Which Modality Best Combines Anatomy and Physiology in Non-invasive Cardiac Imaging?
ESR President Minerva Becker reflects on the success of ECR 2026 and her hopes for 2027 Interview:
4th–8th
Ethical AI in Radiology: Performance, People, and Post-market Responsibility
Alex Perkins
From Stage to Suite: Enhancing Interventional Radiology with AI and Robotics
Roli B. Omamuli
AI or Radiologist Interpretation for Prostate Cancer Diagnosis
Ng ABCD et al.
Focal Cortical Dysplasia Type IIb: Correlation of Histological Data with Typical MRI Patterns During Epileptological Scanning
Smirnova A et al.
Evaluating the Use of Complementary Therapies Amongst Patients Undergoing Radiotherapy in Malta
Xuereb and Borg Grima
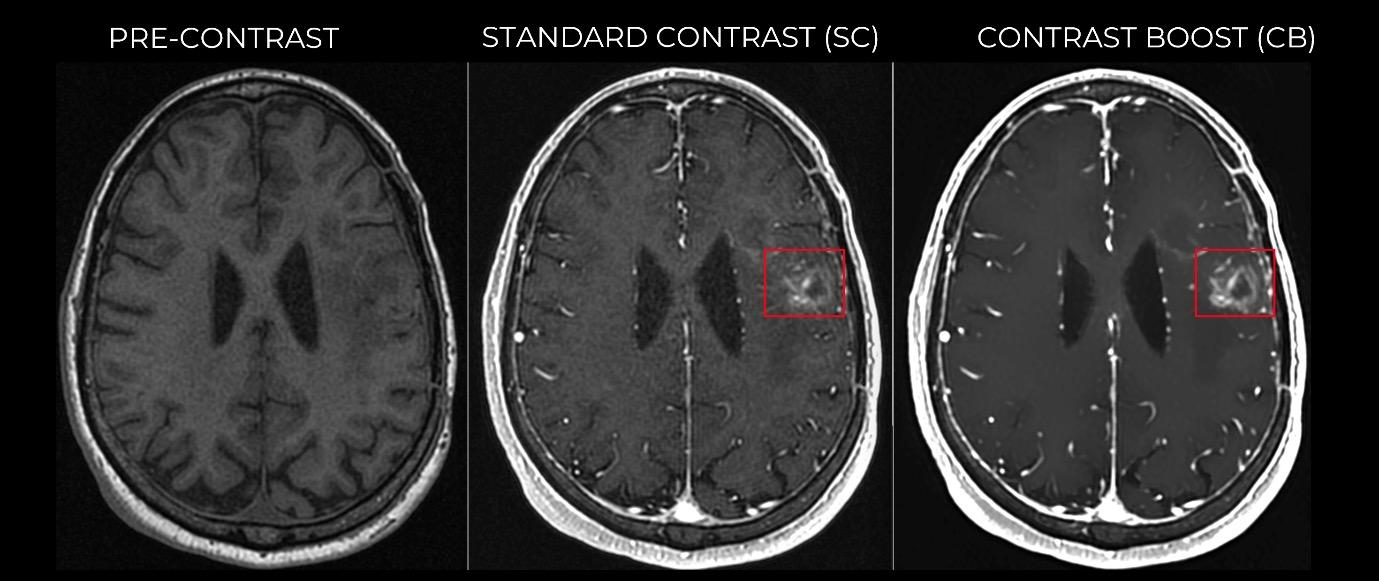
Deep Learning Amplifies the Benefits of High Relaxivity in Brain MRI: A Quantitative Assessment of a Contrast Boosting Algorithm Using Gadopiclenol
Pasumarthi
Congress Interviews
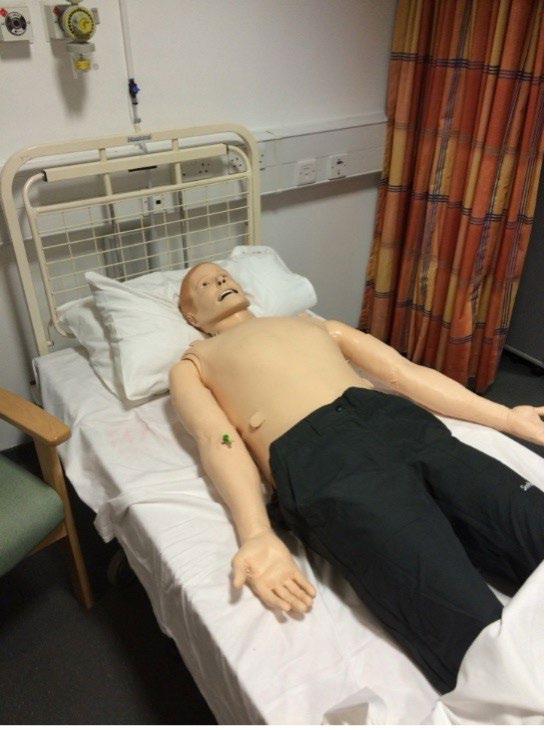
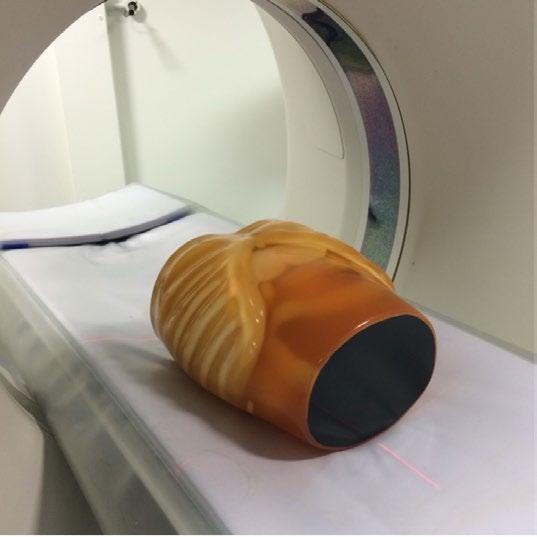
Simulation in Diagnostic Radiography Training: A Replacement for Clinical Placements?
Editor's Pick: Universal Noninvasive Cardiac Imaging: Which Modality Best Combines Anatomy and Physiology? Saulat
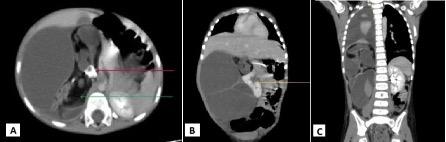
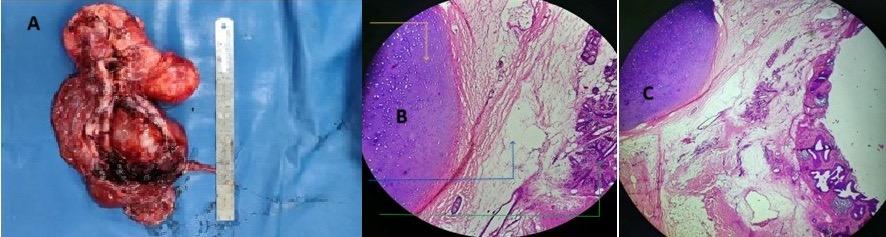
Imaging Features of Mature Retroperitoneal Teratoma in a Paediatric Patient: A Case Report
Editorial Board
Editor-in-Chief
Dr Yasmeen Malik
St George's University of London, UK
Malik is Senior Lecturer Therapeutic Radiography, Postgrad Research Lead, Course Admissions Tutor, Kingston and St George’s Joint Faculty, Faculty of Health, Social Care and Education, School of Allied Health, Social Care & Midwifery
St George’s University of London, UK.
Prof Christian Jürgens
Hospital Reinbek St. Adolf-Stift, Germany; Universität zu Lübeck, Germany
Prof Aad van der Lugt
Erasmus University Medical Center, the Netherlands
Dr Çetin Erol
Rıdvan Ege Hospital, Ufuk University School of Medicine, Ankara, Türkiye
Prof Eduard Ruiz-Castañé
Fundació Puigvert, Spain
Dr Olusola Michael Adeleke
NHS England, UK
Prof Roger Dmochowski
Vanderbilt University Medical Center, USA
Dr Luke Dixon
Imperial College Healthcare NHS Trust, UK
Dr Sanjog Kalra
Einstein Medical Center, USA
Dr Paul Bezzina
University of Malta, Malta
Dr Nicholas Kipshidze
New York Cardiovascular Research, USA
Prof Jean de la Rosette
Istanbul Medipol University, Türkiye
Dr Sophie Willis
University of Lincoln, UK
Aims and Scope
EMJ Radiology is an open access, peer-reviewed ejournal committed to helping elevate the quality of radiology practices globally by publishing high-quality content on the latest developments in medical technologies.
The journal is published annually, six weeks after the European Congress of Radiology (ECR), providing the latest developments in the field, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. Additionally, it covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ Radiology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. EMJ Radiology is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
EMJ Radiology endeavours to increase knowledge, stimulate discussion, and contribute to a better understanding of radiology and the latest technological advances in the field. Our focus is on research that is relevant to radiologists. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance knowledge and inform of coming trends affecting clinical practice in radiology.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®.
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication
Launch Date: 2020
Frequency: Yearly Online ISSN: 2633-9978
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (ECR 2026) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Vienna, Austria, the location of ECR 2026.
Niamh Holmes, Roli Omamuli, Alexander Perkins, Katrina Thornber, Aleksandra Zurowska
Reporter
Anna Caldwell
Creative Director
Tim Uden
Design Manager
Stacey White
Senior Designers
Tamara Kondolomo, Owen Silcox
Designers
Shanjok Gurung, Fabio van Paris
Junior Designers
Fraser Hoey, Helena Spicer, Caleb Wylie
Head of Marketing
Stephanie Corbett
Commercial Director
Oz Desai
Chief Executive Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chairman
Spencer Gore
Welcome
Dear Readers,
I am delighted to welcome you to the 2026 issue of EMJ Radiology, which brings together an impactful selection of content exploring the most influential topics in the field. This issue presents highlights from the European Congress of Radiology (ECR) 2026, featuring a collection of research highlights and commentaries on some of the most inspiring sessions that brought the theme ‘Rays of Knowledge’ to life.
Over the past year, radiology has seen remarkable progress, particularly in the rapid evolution of AI for image interpretation, the expansion of advanced imaging technologies, and the growing integration of data-driven decision support within clinical workflows. These developments are reflected throughout this issue, alongside in-depth interviews with key opinion leaders providing timely perspectives on the implementation of breast cancer screening, quantitative imaging, and the operational and workforce challenges facing radiology departments as innovation continues to accelerate. Furthermore, we are delighted to present exclusive interviews from a number of experts who made ECR 2026 such a success.
Our peer-reviewed content explores non-invasive cardiac imaging, offering valuable insights into both clinical and operational considerations, and includes an exciting case report following the development of mature retroperitoneal teratoma in a paediatric patient. Readers will also find a feature article examining the role that simulation plays in diagnostic radiography training compared to clinical placements.
I would like to take this opportunity to thank our amazing Editorial Board, peer reviewers, interviewees, and contributing authors for bringing together another great issue.
Bertie
Pearcey
Editorial Co-ordinator
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
Stay at the Forefront of Modern Medicine
High-level perspectives. Global experts. Essential updates.
Join us for conversations with the minds shaping healthcare's future. Gain the distilled insights you need to lead in your field and make maximum impact.
Jonathan Sackier: Non Executive Director & CMO, AiM Medical Robotics, Florida, USA
Saranya Ravindran: Paediatric Emergency Medicine Registrar, Imperial College Healthcare NHS Trust
Catherine Glass: Associate NHS GP and Senior Appraiser, NHS England
Foreword
Dear Colleagues,
I am delighted to introduce this latest issue of EMJ Radiology, which brings together a rich and thoughtfully curated collection of contributions spanning peer-reviewed research, professional perspectives, and developments across the wider radiology landscape.
This issue reflects the continued evolution of radiology as a dynamic and interdisciplinary field, with particular emphasis on the integration of emerging technologies within clinical practice. Notably, features exploring the ethical and practical application of AI, alongside advances in robotics and interventional techniques, highlight a discipline that is increasingly focused not only on innovation but also on meaningful and responsible implementation.
The inclusion of coverage from the European Congress of Radiology (ECR) 2026 offers valuable insight into current international priorities, including the growing recognition of underreported conditions such as oligometastatic disease, and the use of combined imaging approaches to enhance diagnostic precision in complex conditions such as intracranial atherosclerotic disease. These developments underscore a broader shift towards more nuanced, data-informed, and patient-centred models of care.
Equally important is the continued emphasis on education and workforce development.
Reflections from leaders within the European radiography community highlight the importance of accessible, highquality education and the need to support radiographers as key contributors to service innovation, leadership, and the translation of technological advances into improved patient outcomes.
The peer-reviewed articles presented in this issue include work focused on optimising cardiac imaging and rare clinical presentations. There is a clear throughline: a commitment to improving diagnostic accuracy, enhancing clinical decisionmaking, and ultimately strengthening patient care.
These developments underscore a broader shift towards more nuanced, data-informed, and patientcentred models of care
I would like to extend my thanks to all authors, reviewers, and members of the Editorial Board for their contributions to this issue. I hope that readers find the content both informative and thought-provoking, and that it supports ongoing reflection and development within practice.
Sophie Willis University of Lincoln,
UK
ECR 2026
Radiologic imaging reveals otherwise hidden anatomical structures, and allows us to distinguish between normal and pathological findings
Review of the European Congress of Radiology (ECR) 2026 Congress Review
THIS SPRING, Vienna, Austria, once again took centre stage as it welcomed the global radiology community for the European Congress of Radiology (ECR) 2026. Drawing a growing international audience, with participation rising by 9% and more than 11,000 abstracts submitted, this year’s Congress highlighted both the scale and momentum of a specialty at a pivotal moment of transformation.
Opening in spectacular fashion, the ceremony blended science with artistry, as a live performance of ‘O Fortuna’ by the Vienna Art Orchestra and Neue Wiener Stimmen Choir, accompanied by a striking light display, set the tone for a congress built around this year’s theme: ‘Rays of Knowledge’. As the final notes gave way to rapturous applause, Congress President Minerva Becker took to the stage, introducing a concept inspired by Athena, the Greek goddess of wisdom. Drawing on the symbolism of Athena’s owl, Becker reflected on radiology’s unique ability to illuminate what lies beneath the surface, “Radiologic imaging reveals otherwise hidden anatomical structures, and allows us to distinguish between normal and pathological findings.”
Framing her address around the future of the discipline, Becker positioned radiology at a critical crossroads. While some may view the modern radiologist as a figure confined to image interpretation, she firmly rejected this notion, emphasising the specialty’s identity as a clinical discipline. For Becker, the true value of radiologists lies not only in reading images but in answering complex clinical questions, contributing to multidisciplinary
care, and fostering meaningful interactions with both colleagues and patients.
This perspective is set against a backdrop of rapidly increasing demand. Imaging volumes have risen dramatically across Europe, with Becker noting a 33% increase in Switzerland alone over the past decade, far outpacing workforce growth. As a result, radiologists now face mounting reporting burdens and workforce shortages, becoming, in her words, “victims of their own success.”
Amid this pressure, AI emerged as both a challenge and an opportunity. Already embedded in image acquisition and workflow optimisation, AI has contributed to rising volumes but also holds promise in alleviating workload through automation of highvolume, low-complexity tasks. Becker urged a balanced and critical approach, highlighting unresolved questions surrounding clinical integration, ethical responsibility, training, and the risk of deskilling. While some fear a future of automation and obsolescence, she instead called for a reframing of the radiologist’s role, one that recognises the breadth of contributions beyond reporting, from ensuring diagnostic quality and safety to providing essential clinical insight.
“Our purpose is to diagnose disease, sometimes to treat it, and always to engage with patients and clinical partners,” Becker stated, reinforcing that technological advancement does not diminish the specialty’s core mission. Rather, she argued, it offers an opportunity to reclaim time for higher-value, patient-centred activities.
The congress theme resonated strongly throughout the opening session, extending beyond radiologists to the wider imaging community. Patrizia Cornacchione, President of the European Federation of Radiographer Societies (EFRS), welcomed over 1,500 radiographers in attendance, highlighting the essential partnership between radiographers, radiologists, and allied health professionals. Emphasising interdisciplinarity as “the key to quality, innovation, and patient safety,” she noted the importance of collaboration in translating technological advances into meaningful patient outcomes.
The ceremony also celebrated the human dimension of the specialty. A short film featuring young radiologists offered an optimistic perspective on the future, showcasing passion, curiosity, and a strong sense of purpose among the next generation. Their voices stood in contrast to narratives of uncertainty, reinforcing confidence in radiology’s continued evolution.
Recognition of excellence remained a cornerstone of the evening, with the presentation of the European Society of Radiology (ESR) Gold Medals.
Honourees included Regina Beets-Tan, Netherlands Cancer Institute, Amsterdam, the Netherlands; Roberto Maroldi, University of Brescia, Italy; and Peter Mildenberger, University Medical Center Mainz, Germany, each celebrated not only for their scientific achievements, but for their lasting contributions to collaboration, education, and patient-centred care. Their reflections highlighted a unifying message: that radiology’s strength lies in its ability to connect disciplines, bridge knowledge gaps, and continuously advance in the service of patients.
With a membership now exceeding 149,000, the ESR stands as one of the largest and most influential organisations in medical imaging, reinforcing ECR’s role as a central hub for education, innovation, and global exchange. As the opening ceremony drew to a close, Becker returned to the stage with a clear call to action: to focus not only on efficiency or volume, but on the quality, purpose, and impact of radiological practice. “A correct diagnosis is the first step towards every right treatment,” she reminded the audience, emphasising the enduring responsibility at the heart of the profession.
EMJ had the pleasure of attending ECR 2026 and is proud to present key highlights from the diverse abstract sessions in our comprehensive review of ECR 2026 for this issue of EMJ Radiology, alongside an exclusive interview with ECR President Minerva Becker. Continue reading for an indepth look at these pivotal discussions and groundbreaking research from this year’s Congress.
Our purpose is to diagnose disease, sometimes to treat it, and always to engage with patients and clinical partners
Oligometastatic Disease Rarely Reported in Routine Imaging
RESEARCH presented at ECR 2026 suggests that oligometastatic disease (OMD) remains markedly underreported in routine radiology practice, despite its growing clinical relevance and reliance on imaging for diagnosis.1
OMD describes a transitional state of cancer characterised by a limited number of metastatic lesions, where localised treatments such as ablative therapy may offer curative potential. As imaging plays a central role in identifying this state, researchers conducted a large-scale realworld analysis to assess how frequently OMD is referenced in radiology reports across the USA.
Using a real-world imaging data platform, the study evaluated over 33.7 million radiology reports spanning 11 imaging modalities, including CT, MRI, PET/CT, and X-ray, from healthcare providers across 40 states. Despite the extensive dataset, OMD was mentioned in just 164 reports from 109 patients, highlighting its limited integration into routine reporting.
Notably, the majority of OMD references originated from clinicians rather than radiologists. Clinicians included OMD in the clinical indication or patient history in 148 reports, whereas radiologists themselves documented the term in only 18 reports.
OMD was identified across 20 primary tumour types, most commonly breast, lung, and prostate cancers.
CT was the most frequent modality associated with OMD mentions, followed by X-ray angiography, PET/CT, and MRI. Although the first recorded mention of OMD appeared in 2017, usage has increased over time, reaching 33 reports in 2024, suggesting gradual but still limited adoption.
The findings point to a disconnect between the conceptual importance of OMD and its practical application in radiology reporting. Given that imaging is fundamental to diagnosing and guiding treatment decisions in this setting, the authors highlight a need for clearer definitions and standardised reporting guidelines.
However, the retrospective design and restriction to USA-based data limit the generalisability of the results. Further work, particularly in international settings, will be important to determine whether similar patterns exist globally.
Despite the extensive dataset, OMD was mentioned in just 164 reports from 109 patients, highlighting its limited integration into routine reporting
Spectral CT Boosts Accuracy in Bowel Ischaemia Detection, Study Finds
ACCURATE and timely diagnosis of bowel ischaemia remains a critical challenge in emergency imaging, where delays can lead to significant morbidity and mortality. Spectral CT has emerged as a promising technique, offering material-specific reconstructions that may enhance visualisation beyond conventional blended images. A retrospective single-centre study presented at ECR 2026 evaluated whether spectral reconstructions improve diagnostic performance for bowel ischaemia and whether outcomes differ between dual energy CT and photon counting CT platforms.2
The study reviewed 378 consecutive emergency spectral CT examinations performed between January 2023–July 2025 for suspected bowel ischaemia, including 265 dual energy CT and 113 photon counting CT scans. Exclusion criteria comprised absent spectral data, non-diagnostic image quality, incomplete bowel coverage, lack of a reference standard within 72 hours, or patient age under 18 years. Two abdominal radiologists with 4 years of subspecialty experience independently assessed each case. Examinations were first reviewed using blended images, followed by spectral reconstructions after a 4-week washout period to minimise recall bias. Readers assigned suspicion scores on a five-point scale, and duplicate cases were included to evaluate intra-reader repeatability. Statistical analysis employed generalised linear mixed models with random intercepts for both reader and case, alongside DeLong testing for comparison of diagnostic performance.
Spectral CT has emerged as a promising technique, offering material-specific reconstructions that may enhance visualisation
Bowel ischaemia was confirmed in 126 of 378 examinations (33%). Sensitivity improved significantly from 75% with blended images to 87% with spectral reconstructions (p=0.008), while specificity increased from 72% to 86% (p<0.001).
Per-reader area under the curve rose from 0.81 and 0.82 to 0.91 and 0.92, respectively (both p<0.001). Diagnostic confidence improved from scores of 3 to 5 on a seven-point scale. Inter-reader agreement increased from a κ value of 0.56 to 0.71, and intra-reader repeatability was high at 0.82. Stratified analysis demonstrated significantly greater performance gains with photoncounting CT compared with dual-energy CT (interaction p=0.03).
These findings indicate that spectral CT reconstructions substantially enhance diagnostic accuracy, confidence, and agreement in detecting bowel ischaemia, with the greatest benefit observed using photoncounting CT. For clinical practice, integrating spectral reconstructions into emergency CT workflows may improve diagnostic reliability without increasing contrast dose or radiation exposure. However, the single-centre design and limited number of readers may restrict generalisability, and further multicentre studies are warranted to confirm these results and support broader implementation.
Sensitivity improved significantly from 75% with blended images to 87% with spectral reconstructions (p=0.008), while specificity increased from 72% to 86% (p<0.001)
One in Four LI-RADS 3 Liver Lesions Progress Within 1 Year
A NEW multicentre, multinational study presented at ECR 2026 provides important insights into the natural history of indeterminate liver lesions in patients who are cirrhotic. The research examined the 1-year outcomes of LI-RADS 3 observations, lesions of intermediate probability for hepatocellular carcinoma (HCC), on contrast-enhanced MRI across six centres in three countries.3
The retrospective study included 347 patients with 540 LI-RADS 3 lesions, each followed for 12 months. Using LI-RADS v2018 criteria, researchers applied generalised linear mixed-effects models and machine learning approaches, including least absolute shrinkage and selection operator (LASSO) and random forest, to identify predictors of lesion progression.
The findings indicate that approximately one in four indeterminate liver lesions in patients who are cirrhotic progress within 1 year
Results showed that 27% of LI-RADS 3 observations progressed within 1 year, with 13% advancing to LI-RADS 4 (probably HCC) and 14% reaching LI-RADS 5 (definitely HCC). Independent predictors of progression included lesion size (odds ratio [OR]: 1.12 per mm), severe liver dysfunction (Child-Pugh Class C; OR: 8.36), and underlying aetiology, with alcohol-related liver disease showing a protective association (OR: 0.24).
Imaging features such as an enhancing capsule improved risk prediction, increasing the area under the curve from 0.65 to 0.72 (p=0.01). A lesion size threshold of 9.5 mm was associated with higher progression risk.
The findings indicate that approximately one in four indeterminate liver lesions in patients who are cirrhotic progress within 1 year. Integrating clinical parameters, liver function, and imaging features enhances risk stratification and supports more personalised surveillance strategies.
The study has some limitations, including potential selection bias, variability in imaging protocols across centres, and reliance on MRI rather than histopathology for lesion classification. Ancillary features were applied in LI-RADS categorisation but were not analysed independently to reduce inter-reader variability. The research received no external funding and was approved by institutional review boards, with informed consent waived due to its retrospective design.
This multicentre study provides valuable evidence for radiologists and hepatologists, highlighting key predictors of progression in indeterminate liver lesions and informing follow-up strategies for early HCC detection.
Iodine Maps Show High Accuracy for Pericarditis Diagnosis
A NEW study presented at ECR 2026 has demonstrated that iodine maps derived from dual-layer spectral CT can accurately identify pericarditis, offering a promising non-invasive diagnostic tool for clinical practice.4
In this retrospective, single-centre study, researchers evaluated 105 patients who underwent CCTA between February 2023–December 2024 using a dual-layer spectral CT scanner. The cohort included patients with and without pericardial effusion. Investigators measured iodine concentration within the pericardial layers using iodine maps and assessed pericardial thickness on both spectral and conventional reconstructions. Diagnostic performance was evaluated against the European Society of Cardiology (ESC) clinical criteria. The research received no external funding and was approved by an ethics committee.
Findings showed that iodine concentration was significantly higher in patients with pericarditis compared with those without (1.79 mg/mL [interquartile range: 1.11–2.24] versus 0.55 mg/mL [interquartile range: 0.42–0.66]; p<0.0001). Pericardial thickness was also markedly increased in affected patients across both spectral and conventional reconstructions. On iodine maps, a threshold of >0.82 mg/mL achieved an area under the curve of 0.99 (95% CI: 0.94–0.99), with 93.9% sensitivity (95% CI:
79.8–99.3) and 95.8% specificity (95% CI: 88.3–99.1). Using a pericardial thickness threshold of >1.6 mm, iodine maps reached an area under the curve of 1.00 (95% CI: 0.97–1.00), achieving 100% sensitivity (95% CI: 89.4–100) and 100% specificity (95% CI: 95.0–100). Comparable performance was observed with conventional reconstructions at a slightly higher thickness threshold of >1.8 mm.
These results demonstrate the potential value and impressive accuracy of spectral iodine maps in diagnosing pericarditis using both iodine concentration and pericardial thickness measurements.
The authors noted limitations, including the retrospective design, modest sample size, and single-centre setting, as well as the exclusive use of dual-layer spectral CT technology.
Overall, the findings suggest that iodine maps could enhance the non-invasive diagnosis of pericarditis, with potential to refine clinical workflows and support earlier, more accurate treatment decisions.
AI-Based CT Body Composition Metrics Linked to Age and Smoking
RECENT data presented at ECR 2026 indicate that age and smoking status are independently associated with variations in body composition in men.5 These measures were taken from low-dose chest CT scans in participants in a lung cancer screening.5
The authors analysed baseline low-dose CT scans from 4,435 male participants enrolled in the NELSON trial (a study aimed at determining the effectiveness of low-dose CT lung cancer screening). AI-based automated tools were used to quantify skeletal muscle area (SMA) and subcutaneous adipose tissue (SAT) at the thoracic vertebral levels 5, 8, and 10. Measurements across these three levels were combined to generate composite SMA and SAT values, and a fat-to-muscle ratio was calculated for an integrated assessment of body composition. Age was stratified in 5-year intervals, and analyses were adjusted for smoking status and cumulative exposure (pack-years).
Current smokers demonstrated significantly lower levels of both muscle and fat compared with former smokers (p<0.001). Increasing age was associated with a progressive decline in SMA (from 515 cm² in those aged 50–54 years to 472 cm² in those aged ≥70 years; p<0.001) alongside increases in SAT (376 to 443 cm²; p<0.001) and fat-to-muscle (0.70 to 0.90; p<0.001).
These trends remained significant after adjusting for smoking status and pack-years, suggesting that both age and smoking independently influence body composition.
The study demonstrates that body composition measures derived from routine low-dose CT imaging could provide additional clinically relevant information. CT-derived metrics may enhance risk stratification in screening programmes, reflecting their potential practical value.
The findings are observational, and further research is needed to confirm how these imaging markers relate to clinical outcomes in lung cancer screening populations. The
information available does not provide data on potential confounding factors such as weight, height, or overall health status.
These trends remained significant after adjusting for smoking status and pack-years, suggesting that both age and smoking independently influence body composition
Smaller WEB Devices Show Improved Outcomes in Intracranial Aneurysm Treatment
A NEW multicentre study from the WorldWideWEB Consortium (W3C) presented at ECR 2026 suggests that smaller Woven EndoBridge (WEB; MicroVention, Aliso Viejo, California, USA) devices may offer improved anatomic outcomes and lower retreatment rates in the treatment of intracranial aneurysms, without compromising safety or functional outcomes.6
The retrospective analysis included 1,473 adult patients treated with WEB devices across 30 international centres. Patients were stratified by device size into small (≤4.5 mm) and large (>4.5 mm) groups, with an additional subanalysis comparing small and very large (>7.5 mm) devices. The primary outcome was retreatment rate, while secondary outcomes included functional status measured by the modified Rankin Scale (mRS), anatomic occlusion rates, and safety events such as intracranial haemorrhage and thromboembolic complications.
Of the total cohort, 229 patients (15.5%) were treated with small WEB devices
Of the total cohort, 229 patients (15.5%) were treated with small WEB devices. Retreatment rates were significantly lower in this group compared with those receiving larger devices (4.3% versus 8.8%; p=0.037). Small devices were also associated with higher complete occlusion rates both periprocedurally (57.1% versus 36.6%; p<0.001) and at last follow-up (76.2% versus 58.5%; p<0.001). Functional outcomes were comparable between groups, with a median mRS of 1 (1–2) in both cohorts (p=0.88).
Safety outcomes did not differ significantly between small and large devices. Rates of intracranial haemorrhage were 2.6% in the small device group and 0.9% in the large device group (p=0.102), while thromboembolic complications occurred in 3.1% and 3.9% of patients, respectively (p=0.686). In the sub-analysis, very large devices were associated with higher retreatment rates (16.1%; p<0.001) and lower complete occlusion rates both periprocedurally (32.2%; p<0.001) and at follow-up (50.5%; p<0.001), with similar safety profiles.
These findings indicate that smaller WEB devices may provide superior anatomic results while maintaining comparable safety and functional outcomes. The results are particularly notable given the technical challenges associated with deploying smaller devices.
The study is limited by its retrospective design and the absence of core laboratory adjudication for anatomic outcomes, which may introduce variability in assessment.
Overall, this large multicentre analysis supports the use of smaller WEB devices as an effective option in intracranial aneurysm treatment, highlighting their potential to reduce retreatment rates without increasing risk.
Deep Learning MRI Reconstruction Cuts Scan
Time Dramatically
A NEW real-world study presented at ECR 2026 showed that integrating a deep learning reconstruction (DLR) algorithm into musculoskeletal MRI workflows substantially reduced scan times while maintaining image quality and delivering measurable environmental benefits.7
Researchers evaluated the implementation of a DLR technique across a large private radiology network in Brazil, analysing its impact on workflow efficiency, diagnostic image quality, and sustainability in routine outpatient practice. The research received no external funding and was approved by an ethics committee.
The retrospective analysis included 22,165 MRI examinations, comparing 12 months before DLR implementation with 12 months after DLR implementation. Following vendorguided upgrades and protocol optimisation, acquisition times were automatically recorded, and a subset of scans underwent blinded qualitative review using a 5-point Likert scale.
Findings demonstrated a 53% reduction in median scan duration after DLR implementation. The most pronounced improvements were observed in shoulder (62%), wrist (59%), knee (52%), spine (38%), and hip (33%) imaging. These reductions translated into improved patient throughput, decreased scanner idle time, and fewer interruptions related to patient anxiety or motion. Importantly, although some reviewers noted subtle differences in image texture, radiologist assessments indicated that overall image quality remained stable despite the accelerated acquisition.
Beyond operational gains, the study identified notable sustainability advantages. Reduced scan times led to annual energy savings exceeding 2.3 MWh per scanner, corresponding to more than 1 metric ton of avoided carbon dioxide equivalent emissions. These findings suggest that AI-driven reconstruction may contribute to greener imaging practices without sacrificing clinical performance.
The most pronounced improvements were observed in shoulder (62%), wrist (59%), knee (52%), spine (38%), and hip (33%) imaging
The study also emphasised the importance of workflow standardisation and close collaboration between radiologists, technologists, and industry partners as key requirements for successful implementation.
The authors acknowledged limitations, including the retrospective design, limited sampling for image quality assessment, and absence of a formal cost-effectiveness analysis. Nevertheless, the results provide compelling real-world evidence that DLR can enhance efficiency, patient experience, and environmental sustainability in musculoskeletal MRI, supporting its broader adoption in clinical practice.
Combined Imaging Boosts Stroke Prediction in Atherosclerosis
A NEW imaging study presented at ECR 2026 suggests that combining markers of intracranial atherosclerotic plaques with indicators of cerebral small vessel disease (CSVD) could significantly improve the prediction of ischaemic stroke risk.8
Intracranial atherosclerotic disease is a major cause of stroke worldwide, yet accurately identifying patients at the highest risk remains a clinical challenge. While both large artery plaque characteristics and small vessel disease markers have individually been linked to stroke, their combined predictive value has not been well established.
To address this, the researchers analysed 237 patients who underwent contrastenhanced high-resolution vessel wall MRI (HRVW-MRI) between January 2021–April 2024. The median age was 63 years, and approximately two-thirds of participants were male. Among the cohort, 163 patients experienced an ischaemic stroke.
Intracranial atherosclerotic disease is a major cause of stroke worldwide, yet accurately identifying patients at the highest risk remains a clinical challenge
The team evaluated multiple plaque-related imaging features, including intraplaque haemorrhage, enhancement grade, maximum wall thickness, and lumen area. In parallel, they assessed CSVD burden using a composite score (ranging from 0–4) based on four established markers: lacunes, white matter hyperintensities, cerebral microbleeds, and enlarged perivascular spaces.
Statistical analysis showed that several imaging characteristics were independently associated with stroke occurrence. Patients with greater wall thickness, larger lumen area, higher plaque enhancement, and increased numbers of cerebral microbleeds and enlarged perivascular spaces were more likely to have experienced a stroke. Higher overall CSVD burden and more severe white matter hyperintensities were also significant predictors.
Importantly, combining plaque features with CSVD markers resulted in substantially improved predictive performance. The integrated model achieved an area under the receiver operating characteristic curve (AUC) of 0.85, outperforming models based on plaque features alone (AUC: 0.77) or CSVD markers alone (AUC: 0.79).
These findings highlight the additive value of assessing both large and small vessel disease in patients with intracranial atherosclerosis. The authors suggest that a more comprehensive imaging approach could enable better risk stratification and inform clinical decision-making, potentially helping to identify high-risk individuals who may benefit from closer monitoring or more aggressive preventive strategies.
Overall, the study provides further evidence that stroke risk is driven by the complex interplay between different vascular pathologies, reinforcing the need for integrated diagnostic frameworks in cerebrovascular disease.
Glucose Dysregulation Linked to Progression of White Matter Brain Damage
WHITE matter hyperintensities (WMH) are a key imaging marker of cerebral small vessel disease and are associated with stroke, cognitive decline, and functional impairment. Identifying individuals at risk of WMH progression, alongside modifiable biological drivers, remains a clinical priority. A study presented at ECR 2026 aimed to develop a predictive model for WMH progression and to explore whether abnormalities in glucose metabolism contribute causally through microstructural brain damage.9
Using imaging and genetic data from a large population cohort, the analysis focused on both prediction and mechanistic pathways, with the notable finding that glucometabolic dysfunction plays a measurable role in WMH progression.
Among 1,616 participants, 902 demonstrated WMH progression while 714 remained stable
Data were analysed from UK Biobank participants of European ancestry who had serial brain MRI scans and evidence of cerebral small vessel disease. Eight key predictive features were selected using the Akaike information criterion, including age, BMI, cystatin C, glucose, and diffusion MRI-derived metrics such as fractional anisotropy and mean diffusivity. Multiple machine learning models were developed to predict WMH progression. In parallel, structural equation modelling assessed mediation pathways, while bidirectional two-sample Mendelian randomisation used genome-wide association study data to investigate causal relationships between glucose indices, including HbA1c and fasting glucose, and white matter microstructure.
Among 1,616 participants, 902 demonstrated WMH progression while 714 remained stable. Seven machine learning algorithms were tested, with logistic regression and support vector machine models showing the best predictive performance. Structural equation modelling demonstrated that glucose levels partially mediated WMH progression through
isotropic volume fraction, indicating microstructural damage as an intermediate pathway. Mendelian randomisation analyses further showed that genetic predisposition to higher HbA1c was significantly associated with increased free water content in several brain regions, including the left cerebral peduncle, right hippocampal gyrus, left anterior thalamic radiation, and left corticospinal tract.
These findings suggest that glucometabolic dysregulation contributes to WMH progression via microstructural injury, highlighting a potential target for clinical intervention. In practice, tighter glycaemic control may have relevance not only for metabolic health but also for preventing cerebrovascular damage and its neurological consequences. However, the study is limited by its predominantly European cohort, which may restrict generalisability to more diverse populations, and further validation in broader clinical settings is required.
Novel CT Power Save Mode Cuts Idle Energy Without Workflow Disruption
A NOVEL CT power save mode reduced idle energy consumption without disrupting clinical workflows.10 CT scanners, essential for diagnostic imaging, often remain powered on during the intervals between patient examinations. These idle periods constitute a large portion of total on-time, contributing to energy use, associated costs and carbon emissions.
In a 28-week prospective study presented at ECR 2026, a single CT scanner was equipped with the novel power save mode. Power draw was continuously monitored and categorised as active, idle, and power save states. Usability and workflow impact were assessed via a survey of 19 CT technologists.
Across 124 workdays, the power save mode reduced power draw by 26.8% compared with the idle state (1.6±0.1 kW versus 2.1±0.1 kW), resulting in a 15.6% reduction in non-productive energy use and a 7.2% reduction in total operational energy use. Non-productive time accounted for 66.1% of scanner on-hours, with the power save mode active 58.1% of this time. Survey responses from 19 technologists indicated
References
1. Willemink MJ et al. The use of oligometastatic disease in routine radiology practice: a real world data analysis. Abstract. ECR 2026, 4-8 March, 2026.
2. Mankertz FKE et al. Improved detection of bowel ischemia in emergency CT: diagnostic value of spectral reconstructions across DECT and PCCT platforms. Abstract. ECR 2026, 4-8 March, 2026.
3. Asmundo L et al. A multicenter multinational retrospective study of the 1-year natural history of LI-RADS 3 observations in patients with cirrhosis. Abstract. ECR 2026, 4-8 March, 2026.
4. Lanzafame LRM et al. Evaluation of the diagnostic performance of iodine
high awareness of the power save mode (84%), with 79% having manually activated it at least once. All technologists reported the activation process as very easy, and 100% reported no technical issues or workflow disruptions.
These results demonstrate that the power save mode reduces non-productive energy use while maintaining workflow efficiency. Limitations include testing on a single CT scanner model, with relative and absolute savings likely varying by vendor, model, and clinical setting. Similar power save modes may reduce energy use and operational costs in other radiology departments, and future studies could evaluate whether these benefits extend across different scanners and environments.
maps derived from a dual-layer CT for the diagnosis of pericarditis. Abstract. ECR 2026, 4-8 March, 2026.
5. Xin Y et al. Thoracic body composition across age and smoking status in a lung cancer screening cohort: insights from the NELSON study. Abstract. ECR 2026, 4-8 March, 2026.
6. Dugar F et al. Small versus large Woven EndoBridge devices for intracranial aneurysms: results from the WorldWideWEB multicenter study. Abstract. ECR 2026, 4-8 March, 2026.
7. Mendonca J et al. Real-world implementation of a deep learning–based reconstruction algorithm in musculoskeletal MRI: impact on workflow, image quality, and sustainability. Abstract. ECR 2026, 4-8 March, 2026.
8. Zhang J et al. Combining plaques and cerebral small vessel diseases imaging characteristics for ischemic stroke prediction in intracranial atherosclerotic disease. Abstract. ECR 2026, 4-8 March, 2026.
9. Han X et al. Glucometabolic dysregulation drives white matter hyperintensity progression in cerebral small vessel disease: longitudinal evidence from the UK biobank and mendelian randomization analysis. Abstract. ECR 2026, 4-8 March, 2026.
10. Hehenkamp P et al. Reducing idle CT scanner energy consumption between examinations: operational feasibility and impact of a rapid-reactivation power save mode. Abstract. ECR 2026, 4-8 March, 2026.
Ethical AI in Radiology: Performance, People, and Post-market Responsibility
Author: Alex Perkins, EMJ, London, UK
Citation: EMJ Radiol. 2026;7[1]:23-26.
https://doi.org/10.33590/emjradiol/19453N4H
AT THE European Congress of Radiology (ECR) 2026, the session ‘The Art of Ethical AI: Redefining Performance in Radiology’ brought together speakers who argued that ethical AI in radiology cannot be judged by accuracy alone. Chaired by Elmar Kotter, University of Freiburg, Freiburg im Breisgau, Germany, the session explored how regulation, post-market surveillance, and human factors are reshaping what ‘good performance’ means in clinical practice. Across the presentations, one message stood out clearly: AI implementation only works when technical performance, governance, and real-world workflow are considered together.
FROM PRINCIPLES TO PRACTICE: WHAT THE EU AI ACT MEANS FOR RADIOLOGY
Hugh Harvey, Hardian Health, London, UK, emphasised that the EU AI Act (2024) is no longer a future policy question, but a framework already shaping how AI is developed and deployed in radiology. Harvey highlighted how the legislation distributes responsibility across the entire AI lifecycle, from development through to real-world use.
A central component is risk management. Under Article 9, high-risk AI systems must have a risk management system that is established, implemented, documented, and maintained. In practice, this requires developers to embed structured processes within their quality management systems, including assessment of performance in real-world environments, as well as safeguards for data protection, cybersecurity, and adverse event reporting.
Transparency is another key pillar. Article 13 requires developers and distributors to provide deployers with clear and comprehensive information, including
instructions for use, human oversight measures, performance characteristics, technical capabilities, and maintenance requirements. For radiology departments, this ensures that AI tools are not treated as ‘black boxes’, but as systems whose limitations and operational requirements must be understood in clinical context.
Hospitals must also take an active role in ensuring safe and appropriate use
Importantly, Harvey stressed that responsibility does not rest with vendors alone. Article 26 outlines the obligations of deployers, meaning that hospitals must also take an active role in ensuring safe and appropriate use. This includes assigning adequately trained human oversight, monitoring system performance in line with the instructions for use, retaining system logs, and reporting any safety issues to both manufacturers and regulatory authorities.
He also pointed to ongoing efforts to refine how the legislation is implemented
in practice. The proposed ‘digital omnibus’, introduced in November 2025, represents a series of targeted amendments intended to address criticisms of the act and make its requirements more workable for industry and healthcare providers. Among the proposed changes is a shift in responsibility for AI literacy, removing the direct obligation on providers and deployers to deliver training, and instead placing greater emphasis on guidance and support from the European Commission and Member States.
Alongside this, Article 57 introduces regulatory sandboxes at national level, with the prospect of an EU-wide sandbox expected by 2028. Taken together, these developments suggest that while the regulatory framework is already in place, its practical application is still evolving, with increasing focus on balancing oversight, usability, and innovation in clinical AI.
SURVEILLANCE CANNOT STOP AT DEPLOYMENT
While regulation sets the framework, Kicky Gerhilde Van Leeuwen, Romion Health
& Health AI Register, Utrecht, the Netherlands, emphasised that post-market surveillance is what determines whether AI remains safe once it reaches clinical practice. Her presentation focused on a basic, but often neglected question: how do clinicians ensure long-term safety when AI tools are scaled across dynamic healthcare systems?
Van Leeuwen pointed out that many hospitals still validate AI on their own local datasets before use. In the Netherlands, for example, more than 20 out of 70 hospitals have fracture detection tooling, and each tests performance locally first. While understandable, she questioned whether this approach is sustainable. Clinicians would not routinely retest an approved drug or a new CT scanner in every individual hospital population, so why is AI treated differently?
Part of the answer, she suggested, lies in the fact that AI is uniquely sensitive to change. Imaging hardware changes, post-processing changes, algorithms are updated, and patient populations drift over time. This means evaluation cannot be a one-off event. Instead, she described a
continuum that starts with retrospective analysis of available evidence, moves through acceptance testing and piloting in the local workflow, and then continues into post-deployment monitoring.1 That need is especially pressing given the evidence base for commercial tools remains uneven.
Van Leeuwen also highlighted a striking regulatory gap: none of the 13 manufacturers visited by the Dutch Health and Youth Care Inspectorate in 2023/2024 met post-market surveillance requirements. In her view, customer surveys are no substitute for structured monitoring. What matters is measurement across several domains: technical metrics, such as uptime and latency; clinical metrics, such as drift and diagnostic performance; and impact metrics, such as user experience and efficiency. As she put it: “If we want to ensure long-term safety of AI, in a world where the only constant is change, we need post-deployment monitoring.”
WHEN AI CHANGES THE SYSTEM, PEOPLE FEEL IT FIRST
Susan Cheng Shelmerdine, University College London, UK, brought the discussion firmly into the human domain, asking
what happens when radiology embraces AI without accounting for workflow, staff experience, and patient expectations. Using the example of AI-supported lung cancer triage, she showed that the technology initially appeared highly successful. Following implementation, the proportion of patients meeting the national target of 72 hours from abnormal chest X-ray to CT increased from 19.2% to 46.5%, sameday CT rose from 4.0% to 22.1%, and the average time from X-ray to CT fell from 6 days to 3.6 days.2
Yet, this apparent success did not guarantee sustainability. Shelmerdine explained that the pathway was later withdrawn in 2025, illustrating a central lesson of implementation science: adding AI changes the entire system, not just one reporting step. Drawing on the Systems Engineering Initiative for Patient Safety (SEIPS) model, she showed how AI can disrupt relationships between tasks, people, technologies, and organisational processes.3 Early staff feedback reflected this tension. Before deployment, there was cautious optimism, mixed with uncertainty around deskilling, job security, and patient benefit. One month after deployment, feedback turned largely negative, centring on workflow disruption, delays, false
positives, and frustrated patients. By 8 months, views had become more balanced, with staff recognising benefits for same-day CT and patient care, while still calling for better communication and pathway design.4
Ethical AI in radiology is less about whether a tool works in principle and more about whether it can continue to work safely, transparently, and acceptably in practice
This evolution, Shelmerdine argued, reflects the gap between ‘work as imagined’ and ‘work as done’.5 That gap should not automatically be viewed as failure, but as a signal that systems behave differently under real-world constraints. She linked this to what she has previously described as the cycle of over-investment, honeymoon, disinvestment, and eventual reinvestment that often characterises healthcare’s relationship with AI.6
Her presentation also addressed the problem of trust. Clinicians may overtrust, under-trust, or appropriately calibrate their reliance on automation, and those patterns can directly affect
References
1. Antonissen N et al. Artificial intelligence in radiology: 173 commercially available products and their scientific evidence. Eur Radiol. 2026;36(1):526-36.
2. Storey M et al. Early clinical evaluation of AI triage of chest radiographs: time to diagnosis for suspected cancer and number of urgent CT referrals. NEJM AI. 2025;3(1):DOI:10.1056/ AIcs2500539.
3. Carayon P et al. Work system design for patient safety: the SEIPS model.
performance.7 She cited recent evidence suggesting that even when experts are shown detailed feedback about their own performance and an AI system’s strengths and weaknesses, this does not necessarily translate into substantially improved use of AI support.8 For Shelmerdine, the lesson was not that AI should be abandoned, but that responsible implementation must also include responsible withdrawal: clear communication with stakeholders, maintenance of human skills during deployment, and an exit strategy before adoption begins.
CONCLUSION
Taken together, the session suggested that ethical AI in radiology is less about whether a tool works in principle and more about whether it can continue to work safely, transparently, and acceptably in practice. Regulation may define obligations, but it is post-market surveillance and attention to human factors that determine whether those obligations translate into better care. As radiology moves further into AI-enabled practice, success could increasingly depend not on adopting more systems, but on building systems that clinicians, patients, and regulators can realistically live with.
Qual Saf Health Care. 2006;15(Suppl 1):DOI:10.1136/qshc.2005.015842.
4. Togher D et al. Evolution of radiology staff perspectives during artificial intelligence (AI) implementation for expedited lung cancer triage. Clin Radiol. 2025;DOI:10.1016/j. crad.2024.09.010.
5. Hollnagel E, Safety-I and SafetyII: The Past and Future of Safety Management (2014) 1st edition, Oxfordshire: Routledge.
6. Shelmerdine SC. Rethinking our relationship with AI: for better or
worse, richer or poorer? Eur Rad. 2024;DOI:10.1007/s00330-024-11007-9.
7. Parasuraman R, Manzey DH. Complacency and bias in human use of automation: an attentional integration. Hum Factors. 2010;52(3):381-410.
8. Chen C et al. Can domain experts rely on AI appropriately? A case study on AI-assisted prostate cancer mri diagnosis [Internet] (2025) Ithaca: arXiv. Available at: https://arxiv.org/ abs/2502.03482. Last accessed: 26 March 2026.
From Stage to Suite: Enhancing Interventional Radiology with AI and Robotics
Author: Roli B. Omamuli, EMJ, London, UK
Citation:
EMJ Radiol. 2026;7[1]:27-32.
https://doi.org/10.33590/emjradiol/970TBR76
INTERVENTIONAL radiology (IR) is a field where precision, timing, and technical skill converge, making the interventional radiologist comparable to a musician on stage. At the recent European Congress of Radiology (ECR) 2026 session titled ‘The Radiologist as a Performer: How AI Supports the Art of Intervention’, experts explored how augmented reality (AR), virtual reality (VR), robotics, and AI are redefining the art and science that is IR.
OVERLAYING REALITY: AUGMENTED AND VIRTUAL ENVIRONMENTS IN IR
Laetitia Sacenti, Research Fellow at the National Institutes of Health, Bethesda, Maryland, USA, opened the session by framing VR as “an immersive 3D experience though a head-mounted system.” VR replaces the real-world view entirely and has a wide range of applications for physician training, patient rehabilitation, and safety simulations. Simulations can be used to teach students catheterisation and has been shown to improve students’ technical skills.1 This immersive experience is invaluable as it offers a risk-free training environment. However, the benefit is not limited to physicians or those in training, as immersive VR environments may reduce stress during procedures or be used in PTSD exposure therapy.
While VR replaces your entire real-world view with a fully digital environment, AR overlays digital elements onto the real world without replacing it, acting to enhance the real-world image with digital information.2 Saccenti explained that, since radiologists already have 3D medical scan data, creating an AR view of the anatomy in question can be relatively straightforward. In IR, AR is used for 3D visualisation in operating rooms (for example, to help visualise
scatter dose in fluoroscopy to help reduce occupational dose exposure),3 surgical guidance, collaborative work, and patient rehabilitation.
Key technical considerations include accurate registration. Ensuring the digital overlays are perfectly aligned with the real body in the correct position, size, and orientation is important to minimise errors. Another consideration is real-time needle tracking, which keeps the physician aware of the needle tip throughout the procedure. Head-mounted AR systems are hands-free and offer true 3D vision, with the potential for remote team collaboration. Saccenti noted that navigation and guidance systems are most relevant for IR, mainly for image and needle guidance. Early clinical studies demonstrate promising results: Solbiati et al.4 reported high targeting accuracy during AR-guided thermal ablation of 15 liver lesions, achieving complete tumour ablation in all lesions and >90% coverage of a 5 mm periablational margin in 13 of 15 cases, with no intra- or periprocedural complications.
AR is also being implemented on more ubiquitous devices like smartphones and monitors. Saccenti highlighted her team’s work on a 3D-printed smartphone needle guide, which aligns AR overlays with patient anatomy using either 3D models or CT slices.5
Despite the potential of AR, challenges remain that must be addressed before routing clinical adoption, including individual calibration, gesture-based training, precise registration on a moving body, workflow integration, and cost and availability constraints. AI-assisted tools may be the answer to some of these roadblocks for things such as deformable registration, enabling context-relevant information in real time, and enhancing procedural precision.
ROBOTICS: HIGH-PRECISION TOOLS FOR SAFE INTERVENTION
Kornelia Kreiser, Head of Neuroradiology, University Hospital of Ulm, Germany, who also holds an advisory role for Mentice, Gothenburg, Sweden, emphasised that current robotics in IR are better described as a “remote control” or “programmable high-precision tool,” rather than an autonomous robot. This distinction is important, because, while they are programmable and capable of sensing their environment, they require continuous human control and cannot carry out actions automatically.
In non-vascular interventions, such as biopsies and ablations, robotic systems are often table-, floor-, or patient-fixed and can plan needle trajectories with real-time adjustment to tissue movement.6 According to Kreiser, some systems even allow needle manipulation without X-ray guidance, reducing radiation exposure. As Kreiser noted, some of these robotic systems can “specify the precise needle position in terms of the puncture site, depths, and the correct angulation and tilt.”
AI-assisted tools may be the answer to some of these roadblocks for things such as deformable registration
Vascular interventions, by contrast, remain more limited. Procedures require multiple preparatory steps, including sheath insertion, catheter navigation through complex arterial pathways, and manipulation of microcatheters and wires. These are tasks that most current robotic systems cannot fully automate. The dynamic and pulsatile nature of blood vessels, combined with highly variable patient anatomy, may further complicate
robotic control. As Kreiser notes, robotic assistance in vascular IR can improve precision for parts of the procedure, but cannot yet replace the manual skill required for the full intervention.
Newer systems, such as LIBERTY® (Microbot Medical Inc., Hingham, Massachusetts, USA),7 offer disposable, low-cost, single-wire interventions, while SENTANTE™ (Sentante, Kaunas, Lithuania) allows control of multiple devices via a simulator-style interface. LIBERTY® simplifies workflow by reducing the setup to a single arm and a disposable guide, while SENTANTE® allows operators to simulate catheter movements or use a control screen for enhanced precision.
The advantages of robotics in IR are clear: for patients, there is potential for reduced radiation exposure,8,9 shorter procedure times in complex cases, and improved precision. For staff, there is lower occupational radiation exposure due to faster procedures and, therefore, reduced physical strain from heavy lead aprons, as well as minimised human handling errors. Remote control capabilities also open the possibility of tele-interventions, potentially increasing access to procedures in underserved regions and during off-hours, like the da Vinci® (Intuitive Surgical, Inc., Sunnyvale, California, USA) surgical system has done in the last two decades.
Challenges remain, including high costs, logistical complexity, the need for general anaesthesia in most robotic procedures, and limited automation for vascular interventions. Nevertheless, Kreiser envisions a future in which robotic systems could carry out more autonomous steps, such as guiding a catheter from the groin to the carotid artery using imaging data, with integrated sensing to navigate curves and vessel walls safely.
TRANSFORMING THE IR TOOLKIT: AI FOR TRACKING, PLANNING, AND GUIDANCE
Framing IR as a time-dependent discipline, Marco Calandri, Associate Professor of Diagnostic and Interventional Radiology, University of Turin, Italy, described the interventional radiologist as a “performer,” operating not only in space, but in time. Unlike diagnostic radiology, which is largely based on static datasets and retrospective interpretation, IR requires sequential decision-making, real-time adaptation, and precise execution, where outcomes are directly shaped by each procedural step. As Calandri notes, a diagnostic report describes findings, whereas an IR report narrates the procedure, underscoring the importance of timing and progression.
Within this dynamic framework, AI is increasingly redefining the ‘instrument’ of the operator, supporting multiple stages of the interventional workflow. A particularly well-established application is lesion segmentation, where convolutional neural networks and U-Net architectures enable automated identification of tumours and organs at risk. Wasserthal et al.10 demonstrated robust segmentation of over 100 anatomical structures, reducing
standardised volumetric assessment, thereby improving reproducibility across clinical practice and research.
AI is also being applied to procedural planning, particularly in the selection of optimal needle pathways. In a proofof-concept study by Kisting et al.,11 AIgenerated puncture paths for lung biopsy were found to be concordant with expert physician decisions and were considered safe, although prospective validation remains necessary. Despite these promising findings, Calandri suggested that realworld adoption remains limited, placing AI-guided planning in what he described as the “peak of inflated expectations.” In contrast, stereotactic-based planning is a more mature process, less dependent on AI. As demonstrated in the STEREOLAB trial, this approach uses a 3D coordinate system derived from CT or MRI to guide precise probe placement, forming part of a standardised workflow that includes advanced imaging, stereotactic guidance, and ablation confirmation.12
Tracking and navigation represent another critical area, particularly given the challenges of respiratory motion, organ deformation,
and target displacement during procedures. Studies have shown that respiratory phase and motion can significantly impact procedural accuracy and complication rates, highlighting the need for consistent tracking strategies.13 AI offers potential solutions through motion modelling, real-time lesion tracking, and continuous target updating. However, Calandri noted that in many complex interventions performed under general anaesthesia, respiratory motion may be less problematic, and real-time imaging modalities such as ultrasound can already provide effective guidance. Therefore, Calandri positioned the domain of AI tracking closer to the ‘trough of disillusionment’, where technical potential exists, but clinical impact is still being defined.
Beyond tracking, AI is contributing to advanced navigation and trajectory planning through integration with electromagnetic14 and optical systems. These technologies enable features such as collision avoidance, vessel protection, multi-needle coordination, and predictive coverage simulation. While some of these systems are already commercially available, Calandri emphasised the importance of distinguishing truly AIdriven solutions from those based primarily
on optical or electromagnetic control. He also highlighted the need to demonstrate meaningful clinical benefit and long-term financial sustainability.
A further focal development lies in deformable image registration for ablative margin assessment, a critical determinant of local tumour control. In the IAMCOMPLETE study, intraprocedural CT co-registration was feasible in most cases and enabled reproducible margin evaluation, although limitations remained in a subset of patients.15 Work by Lin et al.16 also demonstrated that AI-supported deformable registration not only increases applicability across cases, but also improves predictive performance for residual tumour and 1-year local tumour progression.
Importantly, these technical advances are now translating into clinical outcomes. The COVER-ALL trial showed that AI-based ablation confirmation software significantly increased minimal ablative margins compared with standard assessment (5.9 mm versus 2.2 mm; p<0.0001), with a corresponding trend towards reduction in local tumour progression at 2 years.17 This highlights the potential of AI not only to enhance procedural precision, but also to standardise quality across operators.
Calandri concluded that AI is fundamentally reshaping IR by enhancing the tools available to the operator. However, he cautioned that improved technology does not eliminate the need for expertise: better instruments require expertise, not improvisation. The broader challenge, he suggested, is not simply to enable exceptional individual performance, but to achieve consistent, high-quality outcomes across all practitioners.
Taken together, the perspectives shared by Saccenti, Kreiser, and Calandri illustrate how IR is evolving into a technologically enhanced performance, where visualisation, precision tools, and intelligent systems converge. AR and VR expand how operators perceive anatomy, robotics refines how they act within it, and AI supports decisionmaking across each stage of the procedure. Yet, as these technologies continue to mature, their value will depend not only on technical capability, but on meaningful clinical integration and operator expertise.
As such, the future of IR may not lie in replacing the performer, but in equipping them with increasingly sophisticated instruments to deliver more consistent, precise, and accessible care.
References
1. Mitani H et al. Effectiveness of a virtual reality-based interventional radiology simulator for medical student education. Jpn J Radiol. 2025;43(8):1386-92.
2. Eckert et al. Augmented reality in medicine: systematic and bibliographic review. JMIR Mhealth Uhealth. 2019;7(4):e10967.
3. Troville J et al. A prototype software system for intra-procedural staff dose monitoring and virtual reality training for fluoroscopically guided interventional procedures. J Digit Imaging. 2023;36(3):1091-109.
4. Solbiati L et al. Thermal ablation of liver tumors guided by augmented reality: an initial clinical experience. Cancers (Basel). 2022;14(5):1312.
5. Laetitia S et al. Integrated Needle Guide on smartphone for percutaneous interventions using augmented reality. Cardiovasc Intervent Radiol. 2025;48(7):1042-52.
6. Christou AS et al. Image-guided robotics for standardized and automated biopsy and ablation. Semin Intervent Radiol. 2021;38(5):565-75.
7. Moschovaki-Zeiger O et al. Safety and feasibility study of a novel robotic system in an in vivo porcine vascular model. CVIR Endovasc. 2024;DOI: 10.1186/s42155-024-00425-x.
8. Kim E et al. CT-guided liver biopsy with electromagnetic tracking: results from a single-center prospective randomized controlled trial. AJR Am J Roentgenol. 2014;203(6):W715-23.
9. Püschel A et al. Robot-assisted techniques in vascular and endovascular surgery. Langenbecks Arch Surg. 2022;407(5):1789-95.
10. Wasserthal J et al. TotalSegmentator: Robust segmentation of 104 anatomic structures in CT images. Radiol Artif Intell. 2023;5(5):e230024.
11. Kisting MA et al. Artificial intelligenceaided selection of needle pathways: proof-of-concept in percutaneous lung biopsies. J Vasc Interv Radiol. 2024;35(5):770-9.
12. Paolucci I et al. Study protocol STEREOLAB: stereotactic liver ablation assisted with intra-arterial CT hepatic arteriography and ablation confirmation software assessment. Cardiovasc Intervent Radiol. 2023;46(12):1748-54.
13. Park JY et al. Impact of respiratory phase during pleural puncture on complications in CT-guided percutaneous lung biopsy. J Korean Soc Radiol. 2024;85(3):566-78.
14. Peng M et al. Deep-learning based electromagnetic navigation system for transthoracic percutaneous puncture of small pulmonary nodules. Sci Rep. 2025;15(2547).
15. Hendriks P et al. Intraprocedural assessment of ablation margins using computed tomography co-registration in hepatocellular carcinoma treatment with percutaneous ablation: IAMCOMPLETE study. Diagn Interv Imaging. 2024;105(2):57-64.
16. Lin YM et al. Ablative margin quantification using deformable versus rigid image registration in colorectal liver metastasis thermal ablation: a retrospective single-center study. Eur Radiol. 2024;34(9):5541-50.
17. Odisio BC et al. Software-based versus visual assessment of the minimal ablative margin in patients with liver tumours undergoing percutaneous thermal ablation (COVER-ALL): a randomised phase 2 trial. Lancet Gastroenterol Hepatol. 2025;10(5):442-51.
ECR 2025
Abstract Reviews
Based on highlights from the European Congress of Radiology (ECR) 2026, these abstract reviews showcase advances in AI for diagnostic imaging, innovations in MRI techniques, evolving approaches to cancer care, and developments in radiography education. Together, they reflect key research priorities and technological trends shaping the future of imaging practice and patient-centred care.
AI or Radiologist Interpretation for Prostate Cancer Diagnosis
Authors: *Alexander B.C.D. Ng,1,2 Aqua Asif,1,2 Aishwarya R. Shah,1,2 Alexander Dudko,1,2 Ranya Kumar,1,2 Pawel Rajwa,1,2 Doug Pendse,3 Veeru Kasivisvanathan1-4
1. Division of Surgery and Interventional Science, University College London, UK
2. Centre for Urology Imaging, Prostate, AI and Surgical Studies (COMPASS) Research Group, University College London, UK
3. Department of Radiology, University College London Hospitals NHS Foundation Trust, UK
4. Department of Urology, Comprehensive Cancer Center, Medical University of Vienna, Austria *Correspondence to alexander.ng@ucl.ac.uk
Disclosure: The authors disclose that the PARADIGM trial is supported by The John Black Charitable Foundation, the National Institute for Health and Care Research, the European Association of Urology (EAU) Research Foundation, and Hadyn Cunningham. Ng is supported by the NIHR through a Doctoral Fellowship, outside of the submitted work. Asif is supported by the NIHR through an Academic Clinical Fellowship, outside of the submitted work.
Following the PRECISION trial, prostate multiparametric MRI has been adopted as the first-line investigation for suspected prostate cancer internationally.1 However, international data demonstrates that, due to resource limitations, not every patient who requires a pre-biopsy MRI has been receiving one. The PRIME trial has recently demonstrated the non-inferiority of biparametric MRI to multiparametric MRI for clinically significant prostate cancer detection,2 and this is a step towards allowing more men to be scanned with existing resources.
With the global incidence of prostate cancer predicted to double in the next 20 years,3 the potential adoption of biparametric MRI,2 and the introduction of national MRI screening programmes,4 the demand for prostate MRI is set to rise substantially. Interpretation, however, has a steep learning curve, with optimal performance achieved by expert
genitourinary radiologists.5 With a rising demand for medical imaging and a projected 40% radiologist shortfall by 2027,6 a prompt international solution is warranted.
PARADIGM aims to evaluate whether AI is non-inferior to radiologists in detecting clinically significant prostate cancer (Gleason Grade Group ≥2).7,8
METHODS
PARADIGM is an international, prospective, multicentre, non-inferiority, within-patient, level 1 evidence diagnostic study. Five hundred men will be recruited over 18 months. These men will undergo standard of care MRI with either 1.5 or 3.0 T and at least a pelvic phased array coil. The radiologist and a primary AI algorithm will report the MRI, blinded from each other. The radiologist will then be unblinded and produce a merged report, with the ability to overrule AI findings for safety. Suspicious lesions identified by either AI or the radiologist will undergo targeted biopsies, with optional perilesional and/or systematic biopsies. The primary outcome is the proportion of men with clinically significant cancer. Planned secondary outcomes include the proportion of men with clinically insignificant cancer (Gleason Grade Group 1), test performance characteristics of AI and radiologists, and health economics analysis.
RESULTS
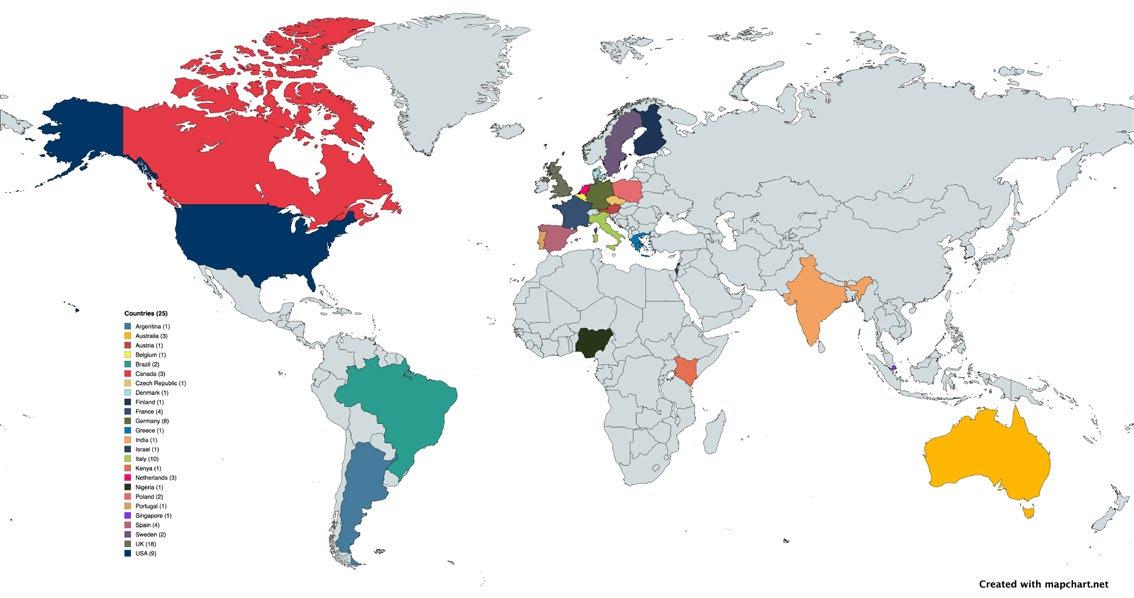
Eighty-one centres from 25 countries (six continents) have expressed an interest in taking part and are undergoing pre-trial MRI quality control (Figure 1). PARADIGM will open to recruitment in October 2026.
CONCLUSION
PARADIGM will provide the first prospective, Level 1 evidence on the diagnostic performance of AI in the detection of clinically significant prostate cancer on MRI.
Figure 1: Eighty-one centres from 25 countries and six continents have expressed interest in taking part in the PARADIGM trial.
References
1. Kasivisvanathan V et al.; PRECISION Study Group Collaborators. MRI-targeted or standard biopsy for prostate-cancer diagnosis. N Engl J Med. 2018;378(19):1767-77.
2. Ng ABCD et al.; PRIME Study Group Collaborators. Biparametric vs multiparametric mri for prostate cancer diagnosis: the prime diagnostic clinical trial. JAMA. 2025;334(13):1170-9.
3. James ND et al. The Lancet commission on prostate cancer: planning for the surge in cases. Lancet. 2024;403(10437):1683-722.
4. Burki T. Prostate Cancer UK launches the TRANSFORM trial. Lancet. 2024;403(10438):1738.
5. de Rooij M et al. ESUR/ESUI consensus statements on multi-parametric MRI for the detection of clinically significant prostate cancer: quality requirements for image acquisition, interpretation and radiologists’ training. Eur Radiol. 2020;30(10):5404-16.
6. The Royal College of Radiologists. Clinical radiology census reports. Available at: https://www.rcr.ac.uk/ news-policy/policy-reports-initiatives/clinicalradiology-census-reports/. Last accessed: 29 February 2024.
7. Ng ABCD et al. Artificial intelligence or radiologist interpretation for prostate cancer diagnosis. Abstract 21227. ECR, 4-8 March, 2026.
8. Ng ABCD et al. Artificial intelligence in prostate cancer diagnosis on magnetic resonance imaging: time for a new PARADIGM. Eur Urol. 2025;88(1):4-7.
Focal Cortical Dysplasia Type IIb: Correlation of Histological Data with Typical MRI Patterns During Epileptological Scanning
Resistant epilepsies account for approximately 30% of all forms of epilepsy, particularly in patients with focal seizures.1,2 One of the main causes of therapyresistant focal epilepsies is focal cortical dysplasias (FCD), which is attributed to abnormal cortical development. Among all abnormalities of cortical development, FCD in surgically treated children amounts to 75%. Among the various variants of FCD, FCD Types Ia and IIb are the most common. FCD Types Ib, Ic, and IIa are extremely rare.2,3 The transmantle sign (TMS) is considered a characteristic feature for visualisation of FCD IIb.4,5 In this study, the authors sought to answer the following questions: is Type IIb FCD always accompanied by a TMS, and will this finding be characteristic of other types of FCD? The aim was to assess the concordance between typical MRI patterns and histologically confirmed FCD IIb, and to determine the diagnostic value of these imaging features.
MATERIALS AND METHODS
The study included 93 patients who had undergone surgery for FCD.6 Based on histopathological examination, all patients were divided into two groups (minimum age in both groups was 3 years): Group 1 with Type I FCD (37 cases) and Group 2 with Type IIb FCD (56 cases). All patients underwent preoperative MRI on 3T scanners using the HARNESS protocol and highresolution T2-weighted sequences (slice thickness 0.6 mm), with an emphasis on identifying cortical abnormalities such as the TMS, cortical thickening, blurred grey-white matter boundary, and increased signal from the subcortical white matter.
RESULTS
As a result of assessing the TMS of interest, the authors identified the following relationships. TMS was detected on MRI in 36 of 56 patients with FCD Type IIb (64.3%; 95% CI: 50.9–76.0%) and in none of the patients with FCD Type I. Demographic data showed a mean age of 17.2±6.4 years in the FCD IIb group (range: 3–32 years), and 57.1% females; and a mean age of 19.5±7.2 years (range: 3–35 years) in the FCD I group, with 51.4% females. The difference between groups was statistically significant (Fisher’s exact test; p<0.0001). Sensitivity was 64.3% and specificity was 100%, with a positive predictive value of 100%, and a negative predictive value of 65.5% (Figure 1).
CONCLUSION
The TMS demonstrates high specificity (100%) for identifying FCD IIb, with statistically significant differences between FCD IIb and FCD I groups (p<0.0001; Fisher’s exact test). However, its moderate sensitivity (64.3%) indicates substantial limitations in the diagnostic value of this marker.
Condition before surgery (A) and after surgery (B). The transmantle symptom was not visualised before surgery. The data were confirmed histologically (C) and immunohistochemically (D, E). C) Accumulation of pathological forms of neurons surrounded by fibrous gliosis, staining with haematoxylin and eosin. D) Balloon cells, vim expression. E) Dysmorphic neurons, expression of neurofilaments.7
References
1. Smirnova A et al. Focal cortical dysplasia IIb type: correlation of histological data with typical MRI patterns during epileptological scanning. Abstract. ECR, 4-8 March, 2026.
2. Blümcke I et al., Surgical Neuropathology of Focal Epilepsies: Textbook and Atlas (2015) Paris: John Libbey Eurotext, p158.
3. Mukhin KY. [Focal cortical dysplasias: clinical and electro-neuroimaging characteristics]. Russian Journal of Child Neurology. 2016;11(2):8-24. (In Russian).
4. Kimura Y et al. Radiologic and pathologic features of the transmantle sign in focal cortical dysplasia: the T1 signal is useful for differentiating subtypes. AJNR Am J Neuroradiol. 2019;40(6):1060-6.
5. Padmanaban V et al. Transmantle focal cortical dysplasia in a patient with drug-resistant epilepsy. BMJ Case Rep. 2022;15(3):e243983.
6. Hom KL et al. Application of preoperative MRI lesion identification algorithm in pediatric and young adult focal cortical dysplasia-related epilepsy. Seizure. 2024;122:64-70.
7. Metodiev D et al. Pathomorphological diagnostic criteria for focal cortical dysplasias and other common epileptogenic lesions-review of the literature. Diagnostics (Basel). 2023;13(7):1311.
Figure 1: Focal cortical dysplasia Type IIb of the right frontal lobe.
Evaluating the Use of Complementary Therapies Amongst Patients Undergoing Radiotherapy in Malta
Authors: Amy Xuereb,¹ *Karen Borg Grima²
1. Radiotherapy Department, Sir Anthony Mamo Oncology Centre, Msida, Malta
2. Radiography Department, University of Malta, Msida, Malta
*Correspondence to karen.borg-grima@um.edu.mt
Disclosure: The authors declare no conflicts of interest. Ethical permission for this study was sought and received from the Faculty of Health Science Research Ethics Committee (FREC) and the University Research Ethics Committee (UREC).
Cancer is a complex and life-altering disease that imposes significant multidimensional effects, adversely influencing patients’ physical health, emotional wellbeing, and psychological functioning.1,2
Complementary therapies (CT) are increasingly being explored by patients with cancer to help manage treatment-related symptoms and improve overall wellbeing.3 CTs can be used alongside conventional cancer treatment to improve quality of life.4 Despite their growing popularity, patients’ awareness of available CTs in Malta and knowledge informing their willingness to utilise such services is still very limited. The use of CTs may vary depending on several factors, including demographic characteristics such as gender, educational level, or age.
Understanding these aspects is important for healthcare professionals when considering the integration of supportive care services within oncology settings. Therefore, this study was designed to address
three primary objectives: (1) to determine whether patient demographic characteristics influence the utilisation of CTs; (2) to investigate patients’ awareness of CTs available locally; and (3) to evaluate patients’ willingness to utilise these locally available CTs.
MATERIALS AND METHODS
This study employed a cross-sectional, non-experimental, prospective descriptive design. A self-designed questionnaire incorporating primarily quantitative items with limited qualitative components was distributed to 140 eligible participants, defined as adult patients undergoing radical radiotherapy. A total of 91 questionnaires were completed and included in the analysis, yielding a response rate of 65%. Data were processed and analysed using IBM SPSS® Statistics version 27 (IBM, Armonk, New York, USA).
Statistical analyses included χ2, Kruskal–Wallis, and Friedman tests, used to assess any associations between variables. Statistical significance was set at p<0.05.
RESULTS
Findings from this study revealed that more than half of the respondents who reported prior use of CTs were female (57.8%). In addition, CT utilisation was most commonly reported among younger patients aged 18–47 years (76.9%). Participants with tertiarylevel education also demonstrated the highest use of CTs (82.6%).
Overall, 88% of respondents reported awareness of at least one CT. The most frequently identified therapies were massage (68.1%), followed by yoga (58.2%), dietary supplements (46.2%), and meditation (46.2%).
The majority of participants (95.6%) indicated that they would be willing to utilise CTs if these were
provided free of charge within the hospital setting. Analysis using the Friedman test indicated the strongest agreement with statements, suggesting that a wider range of CTs should be available in Malta (mean score: 4.27) and that greater patient education regarding these therapies is required prior to their use.
CONCLUSION
The findings demonstrate high awareness of CTs and a strong willingness amongst patients to utilise these services if made available within the state oncology hospital. CT use was more common among younger and more highly educated patients, and participants expressed support for greater availability of these therapies in Malta. These findings highlight the potential value of integrating CTs into oncology services while improving patient education
to support informed use. Radiographers can lead patient informed discussions and contribute to holistic, supportive care pathways by aiding to integrate CTs in a safe and evidence-based practice.
References
1. Borg Grima K, Xuereb A. Evaluating the use of complementary therapies amongst patients undergoing radiotherapy in Malta. Abstract. ECR 2026, 4-8 March, 2026.
2. World Health Organization (WHO). Cancer. 2024. Available at: https://www.who.int/news-room/ fact-sheets/detail/cancer. Last accessed: 13 March 2026.
3. Keene MR et al. Complementary and alternative medicine use in cancer: a systematic review. Complement Ther Clin Pract. 2019;35:33-47.
4. Mentink M et al. The effects of complementary therapies on patient-reported outcomes: an overview of recent systematic reviews in oncology. Cancers. 2023;15(18):4513.
Global Classrooms: Virtual Exchange Strengthens Students' Ethical and Patient Safety Competence
Authors: *Bodil T. Andersson,1 Jenny Gårdling,1 Henra Muller,2 Ida-Keshia Sebelego2
1. Lund University, Sweden
2. Central University of Technology Free State, Bloemfontein, South Africa
*Correspondence to bodil-t.andersson@med.lu.se
Disclosure: Andersson has received support for attending meetings and/or travel from Lund University Department of Health Sciences; and holds an unpaid leadership or fiducial role in the Swedish Society of Radiographers. The other authors have declared no conflicts of interest.
Keywords: Cross-cultural learning, ethics of care, patient safety, radiography education, virtual exchange, virtual module.
In response to growing calls for the internationalisation of radiography education, a sustained biennial virtual exchange was established in 2022 between radiography programmes at Lund University, Sweden, and the Central University of Technology, South Africa. This collaboration, bridging nearly 10,000 kilometres, was designed to prepare students for global professional practice by exposing them to different healthcare contexts while highlighting shared professional values. In this study, the authors evaluated students’ perceptions of these virtual collaborations, which focus on two core annual sessions: ‘Patient Safety’ for second-year students and ‘Ethics of Care from a Global Perspective’ for first-year students. These topics were deliberately chosen as they represent universal challenges in radiography practice, transcending geographical and cultural boundaries.
AIM
The aim of the study was to evaluate radiography student’s perceptions of an educational virtual class collaboration between a South African and Swedish university.1
METHODS
Following the 2024 virtual class collaboration, during which students participated in mixed-country breakout groups for structured discussions, a crosssectional online survey was administrated using QuestionPro (QuestionPro Inc., Austin, Texas, USA). A total of 168 undergraduate students (88 first-year students and 80 second-year students) completed a nineitem instrument combining quantitative fivepoint Likert Scale questions on technical issues, participation, enjoyment, and learning outcomes with two open-ended items capturing qualitative insights and suggestions for improvement.
RESULTS
Quantitative findings showed positive responses across all measured domains: 92% reported enjoyment of the virtual format, 89% felt actively engaged in the discussions, 94% affirmed the sessions’ relevance to their curriculum, and 96% valued the cross-cultural learning aspect. Technical issues were reported as minimal.
Qualitative responses provided rich context for these numerical findings. Students highlighted shared professional values across continents, noting that ‘patients are prioritised everywhere’. Others highlighted the importance of diverse perspective and being ‘exposed to different kinds of ideas’. Additional responses emphasised the discovery of ‘common things in diagnostics’, reinforcing that the radiography profession shares fundamental principles globally. Breakout rooms discussions were described as making
complex topics like ethics of care ‘more plausible’ through active dialogue. Engaging with peers from a different part of the world, yet within the same faculty, was considered ‘an exceptional experience’ because both universities teach ‘practically the same curriculum’. This discovery of common ground was repeatedly cited as a highlight.
CONCLUSION
The identified challenges centred on logistical issues, including occasional noise disruptions in some breakout rooms at the South African venue and a clear need for smaller groups to facilitate more balanced participation. Several students noted that the students from the Lund University were often more vocal than their South African counterparts, suggesting that cultural differences in classroom participation styles warrant attention in future iterations. Students specifically requested more time for discussion and smaller group sizes
to enable deeper engagement with their international peers. Overall, this virtual exchange successfully promoted global knowledge exchange and strengthened understanding of shared ethical values and patient safety principles, demonstrating that virtual classroom collaborations are a valuable, scalable tool for internationalising radiography education2 and preparing students for a globally connected professional future.1,3
References
1. Andersson BT et al. Global classrooms: virtual exchange strengthens students' ethical and patient safety competence. Abstract. ECR 2026, 4-8 March, 2026.
2. Lai C et al. The growing importance of internationalization in radiography education. J Med Imaging Radiat Sci. 2019;50(2):193-4.
3. Kay M, Brogan K. The perceptions and experiences of final year undergraduate diagnostic imaging students when facilitating peer-assisted learning within the simulated learning environment. Radiography. 2024;30(Suppl 2):138-42.
Deep Learning Amplifies the Benefits of High Relaxivity in Brain MRI: A Quantitative Assessment of a Contrast Boosting Algorithm Using Gadopiclenol
1. Subtle Medical Inc., Menlo Park, California, USA
2. Bracco Imaging, Turin, Italy
3. MRI Department, Na Homolce Hospital, Prague, Czechia
*Correspondence to srivathsa@subtlemedical.com
Disclosure: Pasumarthi Venkata, holds stock or stock options in Subtle Medical Inc; and is an employee of Subtle Medical Inc. Colombo Serra is an employee of Bracco Imaging. Vymazal has been a consultant for Bracco Imaging; received a research grant from the Ministry of Health (Czechia); consulting fees from Bracco Imaging and GE HealthCare; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Bracco Imaging and GE HealthCare; support for attending meetings and/or travel from Bracco Imaging; and is a member of the Scientific Board at Charles University, Prague, Czechia. Shankaranarayanan holds stock options in Subtle Medical Inc; and is an employee of Subtle Medical Inc.
Acknowledgements: All patients signed an informed consent form with their approval to use their anonymised data for educational and scientific purposes.
Keywords: Contrast boosting, deep learning (DL), gadopiclenol, gadolinium-based contrast agent (GBCA), high relaxivity.
Gadopiclenol is a high-relaxivity gadoliniumbased contrast agent (GBCA) that enables reduced contrast doses while preserving lesion conspicuity. In parallel, deep learning (DL)-based contrast boosting algorithms have been developed to enhance contrast signals in post-contrast MRI without increasing gadolinium administration. The purpose of this study1 was to quantitatively assess whether a DL-based contrast boosting algorithm can further amplify the benefits of a high-relaxivity GBCA,
improving lesion visualisation and image quality at reduced dose levels in brain MRI.
METHODS
This retrospective study included T1weighted pre-contrast and standard postcontrast MRI examinations from 20 patients undergoing brain MRI, comprising both 2D and 3D acquisitions. All patients were administered gadopiclenol at a reduced approved dose of 0.05 mmol/kg. Precontrast and standard-contrast (SC) images were processed using an FDA-cleared DL-based contrast boosting algorithm to generate contrast-boosted (CB) images. Regions of interest were manually drawn on the largest contrast-enhancing lesion and on adjacent healthy brain parenchyma. Regions of interest defined on SC images were propagated to pre-contrast and CB images through image registration. Quantitative image quality and lesion conspicuity were assessed using contrastto-noise ratio, lesion-to-brain ratio, and contrast enhancement percentage (CEP), with CEP calculated relative to pre-contrast images. Mean values and percentage increases from SC to CB images were computed. In addition, the performance of CB images obtained with gadopiclenol was compared with previously reported CB results using a conventional macrocyclic GBCA (gadoterate meglumine) administered at 0.1 mmol/kg.
RESULTS
Contrast-boosted images demonstrated a marked improvement across all quantitative metrics compared with standard postcontrast images. Mean contrast-to-noise ratio increased from 2.52±0.85 in SC images to 10.38±1.56 in CB images. Mean percentage increase result to be equal to a 314.19% increase. Mean lesion-to-brain ratio improved from 2.55±1.85 to 5.12±1.03. Mean percentage increase result to be equal
to a 118.12% increase. Mean CEP nearly doubled, increasing from 0.99±0.28 in SC images to 1.96±0.35 in CB images. Mean percentage increase result to be equal to a 335.18% increase. Comparative analysis indicated that the percentage increases achieved with gadopiclenol combined with CB are comparable to those observed for gadoterate meglumine at standard dose,2 also showing a noticeable amplification when CB is applied to a high-relaxivity contrast agent.
CONCLUSION
Quantitative analysis demonstrates that the DL-based contrast boosting algorithm significantly enhances lesion conspicuity
and image quality when used in combination with gadopiclenol at a reduced dose. The observed increase in contrast enhancement suggests that CB images obtained with 0.05 mmol/kg gadopiclenol are quantitatively comparable to a doubled contrast dose (Figure 1). These findings support the synergistic use of high-relaxivity contrast agents and DLbased contrast boosting as a strategy for gadolinium dose reduction while maintaining or improving diagnostic performance.
LIMITATIONS
This study is limited by a relatively small sample size and its retrospective design.
Figure 1: Representative axial T1-weighted brain MRI showing pre-contrast (left), standard post-contrast images acquired with gadopiclenol at 0.05 mmol/kg (centre), and deep learning–based contrast-boosted images (right).
The enhancing lesion (red square) is more clearly visualised on contrast-boosted images, with improved conspicuity and delineation compared with standard post-contrast imaging.
References
1. Pasumarthi Venkata S et al. Deep learning amplifies the benefits of high relaxivity in brain MRI: a quantitative assessment of a contrast boosting algorithm using gadopiclenol. Abstract 21892. ECR, 4-8 March, 2026.
2. Pasumarthi Venkata S et al. Deep-learning based contrast boosting improves lesion visualization and image quality: a multi-center multi-reader study on clinical performance with standard contrast enhanced MRI of brain tumors. medRxiv. Preprint doi: https://doi.org/10.1101/2025.06.12.25329347.
Congress Interviews
In these exclusive interviews from the European Congress of Radiology (ECR) 2026, radiology leaders reflect on a Congress marked by collaboration, education, and a shift from innovation to real-world implementation. They highlight how AI is becoming embedded in clinical workflows, alongside advances in imaging that are enhancing diagnosis, prevention, and personalised care. Key themes include multidisciplinary integration, AI readiness, and the growing role of radiology as a strategic, patient-centred discipline driving more effective and equitable healthcare.
Q1Congratulations on such a successful congress! Now that the European Congress of Radiology (ECR) 2026 has concluded, what do you consider its most defining achievements? Were there particular discussions or developments that, in your view as President, best captured the current state of radiology in Europe and beyond?
Looking back, I believe that ECR 2026’s most defining achievement was that it truly lived up to its theme, ‘Rays of Knowledge’. We saw an exceptional level of scientific engagement with a record number of abstracts, well over 11,000, submitted for the Congress. We also know that we had over a 9% increase in the number of participants compared to the previous year, and all of this reflects the vitality of our field and the global willingness to share knowledge across borders.
Perhaps just as importantly, we placed education at the centre of the meeting. This was done through hands-on workshops, the new subspecialty on stage format, broad access through digital ondemand learning, and new types of engaging educational sessions. This combination of scientific excellence and educational accessibility is one of the clearest signs of a healthy, forward-looking radiology community.
What also really impressed me, because this stood out very clearly, was the maturity of the conversations around AI, because, at ECR 2026, AI was not presented as something abstract or futuristic, but increasingly as something that must prove its value in real clinical workflows. This was visible in the AI Theatre, in the Pixel Pandemonium, and in the AI workflow guided tours, and really captures where radiology stands today. So, it's not
about asking whether AI will arrive, but how we implement it responsibly and effectively, in a way that really supports radiologists and improves patient care.
Perhaps the third defining achievement is the way the Congress highlighted the expanding role of radiology far beyond interpretation alone. We had the inaugural on Alzheimer's Day, which was extremely meaningful, because it showed how central imaging has become in early diagnosis, treatment selection, and longitudinal monitoring, at a time when we have new diseasemodifying therapies that are changing all the clinical pathways. Also, the discussions we had about the European Cardiovascular Health Plan underlined the growing role of radiology in prevention, early detection, and multidisciplinary public health strategy. I believe that what ECR 2026 clearly
showed is that radiology is entering a new phase, where we are more connected to patients, more integrated with other specialties, more shaped by intelligent technologies, and more committed than ever to education as the foundation of our progress.
Q2 The theme ‘Rays of Knowledge’ positioned imaging as a source of clarity, integration, and progress in patient care. In hindsight, how successfully do you feel the Congress translated this into tangible learning and collaboration? Were there moments where the theme resonated especially strongly?
Looking back, I really feel that the theme, ‘Rays of Knowledge’, was truly brought to life throughout the Congress, because it was visible, not only in the scientific programme, but also in the
way people learned from each other across subspecialties, disciplines, and borders. There was a real sense that radiology is becoming an even stronger connecting force in patient care, and what resonated especially for me were the moments where imaging was shown as a bridge between technology and clinical practice, a bridge between radiologists and other specialties, and perhaps, ultimately, between knowledge and better outcomes for patients. For me, this is exactly what ‘Rays of Knowledge’ was meant to express: clarity, collaboration, and progress in action.
Q3
AI was another main theme this year, especially in the In Focus programme, ‘The Art of Artificial Intelligence in Clinical Practice’. After hearing the debates and practical examples presented in Vienna, Austria, how would you describe the state of AI integration in everyday radiology? What practical, regulatory, or educational steps are now required for it to become standard practice?
I came away from Vienna feeling genuinely optimistic. What this year’s ECR showed very clearly is that AI and radiology have moved beyond this purely experimental stage, but it is not yet routine everywhere. The debate, as I mentioned earlier, was much more mature this year; it was less about hype and much more about where AI truly adds value in clinical care. For example, we looked at everything, from screening and oncologic follow-up, to ethics, bias regulation, and the AI workflow guided tours. They showed very concrete cases, such as mammography workflows with AI-based work list prioritisation,
integrated reporting, and chest screening workflows. To me, this is the key message: AI is no longer just a side conversation in radiology; it is becoming part of the workflow, but in a careful, targeted, very clinical way.
For AI to become standard practice, three things now matter most, in my opinion. Firstly, on a practical level, systems must integrate smoothly into everyday reporting environments and support radiologists rather than interrupt them. Secondly, on a regulatory level, we need clarity and trust, and the European Society of Radiology (ESR) has rightly highlighted AI literacy, data governance, transparency, human oversight, alignment with medical device regulations, clear responsibilities for deployers, regulatory sandboxes, and strong post-market monitoring as essential foundations for a safe implementation under the European AI Act. Thirdly, on an educational level, AI literacy must now become an integral part of routine professional training, so that radiologists understand not only what these tools can do, but also their limitations.
In other words, if we get these three pillars right, workflow, regulation, and education, then I believe that AI will move from promising innovation to dependable daily practice. Q4
As a radiologist whose expertise revolves largely around the head and neck, did you observe any notable scientific or technological shifts presented this year that may influence head and neck imaging in the near future?
It is a sort of a consensus that head and neck imaging is becoming both more precise
and more practical at the same time. We saw, for example, strong signals around AI-supported analysis and radiomics, including work on outcome modelling, and much more. We're now focusing much more on the impact of imaging on treatment and outcomes. For example, in oropharyngeal cancer, there were also presentations about schwannomas and the impact of imaging on response to treatment, automatic body composition biomarkers from routine CT, and longitudinal Neck Imaging Reporting and Data System (NI-RADS)-based followup for recurrence risk. All of this suggests a near future in which our reports will be increasingly structured, prognostic, and much better integrated in therapeutic decisions, from the reporting point of view.
In terms of the technology side, development stood out; faster MRI through deep learning reconstructions, with reported scan time reductions of up to 50–70%, without loss of diagnostic image quality. Then, photoncounting CT was presented as improving visualisation of the temporal bone and sinonasal imaging, with important attention also paid to radiation doses
Taken together, all of these advantages point to head and neck imaging becoming faster, sharper, and more clinically impactful. I would say that the direction is really encouraging. We're moving towards better characterisation, better follow-up, and, ultimately, more personalised care for our patients.
Q5
ECR has long emphasised radiology’s central role across oncology, emergency medicine, neurology, cardiology, and beyond. How did this year’s Congress strengthen interdisciplinary dialogue in a meaningful way, and how will radiology continue to position itself not as a service specialty, but as a strategic clinical partner?
Radiology will continue to move beyond the idea of being just a simple service specialty
This year's Congress definitely strengthened the interdisciplinary dialogue in a very practical way. We not only had the wellknown ConnAction sessions, 11 scientific sessions dedicated specifically to radiologyconnecting disciplines, but this multidisciplinary spirit was also visible in many other meetings. We had multidisciplinary discussions on lung cancer, Alzheimer's disease, and cardiovascular prevention. We had new formats, such as ‘From Symptom to Diagnosis’, which were new multidisciplinary sessions, and the entire series of radiologic-pathologic correlation. These were not abstract conversations, but they showed radiologists working side by side with other clinical partners. I consider radiology to be a clinical discipline, as I mentioned in my opening ceremony, and that radiologists should be part of multidisciplinary clinical teams, working side by side with other
clinical partners on diagnosis, treatment pathways, and followup. This is the future, and it has already started.
Radiology will continue to move beyond the idea of being just a simple service specialty by being even more present, to the point where clinical decisions are shaped more actively in these multidisciplinary teams, and are more clearly focused on outcomes, not just on imaging. This is where the strategic value of radiology is strongest, and this year's ECR already showed that this shift is well on the way.
Q6
As you close the chapter on ECR 2026, what key insights or responsibilities will the ESR carry forward into the coming year? Where should the radiology community now focus its energy to translate this year’s ‘Rays of Knowledge’ into measurable improvements in patient care?
As we close this chapter on ECR 2026, I think that the ESR carries forward a very clear responsibility, namely, to turn inspiration into implementation. ‘Rays of Knowledge’ placed education at the centre of the Congress, and now we need to help radiology teams to translate what was discussed in Vienna into daily practice through accessible learning on ESR Connect, stronger training standards, and continued support for multidisciplinary imaging.
It also means that keeping quality and safety is very important. We have to keep it firmly in our focus, because the real progress is measured not only by innovation, but by better and more consistent care over longer periods of time for our patients and driving results, not just discussing care at congresses.
So, where should the community focus its energy? Above all, I think of areas where radiology can make a measurable difference quickly: earlier diagnosis, better follow-up in fields such as neurodegeneration, more active involvement in prevention, clinical decision-making, and responsible integration of AI into routine workflows. The ESR has already outlined the key foundation for that with AI literacy, data governance, transparency, human oversight, and post-market monitoring. I think that if we combine these principles with the collaborative spirit that we saw at the ECR 2026, then this year's ‘Rays of Knowledge’ can become something very concrete: faster diagnosis, smarter pathways, and better outcomes for patients across Europe and beyond.
Q7
Planning for ECR 2027 will already be underway. Based on the momentum generated this year, where do you anticipate the most meaningful shifts in European radiology over the next 12 months? Are next year’s key themes already beginning to take shape?
I think perhaps the most meaningful shift over the next 12 months will be from discussion to implementation. ECR 2026 shows where this momentum now lies: practical AI in clinical workflows, a stronger role for imaging in prevention, screening, and a deeper collaboration with our clinical partners in areas such as oncology, neurodegeneration, and cardiovascular health. This is where European radiology can make its next measurable leap for patients.
ECR 2027’s theme, ‘Healthcare Reimagined: Updating the Role of Radiology’, also makes this direction clear. I would expect the coming year to focus on redefining radiology as a more visible, clinical, strategic, and data-driven partner in patient care, with topics such as practical integration of AI into radiology, workflows, redesign, governance, and trust. With the 2027 programme already underway under Matthias Prokop, Radboud University Nijmegen, the Netherlands; and Marie Pierre Revel, Hôpital Cochin, Université Paris Cité, France, the next chapter is clearly beginning to take shape.
Patrizia Cornacchione President, European Federation of Radiographer Societies (EFRS); Assistant Professor, Università Cattolica
A year after we last spoke and with another year’s experience of European Federation of Radiographer Societies (EFRS) presidency, what has changed for radiographers in Europe?
Over the past year, I have seen a clearer shift towards recognising radiographers as clinical professionals who influence outcomes, not only image acquisition. In many departments, radiographers are increasingly involved in protocol optimisation, quality assurance activities, and service improvements that directly affect patient safety and diagnostic quality.
I also sense a stronger European mindset: radiographers are more willing to compare practice across borders, learn from other systems, and build shared approaches. That matters because the challenges are similar everywhere, with fast technological change and rising expectations for quality and patient-centred care. The more we learn together, the faster we reduce variability and improve standards.
Q2 The European Congress of Radiology (ECR) 2026 is themed ‘Rays of Knowledge’, emphasising connection and learning. What does this theme mean for the radiography community?
For radiographers, ‘Rays of Knowledge’ is both literal and symbolic. We work with ‘rays’, but knowledge is what turns technology into safe, consistent, and compassionate care. The theme also highlights connection: knowledge must travel between professions, countries, and
generations, otherwise it stays isolated and its value is limited.
In practical terms, I would translate the theme into measurable improvements in three areas: safety culture, diagnostic quality, and patient experience.
Q3
Radiographers’ visibility at ECR continues to grow across both the main programme and the EFRS programme. What is driving this growth, and why does it matter now?
The growth is driven by reality: radiographers’ roles are evolving and ECR is reflecting that evolution. Radiographers are contributing more actively to research, education, workflow redesign, and the responsible integration of new technologies, such as AI. At the same time, imaging has become more explicitly interdisciplinary; quality and safety are team outcomes, and radiographers are central to that. Why it matters now is simple: the pace of change is high, and the profession needs a strong European platform to share evidence, develop competencies, and build a common language.
Q4
Radiographer registration numbers have increased again postpandemic. What factors do you think are driving radiographers back to ECR?
I don’t think people are just returning to in-person events. They are coming back because the professional needs have intensified. Departments are under pressure, innovation cycles are faster, and many radiographers are looking for
clarity: what skills should I prioritise, what is safe practice, how do we implement change without compromising quality?
Q5
AI is prominently featured at ECR 2026, and you are co-chairing the session on the clinical use of AI by radiographers. What practical or strategic messages do you hope participants will take away?
My first message is that AI is not just a tool, it is a workflow change. It can improve consistency and efficiency, but only when it is integrated with clear governance and accountability. Radiographers should understand what the AI system is designed for, what it needs as input, what it produces as output, and how failures may look in real clinical scenarios.
Second, radiographers must be involved from the start: selection, implementation, training, and monitoring. Radiographers are often the first to identify
acquisition issues, artefacts, and mismatch between a patient’s reality and an algorithm’s assumptions. That makes radiographers essential to safe integration.
Q6
How can radiographers move beyond being users of AI tools to becoming critical decision-makers who ensure these technologies genuinely enhance patient outcomes?
Moving beyond ‘users’ begins with culture. That includes recognising when an output does not fit the patient, pausing the workflow, and escalating appropriately. That is patient safety leadership.
Then, we need structured expertise built on knowledge, skills, and competences: basic AI literacy, awareness of bias and limitations, and practical checklists to support safe and responsible use.
Q7
EFRS is often described as a bridge for the radiography community. How does EFRS help connect people and ideas so that successful approaches can be adopted across countries and settings?
EFRS is a bridge in several ways. First, between national societies and universities, a shared European vision, helping local strengths become collective progress. Second, between students, early-career professionals, and experienced colleagues, so knowledge and leadership are transferred, not lost. Third, between radiographers and the wider imaging team (radiologists, medical physicists, allied professionals), because interdisciplinarity is the foundation of innovation in imaging.
ECR is a key moment where these bridges become tangible. Colleagues meet, compare approaches, and often initiate collaborations that continue
beyond the congress. A good idea becomes transferable when it is outcome-focused and adaptable. The most transferable innovations are often not the most complex ones: a protocol standard that reduces repeats, a safety checklist that improves compliance, a training pathway that strengthens communication, or a workflow change that improves patient experience. EFRS can help by curating these practices, supporting collaboration, and encouraging radiographers to document and share results so others can adopt them realistically.
Q8Radiographers’ roles are expanding in advanced practice and research, and you have emphasised empowering young professionals. What leadership competencies should be prioritised?
Leadership for radiographers today is about responsibility for outcomes. The competencies I would prioritise are clinical practice, educational, research, patient-centred communication, and leadership, particularly when introducing AI or new workflows.
If I had to define success for ECR 2026 in one tangible outcome, it
would be this: radiographers leave with at least one implementable improvement, something that can measurably enhance quality, safety, or patient experience. If that is accompanied by new collaborations, mentorship connections, and shared projects across countries, then ‘Rays of Knowledge’ becomes more than a theme: it becomes a European movement in daily practice.
A good idea becomes transferable when it is outcome-focused and adaptable
1st Vice-President, European Society of Radiology (ESR); Cochin Hospital, Université Paris Cité, France
Q1You are an established thoracic radiologist and became Second Vice-President of the European Society of Radiology (ESR) last year. Looking back, what key professional experiences or decisions most shaped your journey into European radiology leadership?
I think that one of the best decisions I made in my professional career was to engage in ESR activities. I was first involved in the European Society of Thoracic Imaging (ESTI), since I'm a thoracic radiologist. For instance, I would participate in rating the abstracts and evaluating the sessions, and take part in many ESTI meetings, giving lectures. When you give a lecture, you are the first one to benefit, because you prepare and you learn.
My colleagues at the ESTI and I also built a lung cancer screening certification programme. It was a collaborative effort because as early as 2019, we had the feeling that we would go for large population screening, which requires the training of a large number of radiologists.
Having some responsibilities within the ESR was not a long-term plan. I did not anticipate being asked to present my application to become Chair of Communication and Interdisciplinary Affairs, which I accepted, and then to apply for vice presidency, which I also accepted.
I think that what we are doing at the level of the ESR is very important; for instance, the role of advocacy, where we are trying to convince the European Parliament to recommend that member states test the feasibility of lung cancer screening.
For all these reasons, I think it was a very good decision to engage in ESR activities.
Q2
As lead of the SOLACE project in France, you are working at the forefront of lung cancer screening implementation. How can the European Congress of Radiology (ECR) 2026 serve as a catalyst for translating screening research into sustainable, standardised programmes across different European healthcare systems?
At ECR 2026, we had two very important sessions dedicated to lung cancer screening. One was the EIBIR session where we reported on SOLACE. But the session, 'European perspectives of lung cancer screening: more than a decade after NLST and NELSON’, aimed to evaluate its status.
There were also different lectures. One was given by Anna KerpelFronius, National Korányi Institute for Pulmonology, Budapest, Hungary, on SOLACE, where she presented strategies to address the underrepresented population, women, hard-to-reach individuals, and individuals at higher risk of developing lung cancer because of additional risk factors.
Another was a lecture given by Harry De Koning, Erasmus MC, Rotterdam, the Netherlands (also the principal investigator of NELSON), who is currently the principal investigator of the 4-INTHE-LUNG-RUN project. This project is also EU-funded, and the objective was to optimise eligibility and screening intervals and to provide a personalised approach to lung cancer screening.
Marie-Pierre Revel
Then Annemiek Snoeckx, University of Antwerp, Belgium, discussed the additional findings to report. It's a very controversial topic, because we needed to balance burdens and benefits. Lastly, Helmut Prosch, the Medical University of Vienna, Austria, who is the current ESTI president, presented the training programme for radiologists in lung cancer screening.
Q3
The SOLACE study has revealed a higher-thanexpected rate of positive findings among women, with a significant proportion of early-stage cancers detected. How should radiologists and healthcare systems prepare for the downstream clinical implications of expanded screening programmes?
I think it's mainly a question for the healthcare systems, because it's one thing to screen, but once we have a positive screening result, we need to have the management pathway set up. In France, for instance, we request that the delay between a positive screening result and further discussion should not exceed 2 weeks. We also need to evaluate the availability of surgeons, especially those who are able to perform minimally
invasive thoracic surgery. I don't know if there is a sufficient number of surgeons trained in minimally invasive surgery in all member states, so this is, I think, an important question. This is because it is a relatively new field and it requires resources. Roboticassisted surgery is also expensive, and I don't know about the current status of deployment of this new technology. At least in France, I know it's not everywhere. So, based on the number of screened individuals, the eventuality of lung cancer, fortunately, will be relatively rare, but we need to offer the best possible care to these individuals
Q4
One major outcome of the SOLACE trial is that it has culminated in the formation of the European Lung Cancer Screening Alliance (ELCSA). What are the strategic priorities of this alliance, and how do you see it influencing clinical standards, policy development, and patient engagement across Europe?
I think our main objective is to ensure that lung cancer screening can be largely implemented and continued in the countries participating in SOLACE. The screening was possible because of the European funding, but
now it has to be taken on by the national healthcare systems. For this, we can provide updated guidelines, but we will also organise two events per year where we will invite stakeholders to keep them informed about, for instance, the latest advances in cost effectiveness analysis, the best strategies, optimised guidelines, and the status of implementation in different member states.
Q5
You have been actively involved in integrating AI into lung cancer screening. In the context of ECR 2026’s focus on ‘The Art of AI in Clinical Practice’, what are the key principles that should guide responsible and effective AI adoption in screening programmes for lung cancer and beyond?
So, we are using AI as a second reader. This is the main research question of my programme in France, the CASCADE study, where we use AI for detection in lung cancer screening in French women.
Evaluating AI algorithms at different steps in their evolution will be important
There, we will compare the performance of general radiologists who are assisted by AI to the performance of a double reading by chest experts who are not assisted by AI. Based on interim analysis, it's very positive, meaning that AI can help general radiologists to reach the performance of thoracic experts, which is very good because we don’t have enough experts for large population screening.
Then what we are planning to do within SOLACE Plus, if it gets funding, is to benchmark different AI solutions. We need to define a minimal level of performance and an optimal level of performance. Based on this evaluation, I think it will be possible to build an economical model for reimbursement of AI solutions, to have cautious and ethical use of AI. We need to be sure about the performance, evaluating it at different levels of development of AI. I have seen that more recent versions have improved their performance, especially in the detection of subsolid nodules (those with low attenuation that are more difficult to depict) compared to solid nodules. So again, evaluating AI algorithms at different steps in their evolution will be important.
Q6
Where do you see the greatest opportunities for advancement in thoracic imaging and lung cancer prevention over the next 5–10 years, and how is ECR 2026 highlighting these developments?
Firstly, ECR 2026, with its focus on AI, has shown that the use of AI is already there and that it contributes to our efficiency. The objective is to go beyond; for example, to evaluate AI in its capacity of predicting the Agatston score, for the prediction
of coronary artery disease, or other assessments of body composition anomalies, for the prediction of osteoporosis, because there's a way to correct the condition by avoiding the occurrence of vertebral fractures, if they are detected early. We could also detect other anomalies of body composition, like sarcopenia and an increase in fat content, and provide a report, helping us to provide preventive or curative measures for these anomalies. For the time being, these AI tools have not been prospectively validated. So, this is what we need to do next.
Q7
As France prepares for a national lung cancer screening programme, supported by initiatives such as the IMPULSION trial, what further milestones or systemic changes would you hope to see achieved across Europe before ECR 2027?
The first thing is, I would like IMPULSION to start and to be successful in recruiting participants. We are waiting for the last legal authorisation from the National Commission of Informatics and Liberty (CNIL). But we are very well prepared to launch this programme in five regions, before extending to the rest of the regions in France.
I would also like this deployment of lung cancer screening to be the occasion where we are efficient in the denormalisation of tobacco consumption and the fight against the tobacco industry, which is trying to stay alive by developing other products that lead to nicotine addiction. We are now at the peak of the lung cancer epidemic because of the increased prevalence of smoking in women. It's the late consequence of the start of female tobacco consumption in Europe: women
who started to smoke around the 1970s and 80s, which is later than those in the USA.
Now, we are facing the consequences. In the vast majority of the member states, lung cancer is the leading cause of cancer death among women, above breast cancer, which is five times more prevalent. I think that lung cancer screening will be the time to realise just how deleterious smoking is, without blaming smokers; smokers are victims, they are not guilty. It's also the time to be more efficient in smoking cessation strategies and support smokers to help them quit.
ECR 2026, with its focus on AI, has shown that the use of AI is already there and that it contributes to our efficiency
Luís
Curvo Semedo
Faculty of Medicine, University of Coimbra, Portugal; Department of Medical Sciences, University of Aveiro, Portugal; Chair, Imaging department, Local Health UnitAveiro Region, Portugal; National Societies Committee Chairperson, European Society of Radiology, Vienna, Austria
What initially inspired you to pursue a career in radiology, and what in particular drew you to abdominal imaging?
Curiously, my interest in radiology appeared relatively late in my clinical career, despite having had the highest classification of my class in medical school. I was attracted to a more clinical subject, like orthopaedics or surgery, but suddenly I realised that radiology was a way to look inside the body in a way that connects anatomy, pathology, and clinical reasoning. I was particularly attracted to the intellectual challenge of interpreting images and translating them into information that directly helps clinicians and, of course, patients.
Abdominal imaging became a natural focus for me because of the complexity and diversity of diseases affecting the gastrointestinal and hepatobiliary systems. The former, particularly, constitutes an area where imaging plays a crucial role not only in diagnosis, but also in staging, treatment planning, and follow-up, especially in oncology.
Q2
Radiology has changed enormously over the past couple of decades. How have you seen the profession evolve during your career, and how has that influenced the way you practice medicine today?
Radiology has evolved dramatically since I started my career. The big developments in CT, MRI, and even ultrasound have transformed the level of information we can obtain from them. At the same time, the role of radiologists has expanded from simply interpreting images to
becoming an integral member of multidisciplinary clinical teams.
Another major shift has been the developing level of subspecialisation. Today, radiologists often focus on specific areas, such as abdominal imaging, which allows for deeper expertise and more accurate clinical contributions.
Of course, we are witnessing the surge of AI applied to imaging, which I consider to have the potential to be more helpful than harmful, if we know how to use it.
These changes have influenced my practice by reinforcing the importance of collaboration with clinicians and continuous education. Radiology is now more integrated into the entire patient pathway, and radiologists play a key role in guiding diagnosis and treatment decisions, as well as follow-up.
Q3
You combine clinical work, teaching, and leadership roles. How do these different responsibilities complement each other in your professional life, and how do you balance them?
For me, these roles are quite complementary. Clinical work keeps me closely connected to patients and to the real challenges we face in daily practice. Teaching allows me to share knowledge and contribute to the training of the next generation of doctors (particularly radiologists), which I find enormously gratifying.
Leadership roles in professional societies and scientific organisations offer an opportunity
to contribute to the development of radiology at a wider level, through education, research, or professional standards.
Harmonising these responsibilities requires cautious time management and prioritisation. The experience gained in clinical practice updates my teaching and research, while academic and organisational work helps bring new viewpoints and innovations back into clinical care.
The role of radiologists has expanded from simply interpreting images to becoming an integral member of multidisciplinary clinical teams
Q4
Your research focuses on abdominal and oncologic imaging. From your perspective, what are the most exciting developments currently emerging in these areas?
One of the most stimulating developments is the incorporation of advanced imaging techniques with data analysis methods, such as radiomics and AI. These have
the potential to extract much more information from medical images than we customarily could.
In oncologic imaging, in particular, there is rising interest in imaging biomarkers that can help foresee treatment response and guide personalised treatment. Imaging is gradually moving beyond (simple) diagnosis toward supporting precision medicine.
Simultaneously, advances in MRI techniques, multiparametric imaging, and hybrid imaging are helping us better characterise tumours and assess therapy response, which is crucial for improving patient outcomes.
Q5
You did a talk on postoperative imaging of oesophageal cancer, specifically complications and surveillance. What were the key takeaways from this session?
First, it is pivotal to understand the expected postoperative anatomy after oesophageal cancer surgery, as it is the better way to discriminate between normal findings and true complications.
Radiologists should be aware of potential postoperative complications, such as anastomotic leaks, strictures, infections, or conduit-related problems. Prompt
detection through imaging can significantly impact patient management and outcomes.
Another key point is the role of imaging in long-term followup, particularly in detecting recurrence or metastases. CT remains the basis of surveillance, but the interpretation should always be integrated with the clinical context.
Q6 The field of radiology is growing rapidly. In your view, what skills will future radiologists need that were not as essential a generation ago?
Future radiologists will need to be comfortable working with large volumes of digital data and more sophisticated technologies. Dominating AI tools and advanced image analysis will likely become a central part of practice.
Equally significant are communication and collaboration skills. Radiologists must cooperate closely with multidisciplinary teams and contribute dynamically to clinical decision-making.
Also, adaptability and lifelong learning are vital. Radiology is a field that advances very quickly, and professionals must be ready to continuously update their knowledge and skills.
Finally, radiologists will need to prioritise other skills that allow them to achieve a decent worklife balance. Burnout is increasing among radiology professionals and could be a major problem that negatively impacts the already depleted staff.
Q7
You are part of the Scientific Office for the European Congress of Radiology (ECR) 2026. What are your main responsibilities in this role, and what does your work involve in the months leading up to the congress?
Well, I wasn’t part of the Scientific Office, at least formally, even if I contributed to the development of the congress’ scientific programme by reviewing and evaluating abstracts.
However, being part of the Executive Council of the European Society of Radiology (ESR), I had the opportunity to happily perceive, during our regular meetings, that the programme covered the most relevant and innovative topics in radiology.
A balanced programme that combines cutting-edge research, educational content, and practical clinical insights was created. It was a challenging process, but also a very fulfilling one, as it helped shape one of the top scientific meetings in radiology.
Q8 The ECR brings together radiologists from all over the world. From your perspective, what makes this meeting unique compared with other medical conferences?
I guess that its combination of scale, diversity, and educational focus covering virtually every subspecialty within radiology is what makes it so special.
Another distinctive feature is its strong emphasis on education. ECR offers an eclectic choice of teaching sessions, hands-on workshops, and multidisciplinary discussions that are extremely valuable for both trainees and experienced radiologists.
ECR is a place for networking and collaboration, permitting professionals from different countries and healthcare systems to exchange experiences and ideas.
Also, it is the place to be aware of the technical innovations that come from all the vendors that participate in the event.
Let’s not forget that it takes place in one of the loveliest cities in Europe and the World, Vienna, making a return to the ECR a pleasure, year after year.
Q9 Finally, when participants leave the ECR, what do you hope they will take back with them to their hospitals and daily practice?
I hope the attendees leave with new knowledge, additional perspectives, and practical concepts that they can apply in their own departments.
Scientific meetings like this are not only about presenting research; they are also about sharing practices and learning from colleagues around the world. If participants return home with the ability to improve their practice, adopt new procedures, or reinforce collaboration within their teams, then the congress has achieved its purpose.
Ultimately, the goal is always the same: improving patient care through better imaging and stronger professional partnership.
There is rising interest in imaging biomarkers that can help foresee treatment response and guide personalised treatment
Interviews
EMJ had the privilege of speaking with two leading experts in cancer imaging and radiology: Fiona Gilbert, University of Cambridge, UK; and Caroline Chung, The University of Texas MD Anderson Cancer Center, Houston, USA. Gilbert discusses her journey from clinical radiology to breast cancer imaging, highlighting the role of tomosynthesis, MRI, contrast-enhanced mammography, and AI in improving early detection and patient outcomes, also addressing the challenges of implementing new technologies at scale. Chung reflects on her career at the intersection of radiation oncology, quantitative imaging, and data science, exploring how AI, digital twins, and multi-parametric imaging can personalise treatment, enhance precision, and reduce patient burden.
Featuring: Fiona Gilbert and Caroline Chung
Fiona Gilbert
Professor of Radiology, University of Cambridge; AI Lead Advisor, Royal College of Radiologists, London, UK
By working in the clinical arena, I can see what's important, what's less important, and what the next direction of the field might be
After graduating from medical school in 1978, what initially motivated you to specialise in radiology, then specifically in breast cancer imaging?
After my house jobs, I did a year in oncology with the late Sir Kenneth Calman, who trained initially as a surgeon and then moved into oncology. He was one of the youngest professors and set up the oncology unit in Glasgow, UK. That year the first CT scanner was installed in Glasgow Royal Infirmary. We sent patients there to decide whether or not they were responding to treatment, and CT scans had only just begun to be used for that purpose.
I remember saying, “We need to see what’s happening here,” and he asked me why, to which I replied, “Because you need the evidence.” At that point, he told me I should be a radiologist. He
knew my dad was a radiologist in Glasgow. Initially, I decided against it, because I didn't want to follow in my father’s footsteps, but I was a visual thinker. I found it much easier to understand something if I could visualise it. When I was learning in medical school, I'd be able to see where something was written on a page. It was not photographic memory, but it was a very visual memory, and I would learn by writing things down, drawing maps, and things like that. I suppose that aptitude for looking at visual things might have been the start.
When I moved to Aberdeen, I completed my Membership of the Royal College of Physicians. I remember saying I would go into public health, or something like that, and the postgraduate Dean said to me, “You've got your Membership of the Royal College of Physicians, you passed all the exams, you should be
doing something in the hospital.” Therefore, I looked around, and there was radiology training in Aberdeen, so I decided to do that.
Q2 You have worked extensively across academic, clinical, and advisory roles. How has maintaining an active clinical practice influenced your research priorities, particularly when assessing which imaging innovations are most meaningful for improving patient outcomes?
It was a piece of advice that my father gave me. Because he knew I wanted to do research, he said, “Don't give up your clinical work. Make sure that you don't stop being aware of clinical developments, so you've got a really good handle on what's most important in radiology, and how the field has changed. It means you keep much more abreast of what's going on and, therefore, it means your research is more likely to be clinically impactful, because you're working in it on a day-today basis.” I still do breast work in the clinic and stay on top of new developments. My main academic
theme has been new technology assessment, and what the clinical impact on the patient outcome is. By working in the clinical arena, I can see what's important, what's less important, and what the next direction of the field might be.
I’ve been really lucky in my career that there were so many developments going on. CT had just been introduced when I started in radiology training, and that was why we were so excited about it. At the same time, MRI was being developed, and we had a fantastic innovative team of scientists in Aberdeen, where I was working, at the forefront, and that gave me a wonderful opportunity to be really involved at the shop floor level with patients being scanned, and working with the teams there. Fundamentally, they wanted patients to try out their new sequences, and we were able to provide that for them. People talk about being in the right place at the right time. I think, from my career point of view, there was a lot of that. I just happened to recognise the opportunity or be hungry for opportunities at the right times.
Q3
Your research has explored multiple imaging modalities, including tomosynthesis, MRI, contrastenhanced mammography, and AI-assisted interpretation. Which of these technologies currently offers the greatest potential to improve early cancer detection and diagnostic confidence, and why?
I think all of these technologies have a role to play in terms of early diagnosis. The USA has largely moved to tomosynthesis, which is particularly helpful in women who have got mixed density breast tissue. We've completed the PROSPECTS trial in the UK with encouraging results, and I think we will be adopting that technology, at least for some women, and that will increase our cancer detection and reduce our recall rates a little bit, which will be great. However, I think for people who have very dense breast tissue, where we think the mammogram is normal, we should be using AI prediction tools to decide whether or not to offer them additional imaging or bring them back for more imaging a year later.
We should be offering them contrast mammography or abbreviated MRI, a fast MRI examination to make sure that we're not missing a small cancer, to provide earlier diagnosis for those women with dense breast tissue.
There are a lot of different things we should be looking at in the breast screening programme. That is, of course, what makes it difficult for the policymakers, because they don't know which one to implement. In reality, we need to be pushing all of them. We need to be moving ahead and adopting these different technologies now. I can understand the reluctance just to say, ‘okay, we're going to move with this’ because, at a population level, you don't want to be making mistakes. But, in reality, we just need to start doing some feasibility testing in the field at several sites and assessing how it pans out. By putting things in the field, in practice, you learn a huge amount. One of the things we're doing at the moment is the big EDITH trial, where we're replacing one of the two human readers with AI for the detection of breast cancer. The good thing about this trial is that we will end up rolling out the AI across about 30 sites in the UK, so that is fantastic. Almost one-third of the UK sites will have exposure to AI in breast imaging.
Overall, I think we need to persuade the people, depending on which healthcare system you're in, to move to new technology earlier. In some ways, it's not good enough just to sit on the fence for a long time and wait for yet another trial or health economic analysis.
Q4The BRAID trial, the interim results of which were recently published, aims to demonstrate the value of supplemental imaging in women with dense breasts. Could you describe the rationale behind this trial, and the unmet needs it aims to meet?
In the UK, we do 3-yearly screening, and we're the only country to have such a long interval between the screening examinations. So, our problem is that we have a lot of interval cancers. A lot of cancers occur in women presenting symptomatically with a lump in their breast or other symptom(s), and women who have interval cancers have a worse outlook compared to smaller screen detected cancers. So, what we're trying to do is reduce the number of interval cancers and find the cancers a couple of years earlier at the previous screening examination
The motivation for the BRAID trial was that we knew people who had very dense breast tissue had more interval cancers and had larger cancers, so we thought, let's target these women with an additional imaging technique. The question we are trying to answer is which of the imaging techniques was better? Is a fast MRI scan better than a contrast mammogram or whole breast ultrasound? Contrast mammogram is very effective for showing these small cancers. Cancers have lots of blood vessels that take up the iodine and show up brightly on the mammogram, which is fantastic. An MRI, we've known for a long time, is much more sensitive than any of the other techniques, but it's quite costly. A fast MRI scan reduces the cost by about 50%, so we wanted to compare contrast mammography
with fast MRI against the standard supplemental imaging, which is breast ultrasound. That was what the trial was about.
We recruited over 9,000 people across 10 sites in the UK, and randomised them to one arm each. We did the additional imaging and then did a second round of imaging, and we found that the two contrast techniques, abbreviated MRI and contrast mammography, picked up between 16–18 additional cancers per 1,000 women that we screened, compared to ultrasound, which only picked up four additional cancers. We're seeing as many as four-times as many cancers in the contrast arms compared to the ultrasound arm. This was a very exciting study, and we felt that this was definitive evidence that you should be doing contrast techniques, not ultrasound, which is offered in other countries, such as the USA, Italy, and Germany, to women with dense breasts, but, actually, it's not good enough. We should be doing these other tests instead.
Q5The interim results from BRAID suggest significant benefits of supplemental imaging for women with dense breasts. What are your expectations for the full results when they are released in a few years’ time? And how are these set to impact patient outcomes?
What we're seeing with the second-round imaging is another eight cancers per 1,000, which is amazing, because we're only imaging 18 months later. So, if you think about it, in the Breast Imaging-Reporting and Data System (BI-RADS) D category, we've already found eight cancers per 1,000 from the mammogram. So, if you take women with a negative mammogram and offer
them contrast examination, you pick up another 18 cancers per 1,000. Then, 18 months later, you do another contrast examination, and you pick up another eight cancers per 1,000. That's 34 cancers per 1,000 in that 18-month period, which is amazing, but you think, where are all these cancers coming from? And that's why we have to wait for the results of the main study, because we need to look at the number of interval cancers to see if there is a reduction in the interval cancers too. Also, we need to look and see what the next round of mammography cancers are. We'd expect to see a dip in the cancer detection rate of the next round, and certainly a smaller tumour size at the 3-year mark as well, because we've brought the diagnosis forward for so many of these women.
Q6You have been closely involved in the development and evaluation of AI tools for breast imaging, and you are now the Lead AI Advisor at the Royal College of Radiologists. As AI becomes increasingly integrated into clinical practice, where do you see its greatest potential in breast imaging? Are there particular areas where you believe it will have the most meaningful clinical impact?
AI is moving at an extraordinary pace. In the UK, we’re still in the relatively early stages of its widespread adoption, but imaging is leading the way. One of the reasons for that is that radiology has long worked with digital images, providing exactly the kind of structured data that AI systems can be developed and trained on. I think the key is that we're going to get improved standardisation of reporting quality. What previous work has shown is that people who are less confident and less
experienced often show an improvement in their performance when they're using AI tools, with prompts, etc., whereas, for the more experienced readers, we often don't see much of a change. While not everybody can be seen by the best musculoskeletal radiologist in the country, often the AI can help lift many people up towards that level, which I think is one of the important things.
AI is moving at an extraordinary pace
Secondly, I think it's going to make us monitor the performance of the AI and look at human interaction with the AI. In breast work, we've been very used to regular quality assurance and performance monitoring (how many cancers do I detect a year? How many cases do I recall from screening?). There are a number of metrics on which I'm measured. I think that kind of audit will become more mainstream across radiology.
I also think, quite shortly, we're going to see a shift to autonomous reporting of high-confidence normal examinations. About 30% of all our examinations are normal. They are the people who are referred because we need to exclude ‘X, Y, and Z’, and we end up with a normal chest X-ray or normal CT. We already know that when you look at the chest X-ray algorithms, it's trying to pick up around 20 different conditions. If it's a high-confidence normal examination, then it is genuinely normal. When you compare that with a whole group of different reporters, then you actually get more accurate results with the AI than you do with this variable
group of people that are reporting the chest X-ray. So, I think we will see a shift towards AI being used for this purpose in very controlled circumstances, because we need to get the public to understand what we're trying to do. We're not trying to save money. We're trying to free up capacity so that we can deliver a better radiology service in a more timely way and do better for patients. We know that radiologists are going to be doing more complex imaging and reporting, but I think we're going to be able to use the AI tools in some areas for cases that are genuinely normal. It'll be able to cut down maybe 30% of the normal reporting because the AI tools will be sufficiently confident to say this is definitely normal, and the miss rate would be much less than a human reporter. It is very important that we improve the delivery of radiology services by having more radiologists to match the 8% year on year rise in imaging tests, and AI will help us deliver radiology services more efficiently. Clinicians are increasingly dependent on imaging: like me, they want to “see” what is going on. I think that's a better service for the public, which is why I think that is one of the shifts we are going to see.
A very important aspect of introducing a new system such as AI is patient safety. It is essential to audit the performance of AI and the human interaction. However, with uncommon errors, a centralised reporting system could be helpful, so that if there is an adverse event in one hospital, it can be reported, and patterns of adverse events can be recognised more quickly around the country. In summary, if a trust has one adverse event in a year, then they might not think anything of it, but if we see the same adverse events from
20 different hospitals, that needs to be collated and something needs to be acted on quickly. That’s what the Medicines and Healthcare Products Regulatory Agency (MHRA) are looking at; I think they are looking at strengthening their yellow card system, which is used mainly for drug and medical device reporting currently.
Q7Despite strong evidence for emerging imaging technologies, adoption into routine clinical practice can be slow. From your experience, what are the most significant barriers, whether technical, organisational, or educational, to implementing innovations, such as AI or supplemental screening?
There are a number of things that need to be put in place. While several trusts have implemented AI for chest X-rays, we still need to encourage trusts to embrace AI technology. Our IT departments and governance are still quite apprehensive about it, so we need to do things in terms of reassuring different areas of the workforce that these tools are safe. I think there needs to be some kind of centralised system whereby we can have shared documents and risk assessments for AI tools, which can help protect identifiable patient information in a trust, as each trust is legally responsible for patient data. That shouldn't change; that is sacrosanct, and trusts get very nervous when an AI tool is introduced and is scurrying around all the identifiable data. So, we need to harmonise these Data Protection Impact Assessment (DPIA) documents, which provide a reassurance to the trust, and make sure that, however it's being used, their data is going to be safe.
There needs to be some kind of national accreditation or
national approval body, which says, ‘yes, this is good to go’. Then, the trust might not have to spend so much time scrutinising whatever the particular tool is and confirming whether it works in a UK population. There are no ethnic biases or other biases that we should be worried about. The information governance is being properly considered, and that means it can be rolled out more quickly across trusts to streamline that deployment.
Then, we need to be very clear about how we're going to monitor these tools. We need to make sure that trusts have generic tools in place so that they can just press a button on one of their dashboards and confirm a tool is performing correctly, basically auditing it. This does not need to be a continuous monitoring system, but there should definitely be a monitoring system in place, running in the background, so that a trust can easily pull out data to say the performance is not drifting, the radiologists are still reporting the correct number of abnormals, and so on.
There is quite a lot of work to do, but I think people are aware of that, and of course, it's upskilling the workforce too, so that they feel comfortable in using AI and understand the limitations of a particular tool. For example, so they don't start using a tool that's designed for adults in a paediatric population.
Q8 Equity is an important consideration in imaging across geographical areas, with variation in access to advanced imaging remaining a challenge. What practical steps can/should healthcare organisations take to ensure more equitable access to improved screening and diagnostic tools?
GPs have a big role to play in ensuring equity of access to all kinds of imaging and screening services
I think policymakers are really focussed on this, and they want to do whatever they can to ensure that everybody's invited, that we look and see why people don't come for imaging early, why they don't see the general practitioner (GP), and why they don't access their screening. There is a lot of work going on to understand what happens in different demographic patterns, different geographic areas, different ethnicities. There are all kinds of things that influence behaviour, so it’s very much an important topic to always consider, particularly when we're looking at changing access to a system. Although many people have mobile phones and can receive text messages, it's still not universal, and emails and online activity can be quite a barrier for some people, so we have to always ensure that people can be supported, whether it's through their GP, which is often a good mechanism to do so, or otherwise. People say, ‘they could go to a library and access online material there’, but I think people are reluctant to go and consider their private healthcare matters unless it is with someone appropriate. I think GPs have a big role to play in ensuring equity of access to all kinds of imaging and screening services. We also need to do what we can to support the GPs. It's not fair just to shift the weight onto them. We need to put tools in their hands to allow for improved access. We need to make it as easy for the GPs as possible.
Q9
For healthcare professionals working in breast cancer today (and those of the future), what practical steps can they take to ensure they are delivering the highest standard of care to their patients?
The amazing thing that's happened with breast cancer, apart from all the imaging and the incredible technological developments, is that the drugs are so much better. Now that the treatments are so much better, we can minimise treatments and ensure that the right person
receives the right treatment for them; advances in personalised medicine are amazing.
I think for people coming into breast imaging, it's really important to be hopeful about the specialty. I think our role is going to change slightly over time, because we're going to see more and more people who are living with breast cancer. We're going to be seeing more people with metastatic disease living longer, so I think we need to make sure that we are very familiar with the different techniques and
also interventional techniques, such as vacuum excisions using image guidance and cryotherapy, which are fantastic. There are all kinds of developments that are coming our way, which are presenting amazing opportunities for radiology. It's fantastic. The future of the specialty of radiology is very bright.
The future of the specialty of radiology is very bright
Caroline Chung
Division of Radiation Oncology and Division of Diagnostic Imaging,
The University of Texas MD Anderson Cancer Center, Houston, Texas, USA
We can start to really aspire to get in vivo biological understanding from our radiological images, which would be a really helpful tool, particularly in the CNS space
What first drew you to radiology, in particular the intersection of oncology, imaging, and data science? How has it shaped your career path since?
Clinically, I trained as a radiation oncologist, but since the start of my career I've had a faculty role, cross-appointed between radiation oncology and diagnostic imaging (or radiology) due to my research focus on the use of quantitative imaging in personalised cancer therapy. This intersection, together with my training, led me to focus on questions like: can we actually extract quantitative imaging biomarkers or surrogates of tumour biology behaviour response to therapy?
As a radiation oncologist, I was very interested in mapping out resistant or aggressive subregions of tumour with imaging, as these are areas could benefit from treatment intensification with locally directed therapy like radiation therapy. At the start of my career, a lot of my work was in that translational space, working right from early mouse models of brain tumours through to clinical trials, and trying to translate those quantitative imaging biomarkers, both from the pre-clinical to clinical space. In recent years, a lot of my focus has been on clinical research development and how we actually translate what is developed in research into clinical practice.
Q2 Your clinical practice focuses on malignancies of the central nervous system (CNS). How have advances in imaging, quantitative analysis, and data integration changed the way clinicians detect, characterise, and monitor CNS tumours during your career?
There have been lots of new imaging techniques. In term of MRI, we have identified many novel sequences and various quantitative data we can extract from images, and how have the ability to leverage emerging analytic pipelines (including some using AI) in multi-parametric MRI analysis. Combining MRI with PET and other imaging modalities over the course of time has been something that has also generated new insights in the CNS tumour space. I think what's most interesting is that each of those modalities brings us different information. What remains unanswered is how do we actually integrate and extract the meaningful pieces of what each of these modalities are contributing? And how do you meaningfully map them together spatially to best represent the underlying biology?
Another gap is being able to extract quantitative measures and tying them back to the underlying biology. We do need more research in the space. If we can get spatially resolved and temporally resolved biopsy specimens so that we can correlate true pathology to the imaging, we will be closer to understanding what the imaging signals represent biologically. Gathering enough of this kind of information, we can start to really aspire to get in vivo
biological understanding from our radiological images, which would be a really helpful tool, particularly in the CNS space, where a biopsy currently means a craniotomy, or some form of invasive access through the skull, into the brain. Having those in vivo imaging biomarkers would be incredibly useful to accelerate our understanding, but also to inform treatment selection and treatment response assessment, particularly as systemic therapies are becoming more and more biologically targeted, as opposed to using generic cytotoxic agents to treat cancer.
Q3You have an extensive and highly influential research portfolio. What key areas is your research currently focusing on? What results are you expecting, and how do you see this work translating into meaningful improvements in patient outcomes and clinical decision making?
I think I'll start with the big picture and then break it down to some of the fundamental, foundational gaps that we continue to have; gaps that we're also trying to tackle with a lot of the computational capabilities that
are emerging, including AI and physics-informed models.
There's real aspiration in terms of the personalised medicine space to build digital twins that will journey along with that patient. And it doesn’t necessarily mean an entire human being digital twin, although that is an aspirational blue-skies goal in the field. It could be that, for a patient with cancer, we could build a model of their particular tumour and the surrounding biology so we can anticipate or model and simulate how different treatments might work and see which would result in the best possible outcome for that patient, which would reduce the kinds of toxicities that patient might experience. Building in these aspects would help us move toward truly data-informed, personalised decision-making processes above and beyond what we have today. Currently, evidence-based medicine relies on the results from trials and data that reflect population averages.
Moving into some gaps that we currently have in the imaging space, in order to measure biological changes across time in the imaging, we need to consider the level of uncertainty
or variability of the imaging measurement from scan to scan. People go to different scanners or different institutions, which may have different protocols; not all patients stay in one hospital for the entirety of their care. Some of the fundamental work that I've been pursuing with others in terms of the quantitative imaging is figuring out a way to meaningfully cross-calibrate these differences to determine true biological change. We know there's going to be some level of heterogeneity because machines will always get upgraded, and it is great to have technology advance over time, but how do you calibrate the measurement at one time point versus another? I serve as the Co-president for the Quantitative Medical Imaging Coalition (QMIC),1 which is a non-profit organisation that aims to serve as a trusted third party across a growing network of dedicated imaging experts, imaging physics experts, academic institutions and organisation, industry partners, etc., who are working to help enable quantitative imaging practices. This community will need to work together to facilitate the realisation of the full potent emerging technologies like digital twins, because patients will travel
between institutions. It will need to be an international effort, and the problem is global when it comes to creating quantitative measurements.
The second point is that if we want to leverage the growing capabilities of AI, it’s sensitive to the data itself. I'm sure everyone's aware of the phrase ‘garbage in, garbage out’. But what that really means from an imaging standpoint is we need to know how much uncertainty you have in your measurement, which will also depend on how your images are acquired, and if you are looking to measure a change across time, the differences between time point A and at time point B matter. Otherwise, we wouldn't know if something is a true biological signal or just a detection of the technical noise. What we're after in terms of personalised medicine is deciphering and teasing out the biological signal and the change that's happening to inform clinical decisions, while figuring out how to alleviate or account for all of the technical noise that comes with real-world data.
Q4Through initiatives such as the Tumor Measurement Initiative (TMI) and your leadership at the Institute for Data Science in Oncology, you’ve helped build infrastructure to enable clinically meaningful use of data. For quantitative imaging to truly support precision medicine, particularly in the context of tumour heterogeneity, reproducibility and standardisation are critical. What role do coalitions and collaborative frameworks, such as the Quantitative Imaging Biomarkers Alliance, play in making quantitative imaging clinically reliable? And what steps should institutions take to align with these standards and realise the full value of a quantitative approach?
collect enough metadata and have enough descriptors around how that data was captured, we can at least start to understand how data at one time point is different from another time point.
There's real aspiration in the personalised medicine space to build digital twins that will journey along with that patient
Imaging data have been treated as ‘images’ for many years, born out of initial film-based radiology, but the digital capture of medical imaging data brings forward many opportunities to treat imaging data as ‘assays’ of measurements. This shift in perspective introduces the need for changes in radiology practices and workflows that would also bring a lot of benefits in regards to efficiency, quality, and enabling emerging technology like AI. Within TMI, we aimed to consider the entire imaging chain from image acquisition, image processing, and analysis to improve the consistency, precision, and transparency across this process.
While the quantitative approach is not necessarily all about standardisation, as technology and practices will evolve and advance over time, some level of standardisation is helpful, and it is more important to standardise how we collect the information, so that we know how to crosscalibrate the data even if they are different, whether it's imaging data or any other data. If we
I refer to finding and using ‘fit-forpurpose’ data. Sometimes you can work with noisy data, depending on your purpose. If you're just looking at general patterns or trends, you can potentially work with noisy data in that exploratory space. But if you're trying to make a very specific decision about, let's say, a clinical decision around a patient, you would want to have more precise and less noisy data to have greater confidence. Right now, in medicine, a lot of the work is still fairly manual. Humans are nearly always in the loop. But as we start to introduce more tools along this process, it may not be so transparent to the human in the loop what assumptions have been made, or what uncertainties are being integrated into the outputs they're looking at and using as they make decisions.
As we start to think about how we're going to use these tools, there needs to be a collaborative endorsement and adoption of a certain practice of how data is captured, as well as communicated from one group to another. That coordination really relies on coalitions, communities, and even perhaps, to some level, regulatory bodies that would actually help bring forward and highlight the importance. Some of that may come through policy changes, but it also requires awareness and a willingness to adapt, because it ultimately benefits all of these different communities if we move toward a truly coordinated health system. From a data perspective, I would say we still have a long way to go.
I also think that there has been a lot of effort on the technical interoperability. The Digital Imaging and Communications in Medicine (DICOM) standards have helped allow imaging data in digital form to move from one centre to another. That's step one, which we’re improving at. The next step is that we need the understanding of how imaging data set A differs from imaging data set B. For instance, if we're taking measurements from each, how do we account for that difference in how the images were acquired and processed? That will be impacted by details such as what tracer or contrast agent was used, how it was injected, as well as all of the imaging parameters for the acquisition that is captured by the scanner.
Q5While AI tools are increasingly being introduced into clinical workflows, concerns remain around reliability, bias, and real-world performance. What practical guidance would you offer clinicians to help them safely evaluate, implement, and monitor these tools? And how might this ultimately improve patient care?
be more readily feasible at larger centres and systems at this time because they have the resources to do this). Figuring out how to facilitate and enable all clinics to be able to carry out local validation is something that is still being worked on, and how to do that in the most efficient way is something that is not solved yet.
That coordination really relies on coalitions, communities, and even perhaps, to some level, regulatory bodies that would actually help bring forward and highlight the importance
The field is moving very quickly, and the regulatory bodies are trying their best to keep up and create established benchmarks that are needed for regulatory approval as best as they can. What’s becoming apparent is that getting through regulatory approval is really only step one. Whether it works in your environment or not will depend on whether the training and test data set that was used for regulatory approval looks anything like your data at any given time.
Not all of these details necessarily require more work to capture. It's about allowing the metadata to flow and having people recognise that that metadata is really important. Achieving these practices will bring forward the transparency in the data needed for meaningful calibration of the measurements.
This could mean variations in anything from the types of diseases that are more predominant in your area, to your local demographic makeup in terms of your patient population. It may also depend on the technical aspects of the scanners and protocols you are using. So there's the human biology side, and the technical side. If the technical nuances of how you're acquiring your images are very different from what was used in your training and test set, this model may not perform well in your environment.
Because of this, there’s a growing recognition that local validation is really important to understand whether a model works in your particular setting, regardless of whether it has regulatory approval. In essence, FDA approval does not mean it works everywhere by default. So, you do need to test locally (this may
I would argue that some of the pieces I mentioned earlier (having enough metadata around the data, and having the groups developing these models provide clear descriptions of their data) would help centres at least crosscompare. That could help alleviate the need for a thousand different validation exercises. There are a lot of models out there now, especially in the radiology space, and you don’t want to be testing and validating every single one. You want to identify the ones that are most likely to be relevant to you, and that will be assisted by greater transparency.
There have been discussions around what people call the metadata around the models and descriptions of the model itself. I think it would also help to have additional descriptions around the data used to develop that model. Not revealing the dataset itself, but describing how the data were acquired, the metadata around that data. That would at least allow centres to ask, at a surface level, whether it’s worth going through a full validation exercise. That kind of approach could start to bring some efficiency.
Beyond the initial validation and implementation, ongoing monitoring of model performance is also a critical step, as the data can change across the model lifecycle.
Q6You’ve previously highlighted the concept of ‘digital toxicity,’ where digital tools can unintentionally increase the burden for patients. How can clinicians and healthcare systems balance the benefits of digital technologies with the need to minimise burden and protect patient wellbeing?
It's definitely a concept we need to keep in mind as we continue to introduce digital tools into healthcare. At my organisation, we wrote an article on digital toxicity to bring awareness of the term to the oncology community,2 and we've been proactive about working to coordinate patientreported outcomes, surveys, other patients engagements across the institution, and gathering feedback; it's all very important. For instance, someone with cancer will see multiple specialists, and if the practices across specialties are not coordinating with each other, it's highly possible that same patient could be asked to fill out the same, if not similar surveys over a very short period of time.
We have met to review what surveys are going out for research and for clinical practice. How do we proactively mitigate redundant questionnaires that ask the same or very similar questions? This is a proactive activity that doesn't actually cost a lot of money; it's
all about coordination. And I think that this is something we do need to really think about, not only across organisations, but across the system. It's more challenging at the system level, but from a patient perspective, I'm sure that they would appreciate not having to fill out the same forms multiple times.
At my organisation, we wrote an article on digital toxicity to bring awareness of the term to the oncology community
It is a fine balance. We need to be confident that we have the right person and the right information, and that records are not being duplicated. In organisations with large volumes of patients, it is entirely possible to have patients with exactly the same first and last name and even possibly the same year of birth. In those cases, repeated clarifying questions can serve a clear safety purpose. The challenge is finding the right balance between repeated digital interactions with questions, surveys, forms, etc., and ensuring that processes are still convenient for patients while remaining safe and accurate.
The other aspect of digital toxicity is that many of the tools we use now could be improved simply by coordinating the flow of data more effectively. If systems spoke to each other better, people might not need to repeatedly enter the same information, even sometimes something as basic as demographic details. Other sectors, particularly marketing, have become very good at this. In healthcare, however, there are important privacy considerations that we have to work through carefully, and that is partly why some of this repetition is very intentional.
Another area where this balance comes into play is in the administrative burden that patients increasingly navigate in digital systems. There is a lot of discussion around how emerging tools might help alleviate that burden. In the USA, for example, this often relates to insurance approvals and similar processes. The question is how we can use new technologies to gather the necessary information in a way that is simpler and more intuitive, so that patients do not have to work their way through dense legal language just to understand what information is required to secure approval for treatment.
Q7You are a strong advocate for bringing together a network that cuts across clinical, research, administrative, education, industry, and STEM to bring forward mentorship, sponsorship, and lifelong learning to grow leadership across the cancer space, including through your role as Chair of Women in CancerAll in Cancer. How has this work contributed to meaningful change, and what more can institutions and leaders do to support the next generation of clinicians and researchers?
We call it Women in Cancer-All in Cancer, because we started out being a women's physicians organisation, and we actually grew to be very multidisciplinary and interdisciplinary, encompassing everyone. This is because people who weren’t women were saying: “Why can't I access these resources? This is very helpful.” And I said, “Of course, all should have access to this.” Currently we have a series that was intended to be just a 1-year series, but we've continued it on due to its popularity, and it's called “strengthening through perspectives.” If you really pause and think about that phrase, it shows that the professional challenges, the relationship challenges, and individuals’ internal challenges, whether it be imposter syndrome, negotiation, finding one’s voice or purpose or something else, are common to everybody. Everyone experiences them, but they may not realise others are on that same journey, and yet different areas and different fields or different domains of work will address it in different ways, and we can always learn from each other’s mistakes as well as successes. Also, the time to really think through and invest in personal and professional growth
is limited, so finding ways to hear from others from across the field is going to be really important.
My second point is that medicine is no longer hanging up your shackle on a wall and opening up a clinic by yourself. Medicine is growing increasingly interdisciplinary with the integration of technology. There's an increasing number of people in STEM who are coming to support medicine, people who are very dedicated and just as passionate about that patient outcome and making things better. Sharing perspectives across fields will be key to working effectively together.
We can make great discoveries, but we're not built to disseminate this out into the public across multiple markets
ones aligned with various cancer meetings including the American Society for Clinical Oncology (ASCO) and the Canadian Clinical Trials Group (CCTG). We've had interest from people outside of cancer, although we are called Women in Cancer-All in Cancer, because I think that everyone is realising that the resources and the approaches that we're taking from interactive workshops, fireside chats, and dynamic panels to leadership training is something that is applicable to their domains, regardless of where they are.
Q8
Looking ahead, what excites you most about the future of radiation oncology and quantitative imaging, and how do you see data enabling more personalised, precise, and equitable care over the next 5–10 years?
An example is that public–private partnerships and industry engagement are something that is clearly necessary for us within academia. We can make great discoveries, but we're not built to disseminate this out into the public across multiple markets; we have to partner with industry to actually make that impact happen. It needs to be coming from across fields. As the chair of WinC-AlinC, I would encourage any organisation to reach out and engage with us. We're very open to networking and partnering. For example, we have partnered with multiple organisations across radiation oncology to hold a joint hybrid meeting at the American Society for Radiation Oncology (ASTRO) Annual Meeting for the past 2 years, and we've had other
I think that integrating the quantitative imaging aspects, teasing out in vivo biology, and really pushing the breadth of what we can manipulate and achieve with radiation delivery could be very transformative. We're just scratching the surface of all that we can do with how we're actually delivering radiation.
Today, we’ve become very good at delivering radiation with a high degree of precision to exactly where we want it and currently it is largely delivered with what we call standard fractionation, hypofractionation, and stereotactic radiosurgery schedules. But there are emerging approach such as FLASH radiotherapy, delivering ultrahigh doses of radiation at super speeds, and lattice radiotherapy, delivering a mesh where some areas are treated and others are intentionally spared to have different effects on the tumour, normal tissues, and immune response. These capabilities
simply weren’t technically feasible if you rewound 15 years, but they are possible today.
Beyond the physical rate and shape of the delivery, there are still many other ways to affect the biology. How many ways can we actually modulate the dose of radiation each day or each week to certain areas while avoiding others? What portions should we be sparing? Where are the
References
1. Quantitative Medical Imaging Coalition (QMIC). Advancing Healthcare through quantitative medical imaging. Available at: https://qmic.org/. Last accessed: 24 March 2026.
immune cells sitting or circulating? There's a lot of potential to unpack there, and I think that’s really exciting. Once we start thinking about individualising that for each patient, feeding in and calibrating models to individual patient data, we're no longer saying this is a protocol that everyone goes through. We're taking the data from one patient, and fine-tuning that radiation treatment plan biologically, not just spatially,
2. Gibbons C et al. Emergence of Digital Toxicity and the Need for an Integrated, Patient-Centric Approach to the Development, Evaluation, and Use of Digital Health Tools for Oncology. JCO Clin Cancer Inform. 2024;8:2300105.
where we're targeting the tumour, but biologically manipulating how we're delivering that radiation to maximise the outcomes in terms of controlling or eradicating the tumour and minimising the side effects. We're just getting started making dramatic changes in the outcomes of radiotherapy. Not that they're not already exciting, but I think we're just getting started. Now is really an exciting time.
Simulation in Diagnostic Radiography Training: A Replacement for Clinical Placements?
Authors: *Andrew England,1,2 Clare Rainey,1 Laura McLaughlin,1 Mark McEntee1,3,4
1. University College Cork, Ireland
2. UCL University College, Odense, Denmark
3. The University of Sydney, Australia
4. University of Southern Denmark, Odense, Denmark *Correspondence to aengland@ucc.ie
Disclosure: England is an Advisory Board Member of the European Federation of Radiographer Societies (EFRS) and member of the RoClub International Advisory Board. Rainey sits on the International Advisory Panel for the Journal of Medical Radiation Sciences. McEntee is currently Vice-President of the EFRS and Deputy Editor for the Journal of Medical Imaging and Radiation Sciences. McLaughlin has declared no conflicts of interest.
Demand for medical imaging is increasing at unprecedented rates1 and many healthcare systems are struggling to cope.2 Reports from the UK NHS suggest that the demand for CT and MRI scans in England is growing by >5% per year.2 The main drivers for these increases are both growth and ageing of the global population.3 In response, workforces have been shown to grow; for example, in the UK, the radiology workforce grew by 6.3% in 2023.4 Although growth was evident, increases in service demand of approximately 11% were still noted for CT and MRI scans in the same year.4 Despite evidence of growth, respondents to a UK Diagnostic Radiography Workforce 2022 Census reported average staff vacancy rates in the region of 12.8%.5 Therefore, the growth rate does not hold pace with current vacancy rates. With rising demands for imaging unlikely to change in the foreseeable future,
workforce challenges will likely continue and possibly worsen.6 A traditional response to workforce challenges is a promise to train more healthcare professionals.7 Whilst increased capacity is possible within higher education institutions, the accompanying access to clinical placements is a major global challenge8-10 and is a key limiting factor when seeking to increase the number of diagnostic radiography students admitted for training. Given the significance of the problem, higher education institutions have been asked to consider alternatives to support increases in student training capacity. Such alternatives have included an increased role for clinical simulation11-13 and alternative work-integrated learning, e.g., university-based, industry, and within independent imaging providers. Over recent years, particular growth and interest have been reported using medical simulation. This growth has resulted mainly from recent advancements in profession-specific simulator technologies but also responses
to training needs during the COVID-19 pandemic.14 There are now increased options available in terms of 1) the range and quality of simulation possibilities for diagnostic radiography education and 2) the roles for simulation within the curriculum, particularly the potential impact on the requirements for traditional clinical placements. This article, through a review of relevant peerreviewed literature and policy documents, aims to highlight the range of simulation possibilities within pre-registration diagnostic radiography training and discuss the potential for simulation in terms of substituting or supporting the traditional clinical placement experience.
According to Issenberg and Scalese,15 simulation aims “to imitate real patients, anatomic regions, or clinical tasks or to mimic real-life situations in which healthcare services are delivered.” Within the diagnostic radiography field, different simulators exist (Table 1), including parttask trainers, simulated patients, simulated environments, virtual reality and haptic systems, computer-based simulators, and integrated simulators.17
It is clear by the vast array of simulation options available that ‘one size does not fit all’. Within any curricula, inclusive pedagogies must be balanced to cater to the full range of learners.18 Currently, the inclusion of simulation in training curricula is governed by multiple factors. These include budgets, simulator availability and quality, student attendance patterns, institutional pedagogical culture, and access to university clinical skills facilities and traditional clinical placements. In many jurisdictions, national regulatory agencies may also place restrictions regarding the use of simulation within radiography education. For example, as part of the UK Nursing and Midwifery Council (NMC) COVID-19 recover programme, up to 600 hours of simulated practice learning experience was permitted.19 By contrast, the UK Royal College of Occupational Therapists (RCOT) provided simulation guidance in the region of 40 hours.20 It is important to note that whilst the quantity of simulation is important, quality remains a significant factor. The quality of simulation technology is likely to also play
a significant role in the wider utilisation and adoption. Within radiography education, in the UK, the Society and College of Radiographers (SCoR) has proposed 120 hours of simulation as a recommendation within pre-registration curricula.21
The landscape of simulation within diagnostic radiography education has rapidly evolved; however, detailed guidance, although originally sparse, is now growing. The European Federation of Radiographer Societies (EFRS), in 2021, published a Preliminary Statement on Simulation in Radiography Education.22 Whilst acknowledging many potential advantages for including simulation, this statement also highlighted distinct challenges. These include the need for evidence of the efficacy of using simulation for competency assessments, requirements for educator training in the effective use of simulation, and the need to provide a detailed scope of the requirements for simulation with reference to those technologies focusing specifically on diagnostic radiography. During 2025, the UK SCoR published a simulation model23 and a position statement on the use of simulation in enhancing pre-registration education.21 Outside of radiography education, there are internationally accepted standards for simulation. The Association for Simulated Practice in Healthcare (ASPiH) Standards, published in 2023, focus on elements of theory and evidence-based-practice which are applicable across the broad spectrum of health and care training programmes.24 Other standards and best practice documents have been published, including those from the International Nursing Association for Clinical Simulation and Learning (INACSL),25 Society for Simulation in Healthcare (SSH),26 and the Association of Standardized Patient Educators (ASPE).27 Educators should embrace such documents when designing and implementing simulation into curricula.
Correct selection of a simulation option includes the choice of technology and the role. In many institutions, this includes teaching, learning, and assessments. Decisions regarding the fit of simulation will largely be based on the intended learning outcomes and the previously identified factors, i.e., availability. To alleviate some
Table 1: Summary of simulation options available within diagnostic radiography.
Computer-based simulation
VR
Use of ProjectionVR™ or ScanLabMR to simulate the procedural steps in an X-ray examination.
Use of X-Ray Pro VR Suite to simulate the procedural steps in an X-ray examination.
AR Limited applications in DR training.
MR
Limited applications in DR training.
Simulated participants Explain imaging examinations to an actor.
Simulated clinical immersion
Procedural simulation
Part-task trainers
Manikins
Low technology
Hands-on practice in university or college clinical skills lab, i.e., X-ray room.
• Self-directed
• Accessible
• Repeat practice
• Objective metrics
•Reduced requirement for fixed X-ray facilities
•Solo use
•Real-world environment
•Solo user
•Great potential for visual and spatial learning
•Highly repeatable
•Targeted feedback
•Good replication of real patients
•High realism
•Actual work environment
Disadvantages
• Technology dependent
• Limited feedback
•Hardware/software costs
•Nausea/vertigo
•Limited haptics
•Setup costs
•Access to the clinical environment needed
• Blurring between AR/VR.
•Logistic and resource intensive
•Psychological safety of participants
•Resource and cost intensive
•Requires imaging suite access
High technology
Upper limb simulator for intravenous cannulation.
Use of the PIXY Phantom in skills labs.
Use of the PIXY Phantom to practice different radiological examinations in a skills lab.
SimMan® 3G used in an anaphylaxis scenario following iodinated contrast administration.
challenges of increasing the radiographer workforce, one of the dominant questions is to what extent can simulation replace the traditional clinical placement environment? Questions have arisen as to whether radiography training could be delivered
with significant utilisation of simulation and without seeking or severely limiting access to the clinical environment. Some commentators might suggest that this could be a step too far.28 Technical glitches and an inability to directly palpate the patient
have been highlighted within the literature as potential issues with some simulators.29 Still, some advocate that, given contemporary developments in pedagogies and simulator technologies, simulation could substantially increase its position within training curricula. Much needed guidance on this has arrived from a report delivered in conjunction from the University of Bradford, Society of Radiographers (SOR), and NHS England.21 Within the UK, 120 hours of simulation education is now recommended for preregistration radiography education. Such developments help foster wider discussions regarding a review of the role of traditional clinical placements and the requirement for a preset quality of ‘clinical’ placement hours. For example, in Ireland, the State regulator, CORU, has reduced the requirement for formal clinical placement hours from 1,200 to 1,000.30,31 Several institutions now advertise in their marketing literature that clinical experience will be a composite of time within clinical departments and university simulation suites, in addition to other pedagogical approaches.32,33
The degree to which the increased use of simulation can expand clinical placement capacity is not currently known. However, in some institutions, a larger student capacity has been possible due to the wider incorporation of simulation support within training curricula.34 In these instances, it is likely that simulation has been introduced to provide essential clinical skills training within the academic environment. Formal robust and objective evaluations of the ability of simulation to achieve the required learning objectives are limited within radiography education. Outside of radiography, studies have shown that simulation can improve clinical skills.35-37 Can simulation be used to train more radiographers? The role of simulation in the aviation industry is not designed to support the training of more pilots. The role of simulation in these instances is to provide experience and evaluations of competencies in rare scenarios, for example, engine failure or extreme adverse weather conditions.38 Even despite the restricted role of simulation in aviation, roles are diversifying and even commercial computer-based flight simulators are considered as ‘flying hours’ by
Note the placement of an intravenous cannula in the right arm, and as such, this mode of simulator could be used in relation to the training of contrast administration during radiological examinations or the management of anaphylaxis.
Figure 1: An example of a high-fidelity simulator used in nursing and midwifery education.
some regulatory authorities.39 Within other areas of healthcare, simulators are a popular training option. For example, virtual reality simulation is reported to play a crucial role in modern surgical training and avoids the need to train ‘on the patient’.40 Similarly, in anaesthesia, the use of simulators in clinical skills training has been an option for over 60 years.41 Likewise, simulation has been used widely in nursing and midwifery education (Figure 1) and has been documented as a valuable strategy for teaching, learning, and evaluating clinical skills.42
Bridge and colleagues43 conducted a Delphi study to assess stakeholders’ opinions regarding partially replacing traditional clinical training hours with simulation for the nursing, occupational therapy, orthoptics, physiotherapy, and radiography professions. The consensus opinion from this study was that between 11–30% of clinical training time could be replaced by a simulated placement. While supporting a reduction, stakeholders in the study by Bridge et al.43 did not advocate the complete replacement of clinical
placements by simulation. They also did not consider the potential of simulation as a part replacement to current clinical placement rotations. For example, if used with traditional placements, could simulation accelerate the time required to reach designated competencies?
Public perception and acceptance of the role of simulation in pre-registration training is paramount (Figure 2). There is consensus in the literature that the public supports the growth of simulation and favours those demonstrating higher levels of fidelity. Despite this, many would argue that simulation is a supplementary tool and not a direct replacement for experience with patients. By way of an example, patients were more accepting of medical students performing a procedure if they had undertaken training on a simulator, although there were some exceptions, including suturing and intubation tasks.44 A successful health service is based around public confidence in the competencies of the healthcare professionals who work within. Many in wider society might question a bus
Note perceptual differences from real patients may reduce realism.
Figure 2: An example of an abdominal anthropomorphic phantom used in CT training.
driver who has solely trained on a simulator or agree to undergo a surgical procedure that has only ever been performed on a simulator. Arguably, traditional clinical placements are not perfect either, and there are frequent media reports about healthcare errors relating to clinical malpractice. A further study, based in surgery, investigated patient and public perceptions of simulation training and reported that both groups were accepting, but improved access and technological developments for simulators were required.45
Defining the role for simulation within pre-registration training is multifactorial. Questions arise, such as should the role, quality, and quantity of simulation in preregistration radiography training be based on robust empirical evidence? One might argue that other areas of radiography training are not subject to such rigor. Also, is it within an educator’s professional role to determine the most appropriate pedagogical approach? Given the rise in availability and complexity of simulation, its use is likely to increase. Managing and harmonising the use of simulation is only likely to be achieved with clear guidance from professional bodies and regulators; fortunately, this is now arriving. If clinical placement provision were an infinite resource, it is likely that discussions regarding simulation and changes to teaching and learning practices would be fewer and far between. This is not the world we live in and demands on healthcare will continue to rise at unprecedented levels. Meeting the challenges of the day will require all hands to the pumps. Achieving this requires inclusion of simulation within all aspects of teaching and learning, but knowing that it is an educational tool to be used alongside others. Developing a
References
1. Maskell G. Why does demand for medical imaging keep rising? BMJ. 2022;379:o2614.
2. NHS England. Diagnostics recovery and renewal. 2020. Available at: https://www.england.nhs.uk/ wp-content/uploads/2020/10/ BM2025Pu-item-5-diagnostics-
stronger evidence base is likely to help with acceptance and procurement but should not preclude the use of simulation in the interim. Professional bodies and regulators must continue to help develop the evidence and guide the inclusion of simulation within health professional training.
CONCLUSION
When considering the current simulation status in diagnostic radiography training, the conclusion is that it is both a substitute and an adjunct. Clinical placement time is decreasing in many jurisdictions but is not being eliminated entirely, possibly because of the increased use of simulation. Simulation is not without frailties, in that annual subscriptions can be expensive and technical support is often required to ensure effective utilisation. Many radiography schools with relatively low cohort sizes may feel that access to a physical skills X-ray room is sufficient. As cohorts grow, the time available for individual students to learn in a physical environment will become less and, possibly, simulation can then play a part. Simulation also provides opportunities to learn about rare events and, thus, is instrumental as an accompaniment to training. Given how quickly technology can advance and the recent milestones that we have seen in AI, it might one day be possible for all clinical training to be simulator-based; for better or worse, we are not there yet. The landscape of simulation with diagnostic radiography looks bright, and all stakeholders should encourage the responsible development and implementation of such technologies into practice.
recovery-and-renewal.pdf. Last accessed: 10 March 2026.
3. Royal College of Radiologists (RCR). Clinical radiology workforce census 2022. 2022. Available at: https:// www.rcr.ac.uk/media/qs0jnfmv/rcrcensus_clinical-radiology-workforcecensus_2022.pdf. Last accessed: 10 March 2026.
4. Royal College of Radiologists (RCR). Clinical workforce census report 2023. 2023. Available at: https:// www.rcr.ac.uk/media/5befglss/rcrcensus-clinical-radiology-workforcecensus-2023.pdf. Last accessed: 10 March 2026.
5. Society & College of Radiographers (SoR). Diagnostic radiography workforce UK census 2022. 2022.
Available at: https://www.sor.org/ getmedia/6994cd5d-0155-4a7ea8a7-32a9bbda81c3/DiagnosticRadiography-Workforce-UK-Census2022-report.pdf. Last accessed: 10 March 2026.
6. Kalidindi S, Gandhi S. Workforce crisis in radiology in the UK and the strategies to deal with it: is artificial intelligence the saviour? Cureus. 2023;15(8):e43866.
7. Department of Health and Social Care. NHS workforce stats for May 2023: record numbers of doctors and nurses in NHS. 2023. Available at: https:// healthmedia.blog.gov.uk/2023/05/25/ nhs-workforce-stats-for-may-2023record-numbers-of-doctors-andnurses-in-nhs/. Last accessed: 10 March 2026.
8. Williams P et al. Clinical education and training: using the nominal group technique in research with radiographers to identify factors affecting quality and capacity. Radiography. 2006;12(3):215-24.
9. Kyei K et al. Challenges faced by radiography students during clinical training. Clin Med Res. 2015;4(31):36-41.
10. Fairbrother M et al. A new model of clinical education to increase student placement availability: the capacity development facilitator model. Asia-Pac JCoop Educ. 2016;17(1):45-59.
11. Kong A et al. The role of simulation in developing clinical knowledge and increasing clinical confidence in first-year radiography students. Focus Health Prof Educ. 2015;16(3):29-44.
12. Partner A et al. First year student radiographers’ perceptions of a oneweek simulation-based education package designed to increase clinical placement capacity. Radiography (Lond). 2022;28(3):577-85.
13. England A et al. Clinical radiography education across Europe. Radiography (Lond). 2017;23(Suppl 1):S7-S15.
14. Bridge P et al. International audit of simulation use in pre-registration medical radiation science training. Radiography (Lond). 2021;27(4):1172-8.
15. Issenberg SB, Scalese RJ. Simulation in health care education. Perspect Biol Med. 2008;51(1):31-46.
16. Goodwin B, Nestel D. Demystifying simulators for educators in healthcare. Int J Healthc Simul. 2024;DOI:10.54531/muif5353.
17. Vestbøstad M et al. Research on simulation in radiography education: a scoping review protocol. Syst Rev. 2020;9(1):263.
18. Linaker KL. Pedagogical approaches to diagnostic imaging education: a narrative review of the literature. J Chiropr Humanit. 2015;22(1):9-16.
19. Nursing and Midwifery Council (NMC). Current recovery programme standards NMC. 2022. Available at: https://www.nmc.org.uk/globalassets/ sitedocuments/education-standards/ current-recovery-programmestandards.pdf. Last accessed: 10 March 2026.
20. Royal College of Occupational Therapists (RCOT). Learning and development standards for pre-registration education Revised Edition. 2019. Available at: https://www.rcot.co.uk/exploreresources/standards-guidelines/ learning-development-standards. Last accessed: 10 March 2026.
21. College of Radiographers (CoR) Position statement: College of Radiographers update on practicebased learning hours for preregistration diagnostic radiography and therapeutic radiography programmes. 2025. Available at: https://www.sor. org/getmedia/180b6671-57d7-4d4fa0f4-bbf9c8e8d9e6/1-2-PositionStatement-PBL_D1-3_final-for-upload. Last accessed: 10 March 2026.
22. European Federation of Radiographer Societies (EFRS). EFRS preliminary statement on simulation in radiography education. 2021. Available at: https:// api.efrs.eu/api/assets/posts/257. Last accessed: 10 March 2026.
23. College of Radiographers (CoR). The role and efficacy of simulation in preregistration education and training of diagnostic radiographers: a simulation model for pre-registration diagnostic radiography education and training. 2025. Available at: https://www.sor. org/getmedia/cd77c5cf-780d-4087a21e-64e468042e71/1-3-Simulationmodel-report_plus-appendix-NEWfinal-for-upload-v3. Last accessed: 10 March 2026.
24. Diaz-Navarro C et al. The ASPiH standards 2023: guiding simulationbased practice in health and care. Int J Healthc Simul. 2023;DOI:10.54531/ nyvm5886.
25. Committee IS et al. Onward and upward: introducing the Healthcare Simulation Standards of Best PracticeTM. Clin Simul Nurs. 2021;58:1-4.
26. Diaz-Navarro C et al. Global consensus statement on simulation-based practice in healthcare. Simul Healthc. 2024;19(3):e52-9.
27. Lewis KL et al. The Association of Standardized Patient Educators (ASPE) standards of best practice (SOBP). Adv Simul (Lond). 2017;2:10.
28. Bokken L et al. Strengths and weaknesses of simulated and real patients in the teaching of skills to medical students: a review. Simul Healthc. 2008;3(3):161-9.
29. O'Connor M et al. 3D virtual reality simulation in radiography education:
the students' experience. Radiography (Lond). 2021;27(1):208-14.
30. CORU. Criteria for education and training programmes for radiographers. 2013. Available at: https://coru.ie/ health-and-social-care-professionals/ education/criteria-and-standardsof-proficiency/criteria-for-educationand-training-programmes-forradiographers1.pdf. Last accessed: 10 March 2026.
31. CORU. Regulatory impact assessment - revised standards of proficiency and criteria for education and training programmes (radiographers and radiation therapists). 2024. Available at: https://coru.ie/public-protection/ publications/consultation-reports/ radiographers-registration-board/1regulatory-impact-assessment-rrbstandards-and-criteria-vfinal.pdf. Last accessed: 10 March 2026.
32. Keele University. Keele trains next generation of radiographers using virtual reality in regional first. Available at: https://www.keele.ac.uk/about/ news/2024/november/virtual-reality/ radiographers-staffordshire-training. php#:~:text=The%20software%20 covers%20a%20full,simulation%20 suite%20at%20Keele%20University. Last accessed: 10 March 2026.
33. University College Dublin (UCD). Radiography BSc (NFQ Level 8). Available at: https://hub.ucd.ie/ usis/!W_HU_MENU.P_PUBLISH?p_ tag=COURSE&MAJR=MDS4&KEY WORD=bsc%20radiography. Last accessed: 10 March 2026.
34. University of Cumbria. The University of Cumbria empowers the next generation of diagnostic radiographers with immersive training opportunities. Available at: https://news.cumbria. ac.uk/news/the-university-of-cumbriaempowers-the-next-generationof-diagnostic-radiographers-withimmersive-training-opportunities. Last accessed: 10 March 2026.
35. Bergmann J et al. Virtual reality to augment robot-assisted gait training in non-ambulatory patients with a subacute stroke: a pilot randomized controlled trial. Eur J Phys Rehabil Med. 2018;54(3):397-407.
36. Mackay EC et al. Simulation as an effective means of preparing trainees for active participation in MDT meetings. Future Healthc J. 2024;11(1):100017.
37. Lembo D et al. Early introduction of simulation in the medical curriculum: the MedInTo perspective. Front Med (Lausanne). 2023;10:1280592.
38. Lazic D et al. The role of flight simulation in flight training of pilots for crisis management. South Florida J Dev. 2022;3(3):3624-36.
39. Rizvi SAQ et al. Exploring technology acceptance of flight simulation training
devices and augmented reality in general aviation pilot training. Sci Rep. 2025;15(1):2302.
40. Sparn MB et al. Virtual reality simulation training in laparoscopic surgery - does it really matter, what simulator to use? Results of a cross-sectional study. BMC Med Educ. 2024;24(1):589.
41. Abrahamson S. Sim One--a patient simulator ahead of its time. Caduceus. 1997;13(2):29-41.
42. World Health Organization (WHO). Simulation in nursing and midwifery education. 2018. Available at: https://
iris.who.int/server/api/core/bitstreams/ dd106982-ce37-47bf-a134296a4a69d3de/content. Last accessed: 10 March 2026.
43. Bridge P et al. Simulated placements as partial replacement of clinical training time: a delphi consensus study. Clin Simul Nurs. 2022;68:42-8.
44. Graber MA et al. Does simulator training for medical students change patient opinions and attitudes toward medical student procedures in the emergency department? Acad Emerg Med. 2005;12(7):635-9.
45. Burton OE et al. Patient and public perceptions of simulation training in neurosurgery: a two-stage cross-sectional survey. World Neurosurg. 2025;196:123746.
Universal Non-invasive Cardiac Imaging: Which Modality Best Combines Anatomy and Physiology?
Editor's Pick
This review provides a timely and comprehensive synthesis of the current landscape, examining key modalities, including coronary CT angiography with fractional flow reserve, PET-coronary CT angiography, and cardiovascular magnetic resonance. In doing so, it highlights the growing potential of hybrid imaging to improve diagnostic specificity, better characterise functionally significant disease, and reduce reliance on invasive diagnostic pathways. Particularly notable is the discussion of PET-coronary CT angiography, which offers enhanced specificity through the combined assessment of myocardial perfusion and coronary anatomy within a single imaging session. Importantly, the authors do not overlook the ongoing challenges associated with these approaches, including issues of cost, accessibility, and the evolving role of AI in image acquisition and interpretation. These considerations are critical as the field moves towards wider implementation.
Sophie Willis
University of Lincoln, UK
Authors: Faiz Saulat,1 Rushi Patel,1 David King,1 Tawfiq Khasawneh,1 Noah Blaker,1 Shengyi Fu,1 Christian Eskander,1 Caroline Lunny,2 Anjalika Chalamgari,2 Jonathan Van Name,1 Kosidinma Oguejiofor,2 *David Winchester3
1. Department of Medicine, University of Florida, Gainesville, USA
2. College of Medicine, University of Florida, Gainesville, USA
3. Division of Cardiovascular Medicine, University of Florida, Gainesville, USA
*Correspondence to David.Winchester@medicine.ufl.edu
Disclosure: Winchester serves on the American Society of Nuclear Cardiology Board of Directors and the American College of Cardiology Board of Trustees. The other authors have declared no conflicts of interest.
Cardiac imaging is crucial for diagnosing and managing coronary artery disease. While most imaging modalities focus on either anatomical or physiological assessment of coronary artery disease, novel hybrid techniques capable of providing both in a single imaging session represent an important advancement in the field. This review summarises the technique, diagnostic performance, clinical utility, limitations, and cost-effectiveness of the principal hybrid modalities: coronary CT angiography (CCTA) c, PET with CCTA (PET-CCTA), and cardiovascular magnetic resonance (CMR) imaging. CCTA with fractional flow reserve applies computational fluid dynamics modelling to standard CCTA data to derive non-invasive fractional flow reserve estimates without additional radiation or contrast exposure. Diagnostic accuracy, at appropriate values, can be high enough to reduce rates of invasive coronary angiography. The application of AI to CCTA for automated plaque quantification and stenosis grading is promising but currently limited by its discordance with invasive angiography. PETCCTA combines myocardial perfusion imaging with coronary anatomy in a single session with higher specificity than CCTA alone, but at the cost of greater radiation exposure. Finally, CMR provides radiation-free tissue characterisation across multiple techniques such as stress perfusion, late gadolinium enhancement, and strain imaging, each with their unique features. Taken together, PET-CCTA currently offers the most robust integration of anatomy and physiology, while CMR continues to advance rapidly as a compelling alternative, particularly where radiation-free evaluation is preferred. The authors have summarised key evidence on how these hybrid approaches enhance detection of obstructive coronary stenosis, guide therapeutic decisions, and how these technologies are implemented today.
Key Points
1. Non-invasive cardiac imaging modalities typically address either anatomical or physiological assessment of coronary artery disease. Emerging hybrid techniques address both in a single imaging session, potentially reducing unnecessary invasive procedures.
2. This narrative review evaluates the diagnostic performance, clinical utility, limitations, and cost-effectiveness of coronary CT angiography (CCTA) with fractional flow reserve, PET-CCTA, and cardiovascular magnetic resonance imaging as hybrid approaches integrating coronary anatomy with functional assessment.
3. PET-CCTA currently offers the most robust combined anatomical–physiological assessment, while cardiovascular magnetic resonance imaging provides compelling radiation-free alternatives. Clinicians should tailor modality selection to patient-specific factors and clinical context.
INTRODUCTION
Non-invasive cardiac diagnostic imaging is an integral component of coronary artery disease (CAD) identification, risk stratification, and disease management. The anatomic and physiologic information derived from the different imaging modalities shapes the disease and treatment course.1 Most imaging techniques excel at either anatomic or physiologic information about CAD. CT is excellent for assessing anatomic changes of the structures of the heart, and coronary CT angiography (CCTA) has become one of the most frequently used non-invasive imaging modalities to diagnose
CAD, specifically in patients presenting with angina with no history of CAD.1 In contrast, PET is limited in its ability to provide anatomic data but excels at assessing physiologic information.2 Cardiovascular magnetic resonance (CMR) imaging and its various techniques can provide both structural and functional information.3
Both anatomic and physiologic variables are valuable in making clinical decisions, and novel hybrid techniques have been developed to provide both in a single non-invasive imaging test. Examples include CCTA with fractional flow reserve (CCTA-FFR) and cardiac PET with
CCTA (PET-CCTA). Advances in CMR imaging techniques have also allowed for improvements in coronary magnetic resonance angiography (CMRA), CMR with strain imaging, CMR–PET, and more to offer similar anatomic and physiologic data. Blending anatomic and physiologic imaging techniques can potentially expedite risk stratification, enhance clinical understanding, and reduce unnecessary invasive procedures.4 Recent trials have demonstrated that many patients with stable coronary disease can be managed conservatively, helping clinicians identify patients who can be safely treated without invasive procedures.5 This review provides an overview of the current hybrid cardiac imaging modalities and discusses their techniques, advantages and disadvantages, outcomes, utility, and cost in the diagnosis and management of CAD.
CARDIAC CT
CCTA involves intravenous administration of contrast to enhance visualisation of the coronary arteries during a high-resolution, ECG-gated CT scan. According to the 2021 guidelines from the American Heart Association (AHA) and the American College of Cardiology (ACC), CCTA has Class I-A evidence in intermediate-risk patients with acute chest pain and no known CAD, and Class IIa-B non-randomised evidence in patients with inconclusive or abnormal stress testing.6 Because of its high negative predictive value for ruling out significant disease, defined as >70% luminal stenosis in at least one major coronary artery or >50% stenosis in the left main coronary artery, the use of CCTA in the diagnostic and management pathways of CAD is increasing.1,6 Two pivotal randomised trials have since provided long-term outcome data reinforcing CCTA’s value beyond its established rule-out capability. In the PROMISE trial (N=10,003; median follow-up 10.6 years), initial test selection did not affect mortality, but any CCTA abnormality, including non-obstructive disease, conferred elevated long-term risk (adjusted hazard ratio: 1.99–3.44), whereas only severely abnormal stress results were prognostically significant.7 The SCOT-
HEART trial (N=4,146; 10-year follow-up) demonstrated that adding CCTA to standard care reduced coronary heart disease death or non-fatal myocardial infarction (hazard ratio: 0.79; 95% CI: 0.63–0.99; p=0.044), driven by increased preventive therapy use without excess revascularisation.8 These findings underscore that CCTA’s detection of atherosclerosis provides a managementrelevant anatomic foundation upon which hybrid physiologic assessments can build.
CCTA-FFR
CCTA-FFR is an adjunct to CCTA that provides FFR measurements calculated through computational fluid dynamics modelling algorithms, with the goal of non-invasively determining the severity of coronary stenosis.9-11 CCTA-FFR is an add-on test that does not require additional exposure to radiation or administration of contrast agents beyond those used for acquisition of the original CCTA.11 It uses advanced computational models to build a 3D, patient-specific model of coronary anatomy and provide FFR estimates for each lesion. These models are calibrated against invasive coronary angiography (ICA) FFR, in which values ≥0.80 can rule out ischaemia.12
In a systematic review published in 2017, the authors concluded that the diagnostic accuracy of CCTA-FFR varies markedly across the spectrum of CAD. Accuracy was highest when lesions were identified with CCTA-FFR values lower than 0.63 or above 0.83, but lower with values between 0.63–0.83, where FFR is most needed to help rule in or out ischaemic lesions.13 Ultimately, the authors suggested that by using CCTA-FFR in combination with patient-specific factors, clinicians may be able to identify cases in which cost and risk of an ICA may safely be avoided. Other trials and systematic reviews have offered similar findings and conclusions for CCTA-FFR to be used as an adjunct to clinical acumen.14-16 Limitations of CCTA-FFR are similar to standard CCTA: motion artefact, obstruction to the lumen by coronary artery calcification, use of iodinated contrast, and ionising radiation.17 Coronary calcification is especially prevalent in patients with longstanding chronic
kidney disease or diabetes, in whom heavy vascular calcification frequently produces blooming artefacts that obscure luminal assessment and reduce CCTA diagnostic accuracy.17 CCTA-FFR-specific limitations include reduced validity in patients with coronary stents, bypass grafts, coronary anomalies, transcatheter aortic valve replacement, and more.4,17
CCTA-FFR Discussion
A brief note regarding limitations in CCTAFFR: emerging photon-counting detector CT offers improved spatial and contrast resolution and reduced artefact, with particular advantages for evaluating heavily calcified vessels and small-calibre stents. In a comparative study, photon-counting detector CT demonstrated significantly higher diagnostic accuracy than conventional CT for detection of >50% and >70% stenosis at the patient, vessel, and segment level, reducing use of ICA.18
When it comes to financial implications, the PLATFORM trial found that when CCTA-FFR was used prior to percutaneous coronary intervention in patients with stable, new onset chest pain, total healthcare costs were 33% lower at 1 year.19 The UK-based FORECAST trial and its USA cost analysis found that CCTA-FFR did not significantly reduce overall cardiovascular care costs at 9 months compared to CCTA or stress imaging alone, though it did reduce the rate of ICA.20,21 Another UK-based study showed that CCTA-FFR was slightly more expensive than CCTA alone, with a mean per-patient increase of 44.97 GBP, but it accelerated time to definitive diagnosis and reduced unnecessary invasive procedures.22 Although there may be slightly higher upfront costs with CCTA-FFR depending on the healthcare system, reducing the rate of invasive procedures may decrease overall healthcare costs in the long term.
AI in Cardiac CT
Beyond computational modelling, AI techniques have emerging applications in CCTA, particularly in image acquisition, reconstruction, and interpretation.23,24 The REVEALPLAQUE study applied an AI
algorithm to compare plaque assessment on CCTA with intravascular ultrasound (IVUS).25 Clinically stable patients with known CAD underwent CCTA-FFR, followed by ICA and IVUS. CCTA images were processed with an AI algorithm, which calculated total plaque volume, lumen volume, vessel volume, calcified plaque volume, and noncalcified plaque volume. Compared with IVUS, the system performed well regarding its primary endpoint of total plaque volume and secondary endpoints, including calcified plaque volume, non-calcified plaque volume, lumen volume, and vessel volume (r=0.91, 0.91, 0.87, 0.93, and 0.94, respectively; p<0.001 for all). However, performance was weaker for low-attenuation plaques (r=0.28). The spatial resolution of CCTA (approximately 0.5 mm) is lower than that of IVUS (approximately 0.04–0.20 mm), which may reduce sensitivity for detecting small or thin low attenuation plaques, particularly in smaller vessels. A CREDENCE trial substudy compared AI-enhanced CCTA to ICA.26 While the authors of this study are confident in their results showing similar accuracy between AI-enhanced CCTA and ICA, there were significant inconsistencies identified. False positives occurred when AI-enhanced CCTA overestimated stenosis due to high calcification or poor lumen opacification. False negatives occurred when AI-enhanced CCTA detected significant stenosis that ICA did not confirm. Among 157 vessels classified as having ≥70% stenosis by AIenhanced CCTA, 62 cases (39.4%) were discordant with ICA findings. Notably, 41 of these discordant cases demonstrated FFR <0.8, suggesting that AI-enhanced CCTA may capture physiologic significance that traditional ICA underestimates, due to its 2D assessment compared with 3D AIbased analysis. However, the authors did not address diagnostic and management challenges in the remaining 21 cases where AI detected significant stenosis without true functional lesions (patients who may be exposed to unnecessary invasive testing).
AI in Cardiac CT Discussion
Given the current limitations of AI-enhanced CCTA, it remains unclear whether this technology should be routinely incorporated into the diagnosis and management of CAD.
Present models lack precision in evaluating lesions, particularly low-attenuation plaque. The degree of discordance between AI and physician interpretation remains substantial and may result in ambiguous findings that lead to unnecessary invasive testing on an individual basis. Nonetheless, existing studies underscore that, while AI-enabled CCTA is not yet perfected, it is an active area of research and a promising avenue for future growth.
With continued advancements, AI models are expected to support physicians more effectively, narrowing the gap between computer- and physician-read CCTA. Its potential cost-effectiveness will depend largely on the ability to reliably rule out ischaemia-provoking CAD and thereby reduce the need for downstream invasive testing, such as ICA.27
PET with Cardiac CT
PET myocardial perfusion imaging uses radiotracers to provide detailed information on myocardial perfusion and metabolic activity, which is crucial for evaluating the functional significance of CAD.2 It is particularly useful for detecting ischaemia and assessing myocardial viability. Diagnosing CAD via PET has sensitivities of 90–94% and specificities of 79–90%.28 PET can be performed as a myocardial perfusion study alone or in conjunction with coronary flow reserve (CFR). PET-derived CFR is a quantitative, non-invasive measure of the ratio between maximal (hyperaemic or stress) and resting myocardial blood flow, obtained using PET tracers administered during the scan.29,30 CFR is measured by acquiring dynamic PET images at rest and during pharmacologic vasodilation, followed by kinetic modelling to quantify the coronary circulation’s ability to augment blood flow in response to increased myocardial demand. When applied to obstructive CAD, this technique has demonstrated a sensitivity of 90% and a specificity of 88%.31
PET-CCTA Hybrid Imaging
The novel PET-CCTA hybrid imaging modality combines PET myocardial perfusion imaging and CCTA in a
single session, providing simultaneous anatomical and physiological assessment of CAD.32 This integration theoretically enhances the diagnostic accuracy for non-invasively detecting CAD, evaluating tissue ischaemia in the same imaging session, and maintaining the ‘rule out’ feature of CCTA alone.33-35 The process of capturing PET-CCTA images starts with CCTA performed first, followed by PET, often using radiotracers (most commonly rubidium-82 [82Rb] or 13N-ammonia [13NH3]) and pharmacologic stressors, such as regadenoson.36 Fused comprehensive images show both anatomical and physiological information, allowing direct correlation of perfusion defects with specific coronary lesions. A 2018 metaanalysis compared hybrid imaging to CCTA for the diagnosis of obstructive CAD. It showed that PET-CCTA had a sensitivity and specificity of 87% and 96%, respectively, compared to 90% and 66% for CCTA alone.37 While the change in sensitivity was not statistically significant, the improvement in specificity was p<0.05. The authors discuss that the increased specificity makes PET-CCTA and other hybrid imaging modalities efficient, noninvasive diagnostic tools to help rule in lesions that may be intervenable and avoid targeting non-functionally limiting lesions. Similar findings were reported in a prospective study of 208 patients that compared multiple non-invasive imaging modalities against invasive FFR as the reference standard.38 PET-CCTA improved specificity to 92% compared with 84% for PET alone, but decreased sensitivity to 74% from 87%. The authors attributed the reduction in sensitivity largely to the small sample size. Nonetheless, the higher specificity supports PET-CCTA’s ability to identify lesions appropriate for invasive targeting based on functional as well as anatomical data.
PET-CCTA Discussion
Given the mixed evidence regarding sensitivity, CCTA alone remains a reasonable option for low-risk patients without prior CAD when the clinical aim is to rule out disease. However, PET-CCTA may offer particular value in patients with known non-
obstructive CAD who present with new or progressive symptoms, or in cases where CCTA is limited, such as heavily calcified lesions that are frequently overestimated. Limitations of PET-CCTA include higher radiation exposure compared with CCTA alone, owing to the combined CT and PET components.39 The use of iodinated contrast agents also poses risks in patients with severe renal dysfunction or contrast allergy.6 Accessibility remains a challenge, as PETCCTA requires specialised hybrid scanners and radiotracer supply (e.g., on-site cyclotron for 13NH3 or generator for 82Rb), which are not universally available. Cost is another barrier: patients utilising in-network radiology providers pay on average 319 USD for PET myocardial perfusion studies, with some estimates exceeding 1,000 USD.40
Cost analyses directly comparing PETCCTA with other non-invasive modalities are limited, though it is anticipated to be more expensive than PET alone.
CMR IMAGING
CMR imaging allows assessment of cardiac function, ischaemia, viability, and tissue characterisation within a single scan.41 Over the past decade, numerous studies have established its role in stable CAD, contributing important technical advances, large-scale clinical validation, and prognostic data. As a result, CMR has emerged as a valuable tool for diagnosis and risk stratification in CAD.6,31 CMR offers several advantages over other imaging modalities. It is particularly useful in patients where minimising radiation exposure is important, such as younger individuals or pregnant women. Compared with nuclear imaging, CMR provides superior spatial resolution, and, unlike echocardiography, it is not limited by acoustic window constraints.42 It also provides better temporal resolution than cardiac CT.43 These characteristics make it a strong modality for evaluating ventricular anatomy and function, including wall motion abnormalities.
Stress Perfusion CMR
Stress perfusion CMR is unique in its ability to directly visualise the myocardium
during stress. Its high spatial resolution allows comparative assessment both between myocardial segments and between the epicardium and endocardium. Tissue characterisation with T1, T2, late gadolinium enhancement (LGE), and blood oxygen level-dependent imaging enables identification of scar, haemorrhage, oedema, and regional hypoxaemia.
Multiple meta-analyses and prospective multicentre studies report a sensitivity of 78.9–91.0%, a specificity of 81.0–86.8%, and an area under the curve of 0.84–0.87 for detecting significant CAD, defined as ≥70% stenosis by ICA or FFR. Negative predictive value is high, with 1-year event rates for cardiovascular death <1% following a negative test.31,44-48 Another technique, CMRA, visualises the coronary arteries directly using MRI.49,50 CMRA can also provide information on coronary artery distensibility, plaque characteristics, and plaque inflammation.50 Depending on the protocol, vasodilators, inotropes, or exercise are used to evaluate myocardial blood flow under stress, followed by administration of a gadolinium-based contrast agent to assess myocardial scar and viability.51 According to the American College of Radiology (ACR), non-contract CMRA is most useful for visualising the coronary tree in symptomatic patients with intermediate or high pretest probability, particularly for ruling out significant CAD. Its diagnostic yield is further enhanced when combined with stress perfusion and/or LGE CMR protocols, which add functional information.31 CMRA alone can identify significant coronary artery stenoses, with recent multicentre studies demonstrating a sensitivity of 88–96% and a negative predictive value of up to 93% for detecting ≥50% stenosis. However, specificity and positive predictive value remain more modest (typically 68–79%).31,52,53 Despite these advances, CMRA remains technically challenging to perform.
Late Gadolinium Enhancement CMR
LGE CMR is highly accurate for detecting significant CAD, demonstrating a sensitivity of 89%, a specificity of 94% in patients with new left ventricle dysfunction, and diagnostic accuracy of 92%. 54 LGE is also
a strong independent predictor of adverse cardiac events 55 When combined with stress perfusion imaging, LGE provides complementary diagnostic and prognostic information, with the absence of both findings conferring a very high negative predictive value for major adverse cardiac events 56 CMR strain imaging is another promising non-invasive modality. Strain CMR refers to the quantitative assessment of myocardial deformation using computational models, such as feature tracking, strain-encoded imaging, myocardial tagging, or displacement encoding with stimulated echoes 57,58 These methods quantify myocardial fibre shortening or lengthening in longitudinal, circumferential, and radial directions, providing a sensitive marker of subclinical myocardial dysfunction that often precedes reductions in ejection fraction or echocardiographic evidence of wall motion abnormalities.58,59 CMR strain imaging is particularly useful in patients requiring detailed quantification of ischaemic, nonischaemic, or valvular heart disease. Both left ventricular long-axis measurements and circumferential or longitudinal strain values are expressed as negatives, with thresholds greater than –17% and –20% considered pathologic, respectively.58
CMR Strain Imaging
In the context of CAD, CMR strain imaging is valuable for both diagnosis and risk stratification. Strain analysis can detect regional and global myocardial dysfunction due to ischaemia or infarction, even when conventional markers, such as ECG, troponin, and ejection fraction, remain preserved. In a study of 108 patients, fast strain encoded CMR and feature tracking CMR demonstrated a sensitivity of 82%, a specificity of 87%, and a negative predictive value of 96% for flow-limiting CAD confirmed by ICA in patients presenting with acute chest pain.60 The authors concluded that CMR strain outperformed traditional markers, such as ECG and troponin dynamics, providing a high negative predictive value for ruling out flow-limiting CAD.
For prognostication, reduced global or regional strain measured by CMR is
independently associated with major adverse cardiac events in patients with known or suspected CAD.61 Recent studies show that stress CMR with strain analysis, particularly global circumferential strain, adds incremental prognostic value to conventional CMR parameters and can predict cardiac death, nonfatal myocardial infarction, and heart failure hospitalisation.61,62 Notably, CMR strain assessment has been reported to provide prognostic utility comparable to CMR stress perfusion imaging, which is especially relevant for patients with contraindications to gadolinium.62 CMR strain analysis has also been effective in measuring myocyte recovery following cardiac injury.58
CMR-PET
CMR-PET is a hybrid imaging modality that combines the high spatial and tissue characterisation capabilities of CMR with the molecular and quantitative perfusion imaging of PET.63-65 This approach enables simultaneous or sequential acquisition of anatomical, functional, and metabolic data, offering comprehensive assessment of coronary artery anatomy, myocardial tissue characteristics, blood flow quantification, and detection of inflammation or metabolic activity. A 2024 review article highlighted recent advances in CMR-PET technology.63 A small portion of their review discussed the utility of this hybrid imaging as it relates to myocardial perfusion. With respect to CAD, only limited data exist: in a small study of 15 patients, Kero et al.66 assessed 15O-water myocardial blood flow using CMR-PET and reported good correlation and moderate agreement with simultaneous dynamic contrast-enhanced MR assessments. To date, no large-scale, prospective studies or meta-analyses have directly compared CMRPET with other modalities for CAD diagnosis.
CMR Discussion
Despite its strengths, CMR is limited in certain patient populations depending on the protocol. It is contraindicated in patients with non-MRI-conditional implanted devices and requires caution in those with severe renal dysfunction, due to the risk of nephrogenic systemic
fibrosis with gadolinium, although many indications do not require contrast. Severe claustrophobia can also pose challenges, though newer open-bore and upright scanners are improving accessibility. Patient participation, such as breathholding, may also be limiting.6 Compared with CCTA, CMR has lower spatial resolution (2.0 mm versus 0.4–0.6 mm), significantly longer acquisition times (up to 1 hour), and more complex planning requirements.49 These remain barriers to widespread adoption, though advances in acquisition speed are improving tolerability. Careful patient selection and consideration of these limitations remain essential when choosing CMR for CAD evaluation.
Cost-effectiveness has also been studied. The 2021 AHA and ACC guidelines on chest pain cite UK-based studies, showing that CMR strategies are more cost-effective than single-photon emission CT, CCTA, or immediate ICA in patients with lowto-intermediate pretest probability of CAD, with comparable or lower costs.6 The inherent redundancy in CMR data acquisition allows cross-verification of findings, for example, the same myocardial segment can be assessed in short-axis and long-axis cine images, as well as through perfusion and tissue characterisation, helping mitigate incomplete coverage, motion artefacts, or segmentation errors.67 CMR is particularly valuable in evaluating conditions that mimic or coexist with
1. Weir-McCall JR et al. National trends in coronary artery disease imaging: associations with health care outcomes and costs. JACC Cardiovasc Imaging. 2023;16(5):659-71.
2. Bengel FM et al. Cardiac positron emission tomography. J Am Coll Cardiol. 2009;54(1):1-15.
3. Stuber M, Weiss RG. Coronary magnetic resonance angiography. J Magn Reson Imaging. 2007;26(2):219-34.
4. Rajiah P et al. CT fractional flow reserve: a practical guide to application, interpretation, and problem solving. Radiographics. 2022;42(2):340-58.
5. Maron DJ et al. Initial invasive or conservative strategy for stable coronary disease. N Engl J Med. 2020;382(15):1395-407.
CAD, such as myocarditis, takotsubo cardiomyopathy, or myocardial infarction with non-obstructed coronary arteries.6 In the USA, a cost analysis using data from the Stress CMR Perfusion Imaging in the United States (SPINS) registry found that a CMRfirst strategy can serve as a cost-effective gatekeeper prior to invasive angiography in patients with stable chest pain syndromes.68 However, additional USA-based costeffectiveness data comparing CMR with other non-invasive modalities remain limited.
CONCLUSION
Among the available modalities, PETCCTA currently provides the most robust integration of anatomy and physiology, offering improved specificity for identifying functionally significant lesions and guiding invasive management when appropriate. CCTA remains the first-line anatomic test, due to accessibility and its ability to exclude CAD, with AI and FFR CT promising to strengthen its physiologic relevance. CMR adds unique value through radiation-free tissue characterisation and emerging strain techniques, making it an ideal complement in select populations. Taken together, while each modality has a role, hybrid PET–CCTA best exemplifies the combined anatomic–physiologic approach today, with CMR advancing quickly as a strong contender.
6. Gulati M et al. 2021 AHA/ACC/ASE/ CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. J Cardiovasc Comput Tomogr. 2022;16(1):54-122.
7. Douglas PS et al. Survival after initial stress testing vs anatomic testing in suspected coronary artery disease: long-term follow-up of the PROMISE randomized clinical trial. JAMA Cardiol. 2025;10(10):1050-4.
8. Williams MC et al. Coronary CT angiography-guided management of patients with stable chest pain: 10year outcomes from the SCOT-HEART randomised controlled trial in Scotland. Lancet. 2025;405(10475):329-37.
9. Min JK et al. Diagnostic accuracy of fractional flow reserve from anatomic CT angiography. JAMA. 2012;308(12):1237-45.
10. Zarins CK et al. Computed fractional flow reserve (FFTCT) derived from coronary CT angiography. J Cardiovasc Transl Res. 2013;6(5):708-14.
11. Tesche C et al. Coronary CT angiography-derived fractional flow reserve. Radiology. 2017;285(1):17-33.
12. Lotfi A et al. Expert consensus statement on the use of fractional flow reserve, intravascular ultrasound, and optical coherence tomography: a consensus statement of the Society of Cardiovascular Angiography and Interventions. Catheter Cardiovasc Interv. 2014;83(4):509-18.
13. Cook CM et al. Diagnostic accuracy of computed tomography-derived fractional flow reserve: a systematic review. JAMA Cardiol. 2017;2(7):803-10.
14. Koo BK et al. Diagnosis of ischemiacausing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCOVER-FLOW (Diagnosis of ischemia-causing stenoses obtained via noninvasive fractional flow reserve) study. J Am Coll Cardiol. 2011;58(19):1989-97.
15. Baumann S et al. Comparison of coronary computed tomography angiography-derived vs invasive fractional flow reserve assessment: meta-analysis with subgroup evaluation of intermediate stenosis. Acad Radiol. 2016;23(11):1402-11.
16. Driessen RS et al. Comparison of coronary computed tomography angiography, fractional flow reserve, and perfusion imaging for ischemia diagnosis. J Am Coll Cardiol. 2019;73(2):161-173.
17. Nazir MS et al. Opportunities and challenges of implementing computed tomography fractional flow reserve into clinical practice. Heart. 2020;106(18):1387-93.
18. Boussoussou M et al. Comparative analysis of photon-counting and energy-integrating detector CT to identify obstructive coronary artery disease. Eur Radiol. 2025;DOI:10.1007/ s00330-025-12118-7.
19. Douglas PS et al. 1-Year outcomes of FFRCT-guided care in patients with suspected coronary disease: the PLATFORM study. J Am Coll Cardiol. 2016;68(5):435-45.
20. Curzen N et al. Fractional flow reserve derived from computed tomography coronary angiography in the assessment and management of stable chest pain: the FORECAST randomized trial. Eur Heart J. 2021;42(37):3844-52.
21. Hlatky MA et al. Randomized comparison of chest pain evaluation with FFRCT or standard care: factors determining US costs. J Cardiovasc Comput Tomogr. 2023;17(1):52-9.
22. Graby J et al. Real-world clinical and cost analysis of CT coronary angiography and CT coronary angiography-derived fractional flow reserve (FFRCT). Clin Radiol. 2021;76(11):862.e19-28.
23. Han D et al. Deep learning analysis in coronary computed tomographic angiography imaging for the assessment of patients with coronary artery stenosis. Comput Methods Programs Biomed. 2020;196:105651.
24. Mastrodicasa D et al. Use of AI in cardiac CT and MRI: a scientific statement from the ESCR, EuSoMII, NASCI, SCCT, SCMR, SIIM, and RSNA. Radiology. 2025;314(1):e240516.
25. Narula J et al. Prospective deep learning-based quantitative assessment of coronary plaque by computed tomography angiography compared with intravascular ultrasound: the REVEALPLAQUE study. Eur Heart J Cardiovasc Imaging. 2024;25(9):1287-95.
26. Griffin WF et al. AI evaluation of stenosis on coronary CTA, comparison with quantitative coronary angiography and fractional flow reserve: a CREDENCE trial substudy. JACC Cardiovasc Imaging. 2023;16(2):193-205.
27. Kim Y et al. Atherosclerosis Imaging Quantitative Computed Tomography (AI-QCT) to guide referral to invasive coronary angiography in the randomized controlled CONSERVE trial. Clin Cardiol. 2023;46(5):477-83.
28. Nandalur KR et al. Diagnostic performance of positron emission tomography in the detection of coronary artery disease: a meta-analysis. Acad Radiol. 2008;15(4):444-51.
29. Di Carli MF. PET perfusion and flow assessment: tomorrows' technology today. Semin Nucl Med. May 2020;50(3):227-37.
30. Schindler TH et al. Quantitative assessment of myocardial blood flow-clinical and research applications. Semin Nucl Med. 2014;44(4):274-93.
31. Litmanovich D et al. ACR Appropriateness Criteria® chronic chest pain-high probability of coronary artery disease: 2021 update. J Am Coll Radiol. 2022;19(5S):S1-18.
32. Kaufmann PA, Di Carli MF. Hybrid SPECT/CT and PET/CT imaging: the next step in noninvasive cardiac imaging. Semin Nucl Med. 2009;39(5):341-7.
33. Kajander S et al. Cardiac positron emission tomography/computed tomography imaging accurately detects anatomically and functionally significant coronary artery disease. Circulation. 2010;122(6):603-13.
35. Sarikaya I. Cardiac applications of PET. Nucl Med Commun. 2015;36(10):971-85.
36. Nakazato R et al. Myocardial perfusion imaging with PET. Imaging Med. 2013;5(1):35-46.
37. Rizvi A et al. Diagnostic performance of hybrid cardiac imaging methods for assessment of obstructive coronary artery disease compared with standalone coronary computed tomography angiography: a meta-analysis. JACC Cardiovasc Imaging. 2018;11(4):589-99.
38. Danad I et al. Comparison of coronary CT angiography, SPECT, PET, and hybrid imaging for diagnosis of ischemic heart disease determined by fractional flow reserve. JAMA Cardiol. 2017;2(10):1100-7.
39. Knaapen P et al. Cardiac PET-CT: advanced hybrid imaging for the detection of coronary artery disease. Neth Heart J. 2010;18(2):90-8.
40. Rosenkrantz AB et al. Out-ofpocket costs for advanced imaging across the US private insurance marketplace. J Am Coll Radiol. 2018;15(4):607-14.e1.
41. Motwani M et al. Role of cardiovascular magnetic resonance in the management of patients with stable coronary artery disease. Heart. 2018;104(11):888-94.
42. Saeed M et al. Cardiac MR imaging: current status and future direction. Cardiovasc Diagn Ther. 2015;5(4):290-310.
43. Lin E, Alessio A. What are the basic concepts of temporal, contrast, and spatial resolution in cardiac CT? J Cardiovasc Comput Tomogr. 2009;3(6):403-8.
44. Arai AE et al. Gadobutrol-enhanced cardiac magnetic resonance imaging for detection of coronary artery disease. J Am Coll Cardiol. 2020;76(13):1536-47.
45. Ricci F et al. Diagnostic and prognostic value of stress cardiovascular magnetic resonance imaging in patients with known or suspected coronary artery disease: a systematic review and meta-analysis. JAMA Cardiol. 2023;8(7):662-73.
46. Arai AE et al. Stress perfusion cardiac magnetic resonance vs SPECT imaging for detection of coronary artery disease. J Am Coll Cardiol. 2023;82(19):1828-38.
47. Kiaos A et al. Diagnostic performance of stress perfusion cardiac magnetic resonance for the detection of coronary artery disease: a systematic review and meta-analysis. Int J Cardiol. 2018;252:229-33.
48. Mieres JH et al. Role of noninvasive testing in the clinical evaluation of women with suspected ischemic heart disease: a consensus statement from the American Heart Association. Circulation. 2014;130(4):350-79.
49. Hajhosseiny R et al. Coronary magnetic resonance angiography: technical innovations leading us to the promised land? JACC Cardiovasc Imaging. 2020;13(12):2653-72.
50. Kato Y et al. Non-contrast coronary magnetic resonance angiography: current frontiers and future horizons. MAGMA. 2020;33(5):591-612.
51. Bluemke DA et al. Noninvasive coronary artery imaging: magnetic resonance angiography and multidetector computed tomography angiography: a scientific statement from the american heart association committee on cardiovascular imaging and intervention of the council on cardiovascular radiology and intervention, and the councils on clinical cardiology and cardiovascular disease in the young. Circulation. 2008;118(5):586-606.
52. Nazir MS et al. High-resolution noncontrast freebreathing coronary cardiovascular magnetic resonance angiography for detection of coronary artery disease: validation against invasive coronary angiography. J Cardiovasc Magn Reson. 2022;24(1):26.
53. Kato S et al. Assessment of coronary artery disease using magnetic resonance coronary angiography: a national multicenter trial. J Am Coll Cardiol. 2010;56(12):983-91.
54. Di Bella G et al. Usefulness of late gadolinium enhancement MRI combined with stress imaging in predictive significant coronary stenosis in newdiagnosed left ventricular dysfunction. Int J Cardiol. 2016;224:337-42.
55. Liu T et al. Late Gadolinium enhancement amount as an independent risk factor for the incidence of adverse cardiovascular events in patients with Stage C or D heart failure. Front Physiol. 2016;7:484.
56. Steel K et al. Complementary prognostic values of stress myocardial perfusion and late gadolinium enhancement imaging by cardiac magnetic resonance in patients with known or suspected coronary artery disease. Circulation. 2009;120(14):1390-400.
57. Aletras AH et al. DENSE: displacement encoding with stimulated echoes in cardiac functional MRI. J Magn Reson. 1999;137(1):247-52.
58. Scatteia A et al. Strain imaging using cardiac magnetic resonance. Heart Fail Rev. 2017;22(4):465-76.
59. Rajiah PS et al. Myocardial strain evaluation with cardiovascular MRI: physics, principles, and clinical applications. Radiographics. 2022;42(4):968-90.
60. Riffel JH et al. Feasibility of fast cardiovascular magnetic resonance strain imaging in patients presenting with acute chest pain. PLoS One. 2021;16(5):e0251040.
61. Korosoglou G et al. Systematic review and meta-analysis for the value of cardiac magnetic resonance strain to predict cardiac outcomes. Sci Rep. 2024;14(1):1094.
62. Guglielmo M et al. PROGnostic RolE of strain measurements in stress cardiac MRI in predicting major adverse cardiac events. Int J Cardiol. 2024;412:132337.
63. Kazimierczyk R et al. Cardiac PET/ MRI: recent developments and future aspects. Semin Nucl Med. 2024;54(5):733-46.
64. Whittington B et al. PET-MRI of coronary artery disease. J Magn Reson Imaging. 2023;57(5):1301-11.
65. Manabe O et al. Positron emission tomography/MRI for cardiac diseases assessment. Br J Radiol. 2020;93(1113):20190836.
66. Kero T et al. Evaluation of quantitative CMR perfusion imaging by comparison with simultaneous. J Nucl Cardiol. 2021;28(4):1252-66.
67. Tarroni G et al. Learning-based quality control for cardiac MR images. IEEE Trans Med Imaging. 2019;38(5):1127-38.
68. Ge Y et al. Cost-effectiveness analysis of stress cardiovascular magnetic resonance imaging for stable chest pain syndromes. JACC Cardiovasc Imaging. 2020;13(7):1505-17.
Imaging Features of Mature Retroperitoneal Teratoma in a Paediatric Patient: A Case Report
1. Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, India *Correspondence to dr.swaksh113@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank the Department of Pathology of the Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital for their contributions with the gross specimen and histopathology images, respectively.
Disclaimer: Informed consent for publication, including images of investigations and the child (patient) without including the face, was obtained from the parents of the patient, ensuring complete anonymity.
Mature cystic teratoma is a germ cell tumour with a bimodal peak of occurrence. Common sites of involvement include the pelvis, retroperitoneum, and mediastinum. It manifests with non-specific symptoms of abdominal distension with mass effect. Owing to the large size at presentation, ultrasonography is the first-line investigation; however, it does not always yield all three components. Hence, contrast-enhanced CT is diagnostic, as it enables the identification of all the components of the teratoma. It also delineates the relations with other abdominal organs, facilitating surgical excision and histopathology. The authors present a case of primary retroperitoneal mature cystic teratoma in a 3-year-old child.
In this case, the imaging findings are sufficient to arrive at a probable histopathological diagnosis and obviate the need for pre-operative imaging-guided biopsy. The take home message is the importance of localisation of lesions to the retroperitoneal cavity and to a specific compartment with further classification based on morphological characteristics, like presence of fat, cystic tissue, and calcifications.
Key Points
1. Benign mature cystic teratomas, known as dermoid cysts, are the most common germ cell tumours and have bimodal peak of occurrence. They primarily occur in the gonads, but may arise in the anterior mediastinum, retroperitoneum, or sacrococcygeal region.
2. Mature cystic teratomas contain derivatives of at least two germ cell layers and can show the characteristic presence of cystic components, fat, teeth, or cartilage not seen in unison in other tumours.
3. They can be diagnosed and prognosticated based solely on imaging findings, obviating the need for pre-surgical biopsy, which is crucial, especially in paediatric patients.
INTRODUCTION
Mature cystic teratoma is a germ cell tumour with a bimodal peak of occurrence. It is a benign lesion with very low propensity for malignant transformation and, hence, good prognosis.1 It manifests with non-specific symptoms of abdominal distension with mass effect.2 Therefore, information derived from history and clinical examination is limited. The authors present a case of primary retroperitoneal mature cystic teratoma in a 3-year-old child. In the authors’ case, the imaging findings are sufficient to arrive at a probable histopathological diagnosis. This helps avoid the need for pre-operative biopsies and subjects patients to invasive procedures just once during surgical excision. It highlights the importance of pattern recognition and the use of epidemiological information to arrive at a differential diagnosis, aiding the surgeon in decision-making for excision.
CASE PRESENTATION
A 3-year-old girl presented with vague abdominal pain and distension for 3 weeks. She was brought to the emergency department by her parents, concerned about the enlarging abdomen. She had no gastrointestinal/urinary complaints. There was no pedal oedema or other features of fluid overload. She had no antecedent medical history or past hospital admissions. She had undergone no prior investigations regarding the complaint before visiting the authors’ hospital. Abdominal examination showed a large, palpable lump in the right lumbar region, crossing the midline (Supplementary Figure 1A). The rest of the systemic examination was normal. Blood investigations were suggestive of anaemia. The child was referred for a radiograph of the abdomen, followed by a contrast-enhanced CT scan.
IMAGING FINDINGS
Abdominal radiograph showed a large, homogenous soft tissue opacity occupying the right half of the abdomen with displacement of bowel loops to the left. There was elevation of the right hemidiaphragm with blunting of the right costophrenic angle (Supplementary Figure 1B).
The next investigation performed was an abdominal-pelvic ultrasound, which showed a large, well-defined, mixed echogenicity, retroperitoneal mass containing anechoic cystic spaces and hyperechoic fat. The calcific component seen on the CT scan of the abdomen was not well-appreciated on the abdominopelvic ultrasound, perhaps due to its medial location. There was mild peripheral vascularity within the walls of the mass on Doppler studies.
Owing to the presence of cystic and fatty components, a benign cystic lesion of the retroperitoneum was suspected. Hence, Wilm’s tumour and neuroblastoma were not considered as possible differentials.
Axial contrast-enhanced CT of the abdomen in the venous phase showed a large, well-defined, right retroperitoneal lesion containing macroscopic fat, chunky calcific foci, and cystic components. It was seen displacing the right lobe of the liver anteriorly (Figure 1A). The lesion was seen crossing the midline and displacing the right kidney medially and anteriorly (Figure 1B). It contained solid enhancing component amidst the loculated cystic component. There was right pleural effusion with atelectasis of the underlying lung. The left kidney was seen separately in its native position (Figure 1C).
Figure 1: Contrast-enhanced CT of the abdomen.
A B C
A) Axial contrast-enhanced CT of the upper sections of the abdomen in the venous phase shows a large, well-defined right retroperitoneal lesion containing macroscopic fat (green arrow), chunky calcific foci (pink arrow), and cystic components. It is seen displacing the right lobe of the liver anteriorly. B) Coronal contrast-enhanced CT of the abdomen in the venous phase shows the lesion crossing the midline and displacing the right kidney medially and anteriorly (yellow arrow). C) Coronal contrast-enhanced CT of the abdomen in the venous phase shows the mass to have solid enhancing components. Additional findings of right pleural effusion with atelectasis of the underlying lung are seen. The left kidney is seen separately in its native position.
The displacement of the right lobe of the liver anteriorly, right kidney anteromedially, and bowel loops to the left of the abdomen suggested a right retroperitoneal tumour. The lesion was seen separately from the solid organs and colon, suggesting a primary retroperitoneal tumour. The presence of fat, cystic spaces, chunky calcific foci, and solid enhancing components in a child suggested mature cystic teratoma. Other less likely differentials included cystic neuroblastoma or pleomorphic liposarcoma.
Neuroblastoma was deemed less likely due to the presence of fat and predominant cystic components without encasement of vascular structures. Nephroblastoma was deemed less likely due to the extra-renal origin, presence of fat, and absence of vascular invasion.
In view of a well-delineated, benignappearing lesion of the retroperitoneum without invasion of the surrounding structures, the parents were counselled regarding a good prognosis.
The patient underwent an exploratory laparotomy with complete excision of the retroperitoneal solid-cystic mass. Owing to the non-invasive nature of
the lesion, the paediatric surgeons had easy retroperitoneal access and found maintained fat planes with the displaced kidney and liver, allowing easy surgical excision. Gross pathological examination showed variegated solid-cystic areas on cut section (Figure 2A). On microscopic examination, elements of ectoderm, endoderm, and mesoderm were seen. Areas of mature cartilage, adipose tissue, and glandular epithelium were identified (Figure 2B and 2C). Histopathology confirmed the radiological diagnosis. The child was discharged after a post-operative observation period of 7 days, which was uneventful (Table 1).
Unfortunately, the limitations of the case report were that the authors did not perform an abdominal MRI due to the need for sedation and paediatric anaesthesia owing to long scan times. The authors were also unable to maintain a long-term follow-up of the child to ensure a disease-free outcome.
DISCUSSION
The retroperitoneum is an abdominal cavity lined anteriorly by the posterior parietal peritoneum and posteriorly by the posterior body wall. It is divided into
A) Gross specimen of the resected retroperitoneal lesion. B and C) Histopathology slide showing cartilaginous component (yellow arrow), glandular tissue (green arrow), and adipose tissue (blue arrow) in the resected specimen.
0–3 weeks Symptomatic with pain and abdominal distension
4 weeks Presentation followed by radiologic and laboratory investigations
5 weeks Surgical planning and surgical procedure
6 weeks Post-operative observation
7 weeks Uneventful discharge
Table shows the timeline of the patient from symptom onset to post-treatment discharge.
three compartments by the anterior and posterior perinephric fasciae of Gerota and Zuckerkandl, respectively. These compartments include the anterior and posterior pararenal spaces and the perinephric space. An additional vascular space is seen anterior to the vertebral column in the midline containing the aorta and infrahepatic inferior vena cava. The retroperitoneum contains bowel loops, including the ascending and descending colon and the distal duodenum, solid organs like the kidneys, suprarenals, and the pancreas, and mesenchymal tissue, including fat, muscle, vessels, and nerves.3
Retroperitoneal lesions can arise from one of these organs or from the mesenchyme. Lesions that arise from the mesenchyme are known as primary retroperitoneal and can occur in any of the compartments. Lesions can be localised to the retroperitoneum by observing anterior displacement of peritoneal organs and other retroperitoneal structures. Further, a lesion can be designated as primary retroperitoneal on the basis of the claw Sign, embedded organ sign, and the phantom organ sign.4 Occasionally, very large tumours may be difficult to localise when they occupy the majority of the abdominal cavity owing to size.
Figure 2: Gross specimen and histopathology photo.
Table 1: Timeline of events from symptom onset to discharge.
Further characterisation of the retroperitoneal lesions is done based on morphology, components like cystic spaces, calcification, fat, enhancement, blood supply, and patterns of spread. Cystic primary retroperitoneal lesions can be non-neoplastic, like urinomas, pancreatic pseudocysts, and epidermoid cysts, or neoplastic, like lymphangiomas, teratomas, cystadenomas, and cystic mesotheliomas.5 Similarly, fat-containing primary retroperitoneal lesions include common diagnoses, like lipomas and liposarcomas, or rare lesions, like myelolipomas, teratomas, neurogenic tumours, fat necrosis, and extra-medullary haematopoiesis.6 Growth pattern can be used as an identifying feature in cases of neurogenic tumours, which are elongated and extend along the sympathetic chain or lumbar nerves, and lymphangiomas and lymphomas, which tend to extend and insinuate between adjacent structures.7 Solid primary retroperitoneal lesions can be classified based on tissue of origin into lymphoid, neurogenic, mesodermal, and germ cell neoplasms.8
Retroperitoneal tumours usually present as abdominal distension with vague abdominal pain and, due to non-specific symptoms, are often diagnosed late at large sizes. Occasionally, they may present with secondary symptoms caused by mass effect on adjacent structures, like vessels or ureters.
Teratomas are the most common germ cell tumour. They can be classified into monodermal, mature, or immature types. Immature teratomas are the second most common malignant germ cell tumours after dysgerminomas and consist of immature tissue arising from one or multiple germ cell layers.1 Mature teratomas, known as dermoid cysts, are the most common types of teratomas and are benign in nature. They usually arise from the gonads; however, they may primarily originate in the mediastinum (anterior compartment), retroperitoneum (suprarenal location), sacrococcygeal region, or within the cranial cavity.9 They contain well-differentiated tissues from a minimum of two germinal layers. When arising in the retroperitoneum, they may be difficult to differentiate from neuroblastomas or nephroblastomas.
Teratomas present as abdominal lumps with or without symptoms caused by secondary mass effect. They may also cause vague abdominal pain.2 In children with such symptoms, the first-line investigation is an abdominal ultrasound, which would reveal the solid-cystic nature of the lesion with or without fat/calcifications; however, exact delineation is not always possible due to the large size of the lesion. The most characteristic finding on abdominal ultrasound is the Rokitansky nodule, which appears as a hyperechoic nodule arising from the inner aspect of the cyst. It may contain fat, hair, or calcium.10
Characterisation of the organ of origin and delineation of relations is best performed on contrast-enhanced CT. The typical appearance on contrast-enhanced CT is of a large, well-defined, heterogenous lesion of solid-cystic nature, with fat or calcification in varying proportions.11 MRI is a handy tool in the identification of constituent tissue components in less obvious cases, small foci, or rests of tissue. T1 imaging, especially, can help identify fat and keratin, while T2 imaging can help identify glandular tissue and cartilaginous components.12
Mature cystic teratomas are slow-growing, benign lesions. Rarely, however, they may undergo malignant transformation, most commonly into squamous cell carcinomas. Features suggesting malignant transformation include invasion of adjacent structures and focal irregular wall thickening.13 About 50% of malignant teratomas show elevated α-fetoprotein (AFP) levels in serum. Pathognomonic features include a chemical shift artefact and a fat–fluid level due to contained sebum.13
Preoperative diagnosis based on typical imaging findings can be made. However, surgical excision of the tumour followed by histopathology is usually necessary in atypical cases. Large retroperitoneal teratomas may cause perioperative complications, like rupture of the cyst components, vascular injury, or renal dysfunction despite being benign; however, disease-free survival is seen on follow-up.11
CONCLUSION
The first step in radiological diagnosis of a retroperitoneal lesion is precise localisation of lesions to the retroperitoneal cavity and a specific compartment of the retroperitoneum. Further classification of the lesion is based on morphological characteristics seen on imaging. The concomitant presence of fat, cystic tissue, and calcifications indicates possibility of teratoma in a young child with limited differentials. Contrast-enhanced CT is the investigation of choice and helps identify individual germ cell derivatives; however, definitive diagnosis is based on histopathology post-surgical resection if resectable, or imaging-guided biopsy.
References
1. Moraru L et al. Immature teratoma: diagnosis and management - a review of the literature. Diagnostics (Basel). 2023;13(9):1516.
2. Tiu A et al. Primary retroperitoneal mature cystic teratoma (dermoid cyst) in a 51-year-old male: case report and historical literature review. SAGE Open Med Case Rep. 2017;5:2050313X17700745.
3. Tirkes T et al. Peritoneal and retroperitoneal anatomy and its relevance for cross-sectional imaging. Radiographics. 2012;32(2):437-51.
4. Gulati V et al. Solid primary retroperitoneal masses in adults: an imaging approach. Indian J Radiol Imaging. 2022;32(2):235-52.
5. Mota MMDS et al. Practical approach to primary retroperitoneal masses in adults. Radiol Bras. 2018;51(6): 391-400.
6. Shaaban AM et al. Fat-containing retroperitoneal lesions: imaging characteristics, localization, and differential diagnosis. Radiographics. 2016;36(3):710-34.
7. Nishino M et al. Primary retroperitoneal neoplasms: CT and MR imaging findings with anatomic and pathologic diagnostic clues. Radiographics. 2003;23(1):45-57.
8. Gupta A et al. Primary retroperitoneal masses: a pictorial essay. J Gastrointest Abdom Radiol. 2024;7(1):65-72.
9. Safaei N et al. Large retroperitoneal teratoma presenting with unilateral hydronephrosis in an infant: a case report and review of the literature. Case Rep Oncol. 2023;16(1):1041-7.
10. Bernot JM et al. Mature cystic teratoma: AIRP best cases in radiologic-pathologic correlation. Radiographics. 2017;37(5):1401-7.
11. Kawano T et al. Retroperitoneal teratomas in children: a single institution experience. Surg Today. 2022;52(1):144-50.
12. Nakayama T et al. Diffusion-weighted echo-planar MR imaging and ADC mapping in the differential diagnosis of ovarian cystic masses: usefulness of detecting keratinoid substances in mature cystic teratomas. J Magn Reson Imaging. 2005;22(2):271-8.
13. Rajiah P et al. Imaging of uncommon retroperitoneal masses. Radiographics. 2011;31(4):949-76.