

A comprehensive guide to understanding your 2026 employee benefits program

A comprehensive guide to understanding your 2026 employee benefits program
Coverage
Medical Coverage Assured Benefits Administrators (ABA) 800-247-7114
Health Care Advocacy Trinity Care (TC)
$0 Surgery, Imaging, and Maternity Care Patient Navigator
Telemedicine Call-A-Doc
www.abadmin.com
423-TCG-CARE (423-824-2273) free@tcnavigator.com
423-TCG-CARE (423-824-2273) free@tcnavigator.com
844-362-2447 www.247calladoc.com
Dental Coverage Guardian 888-482-7342 www.guardianlife.com
Vision Coverage Guardian/Davis Vision 888-600-1600 www.guardianlife.com Life and AD&D Insurance
Long Term Disability
Accident Insurance
Critical Illness Insurance
888-482-7342 www.guardianlife.com
888-482-7342 www.guardianlife.com
888-482-7342 www.guardianlife.com
888-482-7342 www.guardianlife.com
Hospital Indemnity Insurance Guardian 888-482-7342 www.guardianlife.com
Employee Assistance Program ComPsych GuidanceResources 855-239-0743 www.guidanceresources.com
Human Resources Mary Norbury 817-370-3222 mnorbury@pandai.com

Employee benefits can be complicated. The Higginbotham Employee Response Center can assist you with the following: Enrollment support Benefits information Claims and billing questions Eligibility issues
Call or text 866-419-3518 . Email helpline@higginbotham.net Monday through Friday from 7:00 a.m. to 6:00 p.m. CT. Se habla español.
If you leave a voicemail message after 3:00 p.m. CT, your call will be returned the next business day. You can also email your questions or requests.
We are pleased to offer a full benefits package to you and your eligible dependents. Read this guide to know what benefits are available to you.
Our benefits program offers one or more medical plan options. To help you make an informed choice, review each plan’s Summary of Benefits and Coverage, available from Human Resources.
If you (and/or your dependents) have Medicare or will become eligible for Medicare in the next 12 months, federal law gives you more choices for your prescription drug coverage.
Who is Eligible
When to Enroll
When Coverage Starts
A regular, full-time employee working an average of 30 hours or more per week
By the deadline given by Human Resources
First of the month after completing 30 days of full-time employment
A regular, full-time employee working an average of 30 hours or more per week
During OE or for a QLE
OE: Start of the plan year
OE: Open Enrollment
QLE: Qualifying Life Event
Your legal spouse
Children under age 26 regardless of student, dependency, or marital status
Children age 26 or older who are fully dependent on you for support due to a mental or physical disability and who are indicated as such on your federal tax return
During OE or for a QLE
When covering dependents, you must enroll for and be on the same plans
QLE: Ask Human Resources Ask Human Resources
You may only enroll for or make changes to coverage during the plan year if you are a new hire or if you have a QLE, such as:




FMLA, COBRA event, judgment, or decree
Becoming eligible for Medicare, Medicaid, or TRICARE
Receiving a Qualified Medical Child Support Order
You have 30 days from the event to notify Human Resources and complete your changes You may need to provide documents to verify the change.
Gain or loss of benefits coverage
Change in employment status affecting benefits
Significant change in cost of spouse’s coverage
Enrolling in benefits is simple through BenefitsInHand.
Go to www.benefitsinhand.com
1. Click the New User Registration link. Once you register, you will use your username and password to log in.
2. Enter your personal information and company identifier of P&AI and click Next
3. Create a username (work email address recommended) and password, then check the I agree to terms and conditions box before you click Finish
4. If you used an email address as your username, you will receive a validation email to that address. You may now log in.
Go to www.benefitsinhand.com
1. Click the Start Enrollment button to begin.
2. Confirm or update your personal information and click Save & Continue
3. Edit or add dependents who need to be covered on your benefits. Once all dependents are listed, click Save & Continue
4. Follow the steps on the screen for each benefit to select or decline coverage. To decline coverage, click Don’t want this benefit? and select the reason for declining.
5. When you finish making your benefit elections, review each of them. If correct, click the Click to Sign button to complete and submit your enrollment elections.

Call or text a bilingual representative at 866-419-3518 Monday through Friday from 7:00 a.m. to 6:00 p.m. CT. If you leave a message after 3:00 p.m. CT, your call or text will be returned the next business day. Email questions or requests to helpline@higginbotham.net
The medical plan we offer works a little differently than you may be used to with a traditional medical plan.
The medical plan we currently offer is a self-funded plan. This means our company pays for all our employee medical claims – not the insurance carrier. So, whom you call for support and how you obtain care are slightly different. Our medical plan is designed to provide the highest level of care from board-certified providers, and to save you time and money.
Pritchard & Abbott, Inc. hired ABA as a third-party administrator (TPA) to manage our medical plan. This means you will go to ABA for everything related to your medical plan, including:
Claims questions
Benefits questions and assistance
In-network provider lookup
Even though a big insurance carrier logo may be on your medical ID card, always call our TPA with benefits-related questions.
Our medical plan also offers additional programs and services that help limit your out-of-pocket costs and provide ongoing support for health care and prescription needs.
Be sure that your doctors have your current medical ID card so they bill correctly!
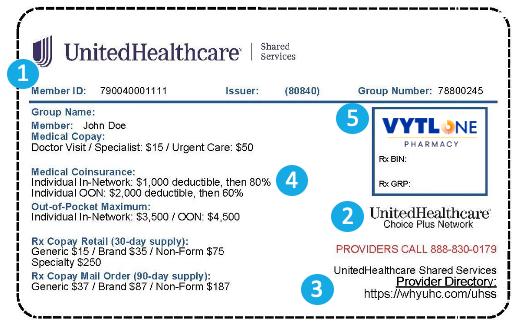
Our TPA does not have its own network of doctors, so it “rents” the provider network we use. That’s why UnitedHealthcare (UHC) appears on your medical ID card. The doctor will recognize and bill UHC, but UHC will always send the bill to our TPA. Always call our TPA – not the medical carrier – if you have a claims or billing issue. If you try to call UHC’s representatives to help you, they will not be able to do so because you will not be in their system as a member of their plan. You are a member of the ABA plan, which “rents” UHC’s provider network.
Administrator: ABA | Network: UHC Choice Plus
Our medical plan protects you and your family from major financial hardship in the event of illness or injury. The Medical Plan ABA 1000 plan is a PPO.
A Preferred Provider Organization (PPO) plan allows you to see any provider when you need care. When you see innetwork providers, you will pay less and get the highest level of benefits. You will pay more for care if you use out-of-network providers. When you see in-network providers, your office visits, urgent care visits, and prescription drugs are covered with a copay, and most other services are covered at the deductible and coinsurance level.
Prescription Drugs – Mail Order Up to 90-day supply
Generic
Preferred brand name
Non-preferred brand name
Specialty

$0 Surgery, Imaging and Maternity Care
ABA administers all of our medical benefits and claims. You have access to UnitedHealthcare’s network of providers.
ABA Member Website and Customer Service Number
Visit www.abadmin.com or call 800-247-7114
Review claims and Explanation of Benefits (EOB) statements
Check your eligibility statements
Review deductibles, out-ofpocket maximums, copays, and coinsurance statements
Access ID cards
Download important documents
Update member information
Download the TC Navigator App
Chat with a care guide to:
Save time and money on services
Get a referral
Schedule an appointment
Answer your benefits questions
Get on-demand virtual care
See all your benefits information
Get digital ID cards
View and download documents

Scan the code to download the TC Navigator app.
Need one of the following treatments or procedures? Call ahead and get it at NO COST. A Trinity Care patient navigator will help you find a provider, set up appointments, and take care of all billing and claims.
Surgery
Imaging
Colonoscopy
Upper endoscopy test
Physical therapy
Durable medical equipment
Specialty medication
Maternity program (free diapers and wipes!)
Mammogram
Call 423-824-2273 or email free@tcnavigator.com to learn more or get started.
Schedule a virtual care visit for FREE – right from the app!
You will be issued a new ID card. Here is some important information you need to know regarding your plan:
Our Third-Party Administrator (TPA) is Assured Benefits Administrators
The TPA processes and pays your claims. Payor ID: 39026
We utilize the UnitedHealthcare Choice Plus Network

Find a doctor at https://www.uhc.com/find-a-doctor (always call providers to confirm they are in-network).
Our Pharmacy Benefits Manager (PBM) is VytlOne (formerly known as Maxor).
Information to submit claims by mail and electronically.
Provider contact for eligibility, benefits, and pre-authorizations.
Member services for eligibility, benefits, claims, and more.
Telemedicine for phone and video consultations with a physician.
For free surgeries, imaging, and other services, contact:
Call 423-TCG-CARE (423-824-2273).
Email free@tcnavigator.com
Your member information and group identifier.
Provider network (not for eligibility and benefits verification, this is NOT the carrier).
Website for provider search.
Your specific plan benefits.
Pharmacy Benefit Manager (PBM) information to process prescription claims.
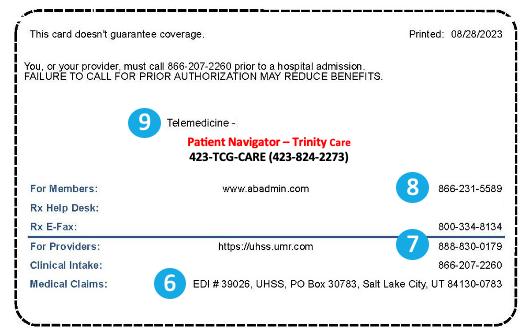
Verification of eligibility and benefits, preauthorizations, and customer service:
Call 800-247-7114 Email customerservice@abadmin.com
Your Medical Mobile App

Whether you are trying to understand your medical coverage, seeking care, or managing expenses, the TC Navigator app is your personal all-in-one solution.

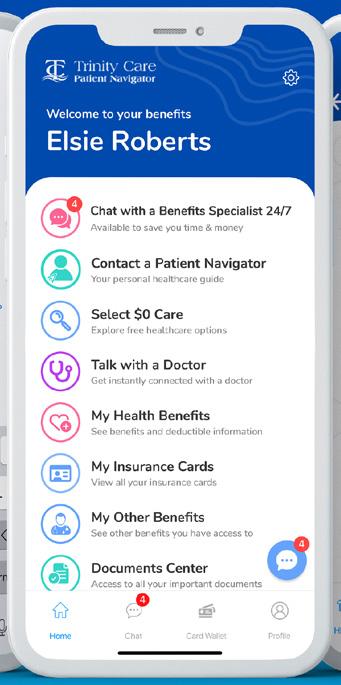
Find a doctor or clinic.
Get FREE on-demand telemedicine.
See all your benefits information.
Get digital ID cards.
View and download documents.
Use the TC Navigator app to chat by text with a care guide to get expert benefits advice and help finding the best care at the best price.
Save time and money on services.
Get a referral.
Schedule an appointment.
Answer your benefits questions.

Download Today!
Scan the code to download the TC Navigator app.
If you are enrolled in the medical plan, you have access to our concierge service, Trinity Care Patent Navigator. When you call 423-TCG-CARE (423-824-2273) ahead of time, you can get free surgery, imaging, and maternity care – plus, your navigator will take care of all the details for you. Call or email free@tcnavigator.com for more information.
With Patient Navigator, you can access no-cost, highquality surgeries through direct contracts with over 4,000 surgical centers nationwide.
No Deductible
No Coinsurance
$1,000 Incentive
Paid Travel and Hotel
$100 Per Diem
Call Patient Navigator to confirm your procedure is eligible. Your dedicated navigator will guide you through every step of the process.
Get your imaging done easily and at no cost through Patient Navigator when you follow these simple steps:
Step 1 – Call: Contact Patient Navigator before obtaining any imaging services.
Step 2 – Choose: Select your preferred location (home or work area), time of day (AM or PM), and part of the week that works best for you.
Step 3 – Schedule: Your Patient Navigator will handle the scheduling for you.
Step 4 – Attend: Simply show up—no medical ID card or payments needed.
Step 5 – Done! Your physician will receive all imaging and reports directly.
NOTE: To qualify for 100% coverage, you must contact Patient Navigator before any imaging services are performed and follow the outlined process.
423-TCG-CARE (423-824-2273)
MRIs (open and closed)
CT Scans
PET Scans
Ultrasounds
Mammograms
X-rays
Bone Density (DXA)
Nuclear Medicine
Arthrogram
Echocardiogram
Ouma Health, in partnership with Trinity Care Navigation, offers total maternity telehealth — a no-cost benefit for you and your spouse. Ouma connects you 24/7 with world-class pregnancy experts to support you from planning through postpartum. Your Care Team includes:
Maternal-Fetal Medicine Physicians: High-risk pregnancy specialists.
Behavioral Health Experts: Support for emotional well-being and postpartum care.
Lactation Consultants: Live, personalized breastfeeding guidance.
As a special bonus, receive free diapers and wipes for one year after your baby is born.
Enroll by your 14th week of pregnancy (unless otherwise approved) at www.oumahealth.com/partners/trinity
Your medical coverage includes prescription benefits for retail, mail order (home delivery), and specialty drugs.
Pharmacy Benefits Manager:
Your pharmacy benefits manager (PMB) controls prescription drug costs by negotiating discounts on medications. Covered drugs are listed in the Prescription Drug List. If you take maintenance medications, review the list with your doctor to see which ones are covered and available. If your medication is not listed, call the phone number on your member ID card.
Use any participating retail pharmacy to fill short-term, non-specialty medications. Retail pharmacies often fill or refill 30- to 90-day supplies.
If you take medication on a daily basis, consider using home delivery. It is a convenient, low-cost option that delivers up to a 90-day supply right to your home. You will need to set up an online pharmacy account and/or download the app to easily manage your prescriptions.
If you need a specialty drug to treat a complex or chronic condition, you will be asked to enroll in a specialty drug program. It offers support to ensure the medication works well for you and costs as little as possible. If you do not enroll in the program, the specialty drug may not be covered. Certain exclusions and limitations apply.
If you need a high-cost medication, call Patient Navigator first at 423-824-2273 to see if they can offer it for free.
Your new ID cards will show VytlOne for pharmacy.

Generic drugs are a safe and effective option to brand-name drugs – and they cost much less! They have the same active ingredients, strength, and dosage as brand-name drugs, and they also meet the same rigorous quality and safety standards set by the Food and Drug Administration.
Preventive care is the care you receive to help prevent chronic illness or disease. It includes exams, lab work, screenings, immunizations, and counseling to prevent health problems, such as diabetes or heart disease.
Cholesterol screening
Blood pressure screening
Colorectal cancer screening
Lung cancer screening
Hepatitis B screening
Well visits
Bone density screening
Obesity screening
Diabetes type 2 screening
Depression screening
Mammograms
Cervical cancer screening
Immunizations
Dental cleanings and exams
Vision screening
Physical exam
Blood tests for iron and cholesterol
Anxiety screening
Growth screening
Hearing screening
Hepatitis B screening
Depression screening
Alcohol, tobacco, and drug use assessments
Tuberculosis screening Immunizations
Dental cleanings and exams
Vision screening
Why should I get preventive care?
Preventive care is the fastest and best way to uncover potential risks and avoid chronic health conditions.
Are all screenings, tests, and procedures covered under preventive care?
No. Your doctor will be able to advise you as to the preventive care you need or should obtain, based on your medical and family history.
did
Autism screening
Blood screening
Depression screening
Developmental screening
Hearing screening
Obesity screening and counseling
Hypothyroidism screening
Behavioral assessments
Well visits
Immunizations
Dental cleanings and exams
Oral health risk assessment
Vision screening
Diagnosis codes on the doctor’s bill must meet certain insurance company conditions for them to be processed as preventive and covered at 100%. If you have a medical complaint, or your doctor finds a specific medical issue during your preventive care doctor’s visit, a diagnosis code for that issue or complaint will be on your bill. As a result, the insurance company may process the bill for a specific medical condition, not preventive care. In this case, you must pay the copay or portion of your deductible.
Your medical coverage offers telemedicine services so you can connect anytime day or night with a board-certified doctor via your mobile device or computer.
Carrier:
Call-A-Doc (medical) and Trinity Captive Group (mental health)
While telemedicine does not replace your primary care physician, it is a convenient and cost-effective option when you need care and:
Have a non-emergency issue and are considering an after-hours health care clinic, urgent care clinic, or emergency room for treatment
Are on a business trip, vacation, or away from home
Are unable to see your primary care physician
Use telemedicine for minor conditions such as:
Sore throat
Headache
Stomachache
Cold/flu
Allergies
Dermatology
Primary care
Fever
Urinary tract infections
Do not use telemedicine for serious or life-threatening emergencies.
Your telemedicine with Trinity Captive Group via the TC Navigator app gives you access to providers nationwide who can provide counseling and medication for depression, anxiety, substance abuse, serious conditions, and specialized care for children and adolescents.

Becoming familiar with your options for medical care can save you time and money.
Non-Emergency Care
Access to care via phone, online video, or mobile app whether you are home, work, or traveling; medications can be prescribed.
24 hours a day, 7 days a week
Generally, the best place for routine preventive care; established relationship; able to treat based on medical history.
Office hours vary Infections
Sore and strep throat Vaccinations
Minor injuries/sprains/strains
Usually lower out-of-pocket cost than urgent care; when you can’t see your doctor; located in stores and pharmacies.
Hours vary based on store hours Common infections Minor
When you need immediate attention; walk-in basis is usually accepted.
Generally includes evening, weekend, and holiday hours
HOSPITAL ER
Life-threatening or critical conditions; trauma treatment; multiple bills for doctor and facility.
24 hours a day, 7 days a week
Services do not include trauma care; can look similar to an urgent care center, but medical bills may be 10 times higher
24 hours a day, 7 days a week
Sprains and strains
Minor broken bones
Small cuts that may require stitches Minor burns and infections
Chest pain
Difficulty breathing
Severe bleeding
Blurred or sudden loss of vision
Major broken bones
Most major injuries except trauma Severe pain
Pritchard & Abbott is pleased to offer Low and High dental PPO plans. You will always get the highest level of benefits when you see in-network providers for your care. Out-of-network care is not based on negotiated fees, so you may be responsible for paying more for your care.
If you enroll in a dental plan, you will automatically be enrolled in the Guardian Maximum Rollover Program This program rewards you for going to the dentist regularly to prevent or detect the early signs of serious diseases. If you submit a claim (without exceeding the paid claims threshold of a benefit year), Guardian will roll over part of your unused annual maximum into a Maximum Rollover Account (MRA). This can be used in future years if your plan’s annual maximum is reached. View your MRA statement at www.guardiananytime.com or call 800-541-7846
Helps detect certain medical issues, prolong your eyesight, and correct vision or eye problems.
Regular exams can detect certain medical issues such as diabetes and high cholesterol, in addition to vision and eye problems. You may seek care from any vision provider, but the plan will pay the highest level of benefits when you see in-network providers.
Single vision
Lined bifocals
Lined trifocals
Exam
Lenses
Frames
Enjoy significant out-of-pocket savings with your Full Feature plan by visiting any Davis Vision network location, including popular retail centers like Costco, Walmart, JCPenney, Target, Sam’s Club, Pearle, Visionworks, and Warby Parker
You can also use your in-network benefits online at www.visionworks.com, www.glasses.com, www.warbyparker.com, or www.1800contacts.com
Once every 12 months
Once every 24 months
Once every 12 months
Contacts Once every 12 months
Life and Accidental Death and Dismemberment (AD&D) insurance are important to your financial security, especially if others depend on you for support or vice versa.
If you need more coverage than Basic Life and AD&D, you may buy Voluntary Life and AD&D for yourself and your dependent(s). If you do not elect Voluntary Life and AD&D insurance when first eligible, or if you want to increase your benefit amount at a later date, you may need to show proof of good health. You must elect Voluntary Life and AD&D coverage for yourself before covering your spouse and/or child(ren).
With Life insurance, you or your beneficiary(ies) can use the coverage to pay off debts such as credit cards, loans, and bills. AD&D coverage provides specific benefits if an accident causes bodily harm or loss (e.g., the loss of a hand, foot, or eye). If death occurs from an accident, 100% of the AD&D benefit would be paid to you or your beneficiary(ies). Life and AD&D coverage amounts reduce by 35% at age 65, by 60% at age 70, by 70% at age 75, and by 80% at age 80.
Basic Life and AD&D insurance are provided at no cost to you. You are automatically covered at 2 times your salary up to a maximum of $500,000 for each benefit.
A beneficiary is the person or entity you elect to receive the death benefits of your Life and AD&D insurance policies. You can name more than one beneficiary, and you can change beneficiaries anytime. If you name more than one beneficiary, you must identify how much each beneficiary will receive (e.g., 50% or 25%).
Child(ren)
Increments of $5,000 up to $100,000 not to exceed 50% of employee amount
Birth to 14 days – $100
14 days to age 26 – increments of $1,000 up to $10,000 not to exceed 100% of employee amount
Disability insurance provides partial income protection if you are unable to work due to a covered accident or illness. We offer Long Term Disability (LTD) for you to purchase.
LTD insurance pays a percentage of your monthly salary for a covered disability or injury that prevents you from working for a specific period of time. Benefits begin at the end of an elimination period and continue while you are disabled up to the maximum benefit period.
1 SSNRA: Social Security Normal Retirement Age
2 Benefits may not be paid for any condition treated within three months prior to your effective date until you have been covered under this plan for 12 months.

There are a few situations where you need to answer health questions, enroll for higher amounts of coverage, or request coverage after the initial eligibility period. In all these situations, Guardian’s online Evidence of Insurability (EOI) form keeps things simple.
Electronic EOI can be used for:
Basic Life
Voluntary Life
Voluntary Long Term Disability
1. You will receive a letter or email from your employer or Guardian with instructions and a unique link to submit your EOI form online.
2. First register and create an account at www.guardianlife.com
3. Then simply fill out the form, electronically sign it, and click Submit.
4. Once Guardian receives the form, they will contact you with any questions, before notifying you (and your employer) if the coverage amount changes.
See BenefitsInHand for rates.
Accident insurance provides affordable protection against a sudden, unforeseen accident.
Critical Illness insurance helps pay the cost of non-medical expenses related to a covered critical illness or cancer.
Accident insurance helps offset the direct and indirect expenses such as copayments, deductibles, ambulance, physical therapy, childcare, rent, and other costs not covered by traditional health plans. You will be paid a specific sum of money directly based on the care and services provided for your covered accident. Use the money any way you see fit. See the plan document for full details.
The plan provides a lump sum benefit payment to you upon first and second diagnosis of any covered critical illness or cancer. The benefit can help cover expenses such as lost income, out-of-town treatments, special diets, daily living, and household upkeep costs. See the plan document for full details.
Specific Sum Injuries
Concussions, dislocations, eye injuries, fractures, lacerations, ruptured discs, and more Schedule – varies by
For childhood conditions such as cleft lip or palate, cystic fibrosis, Down syndrome, spina bifida, and more
for rates.
Hospital Indemnity insurance helps you with the high cost of medical care by paying you a cash benefit when you have an inpatient hospital stay or are admitted to an intensive care unit.

You decide how to use the cash, whether it’s to pay for bills, gas, childcare or eldercare, medication, or other out-of-pocket expenses. See the plan document for full details.
Rates
BenefitsInHand for rates.
The Employee Assistance Program helps you and family members cope with a variety of personal and work-related issues.
Administrator:
ComPsych GuidanceResources
This program provides confidential counseling and support services at little or no cost to you to help with:
Relationships
Work-life balance
Stress and anxiety
Will preparation and estate resolution
Grief and loss
Childcare and eldercare issues
Substance abuse
Financial and legal matters
And more

Contact FEDlogic to talk to an advisor and get personalized help understanding and navigating complex federal and state benefit programs like Social Security, Medicare, Medicaid, and disability benefits. Whether you are planning for retirement, have a disability question, or need help coordinating public benefits, FEDlogic provides expert, one-onone guidance to support you and your family.
Visit www.fedlogicgroup.com
Call 877-837-4196.
Email services@fedlogicgroup.com
In October 1998, Congress enacted the Women’s Health and Cancer Rights Act of 1998. This notice explains some important provisions of the Act. Please review this information carefully.
As specified in the Women’s Health and Cancer Rights Act, a plan participant or beneficiary who elects breast reconstruction in connection with a mastectomy is also entitled to the following benefits:
All stages of reconstruction of the breast on which the mastectomy was performed;
Surgery and reconstruction of the other breast to produce a symmetrical appearance; and
Prostheses and treatment of physical complications of the mastectomy, including lymphedema.
Health plans must determine the manner of coverage in consultation with the attending physician and the patient. Coverage for breast reconstruction and related services may be subject to deductibles and coinsurance amounts that are consistent with those that apply to other benefits under the plan.
This notice is being provided to ensure that you understand your right to apply for group health insurance coverage. You should read this notice even if you plan to waive coverage at this time.
Loss of Other Coverage or Becoming Eligible for Medicaid or a state Children’s Health Insurance Program (CHIP)
If you are declining coverage for yourself or your dependents because of other health insurance or group health plan coverage, you may be able to later enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage (or if the employer stops contributing toward your or your dependents’ other coverage). However, you must enroll within 31 days after your or your dependents’ other coverage ends (or after the employer that sponsors that coverage stops contributing toward the other coverage).
If you or your dependents lose eligibility under a Medicaid plan or CHIP, or if you or your dependents become eligible for a subsidy under Medicaid or CHIP, you may be able to enroll yourself and your dependents in this plan. You must provide notification within 60 days after you or your dependent is terminated from, or determined to be eligible for, such assistance.
If you have a new dependent as a result of a marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your dependents. However, you must enroll within 31 days after the marriage, birth, or placement for adoption.
For More Information or Assistance
To request special enrollment or obtain more information, contact:
Pritchard & Abbott, Inc.
4900 Overton Commons Court Fort Worth, TX 76132
817-370-3216
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug coverage with Pritchard & Abbott, Inc. and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to enroll in a Medicare drug plan. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice.
If neither you nor any of your covered dependents are eligible for or have Medicare, this notice does not apply to you or the dependents, as the case may be. However, you should still keep a copy of this notice in the event you or a dependent should qualify for coverage under Medicare in the future. Please note, however, that later notices might supersede this notice.
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this coverage through a Medicare Prescription Drug Plan or a Medicare Advantage Plan that offers prescription drug coverage. All Medicare prescription drug plans provide at least a standard level of coverage set by Medicare. Some plans may also offer more coverage for a higher monthly premium.
2. Pritchard & Abbott, Inc. has determined that the prescription drug coverage offered by the Pritchard & Abbott, Inc. medical plan is, on average for all plan participants, expected to pay out as much as the standard Medicare prescription drug coverage pays and is considered Creditable Coverage. The HSA plan is not considered Creditable Coverage.
Because your existing coverage is, on average, at least as good as standard Medicare prescription drug coverage, you can keep this coverage and not pay a higher premium (a penalty) if you later decide to enroll in a Medicare prescription drug plan, as long as you later enroll within specific time periods. You can enroll in a Medicare prescription drug plan when you first become eligible for Medicare. If you decide to wait to enroll in a Medicare prescription drug plan, you may enroll later, during Medicare Part D’s annual enrollment period, which runs each year from October 15 through December 7 but as a general rule, if you delay your enrollment in Medicare Part D after first becoming eligible to enroll, you may have to pay a higher premium (a penalty).
You should compare your current coverage, including which drugs are covered at what cost, with the coverage and cost of the plans offering Medicare prescription drug coverage in your area. See the Plan’s summary plan description for a summary of the Plan’s prescription drug coverage. If you don’t have a copy, you can get one by contacting Pritchard & Abbott, Inc. at the phone number or address listed at the end of this section.
If you choose to enroll in a Medicare prescription drug plan and cancel your current Pritchard & Abbott, Inc. prescription drug coverage, be aware that you and your dependents may not be able to get this coverage back. To regain coverage, you would have to re-enroll in the Plan, pursuant to the Plan’s eligibility and enrollment rules. You should review the Plan’s summary plan description to determine if and when you are allowed to add coverage.
If you cancel or lose your current coverage and do not have prescription drug coverage for 63 days or longer prior to enrolling in the Medicare prescription drug coverage, your monthly premium will be at least 1% per month greater for every month that you did not have coverage for as long as you have Medicare prescription drug coverage. For example, if nineteen months lapse without coverage, your premium will always be at least 19% higher than it would have been without the lapse in coverage.
For more information about this notice or your current prescription drug coverage: Contact the Human Resources Department at 817-370-3216.
NOTE: You will receive this notice annually and at other times in the future, such as before the next period you can enroll in Medicare prescription drug coverage and if this coverage changes. You may also request a copy.
For more information about your options under Medicare prescription drug coverage:
More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You will get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare prescription drug plans. For more information about Medicare prescription drug coverage:
Visit www.medicare.gov
Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare & You” handbook for their telephone number) for personalized help.
Call 1-800-MEDICARE (1-800-633-4227)
TTY users should call 877-486-2048
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. Information about this extra help is available from the Social Security Administration (SSA) online at www. socialsecurity.gov, or you can call them at 800-772-1213. TTY users should call 800325-0778
Remember: Keep this Creditable Coverage notice. If you enroll in one of the new plans approved by Medicare which offer prescription drug coverage, you may be required to provide a copy of this notice when you join to show whether or not you have maintained creditable coverage and whether or not you are required to pay a higher premium (a penalty).
January 1, 2026
Pritchard & Abbott, Inc. 4900 Overton Commons Court Fort Worth, TX 76132 817-370-3216
THIS NOTICE OF PRIVACY PRACTICES DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
This Notice of Privacy Practices (the “Notice”) describes the legal obligations of Pritchard & Abbott, Inc’s Group Health Plan (the “Plan”) and your legal rights regarding your protected health information held by the Plan under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the Health Information Technology for Economic and Clinical Health Act (HITECH Act). Among other things, this Notice describes how your protected health information may be used or
disclosed to carry out treatment, payment, or health care operations, or for any other purposes that are permitted or required by law.
We are required to provide this Notice of Privacy Practices to you pursuant to HIPAA.
The HIPAA Privacy Rule protects only certain medical information known as “protected health information.” Generally, protected health information (PHI) is health information, including demographic information, collected from you or created or received by a health care provider, a health care clearinghouse, a health plan, or your employer on behalf of a group health plan, from which it is possible to individually identify you and that relates to:
1. Your past, present, or future physical or mental health or condition;
2. The provision of health care to you; or
3. The past, present, or future payment for the provision of health care to you.
I. Contact Information
If you have any questions about this Notice or about our privacy practices, and for any correspondence or requests related to the contents of this Notice, please contact: Pritchard & Abbott, Inc. 4900 Overton Commons Court Fort Worth, TX 76132 817-370-3216
II. Effective Date
This Notice is effective February 15, 2026.
III. Our Responsibilities
We are required by law to:
1. maintain the privacy of your PHI;
2. provide you with certain rights with respect to your PHI;
3. provide you with a copy of this Notice of our legal duties and privacy practices with respect to your PHI; and
4. follow the terms of the Notice that is currently in effect.
We reserve the right to change the terms of this Notice and to make new provisions regarding your PHI that we maintain, as allowed or required by law. If we make any material change to this Notice, we will provide you with a copy of our revised Notice of Privacy Practices.
IV. How We May Use and Disclose Your PHI
Under the law, we may use or disclose your PHI under certain circumstances without your permission. The following categories describe the different ways that we may use and disclose your PHI. For each category of uses or disclosures we will explain what we mean and present some examples. Not every
use or disclosure in a category will be listed. However, all of the ways we are permitted to use and disclose information will fall within one of the categories. Note that we will use and disclose PHI as described below unless otherwise prohibited or restricted by applicable state or other law, and that information can lose its protected status as PHI once re-disclosed by a recipient.
For Treatment. When and as appropriate, we may use or disclose medical information about you to facilitate medical treatment or services by health care providers. We may disclose medical information about you to providers, including doctors, nurses, technicians, medical students, or other hospital personnel who are involved in taking care of you. For example, we might disclose information about you with physicians who are treating you.
For Payment. We may use or disclose your protected health information to determine your eligibility for Plan benefits, to facilitate payment for the treatment and services you receive from health care providers, to determine benefit responsibility under the Plan, or to coordinate Plan coverage. For example, we may tell your health care provider about your medical history to determine whether a particular treatment is experimental, investigational, or medically necessary, or to determine whether the Plan will cover the treatment. We may also share your protected health information with a utilization review or pre-certification service provider. Likewise, we may share your protected health information with another entity to assist with the adjudication or subrogation of health claims or to another health plan to coordinate benefit payments.
For Health Care Operations. We may use and disclose your protected health information for other Plan operations. These uses and disclosures are necessary to run the Plan. For example, we may use medical information in connection with conducting quality assessment and improvement activities; underwriting, premium rating, and other activities relating to Plan coverage; submitting claims for stop-loss (or excess-loss) coverage; conducting or arranging for medical review, legal services, audit services, and fraud and abuse detection programs; business planning and development such as cost management; and business management and general Plan administrative activities. However, we will not use your genetic information for underwriting purposes.
Substance Use Disorder (SUD) Treatment Information. Some of your health information may be part of a SUD patient record and
subject to additional protections under federal law (42 CFR Part 2) governing confidentiality of SUD patient records.
If we receive or maintain any information about you from a SUD treatment program that is covered by 42 CFR Part 2 (a “Part 2 Program”) through a general consent you provide to the Part 2 Program to use and disclose the SUD patient record for purposes of treatment, payment or health care operations, we may use and disclose your SUD patient record for treatment, payment and health care operations purposes as described in this Notice. If we receive or maintain your SUD patient record through specific consent you provide to us or another third party, we will use and disclose your SUD patient record only as expressly permitted by you in your consent as provided to us. In no event will we use or disclose your SUD patient record, or testimony that describes the information contained in your SUD patient record, in any civil, criminal, administrative, or legislative proceedings by any Federal, State, or local authority, against you, unless authorized by your consent or the order of a court after it provides you notice of the court order.
To Business Associates. We may contract with individuals or entities known as Business Associates to perform various functions on our behalf or to provide certain types of services. In order to perform these functions or to provide these services, Business Associates will receive, create, maintain, transmit, use, and/or disclose your PHI, but only after they agree in writing with us to implement appropriate safeguards regarding your PHI. For example, we may disclose your PHI to a Business Associate to process your claims for Plan benefits or to provide support services, such as utilization management, pharmacy benefit management, or subrogation, but only after the Business Associate enters into a Business Associate contract with us.
Treatment Alternatives or Health-Related Benefits and Services. We may use and disclose your protected health information to send you information about treatment alternatives or other health-related benefits and services that might be of interest to you.
As Required by Law. We will disclose your PHI when required to do so by federal, state, or local law. For example, we may disclose your PHI when required by national security laws or public health disclosure laws.
To Avert a Serious Threat to Health or Safety. We may use and disclose your PHI when necessary to prevent a serious threat to your health and safety, or the health and safety of the public or another person. Any disclosure, however, would only be to someone able to help prevent the threat. For example, we may disclose your PHI in a proceeding regarding the licensure of a physician.
To Plan Sponsors. For the purpose of administering the plan, we may disclose PHI to certain employees of the Employer. However, those employees will only use or disclose that information as necessary to perform plan administration functions or as otherwise required by HIPAA, unless you have authorized further disclosures. Your PHI cannot be used for employment purposes without your specific authorization.
In addition to the above, the following categories describe other possible ways that we may use and disclose your PHI without your specific authorization. For each category of uses or disclosures, we will explain what we mean and present some examples. Not every use or disclosure in a category will be listed. However, all of the ways we are permitted to use and disclose information will fall within one of the categories.
Organ and Tissue Donation. If you are an organ donor, we may release your PHI after your death to organizations that handle organ procurement or organ, eye, or tissue transplantation or to an organ donation bank, as necessary to facilitate organ or tissue donation and transplantation.
Military. If you are a member of the armed forces, we may release your PHI as required by military command authorities. We may also release PHI about foreign military personnel to the appropriate foreign military authority.
Workers’ Compensation. We may release your PHI for workers’ compensation or similar programs, but only as authorized by, and to the extent necessary to comply with, laws relating to workers’ compensation and similar programs that provide benefits for workrelated injuries or illness.
Public Health Risks. We may disclose your PHI for public health activities. These activities generally include the following:
1. to prevent or control disease, injury, or disability;
2. to report births and deaths;
3. to report child abuse or neglect;
4. to report reactions to medications or problems with products;
5. to notify people of recalls of products they may be using;
6. to notify a person who may have been exposed to a disease or may be at risk for contracting or spreading a disease or condition;
7. to notify the appropriate government authority if we believe that a patient has been the victim of abuse, neglect, or domestic violence. We will only make this disclosure if you agree, or when required or authorized by law.
Health Oversight Activities. We may disclose your PHI to a health oversight agency for activities authorized by law. These oversight activities include, for example, audits, investigations, inspections, and licensure. These activities are necessary for the government to monitor the health care system, government programs, and compliance with civil rights laws.
Lawsuits and Disputes. If you are involved in a lawsuit or a dispute, we may disclose your PHI in response to a court or administrative order. We may also disclose your PHI in response to a subpoena, discovery request, or other lawful process by someone involved in a legal dispute, but only if efforts have been made to tell you about the request or to obtain a court or administrative order protecting the information requested.
Law Enforcement. We may disclose your PHI if asked to do so by a law-enforcement official.
1. in response to a court order, subpoena, warrant, summons, or similar process;
2. to identify or locate a suspect, fugitive, material witness, or missing person;
3. about the victim of a crime if, under certain limited circumstances, we are unable to obtain the victim’s agreement;
4. about a death that we believe may be the result of criminal conduct; and
5. about criminal conduct.
Coroners, Medical Examiners, and Funeral Directors. We may release PHI to a coroner or medical examiner. This may be necessary, for example, to identify a deceased person or determine the cause of death. We may also release medical information about patients to funeral directors, as necessary to carry out their duties.
National Security and Intelligence Activities. We may release your PHI to authorized federal officials for intelligence, counterintelligence, and other national security activities authorized by law.
Inmates. If you are an inmate of a correctional institution or are in the custody of a lawenforcement official, we may disclose your PHI to the correctional institution or law-
enforcement official if necessary (1) for the institution to provide you with health care; (2) to protect your health and safety or the health and safety of others; or (3) for the safety and security of the correctional institution.
Research. We may disclose your PHI to researchers when:
1. The individual identifiers have been removed; or
2. When an institutional review board or privacy board has reviewed the research proposal and established protocols to ensure the privacy of the requested information and approves the research.
VI. Required Disclosures
The following is a description of disclosures of your PHI we are required to make.
Government Audits. We are required to disclose your PHI to the Secretary of the United States Department of Health and Human Services when the Secretary is investigating or determining our compliance with the HIPAA privacy rule.
Disclosures to You. When you request, we are required to disclose to you the portion of your PHI that contains medical records, billing records, and any other records used to make decisions regarding your health care benefits. We are also required, when requested, to provide you with an accounting of most disclosures of your PHI if the disclosure was for reasons other than for payment, treatment, or health care operations, and if the PHI was not disclosed pursuant to your individual authorization.
VII. Other Disclosures
Personal Representatives. We will disclose your PHI to individuals authorized by you, or to an individual designated as your personal representative, attorney-in-fact, etc., so long as you provide us with a written notice/ authorization and any supporting documents (i.e., power of attorney). Note: Under the HIPAA privacy rule, we do not have to disclose information to a personal representative if we have a reasonable belief that:
1. You have been, or may be, subject to domestic violence, abuse, or neglect by such person; or
2. Treating such person as your personal representative could endanger you; and
3. In the exercise of professional judgment, it is not in your best interest to treat the person as your personal representative.
Spouses and Other Family Members. With only limited exceptions, we will send all mail to the employee. This includes mail relating to the employee’s spouse and other family members who are covered under the Plan and includes mail with information on the use of
Plan benefits by the employee’s spouse and other family members and information on the denial of any Plan benefits to the employee’s spouse and other family members. If a person covered under the Plan has requested Restrictions or Confidential Communications (see below under “Your Rights”), and if we have agreed to the request, we will send mail as provided by the request for Restrictions or Confidential Communications.
Authorizations. Other uses or disclosures of your PHI not described above will only be made with your written authorization. For example, in general and subject to specific conditions, we will not use or disclose your psychiatric notes; we will not use or disclose your PHI for marketing; and we will not sell your PHI, unless you give us a written authorization. You may revoke written authorizations at any time, so long as the revocation is in writing. Once we receive your written revocation, it will only be effective for future uses and disclosures. It will not be effective for any information that may have been used or disclosed in reliance upon the written authorization and prior to receiving your written revocation.
You have the following rights with respect to your PHI:
Right to Inspect and Copy. You have the right to inspect and copy certain PHI that may be used to make decisions about your Plan benefits. If the information you request is maintained electronically, and you request an electronic copy, we will provide a copy in the electronic form and format you request, if the information can be readily produced in that form and format; if the information cannot be readily produced in that form and format, we will work with you to come to an agreement on form and format. If we cannot agree on an electronic form and format, we will provide you with a paper copy.
To inspect and copy your PHI, you must submit your request in writing. If you request a copy of the information, we may charge a reasonable fee for the costs of copying, mailing, or other supplies associated with your request.
We may deny your request to inspect and copy in certain very limited circumstances. If you are denied access to your medical information, you may request that the denial be reviewed by submitting a written request.
Right to Amend. If you feel that the PHI we have about you is incorrect or incomplete, you may ask us to amend the information. You have the right to request an amendment for as long as the information is kept by or for the Plan.
To request an amendment, your request must be made in writing. In addition, you must provide a reason that supports your request.
We may deny your request for an amendment if it is not in writing or does not include a reason to support the request. In addition, we may deny your request if you ask us to amend information that:
1. is not part of the medical information kept by or for the Plan;
2. was not created by us, unless the person or entity that created the information is no longer available to make the amendment;
3. is not part of the information that you would be permitted to inspect and copy; or
4. is already accurate and complete.
If we deny your request, you have the right to file a statement of disagreement with us and any future disclosures of the disputed information will include your statement.
Right to an Accounting of Disclosures. You have the right to request an “accounting” of certain disclosures of your PHI. The accounting will not include (1) disclosures for purposes of treatment, payment, or health care operations; (2) disclosures made to you; (3) disclosures made pursuant to your authorization; (4) disclosures made to friends or family in your presence or because of an emergency; (5) disclosures for national security purposes; and (6) disclosures incidental to otherwise permissible disclosures.
To request this list or accounting of disclosures, you must submit your request in writing. Your request must state the time period you want the accounting to cover, which may not be longer than six years before the date of the request. Your request should indicate in what form you want the list (for example, paper or electronic). The first list you request within a 12-month period will be provided free of charge. For additional lists, we may charge you for the costs of providing the list. We will notify you of the cost involved and you may choose to withdraw or modify your request at that time before any costs are incurred.
You have the right to request a restriction or limitation on your PHI that we use or disclose for treatment, payment, or health care operations. You also have the right to request a limit on your PHI that we disclose to someone who is involved in your care or the payment for your care, such as a family member or friend. For example, you could ask that we not use or disclose information about a surgery that you had.
Except as provided in the next paragraph, we are not required to agree to your request. However, if we do agree to the request, we will honor the restriction until you revoke it or we notify you.
We will comply with any restriction request if (1) except as otherwise required by law, the disclosure is to a health plan for purposes of carrying out payment or health care operations (and is not for purposes of carrying out treatment); and (2) the PHI pertains solely to a health care item or service for which the health care provider involved has been paid in full by you or another person.
To request restrictions, you must make your request in writing. In your request, you must tell us (1) what information you want to limit; (2) whether you want to limit our use, disclosure, or both; and (3) to whom you want the limits to apply-for example, disclosures to your spouse.
Right to Request Confidential Communications. You have the right to request that we communicate with you about medical matters in a certain way or at a certain location. For example, you can ask that we only contact you at work or by mail.
To request confidential communications, you must make your request in writing. We will not ask you the reason for your request. Your request must specify how or where you wish to be contacted. We will accommodate all reasonable requests.
Right to Be Notified of a Breach. You have the right to be notified in the event that we (or a Business Associate) discover a breach of unsecured PHI.
Right to a Paper Copy of This Notice. You have the right to a paper copy of this notice. You may ask us to give you a copy of this notice at any time. Even if you have agreed to receive this notice electronically, you are still entitled to a paper copy of this notice.
If you believe that your privacy rights have been violated, you may file a complaint with the Plan or with the Office for Civil Rights of the United States Department of Health and Human Services. To file a complaint with the Plan, contact the person listed in the Contact Information section of this Notice. All complaints must be submitted in writing. You will not be penalized, or in any other way retaliated against, for filing a complaint with the Office for Civil Rights or with us
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow. gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employersponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa. dol.gov or call 1-866-444-EBSA (3272)
If you live in one of the following States, you may be eligible for assistance paying your employer health plan premiums. The following list of States is current as of July 31, 2025. Contact your State for more information on eligibility.
Alabama – Medicaid
Website: http://www.myalhipp.com/ Phone: 1-855-692-5447
Alaska – Medicaid
The AK Health Insurance Premium Payment Program Website: http://myakhipp.com/ Phone: 1-866-251-4861
Email: CustomerService@MyAKHIPP.com
Medicaid Eligibility: https://health.alaska. gov/dpa/Pages/default.aspx
Arkansas – Medicaid
Website: http://myarhipp.com/ Phone: 1-855-MyARHIPP (855-692-7447)
California– Medicaid
Health Insurance Premium Payment (HIPP) Program Website: http://dhcs.ca.gov/hipp Phone: 916-445-8322
Fax: 916-440-5676
Email: hipp@dhcs.ca.gov
Colorado – Health First Colorado (Colorado’s Medicaid Program) and Child Health Plan Plus (CHP+)
Health First Colorado website: https:// www.healthfirstcolorado.com/
Health First Colorado Member Contact Center: 1-800-221-3943/State Relay 711
CHP+: https://hcpf.colorado.gov/childhealth-plan-plus
CHP+ Customer Service: 1-800-359-1991/ State Relay 711
Health Insurance Buy-In Program (HIBI): https://www.mycohibi.com/ HIBI Customer Service: 1-855-692-6442
Florida – Medicaid
Website: https://www. flmedicaidtplrecovery.com/ flmedicaidtplrecovery.com/hipp/index.html Phone: 1-877-357-3268
Georgia – Medicaid
GA HIPP Website: https://medicaid.georgia. gov/health-insurance-premium-paymentprogram-hipp
Phone: 678-564-1162, Press 1
GA CHIPRA Website: https://medicaid. georgia.gov/programs/third-party-liability/ childrens-health-insurance-programreauthorization-act-2009-chipra
Phone: 678-564-1162, Press 2
Indiana – Medicaid
Health Insurance Premium Payment Program
All other Medicaid
Website: https://www.in.gov/medicaid/ http://www.in.gov/fssa/dfr/
Family and Social Services Administration
Phone: 1-800-403-0864
Member Services Phone: 1-800-457-4584
Iowa – Medicaid and CHIP (Hawki)
Medicaid Website: https://hhs.iowa.gov/ programs/welcome-iowa-medicaid
Medicaid Phone: 1-800-338-8366
Hawki Website: https://hhs.iowa.gov/ programs/welcome-iowa-medicaid/iowahealth-link/hawki
Hawki Phone: 1-800-257-8563
HIPP Website: https://hhs.iowa.gov/ programs/welcome-iowa-medicaid/feeservice/hipp
HIPP Phone: 1-888-346-9562
Kansas – Medicaid
Website: https://www.kancare.ks.gov/
Phone: 1-800-792-4884
HIPP Phone: 1-800-967-4660
Kentucky – Medicaid
Kentucky Integrated Health Insurance Premium Payment Program (KI-HIPP)
Website: https://chfs.ky.gov/agencies/dms/ member/Pages/kihipp.aspx
Phone: 1-855-459-6328
Email: KIHIPP.PROGRAM@ky.gov
KCHIP Website: https://kynect.ky.gov
Phone: 1-877-524-4718
Kentucky Medicaid Website: https://chfs. ky.gov/agencies/dms
– Medicaid
Website: www.medicaid.la.gov or www.ldh. la.gov/lahipp
Phone: 1-888-342-6207 (Medicaid hotline) or 1-855-618-5488 (LaHIPP)
Maine – Medicaid
Enrollment Website: https://www. mymaineconnection.gov/benefits/ s/?language=en_US
Phone: 1-800-442-6003
TTY: Maine relay 711
Private Health Insurance Premium
Webpage: https://www.maine.gov/dhhs/ ofi/applications-forms
Phone: 1-800-977-6740
TTY: Maine Relay 711
Massachusetts – Medicaid and CHIP
Website: https://www.mass.gov/ masshealth/pa
Phone: 1-800-862-4840
TTY: 711
Email: masspremassistance@accenture. com
Minnesota – Medicaid
Website: https://mn.gov/dhs/health-carecoverage/ Phone: 1-800-657-3672
Missouri – Medicaid
Website: http://www.dss.mo.gov/mhd/ participants/pages/hipp.htm Phone: 573-751-2005
Montana – Medicaid
Website: https://dphhs.mt.gov/ MontanaHealthcarePrograms/HIPP Phone: 1-800-694-3084
Email: HHSHIPPProgram@mt.gov
Nebraska – Medicaid
Website: http://www.ACCESSNebraska. ne.gov
Phone: 1-855-632-7633
Lincoln: 402-473-7000 Omaha: 402-595-1178
Nevada – Medicaid
Medicaid Website: http://dhcfp.nv.gov
Medicaid Phone: 1-800-992-0900
New Hampshire – Medicaid
Website: https://www.dhhs.nh.gov/ programs-services/medicaid/healthinsurance-premium-program
Phone: 603-271-5218
Toll free number for the HIPP program: 1-800-852-3345, ext. 15218
Email: DHHS.ThirdPartyLiabi@dhhs.nh.gov
New Jersey – Medicaid and CHIP
Medicaid Website: http://www.state.nj.us/ humanservices/dmahs/clients/medicaid/ Phone: 1-800-356-1561
CHIP Premium Assistance Phone: 609-6312392
CHIP Website: http://www.njfamilycare. org/index.html
CHIP Phone: 1-800-701-0710 (TTY: 711)
New York – Medicaid
Website: https://www.health.ny.gov/ health_care/medicaid/ Phone: 1-800-541-2831
North Carolina – Medicaid
Website: https://medicaid.ncdhhs.gov
Phone: 919-855-4100
North Dakota – Medicaid
Website: https://www.hhs.nd.gov/ healthcare Phone: 1-844-854-4825
Oklahoma – Medicaid and CHIP
Website: http://www.insureoklahoma.org Phone: 1-888-365-3742
Oregon – Medicaid
Website: https://healthcare.oregon.gov/ Pages/index.aspx
Phone: 1-800-699-9075
Pennsylvania – Medicaid and CHIP
Website: https://www.pa.gov/en/services/ dhs/apply-for-medicaid-health-insurancepremium-payment-program-hipp.html
Phone: 1-800-692-7462
CHIP Website: https://www.dhs.pa.gov/ chip/pages/chip.aspx
CHIP Phone: 1-800-986-KIDS (5437)
Rhode Island – Medicaid and CHIP
Website: http://www.eohhs.ri.gov/ Phone: 1-855-697-4347 or 401-462-0311 (Direct RIte Share Line)
South Carolina – Medicaid
Website: https://www.scdhhs.gov Phone: 1-888-549-0820
South Dakota – Medicaid
Website: https://dss.sd.gov Phone: 1-888-828-0059
Texas – Medicaid
Website: https://www.hhs.texas.gov/ services/financial/health-insurancepremium-payment-hipp-program
Phone: 1-800-440-0493
Utah – Medicaid and CHIP
Utah’s Premium Partnership for Health Insurance (UPP) Website: https://medicaid. utah.gov/upp/ Email: upp@utah.gov
Phone: 1-888-222-2542
Adult Expansion Website: https://medicaid. utah.gov/expansion/
Utah Medicaid Buyout Program Website: https://medicaid.utah.gov/buyoutprogram/ CHIP Website: https://chip.utah.gov/
Vermont– Medicaid
Website: https://dvha.vermont.gov/ members/medicaid/hipp-program
Phone: 1-800-250-8427
Virginia – Medicaid and CHIP
Website: https://coverva.dmas.virginia.gov/ learn/premium-assistance/famis-select https://coverva.dmas.virginia.gov/learn/ premium-assistance/health-insurancepremium-payment-hipp-programs Medicaid/CHIP Phone: 1-800-432-5924
Washington – Medicaid
Website: https://www.hca.wa.gov/ Phone: 1-800-562-3022
West Virginia – Medicaid and CHIP
Website: https://dhhr.wv.gov/bms/ http://mywvhipp.com/
Medicaid Phone: 304-558-1700
CHIP Toll-free phone: 1-855-MyWVHIPP (1-855-699-8447)
Wisconsin – Medicaid and CHIP
Website: https://www.dhs.wisconsin.gov/ badgercareplus/p-10095.htm
Phone: 1-800-362-3002
Wyoming – Medicaid
Website: https://health.wyo.gov/ healthcarefin/medicaid/programs-andeligibility/ Phone: 1-800-251-1269
To see if any other States have added a premium assistance program since July 31, 2025, or for more information on special enrollment rights, can contact either:
U.S. Department of Labor Employee Benefits Security Administration www.dol.gov/agencies/ebsa 1-866-444-EBSA (3272)
U.S. Department of Health and Human Services
Centers for Medicare & Medicaid Services www.cms.hhs.gov
1-877-267-2323, Menu Option 4, Ext. 61565
Under the Federal Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA), if you are covered under the Pritchard & Abbott, Inc. group health plan you and your eligible dependents may be entitled to continue your group health benefits coverage under the Pritchard & Abbott, Inc. plan after you
have left employment with the company. If you wish to elect COBRA coverage, contact your Human Resources Department for the applicable deadlines to elect coverage and pay the initial premium.
Plan Contact Information
Pritchard & Abbott, Inc. 4900 Overton Commons Court Fort Worth, TX 76132 817-370-3216
When you get emergency care or get treated by an out-of-network provider at an in-network hospital or ambulatory surgical center, you are protected from surprise billing or balance billing.
What is “balance billing” (sometimes called “surprise billing”)?
When you see a doctor or other health care provider, you may owe certain out-of-pocket costs, such as a copayment, coinsurance, and/ or a deductible. You may have other costs or have to pay the entire bill if you see a provider or visit a health care facility that isn’t in your health plan’s network.
“Out-of-network” describes providers and facilities that have not signed a contract with your health plan. Out-of-network providers may be permitted to bill you for the difference between what your plan agreed to pay and the full amount charged for a service. This is called “balance billing.” This amount is likely more than in-network costs for the same service and might not count toward your annual out-of-pocket limit.
“Surprise billing” is an unexpected balance bill. This can happen when you can’t control who is involved in your care—like when you have an emergency or when you schedule a visit at an in-network facility but are unexpectedly treated by an out-of-network provider.
You are protected from balance billing for:
Emergency services – If you have an emergency medical condition and get emergency services from an out-ofnetwork provider or facility, the most the provider or facility may bill you is your plan’s in-network cost-sharing amount (such as copayments and coinsurance). You cannot be balance billed for these emergency services. This includes services you may get after you are in stable condition, unless you give written consent and give up your protections not to be balanced billed for these poststabilization services.
Certain services at an in-network hospital or ambulatory surgical center – When you get services from an in-network hospital or ambulatory surgical center, certain providers there may be out-of-network. In these cases, the most those providers may bill you is your plan’s in-network costsharing amount. This applies to emergency medicine, anesthesia, pathology, radiology, laboratory, neonatology, assistant surgeon, hospitalist, or intensivist services. These providers cannot balance bill you and may not ask you to give up your protections not to be balance billed.
If you get other services at these in-network facilities, out-of-network providers cannot balance bill you, unless you give written consent and give up your protections.
You are never required to give up your protections from balance billing. You also are not required to get care out-of-network. You can choose a provider or facility in your plan’s network.
When balance billing is not allowed, you also have the following protections:
You are only responsible for paying your share of the cost (like the copayments, coinsurance, and deductibles that you would pay if the provider or facility was in-network). Your health plan will pay outof-network providers and facilities directly.
Your health plan generally must:
• Cover emergency services without requiring you to get approval for services in advance (prior authorization).
• Cover emergency services by out-ofnetwork providers.
• Base what you owe the provider or facility (cost-sharing) on what it would pay an in-network provider or facility and show that amount in your explanation of benefits.
• Count any amount you pay for emergency services or out-of-network services toward your deductible and out-of-pocket limit.
If you believe you have been wrongly billed, you may contact your insurance provider. Visit www.cms.gov/nosurprises for more information about your rights under federal law.
This brochure highlights the main features of the Pritchard & Abbott, Inc. employee benefits program. It does not include all plan rules, details, limitations, and exclusions. The terms of your benefit plans are governed by legal documents, including insurance contracts. Should there be an inconsistency between this brochure and the legal plan documents, the plan documents are the final authority. Pritchard & Abbott, Inc. reserves the right to change or discontinue its employee benefits plans anytime.