Soames’ & southam’s oral pathology 5th edition edition max robinson - Download the ebook now for ful
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
80+ Python Coding Challenges for Beginners: Python Exercises to Make You a Better Programmer. No Prior Experience Needed: 80+ Python Challenges to Launch ... Journey. Katie Millie
The fourth edition of Soames’ and Southam’s Oral Pathology wastheculminationofaprocessofrefinement of bothcontent and production Beingtasked to produce a fifth edition was a major challenge for us More thantenyearshas elapsedsincethefourthedition was printed andasknowledgeofthepathologicalmechanisms underlying oral diseases has advanced, new evidence-based management guidelines and therapies havebecomeavailable Accuratediagnosisisincreasinglybasedonamulti-disciplinaryapproachinvolvingthe integrationofrapidlyevolvingimagingtechniquesandmolecular pathologytests Sounddiagnosis,however, isstillbasedonan informedcliniciantakinganaccuratehistory,makingathoroughclinicalexamination,and selectingappropriatediagnostictests Themoderndentalcareprofessional intrainingand inclinicalpractice hastocontendwithavastly expandedknowledgebase Understandingoforalandmaxillofacialpathology is essentialiftheclinicianistonavigatesuccessfullythroughclinicalguidelines,maketimelyreferralstospecialists,andprovidegoodcarefor patients Thedentalcurriculumhaschangedtoreflectthisexpansionofknowledge High-qualityspecialisttextsarenow availablethatprovideintegratedclinico-pathologicalapproaches to dental caries, periodontal diseases,temporomandibular joint disorders, and oral diseases in children To reflect this we have chosen to reducethe content ofchapters on these topics.Sections on certain diseases thathavebecomelessprevalenthavebeenremovedandnewmaterialondisordersthataremorelikelytobe encountered nowadays has been added This radically revised edition begins with an introductory chapter thatoutlinestheimportanceofclinicalassessmentandhowthesynthesisofadifferentialdiagnosisinformsthe selection offurther investigations,includingthose provided bythecellular pathology laboratory The subsequentchaptersguidethereaderthroughthevariousdiseasesthattheymayencounterintheoralcavity,startingwithacomprehensivesectionontheoralmucosa,whichleadsontoanupdatedchapteronoralcancerand oral potentially malignant disorders Diseases ofthe salivary glandsare dealt withinthesucceedingchapter Thetextthenfollowsthesequenceofthepathologyofteethandsupportingstructures,includingjawcystsand odontogenictumours,alongwithbonedisorders Therearetwonewchapters:onethatdescribestheimportant lesions that clinicians should recognize on the face and lips, and another that explores the differential diagnosisofnecklumps,whichweconsidertobeanimportantpartoftheclinicalexamination Weconclude withachapterontheoralmanifestationsofsystemicdisease,whichhighlightstheimportanceoforaldisease in the context of human disease We hopethat wehave preserved muchoftheexcellent content and character ofthefourthedition Theradiologycontenthasbeenupdatedbyincludingexamplesofcross-sectional imaging Virtually all the photomicrographs have been replaced with carefully selected images to illustrate keypathologicalfeatures Wehavecontinuedthethemeoftabulationandtextboxes,whichsoenhancedthe fourthedition,asweagreewithourpredecessorsthatthesesignificantlyaidlearning.
Wehavepleasureinacknowledgingthehelp wehavereceivedfromour manycolleagues Weparticularly wish to express our gratitude to Dr lain MacLeod, Dr Andrew Carr, and Tony Owens of the Department of Dental andMaxillofacial Radiology,Newcastle DentalSchool for providingmany of the radiological images. JanHowarthoftheDepartmentofMedicalIllustration,NewcastleDentalSchool Colleaguesthathavekindly providedphotographs:DrNickBown,Dr IanCorbett,Professor EmeritusJohnEveson,DrNaikaGill,DrNeil Heath Professor Clifford Lawrence, Dr Pia Nystrom, Professor Vinidh Paleri, Professor Paul Speight, and Dr RachelWilliams Colleagueswhohavetakenthetimetocriticallyreviewdraftsofthemanuscript:DrSonjaBoy, ProfessorJustinDurham,DrGilesMcCracken,ProfessorPhilipPreshaw,andDrMarionRobinson
MR, KH, MP, PS
Acknowledgements
OxfordUniversity Press wishesto acknowledgethecontribution of Professor JV Soames and Professor JC SouthamtothepopulartextbookOral Pathology,thefourtheditionofwhichformsthebasisofthiswork This populartextbookhasenlightenedgenerationsofdentalstudentsaswehopethisnewbookdoestoo
Themostcommonoraldiseasesare dentalcariesandperiodontaldisease (Fig 1.1) The diagnosis andtreatment of these diseases arethe focus of the majority of dentists, dental therapists,and dental hygienists Nevertheless,itistheresponsibilityofthedentalhealthcareprofessionaltoprovideaholisticapproachtomanagementthatensuresboth good oral and general health for their patients A broad knowledge of therange of diseasesthataffecttheoral cavity isessentialandalsoan appreciation that oral disease may be the first sign of an underlying systemic disease Before this knowledge can be applied, the clinician
must obtain an accurate patient history and undertake a systematic clinical examination These key clinical skills underpin both medicine and dentistry, and are an absolute requirement to formulate a differentialdiagnosis Theuseofimagingmodalitiesandlaboratorytestsare often requiredtoreacha definitive diagnosis,andit is the justification andinformedchoiceoftheseadditionalinvestigationsthatwillfacilitate atimelyandaccuratediagnosis Followingdiagnosis,appropriatetreatment can be instituted,the ideal outcome beinga return to health or controlofthepatient’ssymptomsinrecalcitrantchronicdiseases
Fig.1.1 Theoralcavityinhealthanddisease.
Obtaininganaccuratehistory
Historyofthepresentingproblem
Obtainingaclear andprecise clinical history isessential The clinician must listen carefully to the information conveyed by the patient and then use direct questioningto collect additional data to construct an accurate picture of the patient’s problem This can be a significant challenge and requiresexcellent communication skillsto builda good patient-clinicianrelationship
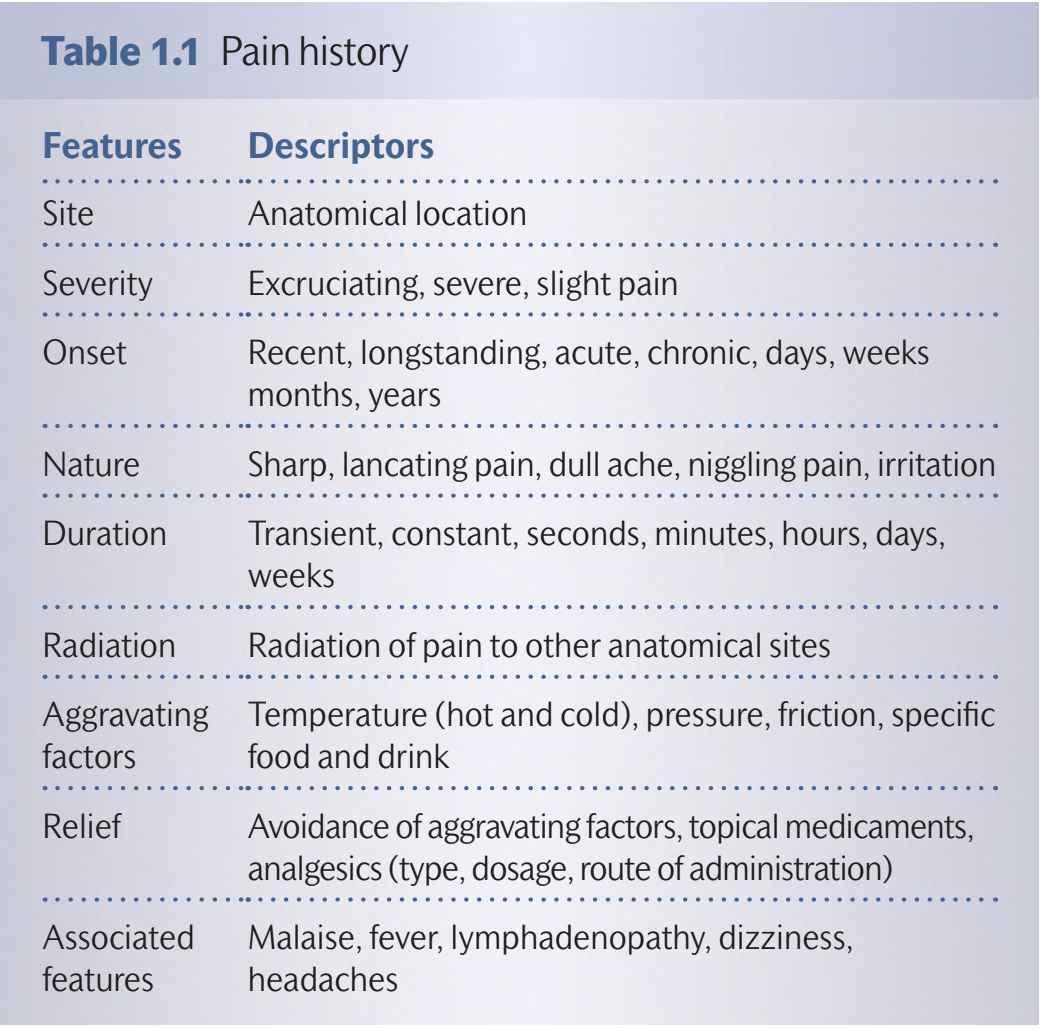
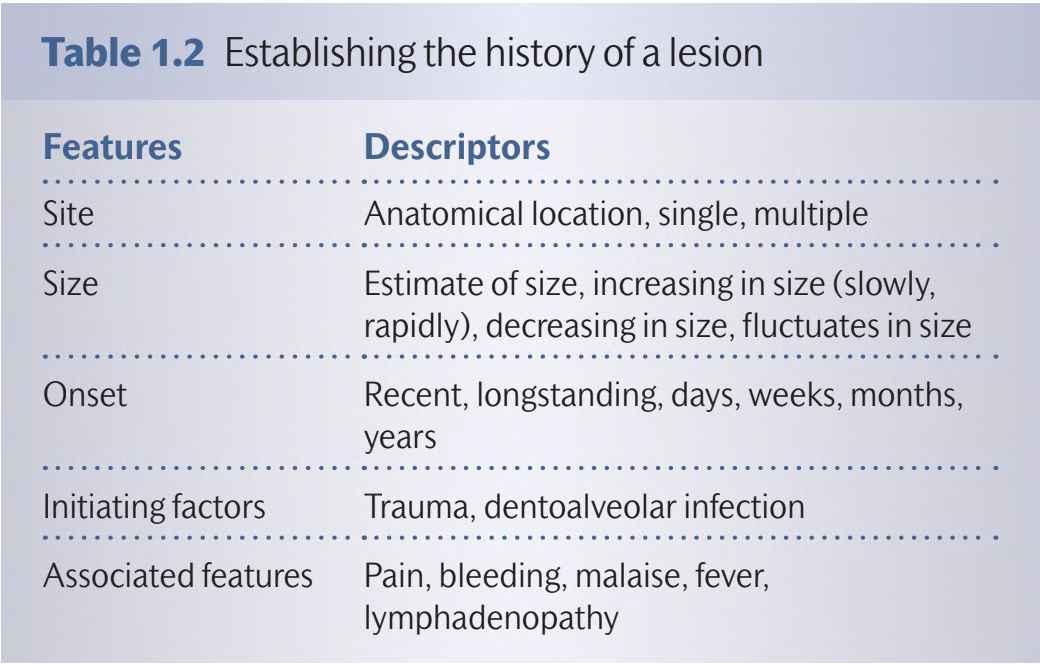
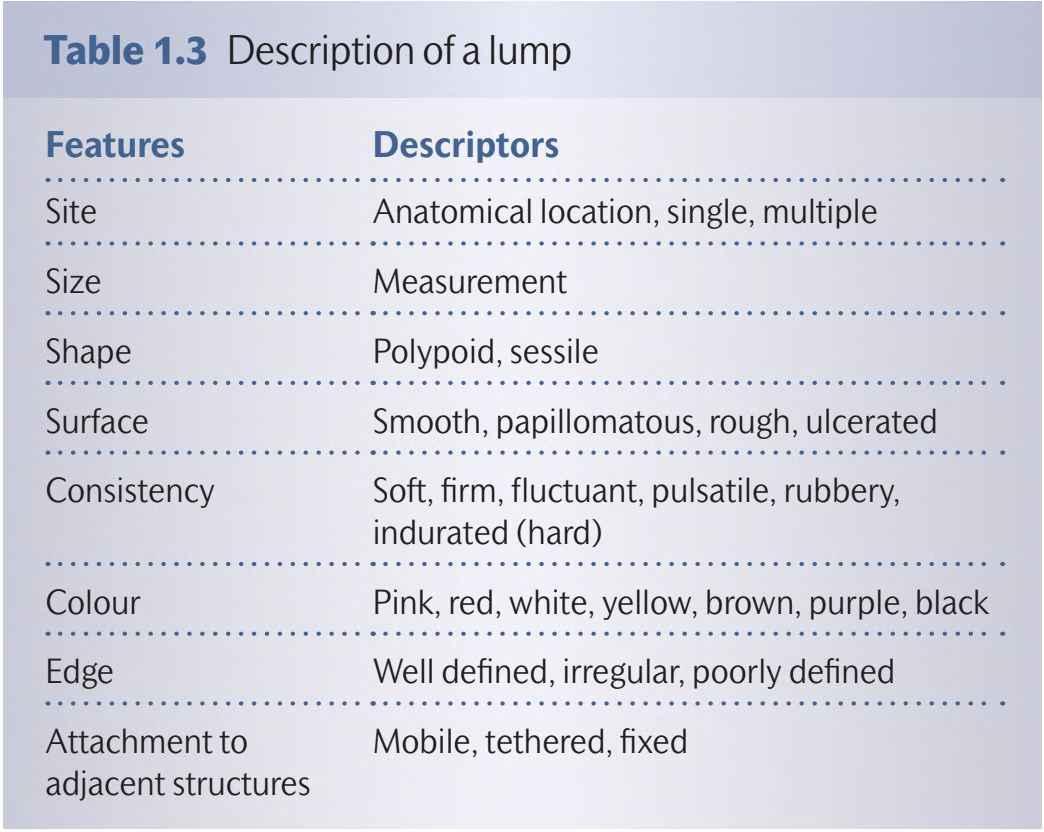
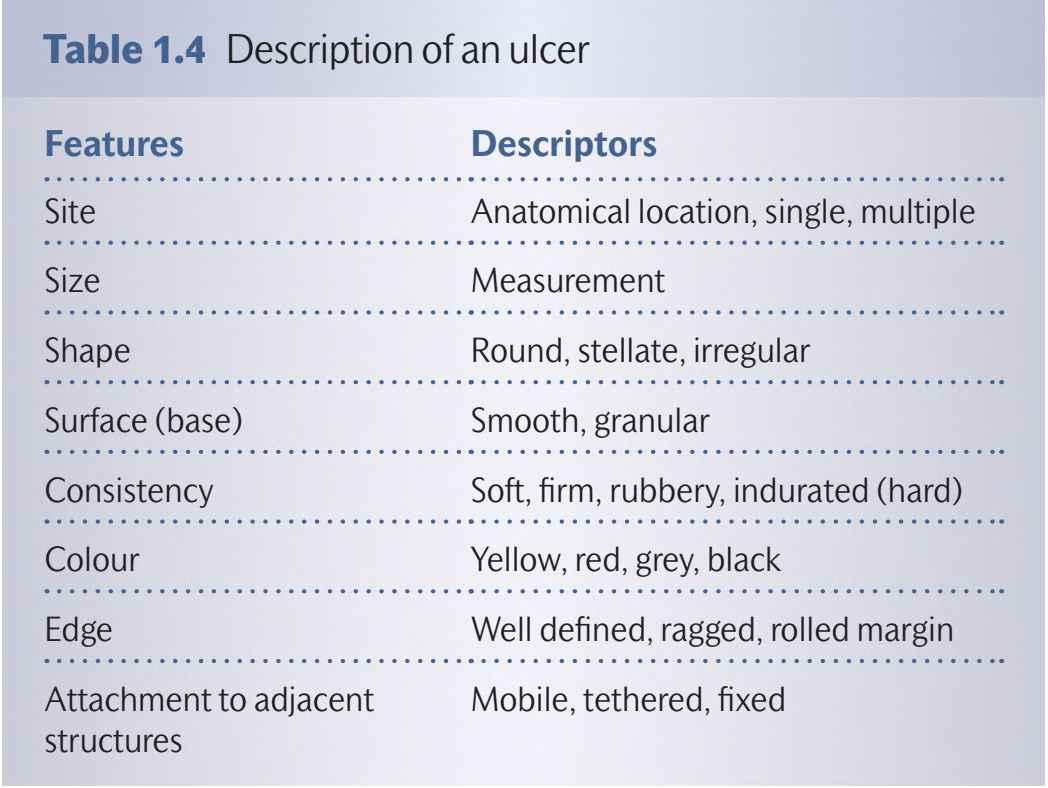
The most common presenting problems relate to pain or the development of a lesion: swelling, lump, ulcer, or white/red patch. To establish a comprehensive pain history, the features listed in Table 1.1 should be addressed Obtaining an accurate history for a lesion is dependent on the patient noticing the abnormality in the first instance and, as a consequence,the information may be rather vague; however, it is important to ascertain the key points listed in Table1.2
(Chapter 10) and highlight any issues relatingto proposed medical or surgicalinterventions
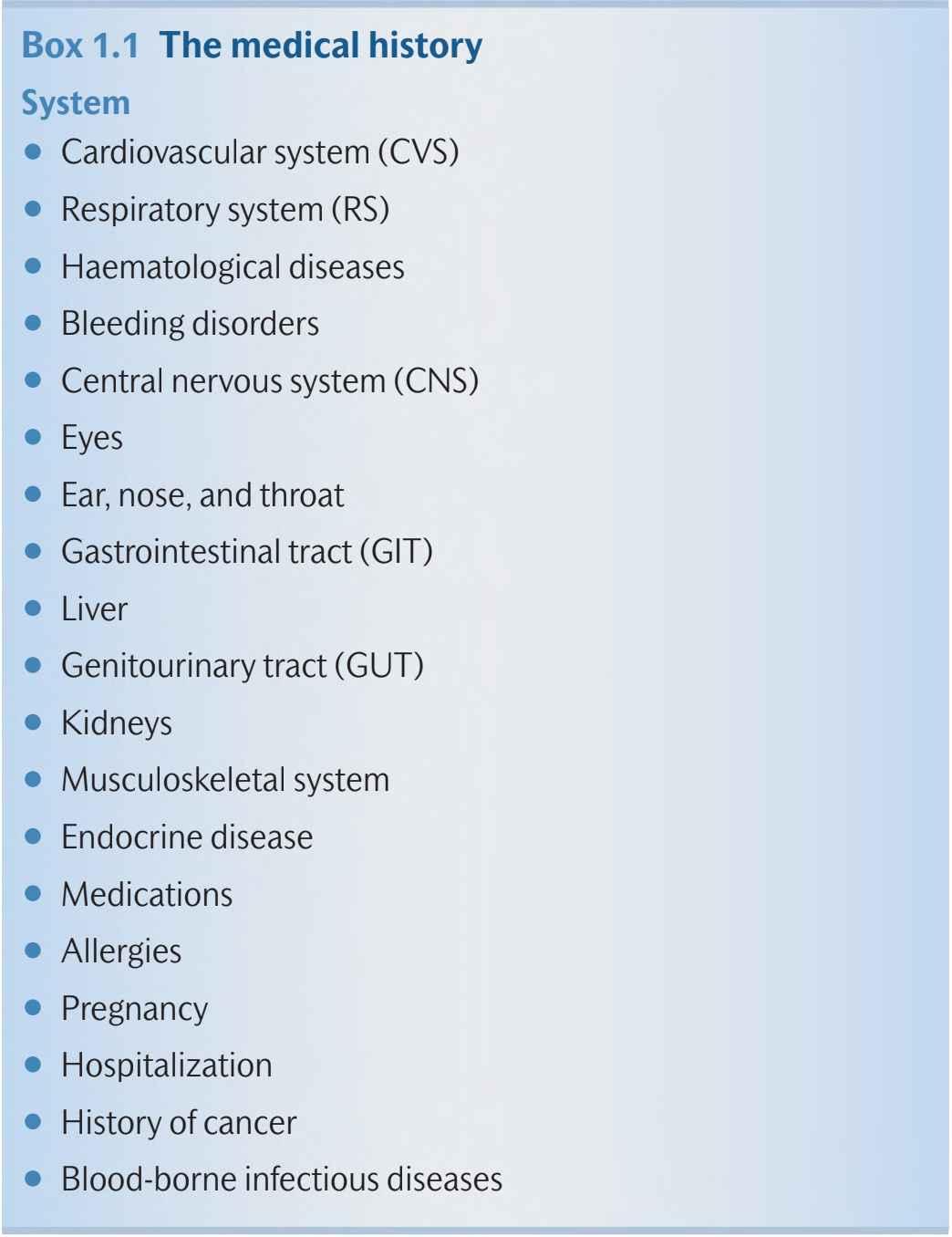
Box1.1 Themedicalhistory
System
•Cardiovascular system(CVS)
•Respiratorysystem(RS)
•Haematologicaldiseases
•Bleedingdisorders
•Centralnervoussystem(CNS)
•Eyes
•Ear,nose,andthroat
•Gastrointestinaltract(GIT)
•Liver
•Genitourinarytract(GUT)
•Kidneys
•Musculoskeletalsystem
Familyhistory
Some diseases are heritable and have a characteristic pedigree that canbemappedovermultiplegenerations,eg haemophilia Otherdiseasesshowapreponderancetoaffectindividualswithinfamilygroups, but it is difficultto predict which individuals will beaffectedandrelatives may suffer toa greater or lesser extent These familialtraits may beheritablewithvariablegeneticpenetranceandexpressivity,or may reflectexposuretosimilarenvironmentalandsocialfactors
•Endocrinedisease
•Medications
•Allergies
•Pregnancy
•Hospitalization
•Historyofcancer
•Blood-borneinfectiousdiseases
Socialhistory
Thesocialhistorymaybeofdirectrelevancetooraldiseaseandgeneral health For example,tobaccoconsumption and alcoholabuseare risk factors for the development of oral cancer, as well as other systemic diseases,eg cardiovascular disease and liver disease Factors suchas occupationandpersonalstatusprovideadditionalinformationandmay influencethecareplan
The physical assessment of a patient starts when the patient enters the surgery.Thecliniciancangaugeanumber of subtlesigns fromthe patient’sgeneralappearanceanddisposition Thecliniciancanquickly establishgeneralhealthandmobility Onceseated,examinationofthe complexionandhandsmayrevealsignsofsystemicdiseases,eg.finger clubbing,nailabnormalities,skindiseases,andeyesigns
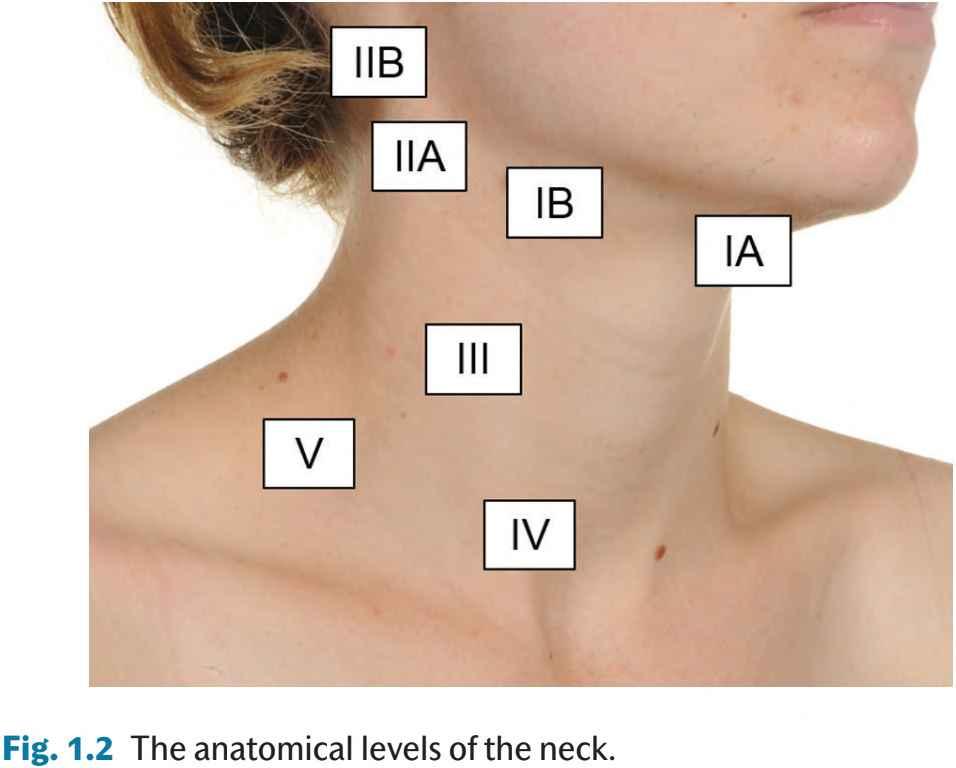
Routineexaminationoftheoro-facialcomplexshouldincludeinspection and palpation ofthe neck The sequence shouldcommence with the submandibular triangle, which contains the submandibular gland and level Ilymphnodes(level IA submental lymph nodes and levelIB submandibular lymphnodes) Thisisfollowedby levelIIlymphnodes, superior part of the deep cervical chain, includingthe jugulodigastric lymph node and level II lymph nodes (levels IIA and MB lymph nodes located anterior and posterior to the accessory nerve, respectively), levelIIIlymph nodes(middle part of the deep cervical chain),level IV lymphnodes(theinferiorpartofthedeepcervicalchain,whichincludes thejugulo-omohyoidlymphnode),andlevelVlymphnodesintheposterior triangle of the neck (Fig 1.2) Finally,the mid-line
Diagnosisoforaldisease
theneck,which includethe larynx,trachea,andthyroid gland,should be examined The presentation of lumps in the neck is covered in Chapter 9 Any lumps, eg enlarged lymph nodes, are described by anatomical site, size, consistency (cystic, soft, rubbery, or hard), relationshiptounderlyingtissues(fixedor mobile),andwhether palpation elicitspain Theparotidglandsarealsoexaminedandpalpatedforany abnormalities
The examination then focuses on assessment of the temporomandibular joints and the muscles of mastication to assess functional abnormalitiesandanymuscletenderness Themusclesoffacialexpression are also assessed, to establish facial nerve function Any sensory
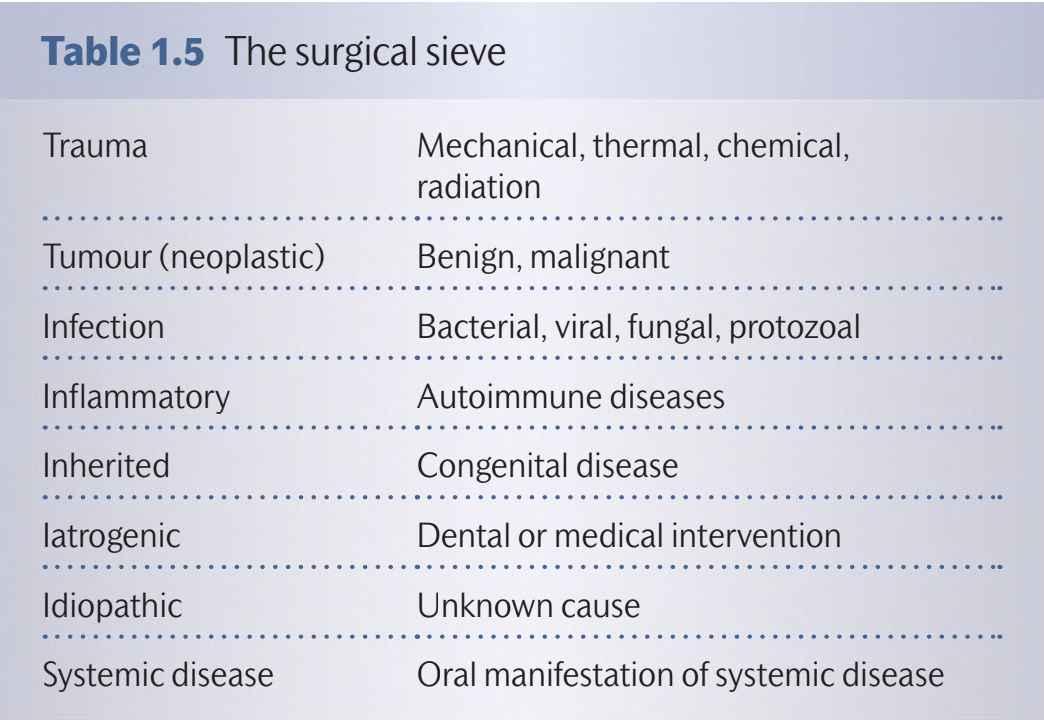
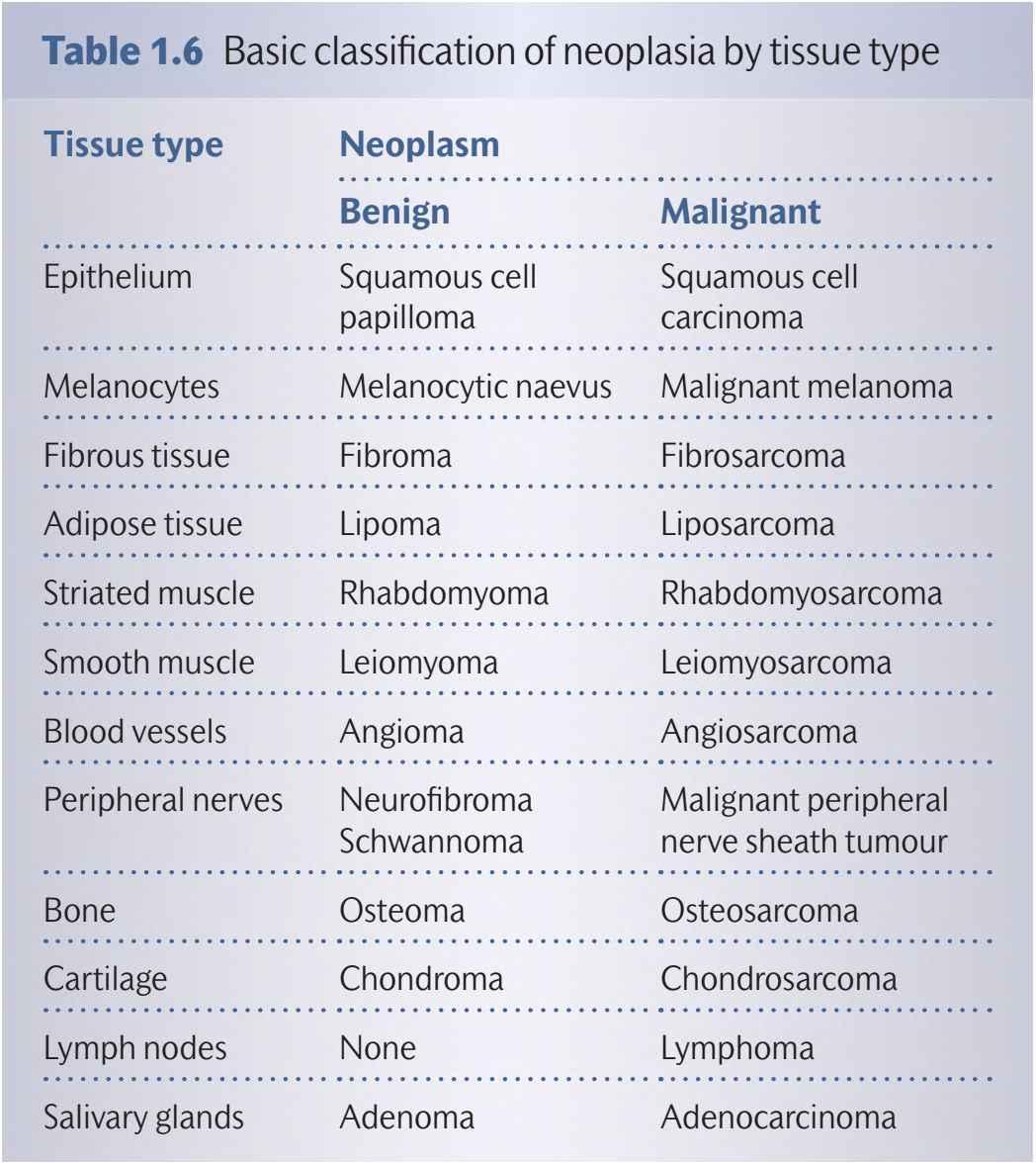
Formulating a differential diagnosis requires the integration of information fromthe history andexamination witha sound knowledge of oral andsystemic diseases Thereareseveral strategiesthatcan facilitatethisthoughtprocess Forexample,the‘surgicalsieve’canbeused to generate a list of diseasesaccordingtoaetiology andpathogenesis (Table1.5) Whenconsideringa neoplasm,visualizingtheanatomical structuresinthevicinityofthelesioncanalsohelptoformulatethedifferential diagnosis(Table1.6) Withincreasingexperienceandclinical acumen it ispossibletofocusa wide differentialdiagnosis,depending on subtleclinical findings andthe likelihoodofa particular disease at a specific anatomical site For example, a swelling in the lower labial mucosa is most likely to be a mucocoele, whereas a similar swelling intheupper labialmucosa ismore likelytobea benignsalivary gland neoplasm Itisworthconsideringthemaximthatcommonentitiesare more likely to be encountered than those that are rare For instance,
Table1.5 Thesurgicalsieve
Trauma Mechanical,thermal,chemical, radiation
Tumour(neoplastic) Benign,malignant
Infection Bacterial,viral,fungal,protozoal
Inflammatory Autoimmunediseases
Inherited Congenitaldisease
Iatrogenic Dentalormedicalintervention
Idiopathic
Systemicdisease Unknowncause
Oralmanifestationofsystemicdisease
Choosingandorderinginvestigations
Once a differential diagnosis has been formulated,ancillary investigationsaretypicallyrequiredtoarriveatthedefinitivediagnosis.Additional informationmay beobtainedby imagingtechniques:ultrasound,radiographs, computerized tomography (CT), and magnetic resonance imaging(MRI) Inthemajorityofcasesanaccuratediagnosiswillrequire theanalysisofabiologicalsamplebyoneofthelaboratory-basedmedical specialties: haematology,clinical chemistry, immunology, medical microbiology,virology,cellular pathology (cytopathology andhistopathology),andmolecularpathology(cytogeneticsandgenetics)
Imagingtechniques
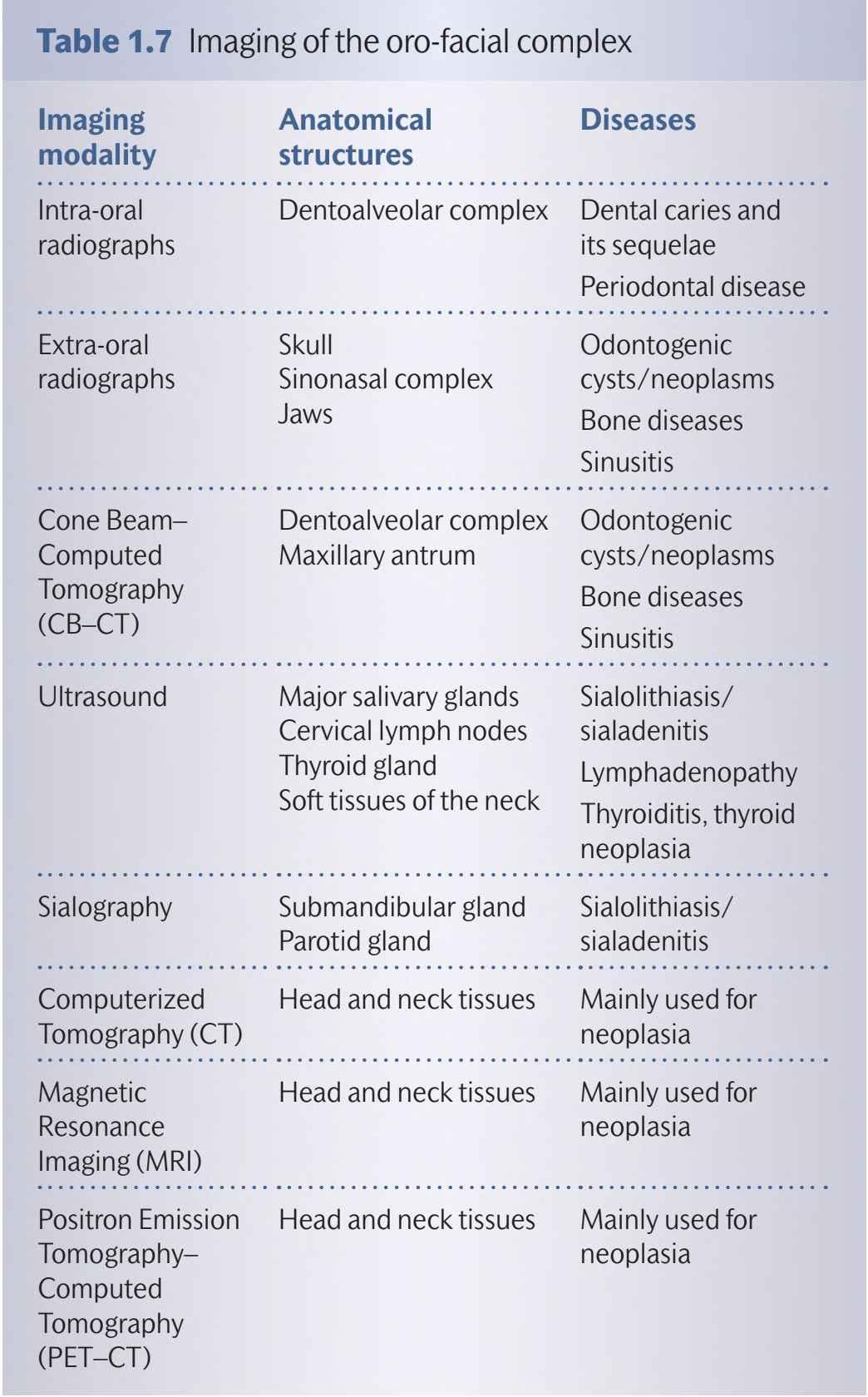
The main imagingtechniques used in the oro-facial complex are listed in Table 1.7 The decision to use imagingas part of the clinical examination is governed by three core principles: justification of the imaging technique,optimizationoftheradiationdose,andlimitingtheamountof
an oro-facial swelling in a patient with a neglected dentition is most likely to be a dentoalveolar infection If the clinical assessment indicates that the lesion is benign,then the differential diagnosis should focusoninfectivecauses,hyperplasticlesions,andbenignneoplasms Conversely,clinicalsignsandsymptomsofadestructivelesionsuggest malignancy
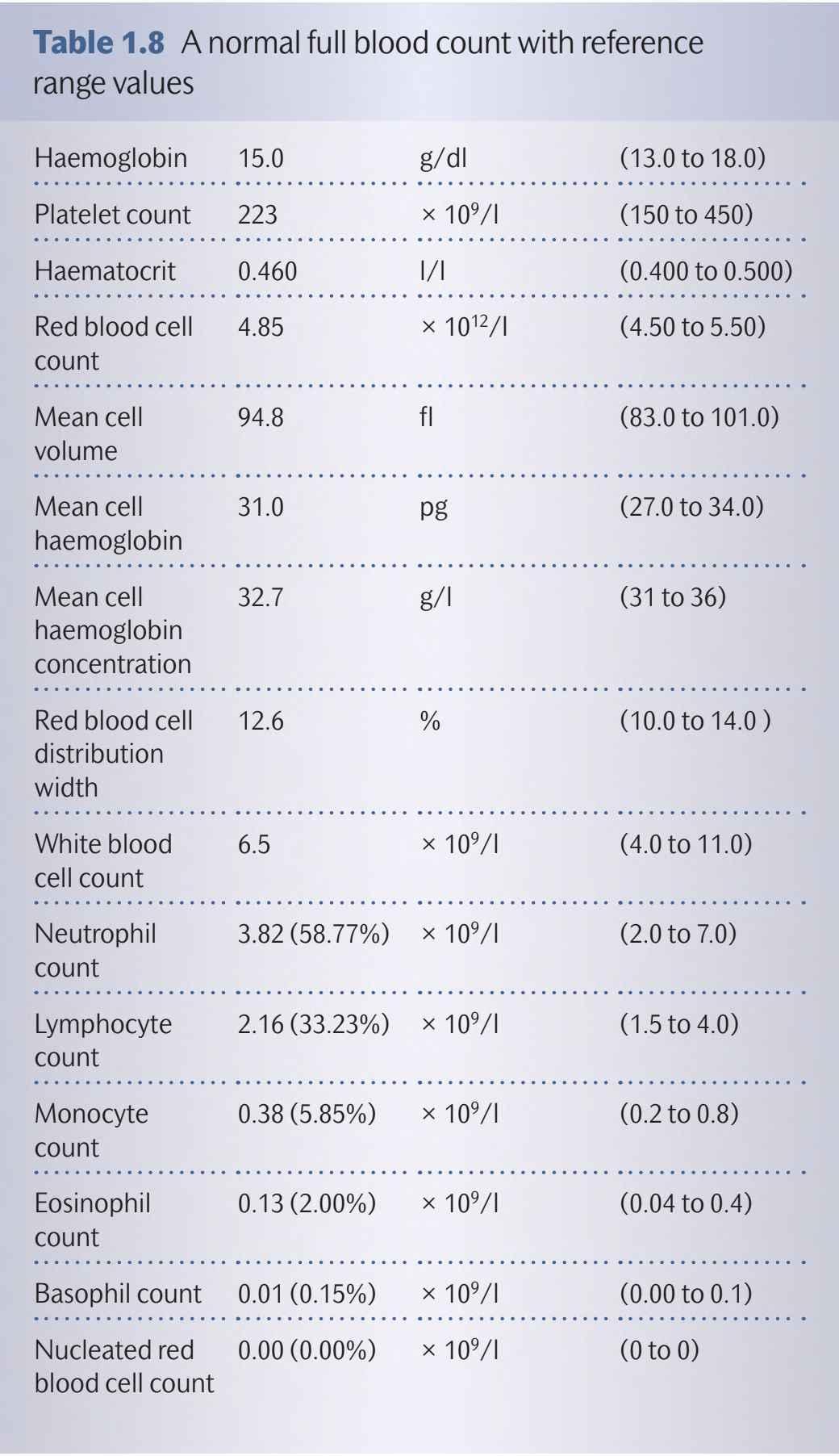
The analysis of biological fluids, mainly blood and urine, can yield important information about the general health of the patient A full bloodcountgivesinformationabouttheconstituentsoftheblood:the erythrocytes,leukocytes,andplatelets(Table1.8) Analysisofthehaemoglobin,redcellcount(RBC),anderythrocytesize(meancellvolume, MCV)maydemonstratethatthepatient isanaemic.Toofew platelets, termed thrombocytopenia, indicates a risk of excessive bleeding
Increased numbers of leukocytes (WBC) may be caused by infection or leukaemia,whereasdepletedleukocytesmay identifyapatientthat is immunocompromised Other blood tests include an assessment of themicronutrientsrequiredfor haematopoiesis,the haematinics:iron, vitaminB12,andfolate,whicharemeasuredbytheserumferritin,serum vitamin B12, and serum or red cell folate, respectively These specific testsareimportantinunderstandingthecauseofanaemia Analysesof bloodglucoseandglycosylatedhaemoglobin(HbA1c)arerequiredfor theassessmentofdiabetesmellitus Urinalysisisoftenusedasasimple screenfor diabetes,haematuria,andproteinuria Anautoimmuneprofile can be usedto screen for autoimmune diseases,such as Sjogren’s syndrome and systemic lupus erythematosus Other immunological assaysareimportantinthediagnosisofhypersensitivityreactions
identification ofthe aetiological agent and determiningthe sensitivity ofthemicroorganismtoavarietyofantimicrobialagentsarecoreactivitiesofthemedicalmicrobiologyservice.
Cellularpathology
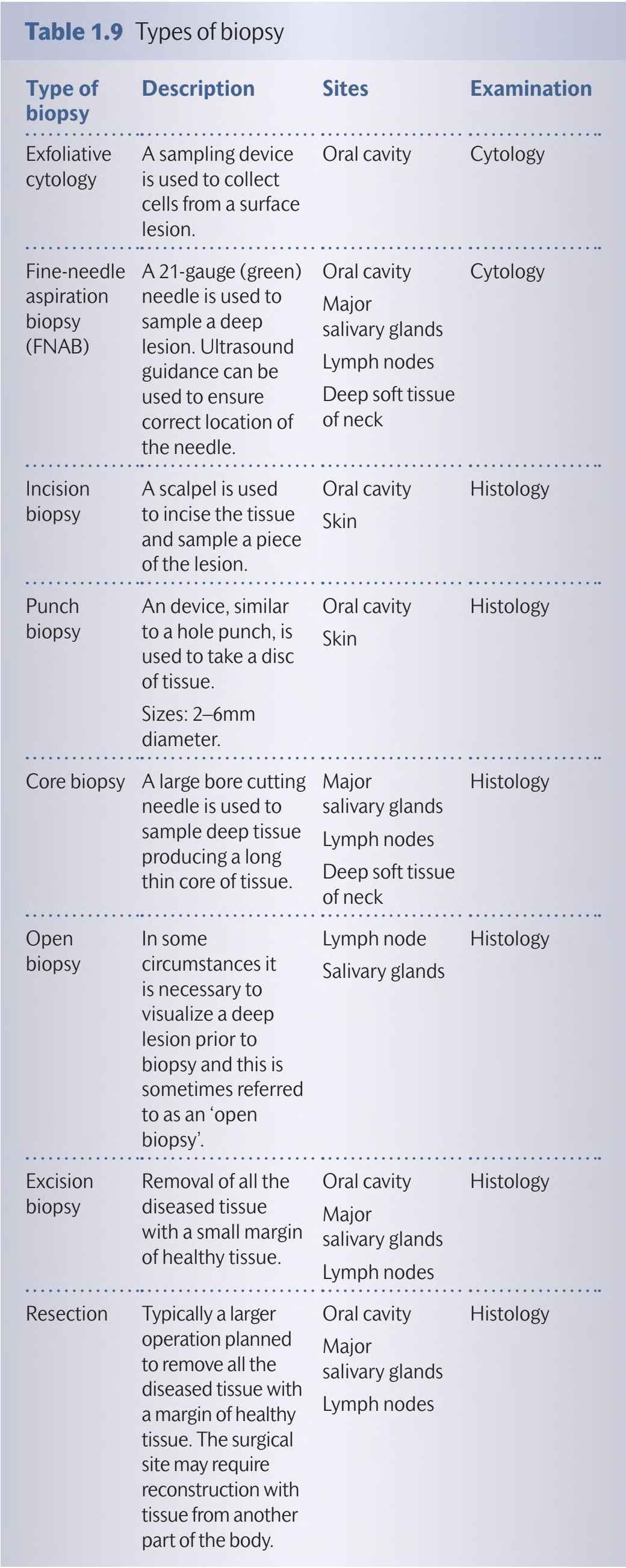
Acquisition of material from a lesion, cells for cytopathology and tissue for histopathology, is the most common method of establishing a definitive diagnosis Avarietyofmethodscanbeusedandareoutlined inTable1.9
Cytology samples, collected by either an exfoliative method (e g brush biopsy) or fine-needle aspiration, can be used to prepare smears on glass slides, which are either air-dried or preserved in an alcohol-based fixative Alternatively, brush biopsies and needle washings can be collected inproprietary liquid-based cytology fluid (e g SurePath,BD or ThinPrep,Hologic) Currently,brush biopsy of oral lesions is not widely used, as most clinicians proceed directly to tissue biopsy However, the brush biopsy is a safe, simple, and
whether the sample is representative of the lesion Fine-needle aspiration biopsy (FNAB) is mainly used during investigation of a lumpintheneckoroneofthemajorsalivaryglands Itisasafe,simple, low-cost technique, which is usually tolerated by patients Multiple needle passes can be employed to increase cellular yield,and some operators use ultrasound guidance to ensure adequate sampling Diagnostic information can be provided rapidly, as there are only a few laboratory steps required to produce a slide for interpretation, and diagnostic accuracy is high. The disadvantages are similar to the brush biopsy and relate tothe adequacy ofthe sample for diagnosis A negative result does not exclude disease It is important to appreciate that the information provided by the cytopathologist requires careful correlation with the clinical examination and any availableimaginginformation
A varietyoftechniquescanbeusedtoacquiretissue for diagnosis (Table1.9) For oral mucosa,the majority of diagnostic biopsies are performed under local anaesthesia Small, clinically benign lesions mayberemovedcompletely byexcisional biopsy For larger lesions, an incisional biopsy technique is used to sample a representative area or areas ofthe lesion,prior to planningfurther treatment It is important to avoid injecting the local anaesthetic solution directly into the piece of tissue to be removed The tissue sample should be handled withcare to avoid distortion,causingstretch and crush artefacts Routine biopsies are placed immediately in a fixative typically neutral buffered formalin (10% formalin in phosphate buffered saline) Fixation prevents tissue desiccation and autolysis; it also hardens the tissue in preparation for laboratory processing Occasionally fresh biopsy material is required for the laboratory investigationoforalblisteringconditions(Chapter2) Freshmaterial can be transported to the laboratory in damp gauze, a proprietary transport medium (provided by the pathology laboratory), or snap frozen in liquid nitrogen Rapid diagnosis can also be attempted usingfresh biopsy material Surgeons sometimes employ this technique during an operation to ensure that the margins of the surgical defect are clear ofcancer, which is referredtoas intra-operative frozensections.
Histology
economictechniquethat isacceptabletopatients Multiplesamples can be taken if there is multi-focal disease or it can be employed as anadjuncttovisual surveillanceduringroutinefollow-up.The disadvantages of thistechnique mainly relateto adequacy of sample and
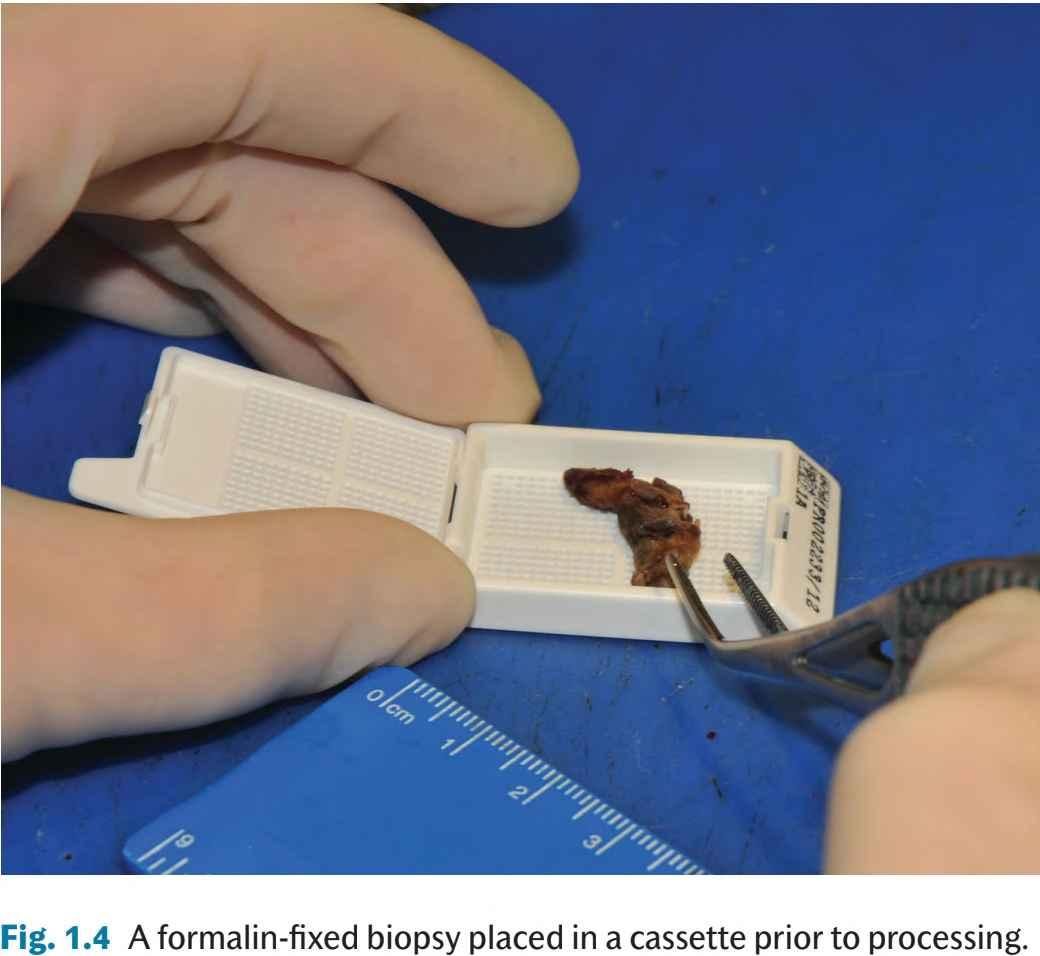
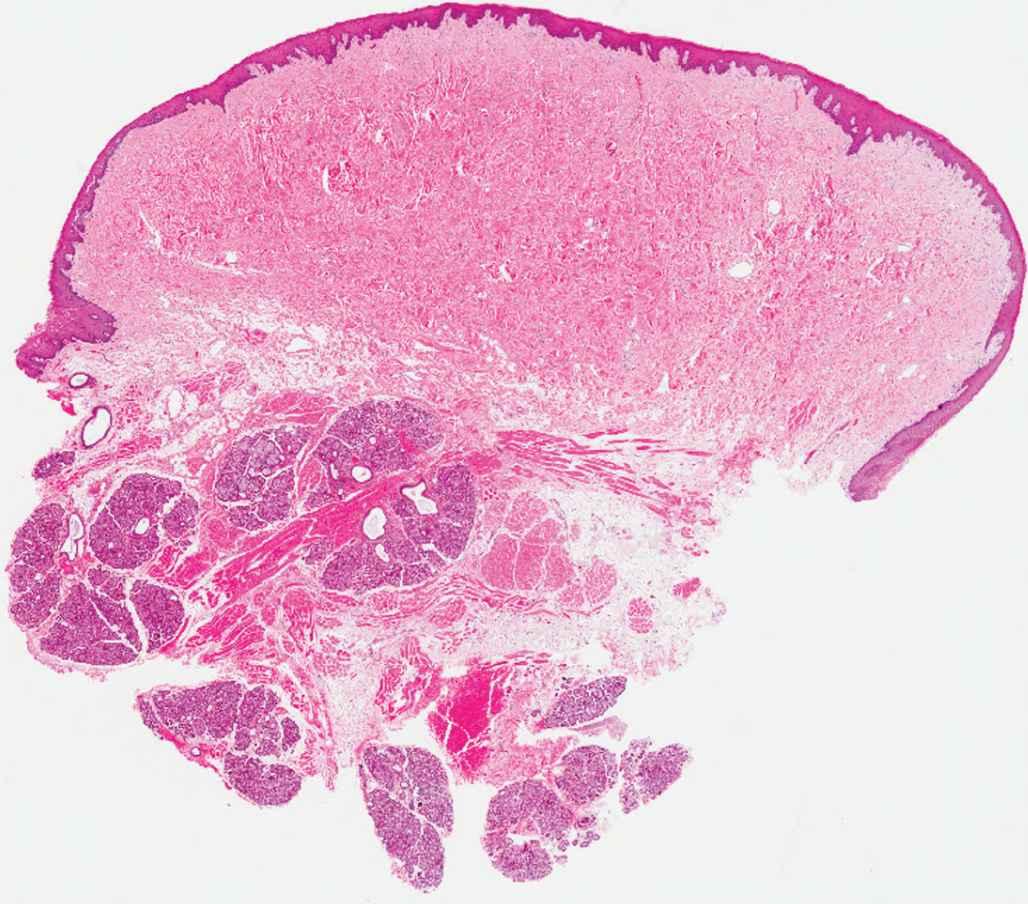
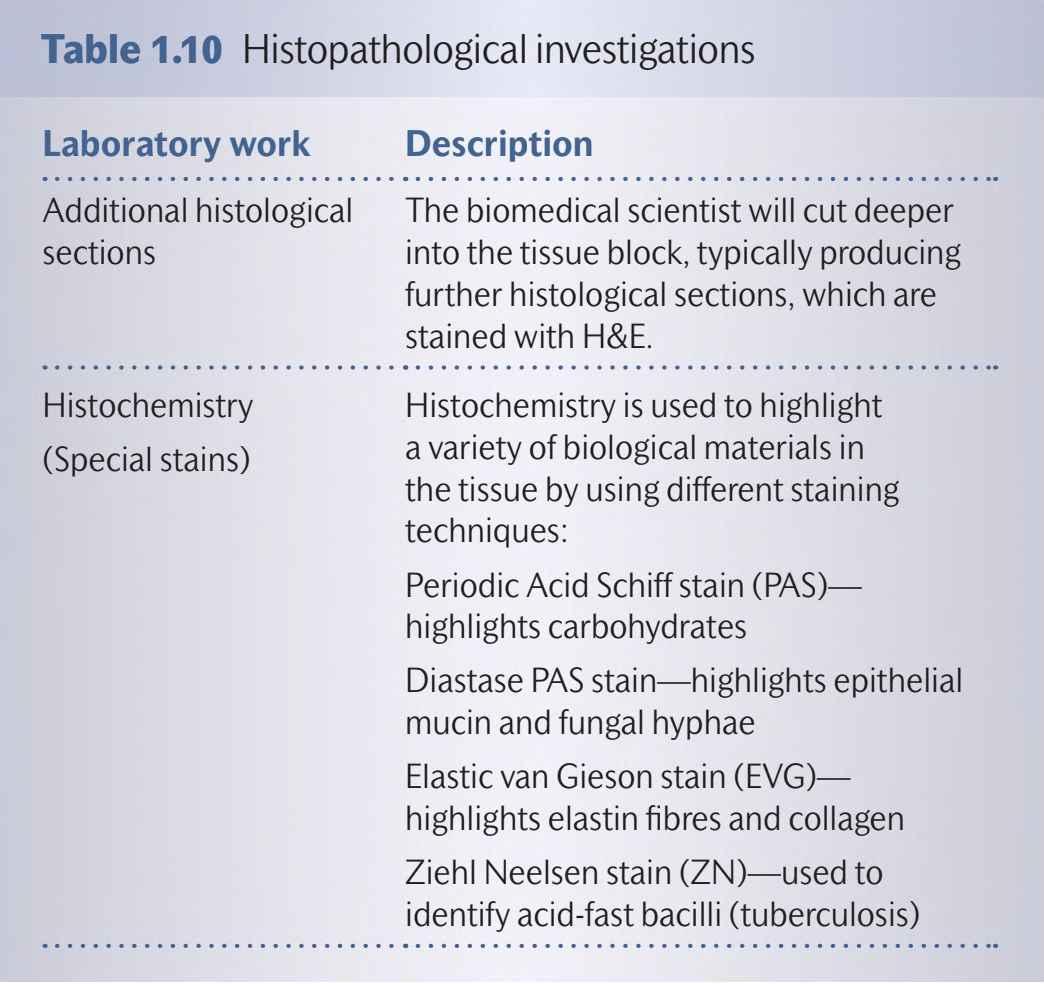
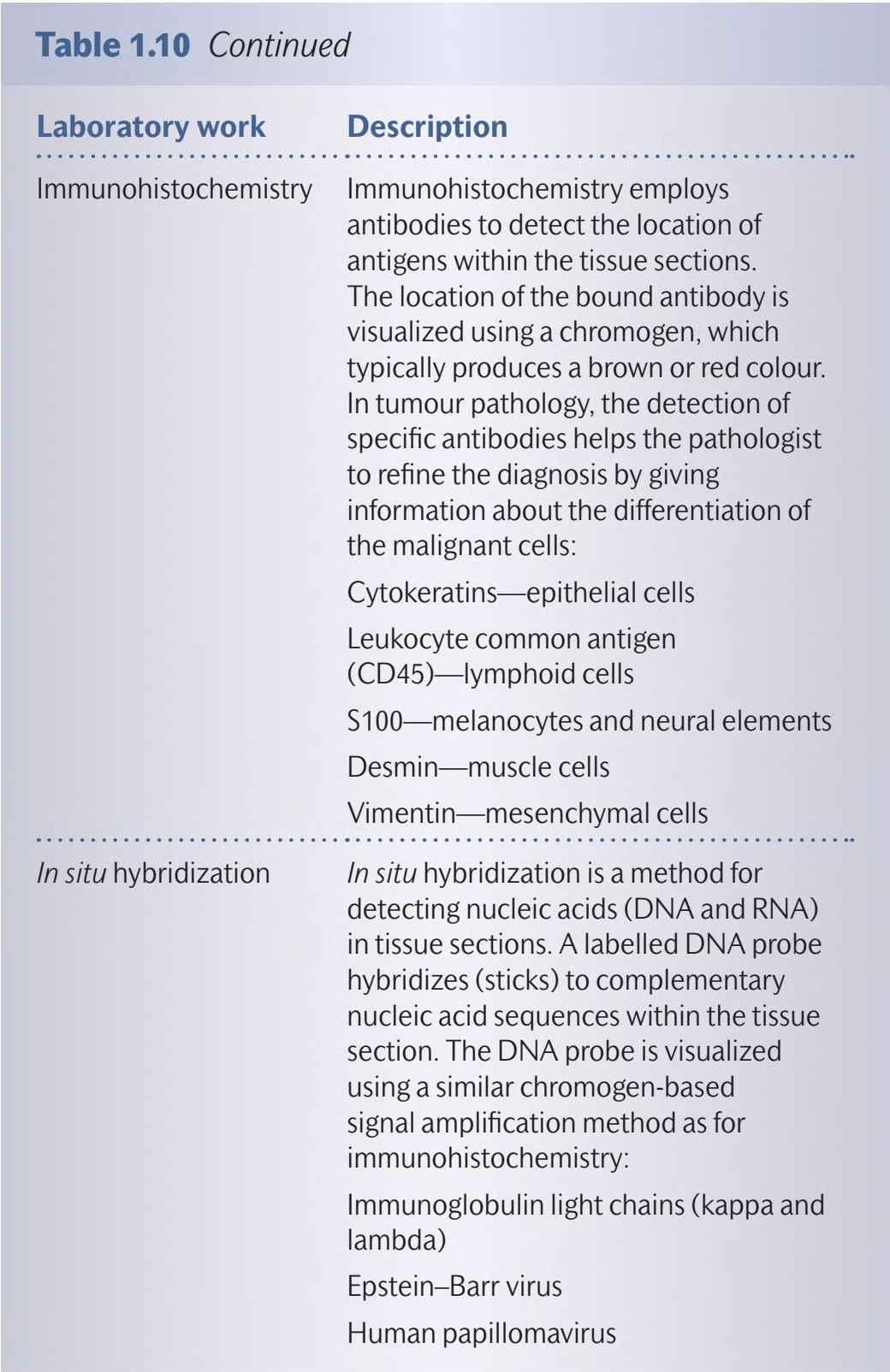
Whenthespecimenarrivesinthelaboratory,itischeckedtoensure thatitiscorrectlylabelledandtheaccompanyingrequestformiscompletedsatisfactorily.Thespecimenisthenassignedauniquespecimen number and starts its journey throughthe laboratory The specimen is retrieved from the container and described; this constitutes the macroscopic description The pathologist may then slice the biopsy toensureoptimal samplingandplacesthetissueintocassettesready fortissueprocessingandembedding(Fig 1.4) Theresultantformalinfixed paraffin-embeddedtissue block isthen ready for sectioningon a rotary microtome (Fig 1.5) Very thin(5pm) sections are mounted on glass slides and stained with haematoxylin and eosin (H&E) (Fig 1.6) Haematoxylinstainscellnucleidarkblueandconnectivetissueglycoproteinslightblue;bycontrasteosinstainsthecytoplasmand connectivetissue collagenfibresareddish pink colour The slidesare then examinedbythe pathologist;insome instancesa diagnosis can berenderedbyexaminingtheH&Estained sectionsalone However, additional stains or immunohistochemistry may be required before a definitive diagnosis can be formulated (Table 1.10). The pathologistwilldescribethesalientmicroscopicfeaturesandprovideeithera definitivediagnosisor adifferentialdiagnosisincasesthatrequirefurther clinico-pathological correlation. A typical histopathology report
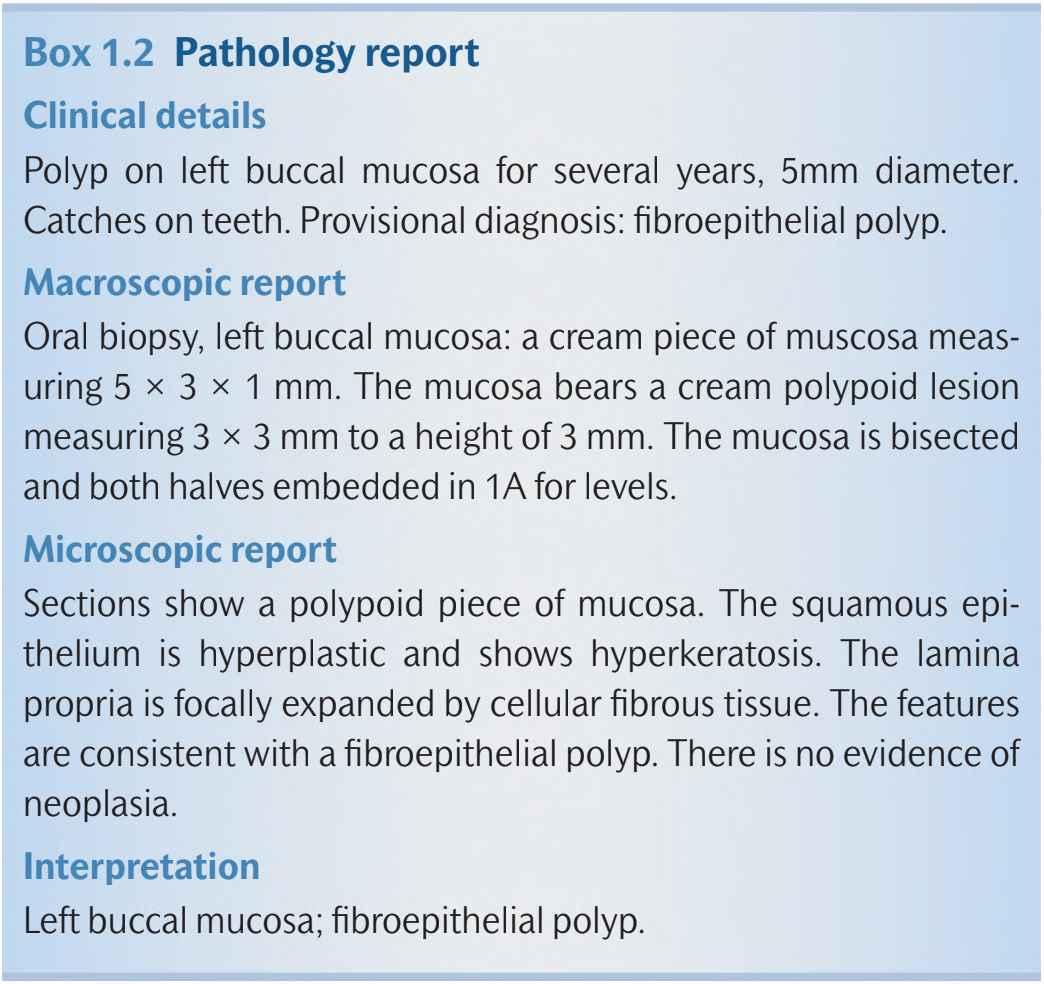
isshowninBox 1.2 Theaveragetimefrombiopsytopathologyreport is around 7 days; however, it is possible to reduce the ‘turn around time’toaround24hforurgentbiopsies Largesurgicalresectionspecimens,particularlythosecontainingbonethatrequiresdecalcification, cantakeuptoa fortnighttoreport
Increasingly,the identificationof genetic abnormalities is beingused to diagnose specific tumours and predict treatment response to targeted therapies. Chromosomal abnormalities, such as amplifications, translocations, and deletions, can be identified by cytogenetics (Chapter 4) Molecular biological techniques can be employed to identify genetic abnormalities such as loss of heterozygosity and specific gene mutations (Chapter 3) Molecular methods such as
The majority of dentists provide services inthe primary care setting It is important that the dental practitioner has the breadth of knowledge to identifyorallesionsandconditionsthatrequirereferralforspecialistcare
In the context of oral disease,patients are usually referredto secondary care for diseases that require further investigations in order to establish a definitive diagnosis and/or specialist medical or surgical interventions Whenconsideringreferringapatient,itisimportanttodiscussthereasons withthepatientandseektheirconsent Thereferralletter shouldinclude patient details and a clear statement about the nature of the condition, including the clinical history, medical history, and clinical examination, alongwithaprovisionalordifferentialdiagnosis Theinformationcontained inthe referral letter is usedtoallocate individual patientsto appropriate
Box1.2 Pathologyreport
Clinicaldetails
Polyp on left buccal mucosa for several years, 5mm diameter. Catchesonteeth Provisionaldiagnosis:fibroepithelialpolyp
Macroscopicreport
Oral biopsy,left buccal mucosa: a cream piece of muscosa measuring 5 x 3 x 1 mm The mucosa bears a cream polypoid lesion measuring3 x 3 mmtoaheight of3 mm The mucosa isbisected andbothhalvesembeddedin1Afor levels.
Microscopicreport
Sections show a polypoid piece of mucosa. The squamous epithelium is hyperplastic and shows hyperkeratosis The lamina propria is focally expandedby cellular fibroustissue The features areconsistentwithafibroepithelialpolyp.Thereisnoevidenceof neoplasia
Interpretation
Leftbuccalmucosa;fibroepithelialpolyp
polymerase chain reaction and in situ hybridization can be used to detect virus infection in oral tissues, e.g. Epstein-Barr virus in hairy leukoplakia (Chapter 2) and high-risk human papillomavirus in oropharyngeal cancer (Chapter 3) Significantly, gene mutation screening is being used to ‘personalize’ targeted cancer drug treatment. Detection of BRAF gene mutations in malignant melanoma is used to select patients that may benefit from vemurafenib Improvingoutcomes for patients with oral cancer requires a similar approach and willbebuiltonanincreasedunderstandingofthe molecular progression of the disease and the identification of‘drugable’molecular targets(Chapter3)
appointmentslots(urgent/routine) Apatientthatpresents withalesion that is consideredto beclinically malignant shouldbe clearly markedas urgent Itisrecommendedthaturgentreferrallettersareaccompaniedby eitheratelephonecalltothespecialistunitor asecureFAXcommunicationofthereferralletter Thisstrategywillensurethatthepatientisableto accessthespecialistcarethattheyrequirequickly IntheUK,suchpatients followacarepathwaythatisknownasthe‘2-weekwait’(2WW)or‘cancer waitingtime’(CWT),whichmeansthatpatientswithsuspectedcancerwill receiveahospital outpatientappointment within2 weeksoftheir urgent referral TheUKNationalCancerPlanindicatesthatnopatientshouldwait longer than1month froman urgent referral for suspected cancer tothe beginningoftreatment,exceptforgoodclinicalreasons
Documentingclinicalinformation
It is important that all stages of the diagnostic process are accurately documented in the clinical notes The record must include dated clinical entries with any radiographs,laboratory reports,andcopies of correspondence Maintainingaproperrecordisnotonlygoodpractice, italsoisessential forclinicalgovernanceandis invaluablefortheresolutionofmedico-legalclaims