Personalized Prognostics: Can Genomic Testing Improve Your Melanoma Management?
Congress Review
12 Advances in Dermatologic Research and Treatment: A Year in Review from the 2025 AAD Annual Meeting
McGrath et al.
Congress Features
16 Advances in JAK Inhibitors for Atopic Dermatitis: Insights from the 2025 AAD Annual Meeting
Leath et al.
20 Updates on Melanoma and Melanocytic Neoplasms from the 2025 AAD Annual Meeting
McGrath et al.
23 Insights on the Intersection of Climate Change, Air Pollution, and Dermatology at the AAD 2025 Annual Meeting Sharma Abstract Reviews
27 Efficacy of Intralesional Vitamin D3 for Treatment of Verruca Vulgaris: A Randomized Control Study
Shah et al.
29 Key Determinants of Aggravation and Therapeutic Resistance in Pediatric Atopic Dermatitis
Essadeq et al.
30 Scarring Alopecias in a Pediatric Trichology Clinic at a Tertiary Care Center
Lima-Galindo et al.
32 Skin Concerns and Knowledge of Cosmetic Procedures in Skin of Color
Hartoyo et al.
34 Ethics of Treating Actinic Keratosis in Patients of Advanced Age
Wahood et al.
35 Acrocyanosis After Immunotherapy: Vasculitis or Vasculopathy?
Lytvyn et al. Congress
53 Editor's Pick: Real-World Use of Bimekizumab Therapy in Patients with Difficult-to-Treat Plaque Psoriasis: A Retrospective Analysis from a Large Academic Center
Hren et al.
60 Nail Psoriasis: A Narrative Review of Manifestations, Diagnosis, and Management
Yorulmaz
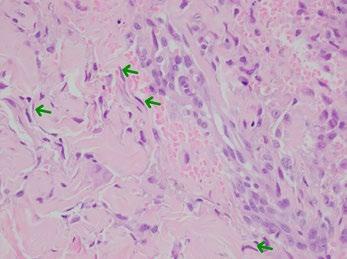
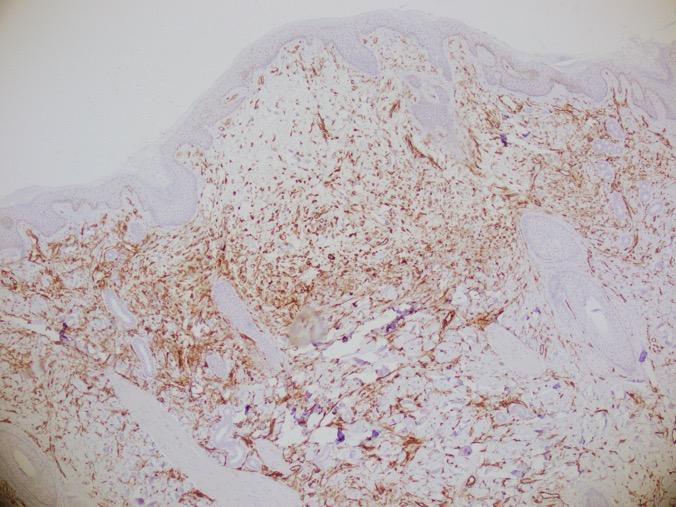
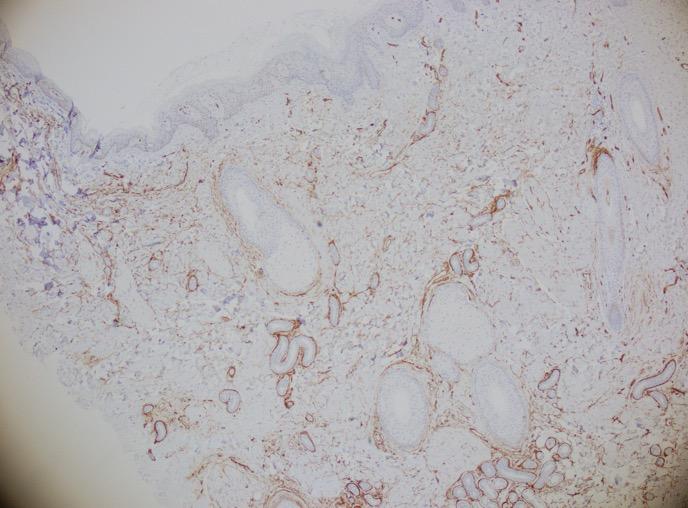
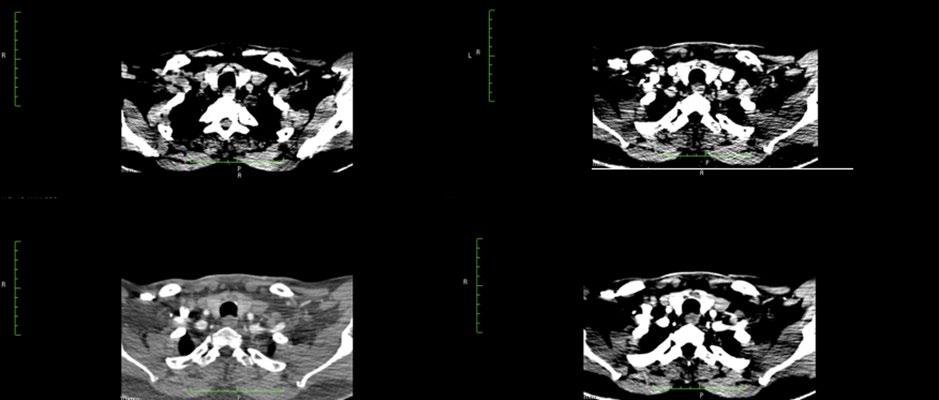
66 Malignancy Unmasked: Cutaneous Angiosarcoma Arising From Scald Burn: A Case Report
Priela et al.
Editorial Board
Editor-in-Chief
Dr Michael Gold
Gold Skin Care Center; Tennessee Clinical Research Center, Tennessee, USA
Dr Todd Schlesinger
Clinical Research Center of the Carolinas, South Carolina, USA
Dr Neal Bhatia
Therapeutics Clinical Research, California, USA
Dr Jacqueline Watchmaker
U.S. Dermatology Partners, Arizona, USA
Dr Brian Hibler
Dermatologist, Private Practice, New York, USA
Dr Leon Kircik
Indiana University Medical Center, Icahn School of Medicine at Mount Sinai Medical Center, New York, USA
Dr Raj Chovatiya
Rosalind Franklin University Chicago Medical School; Center for Medical Dermatoloy and Immunology Research, Illinois, USA
Aims and Scope
AMJ Dermatology is an open access, peer-reviewed eJournal committed to helping elevate the quality of healthcare for skin, hair, and nail diseases. AMJ Dermatology endeavours to increase knowledge, stimulate discussion, and contribute to a better understanding of these conditions.
The journal is published annually, 6 weeks after the American Academy of Dermatology (AAD) Annual Meeting, and features highlights from this event, alongside interviews with experts in the field, reviews of abstracts presented at the event, and indepth features on congress sessions. The journal also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the inhouse Editorial team.
AMJ Dermatology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field, and broaden readers’ professional interests. The journal is managed by a dedicated Editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copyediting, and ensures timely publication.
AMJ endeavours to increase knowledge, stimulate discussion, and contribute to the delivery of world-class updates in the clinical realm. We do not publish veterinary science papers or laboratory studies that are not linked to patient outcomes. Further details on coverage can be found here: www.emjreviews.com/en-us/amj/.
Editorial Expertise
AMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial Team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
• A team of internal and independent medical writers.
Peer Review
Every review article, case report, feature, and research article published in AMJ Dermatology undergoes peer review by at least two independent experts.
On submission, all manuscripts are assessed and undergo a technical check by the AMJ Editorial staff to determine their suitability for the journal and appropriateness for peer review. Editorial staff identify appropriate reviewers who are selected based on their specialist knowledge in the relevant area. All peer review is double-blind.
Following review, manuscripts are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff are responsible for ensuring that necessary amendments to the manuscript have been made, with input from our Editorial Board or the original reviewers where necessary. The Editor of AMJ has final discretion over any proposed amendments. Manuscripts authored by members of the
Editorial Board are subjected to the same double-blind process. Short opinion pieces are published following internal review and publication is at the discretion of the Editor. Congress-related content sponsored or funded by our industry partners undergoes quality control checks independently. Industry-supported content that falls into any of the categories that are eligible for peer review, undergoes the same peer review process.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in dermatology and accept original research, review articles, case reports, and features.
To discuss potential submissions, please email: editorial@americanmedicaljournal.com
To submit a paper, use our online submission site: emj.kriyadocs.com/submissions/submit/emj/emj/login.
Submission details can be found through our website: www.emjreviews.com/en-us/amj/contributors/authors/.
Reprints
All articles included in AMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
AMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®
AMJ is available through the websites of our leading partners and collaborating societies. AMJ publications are all available via our website: www.emjreviews.com/en-us/amj/.
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey White
Designers
Shanjok Gurung, Owen Silcox, Fabio van Paris
Creative Artworker
Dillon Benn Grove
Head of Marketing
Stephanie Corbett
Vice President of Customer Success
Alexander Skedd
Senior Vice President of Business Development
Robert Hancox
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and CEO
Spencer Gore
Contact us
Welcome
Dear Readers,
Welcome to the latest issue of AMJ Dermatology. In this publication, we present expert-led coverage from the American Academy of Dermatology (AAD) Annual Meeting 2025 along with topical articles and interviews framing this defining moment in dermatology.
The rapid expansion of AI sees dermatology research and care moving at a great pace, deemed as a “new era”;1 yet the question remains, how long has this so-called revolution been underway? Perhaps what we are witnessing is not the beginning, but the visible wave of a revolution that has been evolving for decades.
Hospitals in the U.S. are incorporating AI into their health services at a much higher rate than ever before,2 and dermatology is an early adopter of this. This disruptive surge is both game-changing and life-changing: machine learning detects, manages, and triages skin conditions, while freeing up physicians’ time and reducing strain on hospital capacity and waiting lists.
It’s the combination of human and technology that will be the real revolution. Like the human eye, technology is not foolproof. The opportunity is to combine AI into clinical practice in an intentional, responsible way.
Beyond AI, this issue provides a platform for discourse on other major topics at the forefront of innovation, including the impact of air pollution and our changing climate on dermatologic disease, updates on melanoma and melanocytic neoplasms, and JAK inhibitors for atopic dermatitis.
I would like to extend my personal thanks to our Editor-in-Chief Michael Gold, our Editorial Board, peer reviewers, and the Editorial Team for their support in producing this publication and helping realize our vision of elevating the quality of healthcare globally.
Permissions and copyright: accountsreceivable@emjreviews.com
1. The Times. 2025. Available at: https://www. thetimes.com/uk/healthcare/article/globalfirst-as-nhs-hospital-uses-ai-for-instant-skincancer-checks-3clspdmk0. Last accessed: April 4 2025.
2. Baten RAB. Health Aff Sch. 2024;2(10):qxae123.
Anaya Malik Vice President of Content
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
We provoke conversation around healthcare trends and innovation - we also create engaging educational content for healthcare professionals. Join us for regular conversations with physician & entrepreneur, Jonathan Sackier. Listen Now
Foreword
Dear Colleagues,
The AMJ Dermatology journal is a wonderful “recap” of the most important sessions from the recently held American Academy of Dermatology (AAD) Annual Meeting held at the beginning of March 2025 in Orlando, Florida.
With approximately 20,000 attendees, the AAD provides a full and comprehensive look at the recent trends in dermatology, both from a medical and aesthetic point of view. The varied topics and presentations highlight the impressive growth in our understanding of complex skin diseases as we dive into their pathogenesis, allowing us to use targeted therapies, which, in many cases, are changing lives and allowing us to treat our patients safely and effectively.
The AMJ Dermatology journal reviews and summarizes the most important sessions, concepts, and therapies learned at the AAD 2025. Our commentary includes expertled updates in JAK inhibitors for atopic dermatitis, advances in melanoma and melanocytic neoplasms, and reviews from award-winning abstract authors.
The AAD provides a full and comprehensive look at the recent trends in dermatology, both from a medical and aesthetic point of view
Insights, discussions, and meaningful articles allow us to understand how dermatology and dermatologic therapy are exploding in 2025. Also included are interviews with amazing key opinion leaders, teaching us more about what is here now and what we can look forward to in the future.
We are at a novel yet wonderful “age” in dermatology, and we hope that everyone continues the quest for learning with the desire to bring better treatments and outcomes for our patients.
Michael Gold
Gold Skin Care Center, Nashville, Tennessee, USA
Personalized Prognostics: Can Genomic Testing Improve
What is DecisionDx-Melanoma (31-GEP)?
GEP test designed for patients diagnosed with Stage I-III melanoma1
It evaluates the expression of 31 genes to provide a personalized risk assessment for:
• SLN positivity1
• Melanoma recurrence1
The test is integrated with clinicopathologic data for an optimized, personalized risk of recurrence (i31-ROR) and likelihood of SLNB positivity (i31-SLNB)2
Implementation of 31-GEP testing ensures that high-risk patients receive appropriate care.
Optimizing clinic visits and follow-up care for improved patient management
Guiding referrals to surgical oncologists
Identifying low-risk patients who may not need intensive follow-up
What makes 31-GEP testing unique?
Extensive independent validation
It is one of the most validated melanoma prognostic tests, supported by:1,3,9,16
• >50 peer-reviewed studies
• Data from over 10,000 patients
Supporting decision-making regarding SLN biopsies
oncologists7,9,15 Reducing unnecessary surgical procedures by identifying patients with <5% SLN positivity risk
Identifying high-risk SLN-negative patients who may benefit from routine imaging to detect recurrence early
The test at the molecular patients into clinicians management
1. Ferris LK et al. J Am Acad Dermatol. 2017;76(5):818-25.e3. 2. Jarell A et al. J Am Acad Dermatol. 2022;87(6):1312-20. 3. Hsueh EC et al. JCO Precis Oncol. 2021;5:PO.20.00119. 4. Gastman BR et al. J Am Acad Dermatol. 2019;80(1):149-57.e4. 5. Gerami P et al. J Am Acad Dermatol. 2015;72(5):780-5.e3. 6. Bailey CN et al. JCO Precis Oncol. 2023;7:e2300044.
7. Zager JS et al. BMC Cancer. 2018;18(1):130.
Comprehensive, actionable risk prediction
The independently validated 31-GEP score is integrated with clinicopathologic features through two proprietary algorithms to inform:
• SLN positivity (i31-SLNB): 31-GEP score combined with age, ulceration, Breslow thickness, and mitotic rate11,17
• Risk of recurrence (i31-ROR): 31-GEP score combined with age, ulceration, Breslow thickness, mitotic rate, SLN status, and tumor location2,18
8. Jarell A et al. Future Oncol. 2021;17(36):5023-31.
9. Farberg AS et al. Dermatol Ther (Heidelb). 2022;12(4):807-23.
10. Mulder EEAP et al. Br J Dermatol. 2021;184(5):944-51.
11. Whitman ED et al. JCO Precis Oncol. 2021;5:PO.21.00162.
12. Glazer et al. J of Skin. 2022;6:474-81.
13. Guenther JM et al. World J Surg Oncol. 2025;23(1):5.
14. Guenther JM et al. (In press). A prospective, multicenter
Proven clinical impact
It is the only melanoma test associated with improved patient survival:6,16
• MSS4,7,8
• RFS4,7,8
• DMFS4,7,8
• OS6,11
analysis of recurrence-free survival after sentinel lymph node biopsy decisions influenced by the 31-GEP. Cancer Medicine.
15. Dhillon S et al. Arch Dermatol Res. 2023;315(8):2295-302.
16. Durgham RA et al. Cancers (Basel). 2024;16(21):3714.
17. Tassavor M et al. Anticancer Res. 2023;43(10):4511-6.
18. Pariser D at al. SKIN J Cutan Med. 2024;8(2):s386.
Provides personalized risk assessment for melanoma patients through molecular-level tumor analysis, supported by extensive clinical evidence from over 10,000 patients across 50+ peer-reviewed studies.1,3,9,16
Abbreviations
Studies show improved risk stratification of patients with early-stage melanoma compared to AJCC alone.1-5,8
Real-world data indicate that using the test in clinical decision-making improves patient survival.6
Routine imaging guided by 31-GEP results in earlier detection of melanoma.15
Improves clinical decision-making by helping physicians identify appropriate candidates for SLNB and enabling early interventions for high-risk patients.1,7,9,15
Demonstrates real-world impact on patient survival through better risk stratification and optimized treatment planning, making it the only melanoma test with proven survival benefits.4,6-8,11,16
At the 2025 American Academy of Dermatology (AAD) Annual Meeting, Adela Rambi Cardones and Kevin Wang led a session highlighting top basic science and clinical dermatology literature. Topics included Merkel cell carcinoma surveillance, monkeypox, Trichophyton mentagrophytes genotype VII, bimekizumab for hidradenitis suppurativa (HS), spatial proteomics for drug target discovery, and atopic dermatitis (AD).1
MERKEL CELL CARCINOMA
Circulating tumor DNA (ctDNA), consisting of fragments of mutated DNA from brokendown tumor cells, can be detected in the blood and serves as a biomarker for Merkel cell carcinoma recurrence. A study involving 319 patients found that ctDNA levels in the blood were both sensitive (>93%) and specific (>85%) in detecting clinically evident disease, which was defined as evidence of Merkel cell carcinoma on imaging or physical exam. Patients with higher ctDNA
levels at any time during tumor surveillance (median follow-up time of 267 days) had a significantly increased risk of recurrence even after controlling for other factors, such as stage and immunosuppression. Higher ctDNA levels also correlated with increased tumor size.2 The study’s findings suggest ctDNA testing can be used to assist in detecting Merkel cell carcinoma recurrence, though additional studies are needed to determine if the test can improve diseasespecific survival.
MONKEYPOX
A global outbreak of Clade II monkeypox (Mpox) occurred in 2022, while an outbreak of Clade I Mpox has been ongoing in the Democratic Republic of the Congo since 2023. Clade I Mpox is associated with a higher fatality rate. The first case of Clade I Mpox in North America was observed in a US citizen that had recently traveled to East Africa. Upon returning home, he developed unilateral inguinal lymphadenopathy, fever, headache, and pustular lesions on his trunk and extremities. Of note, the patient reported
no sexual activity during his travel. His overall disease course was mild, and JYNNEOS (Bavarian Nordic, Copenhagen, Denmark) post-exposure prophylaxis was administered to his housemate and travel companions.3 When the characteristic rash is present, physicians should consider the possibility of Clade I Mpox in those returning from endemic African regions, even without a stated history of sexual activity. They should also recognize that Clade I MPox can have a more severe disease course, though this was not observed in this particular case.
TRICHOPHYTON MENTAGROPHYTES GENOTYPE VII
A newly emerging dermatophyte, Trichophyton mentagrophytes genotype VII, has been identified, primarily affecting immunocompetent men who have sex with men in New York City. It presents as annular, scaly plaques on the face, trunk, groin, and genitals, sometimes accompanied by pustules and nodules. Diagnosis requires culture and sequencing for proper identification. Unlike many other
tinea infections, oral antifungals are typically needed for treatment (e.g. terbinafine 250 mg daily for 3 months). Another emerging dermatophyte stemming from South Asia is Trichophyton indotineae. This dermatophyte is often resistant to standard clinical doses of terbinafine and may require higher doses or treatment with another antifungal, such as griseofulvin. The AAD has provided guidance on sending samples for further testing.4
HIDRADENITIS SUPPURATIVA
The current US FDA approved biologic treatments for HS include adalimumab, secukimumab, and bimekizumab. The IL-17 pathway plays a role in both the acute and chronic phases of HS, and targeting both phases is important for disease resolution. Bimekizumab is the newest FDA-approved biologic on the market for HS, with the unique ability to bind to all IL-17 homo- and heterodimers, specifically IL-17A and IL-17F. A 16-week study examining the efficacy of bimekizumab in moderate-to-severe HS demonstrated that roughly half of patients on therapy achieved at least a 50% reduction in the number of abscesses and inflammatory nodules compared to baseline, with these clinically meaningful responses being rapid and sustained.5 There are no head-to-head studies available to evaluate the efficacy of bimekizumab compared to the other approved HS biologics. Additional studies are needed to identify new targets for HS therapeutics, as not all patients have an adequate response to TNF-α or IL-17 inhibitors.
BASIC SCIENCE: SPATIAL PROTEOMICS
Spatial proteomics uses AI-driven tools to map protein expression within tissues, helping identify new drug targets and advance precision medicine. The process involves using immunohistochemistry to stain tissues for all available protein markers, followed by computational separation of cells based on their protein profiles with the
assistance of mass spectrometry. By understanding which cell types express which proteins, scientists can gain a better understanding of the disease pathophysiology at a molecular level.6
The utility of spatial proteomics in dermatology is already being seen in toxic epidermal necrolysis (TEN), a severe drug-induced T cell-mediated hyperinflammatory condition. To date, there is a paucity of large-scale trials evaluating the efficacy of commonly used TEN treatments, in large part due to the condition’s rarity and rapid progression. To develop a more targeted therapy approach, researchers used spatial proteomics to determine the protein expression within tissue affected by TEN. They found that levels of phosphorylated STAT1 and IFN I and II were significantly elevated. Since JAK inhibitors are known to reduce interferon signaling through the JAK/STAT pathway, researchers decided to utilize this drug as a new therapy for TEN. A recent study examining the efficacy of acute dosing of abrocitinib (200 mg followed by 100 mg) for TEN displayed promising results, with all seven patients treated experiencing at least 95% re-epithelialization.6 However, more research is needed to determine whether JAK inhibitors are efficacious across various TEN molecular profiles, and head-tohead trials will be needed to determine if they can reduce mortality relative to more longstanding therapies.
Management of AD continues to evolve, with topical JAK inhibitors emerging as a potential treatment; however, misinformation from non-dermatology specialties has led to confusion in treatment recommendations
ATOPIC DERMATITIS
Management of AD continues to evolve, with topical JAK inhibitors emerging as a potential treatment; however, misinformation from nondermatology specialties has led to confusion in treatment recommendations.7 There are concerns regarding the frequency of topical steroid use, with allergists and immunologists recommending once-daily application, while dermatologists recommend twice-daily use. Additionally, bleach baths are beneficial for all cases of atopic dermatitis and should not be restricted to only severe cases, despite incorrect guidance from non-dermatology
References
1. Cardones ARG, Wang KC. Year-inReview: notable articles from basic and clinical sciences literature. AAD, March 7, 2025.
2. Akaike T et al. Circulating tumor DNA assay detects Merkel cell carcinoma recurrence, disease progression, and minimal residual disease: surveillance and prognostic implications. J Clin Oncol. 2024;42(26):3151-61.
3. Bekele SG et al. Knowledge of human monkeypox virus infection among
specialists. Allergists and immunologists have also advised against the use of systemic treatments such as methotrexate, cyclosporine, and mycophenolate mofetil, despite lacking the evidence or expertise to make these recommendations. Dermatologists must reclaim primary decision making for their diseases, ensuring that treatment decisions are guided by dermatology expertise. The AAD guidelines for AD have not been updated since 2014, highlighting the need for dermatologists to summarize current evidence-based recommendations and make them readily accessible on the AAD website.
healthcare providers and associated factors in Addis Ababa, Ethiopia. Am J Trop Med Hyg. 2024;111(5):1078-81.
4. Zucker J et al. Notes from the field: Trichophyton mentagrophytes genotype vii - New York City, April–July 2024. MMWR Morb Mortal Wkly Rep. 2024;73(43):985-8.
5. Kimball AB et al. Efficacy and safety of bimekizumab in patients with moderateto-severe hidradenitis suppurativa (BE HEARD I and BE HEARD II): two 48-week, randomised, double-blind,
ATOPIC dermatitis (AD) is one of the most common chronic inflammatory skin diseases in the world, affecting 15–25% of children and 3–7% of adults.1,2 Beyond its physical burden, AD is associated with allergic, cardiovascular, and psychiatric comorbidities, further reducing patients’ quality of life.3,4 Given its chronic and systemic nature, effective long-term management of AD is essential and makes newer therapies increasingly important.5 JAK inhibitors (JAKi) in particular have emerged as a novel medication class that modulate both Th1 and Th2 pathways, offering a promising treatment alternative for patients with moderate-to-severe AD. The recent 2025 American Academy of Dermatology (AAD) Annual Meeting featured several updates and reviews on JAKi by leading experts in the field, which the authors summarize in greater detail below.
Eric Lawrence Simpson, Oregon Health & Science University, Portland, started the conference with a presentation entitled, “Systemic therapy for adults – what’s here/ what’s coming?” on systemic therapies for AD. In that discussion, he noted that JAKi should warrant consideration as a first-line systemic therapy for AD. Despite the advent of dupilumab for AD treatment, recalcitrant disease persists for many patients. Simpson emphasized that treatment alternatives such as JAKi are “good choice(s) for inadequate response to biologics”, also noting that JAKi
have demonstrated greater efficacy in headto-head studies with dupilumab. The efficacy and safety of particular JAKi were covered in further detail by subsequent presenters.
LATEST UPDATES ON JAK INHIBITORS
Abrocitinib
Shawn Kwatra, University of Maryland School of Medicine, Baltimore, highlighted key
clinical trials that established efficacy and safety standards for JAKi in the treatment of AD in his presentation entitled, “JAK inhibitors for atopic dermatitis, prurigo nodularis, and pruritus”. His presentation started with a review of JADE MONO-1 and 2, which compared abrocitinib 100 mg, 200 mg, and placebo, in the treatment of moderate-tosevere AD in participants ≥12 years of age. At Week 12, a significantly greater percentage of participants taking abrocitinib had achieved Investigator Global Assessment (IGA) scores of 0/1 and had reductions of at least 75% in Eczema Area and Severity Index (EASI) scores (EASI-75), compared to placebo. Additionally, he noted that abrocitinib resulted in significant itch relief by Week 2 compared to placebo.
Kwatra next discussed JADE COMPARE, a trial that compared abrocitinib 200 mg and 100 mg to dupilumab 300 mg and placebo for the treatment of moderate-to-severe AD in adults. Similar to the JADE MONO trials, the primary endpoints at Week 12 showed significant improvements in IGA and EASI-75 for abrocitinib 200 mg and 100 mg compared to placebo. He also discussed that abrocitinib
200 mg also resulted in faster itch relief compared to dupilumab and placebo. He also explained that the secondary endpoints for abrocitinib, including IGA and EASI-75 at Week 16, did not differ significantly from dupilumab.
Kwatra concluded his abrocitinib discussion with the JADE EXTEND trial, which evaluated the efficacy and safety of abrocitinib in participants previously treated with dupilumab in JADE COMPARE. Interestingly, patients who responded to dupilumab maintained their benefits when treated with abrocitinib, but many patients who did not respond
Atopic dermatitis is one of the most common chronic inflammatory skin diseases in the world, affecting:
15-25 of children % of adults
3-7 %
to dupilumab achieved improved skin clearance and itch relief by Week 12 when taking abrocitinib. Kwatra emphasized that abrocitinib may provide a viable alternative treatment for patients with AD who do not respond adequately to dupilumab.
Upadacitinib
Kwatra’s session continued with a review of the Measure Up 1 and 2 trials, which evaluated and compared the efficacy of upadacitinib 30 mg and 15 mg versus placebo, for patients with moderate-to-severe AD >12 years of age.7 At Week 16, patients on both upadicitinib dosages demonstrated significant improvements in IGA and EASI-75 compared to placebo. Furthermore, Kwatra emphasized that in both trials, upadacitinib demonstrated a significant improvement in itch compared to placebo as early as 1 week into treatment. He concluded this portion of his presentation with a brief review of the safety data, which showed that no major safety signals occurred in these trials.
Eichenfield concluded that topical ruxolitinib presents a promising non-steroidal treatment option for AD, especially amid growing patient concerns over topical corticosteroids
Ruxolitinib
In his talk entitled, “Topical therapy”, Lawrence F. Eichenfield, University of California San Diego School of Medicine, La Jolla, California, reviewed the TRuEAD1 and TRuE-AD2 trials, which were the pivotal trials that investigated the efficacy and safety of topical ruxolitinib for patients aged ≥12 years with mild-to-moderate AD. In both trials, he noted that patients applying ruxolitinib 0.75% and 1.5% experienced significant improvements in IGA after 8 weeks, compared to vehicle. Ruxolitinib 1.5% also significantly reduced itch within 12 hours compared to vehicle. Eichenfield concluded that topical ruxolitinib presents a promising non-steroidal treatment option
for AD, especially amid growing patient concerns over topical corticosteroids.
PEDIATRIC USE
Amy S. Paller, Feinberg School of Medicine, Chicago, Illinois, presented her talk entitled, “Systemics for pediatric patients – are we there?”, and reviewed a 2025 network metaanalysis comparing the efficacy of JAKi versus dupilumab in pediatric patients with AD. Risk differences (RD) for clinical improvement were estimated using a random-effects model. Upadacitinib 30 mg demonstrated the highest efficacy (RD 0.62), which Paller interpreted as: “62% more patients achieved clinical improvement compared to placebo.” Other treatments included dupilumab 300 mg combined with topical corticosteroids (TCS; RD 0.43), abrocitinib 100 mg (RD 0.40), and abrocitinib 200 mg (RD 0.40). Of note, baricitinib doses below 2 mg showed no benefit over placebo. Paller did acknowledge some limitations with the analysis, such as the inclusion of only eight randomized controlled trials, and the incongruence in enrollment ages between JAKi and dupilumab trials. She concluded that oral JAKi may be favorable for managing AD flares and could offer added benefit for patients with concurrent vitiligo or alopecia areata.
SAFETY
In his talk entitled, “Understanding the safety profile of JAK inhibitors and monitoring patients”, Brett King, Yale University School of Medicine, New Haven, Connecticut, focused on the safety of JAKi and reviewed adverse events linked to JAKi use, as identified in the ORAL trial, which compared the efficacy and safety of tofacitinib and TNF-α inhibitors in patients with rheumatoid arthritis (RA), and ultimately led to the development of the box warnings carried by the medication class.
King initially summarized the common side effects of JAKi, including upper respiratory infections, headaches, nasopharyngitis,
nausea, and acne. He then discussed the ORAL study results, which revealed an increased risk for malignancy and all-cause mortality, including sudden cardiovascular death, major adverse cardiac event (MACE), and thrombosis among JAKi users, especially those with a history of smoking. King importantly pointed out, however, that the study population consisted of highrisk patients who were aged ≥50 years, had a diagnosis of RA, and had at least one additional cardiovascular risk factor. Additionally, every participant was also taking methotrexate, and half of the patients were concurrently on systemic corticosteroids.
King then raised an important question: “Are the risks of JAKi in AD the same as in RA?” He suggested that the answer is no: a study comparing the safety of baricitinib in RA and AD found higher incidences of venous thromboembolism, MACE, and malignancy in RA than in AD. He noted that JAKi have a more favorable safety profile in dermatologic diseases, but advised that clinicians should exercise caution when treating patients who are over 65 years of age, obese, or have a history of smoking, diabetes, coronary artery disease, thromboembolism, or malignancy. Prior to JAKi initiation, he recommended comprehensive infectious disease screening, including a hepatitis panel and HIV and tuberculosis testing, and baseline chemistry, blood count, lipid panel, and liver function tests. He advised repeat fasting lipids, aspartate aminotransferase, alanine aminotransferase, and complete blood count with differential at Week 4; repeat aspartate aminotransferase, alanine
References
1. Flohr C, Mann J. New insights into the epidemiology of childhood atopic dermatitis. Allergy. 2014;69(1):3-16.
2. Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016;387(10023):1109-22.
aminotransferase, and complete blood count every 3–6 months or after dose increases; and repeat tuberculosis screening annually. He also reinforced the importance of up-to-date vaccinations, annual skin checks, and ageappropriate cancer screening. He concluded his talk by outlining the discrepancy in the risks and benefits associated with JAKi use compared to the impact of untreated AD; a compelling argument for the use of these medications for this inflammatory dermatosis.
Prior to JAKi initiation, he recommended comprehensive infectious disease screening, including a hepatitis panel and HIV and tuberculosis testing, and baseline chemistry, blood count, lipid panel, and liver function tests
CONCLUSION
As summarized by the leading dermatology experts at AAD, JAKi are a unique class of medications that target the Th1 and Th2 pathways, offering broader immune modulation, and thus, therapeutic indications than Th2-predominant biologics. While JAKi slightly increase infection risk and carry an associated box warning, they are efficacious, safe, and well tolerated, as seen in data released over the last 4–6 years, which further supports that thromboembolic, malignancy, and MACE risks remain low. JAKi are a valuable contribution to the treatment armamentarium for AD and present a treatment option for patients who are inadequately treated with other therapies and/or are in need of rapid improvement.
3. Gonzalez-Uribe V et al. Comorbidities & burden of disease in atopic dermatitis. Asian Pac J Allergy Immunol. 2023;41(2):97-105.
4. Ali F et al. Counting the burden: atopic dermatitis and health-related quality of life. Acta Derm Venereol. 2020;100(12):adv00161.
5. Silverberg JI et al. Burden of disease and unmet needs in atopic dermatitis: results from a patient survey. Dermatitis. 2023;34(2):135-44.
Updates on Melanoma and Melanocytic Neoplasms from the 2025 AAD Annual Meeting
Authors: Joseph McGrath,1,2 Nathan Kattapuram,3 Gunther Grinde,4 *Divya Sharma1
1. Department of Dermatology, University of Nebraska Medical Center, Omaha, USA
2. University of Minnesota Medical School, Minneapolis, USA
3. Georgetown University School of Medicine, Washington D.C., USA
4. University of Nebraska Medical Center, Omaha, USA
*Correspondence to disharma@unmc.edu
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: McGrath and Kattapuram contributed equally to this work.
Keywords:
American Academy of Dermatology (AAD) Annual Meeting, cancer biology, dermoscopy, melanoma, melanocytic neoplasms, overdiagnosis, 31-GEP.
The American Academy of Dermatology (AAD) Annual Meeting is where many of the largest breakthroughs within the field of dermatology are presented. This year’s meeting provided numerous sessions on melanoma and melanocytic neoplasms with insightful updates as detailed below in tumor biology, genetic testing, and concerns regarding overdiagnosis of melanoma.
PLENARY: 2025 LILA AND MURRAY GRUBER MEMORIAL CANCER RESEARCH AWARD AND LECTURESHIP
Cancer biology is imperative to enhancing our understanding of melanoma, and it not only involves the study of malignant cells, but also cells in the tumor microenvironment. Single-cell RNA sequencing allows investigators to profile millions of cells within solid tumor microenvironments and can be linked to traditional pathologic staining methods. For example, single-cell omics from the Histology Analysis Framework (SCHAF) can be used to computationally resolve single-cell molecular profiles from standard hematoxylin and eosin (H&E) images.
This is one of many techniques that streamline elaborate biomolecular phenotyping of cancers down to the cellular level.
Cancer biology is imperative to enhancing our understanding of melanoma
SCHAF and spatial proteomics have been used to show how malignant cells can promote T cell exclusion in melanoma, which is predictive of immunotherapy resistance. Computational modeling was subsequently used to discover that CD4/CD6 inhibition can reverse these T cell exclusion signatures, which suggests a drug targeting these receptors could represent a promising
mode of addressing melanoma immunotherapy resistance.
The use of SCHAF and spatial proteomics to better understand the genotype and phenotype of each individual tumor cell underlies the direction of cancer research in the era of immunotherapy. The hope is that these methods can be used to develop additional melanoma therapies, such as individualized neoantigen cancer vaccines.1
THE 2025 DEBATES: CONTROVERSIES IN DERMATOLOGY
A significant number of melanomas are considered thin, with a Breslow depth less than 1 mm. Only about 5% of these thin melanomas will have occult metastases, and as such, they do not routinely get sentinel lymph node biopsy or imaging. However, roughly one-third of melanoma deaths stem from patients with thin melanomas.2 With this in mind, the question becomes whether tumor profiling using the 31-GEP test, a form of RNA transcriptomics, can inform decisionmaking for patients with melanoma.
The 31-GEP test has been validated for melanomas with a Breslow depth >0.3 mm. Patients with tumors that fall into a low-risk class (Class 1A) have a greater survival rate than those that fall into an intermediate (Class 1B/2A) or high-risk (Class 2B) class.3 In addition, one study found that patients undergoing 31-GEP testing had a 29% decrease in melanoma specific survival relative to patients who did not undergo testing.4 Proponents of the test also state that it can guide decisions around whether to perform imaging or sentinel lymph node biopsy, particularly in melanomas that have a Breslow depth between 0.3–0.8 mm, as these cancers would classically be labeled as very low-risk (5-year survival ~99%) based on the current American Joint Committee on Cancer (AJCC) 8th edition staging system.5 For example, if a patient has a Stage 1A melanoma (Breslow depth <0.8 mm without ulceration) but the melanoma falls into the
31-GEP high-risk class, a physician may choose to obtain a sentinel lymph node biopsy or imaging that would otherwise have not been indicated by the current guidelines.2
Critics of the 31-GEP test state that management is rarely altered by the test. These critics mention a study that suggested melanoma management was not altered in ~80% of cases that underwent 31-GEP testing.6 Most of the melanomas that received altered management secondary to 31-GEP testing were AJCC Stage 1A. While some patients in Stage 1A could receive more appropriate surveillance with the use of 31-GEP testing, critics are unsure if the use of healthcare resources is justified, given that each 31-GEP test costs ~7,000 USD. Other criticisms of the 31-GEP test include: 1) the test is typically only run on the more superficial portion of the melanoma collected from the biopsy and may miss more aggressive components of the tumor profile that occur deeper within the melanoma; and 2) there is not enough data available to demonstrate that 31-GEP testing is superior to the current prognostic indicators used in melanoma.7
Ultimately, additional studies and further discussion will be needed to determine if patients could benefit from more widespread use of the 31-GEP test.
roughly one-third of melanoma deaths stem from patients with thin melanomas
APPROACH TO MELANOMA DIAGNOSIS
Melanoma incidence in the United States has increased drastically in the last 40 years, with incidence among White men increasing two-fold and incidence among White women increasing three-fold. However, melanoma mortality has been fairly stable during the same time period; though some decrease has been noted, likely secondary to improved therapeutics, such as immunotherapy.
The epidemiological signature points to a potential overdiagnosis of melanoma, particularly among White patients. One study utilizing the SEER database estimated that ~65% of melanomas in White women and 50% of melanomas in White men were the product of overdiagnosis in 2018.8
While the reasons for overdiagnosis are not entirely clear, it is likely that population-based screening is playing a role. There is minimal evidence to suggest melanoma screening among the general population reduces mortality, but there is plentiful evidence demonstrating an increase in melanoma detection with screening. For example, one quality initiative study in the United States found that increased screening led to a 2.5fold increase in melanoma detection.9 Along with increased screening, physician concern about the liability associated with missing a melanoma diagnosis may also contribute to overdiagnosis.
References
1. Regev A. Plenary - 2025 Lila and Murray Gruber memorial cancer research award and lectureship. AAD, March 9, 2025.
2. Cotter D. The 2025 debates: controversies in dermatology – the clinical utility of molecular testing in melanoma and keratinocyte carcinomas Part 2. AAD, March 9, 2025.
3. Keller J et al. Prospective validation of the prognostic 31‐gene expression profiling test in primary cutaneous melanoma. Cancer Med. 2019;8(5):2205-12.
4. Bailey CN et al. 31-gene expression profile testing in cutaneous melanoma and survival outcomes in a population-
Given that overdiagnosis of melanoma can lead to unnecessary procedures and testing for patients, it is crucial to identify and address the underlying causes behind melanoma overdiagnosis.10
DERMOSCOPY FOR THE NON-DERMOSCOPIST
Dermoscopy can be crucial for differentiating between benign and malignant pigmented lesions. Several high-yield dermoscopy tips for detecting suspicious pigmented lesions include: 1) examining the lesion for angulated lines in patients with sun-damaged skin; 2) white streaks in melanomas are finer than they are in basal cell carcinomas, and they often sparkle when rotating the dermatoscope; 3) think about performing a deeper biopsy on lesions with an irregular pattern of blue pigment; and 4) a negative network within a nevus may be a sign of melanoma.11
based analysis: a seer collaboration. JCO Precis Oncol. 2023;7:e2300044.
5. Keung EZ, Gershenwald JE. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: implications for melanoma treatment and care. Expert Rev Anticancer Ther. 2018;18(8):775-84.
6. Pazhava A et al. 31-GEP (Decisiondx): a review of clinical utility and performance in a Mayo Clinic cohort. Int J Dermatol. 2025;64(3):563-70.
7. Chu E. The 2025 Debates: Controversies in dermatology – the clinical utility of molecular testing in melanoma and keratinocyte carcinomas part 1. AAD, March 9, 2025.
8. Adamson AS et al. Ecological study estimating melanoma overdiagnosis in the USA using the lifetime risk method. BMJ Evid Based Med. 2024;29(3):156-61.
9. Adamson AS et al. Estimating overdiagnosis of melanoma using trends among black and white patients in the US. JAMA Dermatol. 2022;158(4):426-31.
10. Adamson A. Approach to melanoma diagnosis – scope and harm of melanoma overdiagnosis. AAD, March 9, 2025.
11. Berry E et al. Dermoscopy for the nondermoscopist. AAD, March 9, 2025.
Insights on the Intersection of Climate Change, Air Pollution, and Dermatology at the AAD 2025 Annual Meeting
Authors: *Divya Sharma1
Affiliations:
1. Department of Dermatology, University of Nebraska Medical Center, Omaha, USA
*Correspondence to disharma@unmc.edu
Disclosure: The author has declared no conflicts of interest.
Keywords:
Air pollution, climate change, dermatology, environment, regulated medical waste
Citation: Dermatol AMJ. 2025;2[1]:23-25.
https://doi.org/10.33590/dermatolamj/VADV4402
The impact of air pollution and our changing climate on dermatologic disease is a new and emerging area of research. The American Dermatological Association (ADA) recently published a policy statement highlighting the importance of recognizing and addressing the dermatologic implications of climate change.1 At this year’s American Academy of Dermatology (AAD) Annual Meeting, experts within this area discussed the latest breakthroughs and provided valuable, clinically oriented insights in a session entitled, “Skin-Environmental Interface: Dermatologic Challenges of our Changing Climate and Environment”.2
A VARIEGATED THREAT
This session was directed by Eva Parker, a Co-Chair of the AAD’s Expert Resource Group on Climate Change and Environmental Issues. Parker provided the first lecture within this session by giving the audience an introduction into the complex interplay between our changing climate and skin disease. In particular, she highlighted the growing evidence that climate change is affecting human health in a myriad of ways. “Basically, every organ system is impacted,” Parker noted, when discussing the multifactorial threat climate change is to human health. This includes worsening asthma and allergic disease, further
burdening patients with cardiovascular disease, and finally, worsening skin diseases.
Next, David Fivenson, Fivenson Dermatology, Ann Arbor, Michigan, provided an insightful presentation on the importance of advocacy and how to get started at the local, state, and national level. Moreover, he provided tips to
Just as concerning as their ubiquitousness is the potential link Belzer provided between PFAS and dermatologic diseases, such as psoriasis and atopic dermatitis
optimize one’s practice to be more climate friendly. Importantly, Fivenson emphasized utilizing an online tool known as My Green Doctor (My Green Doctor Foundation, Jacksonville Beach, Florida). He noted this practice management resource provides step-by-step guidance to any practicing physician on how to make minor changes, which can have lasting, positive results on the environment.
HIDDEN CONTAMINANTS
Annika Belzer, a dermatology resident at the University of California-San Francisco, California; and Dennis Niebel, a leader in the intersection of climate change and dermatology, University Hospital Regensburg, Germany, both gave captivating talks on the accumulation of forever chemicals and microplastics in dermatologic products, respectively. Belzer provided an overview of what these forever chemicals consist of, primarily a compound known as polyfluoroalkyl substances (PFAS), and how commonplace they are in our world. Just as concerning as their ubiquitousness is the potential link Belzer provided between PFAS and dermatologic diseases, such as psoriasis and atopic dermatitis. Similarly, Niebel provided an introduction on what constitutes microplastics and their harmful impact on the environment. Of note, he emphasized that
microplastics can be present in dermatologic products as well, with unknown implications on the structure and function of the skin.
THE DEVIL IS IN THE DETAILS
The session’s focus then shifted from potential contaminants in dermatologic products to reducing waste in the dermatology clinic. Divya Sharma, a dermatology resident at the University of Nebraska Medical Center, Omaha, provided a practical, engaging lecture on tips for providers to minimize production and disposal of regulated medical waste. Initially, he described what regulated medical waste is defined as. Or rather, he discussed how the definition is often variable and subject to change depending on one’s state and institution. He attributed this ambiguity to the reason why many studies show excessive amounts of non-regulated waste that are often disposed of in regulated medical waste containers. Additionally, he noted that the disposal of regulated medical
The first tip he provided was to work with your institution and state to better understand the guidelines and definition of regulated medical waste
waste is more costly and more harmful to the environment than traditional municipal waste. The first tip he provided was to work with your institution and state to better understand the guidelines and definition of regulated medical waste. Of note, he provided evidence from the United States Center for Disease Control (CDC) stating that: “Just because an item has been in contact with blood, it is not necessarily regulated medical waste.” Additionally, his tips also included educating staff and team members on proper disposal of waste, performing waste audits, and optimizing the location of waste containers.
References
1. Parker ER et al. The voice of the American Dermatological Association: 2025 official policy statement on climate change. J Invest Dermatol. 2025;10:S0022-202X(25)00003-X.
CONCLUSION
The focal points of this session included the importance of recognizing how dermatologic disease is impacted by air pollution and climate change, how finding resources and organizations to advocate for our climate is imperative as dermatologists, the importance of identifying and further researching the harmful role of contaminants in dermatologic products, and the importance of proper disposal of regulated medical waste.
2. Parker ER et al. Skin-environmental interface: dermatologic challenges of our changing climate and environment. AAD Annual Meeting 2025, March 9, 2025.
AAD 2025
Abstract Reviews
This issue features original research by abstract presenters at the 2025 American Academy of Dermatology (AAD) Annual Meeting. From therapeutic innovations in warts and atopic dermatitis to nuanced challenges in ethics, hair disorders, and immunotherapy complications, these abstracts reflect the current clinical landscape in dermatology.
Efficacy of Intralesional Vitamin D3 for Treatment of Verruca Vulgaris: A Randomized Control Study
Cutaneous warts are benign epithelial lesions caused by human papillomavirus (HPV) and are common entities, affecting nearly 10% of the United States population.1 While most warts spontaneously resolve, the immunocompromised are susceptible to recalcitrant warts, which often require medical treatment.2 Most current therapies use either physical or chemical destruction for wart removal, but these treatments are associated with adverse effects.3 Intralesional vitamin D3 has the potential to demonstrate a stronger treatment response due to its ability to stimulate the immune system at the injection site via cell-mediated immunity.
METHODS
The authors sought to test the efficacy of intralesional vitamin D3 for wart treatment in a sample size of 70 patients over a 3-month period. Efficacy was determined as “excellent” if there was greater than a 90%
reduction in both size and number of lesions, “good” if there was a 60–89% reduction, and “fair” if there was less than a 60% reduction.
RESULTS
Treatment efficacy was excellent in 20 (28.6%) patients, good in 29 (41.4%) patients, fair in 18 (25.7%) patients, and poor in three (4.3%) patients (Figure 1A and 1B). Patients in the younger age group had a higher treatment efficacy compared to other treatment groups.
Figure 1: Cutaneous warts before (A) and after (B) treatment with intralesional vitamin D.
CONCLUSION
In conclusion, intralesional vitamin D3 has promising qualities as a treatment for cutaneous warts and should be considered at the clinician’s discretion. Vitamin D is an innovative approach for treating warts without the various side effects posed by other commonly used agents. The unique features of this treatment modality, including its simplicity, safety, and efficiency, make it a promising option for a very common cutaneous condition.
References
1. Witchey DJ et al. Plantar warts: epidemiology, pathophysiology, and clinical management. J Am Osteopath Assoc. 2018;118:92-105.
2. Shalaby ME et al. Diagnostic and therapeutic implications of vitamin d deficiency in patients with warts: a case-controlled study. J Cosmet Dermatol. 2022;21:1135-42.
3. Bikle DD. The vitamin D receptor as tumor suppressor in skin. Adv Exp Med Biol. 2020;1268:285-306.
4. Fathy G et al. Intralesional vitamin D3 versus Candida antigen immunotherapy in the treatment of multiple recalcitrant plantar warts: a comparative case-control study. Dermatol Ther. 2019;32(5):e12997.
Key Determinants of Aggravation and Therapeutic Resistance in Pediatric Atopic Dermatitis
Authors: *Ouissal Essadeq,1 Narjess Er-rachdy,1
Laila Benzekri,1 Nadia Ismaili1
1. Dermatology Venerology Department, Ibn Sina University Hospital Center, Mohammed V University, Rabat, Morocco *Correspondence to essadeq.ouissal@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Atopic dermatitis (AD) is a chronic skin condition affecting children, often influenced by various environmental and behavioral factors. This study aims to assess the impact of several aggravating factors and resistance to treatments in AD among patients under 18 years of age.
MATERIALS AND METHOD
This cross-sectional study included 90 pediatric patients. Examined factors included habitat type, breastfeeding practices, timing of solid food introduction, exposure to irritating textiles, laundry methods, bath frequency, cleaning products used, tobacco exposure, allergens (dust mites, pet dander, pollen), presence of pets,
sweating, stress, use of emollients, misuse of topical corticosteroids, repeated use of broad-spectrum antibiotics, and occurrences of contact eczema and skin irritations. Biological analyses included measurement of vitamin D levels, total IgE, and a blood panel (complete blood count, C-reactive protein, and allergy tests).
RESULTS
Preliminary data indicates a significant correlation between certain environmental and behavioral factors, such as exposure to irritating textiles, stress, and misuse of topical corticosteroids, with worsening symptoms and increased resistance to treatments. Conversely, regular use of emollients appears to positively impact symptom control. Exposure to domestic allergens and irritants also plays a crucial role in exacerbating the condition. A notable proportion of participants showed vitamin D deficiency and persistent inflammatory states.
CONCLUSION
This study highlights the significant influence of external and behavioral factors on the severity and treatment resistance in pediatric atopic dermatitis. Proactive management of these factors could potentially improve therapeutic outcomes and patient quality of life.
Scarring Alopecias in a Pediatric Trichology Clinic at a Tertiary Care Center
Authors: Anabell Andrea Lima-Galindo,1 Miguel Bonifacio Favela-Gálvez,1 Sonia Ocampo-Garza,1 Jorge Ocampo-Candiani,1 *Erika Alba-Rojas1
1. Dermatology Department, Hospital Universitario Dr. José Eleuterio González, Universidad Autónoma de Nuevo León, Monterrey, Mexico *Correspondence to eri9ar@yahoo.com
Disclosure: The authors have declared no conflicts of interest
Scarring alopecias (SA) are uncommon, and despite their morbidity, research on pediatric patients remains limited.1,2 Data on the most effective treatment strategies and clinical outcomes in this population are also insufficient.
This study aimed to describe the demographic and clinical characteristics, comorbidities, treatment approaches, and outcomes of pediatric patients with SA managed at the authors’ institution over the past 5 years (January 2019–September 2024).
METHODS
A retrospective review was conducted on patients under 16 years of age diagnosed with alopecia at the Trichology Clinic of the Dermatology Department at Hospital Universitario Dr. José Eleuterio González, Monterrey, Mexico between January 2019–September 2024. Patients with diagnostic uncertainty were excluded.
Clinical notes, pathology reports, laboratory data, and photographs were manually
reviewed. Comorbidities, medical treatments, and treatment responses were assessed for all patients.
RESULTS
The study included 226 patients under the age of 16 years diagnosed with alopecia, with a mean age at diagnosis of 8.9±3.8 years and no significant sex predominance. Among them, 24 patients (10.6%) had scarring alopecia (Table 1), which was more common in males (66.6%) and was associated with an older mean age at diagnosis (11.6±3.3 years).
Table 1: Types of scarring alopecias in pediatric patients at the Trichology Clinic of the Dermatology Department, Hospital Universitario Dr. José Eleuterio González (2019–2024).
Type of alopecia Frequency, n (%)
Dissecting cellulitis 14 (58%)
Folliculitis decalvans 4 (17%)
Kerion Celsi or inflammatory tinea 4 (17%)
Aplasia cutis 1 (4%)
Linear morphea 1 (4%)
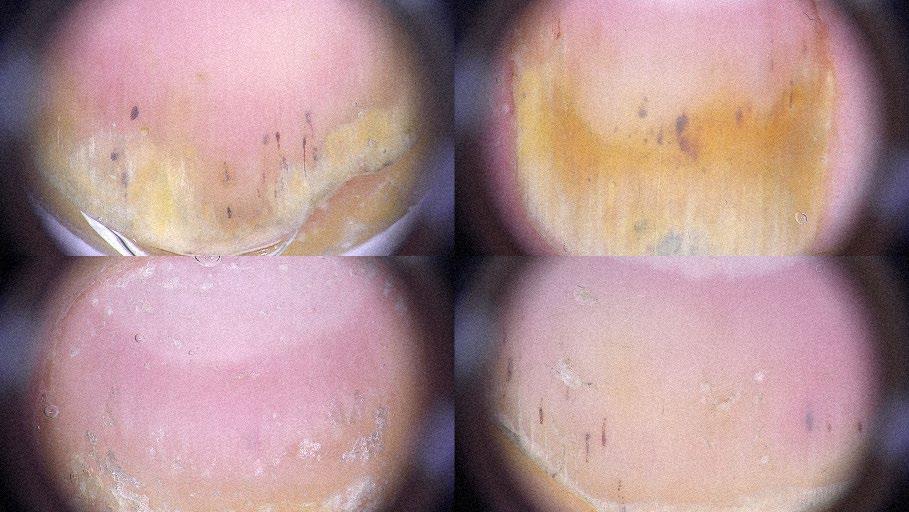
The average time for SA from onset to diagnosis was 10.7±12.1 months. Symptoms were reported by 45% of patients, with pruritus and pain being the most common (25%). A biopsy was necessary for diagnosis in 20% of cases, while the remaining patients
were diagnosed clinically. Dissecting cellulitis was the most frequent form (58.3%) (Figure 1), followed by folliculitis decalvans (16.6%). Among the patients with available anthropometric data for these two conditions, 41.8% were overweight or obese (BMI >25). Other forms of SA (25%) included linear morphea, aplasia cutis, and cases secondary to Kerion Celsi or inflammatory tinea.
Figure 1: (A–B) Multiple alopecic plaques in the parieto-occipital region with erythematous, fluctuant nodules in an 11-year-old male; (C) Dermoscopy reveals black dots, yellow dots, and erythematous areas with polymorphic vessels.
Most used treatments included intralesional steroids, topical minoxidil, topical steroids, doxycycline, or azithromycin. Additionally, low-dose isotretinoin (0.3–0.5 mg/kg/day) was administered to 64% of patients with dissecting cellulitis, resulting in partial or complete improvement.
On average, patients in this study experienced hair loss for 10–11 months before receiving a diagnosis. In scarring alopecias, early treatment is crucial to reducing symptoms and slowing disease progression. Biopsy is a valuable tool for confirming the diagnosis, particularly in cases where clinical presentation is not definitive.
CONCLUSION
In the authors’ clinic, dissecting cellulitis of the scalp was the most common cause of scarring alopecia, diagnosed in 14 cases. To date, fewer than 20 pediatric cases have been reported in the literature, suggesting that this condition may be underdiagnosed in the pediatric population. Based on their experience, low-dose isotretinoin (0.3–0.5 mg/kg/day) has shown favorable outcomes, achieving partial or complete remission in most pediatric patients.
The limited data on pediatric scarring alopecia highlight the need for further research. Treatment remains a challenge, as many therapies used in adults are not approved for children. Establishing safe and effective therapeutic options is essential to halt disease progression in the pediatric population.
References
1. Imhof RL et al. The spectrum of pediatric scarring alopecia: a retrospective review of 27 patients seen at Mayo Clinic. Pediatr Dermatol. 2021;38(3):580-4.
2. Aşkın Ö et al. Association of alopecia with selfesteem in children and adolescents. Int J Adolesc Med Health. 2020;34(5):315-8.
Skin Concerns and Knowledge of Cosmetic Procedures in Skin of Color
Authors: Mara Hartoyo,1 Rachel R. Lin,1
Janeth Campbell,2 Danyelle Dawes,1
Heather Woolery-Lloyd,1 *Alyx Rosen Aigen1
1. Dr. Phillip Frost Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, Florida, USA
2. Medstar Washington Hospital Center, Washington D.C., USA
*Correspondence to acr50@med.miami.edu
Disclosure: The authors have declared no conflicts of interest to disclose. No funding was received for this research.
Keywords: Cosmetics, cosmetic concerns, cosmetic procedures, skin of color 9SOC), women of color.
In the United States, patients with skin of color (SOC) face significant healthcare disparities.1,2 Recognizing and addressing the cosmetic concerns of SOC patients through tailored treatment is paramount to achieving equitable care.3 This study aims to identify cosmetic skin concerns among women of color, quantify the level of distress associated with these concerns, and compare findings to that of non-women of color. Additionally, the authors aim to compare the interest in modern cosmetic procedures between women of color and women not of color.
Table 1: Skin concerns in women of color versus women not of color.
MATERIALS AND METHODS
The authors conducted a cross-sectional survey study in multiple University of Miami dermatology clinics. Participants had to be ≥18 years of age, identify as a woman, and complete the Qualtrics survey in its entirety, which assessed skin type, cosmetic concerns, and interest in cosmetic procedures. Participants rated their concerns from 0–10, with 0 being no concern and 10 being extremely concerned. SOC participants were defined as those with Fitzpatrick skin type IV–VI and non-SOC as I–III.
RESULTS
Of the 136 surveyed, 38% self-identified as having Fitzpatrick skin ype IV–VI, whereas 62% had Fitzpatrick skin type I–III. Top concerns for SOC patients included hair loss/ thinning, uneven skin tone, and unwanted facial hair, while top concerns for non-SOC patients were facial laxity, fine lines, and wrinkles (Table 1). SOC patients were most interested in laser tattoo removal and laser hair removal, while non-SOC patients were most interested in intense pulsed light therapy and microneedling. Microneedling with radiofrequency was the least understood cosmetic procedure amongst all patients
CONCLUSION
Notably, cosmetic concerns and interests in SOC patients were distinct from those in non-SOC patients, emphasizing the importance of a tailored approach during cosmetic consultation. Allowing adequate time for patients to express their concerns and expectations can improve cosmetic care and optimize the dermatologistpatient therapeutic alliance.
References
1. Center for American Progress. Demographic Growth of People of Color. 2015. Available from: chromeextension://efaidnbmnnnibpcajpcglclefindmkaj/ https://cdn.americanprogress.org/wp-content/ uploads/2015/08/05075256/PeopleOfColorDemocracy-FS.pdf. Last accessed: January 15 2025.
2. Narla S et al. Racial disparities in dermatology. Arch Dermatol Res. 2023;315(5):1215-23.
3. Onalaja AAT, Susan C, "Defining Skin of Color," Li BS, Maibach HI (eds.), Ethnic Skin and Hair and Other Cultural Considerations (2021) 1st edition, Cham: Springer Cham, pp. 3-18.
Ethics of Treating Actinic Keratosis in Patients of Advanced Age
This ethics discussion highlights the complexities of treating actinic keratoses (AK) in elderly patients, particularly those in their ninth decade of life or beyond.1 AKs are recognized as precursors to squamous cell carcinoma,2 and timely interventions can reduce the likelihood of progression to invasive disease.3,4
ETHICAL ANALYSIS
Clinicians must carefully balance the principles of beneficence and nonmaleficence, as treatments such as cryotherapy and topical therapies (e.g., 5-fluorouracil with calcipotriol) may cause discomfort, scarring, or dyspigmentation.2 These adverse effects can be especially concerning in older patients whose overall quality of life and comfort may be prioritized over aggressive treatment.
Financial factors also weigh into decisionmaking. Although cryotherapy is relatively
quick and frequently reimbursed,5 it may pose an economic burden on patients and their caregivers. The principle of justice requires that medical resources be allocated wisely, taking into account both the cost to the healthcare system and the patient’s out-ofpocket expenses. Clinicians should remain mindful of whether frequent, potentially painful procedures for minor lesions offer a net benefit for a frail patient with multiple comorbidities.
Finally, respecting patient autonomy is essential. Involving the patient when capacity is intact and any caregivers in discussing goals of care helps clarify the most ethically appropriate management strategy. For some individuals, cosmetically unimportant or minimally symptomatic AKs may not warrant aggressive treatment, particularly if other medical issues take precedence.
CONCLUSION
Ultimately, ethical AK management in advanced age requires a patient-centered approach that integrates clinical judgment, compassionate care, and open communication.
References
1. Wahood S et al. Ethics of treating actinic keratoses in patients of advanced age. Abstract 64667. American Academy of Dermatology Annual Meeting, March 7-11, 2025.
2. Worley B et al. Treatment of actinic keratosis: a systematic review. Archives of Dermatological Research. 2023 Jul;315(5):1099-108.
3. Green AC, Olsen CM. Cutaneous squamous cell carcinoma: an epidemiological review. Br J Dermatol. 2017;177(2):373-81.
4. Dika E et al. Pain evaluation in patients affected by cutaneous squamous cell carcinoma and actinic keratosis: an observational study. G Ital Dermatol Venereol. 2016;152(5):413-7.
5. Yeung H et al. Use and cost of actinic keratosis destruction in the Medicare Part B fee-for-service population, 2007 to 2015. JAMA dermatology. 2018;154(11):1281-5.
Acrocyanosis After Immunotherapy: Vasculitis or Vasculopathy?
Authors: *Yuliya Lytvyn,1 Megan E. Himmel,2 Carrie Ye,3 Jarek Szlichta,4 Shahin Jamal,5,6 Alexandra Saltman2
1. Division of Dermatology, Department of Medicine, University of Toronto, Canada
2. Division of Rheumatology, Department of Medicine, University of Toronto, Canada
3. Division of Rheumatology, Department of Medicine, University of Alberta, Edmonton, Canada
4. Department of Electrical Engineering and Computer Science, York University, Toronto, Canada
5. Division of Rheumatology, University of British Columbia, Vancouver, Canada
6. Arthritis Research Canada, Vancouver, Canada
*Correspondence to Julia.lytvyn@mail.utoronto.ca
Disclosure: The authors have declared no conflicts of interest.
Keywords: Cancer immunotherapy, digital ischemia, immune checkpoint inhibitor (ICI), oncology, rheumatic immune related adverse event, vasculitis.
Acral digital ischemia associated with immune checkpoint inhibitor (ICI) use is a rare and poorly understood toxicity.
METHODS
The authors report eight cases of acral digital ischemia post-ICI from the Canadian Research Group of Rheumatology in ImmunoOncology (CanRIO) retrospective cohort between 2017–2023, and compare them to the existing 14 reported cases in the
literature.1-14 Integrating the findings, they propose a hypothetical pathogenesis and approach to treatment.
RESULTS
In comparison to previously reported cases, the CanRIO cases had earlier onset after ICI exposure (median: 6 weeks versus 10 weeks), were mostly seronegative (33% versus 63%), and were treated more aggressively with a combination of immunosuppression, vasodilation, and antiplatelet agents (triple therapy). Angiography in all cases did not find evidence of proximal vasculitis; distal imaging uniformly showed small vessel occlusion, but no vasculitis. All CanRIO cases that received triple therapy had either stabilization or resolution of cyanosis, while management with separate therapies led to poorer outcomes. There were no amputations in the CanRIO group, where 5/10 in the literature that were not managed by triple therapy required amputation.
CONCLUSION
Acral digital necrosis is a rare immunerelated adverse event associated with ICI therapy, with unknown pathogenesis or optimal treatment. The eight cases from CanRIO were identified early and received aggressive “triple therapy” with resolution of cyanosis, contrasting with previously reported cases. The authors hypothesize that ICI-associated acral digital necrosis is a new iatrogenic disease triggered by an underlying inflammatory vasculopathy with distal vessel occlusion, leading to ischemia and requiring early initiation of vasodilation and antiplatelet/anticoagulant therapy.
References
1. Thoreau B et al. Acute lower limb ischaemia and diabetes in a patient treated with anti-PD1 monoclonal antibody for metastatic melanoma. Acta Derm Venereol. 2017;97(3):408-9.
2. Gambichler T et al. Paraneoplastic acral vascular syndrome in a patient with metastatic melanoma under immune checkpoint blockade. BMC Cancer. 2017;17(1):327.
3. Le Burel S et al. Onset of connective tissue disease following anti-PD1/PD-L1 cancer immunotherapy. Ann Rheum Dis. 2018;77(3):468-70.
4. Padda A et al. Ipilimumab induced digital vasculitis. J Immunother Cancer. 2018;6(1):12.
5. Comont T et al. Immune checkpoint inhibitor-related acral vasculitis. J Immunother Cancer. 2018;6(1):120.
6. Khaddour K et al. Acral vascular necrosis associated with immune-check point inhibitors: case report with literature review. BMC Cancer. 2019;19(1):449.
7. Franco F et al. Nivolumab-associated digital smallvessel vasculitis in a patient with an advanced renal cell carcinoma. Immunotherapy. 2019;11(5):379-84.
8. Reijers ILM et al. Acrocyanosis after neoadjuvant ipilimumab plus nivolumab: a case report. Clin Exp Rheumatol. 2020;38(5):1031-2.
9. Zenati N et al. [Digital ischaemia with fingertip ulcers during ipilimumab therapy]. Ann Dermatol Venereol. 2020;147(3):212-6. (In French).
10. O'Connor P et al. Acral vascular syndrome during an immune checkpoint inhibitor. BMJ Case Rep. 2020;13(5):e233463. Erratum in: BMJ Case Rep. 2021;14(2):e233463corr1.
11. Grand J et al. An unusual case of digital cyanosis. J Am Coll Cardiol. 2022;79(Suppl 9):3292.
12. Thomas A et al. Pembrolizumab-associated acral necrosis and esophageal necrosis. Curr Probl Cancer Case Rep. 2022;8(1):100193.
13. Kefas J et al. Small vessel vasculitis and dry gangrene secondary to combined CTLA-4 and PD-1 blockade in malignant mesothelioma. BMC Rheumatol. 2022;6(1):10.
14. Yerolatsite M et al. Digital ischemia: a rare immune-related adverse event of immune checkpoint inhibitors - case report and review of the literature. Rheumatol Int. 2024;44(12): 3141-49.
Congress Interview
Lindsay Ackerman shares her vision for the future of hidradenitis suppurativa treatment and the growing role of personalized care in dermatology. She also discusses the importance of advocacy, mentorship, and the life-saving impact of the specialty. In this interview, which includes insights from American Academy of Dermatology (AAD) 2025, Ackerman reflects on the evolving landscape of dermatology and shaping the next generation.
Lindsay Ackerman
Nominating Committee Member, American Academy of Dermatology (AAD); Chief of Dermatology, Banner University Medical Center Phoenix; President, Medical Dermatology Specialists Phoenix, Arizona, USA
Citation:
Q1Not every patient with hidradenitis suppurativa responds like another
Given the promising results of upadacitinib in your recent Phase II trial, what do you think are the key challenges in translating these findings to broader clinical practice, particularly regarding long-term efficacy and safety in the hidradenitis suppurativa (HS) patient population?
It's phenomenally satisfying to see the investments that the industry has made in trying to continue to move the needle forward in the science of treating HS. It is an incredibly, incredibly burdensome disease, oftentimes a disease that patients will say is “unlivable”. The onus is on all of us from every angle of healthcare to try to figure out how best to manage this population. It is anything but simple. The challenges arise from there being a sort of alphabet soup of different cytokines and inflammatory mediators that are driving critical pathways that influence the physiology and outcomes of HS. One problem that's well understood by those of
us in the clinical world is that not every patient with HS responds like another, and sometimes you'll have a particular therapy that works brilliantly well on its own for one but sort of doesn't touch another. Many patients with more advanced disease may need multi-modal therapy. However, specifically relating to your question with regard to upadacitinib in Phase II, I think that there were really reassuring findings, specifically in the population of patients that had failed anti-TNF therapy, which give us reason to believe, both from the foundation in science and from the clinical experience in the patient population in Phase II, that upadacitinib may be a really good treatment option for these particular patients.
To my knowledge, to date, upadacitinib is approved for eight indications in the USA and down to the age of 2 years in two indications. And to my knowledge, in our Phase II trial, in HS, there were no new safety signals, which is again really remarkable
and reassuring when it comes to treating this patient population, because this is oftentimes going to be a long ride for them. This isn't something that'll be over and done quickly.
Q2
How are advancements in our understanding of HS pathogenesis, particularly regarding biomarkers and genetic factors, contributing to the development of more personalized biologic therapies?
I can say that I don't believe we are there yet, but this is an extraordinarily critical piece of the equation, in my mind, that will really be the next iteration of the way we treat patients. Certainly, I think it could even be the next iteration of the way we develop our pharmacologic interventions. Patients, again, with HS are anything but exactly the same from person to person. If we can find specific biomarkers that we can measure genetic components to the equation of their inflammation, it may be
absolutely game-changing in taking us from a place where we have to go from one therapeutic option to trialing another therapeutic option, oftentimes trying many before we land on something that might work well, to narrowing that timeframe substantially, and maybe even just giving us a near complete direction on which angle we need to take in modifying one's disease activity in HS by utilizing biomarkers and genetics. I see this as an incredibly promising part of the future of HS treatment.
Q3
Your commitment to dermatology extends beyond practice, with roles such as the Women's Dermatologic Society (WDS) Ethics Committee member and your leadership in state and national dermatology organizations. How important is it for dermatologists to get involved in these associations, and what can they do to help drive positive change within the specialty?
I can say that it is a part of my life that I enjoy thoroughly, and in
actuality, I probably even enjoy my clinical work more because of the advocacy work that I am involved in. I've been involved in various different levels, as you've mentioned, of several different organizations throughout my career, from the American Academy of Dermatology (AAD) to the Dermatology Foundation, the WDS, the Arizona Medical Association (AMA), and many others. I think it's an incredibly satisfying part of the work that I do in dermatology to make sure that the work I do within my practice extends well beyond just those four walls to help patients near and far, to know that I'm supporting the future of our precious specialty in dermatology. We are so fortunate to be able to have a tremendously important skill set and a knowledge base where we get to help patients every day, and the work that I do beyond the four walls of my practice, in advocacy, is to cement that we as dermatologists are at the table with regard to decision making as to future opportunities for our specialty, and the patients we treat.
We are so fortunate to be able to have a tremendously important skill set and a knowledge base where we get to help patients every day
These issues span from Medicare reimbursement reform to scope of practice, to truth in advertising; all things that are critical to making sure that patients get the best of care, and transparent care. All of it feels like it's a critical part of the work that I do. I would say that not everybody is able to find the time, but for many of these organizations, even just by being a member you get to amplify the voice of the institution itself. I want to remind my peers to never shy away from joining one or more of these advocacy organizations if you believe in their cause, because just your membership dues alone will actually help to service their mission statement.
Q4As an educator, what do you hope to instill in the next generation of dermatologists?
That's, I think, really a precious question to ask, thank you for doing so. I will say that you can always teach the science of medicine. There will be an indefinite supply of resources that our younger generation of dermatologists are incredibly efficient at obtaining. They are good at “resource utilization”. Where I like to uniquely come into the equation in education is that I like to mentor by inspiring those who come behind me to really understand the value of the work we do, and the relationships we share with our patients in doing it. There are many times when I'll walk into a room and it's just joyful for me to see someone that I haven't seen in 6 months. Maybe even we share a lovely, warm embrace. More than anything, I think that when we recognize that we can play such an important role in someone's greatest asset, their health, it doesn't become mundane and
routine, and sometimes, for lack of a better term, “old”. It's always an exciting and feel-good moment to walk into an exam room over and over again during our busy clinical days and realize they're looking to us for something. Our patients are with us to ask a question that’s really important to them.
They're there to have some need met, and we are gifted with the skill set that can do it. Sometimes it might be something that we consider somewhat trivial in the overall scope of healthcare, but one of the neatest parts of dermatology is you never know what's behind ‘Door number 2’. You might just be walking into someone who has a new onset rash, and you're diagnosing lymphoma, or you're going to diagnose from that rash that they're at risk of a bone marrow problem, or a lung cancer, or something else that could be really critical to understand. So, what I want to instill in the next generation of dermatologists is this compelling idea that there's always something before you that makes it worth your time and that really should give you a tremendous amount of fulfillment in the career choice that you've made. Trying to keep the momentum behind them and allow them to take the trajectory of their career into a place of positivity, rather than, “I'm worrying about how many vacation days I'm going to get next year in my contract,” or “I don't want to see too many of this type of exam with hair loss on my schedule anymore.” It's like a refocus on what they're doing with their day, why, and how cool it really is to be a dermatologist. If they can feel that, then they're going to have a much more fulfilling career than they would if they were caught
in the weeds of what their salary renegotiation is going to look like, or where they are going on their next vacation.
Q5 Congratulations on the launch of your new online medical docuseries, “Skintellagent with Dr. Lindsay Ackerman”. What can you tell us about this new venture and what do you aim to achieve?
“Skintellagent with Dr. Lindsay Ackerman” is a new medical docuseries that I have executive produced and am extraordinarily excited to have launched recently on YouTube.1 The entire purpose of this medical docuseries is to undress what dermatology really is, who we serve, and how skin is often an incredible window to consequential internal pathology. We, as dermatologists, have been given a skill set that allows us to really read the tea leaves. We can look at skin eruptions of various sizes, shapes, colors, and distributions, and from that alone, we can know that it's imperative we start working our patient up for a bone marrow malignancy, or fungal pneumonia, or metastatic breast cancer, or, well, you name it. I think that we have been given, in dermatology, a tremendous amount of visibility in the public eye. That is to say, there have been a number of platforms that have capitalized on the economy-ofinterest in “all things skin-related”. However, the dialogue has been so utterly focused on cosmetic dermatology, and on things within the scope of what we do that are very skin surface-limited, that we have lost our standing in the House of Medicine as a subspecialty of medicine that deals with critically
important diseases. My aim is to touch patients far and wide. I would love to change the public perception of dermatology from our position in the House of Medicine, to the opinion of our legislators and payers who make the rules that we have to play by. And, ultimately, I really hope that I can change what I see as a critical problem in the medical dermatology physician pipeline. I love it all, and I do it all. But by glamorizing that part of our dermatology specialty so much, we must remain vigilant that we don't find ourselves leaving behind our most vulnerable patients. That is what “Skintellagent with Dr. Lindsay Ackerman” is out to change. I want to educate, and I want to make complex medical dermatology “sexy” again.
Q6What were the most exciting trends or developments in dermatology that you were a part of at the AAD Congress, and how will they impact patient outcomes?
Health equity continues to be a focus of many organizations and many biopharmaceutical companies that are intent on ensuring that, within dermatology, we continue to increase the scope of visibility of diseases that arise
more frequently in patients with skin of color, and that we have education of the presentation of the entire array of dermatologic findings in various skin types. We also must remain vigilant that we are enrolling a broad array of demographics, and skin tones, into clinical trials. All of that gives me tremendous joy to see.
I was the producer of new medical peer-to-peer educational video content for L'Oreal Dermatological Beauty, “Derm Detective: Demystifying Dermatology with Dr. Lindsay Ackerman”, on their site, which is a site for healthcare providers of any type. I think there are about 225,000 US subscribers to this content on their website,2 where we are describing, in a peerto-peer masterclass style, certain diseases of major consequence in dermatology. We launched six episodes on their website, and that was an exciting thing for all of us. I think that will impact patient outcomes favorably because we will be reaching providers of all different levels of training and all different specialties to better understand from both the patient perspective, and physician perspective, both the experience of living with disease and working through it, to the details
surrounding pathophysiology, diagnosis, and treatments.
I was also part of the hospital consultative dermatology session on the last Monday of AAD, where I was able to speak to a room full of interested dermatologists and provide details about how I provide consultative care in the inpatient setting, as an outpatient dermatologist running a medical practice. Essentially, how we make hospital consults both efficient and effective for patients.
Exciting scientific trends we continue to see include an explosion of the implementation of JAK inhibitors and targeted, specific immunomodulators in the treatment of chronic autoimmune and autoinflammatory diseases within dermatology, which is, in the world within which I work, so incredibly satisfying to see that this work continues to dive deeper and deeper, yielding better and better outcomes for our most challenging patients to treat.
Q7 What sessions or updates did you find most surprising at AAD 2025?
“Allies and Bystanders” was a great session. It gave insight into
objective analyses surrounding harassment in the workplace. It was very eye-opening and also saddening at the same time. As a woman in medicine, unfortunately, I'm one of many who still feel, at times, as though we are treated unfairly. That, through scientifically validated data, is something that happens across many different aspects of healthcare delivery, whether that's from our corporate leaders, colleagues, or patients. It might be that it's happening in ways that are totally unintentional, especially by patients. But, for example, calling a female physician by her first name, rather than “Dr. Ackerman”, or making a comment
References
1. SKINTELLAGENT with Dr. Lindsay Ackerman. Available at: https://www. youtube.com/@skintellagent. Last accessed: 3 March 2025.
that's supposed to be a compliment about one’s physical appearance, but doing so in a way that really is not professional or appropriate during a physical examination. I honestly had felt a little bit more alone going through those experiences, prior to the session. Now I realize, unfortunately, I am anything but alone. However, the session did offer some quality examples and tips on ways to handle this type of harassment, whether you are the one being harassed or if you are a bystander bearing witness. I'm really glad I attended that session. It was empowering and validating.
Q8
What did you most enjoy about being at AAD 2025?
I always get so much out of the camaraderie of seeing so many friends from all over the country who are all equally engaged and excited about the privilege of what we get to do. My colleagues and friends are genuinely interested in learning, interested in helping to promote the science of dermatology, and helping to treat the breadth of what we need to do to meet the needs of our patients. Networking with all of them, to me, is always really enjoyable and comparable to the satisfaction I get from attending the scientific lectures.
2. L'Oréal Dermatological Beauty. Derm Detective: Demystifying Dermatology with Dr. Lindsay Ackerman. Available at: https://www.lorealdermatologicalbeauty. us/dermdetective. Last accessed: 3 March 2025.
Interviews
In this issue, we present two insightful interviews with renowned dermatology researchers. First, Richard Gallo discusses the intricate relationship between the skin microbiome, immune system, and emerging microbiome-based therapies. Keith Choate delves into groundbreaking discoveries in dermatogenetics, from rare inherited disorders to gene-based therapies. These conversations highlight the evolving landscape of dermatology, from bench to bedside.
Featuring: Richard Gallo & Keith Choate
Richard Gallo Professor and Chair, Department of Dermatology, University of
California San Diego, USA
Even within a single individual, the skin microbiome can differ considerably between various locations on the skin
Given the complex interplay between the skin, microbiome, and immune system, how do you envision the future of dermatology in terms of personalized medicine approaches that consider the unique microbial profile of each patient?
The speed and cost for accurately assessing the microbiomes of skin and gut are becoming less of a barrier. At present, many groups are making good progress at identifying microbes that are potentially beneficial or capable of promoting disease. Currently, we are not quite at the place in knowledge or technology that would compel microbiome profiling as an important diagnostic test, but I think we will get there.
Q2
Could you elaborate on the specific characteristics that define a “healthy” skin microbiome and how we can measure and assess this in individual patients?
The gut microbiome produces many factors with varying functions. Some microbes enable absorption of nutrients or drugs, others produce factors that kill pathogens, and still others change the functions of cells in the intestine. On the skin some microbes dampen inflammation, protect against environmental damage, strengthen the skin barrier, and fight other bacteria that could cause infection. There's a wide variety of different organisms that participate in those functions, and there are likely other functions that have yet to be discovered. A healthy microbiome should have a variety of these, and this varies between different individuals.
One way to define a healthy microbiome is to understand the genes and metabolic pathways that confer those beneficial behaviors and then measure them using metagenomic or metabolomic approaches.
On the other side of the coin, there's organisms that harm the skin, especially when they're over abundant. We know a lot about those already. Some of those are classic pathogens like Staphylococcus aureus or its drugresistant strain, methicillin-resistant Staphylococcus aureus. When these bacteria colonize the skin, it indicates an unhealthy microbiome, and that can be measured as well. Essentially, both beneficial and harmful microorganisms can be studied and measured by knowing how they work.
Even within a single individual, the skin microbiome can differ considerably between various locations on the skin, but there are certain characteristics of beneficial functions and negative functions, and the better we understand that the better we will be able to intervene and promote skin health, prevent disease, and develop targeted therapies for skin conditions.
Q3Your research has highlighted the role of antimicrobial peptides (AMP) in skin health. Can you discuss the potential for developing novel therapeutic strategies that modulate AMP production or activity to treat skin diseases?
There are hundreds of different AMPs, some are inflammatory and some are regulatory, and they can be influenced by many factors. AMPs benefit us by protecting against infection, but when AMPs are in excess, they can drive inflammation and also contribute to inflammatory diseases.
We know that some diseases occur because AMPs are too low (e.g., atopic dermatitis), while in other diseases (e.g., rosacea, and psoriasis), AMPs are too high and either drive disease manifestations or make complications worse. Several current therapeutics seem to work by correcting these AMP defects. We continue to look for strategies to influence AMP production specifically.
A good example of AMP modulation in therapy is a drug we use for eczema that blocks the IL-4 receptor. One of the consequences of doing that is that AMP levels increase when they are abnormally low.
This shows that we are already influencing AMP expression therapeutically, although not intentionally. What we haven't done a very good job of yet is developing drugs that specifically target AMPs alone. While some strategies have been explored, they are still in the early stages. One of the interesting observations several years ago was that vitamin D helps improve AMP expression in humans, and there was some interest in looking at that at one point, but we are still a long way away from being able to intervene directly.
Q4 How do you see the role of bacteriotherapy evolving in the treatment of skin diseases, and what do you believe are the key challenges and opportunities in developing safe and effective bacteriotherapy approaches?
The goal of bacteriotherapy is to identify specific bacteria that help us and the genes responsible for beneficial functions, then use bacteria that express these genes to restore functions that are essential to skin health. As you probably know, we're involved in bacterial therapy trials now and have published on that. We have identified many beneficial organisms and, more importantly, the genes within these organisms
that provide those beneficial effects. By understanding these genes, we can then deliver them back to the skin, especially in situations like eczema, where those bacteria are missing.
This approach is somewhat like stem cell replacement therapy, where we restore something essential by reintroducing it in a living cell. However, one of the biggest challenges in this field has been misleading claims by some in the probiotic market. Many products make bold, often unbelievable statements without a clear understanding of how or if they actually work. And although some consumers have had good experiences with currently available probiotics, many have minimal activity or no activity at all. This has led to growing skepticism about the microbiome and probiotic field. That is probably the major obstacle right now, the exploitation of the probiotic market by false claims, leading to skepticism that has hindered investment and further progress.
Overall, I believe bacteriotherapy will revolutionize the treatment of several skin disorders. They are very safe and are not immunosuppressive, so this provides a whole new tool for therapy.
Given the growing concern about antibiotic resistance, how can we develop microbiome-based therapies that minimize the risk of antibiotic resistance while effectively treating skin conditions?
One of the remarkable things about the evolution of these genes is that many of them are very carefully
regulated, they're not expressed when we don't need them and are also very selective.
The natural antimicrobials often specifically target one pathogenic species of bacteria while leaving many other microbes unharmed. This selectivity and careful regulation are a hallmark of the natural anti-microbial functions.
Antibiotics are not like that, they're very potent, but they're over-prescribed, which puts pressure on the pathogens to develop resistance. Antibiotics also have widespread activity, so they kill both pathogens and non-pathogens alike, somewhat weakening the immune system by killing beneficial bacteria. By learning from the strategies used by the microbiome and our host genome to fight infections, we may be able to adopt a more strategic approach. With microbiome-based therapies as a first-line approach, we can reserve pharmaceutical antibiotics for situations when they are most needed, therefore resisting the development of antibiotic resistance.
Therefore, microbiome-based therapies deploy strategies that have worked on an evolutionary timescale throughout nature. It is a perfect way to decrease antibiotic use and minimize resistance.
Microbiome-based therapies deploy strategies that have worked on an evolutionary timescale throughout nature
Q6Your research has highlighted the importance of understanding skin microbiome in the context of disease. How can we better integrate this knowledge into clinical practice and patient care?
It is a very complicated system with a lot of factors, including metabolic factors produced by the microbiome. We need to understand if they're missing or if they're overabundant. Knowing that would provide valuable insights for physicians and lead to better therapeutic strategies for patients. The problem is that we are still learning. The other problem is it can be quite expensive and slow to measure. We need technology that works quickly and accurately
with reasonable expense, and the knowledge to know what to measure. Overall, I think it is important to continue to focus on research, education, and communication, but with a key goal to show scientific justification and demonstration of true efficacy.
Q7How can we leverage advances in genomics, metabolomics, and other "omics" technologies to further our understanding of the skin microbiome and its role in skin health and disease?
These tools let us look more closely at the microbiome, but they need to be applied in ways that are relevant to disease pathophysiology.
There has been too much microbiome analysis for the sake of analysis alone without any clear hypothesis-driven questions. This has changed in the last few years, and the future is bright for this field.
Ideally, we will reach a situation that allows us to utilize various “omics” approaches, such as metabolomics, genomics, and proteomics, quickly and affordably. When this is combined with bioinformatics, particularly through the use of machine learning, the highly complex information of the microbiome can be decoded and used diagnostically and therapeutically.
Keith Choate
Aaron B. and Marguerite Lerner Professor and Chair of Dermatology, Yale School of Medicine; Chief of Dermatology,
Yale New Haven Hospital, Connecticut, USA.
In medicine and science, we have the opportunity to be of service
Q1Part of your research focus is on rare inherited and mosaic skin disorders. What initially drew you to this area of dermatogenetics, and what continues to drive your passion for this field?
You know, it was an interesting journey. I had very early exposure to genetic skin diseases when I was an undergraduate researcher working with Paul A. Khavari at Stanford University, California, USA. I started my undergraduate research career thinking about how we could do targeted growth factor receptor dimerization to treat wounds and other skin conditions, but at the same time, some of the fundamental discoveries in human genetics were being made, and some of the viral vectors to do gene delivery were also being developed. I remember when Khavari came to me in the lab one day when I was a research assistant and said, “Why don't we do gene therapy for genetic skin disease?”
It was also really a wonderful opportunity because, essentially, what we needed to do was identify a disease to treat. At that point, recessive loss of function mutations in the transglutaminase 1 gene, TGM1 had just been found in lamellar ichthyosis. Gary Nolan at Stanford University was working on retroviral delivery technologies, episomal ones in particular, that could produce high titer viruses that we could use to infect human cells.
Others were doing critical work in developing skin equivalents that we would be able to use as well. So,
I learned how to develop reliable ways to culture keratinocytes from patient biopsies. Khavari also set me up with Mary Williams, who was running an ichthyosis clinic at the University of California San Francisco, USA. He and I would drive together up to Mary Williams' clinic, where I would have the opportunity to meet patients who had ichthyosis, to get skin biopsies, and then drive them back to the lab, where I would culture cells.
I remember quite vividly the experience that I had there with patients who had ichthyosis. In particular, one day I was traveling, not with Khavari, but with one of our research assistants, and this very beautiful young woman came in for a visit and a biopsy. When it came time to do the biopsy, as Williams started to remove the layers and layers of foundation, revealed underneath what appeared to be flawless skin was this very deeply red and deeply fissured and scaly skin. I also noticed that the patient was becoming very unsettled by the people who were present in the room and became tearful at one point. When we left the room, my colleague turned to me and she said, “Why do such terrible things happen to good people?” Which is, of course, one of those fundamental questions that all of us ask at various points in our lives.
At that point, I was 20 years old, and I was in the midst of really coming to an understanding of who I was. Here I was in the laboratory looking at genetic disease, where we would take cells
from patients who had recessive loss of function mutations, use retroviral delivery vectors to replace TGM1, and it ended up being a perfect experiment. I was doing an enzymatic transglutaminase assay that cross-linked putrescine to casein, which was a horrific assay that smelled as bad as it sounds. I remember being at the scintillation counter and looking at the results that were coming out. When we looked at normal keratinocytes, we got a value of, say, 5,000, and when we looked at patient keratinocytes, we got a value of zero. But when I looked at each of the corrected patient cell cultures where we had done the retroviral transduction, we went right back to 5,000 precisely, every time. It turned out that there were reasons that we couldn't overcorrect these cells that have to do with the way that TGM1 is translationally regulated.
It was at that moment that I saw that we were actually going to be able to do gene therapy for lamellar ichthyosis. We would take those corrected keratinocytes and ultimately put them onto a side of a cellular cadaveric dermis, which is a technique that I learned from Dan Medalie from Shriners Burns Hospital, Galveston, Texas, USA, and do the first ex vivo gene therapy for a skin disease. To be 20 years old and to be able to see the fact that we could do real and meaningful things in the laboratory that are relevant to patients' lives and help to address that question of bad things happening to good people. It was this incredibly motivating and awe-inspiring experience.
We talk about how we have these epiphanies that happen in our lives, and I would say that altogether, that experience really was an epiphany and was the beginning of what would be a career in rare disease.
So, I pursued the dermatology physician–scientist training program at Yale, and at this point went back to the laboratory with a focus in rare disease, recognizing that while we had begun the process of discovering genes that were relevant to rare disease and dermatology, there was just so much more that was yet not understood. Now here I am, 20 years later, looking at this and realizing that we've made a lot of progress, but there's still even more to do.
In medicine, we are motivated by a lot of things, and one that has always been important for me is the idea that, in medicine and science, we have the opportunity to be of service. We have the opportunity to actually make a difference in patients’ lives, and sometimes in many patients’ lives.
Q2As your laboratory has identified the genetic basis of over a dozen disorders, could you share a discovery that was particularly surprising or impactful in advancing our understanding of skin biology?
Our group has been lucky to have had the opportunity to systematically unlock many genetic causes of both mosaic diseases, which are, at their heart, epidermal differentiation disorders. There are many stories that I could tell, but I think probably one of the ones that is most significant to me is the discovery that we made in the treatment of porokeratosis. Porokeratosis has many different clinical manifestations. It can appear as a linear stripe, and when these linear stripes appear, they can have multiple different configurations. They can be intensely inflammatory, and in those states, they're often called inflammatory linear verrucous epidermal naevus. They can be atrophic or hypertrophic, or localized to specific parts of the body. In general, they are fairly disfiguring. So, we set out to understand the genetic basis of linear porokeratosis and found that it was a disorder that featured second hit somatic mosaicism; that is, all of these individuals had one
inactivating mutation that was present in their germline, and during development, they acquired a second mutation that inactivated the same gene. All of these patients had mutations in genes that fell within the mevalonate kinase pathway.
The mevalonate kinase pathway makes farnesyl pyrophosphate, a critical metabolite used in a variety of different reactions, as well as cholesterol. Amy Paller, Feinberg School of Medicine, Chicago, Illinois, and Peter Elias, University of California San Francisco, previously had shown in CHILD syndrome, which also features a defect in cholesterol biosynthesis, that if you were to perform upstream blockade of the pathway using an HMG-CoA reductase inhibitor, also known as a “statin”, and supply the end product, cholesterol, that you could improve CHILD syndrome.
We immediately realized that the same would be true for these protean manifestations of porokeratosis. So, we initiated a trial in patients who had these severe forms of linear porokeratosis, and we took these patients with inflammatory linear verrucous epidermal naevus who have this terribly, terribly inflammatory
disease, and found that within 12 weeks, we took them from severe disease to essentially no disease, which was very exciting for us.
Then we also realized that while these were extraordinarily rare manifestations of disease, there's a huge cohort of patients that have another distinct disorder called disseminated, superficial actinic porokeratosis (DSAP). Others would show that DSAP results from second hit somatic mosaicism in exactly the same genes we found in linear porokeratosis but is primarily due to UV-induced changes that show up all over the body. These patients have progressive development of dozens to hundreds to thousands of scaly lesions on their extremities, which also increase their risk of progression to squamous cell carcinoma.
We also showed that if we treated these patients who had DSAP with cholesterol-lovastatin ointment, we could also completely reverse their disease. This was particularly exciting for me as a practicing dermatologist because we had been using disfiguring, ineffective treatments for these patients, such as anti-metabolites or carbon dioxide laser. The fact of the matter was, every time we would use one
of these destructive therapies, the disease would just come roaring back again because we weren't treating the fundamental genetic defect, and so this was really the first pathogenesis-based therapy for DSAP.
Patients, even though they now don't need to do this, come from around the world to my clinic because they want to meet the scientific team that made the discovery that led to an effective therapy for them. So, I think that it's particularly rewarding when you can make a genetic discovery connected to what's known in the literature and then actually move it into having a therapeutic that changes patients’ lives.
Q3Your work on revertant mosaicism in ichthyosis with confetti has provided fascinating insights into spontaneous self-correction of genetic mutations. How might these findings inform future therapeutic strategies for genetic skin disorders?
I think that disorders that feature revertant mosaicism, which are relatively few, present a really interesting opportunity. One is cell-based therapy. If a patient has reverted mosaicism, it by definition means that the corrected clones have greater fitness than the surrounding affected skin. We've seen that in epidermolysis bullosa (EB), for example, it's possible to use reverent cell therapy to treat disease.
It raises a really important question though; in the great majority of genetic diseases, we don't see revertant mosaicism. So, if reversion is happening, the clones that arise are not lions. They are just a gazelle in a field of gazelles, and they're just existing in this herd, and there's no pressure to allow corrections to expand. So, the work that we've done in revertant mosaicism has helped us to understand a little bit more about how cells become lions.
Patients come from around the world to my clinic because they want to meet the scientific team that made the discovery that led to an effective therapy for them
It also turns out that this intercellular competition that we see in revert mosaicism is one of the reasons that EB is one of the first disorders for which we're seeing effective gene therapy. The moment that you put a correct cell into the field of affected skin, it has a selective advantage, and so it becomes the lion in the Serengeti and has the capacity to expand.
To be able to achieve effective gene therapy for all of those other diseases that don't feature revertant mosaicism, we're going to need to be able to do two things. One is that we're going to need to be able to develop the most effective way to deliver genetic cargo to every single cell within the epidermis. But we also are going to need to be able to give them that selective advantage that's going to allow them to overtake the adjacent affected skin. This is an area that we have had a long-standing interest in, and I think it's where there's a lot of discovery left to be done.
What are the biggest challenges in identifying novel genetic causes of mosaic skin disorders, particularly in distinguishing pathogenic mutations from benign genetic variations?
One of my favorite things to do in the lab is to do something that we call ‘running the books’. We have a whole room filled with binders, and these binders have photographs of patients. We try to look at the clinical presentation of the patient and then look at the genetic data to see if we have a match. Depending on the disorder, a fraction of cases are instantly solved. You look at the epidermal nevus and you say, “Oh, there's a RAS mutation; we know RAS mutations cause epidermal nevi, so this is solved.” But it's looking at the unsolved cases that's really exciting, because when you look at those unsolved cases in general, they are disorders that aren't present in any of the textbooks. These are extraordinarily rare manifestations of disease where a physician's clinical insight has led them to realize that it's genetic for a variety of reasons, ranging from the age of onset to the specific pattern of disease that they're seeing, or the more clinical or histopathologic pathology. Then it's a question of matching, because you need to not only have a unique manifestation of disease and a good candidate gene mutation, but also need to have more than one patient who has the same disease and mutations in the same gene.
Oftentimes we find ourselves relatively stalled in terms of being able to progress to reporting a new genetic cause of disease because we have just one case. A lot of my time is spent going out to other institutions and speaking
at meetings to tell our genetic stories. It's when I talk about our discoveries that people contribute their own rare, unusual cases. Often it’s these cases that have allowed us to find a match to our singleton kindreds, proving that another patient who has this ultra rare manifestation of disease also has mutations in the same pathway.
I find myself from time to time calling patients we met 10 or 15 years ago and saying, “I bet you never thought you'd hear from me again, but we have continued working this whole time to try to find an answer for you, and we finally enrolled someone else who has the same disease as you do.” This is true for mosaic diseases. This is true for these epidermal differentiation disorders. The challenge is simply a numbers game. We need to be able to find enough patients with rare manifestations of disease and have the right genomic tools to be able to identify all kinds of variations that can contribute to disease, both coding and non-coding variations, and then ultimately have multiple individuals that have mutations in the same gene or pathway.
Our department acts like a hub for these patients, which involves a lot of communication with physicians. We have both physician-facing and patient-facing portals, and both contact us. It's really interesting because, ultimately, we have become sort of a home for people who don't have an answer. These are people who are searching for an answer, and sometimes they clearly have a genetic disease, and other times they don't have a genetic disease at all, and they're just inadequately managed. We straddle this clinical, translational
world, where we need to be able to say either yes, you have a genetic disease, we're interested, we want to help you, or no, you don't have a genetic disease, but we'll talk with your physician to help to point you in the direction of therapies that are going to make a difference.
That's where it's good to have both. As a physician and as a translational scientist, ultimately, we can do good in patients' lives, both by helping them to get genetic answers when they have a genetic disease and sometimes developing new therapeutics. But also, for those others who are sort of wandering in the desert, we can help to point their clinicians in the direction of other ways to treat what they have.
Q5
In addition to your research, you mentor students and train physicians. What do you find most rewarding about working with the next generation of physician–scientists, and what advice do you give them about pursuing careers in dermatology and genetics?
I spend a lot of my time thinking about the next generation because my early career exposures in other people's research environments were the nucleus of my epiphany, exposure, and excitement about what I do today. I think one of the greatest gifts that we have as physicians and scientists is to inspire a new generation of individuals to enter the field, and often for those individuals to take up completely new approaches.
I have been incredibly lucky to have had students and physician–scientist fellows in my research group who've brought new
technologies and new approaches to the diseases that have allowed us to do completely new things. I think it's mutually beneficial; you bring in new talent and new ideas and provide trainees with the runway that's necessary for them to make new discoveries. I also do this as a Chair of my department and as an Associate Dean for Physician–Scientist Development at Yale.
If you look closely at the fundamental discoveries that have changed human health, physician–scientists have been at the center of the great majority. This is because they bring an understanding of disease physiology and of patient experience, and also extra motivation to actually change lives that is so critical. I am a huge believer in the importance of having people who are dually engaged both in fundamentally understanding disease from their exposures in clinical medicine and also having the tools that they need to ask big, basic, and translational questions that are ultimately relevant to pushing forward our understanding of disease.
Q6Genetic research has led to novel therapeutic approaches for skin disorders. How do you see the role of gene-based therapies evolving in dermatology over the next decade?
I think that we have a lot more to learn still. Every time we identify a new gene, we gain insight into how the dysfunction of that gene contributes to disease and a little bit of insight into how that gene functions in normal skin development or differentiation. However, I think that we're now coming to understand that genes exist within the context of an environment. This can be, and we're coming to understand this more
and more, the contributions of the microbiome. That is, what are the commensal microbes that are present both on our skin and in our gut, and what are the other factors that we encounter in daily life, like pollution, that impinge upon our unique genetic makeup to manifest in the diseases that we see? We have a tremendous amount more work to do to understand the commonalities that underlie the now greater than probably 70 genes that cause ichthyosis.
We are now pivoting to think about these diseases of epidermal differentiation more globally and trying to understand how mutations in individual genes activate common pathways that lead to scaling and redness. This is with the idea that perhaps our best therapies are not necessarily going to be gene therapies, but they're going to again be pathogenesis-based therapies.
We need to be thinking globally about pathways affecting epidermal differentiation that might be relevant broadly. We're seeing a lot of repurposing of therapeutics from the oncologic space to treat rare diseases. We also need to better understand the contributions of the microbiome to disease and think about how we might be able to therapeutically manipulate the microbiome to do meaningful things. We need to be looking at how we can achieve the replacement of things that are missing within the skin via topical approaches. These may not be gene therapies. These may be protein therapies. They may be small molecule therapies. We are keeping a very open mind, and at the same time, we've seen important advances in gene therapy in EB, and I think we are currently waiting for some transformational discoveries.
We are now pivoting to think about these diseases of epidermal differentiation more globally and trying to understand how mutations in individual genes activate common pathways that lead to scaling and redness
Maybe this will come from better understanding lions and gazelles and the world of revert mosaicism, but maybe it will also come from just being much better able to deliver genetic cargo easily to stem cells within the skin. I think that remains one of the biggest barriers that we have to being able to do gene therapy broadly across both rare and common diseases that share overlapping features with some of the rare diseases that we see in clinical practice.
Ultimately, what we need is a systems biology approach that considers what's the genome, what's the transcriptome, what's the microbiome, and then what's the metabolism, and then ultimately integrates those things to identify what the appropriate targets are as we think broadly about advancing therapies for disease.
Q7What are the biggest unanswered questions in dermatogenetics today, and what breakthroughs do you hope to see in the near future?
There are a lot of monogenic causes of disease that we have the opportunity to discover, and so we need to continue pushing forward until we understand all of the single genes that can contribute to disease. We know there are 30,000 genes in the genome, and we probably have a superficial understanding of the function of about 5,000. We're also now discovering significant phenotypic expansion, where we thought mutations in one gene caused one disease, but in fact, mutations in one gene can cause multiple distinct diseases, one more different from the next.
Functionalizing the genome is the next thing that we need to do, understanding not only how individual variants cause disease but also how gene-environment interactions and polygenic risk factors impinge upon the individual genetic mutations to manifest in disease.
I'm constantly telling students in the lab this: “You can't be just a computational biologist. You can't just be a person who looks for individual mutations. You have to be a classical biologist as well.” We find that we are often going back to basic, fundamental things about protein chemistry, about cell biology, about electron microscopy, about lipid biosynthesis. You really need to be full-spectrum biologists to be able to make an impact on trying to push forward our understanding of skin biology.
Real-World Use of Bimekizumab Therapy in Patients with Difficult-to-Treat Plaque
Psoriasis:
A Retrospective Analysis from a Large Academic Center
Editor's Pick
While clinical trials support the efficacy of bimekizumab, real-world data in difficult-to-treat cases is not as evident. This study provides insight into its use in patients who have cycled through multiple systemic therapies, offering a practical perspective beyond randomized controlled trials. By addressing a critical gap, this research enhances understanding of bimekizumab’s effectiveness in real clinical settings.
Michael H. Gold
Medical Director, Gold Skin Care Center, Nashville; Medical Director, Tennessee Clinical Research Center, Nashville, Tennessee, USA
Authors: M. Grace Hren,1,2 Isabel C. Silva,1 Sreekar Miriyala,1 Annie Chang,1 *Saakshi Khattri1
1. Icahn School of Medicine at Mount Sinai, New York, USA
2. Renaissance School of Medicine, Stony Brook University, New York, USA *Correspondence to saakshi.khattri@mountsinai.org
Disclosure: Khattri is an employee of Mount Sinai and a consultant for AbbVie, Eli Lilly, Janssen, and Novartis. She is on the speaker bureau for UCB, Janssen, Lilly, Regeneron, and AbbVie. She receives research funding from AbbVie, Pfizer, Incyte, and Takeda.
Bimekizumab is a humanized monoclonal IgG1 antibody that selectively inhibits IL-17A and IL-17F, two cytokines that play a critical role in psoriasis vulgaris pathogenesis. Randomized clinical trials demonstrating the superiority of bimekizumab compared to placebo and other injectable biologics led to its approval by the United States FDA for moderate-to-severe plaque psoriasis. Due to the often-strict inclusion/exclusion criteria of randomized clinical trials, patient characteristics in real practice may drastically differ. Thus, the authors sought to investigate the use of this medication among real-world patients at their large academic center.
Charts of patients prescribed bimekizumab between October 2023–April 2024 with a diagnosis of moderate-to-severe plaque psoriasis and follow-up within 6 months of medication initiation were included. Results showed that of the 24 patients prescribed bimekizumab, 83.3% (n=20) had concurrent diagnoses of psoriasis and psoriatic arthritis. At bimekizumab initiation, all patients had a baseline body surface area (BSA) affected by psoriasis of ≥10%, with mean BSA being 13.4%. After a mean of 163.5 days of therapy, BSA decreased to 3.8%. Overall, 83.3% of patients experienced a decrease in BSA after initiating bimekizumab, with 37.5% of patients obtaining a BSA of 0% (skin clear). Aligning with clinical trials, this study reinforces bimekizumab as a useful therapeutic option for moderate-to-severe plaque psoriasis. Future real-world research investigating bimekizumab would benefit from increased size and longer follow-up. Despite limitations, this study supports bimekizumab as an appropriate option for treatment of moderate-to-severe plaque psoriasis among patients in real clinical practice.
Key Points
1. Psoriasis affects 2–3% of the population worldwide, with about 30% of these patients developing psoriatic arthritis.
2. This retrospective review presents 24 patients with difficult-to-treat psoriasis who had failed prior systemic therapies and were initiated on bimekizumab with positive effects.
3. Bimekizumab can be considered as a next-step therapy for bio-experienced patients, even for patients who have failed another IL-17 inhibitor.
INTRODUCTION
Bimekizumab is a humanized monoclonal IgG1 antibody that selectively inhibits IL-17A and IL-17F, two cytokines that play a critical role in psoriasis vulgaris pathogenesis.1 Randomized clinical trials (RCT) demonstrating the superiority of bimekizumab compared to placebo and other injectable biologics and its clinical safety led to its approval by the United States FDA for moderate-to-severe plaque psoriasis.2 Presently, few studies have investigated the effectiveness of bimekizumab in real clinical practice.3 Due to the often strict inclusion/exclusion criteria of RCTs, patient characteristics in real practice may drastically differ, making real-world studies imperative.4 Herein, the authors describe the use of bimekizumab among 24 patients with difficult-to-treat plaque psoriasis, the majority of whom had previously cycled through multiple systemic therapies.
METHODS
Charts of patients prescribed bimekizumab for psoriasis between October 2023 (time of United States FDA approval) to April 2024 at a large academic center in the United States were retrospectively retrieved and reviewed. For inclusion, a diagnosis of moderate-to-severe plaque psoriasis and follow-up within 6 months of bimekizumab initiation was necessary. The authors defined “difficult-to-treat plaque psoriasis” as that which was refractory to at least two prior systemic therapies.
RESULTS
Of the 24 patients prescribed bimekizumab, 83.3% (n=20) had concurrent diagnoses of psoriasis and psoriatic arthritis; the remaining 16.7% (n=4) of patients had psoriasis only (Table 1). At bimekizumab initiation, all patients had a baseline body surface area (BSA) affected by psoriasis of ≥10%, with
mean BSA being 13.4±7.8 (Figure 1). At the start of treatment, the mean age and number of failed systemic therapies was 54.6 years and 4.5 therapies, respectively. All patients (except one) were bio-experienced, and 87.5% of patients had previously cycled through at least two systemic options, with either an inadequate response or secondary loss of efficacy to each.
Immediately prior to bimekizumab switch, 66.7% of patients were on an IL-17A or IL-17RA inhibitor, 20.8% of patients were on an IL-23 inhibitor, 8.33% of patients were on a TYK2 inhibitor, and one patient was on a TNF-α inhibitor. After a median of 184 days of therapy, BSA decreased to 3.8%. Overall, 83.3% of patients experienced a decrease in BSA after initiating bimekizumab, with 37.5%
Figure 1: Change in body surface area (%) from initial follow-up visit.
of patients obtaining a BSA of 0% (skin clear). In contrast, after an average of 119.25 days of therapy, 16.7% of patients experienced no change in disease severity. No patients clinically worsened while prescribed bimekizumab. Four patients experienced adverse events, with two of these resulting in bimekizumab discontinuation (gastrointestinal symptoms, injection site reaction [ISR]).
DISCUSSION
To the authors’ knowledge, this study is the first analysis of bimekizumab use in clinical practice in the United States. Aligning with clinical trials, this study reinforces bimekizumab as a useful therapeutic option for moderate-to-severe plaque psoriasis.1,2,5 In the Phase III bimekizumab randomized clinical trials (BE READY, BE RADIANT, BE VIVID, BE SURE),1,5-7 patients were excluded if they had experienced a primary failure to an IL-17 inhibitor or had failed more than one biologic other than an IL-17 inhibitor. Further, in each of the four trials, less than half of the patients were bio-experienced.1,5-7 In contrast, 21 out of the 24 patients included
in this study had attempted multiple biologics or systemic medications to treat their plaque psoriasis prior to attempting treatment with bimekizumab. Twenty-two patients had attempted an 1L-17 inhibitor, with 15 trialing secukinumab, 12 trialing ixekizumab, and eight trialing brodalumab (Table 1). Additionally, patients with certain comorbidities were excluded from the bimekizumab trials, for example those with hepatitis C infection. Although only one of the patients included in this study reported chronic hepatitis C infection, this patient had an improvement in affected BSA after starting therapy with no adverse events noted. Regarding special site involvement, nine patients had scalp psoriasis, with four achieving clearance, three achieving mild improvement, and two showing no improvement. Two patients had facial psoriasis that cleared after bimekizumab initiation, and three patients had palm/sole psoriasis with mild improvement. No patients presented with genital psoriasis.
Interestingly, oral candidiasis was a frequently reported adverse event in the bimekizumab clinical trials but was observed in only one patient in this study. This may be due to limited follow-up and small sample size.
Table 1: Real-world use of bimekizumab in 24 patients with difficult-to-treat plaque psoriasis.
*Because this was a retrospective study, data for patients were recorded when patients returned for visits, BSA was used as a proxy for disease severity as PASI scores were not consistently reported.
†Duration of bimekizumab was calculated from the date of initiation of bimekizumab to the date of most recently known follow-up.
Also of note, ISR was reported in a small percentage in each of the four clinical trials; however, in this study, it was reported by two patients, with one patient requiring bimekizumab discontinuation due to ISR. As bimekizumab was only recently approved by the FDA, the duration of treatment with bimekizumab is limited by this constraint, as evident in this study.
CONCLUSION
Future real-world research investigating bimekizumab would benefit from increased size and longer follow-up. Despite limitations, this study supports bimekizumab as an appropriate option for treatment of moderateto-severe plaque psoriasis among patients in real clinical practice, even those who previously failed multiple systemics and/ or biologic therapies. Bimekizumab may be considered as a next-choice biologic therapy in biologic experienced patients who might have failed a prior biologic for psoriasis.
References
1. Gordon KB et al. Bimekizumab efficacy and safety in moderate to severe plaque psoriasis (BE READY): a multicentre, double-blind, placebo-controlled, randomised withdrawal phase 3 trial. Lancet. 2021;397(10273):475-86. Erratum in: Lancet. 2021;397(10280):1182.
2. Burshtein J et al. The efficacy and safety of bimekizumab for plaque psoriasis: an expert consensus panel. Dermatol Ther (Heidelb). 2024;14(2):323-39.
3. Cirone KD, Lovegrove FE. Real-world experience using bimekizumab for
the treatment of moderate-to-severe psoriasis from a single outpatient dermatology clinic. J Cutan Med Surg. 2024;28(1):78-9.
4. Rogers JR et al. Comparison of clinical characteristics between clinical trial participants and nonparticipants using electronic health record data. JAMA Netw Open. 2021;4(4):e214732.
5. Strober B et al. Bimekizumab efficacy and safety in patients with moderate to severe plaque psoriasis: Two-year interim results from the open-label extension of the randomized BE RADIANT phase 3b trial. J Am Acad Dermatol. 2023;89(3):486-95.
6. Reich K, et al. Bimekizumab versus ustekinumab for the treatment of moderate to severe plaque psoriasis (BE VIVID): efficacy and safety from a 52-week, multicentre, double-blind, active comparator and placebocontrolled phase 3 trial. Lancet. 2021;397(10273):487-98. Erratum in: Lancet. 2021;397(10275):670.
7. Thaçi D et al. Safety and efficacy of bimekizumab through 2 years in patients with moderate-to-severe plaque psoriasis: longer-term results from the BE SURE randomized controlled trial and the open-label extension from the BE BRIGHT trial. Br J Dermatol. 2023;188(1):22-31.
Author:
Nail Psoriasis: A Narrative Review of Manifestations, Diagnosis, and Management
*Ahu Yorulmaz1
1. Ankara Bilkent City Hospital, Ankara, Türkiye *Correspondence to ahuyor@gmail.com
Disclosure: The author has declared no conflicts of interest.
Psoriasis is a common, chronic inflammatory dermatosis, and patients with psoriasis often develop nail involvement. It is estimated that up to 90% of patients experience nail lesions at least once in their lifetime. Nail psoriasis (NP) occurs when psoriatic inflammation affects the nail matrix, nail bed, or both. The clinical manifestations of NP vary depending on the location and severity of the inflammation. Common signs include pitting, splinter hemorrhages, salmon patches, and distal onycholysis. Although cutaneous psoriasis is considered more severe in individuals with nail involvement, there is no clear relationship between the duration, severity, and clinical presentations of cutaneous psoriasis and NP patterns. NP is notable for an increased prevalence of arthritis among patients and is considered a significant clinical burden due to its association with arthritis and its slow or poor response to many therapeutic agents. Effective reassurance and patient education are essential components of NP management. This review summarizes clinical manifestations and diagnostic and therapeutic strategies for NP.
Key Points
1. Nail involvement is common in psoriasis. It is estimated that up to 90% of patients with psoriasis experience nail lesions at least once in their lifetime. Nail psoriasis (NP) poses a considerable burden, not only because it may cause functional impairment and pain but also it has been identified as a risk factor for the development of psoriatic arthritis.
2. NP has diverse clinical manifestations. It has been demonstrated that some features of NP are seen more commonly in patients with psoriatic arthritis. Detection of these features is crucial for proper patient management, since it may lead to complete change in the treatment strategies to prevent joint damage.
3. This review summarizes clinical manifestations and diagnostic and therapeutic strategies for NP.
INTRODUCTION
Psoriasis is a chronic inflammatory dermatosis affecting 1–2% of the global population.1 Nearly half of psoriasis patients experience nail involvement, with a lifetime risk of developing nail psoriasis (NP) reaching up to 90%.1,2 NP presents a significant clinical burden, not only because of its cosmetic impact but also due to its association with psoriatic arthritis (PsA).3 The increased prevalence of NP among patients with PsA4 indicates that NP may predict PsA development.5 Early detection of nail involvement in psoriasis is critical as it may lead to the timely diagnosis and management of PsA, preventing irreversible joint damage.5 Dermatologists play an important role in the multidisciplinary management of NP. Diagnosing NP in cases with isolated nail involvement without cutaneous psoriasis, which occur in about 5% of patients, can be challenging.1,6 This review explores the clinical manifestations, diagnosis, and treatment of NP, offering insights into diagnostic and therapeutic strategies for complex cases.
CLINICAL MANIFESTATIONS OF NAIL PSORIASIS
NP presents with various clinical manifestations. While cutaneous psoriasis is often considered more severe in individuals with nail involvement, there is no clear relationship between NP patterns and the clinical presentations of psoriasis.1 Psoriasis can manifest in four primary clinical variants: plaque psoriasis, guttate psoriasis, erythrodermic psoriasis, and pustular psoriasis. For example, erythrodermic psoriasis, a potentially lifethreatening condition, may present with distal onycholysis on a few fingernails; whereas acral pustular psoriasis, a subtype affecting the hands and feet, may result in onychodystrophy affecting all nails. A rare variant of acral pustular psoriasis, acrodermatitis continua of Hallopeau (ACH),7 is characterized by vesiculopustular lesions on the distal phalanges and is a nail disease.8
The European Rare and Severe Psoriasis Expert Network (ERASPEN) classifies ACH as a localized pustular psoriasis, characterized by persistent (>3 months) sterile pustules affecting the nail apparatus.9 Palmoplantar pustulosis, the other variant of acral pustular psoriasis, can cause nail lesions in a mild or severe pattern. Nails are always affected in ACH but not in palmoplantar pustulosis.9
The most common NP findings include pitting, distal onycholysis, splinter hemorrhages, and salmon patches. Nail lesions arise when psoriatic inflammation affects the nail bed, nail matrix, or both. Damage to the nail matrix leads to clinical signs such as pitting, Beau’s lines, leukonychia, trachyonychia, red spots on the lunula, thick nail plates, and nail plate crumbling. Conversely, involvement of the nail bed results in distal onycholysis, splinter hemorrhages, salmon patches, and subungual hyperkeratosis.1,10 Pustular psoriasis causes pustules within the nail bed in ACH, which results in nail plate destruction.8
Findings of NP vary among patients, and patients generally manifest with both nail bed- and matrix-related findings. However, in some patients, nail bed-related findings typically appear together, whereas in others, matrix-related findings cooccur. One of the most common NP patterns involves distal onycholysis, splinter hemorrhages, and salmon patches coinciding with pitting, the most common matrix-related finding (Figure 1). Pitting, being the most common matrix-related finding, can occur alone or alongside other lesions. It can be diffusely scattered or localized in a few areas.11,12 Pitting can also occur in other nail diseases, such as alopecia areata, lichen planus, and dermatitis. Psoriatic pits are deeper and irregular and give the nail a rough appearance when compared with pits caused by other nail diseases. Alopecia areata is a common disease, in which pitting is frequently observed. Pits in alopecia areata are generally evenly distributed and superficial and give a shiny appearance.13,14 Ten pits in one nail or more than 50 pits on all nails have been considered evidence
Note sharply demarcated, silvery scaly, erythematous plaques and typical lesions of nail psoriasis, including distal onycholysis with erythematous border, salmon patches, pitting, and Beau’s lines.
of psoriasis.1 Although pitting is not a pathognomonic lesion for NP, it may be a diagnostic finding if these criteria are met.
Salmon patches are NP-pathognomonic lesions representing psoriatic plaques on the nail bed. When they are seen, clinicians can make an accurate diagnosis of NP. They are translucent, amber-colored, yellowish-red to yellowish-brown spots on the nail bed that resemble oil droplets. In general, they have an erythematous rim, which is a very characteristic finding for NP. Distal onycholysis in NP also has the typical erythematous border. Salmon patches and distal onycholysis are related lesions in NP. When a salmon patch reaches the hyponychium, the parakeratosis that causes it breaks out, and distal onycholysis develops.1,11,12 This erythematous border distinguishes psoriatic onycholysis from distal onycholysis seen in other diseases, such as onychomycosis and traumatic onycholysis.1,11,12,15,16
Dermoscopic features of NP include distal onycholysis with erythematous border, salmon patches, splinter hemorrhages, nail bed red spots, red spots on the lunula, longitudinal erythema of the nail bed, mottled lunula, fuzzy lunula, pitting, multiple white dots, dilated nail bed capillaries, dilated hyponychial capillaries, subungual hyperkeratosis, nail plate crumbling, and pseudopitting.11,12,17 Pseudopitting is a recently described feature of NP, which is characterized by pits seen above salmon patches.17 However, there are nonspecific NP lesions that are matrix-related and visible to the naked eye. Trachyonychia, longitudinal ridging, leukonychia, Beau’s lines, and nail plate thickening are among them, and they can be seen in other diseases, such as onychomycosis, lichen planus, and idiopathic trachyonychia.1,10,14,15,18,19 Differentiation of NP from these diseases is mainly based on the detection of characteristic NP lesions, such as salmon patches or distal onycholysis with erythematous border.11
Figure 1: Clinical image of a patient with psoriasis.
DIAGNOSING NAIL PSORIASIS
NP is generally easy to diagnose when typical skin and nail lesions are present. Psoriasis has distinctive skin lesions that are mostly sharply demarcated, silvery scaly, erythematous papules and plaques on the scalp, lumbosacral region, and extensor surfaces of the elbows and knees.7 However, in isolated NP cases or atypical presentations, dermoscopy or a nail biopsy may be required. While histopathology remains the gold standard for NP diagnosis, nail biopsy is rarely used due to its invasiveness. Several characteristic and common dermoscopic features of NP have been described (Figure 2), allowing clinicians to make an accurate diagnosis of NP without the delay and discomfort associated with the nail biopsy procedure. Furthermore, nail biopsy requires expertise. Unless the tissue specimen is taken from a specific area, nail biopsy in NP is usually associated with diagnostic errors.1,11,12
Dermoscopy, a non-invasive imaging technique, has proven effective in diagnosing NP and differentiating it from other nail disorders, such as onychomycosis, lichen planus, trachyonychia, and nail trauma.1 Onychomycosis has typical dermoscopic features such as longitudinal streaks and patches, a jagged proximal edge with spikes of the onycholytic area, subungual hyperkeratosis, brown-black pigmentation, multicolored pigmentation, and leukonychia. Onychomycosis is distinguished from other nail diseases by its whitish-yellow longitudinal streaks and patches.15 However, the most significant difference between onychomycosis and NP is distal onycholysis. Onychomycosis has a jagged proximal edge, whereas NP has a round linear proximal edge and an erythematous border.1,11,12,15
Nail lichen planus is another nail disorder frequently mistaken for NP. Typical clinical features include pterygium
A) Distal onycholysis with erythematous border, splinter hemorrhages, and dilated nail bed capillaries. B) A large salmon patch. C) Diffuse pitting. D) A typical combination of features; nail bed-related findings cooccur with pitting.
Figure 2: Dermoscopic features of nail psoriasis.
unguis, longitudinal ridging, fissuring, distal splitting, subungual hyperkeratosis, onycholysis, trachyonychia, red lunula, and onychoatrophy. Pterygium, a typical sign of lichen planus, is easily visible to the naked eye. However, dermoscopy is particularly useful for detecting subtle changes, such as red lunula.18,20
Common nail lesions associated with traumatic nail dystrophy include thickened nail plates, yellowish discoloration, leukonychia, splinter hemorrhages, and distal onycholysis. Although the patient’s history often reveals the diagnosis, distinguishing nail trauma from NP can be challenging. One of the most significant differences is the presentation of distal onycholysis. Nail trauma typically causes distal onycholysis with a proximal linear edge, surrounded by a typical pale pink bed. In contrast, NP presents with an erythematous border around distal onycholysis. Dermoscopy in nail trauma often reveals hemorrhagic spots and streaks, the primary indicators of subungual hemorrhage. Although splinter hemorrhages are common in NP, they do not follow a globular pattern. Nail trauma, however, is characterized by peripheral fading and satellite globules associated with subungual hemorrhage.16
TREATMENT OF NAIL PSORIASIS
Treating NP is often challenging. Compared with cutaneous lesions, nail lesions improve slowly due to the slow growth rate of the nail plate. Topical treatments are less effective because of limited drug penetration through the nail plate. Systemic treatments are recommended for cases with widespread cutaneous involvement and PsA. In isolated NP or cases with limited cutaneous involvement, treatment decisions require careful consideration of the safety and economic implications of systemic treatments. The best approach to treating NP involves a patient-centric strategy, as the disease causes pain, functional impairment, and a significant reduction in quality of life. General prophylactic measures, such as
avoiding minor trauma, are recommended for all patients. Physician–patient shared decision-making is crucial, particularly in challenging cases like isolated NP.1,21-24
All patients should be advised to follow general prophylactic measures. For instance, patients should avoid behaviors that trigger Koebnerization, such as nail biting, manicures, and wearing tight-fitting shoes. Gloves should be worn during wet or dirty work, and frequent contact with water should be avoided. Hands and feet must remain dry, and nails should be kept short. Emollients should be applied liberally to all nail surfaces.22
Systemic agents are recommended for patients with moderate-to-severe cutaneous psoriasis. However, patients with mild skin disease or no cutaneous involvement may receive either topical or systemic treatment, depending on individual cases. Patients with PsA should receive systemic treatments regardless of nail and skin severity. According to expert consensus, for patients with no or mild cutaneous involvement, the number of nails affected can determine whether topical or systemic therapy should be used. For instance, patients without cutaneous involvement or with mild skin disease who have NP in up to three nails should receive topical therapy, whereas those with NP in more than three nails may receive either topical or systemic therapy.1,22
Topical treatments include corticosteroids, vitamin D analogs, retinoids, calcineurin inhibitors, and keratolytic agents. Topical corticosteroids are the cornerstone of treatment. Potent and superpotent topical corticosteroids are typically preferred due to limited drug penetration through the nail plate. They can be applied once or twice daily, with or without occlusion, for 4–6 months. Intermittent therapy is usually preferred over continuous therapy to minimize side effects such as skin atrophy, telangiectasias, and tachyphylaxis.1,21-24
Patients with PsA or moderate-tosevere cutaneous psoriasis should receive systemic treatment, as nail lesions improve in tandem with cutaneous lesions. Several systemic therapeutic agents are available for NP, including conventional antipsoriatics such as methotrexate, cyclosporin A, and acitretin, which vary in effectiveness. Additionally, small molecules like apremilast and biologics have expanded treatment options for NP. Biologics, TNF-α inhibitors (etanercept, adalimumab, certolizumab, infliximab), IL-17 inhibitors (secukinumab, bimekuzumab, brodalumab, ixekizumab), IL-12/23 inhibitor (ustekinumab), and IL23 inhibitors (tildrakizumab, guselkumab, risankizumab) are highly effective in treating psoriasis because they inhibit specific immune pathways. However, they are more expensive. They have a favorable safety profile compared to conventional
References
1. Haneke E. Nail psoriasis: clinical features, pathogenesis, differential diagnoses, and management. Psoriasis (Auckl). 2017;7:51-63.
2. Canal-García E et al. Nail psoriasis. Actas Dermosifiliogr. 2022;113(5):481-90.
3. Manhart R, Rich P. Nail psoriasis. Clin Exp Rheumatol. 2015;33(5):7-13.
4. Cengiz G et al. The impact of nail psoriasis on disease activity, quality of life, and clinical variables in patients with psoriatic arthritis: a cross-sectional multicenter study. Int J Rheum Dis. 2023;26(1):43-50.
5. Raposo I, Torres T. Nail psoriasis as a predictor of the development of psoriatic arthritis. Actas Dermosifiliogr. 2015;106(6):452-7.
6. Radtke MA et al. Nail psoriasisa treatment challenge. J Dtsch Dermatol Ges. 2013;11(3):203-19.
7. Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945-60.
8. Yorulmaz A, Yalcin B. A painful periungual red spot in a patient with onychodystrophy. Skin Appendage Disord. 2017;3(2):67-9.
9. Navarini AA et al. European consensus statement on phenotypes of pustular
systemic therapies, yet they can be associated with severe side effects. TNF-α inhibitors should be avoided in patients with congestive heart failure, a personal or family history of demyelinating disease, and a malignancy history. IL-17 inhibitors should be avoided in patients with inflammatory bowel disease. Suicidal ideation has been shown in patients receiving brodalumab and bimekizumab, thus they should be avoided in patients with a history of mental health disorder. Detailed examination is vital in patients with a history of malignancy or hepatitis B and C infections when prescribing IL-23 inhibitors.1,21-25 New therapeutic options are being sought in the management of NP, including lasers.26 All NP treatments require a long time to show their effects, and treatment success depends not only on the therapeutic agent’s type and effectiveness but also on patient-related factors.1,21-24
10. Baran R. The burden of nail psoriasis: an introduction. Dermatology. 2010;221:1-5.
11. Yorulmaz A. Dermoscopy: the ultimate tool for diagnosis of nail psoriasis? A review of the diagnostic utility of dermoscopy in nail psoriasis. Acta Dermatovenerol Alp Pannonica Adriat. 2023;32(1):11-5.
12. Yorulmaz A, Aksoy GG. Dermoscopic features of nail psoriasis: revisited. Skin Appendage Disord. 2022;8(5):389-98.
13. Singh SK. Finger nail pitting in psoriasis and its relation with different variables. Indian J Dermatol. 2013;58(4):310-2.
14. Yorulmaz A. Idiopathic trachyonychia (twenty-nail-dystrophy). J Cutan Med Surg. 2022;26(4):436.
15. Yorulmaz A, Yalcin B. Dermoscopy as a first step in the diagnosis of onychomycosis. Postepy Dermatol Alergol. 2018;35(3):251-8.
16. Yorulmaz A, Yalcin B. A novel dermoscopic feature in traumatic onycholysis. Our Dermatol Online. 2018;9(3):307-9.
17. Yorulmaz A. Dermoscopy reveals pseudopitting of the nail in psoriasis. Dermatol Pract Concept. 2023;13(4):e2023240.
18. Yorulmaz A et al. Nail lichen planus: a
patient with atypical presentation. Our Dermatol Online. 2018;9(4):434-6.
19. Yorulmaz A. Diphenylcyclopropenone alleviates trachyonychia in alopecia universalis. Int J Dermatol. 2024;DOI:10.1111/ijd.17240.
20. Yorulmaz A et al. Palmoplantar lichen planus with papular oral lesions: case report and a brief review of the literature. Turkiye Klinikleri J Dermatol. 2015;25(1):15-9.
21. Thomas L et al. Management of nail psoriasis. Clin Exp Dermatol. 2021;46(1):3-8.
22. Rigopoulos D et al. Recommendations for the definition, evaluation, and treatment of nail psoriasis in adult patients with no or mild skin psoriasis: a dermatologist and nail expert group consensus. J Am Acad Dermatol. 2019;81(1):228-40.
23. Hwang JK, Lipner SR. Treatment of nail psoriasis. Dermatol Clin. 2024;42(3):387-98.
24. Rigopoulos D et al. Management of nail psoriasis. Dermatol Clin. 2021;39(2):211-20.
25. Wride AM et al. Biologics for psoriasis. Dermatol Clin. 2024;42(3):339-55.
26. Jaalouk D et al. Lasers for the treatment of nail psoriasis: a systematic review. Int J Dermatol. 2024;DOI:10.1111/ijd.17304.
Malignancy Unmasked: Cutaneous Angiosarcoma Arising From Scald Burn: A Case Report
Authors: *Donnilyn G. Priela,1 Maria Franchesca S. Quinio-Calayag1
1. East Avenue Medical Center, Quezon City, Philippines *Correspondence to donnellpriela@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 10.17.24
Accepted: 02.26.25
Keywords: Case report, cutaneous angiosarcoma, diagnosis, malignancy, scald burn.
Cutaneous angiosarcoma is a rare and aggressive malignancy. This case highlights its unusual presentation following a scald burn, emphasizing the importance of early detection and the challenges in management. A 66-year-old male presented with progressive erythematous plaques on his scalp and face following a scald burn. Examination revealed indurated, violaceous patches with satellite nodules. Histopathology confirmed cutaneous angiosarcoma. Imaging showed extensive local invasion. The patient declined further treatment, and the disease progressed rapidly. Clinicians should maintain a high index of suspicion for angiosarcoma in non-healing post-traumatic lesions. Early biopsy and multidisciplinary management are crucial.
Key Points
1. Cutaneous angiosarcoma is a rare and aggressive malignancy originating from blood or lymphatic vessels, often affecting elderly Caucasian males. Trauma, such as scald burns, may rarely predispose individuals to its development.
2. This case study details a 66-year-old male presenting with extensive erythematous plaques following a scald burn, later diagnosed with cutaneous angiosarcoma through biopsy and imaging. Despite aggressive local progression, the patient declined treatment, highlighting ethical dilemmas in patient autonomy.
3. Early detection through suspicion and biopsy is critical in managing cutaneous angiosarcoma, especially in unusual presentations like post-burn lesions. Multidisciplinary collaboration is essential for treatment planning, considering factors like advanced age and patient preferences, which may influence therapeutic decisions and outcomes.
INTRODUCTION
Angiosarcoma is a rare and aggressive malignant neoplasm that arises from endothelial cells of blood or lymphatic vessels, accounting for approximately 1–2% of all soft tissue sarcomas.1 This malignancy predominantly affects older adults, with a higher incidence observed in elderly Caucasian males.2 Primary cutaneous angiosarcoma typically presents as solitary or multifocal ecchymotic lesions, most commonly affecting the face, scalp, or neck.2,3 Several risk factors have been associated with its development, including chronic lymphedema, prior exposure to ionizing radiation, environmental carcinogens such as vinyl chloride and arsenic, and immunosuppression.1-3 Due to its aggressive nature and high metastatic potential, angiosarcoma is associated with a poor prognosis, particularly in cases where diagnosis and treatment are delayed.4
The authors present a case of biopsyconfirmed angiosarcoma in a 66-year-old male who exhibited characteristic cutaneous lesions but declined treatment despite a multidisciplinary management approach. This case highlights the diagnostic challenges of angiosarcoma, the importance of collaborative care in treatment planning, and the ethical considerations surrounding patient autonomy in medical decision-making. Four months after diagnosis, the patient died, emphasizing the critical role of early detection and timely intervention in improving survival outcomes. This case underscores the need for heightened clinical awareness and patient education to facilitate early diagnosis and optimize treatment strategies for angiosarcoma.
CASE SUMMARY
A 66-year-old male presented with a sixmonth history of progressively enlarging erythematous plaques on the left cheek, originating from a scald burn caused by splashed cooking oil.
A few weeks after the burn, the patient noted the sudden appearance of a painless bruiselike lesion on the left cheek, associated with minimal brownish discharge. Two months later, the lesion gradually extended to involve the entire left face and scalp, accompanied by induration, hemorrhagic crusting, and severe pain that the patient rated 8/10. The patient self-medicated with thimerosal tincture and herbal washes, which proved ineffective. Initial consultations led to a diagnosis of an infected wound, and management included oral and intravenous antibiotics, as well as debridement. A biopsy was then performed and revealed only acute and chronic inflammation. Despite these interventions, the lesions persisted and progressively worsened. A referral to a private dermatologist prompted reevaluation, leading to the recommendation for a repeat biopsy.
The patient’s family history was noncontributory. There were no similar lesions in the family, nor any history of malignancies. The patient had no prior history of skin cancer, immunosuppression, or any known risk factors for cutaneous angiosarcoma.
A cutaneous examination revealed multiple well-defined, irregularly shaped erythematous plaques with extensive ulcerations, serosanguineous discharge, and hemorrhagic crusts. These lesions were predominantly located on the left side of the face, extending to the anterior scalp, left periorbital region, and left preauricular area, with several satellite lesions noted on the right frontal, temporal, and maxillary regions (Figure 1). Dermoscopy findings were nonspecific, revealing structureless red-toviolaceous or bluish areas interspersed with small yellow globular structures.
Three months after the first biopsy, a repeat incision biopsy was done and revealed irregular, anastomosing vascular channels filled with erythrocytes, some of which were lined by atypical large endothelial cells infiltrating between collagen bundles. Marked extravasation of erythrocytes was observed, along with diffuse lymphocytic infiltrates and atypical pleomorphic cells, some displaying
Erythematous plaques with extensive ulcerations, serosanguineous discharges, and hemorrhagic crusts on the left side of the face extending to the left anterior scalp, the left periorbital area, and the left pre-auricular region. Several satellite foci are seen on the right frontal area, right temporal, and maxillary area.
darkly staining nuclei, while others exhibited abundant cytoplasm with vesicular nuclei and prominent nucleoli. A few cells demonstrated a spindle-shaped configuration. These atypical cells were predominantly located in the papillary dermis in a diffuse pattern, with extension into the deeper dermis and infiltration between collagen bundles (Figure 2A-D). Immunohistochemical analysis showed positivity for CD31 (Figure 3A) and CD34 (Figure 3B).
A contrast-enhanced CT and angiography of the head demonstrated a multifocal, illdefined, extracranial superficial enhancing mass predominantly involving the left side of the head. The lesion was closely associated with the temporalis muscle and the anteroinferior aspect of the globe, receiving vascular supply from branches of the external carotid artery, including the posterior auricular, superficial temporal, and facial arteries. Additional smaller lesions were observed in the right frontal, temporal, and parietal regions (Figure 4). No cervical lymphadenopathy was detected bilaterally.
Metastatic evaluation, including chest and abdominal radiography as well as liver ultrasonography, yielded negative findings.
The diagnosis of cutaneous angiosarcoma was confirmed through clinical, histopathological, and imaging findings. Due to the extensive size and critical location of the tumor, involving the scalp, face, and periorbital region, a multidisciplinary team comprising dermatologists, plastic surgeons, medical oncologists, and ophthalmologists was assembled to manage the case. The multidisciplinary meeting led to the proposal of neoadjuvant chemotherapy with paclitaxel to reduce the tumor size, followed by a definitive wide excision and reconstruction. However, after chemotherapy was suggested, the patient declined all forms of medical and surgical treatment. The decision was influenced by financial constraints and concerns about his advanced age. Socioeconomic factors, including the cost of cancer treatment and limited access to specialized care, played a critical role in the patient’s reluctance to proceed with
Figure 1: Extensive ulcerated angiosarcoma of the face and scalp.
2A) Crack-like vascular spaces between collagen bundles. 2B) Irregular anastomosing vascular channels lined by atypical large endothelial cells (green arrows) with conspicuous dissecting of collagen (yellow stars). 2C) Marked RBC extravasation (yellow circles) admixed with lymphocytes (L) and atypical pleomorphic cells (green arrows). 2D) Spindle-shaped atypical endothelial cells (green arrows).
RBC: red blood cells.
therapy. Despite detailed counseling on the aggressive nature of angiosarcoma and the potential benefits of treatment, the patient chose not to proceed with the proposed management plan.
In the months following the diagnosis, the patient experienced rapid tumor progression and a significant decline in functional status. Despite the provision of symptomatic management and palliative care, the patient’s condition continued to deteriorate, culminating in death within four months of the initial diagnosis.
DISCUSSION
Angiosarcoma, a rare and aggressive malignant neoplasm of endothelial origin, arises from blood or lymphatic vessels and is characterized by uncontrolled endothelial cell proliferation. Representing less than 2% of all soft tissue sarcomas, angiosarcoma predominantly affects adults and elderly individuals.1,2 Cutaneous angiosarcoma, the most common subtype, typically manifests as solitary or multifocal bruise-like patches or plaques, most often involving the face, scalp, or neck regions.2,3 It occurs more frequently in older men and shows a marked predilection for the head and neck areas, particularly the Wilson-Jones type, which represents less than 0.1% of all head and neck cancers.5
Figure 2: Hematoxylin and eosin stain
Article
Figure 3: Immunohistochemistry.
A B
3A) CD31 stained the atypical large pleomorphic cells and endothelial cells of the blood vessels. 3B) CD34 stained the atypical endothelial cells of the blood vessels highlighting their proliferation in the dermis while dissecting collagen bundles.
4: CT images of the lesion.
Cutaneous angiosarcoma of the scalp and face is rare, and its occurrence following burn trauma is even more uncommon. This case underscores the rarity of cutaneous angiosarcoma arising from a scald burn, a phenomenon rarely reported in the Philippines. While burns have been associated with the development of malignant neoplasms such as squamous
cell carcinoma, basal cell carcinoma, and melanoma,6,7 this represents the first documented case of cutaneous angiosarcoma emerging from a scald burn in the country.
Existing literature suggests that trauma, including burns, may contribute to the development of angiosarcoma,8 although
Figure
the precise pathophysiological mechanisms remain poorly understood. Several studies have reported cases of angiosarcoma arising in areas subjected to prior trauma or chronic inflammation.8-10 Several studies have proposed that burn-induced trauma may facilitate the development of this malignancy by promoting chronic inflammation, angiogenesis, and abnormal vascular proliferation in the affected tissue.11,12
The differential diagnosis of cutaneous angiosarcoma includes various conditions that may mimic its clinical presentation, such as inflammatory disorders like rosacea, erysipelas, and cellulitis, as well as allergic reactions, arthropod bites, or bruises. For example, a 70-year-old male with worsening facial edema, initially suspected to be due to an infection, was ultimately diagnosed with cutaneous angiosarcoma following biopsy.13 Similarly, a 75-year-old male presenting with persistent erythematous patches on the face, initially misdiagnosed as rosacea, was later diagnosed with cutaneous angiosarcoma after the lesions progressed to purpura and violaceous plaques.14 The variability in clinical presentation often leads to delays in diagnosis.
As highlighted by Asgari et al.15 the HeadTilt Maneuver, where the patient tilts their head below heart level for 5-10 seconds, can be a useful diagnostic tool for vascular neoplasms like cutaneous angiosarcoma. This maneuver increases vascular engorgement and enhances the violaceous appearance of the lesion, helping to define tumor borders and identify skip areas, which is crucial for surgical planning. Early diagnosis is essential, as untreated cutaneous angiosarcoma can rapidly progress, infiltrating surrounding tissues and leading to complications such as edema, ulceration, and hemorrhage. At the time of diagnosis, the average tumor size is typically 3–5 cm.16
The rarity of cutaneous angiosarcoma is reflected in the limited number of case reports available in the literature. The occurrence of cutaneous angiosarcoma
following a burn injury, as observed in the authors’ patient, is exceptionally uncommon. Bhatti et al.8 reported a case of a 91-year-old female who developed pruritic red patches on her scalp following a burn from a salon hair dryer. Despite various clinical diagnoses and treatments, the lesion progressed into a large purplish mass with persistent bleeding. An incisional biopsy confirmed the diagnosis of angiosarcoma, exhibiting a similar presentation to the current case of cutaneous scalp angiosarcoma following a burn.
A comprehensive diagnostic workup, including biopsy and imaging, is crucial for the accurate diagnosis of cutaneous angiosarcoma. Imaging is essential to assess the extent of the lesion and rule out metastatic disease. MRI is the preferred modality for evaluating localized disease, as it provides superior soft tissue contrast, aiding in the assessment of tumor extent and involvement of adjacent tissues. CT is primarily utilized to detect metastatic disease and monitor treatment response, especially in organs such as the lungs and liver. Imaging findings should be interpreted in conjunction with the patient’s clinical history and demographics, and biopsy remains critical for a definitive diagnosis.16
Biopsy is essential for confirming the diagnosis of angiosarcoma, with histopathological examination typically revealing vessel-like structures forming anastomosing networks, cellular atypia, mitotic figures, and multilayered endothelial lining. In poorly differentiated areas, the tumor may display sheet-like growth patterns, often accompanied by hemorrhage and necrosis. Immunohistochemical staining with endothelial markers such as CD34, CD31, von Willebrand factor, Ulex europaeus agglutinin 1, and vascular endothelial growth factor plays a critical role in further confirming the diagnosis. In this case, both CD31 and CD34 stains were positive, which conclusively confirmed the diagnosis of angiosarcoma.17
The definitive management of angiosarcoma requires surgical intervention to achieve
an oncologically appropriate margin. A multidisciplinary approach, combining surgery, radiation, chemotherapy (e.g., paclitaxel), and immuno-oncology agents, is essential for optimal treatment. Radiation therapy is employed for residual disease or when surgical resection is not feasible, while chemotherapy may be used to reduce tumor size or manage advanced disease. In cases of unresectable cutaneous angiosarcoma, treatment options include radiation, chemotherapy, palliative surgery, or supportive care to alleviate symptoms. Palliative care plays a critical role in enhancing the patient’s quality of life, as the prognosis for advanced cutaneous angiosarcoma remains poor.1,18,19
Socioeconomic and psychological factors also significantly influence treatment decisions in cutaneous angiosarcoma. Financial constraints, limited access to specialized care, and treatment costs can delay diagnosis and impact adherence. Psychological distress, fear of disfigurement, and lack of social support may also lead patients to decline aggressive treatments.
In this case, the patient was diagnosed with cutaneous angiosarcoma involving extensive areas of the scalp, face, and surrounding structures, making the disease locally advanced and unresectable. The rapid progression of the large tumor rendered surgical intervention unfeasible, and the treatment plan shifted to focus on radiotherapy to control local growth and alleviate symptoms. Chemotherapy with paclitaxel was also initiated to reduce the tumor size. Additionally, palliative care was considered to manage symptoms, as the patient expressed reluctance toward aggressive treatments. Despite these interventions, the prognosis remained poor, given the aggressive nature of the disease and the advanced stage at presentation.
The overall prognosis for scalp angiosarcoma is generally unfavorable, primarily due to its aggressive nature, high likelihood of local recurrence, and metastasis. Prognostic
factors associated with a poor outcome include being over 70 years of age, a tumor size greater than 5 cm, and the tumor being located on the head or scalp. As noted by Pawlik et al.19 cutaneous angiosarcoma typically follows a rapidly fatal course, particularly when diagnosed at a dvanced stages.
In the case of the authors’ patient, the challenge in diagnosing cutaneous angiosarcoma, due to its deceptive clinical presentation, coupled with the progression to an advanced stage before detection, reflects these observations. The advanced stage of the tumor at presentation, along with its location on the scalp, rapid progression, and the patient’s age, aligns with key risk factors for a poor prognosis. These factors underscore the challenges in managing cutaneous angiosarcoma and emphasize the critical importance of early detection to improve survival outcomes.
CONCLUSION
Cutaneous angiosarcoma of the scalp and face is a rare and aggressive malignancy that can present in a deceptive manner, often following injuries such as minor burns or lesions that are initially misdiagnosed or inadequately treated. This case underscores the importance of maintaining a high level of suspicion for angiosarcoma in lesions of the face and scalp, as early detection is crucial for improving survival outcomes. The challenges associated with managing angiosarcoma are further exacerbated by treatment delays, emphasizing the need for prompt intervention and effective communication with patients. A multidisciplinary approach, involving dermatopathology, surgery, and oncology, is essential to optimize treatment outcomes and address the complexities of this devastating malignancy.
Future research should focus on elucidating the precise mechanisms by which trauma, including scald burns, contributes to the
development of cutaneous angiosarcoma. Understanding the molecular and inflammatory pathways involved may provide insights into early biomarkers for detection and potential therapeutic targets.
This case also highlights the importance of addressing financial and psychological barriers to treatment. A comprehensive, patient-centered approach that integrates oncologic care with financial assistance and psychosocial support is crucial to improving treatment adherence and overall outcomes.
References
1. Cao J et al. Angiosarcoma: a review of diagnosis and current treatment. Am J Cancer Res. 2019;9(11):2303-13.
2. Young RJ et al. Angiosarcoma. Lancet Oncol. 2010;11(10):983-91.
3. Patel SH et al. Angiosarcoma of the scalp and face: the mayo clinic experience. JAMA Otolaryngol Head Neck Surg. 2015;141(4):335-40.
4. Wang L et al. Clinicopathological features and prognostic factors in angiosarcoma: a retrospective analysis of 200 patients from a single Chinese medical institute. Oncol Lett. 2017;14(5):5370-78.
5. Ramakrishnan N et al. Cutaneous angiosarcoma of the head and neck - a retrospective analysis of 47 patients. Cancers. 2022;14(15):3841.
6. Lindelöf B et al. Burn injuries and skin cancer: a population-based cohort study. Acta Derm Venereol. 2008;88(1):20-2.
Future efforts should focus on developing accessible healthcare strategies, particularly in resource-limited settings, to ensure timely diagnosis and intervention for patients with this rare and challenging malignancy.
Patient Consent
Written informed consent was obtained from the patient for the publication of this case report, including clinical details and images. Efforts have been made to anonymize the data to maintain confidentiality.
7. Lee HB et al. Malignant melanoma on a thermal burn scar. Arch Craniofac Surg. 2019;20(1):58-61.
8. Bhatti Z et al. Extensive cutaneous scalp angiosarcoma. Cureus. 2018;10(6):e2868.
9. Ikeda H et al. A case of a motor vehicle collision suspected as associated with development of angiosarcoma. Leg Med (Tokyo). 2024;67:102332.
10. Jung YJ et al. A clinicopathologic feature and survival analysis of cutaneous angiosarcoma: a single tertiary center study. Ann Dermatol. 2024;36:e62.
11. Kowal-Vern A, Criswell BK. Burn scar neoplasms: a literature review and statistical analysis. Burns. 2005;31(4):403-13.
12. Jackson JR et al. The codependence of angiogenesis and chronic inflammation. FASEB J. 1997;11(6):457-65.
13. Bajaj S et al. A novel presentation of cutaneous angiosarcoma: a case report and review. Indian J Med Paediatr
Oncol. 2017;38(3):363-6.
14. Wong A Flores J. Cutaneous angiosarcoma of the head and neck resembling rosacea: a case report. SAGE Open Med Case Rep. 2020;8:2050313X20940419.
15. Asgari MM et al. Head-tilt maneuver for vascular neoplasms. Dermatol Rev. 2007;9(6):295-301.
16. Bhaludin BN et al. Imaging features of primary sites and metastatic patterns of angiosarcoma. Insights Imaging. 2021;12(1):176.
17. Selim A et al. Angiosarcoma: a case report and review of the literature. Cutis. 2005;76(5):313-7.
18. Rampinelli H et al. Cutaneous angiosarcoma. Case Rep Dermatol. 2018;10:55-60.
19. Pawlik TM et al. Cutaneous angiosarcoma of the scalp: a multidisciplinary approach. Cancer. 2003;98(8):1716-26.