James Rogers, MDSanjay Havaldar, MD Vu Le, MD Jim Blaine, MD John Steinberg, MD Taylor Brooks, MD Rachelene Middleton, MD Barbara Hover Jaya Lafontaine, MD






Editor's
President's Page
Remembering the Duff Brothers
Michael Clarke, MD..............................................................6
What is the definition for the practice of medicine
Brian Biggers, MD...................................................................8
GCMS Rocky Mountain Medicine 2026
Jim Blaine, MD ...........9
Estate Planning Essentials for Physicians
Carley Lynn...........................................................................10
Aesthetics: How to Choose a Safer Provider in a Very Crowded, Poorly Regulated Space
Murphy Mastin, MD......................................................
GCMSA Alliance
Covid-19 Vaccine Efficacy: Where Are We Now?
Minh-Thu Le, MD.................................................................14
IRS Updates in 2026 that Could Reshape Your Retirement Strategy
Cody Bean.............. ...........................................................19
Finding the Lost Chord: Rediscovering Music in Medicine
Bethany Thompson-Gordon..............................................20
Editor’s Note: All materials for the Journal must be submitted by the first of the month prior to publication.
Co-Editors:
Jim Blaine, MD
Minh-Thu Le, MD
Junior Co-Editor: Andrew K. Le
Managing Editor: Dalton Boyer
Editorial Committee:
Michael S. Clarke, MD
David Barbe, MD
Jaya LaFontaine, MD
Dalton Boyer
Andrew Le
Jean Harmison
Barbara Hover
Melissa Ganies, MD, FACP, FAAHPM President
Vu Le, MD
Secretary
Jim Blaine, MD
Treasurer
James Rogers, MD Immediate Past President
Council Members:
Barbara Hover
James Rogers, MD
Melissa Gaines, MD
Rachelene Middleton, MD
Jim Blaine, MD
Sanjay Havaldar, MD
Jaya LaFontaine, MD
John Steinberg, MD
Taylor Brooks, MD Vu Le, MD
Managing Director: Jean Harmison



Executive Office: 4730 S. National Ave. Suite A1 Springfield, MO 65810 email: director@gcms.us www.gcms.us
All
by Minh-Thu Le, MD
“We are troubled on every side…”
Amazingly, we made it to another year. Not to be the bearer of bad news, but these last few months have been di icult for our medical community. That’s just the elephant in the room. As we are in the throes of winter, we wonder how we are to navigate the changes in public medicine as we know it. We also wonder if what we are doing with our patients is enough. We wonder if we are still the trusted voices in our clinics, our hospitals, our communities and our families. But what we have is us and our community. We have each other.
In this issue, it’s not just “business as usual.” GCMS has had an astounding year, and I’m reminded of the 150th year benefit gala we just had and looking forward to this year’s bash. That banquet was fire, as the kids would say. But it reminded me of the community we have in each other and how these connections keep us grounded, level, and knowing that what we do does make a di erence in our clinics, hospitals, families and communities.

Speaking of the issue, you will immediately see that we have a new president! We proudly introduce Dr. Melissa Gaines, also coming o a pretty remarkable year herself. We are honored to have Dr. David Barbe grace our pages again, talking about a pretty big thing—a bill you may have heard of that is also making our lives, uh, interesting. And on the flip-side, a er five years not writing about COVID-19, I summarized a few interesting research articles about the virus that continues to vex us. And maybe to encourage us to keep up the good fight. Dr. Brian Biggers, as he finishes up his year as MSMA president, reminds us of the other battles we should continue to be concerned.
Our alliance continues to focus on families and our community, especially our children, who will always need us. It is they that inspired the “Light in the Window” initiative introduced in this issue. Our financial sponsors and partners continue to help us provide for those families and loved ones, well into the future.
Bethany Thompson-Gordan, 4th year Mizzou medical student and recipient of GCMS’s Singing Doctor’s Scholarship, writes about what this means to her.
And for something completely di erent, talking about the wild west of aesthetics, Dr. Murphy Mastin helps us navigate the milieu of the types of professionals that may be providing these services, and reminds us that who we go to matters.
You’ll see how hard GCMS is working for this community, with our new council members, and their induction just a couple weeks ago. I was honored to give their oath to them.
So although we are “troubled on every side, we are not distressed, we are perplexed, but not in despair.” Paul, the apostle, wrote these words to the Corinthian church, as they navigated factions, false leaders, and arrogant teachings. In times as these, strength comes from unity, and unity comes in community, a group of physicians doing all we can for the good of our community. That is still our calling.
By Melissa Gaines, MD, FACP, FAAHPM
As I step into the role of President of the Greene County Medical Society, I am deeply honored to serve an organization that has long supported physicians across our region. Professionally, my career has centered on practice innovation, physician leadership, and end-oflife care, with a particular focus on geriatric, hospice, and palliative medicine. Over the years, I have had the privilege of serving in clinical, advisory, and board leadership roles, always guided by the belief that caring well for patients requires that we also care well for physicians. Those experiences have shaped my commitment to building systems, programs, and communities that support both professional excellence and human connection in medicine.
Outside of medicine, my greatest joy comes from my family. I am grateful for the love and support of my husband, Dustin, and our family, who keep me grounded and remind me daily of what truly matters. Our home is also shared with our beloved pets, who provide constant companionship and the kind of unconditional presence we all need more of in our lives.
The start of a new year naturally invites reflection and goal setting, and 2025 was a particularly meaningful year for me personally and professionally. One of the highlights was being part of The Soft Surrender , a documentary by Randy Bacon that explores hospice care in Southwest Missouri. This project gave voice to patients, families, and clinicians navigating life’s most sacred moments. I am thrilled that the film has been selected by the education committee as a featured presentation at the National Academy of Hospice and Palliative Medicine meeting in San Diego this March. It was a reminder that our stories, when told honestly, have the power to educate, heal, and connect us beyond our local community.
As I look toward 2026, I am also setting a few personal goals. I hope to improve my spiritual disciplines and, in a more aspirational sense, commit to Mediterraneanstyle meal preparation to support my own health and well-being. Like many of you, I am aware that statistics tell us only about 1% of people continue their New Year’s resolutions into the next year. With that in mind, I am embracing the idea of “stretch goals”—not perfection, but intentional progress.
That same mindset applies to my vision for GCMS. The year 2025 was a landmark year for our organization. GCMS successfully hosted its first GCMS BASH, raising funds

for the GCMS Foundation, and the Foundation made its first donation to Drury University an exciting investment in education and our future workforce. In addition, the Alliance celebrated 100 years of supporting physicians, a milestone that speaks to the enduring strength and relevance of organized medicine in our region.
Over the next two years as President, my goal is to lead meaningful change by strengthening the relationships between GCMS counsel, the GCMS Foundation, and the Alliance. Together, these three organizations have the potential to create a more cohesive, supportive, and resilient physician community. Physician resilience is not built in isolation, but grows from connection, shared purpose, and mutual support.
Only by developing a strong, engaged community of physicians will we make a meaningful impact on our ability to educate patients, promote health, and advocate effectively within our larger community. Perhaps my biggest stretch goal is for GCMS Council to serve as a true platform for social connection, educational opportunities, and advocacy. Not only for physicians’ health and wellbeing, but also for the public health of the patients we serve.
I am incredibly thankful for the opportunity to lead, to listen, and to serve as your President. I look forward to the work ahead and to continuing this journey together reflecting on where we’ve been, setting bold goals for where we are going, and supporting one another along the way.



Mission Statement Bringing physicians together to improve the health of our community.



Tailored Tax, Wealth Management, and Family Office to help you prepare for what’s next.











By Michael Clarke, MD
The years 2024 and 2025 saw a decline in the number of deaths among the Medical Society membership. However, John and Jim Duff were notable exceptions during this period. These brothers were highly regarded internists within the medical community, and their patients held them in especially high esteem. As twins, both were born on June 1, 1954, and shared not only their profession but also a deep connection throughout their lives. Jim Duff passed away on September 19, 2024, while John Duff followed a little over a year later, on October 23, 2025.
At the retired physicians’ Christmas luncheon, held at Hickory Hills Country Club, President Keith Laferriere paid tribute to the Duff brothers and their remarkable contributions. Both John and Jim were alumni of the University of Missouri Medical School in Columbia, Missouri, where they laid the foundation for their distinguished medical careers.

After completing his medical degree, John Duff began his career at the Cox Hospital network, taking on an administrative role at Cox North. Demonstrating a commitment to furthering his expertise, John pursued and earned a business degree in hospital administration from Washington University in St. Louis. His dedication and leadership led him to the position of Senior Vice President of Hospital Services. In the later years of his life, John was diagnosed with Alzheimer’s disease, which sadly brought his medical practice to an early end.

Jim Duff, like his brother, spent his early years in Fort Wayne, Indiana, before the family relocated to Ozark, Missouri. Their move paved the way for both brothers to attend and succeed at the state medical school in Columbia. Outside of medicine, Jim was known for his love of the outdoors and his devotion to his family. Together with his wife, Carla, Jim organized numerous adventure trips for their family, creating lasting memories.

The Greene County Medical Society has honored the lives and careers of John and Jim Duff, recognizing their dedication and service. Since 1873, the society has represented physicians in Southwest Missouri. Two of its notable subgroups—the Greene County Medical Society Journal and the Retired Physicians—were established around 1940. The journal now boasts a circulation of just over 1,500, with about half of the recipients being MDs and DOs.
Friends, colleagues, and the broader medical community deeply mourn the loss of the outstanding Duff brothers. Their legacy and presence will be truly missed.

By Brian Biggers, MD, President, MSMA
Recently a lawsuit was filed against the state of Missouri by a nurse practitioner seeking independent practice. One of the arguments is that nurse practitioners pay $50,000 for a collaborating physician. I have never heard of a value like this in the past. One should first ask why it takes that much? Another question which has arisen is, “What is the definition for the practice of medicine?”
One would think that this question would be easy to answer, but the state of Missouri does not have this defined. In 1907, Harry Huchins from the University of Michigan Law School wrote, “In a popular sense, and as ordinarily understood the practice of medicine is the applying of medical or surgical agencies for the purpose of preventing, relieving, or curing disease, or aiding natural functions, or modifying or removing the results of physical injury.” Additional comments from this said that there are interpretations related to legality.
Some states such as Washington have defined this as: A person is practicing medicine if he or she does one or more of the following:
(1)O ers or undertakes to diagnose, cure, advise, or prescribe for any human disease, ailment, injury, infirmity, deformity, pain, or other condition, physical or mental, real, or imaginary, by any means or instrumentality.
(2) Administers or prescribes drugs or medicinal preparations to be used by any other person.
(3)Severs or penetrates the tissues of human beings.
(4)Uses on cards, books, papers, signs, or other written or printed means of giving information to the public, in the conduct of any occupation or profession pertaining to the diagnosis or treatment of human disease or conditions the designation "doctor of medicine," "physician," "surgeon," "m.d.," or any combination thereof unless such designation additionally contains the description of another branch of the healing arts for which a person has a license: PROVIDED HOWEVER, That a person licensed under this chapter shall not engage in the practice of chiropractic as defined in RCW 18.25.005.
So why is the definition so important?

As physicians, we are navigating trying times. We face mounting pressures on all fronts. We have people who want to practice medicine but do not have the appropriate training as physicians. What many people fail to realize is the sacrifice made to become a physician. It takes every member of the healthcare team to deliver excellent care, but someone must be the captain of the ship. This is why we fight the scope of practice debate.
Recently the state of California ruled that a nurse with a doctorate cannot be called doctor in relation to a patient. Why, because this is confusing to patients. Many patients fail to realize that titles or di erences in healthcare professionals. There are patients who see a white coat and assume that the person is a physician. Even some of our legislators have di iculties with di erences in training. Not until we discuss training and experience do they understand. I once knew a nurse practitioner who went through medical school. This individual was confident going in but had di iculties with the first block. It was an eye-opening experience because the training, rigor and expectations were far di erent than the prior training.
If one wants to provide the same level of care as a physician, then that individual should have gone to medical school. There should not be an alternative to independent practice. As physicians, we have the same discussion with assistant physicians. We will not allow an alternative path for these physicians who have not gone through the appropriate training a er medical school.
By defining the practice of medicine, we will continue to improve the quality of healthcare for this state and the patients we serve.

President Melissa Gaines has chosen Estes Park Colorado and the Rocky Mountain National Park as our site for the GCMS Rocky Mountain Medicine site for 2026; July 18 through 25, 2026. CME meetings will be July 20,21, and 23. CME will qualify as AMA Cat I. Tuition will be $250 for GCMS members and $300 for non members.
We have reserved a block of condos at the Estes Park Condos. These units are only a mile from the famous Rocky Mountain National Park (RMNP) entrance. The RMNP Fall River is stocked with Rainbow trout and runs directly out of the park and in front of our condos. There is a community hot tub, but many of the condos have their own private hot tub as designated by the (HT) on their number. We have reserved a total of 25 condos. We have 4 one bdrm condos and 11 two bdrm condos in Creekside Suites which are closest to the Fall River meeting room and the community hot tub. We have also 5 one bdrm and 5 two bdrm condos in the Bugle Point A suites; many of these have private hot tubs. That gives us 25 condos reserved for 60 days, but any non reserved condos will be released to the public a er the 60 days.

Please check out the web site https://estesparkcondos.com/ and select your condo from the following list we have reserved:
• Creekside Suites: 2 Bed 1 Bath: 2,3,4,5,9,10,11,18,19,20, and 21(HT)
• Creekside Suites: 1 Bed 1 Bath: 1,12,16, and 22
• Bugle Pointe A: 2 Bed 2 Bath: A9(HT), A10, A11, A12, A14, A15
• Bugle Pointe A: 1 Bed 1 Bath: A2(HT), A5(HT), A13(HT), A16(HT)
Please check out the site map on the web site to see the location of the condos and their proximity to the community hot tub and Fall River meeting room.
When you have made your choice, call the number on the web site, identify yourself as a Greene County Medical Society attendee and reserve your condo choice (you will receive a 10% discount).
Once you have made your reservation, please report your reservation to this email (jimblaine@aol.com) and we will remove your condo from the available condo list.
We plan to be approved for 12 hours of AMA Cat I CME. Attendees are encouraged, but not mandated to do a 45 minute presentation with an additional 10 minutes for question and answer.
Please let us know if you have any questions
Melissa Gaines and Jim Blaine, co-chairs 417 861-9286
Q&A with Shane Rader, J.D. and Carlee Lynn, CFP®

Having a team of knowledgeable professionals is crucial when it comes to completing your estate plan and protecting your family, assets, and wishes. Local professionals Shane Rader (Attorney, Kembell, Woods, & Martinsen) and Carlee Lynn (Certified Financial Planner®, Forvis Mazars) focus on guiding physicians through their estate planning journey. Below, they share insights tailored specifically for physicians.
1)Estate planning sounds serious—what exactly is it, and what kinds of goals does it help people achieve? For many clients, taking care of their estate planning is a lot like going to the dentist’s o ice. Contemplating your future demise is just about as exciting as having your teeth worked on. While we certainly would agree that there are more enjoyable activities in life than estate planning, there is great value in being prepared for the inevitable. Estate planning is much more than just a post-death transfer of assets. When done right, estate planning allows for smooth legal transitions through life’s uncertainties and final stages. The clients who are most eager to have deep and meaningful discussions about their estate planning are o en those who have had a bad experience where a friend or family member did not take the time to put a proper estate plan in place.
2) Is there an ideal time in a physician’s career to complete an estate plan? Whether you are in medical school and only need simple durable powers of attorney and beneficiar y designations, or you are an established practitioner needing a trust—everyone should have an estate plan in place. The most common seasons of life when people consider estate planning are when children are born, when parents become empty nesters, and when we lose loved ones. The truth is, our death will always impact others, so there is never a bad time to consider establishing an estate plan.
3)When it comes to estate planning, how important is it for physicians to work with an attorney who focuses on this area—does it really make a di erence? Of all people, physicians understand the value of going to a specialist in a clinical setting. Estate planning, especially for those with a higher net worth, can get complicated fast. Estate planning attorneys are ver y mindful of updates to tax law, state law, and can advise clients about the gi tax, estate tax, and Generation-Skipping Transfer Tax (GSTT).
4)Do physicians need to approach estate planning di erently than other professionals? It is important to be mindful of liability exposure for physicians. As part of the planning process, liability can both be isolated and mitigated. Liability can be isolated using an LLC or other business structures where the proper formalities were followed. Liability can be mitigated through insurance, so for physicians understanding the coverage your existing malpractice policy provides is key. For married couples, it can also be mitigated by titling assets as Tenants By The Entirety. Working with your attorney and financial advisor to understand the titling and values of your
assets is a worthwhile conversation to have, as everyone’s situation is unique.

5)What are some of the most common estate planning missteps physicians tend to make—and how can they steer clear of them? O entimes, physicians take the time to put together a solid and well-dra ed estate plan. However, they fail to revisit the plan and consider how changes in family dynamics or the tax law impact their plan over time. For example, there have been high-impact reforms to Missouri law and the federal estate tax regime over the past 20 years. Reviewing your estate plan every five years is a recommended best practice.
6) Are there recommendations that were common in the mid-2000s that may no longer be as relevant today? Significant changes have occurred over the past 20 years. Physician households have traditionally been concerned with incorporating creditor protection into their estate planning. Thankfully, there have been many advances on that front in Missouri law. Twenty years ago, spouses would usually set up separate revocable trusts, which did not have Tenancy By The Entirety (TBTE) protection. It wasn’t until 2011 that Missouri law allowed for the creation of a joint qualified spousal trust, which enables married couples to establish a Trust that has the same TBTE protection that they are familiar with on financial accounts and real estate. For plans dra ed before 2011, we sometimes see physician households use the “safe spouse” strategy. This is where the majority of the couple’s assets are transferred to the spouse with the less risky profession. This approach is not favored, as it assumes that you can predict future liability events. The plan can easily go awry if the safe spouse is unexpectedly involved in a liability event, e.g., car accident, leaving the couple’s assets open to attachment by creditors.
7)With estate tax exemptions now set at higher levels—$15 million for individuals and $30 million for married couples in 2026—how have planning priorities and strategies shi ed for physicians? Over the past couple of years, we have had clients waiting to see what might happen with the estate tax exemption, which was temporarily increased under the Tax Cuts and Jobs Act of 2017 (TCJA). The increased exemption was scheduled to sunset (decrease) at the end of 2025 with a number of other temporary provisions in TCJA. However, as a result of the One Big Beautiful Bill Act that passed in July 2025, which permanently increased the exemption to $15 million per individual (indexed for inflation) beginning in 2026, a lot of clients have been able to pivot from gi ing strategies (necessary if the exemption were to decrease) to a more steady and forward-thinking approach. For a lot of our married clients who do not yet have a taxable estate, disclaimer planning, and the flexibility that it provides, is the most advantageous trust structure. However, it is never too early for high-net-worth physicians to begin discussing gi ing strategies to incorporate in their estate plan .
By Murphy Mastin, MD, Dermatology
Aesthetic medicine today really is a “world is your oyster” situation. Botox, filler, lasers, body contouring, skin tightening. There are more options than ever, and many of them can be done well, safely, and with beautiful results. The problem is that in Missouri, and honestly much of the United States, aesthetics is not regulated in a way that makes it easy for patients to know who is actually qualified. In cities like Springfield, there are so many places o ering aesthetic treatments that it can feel overwhelming. And the reality is that it is a bit of the wild west. That does not mean aesthetics is unsafe. It means patients need a framework for due diligence.
First, it is important to understand that aesthetic medicine is still medicine. These are not spa services. Neuromodulators a ect nerves and muscles. Dermal fillers alter facial structure and, in rare but real cases, can compromise blood flow. Lasers and energy based devices intentionally deliver heat or light into the skin to create controlled injury. When done correctly, these tools are incredibly e ective. When done poorly, they can result in burns, scarring, pigment changes, infection, asymmetry, and long term complications. The di erence almost always comes down to training, anatomy knowledge, and systems, not branding.
One of the most important things to look for is who is medically responsible for your care. Ideally, procedures are performed by or directly supervised by a physician with deep training in facial anatomy and skin biology. Dermatologists, plastic surgeons, ENT physicians, facial plastic surgeons, and oculoplastic surgeons all fall into this category. Patients should feel comfortable asking who the medical director is and where that physician is located, particularly if procedures are being performed by non-physician providers. Knowing whether the supervising physician is local and available is a reasonable and important part of assessing safety.
Non-physician providers such as nurse practitioners, physician assistants, and registered nurses can also be excellent aesthetic providers. Many are highly skilled. However, outcomes and safety depend heavily on the quality of their training, the experience of the supervising physician, and whether clear protocols exist for complications. A clinic should be able to clearly explain who is doing your procedure, what their training is, and who steps in if something goes wrong.
The consultation itself is very telling. A safe aesthetic practice approaches consultations like a medical visit, not a sales pitch. You should be asked about your medical history, medications, supplements, prior aesthetic treatments, and your goals. A thoughtful provider explains risks, alternatives, and realistic outcomes and is comfortable recommending against treatment if something is not appropriate. If the consult feels rushed, heavily scripted, or focused on packages and promotions rather than anatomy and planning, that is a red flag.
Transparency around products matters. FDA approved

neuromodulators and fillers should be used, properly sourced, and documented. You should know what is being injected and why. If pricing seems dramatically lower than everywhere else, it is reasonable to ask questions. In cash pay medicine, extreme discounts can sometimes signal excessive dilution, inappropriate sourcing, or lack of experience. High quality care is not about being expensive, but it is about being accountable.
For lasers and energy based devices, safety depends on understanding skin type, pigmentation risk, and proper settings. A good provider asks about recent sun exposure, tanning, melasma history, prior reactions, and skincare use. They explain downtime honestly and give clear pre and post care instructions. Be cautious of anyone who claims a device is safe for everyone with no downtime and guaranteed results. Those claims usually reflect marketing, not medicine.
Another critical but o en overlooked issue is complication preparedness. For fillers, this means having reversal agents available, knowing how to recognize vascular compromise, and having a plan for urgent evaluation and referral. For lasers, it means knowing how to manage burns, infections, and pigment changes. Protocols matter, but the ability to recognize and manage complications in real time is what separates someone following a checklist from an experienced clinician. You do not need a provider who scares you. You need one who is prepared. Asking what happens if something does not look right a erward is a reasonable and important question.
Social media can help, but it should not be the deciding factor. Look for consistency, natural results, and respect for individual anatomy. Overly filtered photos, identical faces, or trend driven extremes should prompt caution. Experience shows up in restraint and balance, not in chasing whatever is popular this month.
At the end of the day, trust how the process feels. You should feel heard, informed, and safer a er your visit, not pressured or rushed. The best aesthetic providers are comfortable setting boundaries and saying no when something is not in a patient’s best interest.
Aesthetics can be empowering, confidence boosting, and genuinely fun. But it should always be grounded in medicine, anatomy, and patient safety. As physicians, we recognize that aesthetics occupies a unique space where elective care still demands medical rigor. In an environment with variable regulation, patient education and professional accountability remain the strongest safeguards.
References:
1. U.S. Food and Drug Administration. Dermal fillers: FDA safety communication. Updated 2023. 2. DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthetic Surg J. 2014;34(4):584–600.
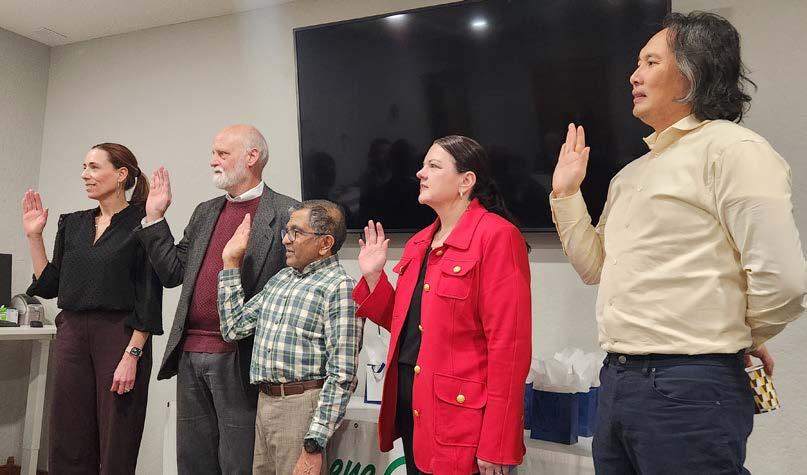
Several members and their spouses were in attendance at the annual GCMS meeting January 15, 2026. Dr. Jim Rogers was the master of ceremonies and outgoing President handing the baton over to Dr. Melissa Gaines for 2026.
GCMS Together is the focus this year, with the Greene County Medical Society and its council, the Greene County Alliance, and the Green County Medical Society Foundation all focussed on one project this year.
A celebration of 2025 was in order and we were reminded of scholarships given this year to MU and Drury students. New council members were installed after repeating the oath after Dr. MinhThu Le, former GCMS President. Dr. Rachelene Middleton (new council member), Dr. Jim Rogers (immediate past president), Dr. Sanjay Havaldar (treasurer), Dr. Vu Le (secretary), and Dr. Melissa Gaines (President) were all in attendance to take their oaths of office. Cathy Leibould represented the Alliance and introduced their
new initiative, “A Light in the Window,” where they will raise monies for Alliance projects.
This idea was attributed to Dr. Barbe’s wife, Debbie Barbe, as a reminder to physician families that there is a loved one waiting for someone to come home safely. Gaines Real Estate promised $500.00 to the project that evening. We are looking forward to a productive and successful year!



























































































By Barbara Hover, Alliance Chair
GCMS Alliance celebrated the holidays with a fun filled annual meeting on December 11, 2025. A tasty brunch was followed by a short business meeting.
Debbie Barbe presented our new project “A Light in the Window”. She stated, “A light in a window is frequently understood to be synonymous with hope and welcome, indicating there is food and shelter for those in need or traveling.

Start a family tradition with us by purchasing one of these electric candles. Give it to a child to place it in his or her bedroom window or a window that faces the road where mom or dad returning home will see it first. The candle could be used by mom and dad to welcome home a student from college or friends or family coming to visit. It will be your own secret symbol between you and the ones you love; a symbol to share as you turn it on each evening.
The Bellamy Brothers sing a beautiful song, “Let Your Love Flow.” One verse reads “there’s a reason for the warm sweet nights and there’s a reason for the candle lights, must be the season when those love rights shine all around us.”

Shine a light for the weary traveler arriving home from the ER, OR, clinic, hospital, or place far away. The welcome starts in the window before they come through the door. It will give those waiting a loving, fun thing to do as they switch on the light of their very own candle.
Have you ever wished for one more way to say, “I love you?” Here is your chance to say it every day as they return home. Lights were given to those in attendance and additional ones may be purchased for $5 from GCMSA.
We then played the game Heads or Tails. Dr. John Mihalevich was our winner and received the door prize. Our new fiscal year began January 1 and we hope you join or renew your membership online or through this link. https://gcms.us/ Alliance. Thank you and have a Happy New Year.


By Minh-Thu Le, MD, Allergy/ Clinical Immunology, Ferrell Duncan Clinic, Cox Medical Group, Associate Professor, University of Missouri-Columbia, Springfield Clinical Campus
It’s been over 5 years since the SARS-CoV-2 virus took over the global stage and over 7 million souls have succumbed to its scourge with over 770 million of us getting infected. Getting a booster shot is as fast as going to the local pharmacy, or it should be. In the US, we have had mixed messaging and severe vaccine hesitancy in these five years. However, the body of research is clear that COVID vaccines, and specifically, mRNA vaccines, play a vital role in significantly decreasing morbidity and mortality.
I will quickly summarize several articles to confirm what I believe to be the “low-hanging fruit” of encouraging all our patients to be vaccinated at least yearly (and in those 65 years and up, or with immunodeficient states, every 6 months) to COVID-19. With the current HHS secretary recommending a “shared decision making” approach between clinicians and patients at this time prior to getting a booster, if we don’t have the conversation with our patients, they are much less likely to get a COVID vaccine.
A couple studies were published recently about the e icacy of COVID vaccines based on nationally collected data. The most impressive was the cohort study of all-cause mortality out of France which analyzed 29 million people from 18-59 years of age and followed for four years, vaccinated with at least one dose of an mRNA vaccine. This age group was chosen due to the fact that they are more likely to have less severe disease and confirmed lower mortality than the higher age brackets, and analyses of vaccinated verses unvaccinated would be able to show more if vaccination decreased mortality and mobility in a seemingly healthier population sample. Pharmacoepidemiological studies prior could not distinguish if vaccines were helpful due to “unmeasured confounders or a healthy vaccinee bias.” A cohort study had not been done on this patient group for long-term mortality, according to the authors. Their objective was to determine the risk of all-cause mortality at 4 years in this population.
What they found was not just statistically significant, but striking. Their methods were sound in analyzing databases (the national hospital discharge database, the COVID-19 vaccine database, and the National Health State System) with everyone having an individual anonymous number that follows them all their lives, 68 million residents. Because they have a one payor system, since 2006, all insurance claims are in the National Health Data System (SNDS), and every diagnosis code associated with any individual from birth to death can be crossreferenced. The National hospital discharge database has reimbursement information for inpatient care, diagnoses, and procedures. Also, the death registry (CepiDc registry) was used to match to individuals using date of birth, sex, and residence.

They gave a 6-month grace period a er vaccination index date and used a random date (found by replicating the index dates for a vaccinated person and applying it to an unvaccinated randomized individual) to avoid “immortal time bias.” Twenty-six million were vaccinated, 2.9 million were not. They were then followed for a median time frame of 45 months. They additionally looked at the 6 months a er vaccination in the vaccinated group to see if mortality a er vaccine increased at all, which it actually showed the opposite: increased survival of the vaccinated group compared to unvaccinated. Individuals who were alive from November 1, 2021 were included and had received at least one mRNA vaccine between May 1 and October 1, 2021, the time where mass vaccinations occurred in France.
They looked at socioeconomic variables, subdivided age categories, identified 41 separate comorbidities, with additional ones of obesity, smoking, and alcohol disorders and history of severe COVID infection. Vaccinated individuals were older, had more cardiometabolic comorbidities, and were more frequently women.
They ridded the study of as much confounding variables as they could, including two negative control outcomes (NCOs): hospitalization for traumatic injury and hospitalization for unintentional injury (both using ICD-codes to delete them from their analysis).
Over the 4-year period, vaccinated individuals had a 74% lower risk of death from severe COVID-19 (0.26 [95% CI, 0.22-0.3]) and a 25% lower risk of all-cause morality (0.75 [95% CI, 0.750.76]). Additionally, mortality was 29% lower within 6 months following COVID-19 vaccination (relative incidence, 0.71 [95% CI, 0.69-0.73]).
Now for more evidence that continuing to get vaccinated is the right choice for the vast majority of individuals.
One study you may not have seen was out of Kosovo, a middleincome economy, with a population of 1.5 million people. I think we can extrapolate at least some of this study and apply it to cities and areas like here in the Greene County/ Springfield, MO metro area, where we have about 1 million lives and largely poor to middle class socioeconomically. The Pfizer mRNA vaccine was the most widely used vaccine in Kosovo, followed by the AstraZeneca adenoviral-vectored vaccine. (Raise your hand if you remember me writing about this one in 2021!) About 46% of their population received the 2-dose primary series vaccination, 6% with one additional booster, and 4% with two boosters. Few vaccine boosters were administered during 2023 and 2024. Looking at our own data for COVID-19 primary series uptake, Springfield/Greene County had 52-61% vaccination
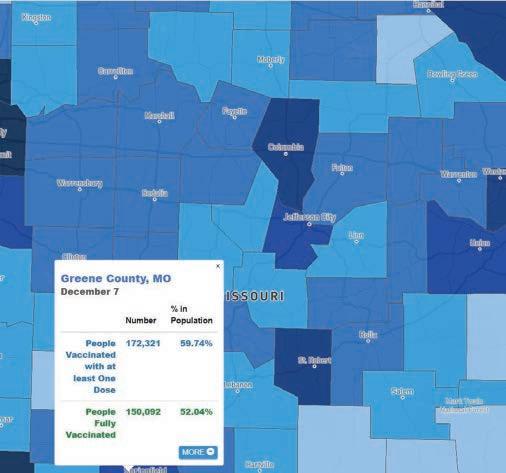
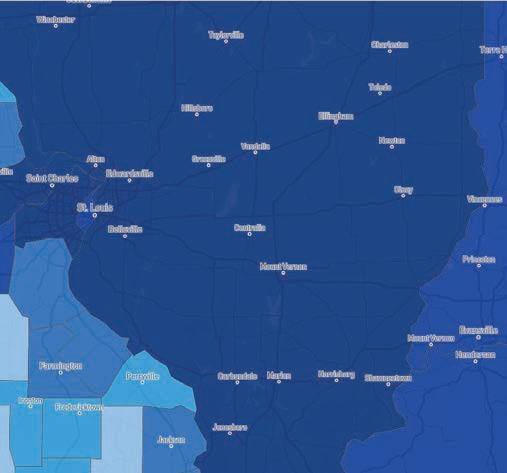

with the primary series, with surrounding counties between 3451%, so likely averaged around 45-50%. (see graphic above). I could not find booster data in our area, but I would assume it is much lower and similar to the Kosovo data.
Theirs was a test-negative case control study of adults 18 years and older. Per JAMA’s Guide to Statistics and Methods, “In a test-negative design, the study population consists of people tested for the disease of interest, typically because they exhibit specific symptoms. Those with positive diagnostic test results are test-positive cases. Test-negative controls meet the criteria for testing but have negative diagnostic test results. Thus, their symptoms are due to a cause that the vaccine does not target.”
Their study had just 564 patients, but confidence intervals still showed significance. What they saw was a 72% decrease in hospitalizations at 14-197 days post-vaccination (95% CI: 3089%), and 26% decrease at 180-364 days post-vaccination (95% CI 33-59%). Of note, the longer post-vaccination one was, the higher the rate of morbidity and mortality. The wide confidence interval was likely partly due to the wide range of ages in the adult study.
Lastly, someone in the CDC still has a job and is doing the work needed to add to the body of evidence that children are also benefitting from booster doses of mRNA vaccines. The Morbidity Mortality Weekly Report from December 11, 2025 showed significant decrease in ER/UC visits in children having had the booster COVID vaccine for the 2024-2025 COVID season. This was also a test-negative case control study for vaccine e icacy (VE).
The data was taken from the Virtual SARS-CoV-2, Influenza and Other respiratory viruses Network (VISION), a multi-site electronic health record (EHR)- based network in nine states used to estimate vaccine e ectiveness. This included 256 EDs/ UCs. They included children aged 9 months-17 years who visited

one of these sites from August 29, 2024- September 2, 2025.
Excluded were those that had a vaccine <7 days before presentation or received a dose <2 months prior to another COVID-19 dose unless part of an initial series, and if they were also positive for influenza at the same time as COVID. All children were included regardless of prior COVID infections.
They separated their groups into ages 9 months-4 years, and 5-17 years due to di erences in vaccine recommendations of these two groups. Among the first group, about 44,500 encounters met inclusion criteria, with about 1,300 case patients and about 43,000 control patients. Twelve (<1%) of case patients and 1,847 (4%) control patients received a 2024-2025 COVID-19 vaccine dose. E ectiveness of a 2024-25 COVID-19 vaccination against a COVID-19 associated ED/UC visit was 76% (95% CI= 58–87%) during the first 7-179 days a er vaccination and 77% (95% CI= 62-86%) during the first 7-299 post-vaccination.
In the 5–17-year-old group, about 53,500 encounters met criteria, with 1,325 (2%) case patients and 52,142 (98%) control patients. Twenty-six case-patients (2%) and 2,462 (5%) control patients had a current vaccine dose. E ectiveness of a 202425 COVID-19 vaccination against a COVID-19 associated ED/ UC visit was 56% (95% CI= 35-70%) during the first 7-179 days a er vaccination and 45% (95% CI= 25-59%) during the first 7-299 post-vaccination. Results were similar upon further stratification of this group (5-11 years, 51%, and 12-17 years, 61%, with overlapping CIs).
Several limitations were discussed: COVID-19- like illnesses potentially not being the primary complaint and therefore not documented, misclassification of vaccine status (but previous studies of vaccine status have yielded similar VE estimates), smaller sample size than other studies on VE decreasing power of study, with wider CIs, low vaccination status of children may
reduce generalizability, and residual confounding variables such as behavioral modification to prevent COVID exposure (not going to ER/UC and outpatient antiviral treatment) may remain.
Overall, this study is very convincing in getting children booster doses to prevent illness and UC/ER visits.
The CDC in November also made the recommendation that a second COVID vaccine this season from 2-6 months, and ideally, 6 months, a er the first, should be recommended to all those with increased risk of poor outcome with moderate to severe immunodeficient states and all those 65 years old and older. I tend to remind everyone that obesity is an immunodeficiency state for COVID-19, and also asthma, COPD, heart disease, cancer, autoimmune states with immune suppressant/modulatory medication (i.e. prednisone) and diabetes, among others. The majority of American adults would qualify for a second dose. This is based on literature that the vaccine antibody wanes substantially a er 4-6 months, and severe infections increase (as seen in the Kosovo study). You know that patient that still gets COVID a er vaccination? It’s important to ask when they were vaccinated, and if over 4-6 months prior, then their protection had already waned. One recent European study that may have led to this recommendation showed that only 3% of hospitalized patients had received a COVID-19 vaccine within the past 12 months.
I know I said “lastly” already, but I just want to mention a recently published study on long-COVID as an occupational disease. A population-based study out of Spain published in BMJ Occupational & Environmental Medicine showed 44% higher odds of long-COVID with certain occupations, including healthcare, social workers, teachers, retail workers, transport workers and security sta . This risk was still significant when other confounding variables were controlled (obesity, multiple co-morbid conditions, severe/repeated infections, female sex). Workplace conditions that amplified this risk were working onsite during the pandemic, inconsistent use of high-quality respirators, and regularly commuting by public transportation. Since we are in a very high-risk field (and may know colleagues, friends and family with long-COVID that may have had to leave the workforce because of it), I think it is important for us to protect ourselves and families as well. We should be the first to get every COVID-19 booster, wearing PPE, and taking precautions when traveling to decrease our own risk for longCOVID. A er all, we are really the only trusted voices in many of our circles and for our patients and without us, they are likely to su er more.
I still have patients that are resistant to the COVID vaccine, but many more that had the primary series and willing to get the booster if I just mention it. It gets easier the more you ask. I mention the most recent studies on why I’m recommending it pretty much universally for everyone. I’ve had every COVID vaccine variant available. It’s typically available the first of September. My kids and husband have had all of them as well. The last time I had COVID was in 2021 and hope to never have it again. And for those that had reactions to mRNA or may not have made good antibody responses, I remind people
that a new protein-recombinant vaccine with the most recent available COVID strain is available as well!
So pick that low-hanging fruit. It takes five seconds to mention that we still recommend getting every new COVID-19 booster to protect yourself and your loved-ones!
References:
1. COVID-19 mRNA Vaccination and 4-Year All-Cause Mortality Among Adults Aged 18 to 59 Years in France.Laura Semenzato, PhD, MSc1; Stéphane Le Vu, PhD1; Jérémie Botton, PhD, PharmD, MPH1,2 et al. JAMA Network Open. Vol. 8, No. 12. https://jamanetwork.com/journals/ jamanetworkopen/fullarticle/2842305
2. JAMA Guide to Statistics and Methods. Edward H. Livingston, Roger J. Lewis.
https://jamaevidence.mhmedical.com/book.aspx?bookid=2742 https://jamaevidence.mhmedical.com/content.aspx?bookid=2742§io nid=292454805
3. COVID‐19 Vaccine Effectiveness Against Hospitalizations and Severe Outcomes in Kosovo, 2022–2024: A Test-Negative Case–Control Study. Besfort Kryeziu 1,2,3,✉, Sandra Cohuet 4, Ariana Kalaveshi‐Osmani 1,3, Zana Kaçaniku-Deva 1, Pranvera Kaçaniku-Gunga 1, Iris Finci 5, Miguel Angel Sanchez 4, James Humphreys, 4,Naser Ramadani 1,3, Edita Haxhiu 3, Kostas Danis 2, Angela M C Rose 4, Isme Humolli 3,6,✉, Mark A Katz 5Influenza Other Respir Viruses. 2025 Sep 8;19(9):e70152. doi: 10.1111/ irv.70152. https://pmc.ncbi.nlm.nih.gov/articles/PMC12417103/
4. Greene County, MO COVID‐19 Vaccine Tracker. https://data.news‐leader. com/covid‐19‐vaccine‐tracker/missouri/greene‐county/29077/
5. COVID-19 Hospitalizations, Vaccine Uptake, Vaccination Guidelines, and Vaccine Availability in Six Middle‐Income Countries and Areas in Europe, May 2022–April 2024. Erin Rachel Whitehouse 1,✉, Paul Elish 1, Elona 2, Dragan Kochinski 3, Dragana Plavsa 4, Giorgi Chakhunashvili 5, Besfort Kryeziu 6, Sayragul Abdyldaeva 7, Miguel Angel Sanchez Ruiz 8, Sandra Cohuet 8, James Humphreys 8, Kujtim Mersini 9,10, Oksana Artemchuk 11, Maja Stosic 4, Olgha Tarkhan-Mouravi 5, Ariana Kalaveshi 6, Dinagul Otorbaeva 7, Kristina Stavridis 3, Silvia Bino 2,10, Marc‐alain Widdowson 11, Eva Leidman 1, Iris Finci 11, Mark A Katz 11Influenza Other Respir Viruses. 2025 Jun 18;19(6):e70126. doi: 10.1111/irv.70126. https://pmc. ncbi.nlm.nih.gov/articles/PMC12176449/
6. Effectiveness of 2024–2025 COVID‐19 Vaccines in Children in the United States — VISION, August 29, 2024–September 2, 2025. Weekly / December 11, 2025 / 74(40);607–614. https://www.cdc.gov/mmwr/volumes/74/wr/ mm7440a1.htm
7. 2025–2026 COVID‐19 Vaccination Guidance. https://www.cdc.gov/covid/ hcp/vaccine‐considerations/routine‐guidance.html
8. Occupational factors of Long-COVID in a population-based cohort in Catalonia: the COVICAT study. Sara De Matteis, Dario Consonni, Ana Espinosa, Rafael de Cid, Natalia Blay Magriña, Gemma Castaño-Vinyals, Marianna Karachaliou, Miguel Angel Alba Hidalgo, Kyriaki Papantoniou, Judith Garcia‐Aymerich, Manolis Kogevinas, Kurt Straif. https://oem.bmj. com/content/82/Suppl_2/A58.3
For those wanting to read Dr. Le’s articles on the COVID vaccine platforms from 2020-2021, contact the GCMS o ice at 417-8871017, or email the author at minh-thu.le@coxhealth.com.


Roy Gaines















By : Cody Bean, Financial Planning Specialist for Arvest Wealth Management
Thanks to updated IRS rules for 401(k), 403(b), and IRA contributions, 2026 is poised to be a pivotal year for retirement planning. These new rules offer valuable opportunities to accelerate savings, especially for those aged 50 and older. There’s also an important update that high earners should be aware of. Here’s a look at key changes to help you evaluate your tax strategy with the goal of fully optimizing your retirement plan. Arvest does not provide tax advice, so it's important to consult your tax advisor about your strategy.
The standard catch-up limit for those aged 50-59 and over 64 increases.
For 2026, the standard-catch-up limit rose from $7,500 to $8,000 for 401(k) and 403(b) plans. The standard contribution also increased from $23,500 to $24,500, resulting in a total maximum contribution of $32,500.
Super catch-up contributions remain the same For employees ages 60 through 63, the “Super Catch-Up” contribution limit remained the same at $11,250 for 401(k) and 403(b) plans.
Mandatory Roth catch-up contributions have been implemented for high earners.
If your Social Security (FICA) wages from 2025 were greater than $150,000, your catch-up and super catch-up contributions must now be Roth contributions, meaning you pay taxes now, but future withdrawals, including earnings, can be tax-free if you’re age 59½ or older or the account has been open at least five years. If your employer’s retirement plan does not currently allow Roth contributions, you may not be able to make catch-up contributions in 2026 unless the plan is updated.
Pre-tax or after-tax flexibility remains for those who earned less than $150,000. If you earned less than $150,000 last year, your catch-up and contributions can be made on a pre-tax basis to reduce taxable income now or on an after-tax Roth basis, where contributions grow tax-free and qualified withdrawals in retirement are not taxed
IRA contribution limits increase. Traditional and Roth IRA contribution limits for 2026 increased to $7,500 (up from $7,000) for those under 50. For those 50 and older, the maximum increased to $8,600 (up from $8,000) when including the catch-up contribution limit of $1,100.

Roth IRA income limits increase. The income limit for single filers increased from $150,000 to $153,000 in 2026. If your Modified Adjusted Gross Income (MAGI) is between $153,000 and $168,000, you’re eligible to contribute a portion of the full amount. The limit increased to $242,000 for those filing jointly. For those whose MAGI is between $242,000 and $252,000, they’ll also be able to contribute a portion of the full amount.
To make the most of your retirement savings in 2026, consider taking these steps:
1.Review your contributions – Make sure you’re taking full advantage of the current catch-up and super catch-up limits and maximizing your catch-up or super catch-up opportunities.
2.Evaluate your tax strategy – Roth contributions can be a smart choice if you expect to be in a higher tax bracket later or want more flexibility in retirement.
3.Stay informed – Consult your financial advisor or tax professional to review your options, determine the best strategy for your situation and align your contributions with your long-term goals.
4.Act early – Making adjustments early in the year can help you integrate the new rules smoothly into your retirement plan.
Understanding how these 2026 changes may impact your retirement plan can give you greater control over your holistic financial plan. With proactive planning, informed adjustments, collaboration and guidance from your financial and tax professionals, you can continue to build your wealth, protect what you’ve built, and work toward your goals with more resources, security and peace of mind.

By: Bethany D. Thompson-Gordon, M4, University of Missouri School of Medicine –Columbia, MO, Springfield Clinical Campus
Music has always been a meaningful part of my life. I began learning to play the piano by ear at the age of five and eventually shared my love of music through singing and playing in my church. Music became my emotional outlet; I would express myself through the keys and my voice, whether I was celebrating a happy moment or needed to find my way out of a rut on a difficult day.
As I began to pursue medicine—balancing prerequisites, shadowing, and volunteering—time for music became increasingly scarce. By the time I started medical school, I felt I had lost touch with the musical side of myself that brought me so much joy.
I found that side of myself again as a co-founder and former vice president of Mizzou Med Musicians, a music interest group I helped start in 2022. I have loved using music to connect with others, whether performing for patients, at school events, or in the community. Singing with fellow students has provided some of my fondest memories of medical school.
Now a fourth-year medical student at the University of Missouri School of Medicine, I am completing my clinical rotations at the Springfield Clinical Campus. During my time here, I learned about the legacy of the Singing Doctors and listened to recordings of their humorous musical performances from decades ago. I felt a special connection to their mission as physicians who once shared the joy of music with their community.
Receiving the Singing Doctors of Springfield Scholarship is especially meaningful to me, as it celebrates both medicine and music—the two passions that have shaped who I am today. This scholarship makes a tangible difference in my final year of medical school. It assists with school expenses and the costs associated with applying to Family Medicine residency programs, helping me find the program that will be the best fit for my future. I am truly grateful for the generosity of the donors; their support lightens my financial burden and reminds me why I chose this path—to help others, to keep learning, and to find everyday joy in both medicine and music.


The Singing Doctors of Greene County Medical Society were featured on the cover of the March/April 2025 cover of the GCMS Journal. While the Singing Doctors' specific endowment moved to the University of Missouri, the GCMS Foundation continues to manage other local community health projects and charitable initiatives in the Springfield area.
Origin: Founded in 1958 by Dr. Jim Brown to provide entertainment for the annual GCMS banquet without a budget.
Funding: The money was raised through local performances and record sales until the group stopped performing in 1989.
Purpose: To support medical students from southwest Missouri, often specifically those attending the University of Missouri.
Current Status: The fund remains active and continues to help MU medical students.

Direct Primary Care
ASCENT DIRECT PRIMARY CARE, LLC
MATTHEW GREEN, DO H
Family Medicine
Bringing physicians together to improve the health of our community.
Dermatology, Procedural
MICHAEL H. SWANN, MD H
BRETT NEILL, MD
MICHAEL KREMER, MD
JOHN CANGELOSI, MD
AUTUMN BERTHOLDI, PA-C
PATSY DUGGAN, PA-C
LORI MILLER, NP-C
HANNAH LEE, FNP-BC
BROOKLYN FORT, FNP-C
3850 S. National Ave, Suite 705 Spring eld, MO 65807 (Located inside Hulston Cancer Building-7th oor)
1240 E. Independence Spring eld, MO 65804
Phone: 417-888-0858 • Fax: 417-889-0476 www.swanndermatology.com
Hollister Location 590 Birch Rd, Ste 2c Hollister, MO 65672
PH. 417-690-3858 Fax 417-690-3862
Monett Satellite Location (Inside CoxHealth Urgent Care) 2200 E. Cleveland Ave Monett, MO 65708
Phone: 417-888-0858 • Fax: 417-889-0476
Lebanon Location 331 Hospital Drive Suite C Lebanon, MO 65536
Phone : 417-344-7200 Fax : 417-344-7299
To Advertise in
Please Note: Changes to ads will be made quarterly and must be submitted in writing. H Denotes GCMS Membership “A” Denotes GCMS Applicant
GCMS Member Ad Rates: $10.00
Family Medicine
COXHEALTH
FAMILY MEDICINE RESIDENCY
FAMILY MEDICAL CARE CENTER
www.ascentdpc.com
417-595-0956
413 N McCroskey, Ste 2 Nixa, MO 65714
EYE SURGEONS OF SPRINGFIELD, INC.
C. BYRON FAULKNER, MD H Comprehensive Cataract Ophthalmology
JUDD L. McNAUGHTON, MD H Comprehensive Cataract Ophthalmology Diplomates, American Board of Ophthalmology
1330 E. Kingsley St. • Spring eld, MO 65804 Phone 417-887-1965 • Fax 417-887-6499 417eyecare.com
MATTAX • NEU • PRATER EYE CENTER
JAMES B. MATTAX, JR., MD, FACS H American Board of Ophthalmology
LEO T. NEU III, MD, FACS H American Board of Ophthalmology
DAVID NASRAZADANI, MD
DREW A. YOUNG, MD
THOMAS PRATER, MD, FACS H American Board of Ophthalmology
JACOB K. THOMAS, FACS, MD H American Board of Ophthalmology
BENJAMIN P. HADEN, MD H American Board of Ophthalmology
MICHAEL S. ENGLEMAN, OD
MARLA C. SMITH, OD
MATTHEW T. SMITH, OD
1265 E. Primrose Spring eld, MO 65804 417-886-3937 • 800-995-3180
3800 S National Ste 700 Springfield, MO 65807 (417) 269-8817
AMERICAN BOARDOF FAMILY MEDICINE
Marc Carrigan, MD
Cameron Crymes, MD
Kristin Crymes, DO
Kristen Glover, MD
Kyle Griffin, MD
Shelby Hahn, MD
Laura Isaacson, DO
Evan Johnson, MD
Katie Davenport-Kabonic, DO
Michael Kabonic, DO Jessica Standeford, MD
WOMAN’S CLINIC www.womansclinic.net
Leaders in Minimally Invasive Gynecology & Infertility
DONALD P. KRATZ, MD, FACOG H American Board of Obstetrics and Gynecology
AMY LINN, FNP-BC American Academy of Family Nurse Practitioners
ANGIE JONES, WHNP-BC 1135 E. Lakewood, Suite 112 Spring eld, MO 65810
Located inside Tri-Lakes Family Care 1065 Hwy 248 Branson, MO 65616
Phone 417-887-5500
Fax 883-8964 or toll free 877-966-2607
Monday-Thursday 8am-4:30pm Friday 8am-12pm
MERCY CLINIC–INTERNAL MEDICINE WHITESIDE
RAJ ANAND, MD
JAMES T. ROGERS, JR. MD, FACP H Board Certi ed in Internal Medicine
MARIA DELA ROSA, MD
NELSON DELA ROSA, MD
AMANDA MCALISTER, MD
ALEJANDRA ROA, MD
KELLY TRYGG, MD
GABBY BONNER, NP
STEVEN BOWLIN, MD Board Certi ed in Internal Medicine
STEPHANIE HOVE, NP
CARRIE KUGLER, PA
COURTNEY WEATHERFORD, PA
JENNIFER WHITE, PA
VICTOR GOMEZ, MD
Board Certi ed in Internal Medicinee
2115 S. Fremont, Suite 2300 Spring eld, MO 65804
Phone 417-820-5600 Fax 417-820-5606
MERCY CLINIC UROLOGY (FREMONT)
ERIC P. GUILLIAMS, MD, FACS H American Board of Urology
ROBERT D. JOHNSON, MD, FACS H American Board of Urology
TYRUN K RICHARDSON, MD American Board of Urology
Phone 417-820-0300
Fax 417-882-9645
1965 S Fremont, Ste. 370 Spring eld, MO 65804
ADULT MEDICINE & ENDOCRINOLOGY
JONBEN D. SVOBODA, MD, FACE, ECNU
American Board of Endocrinology
JAMES T. BONUCCHI, DO, ECNU, FACE
American Board of Endocrinology
NICOLA W. GATHAIYA, MD, ECNU, FACE, CCD
American Board of Internal Medicine
American Board of Endocrinology
STEPHEN M. REEDER, MD, FACP
American Board of Internal Medicine
ANA MARCELLA RIVAS MEJIA, MD, CCD
American Board of Internal Medicine
American Board of Endocrinology
JACQUELINE L. COOK, FNP-BC, CDCES, CCD
KELLEY R. JENKINS, FNP-C, CDCES
ALINA CUMMINS, PA-C
STACY GHOLZ, FNP-C
SHELLEY L. CARTER, DNP
JESSICA A. CROUCH, FNP-C
Phone (417) 269-4450
960 E. Walnut Lawn, Suite 201 Springfield, MO 65807
Nephrology

SPRINGFIELD NEPHROLOGY ASSOCIATES, INC.
1911 South National, Suite 301 Spring eld, MO 65804
Phone 417-886-5000 • Fax 417-886-1100 www.spring eldnephrology.com
STEPHEN E. GARCIA, MD H
American Board of Internal Medicine
American Board of Nephrology
ETHAN T. HOERSCHGEN, MD
American Board of Internal Medicine
American Board of Nephrology
GISELLE D. KOHLER, MD H
American Board of Internal Medicine
American Board of Nephrology
DAVID L. SOMMERFIELD, MD
American Board of Internal Medicine
American Board of Nephrology
SUSAN A. WOODY, DO H
American Board of Internal Medicine
American Board of Nephrology
SPRINGFIELD
NEUROLOGICAL AND SPINE INSTITUTE
CoxHealth Jared Neuroscience
West Tower • 3801 S National, Ste 700 Spring eld, MO 65807 • 417-885-3888
Neurosurgery:
H. MARK CRABTREE, MD, FACS
EDWIN J. CUNNINGHAM, MD
MAYUR JAYARAO, MD
J. CHARLES MACE, MD, FACS H
CHAD J. MORGAN, MD
MICHAEL L. MUMERT, MD
SALIM RAHMAN, MD, FACS
ANGELA SPURGEON, DO
ROBERT STRANG, MD
Interventional Neuroradiology
MICHAEL J. WORKMAN, MD
Physiatry:
TED A. LENNARD, MD
KELLY OWN, MD
JESSE STOKKE, DO
Physician Assistants:
JOSHUA BARBIERI, PA-C
MARK BROWN, PA-C
ERIC CHAVEZ, PA-C
KEVIN STOKES, PA-C
HEATHER TACKETT, PA-C
Nurse Practitioner:
EMILY CROUSE, NP-C
MINDY GRANT, NP-C
ROZLYN MCTEER, FNP
BRANDON RUBLE, ACNP-AG
ALYSSA CHASTAIN, FNP
Obstetrics/Gynecology
COXHEALTH
PRIMROSE OB/GYN
MARCUS D. MCCORCLE, MD, FACOG
Diplomate, American Board of Obstetrics and Gynecology
THOMAS M. SHULTZ, MD, FACOG
Diplomate, American Board of Obstetrics and Gynecology
GREGORY S. STAMPS, MD, FACOG
Diplomate, American Board of Obstetrics and Gynecology
P. MICHAEL KIDDER, DO, FACOOG
Diplomate, American Osteopathic Board of Obstetrics & Gynecology
Phone 882-6900
1000 E. Primrose • Suite 270 Spring eld, MO 65807
SPRINGFIELD OB/GYN, LLC
MATTHEW H. TING, MD, FACOG H
American Board of Obstetrics & Gynecology
909 E. Montclair, Suite 120 Spring eld, MO 65807
Phone 417/882-4466 • Fax 417/890-5631
ONCOLOGYHEMATOLOGY
ASSOCIATES OF SPRINGFIELD, MD, P.C.
WILLIAM F. CUNNINGHAM, MD, FACP
American Board of Internal Medicine
American Board of Medical Oncology
JIANTAO DING, MD H
American Board of Internal Medicine
American Board of Hematology
American Board of Medical Oncology
ROBERT J. ELLIS, MD, FACP
American Board of Internal Medicine
American Board of Hematology
American Board of Medical Oncology
BROOKE GILLETT, DO
American Board of Internal Medicine
American Board of Medical Oncology
V. ROGER HOLDEN, MD, PhD
American Board of Hematology
American Board of Medical Oncology
DUSHYANT VERMA, MD, FACP
American Board of Internal Medicine
American Board of Hematology
American Board of Medical Oncology
Springfield Clinic 3850 S. National, Ste. 600 Spring eld, Missouri 65807
Monett Clinic 802 US Hwy 60 Monett, Missouri 65708
Phone 882-4880
Fax 882-7843
Visit our website: www.ohaclinic.com
MERCY CLINIC–EAR, NOSE & THROAT
BENJAMIN L. HODNETT, MD, PHD H
ERICH D. MERTENSMEYER, DO, FAOCOO
AARON R. MORRISON, MD
RAJEEV MASSON, MD
MARK J. VAN ESS, DO, FAOCOO
Diplomates, American Board of Otolaryngology
SHELBY BRITT, PA
MELISSA COONS, FNP
TAHRA LOCK, NP
ELIZABETH (BETSY) MULLINGS, FNP
PAUL STRECKER, FNP
Audiology
JASON BOX, AuD, CCC-A
MAMIE JAYCOX, AuD, CCC-A
JENNIFER PLOCH, AUD
ALLISON WHITE, AUD, CCC-A
Phone 417-820-5750 Fax 417-820-5066
1229 E. Seminole, Ste. 520 Spring eld, MO 65804
MERCY CLINIC–FACIAL PLASTIC SURGERY
MATTHEW A. KIENSTRA, MD, FACS
American Board of Facial Plastic & Reconstructive Surgery American Board of Otolaryngology
Phone 417-887-3223
1965 S. Fremont, Ste. 120 Spring eld, MO 65804 facialplasticsurgeon.com
JAMES E. BRIGHT, MD H Diplomate, American Board of Psychiatry & Neurology.
Practice Limited to: Adult Psychiatry
Phone 882-9002
1736 E. Sunshine, Ste. 400 Spring eld, MO 65804

At Arvest we understand how valuable your time is. Our Private Bankers proudly serve our local medical community with dedicated financial expertise. Let an experienced Private Banker coordinate your full financial picture, including your business needs. With specially tailored services, we’re here to take tasks o your plate & make every life stage easier.
Call us today to learn more.
CHANGE SERVICE REQUESTED