATION OF HELICOBACTER PYLORI INFECTION WITH METABOLIC SYNDROME AND LIVER-RELATED METABOLIC DYSFUNCTION IN TAIWANESE ADULTS: A CROSSSECTIONAL STUDY
Yen-Nien Chen1, Ai-Ru Chen1,2, Tzu-Chan Hong1, Yih-Jin Hu2, Ming-Shiang Wu3, Jyh-Ming Liou1,3
1Department of Medicine, National Taiwan University Cancer Center, National Taiwan University College of Medicine, Taipei, Taiwan 2Department of Health promotion and Health Education College of Education, National Taiwan Normal University, Taipei, Taiwan 3Department of Internal Medicine, National Taiwan University Hospital, National Taiwan University College of Medicine, Taipei, Taiwan
幽門螺旋桿菌感染與臺灣成人代謝症候 群及肝臟相關代謝功能障礙的關聯:一 項橫斷式研究
陳彥年1 陳艾如1,2 洪子瞻1 胡益進2 吳明賢3 劉志銘1,3
1 國立臺灣大學醫學院附設醫院癌醫中心分院綜合內 科部
2 國立臺灣師範大學健康促進與衛生教育學系 3 國立臺灣大學醫學院附設醫院內科部
Background: Helicobacter pylori (H. pylori) is a common, chronic infection associated with peptic ulcers and an increased risk of gastric cancer. Recent studies suggest that H. pylori may also be linked to metabolic disorders, including metabolic syndrome (MetS) and metabolic dysfunction-associated steatotic liver disease (MASLD). Although evidence indicates a connection between H. pylori infection and components of MetS and liver steatosis, the clinical significance of these associations remains uncertain.
Aims: This study aimed to investigate the association between H. pylori infection and metabolic syndrome (MetS), metabolic dysfunction-associated steatotic liver disease (MASLD), and liver fibrosis in a Taiwanese adult population.
Methods: This cross-sectional study included 2,343 adults who underwent self-paid health check-ups at a medical center in northern Taiwan between 2021 and 2024. Active H. pylori infection was assessed using the ¹³C-urea breath test, and MetS was defined
based on national guidelines. MASLD was diagnosed by the presence of ultrasound-detected hepatic steatosis and at least one metabolic risk factor. Liver fibrosis risk was evaluated using non-invasive indices, including FIB-4, FAST, and Agile scores. Multivariable logistic and linear regression models were used to analyze associations, adjusting for potential confounders including age, sex, education level, lifestyle factors, hepatitis B and C infection, liver enzymes, and insulin resistance.
Results: The study found that H. pylori infection was significantly associated with metabolic syndrome (adjusted OR = 1.81, 95% CI: 1.23–2.67, p = 0.003) and higher LDL cholesterol and HbA1c levels, independent of obesity or liver fat. No significant associations were found with MASLD, any grade of hepatic steatosis, or liver fibrosis indices. However, individuals with H. pylori infection showed a tendency toward metabolic abnormalities, including higher LDL and HbA1c levels.
Conclusions: H. pylori infection is independently associated with metabolic abnormalities and may serve as a modifiable risk factor in cardiometabolic health assessments. These findings highlight the potential clinical utility of considering H. pylori infection as a marker for metabolic risk, providing a basis for future screening and prevention strategies.
P.001
SUMMIT: A NOVEL DEEP LEARNING MODEL USING SERIAL IMPUTATIONFREE CLINICAL DATA FOR HCC RISK PREDICTION IN CHRONIC HEPATITIS B
Tung-Hung Su1, Yi-Hsien Hsieh2, Shao-Wu Lee3, Fen-Fang Chen1, You-Hsiang Wang2, Francis SK Poon3, Wei-Yu Kao4, Weichung Wang5, Che Lin2,6,7,8, Jia-Horng Kao1
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Graduate Institute of Communication Engineering, National Taiwan University, Taipei, Taiwan
3Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
4Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taipei Medical University Hospital, Taipei, Taiwan
5Institute of Applied Mathematical Sciences, National Taiwan University, Taipei, Taiwan
6Department of Electrical Engineering, National Taiwan University, Taipei, Taiwan
7Smart Medicine and Health Informatics Program, National Taiwan University, Taipei, Taiwan
8Center for Advanced Computing and Imaging in Biomedicine, National Taiwan University, Taipei, Taiwan
SUMMIT:利用連續且無需補值的臨床資 料預測慢性 B 型肝炎患者的肝細胞癌風 險的深度學習模型
蘇東弘1 謝依諴2 李少武3 陳芬芳1 王宥翔2 潘錫光3 高偉育4 王偉仲5 林澤2,6,7,8 高嘉宏1
1 國立臺灣大學醫學院附設醫院胃腸肝膽科
2 國立臺灣大學電信工程學研究所
3 臺中榮民總醫院胃腸肝膽科
4 臺北醫學大學附設醫院胃腸肝膽科
5 國立臺灣大學應用數學科學研究所
6 國立臺灣大學電機工程學系
7 國立臺灣大學智慧醫療與健康資訊碩士學程
8 國立臺灣大學尖端生醫計算及影像研究中心
Background: Identifying high-risk patients for
hepatocellular carcinoma (HCC) among individuals with chronic hepatitis B (CHB) is crucial for timely surveillance. Although several risk scores have been developed, they often require complete data for calculation at a specific moment.
Aims: We aimed to create an HCC prediction model using serial laboratory and clinical data that accommodates missing values.
Methods: Patients with CHB who were not receiving antiviral therapy and were followed longitudinally at a tertiary medical center in Taiwan were screened. We excluded patients with prior malignancy, hepatitis C, HIV, liver transplantation, or a followup duration of less than five years. Laboratory data (including complete blood count, liver function tests, renal and glucose profiles, and viral markers), abdominal ultrasonographic findings, and hospital admissions within one year before the index date were summarized at three-month intervals. We applied our Scalable nUMerical eMbeddIng Transformer (SUMMIT) model to predict fiveyear HCC development without requiring data imputation. The performance of the SUMMIT model was compared with traditional HBV risk scores (e.g., REACH-B). An external validation was conducted using data from another tertiary medical center. Model performance was evaluated using AUROC, AUPRC, sensitivity, specificity and the C-index, where threshold-sensitive metrics were obtained with a decision threshold maximizing the Youden index on the training set.
Results: A total of 12,455 untreated CHB patients were included, with a median age of 49 years; 53% were male. Of these, 7,060 (HCC: 261, 3.7%) were assigned to the training set, while 4708 patients (HCC: 179, 3.8%) and another 687 patients (HCC: 46, 6.7%) who could calculate the REACH-B score were assigned as two testing sets. Compared with logistic regression, support vector machine, random forest, and XGBoost models, the SUMMIT model achieved significantly higher AUROC (0.902), AUPRC (0.317; baseline: 0.023), sensitivity (0.750), specificity (0.877), and C-index (0.898) for predicting five-year HCC development. These metrics outperformed those of traditional models such as REACH-B (AUROC: 0.794), CU-HCC (AUROC: 0.868), RWS-HCC (AUROC: 0.856), and AGED (AUROC: 0.756) scores. The sensitivity of the SUMMIT model increased as the time approached HCC development. Using the external validation dataset (n = 9,038), the AUROC and AUPRC were 0.792 and 0.024 (baseline: 0.007),
respectively.
Conclusions: The SUMMIT model accurately estimates HCC risk using serial laboratory and clinical data in untreated CHB patients and accommodates missing data. It outperformed other machine learning algorithms and traditional HBV risk scores and was validated externally.
P.002
END-OF-THERAPY HBSAG, HBCRAG, AND HBV RNA PREDICT 8-YEAR OUTCOMES AFTER NUCLEOS(T)IDE ANALOGUE CESSATION IN CHRONIC HEPATITIS B
Meng-Ju Lin1, Tung-Hung Su2,3, Chun-Jen Liu2,3, Hung-Chih Yang2,3, Jyh-Ming Liou2, Tai-Chung Tseng2,3, Chen-Hua Liu2,3, Chun-Ming Hong2, Pei-Jer Chen2,3, Jia-Horng Kao2,3,4
1National Taiwan University Hospital, Taipei, Taiwan
2Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
3Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
4Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan
慢性 B 型肝炎病人在停用口服抗病毒藥 物時之 B 型肝炎表面抗原、核心相關抗 原及病毒核醣核酸可預測停藥後之八年 預後
林孟儒1 蘇東弘2,3 劉俊人2,3 楊宏志2,3 劉志銘2 曾岱宗2,3 劉振驊2,3 洪俊銘2 陳培哲2,3 高嘉宏2,3,4
1 國立臺灣大學醫學院附設醫院
2 國立臺灣大學醫學院附設醫院胃腸肝膽科
3 國立臺灣大學醫學院附設醫院肝炎研究中心
4 國立臺灣大學醫學院臨床醫學研究所
Background: Finite nucleos(t)ide analogue (NA) therapy may facilitate hepatitis B surface antigen (HBsAg) clearance in chronic hepatitis B (CHB) patients; however, virological relapse (VR, HBV DNA > 2000 IU/mL) and clinical relapse (CR, VR and ALT > 2-fold upper limit of normal) are common.
Aims: To investigate the role of quantitative HBsAg, hepatitis B core-related antigen (HBcrAg), and HBV RNA to predict post-treatment outcomes.
Methods: Non-cirrhotic CHB patients who discontinued NA therapies in a tertiary medical center were prospectively enrolled and followed at the 1st, 3rd, and every 3 months after treatment cessation. Serum HBsAg, HBcrAg, and HBV RNA levels at the end-of-therapy (EOT) were quantified and logarithmically transformed or categorized to
predict VR, CR, and HBsAg seroclearance.
Results: Among the 260 patients (39.6% initially HBeAg-positive) included, 74.6% fulfilled the Asian Pacific Association for the Study of the Liver (APASL) guidance for stopping NAs. Most patients received entecavir (60.0%) or tenofovir-based therapies (31.1%). The median treatment and follow-up duration were 37 months and 7.9 years. At EOT, HBV RNA levels were <5, 5–10, and ≥10 copies/mL in 39.2%, 25.0%, and 35.8% of patients, respectively. VR and CR occurred in 88.1% and 56.9%, while 8.8% achieved HBsAg seroclearance. Multivariable Cox regression analysis showed that age (adjusted HR [aHR]: 1.02), tenofovir use (aHR: 1.61), HBsAg (aHR: 1.26), and HBV RNA (aHR: 1.69) predicted VR, while age (aHR: 1.02), HBcrAg (aHR: 1.26), and HBV RNA (aHR: 1.34) predicted CR. HBV RNA ≥10 copies/mL increased VR and CR risk by 2.16-fold and 1.57-fold, respectively. Detectable HBV RNA (≥5 copies/mL) at EOT stratified HBsAg seroclearance risk, but a low HBsAg level (aHR: 0.23) was the only significant predictor.
Conclusions: EOT HBsAg, HBcrAg, and HBV RNA predict relapses after NA cessation. A low HBsAg level at EOT was the strongest predictor of subsequent HBsAg seroclearance.
P.003
HIGHER HBV DNA LEVELS ASSOCIATED WITH RISK OF LIVERRELATED DEATH IN HBEAGNEGATIVE, BUT NOT IN HBEAGPOSITIVE CHB PATIENTS
Hsuan-Chia Kuo1, Tai-Chung Tseng2,3,4, Chien-Jen Chen7, Chun-Jen Liu2,3,5, Tung-Hung Su2,3, Hung-Chih Yang2,5,6, Wan-Ting Yang3, Chen-Hua Liu2,3, Pei-Jer Chen2,3,4,5,6, Hwai-I Yang7,8,9,10,11, Jia-Horng Kao2,3,4,5
1Department of Internal Medicine, Division of Gastroenterology and Hepatology, National Taiwan University Hospital Yun-Lin Branch, Yunlin, Taiwan
2Department of Internal Medicine, Division of Gastroenterology and Hepatology, National Taiwan University Hospital, Taipei, Taiwan
3Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
4Department of Medical Research, National Taiwan University Hospital, Taipei, Taiwan
5Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
6Department of Microbiology, National Taiwan University College of Medicine, Taipei, Taiwan
7Genomics Research Center, Academia Sinica, Taipei, Taiwan
8Institute of Clinical Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
9Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
10Biomedical Translation Research Center, Academia Sinica, Taipei, Taiwan
11Doctoral Program of Clinical and Experimental Medicine, National Sun Yat-Sen University, Kaohsiung, Taiwan
2 國立臺灣大學醫學院附設醫院胃腸肝膽科
3 國立臺灣大學醫學院附設醫院肝炎研究中心
4 國立臺灣大學醫學院附設醫院醫學研究部
5 國立臺灣大學臨床醫學研究所
6 國立臺灣大學微生物學科暨研究所
7 中央研究院基因體研究中心
8 國立陽明交通大學臨床醫學研究所
9 高雄醫學大學醫學研究所
10 中央研究院生醫轉譯研究中心
11 國立中山大學臨床暨實驗醫學博士學位學程
Background: Chronic hepatitis B (CHB) is a major contributor to global liver-related mortality. Although serum HBV DNA is a key prognostic marker, the relationship between viral load and liverrelated death (LRD) may differ according to hepatitis B e antigen (HBeAg) status.
Aims: We aimed to investigate how baseline HBV DNA relates to LRD in HBeAg-negative and HBeAgpositive patients, respectively, in the REVEAL-HBV and ERADICATE-B cohorts.
Methods: We pooled data from 6,250 treatmentnaive, non-cirrhotic CHB patients in the REVEALHBV and ERADICATE-B cohorts and stratified them by baseline HBeAg status. Cox proportional hazards models were used to assess the association between HBV DNA (log₁₀ IU/mL categories) and LRD, adjusting for age, sex, and ALT.
Results: During a median follow-up of 26.5 years, 458 patients experienced LRD. Among 5,189 HBeAg-negative patients, LRD risk increased dosedependently with baseline HBV DNA (p-for-trend < 0.001) and appeared to plateau at ≥ 5 log₁₀ IU/mL. Patients with HBV DNA ≥ 7 log₁₀ IU/mL had roughly a seven-fold higher LRD risk than those with < 3 log₁₀ IU/mL (HR of 6.95 with 95% CI: 4.13-11.68). In contrast, among 1,061 HBeAg-positive patients with HBV DNA ≥ 4 log₁₀ IU/mL, LRD risk showed no clear gradient across HBV DNA categories. These patterns remained similar after multivariable adjustment.
Conclusions: Baseline HBV DNA is a strong, dosedependent predictor of LRD in HBeAg-negative CHB, whereas its prognostic value is markedly attenuated in HBeAg-positive disease. Accordingly, the role of HBV DNA in predicting LRD should be examined separately in CHB patients with different HBeAg status.
P.004
PHASE-SPECIFIC IMPACT OF HBV GENOTYPE ON HBSAG DECLINE KINETICS DURING AND AFTER NUCLEOS(T)IDE ANALOGUE THERAPY IN HBEAG-NEGATIVE CHB
Wen-Juei Jeng1,3, Chien-Hung Chen2,3, Yen-Chun Liu1,3, Rong-Nan Chien1,3
1Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
2Department of Gastroenterology and Hepatology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
3College of Medicine, Chang Gung University, Taoyuan, Taiwan
HBV 基因型對 HBeAg 陰性慢性 B 型肝 炎患者核 苷 (酸)類治療期間及停藥後 HBsAg 下降動力學之不同影響
鄭文睿1,3 陳建宏2,3 劉彥君1,3 簡榮南1,3
1 林口長庚紀念醫院胃腸肝膽科系
2 高雄長庚紀念醫院胃腸肝膽科系
3 長庚大學醫學院
Background: In HBeAg-negative chronic hepatitis B (CHB), serum HBsAg kinetics serve as a surrogate marker for functional cure. While host and viral factors influencing HBsAg decline during nucleos(t) ide analogue (Nuc) therapy have been identified, genotype-specific differences in HBsAg kinetics across treatment phases remain unclear.
Aims: We investigated whether HBV genotype (GT) differentially modulates HBsAg reduction during active Nuc treatment and after treatment cessation.
Methods: A total of 614 non-cirrhotic HBeAgnegative CHB patients [GT-B: 535 (87.1%), GT-C: 79 (12.9%)] treated with finite-course Entecavir (ETV) or Tenofovir Disoproxil Fumarate (TDF) according to APASL stopping criteria at Chang Gung Memorial Hospital (CGMH)-Linkou, Taiwan, were included. HBsAg levels were assessed at the start of treatment (SOT), end-of-treatment (EOT), and last followup. Two propensity score–matched (PSM) cohorts were constructed: PSM-cohort 1 (n = 158) for ontreatment analysis (matched by age, sex, treatmentnaïve status, Nuc agent, and SOT ALT, HBV DNA, and HBsAg levels); and PSM-cohort 2 (n = 132) for off-treatment analysis (matched by EOT age, sex,
Nuc agent, and baseline laboratory parameters). Generalized linear regression was used to identify predictors of HBsAg reduction. A multivariable linear mixed model (LMM) was employed to evaluate genotype-by-phase interaction. External validation was conducted in an independent cohort of 701 patients [GT-B: 541 (77.2%), GT-C: 160 (22.8%)] from CGMH-Kaohsiung.
Results: In PSM-cohort 1, patients with GT-B exhibited significantly greater on-treatment HBsAg reduction compared to those with GT-C (–0.21 vs. –0.05 log10 IU/mL/year, p < 0.001). In PSM-cohort 2, GT-C patients demonstrated a significantly faster offtreatment decline (–0.22 vs. –0.08 log10 IU/mL/year, p = 0.001) and a higher HBsAg loss rate (15.2% vs. 0%, p = 0.001). Similar trends were observed in the external validation cohort. In the full cohort, GT-B (β = 0.194, p < 0.0001), older age at SOT, and higher SOT ALT, HBV DNA, and HBsAg levels were independently associated with a greater on-treatment HBsAg decline. For off-treatment decline, GT-C (β = –0.1669, p = 0.0057), younger EOT age, and lower HBsAg at EOT were independent predictors. A LMM confirmed a significant genotype-by- phase interaction (p = 0.0144), indicating that HBV genotype differently modulates HBsAg reduction kinetics across treatment phases. Following Nuc cessation, GT-C patients exhibited accelerated HBsAg decline, whereas GT-B patients showed stable HBsAg levels.
Conclusions: HBV genotype modulates HBsAg reduction kinetics in a phase-specific manner. GT-B is associated with a greater decline during Nuc therapy, whereas GT-C shows enhanced off-Nuc HBsAg reduction and subsequent HBsAg loss. These findings underscore the need for genotype-specific immunologic studies to elucidate underlying mechanisms.
P.005
TOWARDS TRANSPARENT AI: RADIOMICS-DRIVEN DIAGNOSIS OF LIVER LESIONS ON NON-CONTRAST MRI
Sulagna Mohapatra1, Chun-Ying Wu1,2,3,4,5,6, Pushpanjali Gupta1,2,4, Yao-Chun Hsu7,8, Che-Lun Hung1,2, Yuan-Chia Chu9,10, Chia-Sheng Chu11,12
1Health Innovation Center, National Yang Ming Chiao Tung University, Taipei, Taiwan
2Institute of Biomedical Informatics, National Yang Ming Chiao Tung University, Taipei, Taiwan
3Microbiota Research Center, National Yang Ming Chiao Tung University, Taipei, Taiwan
4Institute of Public Health, National Yang Ming Chiao Tung University, Taipei, Taiwan
5Division of Translational Research, Taipei
Veterans General Hospital, Taipei, Taiwan
6Department of Public Health, China Medical University, Taichung, Taiwan
7Division of Gastroenterology and Hepatology, E-Da Hospital, Kaohsiung, Taiwan
8School of Medicine, I-Shou University, Kaohsiung, Taiwan
9Information Management Office and Big Data Center, Taipei Veterans General Hospital, Taipei, Taiwan
10Department of Information Management, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan
11Division of Gastroenterology and Hepatology, Taipei City Hospital Yang Ming Branch, Taipei, Taiwan
12Program of Interdisciplinary Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
Background: Manual identification of focal liver lesions (FLLs) on multi-sequence MRI is often timeconsuming and prone to errors due to inter-lesion heterogeneity and observer variability. To foster clinical adoption of artificial intelligence (AI) tools, model explainability is critical. Moreover, advancing diagnostic techniques based on non-contrast MRI is essential for reducing patient exposure to contrast agents and improving overall safety.
Aims: To develop an explainable, non-invasive radiomics-based system (RaNC-FLLD) that classifies
benign and hepatocellular carcinoma (HCC) lesions using non-contrast MRI, applicable to both cirrhotic and non-cirrhotic populations.
Methods: This retrospective study included 595 patients (246 cirrhotic, 349 non-cirrhotic) with MRI data acquired between January 2005 and December 2019. A total of 1,449 nodules (906 benign, 543 HCC), each larger than 0.3 cm, were analyzed. Fortyeight gray-level co-occurrence matrix (GLCM)-based radiomics features were extracted from T2-weighted and FIESTA non-contrast MRI sequences. Feature relevance was evaluated using SHapley Additive exPlanations (SHAP), identifying 24 key predictors. The selected CatBoost classifier, optimized for performance, was compared against eight other advanced machine learning models.
Results: Combining T2 and FIESTA sequences yielded an AUC of 0.97 in nodule-wise analysis, outperforming T2 (0.95) and FIESTA (0.94) individually. While contrast-enhanced arterial-phase MRI achieved perfect specificity and precision (1.00), it suffered from limited sensitivity (0.72). In contrast, the Rad-FLLD system using T2+FIESTA achieved high and balanced metrics: sensitivity (0.98), specificity (0.96), and precision (0.94). In size-based subgroup analysis, for lesions ≤1.5 cm, true positive rates (TPRs) were 0.69 (benign) and 0.91 (HCC) in cirrhotic patients, and 0.96 and 1.00, respectively, in noncirrhotic patients. For lesions >1.5 cm, the model achieved 100% accuracy in both groups.
Conclusions: The proposed RaNC-FLLD system, leveraging explainable AI and non-contrast MRI radiomics from T2 and FIESTA sequences, accurately distinguishes benign from HCC lesions larger than 0.3 cm. This approach enhances diagnostic accuracy, reduces reliance on contrast agents, and streamlines clinical workflows.
P.006
ANGIOPOIETIN-LIKE
4
AS A PREDICTIVE BIOMARKER FOR IMMUNOTHERAPY RESPONSE IN HEPATOCELLULAR CARCINOMA
Huang-Pin Chen1, Meng-Wei Lin1, Hung-Tsung Wu2, Hsin-Yu Kuo1
1Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan
2Department of Internal Medicine, School of Medicine, College of Medicine, National Cheng Kung University, Tainan, Taiwan
血清血管生成素樣蛋白
胞癌免疫治療反應的預測性生物標誌
1 國立成功大學醫學院附設醫院內科部
2 國立成功大學醫學系內科學科
Background: Hepatocellular carcinoma (HCC) ranks as one of the most prevalent cancer globally and the also the leading cause of cancer-related mortality. In recent years, immune checkpoint inhibitors have demonstrated encouraging outcomes in the management of advanced HCC and are recommended as a first-line option for systemic therapy in these patients. However, there is still no robust, clinically validated biomarker to predict the treatment responses for HCC patients receiving immunotherapy combinations. Although it was known that angiopoietin-like protein 4 (ANGPTL4) is associated with HCC stage, the role of ANGPLT4 in predicting treatment responses of immune therapy were still unknown.
Aims: To investigate if serum ANGPTL4 concentrations could serve as a novel biomarker for predicting treatment response of immune therapy in patients with advanced HCC.
Methods: A total of 70 subjects with HCC receiving immunotherapy in National Cheng Kung University Hospital from 2019 to 2025 and treated with at least one dose of immune checkpoint inhibitor (ICI) therapy, including pembrolizumab, nivolumab, or atezolizumab plus bevacizumab was retrospectively enrolled in the present study. We evaluated the radiologic responses of the tumors by modified Response Evaluation Criteria in Solid tumors
(mRECIST). Serum levels of angiopoietin-like protein 4 were quantified using a commercially available enzyme-linked immunosorbent assay (ELISA).
Results: The baseline characteristics, including age, sex, body weight, Barcelona Clinic Liver Cancer classification (BCLC) stage and Child–Pugh class showed no significant differences between responder (N = 34) and non-responder groups (N = 36). The mean baseline plasma concentration of ANGPLT4 was significantly lower in the responder group, as compared with non-responder group (83.23 ± 26.30 ng/ml vs. 106.64 ± 47.74 ng/ml; p = 0.013). According to the multivariate logistic regression analysis, we found that treatment response was independently associated with plasma concentration of ANGPLT4 after adjustment for the confounding factors such as age, sex, body weight, performance status and BCLC stage.
Conclusions: Our study demonstrates that lower baseline serum ANGPTL4 concentrations are independently associated with a favorable treatment response in patients with advanced HCC receiving immunotherapy. These findings suggest that serum ANGPTL4 may represent as a predictive biomarker to support precision medicine approaches and inform individualized treatment strategies for HCC.
P.007
INCIDENT TYPE 2
PREDIABETES
Yu-Ping Chang1, Ji-Yuh Lee2, Chi-Yi Chen3, Wei-Yu Kao4, Chih-Lin Lin5, Sheng-Shun Yang6, Yu-Lueng Shih7, Cheng-Yuan Peng8, Fu-Jen Lee9, Ming-Chang Tsai10, Shang-Chin Huang11, Tung-Hung Su12,13, Tai-Chung Tseng12,13, Chun-Jen Liu12,13, Pei-Jer Chen12,13, Jia-Horng Kao12,13, Chen-Hua Liu12,13
1Department of Internal Medicine, National Taiwan University Biomedical Park Hospital, Hsinchu, Taiwan
2Department of Internal Medicine, National Taiwan University Hospital, Yunlin, Taiwan
3Division of Gastroenterology and Hepatology, Department of Internal Medicine, Ditmanson Medical Foundation Chiayi Christian Hospital, Chiayi, Taiwan
4Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taipei
Medical University Hospital, Taipei, Taiwan
5Department of Gastroenterology, Taipei City Hospital, Taipei, Taiwan
6Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung
Veterans General Hospital, Taichung, Taiwan
7Division of Gastroenterology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
8Center for Digestive Medicine, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan
9Division of Gastroenterology and Hepatology, Department of Internal Medicine, Fu Jen
Catholic University Hospital, New Taipei City, Taiwan
10Division of Gastroenterology and Hepatology, Department of Internal Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan
11Department of Internal Medicine, National Taiwan University Hospital Bei-Hu Branch, Taipei, Taiwan
12Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
13Hepatitis Research Center, National Taiwan
University Hospital, Taipei, Taiwan
C 型肝炎接受直接作用型抗病毒藥物治療 後達到治癒的患者,其第二型糖尿病與 糖尿病前期之發生風險
張鈺屏1 李基裕2 陳啟益3 高偉育4 林志陵5 楊勝舜6 施宇隆7 彭成元8 李輔仁9 蔡明璋10 黃上秦11 蘇東弘12,13 曾岱宗12,13 劉俊人12,13 陳培哲12,13 高嘉宏12,13 劉振驊12,13
1 新竹臺大分院生醫醫院竹北院區內科部
2 台大醫院雲林分院斗六院區內科部
3 嘉義基督教醫院消化內科
4 臺北醫學大學附設醫院內消化內科
5 臺北市立聯合醫院消化內科
6 臺中榮民總醫院胃腸肝膽科
7 三軍總醫院消化內科
8 中國醫藥大學附設醫院消化內科
9 天主教輔仁大學附設醫院肝膽腸胃科
10 中山醫學大學附設醫院肝膽腸胃科
11 國立臺灣大學醫學院附設醫院北護分院內科部
12 國立臺灣大學醫學院附設醫院內科部
13 國立臺灣大學醫學院附設醫院肝炎研究中心
Background: Data regarding the risk of incident type 2 diabetes (T2D) and prediabetes among patients with hepatitis C virus (HCV) achieving direct-acting antivirals (DAAs)-induced sustained virologic response (SVR12) remains limited.
Aims: Investigate the glycemic status, including the incidence of type 2 diabetes and prediabetes, among patients with chronic hepatitis C virus infection who have achieved SVR12 following treatment with DAA.
Methods: A total of 1079 patients, including 589 with normoglycemia and 490 with prediabetes, who underwent biannual fasting glucose and glycosylated haemoglobin (HbA1c) assessment for a median post-SVR12 follow-up of 5.5 years, were enrolled. We reported the crude (cIRs) and age-standardised incidence rates (ASIRs) of T2D and prediabetes. Factors associated with incident T2D and prediabetes were assessed using the Cox proportional hazards models.
Results: The cIRs of T2D and prediabetes were 1.18 and 8.99 per 100 person-years of follow-up (PYFU), respectively. Additionally, the ASIRs of T2D and prediabetes were 1.09 (95% CI: 0.76–1.53) and 8.47 (95% CI: 7.23–9.90) per 100 PYFU. Prediabetes (ad- justed hazard ratio [aHR]: 4.71; 95% confidence interval (CI): 2.55–8.70, p < 0.001), body mass index
(BMI) per kg/m² increase (aHR: 1.17; 95% CI: 1.09–1.26, p < 0.001) and liver stiffness measurement (LSM) per kPa increase (aHR: 1.05; 95% CI: 1.02–1.09, p = 0.001) were associated with a higher risk of incident T2D. Age per year increase (aHR: 1.02; 95% CI: 1.01–1.03, p < 0.001) was associated with a higher risk of incident prediabetes.
Conclusions: The incidence rates of T2D and prediabetes remain substantial among patients after HCV eradication. Lifestyle modification, drug therapy and regular monitoring of glycemic status are crucial for patients at risk of developing T2D and pre- diabetes following HCV clearance.
P.008
HEPATOTOXIC-LIKE
CD38+HLADR+PD1+CD8+ T CELLS
DEFINE A FUNCTIONALLY DISTINCT SUBSET ASSOCIATED WITH HBSAG REDUCTION AND HBV-SPECIFIC IMMUNITY IN CHB
Hsiang-Wei Huang2, Wen-Juei Jeng1,2, Chia-Wei Lin2, Yen-Chun Liu1,2, Jian-He Fan2, Thi Kim Duyen Nguyen2, Wei-Ting Ku2, Cheng-Heng Wu2, Chun-Yen Lin1,2
1Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
2College of Medicine, Chang Gung University, Taoyuan, Taiwan
類肝毒性 CD38 + HLA-DR + PD1 + CD8 + T 細
胞:慢性 B 型肝炎中與 HBsAg 降低及
HBV 特異性免疫相關之功能性亞群
黃祥瑋2 鄭文睿1,2 林家緯2 劉彥君1,2 方健合2 阮金緣2
古唯鼎2 吳承衡2 林俊彥1,2
1 林口長庚紀念醫院胃腸肝膽科系
2 長庚大學醫學院
Background: Chronic hepatitis B (CHB) is characterized dysfunctional HBV-specific CD8+ T cell responses. Recent studies suggest CD38+HLADR+CD8+ T cells with hepatotoxic, innatelike features may contribute to liver inflammation in chronic hepatitis C. However, their relationship with HBV-specific immunity remains unclear.
Aims: This study aimed to characterize these T cell subsets and evaluate their association with HBVspecific immune response in CHB patients.
Methods: A total of 43 CHB patients with ALT ≥2× the upper limit of normal (ULN) were prospectively enrolled at a treatment-free timepoint. Peripheral CD8+ T cells were analyzed using a single-cell RNA sequencing (scRNAseq) approach. Flow cytometry was subsequently performed to validate cell phenotypes. HBV-specific T cell responses (Core, polymerase, X, and S peptides) were evaluated by IFN-γ ELISPOT. Associations between T cell subsets, HBV-specific immunity, and on-treatment HBsAg reduction velocity were analyzed by linear regression analysis.
Results: A cluster of peripheral CD8+ T cells, recognized as CD38+HLADR+CD8+ T cells with a
hepatotoxic transcriptome profile (Gehring et al., J Clin Invest, 2023) was identified by a scRNAseq approach using unsupervised clustering. This cluster showed a distinct transcriptional signature enriched in NK receptor pathways and cytokine-responsive modules, and exhibited significantly higher innatelike scores compared to the other CD8+ T cell clusters. This CD38+HLADR+CD8+ T cell cluster was further subclustered into PD1+ and PD1- subsets. In CHB patients with active hepatitis before treatment, the frequency of PD1+CD38+HLADR+CD8+ T cells was significantly associated with the velocity of ontreatment HBsAg reduction (estimate: 0.626, p < 0.01). Furthermore, this subset was significantly correlated with HBV Core- and S-specific T cell responses as measured by ELISPOT (estimates: 7.511, p < 0.01; 3.812, p < 0.05, respectively). These associations were not observed in the PD1-CD38+HLADR+CD8+ T cell subset, suggesting functional heterogeneity within this hepatotoxic CD8+ T cell cluster and a potential link to the rejuvenation of HBV-specific CD8+ T cells. Conclusions: PD1+CD38+HLADR+CD8+ T cells display hepatotoxic transcriptomic features. The frequency of this subset is significantly associated with HBV Core- and S-specific T cell responses and subsequent on-treatment HBsAg reduction. Therefore, this subset may be closely related to the recovery of HBV-specific CD8+ T cell responses and contribute to HBsAg seroclearance.
P.009
ASSOCIATION OF HBV VIRAL MARKERS AND HCC RISK IN HBVRELATED CIRRHOSIS PATIENTS UNDER LONG-TERM ENTECAVIR THERAPY
Hung-Husan Pan1, Tung-Hung Su1, Tsung-Hui Hu2, Wan-Long Chuang3, Wei-Wen Su4, Chun-Che Lin5, Cheng-Yuan Peng6, Chia-Chi Wang7, Yao-Chun Hsu8, Yi-Wen Huang9, Kuo-Chih Tseng10, Chih-Lin Lin11, Sheng-Shun Yang12, Fat-Moon Suk13, Shih-Jer Hsu1, Tsung-Ming Chen14, Ming-Jong Bair15, Cheng-Kuan Lin16, Tai-Chung Tseng1, Jia-Horng Kao1
1Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Division of Hepatogastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan
3Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
4Department of Gastroenterology and Hepatology, Changhua Christian Hospital, Changhua, Taiwan
5Division of Gastroenterology, Department of Internal Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan
6Division of Hepatogastroenterology, Department of Internal Medicine, China
Medical University Hospital, Taichung, Taiwan
7Division of Gastroenterology, Department of Internal Medicine, Taipei Tzuchi Hospital, the Buddhist Tzuchi Medical Foundation, Taipei, Taiwan
8Division of Gastroenterology and Hepatology, E-Da Hospital, Kaohsiung, Taiwan
9Liver Center, Cathay General Hospital Medical Center, Taipei, Taiwan
10Department of Hepatology, Buddhist Tzu Chi General Hospital, Da-Lin Branch, Chiayi, Taiwan
11Department of Gastroenterology, Ren-Ai Branch, Taipei City Hospital, Taipei, Taiwan
12Division of Gastroenterology, Department of Internal Medicine, Taichung Veterans General
Hospital, Taichung, Taiwan
13Division of Gastroenterology, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan
14Division of Hepato-Gastroenterology, Department of Internal Medicine, and Department of Medical Research, Tungs’ Taichung MetroHarbor Hospital, Taichung, Taiwan
15Division of Gastroenterology and Hepatology, Department of Internal Medicine, Mackay Memorial Hospital, Taitung, Taiwan
16Department of Internal Medicine, Far Eastern Memorial Hospital, Taipei, Taiwan
B 型肝炎合併肝硬化病患接受長期 Entecavir 治療下 B 型肝炎病毒標記與肝 癌風險之相關性
潘弘軒1 蘇東弘1 胡琮輝2 莊萬龍3 蘇維文4 林俊哲5 彭成元6 王嘉齊7 許耀峻8 黃奕文9 曾國枝10 林志陵11 楊勝舜12 粟發滿13 徐士哲1 陳宗勉14 白明忠15 林政寬16 曾岱宗1 高嘉宏1
1 國立臺灣大學醫學院附設醫院內科部
2 高雄長庚紀念醫院胃腸肝膽科暨長庚大學醫學院
3 高雄醫學大學附設中和紀念醫院內科部
4 彰化基督教醫院胃腸肝膽科
5 中山醫學大學附設醫院胃腸肝膽科
6 中國醫藥大學附設醫院胃腸肝膽科
7 台北慈濟醫院胃腸肝膽科
8 義大醫院胃腸肝膽科
9 國泰綜合醫院肝臟中心
10 大林慈濟醫院肝膽腸胃科
11 臺北市立聯合醫院仁愛院區肝膽胃腸科
12 臺中榮民總醫院胃腸肝膽科
13 臺北市立萬芳醫院胃腸肝膽科
14 童綜合醫院肝膽腸胃科暨醫學研究部
15 台東馬偕紀念醫院胃腸肝膽科
16 亞東紀念醫院內科部
Background: The risk of hepatocellular carcinoma (HCC) is reduced but not eliminated after nucleos(t) ide analogue (NA) therapy in chronic hepatitis B (CHB) patients.
Aims: We aimed to investigate the role of HBV RNA, hepatitis B core-related antigen (HBcrAg), and quantitative hepatitis B surface antigen (qHBsAg) in predicting HCC in cirrhotic CHB patients receiving long-term entecavir therapy.
Methods: This retrospective cohort study included patients with CHB-related cirrhosis who had been under entecavir for a median duration of 6.2 years from medical centers in Taiwan. Serum levels of HBV RNA, HBcrAg, and qHBsAg were quantified by automated assays. Correlation among viral markers was assessed using Pearson correlation coefficients. Multivariable Cox proportional hazards regression models were used to identify predictors for HCC development and sustained detectability of HBV RNA.
Results: Overall, 451 CHB-related cirrhosis patients were included. The mean age was 60, the median HBV RNA level was 0.7 (log10 copies/ml), the median HBcrAg level was 3.2 (log10 U/ml), and the median qHBsAg level was 2.4 (log10 IU/mL). After a median follow-up of 3.3 years, 55 patients developed HCC. There was a positive correlation between HBV RNA and HBcrAg (r = 0.4515). Among patients with undetectable HBV DNA, 55.3% still had detectable HBV RNA. After adjustment for confounding factors, higher gamma-glutamyl transferase (γ-GT) levels (hazard ratio [HR], 1.01; 95% confidence interval [CI], 1.00–1.01), positive HBeAg (HR: 2.29; 95% CI: 1.16–4.54), detectable HBV DNA (HR: 2.41; 95% CI: 1.11–5.21), HBcrAg >3.23 U/ml (HR: 1.75; 95% CI: 1.10–2.77) and shorter ETV treatment duration (HR: 0.88; 95% CI: 0.79–0.97) significantly predicted sustained HBV RNA detectability. In multivariate analysis, age (HR: 1.04, 95% CI: 1.01–1.07), FIB-4 (HR: 1.11, 95% CI: 1.02–1.22) and AFP levels (HR: 1.01, 95% CI: 1.00–1.01) were predictive of the development of HCC, while serum HBV RNA, HBcrAg, and qHBsAg were not.
Conclusions: Among CHB-related cirrhotic patients receiving 6-year entecavir therapy, higher γ-GT and HBcrAg levels, positive HBeAg, detectable HBV DNA, and shorter duration of ETV treatment were associated with sustained HBV RNA detectability. Older age, higher FIB-4 index, and elevated AFP levels were associated with increased risk of HCC development, while serum levels of HBV RNA, HBcrAg, and qHBsAg were not predictive of HCC.
P.010
THE EFFECT OF SHARE DECISION MAKING IN THE TREATMENT OPTIONS OF PATIENTS WITH CHRONIC HEPATITIS B AFTER DUE OF NATIONAL HEALTH INSURANCE
Ai-Lien Liao1,2, Li-Ya Tsai2, Ming-Jong Bair1,2, Chun-Han Cheng1, Huan-Lin Chen1
1Department of Hepatobiliary Gastroenterology, Taitung Mackay Memorial Hospital, Taitung, Taiwan
2Asia University Nursing Master Program (Taitung Class)
以醫病共享決策方案介入慢性 B 型肝炎 患者健保藥物給付療程到期後的治療選 擇之成效探討
廖愛蓮1,2 蔡麗雅2 白明忠1,2 鄭羣翰1 陳煥霖1
1 台東馬偕紀念醫院胃腸肝膽專科 2 亞洲大學護理學系碩士在職專班(台東班)
Background: For patients with hepatitis B who need to stop taking antiviral drugs after the expiration of the health insurance treatment course, we analyze and understand the advantages and disadvantages of stopping and taking drugs at their own expense after the expiration of antiviral drugs, and make decisions after explaining the pros and cons, respect, support and affirm their decision-making choices, evaluate the effectiveness of the intervention of the doctorpatient sharing, and track the indicators of hepatitis recurrence.
Aims: (1) To explore the treatment options (stopping or taking drugs at your own expense) of chronic hepatitis B patients after the expiration of the health insurance drug payment course after SDM intervention. (2) To explore the SDM effectiveness evaluation of chronic hepatitis B patients after the expiration of the health insurance drug payment course. (3) To understand the correlation between SDM satisfaction and hepatitis recurrence of different medication options for chronic hepatitis B patients after the expiration of the health insurance drug payment course.
Methods: This study is a quasi-experimental study with a single-group before-after control study design for convenient sampling. The subjects were 70 patients in the outpatient department of the hepatobiliary and gastroenterology department of a regional teaching hospital in the eastern region
whose oral antiviral drug treatment course for chronic hepatitis B had expired. After SDM intervention, they were divided into a discontinuation group and a self-paid medication group according to their actual treatment choices. Relevant statistical analysis was performed to explore the correlation and predictive ability of each variable.
Results: Choices after expiration of hepatitis B drugs: 60% (N = 42) chose to stop taking the drugs, and 40% (N=28) chose to continue taking the drugs at their own expense; Hepatitis recurrence: 48 people (70%) did not have it, and 22 people (30%) had recurrence, and the average overall SDM satisfaction was 4.45 points (out of 5 points); Treatment choice and hepatitis recurrence The hepatitis recurrence rate of patients who took self-paid drugs was significantly lower than that of patients who stopped taking the drugs (p < 0.01). Treatment choice was significantly negatively correlated with hepatitis recurrence (r = -0.501, p = .000), indicating that continuous medication can effectively reduce the risk of recurrence. In addition, the history of hepatitis B medication (number of months) was a significant variable affecting treatment choice (p = .002), and the longer the medication time, the more likely the patient was to choose self-paid treatment; economic status was also a significant predictor (p = .019). Overall, the degree of SDM participation was related to treatment selection and relapse results, but did not affect the overall satisfaction of patients with the SDM process (average 4.45 points, p = .550).
Conclusions: he results of this study confirm the feasibility and clinical value of SDM in the treatment decision-making of chronic hepatitis B patients. The treatment choice was significantly associated with the relapse situation, indicating that the treatment choice has a key impact on the subsequent disease control; the longer the medication time, the more inclined to choose self-paid continuous treatment, and the long-term medication experience may enhance the confidence and recognition of continuous treatment. The degree of SDM participation and satisfaction indicate that the treatment choice itself does not affect the patient’s overall evaluation of the SDM process. In the decision-making situation of the expiration of drug payment, strengthen patient informed participation and improve the continuity and effectiveness of subsequent treatment; through the SDM process, it can effectively improve the patient’s participation and cognition of their own treatment choices, and help them make more appropriate choices based on their personal health status and economic considerations.
P.011
THE CLINICAL EFFICACY OF TENOFOVIR ALAFENAMIDE RETREATMENT IN CHRONIC HEPATITIS B PATIENTS WITH CLINICAL RELAPSE AFTER DISCONTINUATION OF ORAL ANTIVIRAL THERAPY
Tung-Hung Su1, Yao-Chun Hsu2, Yu-Jen Fang3, Chih-Lin Lin4, Chia-Chi Wang5, Kuo-Chih Tseng6, Chi-Yi Chen7, Jia-Horng Kao1
1Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Division of Gastroenterology and Hepatology, E-Da Hospital, Kaohsiung, Taiwan
3Department of Internal Medicine, National Taiwan University Hospital, Yun-Lin Branch, Yun-Lin, Taiwan
4Department of Gastroenterology, Ren-Ai Branch, Taipei City Hospital, Taipei, Taiwan
5Division of Gastroenterology, Department of Internal Medicine, Taipei Tzuchi Hospital, the Buddhist Tzuchi Medical Foundation, Taipei, Taiwan
6Department of Hepatology, Buddhist Tzu Chi General Hospital, Da-Lin Branch, Chiayi, Taiwan
7Department of Internal Medicine, Chia-Yi Christian Hospital, Chiayi, Taiwan
慢性 B 型肝炎患者口服抗病毒治療停 藥後發生臨床復發後使用 Tenofovir Alafenamide 再次治療療效評估
蘇東弘1 許耀峻2 方佑仁3 林志陵4 王嘉齊5 曾國枝6 陳啟益7 高嘉宏1
1 台大醫院胃腸肝膽科
2 義大醫院胃腸肝膽科
3 台大醫院雲林分院胃腸肝膽科
4 臺北市立聯合醫院仁愛院區胃腸科
5 台北慈濟醫院胃腸肝膽科
6 佛教大林慈濟醫院胃腸肝膽科
7 嘉義基督教醫院胃腸肝膽科
Background: Retreatment is frequent in patients with chronic hepatitis B (CHB) who developed clinical relapse after cessation of oral antiviral therapy. Whether retreatment using the original regimen or switching to tenofovir alafenamide (TAF) would be beneficial remains unclear.
Aims: We aimed to investigate the clinical
effectiveness of switching to TAF after clinical relapse.
Methods: This multicenter study enrolled CHB patients who experienced clinical relapse after discontinuing entecavir or tenofovir disoproxil fumarate [TDF] and switched the regimen to TAF for 48 weeks of retreatment. The primary endpoint was the rate of virological remission (HBV DNA <20 IU/ mL), and the secondary endpoints were the rate of ALT normalization (<41 U/L), the change of HBsAg level, renal function, body weight and lipid profiles.
Results: The CHANGE (Chronic Hepatitis b patients switch to tAf after discontinuation of Nucleoside analoGuE) study (NCT04496882) included 48 patients previously treated with entecavir (n = 27) or TDF (n = 21) for a median duration of 3.2 years. At TAF retreatment, the median age was 48 years, 12.5% was HBeAg positive and HBV DNA was 6.5 log10 IU/mL. The virological remission rate was 58%, 77%, and 77% at 24, 36, and 48 weeks of therapy. The ALT normalization rate was 77%, 90%, and 85%, respectively. After 48-week TAF therapy, both their median HBsAg (3.3 to 2.7 log10 IU/mL, P < 0.001) and HBcrAg (6.1 to 3.2 log10 IU/mL, P < 0.001) declined significantly. Four of 6 (67%) HBeAg-positive patients cleared their HBeAg. There was a significant reduction of liver fibrosis by M2BPGi level (0.88 to 0.63 C.O.I., P < 0.001). There was a significantly increase of serum creatinine (0.85 to 0.89 mg/dL, P = 0.022), T-CHO (179 to 187 mg/dL, P = 0.019), TG (81 to 94 mg/dL, P = 0.016), and LDL (105 to 118 mg/ dL, P < 0.001), and a significantly reduction of HDL (59 to 55 mg/dL, P = 0.049), while their body weight remained stable. The change of T-CHO, TG, and HDL after 48-week TAF therapy were insignificant if patients switched from TDF to TAF. The compliance was >90% and no significant adverse events were reported.
Conclusions: TAF re-treatment after off-therapy relapse is safe and effective in viral suppression, ALT normalization and liver fibrosis improvement. The renal function and lipid profiles should continue to be monitored.
P.012
COMPARATIVE LONG-TERM OFFTREATMENT OUTCOMES IN HBEAGNEGATIVE CHRONIC HEPATITIS
B: PROPHYLACTIC THERAPY IN CANCER PATIENTS VS. FINITE THERAPY IN NON-CANCER PATIENTS
Hsin-Che Lin1, Yen-Chun Liu1 2, Wei Teng1, Chao-Wei Hsu1 2, Rachel Wen-Juei Jeng1, Rong-Nan Chien1 2
1Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan
2College of Medicine, Chang Gung University, Taoyuan, Taiwan
HBeAg 陰性慢性 B 型肝炎停藥後長期結 果比較:癌症患者預防性治療 vs.
林歆哲1 劉彥君1 2 滕威1 許朝偉1 2 鄭文睿1 簡榮南1 2
1 林口長庚紀念醫院胃腸肝膽科系
2 長庚大學醫學院
Background: Guidelines recommend finite prophylactic nucleos(t)ide analogue (NUC) therapy for cancer patients with chronic hepatitis B (CHB) receiving chemotherapy. However, the long-term outcomes after stopping Nuc therapy, such as clinical relapse or changes in HBsAg kinetics, and their relationship with immunosuppressive agents or cytotoxic drugs, remain unclear.
Aims: We aim to investigate the off-NUC clinical course focusing on relapse and HBsAg loss between prophylactic (cancer) and non-cancer CHB patients after NUC therapy.
Methods: Non-cirrhotic, HBeAg-negative CHB patients with cancer who discontinued prophylactic NUC 6 months after the end of chemotherapy (C/TCHB cohort) were compared to non-cancer HBeAgnegative CHB patients treated with finite Nuc per APASL guidelines (CGMH off-Nuc cohort). Clinical relapse (CR) was defined as HBV DNA ≥2000 IU/ mL with ALT >2 times the upper limit of normal (ULN). Hepatic decompensation (HD) was defined as total bilirubin ≥2 mg/dL and INR ≥1.5, with or without ascites or encephalopathy. Multivariate Cox regression was performed to evaluate the hazard of off-Nuc CR in the C/T-CHB cohort. One to one
propensity score matching (PSM) was performed based on age, sex, NUC agent, pretherapy HBV DNA, and ALT and HBsAg at end of treatment (EOT). Kaplan-Meier and log-rank tests were used to compare outcomes.
Results: Among 126 C/T CHB and 1815 CGMH offNuc patients, the C/T-CHB group had fewer males (46% vs. 79%; P < 0.001), and lower pretreatment HBV DNA (3.1 vs. 6.2 log10 IU/mL; P < 0.001), lower ALT (25 vs. 160 U/L; P < 0.001), and shorter treatment duration (42 vs. 156 weeks, P < 0.001). Multivariate Cox regression showed a lower risk of CR in the C/T CHB group [adjusted HR: 0.38; 95% CI: 0.22–0.66, P < 0.001], after adjusting for age, sex, prior treatment, Nuc agent, pretherapy HBV DNA, treatment duration and EOT HBsAg. In the matched cohort (n = 99 per group, median follow-up: 3.7 years), the 5-year cumulative CR incidence was lower in the C/T-CHB group (29% vs. 71%, p < 0.01). Relapse severity was also lower (ALT ≥10x ULN: 5% vs. 23%, P < 0.01; ALT ≥1000 IU/mL: 0 vs. 8%, p = 0.01). HD incidence was low in both groups (5-year: 3.3% vs.4.7%, P = 0.71).
HBsAg loss was four times more frequent in the C/TCHB group (5 years: 6.7% vs. 1.8%, p = 0.097), though not statistically significant.
Conclusions: HBeAg-negative non-cirrhotic CHB patients with cancer had a lower incidence and severity of clinical relapse after stopping NUC therapy than non-cancer patients. A trend toward higher HBsAg loss in the cancer group warrants further immunological investigation.
P.013
PREVENTING HEPATITIS B REACTIVATION IN CANCER PATIENTS ON CHEMOTHERAPY: IMPACT OF AN ELECTRONIC REMINDER SYSTEM
I-Ling Liu, Wan-Yu Lin, Ya-Huei Zeng, Hsu-Heng Yen, Yang-Yuan Chen, Pei-Yuan Su Division of Gastroenterology and Hepatology, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan
電子提醒系統於預防化療癌症患者 B 型 肝炎再活化之成效
林婉瑜
Background: According to Taiwan Centers for Disease Control, HBV vaccination program was launched to reduce the incidence of acute HBV infection to 0.5% per 100,000 in 2016. Survey of hepatitis B virus infection status showed the overall seropositivity rates for HBsAg and anti-HBc in Taiwan were 4.05% and 21.3%, respectively after 35 years of vaccination (Chang, KC et al, 2024). Hepatitis B surface antigen (HBsAg) positive in cancer patients receiving chemotherapy has been defined as the high risk (>10%) population of hepatitis B reactivation that is a life-threatening complication, and prophylaxis is definitely needed in clinical practice (APASL 2021). The prophylaxis of Hepatitis B becomes the first important step for the safety and quality of care. Nucleos(t)ide analogs (NUCs) are the main treatment for CHB and reimbursed by the Taiwan national health insurance since 2020, but the enrollment rate could not be completed in the practice. 10% (3/30) of decompensated CHB patients combined with cancer who were undergoing chemotherapy in our hospital from 2018 to 2019.
Aims: The purpose of this report is to see the efficacy of this electronic reminder system in a medical center.
Methods: The target population is our outpatients who are HBsAg or Anti-HBc seropositive undergoing chemotherapy and have not received prophylactic antiviral therapy. Using an electronic reminder system to improve enrollment rate for this specific population. The name list of potential high risk patients will be updated immediately in our case management system. We set up this electronic reminder system to see the efficacy of enrollment rate,
and have started it from 2021. The target population will receive a referral sheet from outpatient nurse, and the doctor will get a reminding message for their outpatients’ referral during clinical practice.
Results: The annual percentage of enrollment rate before and after using reminder system for outpatients showed a significant increase. The enrollment rate was under 50% in 2019 and 2020. We can see the efficacy from the data that most enrollment apparently rely on electronic reminder system from 2021 to 2024 (Figure 1). Furthermore, the enrollment rate for high risk of HBsAg seropositive cancer patients with chemotherapy were over 90% in 2021, and optimized to the target of 100% in both 2023 and 2024 (Figure 2). The percentage of decompensated CHB patients combined with cancer who were undergoing chemotherapy remained 0% (0/18) in our hospital from 2023 to 2024.
Conclusions: 77.5% to 88.8% of the enrollment were based on using this electronic reminder system between 2021 and 2024. Prophylactic antivirals for HBsAg seropositive high risk cancer patients undergoing chemotherapy were achieved over 90% after 2021, and had been completed 100% from 2023 to 2024. The data showed the reminder system and referral process could be helpful in preventing the severe adverse events and to increase awareness of this potentially critical complication in the clinical care.
P.014
RISK FACTORS FOR HEPATIC DECOMPENSATION FOLLOWING HEPATITIS B VIRUS REACTIVATION IN RESOLVED HEPATITIS B PATIENTS UNDERGOING IMMUNOSUPPRESSIVE THERAPY
Chien-Ming Chen, Pei-Yuan Su, Yang-Yuan Chen
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan
B 型肝炎病患接受免疫抑制治療後再活化 之肝功能失代償風險因子分析
Background: Hepatitis B virus (HBV) reactivation is a clinically significant complication in patients with resolved HBV infection undergoing immunosuppressive therapy. While reactivation is frequently asymptomatic, a notable proportion of patients may progress to hepatic decompensation, leading to increased morbidity and adverse clinical outcomes. Despite its importance, the determinants of hepatic decompensation following HBV reactivation have not been clearly established in resolved hepatitis B patients.
Aims: To investigate the clinical characteristics and identify potential risk factors for hepatic decompensation in patients with resolved HBV infection who developed HBV reactivation during or after immunosuppressive therapy.
Methods: We retrospectively analyzed 23 cancer patients with resolved HBV infection—defined as HBsAg-negative and anti-HBc-positive with normal baseline alanine aminotransferase (ALT) levels— who experienced HBV reactivation during or after receiving immunosuppressive therapy at Changhua Christian Hospital. None of the patients received prophylactic antiviral treatment. HBV reactivation was defined as HBsAg seroconversion accompanied by a ≥1 log increase in HBV DNA levels. Patients were categorized into two groups based on the presence (n=10) or absence (n=13) of hepatic decompensation, which was defined by the occurrence of hepatic encephalopathy, coagulopathy INR of ≥1.5, jaundice, or ascites. Clinical parameters compared between the two groups included age, sex, cancer type, liver cirrhosis, hypertension, type 2 diabetes
mellitus, immunosuppressive regimen, use of rituximab-based regimens, nucleos(t)ide analogue (NUC) treatment after reactivation included tenofovir alafenamide (TAF), tenofovir disoproxil fumarate (TDF), entecavir (ETV) and Telbivudine, duration of immunosuppressive therapy, history of bone marrow transplantation, and anti-HBs status. Immunosuppressive regimens were further stratified by HBV reactivation risk into four categories: rituximab-based regimens, anthracyclinecontaining regimens, immunosuppressive therapy (e.g., tyrosine kinase inhibitors), and other chemotherapy regimens.
Results: Of the 23 patients, 10 (43.5%) developed hepatic decompensation. The presence of underlying liver cirrhosis was the only factor significantly associated with decompensation (40% vs. 0%, p = 0.024). Although older age (p = 0.098) and rituximab-based therapy (p = 0.09) were more frequent in the decompensated group, the differences were not statistically significant. Other variables, including cancer type, hypertension, type 2 diabetes mellitus, immunosuppressive regimen category, post-reactivation NUC use, duration of immunosuppressive therapy, bone marrow transplantation, and anti-HBs status, did not differ significantly between groups. During follow-up, 14 patients (60.9%) died; however, none of the deaths were attributed to liver-related causes. One decompensated patient underwent living donor liver transplantation but subsequently died of pneumonia.
Conclusions: In patients with resolved HBV infection who experience reactivation during or after receiving immunosuppressive therapy, the presence of underlying cirrhosis is a significant predictor of hepatic decompensation. While advanced age and rituximab exposure may contribute to increased risk, they were not statistically significant in this study. Enhanced surveillance and early intervention may be warranted for cirrhotic patients undergoing immunosuppressive therapy to mitigate the risk of decompensation.
P.015
ON-TREATMENT CHANGE IN APRI AND FIB-4 VALUES TO PREDICT RISK FACTORS ASSOCIATED WITH THE DEVELOPMENT OF HEPATOCELLULAR CARCINOMA IN CHRONIC HEPATITIS B TREATED WITH NUCLEOS(T)IDE ANALOGUE –PING-TUNG COUNTY EXPERIENCE
Shi-Chi Wen1, Wu-Hsien Kuo2, Chao-Wen Hsueh1, Hsin-Yeh Chen1, Kai-Yao Yang3, Chou-Yuan Ko3, Jyan-Wei Huang6, Pei-Yu Lee4, Hsin-Yi Shen5, Yu-Fen Chen5, Yu-Hsuan Yao5, Xiu-Ru Jian5, Chian-Ya Huong5, Ji-Xuan Zhuo5, Di-Lan Tsai5
1Division of Gastroenterology, Department of Internal Medicine, Pao-Chien Hospital, Pingtung, Taiwan
2Yuan-Sheng Branch, Yuan-Zuong Hospital, Changhua, Taiwan
3Kaohsiung Armed Forces General Hospital, Kaohsiung, Taiwan
4Case Manager, Nursing Department, PaoChien Hospital, Pingtung, Taiwan
5Endoscopy Room, Nursing Department, PaoChien Hospital, Pingtung, Taiwan
6Pingtung Branch, Kaohsiung Armed Forces General Hospital, Pingtung, Taiwan
屏東地區慢性 B 型肝炎患者核 苷 酸類似 物治療前後以 APRI FIB-4 值評估纖維化
差異性預測肝癌發生風險及其相關因素 分析
文士祺1 郭武憲2 薛肇文1 陳興曄1 楊凱堯3 柯朝元3
黃健維6 李珮育4 沈欣怡5 陳郁棻5 尤郁嫙5 簡秀如5 洪千雅5 卓季萱5 蔡迪蘭5
1 寶建醫院肝膽胃腸內科
2 員榮醫院員生分院肝膽胃腸內科
3 國軍高雄總醫院肝膽胃腸內科
4 寶建醫院護理部個案管理師
5 寶建醫院護理部內視鏡室
6 國軍高雄總醫院屏東分院肝膽胃腸內科
Background: Chronic hepatitis B (CHB) remained a global epidemic and one of the leading causes of hepatocellular carcinoma (HCC) worldwide. Nucleos(t)ide analogue (NUC) such as tenofovir, entecavir has been approved to be a first line
therapy for treatment of chronic hepatitis B (CHB). Noninvasive fibrosis indices can help identify the risk of HCC in patients with CHB receiving NUC therapy with the lowest risk of HCC.
Aims: We used predictive score system to investigate the performance of on-treatment change in APRI and FIB-4 values for HCC risk in patients with CHB treated with NUC. We aimed to determinate risk factors associated with the HCC occurrence.
Methods: We retrospectively enrolled 129 treatment naïve patients with CHB who received tenofovir or entecavir therapy in Ping-Tung County between Nov 2013 and Nov 2023. We conducted this study to investigate the risk of HCC according to the prognostic performance of on-treatment change (after treatment minus baseline) in APRI and FIB-4 values assessed by Received operating curves (ROCs) and evaluate the prognostic significance of various baseline factors such as age, sex, cirrhosis, laboratory tests by Cox proportional hazard model associated with development of HCC. KaplanMeier analysis and log-rank test were performed to estimate and compare free curve between low and high risk in this real-world setting.
Results: The median age at baseline was 60.3 ± 12.1years. Of the patients, 99 (76.7%) were male, 76 (58.9%) were cirrhotic, 9 (30.2%) were diabetic, 75 (58.1%) were Tenofovir. Twenty-nine (22.5%) had HBeAg (+), and 22 (17.1%) had varices. The total of 23 (17.8%) developed HCC during median treatment duration of 5.81 ± 3.29 years and follow-up period 9.52 ± 4.56 years. Most of the patients had achieved a time to virological response (VR) of 8.99 ± 6.58 months and VR (12M) (81.4%). We compared the laboratory variables and noninvasive fibrosis indices at baseline and after treatment among patients with HCC and without one. Higher percentage of diabetes mellitus (DM), cirrhosis, varices, alfa-fetoprotein (AFP) at baseline and after treatment, APRI, FIB-4 values at baseline after treatment and presence of the on-treatment change were observed in the patient with HCC. In all the patients, cirrhosis status, DM, varices, AFP (baseline), AFP (after-treatment), APRI (median value after-treatment), FIB-4 (median value after-treatment), and the proportion of patients with APRI ≥0.7455 (optimal cut-off value change), △APRI ≥0 (median value on-treatment change), FIB-4 (optimal cut-off change) ≥3.8575, FIB4 (optimal cut-off value change) ≥4.3925 and △FIB4 ≥0 (median value on-treatment change) showed significant difference associated with HCC according
to univariate Cox regression analysis. Base on multivariate Cox proportional hazard model, factors with AFP (HR: 1.001, 95% CI: 1.000–1.002, p = 0.002) and APRI ≥0.7455 (HR: 5.973, 95% CI: 1.234–28.906, p = 0.026) were determined to be independent predictors of HCC.
Conclusions: HCC development was independently associated with DM, cirrhosis, varices, AFP among patients with CHB. The present study provides evidence in predicting the relevant role that APRI and FIB-4 kinetics during NUC therapy may play in predicting future HCC risk.
P.016
REAL-WORLD EFFECTIVENESS OF ENVIR IN CHRONIC HEPATITIS B: A 3-YEAR RETROSPECTIVE COHORT STUDY
Chung-Hsin Chang, Yi-Jie Huang, Yen-Chun Peng
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung Veterans General, Taichung, Taiwan
Envir 在慢性 B 型肝炎治療中的實際效 果:一項為期 3 年的回顧性隊列研究
張崇信 黃儀倢 彭彥均 臺中榮民總醫院胃腸肝膽科
Background: Entecavir is recommended as a firstline therapy for chronic hepatitis B (CHB). Envir is a generic formulation of entecavir.
Aims: This study aimed to evaluate the real-world effectiveness of Envir in patients with CHB.
Methods: From August 2017 to November 2021, 32 patients with CHB who received Envir 0.5 mg daily at Taichung Veterans General Hospital were retrospectively enrolled. Virological and biochemical responses were assessed throughout the treatment period.
Results: A total of 32 CHB patients were included in the final analysis. The median age was 52.34 years (IQR: 46.15–57.85), and 50% were male. Two patients (5.9%) were HBeAg-positive. The median baseline HBV DNA level was 4.00 log IU/mL (IQR: 0–6.32), the median quantitative HBsAg (qHBsAg) level was 2.94 log IU/mL (IQR: 2.49–3.36), and the median ALT level was 29.5 U/L (IQR: 20–61.5). The median qHBsAg levels at baseline and at months 6, 12, 18, 24, 30, and 36 were 2.94, 2.99, 2.94, 2.79, 2.80, 2.68, and 2.68 log IU/mL, respectively.
Conclusions: Envir, a generic formulation of entecavir, demonstrated stable virological and biochemical responses in patients with CHB over a 36-month treatment period. The gradual decline in qHBsAg levels suggests sustained antiviral activity. These findings support the long-term effectiveness of Envir in the real-world management of CHB patients.
P.017
BASELINE AND LONGITUDINAL BIOMARKERS PREDICT HCC IN CHRONIC HEPATITIS C: A COHORT STUDY
Yi-Lin Li, Pei-Lun Lee, Hung-Da Tung, Tang-Wei Chuang, Chun-Ta Cheng, Mai-Gio Pang, Ting-Yi Huang, Jyh-Jou Chen Division of Gastroenterology and Hepatology, Chi Mei Hospital, Liouying, Tainan, Taiwan
基線與縱向生物標誌預測 C 型肝炎患者 肝細胞癌風險之世代研究
奇美醫療財團法人柳營奇美醫院肝膽胃腸科
Background: Hepatocellular carcinoma (HCC) remains a major complication in patients with chronic hepatitis C. Identifying reliable biomarkers that predict HCC risk at baseline and during follow-up is crucial for optimizing surveillance and early intervention. Baseline noninvasive biomarkers, including the Fibrosis-4 (FIB-4) index and alpha-fetoprotein (AFP), have been identified as potential predictors of HCC development in patients with chronic hepatitis C (CHC). However, most evidence is derived from single time-point measurements; whether biomarkers at different time points or dynamic changes provide additional prognostic value has not been systematically examined.
Aims: We investigated the impact of baseline and longitudinal variations of biomarkers on subsequent HCC development in CHC patients.
Methods: We conducted a retrospective cohort study of 271 treatment-naïve CHC patients from 1999 to 2015. FIB-4 and AFP were collected at baseline and 3-year intervals. Multivariable Cox and logistic regressions were used to evaluate predictors of HCC and the impact of FIB-4 trajectory (improved, stable, worsened).
Results: Over a median 9.4-year follow-up, 29.9% of patients developed HCC. Baseline FIB-4 >3.25 significantly predicted HCC (adjusted HR 7.47, p<0.01). At 3 years, cirrhosis and AFP ≥20 ng/mL were independent predictors. Patients with worsened FIB-4 had the highest HCC incidence (41.4%) with adjusted OR 2.11.
Conclusions: High baseline and rising FIB-4 scores are strong predictors of HCC in CHC. These findings support incorporating dynamic biomarker monitoring into routine surveillance. Longitudinal changes may better identify patients needing intensified follow-up.
P.018
PROTECTIVE EFFECTS OF STATINS ON PULMONARY FUNCTION IN PATIENTS WITH PERSISTENT HYPERLIPIDEMIA: A RETROSPECTIVE COHORT STUDY
Ying-Ying Yang1,3,4,5, Hsiao-Chin Shen1,2,3, Che-Hao Tseng1, Hsiao-Yun Yeh1, Chien-Wei Su1,3,4,5, Diahn-Warng Perng2, Ming-Chih Hou4, Han-Chieh Lin4
1Department of Medical Education, Taipei
Veterans General Hospital, Taipei, Taiwan
2Department of Chest, Taipei Veterans General Hospital, Taipei, Taiwan
3Faculty of Medicine, School of Medicine, National Yang-Ming Chiao Tung University, Taipei, Taiwan
4Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taipei
Veterans General Hospital, Taipei, Taiwan
5Division of General Medicine, Department of Internal Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
Statin 他汀類藥物對持續性高血脂症患者 肺功能的保護作用:一項回顧性世代研 究
楊盈盈1,3,4,5 沈曉津1,2,3 曾哲皓1 葉筱芸1 蘇建維1,3,4,5 彭殿王2 侯明志4 林漢傑4
1 臺北榮民總醫院教學部
2 臺北榮民總醫院胸腔部
3 國立陽明交通大學醫學系
4 臺北榮民總醫院胃腸肝膽科
5 臺北榮民總醫院一般內科
Background: Pulmonary function tests offer crucial parameters for evaluating lung health and predicting clinical outcomes. Hyperlipidemia, a prevalent metabolic disorder, has been linked to declining pulmonary function. Statins are an essential therapy for lowering lipid levels in hyperlipidemia.
Aims: This study aims to investigate the therapeutic potential of statins in mitigating the decline in pulmonary function.
Methods: This is a retrospective cohort study. Out of 8286 patients who underwent spirometry testing from January 2018 to December 2020, 492 patients were included in the final analysis. The relationship between statin usage, dosage, along with other
biometric indices and spirometry parameters were evaluated. Multivariate logistic regression analyses were employed to assess the association between statin use and the decline in pulmonary function.
Results: In patients with persistent hyperlipidemia, the use of statins was associated with a higher predicted percentage of forced expiratory volume in 1 second (FEV1) compared to non-users (84.0% vs 78.0%, p = 0.015). Logistic regression models further revealed that statin use independently prevented FEV1 decline, irrespective of dosage (adjusted OR 0.036, 95% CI: 0.002–0.618 in lower statins dose group and adjusted OR 0.170, 95% CI: 0.019–1.552 in higher statins dose group).
Conclusions: The findings suggested that statin usage, regardless of dosage, independently mitigated the decline in pulmonary function among patients with persistent hyperlipidemia. Early initiation of statin therapy may hold promise for individuals experiencing hyperlipidemia and declining pulmonary function.
P.019
Fang-Chi Yang, I-Ling Liu, Ching-Chun Lin, Pei-Yuan Su, Hsu-Heng Yen
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan
醫學中心邁向全面 C 型肝炎篩檢的實務 困境
楊芳琦 劉怡伶 林靜君 蘇培元 顏旭亨
彰化基督教醫院胃腸肝膽科
Background: In response to the World Health Organization’s (WHO) goal of eliminating viral hepatitis as a major public health threat by 2030, Taiwan’s Ministry of Health and Welfare has launched the “Hepatitis C Elimination by 2025” initiative. The target is for 90% of hepatitis C patients to be diagnosed and over 80% to receive treatment by 2025. Although free screenings are available and directed by the Health Promotion Administration (HPA) in Taiwan, some outpatients with chronic conditions who have regular follow-up visits and blood tests still have less willingness to participate hepatitis C screening. This free screening has age and timing limited. We have analyzed the data of outpatient department with the lowest willingness to participate screening were Endocrinology & Metabolism, Cardiology, and Neurology. 1,065 diabetes patients in the Endocrinology department had not completed hepatitis C screening, with a screening completion rate of 84.7% in January 2025. In address to this issue, the local Public Health Bureau (PHB) initiated a Hepatitis C screening project which targeting this specific group and simplifying the process of screening at outpatient of Endocrinology & Metabolism department. The purpose of this study is to compare the effectiveness of HPA screening program and PHB screening project.
Aims: The aim of this study is to compare the effectiveness of HPA screening program and PHB screening project.
Methods: HPA screening program and PHB screening project were analyzed and compared from May 1, 2024, to May 30, 2025. HPA screening program provides individuals aged 45–79 a onetime free hepatitis B and C screening. Patients must
present their National Health Insurance card at the health checkup desk to verify eligibility. When a test order is issued, blood test must be done on the same day. On the other hand, PHB screening project targets diabetes outpatients, and has no age limited. Computer system will verify patients’ eligibility, and test orders will be issued along with the prescription. Blood test can be done at the next follow-up clinic visit.
Results: 1,836 individuals participated HPA screening program, 51.9% were female. 759 individuals were completed in PHB screening project, in which 11.2% (n = 85) were aged over 79 years old, and 31.9% (n = 242) age were under 45. 52.7% were male in PHB screening project. Hepatitis C antibody positivity rate were 1.1% and 1.6% in HPA screening program and PHB screening project respectively. HCV RNA positivity rate was significantly higher in PHB screening project 58.3% than HPA screening program 28.6%. In addition, Hepatitis C Treatment rates in PHB screening project was 100%, and HPA screening program was 83.3%. This was because patients’ condition were not able to compliant with clinic visits and take medication. Furthermore, we divided the group of PHB screening project into 3 subgroups by age, and analyzed the positive rate of Hepatitis C antibody and HCV RNA. Hepatitis C antibody positive rate were 1.2% aged under 45 (n = 3), 1.4% aged between 45 and 79 (n = 6), 3.5% aged Over 79(n = 3). HCV RNA positive rate were 33.3% aged under 45 (n = 1), 50% aged between 45 and 79 (n = 3), 100% aged over 79 (n = 3). This showed both positive rate of Hepatitis C antibody and HCV RNA were higher than the group in HPA screening program, especially the aged over 79.
Conclusions: Although the hepatitis C screening system established by the Health Promotion Administration (HPA) is comprehensive and covers a large population, its process remains cumbersome, restricted by age and specific timeframes. Low participation rate results in a limited detection rate of true-positive cases, and successful implementation still relies heavily on additional manpower from healthcare institutions to support promotion and health education. In contrast, PHB screening project adopts a proactive screening strategy targeting high-risk groups, such as patients on diabetes medications. This also covers a wider age range and detected higher antibody and RNA positivity rates, particularly aged over 79 the HCV RNA positivity rate reached 100%. It is a potentially high-risk population
that has been overlooked under the current HPA policy framework. PHB screening project simplified workflow and clearly defined objectives, this improve individuals willingness to receive screening and treatment. Future efforts could be focus on cross-sector collaboration with local health bureau support, expanding the program to other internal medicine outpatient clinics as a key strategy to confront the barrier for hepatitis C screening among high-risk populations. Working collectively toward the national goal of eliminating hepatitis C by 2025.
P.020
EFFECT OF MANDARIN VERSUS TAIWANESE LANGUAGE ON ANIMAL NAMING TEST PERFORMANCE FOR RAPID SCREENING OF MINIMAL HEPATIC ENCEPHALOPATHY
Hsin-Che Lin, Chun-Yen Lin, Rong-Nan Chien, Chien-Hao Huang
Department of Gastroenterology & Hepatology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
語言對 Animal Naming Test 用於快速篩 檢最輕微肝性腦病變的影響:國語與台 語的比較
林歆哲 林俊彥 簡榮南 黃建豪 林口長庚紀念醫院肝膽腸胃科
Background: Minimal hepatic encephalopathy (MHE) is a subclinical cognitive impairment in liver cirrhosis that increases the risk of overt HE and worsens long-term outcomes. Animal naming test (ANT1) is a brief, simple verbal fluency test proposed for rapid detection of MHE. However, its performance across different native languages remains unclear.
Aims: Our aims were (1). to validate the diagnostic performance of ANT1 for MHE 2. to determine whether ANT1 performance differs between Mandarin- and Taiwanese-speaking populations.
Methods: A prospective cohort study was conducted, including sixty-five compensated liver cirrhotic patients with ten healthy controls. All participants underwent ANT1, psychometric hepatic encephalopathy score (PHES), and mini-mental state examination (MMSE). Cirrhotic patients also underwent quantified electroencephalogram (EEG) to confirm MHE through characteristic slowing. Receiver operating characteristic (ROC) analysis was used to compare the prediction performance of the psychometric tests. Statistical analyses were performed using SAS Studio, and statistical significance was determined by 2-tailed tests, with significant set at a P value less than 0.05.
Results: Among the 65 liver cirrhotic patients, 16 patients developed MHE confirmed by PHES and/or quantified EEG. Compared to non-HE patients, those with MHE had significantly lower PHES score (-2 vs. 0, P = 0.002), ANT1 score (14.6 vs. 18.4, P = 0.015) and SANT1 score (15.8 vs. 19, P = 0.021). In subgroup
analysis, Mandarin-speaking MHE patients had significantly lower ANT1 (12 vs. 18, P = 0.02) and SANT1 (15 vs. 18, P = 0.02) scores compared to the non-HE patients. However, in Taiwanese-speaking patients, no significant differences were found (18 vs. 19, P = 0.19; 18 vs. 19.5, P = 0.39). ROC analyses indicated ANT1 had superior accuracy in Mandarin (AUROC 0.760; 95% CI: 0.677–0.949), compared to Taiwanese speakers (AUROC 0.679; 95% CI: 0.423–0.926).
Conclusions: ANT1 is a useful tool for rapid detecting MHE in Taiwan populations, particularly among Mandarin-speaking individuals. Its diagnostic accuracy may be attenuated in Taiwanese-speaking populations, highlighting the need for languagespecific calibration.
P.021
APRI INDEX OUTPERFORMS AFP AND DIABETES IN PREDICTING FIBROSIS-4 SCORE REGRESSION IN TREATMENT-NAIVE CHRONIC HEPATITIS C PATIENTS ACHIEVING SUSTAINED VIROLOGICAL RESPONSE AFTER GLECAPREVIR/ PIBRENTASVIR TREATMENT
Fu-Chih Hung1, Yi-Hao Yen2
1Hung Fu Chih Clinic, Pingtung, Taiwan 2Division of Hepatogastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
APRI 指數優於 AFP 與糖尿病在預 測 C 型肝炎病患在接受 Glecaprevir/ Pibrentasvir 治療達到病毒學治癒後的肝 纖維化改善(FIB-4 指數下降)
洪福枝1 顏毅豪2
1 洪福枝診所肝膽腸胃內科
2 高雄長庚紀念醫院胃腸肝膽科系
Background: Glecaprevir/Pibrentasvir (Maviret) is a highly effective pangenotypic direct-acting antiviral (DAA) regimen for treating chronic hepatitis C (CHC) across all genotypes. In community-based settings, family physicians play a critical role in post-treatment follow-up, particularly for patients with indeterminate liver fibrosis. This study aimed to identify non-invasive serum-based predictors of hepatic fibrosis regression, offering practical tools for risk stratification.
Methods: Between May 2019 and October 2024, 60 treatment-naive CHC patients were enrolled from a single community clinic in Taiwan. Laboratory data were collected at baseline, week 4, end of treatment (week 8, EOT) and 12 weeks post-treatment. Variables included demographic characteristics, virological parameters included HCV RNA viral load, genotype and HBsAg, and biochemical markers. The aspartate aminotransferase to platelet ratio index (APRI) and Fibrosis- 4 (Fib-4) score were calculated at baseline, week 8 (EOT) and at 12 weeks post-treatment. One patient (1.7%) was lost to follow-up after the end of tretment. Two patients had concurrent chronic hepatitis B coinfection, and another one was diagnosed with hepatocellular carcinoma (HCC) one
month after treatment, all were included for study. Multivariate logistic and multiple linear regression analyses were used to identify independent predictors of Fib-4 score regression.
Results: Of the 60 CHC treatment-naive patients treated with Glecaprevir /Pibrentasvir, 59 (98.3%) achieved sustained virological response (SVR). Fib4 score regression (≥0.245 decrease) was observed in 37.3% of patients. The cohort comprised 30 males and 29 females, with a mean age of 63.9 years. The most common genotype was 1b (42.4%).
Univariate logistic regression analysis evaluated the impact of age (≥66 vs. <66 years), gender, diabetes mellitus (DM), chronic kidney disease, genotype, ALT level (≥37.5 vs. <37.5 IU/mL), baseline APRI index (≥0.65 vs. <0.65), albumin (≥4.35 vs.<4.35 g/ dL), AFP (≥3 vs. <3 ng/mL), and baseline log₁₀ HCV RNA viral load (≥6.48 vs. <6.48). Multivariate logistic regression analysis identified DM, baseline APRI ≥0.65, and AFP ≥3 ng/mL as significant predictors of Fib-4 score regression in patients achieving SVR. However, in linear regression models confirmed, only pretreatment APRI index ≥0.65 remained a statistically significant (p < 0.001), demonstrating a strong quantitative association with Fib-4 score regression. The final predictive model was Fib-4 score regression = −0.0096 − 0.2971 × DM − 0.0141 × pretreatment AFP + 1.2777 × pretreatment APRI, R² = 0.612, p < 0.001, only APRI index was significant with p < 0.001.
Conclusions: Pretreatment APRI index emerged as the most consistent and robust non-invasive predictor of Fib-4 score regression following Glecaprevir/Pibrentasvir therapy across both logistic and linear regression models. Patients with baseline APRI ≥0.65 were more likely to experience better Fib-4 score regression. While DM and elevated AFP levels were associated with the likelihood of regression, only APRI index significantly predicted its magnitude. These findings support the use of APRI index as a simple, accessible tool for post-treatment fibrosis monitoring in primary care.
P.022
Takuma Imamura, Tatsuya Kakegawa, Mari Hayashi, Hidehito Honda, Hiroshi Takahashi, Hirohito Takeuchi, Katsutoshi Sugimoto, Takao Itoi
Department of Gastroenterology and Hepatology, Tokyo Medical University, Tokyo, Japan
Background: Surgical fenestration is one of the treatment options for symptomatic hepatic cysts. However, because it is an invasive procedure, less invasive treatments are preferred for elderly patients. Percutaneous sclerotherapy using ethanol or minocycline has also been associated with pain in some cases. In recent years, percutaneous sclerotherapy using polidocanol foam has been increasingly reported as a less invasive and effective treatment option.
Aims: To evaluate the efficacy of polidocanol foam for the treatment of symptomatic hepatic cysts in elderly patients.
Methods: We evaluated three cases aged 75 years or older who underwent percutaneous sclerotherapy with polidocanol foam at our institution. In all cases, an 8-Fr drainage tube was percutaneously inserted into the hepatic cyst via a transhepatic approach, and cystic fluid was aspirated as completely as possible. A second injection was administered 7 days later. Results: The mean age at the time of treatment was 80 years. The average maximum cyst diameter was 13.6 cm, and the mean cyst volume was 7.48 x 103 cm³. On follow-up CT performed more than three months after treatment, the mean cyst volume reduction rate was 85.8%. No significant complications, including pain, were observed.
Conclusions: Ultrasound-guided percutaneous sclerotherapy using polidocanol foam for symptomatic hepatic cysts is a simple and low-risk procedure. It was found to be an effective treatment option even for elderly patients.
P.023
MIXED NEUROENDOCRINE NONNEUROENDOCRINE NEOPLASMS AND ADENOCARCINOMAS WITH NEUROENDOCRINE DIFFERENTIATION: CLINICAL EXPERIENCE FROM A
Yu-Jou Tsai1, Jung-Pin Tseng1, I-Hao Tseng1, Tung-Bo Chao2, Tak-Kee Choy2, I-Tsou Tseng3
1Section of Gastroenterology, Department of Internal Medicine, Yuan’s General Hospital, Kaohsiung, Taiwan
2Section of Colorectal Surgery, Department of Surgery, Yuan’s General Hospital, Kaohsiung, Taiwan
3Section of Digestive Surgery, Department of Surgery, Yuan’s General Hospital, Kaohsiung, Taiwan
混合型神經內分泌腫瘤與含神經內分泌 分化之腺癌:南臺灣某一區域醫院之臨 床分析
蔡毓洲1 曾榮斌1 曾逸豪1 趙東坡2 蔡達基2 曾譯諏3
1 阮綜合醫院消化內科
2 阮綜合醫院大腸直腸外科
3 阮綜合醫院消化外科
Background: According to the World Health Organization (WHO) classification, mixed neuroendocrine non-neuroendocrine neoplasms (MiNENs) are defined as digestive system neoplasms comprising at least 30% of both neuroendocrine and non-neuroendocrine components. Both MiNENs and adenocarcinomas with neuroendocrine differentiation (Adeno-NEs) in digestive system represent rare and heterogeneous malignancies that pose considerable diagnostic and therapeutic challenges.
Aims: Given the heterogeneity of MiNENs and Adeno-NEs, as well as the current lack of standardized treatment protocols, we conducted a retrospective study to evaluate clinical features, treatment modalities, and outcomes of patients diagnosed with these tumors at a regional hospital in southern Taiwan. This study aims to contribute to the improvement of disease management and prognosis.
Methods: A retrospective review of patients
diagnosed with MiNENs or Adeno-NEs between 2014 and 2024 was performed. Clinical data including patient demographics, tumor location and stage, presenting symptoms, imaging findings, tumor markers, pathological characteristics, treatment approaches, and survival outcomes were collected and analyzed.
Results: A total of eight patients (5 males and 3 females), with a median age of 67 years (range: 52–84 years), were included in the study. Four patients were diagnosed with MiNENs, with primary tumors located in the transverse colon, ascending colon, gallbladder, and rectosigmoid junction. Three of these patients developed distant metastases either before or after initial treatment. All MiNEN patients underwent surgical intervention, with a median overall survival of over 23 months. The remaining four patients were diagnosed with Adeno-NEs, with tumor locations in the liver, transverse colon, colon, and duodenum. At diagnosis, two patients had lymph node metastases and one had distant metastasis. Only two patients underwent surgical intervention and still alived so far, achieving survival durations of more than 26 months and 6 months respectively. The other two patients refused further treatments and received only supportive care, with survival durations of less than 2 months.
Conclusions: Our findings suggest that patients with MiNENs or Adeno-NEs who receive aggressive treatment, particularly surgical intervention, may experience improved survival outcomes even in the presence of lymph node or distant metastases. Further large-scale studies are warranted to establish standardized treatment guidelines for these rare and complex malignancies.
P.024
ASSOCIATION BETWEEN PRETREATMENT NEUTROPHIL-TOLYMPHOCYTE RATIO AND CHANGES IN FIB-4 INDEX AFTER ANTIVIRAL THERAPY FOR HEPATITIS C
Wei-Ting Chiang, Guan-Hua Li, Tsung-Ming Chen, Pi-Teh Huang
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Tungs’ Taichung MetroHarbor Hospital, Taichung, Taiwan
治療前中性球淋巴球比值與
江偉廷 李冠華 陳宗勉 黃彼得
童綜合醫院胃腸肝膽科
Background: Neutrophil-to-lymphocyte ratio (NLR) is an accessible marker of systemic inflammation and has been associated with prognosis in various chronic conditions, including cardiovascular diseases, malignancies, and liver fibrosis. In patients with chronic hepatitis C virus (HCV) infection, FIB-4 correlates with liver disease prognosis. However, whether baseline NLR can predict fibrosis improvement following direct-acting antiviral (DAA) therapy remains uncertain.
Aims: This study aims to investigate whether pretreatment NLR is associated with the degree of liver fibrosis improvement, as measured by the FIB-4 index, following DAA therapy, and whether different DAA regimens (Epclusa vs Mavyret) are associated with differing treatment outcomes.
Methods: This retrospective study enrolled adult patients diagnosed with HCV and treated with either Epclusa or Mavyret in a regional hospital in 2023. Blood tests were performed at baseline and again at the time of sustained virologic response (SVR) to calculate both FIB-4 and NLR. The post-topre-treatment FIB-4 ratio (F4R) was used to quantify treatment effect. Patients were stratified into three groups based on F4R: <0.8 as the “improved” group, 0.8–1.2 as the “no change” group, and >1.2 as the “worsened” group. NLR values were compared across patient groups stratified by FBR using the Kruskal-Wallis test. To improve robustness, outliers were removed using the interquartile range (IQR) method.
Results: A total of 76 patients who completed
treatment and follow-up were included, with 62 receiving Epclusa and 14 receiving Mavyret. After excluding four extreme NLR outliers, the final analyzed cohort consisted of 72 patients. Among the 72 patients, the improved group included 32 individuals with a median F4R of 0.603 (mean 0.591); the no-change group included 33 patients with a median of 1.002 (mean 0.993); and the worsened group included 7 patients with a median of 1.238 (mean 1.319). The distribution of baseline NLR differed significantly across the three F4R groups (Kruskal-Wallis H = 7.54, p = 0.023), with the lowest median NLR observed in the improved group and the highest in the worsened group.
Conclusions: Pretreatment NLR may be associated with the degree of liver fibrosis improvement after antiviral therapy for HCV. After excluding outliers, baseline NLR significantly differed across response groups, supporting its potential as a predictive biomarker for DAA. While no significant difference was observed between DAA regimens, further investigation with larger samples is warranted.
P.025
SERIAL INCREASES OF ALPHAFETOPROTEIN LEVELS PREDICT THE RISK OF CHRONIC HEPATITIS B-RELATED HEPATOCELLULAR CARCINOMA
Tung-Hung Su1,2, Yun-Chun Wu3, Shang-Chin Huang1,2,4, Chun-Ming Hong5, Shih-Jer Hsu1,2, Tai-Chung Tseng1,2,6, Chen-Hua Liu1,2, Hung-Chih Yang1, Chun-Jen Liu1,2, Pei-Jer Chen1,2,4,6, Jia-Horng Kao1,2,4,6
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan
3Roche Products Ltd, Taipei, Taiwan
4Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan
5Division of Multidisciplinary Medicine, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
6Department of Medical Research, National Taiwan University Hospital, Taipei, Taiwan
甲型胎兒蛋白濃度的序列上升可預測慢 性 B 型肝炎相關肝細胞癌的風險
蘇東弘1,2 吳昀麇3 黃上秦1,2,4 洪俊銘5 徐士哲1,2 曾岱宗1,2,6 劉振驊1,2 楊宏志1 劉俊人1,2 陳培哲1,2,4,6
高嘉宏1,2,4,6
1 國立臺灣大學醫學院附設醫院胃腸肝膽科
2 國立臺灣大學醫學院附設醫院肝炎研究中心
3 羅氏大藥廠股份有限公司
4 國立臺灣大學臨床醫學研究所
5 國立臺灣大學醫學院附設醫院整合醫學科
6 國立臺灣大學醫學院附設醫院醫學研究部
Background: Alpha-fetoprotein (AFP) has been used as a diagnostic and prognostic marker for hepatocellular carcinoma (HCC). However, the low sensitivity limits its usefulness for HCC surveillance. Aims: In this study, we aimed to evaluate the serial changes of AFP as a predictive marker for HCC and whether it could perform better than a single AFP measurement.
Methods: We conducted a retrospective cohort study to screen eligible patients with chronic
hepatitis B followed in a tertiary medical center in Taiwan from 2006 to 2021. They received regular HCC surveillance with abdominal ultrasonography and AFP biannually. Those with prior liver malignancies, follow-up less than 1 year, and pregnant women were excluded. Several time-varying AFP parameters were generated from longitudinal AFP measurements. These include the last recorded values, average values, and slope of change over various time windows. The slope would be assigned as zero if there is only a single AFP measurement. A Cox proportional hazards model with timedependent AFP parameter was built to identify the risk predictors of HCC incidence. Statistical analysis was performed using the R statistical software. Results: Overall, 42,552 patients with chronic hepatitis B were screened, after a 10% random sampling and excluding ineligible patients, and finally, 3258 patients were included for further analyses. The median age was 50 years, and 56% were men. In this cohort, 5.7% had cirrhosis, 4.9% had HCV-coinfection, and 29.9% received antiHBV therapy. After a median follow-up of 7.8 years, 125 patients developed HCC. Older age, male sex, cirrhosis, diabetes, a 6-month AFP increase rate, and HBV antiviral therapy were factors predictive of HCC. After adjustment for confounding factors, the 6-month AFP increase rate (HR: 1.02, P = 0.003) was predictive for the development of HCC with an AUROC of 0.845. It was also confirmed in a subgroup of patients with two or more AFP measurements as a sensitivity analysis. Before HCC development, the last 6-month AFP increase rate was 0.41 vs. 0.01 ng/ mL in the HCC and non-HCC patients, respectively. Conclusions: A 6-month AFP increase rate is a significant predictor for the development of HCC in patients with chronic hepatitis B. AFP should be serially monitored and judged to improve HCC surveillance.
P.026
NIVOLUMAB FOR THE PATIENTS WITH UNRESECTABLE HEPATOCELLULAR CARCINOMA: A RETROSPECTIVE STUDY
Chia-Ming Lin1, Kuan-Chun Hsueh1,2
1Division of General Surgery, Department of Surgery, Tungs’ Taichung Metroharbor Hospital, Taichung, Taiwan
2Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan
Nivolumab 用於不可切除之肝細胞癌患
林家名1 薛冠群1,2
1 童綜合醫療社團法人童綜合醫院一般外科
2 國立中興大學醫學院學士後醫學系
Background: The optimal treatment following firstline systemic therapy for unresectable hepatocellular carcinoma (uHCC) remains uncertain.
Aims: This study aimed to evaluate the efficacy and safety of nivolumab as a second-line treatment in patients with uHCC.
Methods: We retrospectively reviewed patients with uHCC who received nivolumab more than 3 cycles as second-line systemic therapy between January 2019 and March 2025. Prior treatments with sorafenib and/ or lenvatinib and concurrent interventions during nivolumab therapy were included. Nivolumab was administered at 1–3 mg/kg every 3 weeks, based on clinical evaluation and patients’ decisions. Treatment response, overall survival (OS), progression-free survival (PFS), and treatment-related adverse events (TRAEs) were assessed.
Results: A total of 45 patients received nivolumab therapy, 23 met the inclusion criteria; 19 were male. The median age was 66 years (IQR, 57.0-71.5). The median follow-up duration was 15.1 months (IQR, 5.7–27.3), and the median duration of nivolumab therapy was 4.3 months (IQR, 2.9–8.4). Hepatitis B, C, and non-B/non-C etiology were observed in 15, 2, and 5 patients, respectively. 20 patients were identified as Child-Pugh class A. 10 patients had Barcelona Clinic Liver Cancer (BCLC) stage B disease, and 13 had stage C. The objective response rate was 47.8%, and the disease control rate was 73.9%.
Median OS and PFS were 15.1 (95% CI, 12.1-26.1) and 10.5 (95% CI, 8.8-24.4) months, respectively.
Grade 3/4 TRAEs occurred in 5 patients (21.7%). Concurrent treatments included transarterial chemoembolization (17.4%), radiofrequency ablation (13.0%), radiotherapy (13.0%), and tyrosine kinase inhibitors (30.4%). Combination therapy with local interventions showed improved disease control rate compared to nivolumab alone (76.9% vs. 70.0%).
Conclusions: Second-line nivolumab therapy for uHCC demonstrated a manageable safety profile and promising efficacy. The combination of nivolumab and local-regional treatment may enhance disease control compared to nivolumab monotherapy for uHCC patients.
P.027
BASELINE LIVER TUMOR
SIZE AS A PREDICTIVE LIVERSPECIFIC RESPONSE FACTOR IN UNRESECTABLE HEPATOCELLULAR CARCINOMA PATIENT RECEIVING IMMUNE CHECKPOINT INHIBITORS
Meng-Wei Alan Lin1, Huang-Pin Chen1, Meng-Wei Lin1, Hung-Tsung Wu2, Hsin-Yu Kuo1
1Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan
2Department of Internal Medicine, School of Medicine, College of Medicine, National Cheng Kung University, Tainan, Taiwan
治療前肝腫瘤大小可作為無法切除肝細 胞癌患者接受免疫檢查點抑制劑治療時 之肝臟特異性反應預測因子
林孟葳1 陳煌斌1 林孟緯1 吳泓璁2 郭欣瑜1
1 國立成功大學附設醫院內科部
2 國立成功大學醫學系內科學科
Background: Hepatocellular carcinoma (HCC) is one of the leading causes of cancer-related mortality worldwide, and immune checkpoint inhibitors (ICIs) have become the established first-line therapy for unresectable HCC. However, specific predictive markers for treatment response in patients with unresectable HCC undergoing ICIs therapy remain limited.
Aims: To determine whether baseline liver tumor size could serve as a predictive factor in patients with unresectable HCC receiving ICIs.
Methods: A total of 80 patients with unresectable HCC receiving atezolizumab and bevacizumab were retrospectively enrolled. Clinical and radiological parameters associated with therapeutic response were recorded. Continuous variables were compared by independent t-test, and Pearson chisquare analysis was applied to compare categorical variables. Survival curve was calculated using the Kaplan-Meier method and compared by log-rank test.
Results: In the evaluation of liver-specific responses, 10 patients (12.5%) achieved a complete response, 21 (26.3%) had a partial response, 36 (44.9%) exhibited stable disease, and 13 (16.3%) showed progressive
disease. The organ-specific objective response rate (OSRR) was 38.8% for the liver, and the liver-specific disease control rate was 83.8%. Responders had significantly smaller baseline liver tumor sizes prior to ICI treatment compared to non-responders (58.7 ± 6.5 mm vs. 82.4 ± 7.0 mm, p = 0.015). Patients with liver tumors smaller than 110 mm demonstrated a higher OSRR (28/60; 47%) than those with tumors larger than 110 mm (3/20; 15%) (p = 0.012). Kaplan–Meier analysis showed a significant difference in overall survival between liver-specific responders and non-responders (p = 0.002).
Conclusions: Liver-specific response to ICI therapy was associated with smaller baseline liver tumor size and improved survival. Patients with liver tumors ≤110 mm had significantly higher response rates. These findings suggest that baseline liver tumor size may serve as a predictive marker for treatment efficacy and clinical outcomes.
P.028
DEVELOPMENT AND VALIDATION OF AN AST/ALTBASED PROGNOSTIC MODEL FOR ALCOHOL-RELATED HEPATOCELLULAR CARCINOMA: A COHORT STUDY FROM EASTERN TAIWAN
Wei-Hao Huang1, Yen-Hsiang Wang2, Ming-John Bair3, Ping-Jen Hu1,4
1Department of Internal Medicine, Division of Gastroenterology, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan
2Graduate Institute of Medical Sciences, College of Medicine, Taipei Medical University, Taipei, Taiwan
3Division of Gastroenterology, Department of Internal Medicine, Taitung Mackay Memorial Hospital, Taitung, Taiwan
4TMU Research Center for Digestive Medicine, Taipei Medical University, Taipei, Taiwan
基於 AST/ALT 比值之酒精性肝細胞癌預 後模型之發展與驗證:來自東台灣的世 代研究
黃韋豪1 王彥翔2 白明忠3 胡炳任1,4
1 衛生福利部雙和醫院消化內科
2 臺北醫學大學醫學系
3 台東馬偕紀念醫院消化內科
4 臺北醫學大學消化醫學研究中心
Background: As viral hepatitis becomes increasingly controlled under global elimination initiatives, alcohol-related liver disease is emerging as a predominant cause of hepatocellular carcinoma (HCC), particularly in regions with high alcohol consumption like Eastern Taiwan. Existing HCC prognostic models primarily target viral etiologies and are often too complex for practical use. The predictive role of AST/ALT ratio in alcohol-related HCC survival remains unclear.
Aims: To develop and validate simplified prognostic models—including an AST/ALT-based model and a multivariate laboratory model—for predicting 6-month and 2-year survival in patients with alcoholrelated HCC.
Methods: This retrospective cohort study included 353 patients with alcohol-related HCC from Taitung MacKay Memorial Hospital between 2006 and 2016.
Patients were randomized into training (n = 235) and validation (n = 118) cohorts. AST/ALT ratios and other laboratory markers (albumin, platelet count) were analyzed using Cox and logistic regression models. ROC curve analysis evaluated model performance. Results: An AST/ALT model and a multivariate model (albumin, platelets, AST/ALT) were constructed. The AST/ALT model yielded AUCs of 0.713 and 0.651 for 6-month and 2-year survival, respectively, in the training cohort. The multivariate model showed superior performance, with AUCs of 0.781 (6-month) and 0.727 (2-year) in the training cohort, and 0.684 and 0.628 in the validation cohort. Lower AST/ALT ratios were significantly associated with poorer survival.
Conclusions: We present the first validated survival prediction models specifically for alcohol-related HCC using simple and accessible clinical parameters. These tools may enhance timely clinical decisionmaking in settings where alcohol is a dominant HCC etiology.
P.029
PROGNOSTIC DETERMINANTS AND TREATMENT STRATEGIES ASSOCIATED WITH LONG-TERM SURVIVAL IN EARLY-STAGE HEPATOCELLULAR CARCINOMA: A RETROSPECTIVE COHORT STUDY
Kuan-Chen Pan1, Hui-Ling Huang1,2, Sheng-Nan Lu1,2,3, Te-Sheng Chang1
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Chiayi Chang Gung Memorial Hospital, Chiayi, Taiwan
2Department of Nursing, Chiayi Chang Gung Memorial Hospital, Chiayi, Taiwan
3Division of Hepato-Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
早期肝細胞癌長期存活相關的預後決定 因素和治療策略:一項回顧性隊列研究
潘冠塵1 黃惠玲1,2 盧勝男1,2,3 張德生1
1 長庚醫療財團法人嘉義長庚紀念醫院腸胃內科
2 長庚醫療財團法人嘉義長庚紀念醫院護理部
3 長庚醫療財團法人高雄長庚紀念醫院胃腸肝膽科系
Background: Hepatocellular carcinoma (HCC) remains a major cause of cancer-related mortality worldwide and is particularly prevalent in Taiwan. While curative treatments offer favorable outcomes for early-stage HCC, prognostic factors change and option medical strategy remain uncertain in long term survival early-stage HCC.
Aims: This study aims to focused on the following key questions: (1) Do the prognostic factors for earlystage HCC change in patients who survive more than five years, and which of these factors are associated with long-term survival? (2) What are the curative treatment and stage progression rates among earlystage HCC patients who achieve long-term survival? (3) What clinical characteristics and treatment strategies are associated with higher tumor free status and favorable long-term outcomes?
Methods: This retrospective study analyzed 1,144 patients with BCLC stage 0 or A HCC from a cancer registry (2011–2020), followed through 2023. Prognostic factors were evaluated using Cox regression. Subgroup analyses were performed on patients who survived over five years, and further
stratified into 5–10 years and >10 years survival groups to assess treatment outcomes and tumorfree status (TFS).
Results: Age >65, Child-Pugh B, and non-curative treatment were consistent poor prognostic factors; HBV-related HCC was associated with improved survival. Among patients surviving >10 years, higher TFS rates and lower stage progression were observed compared to those surviving 5–10 years. Curative treatment significantly increased the likelihood of achieving TFS (p = 0.044).
Conclusions: Long-term survival in early-stage HCC is influenced by age, liver function, viral etiology, and treatment strategy. Curative treatments significantly improve outcomes, and maintaining curative treatment options is crucial for patients who experience recurrence while still in the early stage of HCC.
P.030
PRIMARY HEPATIC SARCOMA: CASE SERIES AND REVIEW OF THE LITERATURE
Guan-Hua Li1, Pi-Teh Huang1, Kuan-Chun Hsueh2,3
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Tung’s Taichung MetroHarbor Hospital, Taichung, Taiwan
2Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan
3Division of General Surgery, Department of Surgery, Tung’s Taichung MetroHarbor Hospital, Taichung, Taiwan
原發性肝臟肉瘤
李冠華1 黃彼得1 薛冠群2,3
1 童綜合醫院肝膽腸胃科
2 國立中興大學學士後醫學系
3 童綜合醫院一般外科
Background: Primary hepatic sarcoma (PHS) is a rare, aggressive and malignant liver neoplasm, accounting for less than 1% of all primary liver cancers. Common types include angiosarcoma, embryonal sarcoma, leiomyosarcoma, and malignant fibrous histiocytoma. Clinical manifestations, laboratory data and imaging characteristics often lack specificity. There is no valid guideline for treatment choices. Despite of advancements in treatments, the prognosis of PHS remains poor and mostly depends on clinicians’ experiences and decisions.
Aims: The aim of this study was to report the management of PHS in our hospital. We also review some relevant literature to find out the relationship between clinical parameters and outcome and to help guide the possibly effective treatment strategies.
Methods: We retrospectively reviewed the clinical data of 9 patients who were diagnosed with PHS in our hospital between 2014 and 2024. Patients’ demographic information, liver function, abdominal images, treatments, tumor characteristics, and survival data were collected. Definite diagnosis was confirmed by combining clinical image and histopathological reports. Tumor subtypes such as angiosarcoma were confirmed by pathology and immunohistochemistry. Statistical analysis
was performed to assess correlations between clinical parameters and survival days. Furthermore, specific attention was given to evaluating the impact of comorbidities, tumor size, and treatment interventions on patient prognosis.
Results: A total of 9 patients (6 males and 3 females) were included in this chart review, with the baseline clinical characteristics of the patients are shown in Table 1. The median age of the patients was 71 years (range 39–86 years). All patients initially presented with abdominal pain or distension and preserved liver function status, and three of whom had tumor rupture with hemoperitoneum on abdominal Computed Tomography. Tumor sizes ranged from 5 cm to 16 cm at initial diagnosis, rapid progression was observed in two patients with increasing at least 4 cm in diameter within 6 months. Among them, five patients found solitary lesion, three had more than 3 tumors, and one presented as an infiltrative tumor. The median survival after the diagnosis of PHA is 66 days (range: 5–289 days). Treatment approaches were diverse. Liver resection had been performed for four patients, with postoperative survivals of 5, 52, 93 and 289 days, respectively. Two patients who underwent chemotherapy survived 79 and 174 days. One patient who received trans-arterial chemoembolization (TACE) survived 61 days. Two patients who received supportive care survived 41 and 66 days, respectively.
Conclusions: Primary hepatic sarcoma, especially angiosarcoma, is associated with extremely poor prognosis, particularly in patients presenting with metastatic disease or tumor rupture. Early diagnosis, possible radical surgical resection and chemotherapy might provide the chance of longer survival.
P.031
CONDITIONAL SURVIVAL AFTER LIVER RESECTION FOR EARLYSTAGE HEPATOCELLULAR CARCINOMA
SinHua Moi2, YuehWei Liu3, CheeChien Yong3, ChihChi Wang3, WeiFeng Li3, ChihYun Lin4, YiHao Yen1
1Division of Hepatogastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
2Kaohsiung Medical University
3Liver Transplantation Center and Department of Surgery, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
4Biostatistics Center, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
早期肝細胞癌病患接受手術切除其附有
條件的存活率
魏芯樺2 劉約維3 楊志權3 王植熙3 李偉鋒3 林芷芸4
顏毅豪1
1 高雄長庚紀念醫院胃腸肝膽科系
2 高雄醫學大學
3 高雄長庚紀念醫院一般外科
4 高雄長庚紀念醫院生物統計中心
Background: Conditional survival (CS) is a measure of prognosis of patients who have already survived several years since diagnosis.
Aims: However, few studies have investigated the CS of patients who underwent liver resection (LR) for early-stage hepatocellular carcinoma (HCC).
Methods: We enrolled 942 consecutive patients who underwent LR for HCC with pathology-defined American Joint Committee on Cancer (AJCC) 7th edition stage 1 or 2 disease. The three-year CS was calculated as CS = S(x + 3)/S(x) and represented the probability of surviving an additional three years, given that the patient had already survived x years.
Results: The one-, three-, and five-year survival rates were 97.1%, 86.7%, and 76.1%, respectively, and were lower in cases with AJCC stage 2 disease, alpha-fetoprotein level of ≥20 ng/ml, presence of cirrhosis, anti-hepatitis C virus positivity, age >65 years, and Model for End-Stage Liver Disease score of >9. However, the three-year CS indicated that these variables were associated with shortened survival only in the first two years. From the third year after
LR, the probability of survival of patients was similar between subgroups.
Conclusions: CS is useful for providing a dynamic evaluation of survival during postoperative followup.
P.032
AMENTOFLAVONE POTENTIATES THE IN VIVO THERAPEUTIC EFFICACY OF REGORAFENIB AGAINST HEPATOCELLULAR CARCINOMA PROGRESSION
Jyun-Wei Wang, Chung-Hung Chen, Sheng-Lei Yan, Yung-Hsiang Yeh, Huai-Yi Huang
Division of Gastroenterology, Department of Internal Medicine, Chang Bing Show Chwan Memorial Hospital, Changhua, Taiwan
穗花杉雙黃酮增強癌瑞格在活體內對抗 肝細胞癌進展的治療效果
王俊偉 陳忠宏 顏聖烈 葉永祥 黃懷毅 彰濱秀傳紀念醫院胃腸肝膽科
Background: Regorafenib, an oral multikinase inhibitor, has been approved for the treatment of hepatocellular carcinoma (HCC), exerting its antitumor activity primarily through the inhibition of angiogenic and oncogenic kinase signaling pathways. Efforts to enhance its therapeutic efficacy against HCC have been the subject of ongoing investigation. Several studies have reported that natural compounds isolated from medicinal plants sensitize HCC cells to regorafenib. Amentoflavone, a functional bioflavonoid, exhibits anticancer properties, including the suppression of tumor growth, invasion, and angiogenesis. Notably, amentoflavone has been shown to potentiate the anti-HCC efficacy of sorafenib, the parent compound of regorafenib. Therefore, whether amentoflavone can similarly enhance the therapeutic effects of regorafenib against HCC remains to be elucidated.
Aims: The major goal of the present study was to verify the inhibitory efficacy and mechanism of amentoflavone in combination with regorafenib in HCC in vivo.
Methods: An HCC xenograft model was established using Huh7-bearing mice. Mice were treated with amentoflavone, regorafenib, or the combination of both for 20 days. Tumor growth was monitored using a digital caliper. Immunohistochemistry (IHC) staining was used to evaluate apoptotic signaling, nuclear factor-kappaB (NF-κB) activity, and expression of NF-κB downstream effector proteins. Results: The results indicate that amentoflavone potentiates the antitumor effects of regorafenib by promoting apoptosis and inhibiting tumor growth.
This combinational effect is associated with a significant downregulation of NF-κB activity and reduced expression of its downstream effectors, MMP-9 and VEGF, which play crucial roles in tumor invasion and angiogenesis. In addition, H&E staining and biochemical analyses showed that the administered drug doses did not cause toxicity in the mice.
Conclusions: Based on the overall findings, we suggest that amentoflavone enhances the in vivo therapeutic efficacy of regorafenib against hepatocellular carcinoma progression by promoting apoptosis and inhibiting NF-κB activation.
P.033
A TRICYCLIC ANTIDEPRESSANT IMIPRAMINE SUPPRESSES HEPATOCELLULAR CARCINOMA PROGRESSION
Huai-Yi Huang, Kuan-Wei Liu, Jyun-Wei Wang, Chung-Hung Chen, Sheng-Lei Yan, Chien-Hua Chen, Yung-Hsiang Yeh
Division of Gastroenterology, Department of Internal Medicine, Chang Bing Show Chwan Memorial Hospital, Changhua, Taiwan
三環類抗憂鬱藥妥富腦抑制肝細胞癌進 展
黃懷毅 劉觀偉 王俊偉 陳忠宏 顏聖烈 陳建華 葉永祥 彰濱秀傳紀念醫院胃腸肝膽科
Background: The epidermal growth factor receptor (EGFR), a receptor tyrosine kinase, plays a crucial role in the progression of hepatocellular carcinoma (HCC) by activating downstream signaling pathways that promote tumor cell proliferation, resistance to apoptosis, angiogenesis, tissue invasion, and metastasis. Elevated EGFR activity is often associated with poor clinical outcomes in HCC patients. Recent evidence suggests that certain antidepressants may possess anti-HCC properties, highlighting a novel area of therapeutic investigation. Imipramine, a tricyclic antidepressant, has been reported to inhibit the proliferation of HCC cells; however, its underlying anti-HCC mechanisms remain largely unclear.
Aims: The primary objective of this study was to evaluate the anti-HCC effects of imipramine both in vitro and in vivo.
Methods: HCC cell lines and HCC xenograft mouse models were employed. Imipramine treatment was administered, followed by assessments of tumor cell proliferation, invasion capacity, apoptotic induction, and EGFR signaling activity. These evaluations were conducted using cell viability assays, digital caliper measurements, flow cytometry, invasion assay, Western blotting, and immunohistochemical staining.
Results: Our results demonstrate that imipramine significantly suppresses HCC cell proliferation in vitro and inhibits tumor growth in vivo. Furthermore, imipramine treatment effectively attenuates EGFR signaling and reduces the invasive potential of HCC cells. Importantly, imipramine induces apoptosis through both extrinsic and intrinsic pathways.
Conclusions: These findings suggest that imipramine exerts potent anti-HCC effects and may serve as a promising therapeutic agent for the treatment of hepatocellular carcinoma.
P.034
EARLY OUTCOMES OF RFA IN DIABETIC VS. NON-DIABETIC HCC
Po-Jung Chen, Chen-Chun Lin, Hao-Tsai Cheng, Shu-Wei Huang, Cheng-Ju Lee, Ming-Yao Su
Division of Hepatogastroenterology, Department of Internal Medicine, New Taipei Municipal Tucheng Hospital, New Taipei City, Taiwan
糖尿病與非糖尿病肝癌病人接受射頻燒 灼術後早期預後比較
陳柏融 林成俊 鄭浩材 黃書偉 李誠儒 蘇銘堯
新北市立土城醫院(委託長庚醫療財團法人興建經 營)胃腸肝膽科
Background: Hepatocellular carcinoma (HCC) is one of the leading causes of cancer-related mortality worldwide. For patients with early-stage disease, radiofrequency ablation (RFA) is a widely accepted curative treatment option. Diabetes mellitus (DM) has been increasingly recognized as a potential risk factor for HCC development and may also influence tumor behavior and treatment outcomes. However, the prognostic impact of DM on HCC patients undergoing RFA remains unclear.
Aims: The aim was to investigate whether DM affects tumor recurrence and short-term outcomes in patients with HCC who received curative RFA.
Methods: This retrospective cohort study was conducted at New Taipei Municipal Tucheng Hospital and included patients with HCC who underwent curative-intent RFA between June 2, 2020, and June 3, 2025. Inclusion criteria were: age ≥20 years, imaging- or pathology-confirmed HCC, and RFA as the initial treatment. Exclusion criteria included incomplete ablation, concurrent cancer therapies, extrahepatic metastasis, BCLC stage C, and follow-up <3 months. Patients were divided into DM and non-DM groups based on medical records and use of antidiabetic medications. Baseline variables included age, sex, BMI, liver disease etiology, cirrhosis, Child–Pugh score, laboratory values (albumin, bilirubin, creatinine), AFP levels, tumor size and number, and metformin use. Outcomes included recurrence, survival, and followup time. Statistical analyses included t-tests for continuous variables, Chi-square/Fisher’s exact tests for categorical variables, and Kaplan–Meier survival
analysis with log-rank testing. A two-tailed p < 0.05 was considered statistically significant.
Results: A total of 43 HCC patients were included, with 22 in the non-DM group and 21 in the DM group. Baseline characteristics, including liver function, AFP, tumor size, and tumor number, were comparable between groups (p > 0.05). The DM group had a significantly shorter follow-up duration (14.6 ± 12.8 vs. 22.6 ± 14.7 months, p = 0.032). The distribution of BCLC stage was not significantly different between groups. A higher proportion of DM patients were classified as stage 0 compared to non-DM patients (38.1% vs. 13.6%, p = 0.162). Local tumor recurrence occurred in 19.0% of DM and 22.7% of non-DM patients (p = 0.578). Distant recurrence was noted in 19.0% of DM vs. 31.8% of non-DM patients (p = 0.337). Overall recurrence rates were 38.1% in DM and 45.5% in non-DM (p = 0.602). During followup, 2 patients in the DM group died (9.5%), while no deaths occurred in the non-DM group (p = 0.138). Kaplan–Meier analysis showed no significant difference in disease-free or overall survival between groups.
Conclusions: In this retrospective study of patients with HCC undergoing curative RFA, no significant difference in recurrence or overall survival was found between DM and non-DM groups. However, the DM group had a shorter follow-up duration and a higher mortality rate, suggesting a possible trend toward poorer prognosis. The lower recurrence rate in the DM group may be underestimated due to early death or limited follow-up. Our sample size and number of events were limited, which may have reduced statistical power. Despite these limitations, consistent inclusion criteria and standardized treatment strengthen the internal validity of our findings. Further studies with larger cohorts and longer follow-up are needed to clarify the impact of DM on HCC prognosis.
P.035
IMPACT OF IMMEDIATE TRANSARTERIAL EMBOLIZATION (TAE) ON PROGNOSIS OF HEPATOCELLULAR CARCINOMA (HCC) RUPTURE AND HEMORRHAGE IN THE EMERGENCY DEPARTMENT: A RETROSPECTIVE COHORT STUDY
Chia-Lun Liu, Hsuan-Hwai Lin
Division of Gastroenterology, Department of Internal Medicine, Tri-Service General Hospital, Taipei, Taiwan
肝細胞癌破裂病患接受即時與延遲動脈 栓塞治療之臨床預後比較:回溯性研究 劉家綸 林煊淮 三軍總醫院胃腸科
Background: Hepatocellular carcinoma (HCC) rupture is a life-threatening emergency with high early mortality. Transarterial embolization (TAE) has emerged as the preferred intervention to achieve hemostasis. However, the impact of TAE timing— especially immediate versus delayed embolization— on clinical outcomes remains under debate.
Aims: To compare the clinical outcomes of immediate TAE (<6 hours), delayed TAE (>6 hours), and nonembolization management in patients presenting with ruptured HCC in the emergency department (ED), focusing on mortality and complication rates.
Methods: This retrospective cohort study included adult patients (≥18 years) with confirmed HCC rupture and hemorrhage diagnosed by contrastenhanced imaging. Patients were categorized into three groups based on treatment: immediate TAE, delayed TAE, and other management (conservative or surgery without embolization). Primary outcome was in-hospital mortality; secondary outcomes included 30-day and 90-day mortality, major complications, and 1-year survival. Statistical analyses included Kaplan-Meier survival curves, chisquare tests, and Cox proportional hazards models adjusting for clinical covariates.
Results: Both immediate and delayed TAE groups demonstrated significantly lower in-hospital and 90-day mortality compared to the non-embolization group (p < 0.05). No statistically significant difference in survival was observed between the immediate and delayed TAE groups (p > 0.05). Similarly, complication
rates—including rebleeding, infection, and acute kidney injury—were comparable between the two TAE groups, and lower than in the non-embolization cohort. Cox regression analysis confirmed that TAE, regardless of timing, was independently associated with improved survival.
Conclusions: Immediate and delayed transarterial embolization offer comparable survival outcomes and complication profiles in the management of ruptured HCC. Compared to non-embolization strategies, both TAE approaches significantly improve prognosis, supporting the importance of embolization regardless of time-to-treatment when feasible.
P.036
DISCLOSING THE POTENTIAL THERAPEUTIC EFFECT OF PROBIOTIC- BACTEROIDES EGGERTHII ON FATTY LIVER DISEASE: A MOUSE MODEL STUDY
Kun-Feng Wu1, Li-Wei Chen1, I-Wen Wu4, Shih-Ci Su5, Liang-Che Chang3, Tzu-Chien Cheng3, Cheng-Kai Syu2
1Department of Gastroenterology and Hepatology Chang-Gung Memorial Hospital and University at Keelung 2Department of Nephrology, Chang-Gung Memorial Hospital and University at Keelung 3Department of Pathology, Chang-Gung Memorial Hospital and University at Keelung 4Division of Nephrology, Department of Internal Medicine, Taipei Medical University Hospital, Taipei
5Core Laboratory for Human Whole-Genome Disease Research Chang-Gung Memorial Hospital
探討益生菌 Bacteroides eggerthii 對脂肪
肝之潛在治療效果:小鼠模式研究 吳坤峯1 陳立偉1 吳逸文4 蘇仕奇5 張良慈3 鄭子謙3
許程凱2
1 基隆長庚紀念醫院胃腸肝膽胰內科
2 基隆長庚紀念醫院腎臟內科
3 基隆長庚紀念醫院病理科
4 台北醫學大學附設醫院腎臟內科
5 基隆長庚紀念醫院人類全基因體疾病研究核心實驗 室
Background: The gut microbiota has been demonstrated to closely correlate with the occurrence and development of many human diseases, including obesity, diabetes and metabolicdysfunction associated steatotic liver disease (MASLD). Many factors related to a disrupted gut microbiome, including the increased intestinal permeability, the altered bile acid metabolism, and the lipopolysaccharide (LPS)-activated low-grade inflammation, are involved in the pathogenesis of MASLD. The signaling in the gut-liver axis is a potential target for designing drugs against MASLD. Bacteroides eggerthii (B. eggerthii) has been found to contribute to lipopolysaccharide and secondary bile acid biosynthesis, which may influence the
development of fatty liver disease or steatohepatitis by regulating inflammatory reactions and steatosis formation. Bacteroides were found to be depleted in high fat high cholesterol diet-fed mice, which was corroborated in human hypercholesteremia patients.
Aims: In this study, we evaluated the therapeutic effects of B. eggerthii, on steatohepatitis in high fat diet (HFD)-fed mice and try to identify a beneficial gut-liver axis for the treatment of MASLD.
Methods: From March, 2023 to February, 2025, the commercial product of B. eggerthii and male C57BL/6 mice were used. Multiplex immunoassay cytokines analysis was applied. We examined the profile of serum cytokines/chemokines, and histological immunohistochemical (IHC) quantitative analyses, including Ki67 (cell proliferation), CK18 (apoptosis), LC3B (autophagy) and 4 HNE (oxidative stress) staining.
Results: Higher mean values of body weight, plasma BUN, cholesterol, triglycerides, TNF-α, IL-1β, IL-18, IP-10, MCP-3, and leptin were found in mice of the HFD group compared to those fed a normal chow diet. After B. eggerthii gavage, there were no significant differences in cytokine levels between mice in the normal chow diet group. However, in HFD-fed mice, the mean levels of TNF-α, IL-1β, and IL-18 were lower after B. eggerthii gavage. A higher mean value of IP-10, but no significant differences in MCP-3 and leptin, were observed after B. eggerthii gavage. Histologically, prominent hepatic steatosis and higher inflammatory scores were found in the livers of HFD-fed mice compared to those on normal chow. However, no statistical difference in liver fibrosis was noted by trichrome staining. There were no significant differences in quantitative immunohistochemical analyses of Ki-67, CK18, or LC3B, regardless of B. eggerthii gavage. Only 4-HNE staining was significantly lower in HFD-fed mice treated with B. eggerthii compared to untreated mice.
Conclusions: High-fat diet (HFD) feeding in mice induced increases in body weight, cholesterol, triglycerides, and proinflammatory cytokines. After B. eggerthii gavage, lower mean levels of TNF-α, IL-1β, and IL-18 were observed in HFD-fed mice. In addition, 4-HNE staining was reduced in HFD-fed mice treated with B. eggerthii compared to those without treatment. However, no significant differences were found in other immunohistochemical markers, including Ki-67, CK18, and LC3B. The decrease in 4-HNE may reflect reduced oxidative stress following B. eggerthii administration.
P.037
LIFESTYLE FACTORS AND FATTY LIVER DISEASE: A FIVE-YEAR ANALYSIS FROM A MAJOR HEALTH EXAMINATION CENTER IN TAIWAN
Hsin-Yi Chen1, Ting-Shuo Chen3, Hsiu-Tzu Hsieh3, YiH-Sien Kuo3, Chih-Sheng Hung1, Chih-Sheng Hung1,2, Jui-Ting Hu1,2, Sien-Sing Yang1, 2
1Division of Digestive Medicine, Cathay General Hospital Medical Center, Taipei, Taiwan 2School of Medicine, College of Medicine, FuJen Catholic University, New Taipei City, Taiwan 3Cathay Healthcare Management Co., Ltd., Taipei, Taiwan
生活型態因素與脂肪肝疾病之關係:臺 灣主要健康管理中心的五年分析 陳信宜1 陳丁碩3 謝秀梓3 郭怡賢3 黃鼎鈞1 洪志聖1,2 胡瑞庭1,2 楊賢馨1, 2
1 國泰綜合醫院消化內科
2 輔仁大學醫學系
3 國泰健康管理顧問股份有限公司
Background: Fatty liver disease (FLD) is a rising public health concern globally. But multiple factors were very complex in FLD.Lifestyle habits are shifting rapidly, coinciding with increasing rates of metabolic syndrome and liver disease in Taiwan.
Aims: This study aims to collect the association between lifestyle behaviors and FLD prevalence based on a large-scale health examination program from a major health examination center.
Methods: From 2019 to 2023, we collected who 566,199 individuals underwent health examinations, of which 514,147 had valid ultrasound data. Among them, 366,421 participants consented to research. FLD was classified into mild, moderate, and severe by abdominal sonography. Logistic regression and chisquare tests were used to analyze the relationship between FLD and lifestyle variables, including alcohol consumption, exercise, sleep duration, smoking, and betel nut chewing.
Results: The overall FLD prevalence was 48.5%, with 26.68% mild, 18.07% moderate, and 3.75% severe. FLD prevalence increased with age and was higher in males across all age groups. Significant associations were found between FLD and the following lifestyle behaviors: lack of physical activity (OR = 0.69 to
0.40), short sleep duration (<6 hours; OR = 1.13 to 1.22), smoking (OR=1.65), betel nut chewing (OR = 2.74), and daily alcohol use (confounding effects observed in severe cases). A model using only lifestyle variables achieved an AUC-ROC of 0.8606, indicating strong predictive power.
Conclusions: 1. This study appeared the critical role of lifestyle in the development and progression of FLD. 2. We should prioritize health education campaigns that promote regular exercise, adequate sleep, smoking cessation, and the reduction of betel nut use on public health policies in Taiwan. 3. We should support the implementation of communitylevel interventions to combat the growing burden of FLD.
P.038
PLASMA AMMONIA AS A PROMISING BIOMARKER OF ALTERING IMMUNOMETABOLISM: A 4-YEAR PROSPECTIVE CASECONTROL STUDY OF STEATOTIC LIVER DISEASE
Yu-Jhou Chen1, Ming-Ling Chang2,3
1Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital at Linkou, Taoyuan, Taiwan
2Division of Hepatology, Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital at Linkou, Taoyuan, Taiwan
3Department of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan
血漿氨為免疫代謝異常的潛力生物標 記:一為期 4 年的脂肪肝前瞻性病例對 照研究
陳昱州1 張明鈴2,3
1 林口長庚紀念醫院胃腸肝膽科系
2 林口長庚紀念醫院胃腸肝膽科系肝臟科
3 長庚大學醫學系
Background: Elevated plasma ammonia is associated with systemic toxicity in advanced liver disease. However, the clinical significance of plasma ammonia of the disease severity and outcomes in patients with steatotic liver disease (SLD) remains elusive.
Aims: We aimed to address the above knowledge gap.
Methods: A 4-year prospective case-control study of SLD was conducted in a tertiary care center. Results: Of 513 enrolled patients, 257 (50.1%) were men and 413 (80.5%) had SLD. Higher plasma ammonia levels were noted in patients with than those without SLD (60.9 ± 26.6 vs. 54.2 ± 23.8 μg/ dL, p=0.001). Baseline levels of homeostatic model assessment for insulin resistance (ß: 0.587; 95%CI ß: 0.064 ~ 1.109), mean corpuscular volume (-0.725; -1.147 ~ -0.303), mean corpuscular hemoglobin concentration (4.648; 1.830 ~ 7.466), and platelet count (0.066; 0.024 ~ 0.108) were associated with baseline ammonia levels. Ammonia levels paralleled with both the severity of SLD [ammonia levels: no SLD, 54.2 ± 23.8 μg/dL; mild-moderate SLD, 60.2
± 26.2 μg/dL; severe SLD, 69.3 ± 30.8 μg/dL, p < 0.001] and the scores of cardiometabolic risk factors (CMRFs) [CMRF (0-2), 55.3 ± 23.6 μg/dL; CMRF (3-4), 59.6 ± 26.9 μg/dL; CMRF (5), 64.4 ± 27.2 μg/dL; p < 0.001]. Longitudinally, ammonia levels decreased (53.6 ± 24.6 vs. 65.6 ± 30.0 μg/dL, p < 0.001) in patients with improved SLD severity, while elevated ammonia levels were associated with infectionrelated events (OR: 1.018; 95%CI OR: 1.001 ~ 1.036, p = 0.004).
Conclusions: Insulin resistance and hematologic indices were associated with plasma ammonia levels, which parallel the SLD severity and CMRF scores. The longitudinal changes of ammonia levels correlated with the SLD progression and the presence of infected events. These findings highlight plasma ammonia as a promising biomarker of altering immunometabolism and the associated diseases, particularly in patients with SLD.
P.039
EFFICACY OF JING SI HERBAL TEA IN NON-ALCOHOLIC FATTY LIVER DISEASE: A DOUBLEBLIND, RANDOMIZED, PLACEBOCONTROLLED STUDY
Kuan Fu Liao1, Cheng-Chan Yu2,3, Sheng-Chun Chiu4,5,6
1Division of Hepato-gastroenterology, Department of Internal Medicine, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwan
2Division of General Surgery, Department of Surgery, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwan
3Graduate Institute of Integrated Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan
4Department of Research, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwan
5Department of Laboratory Medicine, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwan
6Division of Basic Medical Sciences, College of Nursing, Tzu Chi University, Hualien, Taiwan
淨斯本草飲對非酒精性脂肪肝的療效: 一個雙盲隨機化對照研究
廖光福1 余政展2,3 邱勝軍4,5,6
1 台中慈濟醫院消化系內科
2 台中慈濟醫院一般外科
3 中國醫藥大學中西醫結合研究所
4 台中慈濟醫院研究部
5 台中慈濟醫院醫學檢驗部
6 慈濟大學護理學院
Background: Non-alcoholic fatty liver disease (NAFLD), as the population suffering from obesity gradually increases, has become the most common liver disease in developed and developing countries. The global prevalence of NAFLD is now around 25%, growing rapidly about 30% in Taiwan. NAFLD has a higher prevalence rate in patients with metabolic syndrome, diabetes, dyslipidemia, and obesity. Despite the most efficient treatments are weight loss and exercise, pharmacological strategies are still urgently needed. Thus, developing a natural compound that can prevent or treat NAFLD has
become an importantarea of research.
Aims: This study aims to explore the effects of Jing Si Herbal tea (JSHT) on reducing blood cholesterol levels, alleviating NAFLD symptoms, and regulating energy balance in lipid synthesis and metabolism.
Methods: Adults with NAFLD but without other hepatitis disease were included. Participants underwent physical evaluations, pre-treatment blood sampling, and were randomly assigned to JSHT or placebo groups for 24 weeks. Post-treatment, blood sampling and evaluations were done. NAFLD activity scores and liver steatosis grading were evaluated and ranked by abdominal ultrasound.
Results: 70 patients (median age 54 years, range 20–67 years, 74.3% female) were studied. Both JSHT and placebo groups were similar at baseline. No significant differences were observed between the two groups for AST, ALT, total cholesterol, TG, HDL-C and LDL-C. However, the JSHT group showed a trend toward lower NAFLD activity scores (P = 0.042) and liver steatosis grading (P = 0.01) than the placebo group (within-group difference).
Conclusions: After 24 weeks of treatment, the JSHT group showed improvement in NAFLD activity scores and liver steatosis grading compared to the placebo group. This study suggests that JSHT has potential therapeutic role in patients with NAFLD.
P.040
EXTRAHEPATIC MANIFESTATIONS OF METABOLIC DYSFUNCTIONASSOCIATED STEATOTIC LIVER DISEASE
Chia-Hsun Tsai1, Tuck-Siu Wong1, Chung-Yi Lin1, Chia-Lu Hsu2, Ching-Sheng Hsu1
1Center for Digestive Medicine, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwan
2Department of Medical Research, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwan
Background: Metabolic dysfunctionassociated steatotic liver disease (MASLD) is the most common liver disease worldwide and is closely linked to obesity, insulin resistance, type 2 diabetes, and dyslipidemia. In addition to liver disorders, recent studies have shown a close association between it and extrahepatic disorders.
Aims: We aim to study the association between extrahepatic diseases and MASLD.
Methods: We conducted a narrative review of research papers on the extrahepatic diseases in MASLD and their clinical significance.
Results: MASLD may range from simple steatosis to steatohepatitis (metabolic dysfunctionassociated steatohepatitis), which can progress to fibrosis, cirrhosis, or liver cancer. Beyond liverrelated issues, MASLD is a systemic disease strongly associated with extrahepatic complications such as cardiovascular disease (CVD), chronic kidney disease (CKD), cancers, endocrine disorders, musculoskeletal problems, and sleep apnea. CVD and cancer are the leading causes of death in MASLD patients, with liverrelated mortality ranking third. Fibrosis severity is the key predictor of overall and causespecific mortality. MASLD significantly increases the risk and progression of type 2 diabetes, CVD, and CKD. It is also linked to increased risks of extrahepatic cancers, particularly colorectal, pancreatic, and breast cancers. Endocrine conditions such as hypothyroidism and polycystic ovary syndrome and musculoskeletal disorders, including sarcopenia and osteoporosis,
frequently cooccur with MASLD. Obstructive sleep apnea independently contributes to the severity of liver disease and shares overlapping metabolic pathways. Surgical and transplant outcomes are worse in patients with MASLD due to impaired liver regeneration and increased postoperative risks.
Conclusions: Although the recent approval of resmetirom offers a new therapeutic option, whereas lifestyle changes remain the cornerstone of management. Given the multisystemic impact of MASLD, a patientcentered approach is essential for effective treatment and improved longterm results.
P.041
AMOXICILLIN/VONOPRAZAN/ BISMUTH THERAPY ACHIEVES HIGHER ERADICATION RATE THAN VONOPRAZAN/AMOXICILLIN AND CLARITHROMYCIN/AMOXICILLIN/ RABEPRAZOLE THERAPIES FOR ANTI-H. PYLORI TREATMENT – A PRELIMINARY REPORT
Wei-Lin Chiu1,9, Ping-I Hsu1,9, Ming-Jen Sheu2,9, Chih-An Shih3,9, Chien-Lin Chen4,9, Feng-Woei Tsay5,9, Chao-Hung Kuo6,9, Jyh-Chin Yang7,9, Chang-Bih Shi1,9, Wei-Yi Lei4,9, Sung-Shuo Kao8,9, Tzung-Jiun Tsai5,9, Deng-Chyang Wu6,9
1Division of Gastroenterology, Department of Medicine, Tainan Municipal An Nan Hospital, China Medical University, Tainan, Taiwan
2Division of Hepatogastroenterology, Department of Internal Medicine, Chi Mei Medical Center, Tainan, Taiwan
3Division of Gastroenterology and Hepatology, Department of Internal Medicine, Antai Medical Care Corporation, Antai Tian-Sheng Memorial Hospital, Pingtung, Taiwan
4Division of Gastroenterology and Hepatology, Department of Internal Medicine, Hualien Tzu Chi Hospital, Hualien, Taiwan
5Division of Gastroenterology and Hepatology, Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
6Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
7Division of Gastroenterology, Department of Internal Medicine, Hospital and College of Medicine, National Taiwan University, Taipei, Taiwan
8Division of Gastroenterology, Department of Internal Medicine, Pingtung Veterans General Hospital, Pingtung, Taiwan
9Taiwan Acid-related Disease & Microbiota (TARD-M) Consortium 「 Amoxicillin/Vonoprazan/Bismuth 三 合療法」之幽門螺旋桿菌除菌除菌率
邱魏嶙1,9 許秉毅1,9 許銘仁2,9 石志安3,9 陳健麟4,9
蔡峯偉5,9 郭昭宏6,9 楊智欽7,9 施長碧1,9 雷尉毅4,9
高崧碩8,9 蔡騌圳5,9 吳登強6,9
1 臺南市立安南醫院消化內科
2 奇美醫院胃腸肝膽科
3 安泰醫院胃腸肝膽科
4 花蓮慈濟醫院肝膽腸胃科
5 高雄榮民總醫院胃腸肝膽科
6 高雄醫學大學附設醫院胃腸內科
7 國立臺灣大學醫學院附設醫院胃腸肝膽科
8 屏東榮民總醫院胃腸肝膽科
9 台灣胃酸相關疾病暨微菌叢聯盟
Background: Vonoprazan–amoxicillin dual therapy offers a compelling advantage over traditional multi-antibiotic regimens such as bismuth quadruple, concomitant, hybrid, and clarithromycincontaining triple therapies for H. pylori eradication from the perspectives of antibiotic stewardship and environmental sustainability. However, the efficacy of high-dose vonoprazan–amoxicillin dual therapy varies across countries. Recently, we developed a novel high-dose vonoprazan–amoxicillin–bismuth triple therapy that achieved an eradication rate of ≥95%.
Aims: To compare the efficacy of 14-day vonoprazan–amoxicillin–bismuth triple therapy, vonoprazan–amoxicillin dual therapy, and clarithromycin–amoxicillin–rabeprazole standard triple therapy as first-line treatments for H. pylori infection.
Methods: In this multicenter, randomized, openlabel trial, adult patients with H. pylori infection were enrolled from seven centers across Taiwan. Participants were randomly assigned (1:1:1) to receive one of the following regimens for 14 days: high-dose vonoprazan–amoxicillin–bismuth triple therapy, high-dose vonoprazan–amoxicillin dual therapy, or clarithromycin–amoxicillin–rabeprazole standard triple therapy. The primary outcome was the H. pylori eradication rate, assessed in the modified intention-to-treat population.
Results: Between November 2023 and April 2025, a total of 360 patients were recruited. The prevalence of antibiotic resistance among H. pylori strains was 1.9% for amoxicillin, 26.3% for clarithromycin, 21.0% for metronidazole, and 4.9% for tetracycline. In the modified intention-to-treat analysis, the eradication rate was 98.4% (115/117) in the vonoprazan–
amoxicillin–bismuth triple therapy group, 87.2% (102/117) in the vonoprazan–amoxicillin dual therapy group, and 87.1% (101/116) in the clarithromycin–amoxicillin–rabeprazole standard triple therapy group. Vonoprazan–amoxicillin–bismuth triple therapy demonstrated significantly higher efficacy than vonoprazan–amoxicillin dual therapy (Difference: 11.1%; 95% confidence interval: 4.7% to 17.7%; p < 0.001). It was also superior to clarithromycin–amoxicillin–rabeprazole triple therapy (Difference: 11.3%; 95% confidence interval: 4.7% to 17.7%; p < 0.001). The incidence of adverse events was comparable across groups (10.0%, 9.2%, and 17.5%, respectively), as was drug adherence (96.7%, 95.8%, and 95.8%, respectively).
Conclusions: Fourteen-day vonoprazan–amoxicillin–bismuth triple therapy achieved a significantly higher eradication rate than both vonoprazan–amoxicillin dual therapy and clarithromycin-based triple therapy. Importantly, it aligns with key principles of antibiotic stewardship by minimizing antibiotic overuse and reducing ecological and microbiological harm.
P.042 IS A NEGATIVE FECAL IMMUNOCHEMICAL TEST REASSURING? THE CUMULATIVE RISK OF COLORECTAL CANCER AFTER MULTIPLE NEGATIVE
Chien-Hua Chen, Chi-Chieh Yang, Kwei-Ming Chen
Division of Gastroenterology, Department of Internal Medicine, Show Chwan Memorial Hospital, Changhua, Taiwan
糞便潛血陰性反應是否可以保證沒有大 腸癌
陳建華 楊基滐 陳奎閔 秀傳紀念醫院胃腸肝膽科
Background: Colorectal cancer (CRC) risk is approximately 0.1% based on registry data, and fecal immunochemical tests (FITs) identify about 5% of screened individuals as positive.
Aims: To evaluate whether a negative FIT result is reassuring regarding CRC risk and to assess the CRC and all-cause mortalities after multiple FITs.
Methods: This retrospective cohort study enrolled 141,982 Taiwanese individuals aged ≥50 who underwent self-paid medical screening from 1994 to 2008. CRC cases and all-cause deaths were identified through the National Cancer Registry and National Death File. A negative FIT was defined as <20 μg Hb/g.
Results: There were 987 CRC cases following a negative FIT and 713 following a positive FIT. Among 133,369 individuals with one negative FIT, 113 CRC cases were registered within two years and 803 within ten years; only 15% occurred within the first two years. The overall incidence was 1.27/1,000 person-years, decreasing by 63% to 0.80/1,000 person-years after one negative FIT. With repeated biennial negative FITs, CRC risk declined to 63%, 53%, 33%, 23%, and 10% over ten years. All-cause mortality decreased from 1,106/100,000 personyears to 511/100,000 person-years. Notably, 84% of the cohort had consistently negative FIT results across five rounds.
Conclusions: Two-thirds of the ten-year CRC risk remained in individuals following one negative FIT. The risk after a negative FIT result emerged after two years, highlighting the importance of continuing biennial FIT screening. Consistently negative FITs
were associated with reduced CRC risk and a lower all-cause mortality. This study is limited by the lack of confirmatory colonoscopy in FIT-negative individuals, which may lead an underestimation of CRC incidence.
P.043
IMPACT OF CLINICALLY SIGNIFICANT PORTAL HYPERTENSION ON SURVIVAL IN PATIENTS WITH CHOLANGIOCARCINOMA: A COHORT STUDY FROM TAIWAN
Ying-Fan Chen, Yu-Jen Chen
Division of Gastroenterology and Hepatology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
臨床顯著性門脈高壓對膽道癌患者存活 影響之探討:一項臺灣回溯性世代研究
陳膺帆 陳宥任
臺北榮民總醫院胃腸肝膽科
Background: Cholangiocarcinomas (CCAs) are aggressive malignancies with increasing global incidence and mortality. In Taiwan, the rise in CCA has been notable, even among younger populations. Despite advances in systemic therapy and selective use of liver transplantation or locoregional treatments, the prognosis remains poor, largely due to late presentation and limited curative options. Clinically significant portal hypertension (CSPH), frequent relevant to complications such as ascites, varices and thrombocytopenia, reflects impaired hepatic reserve and is common in cirrhotic patients. However, its prognostic significance in CCA remains unclear.
Aims: To investigate the impact of CSPH on overall survival (OS) in patients with CCA.
Methods: We retrospectively analyzed 841 patients with histologically confirmed CCA at Taipei Veterans General Hospital (2013–2024). CSPH was defined by the presence of at least one of the following: moderate ascites, esophageal varices, or splenomegaly with thrombocytopenia. Demographic, laboratory, and clinical data were compared between CSPH and non-CSPH groups. OS was estimated using KaplanMeier analysis and evaluated using Cox proportional hazards models. Subgroup analyses were conducted based on tumor location (iCCA vs. eCCA), surgical status, and disease stage.
Results: Among the 841 patients, 194 (23%) had CSPH. Compared with non-CSPH patients, those with CSPH were more likely male (64.9% vs. 57.0%, p = 0.049) and had worse liver function parameters, including lower platelet count (184K vs. 224K/
μL, p < 0.001), higher INR (1.14 vs. 1.08, p < 0.001), lower albumin (3.65 vs. 3.80 g/dL, p = 0.001), higher total bilirubin (1.04 vs. 0.75 mg/dL, p = 0.001), and elevated FIB-4 score (3.08 vs. 2.08, p < 0.001). Fewer CSPH patients underwent surgery (26.8% vs. 38.3%, p = 0.03). After a median follow-up of 374 days, 293 deaths occurred. Median OS was significantly shorter in the CSPH group (260 vs. 412 days, p < 0.001). Subgroup analysis showed CSPH was associated with poor survival in both iCCA and non-surgical patients. Multivariate Cox analysis identified CSPH, high FIB-4 (>2.67), ALBI grade 2/3, eCCA, late tumor stage, non-surgical treatment, and Child-Pugh B/C as independent predictors of worse survival.
Conclusions: CSPH is an independent predictor of poor survival in patients with CCA and is associated with reduced surgical eligibility. Incorporating CSPH into routine prognostic evaluation may enhance risk stratification and guide treatment decisions. Prospective studies are warranted to confirm these findings and develop targeted strategies for this high-risk subgroup.
P.044
MOLECULAR FEATURES OF INTERVAL CANCER AFTER A NEGATIVE FECAL IMMUNOCHEMICAL TEST: ANALYSIS OF SAMPLING DATA FROM TAIWAN COLORECTAL CANCER SCREENING PROGRAM
Te-Yao Hsueh1, Wen-Feng Hsu1, Kai-Sheng Liao2, Chu-Kuang Chou2, Pi-Chun Chuang1, Yen-Nien Chen3, Li-Chun Chang1, Ming-Shiang Wu1, Han-Mo Chiu1
1Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
3Department of Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
糞便免疫潛血檢測陰性後間隔大腸直腸 癌之分子特徵:臺灣大腸直腸癌篩檢計
畫之樣本分析
薛德曜1 許文峰1 廖凱聖2 周莒光2 莊弼鈞1 陳彥年3
張立群1 吳明賢1 邱瀚模1
1 台大醫院內科部
2 嘉義基督教醫院內科部
3 台大醫院癌醫分院內科部
Background: Fecal immunochemical test (FIT) interval cancers (IC) occur when colorectal cancer (CRC) develops after a negative FIT result, reducing the overall effectiveness of screening programs as IC are more advanced in stage. Previous research has shown that FIT has significantly lower sensitivity for detecting sessile serrated lesions (SSLs) than for conventional adenomas. The serrated pathway has distinct molecular characteristics involving two mechanisms: BRAF mutations and the CpG island methylator phenotype (CIMP), both linked to Consensus Molecular Subtype 1 (CMS1). Whether CMS1 CRCs are more likely to contribute to FIT IC, however, remains unclear.
Aims: This study aims to compare the clinical and molecular features of FIT IC and screening-detected CRCs within the Taiwan CRC Screening Program, focusing on their differences in CMS category.
Methods: In this case-control study, we identified
FIT ICs within the Taiwan CRC Screening Program between 2015 and 2019 and linked to the screening database at the screening hubs located in northern (National Taiwan University Hospital) and southern (Chia-Yi Christian Hospital) Taiwan. Those FIT interval cancer diagnosed and treated in these two centers were included in this study. Age- and gendermatched screening-detected CRCs were selected as control groups also from the same centers. Adequate DNA was isolated from paraffin-embedded cancer specimens. Whole-exome sequencing (WES) was conducted to analyze mutations in genes implicated in CRC, and methylation analysis was performed to assess methylation status.
Results: A total of 118 FIT ICs and 106 cases of screening-detected CRCs were included. Significant differences were observed in tumor location, with FIT interval cancers more frequently located in the proximal colon compared to screening-detected CRCs (p < 0.001). Molecular analysis revealed that CIMP-high status, microsatellite instability (MSI), and BRAF mutations, the key features of CMS1, were significantly more common in FIT interval cancers than in screening-detected CRCs (CIMP-high: 81.9% vs. 29.5%, p < 0.0001; MSI: 67.5% vs. 9.6%, p < 0.0001; BRAF mutations: 39.8% vs. 4.9%, p < 0.001). Somatic copy number alteration (SCNA)-high, associated with CMS2 and CMS4, was more prevalent in screening-detected CRCs (86% vs. 22%, p < 0.001). KRAS mutations, characteristic of CMS3, showed no significant difference between these two groups (p = 0.52). Additionally, the proportion of gene mutations linked to CRC progression, including GOLGA6L9, TRPM4, PNPLA7, and ZC3H13, were significantly higher in FIT ICs.
Conclusions: FIT ICs have distinct molecular characteristics linked to CMS1, indicating a greater likelihood of aggressive molecular pathways, which is consistent with clinical observation and previous research. Furthermore, there are some specific gene mutations that were significantly more common in FIT ICs, suggesting unique mechanisms of progression.
P.045
GUT MICROBIAL SIGNATURES OF INFLAMMATORY BOWEL DISEASE: A TAIWANESE COHORT
Yun-Chu Chen1, Chia-Hung Tu1, Yen-Nien Chen3, Yu-Ting Kuo2, Ming-Lun Han2, Ping-Huei Tseng1, Han-Mo Chiu1, Ming-Shiang Wu1, Chieh-Chang Chen1
1Department of Internal medicine, National Taiwan University Hospital, Taipei, Taiwan
2Department of Integrated Diagnostics & Therapeutics, National Taiwan University Hospital, National Taiwan University, Taipei, Taiwan
3Department of Internal Medicine, National Taiwan University Cancer Center, Taipei, Taiwan 發炎性腸道疾病的腸道菌叢特徵:台灣 族群研究
陳韻竹1 凃佳宏1 陳彥年3 郭雨庭2 韓明倫2 曾屏輝1 邱瀚模1 吳明賢1 陳介章1
1 國立臺灣大學醫學院附設醫院內科部
2 國立臺灣大學醫學院附設醫院綜合診療部
3 國立臺灣大學醫學院附設醫院癌醫中心分院綜合內 科部
Background: Inflammatory Bowel Disease (IBD), encompassing Crohn’s Disease (CD) and Ulcerative Colitis (UC), is a chronic inflammatory condition of the gastrointestinal tract. The incidence of IBD is rising in newly industrialized regions, including Taiwan. Gut microbiota dysbiosis is recognized as a key factor in IBD pathogenesis, but studies characterizing these microbial imbalances in Asian patient cohorts remain limited.
Aims: This study aimed to characterize the gut microbial signatures of IBD in a Taiwanese cohort, identify specific bacterial taxa associated with IBD, and distinguish between IBD subtypes and healthy controls using high-throughput sequencing.
Methods: We collected fecal samples from patients with IBD (n = 98; 51 UC, 47 CD) and healthy controls (n = 57). Bacterial genomic DNA was extracted, and the V3-V4 hypervariable regions of the 16S rRNA gene were amplified and sequenced. The QIIME2 pipeline was used for data processing, and taxonomy was assigned using the SILVA 138 database. Alpha diversity was calculated, and Linear Discriminant Analysis Effect Size (LEfSe) was employed to identify
differentially abundant microbial taxa between groups.
Results: IBD patients exhibited significantly lower alpha diversity compared to healthy controls, with a more pronounced reduction in CD. LEfSe analysis revealed a significant depletion of butyrateproducing Firmicutes, such as Faecalibacterium and Roseburia, in the IBD cohort. Conversely, there was a marked enrichment of pro-inflammatory taxa, including Escherichia-Shigella, Streptococcus, and other members of the Proteobacteria phylum in IBD patients. Distinct microbial signatures were also identified between UC and CD, highlighting different pathophysiological microbial shifts.
Conclusions: Taiwanese IBD patients demonstrate significant gut microbial dysbiosis, characterized by a loss of beneficial, butyrate-producing bacteria and an expansion of potentially proinflammatory organisms. These findings enhance our understanding of IBD pathogenesis in this specific population and underscore the potential for microbial-based diagnostic and therapeutic strategies.
P.046
TEMPORAL RISK MODELING OF COLORECTAL POLYP FORMATION ASSOCIATED WITH METABOLIC SYNDROME: EVIDENCE FROM A LARGE-SCALE TAIWANESE HEALTH SCREENING COHORT
Ting-Shuo Chen1, Ting-Chun Huang2, Hsiu-Tzu Hsieh1, Chi-Jung Huang3, Chih-Sheng Hung2, Cheng-Yu Hung4, Yi-Hsien Kuo1
1Cathay Healthcare Management Co., Ltd., Taipei, Taiwan
2Division of Gastroenterology and Hepatology, Department of Internal Medicine, Cathay General Hospital, Taipei, Taiwan
3Department of Medical Research, Cathay General Hospital, Taipei, Taiwan
4Cathay General Hospital, Taipei, Taiwan
代謝症候群與大腸瘜肉形成之時間序列 風險分析:臺灣健檢族群的大規模實證 研究
陳丁碩1 黃鼎鈞2 謝秀梓1 黃紀榕3 洪志聖2 洪正昱4 郭怡賢1
1 國泰健康管理顧問股份有限公司
2 國泰綜合醫院消化內科
3 國泰綜合醫院醫學研究部
4 國泰綜合醫院
Background: Colorectal polyp, particularly adenomatous type, is a precancerous lesion that may progress to colorectal cancer (CRC) over 10–15 years. While colonoscopic removal reduces the incidence and mortality of CRC, current surveillance remains largely age-driven. Metabolic syndrome (MetS)—a cluster of risk factors including abdominal obesity, high blood pressure, high blood sugar, high triglycerides, and low high-density lipoprotein (HDL) cholesterol—is increasingly prevalent and associated with a 30%–40% elevated risk of CRC and polyps. However, most prior studies are cross-sectional, limiting insight into the temporal sequence of metabolic dysfunction and polyp formation. With rising rates of early-onset CRC and expanding preventive check-up systems in Asia, realworld, time-sensitive evidence is urgently needed. This study leverages a large Taiwanese screening cohort to examine time-dependent associations
between MetS (and its components) and colorectal polyp risk, stratified by age and sex. The findings aim to inform risk-adapted surveillance strategies that extend beyond age-based thresholds.
Aims: This study aimed to investigate the longitudinal relationship between metabolic syndrome (MetS) and the development of colorectal polyps in a large Taiwanese health screening cohort. Specific objectives were to: (1) Quantify the time-dependent risk of colorectal polyp formation associated with MetS using Cox proportional hazards models. (2) Disaggregate the contributions of individual MetS components—particularly abdominal obesity and hypertriglyceridemia—as independent risk factors. (3) Identify high-risk subgroups by examining ageand sex-specific risk gradients, with a focus on younger adults who may be missed by age-based screening. By aligning with real-world preventive care workflows, this study supports the development of scalable, precision-guided surveillance models for the early detection of neoplasia.
Methods: This retrospective cohort study analyzed 75,188 adults (mean age 42.48 years, 55.89% male, 44.11% female) who underwent metabolic and colonoscopic screening at Cathay Health Management centers (2019–2023). Participants with incomplete colonoscopy or suspected malignancy were excluded. Metabolic syndrome (MetS) was defined per national criteria (≥3 of abdominal obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL cholesterol). The primary outcome was the detection of first-time colorectal polyps via colonoscopy. A time-to-event framework was employed to model the temporal relationship between metabolic risk and polyp development. Follow-up began at the initial screening or the onset of MetS and ended at the first polyp diagnosis or the last check-up. Cox proportional hazards models were used to estimate hazard ratios, adjusted for age and sex. We conducted additional models to assess the independent effects of each MetS component and stratified risks by age and sex to reveal subgroupspecific trajectories. A reverse-time model was used to assess potential reverse causality. Analyses were performed in Python with significance set at p < 0.05.
Results: Among 75,188 adults screened between 2019 and 2023, 23,768 individuals (31.6%) were diagnosed with colorectal polyps. In adjusted Cox models, metabolic syndrome (MetS) was associated with a 35% increased hazard of polyp development
(HR = 1.35, 95% CI: 1.31–1.39, p < 0.005), with moderate model discrimination (C-index = 0.67).
Male sex (HR = 1.46) and older age (HR = 1.03 per year) were also significant predictors. Stratified analyses revealed a U-shaped association between MetS and polyp risk, with the strongest associations observed in individuals under 30 years old (HR = 1.57) and those over 70 years old (HR = 1.46). Males < 30 years old showed the highest risk (HR = 1.58), whereas the association in females <30 years old did not reach significance. Component analysis showed abdominal obesity (HR = 1.22) and elevated triglycerides (HR = 1.15) as the strongest independent predictors. These risks were highest in females <30 years old (HR = 1.72 for abdominal obesity, 1.72 for triglycerides) and males ≥70 years old (HR = 1.66 for triglycerides). Reverse-time analysis indicated no significant association between prior polyps and later MetS onset (HR ≈ 1.2 × 10⁹, p = 0.82), supporting the directionality of MetS → polyp development.
Conclusions: This large-scale, time-to-event analysis demonstrates that metabolic syndrome (MetS) is a consistent, time-dependent risk factor for colorectal polyp development—particularly among adults under 30 and over 70 years of age. Abdominal obesity and hypertriglyceridemia emerged as the strongest metabolic drivers, reinforcing the importance of visceral adiposity and lipid dysregulation in early neoplastic changes. This study supports a shift away from age-based screening toward metabolically informed surveillance and earlier, more personalized colorectal cancer prevention strategies, especially in younger populations with rising metabolic burdens.
P.047
METABOLIC SYNDROME AND COLORECTAL ADENOMA IN ADULTS UNDER 50 YEARS OLD: A DATADRIVEN ANALYSIS OF HEALTH EXAMINATION DATA FOR HEALTH PROMOTION
Hsiu-Tzu Hsieh1, Ting-Chun Huang2, Ting-Shuo Chen1, Chi-Jung Huang3, Cheng-Yu Hung1, Chih-Sheng Hung1
1Cathay Healthcare Management Co., Ltd., Taipei, Taiwan
2Division of Gastroenterology, Cathay General Hospital, Taipei, Taiwan
3Department of Medical Research, Cathay General Hospital, Taipei, Taiwan
健康檢查數據分析在健康促進的運用 探討 50 歲以下成人代謝症候群與大腸腺 瘤的關聯
謝秀梓1 黃鼎鈞2 陳丁碩1 黃紀榕3 洪正昱1 洪志聖1
1 國泰健康管理顧問公司
2 國泰綜合醫院消化內科
3 國泰綜合醫院醫學研究部
Background: Early detection of colorectal polyps and resect them is very important for the prevention of colorectal cancer (CRC). In Taiwan, self-paid health examination mainly serves healthy people and subhealthy individuals, who, due to their higher health literacy and financial support from their employers, leading them to proactively choose colonoscopy screening, thus providing research subjects different from disease cases. We enrolled 38,378 colonoscopy cases from a center of healthcare management from 2021 to 2023, to explore the correlation between colorectal polyps and metabolic syndrome (MetS) and its indicators, the purpose is to provide precise and timely medical advice among high-risk metabolic groups to reduce the possibility of CRC.
Aims: The progression of Early-Onset Colorectal Cancer (EOCRC) has significant socioeconomic impacts on families and society, necessitating proactive prevention and control measures. In Taiwan, the number of new diagnoses of CRC is significantly increasing among those aged 40 to 49 years from previous reports. Starting in 2025, Health administration department of Taiwan aims to increase the screening rate of immunochemical
fecal occult blood tests (iFOBT) and enhance early detection of colorectal polyps. This initiative includes expanding free stool iFOBT screening to individuals aged 45 and those aged 40–44 with a family history of CRC. Based on test results, individuals can opt for further examination through Taiwan’s National Health Insurance or self-paid colonoscopy. We analyzed the health examination data of adults under 50 years old to improve public health literacy and plan colonoscopy screening, with the goal of providing timely and precise medical recommendations for young and high-risk metabolic populations to reduce the likelihood of EOCRC.
Methods: Colorectal adenomas have a higher potential to develop into CRC. The analysis focuses on 38,378 individuals under the age of 50 who underwent colonoscopy at a health examination center in Taiwan between 2021 and 2023. Among them, 20,728 were male and 17,650 were female, with an average age of 37.9 years. Of these, 43.6% (16,739 cases: 9,444 males and 7,295 females) were aged 40 to 49. The study employs descriptive statistics and multivariate logistic regression to analyze the association between metabolic syndrome and the risk indices of colorectal adenomas.
Results: 13.0% of 38,378 cases were hyperplastic polyps, 3,420 cases (8.9%) were adenoma polyps with 66.2% being male and 33.8% being female. A total of 4,516 caese (11.8%) were diagnosed with MetS. Aamong them, 14.0% (633/4,516: 550 males and 83 females) were adenoma-positive. The odds ratio (OR) of adenoma-positive with MetS was 2.009 (95% CI: 1.829–2.207; P < 0.0001) compared without MetS. Elevated triglyceride levels (>150 mg/dL) and high fasting blood glucose (≥100 mg/dL) were associated with an increased adenoma risk, with ORs of 1.893 (95% CI: 1.746–2.052; P < 0.0001) and 1.771 (95% CI: 1.626–1.930; P < 0.0001), respectively. Of 16,739 cases aged 40 to 49, 12.4% (2,079/16,739) had adenomas and 15.7% (2,626/16,739) had MetS. Among those with MetS, 17.1% (450/2,626) also had adenomas, with an OR of 1.733 (95% CI: 1.542–1.948; P < 0.0001). The co-occurrence rate of MetS and adenomas was higher in males (19.3%; 393/2,040) than in females (9.7%; 57/586). Key metabolic syndrome indicators differed by sex, with elevated triglyceride levels (OR = 1.449; 95% CI: 1.287–1.632; P < 0.0001) being a significant factor in males, whereas low high-density lipoprotein cholesterol (HDL-C) (OR = 1.431; 95% CI: 1.171–1.748; P < 0.0001) was more relevant in females.
Conclusions: This study revealed a strong association between metabolic syndrome and the occurrence of colorectal adenomas, potentially correlating positively with the incidence of CRC. Notably, elevated triglyceride levels and high fasting blood glucose significantly increased the risk index for colorectal adenomas in individuals with comorbid metabolic syndrome. Triglycerides emerged as a key indicator in men, while HDL-C was crucial in women observing MetS in the 40–49 age group. Future research could explore the differences in metabolic indicators between genders across various age groups Self-paid health examination organizations using examination data analysis and strive to make health information and services easily accessible, understandable, and applicable to the public, beneficial to the prevention and control of metabolic syndrome and EOCRC in young adult group.
P.048
INTESTINAL ULTRASOUND PREDICTS OUTCOMES IN HOSPITALIZED PATIENTS WITH CLOSTRIDIOIDES DIFFICILEASSOCIATED DIARRHEA
Hsin-Yun Wu1,2, Zhi-Che Chen2, Hung-Yao Lin2,3, Yun-Chu Chen2, Chien-Chih Tung2, Meng-Tzu Weng2,4, Chu-Su Yu5, Yu-Tsung Huang5, Hsiu-Po Wang2, Shu-Chen Wei2
1Department of Internal Medicine, National Taiwan University Hospital Jinshan Branch, New Taipei City, Taiwan
2Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
3Department of Internal Medicine, National Taiwan University Hospital Hsin-Chu Branch, Hsinchu, Taiwan
4Department of Medical Research, National Taiwan University Hospital Hsin-Chu Branch, Hsinchu, Taiwan
5Department of Laboratory Medicine, National Taiwan University Hospital, Taipei, Taiwan
腸道超音波可預測住院之困難梭狀桿菌 感染相關腹瀉患者的預後
吳心耘1,2 陳知澈2 Hung-Yao2,3 陳韻竹2 董建志2
翁孟慈2,4 Yu5 Yu-Tsung5 王秀伯2 魏淑鉁2
1 國立臺灣大學醫學院附設醫院金山分院內科部
2 國立臺灣大學醫學院附設醫院內科部
3 國立臺灣大學醫學院附設醫院新竹臺大分院內科部
4 國立臺灣大學醫學院附設醫院新竹臺大分院醫學研 究部
5 國立臺灣大學醫學院附設醫院檢驗醫學部
Background: Clinical course of Clostridioides difficileassociated diarrhea (CDAD) is heterogeneous. Evidence for intestinal ultrasound (IUS) application on CDAD remains limited.
Aims: We aim to demonstrate serial IUS changes during treatment and establish predictors of clinical outcomes.
Methods: In this prospective observational study, we enrolled hospitalized adults with CDAD from January to December 2024. Diagnosis required ≥3 unformed stools per day and dual positive results of C. difficile glutamate dehydrogenase, toxin A/B, or toxin polymerase chain reaction. IUS was performed
within 48-hours of treatment initiation (D0), then every 3 days. Parameters assessed included bowel wall thickness (BWT), bowel wall flow (BWF), bowel wall stratification (BWS), and inflammatory fat (iFat). Milan ultrasound criteria (MUC) and International Bowel Ultrasound Segmental Activity Score (IBUSSAS) were derived. Unfavorable outcomes included treatment failure and/or recurrence.
Results: Among 53 patients (median age 68, male 56.6%), 88.7% received vancomycin for a median of 10 days. Severe or fulminant disease occurred in 34%.
The median Charlson Comorbidity Index (CCI) was 7. D0 fecal calprotectin was 248.5 µg/g. The median D0 maximal (max) BWT was 3.4 mm, mostly in the sigmoid (46.9%) and descending colon (24.4%). BWF, iFat, and loss of BWS were observed in 42.9%, 10.2%, and 16.3% respectively. Unfavorable outcomes occurred in 30.2%. D0 max BWT (3.0 vs 5.6 mm; p = 0.004), D0 MUC (4.5 vs 9.7; p = 0.008), and D0 IBUSSAS (16.6 vs 31.0; p = 0.038) were significantly higher in patients with unfavorable outcomes.
Conclusions: IUS delineated colonic inflammation in CDAD, particularly in distal colon. D0 max BWT, MUC, and IBUS-SAS predicted unfavorable outcomes.
P.049
Li-Jen Chang, Chang-Chao Su, Tsung-Jung Tsai, Po-Chun Yang, Chu-Kuang Chou, Chi-Yi Chen, Po-Yueh Chen
Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
光譜影像技術於早期食道癌偵測之評估
張力仁 蘇昶昭 蔡崇榮 楊博鈞 周莒光 陳啟益 陳柏岳
戴德森醫療財團法人嘉義基督教醫院內科部
Background: Esophageal carcinoma (EC) is the eighth most prevalent cancer and the sixth leading cause of cancer-related mortality worldwide. Early detection is vital for improving prognosis, particularly for dysplasia and squamous cell carcinoma (SCC). Narrow-band imaging (NBI) system could enhance the early detection rate of esophageal cancer; however, it remains underutilized due to hardware limitations regarding various endoscopy systems.
Aims: We aim to integrate hyperspectral imaging (HSI) with a novel spectral band selection algorithm, the Spectrum-Aided Vision Enhancer (SAVE), to transform conventional white-light image (WLI) endoscopic images into high-fidelity spectral representations to improve the detection of EC stages and anatomical locations.
Methods: This study evaluates a hyperspectral imaging conversion method, the SpectrumAided Vision Enhancer (SAVE), for its efficacy in enhancing esophageal cancer detection compared to conventional white-light imaging (WLI). Five deep learning models (YOLOv9, YOLOv10, YOLO-NAS, RTDETR, and Roboflow 3.0) were trained and evaluated on a dataset comprising labeled endoscopic images, including normal, dysplasia, and SCC classes.
Results: Across all five evaluated deep learning models, the SAVE consistently outperformed conventional WLI in detecting esophageal cancer lesions. For SCC, the F1 score improved from 84.3% to 90.4% in regard to the YOLOv9 model and from 87.3% to 90.3% in regard to the Roboflow 3.0 model when using the SAVE. Dysplasia detection also improved, with the precision increasing from 72.4% (WLI) to 76.5% (SAVE) in regard to the YOLOv9 model. Roboflow 3.0 achieved the highest F1 score for
dysplasia of 64.7%. YOLO-NAS exhibited balanced performance across all lesion types, with the dysplasia precision rising from 75.1% to 79.8%. Roboflow 3.0 also recorded the highest SCC sensitivity of 85.7%. In regard to SCC detection with YOLOv9, the WLI F1 score was 84.3% (95% CI: 71.7%–96.9%) compared to 90.4% (95% CI: 80.2%–100%) with the SAVE (p = 0.03). For dysplasia detection, the F1 score increased from 60.3% (95% CI: 51.5%–69.1%) using WLI to 65.5% (95% CI: 57.0%–73.8%) with SAVE (p = 0.04). These findings demonstrate that the SAVE enhances lesion detectability and diagnostic performance across different deep learning models.
Conclusions: The amalgamation of the SAVE with deep learning algorithms markedly enhances the detection of esophageal cancer lesions, especially squamous cell carcinoma and dysplasia, in contrast to traditional white-light imaging. This underscores the SAVE’s potential as an essential clinical instrument for the early detection and diagnosis of cancer.
P.050
IMPACT OF ALDH2 POLYMORPHISM ON ESOPHAGEAL SQUAMOUS CELL CARCINOMA TREATMENT OUTCOMES IN A SOUTHERN SINGLE MEDICAL CENTER COHORT
Chi-Sheng Yang1, Bo-Rong Chen2, Yu-Ching Huang3, Jyun-Han Lu1, Song-Wei Wang1, Yao-Kuang Wang1,3, I-Chen Wu1,3, Yi-Hsun Chen1,2
1Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
2School of Post Baccalaureate Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
3School of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
ALDH2 多型性對食道鱗癌治療預後影響 之研究:以南部單一醫學中心為例
楊啓昇1 陳柏榮2 黃郁清3 盧俊翰1 王崧維1 王耀廣1,3
吳宜珍1,3 陳以勳1,2
1 高雄醫學大學附設中和紀念醫院胃腸內科
2 高雄醫學大學學士後醫學系
3 高雄醫學大學醫學系
Background: Esophageal squamous cell carcinoma (ESCC) is one of the top ten cancers in Taiwan in terms of both incidence and cancerrelated mortality. Unlike Western countries, where esophageal adenocarcinoma is more common, ESCC accounts for the majority of esophageal cancer cases in the Taiwanese population. The Aldehyde dehydrogenase 2 (ALDH2) gene mutation is a prevalent variant among East Asians, and recent literature has increasingly explored its potential association with ESCC.
Aims: This study aimed to evaluate the clinical characteristics and treatment outcomes of ESCC patients with different ALDH2 genotypes.
Methods: In a retrospective cohort from January 2016 to February 2022 in Kaohsiung Medical University Hospital, 438 ESCC patients were initially enrolled. After excluding patients without ALDH2/ ADH1B (n = 6), 432 patients (411 males and 7 females) were analyzed. Patients were categorized into ALDH2*1 (wild-type) (n = 116) and ALDH2*2
(n = 316) groups. Demographics, alcohol history, tumor staging, overall survival (OS) and progressionfree survival (PFS) were compared between these groups.
Results: The results revealed that patients with the ALDH2*2 genotype were diagnosed at a younger age than those with ALDH2*1 (57.6 vs. 60.6 years, p = 0.004). They also reported lower lifetime alcohol exposure (28.2 vs. 33.1 alcohol-years, p < 0.01). There was a trend toward more advanced tumor staging in ALDH2*2 carriers (p = 0.063) and shorter PFS (10.48 vs. 14.3 months, p = 0.127), although no difference of OS was revealed between these two groups (31.5 vs 31.7 months, p = 0.96).
Conclusions: These findings suggest that the ALDH2 mutation may play a significant role in the progression and prognosis of ESCC. ESCC patients with the ALDH2*2 allele present at a younger age, with lower alcohol consumption and a trend toward poorer clinical outcomes. These findings suggest ALDH2 mutation may influence both the development and progression of ESCC, warranting further investigation into personalized management strategies.
P.051
ENDOSCOPIC VACUUM THERAPY FOR ESOPHAGEAL TRANSMURAL DEFECTS AFTER ESOPHAGECTOMY OR ENDOSCOPIC PROCEDURES: THE FIRST CASE SERIES IN TAIWAN
Kuan-Ting Liu, Chi-Huan Wu, Puo-Hsien Le, Bo-Huan Chen, Cheng-Hui Lin, Yung-Kuan Tsou
Department of Gastroenterology and Hepatology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
內視鏡負壓治療用於食道切除術或內視 鏡手術後食道全層缺損:台灣首例病例 系列報告
劉冠廷 吳季桓 李柏賢 陳博煥 林政輝 鄒永寬 林口長庚紀念醫院胃腸肝膽科系
Background: Endoscopic vacuum therapy (EVT) has emerged as a promising treatment for esophageal perforation (EP) and esophageal anastomotic leak (EAL).
Aims: This study evaluated the efficacy, safety, and feasibility of a customized EVT system in Taiwanese patients.
Methods: A retrospective analysis was conducted on 25 patients treated with EVT for EP (n = 2) or EAL (n = 23) at a single center. EVT was performed using either endoscope-assisted or guidewire-assisted sponge placement. Primary outcomes included clinical success (de-fined as complete closure of perforation or resolution of leak and necrosis) and treat-mentrelated safety.
Results: The cohort had a median age of 61 years, with 92% being male. Among EAL patients, 52.2% had macro-leaks and 47.8% had micro-leaks. EVT was initiated a median of 1 day post-diagnosis, with a median treatment duration of 14 days and two sponge exchanges. Clinical success was achieved in 68% of patients overall, including 100% in EP cases, 58.3% in the macro-leak group, and 72.7% in the micro-leak group. Because most pa-tients underwent EVT under mild to moderate sedation, three (12%) discontinued treatment due to discomfort. No major adverse events, 30-day mortality, or in-hospital mortality occurred. Logistic regression identified no significant predictors of treatment success.
Conclusions: Customized EVT is a safe, feasible, and effective treatment for EP and EAL in Taiwan, with an acceptable success rate and minimal complications. These findings support the use of EVT as a first-line or rescue therapy for esophageal transmural defects.
P.052
SAFETY AND EFFICACY OF EUS GUIDED HEPATICOGASTROSTOMY WITH DEDICATED PLASTIC STENT
Yi-Lin Lin1, Jiann-Hwa Chen1,2, Wei-Chih Su1, Hung-Da Chen1,2, Lung-Yuan Hsu1,2, You-Chen Chao1,2
1Division of Gastroenterology and Hepatology, Buddhist Tzu Chi Medical Foundation, Taipei Tzu Chi Hospital, Taipei, Taiwan
2School of Medicine, Tzu Chi University, Hualien, Taiwan
內視鏡超音波導引下特殊塑膠支架使用
Background: Background: Percutaneous transhepatic biliary drainage (PTBD) is commonly used to relieve biliary obstruction when endoscopic retrograde cholangiopancreatography (ERCP) fails. However, concerns regarding quality of life remain. Recently, interventional endoscopic ultrasonography (iEUS) has emerged as a potential alternative to PTBD.
Aims: Aim: To evaluate the clinical success rate, procedure time, reintervention rate, and adverse event rate of a dedicated plastic stent used in EUSguided hepaticogastrostomy (EUS-HGS) at a single medical center.
Methods: Methods: Patients included in this study had failed ERCP due to an unreachable major papilla, inaccessible biliary tree, or surgically altered anatomy. Following successful EUS-guided puncture of the target bile duct using a 19-gauge Olympus EZ Shot III needle, tract dilation was performed with a 7 Fr. soft or hard ES® dilator (Zeon Medical Inc., Tokyo, Japan). A 7 Fr. 14 cm IT® plastic stent (Gadelius Medical K.K.) was then deployed into the B2 or B3 bile duct under EUS and fluoroscopic guidance. Clinical success was defined as a reduction in serum bilirubin to less than half of the baseline value within two weeks. Adverse events were defined as any complication occurring within one-week post-procedure. Data on clinical success, procedural time, and adverse events were collected.
Results: Results: A total of 14 patients (7 males, 7 females) were enrolled, of whom 8 had malignant
biliary obstruction. The technical success rate was 92.9% (13/14), and the clinical success rate was 85.7% (12/14). The overall adverse event rate was 14.3% (2/14), including one case of severe abdominal pain and one case of fever with cholangitis. Both patients were managed conservatively. The reintervention rate was 14.3% (2/14). The average procedural time was 42.3 ± 5.2 minutes, measured from bile duct puncture to successful stent placement.
Conclusions: Conclusion: EUS-guided HGS may serve as an effective alternative for biliary drainage in cases where ERCP fails or PTBD is not feasible. However, further studies are needed to determine whether EUS-guided biliary drainage can be considered a primary intervention for biliary obstruction.
P.053
THE EFFECTIVENESS OF A TRANSPARENT CAP IN THE ENDOSCOPIC REMOVAL OF BONY FOREIGN BODIES FROM THE ESOPHAGUS: A RETROSPECTIVE STUDY
Sheng-Chun Lin, Hsueh-Chien Chiang
Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan
透明帽在內視鏡移除食道骨質異物中的
林聖淳 姜學謙
國立成功大學醫學院附設醫院內科部
Background: Esophageal foreign body impaction is an emergent or urgent indication for endoscopic removal. Among all types of esophageal foreign bodies, ingestion of sharp-pointed objects like bony foreign bodies should be removed as soon as possible within 6 hours to avoid severe complications. Endoscopic removal of a bony foreign body is accompanied by risks, such as perforation, fistula formation, or severe infection. The use of a transparent cap attached to the tip of the endoscope has become an increasingly recommended technique for the removal of esophageal foreign bodies to enhance visualization, protect esophageal mucosa, and increase technical success. However, whether a transparent cap is recommended for removing bony foreign bodies is uncertain.
Aims: This study aimed to investigate the real-world effectiveness of a transparent cap in endoscopic removal of a bony foreign body.
Methods: From January 1, 2010-May 30, 2025, patients with reported bony esophageal foreign body for endoscopic removal were retrospectively analyzed. Patients’ characteristics, foreign body characteristics, and endoscopic procedures were assessed. The main outcome was the technical failure rate of endoscopic removal of a bony foreign body.
Results: A total of 595 patients with bony esophageal foreign bodies underwent EGD removal during the study period: 216 underwent the transparent cap-assisted method and 379 underwent the conventional method. Among these foreign bodies,
fish bones accounted for the majority (91.4%), followed by chicken bones (6.5%), duck bones (1.5%), and pork bones (0.5%). A total of 37 patients (6.2%) had unsuccessful endoscopic removal of foreign bodies. The technical failure rate of bony foreign body removal was lower in the cap-assisted group than in the conventional group (3.2% vs 7.9%, P = 0.022). Logistic regression analysis discovered that fish bone, larger size (>2 cm), needle-shaped, embedded foreign body led to a higher failure rate of endoscopic removal. Multivariate logistic regression analysis confirmed that the use of a transparent cap had a lower risk of technical failure (RR: 0.05, 95% CI: 0.01-0.17, P < 0.001).
Conclusions: The use of a transparent cap is an effective method to reduce the technical failure rate for endoscopic removal of an esophageal bony foreign body.
P.054
REDUCING BIOMEDICAL WASTE IN THE PAINLESS ENDOSCOPY UNIT THROUGH CAUSE ANALYSIS AND STRATEGIC INTERVENTIONS
Chih-Hung Lin, Chih-Sheng Hung, Jui-Ting Hu, Chi-Kun Chiang, Ting-Chun Huang, Hsin-Yu Chen
Division of Digestive Medicine, Department of Internal Medicine, Cathay General Hospital, Taipei, Taiwan
透過原因分析與策略性介入以降低無痛
陳信佑
國泰綜合醫院消化內科
Background: According to the 2020 statistics from the Environmental Protection Administration (EPA) of the Executive Yuan, healthcare institutions in Taiwan have generated an average of approximately 120,000 metric tons of medical waste annually over the past five years, with infectious waste accounting for about 30,000 metric tons per year (EPA, Executive Yuan, 2020). The increase or improper handling of infectious waste may heighten the risk of needlestick injuries, exposure to toxic substances, environmental pollution, and the spread of infectious diseases among healthcare workers and the public. Moreover, infectious waste contains a significant amount of plastic materials, and incineration as a treatment method can result in secondary pollution and increased carbon emissions. Therefore, implementing proper classification and recycling of clinical medical materials, along with identifying strategies to reduce the generation of infectious medical waste, can help promote the principles of a circular economy and support ESG (Environmental, Social, and Governance) sustainability practices.
Aims: The General Affairs Department of our hospital compiles monthly statistics on the total volume of infectious medical waste generated by each unit. Over the past two years, the painless endoscopy unit has shown an increasing trend in the amount of infectious waste compared to two years prior, thereby elevating the medical risks faced by healthcare and sanitation personnel. Therefore, this study aims to identify the possible causes of the increased infectious waste and to develop effective improvement strategies, with the ultimate goal of
reducing the volume of infectious medical waste generated in the painless endoscopy unit.
Methods: From January 2023 to the end of April 2024, the average monthly patient volume for painless endoscopic procedures in our hospital was approximately 850 cases, with no significant increase over time. However, the total amount of infectious medical waste generated during this period showed a gradual upward trend. One key contributing factor identified was improper handling during the collection and disposal process of infectious waste. To address this issue, a checklist was developed to evaluate the classification and disposal behaviors of medical personnel in the painless endoscopy unit. This checklist was based on the “Medical Waste Management Information Platform” provided by the Environmental Protection Administration of the Executive Yuan, and the hospital’s internal guidelines titled “Infection Control for Waste Disposal” formulated by the Infection Control Office. Each endoscopic case was treated as a unit of observation. The waste classification behavior of the medical staff was recorded at three stages—before, during, and after each procedure—to determine whether the handling was performed correctly. The observation period lasted five days, from May 6 to May 10, 2024. A total of 114 procedures were observed during this period. Among them, 48 instances of incorrect behavior were recorded, resulting in a compliance rate of 57.9%. The most common issue was misclassification due to unclear labeling on waste bins, accounting for 17 cases (35.4%), followed by improper bin placement affecting workflow and causing errors in 13 cases (27.1%), and failure to drain liquid from disposable medical items before disposal in 11 cases (23%). Together, these three categories accounted for approximately 85.4% of all observed errors.
Results: Based on the analysis, the unit developed targeted improvement strategies addressing the three main issues. For example, to resolve the misclassification caused by unclear labeling on waste bins, additional textual labels were added to indicate the type of waste each bin is designated for, along with pictorial guides placed above the bins to enhance clarity. Two months after implementing the improvement measures, data were collected over a five-day period from December 20 to December 25, 2024. A total of 114 procedures were observed. Only two incidents of incorrect infectious waste disposal were recorded, resulting in a compliance rate of
98.2%. This represents a substantial improvement compared to the pre-intervention compliance rate of 57.9%, marking a 70% increase in accuracy. In addition, the average monthly volume of total waste was calculated before and after the intervention, showing a reduction from 330 kg to 188 kg—a decrease of 142 kg per month.
Conclusions: By analyzing the causes of infectious waste volume exceeding the baseline and implementing targeted interventions, this project successfully reduced the total volume of infectious medical waste generated after painless endoscopic procedures, thereby also minimizing the risk of secondary pollution. The average monthly waste volume decreased by 142 kilograms following the intervention. Based on estimations using high-temperature incineration treatment, this reduction corresponds to an approximate decrease of 284 kilograms in carbon dioxide emissions. The intervention proved to be effective and has the potential to be extended to other hospital units, thereby promoting the principles of circular economy and reinforcing ESG (Environmental, Social, and Governance) sustainability practices.
P.055
Kuan-Hui Wu, Cheuk-Kay Sun
Division of Gastroenterology and Hepatology, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan
經皮內視鏡胃造口術後肉芽組織生成之 臨床與生化預測因子分析
吳冠輝 孫灼基 新光吳火獅紀念醫院胃腸肝膽科
Background: Granulation tissue formation around percutaneous endoscopic gastrostomy (PEG) sites is a common complication that may result in bleeding, local irritation, infection, or the need for additional treatment. The predictive factors for its development are not yet fully understood.
Aims: To identify clinical and laboratory predictors associated with percutaneous endoscopic gastrostomy (PEG) wound granuloma formation in patients undergoing PEG replacement.
Methods: We retrospectively analyzed 113 patients who underwent PEG exchange at Shin Kong Wu Ho-Su Memorial Hospital between January 1, 2021, and December 31, 2024. Collected data included demographic characteristics, comorbidities, PEG indications, and laboratory markers such as serum albumin, HbA1c, hemoglobin (Hb), white blood cell (WBC) count and absolute neutrophil count (ANC). Continuous variables were compared using Student’s t-test and categorical variables using the chi-square test.
Results: Granulation tissue developed in 47 out of 113 patients (41.6%). There were no significant differences in demographic or clinical characteristics between the granuloma and non-granuloma groups. Among laboratory markers, a higher WBC count and absolute neutrophil count (ANC) were associated with a lower incidence of granulation tissue formation (p < 0.05), while a higher basophil percentage and basophil count were significantly associated with increased risk of granulation tissue (p < 0.05).
Conclusions: A higher basophil count may serve as a positive predictor, while an elevated WBC count and ANC may be protective against PEG wound granuloma formation. These findings suggest a nuanced inflammatory response and may help clinicians identify patients at risk for developing this complication.
P.056
PERFORMANCE OF THE GLASGOWBLATCHFORD SCORE AS A PREPROCEDURE RISK STRATIFICATION TOOL FOR ACUTE UPPER GASTROINTESTINAL BLEEDING IN TAIWAN
Che-Yu Rau1, Jer-Wei Wu2, Chieh-Chang Chen1, Ming-Lun Han2, Li-Chun Chang1, Hsiu-Po Wang1, Wei-Chih Liao1, Ping-Huei Tseng1,2
1Division of Gastroenterology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Division of Endoscopy, Department of Integrated Diagnostics & Therapeutics, National Taiwan University Hospital, Taipei, Taiwan
Glasgow-Blatchford Score 作為台灣急性
上消化道出血內視鏡前風險分層工具之 表現評估
饒哲宇1 吳哲瑋2 陳介章1 韓明倫2 張立群1 王秀伯1 廖偉智1 曾屏輝1,2
1 國立臺灣大學醫學院附設醫院胃腸肝膽科 2 國立臺灣大學醫學院附設醫院綜合診療部內視鏡科
Background: Acute upper gastrointestinal bleeding (AUGIB) is a significant clinical issue, and some cases need urgent endoscopy with prompt intervention. The Glasgow-Blatchford Score (GBS) is mostly recommended as a pre-endoscopic risk stratification tool to identify patients requiring endoscopic intervention. However, the actual performance of GBS for patients with AUGIB remains unclear in Taiwan.
Aims: This study aimed to assess the performance of using GBS as a pre-procedural tool for risk stratification in patients with AUGIB at the National Taiwan University Hospital (NTUH).
Methods: We conducted a retrospective study in our prospectively established cohort, which included patients who were consulted for evaluation and management of AUGIB from October 2024 to May 2025. Detailed information regarding the indications, vital signs, laboratory data, endoscopic findings, and treatment outcomes were recorded. Our primary outcome was bleeder detection rate during the endoscopic examinations.
Results: A total of 715 patients (mean age, 70.3
± 11.5 years; male, 54%) were analyzed, with 410 (57.4%) from the emergency department setting and 305 (42.6%) from the inpatient setting. The median GBS was 11 (range, 0–20). Among all endoscopic examinations, bleeder was identified in 403 cases (56.3%), of whom 50.2% had non-variceal etiologies, while variceal bleeding accounted for 6.1%. However, 286 cases (40%) yielded negative findings. For the subgroup of patients with GBS > 1, the bleeder detection rate was only 45.5%, and patients with identified bleeders had similar baseline characteristics, vital signs, and hemoglobin levels compared to those without identified bleeders.
Conclusions: In the present study, nearly half of the endoscopic exams yielded negative results without further necessities of endoscopic intervention in AUGIB patients with GBS more than 1. Hence, further refinement of the widely-used risk stratification method to improve endoscopic yield and treatment outcome is warranted.
P.057
Yoen-Young Chuah1,15, Jyh-Chin Yang2,15, Hsi-Chang Lee3,15, Yu-Hwa Liu4,15, Chia-Long Lee5,15, Sz-Iuan Shiu6,15, Deng-Chyang Wu7,15, Chao-Hung Kuo8,15, Feng-Woei Tsay9,15, Seng-Kee Chuah10,15, Chien-Lin Chen11,15, Sung-Shuo Kao12,15, Chih-An Shih13,15, Ming-Jen Sheu14,15
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Ping Tung Christian Hospital, Pingtung, Taiwan
2Division of Gastroenterology, Department of Internal Medicine, Hospital and College of Medicine, National Taiwan University, Taipei, Taiwan
3Division of Gastroenterology and Hepatology, Department of Internal Medicine Taipei City Hospital, Renai Branch, Taipei, Taiwan
4Division of Gastroenterology, Department of Internal Medicine Shin Kong Wu Huo-Shih Memorial Hospital, Taipei, Taiwan
5Division of Gastroenterology and Hepatology, Department of Internal Medicine, Cathay General Hospital, Taipei, Taiwan
6Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
7Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
8Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
9Division of Gastroenterology and Hepatology, Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
10Division of Hepatogastroenterology, Department of Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, and Chang Gung University College of Medicine, Taoyuan, Taiwan
11Division of Gastroenterology and Hepatology, Department of Internal Medicine, Hualien Tzu
Chi Hospital, Hualien, Taiwan
12Division of Gastroenterology, Department of Internal medicine, Pingtung Veterans General Hospital, Pingtung, Taiwan
13Division of Gastroenterology and Hepatology, Department of Internal Medicine, Antai Medical Care Corporation, Antai Tian-Sheng Memorial Hospital and Department of Nursing, Meiho University, Pingtung, Taiwan
14Division of Hepatogastroenterology, Department of Internal Medicine, Chi Mei Medical Center, Tainan, Taiwan.
15Taiwan Acid-related Disease & Microbiota (TARD-M) Consortium
BE GOOD 研究:一項關於巴瑞特食道的 綜合性調查 腸胃優化、觀察與診斷
蔡元榮1,15 楊智欽2,15 李熹昌3,15 劉玉華4,15 李嘉龍5,15 許斯淵6,15 吳登強7,15 郭昭宏8,15 蔡峯偉9,15 蔡成枝10,15
陳健麟11,15 高崧碩12,15 石志安13,15 許銘仁14,15
1 屏東基督教醫院胃腸肝膽科
2 國立臺灣大學醫學院附設醫院胃腸肝膽科
3 臺北市立聯合醫院仁愛院區消化內科
4 新光吳火獅紀念醫院胃腸肝膽科
5 國泰綜合醫院腸胃內科
6 臺中榮民總醫院胃腸肝膽科
7 高雄醫學大學附設醫院 胃腸內科
8 高雄醫學大學附設醫院 胃腸內科
9 高雄榮民總醫院胃腸肝膽科
10 高雄長庚紀念醫院胃腸肝膽科系
11 花蓮慈濟醫院肝膽胃腸科
12 屏東榮民總醫院
13 安泰醫院胃腸肝膽科
14 奇美醫院胃腸肝膽科
15 台灣胃酸相關疾病暨微菌叢聯盟
Background: Barrett’s esophagus (BE) is a premalignant condition characterized by the replacement of normal esophageal squamous epithelium with columnar-lined epithelium, typically as a result of chronic gastroesophageal reflux disease (GERD). The presence of intestinal metaplasia is considered a key histologic feature for the diagnosis of BE in many international guidelines, although this criterion remains debated. Management strategies for BE include acid-suppressive therapy, primarily with proton pump inhibitors (PPIs), and routine endoscopic surveillance to monitor for dysplastic progression and reduce the risk of
esophageal adenocarcinoma. However, variations in diagnostic criteria and treatment practices persist across different regions and clinical settings. Understanding local practice patterns is essential for identifying gaps in care and aligning management with evidence-based guidelines. In Taiwan, limited data exist regarding gastroenterologists’ real-world approaches to the diagnosis and management of BE. Aims: 1. To assess gastroenterologists’ diagnostic and management approaches to Barrett’s esophagus (BE), including the role of intestinal metaplasia and strategies for symptomatic and asymptomatic patients. 2. To identify factors influencing the use of acid-suppressive therapy and endoscopic surveillance practices in patients with BE, particularly in the context of GERD and non-dysplastic disease. Methods: This cross-sectional, anonymous questionnaire-based study was conducted among gastroenterologists practicing in various healthcare settings—including medical centers, regional hospitals, local hospitals, and private clinics—across different regions of Taiwan. A 13-item electronic or paper-based questionnaire was distributed to attendees of the Taiwan Digestive Disease Week Conference held from October 5 to October 6, 2024. Results: A total of 207 gastroenterologists participated in the survey. Among them, 51.2% reported diagnosing Barrett’s esophagus based on the presence of intestinal metaplasia in pathology reports. The majority (86.5%) indicated that they prescribe acid-suppressive therapy for asymptomatic patients with Barrett’s esophagus. Additionally, 73.4% reported prescribing proton pump inhibitors (PPIs) for a duration of 12 months for the prevention of esophageal adenocarcinoma. Similarly, 69.6% of respondents stated that they would schedule a follow-up endoscopy within 12 months as part of cancer surveillance in patients without dysplasia.
Conclusions: In clinical practice in Taiwan, approximately half of Barrett’s esophagus diagnoses are based on histologic confirmation of intestinal metaplasia. Proton pump inhibitors are frequently prescribed irrespective of symptom status, and endoscopic surveillance within 12 months is commonly performed in patients with nondysplastic Barrett’s esophagus. These management patterns may not be entirely consistent with current international guideline recommendations.
P.058
GASTROINTESTINAL PROTECTIVE EFFECT OF RABEPRAZOLE IN PATIENTS TREATED WITH ASPIRIN AND TICAGRELOR AFTER PERCUTANEOUS CORONARY INTERVENTION FOR ACUTE CORONARY SYNDROME
Jinho Hwang1, Cheal-Wung Huh1, Yong-Cheol Kim2, Hye-Kyung Hyun1
1Department of Gastroenterology and Institute of Gastroenterology, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin, Korea
2Department of Cardiology, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin, Korea
Background: Background: Patients with acute coronary syndrome (ACS) on ticagrelor-based dual antiplatelet therapy (DAPT) have an increased risk of gastrointestinal (GI) bleeding. However, data on the protective effect of proton pump inhibitors against DAPT-induced gastric mucosal injury in this setting are limited.
Aims: To find the PPI agent that have protective effect against DAPT-induced gastric mucosal injury
Methods: Methods: This is a prospective, singlecenter, open-label, single-arm trial enrolling ACS patients treated with DAPT, including aspirin and ticagrelor, after percutaneous coronary intervention (PCI) in South Korea. Patients received 20 mg of rabeprazole once daily for 8 weeks. The primary outcome was the proportion of patients with a modified Lanza score (MLS) of 0-5 on upper endoscopy at 8 weeks, compared to baseline endoscopy. Secondary outcomes included GI symptom scores and safety assessment.
Results: Results: Among 50 patients included in the per-protocol analysis, the mean MLS at baseline and 8 weeks was 1.7 ± 0.9 and 1.6 ± 0.9, respectively, with no significant change (P=0.102). Similarly, in the highrisk patients for GI bleeding (76.0%, 38/50), there was no significant difference in MLS after 8 weeks of treatment with rabeprazole compared to baseline MLS, consistent with the overall study population. GI symptom scores including the Nepean dyspepsia index-Korean (NDI-K), gastroesophageal reflux disease-questionnaire (GERD-Q), and GERD-healthrelated quality of life (GERD-HRQL) questionnaire,
showed no significant changes from baseline in both the overall cohort and the high-risk group. There were no major bleeding or major adverse cardiac events.
Conclusions: Conclusions: Rabeprazole demonstrated a protective effect against gastric mucosal injury in ACS patients on ticagrelor-based DAPT.
P.059
COMPARISON OF GASTROINTESTINAL FOREIGN BODY REMOVAL BETWEEN A MEDICAL CENTER AND A DISTRICT HOSPITAL: A 10-YEAR RETROSPECTIVE STUDY
Kuan-Yu Chi, Yang-Yuan Chen, Hsu-Heng Yen
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan
內視鏡移除腸胃道異物:醫學中心與地 區醫院的十年資料比較
紀冠羽 陳洋源 顏旭亨
彰化基督教醫院胃腸肝膽科
Background: In Taiwan, although district hospitals are widely accessible, many patients preferentially seek care at medical centers, even for conditions such as upper gastrointestinal (UGI) foreign body ingestion that can often be managed at lower-tier facilities. Whether this referral pattern reflects actual differences in clinical outcomes remains unclear.
Aims: This study aimed to compare clinical characteristics and outcomes of patients who underwent UGI endoscopic foreign body removal at a medical center versus a district hospital over a 10year period.
Methods: We retrospectively analyzed adult patients (aged ≥18 years) who underwent UGI endoscopic foreign body removal at Changhua Christian Hospital (CCH, medical center) and Yuanlin Christian Hospital (YCH, district hospital) between August 1, 2015, and March 31, 2025. Exclusion criteria included patients under 18 years, procedures for unrelated therapeutic indications, absence of a foreign body, or incomplete records. Demographics, clinical characteristics, foreign body type and location, and complication rates were compared.
Results: Of 1,354 identified patients, 660 met the inclusion criteria (CCH: 523; YCH: 137). Patients at YCH were significantly older (mean age 65.3 ± 15.6 years vs. 61.8 ± 16.9 years, p = 0.02). The most common foreign body was fish bones (27.3%), and the most frequent location was the upper third of the esophagus (36.5%), consistent across both sites. The overall complication rate was 4.8%, with no significant difference between hospitals (CCH: 3.6%, YCH: 5.8%; p = 0.54). Only 0.9% of cases required surgical intervention, all of which were successfully
managed.
Conclusions: Despite age differences between patient groups, complication rates and surgical intervention needs were comparable between the medical center and district hospital. These findings suggest that district hospitals are equally capable of safely and effectively performing UGI foreign body removal, supporting decentralization and efficient utilization of healthcare resources.
P.060
CAPSULE ENDOSCOPY: TRENDS AND ADVANCEMENTS IN GI DIAGNOSTICS — APPROACHES, APPLICATIONS, AND FUTURE PERSPECTIVES
Chang-Chao Su, Chu-Kuang Chou, Po-Chun Yang, Li-Jen Chang, Shu-Hsien Lin, Tsung-Jung Tsai, Kok-Yean Koh, Ming-Tse Hsu, Chi-Yi Chen, Po-Yueh Chen
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
膠囊內視鏡:胃腸診斷的現況、技術進 步與未來展望
蘇昶昭 周莒光 楊博鈞 張力仁 林淑賢 蔡崇榮 許國衍
許銘澤 陳啟益 陳柏岳
戴德森醫療財團法人嘉義基督教醫院胃腸肝膽科
Background: Capsule endoscopy (CE), introduced in 2000 by Gavriel Iddan, has transformed gastrointestinal (GI) diagnostics by enabling noninvasive visualization of the digestive tract, especially the small intestine, an area often inaccessible to traditional endoscopy. CE is widely used for diagnosing conditions such as gastrointestinal bleeding, Crohn’s disease, and small bowel cancer, offering greater patient comfort and reduced procedural risk compared to conventional methods.
Aims: This study aims to systematically evaluate existing CE technologies, assess their clinical readiness, and explore the potential of artificial intelligence (AI) to enhance diagnostic accuracy and efficiency.
Methods: A comparative review was conducted across five primary CE types: steerable, magnetic, robotic, tethered, and hybrid. Key performance metrics were analyzed, including image resolution (256 × 256 to 640 × 480 pixels), field of view (140° to 360°), battery life (8–15 hours), and frame rates (2–35 frames per second with motion-adaptive capture). The study also evaluated AI applications in image interpretation and CE system integration.
Results: The analysis revealed considerable variability in CE platform capabilities. While significant advancements have improved image quality, navigation, and operational time, limitations
persist, particularly the inability to perform biopsies or therapeutic interventions. AI-based approaches remain underutilized but show substantial promise in enhancing lesion detection, classification, and workflow automation.
Conclusions: Capsule endoscopy has made notable progress in technical and clinical domains; however, diagnostic limitations persist. AI integration represents a critical next step for overcoming current challenges, improving diagnostic precision, and shaping the development of future CE systems. Further innovation and clinical validation are essential to fully realize CE’s potential in GI diagnostics.
P.061
CLARITY-GASTRIC 01: A RANDOMIZED PHASE 3 STUDY OF SONESITATUG VEDOTIN (AZD0901), A CLAUDIN18.2 (CLDN18.2)TARGETED ANTIBODY-DRUG CONJUGATE, IN SECOND- OR LATERLINE (2L+) ADVANCED GASTRIC OR GASTROESOPHAGEAL JUNCTION CANCER (GC/GEJC)
I-Chen Wu1, Kohei Shitara2, Yelena Y. Janjigian3, Elena Elimova4, Jun Zhang5, Ming-Huang Chen6, Elizabeth Smyth7, Jeeyun Lee8, Rui Miao9, Silver Liu9, Marielle Holmblad10, Osama E. Rahma11, Rui-Hua Xu12
1Division of Gastroenterology, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
2Department of Gastroenterology and Gastrointestinal Oncology, National Cancer Center Hospital East, Kashiwa, Japan
3Gastrointestinal Oncology Service, Memorial Sloan Kettering Cancer Center, New York, NY, USA
4Department of Medical Oncology and Hematology, Princess Margaret Cancer Centre, Toronto, ON, Canada
5Department of Oncology, Rui Jin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
6Department of Oncology, Taipei Veterans General Hospital, Taipei, Taiwan
7Department of Oncology, Oxford University Hospitals NHS Foundation Trust, Oxford, UK
8Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
9R&D China, AstraZeneca, Shanghai, China
10Oncology R&D, Late-Stage Development, AstraZeneca, Gaithersburg, MD, USA
11Global Oncology R&D, AstraZeneca, Waltham, MA, USA
12Department of Medical Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer,
Sun Yat-sen University, Guangzhou, China
Background: Prognosis is poor in 2L and 3L+ GC/GEJC. New treatment options are needed. Sonesitatug vedotin, a potential first-in-class CLDN18.2-targeted antibody conjugate, has demonstrated clinical activity in a Phase 1 advanced GC/GEJC study.
Aims: CLARITY-Gastric 01 (NCT06346392), a randomized, open-label, sponsor-blinded, global Phase 3 study will assess outcomes of sonesitatug vedotin versus investigator’s choice of therapy after ≥1 prior therapy for advanced GC/GEJC expressing CLDN18.2.
Methods: Participants will be randomized 1:1:1 to sonesitatug vedotin dose level 1 intravenous (IV) every 3 weeks (Q3W; Arm 1), sonesitatug vedotin dose level 2 IV Q3W (Arm 2), or investigator’s choice of therapy (2L: ramucirumab + paclitaxel, paclitaxel, or docetaxel [for participants with contraindication to ramucirumab only]; 3L+: irinotecan, TAS-102 [excluding China], or apatinib [China only]; Arm 3). In January 2025, sonesitatug vedotin monotherapy dose was determined to be 2.2 mg/kg (Arm 2). Arm 1 was closed for enrollment. Randomization will continue in a 1:1 ratio to Arm 2 and Arm 3. Eligible participants must have histologically confirmed, unresectable, locally advanced or metastatic GC/GEJC (non-HER2+, CLDN18.2 expression). Participants must have disease progression on/ after ≥1 prior regimen and have an ECOG PS 0-1. Participants previously treated with CLDN18.2targeting therapy are excluded. Recruitment has begun; participants are planned to be enrolled across 16 countries in Asia, Europe, and North America. Dual primary endpoints are PFS (intent-to-treat [ITT] participants) and OS (3L+ participants). Secondary endpoints include OS (ITT participants), PFS (3L+ participants), objective response rate and duration of response (ITT and 3L+ participants), and safety/ tolerability. Efficacy endpoints will be analyzed in the ITT population and assess Arm 2 versus Arm 3. Safety/tolerability will be assessed in participants who receive ≥1 study treatment dose.
Conclusions: NA Previously presented at European Society for Medical Oncology - Gastrointestinal Cancers Congress 2024, Final Publication Number: 495TiP, Kohei Shitara et al. Reused with permission.
P.062
INVESTIGATION OF THE ANTITUMOR EFFECTS AND MECHANISMS OF
Yi-Jen Fang1,2,3, I-Tsang Chiang1,3, Kuei-Min Chen1, Chien-Hua Chen1, chi-Chieh Yang1
1Division of Gastroenterology, Department of Internal Medicine, Show Chwan Memorial Hospital, Changhua, Taiwan
2Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan
3Clinical Trial Center, Show Chwan Memorial Hospital, Changhua, Taiwan
樂衛瑪(Lenvatinib)在活體內對大腸直 腸癌的抗腫瘤作用及機轉研究
方怡仁1,2,3 蔣宜蒼1,3 陳奎閔1 陳建華1 楊基滐1
1 秀傳紀念醫院胃腸肝膽科
2 國立中興大學學士後醫學系
3 秀傳紀念醫院臨床試驗中心
Background: The combined application of cytotoxic chemotherapy and molecular targeted therapies has significantly improved the survival of patients with unresectable metastatic colorectal cancer (mCRC). However, for patients who are refractory or unresponsive to standard chemotherapy, prognosis remains poor. This is particularly true for those in good physical condition who are still eligible for further treatment—indicating an unmet medical need. Lenvatinib, an oral multi-targeted tyrosine kinase inhibitor, has been evaluated in large-scale clinical trials. These studies have demonstrated promising clinical activity and favorable tolerability of lenvatinib in mCRC patients who have failed prior standard chemotherapy. Therefore, further investigation into the therapeutic potential of Lenvatinib in colorectal cancer is warranted.
Aims: The primary objective of this study was to verify the anti-tumor efficacy and underlying mechanisms of Lenvatinib in colorectal cancer using an in vivo mouse model.
Methods: A colorectal cancer (CRC) xenograft mouse model was established for this study. Mice bearing CRC tumors were treated with either vehicle or lenvatinib for 20 days. Tumor growth was monitored
using a digital caliper. Tumor tissues were analyzed via immunohistochemistry (IHC) to assess changes in pro- and anti-apoptotic signaling pathways, as well as ERK activity.
Results: Lenvatinib treatment significantly inhibited tumor growth and decreased the expression of antiapoptotic proteins and ERK activity. Furthermore, Lenvatinib induced apoptosis through both intrinsic and extrinsic pathways, as confirmed by IHC analysis.
Conclusions: These findings suggest that Lenvatinib suppresses CRC progression in vivo by inducing apoptosis, downregulating anti-apoptotic signaling, and inhibiting ERK activity. Key words: Lenvatinib, CRC, apoptosis, anti-apoptosis, ERK
P.063
IMPACT OF LOW-RESIDUAL DIET AND BOWEL PREPARATION FOR COLONOSCOPY ON SAME-DAY METABOLIC BLOOD PARAMETERS IN A HEALTH EXAMINATION COHORT
Chan-Yi Lin1,2, Jyh-Ming Liou1,2, Ming-Shiang Wu1, Tzu-Chan Hong1,2
1Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Department of Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
低渣飲食與大腸鏡清腸準備對同日代謝 血液檢查指標之影響:來自健檢族群的 分析
林展毅1,2 劉志銘1,2 吳明賢1 洪子瞻1,2
1 台大醫院內科部
2 台大醫院癌醫分院綜合內科部
Background: Colonoscopy combined with sameday metabolic blood testing is increasingly common in health examination settings. While prior studies have investigated the effects of bowel preparation on electrolytes and liver function, the potential impact of a short-term low-residual diet followed by bowel cleansing on metabolic parameters remains unclear.
Aims: This study aims to evaluate whether shortduration dietary restriction and bowel preparation for colonoscopy distort commonly assessed metabolic blood parameters in a routine health screening population.
Methods: We conducted a retrospective cohort study using health examination records from 2021 to 2024, including individuals who underwent colonoscopy (Colonoscopy group) and those who did not (non-Colonoscopy group). Individuals in the Colonoscopy group followed a two-day low-residual diet followed by same-day bowel preparation with 2 liters of polyethylene glycol (PEG)-based purgative (Niflec). All participants completed a standardized health questionnaire and underwent anthropometric measurements and laboratory testing. To minimize baseline differences between groups, propensity score matching (PSM) was performed using non-laboratory baseline characteristics. Inverse probability of treatment weighting (IPTW) was applied to the imputed
dataset using median imputation, with a completecase analysis conducted as sensitivity testing. Weighted differences in metabolic parameters between groups were estimated using weighted linear regression models with significance testing.
Results: A total of 2,343 individuals were included in the analysis, of whom 1,447 (61.8%) underwent same-day colonoscopy with standardized bowel preparation (Colonoscopy group), while 896 (38.2%) did not (non-Colonoscopy group). After IPTW adjustment, covariate balance was achieved between the two groups. In the Colonoscopy group, glucose levels were significantly lower (effect: −1.74, P=0.015), while total cholesterol (effect: +3.46, P=0.028), LDL (effect: +4.10, P=0.004), HDL (effect: −2.86, P<0.001), and insulin resistance or HOMA-IR (effect: −0.47, P<0.001) were significantly altered. In contrast, there were no significant differences in HbA1c, which is insensitive to short-term metabolic fluctuations, nor in C-reactive protein (CRP) or alphafetoprotein (AFP), which are not directly influenced by dietary restriction or bowel preparation. These findings remained consistent in the sensitivity analysis using the complete-case cohort.
Conclusions: Short-term low-residual diet combined with bowel preparation for colonoscopy can distort selected metabolic blood parameters, particularly glucose and lipid profiles. Although the observed effects are small, they may influence clinical interpretation and should be carefully considered in routine health examination settings involving same-day laboratory testing.
P.064
RIGHT HEMICOLECTOMY WITH COMPLETE MESOCOLIC EXCISION VERSUS CONVENTIONAL CENTRAL LIGATION: A SINGLE-CENTER COMPARATIVE STUDY
Ping-Teng Chu, Jui-Ho Wang, Chao-Wen Hsu
Division of Colorectal Surgery, Department of Surgery, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
右半結腸切除手術合併完全結腸系膜切 除術與傳統中央結紮術:單一醫學中心 比較研究
朱炳騰 王瑞和 許詔文 高雄榮民總醫院大腸直腸外科
Background: Complete mesocolic excision (CME) has emerged as an advanced surgical technique for right-sided colon cancer, emphasizing anatomical planes and central vascular ligation to achieve superior oncological outcomes. However, comprehensive comparative data regarding its perioperative and long-term benefits compared to conventional central ligation remains limited in Asian populations.
Aims: This study aimed to compare the perioperative outcomes, pathological quality, and oncological results between right hemicolectomy with CME and conventional central ligation for right-sided colon cancer in a single-center setting.
Methods: A retrospective comparative study was conducted on 402 consecutive patients who underwent right hemicolectomy for colon cancer between 2015 and 2024 at our institution. Patients were divided into two groups: CME group (n=197) and conventional central ligation group (n=202). Primary endpoints included operative outcomes, pathological quality indicators, and postoperative complications. Secondary endpoints encompassed long-term oncological outcomes including local recurrence and distant metastasis. Statistical analysis was performed to compare perioperative variables, pathological parameters, and survival outcomes between the two groups.
Results: The CME group demonstrated significantly longer operative time compared to the conventional group (177.8 vs 146.3 minutes). However, CME achieved superior pathological quality with
significantly higher lymph node harvest (36.6 vs 21.9 nodes), improved R0 resection rate (99.5% vs 91.1%), and better mesocolic plane integrity (86.8% vs 65.8%). Postoperatively, the CME group showed lower overall complication rates (12.7% vs 19.3%) and shorter hospital stay (11.0 vs 14.6 days). The CME technique resulted in longer specimen length (32.5 vs 25.4 cm) and reduced intraoperative blood loss (92.5 vs 123.9 ml). Both groups showed comparable conversion to open surgery rates and major complication rates (Clavien-Dindo grade ≥3).
Conclusions: Right hemicolectomy with complete mesocolic excision demonstrates superior pathological quality and oncological outcomes compared to conventional central ligation, with improved lymph node harvest, higher R0 resection rates, and reduced postoperative complications. Despite longer operative time, CME appears to be a safe and effective technique that should be considered as the standard approach for right-sided colon cancer surgery. The enhanced pathological quality achieved through CME may translate to improved long-term oncological outcomes, supporting its adoption in specialized colorectal surgery.
P.065 DOES NON-SEDATIVE COLONOSCOPY POSSIBLE? EVALUATION OF PAINFUL SENSATION, CECAL INTUBATION AND ADENOMA DETECTION RATE
Cheng-Ju Lee, Ming-Yao Su
Division of Gastroenterology and Hepatology, Department of Internal Medicine, New Taipei Municipal TuCheng Hospital, New Taipei City, Taiwan
非鎮靜大腸鏡檢查可行嗎?痛覺、盲腸 插入率及腺瘤檢出率評估
李承儒 蘇銘堯
新北市立土城醫院胃腸肝膽科
Background: Colon is a long and tortuous tube, so colonoscopy is more invasive and painful procedure then esophagogastroduodenoscopy.
Aims: To identify factors that predict painful colonoscopy, cecal intubation rate (CIR) and adenoma detection rate (ADR) in non-sedative colonoscopy.
Methods: From January to Aug 2015, A total of 1260 consecutive patients underwent non-sedative colonoscopy were enrolled. This was a prospective, observational study. Prospective data’s collection including patients’ characteristics, previous medical and surgical history, and indications for colonoscopy, bowel preparation status, insertion time and length of colonoscopy. Patients’ anxiety levels were recorded before the procedure and painful sensation were recorded after the procedure by Likert scale from one study nurse blinded to the procedure. Endoscopists’ experiences were recorded also. These factors were analyzed for the correlations of painful sensation, cecal intubation rate (CIR) and adenoma detection rate (ADR).
Results: There were no significant differences for the painful sensation of colonoscopy and the factors mentioned above by univariate analysis except gender and patient’s anxiety level. While, patient’s anxiety level, endoscopist’s experience were correlate with painful sensation of colonoscopy by multivariate analysis. Male and older than 50 years patients had higher ADR. While operator’s experience increased both CIR and ADR.
Conclusions: In our study, high anxiety level of patients, female gender and unexperienced endoscopists may correlate with painful feeling under non-sedative colonoscopy, while experienced endoscopists and male gender had higher ADR.
P.066
TUMOR LOCATION AND DIAGNOSTIC STAGE AS PROGNOSTIC FACTORS IN COLORECTAL CANCER
Tai-An Cheng1, Yen-Ju Chen2, Yuan-Chi Mao1, Chun-Hsiang Wang1, Ruey-Chang Lin1, Kuo-Kuan Chang1, Lein-Ray Mo1
1Department of Hepatogastroenterology, Tainan Municipal Hospital (Managed by Show Chwan Medical Care Corporation), Tainan, Taiwan
2Research Assistant Center, Tainan Municipal Hospital (Managed by Show Chwan Medical Care Corporation), Tainan, Taiwan
腫瘤位置與診斷分期作為大腸直腸癌的 預後因子
鄭泰安1 陳沿如2 毛元治1 王俊雄1 林瑞昌1 張國寬1 牟聯瑞1
1 台南市立醫院(委託秀傳醫療社團法人經營)肝膽 腸胃科
2 台南市立醫院(委託秀傳醫療社團法人經營)醫學 研究輔佐中心
Background: Colorectal cancer (CRC) is the third most prevalent malignancy worldwide and was responsible for approximately 900,000 deaths in 2022. Due to its tendency to remain asymptomatic until reaching advanced stages, many health authorities have introduced organized screening programs aimed at enhancing early detection and thereby reducing both morbidity and mortality.
Aims: This study sought to explore the baseline clinical characteristics of patients diagnosed with early- and advanced-stage CRC and to evaluate prognostic differences based on tumor location and diagnostic stage.
Methods: We performed a retrospective analysis utilizing a comprehensive cancer registry dataset, focusing on gastrointestinal cancers diagnosed between 2015 and 2023. After applying rigorous inclusion and exclusion criteria, 925 patients with confirmed CRC were included in the final analysis. Statistical analyses were conducted using SPSS version 24.0, with a p-value of less than 0.05 considered statistically significant.
Results: Among 917 patients with complete demographic data, 59.0% (541/917) were male, with
most patients aged ≥ 66. The rectum (31.0%), sigmoid colon (26.9%), and ascending colon (13.0%) were the most common primary tumor sites. Preoperative radio or chemotherapy was administered to a small subset (5.3%) to reduce tumor burden. Surgical resection of the primary tumor was performed in 85.9% of cases, regardless of cancer stage. Notably, 12.3% (113/916) of patients experienced recurrence within an average of 1.7 ± 1.3 years post diagnosis. As expected, overall survival declined with advancing disease stage, while recurrence rates increased. Key factors associated with higher recurrence risk included male (hazard ratio = 2.2; 95% confidence interval: 1.0 – 4.6), obesity (HR = 1.9; 95% CI: 1.0 –3.8), perineural invasion (HR = 3.1; 95% CI: 1.6 – 6.2), and greater lymph node involvement (HR = 14.5; 95% CI: 4.3 – 48.7).
Conclusions: In recent years, CRC has shown a notable shift toward affecting younger populations. Rapid changes in socioeconomic conditions and lifestyle factors are believed to contribute to this trend. Strengthening CRC screening, particularly among high-risk groups, is essential. Fecal occult blood tests as an initial screening method, followed by colonoscopy when indicated, remain a cornerstone of effective early detection and prevention strategies.
P.067
THE DETECTION RATE OF COLON POLYP IN HEALTHY INDIVIDUALS FROM A SELF-PAID HEALTHCARE MANAGEMENT SETTING
Ting-Chun Huang1,3,4, Ting-Shuo Chen2, Hsiu-Tzu Hsieh2, Yi-Hsien Kuo2, Chih-Sheng Hung1,3,4
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Cathay General Hospital, Taipei, Taiwan
2Cathay Healthcare Management Co., Ltd., Taipei, Taiwan
3School of Medicine, College of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan
4School of Medicine, National Tsing Hua University, Hsinchu, Taiwan
在健康管理機構中,自費接受大腸鏡檢 查的相對健康成人其大腸瘜肉的檢出率
黃鼎鈞1,3,4 陳丁碩2 謝秀梓2 郭怡賢2 洪志聖1,3,4
1 國泰綜合醫院消化內科 2 國泰健康管理顧問股份有限公司
3 天主教輔仁大學醫學系 4 國立清華大學學士後醫學系
Background: According to current consensus, the polyp detection rate during colonoscopy in Taiwan is approximately 20–25%. However, there is a lack of large-scale studies investigating the prevalence of polyps among relatively healthy individuals who undergo self-paid colonoscopy screening. This study aims to examine the prevalence of colorectal polyps and neoplasms in a relatively healthy adult population that voluntarily opts for self-paid colonoscopy screening.
Aims: The primary outcome of this study is to determine the prevalence and diagnostic yield of colorectal polyps in individuals undergoing screening colonoscopy.
Methods: We conducted a retrospective analysis of relatively healthy adults who underwent health examinations, including colonoscopy, at Cathay Healthcare Management between 2019 and 2023. Lesions were classified based on pathological severity into the following categories: cancer, adenoma, hyperplastic polyp and other related conditions. In cases where multiple pathological diagnoses were identified in a single colonoscopy,
the classification was based on the most severe lesion. Prior to the procedure, participants were asked to provide consent for the use of their data in this analysis. Those who declined were excluded from the final dataset.
Results: This study included data from relatively healthy adults who underwent health examinations at Cathay Healthcare Management between 2019 and 2023. During the study period, a total of 566,199 health examination visits were recorded, among which 103,975 involved colonoscopy, and 28,202 involved subsequent colonoscopic biopsies. Of these, 76,501 participants consented to the inclusion of their data in the research analysis. The average age of this population was 42.48 years. Males accounted for 42,754 cases (55.89%), while females accounted for 33,747 cases (44.11%). The overall detection rate of colorectal cancer and adenomas was 12.82%. Among the 28,202 colonoscopy cases with biopsy, 20,899 participants provided informed consent for data analysis. In this analytic cohort, 80 cases (0.38%) were diagnosed with colorectal cancer, 9,730 cases (46.55%) with adenomas, and 10,420 cases (49.85%) with hyperplastic polyps or other related lesions. When multiple pathological findings were identified in a single examination, classification was based on the most severe diagnosis to avoid duplicate counting.
Conclusions: Among all biopsy-confirmed cases, the combined positivity rate for colorectal cancer and adenomas was 46.94%. This finding indicates that colonoscopies performed at Cathay Healthcare Management demonstrated a relatively high diagnostic yield for neoplastic lesions, reflecting strong detection and pathological assessment capabilities for polypoid abnormalities.
EFFECTIVENESS OF STRUCTURED TRAINING PROGRAM FOR BASIC COLONOSCOPE INSERTION: A SINGLE-CENTER STUDY IN TAIWAN
Hung-Yi Lin1, Chen-Shuan Chung1,2
1Division of Gastroenterology and Hepatology, Far Eastern Memorial Hospital, New Taipei City, Taiwan
2College of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan
結構式訓練課程對基礎大腸鏡插入技巧 之成效:台灣單一中心研究
林宏益1 鍾承軒1,2 1 亞東紀念醫院肝膽胃腸科 2
Background: Previous research has supported the validity of performance measures derived from the use of a physical model colonoscopy simulator— the Kyoto Kagaku Colonoscope Training Model (Kyoto Kagaku Co. Ltd., Kyoto, Japan)—for assessing insertion skills. However, there is a lack of data regarding its use and validation in colonoscopy training programs in Taiwan.
Aims: We assessed the efficacy of structured training program aimed at developing basic colonoscope insertion skills through programmed education course and endoscopic practice using the model simulator model.
Methods: This training study used a pre-test/posttest design. All specialist fellows in Gastroenterology and Proctology who trained at Far Eastern Memorial Hospital (FEMH) between August 2022 and 2025 were included. At baseline, participants completed a basic colonoscopy knowledge questionnaire and performed standardized test cases on a colonoscopy simulator to assess initial performance. Participants then received three hours training sessions covering basic colonoscopy knowledge, insertion techniques and live demonstration by an experienced tutor. After training, the same questionnaire and test cases were repeated to assess performance using the same outcome measures. Outcome measurement included completion cecal intubation rate, time to reach the cecum, maximum insertion depth and loop formation.
Results: A total of 10 trainees—including 7 Gastroenterology and 3 Proctology specialists—
participated in this educational study. Following the training sessions, questionnaire scores improved significantly (85.0 ± 21.0 vs. 41.6 ± 12.6, p < 0.001). Trainees also achieved a markedly higher cecal intubation rate (99% vs. 64%, p <0.001) and significantly shorter insertion times (209.86 ± 121.18 seconds vs. 417.42 ± 184.34 seconds, p < 0.001). In addition, the incidence of loop formation was substantially reduced (1% vs. 51%, p < 0.001).
Conclusions: The findings suggest that the structured training program may serve as an effective method for teaching basic colonoscope insertion skills. Trainees who complete the program appear better prepared to transition to supervised live cases.
P.069
THE TIMING OF WARM WATER SITZ BATH DOES NOT RELIEVE THE SYMPTOMS AFTER LASER HEMORRHOIDOPLASTY FOR PATIENTS WITH GRADE II/III HEMORRHOID: A RETROSPECTIVE STUDY FROM A SINGLE INSTITUTE
Jui-Yun Lin1, Ming-Fang Yin1, Kai-Shing Chang2, Bin-Chin Wu2, Wan-Xin Cheng2, Ho-Hsien Chuan2, Kai-Jei Huang2, Chung-Chieh Cheng2, Yu-Tso Liao2, Ming-Chi Ho2,3, Jin-Tung Liang3
1Department of Nursing, National Taiwan University Hospital, Hsin-Chu Branch, Hsinchu, Taiwan
2Division of Colorectal Surgery, Department of Surgery, National Taiwan University Hospital, Hsin-Chu Branch, Hsinchu, Taiwan
3Division of Colorectal Surgery, Department of Surgery, National Taiwan University Hospital and College of Medicine, Taipei, Taiwan
溫水坐浴之介入時間不會緩解第二 / 三度
痔瘡病人接受雷射痔瘡消融手術術後的 症狀:單一機構的回溯性分析
林瑞筠1 尹銘芳1 張凱行2 吳秉奇2 鄭婉馨2 全賀顯2 黃凱傑2 鄭宗杰2 廖御佐2 何明志2,3 梁金銅3
1 國立臺灣大學醫學院附設醫院新竹臺大分院護理部 2 國立臺灣大學醫學院附設醫院新竹臺大分院大腸直 腸外科
3 國立臺灣大學醫學院附設醫院大腸直腸外科
Background: Laser hemorrhoidoplasty (LHP) is a minimally invasive surgery for grade I-III hemorrhoids. While sitz baths are common after conventional hemorrhoidectomy, their role in LHP recovery is less understood.
Aims: This study aims to evaluate the timing and effects of warm water sitz baths on postoperative recovery after LHP.
Methods: A retrospective study was conducted on patients with symptomatic grade II or III hemorrhoids who underwent laser hemorrhoidoplasty (LHP) between March 2023 and April 2025. The analysis focused on clinical and surgical data, as well as recovery outcomes, specifically comparing patients who received warm water sitz baths on the day of surgery and the first postoperative day. The primary outcome was postoperative pain, measured using
a visual analogue scale (VAS). Secondary outcomes included the incidence of complications such as urinary retention and postoperative bleeding.
Results: Eighty patients were included. Thirty-seven received a sitz bath on the day of surgery, while 43 had it the next day. The average time to start the sitz bath after leaving the operation room was 6.3 ± 3.5 hours for the first group and 21.2 ± 2.1 hours for the second (P < 0.001). No major complications occurred. Postoperative VAS scores and complications did not significantly differ between the groups.
Conclusions: The use of warm water sitz baths on the day of surgery did not demonstrate benefits for patients with grade II/III hemorrhoids undergoing LHP in relation to pain scores and complications. Further prospective studies with a larger participant pool are necessary.
P.070
A
Jen Hao Yeh1, Chao-Wen Hsu2, Chun-Sheng Shen3, Kun-Feng Tsai4, I-Ching Cheng5, Yi-Chia Lee6, Ping-Huei Tseng6, Chu-Kuang Chou7
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, E-Da DaChang Hospital, I-Shou University, Kaosiung, Taiwan
2Division of Colorectal Surgery, Department of Surgery, Kaohsiung Veterans General Hospital, Kaosiung, Taiwan
3Gastroenterology division, Department of Internal medicine, Kaohsiung Municipal HsiaoKang Hospital, Kaosiung, Taiwan
4Department of Internal Medicine, Gastroenterology and Hepatology Section, An Nan Hospital, Tainan, Taiwan
5Aphrodite Paradise Clinic, Taipei, Taiwan
6Department of Internal Medicine, National Taiwan University Hospital, Tainan, Taiwan
7Division of Gastroenterology and Hepatology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
更環保的大腸 ESD :多中心短端刀無針 注射技術臨床研究
葉人豪1 許詔文2 沈群勝3 蔡坤峰4 鄭以勤5 李宜家6 曾屏輝6 周莒光7
1 義大大昌醫院胃腸肝膽科
2 高雄榮民總醫院大腸直腸外科
3 高雄市立小港醫院胃腸肝膽科
4 台南市立安南醫院胃腸肝膽科
5 雅丰纖境腸胃科診所
6 台大醫院內科部
7 戴德森醫療財團法人嘉義基督教醫院胃腸肝膽科
Background: This study evaluates the efficacy and safety of a novel needleless injection technique for colorectal endoscopic submucosal dissection (NITESD).
Aims: This multicenter retrospective study included 191 patients undergoing colorectal ESD at three
institutions between 2019 and 2024. Patients were categorized into NIT-ESD (n = 127) and conventional ESD (n = 64) groups. The primary outcome was resection time. Secondary outcomes included en bloc and R0 resection rates, hybrid ESD conversions, and adverse events. Multivariable linear regression analysis was used to identify independent variables influencing resection time.
Methods: This multicenter retrospective study included 191 patients undergoing colorectal ESD at three institutions between 2019 and 2024. Patients were categorized into NIT-ESD (n = 127) and conventional ESD (n = 64) groups. The primary outcome was resection time. Secondary outcomes included en bloc and R0 resection rates, hybrid ESD conversions, and adverse events. Multivariable linear regression analysis was used to identify independent variables influencing resection time.
Results: The mean resection time was significantly shorter for NIT-ESD compared to conventional ESD (52.8 ± 44.7 vs. 72.6 ± 63.1 min; P = 0.027). En bloc resection rates and R0 resection rates (both 98.4% vs. 95.3%; P = 0.203) were comparable between the two groups. Severe adverse events were also comparable (9.4% vs. 4.7%; P = 0.248) and were managed conservatively in most cases. Only one patient (NIT-ESD group) required surgery due to a delayed perforation. Multivariable analysis identified operator experience and lesion size – but not the use of an injection needle (P = 0.315) – as significant factors influencing resection time (P < 0.001). Moreover, NIT-ESD may reduce approximately 1.89 kg CO₂e per 100 procedures, solely from sparing injection needles.
Conclusions: NIT-ESD appears to be a safe, effective and potentially greener technique for colorectal ESD. Future prospective studies are warranted to validate these findings, assess the learning curve, and explore the cost-effectiveness of NIT-ESD in routine practice.
P.071
ENHANCING ADENOMA DETECTION RATE VIA A DE-IDENTIFICATIONBASED TAGGING
Wei-Lun Hsu1, Yow-Chii Kuo1, Yin-Chen Wang1, Chin-Yuan Yu1, Shih-Hao Young1, Fu-Ming Chang1, Tzu-An Chen2, Huang-Jen Lai2
1Division of Gastroenterology and Hepatology, Department of Medical Affairs, Landseed International Hospital, Taoyuan, Taiwan
2Division of Colorectal Surgery, Department of Medical Affairs, Landseed International Hospital, Taoyuan, Taiwan
透過去識別化標籤平台提升大腸癌篩檢 腺瘤性息肉偵測率之研究
徐偉倫1 郭佑啟1 王尹宸1 余青殷1 楊士豪1 張福銘1 陳子安2 賴煌仁2
1 聯新國際醫院腸胃肝膽科 2 聯新國際醫院大腸直腸外科
Background: Colorectal cancer (CRC) screening significantly reduces CRC mortality through early adenoma detection. However, ensuring timely follow-up colonoscopies remains challenging. We developed a targeted, automated, de-identificationbased tagging platform to improve screening compliance and adenoma detection rates (ADR).
Aims: To evaluate the effectiveness of a precisiontargeted tagging platform in enhancing CRC screening adherence and increasing ADR.
Methods: A de-identification-based tagging platform was implemented using electronic health records (EHRs) to identify two target groups for colonoscopy: Inclusion: Individuals with documented colon polyps on previous colonoscopy performed 2–5 years ago. Exclusion: Colonoscopy performed within the past 2 years or previously diagnosed with CRC. Patients identified through these criteria received SMS notifications and educational digital messages (EDM) containing survey links for followup scheduling. Colonoscopies were performed.
Results: Total 826 SMS had been sent with a successful SMS delivery rate of 97.4%. Of these, 348 persons clicked our SMS link. 79 persons (79/800, 9.9%) registered for GI or colorectal surgery outpatient departments, and 39 (39/79, 49.4%) completed colonoscopies. Adenoma Detection Rate
(ADR) among these patients was 43.6% (17/39). Compared with traditional national FIT screening (ADR = 39.0%; 121/310), the tagging platform demonstrated numerically improved ADR, although this difference did not reach statistical significance (p = 0.583).
Conclusions: The de-identification-based tagging platform significantly improved patient identification, clinical attendance, and follow-up colonoscopy rates for CRC screening. Importantly, patients with previously identified polyps returning for surveillance colonoscopies via this platform showed an ADR comparable to traditional FIT screening. Given the economic feasibility and effectiveness of SMS tagging and outreach, this platform warrants consideration for broader application in CRC screening and surveillance strategies.
P.072
ASSOCIATION BETWEEN MORPHOLOGICAL FEATURES OF COLONIC LATERALLY SPREADING TUMORS AND ADVERSE HISTOPATHOLOGICAL OUTCOMES: A SINGLE CENTER EXPERIENCE IN TAIWAN
Guan-De Li, Chen-Huan Yu, Chen-Shuan Chung
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan
大腸側方擴散性腫瘤形態特徵與不良病 理結果之相關性分析:台灣單一醫學中
李冠德 余臣桓 鍾承軒
Background: Colonic laterally spreading tumors (LSTs) are classified into four morphological subtypes: granular-homogeneous (LST-G-H), granular-nodular mixed (LST-G-NM), nongranular-flat elevated (LSTNG-FE), and nongranular-pseudodepressed (LST-NGPD).
Aims: This study aimed to evaluate the association between LST morphology and adverse histopathological outcomes.
Methods: We retrospectively analyzed 329 colonic LSTs resected endoscopically from 328 patients at Far Eastern Memorial Hospital between May 2010 and October 2024. Clinical, endoscopic, and pathological data were compared across groups.
Results: Among the 329 lesions, the most common subtypes were LST-NG-FE (33.4%) and LST-G-H (33.1%), followed by LST-G-NM (22.2%) and LST-NGPD (11.2%). Deep submucosal invasion (SMI) was observed in 5.5% of cases, with 27% of LST-NG-PD lesions showing deep SMI. Moderately or poorly differentiated adenocarcinoma was identified in 10 lesions (3%), with 7 of these patients (70%) presenting with LST-NG-PD. No cases of deep SMI or poor differentiation were found in the LST-G-H group.
In Fisher’s exact test, both LST-NG-PD (P < 0.001) and LST-G-NM (P = 0.004) were significantly associated with higher deep SMI rate compared with LST-G-H.
Conclusions: The morphological classification of LSTs is associated with their pathological aggressiveness. LST-NG-PD carries the highest risk for deep SMI and poor differentiation, highlighting the importance of accurate endoscopic diagnosis for guiding treatment strategies.
P.073
CHARACTERISTICS AND DIAGNOSTIC ACCURACY OF ENDOSCOPIC ULTRASOUND IN LOWER GASTROINTESTINAL SUBEPITHELIAL LESIONS
Yu-Shiuan Liang1, Li-Chun Chang1, Weng-Fai Wong1,2, Ming-Lun Han1,2, Chieh-Chang Chen1, Chien-Chuan Chen1, Ping-Huei Tseng1,2
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Department of Integrated Diagnostics and Therapeutics, National Taiwan University Hospital, Taipei, Taiwan
下消化道上皮下病灶之內視鏡超音波影 像特徵與診斷準確性分析
梁友瑄1 張立群1 黃永輝1,2 韓明倫1,2 陳介章1 陳建全1 曾屏輝1,2
1 國立臺灣大學醫學院附設醫院胃腸肝膽科
2 國立臺灣大學醫學院附設醫院綜合診療部
Background: Lower gastrointestinal subepithelial lesions (LGI SELs) are being increasingly identified due to the widespread implementation of colorectal cancer screening programs. However, the diagnostic performance of endoscopic ultrasound (EUS) in LGI SELs, as well as the optimal approach for tissue acquisition remain insufficiently defined.
Aims: This study aims to characterize the EUS features of LGI SELs and evaluate the diagnostic yield and procedural outcomes of various tissue acquisition techniques.
Methods: This retrospective single-center observational study included 218 patients with 244 EUS-confirmed LGI SELs between May 2011 to February 2022. Each lesion was assessed using EUS to determine its anatomical location, size, involved GI wall layer(s), echogenicity, heterogeneity, and border characteristics. The diagnostic yield and procedural outcomes of various tissue acquisition techniques were evaluated. In case with conclusive histological diagnosis, the diagnostic sensitivity of EUS was compared with that of colonoscopy.
Results: The mean age was 56.3 years, with 49.7% being male. The majority of SELs were incidentally discovered (67%) and primarily located in the right-
sided colon (45%) and rectum (37%). Histologically, neuroendocrine tumors (NETs) and lipomas were the most frequently diagnosed lesions. EUS revealed distinct imaging characteristics for each lesion type and demonstrated high sensitivity, particularly for NETs (94%) and lipomas (96%). Tissue acquisition using both endoscopic or surgical resection achieved 100% diagnostic yield, significantly outperforming digging biopsy (71%, p < 0.001). Additionally, EUS significantly improved the diagnostic sensitivity for lipomas compared to colonoscopy alone (96% vs. 65%, p = 0.011).
Conclusions: EUS offers valuable characterization of LGI SELs, particularly for rectal NETs and lipomas. En bloc tissue acquisition methods, including endoscopic or surgical resection, demonstrated superior diagnostic yield compared to digging biopsy. EUS significantly enhanced diagnostic sensitivity compared to colonoscopy alone. These findings support the role of EUS as a complementary modality to colonoscopy in the evaluation of LGI SELs.
P.074
Chung-Hung Chen, Jyun-Wei Wang, Kuan-Wei Liu, Huai-Yi Huang, Sheng-Lei Yan, Chien-Hua Chen, Yung-Hsiang Yeh
Division of Gastroenterology, Department of Internal Medicine, Chang Bing Show Chwan Memorial Hospital, Changhua, Taiwan
探討 miR-145 對大腸直腸癌細胞奧沙利 鉑抗藥性的影響
陳忠宏 王俊偉 劉冠瑋 黃懷毅 顏聖烈 陳建華 葉永祥 彰濱秀傳紀念醫院胃腸肝膽科
Background: Oxaliplatin, a third-generation platinum-based chemotherapeutic agent, is widely used for the treatment of colorectal cancer (CRC). Despite its clinical success, the development of resistance to oxaliplatin significantly limits its longterm efficacy. Anti-apoptotic proteins such as cellular FLICE-inhibitory protein (c-FLIP), X-linked inhibitor of apoptosis protein (XIAP), and B-cell lymphoma 2 (Bcl2) have been implicated in mediating this resistance. MicroRNA-145 (miR-145) is a tumor-suppressive miRNA known to inhibit CRC cell invasion and may reduce chemoresistance.
Aims: This study aimed to investigate the effect of miR-145 on oxaliplatin resistance in CRC cells and to determine whether miR-145 modulates the expression of anti-apoptotic proteins.
Methods: Oxaliplatin-resistant CRC cell lines, HT29 OR and HCT116 OR, were developed and used for in vitro experiments. Cells were treated with miR145, oxaliplatin, or a combination of both for 48 hours. Cell viability was assessed using MTT assays. Apoptosis and invasive potential were measured by flow cytometry and invasion assays, respectively. The expression levels of anti-apoptotic proteins (c-FLIP, XIAP, and Bcl-2) were evaluated by Western blotting.
Results: Treatment with miR-145 significantly enhanced oxaliplatin-induced inhibition of cell viability, suppression of invasion, and induction of apoptosis in resistant CRC cells. Furthermore, miR145 reversed the oxaliplatin-induced upregulation of c-FLIP, XIAP, and Bcl-2 proteins.
Conclusions: miR-145 plays an inhibitory role in oxaliplatin resistance by downregulating anti-
apoptotic proteins and promoting apoptosis in CRC cells. These findings suggest that miR-145 may serve as a promising therapeutic target for overcoming chemoresistance in colorectal cancer.
P.075
APPLICATION OF COMPUTERAIDED DIAGNOSIS IN REAL-TIME COLONOSCOPY: THE IMPACT OF MAGNIFICATION ON THE ACCURACY OF COLORECTAL POLYP DIAGNOSIS
Chia-Lun
Liu, Peng-Jen Chen
Division of Gastroenterology, Department of Internal Medicine, Tri-Service General Hospital, Taipei, Taiwan
電腦輔助診斷於即時大腸鏡檢查之應 用:放大倍率對大腸息肉診斷準確性的
劉家綸 陳鵬仁
三軍總醫院胃腸科
Background: Colorectal cancer is a leading cause of cancer-related mortality worldwide. Colonoscopy remains the gold standard for early detection and removal of precancerous polyps. However, diagnostic performance can vary among endoscopists due to differences in experience. Recently, computer-aided diagnosis (CADx) systems have emerged to assist in real-time polyp diagnosis. Yet, the influence of endoscopic magnification on CADx performance remains unclear.
Aims: To evaluate whether endoscopic magnification (1X, 60X, 145X) affects the diagnostic performance of a CADx system in real-time colonoscopy, with a primary focus on sensitivity and secondary outcomes including specificity, PPV, NPV, and accuracy.
Methods: A total of 108 colorectal polyps were analyzed using the CADeye system (Fujifilm, Japan) under three magnification settings during real-time colonoscopy. A CADx output of “Neoplastic” was considered a positive finding. Sensitivity, specificity, PPV, NPV, and accuracy were calculated for each setting. McNemar’s test and chi-square tests were performed to assess statistical significance among magnification levels.
Results: Sensitivity improved significantly with magnification (1X: 64.8%, 60X: 81.3%, 145X: 85.7%; p = 0.0019). Accuracy also increased with magnification (1X: 66.7%, 60X: 76.8%, 145X: 80.5%; p = 0.0368). Specificity decreased at higher magnification (1X: 76.4%, 145X: 52.9%), although the difference was not statistically significant (p = 0.3569). PPV remained consistently high across all
settings (>90%), while NPV remained low (28.8%–40.9%), with no significant differences in either metric (PPV: p = 0.7946; NPV: p = 0.5210).
Conclusions: Higher endoscopic magnification significantly enhances the sensitivity and accuracy of CADx for polyp detection, without compromising predictive values.
P.076
Chi-Hsien Chang, Kwei-Ming Chen, Chi-Chieh Yang, Chien-Hua Chen
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Show Chwan Memorial Hospital, Changhua, Taiwan
大腸憩室糞石的全新內視鏡移除術 張吉賢 陳奎閔 楊基滐 陳建華 秀傳醫療社團法人秀傳紀念醫院胃腸肝膽科
Background: Colonic diverticula are pseudodiverticula that involve only the inner layers of the colonic wall. When the diverticular neck is narrow, retained stool can become compacted and form a fecalith (bezoar). In cases of diverticular bleeding, fecalith impaction may hinder effective hemostasis due to obscured visualization of the bleeding vessel. Conventional methods, such as water irrigation or forceps grasping, are often ineffective in removing fecaliths. Therefore, we developed a novel endoscopic technique for the removal of fecaliths in colonic diverticula.
Aims: To evaluate the efficacy of a novel endoscopic technique for removing fecaliths in colonic diverticula.
Methods: During colonoscopy, we repeatedly inserted the tip of an ERCP cannulation catheter (Olympus Star Tip V) between the fecalith and the diverticular opening while applying water irrigation. This technique facilitated fecalith dislodgement in most cases, except when the diverticulum was in an unfavorable position. Inclusion criteria: presence of diverticular fecaliths identified by colonoscopy, including during health examinations. Exclusion criteria: intolerance to colonoscopy or unstable vital signs during the procedure. Each fecalith removal was considered an independent episode, even when occurring in the same patient.
Results: From October 2020 to July 2022, we attempted 18 fecalith removal episodes in 14 patients using the catheter technique. Successful removal was achieved in 16 episodes involving 12 patients, yielding an overall success rate of 88.9% (16/18). The duration of successful procedures ranged from 12 to 327 seconds, with a mean time of 107 seconds. A major complication occurred in one
patient (1/14, 7.1%) involving colonic perforation, which was located at the distal site of diverticula (hepatic flexure) and not at the site of fecalith removal. No delayed bleeding or diverticulitis was observed.
Conclusions: Fecalith impaction in colonic diverticula may be predisposing factor to diverticulitis or diverticular bleeding. This novel endoscopic technique, applying water irrigation through an ERCP cannulation catheter, is effective and may prove beneficial as a preparatory step before hemostasis in cases of colonic diverticular bleeding.
P.077
COMMUNITY-BASED HELICOBACTER PYLORI SCREENING AND ERADICATION BY EMPIRIC REGIMENS IN SOUTHWESTERN TAIWAN TOWNSHIPS
Yuan-Jie Ding1, Hsiu-Ping Wen1, Wei-Ming Chen1,2, Wei-Lin Tung1, Yun-Yu Heish1,2, Yi-Hsing Chen1, Kao-Chi Chang1, Wen-Hua Chao3, Hong-Hsia Cheng4, Te-Sheng Chang1,2
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Chang Gung Memorial Hospital, Chiayi, Taiwan
2College of Medicine, Chang Gung University, Taoyuan, Taiwan
3Chiayi County Health Bureau, Chiayi, Taiwan
4Cancer Center, Chang Gung Memorial Hospital, Chiayi, Taiwan.
台灣西南部鄉鎮社區型幽門螺旋桿菌篩 檢與經驗性根除治療計畫
丁元捷1 温修平1 陳慰明1,2 童威霖1 謝詠諭1,2 陳奕行1
張國基1 趙紋華3 鄭紅霞4 張德生1,2
1 嘉義長庚紀念醫院胃腸肝膽科
2 長庚大學醫學院
3 嘉義縣衛生局
4 嘉義長庚紀念醫院癌症中心
Background: The recent Taipei Global Consensus recommends screening and eradication of Helicobacter pylori (H. pylori) in populations from regions with a high prevalence of gastric cancer. However, in most areas of Taiwan, the prevalence of H. pylori and the optimal treatment strategy remain unclear.
Aims: This study aimed to assess the prevalence of H. pylori infection among adults aged 50–69 in southwestern Taiwan and to compare the eradication rates between 14-day proton pump inhibitor-based triple therapy and concomitant quadruple therapy. The findings aim to inform effective screening and treatment strategies for community-based H. pylori management.
Methods: Since 2002, the Chiayi County Health Bureau has implemented a county-wide communitybased health promotion program. Stool H. pylori antigen (HpSA) screening was added for individuals aged 50–69 in July 2023. Participants with positive
HpSA results were referred for further consultation. This study analyzed 531 patients who received consultation at Chiayi Chang Gung Memorial Hospital between July 2023 and June 2024.
Results: Among the 5,749 participants who underwent HpSA screening during the study period, 1,470 (25.6%) tested positive. Of the 531 patients evaluated at this hospital, 458 (86.3%) underwent endoscopy, which identified gastric ulcers in 24.5%, duodenal ulcers in 17.0%, and both in 6.6%. Rapid urease test and histological assessment were performed in 315 and 158 patients, respectively, yielding a positivity rate of 87.0% and 86.7% respectively. Among the 443 patients with available follow-up data, eradication rates were 93.9% (245/261) for those receiving 14-day proton pump inhibitor-based triple therapy and 93.1% (149/160) for those receiving concomitant therapy (p = 0.548).
Conclusions: The current prevalence of H. pylori for adults of southwestern Taiwan is approximately 25.6%. Concomitant quadruple therapy and standard triple therapy for 14 days had comparable eradication rates of 93.9% and 93.1%, respectively.
P.078
ENDOSCOPIC DIAGNOSIS OF HELICOBACTER PYLORI INFECTION USING A SIMPLIFIED KYOTO CLASSIFICATION OF GASTRITIS: PRELIMINARY RESULTS FROM A SINGLE-CENTER PROSPECTIVE STUDY
Shu-Wei Huang1, Po-Han Huang1, Hao-Tsai Cheng1, Shu-Ying Chiu2, Yen-Chin Chen3, Ming-Yao Su1
1Department of Gastroenterology and Hepatology, New Taipei Municipal Tucheng Hospital, New Taipei City, Taiwan
2Department of Laboratory Medicine, New Taipei Municipal Tucheng Hospital, New Taipei City, Taiwan
3Molecular Infectious Disease Research Center, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
運用簡化版京都胃炎分類進行幽門螺旋 桿菌感染之內視鏡診斷:單一中心前瞻 性研究初步結果
黃書偉1 黃柏翰1 鄭浩材1 邱淑英2 陳彥瑾3 蘇銘堯1
1 新北市立土城醫院(委託長庚醫療財團法人興建經 營)胃腸肝膽科
2 新北市立土城醫院(委託長庚醫療財團法人興建經 營)檢驗醫學科
3 林口長庚紀念醫院分子感染症醫學研究中心
Background: The diagnostic accuracy of endoscopy for detecting Helicobacter pylori (H. pylori) infection has been relatively low in earlier studies. However, with the introduction of the Kyoto Classification of Gastritis, endoscopic diagnostic performance has significantly improved. Nonetheless, the effectiveness of the simplified Kyoto Classification in detecting H. pylori infection in the Taiwanese population remains unknown.
Aims: To evaluate the diagnostic accuracy of the simplified Kyoto Classification of Gastritis for endoscopic detection of H. pylori infection in a Taiwanese cohort.
Methods: This ongoing prospective, single-center study is being conducted at New Taipei Municipal Tucheng Hospital. Eligible participants were outpatients aged >18 years who required upper gastrointestinal endoscopy and provided written
informed consent. Exclusion criteria included recent use (within 1 month) of proton pump inhibitors (PPIs), antibiotics, or bismuth-containing agents; major systemic illness; use of antiplatelet or anticoagulant agents; history of H. pylori eradication within the past year; or prior gastrectomy. Preliminary results were based on patients enrolled between July 2024 and May 2025. All patients underwent diagnostic upper gastrointestinal endoscopy, and endoscopic images were independently reviewed by three experienced endoscopists who were blinded to the patients’ H. pylori status. The simplified Kyoto Classification was applied, evaluating four features: spotty redness, mucosal swelling, diffuse redness, and nodularity. Each feature was scored using a 3-point scale (0 = absent, 1 = present with low confidence, 2 = present with high confidence), and the total score (range: 0–8) was calculated. H. pylori infection was defined by concordant positive results from the rapid urease test. Patients with a positive urease test also underwent H. pylori culture for confirmation. Diagnostic performance metrics were calculated. Results: A total of 112 patients were enrolled. The mean age was 58.18 ± 12.23 years, and 48.21% were male. Among them, 33.93% tested positive for H. pylori based on the rapid urease test. All rapid urease test positive cases were confirmed by H. pylori culture. ROC curve analysis was performed for each endoscopic feature and the total score. Mucosal swelling had the highest AUROC (0.8867), followed by diffuse redness (0.8601), spotty redness (0.7344), and nodularity (0.6451). The simplified Kyoto score yielded an AUROC of 0.9772. At the optimal cutoff score of ≥2 (based on Youden’s index), the model achieved 94.74% sensitivity, 93.24% specificity, 87.80% PPV, 97.18% NPV, and 93.75% overall accuracy.
Conclusions: The simplified Kyoto Classification demonstrated excellent diagnostic accuracy for H. pylori infection in this preliminary study. A total score ≥2 provided high sensitivity and specificity, supporting its potential as a practical real-time endoscopic screening tool.
P.079
VONOPRAZAN TRIPLE THERAPY VERSUS BISMUTH QUADRUPLE THERAPY IN THE FIRST-LINE TREATMENT OF H. PYLORI INFECTION
Jiunn-Wei Wang1,2,8, Ping-I Hsu3,8, Chang-Bih Shie3,8, Yu-Hwa Liu4,8, Ming-Jen Sheu5,8, Jyh-Chin Yang6,8, Chia-Long Lee7,8, Chao-Hung Kuo1,2, Deng-Chyang Wu1,2
1Division of Gastroenterology, Department of Internal medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
2Department of Medicine, Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
3Department of Medicine, An Nan Hospital, China Medical University, Tainan, Taiwan
4Division of Gastroenterology, Department of Internal Medicine Shin Kong Wu Huo-Shih Memorial Hospital, Taipei, Taiwan
5Division of Hepatogastroenterology, Department of Internal Medicine, Chi Mei Medical Center, Tainan, Taiwan
6Division of Gastroenterology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
7Division of Gastroenterology and Hepatology, Department of Internal Medicine, Cathay General Hospital, Taipei, Taiwan
8Taiwan Acid-related Disease and Microbiota (TARD-M) Consortium
Vonoprazan 的三合療法與 Bismuth 的四 合療法在幽門螺旋桿菌感染一線治療中 的臨床比較
王俊偉1,2,8 許秉毅3,8 施長碧3,8 劉玉華4,8 許銘仁5,8 楊智欽6,8 李嘉龍7,8 郭昭宏1,2 吳登強1,2
1 高雄醫學大學附設中和紀念醫院胃腸內科
2 高雄醫學大學醫學系
3 臺南市立安南醫院消化內科
4 新光吳火獅紀念醫院胃腸肝膽科
5 奇美醫院胃腸肝膽科
6 國立臺灣大學醫學院附設醫院胃腸肝膽科
7 國泰綜合醫院腸胃內科
8 台灣胃酸相關疾病暨微菌叢聯盟
Background: Currently, most international guidelines recommend bismuth quadruple therapy for H. pylori infection in areas with high clarithromycin resistance. However, bismuth quadruple therapy is a complex regimen and has high occurrence of adverse events. Recently, potassium-competitive acid blocker (PCAB) triple therapy has been applied to treat H. pylori infection and can achieve a high eradication rate in some countries.
Aims: To compare the efficacy and safety of vonoprazan/amoxicillin/clarithromycin triple therapy with a 10-day bismuth quadruple therapy as first-line treatments for H. pylori infection in Taiwan.
Methods: We conducted a retrospective cohort study of patients with H. pylori infection treated with either 14-day vonoprazan triple therapy (vonoprazan 20 mg twice daily and amoxicillin 750 mg four times daily) or 10-day bismuth quadruple therapy (tripotassium dicitrato bismuthate 300 mg four times daily, rabeprazole 20 mg twice daily, tetracycline 500 mg four times daily, and metronidazole 500 mg four times daily) between January 2019 and September 2024 at eight hospitals in Taiwan. Post-treatment H. pylori status was assessed at least four weeks following eradication therapy.
Results: The study included 302 patients in the vonoprazan triple therapy group and 306 in the bismuth quadruple therapy group. Intentionto-treat analysis showed that the eradication rates of vonoprazan triple therapy and bismuth quadruple therapy were 90.1% (272/302) and 90.2% (276/306), respectively. The two patient groups had comparable eradication rate. Per-protocol analysis yielded similar results (93.4% vs. 94.6%). Adverse events were significantly fewer in the vonoprazan triple group compared to bismuth quadruple group (15.2% vs. 31.7%, P < 0.01), while drug adherence was comparable between groups (98.0% vs. 93.5%).
Conclusions: Fourteen-day vonoprazan triple therapy and 10-day bismuth quadruple therapy have comparable eradication rates for H. pylori infection in Taiwan. However, the former has fewer adverse events than the latter.
P.080
HELICOBACTER PYLORI INFECTION AS AN INDEPENDENT RISK FACTOR FOR EARLY-ONSET COLORECTAL NEOPLASTIC POLYPS
Tzu-Min Yu1, Jyh-Ming Liou1,2, Ming-Shiang Wu1, Tzu-Chan Hong1,2
1Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Department of Medicine, National Taiwan University Cancer Center, Taipei, Taiwan
幽門螺旋桿菌感染為早發性大腸直腸息 肉之獨立危險因子
游子民1 劉志銘1,2 吳明賢1 洪子瞻1,2
1 台大醫院內科部
2 台大醫院癌醫分院綜合內科部
Background: Previous studies have examined the association between Helicobacter pylori infection and colorectal polyps, but the findings have been inconsistent. Unlike established risk factors such as metabolic syndrome or cigarette smoking, H. pylori infection does not exhibit a clear time-dependent relationship with polyp development. This discrepancy raises the hypothesis that age may act as a key effect modifier in the association between H. pylori infection and neoplastic colorectal polyps.
Aims: We aim to investigate the association between H. pylori infection and colorectal polyps in different age populations.
Methods: We retrospectively analyzed adults in a health examination-based cohort who underwent urea breath tests (UBT) to identify H. pylori infection, colonoscopy, and metabolic syndrome evaluations between 2021 and 2024. We performed logistic regression to assess the risk of colorectal neoplastic polyps. Stratified analyses were conducted based on a cutoff age of 45 years, a guideline-recommended initiation age for endoscopic surveillance.
Results: Among the 1,403 individuals included in the analyses (mean age 50.1 ± 11.6 years, 45.6% male), 266 (19.0%) were diagnosed with metabolic syndrome, 191 (13.6%) tested positive for UBT, and 409 (29.2%) were found to have neoplastic colorectal polyps. UBT positivity was associated with the presence of neoplastic polyps in univariable analysis (OR = 1.45, p = 0.025), but the association disappeared after adjustment for age, sex, smoking, metabolic syndrome, alcohol and history of colon
polyps. In subgroup analysis, a positive UBT result was significantly associated with an increased risk of neoplastic colorectal polyps in adults younger than 45 years (adjusted OR = 2.47, p = 0.027), but not in those aged 45 and older (adjusted OR = 1.05, p = 0.800). Interaction testing confirmed a significant age-modifying effect at the 45-year-cutoff (interaction term OR = 2.53, p = 0.037). Sensitivity analyses across age showed an age-dependent decrease in the influence on H. pylori infection to neoplastic colorectal polyps.
Conclusions: Our findings indicate that H. pylori infection is significantly associated with neoplastic colorectal polyps among adults younger than 45 years, but not in older age groups where traditional metabolic risk factors appear to play a dominant role. This age-specific risk may inform future targeted prevention strategies in younger populations and provide clues for investigating microbial or immunemediated mechanisms in early-onset colorectal neoplastic polyps.
P.081
Taiga Morita
Tsukuba Memorial Hospital, Tokyo Medical Univercity, Ibaraki, Japan
Background: In Japan, the standard regimens for Helicobacter pylori (H. pylori) eradication are potassium-competitive acid blocker (P-CAB), amoxicillin (AMPC), and clarithromycin (CAM) for first-line therapy and P-CAB, AMPC, and metronidazole (MNZ) for second-line treatment. In Japan, the CAM resistance rate is 30%–40%, resulting in notably low first-line eradication success for resistant strains. However, the high efficacy of second-line therapy (>95%) has obscured the applicability of CAM resistance testing, which is well established in Western countries. In Taiwan, H. pylori eradication regimens differ from those in Japan with respect to antimicrobial selection and resistance patterns. Since its insurance approval in Japan in November 2022, we evaluated the clinical utility of polymerase chain reaction (PCR) testing for CAM resistance mutations through treatment analysis.
Aims: To investigate the selection and therapeutic efficacy of eradication treatment regimens based on CAM resistance testing.
Methods: We studied 155 cases diagnosed with H. pylori infection by gastric juice PCR from July 2023 to June 2024. We analyzed the eradication outcomes of 36 CAM-resistant cases, with successful eradication verified by urea breath test performed at least 4 weeks after treatment completion.
Results: There were 19 males and 17 females, aged 30–76 years (mean age, 53.7 years). Three cases had previous eradication attempts with undocumented regimen. Of the 36 cases, 31 received eradication treatment. The drug regimens were P-CAB, AMPC, and CAM in 14 cases and P-CAB, AMPC, and MNZ in 17 cases. Initial eradication therapy was markedly more successful in cases treated with P-CAB, AMPC, and MNZ (88.2%) compared to P-CAB, AMPC, and CAM (42.8%).
Conclusions: Gastric juice PCR testing for CAM resistance supports personalized H. pylori treatment in Japan, potentially improving initial eradication rates. The significant difference in eradication rates between regimens demonstrates the clinical value of resistance testing.
P.082
Yi-Hsiang Huang1, Song-Wei Wang1, Yao-Kuang Wang1,2, Chao-Hung Kuo1,2, Deng-Chyang Wu1,2, Jeng-Yih Wu1,2
1Division of Gastroenterology, Department of Internal Medicine Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
2School of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
台灣南部幽門螺旋桿菌抗生素抗藥性回 顧性分析(2022–2024)
黃奕翔1 王崧維1
1,2
1,2
1 高雄醫學大學附設中和紀念醫院胃腸內科 2 高雄醫學大學醫學系
1,2
Background: The elimination of Helicobacter pylori (H. pylori) has become a critical clinical concern in recent decades, as successful treatment not only reduces the recurrence of peptic ulcers but also lowers the risk of gastric cancer. Among the various factors contributing to treatment failure, the emergence of antibiotic resistance plays the most significant role in the declining eradication rates.
Aims: This study focuses on phenotypic analysis of antibiotic resistance patterns in H. pylori isolates.
Methods: This retrospective study included H. pylori isolates obtained from patients who underwent esophagogastroduodenoscopy (EGD) between January 1, 2022, and December 31, 2024. Bacterial cultures were performed using previously established methods. Antibiotic susceptibility was assessed using the E-test (AB Biodisk, Solna, Sweden). Resistance was defined based on minimum inhibitory concentration (MIC) thresholds: ≥1 mg/mL for clarithromycin, ≥8 mg/mL for metronidazole, ≥1 mg/mL for levofloxacin, ≥0.5 mg/mL for amoxicillin, and ≥1 mg/mL for tetracycline.
Results: A total of 158 H. pylori strains were cultured from 670 subjects. Among them, 102 strains were from treatment-naïve patients and 56 strains from non-naïve patients. In the treatment-naïve group, resistance rates were: clarithromycin 24.5%, metronidazole 29.4%, levofloxacin 31.4%, amoxicillin 1%, and tetracycline 2.9%. In non- naïve patients, the
resistance rates of clarithromycin, metronidazole, levofloxacin, amoxicillin, and tetracycline were 75%, 62.5%, 83.9%, 1.79%, 10.7%, respectively.
Conclusions: According to the World Health Organization (WHO), antibiotic stewardship is a coordinated approach that promotes the appropriate use of antibiotics by ensuring the correct drug, dosage, and treatment duration. This strategy aims to improve clinical outcomes, limit the development of antibiotic resistance, and reduce healthcare-associated infections. Periodic surveillance of antibiotic resistance is essential to guide effective treatment strategies. The data from this study may serve as a reference for selecting optimal H. pylori eradication regimens in Southern Taiwan.
P.083
ENDOSCOPIC AND CLINICAL FEATURES COULD HELP TO IMPROVE THE DIAGNOSTIC DELAY IN H. PYLORI-INFECTED PATIENTS WITH NEGATIVE RESULTS IN EARLIER STUDIES
Yu-Ching Tsai1,2, Chung-Tai Wu2,3, Er-Shiang Yang2, Ming-Tsung Hsieh2, Chun-Te Lee2, Hsiao-Bai Yang4,5, Hsiu-Chi Cheng2,3,6, Bor-Shyang Sheu2,3
1Department of Gastroenterology and Hepatology, Tainan Hospital, Ministry of Health and Welfare, Executive Yuan, Tainan, Taiwan
2Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan
3Institute of Clinical Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan
4Department of Pathology, Ton Yen General Hospital, Hsinchu, Taiwan
5Department of Pathology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan
6Institute of Molecular Medicine, National Cheng Kung University, Tainan, Taiwan
利用內視鏡與臨床特徵可幫助改善幽門 桿菌感染患者的延遲診斷
蔡郁清1,2 吳忠泰2,3 楊貳翔2 謝明宗2 李俊德2 楊曉白4,5 鄭修琦2,3,6 許博翔2,3
1 衛生福利部臺南醫院胃腸科
2 國立成功大學醫學院附設醫院內科部
3 國立成功大學臨床醫學研究所
4 東元綜合醫院病理科
5 國立成功大學醫學院附設醫院病理部
6 國立成功大學分子醫學研究所
Background: We sometimes fail to diagnose H. pylori-infected patients in earlier studies.
Aims: The present study aims to compose a scoring system with patients’ clinical/endoscopic features to improve the delay-diagnosis of H. pylori infection.
Methods: We enrolled 20 H. pylori-infected patients with H. pylori-negative (HP(-)) results in endoscopies within the past 2 years (study group). We also
enrolled 41 age-and sex-matched H. pylori-positive (HP(+)) patients diagnosed in first endoscopies and 53 HP(-) patients without H. pylori infection history to be the control groups (HP(+) controls/HP(-) controls). We compared the clinical/endoscopic features within the study and control groups and composed a scoring system to improve the diagnosis-delay of H. pylori-infections.
Results: The study group patients had higher prevalence of H. pylori eradication history (65% vs. 2.4%, p < 0.001), more corpus and lesion distribution of the bacteria (65% vs. 12.2%, p < 0.001) and lower H. pylori densities (p < 0.01) than the HP(+) controls. The study group patients also had more advanced intestinal metaplasia presence (OLGIM stage III/IV) than the control groups (53.3% vs. 34.1%&18.5%, p = 0.021). We composed a HP-prediction score: 1. HP(-): a. Normal corpus mucosa with regular arrangement of collecting venules (RAC(+)); b. Gastric fundic gland polyps+initial diagnosis as GERD. 2. HP(+): a. More than two of the following: corpus IM and atrophy, corpus dilated subepithelial capillaries, at least Kimura-Takemoto C-1 type atrophy and advanced endoscopic grading of gastric intestinal metaplasia (EGGIM) score; b. Corpus mucosa RAC(-) + no fundic gland polyp + initial diagnosis not GERD. It’s sensitivity, specificity, positive predictive value, negative predictive value, and accuracy to predict HP(+) were 97.44% (95% CI 86.52%–99.94%), 79.07% (95% CI 63.96%–89.96%), 80.85% (95% CI 70.21%–88.32%), 97.14% (95% CI 83.00%–99.58%), and 87.80% (95% CI 78.71%–93.99%). The area under ROC curve was 0.883.
Conclusions: The HP-prediction score could help to improve initial H. pylori-infection diagnosis in our daily clinical work.
P.084
SERUM MICROELEMENT STATUS AND ITS ASSOCIATION WITH DISEASE ACTIVITY IN CROHN’S DISEASE: A CROSS-SECTIONAL STUDY
Tien-Yu Huang1, Chao-Feng Chang1, Peng-Jen Chen1, Yu-Lueng Shih1,2, Wei-Kuo Chang1, Tsai-Yuan Hsieh1
1Division of Gastroenterology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan 2Division of Gastroenterology, Department of Internal Medicine, Taichung Armed Forces General Hospital, Taichung, Taiwan
克隆氏症患者血清微量元素狀態與疾病 活動度之關聯:一項橫斷性研究
1 國防醫學院三軍總醫院胃腸科
2 國軍臺中總醫院腸胃內科
Background: Trace elements such as selenium (Se), zinc (Zn), and copper (Cu) are essential for immune regulation and oxidative balance. Imbalances in these microelements have been linked to inflammatory responses in Crohn’s disease (CD), but clinical correlations remain underexplored.
Aims: To assess serum Se, Zn, and Cu levels and examine their associations with clinical disease activity in patients with Crohn’s disease.
Methods: This cross-sectional study enrolled patients diagnosed with CD and healthy controls. After informed consent, venous blood was collected for trace element analysis at the Toxicology Center of the National Defense Medical Center. Clinical activity was evaluated using the Crohn’s Disease Activity Index (CDAI), Harvey-Bradshaw Index (HBI), CRP, ESR, and fecal calprotectin. Statistical analyses included Mann-Whitney U and Kruskal-Wallis tests using SPSS v20.
Results: A total of 104 participants were included. CD patients demonstrated significantly lower serum Se and Zn levels and higher Cu levels compared to healthy controls. Serum Se and Zn levels were inversely correlated with CDAI, HBI, and CRP, whereas serum Cu showed a positive correlation. Elevated Cu/ Zn and Cu/Se ratios were also significantly associated with higher disease activity scores. Patients with
moderate-to-severe CD had a higher prevalence of Se and Zn deficiency and a more pronounced elevation in Cu-related ratios.
Conclusions: Serum trace element imbalances, notably low Se and Zn and elevated Cu, are associated with increased disease activity in Crohn’s disease. The Cu/Zn and Cu/Se ratios may serve as potential biomarkers for monitoring inflammatory burden and disease progression in CD patients.
A SYSTEMATIC REVIEW AND NETWORK META-ANALYSIS
Chih-Wen Huang, Yang-Yuan Chen
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan
發炎性腸道疾病病患使用生物製劑的懷 孕安全性:系統性回顧與網絡統合分析 黃稚雯 陳洋源 彰化基督教醫院胃腸肝膽科
Background: The safety of biologic therapies during pregnancy in patients with inflammatory bowel disease (IBD) remains an area of clinical concern, particularly with the increasing use of novel agents such as ustekinumab (UST) and vedolizumab (VDZ).
Aims: We conducted a network meta-analysis (NMA) to compare pregnancy-related outcomes among various biologic agents and non-biologics exposure patients.
Methods: This study systematically searched for comparative studies reporting pregnancy outcomes in IBD patients exposed to biologics or conventional therapies (CT). Outcomes evaluated included preterm birth (PB), congenital malformation (CM), low birth weight (LBW), and spontaneous abortion (SA). A NMA model was applied. Subgroup analysis was performed for studies with comparable baseline disease activity between treatment groups.
Results: Twelve studies were included. Anti-TNF agents were not associated with increased risk of any adverse pregnancy outcomes. UST and VDZ were associated with increased risks of CM (UST: OR 2.32 [1.31–4.10]; VDZ: OR 1.98 [1.11–3.52]), and VDZ with LBW (OR 2.17 [1.15–4.11]). These associations were not significant in subgroup analyses limited to studies with similar disease activity. Sensitivity analysis revealed the CM risk for UST was driven by a single influential study, while the LBW risk with VDZ remained consistent.
Conclusions: This is the first NMA to evaluate pregnancy-related safety outcomes across various biologic agents in patients with IBD, including novel therapies such as UST and VDZ. Anti-TNF agents remain the safest option during pregnancy. Although UST and VDZ showed signals of risk in the
overall analysis, these associations were attenuated in subgroup and sensitivity analyses, suggesting potential confounding. Further prospective research is warranted to confirm the safety profile of non–anti-TNF biologics.
P.086
Shu-Hsien Lin, Chu-Kuang Chou, Li-Jen Chang, Chang-Chao Su, Po-Chun Yang, Kok-Yean Koh, Tsung-Jung Tsai, Ming-Tse Hsu, Chi-Yi Chen, Po-Yueh Chen
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan
小腸內膽汁影像與慢性疾病相關性研究
林淑賢 周莒光 張力仁 蘇昶昭 楊博鈞 許國衍 蔡崇榮 許銘澤 陳啟益 陳柏岳
戴德森醫療財團法人嘉義基督教醫院胃腸肝膽科
Background: In capsule endoscopy, bile is often viewed as a confounding factor that obscures small intestinal lesions. However, bile itself plays a significant physiological role in digestion and may reflect systemic disease states. Its appearance and distribution in the small intestine could offer valuable diagnostic information, especially in chronic disease contexts.
Aims: This study investigated the imaging characteristics of small intestinal bile in various chronic diseases using capsule endoscopy. We aimed to assess its diagnostic relevance and spectral properties through hyperspectral image simulation. Methods: We collaborated with the Departments of Gastroenterology and Hepatobiliary Medicine at Chia-Yi Christian Hospital. White light images were obtained using PillCam™ SB 3 capsule endoscopy from 61 patients. After preprocessing, we selected 820 images—410 from the proximal and 410 from the distal small intestine. These included cases from six clinical groups: cardiovascular-related diseases (n = 70), liver-related diseases (n = 50), intestinalrelated diseases (n = 60), kidney-related diseases (n = 50), anemia (n = 60), and healthy controls (n = 120). Bile areas in each image were manually annotated. Using hyperspectral imaging (HSI) simulation and band selection, we converted the white light images into hyperspectral narrow-band images. We applied the CIEDE2000 color difference metric to assess bile color differences between proximal and distal segments. Principal component analysis (PCA) was used to identify spectral patterns associated with
each disease group.
Results: The simulated hyperspectral imaging revealed distinct spectral profiles of bile across disease categories. Color difference analysis via CIEDE2000 showed statistically significant variations between proximal and distal small intestinal bile in several disease groups, particularly in liver-related and cardiovascular conditions. PCA enabled partial separation of disease clusters based on their spectral features, indicating potential diagnostic relevance. Conclusions: This study demonstrates that small intestinal bile, often overlooked in endoscopic imaging, exhibits disease-specific spectral and spatial characteristics. Hyperspectral simulation combined with color and spectral analysis may serve as a non-invasive tool to assist in differentiating chronic diseases via capsule endoscopy. Further validation in larger cohorts could lead to new diagnostic markers in gastrointestinal imaging.
P.087
THE ROLE OF RISANKIZUMAB IN MODERATE-TO-SEVERE CROHN’S DISEASE: DOSE-DEPENDENT BENEFITS REVEALED IN METAANALYSIS
Chao-Feng Chang1, Tien-Yu Huang1, Wei-Kuo Chang1, Po-Feng Huang1
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center
Risankizumab 治療中度至重度克隆氏
Background: Crohn’s disease is a chronic inflammatory condition of the gastrointestinal tract. Interleukin-23 (IL-23) has been identified as a key cytokine in the disease’s pathogenesis. Risankizumab, an IL-23 inhibitor, has shown promise in managing moderate-to-severe Crohn’s disease. Aims: We aim to evaluate the efficacy and safety of Risankizumab in Crohn’s disease through a metaanalysis of randomized controlled trials (RCTs). Meanwhile, dose- and duration-dependent effects into optimal treatment strategies would be explored. Methods: A meta-analysis of four high-quality RCTs including 1,774 patients was conducted. Outcomes included clinical remission, clinical response, and endoscopic remission. Heterogeneity and sensitivity analyses were performed. Meta-regression was used to assess dose- and duration-response relationships. Results: Risankizumab significantly increased the odds of clinical remission (OR = 2.223; 95% CI: 1.630–3.033; p < 0.001; I² < 0.01%); clinical response (OR = 3.618; 95% CI: 2.361–5.545; p < 0.001; I² = 50.95%); endoscopic remission (OR = 5.741; 95% CI: 2.603–12.66; p < 0.001; I² < 0.01%). Also, sensitivity analysis confirmed the robustness of these results. Meta-regression indicated a dose-dependent improvement in all three outcomes. Longer treatment duration was significantly associated with clinical remission but not with other outcomes.
Conclusions: A previous systematic review confirmed the efficacy and safety of IL-23 and IL12/23 inhibitors in moderate-to-severe Crohn’s disease. However, registry-based data on IL-23p19
antagonists remain limited. Our study builds on this by demonstrating dose-dependent efficacy and the benefits of prolonged treatment in achieving clinical remission. Using one-study-removed sensitivity analysis and odds ratios, we show moderate efficacy in improving clinical outcomes.
P.088
VERY EARLY BIOLOGIC THERAPY WITHIN 6 MONTHS OF CROHN’S DISEASE DIAGNOSIS IMPROVES ONE-YEAR STEROID-FREE CLINICAL REMISSION: A SINGLE-CENTER RETROSPECTIVE COHORT STUDY
Yen-Cheng Chang1, Tai-Di Chen1,2,3, Chia-Jung Kuo1,3,4,5,6, Chien-Ming Chen3,7, Chen-Wang Chang6,8,9,10, Jen-Wei Chou6,11,12, Cheng-Tang Chiu1,3,4,5,6, Ming-Yao Su3,6,13, Yu-Bin Pan14, Puo-Hsien Le1,3,4,5,6
1College of Medicine, Chang Gung University, Taoyuan, Taiwan
2Department of Pathology, Chang Gung
Memorial Hospital, Linkou, Taoyuan, Taiwan
3Chang Gung Inflammatory Bowel Disease Center, Linkou, Taoyuan, Taiwan
4Chang Gung Microbiota Therapy Center, Linkou, Taoyuan, Taiwan
5Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
6Taiwan Association for the Study of Intestinal Diseases (TASID), Taoyuan, Taiwan
7Department of Medical Imaging and Interventions, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
8Division of Gastroenterology, Department of Internal Medicine, MacKay Memorial Hospital, Taipei, Taiwan.
9MacKay Junior College of Medicine, Nursing and Management, Taipei, Taiwan
10MacKay Medical College, New Taipei City, Taiwan
11Center for Digestive Medicine, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan
12School of Chinese Medicine, China Medical University, Taichung, Taiwan
13Division of Gastroenterology and Hepatology, Department of Internal Medicine, New Taipei Municipal Tucheng Hospital, Tucheng, New Taipei City, Taiwan
14Biostatistical Section, Clinical Trial Center, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
克隆氏症確診後六個月內極早期使用生
物製劑可改善一年內無類固醇臨床緩解 率:單一中心回溯性世代研究
張晏誠1 陳泰迪1,2,3 郭家榮1,3,4,5,6 陳建銘3,7 章振旺6,8,9,10
周仁偉6,11,12 邱正堂1,3,4,5,6 蘇銘堯3,6,13 潘裕賓14
李柏賢1,3,4,5,6
1 長庚大學醫學系
2 林口長庚紀念醫院解剖病理科
3 林口長庚紀念醫院發炎性腸道疾病中心
4 林口長庚紀念醫院微菌治療中心
5 林口長庚紀念醫院胃腸肝膽科
6 台灣腸道醫學會
7 林口長庚紀念醫院影像診療科
8 馬偕紀念醫院胃腸肝膽科
9 馬偕醫護專校
10 馬偕醫學院
11 中國醫藥大學附設醫院消化系內科
12 中國醫藥大學中醫學院
13 新北市立土城醫院胃腸肝膽科
14 林口長庚紀念醫院臨床試驗中心生物統計組
Background: Early use of biologics improves Crohn’s disease (CD) outcomes. Evidence now indicates that initiating therapy within six months of diagnosis—the “very early” window—may yield additional benefit over the traditional ≤2year target. We therefore compared oneyear outcomes after very early (<6 months) versus early (6–24 months) biologic initiation in routine practice.
Aims: Our findings aim to inform optimal timing of biologic intervention in newly diagnosed CD.
Methods: In this retrospective cohort (March 2018 – June 2025), biologicnaïve adults with CD and ≥52 weeks of followup were stratified by time from diagnosis to first biologic: Very Early (<6 months) or Early (6–24 months). The primary endpoint was steroidfree clinical remission at week 52. Multivariate logistic regression identified variables independently associated with remission.
Results: Ninetysix patients were analysed (Very Early = 52; Early = 44). Baseline characteristics were comparable except for a higher proportion of corticosteroid use in the Very Early group (67.3% vs 43.2%; P = 0.018). At week 52, Very Early initiation produced a lower mean Crohn’s Disease Activity Index (64.82 ± 45.05 vs 96.10 ± 78.18; P = 0.038) and a higher steroidfree clinical remission rate (71.2% vs 45.5%; P = 0.011). Concomitant corticosteroid use fell to 9.6% in the Very Early group versus 25.0% in the Early group (P = 0.033). Very early initiation
remained the strongest independent predictor of steroidfree remission (adjusted OR 3.598, 95% CI 1.445–8.960; P = 0.006)
Conclusions: Initiating biologic therapy within six months of CD diagnosis markedly improves one year steroid free remission and reduces corticosteroid dependence compared with starting therapy at 6–24 months. These real world data support adopting a “very early” biologic treatment strategy to optimise clinical outcomes in newly diagnosed, biologic naïve CD.
P.089
Yen-Hsiang Wang1, Ming-John Bair2, Huan-Lin Chen2, Ping-Jen Hu3, 4
1Graduate Institute of Medical Sciences, College of Medicine, Taipei Medical University
2Division of Gastroenterology, Department of Internal Medicine, Taitung Mackay Memorial Hospital, Taitung, Taiwan
3Department of Internal Medicine, Division of Gastroenterology, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan
4TMU Research Center for Digestive Medicine, Taipei Medical University, Taipei, Taiwan
再評估糞便寄生蟲檢查與嗜酸性球檢測 在寄生蟲感染診斷中的臨床應用價值
王彥翔1 白明忠2 陳煥霖2 胡炳任3, 4
1 臺北醫學大學醫學系
2 台東馬偕紀念醫院消化內科
3 衛生福利部雙和醫院消化內科
4 臺北醫學大學消化醫學研究中心
Background: Parasitic infections have become uncommon in developed healthcare settings, yet they still occur sporadically. Traditional diagnostic tools such as stool ova and parasite (O&P) examination and peripheral eosinophilia remain in use but may have limited sensitivity. Their current clinical utility warrants re-evaluation.
Aims: To assess the diagnostic performance and clinical value of stool O&P testing and eosinophilia in parasitic infections and to compare them with endoscopic findings.
Methods: We conducted a retrospective review of 36 patients diagnosed with parasitic infections via endoscopy at Taitung MacKay Memorial Hospital between 2006 and 2016. Collected data included demographics, clinical symptoms, stool O&P results, eosinophil counts, and endoscopic findings. The diagnostic yields of stool O&P, eosinophilia, and endoscopy were compared.
Results: The most frequently identified parasites were tapeworms and whipworms (25% each), followed by pinworms and hookworms. Stool O&P tests were positive in only 15.8% of cases, and eosinophilia was observed in 50%. In contrast,
endoscopy provided definitive diagnosis through direct visualization of parasites and associated mucosal damage, especially in the cecum. Several patients with negative stool and eosinophil results were diagnosed solely through endoscopy
Conclusions: Stool O&P and eosinophilia demonstrated limited sensitivity in detecting parasitic infections. In clinical settings, especially when suspicion remains high, reliance solely on traditional tests may delay diagnosis. Endoscopy should be considered to confirm diagnosis when conventional tools are inconclusive.
P.090
CHALLENGES AND INEFFICIENCIES IN ACQUIRING CATASTROPHIC ILLNESS CERTIFICATE FOR INFLAMMATORY BOWEL DISEASE PATIENTS IN TAIWAN: INSIGHTS FROM A NATIONAL QUESTIONNAIRE SURVEY
Chi-Hao Chen1, Shu-Chen Wei2,3, Deng-Chyang Wu2,4, Hsu-Heng Yen2,5, Puo-Hsien Le6,7, Chen-Wang Chang2,8, Tien-Yu Huang2,9, Ching-Pin Lin2,10, Jen-Wei Chou2,11, Chen-Shuan Chung2,12, Chi-Ming Tai2,13, Ping-I Hsu14, Wei-Chen Tai2,15, Chiao-Hsiung Chuang2,16, Yen-Po Wang17,18, Wen-Jen Chiang19, Feng-Woei Tsay1,18, Tzung-Jiun Tsai1,2,18
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
2Taiwan Society of Inflammatory Bowel Disease (TSIBD), Taiwan
3Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
4Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
5Division of Gastroenterology, Changhua Christian Hospital, Changhua, Taiwan
6Division of Gastroenterology and Hepatology, Department of Internal Medicine, Chang Gung Memorial Hospital, Taoyuan, Taiwan
7Chang Gung Inflammatory Bowel Disease Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan
8Division of Gastroenterology, Department of Internal Medicine, MacKay Memorial Hospital, Taipei, Taiwan
9Division of Gastroenterology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
10Division of Hepatology and Gastroenterology, Department of Internal Medicine, Chung Shan Medical University Hospital, School of Medicine, Chung Shan Medical University, Taichung, Taiwan
11Center for Digestive Medicine, Department
of Internal Medicine, China Medical University Hospital, School of Chinese Medicine, China Medical University, Taichung, Taiwan
12Division of Gastroenterology and Hepatology, Far Eastern Memorial Hospital, New Taipei, Taiwan
13Division of Gastroenterology and Hepatology, Department of Internal Medicine, E-Da Hospital, I-Shou University, Kaohsiung, Taiwan
14Division of Gastroenterology, Department of Medicine, An Nan Hospital, China Medical University, Tainan, Taiwan
15Division of Hepatogastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
16Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan
17Division of Gastroenterology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
18School of Medicine, College of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
19Excelsior Biopharma Inc., Taipei, Taiwan
台灣發炎性腸道疾病患者取得重大傷病 證明的挑戰與低效性:基於全國問卷調 查的觀察結果
陳繼豪1 魏淑鉁2,3 吳登強2,4 顏旭亨2,5 李柏賢6,7
章振旺2,8 黃天祐2,9 林敬斌2,10 周仁偉2,11 鍾承軒2,12
戴啟明2,13 許秉毅14 戴維震2,15 莊喬雄2,16 王彥博17,18
江文仁19 蔡峯偉1,18 蔡騌圳1,2,18
1 高雄榮民總醫院胃腸肝膽科
2 台灣發炎性腸道疾病學會
3 國立臺灣大學醫學院附設醫院胃腸肝膽科
4 高雄醫學大學附設中和紀念醫院胃腸內科
5 彰化基督教醫院胃腸肝膽科
6 林口長庚紀念醫院胃腸肝膽科系
7 林口長庚紀念醫院發炎性腸道疾病中心
8 馬偕紀念醫院胃腸肝膽科
9 三軍總醫院胃腸肝膽科
10 中山醫學大學附設醫院肝膽腸胃科
11 中國醫藥大學附設醫院消化內科
12 亞東紀念醫院肝膽胃腸科
13 義大醫療財團法人義大醫院胃腸肝膽科
14 臺南市立安南醫院消化內科
15 高雄長庚紀念醫院胃腸肝膽科系
16 國立成功大學醫學院附設醫院內科部
17 臺北榮民總醫院胃腸肝膽科
18 國立陽明交通大學醫學系
19 科懋生物科技股份有限公司
Background: The incidence and prevalence of inflammatory bowel diseases (IBDs), which include ulcerative colitis (UC) and Crohn’s disease (CD), has been increasing in Taiwan. The IBDs are classified as catastrophic illness in National Health Insurance Administration (NHIA), Ministry of Health and Welfare in Taiwan. Expert panels review patients’ clinical history, laboratory and imaging results, endoscopic findings, and pathology reports before confirming and issuing a catastrophic illness certificate (CIC). Patients with CIC are exempt from medical copayments, with reduced medical fees for both inpatient and outpatient services. The IBD patients must have this certificate before applying for advanced therapies, including biologics and small molecule drugs. Without CIC, insurance won’t cover the cost, and patients will need to pay out of pocket. In clinical practice, IBD physicians in Taiwan perceive the success rate of CIC applications to be relatively low. There are no previous reports stating the actual acceptance rate and the causes of rejection of CIC. We developed a questionnaire for IBD specialists to evaluate the submission process and acceptance rate, and to understand the reasons for the low acceptance rate of CIC.
Aims: This observational study aims to assess the current status of CIC application among IBD patients and to identify potential areas for government policy improvement.
Methods: A structured online questionnaire targeting IBD specialists was conducted in Taiwan from February 27 to March 17, 2025. The questionnaire comprised 12 questions, including the basic information and experience of the IBD specialists, CIC application success rate, the process for preparing the supporting materials, and the sequence following the first rejection of CIC.
Results: Fifty-two IBD specialists completed the online questionnaire, 25% were attributed to Taipei division of NHIA (the north Taiwan), 25% to Central division (the central Taiwan), 23% to Kaoping division (the south Taiwan). Most participants were male (92.3%) and aged between 40 and 60 years (82.7%). Half IBD specialists had the IBD caring
experience less than 50 patients. Not all clinical diagnosed IBD patients had CIC. There were 74% of UC and 77% of CD patients holding a CIC in this questionnaire survey. The median time from the first clinical consultation to certificate submission was 2.7 months for UC and 3.8 months for CD. Approved rates on first application were 63% for UC and 58% for CD. We found the regional difference in application success rate between the five NHIA divisions, approximately 60% across most regions, with a slightly lower rate of around 50% in Kaoping division in southern Taiwan. Following a failed application, 92.3% of specialists proceeded with re-submission for CIC after a median interval of 5 months. The top three reasons for application rejection were insufficient diagnostic documentations, absence of typical histopathological features, and a short disease course.
Conclusions: This nationwide questionnaire survey identified a relatively low CIC holding rate among IBD patients. The approval rate for first-time applications was low and showed regional differences. While CIC provides financial benefits and definitive criteria for insurance-covered advanced therapies for IBD patients in Taiwan, there are areas in the application process and verification procedures that need improvement. Simplifying documentation requirements, enhancing communication channels, and addressing regional disparities could significantly improve access to CIC identity.
P.091
THE ROLE OF IMMUNOSUPPRESSANT AGENTS IN THE ERA OF NON-ANTI-TNF BIOLOGICS FOR INFLAMMATORY BOWEL DISEASE: A SINGLE MEDICAL CENTER EXPERIENCE
Wei-Chen Lin1, Chen-Wang Chang1, Ching-Wei Chang1, Tzu-Chi Hsu2, Horng-Yang Wang1
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Mackay Memorial Hospital, Taipei, Taiwan
2Division of Colon and Rectal Surgery, Mackay Memorial Hospital, Taipei, Taiwan
免疫調節劑在發炎性腸道疾病患於生物 製劑( Non-Anti-TNF
醫學中心經驗
林煒晟1 章振旺1 張經緯1 許自齊2 王鴻源1
1 台北馬偕紀念醫院消化科系
2 台北馬偕紀念醫院大腸直腸外科
Background: Recent studies indicate that combining non-anti-TNF therapies with immunosuppressants (IMMs) does not provide additional benefits over monotherapy in maintaining remission for patients with inflammatory bowel disease (IBD). In Taiwan, the National Health Insurance covers biologic therapies for only 54 weeks. As a result, IMMs play a crucial role in sustaining clinical remission in daily practice, even in the era of non-anti-TNF biologics.
Aims: This study aims to evaluate the real-world role of IMMs in IBD patients receiving either anti-TNF or non-anti-TNF therapies.
Methods: We conducted a single-center, retrospective study of IBD patients who received biologics between May 2013 and December 2024. The use of IMMs in patients receiving different biologic therapies was analyzed.
Results: A total of 124 IBD patients received 219 courses of biologic therapy. Of these, 114 patients (52.1%) had Crohn’s disease (CD). The age of biologic agent initiation was younger in CD patients than in ulcerative colitis (UC) patients (40.8 vs. 47.7 years; p < 0.001), while the time from disease onset to biologic agent initiation was longer in the CD group (p < 0.001). Non-anti-TNF agents were prescribed more frequently in the UC group than in the CD
group (66.7% vs. 35.9%; p < 0.001). There was no significant difference in the rate of combination therapy between CD and UC groups (38.6% vs. 41.0%; p = 0.103). In the CD group, combination therapy was more common with non-anti-TNF agents than with anti-TNF agents (43.9% vs. 26.0%; p = 0.060), however, no difference was observed in the UC group (27.1% vs. 25.7%; p = 0.563). Despite the increasing use of non-anti-TNF agents, the rate of IMMs use remained unchanged.
Conclusions: The role of IMMs for IBD in the era of non-anti-TNF biologics remains uncertain. Further research is needed to better understand the effects of IMMs in combination with biologics and their role in maintaining remission after biologic withdrawal.
P.092
OPPORTUNISTIC INFECTIONS IN PATIENTS WITH INFLAMMATORY BOWEL DISEASE RECEIVING BIOLOGIC THERAPIES: A RETROSPECTIVE COHORT STUDY
Ting-Chieh Huang1, Tony Kou1,2,3, Chia-Jung Kuo1,2,3,4, Cheng-Hsun Chiu4,5, Tai-Di Chen3,6, Chien-Ming Chen3,7, Cheng-Tang Chiu1,2,3,4, Ming-Yao Su9, Yu-Bin Pan8, Puo-Hsien Le1,2,3,4
1College of Medicine, Chang Gung University, Taoyuan, Taiwan
2Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
3Chang Gung Inflammatory Bowel Disease Center, Linkou, Taoyuan, Taiwan
4Chang Gung Microbiota Therapy Center, Linkou, Taoyuan, Taiwan
5Division of Pediatric Infectious Diseases, Department of Pediatrics, Chang Gung Memorial Hospital, Taoyuan, Taiwan
6Department of Pathology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan.
7Department of Medical Imaging and Interventions, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
8Biostatistical Section, Clinical Trial Center, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
9Division of Gastroenterology and Hepatology, Department of Internal Medicine, New Taipei Municipal Tucheng Hospital, Tucheng, New Taipei City, Taiwan
接受生物製劑治療之發炎性腸道疾病患 者的伺機性感染:回溯性世代研究
黃鼎杰1 郭偉亮1,2,3 郭家榮1,2,3,4 邱政洵4,5 陳泰迪3,6 陳建銘3,7 邱正堂1,2,3,4 蘇銘堯9 潘裕賓8 李柏賢1,2,3,4
1 長庚大學醫學系
2 林口長庚紀念醫院胃腸肝膽科系
3 林口長庚紀念醫院發炎性腸道疾病中心
4 林口長庚紀念醫院微菌治療中心
5 林口長庚紀念醫院兒童感染科
6 林口長庚紀念醫院解剖病理科
7 林口長庚紀念醫院影像診療科
8 長庚醫療財團法人臨床試驗中心林口分部
9 新北市立土城醫院胃腸肝膽科
Background: Biologic therapies have enhanced disease control in patients with inflammatory bowel disease (IBD), yet they may increase susceptibility to opportunistic infections. However, comparative data on infection risks associated with different biologic agents in Asian populations remain limited. In this study, we evaluated the incidence of Clostridioides difficile infection (CDI), Clostridium innocuum (CI) infection, and cytomegalovirus (CMV) colitis among IBD patients receiving Vedolizumab (VDZ), anti-tumor necrosis factor (anti-TNF) therapy, or Ustekinumab (UST).
Aims: To compare the incidence of opportunistic infections—including CDI, CI infection, and CMV colitis—among IBD patients treated with VDZ, antiTNF agents, or UST, and to identify clinical factors associated with increased infection risk.
Methods: This retrospective cohort study was conducted at a single center and included patients with IBD who initiated treatment withVDZ, antiTNF agents (infliximab or adalimumab), or UST at the Chang Gung IBD Center from January 2017 to December 2024. Opportunistic infections were defined as one of the following: (i) CDI confirmed by toxin-gene PCR, (ii) detection of CI in stool or colonic cultures, or (iii) CMV colitis confirmed via immunohistochemistry on intestinal biopsy. Incidence rates were calculated per 100 patientyears. Kaplan–Meier survival analysis with log-rank testing was used to assess infection-free survival, and multivariable logistic regression was applied to identify independent predictors of CDI.
Results: A total of 614 IBD patients (377 with Crohn’s disease and 237 with ulcerative colitis) were included, contributing 941 patient-years of followup. The incidence rates per 100 patient-years were 3.51 for CDI, 0.85 for CI, and 3.30 for CMV colitis. The risks of CDI and CI were similar among patients treated with VDZ, anti-TNF agents, or UST. However, CMV colitis was significantly more frequent in the anti-TNF group (5.9%) compared to those receiving VDZ (3.4%) or UST (0.5%) (p = 0.020). Multivariable analysis identified acute IBD flare (odds ratio [OR] 3.64; 95% confidence interval: 1.91–6.91), concurrent CMV colitis (OR 6.34; 95% confidence interval: 2.03–19.8), and CI infection (OR 7.79; 95% confidence interval: 1.40–43.3) as independent predictors of CDI.
Conclusions: Treatment with VDZ or UST was
not linked to an increased risk of CDI, CI, or CMV colitis. In contrast, anti-TNF therapy was associated with a greater incidence of CMV colitis. These findings underscore the need for vigilant infection monitoring, particularly during acute disease flares or in patients with refractory IBD.
Weng-Fai Wong1, Yu-Ting Kuo1, Ming-Lun Han1, Chieh-Chang Chen2, Hsiu-Po Wang2
1Department of Integrated Diagnostics & Therapeutics, National Taiwan University Hospital, National Taiwan University, Taipei, Taiwan
2Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
未切除之胰頭癌併阻塞性黃疸患者接受 胰管支架置放對存活影響之回溯性世代 研究
黃永輝1 郭雨庭1 韓明倫1 陳介章2 王秀伯2
1 台大醫院綜合診療部
2 台大醫院內科部
Background: Malnutrition is common in patients with pancreatic head cancer, which can diminish their tolerability of anti-cancer treatments. Pancreatic duct blockage is one of the contributing factors leading to malnutrition.
Aims: This study aimed to clarify whether pancreatic duct stenting offers a survival benefit in patients with unresected pancreatic head cancer.
Methods: This retrospective cohort study identified patients of newly diagnosed pancreatic cancers who received endoscopic retrograde cholangiopancreatography (ERCP) because of biliary tract obstruction from a hospital-based cancer registry between 2007 and 2021. Patients who underwent tumor resection or bypass surgery following ERCP were excluded. The primary outcome was the one-year survival rate in patients with and without a pancreatic stent. Secondary outcomes included overall survival, cancer-specific survival, and changes in weight and nutritional markers following ERCP.
Results: Among 562 patients, 39 (6.9%) received pancreatic stent placement. Most of the patients (90%) did not receive tumor resection because of advanced stage disease. The stent group had a lower one-year survival rate than the non-stent group (18% vs 30%; P = 0.047). The median survival time
appeared to be shorter in the stent group (170 days vs 217 days; P = 0.077). The adjusted Hazard Ratio of pancreatic stent placement was 1.42 (95% CI, 0.752.67; P = 0.282). Additionally, changes in weight and nutritional markers after ERCP did not differ significantly between the groups.
Conclusions: Pancreatic stent placement in unresected pancreatic head cancer with obstructive jaundice does not improve survival or nutritional status.
P.094
Chi-Ying Yang, Wen-Hsin Huang, Hsing-Hung Cheng, I-Liang Chen, Yu-Chen Chang
Center for Digestive Medicine, Department of Internal Medicine, China Medical University Hospital, China Medical University, Taichung, Taiwan
超音波引導下胃囊腫造口術治療胰液積 聚:一個醫學中心的經驗
楊其穎 黃文信 鄭幸弘 陳宜良 張育誠 中國醫藥大學附設醫院消化醫學中心
Background: Pancreatic fluid collection (PFC) is common complications of acute and chronic pancreatitis and categorized into pseudocyst and wall-off necrosis (WON). Symptoms of PFC include nausea, fever, abdominal pain, and in some cases even gastric outlet obstruction and complications such as fistulas and pseudoaneurysms. The endoscopic ultrasound (EUS)-guided gastrocystostomy is minimal invasive procedure for drainage of PFCs. Two type stents are used for endoscopic ultrasound guided gastrocystostomy: double-pigtail plastic stent (DPPS) and lumen-apposing metal stents (LAMS). Some studies reported statistically significantly higher clinical success rates with LAMS, while others showed no significant difference.
Aims: The aim of this study is to evaluate the clinical outcome and safety of EUS-guided gastrocystostomy in different stent types.
Methods: A retrospective study was conducted at China Medical University Hospital from June 2019 to May 2025. A total of 24 patients with symptomatic pancreatic fluid collections underwent EUS-guided gastrocystostomy or duodenostomy. All procedures were performed under real-time EUS guidance. Drainage was performed using either DPPS or LAMS (HotAXIOS, Boston Scientific), depending on the clinical situation. Laboratory data, clinical outcomes, and procedure-related complications were reviewed and analyzed.
Results: A total of 24 patients underwent EUSguided gastrocystostomy, with a median age of 56.5 years; 71% were male. The most common indication
was pancreatic pseudocyst related to alcoholinduced pancreatitis (54%), followed by idiopathic causes (29%) and pancreatic cancer (8.3%). Of the 24 procedures, 7 used a LAMS (HotAXIOS) and 17 used a plastic stent. The transgastric route was employed in 79% of cases, while the transduodenal approach was used in 21%. All HotAXIOS stents were 15 mm in diameter, and plastic stents were all 7-French. The technical and clinical success rates were both 100% in the LAMS group and in the DPPS group, the technical success rate was 100% and the clinical success rate was 71%. No complications occurred in the LAMS group, while a 18% (3/17) complication rate was found in the DPPS group. Early complications (within 30 days) occurred in 2 cases (infection and perforation), and one late complication (infection) was noted. Stent dysfunction, defined as the need for reintervention due to stent occlusion or clinical failure, occurred only in the plastic stent group (3/17, 18%). Two cases underwent stent replacement with LAMS, and one case underwent stent replacement with a plastic stent.
Conclusions: EUS-guided gastrocystostomy is an effective and safe intervention for the treatment of PFC. In this study, the complication rate of LAMS was low and no stent dysfunction occurred, indicating that it has potential advantages over traditional plastic stents.
P.095
Ryosuke Tenma, Yukitoshi Matsunami, Atsushi Sofuni, Takayoshi Tsuchiya, Reina Tanaka, Ryosuke Tonozuka, Shuntaro Mukai, Kazumasa Nagai, Hiroyuki Kojima, Hirohito Minami, Noriyuki Hirakawa, Kyoko Asano, Kazuki Hama, Takao Itoi
Department of Gastroenterology and Hepatology, Tokyo Medical University, Tokyo, Japan
Background: Endoscopic retrograde cholangiopancreatography (ERCP) with transminor papillary stenting for symptomatic pancreas divisum is considered a useful treatment. Recently, EUS-guided pancreatic duct drainage rendezvous technique (EUS-PD RV) has been also applied as an alternative access route for difficult cannulation cases. Aims: This study aimed to clarify the long-term outcomes of trans-minor papillary stenting for symptomatic pancreas divisum.
Methods: 27 symptomatic pancreas divisum patients (19 complete, 8 incomplete) who underwent endoscopic treatment at our institution from Jan. 2014 to Apr. 2024, in whom follow-up was possible for at least 12 months, were retrospectively analyzed. Technical success was defined as successful transminor papillary stenting. Clinical success was defined as no recurrence of acute pancreatitis for a period of 12 months after the initial ERCP, whether the stent was removed or regularly exchanged.
Results: The mean follow-up period was 58.4 months (range 12 – 125). Trans-minor papillary cannulation was successful in 13 of 23 (56.5%), trans-major papillary cannulation with RV was performed in 4, EUS-PD RV was performed in 7. In total, trans-minor papillary stenting was successful in 24 of 27 cases (88.9%). The clinical success was achieved in 87.5% (21/24). Adverse events rate of initial ERCP was 25.9% (7/27), including 6 mild pancreatitis and 1 peritonitis, treated by conservative therapy. 2 cases of clinical failure underwent pancreaticoduodenectomy. Among the 21 cases of clinical success, 4 cases (19%) had a relapse of pancreatitis in the long-term followup, and required re-intervention.
Conclusions: Trans-minor papillary stenting is a safe and effective treatment for symptomatic pancreas divisum. Further data accumulation by multi-center study are warranted.
P.096
Ming-Sheng Chien1, Ching-Chung Lin1,2, Jian-Han Lai1,2
1Division of Gastroenterology, Department of Internal Medicine, Mackay Memorial Hospital, Taipei, Taiwan
2MacKay Junior College of Medicine, Nursing and Management, Taipei, Taiwan
藉由內視鏡超音波辨識胰臟腫瘤與評估 切片的必要性
簡銘陞1 林慶忠1,2 賴建翰1,2
1 台北馬偕紀念醫院消化系
2 馬偕醫護管理專科學校
Background: The incidence of pancreatic cancer is increasing, yet the 5-year survival rate remains low at only 12–13%. One major challenge is the difficulty of early diagnosis, which limits curative surgical options and often leaves patients with only palliative chemotherapy. Traditional imaging modalities such as CT and transabdominal ultrasonography have limited sensitivity, especially for small or anatomically hidden tumors. Endoscopic ultrasound (EUS), with its superior resolution and ability to perform tissue sampling, has emerged as a valuable tool for evaluating pancreatic tumors.
Aims: This mini-review aims to summarize key imaging features of pancreatic tumors using EUS, CE-EUS, and elastography, and to clarify when EUSguided FNA/FNB is warranted to improve diagnostic accuracy and guide clinical decision-making.
Methods: This review synthesizes current literature and clinical studies on EUS and its advanced applications—CE-EUS and elastography—in the diagnosis of solid and cystic pancreatic lesions. It evaluates the diagnostic utility, imaging characteristics, and clinical relevance of each modality, with a particular focus on when tissue sampling is warranted.
Results: The review highlights that EUS, especially when combined with CE-EUS and elastography, effectively distinguishes between benign and malignant pancreatic lesions based on features such as echogenicity, vascularity, and tissue stiffness. CE-EUS improves detection of small tumors and differentiates vascular patterns, while elastography
enhances diagnostic confidence by assessing lesion hardness. EUS-guided FNA/FNB provides high diagnostic yield, particularly for unresectable tumors, lesions with worrisome features, or when neoadjuvant therapy is planned, making it a critical tool for accurate diagnosis and treatment planning.
Conclusions: EUS, particularly when combined with advanced modalities like CE-EUS and elastography, offers excellent sensitivity and diagnostic accuracy for pancreatic tumors, especially small or difficult-tocharacterize lesions. EUS-guided FNA/FNB enhances diagnostic precision and supports clinical decisionmaking. Future developments, including molecular markers and improved lesion characterization, may further enhance diagnostic performance and reduce the need for invasive procedures.
P.097
NON-INFERIOR DIAGNOSTIC ACCURACY OF WIRE-GUIDED VERSUS WIRELESS-GUIDED TRANSPAPILLARY INTRADUCTAL BIOPSY FOR INDETERMINATE BILIARY STRICTURES
Hau-Jyun Su1, Yu-Ting Kuo2, Hsiu-Po Wang2, Ming-Chang Tsai1
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan
2Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
針對膽道狹窄執行膽道內切片 使用導 引絲引導深入的方式不會比傳統徒手深 入差
蘇浩俊1 郭雨庭2 王秀伯2 蔡明璋1
1 中山醫學大學附設醫院肝膽腸胃科
2 台大醫院內科部
Background: Transpapillary intraductal biopsy is commonly performed during endoscopic retrograde cholangiopancreatography to evaluate indeterminate biliary strictures. However, its sensitivity for detecting malignancy remains suboptimal, and performing the procedure using the freehand technique can be technically challenging. A preliminary study with a limited case number demonstrated that transpapillary biopsy could be facilitated by advancing the forceps along a guidewire.
Aims: This study aimed to compare the diagnostic performance of wire-guided versus wireless-guided transpapillary intraductal biopsy in patients with indeterminate biliary strictures.
Methods: From January 2016 to December 2024, 118 patients were retrospectively enrolled following 1:1 propensity score matching. Based on the transpapillary intraductal biopsy method used, patients were categorized into either the wireguided or wireless-guided group, with 59 patients in each. Cytologic and histopathologic findings from the intraductal specimens were compared with the patients’ final diagnoses to assess the diagnostic accuracy for malignant biliary strictures. Logistic regression analysis was performed to identify factors associated with malignancy and to
determine predictors of accurate diagnosis based on intraductal tissue acquisition.
Results: The diagnostic accuracy was comparable between the two groups (wire-guided: 59.32%, wireless-guided: 69.49%; p = 0.085), although the sensitivity was significantly lower in the wire-guided group (wire-guided: 45.45%, wireless-guide: 63.27%; p = 0.013). Elevated serum carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA 19-9) levels were independently associated with malignant biliary stricture (CEA odds ratio: 1.46, p = 0.008; CA 19-9 odds ratio: 1.003, p = 0.001). No factor could predict the accurate diagnosis based on intraductal tissue acquisition.
Conclusions: Transpapillary intraductal biopsy can be performed using either the wire-guided or wireless-guided method for the evaluation of indeterminate biliary strictures. In patients at high risk for malignancy, additional diagnostic modalities should be considered if the etiology remains inconclusive following intraductal tissue acquisition.
P.098
CLINICAL EFFICACY AND SAFETY OF CEFOPERAZONE-SULBACTAM VERSUS OTHER ANTIBIOTICS IN THE TREATMENT OF PATIENTS WITH ACUTE CHOLANGITIS – A MULTICENTER RETROSPECTIVE STUDY
Chieh-Chang Chen1,2, Jiann-hwa Chen3,4, Wen-Hsin Huang5, Tsung-Lin Hsieh5, Li-Wei Chen6, Ming-Chang Tsai7,8, Nai-Jen Liu9, Chi-Huan Wu9, Chen-Shuan Chung10,11, Yi-Chun Chiu12, Chih-Ming Liang12, Cheng-Kun Wu12, Wen-Lun Wang13,14, Ching-Tai Lee13, Ming-Hung Hsu13, Hsiu-Po Wang1.2
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
2Department of Internal Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan
3Division of gastroenterology and hepatology, Taipei Tzu Chi hospital, New Taipei City, Taiwan
4School of medicine, Tzu Chi University, Hualien, Taiwan
5Center for Digestive Medicine, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan
6Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital and Chang Gung University at Keelung, Keelung, Taiwan
7Division of Gastroenterology and Hepatology, Department of Internal Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan
8School of Medicine, Chung Shan Medical University, Taichung, Taiwan
9Department of Gastroenterology and Hepatology, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
10Division of Gastroenterology and Hepatology, Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan
11Department of Electrical Engineering, Yuan Ze University, Taoyuan, Taiwan
12Division of Hepato-Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine,
Kaohsiung, Taiwan
13Division of Gastroenterology and Hepatology, Department of Internal Medicine, E-Da Hospital, I-Shou University, Kaohsiung, Taiwan
14School of Medicine, College of Medicine, I-Shou University, Kaohsiung, Taiwan
Cefoperazone-Sulbactam 與其他抗生素 治療急性膽管炎臨床效益及安全性之比 較 一個多中心回溯性研究
陳介章1,2 陳建華3,4 黃文信5 謝宗霖5 陳立偉6 蔡明璋7,8 劉乃仁9 吳季桓9 鍾承軒10,11 邱逸群12 梁志明12 吳鎮琨12 王文��13,14 李青泰13 徐銘宏13 王秀伯1.2
1 台大醫院消化內科
2 台大醫學院內科
3 台北慈濟醫院胃腸肝膽科
4 慈濟大學醫學系
5 中國醫藥大學附設醫院消化醫學中心
6 基隆長庚紀念醫院胃腸肝膽科
7 中山醫學大學附設醫院肝膽腸胃科
8 中山醫學大學醫學系
9 林口長庚紀念醫院胃腸肝膽科
10 亞東紀念醫院肝膽腸胃科
11 元智大學電機工程學系
12 高雄長庚紀念醫院胃腸肝膽科系
13 義大醫院胃腸肝膽科
14 義守大學醫學系
Background: Acute cholangitis is a severe infection of the biliary tract requiring prompt antibiotic therapy and biliary drainage. Cefoperazone-sulbactam is a widely used broad-spectrum antibiotic, but comparative real-world data on its efficacy and safety against other agents in this setting is lacking and would be valuable for guiding clinical practice. This study aimed to evaluate the clinical efficacy and safety of cefoperazone-sulbactam (C/S) compared to other commonly used antibiotics, primarily flomoxef and ceftriaxone, for the empirical treatment of acute cholangitis.
Aims: This study aimed to evaluate the clinical efficacy and safety of cefoperazone-sulbactam (C/S) compared to other commonly used antibiotics, primarily flomoxef and ceftriaxone, for the empirical treatment of acute cholangitis.
Methods: This was a retrospective, multi-center study conducted across nine hospitals in Taiwan. Data from 389 adult patients hospitalized between January 2022 and July 2024 with a diagnosis of acute
cholangitis, based on the Tokyo Guidelines (TG18), were analyzed. Patients received treatment with C/S (n = 249), Ceftriaxone (n = 37), or Flomoxef (n = 103) for at least three days. The primary endpoint was the clinical outcome (cure or improvement) assessed on Days 4, 7, and 14. Microbiological outcomes and safety profiles were also evaluated.
Results: Baseline characteristics, including disease severity (mostly Grade I/II), comorbidities, and Charlson scores, were comparable among the treatment groups. The most common diagnosis was CBD stone (65%–77%). At Day 4, the C/S group demonstrated a significantly higher clinical response rate (96.8%) compared to the Flomoxef group (93.2%; p = 0.037). No significant differences in clinical or microbiological outcomes were observed at Day 7 or Day 14. All groups showed significant improvements in inflammatory markers (WBC, CRP) and liver function tests. The incidence of adverse events was low (≤5%) across all groups. Vitamin K was administered more frequently in the C/S group (p < 0.001), though no significant differences in PT/ APTT prolongation were noted.
Conclusions: Cefoperazone-sulbactam demonstrated a superior early clinical response rate at Day 4 compared to flomoxef in the treatment of acute cholangitis. With a comparable safety profile, these findings support its use as an effective and safe empirical antibiotic for this condition.
P.099
Chia-Jui Li, Cheuk-Kay Sun
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan
回溯分析總膽管結石復發之風險因子 李家睿 孫灼基 新光吳火獅紀念醫院胃腸肝膽科
Background: Recurrent common bile duct (CBD) stones pose a significant clinical challenge postendoscopic removal. Despite advances in endoscopic techniques, recurrence of CBD stones remains a notable clinical problem, with reported recurrence rates ranging from 4% to over 20%. Identifying risk factors for recurrence can aid in patient management and follow-up planning.
Aims: The primary aim of this study was to investigate the association between various clinical, anatomical, and procedural categorical variables and the recurrence of CBD stones following endoscopic treatment. The goal is to enhance risk stratification, guide clinical follow-up strategies, and ultimately improve the long-term management of patients with choledocholithiasis.
Methods: We retrospectively analyzed categorical variables in patients who had undergone endoscopic treatment for CBD stones in a single center. A recurrence of CBD stone within 6 months and followup period less than one year were excluded. Using chisquare tests, we assessed the relationship between each variable and CBD stone recurrence.
Results: Among the analyzed factors, age ≥65 years (p = 0.0193), male gender (p = 0.0285), and presence of gallbladder (GB) stones (p < 0.05) were significantly associated with recurrence of CBD stones. Other variables, including comorbidities (diabetes, hypertension, dyslipidemia, fatty liver, liver cirrhosis, etc), stone characteristics (diameter, number, position, etc), and endoscopic interventions (endoscopic sphincterotomy, endoscopic papillary balloon dilation, etc), showed no significant association with recurrence.
Conclusions: Older age, male sex, and concurrent GB stones are important risk factors for recurrent CBD stones. These findings suggest targeted monitoring and management may be necessary for these populations.
P.100
CHARACTERISTICS OF BILE CULTURES IN BILIARY OBSTRUCTION PATIENTS WITH POSITIVE BLOOD CULTURES UNDERGOING ERCP
Chun Yang1, Yen-Chun Peng1,2
1Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
2Division of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
接受 ERCP 治療之膽道阻塞患者中,血液 培養陽性時的膽汁培養特徵
楊鈞1 彭彥鈞1,2
1 臺中榮民總醫院內科部
2 臺中榮民總醫院胃腸肝膽科
Background: The Relationship of Positive Bacteremia and Characteristics of Bile Culture in Patients with Acute Biliary Obstruction
Aims: Biliary obstruction, followed by bacteremia is a critical concern, often requiring not only antibiotics therapy, but also advanced treatment, such as endoscopic retrograde cholangiopancreatography (ERCP). This study investigates the relationship between positive blood cultures and bile culture characteristics in patients undergoing endoscopic retrograde cholangiopancreatography (ERCP) for biliary obstruction with etiology as malignant or benign cause.
Methods: We retrospectively analyzed 182 patients who underwent their first ERCP for acute biliary obstruction between January and June 2024. Bile samples collected during ERCP were cultured, and blood culture results within 48 hours of the procedure were reviewed. Patients were categorized into malignant (MBO) and benign biliary obstruction (BBO) groups.
Results: Positive bile cultures were observed in 66% of cases, with BBO patients showing a higher rate (69%) than MBO patients (57%). Polymicrobial infections were more common in BBO, while Gramnegative monomicrobial infections predominated in MBO. Among patients with positive blood cultures, more Gram-negative infections in bile culture pathogens was noted.
Conclusions: There is an association between
positive bacteremia and specific bile culture profiles, especially in malignant obstruction. Identifying microbial patterns through bile cultures can aid in early recognition of systemic infection risk and guide empirical antibiotic choices during ERCP management.
Yuta Kanazawa, Kazumasa Nagai, Noriyuki Hirakawa, Kazuki Hama, Kyoko Asano, Hirohito Minami, Hiroyuki Kojima, Yukitoshi Matsunami, Shuntaro Mukai, Ryosuke Tonozuka, Reina Tanaka, Takayoshi Tsuchiya, Takao Itoi
Department of Gastroenterology and Hepatology, Tokyo Medical University, Tokyo, Japan
Background: Peroral cholangioscopy (POCS) enables direct visualization and targeted endoscopic treatment within the biliary tract. However, in cases of severe ductal stricture, insertion and maneuverability of conventional choledochoscopes can be technically challenging, limiting their effectiveness. in anatomically complex settings.
Aims: Recent advances in scope design have led to the development of ultra-slim cholangioscopes that may address these limitations.
Methods: We report the first clinical application of the Breview Choledochoscope—the world’s thinnest choledochoscope currently available (7.8 Fr; Shanghai SeeGen Photoelectric Technology Co., Ltd.)—for the endoscopic management of a giant common bile duct (CBD) stone.
Results: A 73-year-old man was referred to our institution following a failed ERCP at an outside hospital, where stone extraction was unsuccessful due to its large size and impaction. At our center, ERCP was reattempted using the Breview Choledochoscope. Despite marked narrowing of the bile duct lumen, the scope was advanced into the CBD without resistance. Under direct cholangioscopic visualization, yttrium aluminum garnet (YAG) laser lithotripsy was successfully performed, followed by extraction of the fragmented stones using basket forceps. Final cholangioscopic assessment confirmed complete ductal clearance. While conventional scopes may be hindered by anatomical constraints, the ultra-slim profile of the Breview Choledochoscope allowed for precise navigation, stable access, and effective therapeutic intervention. Saline irrigation and delivery of the laser fiber were performed without any technical difficulties.
Conclusions: To the best of our knowledge, this is the first reported case demonstrating the clinical utility of the Breview Choledochoscope. Its remarkable slimness and maneuverability suggest that it may serve as a promising therapeutic option for various biliary strictures, especially in cases where conventional POCS systems are not applicable.
P.102
DISCONTINUOUS PURIFICATION IN ISLET ISOLATION – A NARRATIVE LITERATURE REVIEW AND LABORATORY EXPERIENCE IN RATS
Ping-Teng Chu1,3, Shu-Hung Huang2,3
1Department of Surgery, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
2Department of Surgery, Kaohsiung Medical University Chung-Ho Memorial Hospital, Kaohsiung, Taiwan
3Graduate Institute of Clinical Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
不連續純化的胰島分離 敘述性文獻回 顧與大鼠實驗室經驗
朱炳騰1,3 黃書鴻2,3
1 高雄榮民總醫院外科部
2 高雄醫學大學附設中和紀念醫院外科部
3 高雄醫學大學臨床醫學研究所
Background: Type 1 diabetes mellitus remains a significant health burden globally, with Taiwan reporting a prevalence of 50 cases per 100,000 individuals and an annual incidence of 2.23 new cases per 100,000 people by 2016. While current management strategies have evolved to include whole pancreas and pancreatic islet cell transplantation, islet transplantation has emerged as a less invasive alternative with considerable therapeutic potential. The development of islet isolation techniques has undergone several critical milestones since Paul Langerhans first described pancreatic islets in 1869. Early pioneering work by Hultquist and Thorell in 1963, followed by Lacy’s proposal of islet transplantation as an alternative to whole pancreas transplantation in 1969, established the conceptual foundation for this therapeutic approach. The field achieved significant technical advancement with Ballinger’s successful reversal of hyperglycemia in diabetic mice through islet transplantation in 1972, and the first human islet transplantation performed by Sutherland’s team in 1974. A major breakthrough occurred in 1988 when Ricordi and colleagues developed a semi-automated method for islet isolation, resolving critical technical challenges in islet cell separation and purification. This advancement, combined with Lake et al.’s introduction of the COBE2991 cell separator in
1989, revolutionized islet purification techniques by enabling large-volume continuous density gradient centrifugation. The COBE2991 system replaced traditional single-use Ficoll or Dextran density gradient centrifugation methods, significantly improving efficiency and standardization. The clinical significance of these technological advances was demonstrated in 2000 when Shapiro and colleagues established the Edmonton Protocol, which standardized donor selection, minimum transplantation volume, and postoperative immunosuppression regimens. This protocol marked a pivotal milestone in islet transplantation history, significantly improving graft survival and function, with seven consecutive patients achieving insulin independence for over one year. However, the discontinuation of the COBE2991 cell processor has created a critical gap in islet purification technology. This has necessitated the urgent development of alternative discontinuous purification methods for islet isolation, particularly important for advancing diabetes treatment capabilities in regions like Taiwan where access to advanced islet processing equipment may be limited. Traditional discontinuous density gradient methods, while simpler and more cost-effective than automated systems, offer several advantages including lower equipment costs, reduced technical complexity, and greater accessibility for research institutions with limited resources. Historical methods using Ficoll-400, Histopaque, and other density gradient materials have demonstrated effective islet separation, though with varying degrees of purity and yield compared to automated systems.
Aims: The primary aim of this narrative literature review is to comprehensively analyze the historical development, technical principles, and clinical applications of discontinuous purification methods for pancreatic islet isolation. Specifically, this study seeks to: Systematically review the evolution of discontinuous islet purification techniques from early manual methods to contemporary approaches, highlighting key technological milestones and their impact on islet isolation efficiency and clinical outcomes. Compare and contrast discontinuous purification methods with automated systems (particularly the COBE2991 cell separator), evaluating their respective advantages, limitations, and suitability for different research and clinical settings. Document and analyze laboratory experience with discontinuous purification techniques in rat islet
isolation, providing practical insights into protocol optimization, yield improvement, and quality assessment methods. Assess the current relevance and future potential of discontinuous methods in the context of modern islet transplantation requirements, particularly addressing the gap created by the discontinuation of automated purification systems. Provide evidence-based recommendations for implementing discontinuous purification protocols in resource-limited settings, with specific focus on their applicability to diabetes research and potential clinical applications in Taiwan and similar healthcare environments. Identify opportunities for technical improvements and standardization of discontinuous methods to enhance their competitiveness with automated systems while maintaining cost-effectiveness and accessibility. Through this comprehensive analysis, we aim to contribute to the advancement of islet isolation techniques and support the continued development of islet transplantation as a viable therapeutic option for Type 1 diabetes, particularly in settings where access to advanced automated purification systems may be limited or unavailable. Methods: A comprehensive literature search was conducted across multiple databases including MEDLINE (PubMed), Web of Science, and Google Scholar, encompassing Medline In-Process and other non-indexed references through March 31, 2024. The search strategy employed controlled medical terminology specifically targeting studies on “islet isolation” or “islet purification,” with language restriction to English publications excluding in-book articles. Articles were systematically filtered using predefined inclusion and exclusion criteria. Inclusion criteria required: (1) original, peer-reviewed articles published in English without publication date restrictions; (2) article titles containing both “islet isolation” or “islet purification” and the target experimental species; and (3) focus on experimental islet isolation procedures. Exclusion criteria eliminated: (1) practical guidelines, unpublished research, editorials, letters, and dissertations; (2) species-inappropriate studies (e.g., canine models); (3) articles not focusing purely on islet isolation experimental steps; (4) poster abstracts only; and (5) studies with unavailable full text or abstracts. This selection process specifically emphasized studies utilizing discontinuous purification methods, particularly those employing traditional density gradient techniques such as Ficoll-400,
Histopaque, and other manual purification approaches that preceded the automated COBE2991 cell separator era. The narrative review approach allowed comprehensive analysis of historical and contemporary discontinuous purification methodologies. Male Sprague-Dawley (SD) rats weighing 200-500 grams were selected as the experimental model based on their genetic uniformity and minimal inter-individual variability, ensuring experimental accuracy and reliability. Female rats were excluded to eliminate potential confounding variables associated with reproductive hormone cycles. All procedures were performed under isoflurane anesthesia to ensure animal welfare and procedural consistency. Dithizone (DTZ) staining was employed as the primary method for islet identification and purity assessment. DTZ functions as a zinc-chelating agent that specifically targets pancreatic beta cells, producing characteristic red staining due to zinc granule presence within beta cells. This staining technique enables clear morphological distinction between islet and nonislet tissue, facilitating accurate quantification and quality assessment of isolated islets. The experimental protocol followed a systematic three-phase approach consistent with established discontinuous purification methodologies: Phase 1: Pancreatic Distention and Dissection Following anesthetic induction, the pancreatic ductal system was accessed and distended using collagenase solution injection, following principles established by Lacy and Kostianovsky (1967). This step ensures optimal enzyme distribution throughout the pancreatic parenchyma while preserving islet architecture. Phase 2: Enzymatic Digestion Controlled enzymatic digestion was performed using collagenase preparations, following protocols adapted from early pioneering work by Scharp et al. (1973). The digestion process was carefully monitored to achieve optimal tissue disaggregation while minimizing islet damage, avoiding the mechanical stress associated with automated systems. Phase 3: Discontinuous Density Gradient Purification Islet purification was accomplished using discontinuous density gradient centrifugation methods, building upon the foundational work of Ficoll-400 gradient techniques established in the pre-COBE2991 era. This approach employed multiple density layers to achieve separation of islets from exocrine tissue, ductal fragments, and other pancreatic components. The purification process utilized: Density gradient
preparation: Multiple Ficoll or Histopaque solutions of varying densities (typically ranging from 1.070 to 1.119 g/mL) Stepwise centrifugation: Low-speed centrifugation protocols to minimize mechanical stress on islets Interface collection: Careful harvesting of islet-enriched fractions from gradient interfaces Washing and resuspension: Multiple washing steps in physiological solutions to remove gradient medium
Results: Presenting various cellular conditions of pancreatic islets stained with DTZ under different magnifications observed in the suspension under the microscope.
Conclusions: This narrative literature review has comprehensively traced the historical evolution of discontinuous purification methods for pancreatic islet isolation, revealing a rich foundation of technical innovation that preceded and continues to complement automated purification systems. The analysis of pre-COBE2991 era literature demonstrates that discontinuous density gradient techniques have been fundamental to the development of modern islet transplantation. Our review confirms that pioneering work from 1911 to the 1980s established the conceptual and technical groundwork for contemporary islet isolation. Bensley’s initial manual dissection techniques (1911), followed by Lacy and Kostianovsky’s introduction of collagenase digestion (1967), and Scharp et al.’s development of Ficoll-400 density gradient purification (1973), collectively created a robust methodological framework that remains scientifically valid and practically applicable today. The literature analysis reveals that while automated systems like the COBE2991 offered advantages in terms of processing volume and standardization, discontinuous methods provide several distinct benefits: (1) significantly lower equipment and operational costs; (2) reduced technical complexity and maintenance requirements; (3) greater accessibility for research institutions with limited resources; and (4) comparable islet viability and functional capacity when properly optimized. Studies comparing various density gradient materials (Ficoll-400, Histopaque, metrizamide, and dextran-40) demonstrate that discontinuous methods can achieve islet purities and yields within acceptable ranges for both research and potential clinical applications. The discontinuation of the COBE2991 cell processor has highlighted the strategic importance of maintaining expertise in discontinuous purification techniques.
Our literature review demonstrates that these methods have shown remarkable adaptability and continuous improvement over decades, with innovations in gradient composition, centrifugation protocols, and quality assessment techniques ensuring their continued relevance in contemporary islet research. Feasibility Demonstration: Our laboratory investigations using Sprague-Dawley rats have preliminarily demonstrated that islet isolation under discontinuous purification conditions is indeed feasible and can produce functionally viable islets suitable for experimental applications. The three-phase protocol encompassing pancreatic distention, enzymatic digestion, and discontinuous density gradient purification successfully yielded morphologically intact islets with preserved beta-cell architecture as confirmed by dithizone staining. Technical Optimization Requirements: While feasibility has been established, our experimental experience confirms that optimizing existing procedural steps to obtain higher yields of viable cells remains a critical objective requiring continued research effort. Specific areas identified for improvement include: (1) refinement of collagenase digestion parameters to minimize islet fragmentation; (2) optimization of density gradient compositions and centrifugation conditions; (3) enhancement of islet recovery techniques from gradient interfaces; and (4) development of improved quality assessment methodologies. Clinical and Research Applications: The combined evidence from literature review and laboratory experience supports the conclusion that discontinuous purification methods represent a viable and valuable alternative to automated systems, particularly in resourcelimited settings or when specialized equipment is unavailable. These techniques maintain the potential to support both fundamental diabetes research and, with appropriate optimization and validation, clinical islet transplantation programs. Technological Evolution: Our findings suggest that rather than viewing discontinuous methods as obsolete technology, the field should recognize them as complementary approaches that offer unique advantages in specific contexts. The historical resilience and continuous improvement of these techniques, combined with modern understanding of islet biology and purification science, creates opportunities for innovative hybrid approaches that combine the accessibility of discontinuous methods with contemporary quality
standards. Strategic Research Priorities: Based on our comprehensive analysis, we identify several priority areas for future research: (1) systematic optimization of discontinuous purification protocols using modern analytical techniques; (2) development of standardized quality assessment criteria specific to discontinuous methods; (3) investigation of novel density gradient materials and compositions; (4) establishment of cost-effectiveness analyses comparing discontinuous and automated approaches; and (5) validation studies assessing the suitability of discontinuous purification-derived islets for clinical applications. In conclusion, this study provides compelling evidence that discontinuous purification methods for pancreatic islet isolation represent both a historically important foundation and a practically relevant contemporary approach. While our laboratory experience preliminarily demonstrates the feasibility of these techniques, the optimization of existing steps to obtain more viable cells remains an achievable goal that warrants continued research investment. The convergence of historical validation, practical accessibility, and ongoing optimization potential positions discontinuous purification methods as essential components of the islet isolation toolkit, particularly valuable in addressing the technical and economic challenges facing diabetes research and treatment in diverse global healthcare environments. The legacy of pre-automated era innovations continues to offer practical solutions for contemporary challenges, ensuring the continued advancement of islet transplantation as a therapeutic modality for Type 1 diabetes mellitus.


