AI and Big Data in Surgery: Emerging Evidence from the Frontline Aleksandra Zurowska
Expert Perspectives on the Use of Subcutaneous Infusion Therapies in Parkinson’s Disease
Prof Markus PeckRadosavljevic Current Chairman and Head of the Department of Gastroenterology and Hepatology, Endocrinology, Rheumatology and Nephrology at Klinikum Klagenfurt am Wörthersee, with expertise in portal hypertension, hepatocellular carcinoma, and HIV-HCV coinfection.
Multiple Micronutrient Supplementation Supports Every Stage of the Pregnancy Journey
Red Flags Raising Suspicion of Eosinophilic Granulomatosis with Polyangiitis: An EGPAware European Consensus
Transforming Ulcerative Colitis Care: AI-Powered Endoscopic Scoring from Clinical Trials to Clinical Practice Flegg and Byrne
Askanase
Kyeremeh
"Radiomics was highlighted as one of the most
Editorial Board
Editor-in-Chief
Prof Markus Peck-Radosavljevic
Klinikum Klagenfurt am Wörthersee, Austria
Current Chairman and Head of the Department of Gastroenterology and Hepatology, Endocrinology, Rheumatology and Nephrology at Klinikum Klagenfurt am Wörthersee, with expertise in portal hypertension, hepatocellular carcinoma, and HIV-HCV coinfection.
Prof Ahmad Awada
Jules Bordet Institute, Belgium
Prof Sorin T. Barbu
“Iuliu Hațieganu” University of Medicine and Pharmacy, Romania
Prof Abdullah Erdem Canda
Yildirim Beyazit University, Türkiye
Prof Ian Chikanza
Harley Street Clinic, UK
Prof Lászlo Vécsei
University of Szeged, Hungary
Dr Pierfrancesco Agostoni
St. Antonius Hospital, the Netherlands
Dr Fernando Alfonso
Hospital Universitario de La Princesa, Spain
Dr Emanuele Angelucci
IRCCS Ospedale Policlinico San Martino, Italy
Dr George Anifandis
University of Thessaly, Greece
Dr Riccardo Autorino
Virginia Commonwealth University, USA
Dr Mátyás Benyó University of Debrecen, Hungary
Prof Andrew Bush
Imperial College London, UK
Dr Hassan Galadari
United Arab Emirates University, United Arab Emirates
Dr Amir Hamzah Abdul Latiff
Pantai Hospital, Malaysia
Dr Lorenz Räber
Bern University Hospital, Switzerland
Aims and Scope
EMJ, the flagship journal of the EMJ portfolio, is an openaccess, peer-reviewed eJournal, committed to elevating the quality of healthcare globally by publishing high-quality medical content across the 18 clinical areas covered in our portfolio. The journal is published quarterly and showcases the latest developments across these clinical areas.
EMJ publishes peer-reviewed research papers, review articles, and case reports across all therapy areas of the EMJ portfolio. In addition, the journal publishes features and opinion pieces create a discussion around key topics in the field and broaden readers’ professional interests. The journal also features interviews with leading experts in various clinical disciplines.
The journal covers advances within the pharmaceutical arena by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ endeavours to increase knowledge, stimulate discussion, and contribute to the delivery of world-class updates in the clinical realm. We do not publish veterinary science papers or laboratory studies that are not linked to patient outcomes. Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
• A team of internal and independent medical writers.
Peer Review
Every review article, case report, feature, and research article published in EMJ undergoes peer review by at least two independent experts.
On submission, all manuscripts are assessed and undergo a technical check by the EMJ Editorial staff to determine their suitability for the journal and appropriateness for peer review. Editorial staff identify appropriate reviewers who are selected based on their specialist knowledge in the relevant area. All peer review is double-blind.
Following review, manuscripts are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff are responsible for ensuring that necessary amendments to the manuscript have been made, with input from our Editorial Board or the original reviewers where necessary. The Editor of EMJ has final discretion over any proposed amendments. Manuscripts authored by members of the Editorial Board are subjected to the same double-blind process. Short opinion pieces are published following internal review and publication is at the discretion of the Editor. Congress-associated content authored by the EMJ Editorial staff undergoes internal quality control checks. Congress-related content sponsored or funded by our industry partners undergoes quality control checks independently. Industry-supported content that falls into any of
the categories that are eligible for peer review, undergoes the same peer review process.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®.
EMJ is available through the websites of our leading partners and collaborating societies.
EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication Launch Date: 2016 Frequency: Quarterly Online ISSN: 2397-6764
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of any event reviews in this issue and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Sheffield, the location of work for the primary author of Editor's Pick.
High-level perspectives. Global experts. Essential updates.
Join us for conversations with the minds shaping healthcare's future. Gain the distilled insights you need to lead in your field and make maximum impact.
Jonathan Sackier: Non Executive Director & CMO, AiM Medical Robotics, Florida, USA
Saranya Ravindran: Paediatric Emergency Medicine Registrar, Imperial College Healthcare NHS Trust
Catherine Glass: Associate NHS GP and Senior Appraiser, NHS England
Editorial Director
Andrea Charles
Editor
Sean Boyle
Managing Editor
Darcy Richards
Senior Copy Editor
Noémie Fouarge
Copy Editors
Meghan Garcka, Sarah Jahncke
Editorial Leads
Helena Bradbury, Ada Enesco
Editorial Co-ordinators
Bertie Pearcey, Alena Sofieva
Editorial Assistants
Niamh Holmes, Roli Omamuli, Alexander Perkins, Katrina Thornber, Aleksandra Zurowska
Reporter
Anna Caldwell
Creative Director
Tim Uden
Design Manager
Stacey White
Senior Designers
Tamara Kondolomo, Owen Silcox
Designers
Shanjok Gurung, Fabio van Paris
Junior Designers
Fraser Hoey, Helena Spicer, Caleb Wylie
Head of Marketing
Stephanie Corbett
Business Unit Lead
Kelly Byrne
Chief Executive Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chairman
Spencer Gore
Welcome
Dear Readers,
It is a great pleasure to welcome you to the first issue of the EMJ Flagship Journal for 2026. In this issue, we spotlight AI in therapeutics and diagnostics, with exclusive interviews with two leading experts.
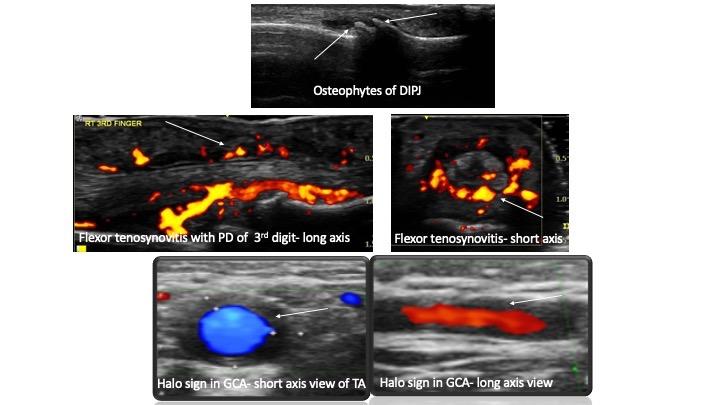
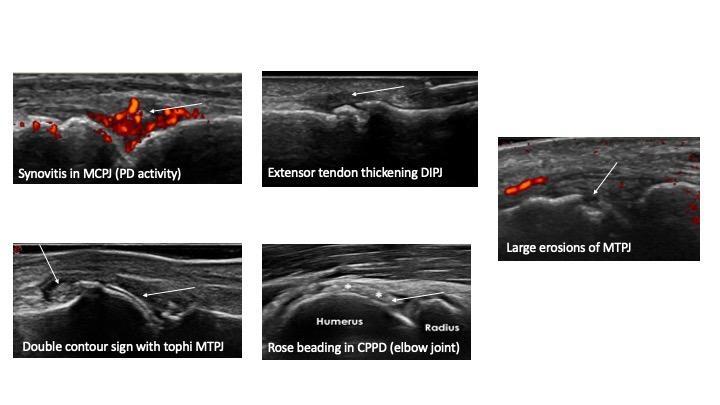
We open with a compelling review on the role of point-of-care ultrasound in rheumatology, reinforcing its value in early diagnosis and precision-guided treatment. We also feature original research exploring patient perspectives on AI in chest X-ray assessment, reminding us that successful technological integration depends as much on communication and trust as on performance.
This issue also addresses the broader determinants of health. Research investigating medication adherence and quality of life among patients with epilepsy in Nigeria proves the ongoing need for psychoeducation and equitable care, while an ecological analysis of air pollution and interstitial lung disease prompts reflection on the environmental influences on respiratory health.
In addition, two case reports demonstrate the value of personalised and multidisciplinary approaches in managing complex clinical cases, from hypermobile Ehlers-Danlos syndrome with gastrointestinal complications to hypersensitivity reactions in ovarian cancer.
I would like to extend my sincere thanks to our Editorial Board, authors, and peer reviewers for their continued dedication and expertise. I hope you find this issue both insightful and relevant to your clinical practice.
Aleksandra Zurowska Editorial Assistant
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
Foreword
Welcome to our first EMJ Flagship issue of 2026. This edition highlights the central theme of AI in therapeutics and diagnostics.
As medicine is entering a period defined not only by discovery, but by integration, the question is no longer whether new technologies, such as AI, will influence healthcare, but how we will ensure they do so responsibly, effectively, and in a way that strengthens clinical judgement rather than replaces it.
In this issue, we place a particular emphasis on AI and its evolving role in therapeutics and diagnostics. Our feature article examines the real-world application of AI across clinical settings and, complementing this, our interview with James Zou offers valuable insight into the scientific and ethical considerations shaping the next generation of machine
learning in medicine. Together, these contributions reflect the ambition and caution required at this pivotal time.
Alongside innovation, this issue also focuses on the complexity of everyday clinical practice. From the expanding use of point-of-care ultrasound in rheumatology to research examining patient acceptance of AI in radiology, medication adherence in epilepsy, and environmental influences on interstitial lung diseases, these articles collectively remind us that progress must remain patient-centred and evidence-led.
I am grateful to our authors, reviewers, and Editorial Board for their expertise and continuous commitment. I hope this issue encourages thoughtful engagement with both the promise and responsibility that accompany medical advancement.
These articles collectively remind us that progress must remain patient-centred and evidence-led
Prof
Markus Peck-Radosavljevic
Professor of Medicine and Chairman, Department of Gastroenterology and Hepatology, Endocrinology, Rheumatology and Nephrology, Klinikum Klagenfurt am Wörthersee, Austria
AI and Big Data in Surgery: Emerging Evidence from the Frontline
AS DATASETS expand and computational tools mature, hepatopancreatobiliary medicine is entering a new phase in which AI is no longer experimental, but increasingly embedded in research and clinical strategy. During the session ‘What’s new in AI and big data in HPB in 2025?’ at the United European Gastroenterology (UEG) Week 2025 in Berlin, Germany, speakers explored how predictive modelling, electronic health record integration, and multi-omics data are redefining risk prediction, surgical planning, and long-term disease surveillance.
AI IN PANCREATIC SURGERY
AI is rapidly reshaping the landscape of surgical oncology. However, its true potential lies not in isolated tools, but rather in the integration of multiple data layers. The talk delivered by Andrew Gumbs, Hôpital Antoine-Béclère, Clamart, France, outlined how AI-driven multi-omics approaches, including radiomics, pathomics, genomics, and surgical video analysis, could redefine personalised cancer care, particularly in pancreatic adenocarcinoma.
Building his argument around the Artificial intelligence, Radiomics, Genomics, Oncopathomics and Surgomics (AiRGOS) project, a pan-European initiative aimed at combining imaging, pathology, genomic, and intraoperative visual data in surgery across multiple centres, he explained how the ambition is to move beyond static tumour boards towards AI-supported decisionmaking, including real-time guidance in the operating room. However, while the computational tools already exist, Gumbs emphasised that legal and regulatory barriers within the EU remain the greatest obstacle to progress, often preventing effective data sharing between institutions.
Radiomics was highlighted as one of the most mature AI applications in oncology. By analysing tumours voxel-by-voxel in
3D, radiomics enables extraction of shape, intensity, and texture features far beyond the human visual capacity. When paired with deep learning, these techniques have demonstrated the ability to stratify tumours by biological behaviour, including early versus late recurrence, even from a single imaging phase. While such models often function as “black boxes,” Gumbs argued that this should not preclude their clinical use, provided AI remains an advisor rather than an autonomous decision-maker.
Radiomics was highlighted as one of the most mature AI applications in oncology
Pathomics, an emerging approach that applies AI and computer vision to digitised histology slides to extract quantitative data on tumour morphology, has increasingly gained attention and may currently represent the most powerful predictive omics in pancreatic cancer. Emerging multicentre data suggest that deep learning applied to pathology images can capture tumour biology with remarkable precision, potentially rivalling or even surpassing genomic approaches in certain contexts.1
Although whole-genome sequencing has become significantly more affordable, its widespread adoption is still constrained by access and funding rather than cost alone.1
Gumbs also addressed ethical considerations around data ownership and consent. Blockchain-based solutions were proposed as a way to give patients transparency and agency over how their data are used, offering a potential framework for fair and traceable data sharing in the future.
In closing, Gumbs stressed that the future of oncology lies in multi-omics integration, not single modality analysis. While Europe risks falling behind due to its regulations, scientific societies and international collaborations are well placed to drive progress. Ultimately, AI-enabled tumour boards could help clinicians move away from trial-and-error treatment strategies towards truly biologically informed, personalised cancer care.
BIG DATA AND AI IN PERSONALISED THERAPY IN METABOLIC LIVER DISEASES
Rising Star awardee Carolin Schneider, RWTH Aachen University Hospital, Germany, continued the session with a talk on harnessing big data and AI to enable personalised therapy in metabolic liver diseases.
Schneider began by framing the scale of the problem: obesity and metabolic liver disease now affect approximately
30% of the global population.2,3 The stepwise progression from steatosis to steatohepatitis, cirrhosis, and ultimately hepatocellular carcinoma presents clear windows for early intervention. However, she emphasised that the pathogenesis of liver disease is multidimensional, shaped by lifestyle, genetics, sex, medication exposure, and broader societal factors.
To address this complexity, Schneider described an ambitious, data-driven research programme built around harmonised international cohorts (Schneider, unpublished data). Collectively, these datasets include more than three million individuals with a mean follow-up of approximately 14 years. Beyond standard clinical information, the cohorts contain detailed demographic and lifestyle data, electronic health records, routine serum biomarkers, whole-genome data, and, in some cases, more than 250 metabolomic parameters. Liver disease serves as the starting point, but the infrastructure is designed to expand into wider gastrointestinal and metabolic conditions.
One key line of investigation focused on lifestyle behaviour. In a cohort of over 100,000 individuals who wore fitness trackers for 1 year, daily step counts were analysed in relation to future metabolic liver disease risk.4 Schneider reported that approximately 7,500 steps per day were associated with a meaningful reduction in risk, while 12,000 steps were linked to roughly halving the risk over 3.5 years. The findings suggest that protective behavioural targets may be more attainable than often assumed.4
Nutrition was examined in more than 210,000 individuals who completed repeated 24-hour dietary questionnaires.5 Higher vitamin E intake was associated with lower liver disease risk, supporting previous clinical observations. When machine learning techniques were applied, using a random forest model trained on 64 nutrients, manganese emerged as a leading associated factor. Higher manganese intake correlated with lower liver disease incidence, even after adjustment for confounders. However, Schneider cautioned that manganese-rich foods, such as nuts and whole grains, may simply reflect an overall healthier dietary pattern, highlighting the hypothesis-generating nature of such analyses.5
Turning to hepatocellular carcinoma, Schneider presented work leveraging UK Biobank data to develop predictive models of increasing complexity. The team described a series of decision tree-based approaches, beginning with anthropometric and lifestyle variables and progressively incorporating electronic health records, laboratory markers, genetic variants, and metabolomic profiles. While the most comprehensive model delivered the highest predictive performance, Schneider highlighted that routine serum biomarkers alone demonstrated substantial predictive value, underscoring the clinical promise of readily available data.
A key focus of the presentation was model bias. Analysis revealed marked sex-based disparities: the algorithm identified 73% of male hepatocellular carcinoma cases, but only 31% of female cases. Schneider
attributed this imbalance to skewed training data and stressed the necessity of subgroup validation and bias-aware model development to avoid perpetuating existing inequities in cancer detection.
Schneider concluded that, while AI offers powerful tools for hepatology, validation, transparency, and bias awareness remain essential. Precision prevention, she suggested, will depend not only on technological innovation, but on careful and equitable implementation. Robust associations validated across multiple cohorts may justify targeted prospective trials with higher probabilities of success. Synthetic trial methodologies and crosscohort transfer learning are emerging strategies, but conventional randomised evidence remains essential.
Future directions include integrating tabular data with imaging modalities, such as ultrasound, to enhance hepatocellular carcinoma risk stratification. Schneider also highlighted ongoing efforts in cross-cohort transfer learning, enabling knowledge derived from large datasets to inform smaller, deeply characterised cohorts, and vice versa.
Ultimately, her message was both ambitious and grounded: precision hepatology will require scale, collaboration, and vigilance. In Berlin, big data was not presented as a futuristic abstraction, but as an evolving infrastructure already reshaping how metabolic liver disease is understood and, potentially, prevented.
AI IMAGING FOR PANCREATIC DISEASES
Closing off the session at UEG Week 2025, Adrian Saftoiu, University of Medicine and Pharmacy of Craiova, Romania, delivered the final talk on the role of AI as an imaging tool in pancreatic diseases, moving from risk prediction models to real-time endoscopic ultrasound (EUS) guidance and emerging applications in pathology and robotics.
Saftoiu began by explaining the central role of EUS in pancreatic cancer diagnosis. Beyond imaging, EUS enables fine-
needle aspiration biopsy for tissue confirmation and supports screening and prognostic assessment. However, with newer techniques such as Doppler flow imaging, contrast harmonic imaging, and elastography, the learning curve has grown increasingly steep. AI, he suggested, offers a way to shorten that curve.
He highlighted large-scale screening efforts such as the Pancreatic Duct Adenocarcinoma Risk Model (PRISM), built using over 1.5 million controls and 35,000 pancreatic ductal adenocarcinoma cases. By integrating clinical data, biomarkers, and imaging features, the model identified high-risk individuals beyond those captured by current guidelines, potentially expanding early detection strategies.6
In CT imaging, Saftoiu referenced work demonstrating that non-contrastenhanced scans can detect pancreatic malignancies with performance comparable to radiologists using contrast-enhanced studies.7 Such findings suggest that AI may extract diagnostic value even from routinely acquired imaging.
Within EUS, earlier artificial neural network models modestly improved differentiation between chronic pancreatitis and pancreatic cancer. However, the field accelerated with convolutional neural networks. Saftoiu described a real-time EUS segmentation system trained on approximately 200 patients and validated on 300 more, capable of identifying pancreatic tissue, cysts, solid tumours, ducts, and even small stones without perceptible lag.8 Its accuracy matched expert operators, offering particular value for less experienced
References
1. Alagarswamy K et al. Should AIpowered whole-genome sequencing be used routinely for personalized decision support in surgical oncology—a scoping review. BioMedInformatics. 2024;4(3):1757-72.
2. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002;346(16):1221-31.
clinicians by guiding biopsy placement and ensuring complete examination.8
Digital pathology represents another advancing frontier. AI models applied to fine-needle aspiration biopsy slides showed near-perfect overlap with expert pathologist annotations in identifying adenocarcinoma regions. Integration with real-time imaging technologies could further streamline diagnosis.
Saftoiu also addressed large language models in clinical interpretation. While tools, such as ChatGPT (OpenAI, San Francisco, California, USA), can describe imaging features and suggest diagnoses, he cautioned that these probabilistic systems remain prone to error and require careful validation. In one clinical example, AI-supported interpretation was helpful but not definitive, reinforcing the need for clinical judgement.
Looking ahead, radiomics may allow AI to extract greyscale information beyond human visual perception, potentially enhancing differential diagnosis. However, questions of standardisation and generalisability remain. Saftoiu advocated for federated learning approaches and cloud-based platforms to enable multicentre collaboration and broader access.
He concluded that AI in pancreatic imaging is already embedded within current systems and will continue expanding into diagnostic support, therapy monitoring, and potentially robotic integration. The challenge now lies not in technological capability, but in rigorous validation and responsible implementation.
3. Lee Y et al. Complete resolution of nonalcoholic fatty liver disease after bariatric surgery: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2019;17(6):1040-60.e11.
4. Schneider CV et al. Physical activity is associated with reduced risk of liver disease in the prospective UK biobank cohort. JHEP Rep. 2021;3(3):100263.
5. Scorletti E et al. Dietary vitamin E intake is associated with a reduced risk of developing digestive diseases and nonalcoholic fatty liver disease. Am J Gastroenterol. 2022;117(6):927-30.
7. Cao K et al. Large-scale pancreatic cancer detection via non-contrast CT and deep learning. Nat Med. 2023;29(12):3033-43.
8. Zhang J et al. Deep learningbased pancreas segmentation and station recognition system in EUS: development and validation of a useful training tool (with video). Gastrointest Endosc. 2020;92(4):874-85.e3.
6. Jia K et al. A pancreatic cancer risk prediction model (Prism) developed and validated on large-scale us clinical data. Ebiomedicine. 2023;98:104888.
Expert Perspectives on the Use of Subcutaneous Infusion Therapies in Parkinson’s Disease
Interviewees:
Rajesh Pahwa,1 Angelo Antonini,2 Robert Hauser,3 Tove Henriksen,4 Stuart Isaacson,5 Regina Katzenschlager,6 Andrew Lees,7 Cathy Magee,7 Michael Soileau8
1. University of Kansas Medical Center, Kansas City, USA
2. University of Padua, Italy
3. University of South Florida, Tampa, USA
4. University Hospital of Bispebjerg, Copenhagen, Denmark
5. Parkinson’s Disease and Movement Disorders Center of Boca Raton, Florida, USA
6. Department of Neurology and Karl Landsteiner Institute for Neuroimmunological and Neurodegenerative Disorders, Klinik Donaustadt, Vienna, Austria
7. National Hospital for Neurology and Neurosurgery, London, UK
8. Texas Movement Disorder Specialists, PLLC, Georgetown, USA
Support: The publication of this article was supported by Convatec.
Disclosure:
Pahwa serves as a consultant for Abbott, AbbVie, ACADIA, Amneal, AskBio, Convatec, Fasikl, Genetech, Insightec, Lundbeck, Merz, Mitsubishi Tanabe, Ono, PhotoPharmics, Supernus, and Theravance; and receives research support from Abbott, AbbVie, Annovis, AskBio, Biogen, Bluerock (Bayer), Cerevance, Cerevel, CND, Michael J Fox Foundation, Neuron23, Ono, Parkinson’s Foundation, Roche, Saluda, Supernus, Teva, Theravance, and TrueBinding.
Antonini has received compensation for consultancy and speaker-related activities from AbbVie, UCB, Stada, Zambon, Bial, Theravance Biopharma, Convatec, Bayer, Ferrer, AskBio, and Novo Nordisk; and receives research support from Horizon2020, the Italian Ministry of University and Research (MUR), the Italian Ministry of Health (MoH), and the European Union (NextGenerationEU – NRRP M6C2 - Investment: 2.1 "Enhancement and strengthening of biomedical research within the NHS”).
Hauser has received speaking fees from Abbvie, Amneal Pharmaceuticals, Kyowa Kirin, Neurocrine Biosciences, and Supernus; consulting fees from Abbvie, ABLi Therapeutics, Alterity Therapeutics, Amneal, Biogen, Cerevance, Cerevel, Clario, Contera Pharmaceuticals, Convatec Inc, Foresee Pharmaceuticals, HanAll Biopharma, Inhibikase, Intrance (PSG), KiefeRx, Knight Therapeutics, Kyowa Kirin, Mitsubishi Tanabe, Nano PharmaSolutions, Neurocrine, Neuroderm, NDP Pharmaceuticals, PhotoPharmics, Regenxbio, Revance, Serina Therapeutics, Stoparkinson, Sumitomo, Supernus, Tarus Therapeutics, Theravance, TrueBinding, UCB, and Zambon; has stock options in Enterin, Inhibikase, and Axial Therapeutics; serves on a scientific advisory board for Stoparkinson, Inhibikase, and PhotoPharmics; has received intellectual property interests from a PD Diary through his University; acknowledges a Center of Excellence grant from the Parkinson Foundation; has received research support from AbbVie, Amneal Pharmaceuticals, Biogen MA, BlueRock Therapeutics, Inc., Cerevance Beta, Inc., Cerevel Therapeutics, F. Hoffman La Roche Ltd, Genentech, Inc., Global Kinetics Corporation, Ipsen, Michael J Fox Foundation, Motric Bio, Inc., Neuron23, Sun Pharma Advanced Research Company, Ltd., Teva Branded Pharmaceuticals, TrueBinding, Inc., and UCB Biopharma SRL, with payment to the university.
Henriksen has received honoraria for talks from AbbVie, Britannia, Nordic Infucare; has served as a principal investigator on a study sponsored by AbbVie and Britannia; and has served as a data monitoring committee board member on a study sponsored by Lundbeck.
Katzenschlager has received research support or fees for consulting or speaking from AbbVie, AOP, Bial, Britannia, EVER Pharma, Merz, Mistubishi Tanabe/Neuroderm, Novartis, Ono, Spirig, Stada, Supernus, UCB, and Zambon.
Solieau has received advisory and/or consulting fees from Abbott, AbbVie, Medtronic, Neurocrine Pharmaceuticals, PhotoPharmics, Praxis Precision Medicines, and Supernus; research support from AbbVie, Amneal Pharmaceuticals, AskBio Inc., Cerevance, Intra-Cellular Therapies, Jazz Pharmaceuticals, PhotoPharmics, Praxis Precision Medicines, Scion Neurostim, Teva, and Vima Therapeutics; grant support from the HDSA; and has served on the speaking bureau for AbbVie, Amneal Pharmaceuticals, Biogen, Kyowa Kirin, Merz, Neurocrine Pharmaceuticals, Supernus, and Teva.
Isaacson, Less, and Magee have not declared any conflicts of interest.
Acknowledgements: Medical writing assistance was provided by Samantha Stanbury, PhD, Stockport, UK. We thank John Davis and Ased Ali, Convatec, for their contribution to the development of the article as reviewers.
Disclaimer: The opinions expressed in this article belong solely to the named interviewees. Interviews covering topics agreed in advance by the contributors were conducted on an individual basis and do not reflect a consensus process, but represent a range of perspectives from experts practising in different regions.
Subcutaneous (SC) infusion therapy with apomorphine first became available for the treatment of Parkinson’s disease (PD) in Europe in the early 1990s. SC infusion options have expanded in recent years to include levodopa-based formulations, and were introduced in the USA in 2024. This article collates expert insights from PD specialists in Europe and the USA, with extensive cumulative experience of using SC infusion therapies to treat their patients, to address knowledge gaps and share best practice with the wider neurology community. To this end, EMJ conducted interviews between December 2025–January 2026 with nine key opinion leaders: Rajesh Pahwa, University of Kansas Medical Center, Kansas City, USA; Michael Soileau, Texas Movement Disorder Specialists, PLLC, Georgetown, USA; Stuart Isaacson, Parkinson’s Disease and Movement Disorders Center of Boca Raton, Florida, USA; Robert Hauser, University of South Florida, Tampa, USA; Angelo Antonini, University of Padua, Italy; Tove Henriksen, University Hospital of Bispebjerg, Copenhagen, Denmark; Regina Katzenschlager, Department of Neurology and Karl Landsteiner Institute for Neuroimmunological and Neurodegenerative Disorders, Klinik Donaustadt, Vienna,
Austria; and Andrew Lees and Cathy Magee from the National Hospital for Neurology and Neurosurgery, London, UK. Based on their insights, this article discusses the SC infusions available for PD and clinical evidence for their efficacy and safety; when and for which patients they should be considered; and how to optimise their use in real-world practice, including proactive skin care and reliable, user-friendly delivery systems.
INTRODUCTION
PD is the second most common neurodegenerative disease,1 characterised by bradykinesia plus rest tremor or rigidity.2 The discovery of levodopa for the treatment of PD revolutionised its management. However, while oral levodopa-based treatment regimens provide symptom control in the short-to-medium term for most patients, long-term levodopa treatment is frequently associated with the eventual development of motor fluctuations and dyskinesia.3 Motor fluctuations can occur as early as the first 1–2 years of treatment with levodopa in some patients, by 5 years in approximately 50% of patients, and by 10 years of treatment, most patients experience OFF episodes.4
The management of motor fluctuations typically involves adjusting the patient’s levodopa regimen by altering the dose and/or dosing frequency or switching to an extended-release formulation; adding an oral or transdermal dopamine agonist (if not already used); adding adjunctive medication such as a catechol-Omethyltransferase or monoamine oxidase-B inhibitor to slow the breakdown of levodopa or dopamine, respectively; or using non-dopaminergic levodopa extenders such as adenosine A2A antagonists or amantadine. However, treatment response can remain unpredictable, especially with advancing disease, and on-demand rescue medication is often required. One factor that contributes to loss of efficacy of oral levodopa is poor absorption due to gastrointestinal (GI) dysfunction, which is a common feature of PD.5,6 It is therefore rational to consider non-oral routes of administration. SC infusion not only bypasses the GI tract, but also provides continuous drug delivery, and, therefore,
continuous dopaminergic stimulation, avoiding the peaks and troughs associated with oral medication.
Until recently, in the USA, progressing beyond oral/transdermal medications as the core treatment regimen has largely required surgical procedures to place a deep brain stimulation (DBS) device or jejunostomy tube for intrajejunal delivery of carbidopa/levodopa enteral suspension (CLES), usually referred to as levodopa/ carbidopa intestinal gel in Europe. The recent introduction of treatments administered via SC infusion, apomorphine and foscarbidopa/foslevodopa (fosCD/ fosLD), provides an alternative therapeutic strategy or a potential intermediate step in the treatment pathway before advancing to surgical options. However, many healthcare professionals in the USA are not yet familiar with the available SC options. There is greater familiarity in Europe, where SC apomorphine has been available for >30 years (with formulations available for delivery by injection or as a continuous SC apomorphine infusion [CSAI]), and SC fosCD/fosLD (infusion solution) was launched in 2024.7
Although CSAI has been available in Europe for several decades, Lees commented that it has tended to be underused.8 The expansion of SC treatment options to include fosCD/fosLD, coupled with their wider availability across regions, makes this an opportune time to examine when and how SC infusion therapies can be used to improve the management of PD. This article brings together the expertise and experience of PD specialists in both Europe and the USA to share their collective knowledge regarding SC infusion as a treatment modality for PD with the wider neurology community.
OVERVIEW OF SC INFUSION THERAPIES FOR PD: CLINICAL EVIDENCE
There are currently two approved products (CSAI and fosCD/fosLD) for the treatment of PD via SC infusion. Clinical evidence for these treatments has been reviewed elsewhere;9 key efficacy and safety data from clinical trials are summarised briefly below.
Apomorphine (Continuous SC Apomorphine Infusion )
The most robust evidence for the efficacy and safety of CSAI comes from the TOLEDO study, a double-blind, randomised, placebocontrolled trial in 106 patients with PD and persistent motor fluctuations, despite optimised oral or transdermal medication.10 After 12 weeks’ double-blind treatment, CSAI reduced mean OFF time by almost 2 hours per day more than placebo (treatment difference: −1.89 hours per day; p=0.0025).10 Reductions in OFF time were sustained throughout a 52-week open-label phase, coupled with increased ON time without troublesome dyskinesia and reductions in mean oral levodopa-equivalent dosage.11 The most common treatment-emergent adverse events (AE) included infusion site reactions (e.g., nodules/erythema), nausea, somnolence, and dyskinesia.10 Six patients (11%) discontinued treatment during the 12-week double blind treatment period for various reasons, including one discontinuation due to infusion site reaction. By the end of the open-label phase, 17% of patients had discontinued CSAI, including four patients (5%) discontinuing due to infusion site reactions.
The InfusON study (NCT02339064) was a 52-week open-label study of CSAI in 99 patients enrolled at 19 centres in the USA, which supported its approval in the USA.12 Results were consistent with those of the TOLEDO study, with mean OFF time reduced by about 3 hours by Week 12, and a corresponding increase in ON time without troublesome dyskinesia and reduction of oral levodopa-equivalent dosage and adjunctive medication use. Improvements were sustained through Week 52, and the majority of patients
reported their symptoms were much or very much improved at Weeks 12 and 52. The tolerability profile was consistent with expected AEs based on TOLEDO and clinical experience in Europe.12
Foscarbidopa/Foslevodopa
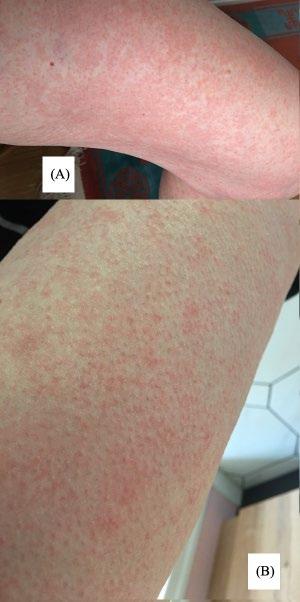
Foscarbidopa and foslevodopa are carbidopa and levodopa prodrugs. The efficacy and safety of fosCD/fosLD for SC infusion were investigated in a 12-week double-blind RCT (NCT04380142)13 and a 52-week open-label study (NCT03781167).14 In the 12-week RCT (N=141), ON time without troublesome dyskinesia increased by a mean of 2.72 hours with fosCD/fosLD versus 0.97 hours with oral carbidopa/levodopa (difference: 1.75 hours; p=0.0083), with a similar reduction in OFF time.13 Infusion site events were common (72% with fosCD/fosLD versus 12% with SC placebo), including erythema, pain, oedema, nodules, and cellulitis; these largely accounted for a higher discontinuation rate (22% versus 1%). Other AEs included dyskinesia, falls, and hallucinations.13
In the 1-year open-label study, all patients (N=244) received fosCD/fosLD, with dosage optimised during the first 4 weeks of treatment.14 Mean ON time without troublesome dyskinesia increased by 3.8 hours from baseline to Week 52, and mean OFF time decreased by 3.5 hours.14 Interim analysis of a long-term extension study indicates that efficacy was sustained in patients who opted to continue treatment for up to 96 weeks.15 Similar to the shorter-term study, the most common AEs in the 52-week open-label study were infusion site reactions, including erythema, nodules, cellulitis, and oedema.14 A total of 107 patients (44%) discontinued treatment within the 1-year study period, including 56 (23%) whose primary reason for discontinuation was AEs. The most common AEs leading to discontinuation were hallucinations, dyskinesia, and infusion site reactions, including erythema, cellulitis and nodules.14 The authors suggested that “the prevention and management of infusion site AEs should be among the top priorities to consider when initiating fosCD/fosLD to promote adherence to therapy.”14 Expert
contributors discuss skin management later in this article.
The ongoing ROSSINI study (NCT06107426) is a real-world observational study investigating the long-term safety and tolerability of fosCD/fosLD.16 An interim analysis found that patients treated with fosCD/fosLD for 6 months (N=105) had statistically significant reductions in mean OFF time (−2.7 hours) and dyskinesia time (−1.7 hours). Improvements were also observed in Movement Disorders Society Unified PD Rating Scale (MDS-UPDRS)
Part III scores and measures of sleep, pain, quality of life, freezing of gait, and GI dysfunction.17
THE PLACE OF SC INFUSION THERAPY IN THE PD TREATMENT PATHWAY
When Should Physicians Consider Introducing SC Infusion Therapies?
Antonini outlined the ‘5-2-1’ criteria as a useful rule-of-thumb used in Europe for recognising patients with advanced PD who might benefit from stepping up treatment. The 5-2-1 rule refers to patients who require oral levodopa dosing ≥5 times daily, or have ≥2 hours per day with OFF symptoms, or have ≥1 hour per day of troublesome dyskinesia.18,19 Antonini explained that these simplified criteria, which are easier to remember than a complex algorithm, are a useful guide for general neurologists to identify patients with advanced PD who may need to be referred to a specialist centre for the next phase of treatment.
Meeting any one of the 5-2-1 criteria is considered sufficient to prompt consideration of device-aided therapies, including SC infusion.18,19 This does not set an excessively high threshold for considering advanced therapy, and Antonini supported early introduction of SC infusion therapy. He cited a post-hoc analysis of the fosCD/ fosLD RCT, focusing on a subgroup of younger patients (≤65 years) at an earlier stage of advanced PD than the overall study population (≤5 years since onset of motor fluctuations; disease duration <10 years in
>90% of patients [n=26]). For most efficacy endpoints, treatment benefit of fosCD/ fosLD in this subgroup was consistent with, and numerically greater than, the overall study population.20 This finding is important, Antonini said, because “it shows that the earlier you use this treatment the better your [outcomes] are.” Lees has longstanding experience with CSAI and welcomed a trend towards its earlier use. In the past, it was unusual to introduce CSAI until approximately 9–10 years after diagnosis, whereas 6–7 years post diagnosis is now more typical.
In practice, it is not just the numerical criteria, but their functional impact that indicates a need to progress beyond oral therapy. Prompts to consider advanced treatment may include loss of independence due to unmanageable fluctuations and difficulty maintaining compliance with oral medication regimes. Patients may be taking levodopa 4–5 times per day and are often advised to avoid taking it close to mealtimes to limit protein interactions, which can affect absorption, making it difficult to integrate medication schedules into daily life. Soileau explained that patients reach a point where the therapeutic window for oral levodopa is very narrow, with a limited dose range that provides adequate relief of motor symptoms without inducing dyskinesia. At this point it becomes difficult to manage symptoms using oral medication, presenting “a good opportunity to try SC therapy.”
Which Patients Are Suitable Candidates for SC Infusion Therapy Versus DBS?
Core eligibility criteria are similar for SC infusion therapy and DBS: a patient experiencing 2–3 hours’ OFF time per day, with OFF episodes causing some functional difficulty, who has tried at least one adjunctive therapy in addition to levodopa could be a candidate for either SC infusion or DBS. Cognitive status might determine treatment selection, as DBS is not suitable for patients with significant cognitive impairment. For SC infusion therapy, patients need to have capacity to operate the pump and infusion set or have support from a caregiver if they cannot manage this themselves, which is not precluded by mild/
moderate cognitive impairment. Patients with severe dementia are not considered suitable candidates for infusion therapy (SC or intrajejunal) due to the risk that, if a patient becomes confused by the presence of the infusion equipment, they might pull out the cannula or disconnect the pump.
For patients who are eligible for either option, the choice is usually determined by patient preference, with physician guidance. Henriksen emphasised the importance of involving patients in treatment decisions, as having the patient ‘on board’ with the treatment selected has been shown to improve compliance. Different treatment options should be presented neutrally, explaining pros and cons of each option without bias, to allow patients to make informed treatment decisions.
The experts interviewed for this article listed several advantages of SC infusion therapy: it is less invasive than surgical options and it is also reversible. If a patient has difficulty managing the pump or does not tolerate SC treatment well, they can simply stop treatment and would still be candidates for DBS. Another advantage is that SC infusions can be started quickly in the clinic, whereas DBS requires extensive assessments and neurosurgical consultation to confirm suitability before the surgery itself can be scheduled. Several experts talked about using SC infusion as a ‘bridging therapy’ for patients awaiting DBS.21 Given the non-invasive and reversible nature of SC infusion therapies, there was broad agreement among the experts that it is usually preferable to try SC infusion before DBS. Antonini described SC infusion as a “good entry point” to device-aided therapy.
The main reason given for some patients expressing a preference for DBS over SC infusion was not wanting to carry an infusion pump around. Additionally, once the DBS device is implanted, patients do not have to think about it, whereas SC infusion requires daily management and skin care.
Table 1 summarises some of the key considerations that might influence selection between SC infusion versus DBS for patients with advanced PD.
Anecdotally, experts suggested that use of CLES, another advanced option that requires both surgery and a pump for drug delivery, appears to have decreased slightly with the availability of fosCD/fosLD as an SC option for continuous infusion of levodopa-based treatment. Selection between DBS, CLES, and CSAI is reviewed elsewhere.22 Results from a network meta-analysis suggested potentially greater OFF time reduction with DBS and CLES than with CSAI.23 However, no direct head-to-head comparative studies have been performed. The network metaanalysis23 pre-dated approval of fosCD/ fosLD, so evaluation of SC infusion therapy was limited to CSAI.
It is not necessarily an either/or choice between different device-aided therapies, but a question of which option to try first. Patients who have undergone SC infusion therapy often subsequently move on to DBS.24 Conversely, patients can have SC infusion therapy added to DBS if they continue to experience OFF episodes or motor fluctuations. As Soileau put it: “Patients can try SC therapy at any point in their journey; having more options sends a very encouraging message to the patient and care-partner.”
Overall, the option of SC infusion therapy may broaden the pool of patients who could benefit from device-aided therapy, as the threshold for consideration of this reversible option may be lower than for more invasive device-aided therapies,9 and some patients for whom DBS would be contraindicated due to cognitive impairment could be eligible for SC therapy. Soileau welcomed the availability of more treatment options (following introduction of SC infusion therapies in the USA), noting that having different options allows physicians to tailor treatment to a patient’s specific OFF symptoms.
For example, DBS might be more suitable than fosCD/fosLD for a patient with levodopa-resistant tremor, whereas freezing gait can be worsened with DBS and CSAI might be more beneficial.
A proposed schema for positioning SC infusion therapies in the treatment pathway is shown in Figure 1. It is important to note
SC infusion
Invasiveness Minimal
Initiation setting
Clinic/home; may be initiated in inpatient setting in Europe
Evaluation Does not need extensive evaluation
Hardware
External; may need carrying case for pump weighing up to approximately 300 g
Ongoing management Daily
Waterproof No*
DBS
Requires surgery under general anaesthetic
Requires admission for surgery
Neurosurgical evaluation; neuropsychological testing to assess cognitive status; anaesthesia clearance
Small internal device
As needed
Yes
*The pump can be removed for showering/bathing using the disconnect feature on the NeriaTM Guard (Convatec, London, UK) infusion set.
DBS: deep brain stimulation; SC: subcutaneous.
that there is no single preferred pathway, and an individualised approach is required to meet patients’ specific needs.
What Factors Influence Treatment Selection
Between CSAI or Foscarbidopa/Foslevodopa?
Once SC infusion has been selected as the preferred therapeutic approach, the next decision is between CSAI or fosCD/fosLD. This must be considered on an individual basis for each patient. No head-to-head studies have directly compared the efficacy and safety of CSAI and fosCD/fosLD. Lees’ group conducted an indirect treatment comparison based on published literature, which suggested comparable efficacy of the two treatments.25 Safety profiles were also broadly similar, though there was a trend towards better tolerability of CSAI, driven by higher rates of infusion site reactions and hallucinations with fosCD/fosLD, which is borne out in real-world clinical experience (as discussed later in this article). Since magnitude of effect is similar across different SC infusion therapies, treatment choice will come down to other factors.
Cost may be one factor;25 however, cost–benefit considerations and reimbursement arrangements for each treatment in different regions are beyond the scope of this article. Based on clinical considerations only, factors that might influence treatment choice include: preference for monotherapy versus adjunctive treatment; infusion duration; prior response to oral levodopa or dopamine agonists (patients who have responded well to oral levodopa, but lost efficacy due to declining GI absorption, are likely to respond to levodopa-based treatment via other routes of administration, while good response to oral/transdermal dopamine agonists might predict good response to CSAI); predisposition to side effects (also based on prior experience with oral levodopa-based medication or dopamine agonists); symptom profile (for example, CSAI can help non-motor symptoms, including apathy); and pump characteristics such as size, weight, and complexity.
The “beauty of having options,” Soileau said, is that you can start one SC treatment and monitor the patient’s response, and, if the response is unsatisfactory, there is
Table 1: Factors that may influence choice of SC infusion versus DBS.
still another SC option to try. Switching SC therapies is relatively easy for the patient as the same infusion set can be used, so their routine of changing needles, and associated steps, would not need to change. Although the pumps differ, patients are familiar with the concept of using a pump for continuous drug delivery.
PRACTICAL MANAGEMENT OF PD USING SC INFUSION THERAPIES: REAL-WORLD CLINICAL EXPERIENCE
This article reflects the perspectives of experts practicing in several European countries and the USA, revealing differences in some aspects of practical management
that are dictated by local health systems. Local logistical considerations are not addressed in detail here. This article focusses on clinical aspects of management, on which there was a high level of agreement between contributors.
Before Initiation
Acceptance of treatment can be improved by proactively discussing the concept of continuous infusion with patients at an early stage in the disease course. Alongside communicating benefits (Antonini explained how he talks to patients about being able to achieve a more constant clinical state and simplifying their treatment regimen), it is important to set realistic expectations. Magee commented
1: Proposed placement of SC infusion therapies in the PD treatment pathway.
*Candidates for infusion therapies should have capacity or support to manage infusion equipment and should not have significant dementia.
†Candidates for DBS should not have significant cognitive impairment.
Patients with OFF time ≥2 hours with some functional difficulty who have tried ≥1 adjunctive medication are eligible for device-aided therapy.
Proposed positioning does not account for approval/reimbursement status of different treatment options in regional healthcare systems, which may dictate eligibility for specific options.
that patients need to be aware that SC treatment is “not a panacea,” and must be prepared for practical aspects of care, including managing the infusion equipment and maintaining good skin management.
Where available, a prophylactic anti-emetic (domperidone) may be administered before starting CSAI. Magee indicated that this is common practice in the UK; however, Pahwa noted that domperidone is not available in the USA and nausea is mitigated through slow titration from a low starting dose.
Initiation and Titration
SC infusion therapy may be initiated in outpatient clinics, in the hospital inpatient setting, or at home; approaches varied between practitioners in different countries, as did the level and nature of nursing support available. Several European experts highlighted benefits of admitting patients as inpatients for a few days to facilitate close monitoring and support during initiation and titration. Lees explained that hands-on support can help patients get over initial ‘teething problems’ with infusion equipment. Specialist centres often take patients referred from a wide area and admit patients for whom it is not practical to travel to the clinic for daily assessments and adjustments during the titration phase. However, inpatient admission is not the best approach for all patients; for example, some patients with neurocognitive deficits may become disoriented by the unfamiliar environment. Magee noted that the COVID-19 pandemic forced a move towards more home-based care, even by specialist centres that had typically provided inpatient care in the UK, by nurses with specialist training under close supervision to guide titration. This approach has been retained where possible for patients who prefer home-based care.
In the USA, SC treatment is initiated in outpatient clinics or at home. The ability to manage patients in the outpatient setting was viewed as an advantage over more invasive treatments that require costly admission for surgery. At the present time, fosCD/fosLD is usually initiated and optimised in day clinics, while CSAI can be
initiated at home, in the clinic, or using a hybrid approach.
Initiation of CSAI is usually performed in the ON state, as infusion is started at a low dose and can take several hours to take effect. Recommendations for initiating CSAI have been published elsewhere.26,27 Briefly, a typical initiation protocol begins at a low dose (1 mg/hr), with dosage increased in small increments (0.5 mg/hr) to a maximum of 6 mg/hr. The speed of the titration depends on the setting and on toleration of treatment. In some European centres, inpatients with excellent tolerability may achieve a steady dose in around 7–10 days under close monitoring. In outpatient and home settings, titration usually proceeds less rapidly over several weeks.26 If the patient was using an oral or transdermal dopamine agonist prior to starting CSAI, this is gradually reduced as it is replaced by CSAI during the titration window to avoid dopamine withdrawal syndrome. Concomitant levodopa is also tapered down. CSAI is generally used as an adjunct to oral levodopa, but a key therapeutic goal is to reduce oral levodopa dosage as far as possible to minimise dyskinesia and reduce the burden of oral medication regimens,9 and some patients ultimately achieve monotherapy with CSAI.
For fosCD/fosLD, the starting dose is guided by the patient’s existing oral levodopa dosage, aiming to replace oral levodopa with an equivalent dose of fosCD/fosLD. A conversion formula that adjusts for molecular weight and bioavailability of foslevodopa versus levodopa is provided in the prescribing information28 and via an online calculator. However, Katzenschlager and Antonini cautioned that this does not account for incomplete GI absorption of oral levodopa. Many patients with impaired GI absorption take high nominal oral dosages to achieve an effective therapeutic dose. As the proportion of the oral dose that ultimately reaches the brain cannot be reliably determined, direct conversion from nominal oral dosage may risk overestimation. Infusion can be started at a lower dose than that calculated based on oral dosage and titrated to find the therapeutic window that reduces OFF time without inducing
dyskinesia. Concomitant dopamine agonists can be withdrawn, ultimately aiming for fosCD/fosLD monotherapy, but should be tapered down gradually, not stopped abruptly, to reduce the risk of dopamine agonist withdrawal syndrome.
Optimising Infusion Duration and Flow Rate
CSAI is usually administered for approximately 16 hours per day, with 8 hours’ break overnight, while fosCD/fosLD is intended for continuous 24-hour infusion. In practice, however, duration can be varied to reflect individual motor patterns, non-motor symptoms, and tolerability.
While some patients may continue CSAI throughout the day and night, this constitutes off-label use. Some centres use transdermal or long-acting oral dopamine agonists to provide dopaminergic treatment during the night for patients stopping infusion overnight. Patients may experience morning OFF episodes after an overnight break from CSAI and require a bolus dose on waking. The infusion pump has an ‘extra dose’ facility to administer a loading dose on restarting infusion in the morning. However, cannulating and reconnecting the pump may be challenging for patients with motor impairment on waking (unless assistance is provided by a caregiver), so some patients instead administer a dose of SC apomorphine using an injection pen, which typically takes effect within approximately 5–15 minutes, or use alternative on-demand medication. Isaacson advised establishing a stable dosage for continuous infusion before enabling the extra dose function.
Although primarily intended for daytime use, Lees outlined an alternative use of CSAI in patients with nighttime symptoms. He described the APOMORPHEE study, a double-blind, placebo-controlled crossover study in 46 patients with PD and moderateto-severe insomnia, in which nighttimeonly CSAI was associated with significant improvement in mean PD sleep scale scores, compared with placebo.29
FosCD/fosLD is now available for patients requiring 24-hour dosing to manage
nighttime symptoms, provide motor control overnight (for example, for patients who need to mobilise to use the bathroom at night), or avoid morning OFF episodes. In Pahwa’s experience, most patients welcome the benefits of 24-hour dosing, but some patients on fosCD/fosLD do break from treatment overnight; for example, if they find it more comfortable to remove the pump to sleep or as a measure to manage side effects. Neuropsychiatric AEs, particularly hallucinations, can manifest as nightmares, and in such cases discontinuing treatment overnight can be beneficial. However, Henriksen noted that patients who interrupt treatment overnight can experience a prolonged morning OFF period, and for this reason, overnight discontinuation is rarely recommended at her centre. Instead, the experts interviewed generally advocated reducing the infusion rate to administer a lower dose overnight.
The fosCD/fosLD pump has base, low, and high flow-rate settings that patients can switch between. The infusion rates delivered at each setting can be adjusted according to clinical need. Antonini suggested setting the low rate at approximately 50% of the base rate to provide substantially lower overnight dosing, whereas Hauser reported using low and high rates set 10% below and above the base rate, respectively. Antonini cautioned against frequent day-to-day changes in flow rate, recommending a simple regimen of base rate during the day and low rate overnight. This approach facilitates interpretation of treatment response to guide dose adjustments at follow-up visits. The pump also includes an ‘extra dose’ function to deliver bolus doses if OFF symptoms emerge, which can be useful for patients experiencing morning OFF symptoms after reduced overnight dosing. However, bolus doses take 2–3 hours to provide benefit, so other on-demand medications with faster onset, such as levodopa inhalation powder or dispersible tablets, may be required.
Using the Infusion Set
A crucial element of the initiation visit, whether in the clinic or at home, is
educating the patient and their caregivers on correct use of the infusion kit. Patients with preserved manual dexterity are often able to manage infusion-set changes independently, although in some cases assistance from a relative or caregiver is required either routinely or during periods of impaired motor function.
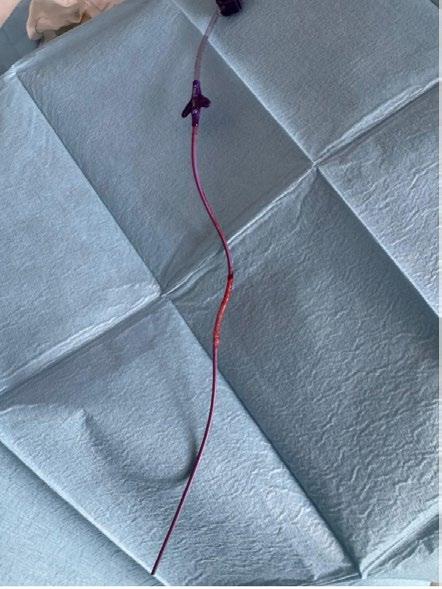
Many centres use an SC infusion set with an automated insertion device to standardise technique and reduce needlestick risk. All contributors to this article reported using the NeriaTM Guard (Convatec, London, UK) infusion set with both CSAI and fosCD/fosLD. This system comprises a soft cannula with a retractable introducer needle, which is secured to the body at the chosen infusion site using an adhesive patch, an insertion device that deploys the needle into the skin, and tubing that connects the cannula to the pump (Figure 2). The introducer needle remains hidden from the patient throughout the process of insertion using the automated device, which may make SC infusion more accessible to patients with needle phobia.
Key considerations for optimal use include:
• Frequent changing: Infusion sets should be changed daily for most patients, as prolonged use could increase risk of infusion site reactions. Although instructions for fosCD/fosLD recommend
changing the infusion set every 72 hours, there was broad agreement among the experts interviewed for this article that it is best practice to change infusion sets more frequently to maintain cleanliness and allow regular repositioning. Most advised patients to change sets daily initially, with the option to extend to every other day if patients tolerate infusions well. Since CSAI is discontinued overnight, a new infusion set is used when the infusion is restarted each day.
• Site selection: A new site should be used each time the infusion set is changed, with systematic rotation to allow adequate healing. Suitable sites with sufficient SC adipose tissue include the abdomen, flanks, thighs, and upper arms. Although abdominal sites close to the umbilicus are recommended in fosCD/fosLD manufacturer instructions,28 this restriction limits site rotation. Using sites over a wider body area allows patients to rotate between sites they find most comfortable and does not affect fosCD/fosLD bioavailability.30
• Hygiene: Rigorous hygiene is essential to minimise infection risk. Patients are taught aseptic technique, including handwashing and cleaning the site
Figure 2: Infusion set for use with continuous subcutaneous apomorphine infusion or subcutaneous foscarbidopa/ foslevodopa pump.
NeriaTM Guard (Convatec, London, UK) soft cannula infusion set with an integrated insertion device.
before applying the adhesive patch. Soileau emphasised the importance of teaching patients and caregivers good hygiene practices, saying “educate, educate, educate,” while Magee concurred that the importance of hygiene “cannot be stressed enough.”
• Cannula insertion: The skin should be pulled taut with the insertion device held flush against the skin so that the needle enters perpendicular to the surface. Full penetration of the dermis is required to ensure delivery into the SC space. The NeriaTM Guard infusion set can be used with a 9 mm or 6 mm cannula; all contributors to this article expressed a preference for the 9 mm cannula to ensure complete penetration of the dermis. The automated insertion device makes it easier for patients to achieve the correct insertion angle and depth compared with older infusion sets that required manual insertion of the cannula/needle.
• Connecting and operating the pump: Tubing should be connected to the pump and primed with solution before attachment to the cannula to avoid introducing air. While infusion rates are programmed by healthcare staff, patients must learn to operate usercontrolled features, such as low/high flow rate selection for fosCD/fosLD and extra doses.
• Post-insertion: Gentle massage of the infusion site after starting the infusion, for example, using a handheld massager, helps disperse medication to reduce nodule formation.
• Troubleshooting: Pain, burning, or visible pooling of medication beneath the skin suggests inadequate needle penetration; in such cases, patients should immediately re-cannulate, using a new infusion set rather than attempting to reposition the existing needle. Infusion solution ‘oozing’ onto the skin also suggests incorrect insertion, as the cannula is primed with medication only after deployment,
during automated insertion with NeriaTM Guard, to prevent the solution from coming into contact with the skin surface. Liquid should be wiped away promptly to avoid irritation.
From a practical perspective, infusion-set design and human factors can be critical success factors for SC therapy.31 For example, automated insertion simplifies training and supports reliable drug delivery by improving consistency of cannula placement, and reduced needle handling improves safety. Magee described such innovations as “gamechanging,” noting that ease-of-use can mean “the difference between infusion therapy working and not working.”
Follow-Up
Experts consistently highlighted the importance of providing support in the early stages of SC infusion therapy to help establish treatment successfully and reduce the risk of discontinuation. Follow-up visits, conducted at home or in the clinic, provide an opportunity to troubleshoot problems with the infusion set or pump and to monitor side effects. Patients should also be able to access support, ideally on a 24-hour basis, to permit prompt reporting of issues that arise, particularly skin reactions.
Managing Adverse Reactions
Infusion site reactions are a potential concern with any infused medication. Skin reactions including nodules, erythema, pain, and cellulitis have been reported with SC infusion therapies for PD.10-14 Effective mitigation of such reactions is important to promote treatment adherence. Good hygiene and frequent changing and repositioning of infusion needles are key steps. Isaacson also suggested that decreasing the infusion flow rate can help ensure medication is absorbed and does not accumulate in the SC space and form nodules, alongside a gentle massage to aid dispersion.
Distinguishing between inflammatory reactions and infection at the infusion site can be challenging in clinical practice. Redness around the site could indicate either; several interviewees recommended
taking photographs and marking the margins of erythema to help monitor changes in size and colour. Heat or pus may indicate infection. Doxycycline, which has anti-inflammatory as well as antibiotic properties, can be prescribed if infection is suspected. Topical corticosteroids can be used to alleviate local inflammation when infection is not suspected.
European experts with longstanding experience with CSAI commented that they had observed a decline in rates of skin problems over the years, owing to a combination of growing experience of managing AEs and improvements in infusion set/needle technology. FosCD/ fosLD, however, is associated with a higher rate of skin complications, including infections and abscesses, which can impact treatment adherence. Magee observed that repeated infections requiring antibiotics had contributed to the decision to discontinue fosCD/fosLD for some patients in her clinic. Specific strategies to manage fosCD/ fosLD-related skin reactions may emerge as clinical experience accumulates.
Aside from skin reactions relating to the mode of administration, patients may experience side effects associated with dopaminergic medication, including neuropsychiatric adverse events, such as hallucinations or psychosis, and nausea. Titrating up slowly from a low starting dose is recommended to reduce the risk of these AEs. Orthostatic hypotension, which is commonly associated with oral dopamine agonists and injectable apomorphine, appears to be less common with CSAI, Soileau observed, possibly reflecting a “gentler, smoother” drug concentration profile.
Advances in SC Infusion Therapy
There have been significant advances in SC infusion technology since CSAI first became available. Speaking based on several decades of experience with CSAI, Lees explained that pumps have become smaller and more ambulatory, and infusion sets have evolved substantially. Modern infusion sets such as NeriaTM Guard provide standardised insertion and reduced needle
handling, and contributors highlighted the availability of the 9 mm cannula option as particularly useful to ensure consistent SC delivery. Lees noted that current needle systems with soft polytetrafluoroethylene cannulas are less irritative than older infusion sets with steel needles, and discontinuation of CSAI because of skin nodules is now uncommon in his clinic. Henriksen has also observed reduced rates of skin problems since introducing NeriaTM Guard compared with older infusion devices that were available when she began using CSAI in her clinic approximately 25 years ago. Overall, Henriksen perceived CSAI as a well-tolerated therapy based on her extensive clinical experience.
As fosCD/fosLD has only recently entered real-world clinical practice, a learning curve for prescribing clinicians is anticipated,32,33 particularly with respect to identifying and managing practical challenges. In real-world settings, clinicians are already adapting manufacturer guidance, for example by changing infusion sets more frequently (daily instead of every 72 hours) and rotating infusion sites across wider body regions, to mitigate risk of skin reactions. Magee emphasised the importance of providing clear instructions to patients regarding these adaptions, as discrepancies between advice from the treating clinician and the manufacturer’s instructions may otherwise lead to confusion.
CONCLUSION
The addition of SC infusion therapies to the treatment armamentarium for advanced PD expands the range of options available to patients who experience motor fluctuations on oral levodopa-based regimens and provides a potential alternative to surgical interventions. Greater choice to select the best treatment to meet patients’ needs was welcomed by experts, particularly in the USA, where SC infusion therapy is a relatively new option. Treatment success with SC infusion therapy is improved by proactive mitigation and effective management of adverse effects, particularly infusion site reactions, to minimise avoidable treatment discontinuation. The overall
‘therapy system’ offers opportunities to further optimise treatment outcomes in real-world practice through dose
References
1. Han S et al. Global, regional, and national epidemiology of neurological disorders and subcategories: incidence and disability-adjusted life years, 1990-2021. Eur J Med Res. 2025;30(1):711.
2. Postuma RB et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591-601.
3. Thanvi BR, Lo TCN. Long term motor complications of levodopa: clinical features, mechanisms, and management strategies. Postgrad Med J. 2004;80(946):452-8.
4. Isaacson SH et al. Should “on-demand” treatments for Parkinson’s disease OFF episodes be used earlier? Clin Park Relat Disord. 2022;7:100161.
5. Ivan IF et al. Gastro-intestinal dysfunctions in Parkinson’s disease (review). Exp Ther Med. 2021;22(4):1083.
6. Mukherjee A et al. Gut dysfunction in Parkinson’s disease. World J Gastroenterol. 2016;22(25):5742-52.
7. AbbVie. AbbVie launches PRODUODOPA® (foslevodopa/ foscarbidopa) for people living with advanced Parkinson’s disease in the European Union. 2024. Available at: https://news.abbvie. com/2024-01-09-AbbVie-LaunchesPRODUODOPA-R-foslevodopafoscarbidopa-for-People-Living-withAdvanced-Parkinsons-Disease-in-theEuropean-Union#:~:text=AbbVie%20 was%20granted%20marketing%20 authorization,Mark%20in%20 November%20of%202023. Last accessed: 27 January 2026.
8. Lees AJ, Bhidayasiri R. The resurrection of apomorphine: a dopamine analogue comparable in potency to L-DOPA. Parkinsonism Relat Disord. 2025;139(Suppl 1):107923.
9. Katzenschlager R, Bergquist F. Continuous subcutaneous infusion therapies in Parkinson’s disease: evidence of efficacy and safety. Parkinsonism Relat Disord. 2025;139(Suppl 1):107905.
10. Katzenschlager R et al. Apomorphine subcutaneous infusion in patients with Parkinson’s disease with persistent motor fluctuations (TOLEDO): a multicentre, double-blind, randomised, placebo-controlled trial. Lancet Neurol. 2018;17(9):749-59.
11. Katzenschlager R et al. Long-term safety and efficacy of apomorphine infusion in Parkinson’s disease patients with persistent motor fluctuations: Results of the open-label phase of the TOLEDO study. Parkinsonism Relat Disord. 2021;83:79-85.
individualisation, structured patient and caregiver education, and reliable delivery via user-friendly infusion equipment.
12. Isaacson SH et al. Continuous, subcutaneous apomorphine infusion for Parkinson disease motor fluctuations: results from the phase 3, long-term, open-label United States InfusON study. J Parkinsons Dis. 2025;15(2):361-73.
13. Soileau M J et al. Safety and efficacy of continuous subcutaneous foslevodopafoscarbidopa in patients with advanced Parkinson’s disease: a randomised, double-blind, active-controlled, phase 3 trial. Lancet Neurol. 2022;21(12):1099109.
14. Aldred J et al. Continuous subcutaneous foslevodopa/foscarbidopa in Parkinson’s disease: safety and efficacy results from a 12-month, single-arm, openlabel, Phase 3 study. Neurol Ther. 2023;12(6):1937-58. Erratum in Neurol Ther. 2023;12(6):1959-60.
15. Aldred J et al. Efficacy and safety of foslevodopa/foscarbidopa monotherapy in patients with Parkinson’s disease. Mov Disord Clin Pract. 2026;13(1):181-90.
16. AbbVie. Real-world study of ABBV-951 subcutaneous infusion to assess change in disease activity in adult participants with Parkinson’s disease (ROSSINI). NCT06107426. https://clinicaltrials.gov/ study/NCT06107426.
17. Jost W et al. Real-world safety and effectiveness of foslevodopa/ foscarbidopa in Parkinson’s disease: ROSSINI study 6-month interim results. Abstract LBA-15. MDS Congress, 5-9 October, 2025.
18. Antonini A et al. Developing consensus among movement disorder specialists on clinical indicators for identification and management of advanced Parkinson’s disease: a multi-country Delphipanel approach. Curr Med Res Opin. 2018;34(12):2063-73.
19. Aldred J et al. Application of the ‘52-1’ screening criteria in advanced Parkinson’s disease: interim analysis of DUOGLOBE. Neurodegener Dis Manag. 2020;10(5):309-23.
20. Antonini A et al. Foslevodopa/ foscarbidopa in younger patients earlier within advanced Parkinson’s disease: post hoc analysis of a randomized trial. Neurol Ther. 2026;15(1):309-24.
21. Olivola E et al. Continuous subcutaneous apomorphine infusion in Parkinson’s disease: causes of discontinuation and subsequent treatment strategies. Neurol Sci. 2019;40(9):1917-23.
22. Dijk JM et al. The choice between advanced therapies for Parkinson’s disease patients: why, what, and when? J Parkinsons Dis. 2020;10(s1):S65-73.
23. Antonini A et al. Comparative effectiveness of device-aided therapies on quality of life and offtime in advanced Parkinson’s disease:
a systematic review and Bayesian network meta-analysis. CNS Drugs. 2022;36(12):1269-83.
24. Potel SR et al. Twenty-five-year experience with apomorphine pump in Parkinson’s disease: a real-life longterm retrospective tolerance study. J Parkinsons Dis. 2025;15(5):970-81.
25. Verin M et al. Licensed subcutaneous infusion therapies in advanced Parkinson’s disease: an indirect treatment comparison and costminimisation analysis. Neurol Ther. 2025;14(5):1919-33.
26. Henriksen T et al. Practical use of apomorphine infusion in Parkinson’s disease: lessons from the TOLEDO study and clinical experience. J Neural Transm (Vienna). 2023;130(11):1475-84.
27. Bhidayasiri R et al. Effective delivery of apomorphine in the management of Parkinson disease: practical considerations for clinicians and Parkinson nurses. Clin Neuropharmacol. 2015;38(3):89-103.
28. AbbVie. Vyalev prescribing information. 2024. Available at: https://www.rxabbvie. com/pdf/vyalev_pi.pdf. Last accessed: 27 January 2026.
29. Cochen de Cock V et al. Safety and efficacy of subcutaneous night-time only apomorphine infusion to treat insomnia in patients with Parkinson’s disease (APOMORPHEE): a multicentre, randomised, controlled, double-blind crossover study. Lancet Neurol. 2022;21(5):428-37.
30. Han YR et al. Bioequivalence of foslevodopa/foscarbidopa continuous subcutaneous infusion to arm, thigh, or flank versus abdomen in healthy and advanced Parkinson’s disease individuals. Clin Park Relat Disord. 2025;13:100359.
31. McGuckin MB et al. Enhancing Parkinson’s and palliative patients’ care: nurse perspectives on the Neria Guard infusion set. Br J Nurs. 2025;34(16):8349.
32. Fung VSC et al. Continuous subcutaneous foslevodopa/foscarbidopa infusion for the treatment of motor fluctuations in Parkinson’s disease: Considerations for initiation and maintenance. Clin Park Relat Disord. 2024;10:100239.
33. Chaudhuri KR et al. Considerations for initiation and maintenance of foslevodopa/foscarbidopa for advanced Parkinson’s disease. Mov Disord Clin Pract. 2026;DOI:10.1002/mdc3.70489.
Interview
James Zou, Associate Professor of Biomedical Data Science at Stanford University, California, USA, joined EMJ for a discussion on AI and its role in transforming clinical research. He discusses the shift towards AI systems that can generate hypotheses, the challenges of deploying AI tools in real-world healthcare, and the growing role of real-world data and wearable technologies in predicting disease and improving trial design.
James Zou
Associate Professor of
Biomedical
Data Science, Stanford University, California, USA
Q1 When did you first become interested in applying AI to clinical research?
I’ve been working at the intersection of AI and biomedicine for about 15 years now, since my PhD. My initial work was more focused on using AI to enable biomedical discoveries. When I came to Stanford, California, USA, in 2016, that’s when I started doing more work on AI for clinical research.
Q2 Your work spans clinical prediction, genomics, and large-scale AI models. When you look at the field today, what’s changed the most since you first started working in healthcare AI?
years, we’ve seen the emergence of much more autonomous AI driven by language models and AI agents. Because these agents are more autonomous, they can start to come up with their own problems. They don’t have to wait for us to define the problem. They can generate hypotheses and even create their own tools.
Q3
From a clinician’s perspective, for example, in dermatology, when diagnosing melanoma, if AI provides a conclusion, a clinician still has to review it. Do you think that will always be necessary, or could we step aside in the near future?
In the last 2 years, we’ve seen the emergence of much more autonomous AI driven by language models and AI agents
I think the biggest change we’ve seen is the shift from viewing AI as a tool to viewing AI as more of an agent or co-scientist.
In the past, when I first started in the field, we would begin with a specific problem in medicine or healthcare and then apply or develop an AI tool to tackle that problem. But in the last 2
Currently, it’s still necessary for human experts and clinicians to provide final judgment and oversight over these AI systems. Not necessarily for every step, but for the most important decisions. For example, the final diagnosis or treatment decision. I think that oversight is still necessary.
Q4
Some studies suggest AI can make fewer mistakes than clinicians. So why do we still need to revise AI decisions?
AI is still a relatively new and emerging technology. The algorithms might work very well on the specific data and hospitals they were trained on, and they could be very reliable there, but if they’re applied in the wild, in new clinics or with different patient populations, there’s still uncertainty about how the models will perform. They might work very well and be robust, but there’s also a chance they could make mistakes.
Because of that uncertainty, at least for now, it’s still useful to have human experts involved in the assessment.
Q5
In your work on Trial Pathfinder, you showed that eligibility criteria can significantly impact both trial enrolment and generalisability. What was the most unexpected insight from that research?
One interesting finding was that we could actually broaden the eligibility criteria. Many existing criteria that determine which patients are eligible for clinical trials are quite restrictive, perhaps overly so.
In our paper, we showed that we could substantially relax some of these criteria. This allows much more diverse and larger patient populations to enrol, including more women, more minorities, and older patients.
Even though we relaxed the criteria to some extent, we found that we could still maintain safety and not incur more adverse events.
trials are often overly narrow and restrictive. There are increasing efforts from drug developers, pharmaceutical companies, and regulators like the FDA and EMA to diversify clinical trial populations.
Q6 Your work relies heavily on real-world clinical data. What are the biggest opportunities and limitations of using real-world data to inform trial design and clinical decision-making?
There are many opportunities to leverage real-world data. One area I’m particularly excited about is using it to create digital twins or to simulate clinical trials synthetically.
Real-world data is very diverse and linked to medical records, so we know the outcomes. We can computationally generate digital or in silico cohorts that mirror patients from different kinds of clinical trials.
We can computationally generate digital or in silico cohorts that mirror patients from different kinds of clinical trials
Do you think this approach will be implemented more widely in clinical trials?
Yes. Since our research, there’s growing recognition that clinical
This is faster and can provide valuable insights. It doesn’t fully replace actual clinical trials, but it helps us design trials more efficiently and make them more inclusive.
One limitation is that real-world data is often messy and noisy compared to curated clinical trial data. Electronic health records often contain missing information, and there are biases in what gets recorded and what doesn’t. We need computational and statistical methods to account for that when leveraging this data.
Q7
There’s a lot of excitement around AI in medicine, but also frustration. Where are we genuinely making progress, and where are we getting stuck?
We published a study looking at how many medical AI devices have been cleared by the FDA. There are already over 1,000 AI medical devices cleared by regulation.
That shows significant technological progress. We have AI-driven devices across many imaging modalities and indications that have gone through FDA review.
Where we’re getting stuck is deployment. When we looked at those 1,000 FDA-cleared devices and measured adoption, for example, through insurance reimbursement data, we found that only a handful are being widely deployed.
A major bottleneck is the economics. How do you reimburse AI algorithms? How do you quantify their value? Headline metrics are often context dependent. You might see excellent performance in a controlled setting like Stanford, but results could differ in a rural clinic or another country.
Companies need a sustainable financial model. The economics of deployment remains a key challenge.
Q8
Fairness and bias are central topics in clinical AI. Has the discussion matured in recent years?
Fairness and bias are critical, especially when AI systems are making important decisions like diagnoses. We need these models
to be robust and work well across diverse populations and settings.
Bias and fairness are components of robustness. I think we’ve made significant progress in understanding how to evaluate models rigorously and test them across different sites and distributions.
There is greater awareness and better techniques now to assess and mitigate potential biases.
Q9
How can clinicians recognise when a system may not generalise to their patient population?
Vendors need to provide transparent statistics. For example, if an AI system for dermatology was trained mainly on European populations, that should be clearly stated.
Clinicians in other regions may then decide to conduct additional testing to ensure the algorithm performs well on different skin tones or populations.
Q10When health systems adopt AI tools, what should they look for beyond headline performance metrics?
Headline metrics are often context dependent. You might see excellent performance in a controlled setting like Stanford, but results could differ in a rural clinic or another country.
Healthcare systems shouldn’t just look at the metrics themselves, but also at the context in which they were generated. They need to ask whether that context is generalisable to their own setting.
Q11Do clinicians today have enough understanding to ensure AI tools are used safely?
There’s still an educational process underway. There are many AI systems available, and there’s also a lot of noise in the space.
We need more experience and better support to help clinicians evaluate and use these AI devices appropriately.
Q12Looking ahead, where is your research headed next?
We’ve been fortunate that several of our research projects have gone through FDA clearance. For example, we developed an algorithm for diagnosing cardiovascular diseases from ultrasound videos. It was evaluated in a clinical trial, cleared by the FDA, and is now being deployed.
Looking ahead, we’re excited about leveraging consumeraccessible wearables to predict health status and disease.
In a recent publication, we showed that by analysing one night of sleep recording, our AI model could predict over 100 different diseases.
Participants from sleep clinics were linked to their medical records, so we knew what future diseases they developed. The model could predict 130 diverse diseases, including cardiovascular disease, dementia, chronic kidney disease, and stroke.
This demonstrates the potential value of data that people can collect even during a single night of sleep.
We developed an algorithm for diagnosing cardiovascular diseases from ultrasound videos
Multiple Micronutrient Supplementation every stage of the pregnancy journey
This infographic has been sponsored by Bayer
Poor
10–15% incidence of perinatal mental health disorders3
women of reproductive age (69%) have ≥1 core nutrient deficiency (iron, zinc, folate)4
Micronutrient deficiencies are associated with adverse pregnancy outcomes.5
Micronutrient needs increase during pregnancy and lactation5 and deficiencies are widespread (Figure 1).4
Figure 2: RBC folate levels after supplementation with MMS containing 800 μg folic acid. 6
Figure 3: Reduction in the risk of NTDs with MMS containing 800 μg folic acid or folic acid alone. 8,9
Pre-conception
Micronutrients, particularly folic acid and vitamins B2, B6, and B12, are crucial for brain and neural tube formation.5
Prior to conception, RBC levels of folate must reach a threshold that is protective against NTDs (>906 nmol/L).5
Clinical study shows that protective folate levels are reached within 4 weeks with an MMS containing 800 μg folic acid (Figure 2).6
MMS containing 800 μg folic acid reduced the risk of NTDs by 92% vs controls (Figure 3).8
References
1. World Health Organization (WHO). 2025. Available at: https://www.who.int/ news-room/fact-sheets/detail/maternalmortality. Last accessed: 12 January 2026
2. World Health Organization (WHO). 2012. Available at: https://www.who.int/news/ item/02-05-2012-15-million-babies-born-
too-soon. Last accessed: 12 January 2026.
3. World Health Organization (WHO). Available at: https://www.who.int/teams/ mental-health-and-substance-use/ promotion-prevention/maternal-mentalhealth. Last accessed: 12 January 2026.
4. Stevens GA et al. Lancet Glob Health. 2022;10(11):e1590-9.
5. Liu J et al. Nutr Rev. 2025;83(12):2352-71.
6. Brämswig S et al. Int J Vitam Nutr Res. 2009;79(2):61-70.
7. Wang Y et al. J Reprod Med. 2017;26: 1196-206.
8. Czeizel AE. Int J Med Sci. 2004;1 (11):50-61.
9. Blencowe H et al. Int J Epidemiol 2010;39:i110-21.
10. Khodova SI, Murashko LE. Consilium Medicum. 2006;8(6):20-3.
11. Lin S et al. Chinese J Pract Gynaecol
Multiple micronutrient iron, folate, and contribute to the
An MMS containing significantly reduced (p<0.0001) and (p<0.005) in at-risk
A study in a Chinese lower rates of with MMS vs folic 25.3%
Figure 4: Incidence women receiving
Folic acid only
Obstet. 2020;36:177-81.
12. Arzhanova ON 5:53-5.
13. Paoletti AM et 2013;29(8):779-83.
Supplementation supports
micronutrient deficiencies in non-pregnant women 15–49 years. 4
MMS are comprehensive formulations developed to support maternal and infant health
MMS are designed to support maternal nutritional needs during preconception, pregnancy, and lactation.5
MMS typically contain up to 800 μg folic acid plus other vitamins and minerals in a single pill taken once daily.5
MMS have been used by millions of women for over 40 years and have a good safety and tolerability profile.5
Pregnancy
micronutrient deficiencies, including and vitamins B2 and B12, the risk of anaemia. 5 containing 800 μg folic acid reduced the risk of anaemia and improved iron status at-risk women.10
Chinese population showed iron deficiency anaemia folic acid alone (Figure 4).11
Incidence of iron-deficiency anaemia in receiving folic acid only vs MMS.11
Abbreviations:
3 months of MMS before and during pregnancy, in women at risk, reduced preterm birth risk 6.6-fold vs previous pregnancies.12
6.6-fold
EMJ. 2026;11[1]:32-33. https://doi.org/10.33590/emj/NTYC9210 reduction in pre-term birth risk
Conclusion
Clinical evidence demonstrates that MMS, particularly formulations containing 800 μg folic acid, can support maternal and fetal health from pre-conception through pregnancy and lactation.
MMS resulted in significant improvements in mood vs a calcium + vitamin D3 treatment (Figure 5).13
Figure 5: Improvements in post-natal mood using the Edinburgh Post-natal Depression Scale.13
Gian Carlo Di Renzo
Zigor Campos Goenaga
Red Flags Raising Suspicion of Eosinophilic Granulomatosis with An EGPAware European Consensus
GSK provided funding towards the EGPAware consensus The information provided in this infographic has been EMJ. 2026;11[1]:34-35. https://doi.org/10.33590/emj/ABOL8230
25
EGPA is a rare, multisystemic disease, often including asthma, that requires MDT management and expert diagnostic evaluation
Diagnosis and treatment of EGPA are often delayed, which highlights the need for early identification
Introduction Study Design
EGPAware is the first large European Delphi study, aiming to establish a multidisciplinary consensus of clinical suspicion criteria for EGPA.
Red flags were ranked by panellists based on CR and on FO
EGPA-treating physicians 53 17 European countries. from
Reference:
1. Hellmich B et al. EULAR Rheumatol Open. 2026;2(1):9-18
• Lung infiltrates/ nodule(s)
• Alveolar haemorrhage/ haemoptysis
Considering ≥6 years old and persistent unexplained EOSINOPHIL levels if untreated or >500 previously received that may have altered eosinophil
• Ischaemic injuries including intestinal ischaemia (including recurrent abdominal pain that is ischaemic in nature† or perforation [gastric, oesophageal, or small intestine])†
Most panellists were rheumatologists or pulmonologists, with 50% having >15 years of experience in EGPA-patient management.
*This figure contains the 25 red flags that achieved highlighted in bold correspond to the 12 most pertinent †Not explained by
consensus and this infographic, and editorial input in the latter. been peer-reviewed as part of Hellmich et al.1
https://doi.org/10.33590/emj/ABOL8230
5 red fags for
Considering a patient with asthma unexplained blood levels of >1,000 cells/µL >500 cells/µL if they received any medication altered the blood eosinophil count infiltrates/ nodule(s) Alveolar haemorrhage/ haemoptysis†
• Vasculitis on biopsy
• Biopsy with infiltrate predominantly eosinophillic
Highest Ranked Red Flags
Most relevant Red Flags based on clinical relevance
Most relevant Red Flags based on frequency of observation
• Clinical or histological diagnosis of glomerulonephritis
• Active urine sediment (haematuria, cellular casts, etc.)
• Pericardial effusion /pericarditis
• Cardiomyopathy (regardless of the diagnostic method, be it clinical, laboratory [e.g., proBNP], or imaging [e.g., echo, MRI])
• Cardiac involvement in young people (<45 years old)
• Nasal polyposis
• Chronic rhinosinusitis
• Palpable purpura
• Skin lesions such as ulcers, urticaria, nodules, or papules†
• Mononeuritis multiplex
• Polyneuropath (presenting as paraesthesia, numbness, tingling, etc.)†
• Cerebrovascular disease in patients <45 years old
achieved consensus among panellists. The signs pertinent red flags based both on CR and on FO. by another cause.
Red flags/signs (1 least relevant: 10 most relevant)
1. Mononeuritis multiplex 3. Vasculitis on biopsy 5. Biopsy with inflammatory infiltrate predominantly eosinophilic
The most frequently observed signs were: 7. Palpable purpura 9. Chronic rhinosinusitis 2. Lung infiltrates/ nodule(s)
Ranking of 10 most relevant red flags based on clinical relevance and frequency of observation (inverse balanced mean: 1 least relevant; 10 most relevant)
Key Takeaways
Clinician awareness of these suspicion criteria will enhance awareness, improve referral rates, and reduce diagnostic delays The most clinically relevant signs were:
Transforming Ulcerative Colitis Care: AI-Powered Endoscopic Scoring from Clinical Trials to Clinical Practice
Authors: *Flegg D,1 Byrne MF1-3
1. University of British Columbia, Department of Internal Medicine, Vancouver, Canada
2. Dova Health Intelligence, Vancouver, Canada
3. Division of Gastroenterology, Vancouver General Hospital, University of British Columbia, Canada
*Correspondence to df19@student.ubc.ca
Disclosure:
Byrne is a founder and shareholder in Dova Health Intelligence. Flegg has declared no conflicts of interest.
Received: 14.10.25
Accepted: 28.01.26
Keywords: AI, automated endoscopic scoring, digital biomarkers, endoscopic disease activity, endoscopy, machine learning, ulcerative colitis (UC), video-based deep learning.
Ulcerative colitis (UC) is a chronic, immune-mediated inflammatory disorder of the colon that follows a relapsingremitting course. Characterised by mucosal inflammation, the disease requires accurate and reproducible monitoring tools to guide treatment, assess response, and evaluate remission. Endoscopic visualisation remains the gold standard for evaluating disease activity, with scores such as the Mayo Endoscopic Subscore (MES) and the Ulcerative Colitis Endoscopic Index of Severity (UCEIS) serving as core endpoints in both routine care and clinical trials.1,2
However, these indices are inherently subjective and prone to inter- and intraobserver variability, even among expert central readers.3,4 Conventional scoring approaches often rely on assessing the most severely affected colonic segment, overlooking the heterogeneity of disease
extent, and failing to capture spatial distribution. Patients with the same MES values may present with different endoscopic disease throughout their colon and significantly different clinical courses.5
The limitations of human scoring have known real-world consequences. They contribute to discordance between clinical symptoms and objective findings, delay therapeutic escalation, and introduce inefficiencies into clinical trials. Reader variability continues to be a key challenge in multicentre trials, where disagreements over endoscopic scores can lead to adjudication processes that slow recruitment and delay trial progression; moreover, such inconsistencies may misrepresent treatment response, complicating endpoint interpretation and trial outcomes.
In this context, AI has emerged as a promising solution to automate, standardise,
and potentially enhance the assessment of endoscopic disease activity in UC. Through deep learning, a subset of AI that mimics the structure and function of the human brain, these systems can process vast volumes of imaging data and learn to recognise specific patterns or features within endoscopy videos. AI offers the potential to reduce reader variability, improve reproducibility, and support realtime decision-making, bringing objective and scalable tools into the hands of clinicians and researchers alike.
THE PROBLEM: VARIABILITY AND LIMITATIONS IN HUMAN SCORING
Despite their widespread use in both clinical practice and clinical trials, current endoscopic scoring systems in UC are plagued by substantial variability. Reproducibility is limited even among expert central readers, with key metrics such as MES and UCEIS showing only moderate agreement.3 Discrepancies over critical thresholds, for example, differentiating MES 1 from MES 2, can directly influence patient eligibility for trials and assessments of therapeutic response.4
One of the core limitations of these indices lies in their design. Both MES and UCEIS are ordinal scales that typically assess only the worst-affected segment of the colon, overlooking the patchiness and extent of disease elsewhere. This segmental bias undermines their ability to reflect the true burden of inflammation and limits their sensitivity to therapeutic change.
In the context of clinical trials, such inconsistencies can introduce operational challenges. Differences in reader interpretation may necessitate adjudication processes, which can add logistical complexity and affect study timelines.6 Subtle features such as endoscopic response and remission, particularly in moderate-to-severe disease or when mucosal healing is minimal, can be challenging to interpret and contribute to interobserver variability, even among experienced reviewers.6,7 Such misclassifications may contribute
to variability in treatment efficacy assessments, which in turn can influence the ability to meet primary endpoints and fully characterise therapeutic benefit.8,9 In clinical practice, variability in scoring may contribute to differences in treatment decisions, including the potential for under-treatment of residual inflammation or overtreatment based on subjective interpretation.
These limitations have underscored the need for more reproducible and scalable solutions. As endoscopic endpoints become increasingly central to clinical trials, especially with treat-to-target strategies, the field must move beyond static, subjective indices. AI offers a compelling path forward by enabling standardised, segmental, and reproducible evaluation of disease severity, with the promise of transforming how UC is assessed across both clinical and research settings.8
ADVANCES IN AI-DRIVEN ENDOSCOPIC SCORING FOR ULCERATIVE COLITIS
AI has rapidly advanced the automation of endoscopic scoring in UC, evolving from early, static image-based classifiers to comprehensive video-based systems. Initial models, trained on thousands of annotated still frames, replicated expert assessments of disease severity but were limited by their reliance on curated, high-quality images and binary outcome predictions.10,11 These approaches offered proof of concept but fell short in capturing the spatial and temporal complexity of colonic inflammation.
Recent developments have shifted towards dynamic, video-based models capable of analysing entire colonoscopy recordings. These systems preserve continuity across frames and allow for segmental evaluation, reflecting the heterogeneous nature of disease more accurately. Several groups have demonstrated strong correlation with central reader assessments using fulllength videos, achieving high inter-rater reliability for endoscopic indices such as MES and UCEIS.12-14
Byrne et al.15 introduced a deep learning model capable of scoring UC activity under both MES and UCEIS at the frame-, section-, and video-level scales. Trained on over one million frames from full-length colonoscopies, the system showed concordance with expert readers. The quadratic weighted kappa used to compare the inter-rater agreement between expert's labels and the model's predictions showed strong agreement (0.87 and 0.88 at frame level; 0.88 and 0.90 at section level; and 0.90 and 0.78 at video level, for MES and UCEIS, respectively).15
Several recent studies have evaluated AI models for automated assessment of endoscopic disease activity in UC using full-length colonoscopy videos. Chaitanya et al.16 described Arges (Janssen R&D, LLC, Raritan, New Jersey, USA), a transformerbased model that captures spatiotemporal patterns across full-length videos to estimate MES and UCEIS scores. Trained on millions of frames from four clinical trials and validated on held-out and prospective datasets (QUASAR), the agreement between the Arges MES output and human reader assessement (k=0.66) closely aligned with the two human expert rate agreement (k=0.71).16 Gutierrez-Becker et al.17 developed a model using spatial region mapping and per-frame MES classification, enabling segmental severity assessment and generating an interpretable Aggregate Disease Severity Score (ADSS).17 Their performance measurements were based on internal validation, using held-out test sets from within their clinical trial data. There was high agreement between the model and central reading at the level of the colon section (k=0.80), and the agreement between central and local reading (k=0.84) suggested a similar interrater agreement between the model and experienced readers.
Stidham et al.18 described the Cumulative Disease Score (CDS), a continuous metric derived from full-length video analysis, validated internally on held-out test sets. CDS was compared with the MES (p<0.0001) and all clinical components of the partial Mayo score (p<0.0001). CDS
showed sensitivity to change, requiring 50% fewer participants to demonstrate endoscopic differences between ustekinumab and placebo than the MES.18 More recently, Byrne et al.19 developed a large-scale AI model trained on 83.6 million video frames that were labelled by three expert central readers across seven categories per video. For the MES, the Intraclass Correlation Coefficient (ICC) for three expert central readers was 0.905, and for the AI model and majority vote from the readers, the ICC was 0.907. The model also outputs continuous frame-by-frame level information on the sub-score characteristics that make up the UCEIS score. Collectively, these systems illustrate a broader shift towards video-based, segmental, and continuous AI-driven assessment of endoscopic disease activity. Rather than replicating human scoring alone, modern AI approaches aim to enhance reproducibility, reduce variability, and increase sensitivity in evaluating disease severity.
AI IN CLINICAL TRIALS AND REAL-WORLD PRACTICE
AI-based endoscopic scoring systems are increasingly being integrated into clinical trials for UC, where they offer improved reproducibility, eliminate reader bias, and streamline adjudication processes. These tools allow for more sensitive detection of treatment effects and facilitate more efficient trial designs by reducing sample size requirements.19 By providing segmental, standardised scores across entire colonoscopy videos, AI systems are helping define more objective trial endpoints.
A recent example is the post-hoc application of AI scoring to the TITRATE study, a randomised trial comparing standard versus personalised guided infliximab dosing in acute severe UC. Although the original expert-read analysis did not meet the primary endpoint, AIbased re-analysis identified significantly higher response and remission rates in the personalised group.9 While requiring prospective validation, these findings suggest that advanced video-based AI systems may reduce reader variability and
increase sensitivity in endpoint evaluation, highlighting their potential to refine clinical trial design.
In clinical practice, similar technologies are being adapted to support real-time disease monitoring and treat-to-target strategies. AI enables consistent scoring without reliance on central reading infrastructure, offering a scalable solution that supports both academic centres and community practices. When integrated into electronic health records or decision support platforms, these tools have the potential to enhance therapeutic decision-making and align care with evolving IBD management guidelines.
BARRIERS TO IMPLEMENTATION
Several barriers to widespread clinical implementation remain. Most AI systems have been developed using curated datasets with high-quality inputs, which may not reflect the variability encountered in routine practice. The reliance on expertannotated training data is labour-intensive and limits scalability. Additionally, model performance often declines with suboptimal video quality, poor bowel preparation, or varying equipment, which highlights the need for robust validation across diverse clinical settings.4,8 A further limitation lies in differentiating UC from other forms of colitis, such as infectious, ischaemic, Crohn’s, or drug-induced colitis. Most AI tools are optimised for activity scoring rather than diagnostic classification, which may reduce their performance in nuanced or atypical cases. Finally, integration into real-world workflows requires solving logistical and regulatory hurdles related to real-time processing, interface design, and
References
1. Schroeder KW et al. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. 1987;317(26):1625-9.
2. Travis SP et al. Developing an instrument to assess the endoscopic severity of ulcerative colitis: the Ulcerative Colitis Endoscopic Index of Severity (UCEIS). Gut. 2012;61(4):535-42.
interpretability. Regulatory approval will be essential, as AI tools must meet safety, accuracy, and transparency standards set by regulatory bodies before widespread clinical adoption.
CONCLUSION
AI has rapidly evolved as a promising tool for standardising endoscopic assessment in UC. From early, static image-based models through convolutional networks, to advanced video-based systems with transformers and self-supervised learning, AI has learned from unlabelled data and now aligns closely with expert central readers. These advancements are reshaping how endoscopic data are interpreted, enabling more reproducible and granular evaluations than traditional indices like MES or UCEIS. Yet, these advancements do not replace human expertise. Hybrid human-AI models will be essential, ensuring AI supports clinical decision-making rather than replacing it.
Looking ahead, as more advanced and validated tools become more integrated into clinical infrastructure, AI is poised not only to transform clinical trials but also to influence everyday practice. Future directions include prospective validation trials, regulatory qualification for clinical use, and seamless integration into practice. Real-time, AI-supported scoring could offer consistent, objective evaluations across practice settings, supporting treat-to-target strategies and enabling more personalised, data-driven care for patients with UC.
3. Mohammed Vashist N et al. Endoscopic scoring indices for evaluation of disease activity in ulcerative colitis. Cochrane Database Syst Rev. 2018;1(1):CD011450.
4. Murino A, Rimondi A. Automated artificial intelligence scoring systems for the endoscopic assessment of ulcerative colitis: how far are we from clinical application? Gastrointest Endosc. 2023;97(2):347-9.
5. Kim B et al. Endoscopic and histological patchiness in treated ulcerative colitis. Am J Gastroenterol. 1999;94(11):3258-62.
6. Hashash JG et al. Inter- and intraobserver variability on endoscopic scoring systems in Crohn’s disease and ulcerative colitis: a systematic review and meta-analysis. Inflamm Bowel Dis. 2024;30(11):2217-26.
7. Osada T et al. Comparison of several activity indices for the evaluation of
endoscopic activity in UC: inter- and intraobserver consistency. Inflamm Bowel Dis. 2010;16(2):192-7.
8. Lee MCM et al. Artificial intelligence for classification of endoscopic severity of inflammatory bowel disease: a systematic review and critical appraisal. Inflamm Bowel Dis. 2025;31(8):2296-310.
9. Gecse KB et al. DOP098 AI tool distinguishes differences in endoscopic disease activity in ulcerative colitis where humans could not: data from the TITRATE trial. J Crohn's Colitis. 2025;20(Suppl 1):jjaf231.135.
10. Stidham RW et al. Performance of a deep learning model vs human reviewers in grading endoscopic disease severity of patients with ulcerative colitis. JAMA Netw Open. 2019;2(5):e193963.
11. Takenaka K et al. Development and validation of a deep neural network for accurate evaluation of
endoscopic images from patients with ulcerative colitis. Gastroenterology. 2020;158(8):2150-7.
12. Gottlieb K et al. Central reading of ulcerative colitis clinical trial videos using neural networks. Gastroenterology. 2021;160(3):710-9.e2.
13. Yao H et al. Fully automated endoscopic disease activity assessment in ulcerative colitis. Gastrointest Endosc. 2021;93(3):728-36.e1.
14. Fan Y et al. Novel deep learning-based computer-aided diagnosis system for predicting inflammatory activity in ulcerative colitis. Gastrointest Endosc. 2023;97(2):335-46.
15. Byrne MF et al. Application of deep learning models to improve ulcerative colitis endoscopic disease activity scoring under multiple scoring systems. J Crohns Colitis. 2023;17(4):463-71.
16. Chaitanya K et al. Arges: spatiotemporal transformer for ulcerative colitis severity assessment in endoscopy videos. arXiv. 2024;DOI:10.48550/arXiv.2410.00536.
17. Gutierrez-Becker B et al. Ulcerative colitis severity classification and localized extent (UC-SCALE): an artificial intelligence scoring system for a spatial assessment of disease severity in ulcerative colitis. J Crohns Colitis. 2025;19(1):jjae187.
18. Stidham RW et al. Using computer vision to improve endoscopic disease quantification in therapeutic clinical trials of ulcerative colitis. Gastroenterology. 2024;166(1):155-67.e2.
19. Byrne M et al. Development and validation of a novel AI-based computer vision solution for ulcerative colitis severity scoring on video for real world using high-volume expertannotated video frames. UEG Journal. 2025;13(Suppl 8):704.
Why Point of Care Ultrasound Is More than the Modern Rheumatologist’s Stethoscope
Editor's Pick
This article explores why point of care ultrasound has become far more than a symbolic extension of the rheumatologist’s stethoscope. Detailing its role in early detection of inflammatory arthritis, first-line assessment of giant cell arteritis, and guidance of intra-articular injections, the authors demonstrate how point of care ultrasound strengthens diagnostic precision and supports faster, more informed treatment decisions in everyday clinical practice.
Authors: Jeanette Tan,1 *Qasim Akram2
1. Department of Rheumatology, Sheffield Teaching Hospitals, UK
2. Department of Rheumatology, EULAR Centre of Imaging, Stockport NHS Foundation Trust, UK
*Correspondence to qasim.akram.qa@gmail.com
Disclosure: Akram has received consulting fees from UCB, Novartis, ADDARC, Esaote, and Cingal; and support for attending meetings and/or travel from UCB, Novartis, and Nordimet. Tan has declared no conflicts of interest.
Point of care ultrasound (POCUS) imaging is a valuable tool in assisting clinicians to assess and manage patients in the acute and elective care environment. In modern rheumatology practice, POCUS has been increasingly used due to its effective role in identifying signs of acute inflammation, particularly with the use of power Doppler signals. There is growing evidence to support the utility of ultrasound (US) in the early and accurate diagnosis of inflammatory arthritis. This can prompt early initiation or escalation of disease-modifying treatment. It can also help to explain non-response to ongoing treatment and rule out other causes of joint symptoms.
The role of US in diagnosing giant cell arteritis, particularly with the ‘halo sign’, is wellrecognised as the first-line investigation modality due its non-invasive and quick-access features in comparison to temporal artery biopsy.
US can also enhance the precision of intra-articular steroid injections. Acknowledging that there can be discrepancies in the use of US in real-life clinical practice, due to reliance on operator dependence and interpretation of findings, the Outcome Measures in Rheumatology
(OMERACT) Ultrasound Working Group have agreed on standardised definitions and scoring symptoms for pathophysiological manifestations in rheumatic diseases.
Further research is needed to improve understanding of the predictive role of US assessment in treat-to-target strategies and in the follow-up of patients, particularly in psoriatic arthritis. It is the authors’ hope that modern rheumatologists will increasingly integrate POCUS as a complementary diagnostic and interventional tool in clinical practice to improve patient outcomes.
Key Points
1. Point of care ultrasound (POCUS) is an important tool for the modern rheumatologist and can be used in daily practice and by the bedside.
2. POCUS enhances diagnostic capability for the practising rheumatologist, enabling quicker treatment decisions.
3. POCUS can be used in a variety of rheumatological diseases ranging from inflammatory arthritis to giant cell arteritis/large vessel vasculitis.
INTRODUCTION
Ultrasound (US) is a very helpful clinical tool in rheumatology due to its low cost, portability, and accessibility for point of care US (POCUS), and it is deemed to be the modern-day rheumatologist’s stethoscope.1,2 It is non-invasive and safe for patients due to the lack of ionising radiation, which enables repeated assessments if needed.
A stethoscope was originally designed to auscultate patients’ cardiovascular and respiratory systems, which is particularly relevant in rheumatology when reviewing patients with extra-articular manifestations of rheumatological conditions, such as interstitial lung disease. However, it has many limitations, including a lack of visualisation of underlying structures and, as a result, possible misinterpretation of pathological disease states.
POCUS, in appropriately skilled hands, offers a more dynamic and accurate assessment of structures in motion, and modalities such as power or colour Doppler can depict blood flow in active disease states and provide live information, which is helpful when making advanced treatment decisions.1 Furthermore, musculoskeletal US (MSUS) can be used to clarify any discrepancy between patient-reported symptoms and a clinician’s assessment.
US improves the detection of extra-synovial pathologies, such as tenosynovitis, and thickened pulleys that may be challenging to clinically assess, and helps avoid over or under estimation of clinical synovitis.3,4 MSUS can help clinicians investigate reasons for a lack of treatment response by identifying any ongoing inflammation or other joint issues to explain the patient’s ongoing symptoms. In patients who struggle with treatment compliance, visualisation of their joints and disease status via US in ‘real time’ can facilitate discussions on consequences of a lack of treatment.5 Therefore, due to its powerful diagnostic and interventional utility, it is more than a stethoscope. POCUS in rheumatology practice lends itself well to being incorporated as part of an early inflammatory arthritis disease monitoring clinic and giant cell arteritis (GCA) Fast Track clinics.
There are several limitations to using MSUS that have to be considered. Deeper structures such as the hips are difficult to image accurately. Image resolution is reduced and power Doppler (PD) signal may be undetectable, making it difficult to assess pathology correctly. It is not useful in assessing axial manifestations of spondyloarthritis,6 and MRI, CT, or X-ray are the preferred imaging modalities in this context.
Table 1: Common features on ultrasound based on Outcome Measures in Rheumatology.7
Synovitis
Tenosynovitis
Erosions
Osteophytes
Enthesitis
Gout (double contour sign)
Presence of hypoechoic synovial hypertrophy regardless of effusion or any grade of Doppler signal.
Abnormal anechoic and/or hypoechoic tendon sheath widening, which can be due to presence of abnormal fluid and/or hypertrophy.
Intra-articular and/or extra-articular discontinuity of bone surface (on two perpendicular planes).
Step-up bony prominence at margins of bone (on two perpendicular planes).
Hypoechoic (lack of homogenous fibrillar pattern and loss of tightly packed echogenic lines after correcting for anisotropy) and/or thickened insertion of tendon close to bone (<2 mm from cortex) with Doppler signal if active; may show erosions, enthesophytes, or calcification if damaged.
Abnormal hyperechoic band over superficial margin of articular hyaline cartilage, independent of angle of insonation; can be irregular or regular, continuous or intermittent, and distinguished from cartilage interface sign.
Gout (tophi) Circumscribed, inhomogeneous, hyperechoic (and/or hypoechoic aggregation), may be surrounded by small anechoic rim.
MSUS is highly operator dependent, which can cause variable quality and interpretation of images obtained.1 Standardisation of scanning protocols and definitions of pathological findings in rheumatological conditions (Table 1), alongside high-quality training of sonographers, are crucial to reduce discrepancies of MSUS reports.7,8 Operator-dependent influences of acquiring and interpreting the images can provide the highest rate of error when assessing for synovitis. This could be due to the standard and type of machine that is used (high end versus handheld, for example), greyscale (GS) and Doppler settings, as well as the lack of use of a standardised approach.8 To minimise this, significant training time is required. With this in mind, the European Alliance of Associations for Rheumatology (EULAR) Outcome Measures in Rheumatology (OMERACT) US task force have developed a highly reliable, standardised, international, and consensusbased rheumatoid arthritis (RA) US synovitis scoring system in the development of US as an outcome measurement tool for joint inflammation assessment in patients with RA. This scoring system evaluates GS and PD using semi-quantitative scoring (0–3), along with a combined score.8 The combined score provides a severity grading score. The application of the proposed EULAR-OMERACT score, as well as a standardised scanning approach for synovitis in RA, can improve the intraobserver reliability both in clinical trials
and routine care.8 Further work is also needed on the optimal number and type of joints that can be examined to evaluate for inflammatory arthritis in a POCUS setting. This, however, remains a major challenge in the wider uptake of US in routine practice. Others include the length of time to train as a competent practitioner, a lack of suitable trainers and training centres, and availability and accessibility to high end US systems.
HOW USEFUL IS ULTRASOUND IN RHEUMATOLOGY PRACTICE?
US can be useful in the RA continuum, as extensively shown in a review by Di Matteo et al.9 For those who are at risk of RA (positive or negative autoantibodies with musculoskeletal symptoms but without clinical synovitis, i.e., subclinical synovitis), US can help to detect subclinical inflammation and/or joint damage (erosive disease) to guide prediction of developing inflammatory arthritis, and provides risk stratification for initiating disease-modifying antirheumatic drugs or biological treatment. Early detection and subsequent treatment in the apparent ‘window of opportunity’ has shown to positively improve disease outcomes and is the basis of Early Inflammatory Arthritis clinics.
In undifferentiated arthritis, US can help differentiate the development of RA or other types of inflammatory arthritis, such as
psoriatic arthritis (PsA). This is supported by various studies, such as in Gutierrez et al.,10 whereby US showed inflammation at the peritenon finger extensor tendon of metacarpophalangeal joints (Figure 1) in a majority of patients with PsA, but in none with RA. Furthermore, Zabotti et al.11 has shown that the detection of one or more extra-synovial US feature provided a sensitivity of 68.0% and a high specificity of 88.1% in diagnosing PsA compared to RA. Extra-synovial changes tend to be more specific for PsA. In addition to peritendinous inflammation, this includes dermal soft tissue oedema, enthesopathy at deep flexor tendon insertion on the distal phalanx, capsular enthesophytes, juxta-articular periosteal reaction, metacarpophalangeal peri-extensor tenonitis. and thickening of the finger pulleys.
US can accurately detect unique findings in crystal arthropathies such as the double contour sign or gouty tophi (Figure 2). In patients with polymyalgia rheumatica, bilateral subacromial subdeltoid bursitis, long head biceps tendon tenosynovitis, trochanteric bursitis, and glenohumeral
or hip joint effusions are typically seen on MSUS. It can also be helpful in diagnosing patients presenting with non-inflammatory joint conditions such as osteoarthritis, fibromyalgia syndrome, and tendinopathies.
Additionally, in patients with established RA, POCUS can be used as an extension to clinical examination by monitoring response to therapy and/or helping clinicians to reconsider the primary diagnosis and ongoing management. It is also useful for patients who develop new symptoms as to whether they are related to active disease or non-inflammatory causes. It can help monitor progression of any structural damage, i.e., joint erosions (Figure 2), and/or disease relapse after tapering of treatment.9
US is effective in the diagnosis of GCA and is recommended as the first-line imaging modality by the EULAR Large Vessel Vasculitis guidelines.12 Integration of US as part of a Fast Track Pathway (GCA) enables a rapid diagnosis of GCA and subsequent treatment. A service evaluation of Fast Track GCA clinics by Kamperidis
Figure 1: Pathological ultrasound in rheumatology.
et al.13 showed that out of 94% of patients scanned, 30% were diagnosed with GCA, which enabled prompt and appropriate steroid-weaning regimens in confirmed cases and discontinuation of steroids in excluded cases. This consequently reduced the demand for outpatient clinics, theatre slots, and staff for temporal artery biopsy and, more crucially, minimised complications of GCA such as blindness or prolonged steroid treatment.
Furthermore, US can help in the accurate placement of steroid needle injections, avoid complications, and possibly improve short-term outcomes.14
BASICS OF ULTRASOUND
US images are formed by a transducer emitting and receiving high-frequency sound waves. The waves generated by the transducer transform electrical potentials into mechanical vibrations, and vice versa. They travel through different densities of tissues, and the transducer receives reflected echoes, which are converted to computer images displayed as GS.1 US gel is used as coupling medium to improve US pulse penetration, as it has similar impedance to human tissue.15
B (brightness/GS) mode frequency is first optimised based on the target structure’s depth and any soft tissue features. This provides morphological information of the anatomical site. For example, if thickened tissue (high impedance) overlies structure, such as in psoriasis, lower frequency enables better sound penetration. B mode gain can then be adjusted for brightness of returning echoes.1
There are two main modes of Doppler imaging (which displays blood flow), including PD and colour Doppler, which allows for the evaluation of blood flow based on the reflection of sound waves (due to movement of red blood cells). PD mode is especially useful in rheumatologic MSUS as it integrates all Doppler signals, regardless of direction, and detects slow blood flow. Detection of increased blood flow by Doppler is an indirect sign of inflammation in structures such as joints, tendons or enthesis, or even erosions. Echogenicity (displayed as brightness) differentiates structures based on the proportion of waves reflected in comparison to subdermal fat (Table 2).
Figure 2: Pathological ultrasound in rheumatology including giant cell arteritis.
Table 2: Differences in echogenicity representing various structures in musculoskeletal ultrasound.1
Hyperechoic Increased reflection (appears white) such as in skin, bone, and tendon (fibrillar pattern in longitudinal view).
Hypoechoic Less reflection (appears grey) such as in synovial proliferation and nerves.
Anechoic No or very minimal reflection (appears black) such as in synovial fluid and blood vessels.
For rheumatological practice, linear transducers are often used to cover medium and higher frequencies. Usually, frequencies between 5–20 MHz are used in rheumatology settings, so more than one probe is usually needed in clinical practice.15 Higher frequency probes enhance image resolution but decrease wave penetration to allow assessment of small joints and superficial entheses or tendons such as finger joints and wrists, whereby linear and/or hockey probes are recommended. Lower frequency probes are preferred for examining deeper structures such as the hip, whereby linear and/or curved probes are recommended.16
ULTRASOUND IN RHEUMATOID ARTHRITIS
Several studies have shown that, although only a minority of ‘at-risk’ individuals have US changes (high score of GS and PD findings) at baseline, these findings are significantly predictive of progression to RA.17 In a study by van der Ven M et al.,18 patients with arthralgia but no synovitis on MSUS had a high negative predictive value for development of inflammatory arthritis over a year. In the ESPOIR cohort, MSUS identified erosions in those with early arthritis, which predicted radiographic erosions 2 years on.19 These patients can be risk stratified to more aggressive treatment.
In patients with sustained remission, studies have found that both MSUS findings of synovitis (including Doppler activity; Figure 2) and hypertrophy may be predictive of unsuccessful tapering or cessation of treatment.20,21
US has shown to be useful in monitoring treatment-related changes to synovitis
and tenosynovitis, including monitoring response to disease-modifying antirheumatic drugs, biologics, or topical treatment (intra-articular injections). It can help in those patients not responding to treatment and those with long-standing disease with new symptoms, i.e., either progressive joint damage, new inflammatory disease, or non-inflammatory sequelae of primary disease.
Several studies have shown that some patients with RA who are in clinical remission do not achieve good functional outcomes and show progression of radiographic disease. This may be due to persistent subclinical synovitis, and US could help identify this.1 Those in remission with subclinical synovitis are at higher risk of disease flare. However, while subclinical inflammation can be seen in up to approximately 90% of patients with RA in remission, only a minority will have flares or radiographic progression. Therefore, the clinical significance of subclinical synovitis remains unclear, especially in the long term. At the same time, in a patient who is symptomatic, a completely normal MSUS without concerning GS or PD findings can be reassuring and prevent over-treatment.1
Using a treat-to-target (T2T) approach has good evidence for the best outcomes in RA, but it remains to be proven whether clinical remission or radiographic remission using US is sufficient. Two large RCTs, TASER and ARCTIC, have demonstrated that a treatment strategy based on US assessment did not lead to an improved clinical outcome in comparison with a conventional clinical T2T approach. Patients in the US tight control group were overtreated without any significant clinical improvement, although radiographic structural progression was reduced.
These studies may have been underpowered to show a true difference between the groups, and they did have some other methodological flaws: for example, there was a lack of wrist assessment in the TASER study and the sonographer was also the treating physician in the ARCTIC study, which could impact the results, but these do highlight that further studies are needed in this regard.22,23
Ultrasound in Psoriatic Arthritis
US can detect subclinical elementary lesions that may help diagnose PsA, especially in patients with psoriasis. MSUS was used in a study by Elnady et al.,24 which showed that in patients with psoriasis, there was a higher prevalence of baseline enthesitis and PD scores in those who developed PsA compared to those who did not.24 MSUS has also improved specificity from 54.4% to 90.4% in screening for early PsA in 140 patients with psoriasis and arthralgia, and no longer suspected in 45 out of 46 PsA patients.25 Koppikar et al.1 found that over 25% of patients with musculoskeletal complaints, but no prior diagnosis of PsA, had at least two joints with sonographic inflammation.1
Currently, there is insufficient evidence to prove the utility of MSUS in the disease monitoring of PsA, but there has been a study by Ruta et al.26 showing PD evidence of subclinical synovitis as a predictor of PsA flare at 6 months in those who are in clinical remission. A study of patients with PsA in remission showed residual US subclinical inflammation in peripheral tissues; a joint or enthesis positive PD signal was found in about 19% and 24% of patients, respectively.1
Ultrasound in Crystal Arthritis
US can be used to differentiate between urate deposition and chondrocalcinosis in crystal arthritis. Calcium pyrophosphate crystals tend to localise within the cartilage and show up as hyperechoic dots or lines, the so called ‘rose beading’ sign (Figure 2),27 and are noted to be reliable findings in the knee, wrist, and acromioclavicular joint.28 Monosodium urate crystals localise either at the interface between cartilage and synovium (as a double contour sign),
in the synovium (as micro-calculi), or in the soft tissue/tendon around the joint, and also show up as hyperechoic.29
With regard to disease monitoring, a study by Peiteado et al.30 showed that US is sensitive in assessing response to urate-lowering therapy, but there was still persistent tophi burden at 2 years despite clinical control.
Ultrasound in Osteoarthritis
Typical US features of osteoarthritis are osteophytes, which appear as a hyperechoic shadow (Figure 1), usually with cartilage changes or disappearance and/or synovitis. US is found to be more sensitive (up to eight times more) than plain radiography to delineate osteophytes in smaller joints, such as finger joints, that are localised dorsally.31
Ultrasound-Guided Procedures
Multiple RCTs in inflammatory arthritis have shown better accuracy in using US, which can reduce complications of procedure, to guide joint injections, but no short-term benefits as improvement was only seen in 6 weeks.32,33 However, in a larger RCT of 244 patients with inflammatory arthritis, there were better patient-reported outcomes of 81% reduction in injection pain, and 38% increase in responder rate.34
Gutierrez et al.10 showed similar improvements in functional, clinical, and US scores by using MSUS guidance over the palpation-guided approach in patients with chronic inflammatory arthritis and tenosynovitis. There seems to be a clear benefit of targeting pathologically active joints through MSUS assessment before the guided injection, as treatment efficacy was observed in moderate PD synovitis.35
Ultrasound in Sjögren’s Syndrome
US also has its role in the diagnosis of connective tissue conditions such as Sjögren’s syndrome. US features such as inhomogeneous and hypoechoic structures in submandibular and parotid glands are indicative of Sjögren’s. Other pertinent US findings for Sjögren’s include atrophic
submandibular glands with sagittal diameter <0.8 cm and enlarged parotids with diameter >2 cm. There is a 63% sensitivity and 99% specificity for diagnosis of Sjögren’s based on international classification criteria, if two or more of the four glands show this pathological pattern.36
Ultrasound in Giant Cell Arteritis
US displays homogenous, hypoechoic circumferential wall thickening (halo sign; Figure 1) with possible features of stenoses or acute occlusions in GCA.37 Use of Doppler US of temporal arteries has shown a sensitivity of 85% and specificities of more than 95% in various studies to diagnose GCA.38 In addition, axillary arteries can be easily examined using US and are found to be more commonly affected in GCA than previously expected.39
The extent of vascular inflammation can be quantified based on halo count (number of temporal artery segments and axillary arteries with a halo sign, ranging from 0–8) and halo score (composite index that incorporates both the number of halos and maximum halo thickness in each region, ranging from 0–48). The combination of halo count and halo score has been shown to support a diagnosis of GCA40 in routine care as they correlate with raised laboratory markers of inflammation and may have a role in monitoring disease activity, especially with the availability of newer biologic treatments.
CONCLUSION
POCUS can be a useful adjunct in facilitating early, confident diagnosis of inflammatory arthritis, and has a role in predicting disease flares and progression, which leads to timely and effective treatment to enhance patient outcomes. In patients with a lack of response to treatment of inflammatory arthritis, US can be used to confirm or refute subclinical inflammation, support patient education with medication compliance, and facilitate shared decision-making on treatment escalation if appropriate.
US can also help to eliminate other causes of musculoskeletal symptoms to avoid misdiagnosis and treatment. There are some limitations in using US, such as operatordependence, training issues, and a lack of agreement on the number of joints and tendons to include for scoring of disease activity. Further research is also warranted to define its role in the follow-up of rheumatoid arthritis and psoriatic arthritis, especially in T2T strategies.
US has also been proven to be a vital diagnostic tool for other rheumatological conditions such as GCA and Sjögren’s syndrome. It can also be used to guide intra-articular steroid injections for precision and response as a common procedure in the management of patients with inflammatory arthritis.
Overall, integrating POCUS into the rheumatology clinic is proving to be more than a modern rheumatologist’s stethoscope as, in trained hands, it can enhance efficiency by reducing clinic visits, improve patients’ education of disease management, and improve patient outcomes.
References
1. Koppikar S et al. Seeing is believing: smart use of musculoskeletal ultrasound in rheumatology practice. Best Pract Res Clin Rheumatol. 2023;37(1):101850.
2. Shriki J. Ultrasound physics. Crit Care Clin. 2014;30(1):1-24.
3. Gazel U et al. Accuracy of physical examination to detect synovial and extra-synovial pathologies in psoriatic arthritis in comparison to ultrasonography. J Clin Med. 2020;9(9):2929.
4. Saku A et al. Experience of musculoskeletal ultrasound scanning improves physicians' physical examination skills in assessment of synovitis. Clin Rheumatol. 2020;39:1091-9.
5. Tan YK et al. A musculoskeletal ultrasound program as an intervention to improve disease modifying antirheumatic drugs adherence in rheumatoid arthritis: a randomized controlled trial. Scand J Rheumatol. 2022;51:1-9.
6. Mandl P et al. EULAR recommendations for the use of imaging in the diagnosis and management of spondyloarthritis
in clinical practice. Ann Rheum Dis. 2015;74:1327-39.
7. Bruyn GA et al. OMERACT definitions for ultrasonographic pathologies and elementary lesions of rheumatic disorders 15 years on. J Rheumatol. 2019;46:1388-93.
8. Moller I et al. The 2017 EULAR standardised procedures for ultrasound imaging in rheumatology. Ann Rheum Dis. 2017;76:1974-9.
9. Di Matteo A et al. The role of musculoskeletal ultrasound in the rheumatoid arthritis continuum. Curr Rheumatol Rep. 2020;22(8):41.
10. Gutierrez M et al. Differential diagnosis between rheumatoid arthritis and psoriatic arthritis: the value of ultrasound findings at metacarpophalangeal joints level. Ann Rheum Dis. 2011;70:1111-4.
11. Zabotti A et al. Early psoriatic arthritis versus early seronegative rheumatoid arthritis: role of dermoscopy combined with ultrasonography for differential diagnosis. J Rheumatol. 2018;45: 648-54.
12. Dejaco C et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice: 2023 update. Ann Rheum Dis. 2024;83:741-51.
13. Kamperidis P et al. E043 Fast track giant cell arteritis service in a district general hospital using ultrasound doppler imaging. Rheumatology. 2024;63(1):keae163.271.
14. Dejaco C et al. EULAR points to consider for the use of imaging to guide interventional procedures in patients with rheumatic and musculoskeletal diseases (RMDs). Ann Rheum Dis. 2022;81:760-7.
15. Schmidt WA, Backhaus M. What the practising rheumatologist needs to know about the technical fundamentals of ultrasonography. Best Pract Res Clin Rheumatol. 2008;22(6):981-99.
16. Canadian Rheumatology Ultrasound Society (CRUS). The CRUS ultrasonography guide. 2020. Available at: https://crus-surc.ca/wp-content/ uploads/2020/06/CRUS-ebookvolume-1-June-12-2020-.pdf. Last accessed: 6 June 2025.
17. Di Matteo A et al. What is the value of ultrasound in individuals “at-risk” of rheumatoid arthritis who do not have clinical synovitis? Healthcare. 2021;9(6):752.
18. Van der Ven M et al. Absence of ultrasound inflammation in patients presenting with arthralgia rules out the development of arthritis. Arthritis Res Ther. 2017;19(1):202.
19. Funck-Brentano T et al. Prediction of radiographic damage in early arthritis by sonographic erosions and power Doppler signal: a longitudinal observational study. Arthritis Care Res. 2013;65(6):896-902.
20. Naredo E et al. Predictive value of Doppler ultrasound-detected synovitis in relation to failed tapering of biologic therapy in patients with rheumatoid arthritis. Rheumatology (Oxford). 2015;54(8):1408-14.
21. Valor L et al. Identifying markers of sustained remission in rheumatoid arthritis patients on long-term tapered biological disease-modifying antirheumatic drugs. Rheumatol Int. 2018;38(8):1465-70.
22. Dale J et al. Targeting ultrasound remission in early rheumatoid arthritis: the results of the TaSER study, a randomised clinical trial. Ann Rheum Dis. 2016;75(6):1043-50.
23. Haavardsholm EA et al. Ultrasound in management of rheumatoid arthritis: ARCTIC randomised controlled strategy trial. BMJ. 2016;354:i4205.
24. Elnady B et al. Subclinical synovitis and enthesitis in psoriasis patients and controls by ultrasonography in Saudi Arabia; incidence of psoriatic arthritis during two years. Clin Rheumatol. 2019;38(6):1627-35.
25. Grobelski J et al. Prospective double-blind study on the value of musculoskeletal ultrasound by dermatologists as a screening instrument for psoriatic arthritis. Rheumatology (Oxford). 2023;62(8):2724-31.
26. Ruta S et al. Utility of power Doppler ultrasound-detected synovitis for the prediction of short-term flare in psoriatic patients with arthritis in clinical remission. J Rheumatol. 2017;44(7):1018-23.
27. Filippou G et al. A “new” technique for the diagnosis of chondrocalcinosis of the knee: sensitivity and specificity of high-frequency ultrasonography. Ann Rheum Dis. 2007;66(8):1126-8.
28. Filippou G et al. Definition and reliability assessment of elementary ultrasonographic findings in calcium pyrophosphate deposition disease: a study by the OMERACT calcium pyrophosphate deposition disease ultrasound subtask force. J Rheumatol. 2017;44(11):1744-9.
29. Thiele RG, Schlesinger N. Diagnosis of gout by ultrasound. Rheumatology (Oxford). 2007;46(7):1116-21.
30. Peiteado D et al. Ultrasound sensitivity to changes in gout: a longitudinal study after two years of treatment. Clin Exp Rheumatol. 2017;35(5):746-51.
31. Keen HI et al. Can ultrasonography improve on radiographic assessment in osteoarthritis of the hands? A comparison between radiographic and ultrasonographic detected pathology. Ann Rheum Dis. 2008;67(8):1116-20.
32. Nordberg LB et al. The impact of ultrasound on the use and efficacy of intraarticular glucocorticoid injections in early rheumatoid arthritis: secondary analyses from a randomized trial examining the benefit of ultrasound in a clinical tight control regimen. Arthritis Rheumatol. 2018;70(8):1192-9.
33. Cunnington J et al. A randomized, double-blind, controlled study of ultrasound-guided corticosteroid injection into the joint of patients with inflammatory arthritis. Arthritis Rheum. 2010;62(7):1862-9.
34. Sibbitt WL Jr et al. A randomized controlled trial of the costeffectiveness of ultrasound guided intraarticular injection of inflammatory arthritis. J Rheumatol. 2011;38(2): 252-63.
35. Gutierrez M et al. Short-term efficacy to conventional blind injection versus ultrasound-guided injection of local corticosteroids in tenosynovitis in patients with inflammatory chronic arthritis: a randomized comparative study. Joint Bone Spine. 2016;83(2):161-6.
36. Wernicke D et al. Ultrasonography of salivary glands -- a highly specific imaging procedure for diagnosis of Sjögren's syndrome. J Rheumatol. 2008;35(2):285-93.
37. Schmidt WA et al. Color duplex ultrasonography in the diagnosis of temporal arteritis. N Engl J Med. 1997;337(19):1336-42.
38. Karassa FB et al. Meta-analysis: test performance of ultrasonography for giant-cell arteritis. Ann Intern Med. 2005;142(5):359-69.
39. Schmidt WA et al. Ultrasound of proximal upper extremity arteries to increase the diagnostic yield in largevessel giant cell arteritis. Rheumatology (Oxford). 2008;47(1):96-101.
40. Molina Collada J et al. Diagnostic value of ultrasound halo count and Halo Score in giant cell arteritis: a retrospective study from routine care. Ann Rheum Dis. 2022;81(9):e175.
Emerging Immunological Pathways in SLE: Immune Trafficking and S1PR1 Modulation as Therapeutic Strategies
Support: The publication of this independently commissioned article was funded through a grant by Viatris.
Authors: *Anca D. Askanase,1 Nathalie Burg,2 Guillermo Valenzuela3
1. Columbia University Lupus Center, Division of Rheumatology, Columbia University College of Physicians & Surgeons, New York, USA
2. Hospital for Special Surgery, New York, USA
3. Integral Rheumatology and Immunology Specialists, Plantation, Florida, USA
*Correspondence to ada20@cumc.columbia.edu
Disclosure: Valenzuela has received grants and/or research support from Mallinckrodt and Artiva Biotherapeutics; speaker fees from Lilly, Amgen, UCB, Pfizer, Genentech, Novartis, BMS, Takeda, Janssen, Centocor, Celgene, Pharmacia, Horizon, Mallinkrodt, Radius, AbbVie, Sanofi, Regeneron, Boehringer Ingelheim, AstraZeneca, Theramex, and Artiva Biotherapeutics; and acted as a consultant for Merck, Lilly, Amgen, Esaote, Sanofi, UCB, Janssen, Horizon, Image Analysis Group, Novartis, Pfizer, Alexion, Genentech, Celgene, Regeneron, AbbVie, Boehringer Ingelheim, Sandoz, Gilead, Exagen, Global Health Living, and Artiva Biotherapeutics. Askanase has been an investigator/consultant for Abbvie, Amgen, AstraZeneca, Aurinia, Biogen, BMS, Cabaletta, Celgene, Eli Lilly, Idorsia, Janssen, Genentech, GSK, Janssen, Mallinckrodt, NKARTA, Pfizer, Sana, Sanofi, and UCB. Burg has served on an advisory board for Viatris.
Acknowledgements: Writing assistance was provided by Rachel Danks, RSD Medical Communications Ltd, Gloucestershire, UK.
Erratum: This article was first published on 5th March 2026. An erratum has since been issued and can be viewed here.
Abstract
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder characterised by loss of immune tolerance, widespread inflammation across multiple organs, and unpredictable flares, which lead to irreversible damage over time. Treat-to-target strategies and guideline-based care recommend treatment with hydroxychloroquine, glucocorticoids, immunosuppressants, and targeted biologics. However, despite these treatments, many patients continue to experience ongoing disease activity and treatment-related toxicities.
PHARMA PARTNERSHIP
This article summarises key immune pathways driving SLE pathogenesis, including nucleic-acid sensing, Type I interferon (IFN) amplification, immune-complex/complementmediated injury, and neutrophil extracellular trap (NET)-related inflammation. It also highlights immune trafficking and spatial organisation as determinants of organ involvement, focusing on chemokine networks and the sphingosine-1-phosphate–sphingosine-1-phosphate receptor (S1P–S1PR) axis as upstream regulators of immune localisation. Building on this rationale, S1PR1 modulation is discussed as an emerging therapeutic strategy, with studies on cenerimod progressing from proof-of-concept to Phase III trials. While multiple immune pathways are reviewed to reflect the complexity of SLE, particular emphasis is placed on immune trafficking and the S1P–S1PR1 axis as an upstream regulatory pathway under active clinical investigation. This review does not aim to provide an exhaustive catalogue of all emerging therapeutic modalities in SLE, but instead focuses on immune trafficking and spatial immune organisation as upstream regulators of disease.
ONGOING UNMET CLINICAL NEEDS IN SLE
SLE is a chronic autoimmune disease characterised by loss of immune tolerance, multisystem inflammation, and unpredictable flares, resulting in heterogenous organ involvement and long-term damage.1,2 SLE can involve multiple organ systems, including the vasculature, central nervous system, lungs, skin, kidneys, and joints, reflecting its underlying biological heterogeneity.3,4 Patients with SLE typically experience substantial impairment in quality of life, increased morbidity, and premature mortality.1,5 Despite advances in disease monitoring and supportive care, a substantial proportion of patients with SLE continue to experience ongoing disease activity, recurrent flares, and reduced survival.2
Over the last decade, efforts to optimise SLE management have increasingly focused on adopting a treat-to-target approach, in which disease remission is targeted through regular review and sequential treatment adjustment.6,7 Current guidelineinformed management emphasises prompt initiation of treatment aimed at achieving remission or low disease activity in order to prevent flares and organ damage, improve prognosis, and enhance quality of life.2,7,8 In clinical practice, hydroxychloroquine is widely regarded as the cornerstone of therapy, with glucocorticoids used for rapid suppression of disease activity and tapered to the lowest feasible dose.2,8
Immunosuppressive agents, including mycophenolate mofetil, azathioprine, methotrexate, and biological agents are also commonly used to achieve and maintain control, particularly in patients with persistent moderate-to-severe disease (Figure 1).2,8
Although steroids are effective for rapid symptom control in SLE, long-term reliance is associated with cumulative toxicity, infections, metabolic complications, cardiovascular morbidity, osteoporosis, and irreversible damage.9,10 Consequently, achieving effective steroid-sparing disease control without compromising safety remains a central priority for the management of SLE.4,8
Recently approved targeted therapies have expanded treatment options in SLE, particularly through modulation of B cell survival and Type I IFN-driven inflammation.4 However, persistent disease activity and the ongoing burden of treatment-related toxicity highlight the need to broaden therapeutic strategies beyond a limited number of dominant immune pathways.4 Increasing attention has therefore been focused towards upstream and under-recognised mechanisms, including immune cell trafficking and tissue-level regulation, as sources of future therapeutic innovation.11,12 These pathways offer a mechanistic rationale for emerging targeted approaches that intervene earlier in the inflammatory cascade, prior to amplification by downstream cytokine and effector pathways.11,13-15
Figure 1: The European Alliance of Associations for Rheumatology (EULAR) recommendations for the treatment of non-renal SLE (2023 update).8
*Mild disease: constitutional symptoms; mild arthritis; rash ≤9% BSA; PLT: 50–100×109 /L; SLEDAI ≤6; BILAG C or ≤1 BILAG B manifestation.
‡Severe disease: major organ threatening disease (cerebritis, myelitis, pneumonitis, mesenteric vasculitis); thrombocytopenia with platelets <20×109 /L; TTP-like disease or acute haemophagocytic syndrome; rash >18% BSA; SLEDAI >12; ≥1 BILAG A manifestations.
§Recommendation of belimumab and anifrolumab as first-line therapy in severe disease refers to cases of extrarenal SLE with non-major organ involvement, but extensive disease from skin, joints, and so on. The use of anifrolumab as add-on therapy in severe disease refers mainly to severe skin disease. For patients with severe neuropsychiatric disease, anifrolumab and belimumab are not recommended.
Top-to-bottom sequence does not imply order of preference (e.g., MTX, AZA, and MMF are equal options for second-line therapy in mild disease or first-line therapy in moderate disease).
Systemic Immune Dysregulation as the Foundation of SLE Pathogenesis SLE is characterised by chronic activation of innate and adaptive immune pathways.16 This chronic inflammatory state is shaped by defects in immune tolerance, persistent nucleic-acid sensing, and dysregulated cytokine networks that together reinforce autoreactivity and systemic immune imbalance.16-18 A central mechanism involves activation of nucleic-acid sensing pathways, including endosomal Toll-like receptors (TLR7 and TLR9), cytosolic RNA sensors such as retinoic acid-inducible gene I (RIG-I)-like receptors, and inflammasome pathways. These sensing processes promote ongoing production of Type I IFNs, cytokines that contribute to immune activation, antigen presentation, and downstream amplification of inflammation.16,18
In parallel, impaired clearance of apoptotic and necrotic debris increases exposure to nuclear antigens, facilitating immunecomplex formation and propagation of autoantibody-driven inflammation.16,17 Complement deficiencies affecting early classical pathway components, particularly C1q, C2, and C4, are strongly associated with SLE because they impair immune-complex handling and clearance of apoptotic debris, further perpetuating inflammatory signalling and tissue injury.17 Together, these systemic abnormalities create a persistent pro-inflammatory environment in which autoreactive immune responses can be initiated and sustained.
Networks of DNA, histones, and neutrophil proteins, known as NETs, that are implicated in the capture of microbes may also be involved in the pathogenesis of SLE by promoting autoantibody formation and serving as adjuvants.16,17 Finally, environmental influences, including UV radiation, viral infection such as Epstein–Barr virus, and epigenetic dysregulation, may further increase susceptibility to immune activation.3,18
While these systemic abnormalities are necessary for disease initiation, they are insufficient to fully explain the organ specificity, persistence, and relapsing nature of tissue inflammation in SLE, and further pathological mechanisms must also be considered.
Immune Cell Trafficking and Spatial Organisation of Inflammation in SLE
Multisystem involvement in SLE depends not only on immune activation but also on the ability of leukocytes to migrate, localise, and persist within target tissues, where they contribute to chronic damage and functional impairment.13,19 Increasing evidence supports the concept that immune cell trafficking and spatial immune organisation are key determinants of disease expression and organ involvement.20 In this context, chemokine–chemokine receptor networks (e.g., CXCR3, CCR5, and their ligands) regulate tissue-specific immune cell recruitment and retention, contributing to organ-specific inflammation in SLE.20
Alongside chemokine-mediated recruitment, the S1P–S1PR axis represents a complementary regulatory system governing immune cell distribution.13-15,21-23 The S1P chemotactic gradient is a principal determinant of lymphocyte egress from secondary lymphoid organs into the lymphatic and vascular circulation via S1P–S1PR1 receptor engagement on B and T lymphocytes.23 In SLE, dysregulation of the S1P–S1PR axis has been proposed to alter immune cell distribution in ways that sustain both systemic and tissue-specific inflammatory activity, highlighting immune localisation as a key determinant of disease expression (Figure 2).14, 22,23
Among the five known S1PR subtypes (S1PR1–5), S1PR1 is highly expressed on naïve and central memory T cells, B cells, and subsets of dendritic cells, where it plays a dominant role in regulating lymphocyte egress from secondary lymphoid organs along S1P gradients. In contrast, S1PR2 and S1PR3 are more broadly expressed across immune and structural cell types, and may exert distinct or context-dependent effects, including influences on vascular tone and permeability.
Immune system
Inflammation
Lymphocyte egress Dentritic cell secretion Neutrophil infiltration and NETosis Macrophage migration and polarisation Pro-inflammatory cytokines Inflammatory pathway
In SLE, S1P functions as an important mediator by regulating both inflammatory and immune responses. On one hand, S1P plays a detrimental role by interacting with different immune cells. The spatial gradient of S1P drives lymphocytes into the peripheral circulation; thereby blockade of the S1P axis may mitigate the autoimmunity severity of SLE. Moreover, S1P is able to influence the function of innate immune cells, such as dendritic cells, neutrophils, and macrophages. On the other hand, as an inflammation-mediated disease, non-resolving inflammation has been regarded as the main contributor to SLE pathogenesis. Indeed, S1P can accelerate the inflammatory condition, which is likely associated with the crucial role of S1P in regulating pro-inflammatory cytokine secretion and signalling pathway activation.14
Adapted from Tian et al.14
G12/13: G protein alpha subunits 12 and 13; Gαi: inhibitory G protein alpha subunit; Gαq: Gq family G protein alpha subunit; Gαs: stimulatory G protein alpha subunit; IFN: interferon; JAK-STAT: Janus kinase-signal transducer and activator of transcription pathway; NETosis: neutrophil extracellular trap formation; NF-κB: nuclear factor kappa B; PI3K-AKT: phosphoinositide 3-kinase–protein kinase B pathway; S1P: sphingosine-1-phosphate; S1PR: sphingosine-1phosphate receptor; SLE: systemic lupus erythematosus; SPHK: sphingosine kinase.
S1PR signalling may also shape SLE pathology through effects that extend beyond lymphocyte trafficking. In addition to regulating immune cell distribution, S1PR activity in endothelial and other
structural cells can influence tissue-level inflammatory responses by modulating vascular permeability, barrier integrity, and inflammatory cell extravasation.23
Figure 2: S1P signalling in the pathogenesis of SLE.14
Endothelial S1PR1 Signalling and Tissue-Level Immune Regulation
Endothelial S1PR1 is emerging as a key regulator of vascular integrity and immune cell entry into inflamed tissues, with direct relevance to multisystem pathology in SLE.24,25 Through its actions on endothelial barrier stability, S1PR1 limits permeability and regulates leukocyte extravasation, thereby shaping the extent and persistence of tissue inflammation.26
Disruption of endothelial barrier function may contribute directly to organ-specific pathology in SLE by increasing vascular permeability and facilitating inflammatory cell extravasation into target tissues.26 Although S1PR signalling is increasingly recognised in vascular biology as a key pathway supporting endothelial integrity, its relevance to tissue-level inflammation in rheumatic disease remains underappreciated.24-26 In parallel, dysregulated immune trafficking can increase the recruitment and retention of leukocytes at sites of injury.20 Together, aberrant immune localisation and impaired endothelial barrier control create a permissive environment for sustained immune cell-tissue interactions, reinforcing local cytokine signalling and antigen exposure.24,27 These conditions may then enable adaptive immune abnormalities to persist and evolve, driving chronic inflammation and long-term autoimmunity.
In this context, S1PR1 modulation may influence not only systemic lymphocyte redistribution but also tissue-level inflammatory dynamics. By stabilising endothelial barrier integrity and regulating leukocyte extravasation, S1PR1 signalling may limit the intensity and persistence of immune-cell infiltration within target organs.24,25 Although indirect, these effects provide a plausible mechanistic basis by which S1PR1-targeted therapies could attenuate local immune activation in addition to altering circulating lymphocyte numbers.
Endothelial dysfunction in specific SLE conditions, including lupus nephritis, neuropsychiatric SLE, and cutaneous disease, may reflect a shared driver of organ-specific inflammation, mediated
through S1PR1 signalling. Framing S1PR1 as a molecular bridge between systemic immune dysregulation and tissue-specific pathology may therefore help align rheumatology perspectives with those of nephrology and neurology, and support therapeutic strategies aimed at restoring barrier function while simultaneously limiting pathological immune cell recruitment.
Dysregulated Lymphocyte Activation and Adaptive Immune Imbalance
Adaptive immune dysregulation is a hallmark of SLE and is central to autoantibody production, immune-complex formation, and organ injury.16 When B cell tolerance is disrupted, autoreactive B cells escape elimination and become activated, promoting autoantibody production and amplifying chronic inflammation.16,28 B cell activating factor (BAFF)/B lymphocyte stimulator (BlyS) overexpression supports survival and differentiation of autoreactive B cells and contributes to aberrant B cell activation and maturation.16 In addition, hyperactivation of nucleic-acid sensing pathways, including TLR7, can promote nucleic-acid-specific autoantibody production and contribute to plasmablast expansion, reinforcing humoral autoimmunity.16
T cell abnormalities contribute further to disease persistence through dysregulated cytokine production and impaired immune regulation. Expansion of Th17 cells and elevated IL-17 expression have been associated with disease activity and may contribute to neutrophil recruitment and increased inflammatory activity.16,17 Quantitative and functional deficiencies in regulatory T cells represent another pathway by which immune tolerance is impaired in SLE.17 Finally, production of most pathogenic IgG lupus autoantibodies occurs in the context of germinal centre reactions that require T follicular help cell-mediated support.11
Amplification Loops Sustaining
Chronic Inflammation in SLE SLE is characterised by amplification loops that perpetuate inflammation even
when individual pathways are partially suppressed.29 Type I IFN signalling enhances antigen presentation, lymphocyte activation, and cytokine dysregulation, and may contribute to a self-reinforcing environment supporting chronic immune activation.29 Immune complexes and complement activation further reinforce tissue injury and promote recruitment of inflammatory cells, strengthening the persistence of organ inflammation.17,28 NET formation and IFN signalling may also interact to create self-sustaining inflammatory circuits that maintain autoantigen exposure and innate immune activation over time.16,17
These interconnected pathways may help explain why many patients experience persistent disease activity and the limited durability of response to therapies targeting downstream pathways.28 Collectively, therefore, these mechanistic insights underscore the rationale for therapeutic strategies that intervene upstream in immune organisation and trafficking. Specifically, the central role of the S1P–S1PR axis in regulating immune cell distribution provides a mechanistic foundation for clinical approaches targeting S1PR1 in SLE.14,15 Emerging translational and early-phase clinical data demonstrating reductions in IFN-associated biomarkers and autoantibody titres further support the biological plausibility of targeting this pathway.
CLINICAL DEVELOPMENT OF TARGETED THERAPIES IN SLE: FOCUS ON S1PR1 MODULATION
Overview
of
Targeted Therapeutic Strategies in Development
Investigational approaches in SLE are increasingly mechanism-driven, with therapeutic strategies targeting immune activation across multiple levels. These include IFN pathway inhibition, alongside B cell and T cell modulation through targeting B cells and key co-stimulatory pathways.3,9,16,27 Intracellular signalling inhibition is also represented, including kinase-directed approaches under
advanced clinical evaluation.3,9,16,27 In addition, immune trafficking modulation is being explored via therapies targeting the S1P–S1PR1 axis to alter immune cell distribution and localisation.9
In this context, modulation of immune ‘spatial organisation’ has emerged as a conceptually distinct strategy.30 Instead of neutralising a single effector cytokine or depleting a specific immune population, trafficking-based approaches aim to alter the distribution of immune cells across lymphoid compartments, circulation, and peripheral tissues.30 This mechanistic strategy is supported by increasing evidence that immune cell localisation and persistence within target tissues influence organ involvement and flare dynamics in SLE.31-34
S1PR modulators are particularly notable because they target a pathway that regulates lymphocyte trafficking, thereby preventing them from migrating to sites of inflammation.35 Consequently, S1PR1 modulation provides a rational bridge between upstream immune organisation and downstream inflammatory outcomes in SLE.
Cenerimod: Mechanistic Rationale
Cenerimod is an oral S1PR modulator developed as a selective S1PR1 modulator for use in SLE.36 Its selectivity for S1PR1 (with activity at S1PR5) is intended to preferentially modulate lymphocyte trafficking while minimising S1PR3associated cardiovascular effects observed with less selective S1PR modulators. In principle, S1PR1 modulation can reduce pathogenic lymphocyte recirculation by limiting lymphocyte egress from secondary lymphoid organs, thereby reducing the availability of circulating autoreactive lymphocytes that can enter tissues and sustain inflammatory responses.37 This mechanism offers wider immune modulation affecting many types of lymphocytes rather than the modulation of a single cytokine.
A key mechanistic advantage of this approach is that it alters immune cell distribution rather than directly eliminating immune cells. This is intended to reduce
pathogenic trafficking while maintaining immune competence and surveillance.38 This is particularly relevant in SLE, where infection risk, cumulative immunosuppression, and treatment toxicity are critical considerations in long-term management.
Preclinical studies have shown that cenerimod causes dose-dependent changes in lymphocyte distribution and immune activity, consistent with its expected pharmacodynamic effects.39 In mouse models of autoimmunity, cenerimod improved survival and reduced circulating inflammatory lymphocytes. In murine lupus models, treatment reduced proteinuria and renal involvement, while in experimental autoimmune encephalomyelitis models, it reduced pathological changes in the brain.37,39
Clinical Trial Development of Cenerimod in SLE
Clinical development of cenerimod in SLE has progressed from proof-of-concept studies, through dose-finding evaluations, and into pivotal Phase III programmes23,36 (Table 1). In an early Phase II randomised trial (NCT02472795), cenerimod demonstrated dose-dependent reductions in lymphocyte counts over 12 weeks, consistent with its expected mechanism of action and pharmacodynamic effects.23 Exploratory clinical outcomes were also evaluated, supporting biological activity and informing subsequent development strategies.23
Pharmacodynamic analyses from earlyphase studies indicate that cenerimod reduces circulating cluster of differentiation (CD)4+ and CD8+ T lymphocytes as well as B lymphocytes, consistent with S1PR1mediated sequestration of recirculating lymphocyte populations.23,35,45 Available data suggest broadly comparable reductions across T cell and B cell compartments rather than selective B cell depletion, reflecting its mechanism of action on lymphocyte egress rather than lineage-specific targeting.23,45 Naïve and central memory subsets, which are highly dependent on S1PR1 signalling for recirculation, appear particularly affected.15
The CARE Phase IIb trial (NCT03742037) evaluated cenerimod in patients with moderate-to-severe SLE receiving background therapy. In this randomised, double-blind study, the primary endpoint was the change in modified Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) at Month 6. Although the primary endpoint was not met, nominal improvement with the 4 mg dose informed selection of the dose used in Phase III trials.36,45
On the basis of these data, the ongoing Phase III studies, OPUS-1 (NCT05648500) and OPUS-2 (NCT05672576), are evaluating the efficacy and safety of cenerimod 4 mg once daily compared with placebo on top of standard of care, with Systemic Lupus Erythematosus Responder Index 4 (SRI4) response at Month 12 as the primary endpoint.40,41 In addition, an OPUS openlabel extension study (NCT06475742) is designed to assess long-term safety and tolerability, addressing the need for sustained safety evaluation in a chronic disease population with long-term treatment exposure.42 As the OPUS-1 and OPUS-2 trials are ongoing and blinded, comprehensive safety data, including detailed characterisation of adverse events, including infections, have not yet been publicly reported.
A key consideration for S1PR modulation in SLE relates to infection risk and background immunosuppression. Concerns around the safety of previous S1PR modulators have been raised in previous clinical trials in other autoimmune conditions, particularly with respect to infection risk.46,47 A meta-analysis of studies in multiple sclerosis reported that fingolimod was associated with a 16% increase in the risk of infection, especially lower respiratory infection and herpes virus infection.46 However, a study of fingolimod 0.5 mg/d for up to 5 years in patients with primary progressive multiple sclerosis showed that long-term infection risk was low, with 54 incidences of all infections over 100 patient-years.48 In terms of SLE, the CARE study showed that cenerimod was well tolerated by patients over a period of 12 months.36 Furthermore, although cardiac events have been linked to S1PR3 activity,
Table 1: Clinical studies of cenerimod in systemic lupus erythematosus.
because cenerimod is S1PR1/5-selective, cardiac risk may be expected to be lower than with less selective agents, supporting a more favourable cardiovascular safety profile.35,49,50
The results of the OPUS open-label extension study will provide further data to allow a full assessment of the long-term safety and tolerability of cenerimod in SLE.42
Many patients with SLE have baseline lymphopenia, raising an important safety consideration for therapies that further reduce circulating lymphocytes. As cenerimod lowers peripheral lymphocyte counts through S1PR1-mediated sequestration, individuals with pre-existing severe lymphopenia may be expected to require exclusion or additional monitoring to mitigate infection risk.
Finally, in preclinical SLE models, treatment reduced anti-double-stranded DNA (dsDNA) levels and lowered IFN-associated and pro-inflammatory biomarkers, including tissue readouts.23 In early clinical studies, cenerimod was associated with reductions in circulating anti-dsDNA titres and decreases in Type I IFN-related activity, including plasma IFN-α and an IFNassociated, whole-blood gene expression profile.23,35 Together, these findings suggest that S1PR1 modulation may attenuate both autoreactive humoral activity and IFNdriven pathways in SLE.
Although S1PR1 modulation primarily reduces lymphocyte egress from lymphoid tissues, the downstream immunological consequences are likely to extend beyond simple sequestration.15 By limiting recirculation of autoreactive T follicular helper cells and B cells, S1PR1 modulation may reduce germinal centre activity and plasmablast differentiation, thereby attenuating ongoing autoantibody production.11,32 In addition, reductions in circulating Type I IFN activity observed in early studies suggest that altered immunecell trafficking may indirectly dampen IFN-driven B cell activation. The observed decreases in anti-dsDNA titres are therefore likely to be multifactorial, reflecting modulation of adaptive immune activation dynamics rather than redistribution alone.23,45
Positioning S1PR Modulation Within the Evolving SLE Treatment Landscape
S1PR modulation represents a mechanistically distinct approach compared with B cell targeted therapies or IFN pathway inhibition, as it targets immune cell localisation and recirculation
upstream of many effector pathways.23,35 In principle, this strategy may allow broader immunomodulation across multiple immune cell subsets by reducing the probability of sustained immune activation within tissues and disrupting trafficking-dependent reinforcement of inflammation.
Potential advantages of this approach include upstream regulation of immune cell localisation and tissue-level inflammation in multiple cellular compartments, which may be relevant across diverse organ involvement where immune infiltration and endothelial dysfunction contribute to pathology.35,51 This may be particularly relevant for the long-term management priorities in SLE, including steroid-sparing disease control and reduction of chronic inflammatory burden.2,8-10
As with any emerging mechanism, the clinical value of S1PR modulation will depend on demonstration of meaningful clinical benefit, durability of response, and an acceptable long-term safety profile in the context of background immunosuppression. Ongoing Phase III trials will be critical in defining efficacy across clinical domains, identifying appropriate patient populations, and clarifying how S1PR modulation may be integrated into treatment algorithms in relation to other targeted therapies.
OVERALL PERSPECTIVE AND FUTURE DIRECTIONS
Current therapies for SLE have meaningfully expanded and now include guidelinesupported use of immunomodulatory agents and targeted biologics.2,8 However, available approaches primarily address a limited subset of dominant immune pathways, leaving mechanisms such as immune trafficking, endothelial regulation, and innate-adaptive crosstalk incompletely targeted.3,15-18,20,22,24,25 This mechanistic gap aligns with persistent unmet needs in routine practice, including incomplete durability of response, ongoing flare burden, and sustained reliance on glucocorticoids in many patients.5
Mechanistic insights into SLE increasingly support a more integrated model in which immune activation is sustained not only by cytokine pathways, but also by the spatial organisation of immune responses. Within this evolving landscape, S1PR modulators expand available strategies by targeting immune cell organisation and localisation, rather than focusing only on the suppression of activation pathways. Cenerimod, a selective S1PR1 modulator, is an example of this approach in SLE and is currently being evaluated in Phase III trials.36,37,45 If ongoing studies confirm clinically meaningful efficacy, acceptable safety, and steroid-sparing potential, S1PR modulation could be an additional or sequential treatment option for patients who remain uncontrolled with existing therapies,
References
1. Ameer MA et al. An overview of systemic lupus erythematosus (SLE) pathogenesis, classification, and management. Cureus. 2022;14(10):e30330.
2. Fanouriakis A et al. Update οn the diagnosis and management of systemic lupus erythematosus. Ann Rheum Dis. 2021;80(1):14-25.
3. Dai X et al. Systemic lupus erythematosus: updated insights on the pathogenesis, diagnosis, prevention and therapeutics. Signal Transduct Target Ther. 2025;10(1):102.
4. Hoi A et al. Systemic lupus erythematosus. Lancet. 2024;403(10441):2326-38.
5. Arnaud L, Tektonidou MG. Longterm outcomes in systemic lupus erythematosus: trends over time and major contributors. Rheumatology (Oxford). 2020;59(Suppl 5):v29-38.
6. van Vollenhoven RF et al. Treatto-target in systemic lupus erythematosus: recommendations from an international task force. Ann Rheum Dis. 2014;73(6):958-67.
7. Piga M et al. Framework for implementing treat-to-target in systemic lupus erythematosus routine clinical care: consensus statements from an international task force. Autoimmun Rev. 2025;24(5):103773.
8. Fanouriakis A et al. EULAR recommendations for the management of systemic lupus erythematosus:
especially when immune trafficking contributes to multisystem involvement.
Future progress in SLE therapeutics will depend on better translating disease mechanisms into effective clinical strategies. This includes integration of mechanistic and clinical trial data and developing a clearer evidence base for combination or sequential targeting of complementary pathways. In parallel, continued investigation into underrecognised mechanisms such as trafficking and tissue-level immune regulation may enable an earlier and more durable interruption of inflammatory cascades, ultimately improving long-term outcomes and reducing the overall treatment burden.
2023 update. Ann Rheum Dis. 2024;83(1):15-29.
9. Tanaka Y. Novel therapies in treatments of SLE. Best Pract Res Clin Rheumatol. 2025;39(4):102101.
10. Stojan G, Petri M. The risk benefit ratio of glucocorticoids in SLE: have things changed over the past 40 years? Curr Treatm Opt Rheumatol. 2017;3(3): 164-72.
11. Crow MK. Pathogenesis of systemic lupus erythematosus: risks, mechanisms and therapeutic targets. Ann Rheum Dis. 2023;82(8):999-1014.
12. Fugger L et al. Challenges, progress, and prospects of developing therapies to treat autoimmune diseases. Cell. 2020;181(1):63-80.
13. Duan L et al. Chemokines and chemokine receptors: potential therapeutic targets in systemic lupus erythematosus. Cytokine. 2024;184:156770.
14. Tian J et al. Role of sphingosine1-phosphate mediated signalling in systemic lupus erythematosus. Prostaglandins Other Lipid Mediat. 2021;156:106584.
15. Cyster JG, Schwab SR. Sphingosine1-phosphate and lymphocyte egress from lymphoid organs. Annu Rev Immunol. 2012;30:69-94.
16. Su X et al. Systemic lupus erythematosus: pathogenesis and targeted therapy. Mol Biomed. 2024;5(1):54.
17. Pandey SP et al. Autoimmune responses and therapeutic interventions for systemic lupus erythematosus: a comprehensive review. Endocr Metab Immune Disord Drug Targets. 2024;24(5):499-518.
18. Sutanto H, Yuliasih Y. Disentangling the pathogenesis of systemic lupus erythematosus: close ties between immunological, genetic and environmental factors. Medicina (Kaunas). 2023;59(6):1033.
19. Fu Q et al. Association of elevated transcript levels of interferon-inducible chemokines with disease activity and organ damage in systemic lupus erythematosus patients. Arthritis Res Ther. 2008;10(5):R112.
20. Yu SL et al. Immunopathological roles of cytokines, chemokines, signaling molecules, and pattern-recognition receptors in systemic lupus erythematosus. Clin Dev Immunol. 2012;2012:715190.
21. Li J et al. S1P/S1PR signaling pathway advancements in autoimmune diseases. Biomol Biomed. 2023;23(6):922-35.
22. Hallisey VM, Schwab SR. Get me out of here: sphingosine 1-phosphate signaling and T cell exit from tissues during an immune response. Immunol Rev. 2023;317(1):8-19.
23. Strasser DS et al. Preclinical to clinical translation of cenerimod, a novel S1P(1) receptor modulator, in systemic lupus erythematosus. RMD Open. 2020;6(2):e001261.
24. Burg N et al. Sphingosine 1-phosphate receptor 1 signaling maintains endothelial cell barrier function and protects against immune complexinduced vascular injury. Arthritis Rheumatol. 2018;70(11):1879-89.
25. Zheng H et al. S1PR1-biased activation drives the resolution of endothelial dysfunction-associated inflammatory diseases by maintaining endothelial integrity. Nat Commun. 2025;16(1):1826.
26. Okuniewska M et al. SPNS2 enables T cell egress from lymph nodes during an immune response. Cell Rep. 2021;36(2):109368.
27. Pan L et al. Immunological pathogenesis and treatment of systemic lupus erythematosus. World J Pediatr. 2020;16(1):19-30.
28. Cyster JG, Wilson PC. Antibody modulation of B cell responsesIncorporating positive and negative feedback. Immunity. 2024;57(7): 1466-81.
29. Caielli S et al. Systemic lupus erythematosus pathogenesis: interferon and beyond. Annu Rev Immunol. 2023;41:533-60.
30. Song B et al. Targeting immune cell migration as therapy for inflammatory disease: a review. Front Immunol. 2025;16:1650760.
31. Ginsberg P et al. Tissue-resident memory T cells in renal autoimmune diseases. Front Immunol. 2023;14:1111521.
32. Chang HD et al. Pathogenic memory plasma cells in autoimmunity. Curr Opin Immunol. 2019;61:86-91.
33. Ahmed A et al. Immunopathogenesis of systemic lupus erythematosus: interplay of innate and adaptive immunity, microbiome dysbiosis, and emerging therapeutic targets. Pathophysiology. 2025;32(4).
34. Yang X et al. Biological targeted therapy for lupus nephritis-the role of BLYS and APRIL. Ren Fail. 2025;47(1):2561791.
35. Hermann V et al. First use of cenerimod, a selective S1P(1) receptor modulator, for the treatment of SLE: a double-blind, randomised, placebocontrolled, proof-of-concept study. Lupus Sci Med. 2019;6(1):e000354.
36. Askanase AD et al. Cenerimod, a sphingosine-1-phosphate receptor modulator, versus placebo in patients with moderate-to-severe systemic lupus erythematosus (CARE): an international, double-blind, randomised, placebo-controlled, phase 2 trial. Lancet Rheumatol. 2025;7(1):e21-32.
37. Kaye AD et al. Evolving treatment strategies for systemic lupus erythematosus in clinical practice: a narrative review. Cureus. 2024;16(12):e75062.
38. Pérez-Jeldres T et al. Targeting sphingosine-1-phosphate signaling in immune-mediated diseases: beyond multiple sclerosis. Drugs. 2021;81(9):985-1002.
39. Piali L et al. Cenerimod, a novel selective S1P(1) receptor modulator with unique signaling properties. Pharmacol Res Perspect. 2017;5(6):e00370.
40. Viatris Innovation GmbH. A research study to evaluate the effects of a new oral medicine called cenerimod in adults with systemic lupus erythematosus (OPUS-1). NCT05648500. https://clinicaltrials. gov/study/NCT05648500.
41. Viatris Innovation GmbH. A research study to evaluate the efficacy and safety of cenerimod in subjects suffering from systemic lupus erythematosus (OPUS-2). NCT05672576. https://clinicaltrials. gov/study/NCT05672576.
42. Viatris Innovation GmbH. Longterm safety and tolerability of cenerimod in adults with systemic lupus erythematosus (OPUS OLE). NCT06475742. https://clinicaltrials. gov/study/NCT06475742.
43. Viatris Innovation GmbH. A research trial to assess if cenerimod is efficacious and safe to treat active lupus nephritis on top of regular
44. Viatris Pharmaceuticals Co., Ltd. A study to evaluate the safety, tolerability, pharmacokinetics and pharmacodynamics of cenerimod in adult Chinese participants with moderate-to-severe systemic lupus erythematosus (SLE). NCT07266090. https://clinicaltrials.gov/study/ NCT07266090.
45. Suffiotti M et al. Pharmacodynamics of the S1P(1) receptor modulator cenerimod in a phase 2b randomised clinical trial in patients with moderate to severe SLE. Ann Rheum Dis. 2025;84(2):284-93.
46. Zhao Z et al. Incidence and risk of infection associated with fingolimod in patients with multiple sclerosis: a systematic review and meta-analysis of 8,448 patients from 12 randomized controlled trials. Front Immunol. 2021;12:611711.
47. Yang X et al. Potential adverse events associated with sphingosine-1phosphate (S1P) receptor modulators in patients with multiple sclerosis: an analysis of the FDA adverse event reporting system (FAERS) database. Front Pharmacol. 2024;15:1376494.
48. Fox EJ et al. Lymphocyte counts and infection rates: long-term fingolimod treatment in primary progressive MS. Neurol Neuroimmunol Neuroinflamm. 2019;6(6):e614.
49. Juif PE et al. Pharmacokinetics, pharmacodynamics, tolerability, and food effect of cenerimod, a selective S1P₁ receptor modulator in healthy subjects. Int J Mol Sci. 2017;18(12):2636.
50. Fryer RM et al. The clinically-tested S1P receptor agonists, FTY720 and BAF312, demonstrate subtypespecific bradycardia (S1P₁) and hypertension (S1P₃) in rat. PLoS One. 2012;7(12):e52985.
51. Xiong Y, Hla T. S1P control of endothelial integrity. Curr Top Microbiol Immunol. 2014;378:85-105.
Patient Views on the Use of AI for Chest X-Ray Assessment
Authors: Andrew Asamoah Kyeremeh,1 Lesley Ann Anderson,2,3 Benjamin Yi Hong Tse,4 Struan Wilkie,4 Andrew Keen,4 *Clarisse Florence de Vries5
1. Clinical Oncology, Mount Vernon Cancer Centre, East and North Hertfordshire NHS Trust, UK
2. Biostatistics & Health Data Science, Institute of Applied Health Sciences, School of Medicine, Medical Science and Nutrition, University of Aberdeen, UK
3. Interdisciplinary Institute, University of Aberdeen, UK
4. NHS Grampian, Aberdeen, UK
5. Glasgow Lab of Health Data Science and AI, Public Health, School of Health and Wellbeing, University of Glasgow, UK *Correspondence to clarisse.devries@glasgow.ac.uk
Disclosure: The authors have declared no conflicts of interest.
Background: Healthcare organisations are experiencing significant challenges and delays in radiological reporting and clinical assessment. AI tools can assist the interpretation of chest X-rays and enable risk stratification.
Objective: To assess patient perspectives on the use of AI in chest X-ray interpretation, focusing on their knowledge, comfort levels, and preferences regarding AI-assisted radiological care.
Methods: A patient survey on AI use in chest X-ray interpretation was conducted at a single UK tertiary hospital. Patients attending their chest X-ray appointment were invited to participate. The survey captured information on their knowledge and perceptions of AI use in the chest X-ray service. Responses were summarised using descriptive statistics. Freetext comments were interpreted using thematic analysis. Correlation analysis assessed relationships between responses.
Results: Of the 175 patients who participated in the study, 149 completed the survey. Overall, 52.1% reported being comfortable with the use of AI in their care, 24.9% were neutral, while 21.9% were uncertain. Only two participants objected to the use of AI in their care. Most (92.6%) would prefer a chest X-ray AI tool to be used as a decision aid, rather than reporting autonomously (4.9%) or not being used at all (2.5%). Patients with higher self-reported knowledge of AI were more likely to be comfortable with the use of AI in their care (p=0.003; τb=0.24). The open-ended responses showed that participants generally accepted the AI’s ability to improve care; however, many indicated that further information was needed.
Conclusion: Patients who self-reported greater knowledge of AI were more likely to accept its use in chest X-ray reporting and prioritisation. This finding highlights the importance of improving public understanding through clear communication and education.
Key Points
1. Understanding patient views can support the successful integration of AI into clinical workflows. This study surveyed 175 patients attending chest X-ray appointments to assess their views regarding AI being used in their care.
2. This study highlights that most patients surveyed supported AI use in chest X-ray reporting, especially when used alongside human expertise. They also approved of AI use for triage to prioritise patients who need urgent clinical evaluation.
3. Findings showed that acceptance of AI use was correlated with patients’ self-reported knowledge of AI. Clear communication and educational efforts can enhance patients’ understanding and comfort with the use of AI in their care.
INTRODUCTION
With the ever-increasing need to improve efficiency and efficacy in clinical care, AI has been drawn to the forefront of healthcare, especially in medical imaging.1 In the year 2023/2024, 47.2 million images required processing within NHS England.2 Of these, general practitioner referrals for chest radiographs accounted for approximately 2.2 million images.2 A small minority of these images will contain indications of serious disease, most notably lung cancer, which requires urgent reporting and further action. Until recently, there were no objective means of risk stratifying large image sets, which would enable clinical staff to report the images of most concern first. AI techniques could assist by prioritising radiographic images for clinician review and identifying areas of suspicion.
Radiology reporting is facing significant challenges. Understaffing and increased demand have led to longer waiting times for radiological review,3 while subsequent outsourcing has resulted in high costs.4 The UK has a 29% shortfall of clinical radiologists, which is estimated to increase to 39% by 2029.4 In 2022/2023, over 700,000 imaging investigations performed in NHS England were not reported within the target of 28 days, a 31% increase from the previous year.3 The cost of managing excess reporting demand in the UK in 2024 was estimated at 325 million GBP.4 AI may help alleviate this burden and enhance service delivery by reducing reporting time and prioritising images of high-risk patients. This could reduce time to diagnosis
and treatment for a range of conditions, including lung cancer and other critical illnesses, improving patient outcomes.
Studies of clinician perceptions on the implementation of AI in clinical settings suggest an optimistic view; however, concerns include the quality and safety of AI systems.5 In recent years, the importance of considering patients’ views on AI used in their care has been recognised.6,7 Findings from surveys suggest that patients would like to know how AI is incorporated into their care, while concerns include lack of human supervision, data privacy, and accountability.6 One of the main underpinnings of medicine is informed consent and the establishment of duty of care. With the introduction of AI, careful consideration of confidentiality and informed consent is required.8
A survey of patient perceptions of the use of AI in the assessment of their radiographs was undertaken. The principal goal of this survey was to provide evidence for future decisions on the implementation of AI into the healthcare system, ensuring that care is tailored to patient needs.
METHODS
Context
The Grampian Radiology Assisted Chest X-Ray Evaluation (GRACE) project prospectively evaluated AI use for chest X-rays in NHS Grampian, UK. This prospective project evaluated Annalise.
ai (now Harrison.ai, Sydney, Australia)’s AI tool Annalise Enterprise CXR (now Harrison. ai chest X-ray), capable of identifying 124 clinical findings.9 The primary evaluation period covered chest X-rays conducted between May 2023–April 2024. The AI tool was fully integrated into the chest X-ray workstream, reading all images and sorting them according to risk. The highest risk images were those identified by the AI as possible lung cancers. These were urgently reported by a small number of radiologists.
The NHS Grampian evaluation, assessing Annalise CXR as a reporting triage, clinical decision support, and education tool, included a 12-month run-in period before the primary evaluation period. This cross-sectional, single-centre survey was conducted during this run-in period, assessing patients’ views on AI use for chest X-rays during early implementation of the AI tool.
Survey Administration
Following research governance consultation, it was advised that the survey could meet the criteria for a service evaluation. GRACE, which assessed the AI tool itself, had previously been registered with NHS Grampian as a service evaluation. This patient-perspective survey was registered under the same pathway. The survey collected anonymous information from patients who were attending their chest X-ray appointments at the Outpatient Radiology Clinic, Aberdeen Royal Infirmary, UK (July–September 2022). No NHS data was collected. Patients were approached and invited to participate during their outpatient radiology clinic visit.
A thorough review of previous research questionnaires that had evaluated patient perceptions of AI in healthcare was conducted to identify the diverse approaches utilised. Based on this review, a self-administered questionnaire was co-designed with clinical, patient, and public involvement (Aberdeen Centre for Health Data Science, School of Medicine, Medical Sciences and Nutrition, UK) and academic input to enable a survey of patient perceptions on the use of AI in radiology in
relation to chest X-ray. Closed questions were utilised along with open-ended questions to enable participants to provide further information.
The questionnaire used for this study (Supplementary Figure 1) was administered in paper format and in English Language only. The survey included a brief introductory statement offering participants a general overview of the purpose of the service evaluation. The range of information captured included patient demographics (sex, age, and educational background), selfperceived knowledge of AI, and patient views on the use of AI in chest X-ray. Completion of the questionnaire was taken as consent to participate. A secure box was provided for submission of completed questionnaires within the radiology department to ensure anonymity of participant responses.
Data Handling and Statistical Analysis
Following completion of the questionnaire administration process, the responses obtained were manually entered into the SPSS program (Version 27; IBM, Armonk, New York, USA). Data entry was reviewed for quality control purposes, ensuring elimination and correction of errors. Statistical analyses were performed in R (version 4.4.2).
Demographic information, including age, sex, and educational background, were summarised using descriptive statistics. Frequency tables and bar charts were used to describe the responses to each question. Responses obtained for the openended questions were manually screened using a thematic analysis framework with corresponding quotes identified.
Using a 95% CI, τb correlation analysis was used to investigate the relationship between 1) patients’ self-reported level of AI knowledge and their overall acceptance of AI in their care; and 2) self-reported AI knowledge and approval of the tool’s triaging ability (determining the order in which chest X-rays are reviewed). τb was selected because it is appropriate for ordinal data with ties. The assumptions for τb (ordinal measurement, independence of observations, and an approximately monotonic association) were considered to be met given the study
design. ‘I do not know’ responses were excluded from the correlation analyses. The 95% CIs were calculated using bootstrapping with 5,000 repetitions.
Nonresponse error could not be formally assessed, as no information was collected on individuals who declined to participate. Statistical significance was defined as p<0.05. Because this was a service evaluation with no prespecified hypotheses, the correlation analyses were considered exploratory, and no formal sample size calculation was performed.
The reporting of the study aligns with the Consensus-Based Checklist for Reporting of Survey Studies (CROSS) guidelines.10
RESULTS
In total, 175 patients participated with most surveys (n=149; 85.1%) completed in full. For eight of the 26 partially completed surveys, one or more answers were missing sequentially at the end of the survey. For the remaining 18, missing answers were interspersed throughout the survey. One participant required assistance in completing the survey due to a language barrier.
Demographic characteristics are shown in Table 1. An equal proportion of men and women completed the survey. Age was normally distributed (mean: 59.1 years; SD: 17.7 years) and ranged from 16–95 years. Most respondents (41.7%) had secondary education as their highest attained education level. There were no significant differences in sex (χ2; p=0.37) or age (two-sample t-test; p=0.21) between participants who fully or partially completed the survey.
Most participants (45.7%; 79/173) indicated that they knew nothing about the use of AI in healthcare, while 39.3% (68/173) said they knew a little (Figure 1).
Participant attitudes towards the use of AI in their care were also assessed. Overall, 52.1% (88/169) of participants either approved or strongly approved of AI integration in their healthcare. A further 21.9% (37/169) expressed uncertainty
(Figure 2). Correlational analysis showed that participants with greater self-perceived knowledge of AI were more likely to be comfortable with the use of AI in their care (p=0.003; τb=0.24; 95% CI: 0.08–0.38). Notably, only two participants objected to the use of AI in their care; both of whom reported having no or limited knowledge of AI.
The subsequent open-ended question, ‘In a few words, can you tell us why?’, was answered by 77 participants. Two main thematic areas were identified: 1) approval and 2) lack of knowledge. Most comments (58.4%; n=45) indicated approval of AI for chest X-rays. Participants cited the prospect of improved care (‘AI aids & speeds up diagnostics’, ‘will improve diagnosis’, ‘advancement in care of patients’, ‘may improve & speed up interpretation of tests’); the reduction of human error (‘not affected by the stresses humans have’); and that it can help support healthcare (‘help with human care’, ‘anything that can help doctors help us can surely only be good’, ‘all information gained can be helpful’). Secondly, 25 comments (32.5%) related to a lack of knowledge, with one representative comment stating: ‘Don’t know enough to have an opinion!’. Only 5 comments (6.5%) indicated a cautious or negative view (‘technology still in infancy’, ‘it depends how much AI is used’).
Participants were further asked about how AI should be used to review their X-ray. Most (92.6%; 151/163) would prefer AI to be used as a decision aid. Only four participants (2.5%) thought AI should not be used at all, while eight participants (4.9%) thought AI should be used alone (without human input).
If this AI tool for chest X-rays were to be used in routine clinical care, 25.0% of participants (41/164) indicated that they would like the opportunity to opt out; 45.1% (74/164) would not require this option, while 29.3% (48/164) responded that they did not know.
When participants were asked about their potential concerns, most (61.8%; 99/160) indicated that the AI tool may make mistakes, while 30% (48/160) had privacy and/or security concerns about their personal data. Several (28.1%; 45/160)
(41.7%) Further education (college, apprenticeship)
(24.0%) Undergraduate
expressed no concerns. Five respondents highlighted other concerns in the freetext section, with four relating to potential negative impacts on care. In one openended response, the participant stated that they were concerned about the threat to personalised care, saying that AI ‘may undermine the care element of treatment by being impersonal’. Another indicated that AI could ‘make decisions based on cost not on chances of survival’.
Most participants (57.9%; 95/164) indicated that they thought that the AI tool would improve their care. Only one participant thought the tool would worsen care, while 34.1% (56/164) stated that they did not know
how it would impact their care. When asked if they thought their doctors may become reliant on the tool instead of their medical expertise, 30.1% (49/163) answered ‘no’, while approximately half (50.9%; 83/163) answered ‘maybe’. Only 3.7% (6/163) participants indicated ‘yes’. The remaining 15.3% of patients (25/163) responded that they did not know.
In total, 116 (70.3%) participants approved of the prioritisation functionality of the chest X-ray AI tool (Figure 3). A total of 39 participants (23.6%) were neutral to this feature, while 10 (6.0%) participants disapproved or strongly disapproved of it. Further correlational analysis showed that
Table 1: Demographic characteristics of survey participants.
Most participants reported knowing little to nothing about AI in healthcare. Two participants did not provide an answer.
While most participants were comfortable with the use of AI in their care, over one-fifth were unsure. Six participants did not provide an answer.
Figure 1: Participant self-reported knowledge of AI in healthcare.
Figure 2: Participant attitudes toward AI use in their healthcare.
respondents with greater self-perceived knowledge of AI were also more likely to approve of the tool’s prioritising functionality (p=0.011; τb=0.18; 95% CI: 0.04–0.31).
There were 41 free-text responses to the final survey question asking participants whether they had any further comments. The three main thematic areas identified were: 1) approval; 2) need for additional information; and 3) AI to be used to support and not replace human decision making. Overall, 15 comments (36.6%) were positive (‘If it helps why not’, ‘great idea’, ‘should be used more’), highlighting that AI could reduce waiting lists and support doctors (‘can speed things up & take pressure off doctors. Great idea’). A further 10 comments highlighted a knowledge gap and a need for further information (‘All too new for me’, ‘I would like to know more about it’). Eight comments highlighted that AI should be used in combination with human expertise, not replace it (‘Could be an incredible tool, but a human should always be involved in any final decisions affecting patient care’), while five were negative/ cautious (‘AI is dangerous’, ‘machines can make mistakes/errors too’).
DISCUSSION
The service evaluation demonstrated support for the use of AI as a decision aid for chest X-ray reporting and prioritisation, indicating a positive reception toward AI-assisted diagnostic workflows. Most participants showed optimism and confidence in the prospect of AI use in the routine delivery of chest X-ray, with very few respondents objecting. Overall, they preferred the tool to be employed as a decision aid augmenting the clinician’s role. Participants wanted more information on how the tool works and how it would be implemented in their care. The survey highlights the need to actively involve and inform patients about new developments in healthcare pathways to improve acceptability to patients.
This study is an important addition to the literature that focuses on patients’ views on the use of AI in healthcare.6,7 Importantly, it highlights that patients generally approve of the use of AI, with many believing that it may improve the care they receive, consistent with prior reports.11-13 However, most participants indicated they knew little to nothing about AI, and many highlighted that they were unsure
Figure 3: Participant attitudes toward AI use in their healthcare.
0
Most participants approved of the AI tool’s risk stratification feature. Ten participants did not provide an answer.
how they felt about its use in their healthcare. With higher self-reported knowledge of AI linked to increased acceptance, these findings suggest a need to provide further information to patients regarding AI tools used in their care.
While some studies have explored patient perspectives on AI use in radiology,14 there is a lack of focused research investigating the views of patients on the use of AI in chest radiography. This study provides preliminary insights into patients’ level of support for the integration of AI for chest X-rays. Additionally, the survey offered participants a free-text section enabling them to express more information about their opinions of using AI in chest X-ray.
The main limitation of this study is the limited generalisability of the findings beyond the local context, as only NHS Grampian patients were included. No specific arrangements were made for language barriers, as English is the primary language of communication in the setting of interest. According to Scotland’s census in 2022, 93% of Aberdeen City residents and 94% of Aberdeenshire residents fell into the category ‘Speaks, reads and writes English’, indicating few would have been excluded.15 One participant used a personal mobile app to translate the questionnaire into their preferred language, which may have introduced inaccuracies and led to inconsistent interpretation of the questions. This response could not be removed as responses were anonymous and non-identifiable. In this study, participants were asked to self-rate their knowledge of AI, which is subjective. Participants were offered a brief introduction to the AI tool on
References
1. Hosny A et al. Artificial intelligence in radiology. Nat Rev Cancer. 2018;18(8):500-10.
2. NHS England. Diagnostic imaging dataset 2023-24 data. Available at: https://www.england.nhs.uk/statistics/ statistical-work-areas/diagnosticimaging-dataset/diagnostic-imagingdataset-2023-24-data/. Last accessed: 1 April 2025.
3. The Royal College of Radiologists. Turnaround times – what are we
the first page of the questionnaire, which sought to standardise participants’ level of knowledge. There are also potential sources of bias. Selection bias may have occurred if individuals with stronger views or greater interest in technology were more likely to participate. Although efforts were made to frame questions neutrally, social desirability bias and aspects of the questionnaire design may still have influenced responses.
Most participants believed that the use of an AI tool in their care was advantageous, but preferred it to be used alongside human decision making and review. A similar conclusion was drawn from a systematic review of anticipated patient challenges with the introduction of AI into healthcare.16 The AI tool being assessed in this study was designed as a decision aid, meaning that decision making about the X-ray findings is the responsibility of the radiologist reading the image and not that of the AI tool. The AI tool is currently being used to prioritise images for radiologist review, giving it an independent function. Despite expressing less support for the autonomous use of AI, most respondents approved of AI use for prioritisation.
In conclusion, this study revealed that few respondents objected to the use of AI technology in the delivery of chest X-ray investigations and that support was greater in those with more knowledge of AI. This patient feedback shows a promising prospect for the use of AI in chest X-ray both for prioritisation of cases and as a decision aid. The findings also draw attention to the need for increased education regarding the use of AI in healthcare.
seeing? Available at: https://www.rcr. ac.uk/news-policy/policy-reportsinitiatives/turnaround-times-whatare-we-seeing/. Last accessed: 4 April 2025.
4. The Royal College of Radiologists. Clinical radiology census reports. Available at: https://www.rcr.ac.uk/ news-policy/policy-reports-initiatives/ clinical-radiology-census-reports/ Last accessed: 1 April 2025
5. Chen M et al. Acceptance of clinical artificial intelligence among physicians and medical students: A systematic review with cross-sectional survey. Front Med. 2022;9:990604.
6. Moy S et al. Patient perspectives on the use of artificial intelligence in health care: a scoping review. J Patient-Centered Res Rev. 2024;11(1):51-62.
7. Koohjani Z et al. Patient’s opinions on the use of artificial intelligence in healthcare: a systematic review. Razavi Int J Med. 2024;12(3):1-11.
8. Murdoch B. Privacy and artificial intelligence: challenges for protecting health information in a new era. BMC Med Ethics. 2021;22(1):122.
9. Harrison.ai. CXR. 2025. Available at: https://harrison.ai/cxr/. Last accessed: 3 November 2025.
10. Sharma A et al. A consensus-based checklist for reporting of survey studies (CROSS). J Gen Intern Med. 2021;36(10):3179-87.
11. Musbahi O et al. Public patient views of artificial intelligence in healthcare: a nominal group technique study. Digit Health. 2021;7:20552076211063682.
12. Richardson JP et al. Patient apprehensions about the use of artificial intelligence in healthcare. Npj Digit Med. 2021;4(1):1-6.
13. de Vries CF et al. Screening participants’ attitudes to the introduction of artificial intelligence in breast screening. J Med Screen. 2021;28(3):221-2.
14. Hemphill S et al. The implementation of artificial intelligence in radiology: a narrative review of patient perspectives. Future Healthc J. 2023;10(1):63-8.
15. UK Data Service. Local authority (CA2019). Available at: https:// statistics.ukdataservice.ac.uk/ dataset/scotland-s-census-2022uv210-english-language-skills/ resource/2674bb2f-20f8-4bbe-9821f3eaa8896160. Last accessed: 25 February 2026.
16. Young AT et al. Patient and general public attitudes towards clinical artificial intelligence: a mixed methods systematic review. Lancet Digit Health. 2021;3(9):e599-e611.
Successful Treatment of a Patient with Hypermobile Ehlers-Danlos Syndrome with Gastrointestinal Complications Through Personalised Artificial Nutrition: A Case Report
1. SOD Dietetics and Clinical Nutrition, AOU delle Marche, Ancona, Italy
2. SOD General and Emergency Surgical Clinic, AOU delle Marche, Ancona, Italy
*Correspondence to silvia.tedesco@ospedaliriuniti.marche.it
Disclosure: The authors have declared no conflicts of interest. Informed consent was obtained from the patient for the publication of this case report.
Acknowledgements: The authors would like to thank Piera Pezzotti (SOD Vascular Surgery, AOU delle Marche, Ancona, Italy) for kindly providing the images included in this article.
An increasing number of studies are highlighting gastrointestinal disorders associated with hypermobile Ehlers-Danlos syndrome (hEDS), particularly in cases where it is accompanied by postural orthostatic tachycardia syndrome and mast cell activation syndrome. The diagnosis of these conditions remains challenging. Gastrointestinal symptoms include chronic small intestinal dysmotility and visceral hypersensitivity. Here, the authors present the case of a young woman with hEDS, postural orthostatic tachycardia syndrome, and mast cell activation syndrome, whose quality of life improved significantly after she started receiving artificial nutrition. This case is of particular interest as, during the initial phase of parenteral nutrition, several central vascular accesses failed prematurely due to an abnormal subcutaneous fibrinoid reaction. Switching to enteral nutrition was crucial in resolving the complications associated with a central venous access, restoring intestinal function, and improving quality of life. This paper will examine the challenges presented by this case in detail, providing notes on the necessary pathophysiology to understand the gastrointestinal complications related to hEDS and evaluating the most effective and sustainable medical and nutritional strategies.
Key Points
1. The article describes a rare vascular complication in a patient with hypermobile Ehlers-Danlos syndrome receiving parenteral nutrition and her subsequent successful management with enteral feeding.
2. This case report highlights the diagnostic and therapeutic challenges of managing severe gastrointestinal dysfunction in a patient with hypermobile Ehlers-Danlos syndrome complicated by postural orthostatic tachycardia syndrome and mast cell activation syndrome.
3. Enteral nutrition could resolve complications associated with central venous access, restore intestinal function, and improve quality of life.
INTRODUCTION
Ehlers-Danlos syndrome (EDS) hypermobility type (hEDS) is an inherited connective tissue disorder that is characterised by joint hypermobility and musculoskeletal pain. It frequently presents with gastrointestinal (GI) symptoms, including chronic small intestinal dysmotility and visceral hypersensitivity.
There are 13 recognised subtypes of EDS.1 Among these, Type 3, the hypermobile variant (hEDS), is the only one without an identified genetic cause or clearly defined pathophysiology. This subtype is most strongly linked to GI symptoms. The lack of a known genetic marker represents a major challenge for diagnosis, as hEDS is currently identified solely based on clinical criteria.
Although not extensively investigated, it can be hypothesised that alterations in the mechano-elastic properties of the GI tract, combined with changes in mechanosensory afferent signalling, may contribute to the development of visceral pain. Sensitisation, defined as a lowered threshold for perceiving sensations originating from visceral organs, could result from this enhanced afferent activity. Moreover, rectal hyposensitivity has been reported in individuals with EDS and is considered a key factor contributing to constipation.
Visceral hypersensitivity is widely recognised as a possible mechanism underlying disorders of gut–brain interaction and may represent a shared pathophysiological process between disorders of gut–brain interaction and EDS.
In addition, studies examining fibroblasts from the skin of patients with EDS suggest that chronic inflammation may also play a contributory role.2
The coexistence of postural orthostatic tachycardia syndrome (POTS), mast cell activation syndrome (MCAS), and hEDS within the same individual is well documented. POTS has been identified as a strong predictor of GI dysmotility in EDS. As previously noted, individuals with hEDS frequently experience GI and orthostatic symptoms, suggesting that GI manifestations observed in POTS may, at least in part, arise from this overlap. Some authors have proposed that the combination of POTS and hEDS represents a distinct POTS subtype, supported by evidence indicating that affected individuals are typically younger, present with more frequent GI symptoms, demonstrate greater multisystem involvement, and show a higher prevalence of non-GI manifestations, such as fatigue, fibromyalgia, and depression, compared with those who have hEDS alone.
When eating-related symptoms result in reduced oral intake, nutritional support should be provided within a multidisciplinary framework.3 The initial strategy should focus on optimising oral intake through dietary adjustments and the use of oral nutritional supplements. Clinically assisted nutrition and hydration are primarily indicated in cases of objectively confirmed malnutrition or electrolyte imbalance and should not be employed solely for symptom management due to the potential iatrogenic risks. If necessary, nasogastric feeding may be initiated, with consideration of long-term
percutaneous endoscopic gastrostomy feeding if tolerated. In cases of severe gastric dysfunction but preserved small intestinal motility and absorptive capacity, post-pyloric feeding may be started via a nasojejunal route, with possible transition to long-term feeding through a percutaneous endoscopic gastrostomy-jejunal tube or a direct jejunal route (such as percutaneous endoscopic jejunostomy, balloon jejunostomy, or surgical jejunostomy), if tolerated. However, insertion of percutaneous feeding tubes carries inherent risks of morbidity and mortality, as well as complications related to wound healing, infection, and overgranulation, issues to which this patient population may be particularly vulnerable.
Intolerance to small intestinal enteral feeding is often driven by pain or discomfort rather than impaired intestinal motility or absorption. In patients with chronic visceral hypersensitivity, food intake may become associated with fear avoidance behaviours. Consequently, chronic pain management, focusing on neuropathic pain agents and psychological interventions with a rehabilitative approach, represents an essential component of multidisciplinary care.
Past medical history
Signs and symptoms at onset
Abnormal laboratory data at onset
The case the authors present is notable for two main features: (1) To their best knowledge, fibrinoid catheter reactions in hEDS necessitating discontinuation of parenteral nutrition (PN) have not been reported before; and (2) the patient has been successfully treated with enteral post-pyloric nutrition.
DETAILED CASE DESCRIPTION
A 24-year-old White woman with hEDS and myopathic features, POTS, and MCAS was referred to the authors’ ambulatory care centre for nutritional counselling. She presented with GI pain, dyspepsia, and hiccups after eating solid foods or oral nutritional supplements. The patient reported that she had experienced these symptoms for several years and had required PN support at another facility. PN was suspended due to intolerance to the administered mixtures, which manifested itself after several weeks of therapy (Table 1).
The patient’s medical history also included reactive hypoglycaemia (she was a continuous glucose monitoring user), polycystic ovary syndrome, ligament laxity with sarcopenia, and hypovitaminosis B12
POTS, MCAS, reactive hypoglycaemia (CGM user), PCOS, ligament laxity with sarcopenia, hypovitaminosis B12 and D due to malabsorption, previous nephrolithiasis and urticarial reactions, allergic rhinitis, and recurrent fever from periodontal infections not previously treated due to an antibiotic allergy
Gastrointestinal pain, dyspepsia, and hiccups after eating solid foods or oral nutritional supplements
Hypovitaminosis D, mild normocytic anaemia (iron deficiency and inflammation), compensated metabolic acidosis, and a reduction in urinary electrolytes over 24 hours (Type I renal tubular acidosis)
Table 1: Patient and disease characteristics at onset.
and D due to malabsorption. She had a history of previous nephrolithiasis and urticarial reactions, which ceased with the start of chronic antihistamine therapy (ebastine 10 mg + cetirizine 10 mg/mL oral drops, 20 drops in the evening, increasable to 30 drops). The patient also had allergic rhinitis and recurrent fever from periodontal infections that had not been previously treated due to antibiotic polyallergies.
During the suspension phase of parenteral therapy, the young woman experienced a progressive reduction in lean body mass, which impaired her mobility. She required a wheelchair due to ligament laxity and frequent joint subluxations. She was subsequently referred to Ancona University Hospital, Italy, for further nutritional evaluation.
During the authors’ initial assessment (Figure 1), she reported experiencing debilitating abdominal pain after consuming solid and liquid foods. She was constipated and bloated. Urine output was consistently low at <500 mL. She consumed 2.5 L of water per day, divided into smaller amounts, due to epigastric pain after drinking liquids. She also underwent daily infusion therapy, receiving 1,000 mL/ day of saline solution and 500 mL/day of rehydrating electrolyte solution.
Her extremely variable dietary history was approximately 356 kcal (mainly dairy products to promote GI tolerance), providing 14.5 g of protein. After discontinuing parenteral support, she began taking four nutritional supplements per day, each containing 300 kcal and 12 g of protein. Ten days before the initial assessment, she stopped taking these supplements due to increased epigastric pain, reflux symptoms, and an increase in episodes of debilitating reactive hypoglycaemia.
Over the previous 2 months, she had experienced progressive weight loss of 2.5 kg, from 55 kg (BMI 18.6 kg/m²) to 52.5 kg (BMI 17.7 kg/m²). On examination, she was found to have normal systemic objectivity except for diffuse abdominal tenderness and muscle hypotrophy.
Laboratory tests showed hypovitaminosis D, compensated metabolic acidosis, mild normocytic anaemia (iron deficiency and inflammation), and a reduction in urinary electrolytes over 24 hours. Blood and urine tests also enabled a diagnosis of Type I renal tubular acidosis to be made (for which treatment with sodium bicarbonate was initiated orally, restoring blood values to normal levels).
The clinical history and medical records indicated chronic functional intestinal insufficiency due to dysmotility, with symptoms so severe as to affect normal eating. Therefore, it was deemed necessary to resume parenteral support once the allergy testing had been completed.
After initiating chronic antihistamine therapy, under protected conditions parenteral mixtures were tested, including some that had already been administered and some that were new. The allergy tests were negative, so, PN was started after placement of a subclavian tunnelled central venous catheter (CVC) on the right.
Three months later, a fever of up to 40 °C appeared, accompanied by pain at the CVC site, increasing during PN infusion, and persisting after the feverish phase. A vascular surgical consultation was therefore performed, raising the possibility of pain at the cuff site due to a subcutaneous fibrinoid reaction, since the CVC showed no signs of malfunction. However, three sets of blood cultures were taken from the CVC and peripheral venous catheter, as well as blood samples for biological indices of inflammation, all of which were subsequently found to be negative. Due to painful symptoms persisting after the fever subsided, 1 month later, the tunnelled CVC was replaced with a non-cuffed tunnelled CVC with subclavian access on the left.
During her check-up 3 months later, she reported experiencing pain in the left clavicle-neck area for approximately 2 weeks while using the CVC in a supine position. The pain was exacerbated by a malfunctioning infusion pump, but subsided when she moved to a semi-sitting position. The chest X-ray showed correct positioning and the
course was within normal limits. Therefore, its use continued.
The patient returned for a check-up the next month, reporting that, a week after the CVC dressing was replaced and the stat lock system was changed, she had experienced pain at the CVC site, radiated to her shoulder and neck. This made it impossible to administer hydration and PN. A few days later, vascular surgery was performed to remove the left central venous access and insert a centrally inserted central catheter in the right subclavian vein. Macroscopic evaluation of the device showed a probable abnormal subcutaneous fibrinous reaction related to the underlying disease (Figure 2). The authors hypothesised that the fibrinous reaction might be linked with connective tissue fragility, inflammatory changes, and abnormal wound-healing patterns in hEDS.
The following month, the patient weighed 61 kg and had a BMI of 20.6 kg/m². Due to a sudden worsening of painful symptoms while using the CVC, she independently reduced her home PN. After discussing the case with the authors’ team and the patient, the authors decided to try enteral nutrition (EN).
A nasogastric tube was therefore inserted, and nasogastric feeding was initiated with five 200 mL boluses. After 2 weeks, given
the patient’s good tolerance of EN, the centrally inserted central catheter was removed and EN continued.
However, 3 months later, an increase in episodes of hypoglycaemia and POTS, as well as a reduction in tolerance to EN boluses and water, accompanied by epigastric pain, necessitated the replacement of the nasogastric tube with a nasojejunal tube. The authors then continued EN by nasojejunal feeding for weight maintenance, initially via an infusion pump, mainly at night, and then in boluses, with good tolerance. This suggests an important role for visceral hypersensitivity and pyloric hypertonicity, which are often present in patients with hEDS and GI symptoms.
DISCUSSION
hEDS is associated with a range of GI disorders, including acid reflux, abdominal pain (particularly following food intake or during enteral feeding), and constipation. Autonomic dysregulation is also frequently observed, most commonly manifesting as POTS, chronic urinary retention due to impaired urethral sphincter relaxation (Fowler’s syndrome), and episodes of hypoglycaemia. MCAS is being increasingly reported, especially among individuals with POTS.
A growing number of patients with joint hypermobility and GI dysmotility are being referred to nutrition support teams for management of weight loss and malnutrition.4
Several interrelated mechanisms may contribute to altered GI function in hEDS:5
• Altered compliance of the GI wall and mechanoreceptor dysfunction: Increased elasticity (compliance) of the GI tract wall may cause excessive distension in response to a given intraluminal pressure, leading to overstimulation of mechanoreceptors.
• Dysmotility: Changes in wall compliance, elasticity, and mechanoreceptor function may also disrupt normal GI motility.
• Visceral hypersensitivity: Direct alterations in neuronal signalling
have been proposed as a potential mechanism underlying visceral hypersensitivity and associated symptoms in hEDS.
• Altered vascular compliance: Venous pooling in the lower limbs, attributed to connective tissue abnormalities within blood vessel walls, has been documented in hEDS. This phenomenon may contribute to the cardiovascular and autonomic manifestations observed in these patients. Similar alterations in splanchnic circulation may occur, potentially playing a role in GI symptom development.
Non-GI mechanisms have also been proposed as contributors to symptoms in hEDS, in particular, autonomic dysfunction. Cardiovascular autonomic manifestations may include orthostatic hypotension, orthostatic intolerance, neurally mediated hypotension, and POTS. Multisystem
Figure 2: Non-cuffed tunnelled central venous catheter.
A) and B) Macroscopic evaluation of the device showed an abnormal subcutaneous fibrinous reaction related to the underlying disease.
involvement is common, and noncardiovascular symptoms, particularly GI issues such as nausea, irregular bowel movements, abdominal pain, bloating, and constipation, are often reported. These symptoms are likely multifactorial and may arise from altered splanchnic circulation, small fibre neuropathy, or changes in vascular compliance associated with generalised tissue laxity in hEDS.
Reduced oral intake due to eating-related symptoms should prompt nutritional evaluation. Nutrition support should be provided in a multidisciplinary context. The primary approach should optimise the oral diet and eventually add oral nutritional supplements. If oral feeding is insufficient or impractical, EN is recommended. In case of intolerance or refusal of EN, a switch to PN is recommended. However, PN with hydration is primarily indicated in case of objectively demonstrated severe malnutrition with electrolyte disturbance.
A literature review was conducted using a systematic approach. The PubMed database was searched, and a manual search was added (last update August 2025). The research showed no hEDS cases treated with artificial nutrition, only several reviews about assessment, diagnosis, and management of GI symptoms in hEDS with discordant results. A standardised therapy has yet to be established, and an integrated management approach is therefore recommended.
If PN is initiated, any iatrogenic complications should prompt a reassessment of the intervention’s risk–benefit profile. Once nutritional status has stabilised, strategies to optimise oral or enteral intake and employ less invasive forms of nutritional support should be explored, with the aim of transitioning to the least invasive approach feasible over the long term.
PN may become a necessary intervention when patients face severe, life-limiting malnutrition and cannot tolerate enteral feeding. Its implementation should be accompanied by appropriate psychological support and close collaboration with the multidisciplinary clinical team.
In this clinical case, PN was crucial in restoring satisfactory nutritional status and adequate lean body mass, enabling the woman to resume normal walking and daily activities. However, the success of the parenteral support was offset by vascular complications, which were probably caused by abnormal fibrinoid reactions in the subcutaneous tissue at the device insertion site. Once this was established, the enteral option was reconsidered, despite not having been initially pursued due to the clinical situation and the patient’s preferences. Enteral feeding allows for slow, small, and concentrated delivery of nutrients. This minimises the sudden shift of blood to the gut and the gastric wall distention, reducing pain and vascular-triggered symptoms (POTS). Moreover, EN remains the most physiological option, preventing gut atrophy, is less labour-intensive and easier to manage than PN, and is significantly cheaper with shorter hospital stays compared to parenteral alternatives.
Switching to enteral support enabled the patient to regain in quality of life, as she no longer had to deal with complicated vascular access and could receive nutrition not only at home. Once the patient had accepted the feeding tube and EN had been started, the next step was to find the most suitable type of administration in accordance with the clinical presentation. Post-pyloric feeding (delivery of nutrients directly into the duodenum or jejunum) was advantageous because of her pyloric hypertonicity and visceral hypersensitivity, bypassing the dysfunctional and painful gastric phase of digestion. Moving the feeding site to the small intestine, which typically remains more functional despite gastric issues, allows for better tolerance of nutritional goals. For patients with hEDS, this route is often a critical step in preventing the need for more invasive artificial nutrition when gastric intolerance is severe. Switching from a nasogastric tube to a nasojejunal tube bypassed gastroparesis and pyloric hypertonicity, resulting in a significant improvement in pain and intestinal discomfort related to the mixture’s administration. Actually, her weight has stabilised and painful symptoms during feeding has been
significantly reduced. In addition, episodes of POTS and hypoglycaemia have decreased, and there has been a marked improvement in mobility and muscle tone, with better activity tolerance.
CONCLUSIONS
GI symptoms, associated comorbidities, both physical and psychological, and nutritional challenges significantly affect morbidity and quality of life in patients with hEDS. The pathophysiology of GI symptoms appears to involve both GI and non-GI mechanisms.6
The co-occurrence of POTS, MCAS, and hEDS within the same individual is well documented, with POTS identified as a strong predictor of GI dysmotility in hEDS.
Nutritional management requires a multidisciplinary approach aimed at stabilising patients and delivering care via the least invasive methods possible, while minimising the risk of iatrogenic complications associated with clinically assisted nutrition.
Optimal care for GI symptoms, psychological comorbidities, POTS, MCAS, and nutritional issues necessitates an integrated approach involving primary care providers and multiple specialties, including nutritionists, dietitians, gastroenterologists, psychologists, cardiologists, orthopaedists, pharmacists, and physiotherapists.
Recognising these patients and understanding the implications of the disorder provides the opportunity to offer timely reassurance, arrange
multidisciplinary care when needed, and minimise unnecessary investigations and therapies, thereby improving these patients’ long-term outcomes.7
In conclusion, this is the case of a young woman with hEDS, POTS, and MCAS, whose quality of life improved significantly after she started receiving artificial nutrition. This case is of particular interest, as, during the initial phase of PN, several central vascular accesses failed prematurely due to an abnormal subcutaneous fibrinoid reaction. Switching to EN was crucial in resolving the complications associated with central venous access, restoring intestinal function, and improving quality of life.
Patient Perspective
Living with hEDS felt like a constant battle against my own body, especially as my GI symptoms worsened to the point where eating became a source of pain rather than nourishment. Before starting EN, my quality of life was severely limited by profound fatigue, sleepless nights, and the anxiety of unpredictable complications and flare-ups. Transitioning to post-pyloric feeding was a significant adjustment, but the impact was transformative. For the first time in years, I am receiving consistent nutrition without the debilitating GI distress that followed every meal. This stability has restored my energy levels, allowing me to engage in daily activities that were previously impossible. While managing a feeding tube has its challenges, the ability to reclaim my life and focus on my future rather than my symptoms has been invaluable. I finally feel like I am managing my condition rather than it managing me.
References
1. Malfait F et al. The 2017 international classification of the Ehlers–Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):8-26.
2. Quigley EMM et al. The suggested relationships between common GI symptoms and joint hypermobility, POTS, and MCAS. Gastroenterol Hepatol (N Y). 2024;20(8):479-89.
3. Lam C et al. Gastrointestinal symptoms and nutritional issues in patients with hypermobility disorders: assessment,
diagnosis and management. Frontline Gastroenterol. 2022;14(1):68-77.
4. Nightingale JMD et al. The management of adult patients with severe chronic small intestinal dysmotility. Gut. 2020;69(12):2074-92.
5. Thwaites PA et al. Hypermobile Ehlers-Danlos syndrome and disorders of the gastrointestinal tract: what the gastroenterologist needs to know. J Gastroenterol Hepatol. 2022;37(9):1693-709.
6. Aziz Q et al. AGA clinical practice update on GI manifestations and autonomic or immune dysfunction in hypermobile Ehlers-Danlos syndrome: expert review. Clin Gastroenterol Hepatol. 2025;23(8):1291-302.
7. Choudhary A et al. A machine learning approach to stratify patients with hypermobile Ehlers-Danlos syndrome/ hypermobility spectrum disorders according to disorders of gut brain interaction, comorbidities and quality of life. Neurogastroenterol Motil. 2025;37(1):e14957.
Predictors of Medication Adherence and Quality of Life Among Patients with Epilepsy in Nigeria
Authors: *Mohammed Yusuf Mahmood,1,2 Ibrahim Abdu Wakawa,1,3 Asma’u Mohammed Chubado Dahiru,1,2 Falmata Baba Shettima,1 Umar Baba Musami,1,3 Anthony Ali Mshelia,1 Ibrahim Adamu Mshelia,1,3 Babagana Kundi Machina2,4
1. Department of Medical Services, Federal Neuro-Psychiatric Hospital Maiduguri, Nigeria
2. Department of Mental Health, College of Medical Sciences, Yobe State University, Damaturu, Nigeria
3. Department of Mental Health, College of Medical Sciences, University of Maiduguri, Nigeria
4. State Specialist Hospital, Damaturu, Nigeria
*Correspondence to mohammedmahmoodyusuf81@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors wish to express their immense gratitude to Donald Morisky for granting Ibrahim Abdu Wakawa kind permission to use the Morisky MAS–8 without any financial cost. The authors empathise with all the patients living with epilepsy around the globe, and extend their heartfelt appreciation to the study participants for consenting to partake in the study and for their patience and perseverance throughout the study. Finally, all thanks and gratitude go to the entire staff of the Epilepsy Clinic of the Federal Neuropsychiatric Hospital, Maiduguri, Nigeria, for the huge support they have given for the success of this work. Yusuf and Wakawa came up with the study concept and the design, and carried out the data analysis and the interpretation of results. Yusuf, Dahiru, and Shettima carried out the data collection and, in addition, participated in the interpretation of results and writing up of discussion. Yusuf, Musami, A. Mshelia, and I. Mshelia wrote the methodology and were also involved in data cleaning and entry into SPSS, while Wakawa and Machina wrote the conclusion and recommendation, in addition to reviewing the whole manuscript.
Received: 01.04.25
Accepted: 09.01.26
Keywords: Epilepsy, medication adherence, quality of life (QOL).
Epilepsy, a chronic neurologic condition, affects nearly 70 million people worldwide, with antiepileptic drugs as the mainstay of management. Medication adherence is key to successful treatment, reducing seizure frequency, and improving quality of Life (QOL). This study assessed sub-optimum adherence, seizure frequency, QOL, and their socio-demographic and clinical predictors. It was a cross-sectional part of a randomised control intervention on psycho-educational effects at Federal Neuro-Psychiatric Hospital, Maiduguri, Nigeria. A total of 410 adult people with epilepsy (aged 19–65 years) on anti-epileptic drugs for at least 3 months participated. Data analysis using SPSS 18 (IBM, Armonk, New York, USA) showed that
64.9% had sub-optimum adherence, 50.8% were seizure-free in the last 3 months, and 51.7% had good QOL. Independent predictors of poor adherence included being married (odds ratio [OR]: 3.13; p=0.047), having focal seizures (OR: 2.20; p=0.001), and frequent seizure episodes (OR: 4.90; p<0.0001). QOL predictors were age of epilepsy onset (OR: 1.90; p=0.033) and seizure frequency (OR: 2.1; p=0.0001). Non-adherence remains high, yet proper seizure control is achievable, leading to better QOL. Socio-demographic and clinical factors significantly influence adherence and QOL, highlighting the need for psychoeducation in routine care.
Key Points
1. High non-adherence: Nearly two-thirds (64.9%) of people with epilepsy reported sub-optimum adherence to antiepileptic drugs, highlighting a major barrier to effective management.
2. Frequent seizures were strongly associated with poor adherence (odds ratio: 4.90) and worse quality of life (QOL) (odds ratio: 2.1); and better control correlated with better QOL.
3. Marital status (married), focal seizure type, earlier age at epilepsy onset, and higher seizure frequency independently predicted poorer adherence or QOL, supporting targeted routine psychoeducation and tailored clinical follow-up.
BACKGROUND AND AIMS
Epilepsy is one of the common disorders known to man, with early accounts of the disorder traced back to antiquity.1 It was originally thought to be a mystical disease by almost all ancient cultures, such as the Greeks, Egyptians, Babylonians, etc. In modern science, it is defined as the occurrence of at least two unprovoked (reflex) seizures occurring more than 24 hours apart, having one unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures occurring over the next 10 years, or presence of a diagnosis of an epilepsy syndrome,2 and affects nearly 70 million people worldwide.2,3 In high-income countries, seven in 1,000 people will develop epilepsy in their lifetime, while 61 in 100,000 will develop new-onset epilepsy each year.4 These figures are about twice as high in low- and middle-income countries (LMIC).2,3 Problems such as obstetric complications, childhood malnutrition, central nervous system infections, and head injuries are possibly responsible for the high incidence, among other causes. The incidence varies with age, found to be higher in extremes
of age and lower among young adults, and higher in LMICs, with 80% of the global burden of epilepsy seen in these countries of the world.2,3
Pharmacotherapy with anti-epileptic drugs (AED) is the mainstay of the management of epilepsy.5 As epilepsy is a chronic condition, patients are usually required to be on longterm treatment with AEDs. Adherence to AEDs, which is the extent to which patients with epilepsy (PWE) follow the mutually agreed recommendations for prescribed medication with healthcare providers,6 is a key determinant of the success of pharmacotherapy among PWE.6-8
Medication non-adherence is generally prevalent among patients with chronic conditions, particularly in LMICs where high out-of-pocket expenditure is prevalent and other socio-cultural and economic factors are influential. In Northeast Nigeria for instance, Wakawa et al.9 reported a 55.7% prevalence of sub-optimal medication adherence among patients with severe mental illnesses. Factors responsible include patronage of traditional and spiritual treatments, male gender, poor insight, and low social support.
Similarly, adherence among patients with hypertension in Nigeria is low, ranging from 14–89%, contributing substantially to uncontrolled hypertension and related complications among this population.10
In the context of epilepsy, studies have equally shown that non-adherence to AEDs is prevalent and may be the most important cause of poorly controlled epilepsy.11 Furthermore, Stanaway et al.12 showed that up to 31% of seizures were precipitated by non-adherence to medication. Adherence to AEDs contributes to seizure control and, hence, improved quality of life (QOL).13 Extant literature suggests that sub-optimum adherence is associated with frequent dosing of several medications and drug side effects, age, and poor attitude to taking medication.11,14 Jones et al.15 in the UK, found that 59% of PWE were nonadherent to their AEDs. Ahmad et al.13 found that only 21.2% achieved high levels of adherence. A study in Laos16 showed nonadherence to AEDs to be at 42.4% among PWE. Finally, Mahmoud et al.11 reported up to 80% prevalence of medication nonadherence in Pakistan. Optimum adherence was associated with literacy, being on monotherapy, and less frequent seizures. Similarly, studies by Johnbull et al.17 in Northern Nigeria, and Hasiso and Desse18 in Southern Ethiopia, reported non-adherence rates of 68% and 67.4%, respectively. The most reported reasons for non-adherence were forgetfulness (75.4%) and running out of pills (10.8%). Factors that affected medication adherence were duration of epilepsy treatment, being married, levels of education, absence of comorbidity, forgetfulness, drug-induced fatigue, poor knowledge of AEDs, and being away from home.17,18 In low-resource settings like Northern Nigeria, paucity of healthcare personnel and infrastructure, coupled with inadequate and limited access to AEDs and out-of-pocket purchase of treatment, significantly contribute to non-adherence, leading to poor seizure control, increased morbidity, and a reduced QOL.17
Addressing medication non-adherence among patients with epilepsy requires multifaceted interventions targeting medical, psychological, social, and systemic
factors. Both randomised controlled and cohort studies have shown that structured psycho-educational programmes are effective in improving medication adherence and hence treatment outcomes among patients with epilepsy.19-22
The World Health Organization Quality of Life (WHOQOL) group defined QOL as the “individuals’ perception of their position in life in the context of the culture and the value system in which they live and in relation to their goals, expectations, standards, and concerns.”23 It is known that epilepsy has a great negative impact on the QOL of affected patients.24,25 Studies have shown that up to two-thirds of PWE who become seizure-free have a QOL similar to that of the general population.26,27 Medication adherence, polypharmacy, experience of public stigma, low household per capita income, seizure frequency, and severity of seizures are some of the factors that affect the QOL of PWE,28-30 in addition to low self-esteem and self-stigma.31 Other factors that affect QOL include depression, poor occupational adjustment, adjustment to seizure, and seizure worries.32 Suurmeijer et al.33 reported, in decreasing order of importance, that “psychological distress,” “loneliness,” “adjustment and coping,” and “stigma perception” contribute significantly to QOL. Studies have shown that the common predictors of poor QOL among patients on AEDs include anxiety disorders, depressive disorders, frequency of seizures, use of multiple AEDs, female gender, and side effects of AEDs.34,35 The most common aspects of QOL affected according to Imam et al.36 were impaired energy in 46.8% of cases, followed by memory problems (34.4%), fear of experiencing another seizure (25.8%), work (16.7%), and social limitations (10.3%).
There is a paucity of documentation on medication adherence among PWE, especially in sub-Saharan Africa and particularly in northeast Nigeria, where this study was conducted. Poverty and low level of education, which characterise the northeast part of Nigeria, out-of-pocket payment of medical services, and poor knowledge about one's own disease have been reported to have negative effects on
medication adherence.37,38 Epilepsy may likely compound the levels of poverty among its patients, and so does ignorance on the topic, which is prevalent in northern Nigeria. These may affect their level of medication adherence and consequently, QOL.
Based on the available literature searched, most published studies that assessed the relationship between epilepsy and QOL are from developed countries.25,27,28,39 If any such studies were conducted in developing countries, they are sparse and thus not readily accessible. Therefore, there is a need to assess the influence of sociodemographic and clinical factors on medication adherence and the attendant interactions with QOL among PWE in northeast Nigeria.
Aims of this Study
The aims of this study were two prongs: firstly, to assess the prevalence of suboptimum medication adherence and the level of QOL among PWE in northeast Nigeria, and secondly, to determine the predictors of medication adherence and QOL among the study participants.
METHODS
This study was part of an interventional study on the effect of a psycho-educational intervention on knowledge of epilepsy (KOE), medication adherence, and QOL among PWE on AEDs attending Federal Neuro-Psychiatric Hospital Maiduguri, a tertiary specialist mental health hospital in Borno State, northeast Nigeria. The study was carried out among 410 patients attending the epilepsy clinic of the hospital who participated in the study. Simple random sampling was used to recruit prospective participants who fulfilled inclusion criteria using a table of random numbers from a total of 1,601 PWE who attended the epilepsy clinic during the study period of 16 weeks. Block randomisation and allocation concealment were used to randomise participants into the intervention and the control groups (in the interventional arm of the study). The psychoeducational programme, adapted from the Modular
Service Package for the Treatment of Epilepsy (MOSES) by Ried et al.40 and tailored to the local context, comprised four modules covering epilepsy awareness, medical aspects, seizure triggers and avoidance, and lifestyle and treatment adherence. Delivered in group sessions by senior psychiatry registrars, it was conducted over two sessions, each held 4 weeks apart, using a structured, didactic, and interactive approach. The eligibility criteria were patients aged 19–65 years, diagnosed with epilepsy by consultant psychiatrists, having been on follow-up visits and AED treatments for at least 3 months, and who had granted informed consent. Exclusion criteria included patients presenting for the first time and patients with comorbid neuropsychiatric conditions, such as intellectual disability, schizophrenia, dementia, multiple sclerosis, etc.
The Statistical Package for the Social Sciences (SPSS) version 18 (IBM, Armonk, New York, USA) was used to analyse the data collected. Whereas descriptive statistics such as mean, range, and standard deviation were used to describe continuous variables, frequencies and percentages were used to analyse categorical variables. Bivariate analysis using the χ2 test was used to explore associations between sociodemographic variables and clinical variables on one hand, and outcome variables on the other hand. Binary logistic regression was then applied to assess independent predictors of suboptimum medication adherence and QOL. Sociodemographic and clinical factors were used as covariates, while sub-optimum medication adherence and QOL were independent variables.
Ethical Consideration
Ethical clearance with reference No: FNPHM/REC/2017/05 from the institutional Ethics Review Board of Federal Neuropsychiatric Hospital, Maiduguri, was obtained before conducting the study. Written informed consent forms explaining the study protocol were given to prospective participants, soliciting consent to participate in the study, while assuring them of utmost confidentiality, as only
codes instead of names will be employed during data collection and analysis. The research was carried out in accordance with the standard of research involving human subjects as enshrined in the Helsinki Declaration.
Measures
Sociodemographic questionnaire: A pre-designed pro forma questionnaire designed by the authors, soliciting the sociodemographic characteristics of the participants (age, educational status, marital status, tribes, and employment status), was used to collect sociodemographic data.
Clinical variables questionnaire: The clinical pro forma designed by the authors was used to collect the clinical variables, which included the following: seizure type (partial, partial with secondary generalisation, generalised), seizure frequency per month, seizure control for over 3 months (with a response of yes or no), epilepsy duration in years, and types and number of AEDs being used for treatment. Seizure frequency was assessed according to the following four categories: 0: no seizures in the last 3 months; 1: one to three seizures in the past 3 months; 2: four to six seizures in the past 3 months; and 3: more than six seizures in the last 3 months. Those with three or fewer seizures in the past 3 months are defined as having less frequent seizures, while those with four or more seizures have frequent seizures.19,22
Patient case files: Patients’ case files were used to obtain relevant clinical data of the participants, such as the classes of seizures, duration of epilepsy, duration of untreated epilepsy and duration of treatment, numbers and types of medications the patients were taking, and electro-encephalography reports and findings.
Medication Adherence Scale (MAS): The Morisky MAS was used to assess the adherence levels of the participants. It is an eight-item, self-administered scale for medication use attitude and behaviour patterns. Developed by Morisky et al.,41 it involves asking the patients about their drug-taking behaviour patterns and it is
validated in sub-Saharan African setting.42 It assesses either the tendency and the extent to which patients forget to take their medication or discontinue it upon feeling better or after their conditions worsens. It also includes the patient’s perception of their treatment plan as either convenient or not.38 Responses are categorised as either ‘Yes’ or ‘No’ for each of the first seven items, with a five-point Likert scale response for the eighth item. Each of the first seven questions is scored as one (1) for a ‘No’ answer and zero (0) for a ‘Yes’ answer. Scores range from 0–8 and are categorised into three adherence levels: a score of 8 indicates high adherence, scores between 5–7 reflect moderate adherence, and scores below 5 denote low adherence. For this study, any score of 7 and below is considered sub-optimum adherence, given the enormity of medication non-adherence in the management of epilepsy. A similar cut-off was adopted by Wakawa et al.9,43 in assessing medication non-adherence among patients with epilepsy and severe mental illness in northeastern Nigeria, as well as by Kretchy et al.44 in assessing non-adherence among outpatients with hypertension and comorbid psychiatric conditions in Ghana. The hospital in which the study was carried out lacks laboratory facilities for serum assessment of drug metabolites for the monitoring of AEDs adherence, which would have been a more objective way of assessing adherence.
Quality of Life in Epilepsy Questionnaire
(QOLIE-31): The QOLIE-31 questionnaire is a 31-item, self-administered instrument specifically designed to measure the QOL of PWE. It was derived from QOLIE-89.45,46 The QOLIE-31 questionnaire consists of seven of the 17 subscales of QOLIE-89. The QOLIE-31 questionnaire has two subscales: the emotional or psychological effects subscale (seizure worry, overall QOL, emotional wellbeing, energy, or fatigue subscales) and the medical and social effects (medication effects, work-driving social limits, cognitive function) subscale. It is scored from 0–100. Responses are summed up to give rise to the subtotal of the subscale scores and the overall total score. Higher scores on the QOLIE-31 indicate better levels of functioning and
QOL. The QOLIE-31 has good psychometric properties, with Cronbach’s alpha internal consistency of 0.85, and a test-retest reliability of (r=0.85).45 Ogundare et al.47 used it in Nigeria. It takes approximately 10 minutes for an individual with normal intelligence to complete it.45 Based on this study, those who scored below the mean score of 50.1 were categorised as having poor QOL and those who scored above the mean were considered to have good QOL. The selection of 50.1, the mean QOL score of the participants, was necessitated by the inability of the authors to access published data on the local average QOLIE-31 score in the study setting. Moreover, the use of a mean score to dichotomise outcome variables aligns with the approach adopted in previous studies, such as Wakawa et al.9 in Nigeria and Kretchy et al.44 in Ghana.
RESULTS
Sociodemographic Characteristics of the Participants
The study participants comprised 230 males (56.1%) and 180 females (43.9%), for a total of 410. The participants’ ages ranged from 19–64 years, with a mean age of 31.6 years and a standard deviation (SD) of ±9.5. The Kanuri tribe was the main ethnicity of the participants, accounting for about half of the study population (193; 47.1%). This is followed distantly by the Hausa tribe (65; 15.9%), then Babur (33; 8.0%), Fulani (31; 7.6%), and other tribes (88; 21.5%). One hundred and sixty-eight (41.0%) of the participants had only Qur’anic education, 113 (27.6%) had high levels of educational attainment (i.e., having ≥12 years of formal education), and the remaining participants had either no education at all (34; 8.3%), or low levels of education (≤11 years of education; 95; 23.2%). Furthermore, approximately half of the participants (187; 45.6%) were unemployed, and 188 (45.9%) were single. Other findings on the sociodemographic characteristics are presented in Table 1.
Clinical Characteristics of the Participants
A total of 223 (54.4%) had focal seizures, whilst 187 (45.6%) had generalised seizures. About 50.0% of study subjects had no seizures in the last 3 months prior to the study. Participants on single drug therapy constituted the vast majority of participants (383; 93.4%), and only 27 (6.6%) were on polytherapy. The mean age of onset and duration of epilepsy in years were 19.12±1.15 (Mean±SD; range: 0–59=59) and 12.32±9.12 (range: 0.5–42=41.50), respectively. The mean duration of untreated seizure in years was 5.23±5.8 (range: 0–32=32), while the mean seizure frequency in the last 3 months was (Mean±SD) (2.46±3.21) (range: 0-14=14). Other clinical characteristics of the participants are presented in Table 2.
Prevalence/Levels of Medication Adherence and Quality of Life
The majority of the study participants (266; 64.9%) had poor medication adherence, and only about half of the participants (212; 51.7%) had good QOL. Furthermore, about 50% of the participants had at least one seizure episode in the last 3 months. Other findings are represented in Supplementary Table 1.
Association
Between
Sociodemographic Characteristics and Medication Adherence
Except for marital status (p=0.031), there were no significant relationships between the participants’ sociodemographic characteristics and levels of medication adherence. Other findings on the relationship between sociodemographic characteristics and medication adherence are presented in Supplementary Table 2.
Association
Between the
Sociodemographic Characteristics and Quality of Life
There was no significant relationship between the sociodemographic
Table 1: Sociodemographic characteristics of the participants.
(Mean±SD: 31.58±9.47; range: 19–61=42)
*High education is having ≥12 years of western education. Low education is <12 years.
†Other major ethnicity assessed included Yoruba, Igbo, Marghi, Bolewa, and Shuwa.
Table 2: Clinical characteristics of the participants.
Variables
Class of Seizure
Age of Onset of Epilepsy, years* (Mean±SD: 19.12±1.15; range: 0–59=59)
Short
Duration of Epilepsy, years (Mean±SD: 12.32±9.12; range: 0.5–42=41.50)
duration (0–15)
(16–30)
Duration of Untreated seizure, years (Mean±SD: 5.23±5.8; range: 0–32=32)
(70.0)
(26.1)
(3.9)
Duration of Treatment, years (Mean±SD: 7.05±6.23; range: 0–40=40) Short
Drugs Combination†
Seizure Frequency‡ (Killifi)19 (Mean±SD: 2.46±3.21; range: 0–14=14) No seizure in last 3 months
(50.8)
*0–15 is a short duration of epilepsy, 16–30 is a medium duration, and >31 is long duration.
†Majority of the patients were on carbamazepine, polytherapy constituted mostly of a combination of two drugs (commonly, carbamazepine and sodium valproate or carbamazepine and phenobarbitone).
‡Seizure frequency categories adopted from Ibinda et al.17 Those with three or fewer seizures in the last 3 months are defined as having less frequent seizures, while those with four or more seizures have frequent seizures.
Association Between Clinical Variables and Medication Adherence
The combination of classes of seizures (p<0.0001), seizure frequency (p<0.0001), and AEDs (p=0.022) had a significant relationship with medication adherence. Other findings are represented in Supplementary Table 3.
Association Between Clinical Variables and Quality of Life
Among the clinical variables assessed, seizure frequency (p<0.0001) and age of onset of epilepsy (p=0.044) had significant relationships with levels of QOL. Other findings are represented in Supplementary Table 4.
Independent Predictors of Medication Adherence and Quality of Life
Class of seizures (p=0.001), seizure frequency (p<0.0001), being married (p=0.047), and AEDs combination (p=0.047) were independent predictors of medication adherence. The age of onset of seizure (p=0.044) and seizure frequency (p<0.0001) had a statistically significant relationship with QOL at bivariate analysis. These same variables were independent predictors of QOL. These findings are depicted in Table 3.
DISCUSSION
Fifty-six percent of the participants were males with a mean age of 31.6 years (±9.5), 41.0% of the participants had only Qur’anic education, 27.6% had high levels of educational attainment (i.e., having ≥12 years of formal education), and the remaining participants had either no education at all (8.3%), or low levels of education (≤11 years of education; 23.2%). Furthermore, approximately half of the participants were unemployed (45.6%) and single (45.9%). Focal seizures were recorded in 54.4% of the participants, while 45.6% had generalised seizures and 50.8% had no seizures in the last 3 months before the study. About 65% (64.9%) had suboptimum medication adherence, and 51.7% had good QOL. The independent predictors of sub-optimum medication adherence were being married, having focal seizures, and frequent seizure episodes, which were more likely to be less adherent to medication than those with lower seizure frequency. The independent predictors of QOL include the age of onset of epilepsy and seizure frequency.
Sub-optimum Medication Adherence
The finding of more than half (64.9%) of the participants in this study having poor
Table 3: Independent predictors of seizure frequency.
medication adherence is in keeping with many previous studies. For example, Ahmad et al.13 reported medication non-adherence of 78.8%. Similarly, Hasiso and Desse18 in Ethiopia found non-adherence of 68%. Although the most common reasons for the non-adherence in the Ethiopian study were forgetfulness (75.4%) and running out of pills (10.8%), other factors such as poverty, outof-pocket purchase of AEDs,49 medication side effects, attitudes to medications, and poor KOE and AEDs may, generally, account for the low levels of adherence found in this study. Furthermore, Johnbull et al.17 in northern Nigeria, and Jones et al.14 in the UK, found 67.4% and 59.0% of PWE were nonadherent to their treatments, respectively. Other concordant findings include studies from Brazil, Nigeria, and Palestine, where they showed non-adherence rates of 66.2%, 67.4%, and 64%, respectively.2,50-52 One strong basis for comparison among these studies is the use of the Morisky MAS.
On the contrary, Gurumurthy et al.51 and a study from Laos showed adherence was found to be 72.3% and 57.6%, respectively, among PWE.16 These two studies were consistent with the studies in the UK (63.6%) and the USA (73%).2,53 The variation in nonadherence rates across studies may be attributable to differences in study designs, as well as the sociodemographic and clinical characteristics of participants. Factors such as socio-cultural attitudes, educational and economic status, and the extent of social or health insurance coverage may also contribute to these disparities.51 Poor KOE, low level of education, unemployment, out-of-pocket payment of medication, and other sociodemographic factors could be responsible for the poor adherence.
Sociodemographic Predictors of Suboptimum Medication Adherence
Participants who were married were three times less likely to be adherent to AEDs, followed by those who were divorced. This result is rather unexpected, as spouses of chronically ill patients could likely serve as treatment helpers, reminding them to take their medication since forgetfulness is a factor for poor adherence.17 The possible explanation for this result could be that
married participants might be shouldering more responsibilities, financial and others, which may distract them from being adherent. Additionally, non-adherence among married participants may be a result of the sexual side effects of the AEDs.54 This finding is in contrast to that of Hasiso and Desse18 in Southern Ethiopia. The index study did not find, however, any significant association between medication adherence and other sociodemographic variables. Gurumurthy et al.51 similarly reported no significant association between age, gender, and medication adherence. Gurumurthy et al.51 and Das et al.,55 both in India, reported a significant relationship between AED adherence and socioeconomic class. This is not in keeping with the findings of this study; differences in sociodemographic characteristics of the participants of the various study settings and the study designs might account for this contrast. Johnbull et al.17 reported similar findings: apart from knowledge of AEDs, there was no significant association between age, sex, educational status, marital status and income or occupational status, and medication adherence.2 In low-resource settings like northern Nigeria, paucity of healthcare infrastructure and personnel and inadequate and limited access to AEDs, coupled with outof-pocket purchase of treatment, significantly contribute to non-adherence, leading to poor seizure control, increased morbidity, and a reduced QOL.17
Clinical Predictors of Sub-optimum Medication Adherence
Class of epilepsy (p<0.0001), seizure frequency (p<0.0001), and AEDs combination (p=0.022) were associated with medication adherence. Participants with focal, less frequent seizures and those on monotherapy were more likely to be adherent to AEDs than those with frequent seizures and those on polytherapy. Multivariate binary logistic regression revealed that all three variables were found to be independent predictors of medication adherence. Participants with focal seizures were about twice as likely (odds ratio [OR]: 2.20; p=0.001; 95% CI: 1.38–3.43) to be non-adherent to medication than those with generalised seizures. Participants
with frequent seizure episodes were five times (OR: 4.90; p<0.0001; 95% CI: 2.02–5.23) more likely to be nonadherent to medication than those with infrequent seizure episodes. Participants on monotherapy were about three times (OR: 3.31; p=0.030; 95% CI: 1.12–9.77) more likely to be adherent to medication than those on polytherapy. The probable explanation for this finding could be that the cost of buying more than one medication and taking more than one drug with multiple-dose regimens may reduce the chances of adherence among the participants. Other clinical variables assessed were not associated with medication adherence. The work of Gabr and Shams56 supports these findings. In addition, Gabr and Shams,56 Bautista and Rundle-Gonzalez,57 and Harimanana et al.16 revealed that monotherapy is more associated with optimum adherence than polytherapy. Higher pill burden and occurrence of side effects, multiple daily dosing schedules, and higher cost of the AEDs were postulated to be the possible reasons. However, Gurumurthy et al.51 showed no significant association between seizure frequency and adherence. Furthermore, Gurumurthy et al.,51 as well as Sweileh et al.,58 showed no significant association between levels of adherence and AEDs combination.2
Duration of epilepsy treatment is likely to have a negative relationship with medication adherence, due to the long duration of pill burden and cost of medication, among other factors, as supported by Hasiso and Desse’s18 study in Southern Ethiopia. Gurumurthy et al.,51 Mbuba et al.,59 El-Shamaa et al.,60 and Kyngäs,61 who all reported that medication adherence was associated with duration of epilepsy treatment and absence or presence of comorbidity, which is contrary to the index study. However, the findings of this study, as well as those of Gurumurthy et al.51 and Gabr and Shams,56 did not support this.
Level of Quality of Life
It is observed that epilepsy significantly impacts negatively on the QOL of the patients.34,62 The concept of QOL in epilepsy encompasses physical health, mental
health, and social health.34 Numerous factors contribute to the low level of QOL seen among PWE. Slightly more than half (51.7%) of the participants had good QOL. This finding may be connected with the fact that about 50.5% of the participants had no seizure episode in the past 3 months before the study. Numerous studies, particularly in Nigeria, have illustrated that there is an inverse relationship between seizure frequency and QOL.37,62 Another possible reason could be that the perception and idea of the concept of QOL may not be well established among the participants, considering their level of education and awareness, and other sociodemographic peculiarities. Social desirability while responding to the questionnaires could also contribute to this finding.
Ranjana et al.63 found a similar pattern they reported the mean QOL (mean±SD) as 64.1±15.97 among their study participants with individual scores ranging from 15.97–100, although they used QOLIE-10, which is an abridged version of the QOLIE-31 used in this study. Gholami et al.,64 however, reported different patterns in which more than 50% of their study participants had a moderate to low QOL, in contrast to more than 50% of healthy controls, who had good to excellent QOL. This finding is supported by the systematic review study of Baranowski.65 Their study is also consistent with many other previous studies carried out across different countries and cultures: Shakir,66 Tunisian,67 and Stavem et al.68 studies compared QOL of PWE to healthy persons.
Sociodemographic Predictors of Quality of Life
None of the sociodemographic characteristics assessed were found to have an association with QOL. This finding is supported by the work of Phabphal et al.69 in Thailand, although the female gender reported by Mosaku et al.37 in Nigeria and poor occupational adjustment reported by Devinsky and Cramer32 contribute significantly to poor QOL. This could be a negative association, as females are more likely to be poor in Africa, while poor occupational adjustment has an indirect relationship with economic capabilities, which
are determinants of QOL. This suggests that clinical factors rather than sociodemographic parameters have more influence on QOL among PWE. Shakir and Al-Asadi,66 however, reported that older patients and those with low education and income levels had lower overall QOL scores.66,69,70
Clinical Predictors of QOL in terms of clinical variables, the age of onset of epilepsy (p<0.0001), and seizure frequency (p<0.0001) were associated with QOL among the participants. Those with the age of onset after the age of 30 years had better QOL than the remaining participants. This means that the shorter the duration patients live with the disease, the better the QOL. Likewise, participants with less seizure frequency had better QOL. These clinical variables (age of onset and seizure frequency) were still found on multivariate logistic regression to predict QOL and for the age of onset (OR: 1.913; 95% CI: 1.054–3.474; p=0.033) and seizure frequency (OR: 2.170; 95% CI: 1.397–3.372; p=0.001). Participants with an earlier age of onset were twice as likely to have poor QOL as those with late ages of onset. Likewise, participants with frequent seizure episodes were about twice as likely to have poor QOL as those with less frequent seizures. Adewuya and Oseni,62 Mosaku et al.37 in Nigeria, Phabphal et al.69 in Thailand, Molugulu et al.71 in India, and Shakir and Al-Asadi66 in Iraq, similarly, revealed that the frequency of seizures predicts poor QOL in PWE.34 Additionally, Mosaku et al.37 found that polytherapy was associated with poor QOL among PWE. Shakir and Al-Asadi66 and Guekht et al.39 also showed duration of epilepsy was significantly associated with QOL scores: the longer the duration, the poorer the QOL. On the other hand, Devinsky and Cramer32 and Suurmeijer et al.33 in the Netherlands showed that the frequency of seizures did not contribute significantly to QOL among PWE, and Suurmeijer et al.33 showed that even the age of onset of epilepsy did not relate to QOL. Furthermore, Suurmeijer et al.33 showed that none of the clinical variables (age at onset, seizure frequency, side effects of AEDs) was predictive of QOL.
LIMITATIONS
This study is not without some limitations. The following were observed to be the limitations of the study:
• The lack of facility for serum assessment of drug metabolites for monitoring of adherence to AEDs, which would have been more objective measures of adherence to medication than the use of Morisky MAS.
• Although using a seizure logbook by PWE for the monitoring of seizure frequency is not common practice in the study setting, the use of logbooks could have added to the objectivity for the reporting of seizure frequencies by the participants, since verbal reporting is more subject to forgetting.
• Because it is a hospital-based and unicentric study, the findings may not be generalised to other settings.
• There was low representation of the populations from other parts of the Northeast geopolitical zone of Nigeria, the catchment area of the study centre, as a result of the security challenges occasioned by the Boko Haram insurgency.
RECOMMENDATION FOR FUTURE DIRECTIONS
Based on the findings of the study, the following recommendations are therefore made:
• The need to incorporate psychoeducation and adherence counselling sessions for PWE as part of the routine clinical services provided for this set of patients.
• The need to conduct a similar study on a larger scale, involving multiple centres across a wider part of the nation.
• The need to have facilities for laboratory serum monitoring of AED levels for clinical and research utilities.
• The need for a study to deeply assess factors that contribute to the high levels of sub-optimum medication adherence observed in the study, and to address them.
CONCLUSION
Based on the outcomes of the study, the following can be inferred: that nonadherence is high among PWE; however,
References
1. Panteliadis CP et al. Historical documents on epilepsy: from antiquity through the 20th century. Brain Dev. 2017;39(6):457-63.
2. Nelson Siewe Fodjo J. Definition, classification, and burden of epilepsy. Epilepsy - Update on Classification, Etiologies, Instrumental Diagnosis and Treatment. IntechOpen; 2021.
3. Fisher RS et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):47582.
4. Beghi E. The epidemiology of epilepsy. Neuroepidemiology. 2020;54(2):185–91.
5. Goldenberg MM. Overview of drugs used for epilepsy and seizures: etiology, diagnosis, and treatment. P T. 2010;35(7):392–415.
6. Fernandez-Lazaro CI et al. Adherence to treatment and related factors among patients with chronic conditions in primary care: a crosssectional study. BMC Fam Pract. 2019;20(1):132.
7. Burkhart PV, Sabaté E. Adherence to long-term therapies: evidence for action. J Nurs Scholarsh. 2003;35(3):207.
8. Dayapoğlu N et al. Evaluation of medication adherence and medication beliefs among patients with epilepsy. Epilepsy Behav. 2021;124:108366.
9. Wakawa AI et al. Prevalence and predictors of sub-optimal medication adherence among patients with severe mental illnesses in a tertiary psychiatric facility in Maiduguri, North-eastern Nigeria. Pan Afr Med J. 2015;21:39.
10. loh GUP et al. Medication adherence and blood pressure control amongst adults with primary hypertension attending a tertiary hospital primary
seizure control can be achieved in a significant proportion of PWE, and a good percentage of patients can have fair QOL. Sociodemographic and clinical factors have significant relationships with and can be independent predictors of medication adherence and QOL.
care clinic in Eastern Nigeria. Afr J Prim Health Care Fam Med. 2013;5(1):446.
11. Mahmoud MR et al. Measuring of non-adherence of epilepsy patients to their medication and its relationship to their beliefs about the disease, and the frequency of seizures: a comparative study between epilepsy patients in Saudi Arabia and egypt. Pak J Med Health Sci. 2022;16(06):479-84.
12. Stanaway L et al. Non-compliance with anticonvulsant therapy as a cause of seizures. N Z Med J. 1985;98(774):150-2.
13. Ahmad N et al. Medication adherence and quality of life in epilepsy patients. Int J Pharm Pharm Sci. 2013;5:401-4.
14. Mitchell WG et al. Adherence to treatment in children with epilepsy: who follows “doctor’s orders”? Epilepsia. 2000;41(12):1616-25.
15. Jones RM et al. Adherence to treatment in patients with epilepsy: associations with seizure control and illness beliefs. Seizure. 2006;15(7):504-8.
16. Harimanana A et al. Associated factors with adherence to antiepileptic drug in the capital city of Lao PDR. Epilepsy Res. 2013;104(1-2):158-66.
17. Johnbull OS et al. Evaluation of factors influencing medication adherence in patients with epilepsy in rural communities of Kaduna State, Nigeria. NM. 2011;02(04):299-305.
18. Hasiso TY, Desse TA. Adherence to treatment and factors affecting adherence of epileptic patients at Yirgalem General Hospital, Southern Ethiopia: a prospective cross-sectional study. PLoS ONE. 2016;11(9):e0163040.
20. Chahal S et al. Impact of a brief structured psychoeducation session on antiepileptic drug adherence and treatment outcome in persons with epilepsy: a prospective cohort study. Ann Indian Acad Neurol. 2021;24(3):361-6.
21. Al-Aqeel S. Strategies for improving adherence to antiepileptic drug treatment in people with epilepsy. Cochrane Database Syst Rev. 2020;10(10):CD008312.
22. May TW, Pfäfflin M. The efficacy of an educational treatment program for patients with epilepsy (MOSES): results of a controlled, randomized study. Epilepsia. 2002;43(5):539-49.
23. World Health Organization (WHO). The World Health Organization quality of life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med. 1995;41(10):1403–9.
24. Akosile CO et al. Quality of life, fatigue and seizure severity in people living with epilepsy in a selected Nigerian population. Seizure. 2021;84:1-5.
25. Tedrus GM de AS et al. Epilepsy and quality of life: socio-demographic and clinical aspects, and psychiatric co-morbidity. Arq Neuropsiquiatr. 2013;71(6):385-91.
26. Siebenbrodt Ket al. Determinants of quality of life in adults with epilepsy: a multicenter, cross-sectional study from Germany. Neurol Res Pract. 2023;5(1):41.
27. Boylan LS et al. Depression but not seizure frequency predicts quality of life in treatment-resistant epilepsy. Neurology. 2004;62(2):258-61.
19. Ibinda Fet al. Evaluation of Kilifi epilepsy education programme: a randomized controlled trial. Epilepsia. 2014;55(2):344-52.
28. Tlusta E et al. Clinical and demographic characteristics
predicting QOL in patients with epilepsy in the Czech Republic: how this can influence practice. Seizure. 2009;18(2):85-9.
29. Hamedi-Shahraki S et al. Health-related quality of life and medication adherence in elderly patients with epilepsy. Neurol Neurochir Pol. 2019;53(2):123-30.
30. Hu C et al. Effects of stigma on the quality of life in patients with epilepsy. Acta Epileptologica. 2024;6(1):10.
31. Jacoby A. Stigma, epilepsy, and quality of life. Epilepsy Behav. 2002;3(6S2):1020.
32. Devinsky O, Cramer JA. Introduction: quality of life in epilepsy. Epilepsia. 1993;34(s4).
33. Suurmeijer TP et al. Social functioning, psychological functioning, and quality of life in epilepsy. Epilepsia. 2001;42(9):1160-8.
34. Akinsulore A, Adewuya A. Psychosocial aspects of epilepsy in Nigeria: a review. Afr J Psychiatry (Johannesbg). 2010;13(5):351-6.
35. Bujan Kovač A et al. Quality of life in patients with epilepsy - single centre experience. Acta Clin Croat. 2021;60(Suppl 3):16-24.
36. Imam I et al The quality of life of chronic epileptic patients in Ibadan, Nigeria. Afr J Med Med Sci. 2003;32(4):367-9.
37. Mosaku KS et al. Quality of life and associated factors among adults with epilepsy in Nigeria. Int J Psychiatry Med. 2006;36(4):469-81.
38. Abdisa L et al. Factors associated with poor medication adherence during COVID-19 pandemic among hypertensive patients visiting public hospitals in Eastern Ethiopia: a cross-sectional study. BMJ Open. 2022;12(10):e064284.
39. Guekht AB et al. Factors influencing on quality of life in people with epilepsy. Seizure. 2007;16(2):128-33.
40. Ried S et al. MOSES: an educational program for patients with epilepsy and their relatives. Epilepsia. 2001;42(Suppl 3):76-80.
41. Morisky DE et al. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67-74.
42. Tandon S et al. Validation and psychometric properties of the 8-item Morisky Medication Adherence Scale (MMAS-8) in Type 2 diabetes patients in sub-Saharan Africa. Diabetes Res Clin Pract. 2015;110(2):129-36.
43. Wakawa IA et al. Prevalence and predictors of medication non-
adherence among patients with epilepsy in Maiduguri. Neurol Res Surg. 2024;7(3):1-9.
44. Kretchy IA et al. Mental health in hypertension: assessing symptoms of anxiety, depression and stress on antihypertensive medication adherence. Int J Ment Health Syst. 2014;8:25.
45. Cramer JA et al. Development and cross-cultural translations of a 31-item quality of life in epilepsy inventory. Epilepsia. 1998;39(1):81-8.
46. Devinsky O et al. Development of the quality of life in epilepsy inventory. Epilepsia. 1995;36(11):1089-104.
47. Ogundare T et al. Quality of life among patients with epilepsy in Nigeria: predictors and barriers to routine clinical use of QOLIE-31. Qual Life Res. 202;30(2):487-96.
48. Boroffka A, Olatawura MO. Community psyciatry in Nigeria—the current status. Int J Soc Psychiatry. 1977;23(4):275-81.
49. Getnet A et al. Antiepileptic drug nonadherence and its predictors among people with epilepsy. Behav Neurol. 2016;2016:3189108.
50. Ferrari CMM et al. Factors associated with treatment non-adherence in patients with epilepsy in Brazil. Seizure. 2013;22(5):384-9.
51. Gurumurthy R et al. An evaluation of factors affecting adherence to antiepileptic drugs in patients with epilepsy: a cross-sectional study. Singapore Med J. 2017;58(2):98-102.
52. Nakhutina L et al. Adherence to antiepileptic drugs and beliefs about medication among predominantly ethnic minority patients with epilepsy. Epilepsy Behav. 2011;22(3):584-6.
53. Faught RE et al. Impact of nonadherence to antiepileptic drugs on health care utilization and costs: findings from the RANSOM study. Epilepsia. 2009;50(3):501-9.
54. Calabrò RS, Cerasa A. Drug-induced sexual dysfunction in individuals with epilepsy: beyond antiepileptic compounds. Medicines (Basel). 2022;9(3):23.
55. Das K et al. Evaluation of socioeconomic factors causing discontinuation of epilepsy treatment resulting in seizure recurrence: a study in an urban epilepsy clinic in India. Seizure. 2007;16(7):601-7.
56. Gabr WM, Shams MEE. Adherence to medication among outpatient adolescents with epilepsy. Saudi Pharm J. 2015;23(1):33-40.
57. Bautista RED, Rundle-Gonzalez V. Effects of antiepileptic drug
characteristics on medication adherence. Epilepsy Behav. 2012;23(4):437-41.
58. Sweileh WM et al. Self-reported medication adherence and treatment satisfaction in patients with epilepsy. Epilepsy Behav. 2011;21(3):301-5.
59. Mbuba CK et al. Risk factors associated with the epilepsy treatment gap in Kilifi, Kenya: a cross-sectional study. Lancet Neurol. 2012;11(8):688-96.
60. El-Shamaa ET, Mahmoud DA. Factors contributing to therapeutic compliance of epileptic patients and the suggestive solutions. J Biol Agric Healthc. 2013;3(2):209-22.
61. Kyngäs H. Compliance with health regimens of adolescents with epilepsy. Seizure. 2000;9(8):598-604.
62. Adewuya AO, Oseni SBA. Impact of psychiatric morbidity on parent-rated quality of life in Nigerian adolescents with epilepsy. Epilepsy Behav. 2005;7(3):497-501.
63. Ranjana G et al. The sociodemographic, clinical and pharmacotherapy characteristics influencing quality of life in patients with epilepsy: a crosssectional study. J Neurosci Rural Pract. 2014;5(Suppl 1):S7-12.
64. Gholami A et al. Quality of life in epileptic patients compared with healthy people. Med J Islam Repub Iran. 2016;30:388.
65. Baranowski CJ. The quality of life of older adults with epilepsy: a systematic review. Seizure. 2018;60:190-7.
66. Shakir M, Al-Asadi JN. Quality of life and its determinants in people with epilepsy in basrah, Iraq. Sultan Qaboos Univ Med J. 2012;12(4):449-57.
67. Mrabet H et al. Health-related quality of life of people with epilepsy compared with a general reference population: a Tunisian study. Epilepsia. 2004;45(7):838-43.
68. Stavem K et al. Health status of people with epilepsy compared with a general reference population. Epilepsia. 2000;41(1):85–90.
69. Phabphal K et al. Quality of life in epileptic patients in southern Thailand. J Med Assoc Thai. 2009;92(6):762-8.
70. Minwuyelet Fet al. Quality of life and associated factors among patients with epilepsy at specialized hospitals, Northwest Ethiopia; 2019. PLoS ONE. 2022;17(1):e0262814.
71. Molugulu N et al. Evaluation of selfreported medication adherence and its associated factors among epilepsy patients in Hospital Kuala Lumpur. J Basic Clin Pharm. 2016;7(4):105-9.
Air Pollution and Interstitial Lung Disease: Insights from the Global Burden of Disease Database
Authors: *Geran Maule,1,2 Alron Harry,3 Ahmad Alomari,1,2 Osama Obeidat,1,2
Abdallah Rayyan,1,2 Joseph Ayim Zamora,1,2 Marianne E. Solano,4
John Rickards,5 Peters Okonoboh1,2
1. University of Central Florida College of Medicine, Orlando, USA
2. Graduate Medical Education Internal Medicine Residency Program, HCA Florida North Florida Hospital, Gainesville, USA
3. American Express, Pheonix, Arizona, USA
4. Internal Medicine Residency Program, Mount Sinai Hospital, Chicago, Illinois, USA
5. Department of Internal Medicine, Mercer University School of Medicine, Macon, Georgia, USA
*Correspondence to geran.maule@ucf.edu
Disclosure: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. This work was supported by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities. The authors have declared no conflicts of interest.
Interstitial lung disease (ILD) represents a heterogeneous group of disorders characterised by inflammation and fibrosis of lung tissues, often linked to significant morbidity and mortality. Increasing incidence of ILD in the USA, coupled with the known impact of air pollution on respiratory diseases, necessitates exploration of the potential relationship between environmental exposures and ILD.
This study examines the correlation between air pollution, specifically particulate matter with a diameter of 2.5 µm or less (PM2.5), nitrogen dioxide, and ozone, and ILD incidence across the USA from 1990–2021, utilising data from the Global Burden of Disease (GBD) database.
The authors performed a retrospective analysis using GBD data, correlating age-standardised ILD incidence rates with state-level pollution exposure metrics for PM2.5, nitrogen dioxide, and ozone. Pollution was measured using Summary Exposure Values (SEV). SEV is a populationweighted exposure metric that reflects both pollutant levels and related health risk. Because PM2.5-specific concentration data were not consistently available for all study years, SEV for ambient particulate matter was used as a proxy. Temporal trends in both variables were assessed, and scatter plots were employed to evaluate statistical associations. Geographic disparities in pollution and disease incidence were visualised with heat maps.
From 1990–2021, ILD incidence increased across all states, despite declining pollution levels. A moderate positive correlation (r=0.51) was identified between pollution exposure and ILD incidence, with higher disease rates observed in states like California and Texas, USA, which have elevated pollution levels. However, in population-weighted regression models, the association between particulate matter exposure and ILD incidence was not statistically significant.
At the state level, air pollution exposure was associated with ILD incidence, but findings from this ecological analysis do not establish causation. Further individual-level longitudinal studies are needed to clarify whether air pollution may contribute to ILD development or progression.
Key Points
1. Interstitial lung disease (ILD) incidence is increasing in the USA, despite declining national pollution levels, highlighting concerns about cumulative environmental exposure and long-term respiratory effects.
2. This state-level ecological analysis used Global Burden of Disease (1990–2021) data to examine associations between age-standardised ILD incidence and population-weighted exposure to particulate matter, nitrogen dioxide, and ozone.
3. Air pollution exposure correlated with ILD incidence at the population level, though causality cannot be established; environmental factors should be considered in clinical assessment, alongside the need for individual-level longitudinal research.
INTRODUCTION
Interstitial lung disease (ILD) encompasses a diverse group of pulmonary disorders characterised by inflammation and fibrosis of the lung interstitium. These conditions can lead to significant morbidity and mortality, making understanding their aetiology essential for public health. Recent epidemiological studies have highlighted a rising incidence of ILD in the USA, prompting an investigation into potential risk factors contributing to this trend.1
Emerging evidence implicates air pollution as a significant factor in idiopathic pulmonary fibrosis (IPF) progression, with studies demonstrating that air pollution, particularly fine particulate matter with a diameter of 2.5 µm or less (PM2.5), nitrogen dioxide (NO₂), and ozone (O₃), can exacerbate pre-existing lung conditions and contribute to the development of new respiratory diseases, including ILD.2-6 Specifically, chronic exposure to PM2.5 and NO₂ has been associated with oxidative stress, inflammation, and fibrosis of lung tissues, which are key mechanisms in
the development of ILD.2,3,5 In addition, air pollution exposure has been shown to exacerbate IPF, one of the most common forms of ILD, potentially accelerating its progression.3,5,6
Updated diagnostic guidelines underscore the importance of identifying environmental factors in patients with ILD, including smoking and occupational exposures.7 This retrospective study investigates the association between air pollution and ILD incidence across the USA, analysing data from national health registries and air quality systems. These findings will inform public health policies and strategies to mitigate the impact of environmental factors on lung health.
METHODS
This study is a secondary analysis of data from the Global Burden of Disease (GBD) 2021 study, produced by the Institute for Health Metrics and Evaluation (IHME). Statelevel age-standardised incidence rates of ILD were extracted for all 50 states in the
USA for the period from 1990–2021. ILD incidence included pulmonary sarcoidosis and excluded pneumoconioses and other occupational lung diseases.
Air pollution exposure data were obtained from the GBD database and included Summary Exposure Values (SEV) for PM2.5, NO₂, and O₃. SEVs represent population-weighted exposure metrics that incorporate both pollutant concentration andassociated health risk. To assess spatial concordance, state-level particulate matter SEVs were compared with annual mean PM2.5 concentrations obtained from the USA Environmental Protection Agency (EPA) Air Quality System (AQS).8 EPA data were aggregated to state-level annual means. Strong agreement between datasets supported the use of GBD SEVs for comparative analyses.
Additional air pollution metrics were derived from EPA AQS regulatory monitoring data. These included annual mean PM2.5 concentrations (µg/m³), annual mean NO₂ concentrations (ppb), and warm-season average daily maximum 8-hour ozone concentrations (ppb). These measures were included to improve comparability with prior epidemiologic studies using regulatory air quality data.
Corresponding ICD-9-CM codes (516. xx and 135) were used for earlier years. Pneumoconioses and occupational lung diseases (J60–J65) were excluded to minimise the confounding effect of occupational exposure. Age-standardised incidence rates were calculated using the GBD global reference population. The authors acknowledge that ICD coding can introduce some misclassification error, particularly in distinguishing subtypes of ILD or separating occupational causes. However, given the large-scale, state-level focus of this study, ICD coding remains the most feasible and standardised method for case identification across multiple decades and regions. Age-standardised rates were based on the GBD global reference population.
Associations between ILD incidence and particulate matter exposure were evaluated using population-weighted linear regression models at the state–year level. Models were weighted by state–year incident counts and adjusted for sex composition and calendar year to account for temporal trends.
The datasets used consist of two primary sources: the Air Pollution Dataset and the ILD and Sarcoidosis Incidence Dataset, both containing detailed information spanning several years across all states in the USA. The Air Pollution Dataset includes data on various types of air pollutants, such as PM2.5, NO₂, and O₃. It is structured with fields representing geographical locations, demographic information (age group, sex), the type of pollutant, and the corresponding exposure levels for each year between 1990–2021. The dataset also includes upper and lower CIs, providing a comprehensive understanding of pollution trends over time.
The ILD and Sarcoidosis Incidence Dataset captures incidence rates of ILD and sarcoidosis across the USA, categorised by state, sex, and age group, with data from 1990–2021. Incidence data were expressed as the number of new cases in a year divided by the mid-year population size. This dataset similarly includes key metrics like incidence value and CIs, allowing for regional and demographic analysis of disease prevalence. Combining these datasets allowed the authors to examine for potential correlations between air pollution and respiratory disease incidence across multiple regions and demographics over a multi-decade period.
To interpret this data, several illustrations were created in Tableau™ (Salesforce Inc., San Francisco, California, USA), starting with geographical heat maps. One heat map depicted the distribution of ILD and sarcoidosis incidence across different states in the USA, with colour intensity representing the magnitude of disease incidence. This visualisation effectively highlighted regional trends, enabling a quick visual comparison of disease prevalence across states. Similar geographical heat maps were created to show the distribution of overall pollution levels by state and the distribution of particulate matter levels by state.
A graph depicting the trends in ILD incidence and pollution levels was constructed using longitudinal data. Both variables were plotted on the same timeline to visualise their temporal relationship and assess potential correlations.
Finally, a correlation plot (scatter plot) was produced to examine the relationship between air pollution and disease incidence. This scatter plot displayed the average air pollution values (from 1990–2021) on the X-axis and the average ILD and sarcoidosis incidence rates over the same period on the Y-axis. Each point represented a state, providing a visual comparison of pollution exposure and disease incidence across regions. This method allowed for a structured visual exploration of potential relationships between these variables.
RESULTS
In this study, the authors do not have a specific breakdown of PM2.5 concentrations. Instead, they have aggregated data on ambient particulate matter. The authors will use ambient particulate matter as a surrogate for PM2.5 due to the absence of PM2.5-specific concentration data across all study years. This measure is widely recognised in air quality and public health research to represent outdoor airborne particles, including fine particulate matter.
EPA-reported national mean PM2.5 concentrations showed a strong temporal correlation with GBD-derived SEVs for particulate matter pollution from 2000–2019 (Pearson r=0.98; Spearman r=0.97; p<0.001). Both datasets demonstrated parallel declining trends over time, with reductions in measured PM2.5 closely mirrored by decreases in modelled SEVs. This high degree of concordance supports the validity of GBD exposure estimates.
In population-weighted models adjusting for sex composition and a linear time trend, the association between particulate matter exposure (SEV) and ILD incidence was smaller and not statistically significant.
Air Pollution Exposure
Overall air pollution exposure, summarised using the GBD’s SEV (0–100 scale), varied widely across states in the USA (Figure 1). The highest levels of exposure were observed in California (20.7018), Illinois (20.3971), and the District of Columbia (20.0578), while the lowest exposure levels were reported in Hawaii (4.5844), Maine (5.2061), and Vermont (7.2544).
Air pollution exposure was additionally assessed using regulatory data from the EPA’s AQS. Particulate matter exposure was measured as annual mean PM2.5 concentrations (µg/m³), aggregated at the state level from ground-based monitoring networks. Gaseous pollutants included NO₂, reported as annual mean concentrations (ppb), and O₃, reported as the warm-season average of the daily maximum 8-hour concentration (ppb), consistent with EPA reporting standards. These measures reflect ambient pollutant concentrations rather than population-attributable risk; states with larger populations may exhibit higher SEVs despite lower or moderate longterm ambient concentrations, as SEVs are population-weighted exposure metrics.
Average ILD Incidence by State
The average age-standardised ILD incidence (per 100,000 persons) varied across states in the USA (Figure 2). The highest averages were observed in California (2,062.58 per 100,000), Florida (1,421.38), Texas (1,400.00), and New York (1,273.22), while Wyoming (33.90), Alaska (36.80), and North Dakota (42.30) reported the lowest averages.
Ambient Particulate Matter Exposure
Ambient particulate matter specifically refers to particles in the outdoor air, measured by their SEV. SEV is a composite metric scaled from 0–100 that reflects both the prevalence of exposure in the population and the relative risk associated with that exposure.
The average PM2.5 SEV across states in the USA varies significantly, with the District of Columbia recording the highest PM2.5 SEV at 18.89, followed closely by Georgia (18.72), California (18.48), Illinois (18.21), and Alabama (17.95; Supplementary Figure 1). These elevated SEVs are typically associated with dense urban areas or states with substantial industrial activity, contributing to higher particulate pollution.
States with the lowest average PM2.5 SEV include Hawaii (2.53), Wyoming (3.45), Maine (4.41), Montana (5.88), and North Dakota (5.99).
These lower SEVs are often found in states with fewer urban centres and less industrial presence, leading to better air quality.Overall air quality was summarised using the Air Quality Index (AQI), a
standardised metric derived from EPAreported concentrations of PM2.5, NO₂, O₃, and other criteria pollutants. Statelevel AQI values were averaged annually to reflect population-level exposure. Use of these EPA-based measures along with SEVs improves interpretability, providing clinically and regulatory familiar units, while preserving consistency with global exposure modelling.
Temporal Trends in Pollution Exposure and ILD Incidence
Air pollution exposure declined across most states in the USA between 1990–2021 (Figure 3). Higher pollution levels were observed in earlier years in states such as California, Illinois, and Georgia, with a general downward trend by 2021. In contrast, age-standardised ILD incidence
Units represent SEV unless otherwise specified. Data reflect state-level annual averages from 1990–2021. Seasonal fluctuations are not captured in this dataset, and ecological bias should be considered when interpreting results.
Figure 1: Heat map of the USA depicting state-wise severity of overall air pollution levels.
2: Heat map of the USA depicting state-wise incidence of ILD.
Units represent SEV unless otherwise specified. Data reflect state-level annual averages from 1990–2021. Seasonal fluctuations are not captured in this dataset, and ecological bias should be considered when interpreting results.
increased over the same period across all USA states (Figure 3). California, Texas, and Florida consistently demonstrated the highest incidence rates, with a largely linear increase from 1990–2021.
Correlation Between Air Pollution and ILD Incidence
The correlation chart between average air pollution exposure and ILD incidence demonstrates a positive relationship with a correlation coefficient (r=0.51; Supplementary Figure 2). States in the USA with higher air pollution levels,
such as California, Texas, and New York, also had higher ILD incidence rates.
The line of best fit indicates a trend where states with greater exposure to pollutants tend to report higher ILD incidence.
DISCUSSION
ILD is linked to chronic exposure to air pollutants. Numerous studies highlight the association between air pollutants, such as PM2.5, NO₂, and O₃, and ILD progression. Recent evidence shows the relationship
Figure
Figure 3: Comparative graph of ILD incidence trends and pollution levels (1990–2021).
Units represent SEV unless otherwise specified. Data reflect state-level annual averages from 1990–2021. Air pollution metrics declined over time across states, whereas ILD incidence increased steadily during the study period. Seasonal fluctuations are not captured in this dataset, and ecological bias should be considered when interpreting results.
between air pollution and ILD. For example, a 2023 systematic review synthesised epidemiologic and mechanistic studies and concluded that long-term exposure to fine particulate matter accelerates fibrotic progression in patients with established ILD.9
The divergence between temporal and spatial patterns observed in this study requires careful interpretation. Although national air pollution levels declined over time, spatial analyses showed higher ILD incidence in regions with greater pollution burden. This is compatible with the effects of cumulative or historical exposure, regional variation in pollution levels, and delayed disease manifestation. Increasing ILD incidence over time may reflect population ageing and changes in disease recognition, including greater use of high-resolution CT and evolving diagnostic criteria.
Prior epidemiologic studies support an association between air pollution exposure and ILD incidence and progression. Long-term exposure to fine particulate
matter has been linked to increased risk of IPF and worse clinical outcomes.1,10,11
Experimental studies suggest oxidative stress and inflammatory pathways contribute to fibrotic remodelling.
The role of particulate matter, particularly PM2.5, is central, as it generates reactive oxygen species that lead to oxidative stress, causing inflammation and tissue remodelling, critical factors in the pathogenesis of ILD.2,3,5,6 In a study by Sesé et al.,12 long-term exposure to PM2.5 was found to significantly increase mortality risk, with a hazard ratio of 7.93 per 10 µg/m³. In the authors’ analysis, states in the USA like California and Texas, with higher levels of air pollution and PM2.5, correlate with elevated ILD incidence, aligning with findings that link air pollution to ILD.1-3,5-7,12,13
Mechanisms of Injury:
Oxidative Stress and Epithelial Damage Research has illuminated the specific biological mechanisms by which pollutants
contribute to lung damage in ILD. Superoxide production, prompted by exposure to PM2.5 and other pollutants, damages the epithelial cells lining the respiratory tract, weakening the lung’s structural integrity and facilitating fibrosis.2,14,15 Studies conducted on animal models show that this reactive oxygen species production results in oxidative stress, directly injuring epithelial cells and disrupting the lung barrier, which triggers inflammation and accelerates fibrotic changes.2
Communities with PM2.5 that contain higher concentrations of metals, like nickel, vanadium, and elemental carbon, face higher hospitalisation risks associated with short-term PM exposure, especially among individuals with pre-existing respiratory conditions.16,17 These metals, common in urban and industrial emissions, exacerbate oxidative stress in the lungs, reinforcing the idea that ILD severity and progression can depend on both the quantity and composition of pollutants in the environment.17
Functional Decline and Forced Vital Capacity
Air pollution is not only associated with ILD onset, but also significantly affects disease progression and functional decline.2,11
Forced vital capacity, a critical marker for ILD progression, declines more rapidly in patients exposed to high levels of PM2.5, highlighting the deteriorating effect of pollution on lung function.2,18 This decline in forced vital capacity is especially concerning as it correlates directly with ILD symptom severity and mortality risk, meaning that patients in highly polluted areas face a faster progression of functional impairment.1,2,11 Pollutant exposure has been associated with epithelial injury.2,5
The geographic distribution of ILD incidence aligns somewhat closely with pollution exposure levels, as states in the USA with elevated pollution, such as California, Texas, and New York, show higher rates of ILD. Conversely, states with lower pollution levels, such as Wyoming and Vermont, report comparatively low ILD incidence. However, additional factors like occupational exposures andlifestyle variables influence
these patterns.19 Occupational studies have shown that individuals in industrial settings, particularly those exposed to dust and other pollutants, face elevated ILD risks and accelerated functional decline.19
Global Perspectives on Air Pollution and ILD
After observing a positive correlation between air pollution and ILD incidence in the USA, the authors sought to extend their analysis to countries such as China and India, where air pollution levels are significantly higher. This expansion aimed to explore whether regions with more severe pollution burdens exhibit stronger associations with ILD incidence and to better understand the global implications of air quality on respiratory health.
In China, where industrial emissions dominate, the correlation between air pollution and ILD is high (r=0.98). In India, a combination of industrial pollution and household air pollution, often from burning biomass fuels, drives a strong correlation (r=0.93) with ILD. Pakistan shows similar results (r=0.94), where many homes rely on polluting energy sources, like wood or coal for cooking. Even in Tajikistan, a country with fewer industrial emissions, ambient particulate matter still has a profound impact, showing a correlation of r=0.93 with ILD.
In contrast, the USA exhibits a more muted relationship between air pollution and ILD, largely due to decades of stringent regulatory efforts, such as the Clean Air Act.20 Despite these protections, ILD rates in the USA are still rising. Other factors, including occupational exposures, delayed disease onset, and differences in healthcare access, may contribute to this pattern.
The Paradox of Declining Pollution Versus Rising ILD Incidence
Despite reductions in air pollution from 1990–2021, ILD incidence has steadily risen, a trend that may have multiple explanations.
Delayed disease manifestation
ILD often develops slowly.2 Fibrosis and lung remodelling likely can manifest long
after initial pollutant exposure.12 Individuals exposed to higher pollution levels in previous decades may only now be experiencing symptoms, contributing to the recent rise in ILD incidence despite improved air quality. This latency effect suggests that historical pollution exposure impacts current ILD trends, emphasising the long-term effects of past environmental conditions.
Ageing population
The demographic shift towards an older population likely amplifies ILD incidence, as age-related changes in lung structure and immune function increase susceptibility to fibrosis.11,21 This ageing trend exacerbates the prevalence of ILD in areas with already high pollution levels, highlighting the compounded risk factors of age and environmental exposure in patients with ILD.
Improved diagnostic precision
Advancements in diagnostic tools, especially high-resolution CT, have allowed earlier and more accurate ILD detection.19,22 This increase in diagnostic precision has likely contributed to the rise in reported ILD cases, paralleling trends seen in other chronic conditions where advanced diagnostic technology has revealed previously undetected cases.2
Other environmental/ occupational exposures
Occupational exposures to dust, chemical fumes, and metal pollutants significantly increase the risk of lung injury and fibrosis. A meta-analysis found that 44% of IPF cases had exposure to vapours, gas, dust, and fumes, with a pooled odds ratio (OR) of 1.8 and a population attributable fraction of 21%.23 Another study identified increased IPF risk associated with metal dust (OR: 1.83), wood dust (OR: 1.62), and pesticide exposure (OR: 2.07).19
Public Health and Policy Recommendations
Evidence suggests that reducing air pollution has immediate and long-term benefits for respiratory health, particularly for elderly populations and individuals with chronic lung conditions.11 Community programmes encouraging individuals to
reduce outdoor activities during peak pollution times and use air filtration indoors could also help mitigate exposure-related ILD risks.24
Monitoring long-term trends in both air quality and ILD incidence may help identify emerging risks and inform future research.21 Long-term cohort studies are especially important to monitor individual pollutant exposure and subsequent health outcomes, providing clearer causal links between pollution and ILD.2,18
Limitations and Future Directions
Several limitations should be considered when interpreting these findings. This study used an ecological design based on aggregated, state-level data, and associations observed at the population level may not reflect individual exposure–outcome relationships. Within-state heterogeneity in air pollution exposure, disease burden, and access to healthcare was not captured. Accordingly, the results should be interpreted as population-level patterns rather than individual risk estimates.
State-level estimates of both ILD incidence and air pollution exposure are subject to temporal and spatial variability. Air pollution concentrations vary within states due to differences in urbanisation, industrial activity, meteorological conditions, and monitoring coverage, while ILD incidence may be influenced by regional variation in diagnostic practices and reporting. The use of annual, state-level averages may therefore obscure short-term fluctuations and within-state heterogeneity, potentially resulting in exposure or outcome misclassification. To reduce the impact of episodic events and measurement variability, analyses focused on longterm trends and multi-year averages. The consistency of spatial patterns observed across multiple exposure metrics, including EPA-based particulate and gaseous measures and SEVs, supports the robustness of the population-level findings.
Population-weighted regression models were used to account for differences in state population size and temporal trends. However, there’s a high likelihood of residual confounding given that important individuallevel risk factors for ILD, such as smoking history, occupational and environmental exposures, socioeconomic factors, and access to specialised diagnostic services, were not directly measured and may have contributed to observed spatial and temporal variation in ILD incidence.
This analysis was also limited by the lack of PM2.5-specific concentration data for all study years, necessitating the use of aggregated ambient particulate matter as a proxy. While this approach is widely used in air quality research, it may introduce exposure misclassification.
Finally, the absence of individual-level data and precise geocoding limited the ability to directly link ILD cases to local air pollution exposure. Future studies using finer geographic resolution, geocoded and time-varying exposure data, and detailed clinical phenotyping will be important for clarifying temporal relationships, dose–response patterns, and potential effect modification by age, smoking, and occupational co-exposures.
References
1. Jeganathan N et al. The prevalence and burden of interstitial lung diseases in the USA. ERJ Open Res. 2021;8(1):00630-2021.
2. Johannson KA et al. Air pollution exposure is associated with lower lung function, but not changes in lung function, in patients with idiopathic pulmonary fibrosis. Chest. 2018;154(1):119-25.
3. Mariscal-Aguilar P et al. Air pollution exposure and its effects on idiopathic pulmonary fibrosis: clinical worsening, lung function decline, and radiological deterioration. Front Public Health. 2024;11:1331134.
4. Tahara M et al. Exposure to PM2.5 is a risk factor for acute exacerbation of surgically diagnosed idiopathic pulmonary fibrosis: a case–control study. Respir Res. 2021;DOI:10.1186 /s12931-021-01671-6.
CONCLUSION
This ecological analysis identified a moderate population-level association between air pollution exposure and ILD incidence in the USA (r=0.51). These findings are consistent with prior epidemiologic studies linking chronic exposure to air pollutants with fibrotic lung disease. However, these associations were observed alongside declining national pollution levels over time and should therefore be interpreted cautiously.
The findings likely reflect a combination of cumulative and historical exposure, regional heterogeneity in pollution burden, population ageing, and changes in diagnostic practices rather than a direct causal relationship. Also, unmeasured factors, such as smoking history, occupational exposures, and socioeconomic differences, may have contributed to the observed variation in ILD incidence across states.
While causality cannot be inferred from this ecological design, the results suggest that geographic differences in air pollution exposure remain relevant to ILD burden at the population level. Further studies incorporating individual-level exposure assessment, finer geographic resolution, and longitudinal follow-up are needed to clarify the role of air pollution in ILD development and progression.
5. Harari S et al. Fibrotic interstitial lung diseases and air pollution: a systematic literature review. Eur Respir Rev. 2020;29(157):200093.
6. Liang L et al. Air pollution and hospitalization of patients with idiopathic pulmonary fibrosis in Beijing: a time-series study. Respir Res. 2022; DOI:10.1186/s12931-022-01998-8.
7. Kim Y, Radoias V. Severe air pollution exposure and long-term health outcomes. Int J Environ Res Public Health. 2022;19(21):14019.
8. U.S. Environmental Protection Agency. Air Quality System Data Mart [Internet database]. Available at: https://www. epa.gov/aqs. Last accessed: 1 October 2025.
10. Conti S et al. Air pollution exposure and risk of idiopathic pulmonary fibrosis.Eur Respir J. 2020;56(2):2000124.
11. Winterbottom CJ et al. Exposure to ambient particulate matter is associated with accelerated functional decline in idiopathic pulmonary fibrosis. Chest. 2018;153(5):1221-8.
12. Sesé L et al. Role of atmospheric pollution on the natural history of idiopathic pulmonary fibrosis. Thorax. 2018;73(2):145-50.
13. Di Q et al. Air pollution and mortality in the medicare population. N Engl J Med. 2017;376(26):2513-22.
9. GBD 2019 Chronic Respiratory Diseases Collaborators. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the Global Burden of Disease Study 2019. EClinicalMedicine. 2023;59:101936.
14. Liu J et al. Particulate matter disrupts airway epithelial barrier via oxidative stress to promote Pseudomonas aeruginosa infection. J Thorac Dis. 2019;11(6):2617-27.
15. Xuedi Z et al. PM2.5 induces inflammatory responses via oxidative stress-mediated mitophagy in human bronchial epithelial cells. Toxicol Res. 2022;11(1):195-205.
16. Bell ML et al. Hospital admissions and chemical composition of fine particle air pollution. Am J Respir Crit Care Med. 2009;179(12):1115-20.
17. Thangavel P et al. Recent insights into particulate matter (pm2.5)-mediated toxicity in humans: an overview. Int J Environ Res. Public Health. 2022;19:7511.
18. Pope CA III . Fine-particulate air pollution and life expectancy in
the United States. N Engl J Med. 2009;360(4):376-86.
19. Park Y et al. Occupational and environmental risk factors of idiopathic pulmonary fibrosis: a systematic review and meta-analyses. Sci Rep. 2021;11(1):4318.
20. Greenbaum DS. The Clean Air Act: substantial success and the challenges ahead. Ann Am Thorac Soc. 2018;15(3):296-7.
21. Dominici F et al. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA. 2006;295(10): 1127-34.
22. Hovinga M et al. CT Imaging of interstitial lung diseases. Multidetector-Row CT of the Thorax. 2016;27:105–30.
23. Gandhi SA et al. The impact of occupational exposures on the risk of idiopathic pulmonary fibrosis: a systematic review and meta-analysis. Ann Am Thorac Soc. 2024;21(3): 486-98.
24. Yoon HY et al. Effects of indoor air pollution on clinical outcomes in patients with interstitial lung disease: protocol of a multicentre prospective observational study. BMJ Open Respir Res. 2024;11(1):e002053.
Overcoming Dual Hypersensitivity to Carboplatin and Paclitaxel in Advanced Ovarian Cancer: A Case Report
Authors: *Intissar Belrhali,1,2 Oumaima lamsyah,1,2 Stephane Ruck,2 Sarah Naciri,1 Hanane Inrhaoun,1 Hind El Yacoubi,1 Salma Najem,1 Siham Lkhoyaali,1 Ibrahim El Ghissassi,1 Hind Mrabti,1 Hassan Errihani1
1. Department of Oncology, National Institute of Oncology, Rabat, Morocco
2. Department of Medical Oncology, Emile Durkheim Hospital Center, Épinal, France
*Correspondence to intissarbelrhali90@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank the patient and her family for their trust and cooperation. The authors also acknowledge the medical and nursing staff of the Department of Oncology for their invaluable support in patient care and data collection.
Disclaimer: This case report describes the clinical course of a single patient. According to institutional policies, ethics committee approval was not required. Written informed consent for publication of the case details and accompanying clinical image was obtained from the patient.
Background: Carboplatin and paclitaxel are standard first-line therapies for advanced ovarian cancer, but hypersensitivity reactions (HSR) may compromise treatment, especially when involving both agents.
Case report: A 71-year-old woman with Stage IIIC ovarian carcinoma and no comorbidities developed sequential HSRs to carboplatin and paclitaxel. After carboplatin, she experienced a delayed generalised maculopapular rash at 24 hours. During paclitaxel infusion, she developed acute chest tightness and desaturation to 85%. Allergy testing (prick, intradermal, patch) was initially equivocal but subsequently negative. Management included corticosteroid/antihistamine premedication, prolonged carboplatin infusion, and a seven-step paclitaxel desensitisation protocol. The patient successfully completed six chemotherapy cycles.
Conclusion: This case emphasises the importance of multidisciplinary collaboration and personalised strategies to ensure continuity of effective oncologic treatment despite HSRs.
Key Points
1. Hypersensitivity reactions to carboplatin and paclitaxel are recognised complications in advanced ovarian cancer and may threaten continuation of first-line chemotherapy.
2. This case report describes sequential hypersensitivity to both agents in a single patient and outlines the diagnostic evaluation and multidisciplinary management approach implemented.
3. Individualised premedication, infusion adjustment, and structured desensitisation protocols can enable safe chemotherapy continuation without compromising short-term oncologic control.
INTRODUCTION
Carboplatin and paclitaxel remain the cornerstone of first-line chemotherapy for advanced ovarian cancer, as recommended by international guidelines, with wellestablished efficacy and survival benefits.1 However, hypersensitivity reactions (HSR) to these agents present a major clinical challenge, sometimes leading to treatment discontinuation and compromising therapeutic efficacy.2
Carboplatin HSRs are typically delayed and may appear after several cycles, often manifesting as cutaneous eruptions or, less frequently, systemic reactions.3 Paclitaxel HSRs, in contrast, usually occur during the first or second infusion, are often non-IgE mediated, and are related to polyoxyl 35 castor oil.4 Dual hypersensitivity to both carboplatin and paclitaxel is uncommon, but represents a critical barrier to treatment continuity.
This case is unique in that it demonstrates sequential hypersensitivity to both carboplatin and paclitaxel in the same patient, managed successfully through a multidisciplinary collaboration between oncologists and allergologists. It highlights the importance of repeated allergy testing, premedication, infusion adjustment, and desensitisation protocols in enabling completion of therapy.
CASE PRESENTATION
A 71-year-old woman with no significant past medical history was diagnosed with Stage IIIC ovarian carcinoma. She was
started on first-line chemotherapy with carboplatin and paclitaxel according to international guidelines.
Carboplatin Reaction
During the second cycle, approximately 24 hours after carboplatin infusion, the patient developed a diffuse maculopapular rash predominantly affecting the thighs and lower limbs. The eruption was pruritic but without mucosal involvement or systemic features, such as fever, dyspnoea, or haemodynamic instability. The lesions resolved with topical corticosteroid treatment within a few days (Figure 1).
Given the suspicion of carboplatin hypersensitivity, the patient underwent allergological testing. The first series included skin prick, intradermal, and patch testing for carboplatin, paclitaxel, and premedication drugs. Results showed a doubtful intradermal reaction to carboplatin at 72 hours. A second series of tests, performed at a distance from the reaction, was completely negative.
Carboplatin was subsequently reintroduced under systematic premedication with intravenous corticosteroids and antihistamines, combined with a prolonged infusion protocol. Under these conditions, treatment was continued with only mild erythematous reactions, without recurrence of generalised rash.
Paclitaxel Reaction
At Cycle 3 (Day 15), during paclitaxel infusion, the patient developed acute chest tightness and oxygen desaturation to 85%.
BAIn addition, she presented with a diffuse erythematous rash involving the abdomen and thighs (Figure 2). The infusion was immediately interrupted, and intravenous corticosteroids and antihistamines were administered, resulting in rapid improvement.
Given the importance of maintaining paclitaxel in the regimen, a seven-step desensitisation protocol over 5 hours was initiated. The patient tolerated this
approach well and was able to complete paclitaxel administration without recurrence of severe reactions.
Outcome
Through close multidisciplinary collaboration between oncologists and allergologists, the patient successfully completed six cycles of carboplatin–paclitaxel chemotherapy. No anaphylactic events occurred, and clinical
Figure 1: Delayed cutaneous hypersensitivity reaction after carboplatin infusion.
A) Maculopapular rash on the thigh. B) Diffuse erythematous eruption with confluent macules and papules.
Figure 2: Diffuse erythematous rash involving the abdomen and thighs during paclitaxel infusion, consistent with acute hypersensitivity reaction.
and radiological follow-up during treatment did not raise concern for early disease progression, suggesting that continuation of chemotherapy through desensitisation did not appear to compromise short-term oncologic control.
A detailed summary of clinical events, diagnostic investigations, and management strategies is presented in Table 1.
DISCUSSION
HSRs to platinum compounds occur in up to 27% of patients with ovarian cancer, especially after multiple cycles.3 They are usually mediated by delayedtype hypersensitivity mechanisms, with clinical manifestations ranging from mild rash to severe systemic reactions.5 In the patient, carboplatin induced a generalised maculopapular eruption within 24 hours, consistent with a delayed reaction. Although
Table 1: Timeline of hypersensitivity management during first-line chemotherapy with carboplatin–paclitaxel in a 71-year-old woman with Stage IIIC ovarian carcinoma.
Month 1
Month 2 (Cycle 2)
Month 2 (Allergy testing #1)
Month 3 (Cycle 3, Day 15)
Month 3 (Allergy testing #2)
Month 3–Month 6 (Cycles 4–6)
Cycle 1 carboplatin–paclitaxel Well tolerated, no toxicity
Cycle 2 carboplatin
Allergy testing #1
Cycle 3 paclitaxel
Allergy testing #2
Cycles 4–6
Generalised maculopapular rash at 24h
Doubtful carboplatin intradermal reaction (72h)
Chest tightness, SpO₂ 85%
Completely negative for carboplatin/paclitaxel
Mild erythema only, no severe reaction
Clinical events, interventions, and outcomes are summarised.
allergy testing showed an equivocal intradermal result initially, a repeat test later returned negative, underlining the variability and limitations of diagnostic tools in nonIgE-mediated reactions.6
Several risk factors have been associated with HSRs to platinum agents and taxanes, including repeated exposure, cumulative dose, a history of atopy or drug allergy, and prolonged platinum-free intervals. Awareness of these factors may help identify patients at higher risk and guide closer monitoring during subsequent cycles. These observations have been highlighted in recent analyses of chemotherapyassociated HSRs.7
Paclitaxel-related HSRs are reported in 10–30% of patients, with severe reactions in 2–5%.4 These reactions are mostly attributed to polyoxyl 35 castor oil, which triggers mast cell activation through a nonIgE-mediated pathway.8 In this case, the patient developed acute chest tightness and desaturation during infusion, which was
Topical corticosteroids
Resolution in a few days
Skin prick, intradermal, patch tests Equivocal result
rapidly reversed after stopping the drug and administering corticosteroids.
Management of chemotherapy-induced HSRs requires a tailored, multidisciplinary approach. Premedication with corticosteroids and antihistamines reduces the incidence of paclitaxel HSRs, while prolonged infusion protocols can minimise carboplatin toxicity.9,10 Desensitisation, performed through gradual reintroduction in multiple steps, has shown high success rates for both carboplatin and paclitaxel.11 In the authors’ patient, a sevenstep paclitaxel desensitisation protocol allowed treatment continuation without recurrence of severe events.
Experience from breast cancer treatment has significantly contributed to the development and validation of desensitisation protocols, particularly for taxane-based regimens. Structured multi-step protocols have enabled many patients with prior HSRs to safely continue first-line therapy without compromising treatment intensity. Lessons from these
settings support the broader applicability of desensitisation strategies across solid tumours, including ovarian cancer.12
An important clinical consideration in patients requiring desensitisation is whether modification of infusion protocols may compromise oncologic efficacy. In this case, continuation of carboplatin and paclitaxel using premedication, prolonged infusion, and a structured desensitisation protocol allowed completion of the planned firstline regimen. Although a formal Response Evaluation Criteria in Solid Tumors (RECIST) response assessment was not the primary objective of this report, no early clinical or radiological signs of progression were observed during treatment. Long-term outcomes, such as progression-free and overall survival, could not be assessed due to the limited follow-up period, which represents an inherent limitation of singlepatient case reports.
The strength of this case lies in the demonstration that, even in the presence of dual hypersensitivity, therapeutic efficacy can be preserved through multidisciplinary management. The main limitation is the absence of confirmatory biomarkers for predicting reactions, emphasising the need for clinical vigilance and individualised strategies.
References
1. Colombo N et al. ESMO–ESGO consensus conference recommendations on ovarian cancer: pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Ann Oncol. 2019;30(5):672-705.
2. Castells M. Hypersensitivity to antineoplastic agents. Curr Pharm Des. 2008;14(27):2892-901.
3. Polyzos A et al. Hypersensitivity reactions to carboplatin administration are common but not always severe: a 10-year experience. Oncology. 2001;61(2):129-33.
4. Weiss RB et al. Hypersensitivity reactions from taxol. J Clin Oncol. 1990;8(7):1263-8.
Take-Away Lesson
Negative allergy tests do not exclude clinical hypersensitivity. Personalised premedication, infusion adjustment, and desensitisation, supported by close oncologist–allergologist collaboration, are essential to ensure both safety and oncologic efficacy in patients with complex chemotherapy-induced HSRs.
CONCLUSION
This case highlights the clinical challenges of managing hypersensitivity reactions to both carboplatin and paclitaxel in advanced ovarian cancer. Despite negative allergy tests, the patient developed reproducible reactions, emphasising that diagnostic tools may not fully predict clinical risk. Through a multidisciplinary approach involving oncologists and allergologists, the use of premedication, prolonged infusion, and desensitisation protocols enabled safe continuation and completion of six chemotherapy cycles. The main take-away message is that individualised strategies and close collaboration across specialties are essential to preserve oncologic efficacy, while ensuring patient safety in the context of complex chemotherapy-induced HSRs.
5. Markman M. Hypersensitivity reactions to carboplatin. Gynecol Oncol. 2002;84(2):353-4.
6. Caiado J et al. Carboplatin-, oxaliplatin-, and cisplatin-specific IgE: cross-reactivity and value in the diagnosis of immediate hypersensitivity reactions. J Allergy Clin Immunol Pract. 2013;1(6):494-500.
7. Tsao LR et al. Hypersensitivity reactions to platinum agents and taxanes: epidemiology, mechanisms, and management. Clin Rev Allergy Immunol. 2022;62(3):432-48.
8. Szebeni J. Complement activationrelated pseudoallergy: a stress reaction in blood triggered by nanomedicines and biologicals. Mol Immunol. 2014;61(2):163-73.
9. Lopez-Gonzalez P et al. Assessment of antihistamines and corticosteroids as premedication in rapid drug desensitization to paclitaxel: Outcomes in 155 Procedures. J Allergy Clin Immunol Pract. 2018;6(4):1356-62.
10. Zanotti KM, Markman M. Prevention and management of antineoplasticinduced hypersensitivity reactions. Drug Saf. 2001;24(10):767-79.
11. Castells MC et al. Hypersensitivity reactions to chemotherapy: outcomes and safety of rapid desensitization in 413 cases. J Allergy Clin Immunol. 2008;122(3):574-80.
12. HJ Park et al. Personalized risk assessment for taxane-induced hypersensitivity reactions: a systematic review and meta-analysis. J Pers Med. 2024;15(1):2.