Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and certain other countries.
Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by license, or under terms agreed with the appropriate reproduction rights organization. Inquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above.
You must not circulate this work in any other form and you must impose this same condition on any acquirer.
Library of Congress Cataloging-in-Publication Data
Names: Selden, Nathan R., editor. | Baird, Lissa C., editor.
Title: Pediatric neurosurgery / edited by Nathan R. Selden, Lissa C. Baird.
Other titles: Pediatric neurosurgery (Selden)
Description: New York, NY : Oxford University Press, [2019] | Includes bibliographical references. Identifiers: LCCN 2018040447 | ISBN 9780190617073 (paperback)
Subjects: | MESH: Central Nervous System Diseases—surgery | Child | Infant | Neurosurgical Procedures | Nervous System Malformations—surgery | Glioma—surgery | Case Reports
Classification: LCC RD593 | NLM WS 340.5 | DDC 617.4/80083— dc23 LC record available at https://lccn.loc.gov/2018040447
This material is not intended to be, and should not be considered, a substitute for medical or other professional advice. Treatment for the conditions described in this material is highly dependent on the individual circumstances. And, while this material is designed to offer accurate information with respect to the subject matter covered and to be current as of the time it was written, research and knowledge about medical and health issues is constantly evolving and dose schedules for medications are being revised continually, with new side effects recognized and accounted for regularly. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulation. The publisher and the authors make no representations or warranties to readers, express or implied, as to the accuracy or completeness of this material. Without limiting the foregoing, the publisher and the authors make no representations or warranties as to the accuracy or efficacy of the drug dosages mentioned in the material. The authors and the publisher do not accept, and expressly disclaim, any responsibility for any liability, loss or risk that may be claimed or incurred as a consequence of the use and/or application of any of the contents of this material.
9 8 7 6 5 4 3 2 1
Printed by Sheridan Books, Inc., United States of America
Contents
Preface vii
Contributors ix
1. Communicating Hydrocephalus 1
Rowland Han and David D. Limbrick, Jr.
2. Obstructive Hydrocephalus 11
Lissa C. Baird
3. Prematurity and Intraventricular Hemorrhage 19
Catherine A. Mazzola and Tatiana Huk Sikorskyj
4. Spinal Cord Tethering 31
Nathan R. Selden
5. Lipomyelomeningocele 41
Christina Sayama
6. Spinal Dermal Sinus Tract 47
Nathan R. Selden
7. Chiari Malformation with Syringomyelia 57
Yiping Li and Bermans J. Iskandar
8. Myelomeningocele 65
Lissa C. Baird
9. Sagittal Synostosis 73
Mark Proctor and Ali Hazama
10. Unicoronal Synostosis 83
Amy Lee and Richard G. Ellenbogen
11. Inflicted Traumatic Brain Injury 93
Beth A. Costine-Bartell and Ann- Christine Duhaime
12. Traumatic Atlanto-Axial Dislocation 101
Douglas Brockmeyer
13. Spastic Quadriplegia 109
David Harter
14. Extratemporal Refractory Epilepsy 117
Vamsidhar Chavakula, Eun-Hyoung Park, and Joseph R. Madsen
15. Hemispheric Refractory Epilepsy 127
Brian J. Dlouhy and Matthew D. Smyth
16. Ruptured Arteriovenous Malformation 141
Edward Smith
17. Moyamoya Disease 149
Edward Smith
18. Vein of Galen Malformation 157
Lissa C. Baird
19. Pineal Tumor 165
Tadanori Tomita
20. Medulloblastoma 177
Amy K. Bruzek, Shawn L. Hervey-Jumper, and Karin M. Muraszko
21. Hypothalamic- Chiasmatic Glioma 187
James Rutka and Angela Coppola
22. Mesial Temporal Glioma 199
Gerry Grant
23. Craniopharyngioma 207
Lissa C. Baird
24. Diffuse Brainstem Glioma 217
Nalin Gupta
25. Posterior Fossa Ependymoma 223
Frederick A. Boop and Jimmy Ming-Jung Chuang
26. Middle Fossa Arachnoid Cyst 231
Amy K. Bruzek and Cormac O. Maher
27. Posterior Fossa Cyst and Hydrocephalus 239
Peter J. Morone and John C. Wellons, III
28. Occipital Encephalocele 247
Molly Hubbard and Daniel Guillaume
29. Nasal Dermoid 257
Hugh J. L. Garton
30. Sinusitus with Subdural Empyema 267
Christina Sayama
31. Ventricular Shunt Infection 275
Christina Sayama
Index 281
Preface
Dear Reader,
I am delighted to introduce this volume of Neurosurgery by Example: Key Cases and Fundamental Principles. Neurosurgical training and practice are based on managing a wide range of complex clinical cases with expert knowledge, sound judgment, and skilled technical execution. Our goal in this series is to present exemplary cases in the manner they are actually encountered in the neurosurgical clinic, hospital emergency department, and operating room.
For this volume, Dr. Lissa C. Baird and I invited a broad range of expert contributors to share their extensive wisdom and experience in all major areas of pediatric neurosurgery. Each chapter contains a classic presentation of an important clinical entity and guides readers through the processes of assessment and planning, decision making, surgical procedure, aftercare, and complication management.“Pivot points”illuminate the changes required to manage patients in alternate or atypical situations.
Each chapter also presents lists of“pearls”for the accurate diagnosis, successful treatment, and effective complication management of each clinical problem. These 3 focus areas will be especially helpful to neurosurgeons preparing to sit for the American Board of Neurological Surgery oral examination, which bases scoring on these 3 topics.
Finally, each chapter contains focused reviews of medical evidence and expected outcomes, helpful for counseling patients and setting accurate expectations. Rather than exhaustive reference lists, chapter authors provide lists of high-priority additional reading recommended to deepen understanding.
The resulting volume should provide you with a dynamic tour through the practice of pediatric neurosurgery, guided by some of the leading experts in North America. Additional volumes cover each subspecialty area of neurosurgery, using the same casebased approach and board review features.
Nathan R. Selden, MD, PhD Campagna Professor and Chair Department of Neurological Surgery
Oregon Health & Science University
Contributors
Frederick A. Boop, MD
Department of Neurological Surgery University of Tennessee
St. Jude Children’s Research Hospital Memphis, TN
Douglas Brockmeyer, MD Department of Neurological Surgery
University of Utah, Primary Children’s Hospital
Salt Lake City, Utah
Amy K. Bruzek, MD, MS Department of Neurosurgery University of Michigan Ann Arbor, Michigan
Vamsidhar Chavakula, MD
Clinical Fellow in Surgery Department of Neurosurgery
Brigham and Women’s Hospital Boston, MA
Jimmy Ming-Jung Chuang, MD Department of Neurological Surgery University of Tennessee
St. Jude Children’s Research Hospital Memphis, TN
Angela Coppola, MD
Division of Neurosurgery
The Hospital for Sick Children Toronto, Ontario, Canada
Beth A. Costine-Bartell, PhD Department of Neurosurgery
Massachusetts General Hospital and Harvard Medical School Boston, MA
Brian J. Dlouhy, MD Department of Neurosurgery
University of Iowa Hospitals and Clinics Iowa City, Iowa
Ann- Christine Duhaime, MD Department of Neurosurgery
Massachusetts General Hospital and Harvard Medical School Boston, MA
Richard G. Ellenbogen, MD, FCAS Department of Neurological Surgery University of Washington Seattle, Washington
Hugh J. L. Garton, MD Department of Neurosurgery University of Michigan Ann Arbor, Michigan
Gerry Grant, MD Department of Neurosurgery
Stanford University Palo Alto, CA
Daniel Guillaume, MD
Department of Neurosurgery
University of Minnesota Minneapolis, MA
Nalin Gupta, MD, PhD
Department of Neurological Surgery
University of California San Francisco UCSF Benioff Children’s Hospital San Francisco, CA
Rowland Han, MD, MSCI
Washington University School of Medicine St. Louis, Missouri
David Harter, MD Department of Neurosurgery
New York University, New York New York, NY
Ali Hazama, MD Department of Neurosurgery
Boston Children’s Hospital and Harvard Medical School Boston, Massachusetts
Shawn L. Hervey-Jumper, MD Department of Neurosurgery University of Michigan
Ann Arbor, Michigan
Molly Hubbard, MD Department of Neurosurgery University of Minnesota Minneapolis, MA
Bermans J. Iskandar, MD Department of Neurological Surgery University of Wisconsin Madison, Wisconsin
Amy Lee, MD Department of Neurological Surgery University of Washington Seattle, WA
Yiping Li, MD
Department of Neurological Surgery
University of Wisconsin Madison, Wisconsin
David D. Limbrick, Jr., MD, PhD
Department of Neurosurgery
Washington University School of Medicine
St. Louis Children’s Hospital St. Louis, Missouri
Joseph R. Madsen, MD Department of Neurosurgery
Boston Children’s Hospital and Harvard Medical School
Boston, MA
Cormac O. Maher, MD Department of Neurosurgery
University of Michigan Ann Arbor, Michigan
Catherine A. Mazzola, MD
Division of Pediatric Neurological Surgery
Goryeb Children’s Hospital of Atlantic Health Systems Morristown, NJ
Peter J. Morone, MD
Department of Neurological Surgery
Vanderbilt University Medical Center
Monroe Carell Jr. Children’s Hospital Nashville, TN
Karin M. Muraszko, MD
Department of Neurosurgery University of Michigan
Ann Arbor, Michigan
Eun-Hyoung Park, MD Department of Neurosurgery
Boston Children’s Hospital and Harvard Medical School Boston, MA
Mark Proctor, MD
Department of Neurosurgery
Boston Children’s Hospital and Harvard Medical School Boston, MA
James Rutka, MD, PhD
Division of Neurosurgery
The Hospital for Sick Children, Toronto Ontario, Canada
Christina Sayama, MD
Department of Neurological Surgery
Oregon Health & Science University Doernbecher Children’s Hospital Portland, Oregon
Tatiana Huk Sikorskyj, R-NP
Division of Pediatric Neurological Surgery at Goryeb Children’s Hospital of Atlantic Health Systems Morristown, NJ
Edward Smith, MD
Department of Neurosurgery
Boston Children’s Hospital and Harvard Medical School
Boston, MA
Matthew D. Smyth, MD
Department of Neurosurgery, Washington University St. Louis Children’s Hospital St. Louis, Missouri
Tadanori Tomita, MD Department of Neurosurgery Northwestern University Feinberg School of Medicine
Ann & Robert H. Lurie Children’s Hospital of Chicago Chicago, Illinois
John C. Wellons, III, MD, MSPH
Department of Neurological Surgery Vanderbilt University Medical Center Monroe Carell Jr. Children’s Hospital Nashville, TN
Communicating Hydrocephalus
Rowland Han and David D. Limbrick, Jr.
Case Presentation
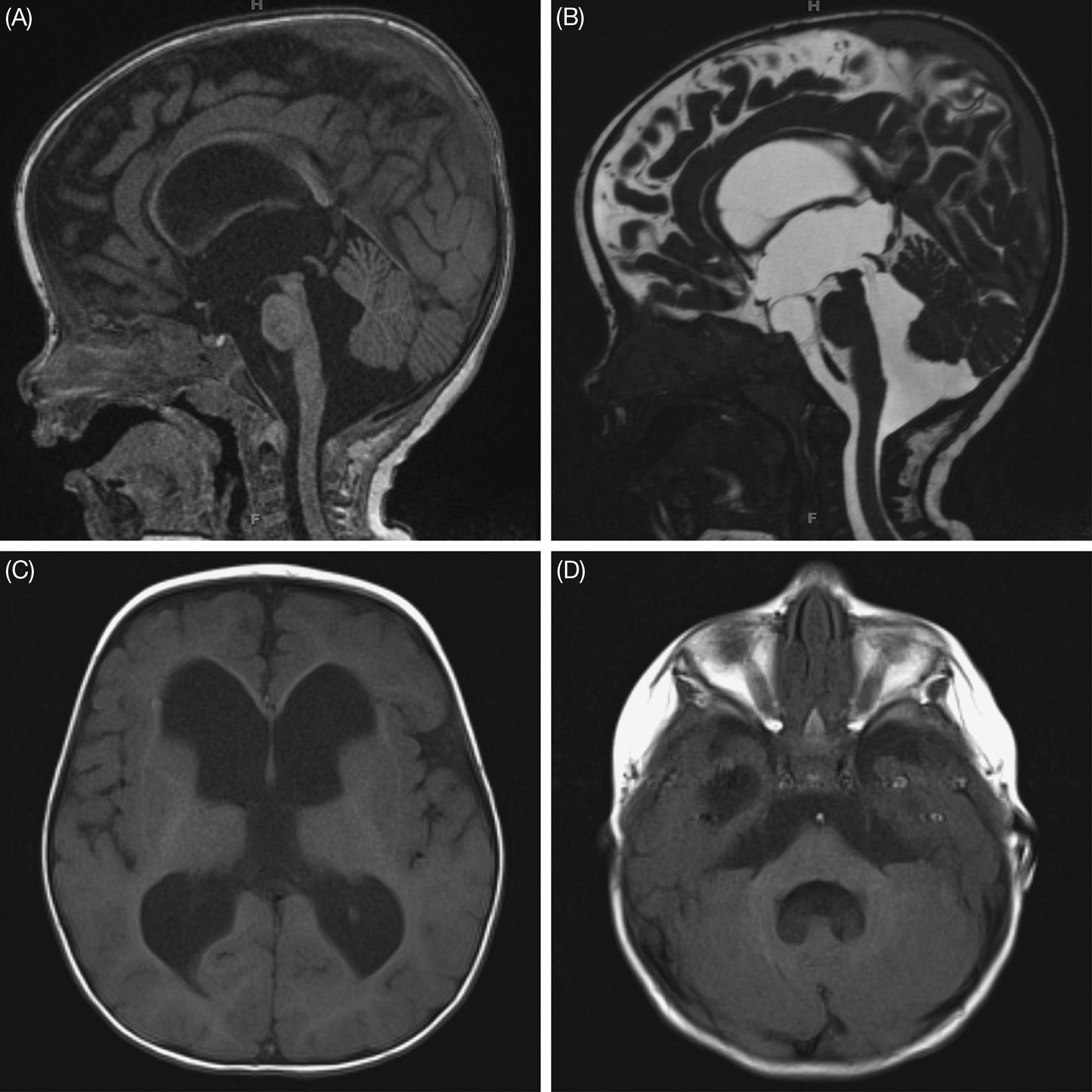
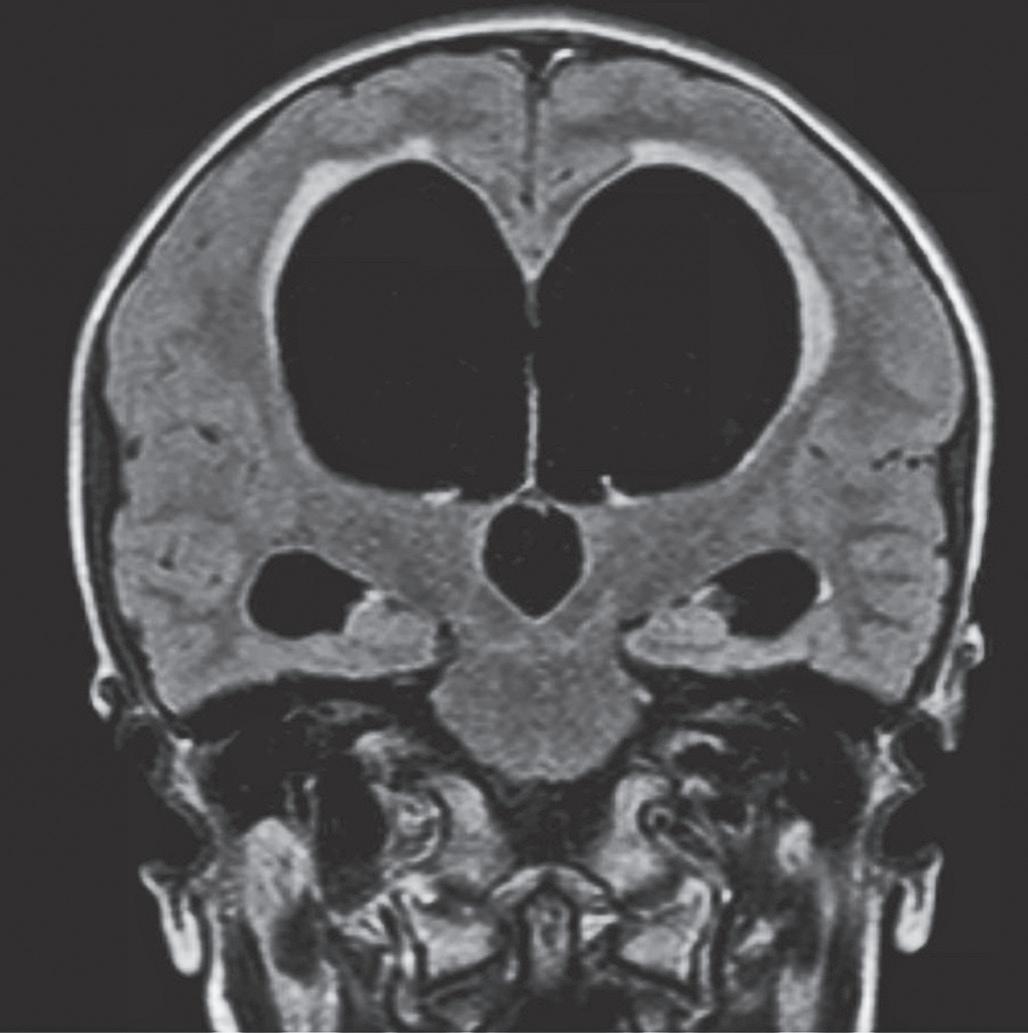
A boy is born at 37 weeks estimated gestational age to a 21-year- old G1P0 mother after a pregnancy complicated by oligohydramnios, intrauterine growth restriction, and pregnancy-induced hypertension. He is delivered by cesarean section for fetal decelerations and weighs 1490 grams with initial orbitofrontal circumference (OFC) of 30 cm. Apgar scores are 8 and 8 at 1 and 5 minutes, respectively. On exam, he is noted to have dysmorphic features including micrognathia, low set ears, and hypospadias. He requires oxygen on the first day of life but is quickly weaned to room air. Head ultrasound on day of life 6 reveals moderate ventriculomegaly involving the bilateral lateral ventricles, third ventricle, fourth ventricle, and prominence of the cisterna magna. Head MRI 2 days later yields similar findings with patency of the foramina of Monro, cerebral aqueduct of Sylvius, and fourth ventricle outlets (Figure 1.1). Over the following weeks, the patient’s OFC progressively increases, his fontanel becomes full, his cranial sutures begin to splay, and he is scheduled for ventriculoperitoneal (VP) shunt placement at 2 months of age.
Questions
1. What is the likely diagnosis?
2. What are signs and symptoms of acute and chronic hydrocephalus?
3. What clinical and radiological parameters prompt diagnosis of hydrocephalus and of communicating versus non- communicating (obstructive) hydrocephalus?
Assessment and Planning
The diagnosis is congenital communicating hydrocephalus (CHC), suggested by apparent dilation of the entire ventricular system with progressive macrocephaly. Infants suspected of developing hydrocephalus should be monitored closely with daily physical examination and serial neuro-imaging (typically head ultrasound or magnetic resonance imaging [MRI]). Signs and symptoms of progressive hydrocephalus in young children include a full and bulging fontanel, splaying of the cranial sutures, OFC crossing growth curves, irritability, nausea/vomiting, and, in severe cases, upgaze paresis, irregular respirations with apneic spells, or bradycardia. OFC increasing at >2 cm/week or crossing the 97th percentile should prompt consideration of hydrocephalus treatment.
Figure 1.1. MRI scans for the presented patient with communicating hydrocephalus, showing (A) sagittal T1, (B) sagittal T2, axial T1 through the (C) lateral ventricles, and (D) fourth ventricle, prior to any shunting procedures. Note the dilation of the entire ventricular system, the patency of the foramina of Monro, cerebral aqueduct of Sylvius, and fourth ventricle outlets, and the flow jet observed in the cerebral aqueduct on sagittal T2.
Radiological findings suggestive of hydrocephalus include ventriculomegaly, with ballooning of the ventricular system, thinning or upward bowing of the corpus callosum, and effacement of the cerebral sulci and Sylvian or interhemispheric fissures. Plain skull radiographs or CT might reveal splaying of the cranial sutures.
Oral Boards Review—Diagnostic Pearls
1. Hydrocephalus results from an imbalance between cerebrospinal fluid (CSF) production and reabsorption. It can be classified as communicating or non- communicating (obstructive), although individual cases generally have components of both.
a. Traditionally,communicatinghydrocephalushasbeenattributedtoimpaired absorption of CSF through arachnoid villi (e.g., from inflammation) or elevation of cranial venous sinus pressure. Rarely, communicating hydrocephalus may result from excessive CSF production such as with a functional choroid plexus papilloma. Radiologically, communicating hydrocephalus is characterized by dilation of the entire ventricular system, including the fourth ventricle, and patency of the foramina of Monro, cerebral aqueduct of Sylvius, and fourth ventricle outlets (foramina of Lushka and Magendie).
b. Non- communicating hydrocephalus occurs as a result of anatomic or functional obstruction to CSF flow. Obstruction can be present at the foramen of Monro, cerebral aqueduct, or fourth ventricle or its outlets. In non- communicating hydrocephalus, the ventricular system is often dilated proximal to the obstruction, while the ventricles distal to the obstruction remain relatively normal in size.
2. Possible symptoms of progressive hydrocephalus include headache, vomiting, lethargy, or irritability. Clinical signs may include a full and bulging fontanel, splayed sutures, papilledema, upgaze paresis/ palsy, OFC greater than the 97th percentile, or frontal- occipital horn ratio (FOR) greater than 0.4– 0.45.
3. Distinction between communicating hydrocephalus and hydrocephalus exvacuo may be difficult in some cases. The latter describes ventriculomegaly resulting from cerebral atrophy, rather than an imbalance in CSF physiology. Radiological characteristics suggesting true hydrocephalus rather than cerebral atrophy may include third ventricular enlargement, periventricular tissue interstitial edema on T2-weighted or FLAIR MRI, and cortical sulci effacement. Clinically, patients with hydrocephalus ex-vacuo typically lack the signs and symptoms of progressive hydrocephalus listed in item 2. The distinction between these 2 entities is important, as CSF diversion surgery is unnecessary for, and perhaps dangerous in, hydrocephalus ex vacuo.
4. Hydrocephalus may follow varying temporal and clinical courses, including rapid progression (acute hydrocephalus), slow progression (chronic hydrocephalus), or spontaneous arrest without intervention. Close monitoring is needed to identify patients requiring surgical intervention, particularly in cases of rapid progression with signs of increased intracranial pressure (ICP).
Questions
1. What are the goals of surgical treatment for CHC?
2. What are the surgical options for treatment, and when should definitive treatment occur?
3. What are the rationale and indications for different shunt designs and constructs?
Decision Making
The primary goals of neurosurgical treatment of CHC should be to optimize neurologic function and neurodevelopment, avoid neurological deficits associated with CHC, and provide symptomatic relief from headaches, nausea, emesis, and other signs and symptoms of increased ICP.
Surgical treatment for CHC requires CSF diversion to decompress the ventricles and normalize ICP. Most commonly, shunts divert CSF to the peritoneal cavity (ventriculoperitoneal, orVP, shunt), though alternate sites such as the right atrium of the heart (VA shunt) or the pleural cavity (V-pleural shunt) may be used in the setting of peritoneal scarring/infection or high central venous pressure, respectively. Infrequently used distal sites include the bone marrow, gall bladder, or other locations.
Valve designs that may be used in CSF shunts include differential pressure, flowcontrol, or programmable valves, each with or without an antisiphon device. Factors that may influence choice of design include the patient’s propensity for under- or overdrainage, the surgeon’s preference or experience, and the perceived need for valve setting adjustments. Current data, however, suggest that valve design does not significantly impact shunt survival.
While shunts effectively reduce ICP and ventriculomegaly, they are associated with short- and long-term risks (refer to the section“Complications and Management”), and although CSF shunting is the most commonly employed treatment for CHC and the focus of this chapter, endoscopic third ventriculostomy (ETV) without or with choroid plexus cauterization (CPC) may be offered as an alternative to shunting in select cases. ETV and ETV- CPC will be discussed elsewhere in this volume.
Questions
1. What steps should be taken in preparation and patient positioning for insertion of a VP shunt?
2. What technical adjuncts are available for assisting with optimal proximal shunt catheter placement, and what is the evidence for their use?
3. What complications are associated with CSF shunting?
Surgical Procedure
Insertion of a VP shunt is a major procedure performed under general anesthesia. The desired implants, including ventricular and distal catheters (with or without antibiotic impregnation) and valve type should be specified ahead of time.The surgeon also selects the side for the shunt depending on the patient’s intracranial anatomy and other cranial or extracranial factors (other recent surgical procedures, skin abrasions, etc.). Barring the presence of more specific factors, the right side is generally chosen for primary shunt insertion in infants given that the right cerebral hemisphere is likely to be non-language dominant, and given that distal shunt tubing in the right abdomen will not interfere with a later gastrostomy placement if indicated. The choice of anterior (coronal) or posterior (occipital or parieto- occipital) entry site may be based on factors such as intracranial anatomy, recent surgical procedures, skull shape, or surgeon experience or
preference; however, the superiority of one or the other remains controversial and is a topic of continued investigation.
For the surgery itself, the patient is positioned supine with a shoulder roll and the neck gently extended to assist in tunneling the distal catheter. If image- guidance is to be used, the device is assembled and registered to the patient’s head, and a trajectory for cannulating the ventricle is planned. The skin is then prepared using an antiseptic solution; many surgeons follow a standard QI protocol for skin preparation and other basic techniques (e.g., the Hydrocephalus Clinical Research Network protocol). The operation begins by making a curvilinear incision at the chosen cranial access site (anterior or posterior), making a burr hole, and placing a ventricular catheter into the lateral ventricle, typically positioning the tip of the catheter near the foramen of Monro. The surgeon may elect to use a free- hand technique or one of several technical adjuncts to assist in optimal catheter placement (ultrasound, endoscope, image- guidance, etc.); although none has been shown to definitively improve shunt survival, there are data to suggest that electromagnetic image– guidance may reduce malfunction rates. After placement of the ventricular catheter, CSF may be sent for culture at the time of catheter insertion to detect any preexisting infection if there is a clinical concern.
The distal catheter is passed from the cranial incision to a ~1 cm incision made in the abdomen at a site chosen by the surgeon, based on patient anatomy or other factors (presence of gastrostomy tube or surgical scars). A parietal passing incision may be required to deliver the distal catheter from an anterior entry point to the abdominal incision. Peritoneal access may be achieved through mini-laparotomy, laparoscopy, minimally invasive port or trocar, or other method. After peritoneal access is established, the shunt is fully assembled, securing both the ventricular and distal catheters to the valve.Variability in implant construct (i.e., unitized shunt versus individual components) and surgical technique dictate the sequence of final shunt assembly. The valve itself fits within a subgaleal pocket fashioned for this purpose, and after verification of shunt patency and function the distal catheter is fed into the peritoneum. In general, ~30 cm of intraperitoneal tubing is implanted in small children to allow for continued growth. All incisions are then irrigated and closed.
Oral Boards Review—Management Pearls
1. Although definitive CSF diversion for CHC is typically accomplished using a VP shunt, other locations for distal catheter placement may be chosen for specific indications or if the peritoneum cannot be used.
2. Use of an anterior versus posterior entry site for the ventricular catheter remains a topic of investigation.
3. Propensity for under- or over- drainage, surgeon preference/experience, and the perceived need for valve setting adjustments often inform valve choice. Current data suggest that valve design does not significantly impact shunt survival.
4. The use of ETV and ETV- CPC as an alternative to CSF shunting will be discussed elsewhere in this volume.
Pivot Points
1. Programmable valves, high-pressure differential pressure valves, or flowcontrol valves may aid in the prevention of CSF over- drainage, especially when used in conjunction with an anti-siphon device, particularly in infants presenting for primary VP shunt insertion in the setting of massive congenital ventriculomegaly.
2. The relationship between CSF shunting or ETV/ETV- CPC, ventricular size, and long-term neurodevelopment and quality of life is complex and likely multifactorial. Children with predominantly obstructive hydrocephalus (such as aquaductal stenosis) are excellent candidates for ETV- CPC and may never need ventricular shunting, particularly if they follow a good developmental course after ETV.
3. Children with concomitant congenital malformations of the abdomen can undergo primary ventricular shunt placement with an alternate distal catheter location, often the pleural space for children who are over 2 kg in weight and do not have pulmonary insufficiency.
Aftercare
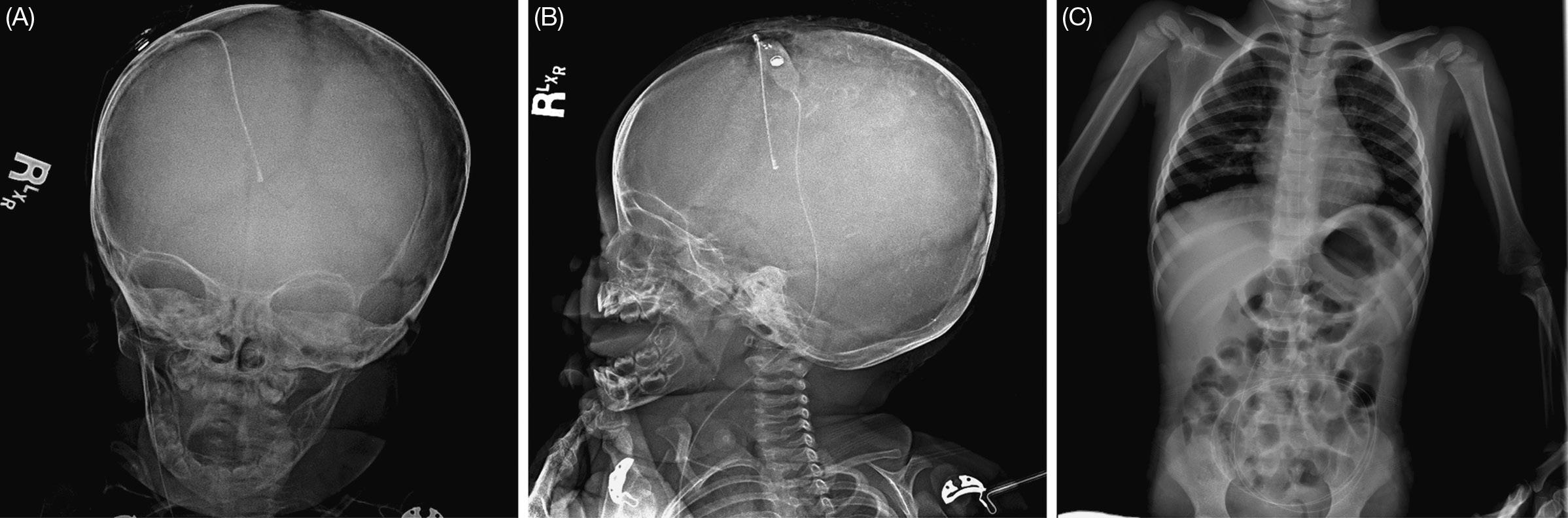
Sterile dressings may be placed after shunt insertion, which can be removed 24 to 48 hours post- operatively. One to 2 doses of post- operative intravenous (IV) antibiotic may be used to prevent CSF infection. A shunt X-ray series, including skull, chest, and abdominal radiographs, may be obtained as baseline imaging and to determine whether immediate revision is required (Figure 1.2). Initial follow-up after shunt placement is usually within 1 month, at which time neuro-imaging may be ordered to confirm shunt function and provide a baseline for subsequent evaluation of any suspected shunt failure episode, although clinical assessment is often sufficient to confirm function. Imaging may show ventricular size continuing to decrease over the course of the first year or
Figure 1.2. VP shunt X-ray series for the presented patient shows the VP shunt assembly. (A and B) AP and lateral skull X-rays, respectively. (C) AP chest and abdomen X-ray.
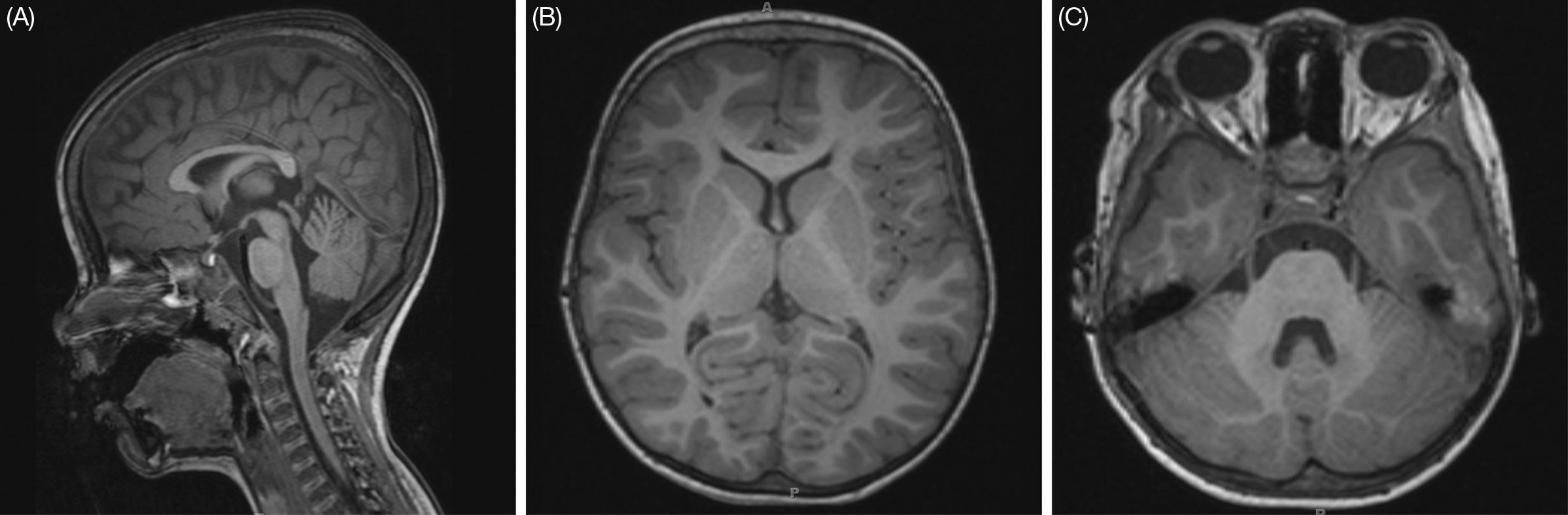
Figure 1.3. MRI scan for the presented patient two years after implantation of the VP shunt. Sagittal T1 (A), axial T1 through the lateral ventricles (B), and axial T1 through the fourth ventricle (C) images show a dramatic reduction and near-normalization in ventricular size.
longer. Additional regular appointments are often scheduled on a several monthly or annual basis.
While long-term imaging may detect subclinical shunt failure, there are concerns about radiation exposure in young children receiving serial CT scans. Thus, monitoring with MRI (Figure 1.3), and in particular rapid brain MRI, is advised. However, the effect of MRI on programmable valve settings must be anticipated, and such valves need to be verified after each MRI.
Complications and Management
Shunt malfunction is common, occurring in 31.3% of children within the first year and 4.5% per year thereafter. The most common cause of shunt malfunction is proximal obstruction of the ventricular catheter, likely from reduced ventricular size and/or ingrowth of the choroid plexus. Other causes of failure include valve malfunction, kinking, fractured tubing, shunt migration, and distal obstruction or malabsorption. Except in rare cases, shunt malfunction requires urgent surgical revision of the shunt. If the ventricles are of sufficient size and the anatomy is favorable, ETV/ETV- CPC can be considered in the setting of shunt malfunction, although success rates in this scenario are lower. Infection is an unfortunate complication of shunt surgery and occurs in up to 6.0% of cases. Shunt infection may be associated with ventriculitis, scarring and loculation of the ventricles, neurological morbidity, and, rarely, death. Risk factors for shunt infection include young age (<6 months), presence of gastrostomy tube, and prior neurosurgery. The most common organisms implicated in pediatric shunt infections are Staphylococcus epidermidis,Staphylococcusaureus,andGram-negativebacilli.Nearlyallcasesofshuntinfection require externalization or removal of the shunt with temporary CSF drainage via an external ventricular drain and treatment with IV antibiotics tailored to the specific infecting organisms. Once serial CSF cultures verify clearing of the infection, the shunt can be re-implanted. Infrequently, cases of shunt malfunction or shunt infection may be
associated with an enlarging, loculated CSF collection in the abdomen (“pseudocyst”), which requires conversion to a VA or other shunt after externalization and antibiotic treatment.
Patients withVP shunts may present with signs and symptoms of shunt over-drainage and intracranial hypotension. Clinically, patients may complain of headaches, often postural, nausea, and vomiting. Neuro-imaging often demonstrates small ventricles and, if contrast is administered, potentially meningeal enhancement. In the setting of large ventricles, over-drainage is also frequently complicated by subdural hematomas or other extra-axial fluid collections. Chronic over- drainage is associated with slit-ventricle syndrome, a condition that causes disabling and often difficult-to-treat headaches. Overdrainage is typically treated by revising the shunt to a higher pressure or flow- control system with an anti-siphon device. Many contemporary shunts have been designed with onboard programmable differential pressure valves, anti-siphon devices, or flowregulated valves to help address this problem.
Although rare, intracranial hemorrhage (epidural, subdural, intra-parenchymal, or intraventricular) may occur as a complication of shunt placement. While such hemorrhages usually resolve spontaneously without any additional intervention, they may be associated with a higher rate of subsequent shunt obstruction and malfunction, especially in cases of intraventricular hemorrhage.When significant hemorrhage is encountered through the ventricular catheter at surgery, the surgeon may elect to convert to an EVD or other temporizing strategy (e.g., valveless shunt) to permit resolution of the hemorrhage and minimize the risk of future shunt malfunction.
Oral Boards Review— Complications Pearls
1. Shunt infection usually requires removal of the shunt with temporary CSF drainage via EVD and treatment with IV antibiotics prior to re-implantation of the shunt. New standardized protocols for shunt insertion including perioperative antibiotics and antibiotic-impregnated catheters have been shown to reduce CSF infection rates.
2. Mechanical shunt failure requires surgical revision and is most commonly caused by proximal obstruction.
3. Problems with over- drainage can be managed with higher-pressure or programmable valves, anti-siphon devices, or flow-regulated valves.
Evidence and Outcomes
Hydrocephalus is the most common surgically treatable neurological problem in the pediatric population. There remains little information on long-term outcomes, and in particular quality of life or functional outcomes, in treated children. A recent volume of Journal of Neurosurgery: Pediatrics was devoted to establishing pediatric hydrocephalus treatment guidelines through systematic reviews of available evidence.While there is Level I evidence to help inform some aspects of pediatric hydrocephalus treatment, these guidelines revealed the dearth of high- quality data to inform the treatment of this disease.There is an urgent need for standardized instruments and care pathways, such as
those created through the Hydrocephalus Clinical Research Network, to inform both clinical treatment and research for this condition. The epidemiology and genetic and environmental factors influencing development of CHC also clearly warrant further directed investigation.
References and Further Reading
O’Hayon BB, Drake JM, Ossip MG, Tuli S, Clarke M. Frontal and occipital horn ratio: A linear estimate of ventricular size for multiple imaging modalities in pediatric hydrocephalus. Pediatr Neurosurg. 1998;29(5):245–249. doi:10.1159/000028730.
Kestle J, Drake J, Milner R, et al. Long-term follow-up data from the shunt design trial. Pediatr Neurosurg. 2000;33(5):230–236. doi:10.1159/000055960.
Whitehead WE, Riva-Cambrin J, Kulkarni A V, et al. Ventricular catheter entry site and not catheter tip location predicts shunt survival: a secondary analysis of 3 large pediatric hydrocephalus studies. J Neurosurg Pediatr. November 2016:1–11. doi:10.3171/2016.8.PEDS16229.
Kestle JRW, Holubkov R, Douglas Cochrane D, et al. A new Hydrocephalus Clinical Research Network protocol to reduce cerebrospinal fluid shunt infection. J Neurosurg Pediatr. December 2015:1–6. doi:10.3171/2015.8.PEDS15253.
Hayhurst C, Beems T, Jenkinson MD, et al. Effect of electromagnetic-navigated shunt placement on failure rates: a prospective multicenter study. J Neurosurg. 2010;113(6):1273–1278. doi:10.3171/2010.3.JNS091237.
Ashley WW, McKinstry RC, Leonard JR, Smyth MD, Lee BC, Park TS. Use of rapid-sequence magnetic resonance imaging for evaluation of hydrocephalus in children. J Neurosurg Pediatr 2005;103(Pediatrics 2):124–130. doi:10.3171/ped.2005.103.2.0124.
Stein SC, GuoW. Have we made progress in preventing shunt failure? A critical analysis. J Neurosurg Pediatr. 2008;1(January):40–47. doi:10.3171/PED-08/01/040.
Simon TD, Butler J, Whitlock KB, et al. Risk factors for first cerebrospinal fluid shunt infection: findings from a multi- center prospective cohort study. J Pediatr. 2014;164(6):1462–1468.e2. doi:10.1016/j.jpeds.2014.02.013.
Pediatric hydrocephalus: systematic literature review and evidence-based guidelines. J Neurosurg Pediatr. 2014;14 Suppl 1.
Kestle JRW, Drake JM, Cochrane DD, et al. Lack of benefit of endoscopic ventriculoperitoneal shunt insertion: a multicenter randomized trial.J Neurosurg. 2003;98(2):284–290. doi:10.3171/ jns.2003.98.2.0284.
Obstructive Hydrocephalus
Lissa C. Baird
Case Presentation
A 12-year- old boy presents to his pediatrician with a 2 month history of fatigue, blurry vision, and balance difficulties while walking. He endorses intermittent mild headaches, and his parents note difficulty with short-term memory and worsening school performance over the previous 6 months. His medical history is significant for a diagnosis of attention deficit hyperactivity disorder (ADHD), and his developmental history is otherwise unremarkable.
A computed tomography (CT) scan ordered by the pediatrician demonstrates ventriculomegaly of the lateral and third ventricles, and a referral is made to pediatric neurosurgery with concern for hydrocephalus. Neurological examination by the neurosurgeon demonstrates mild macrocephaly in an otherwise well-appearing young boy, intact cranial nerve function, normal gait, no motor or sensory deficits, and absence of abnormal reflexes or long tract findings. Funduscopic examination reveals bilateral papilledema.
Questions
1. Should further imaging studies be obtained?
2. What further clinical evaluation should be undertaken?
3. What is the differential diagnosis?
Assessment and Planning
A diagnosis of hydrocephalus is suspected. The presence of papilledema raises concern for elevated intracranial pressure. The history of neurocognitive decline, vision change, and gait dysfunction support this diagnosis. It is important to establish the etiology of the hydrocephalus whenever possible, as the underlying diagnosis will influence the treatment plan, prognosis, and family counseling. The differential diagnosis of ventriculomegaly in the setting of suspected elevated intracranial pressure includes congenital causes of ventricular obstruction such as aqueductal stenosis and fourth ventricular outlet obstruction, as well as obstructive hydrocephalus secondary to mass lesions such as tumor, abscess, vascular malformation, or cyst. Communicating hydrocephalus, ventriculomegaly ex vacuo, and benign familial macrocrania should also be considered, although these are less likely in the absence of a dilated fourth ventricle.
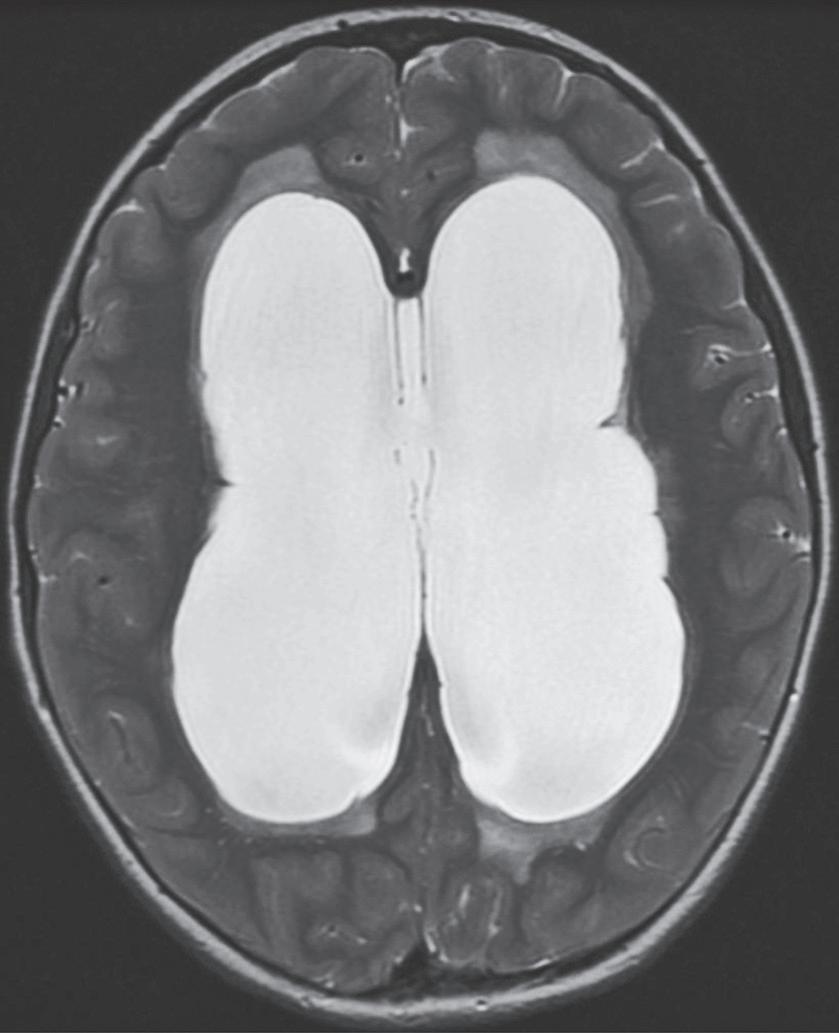
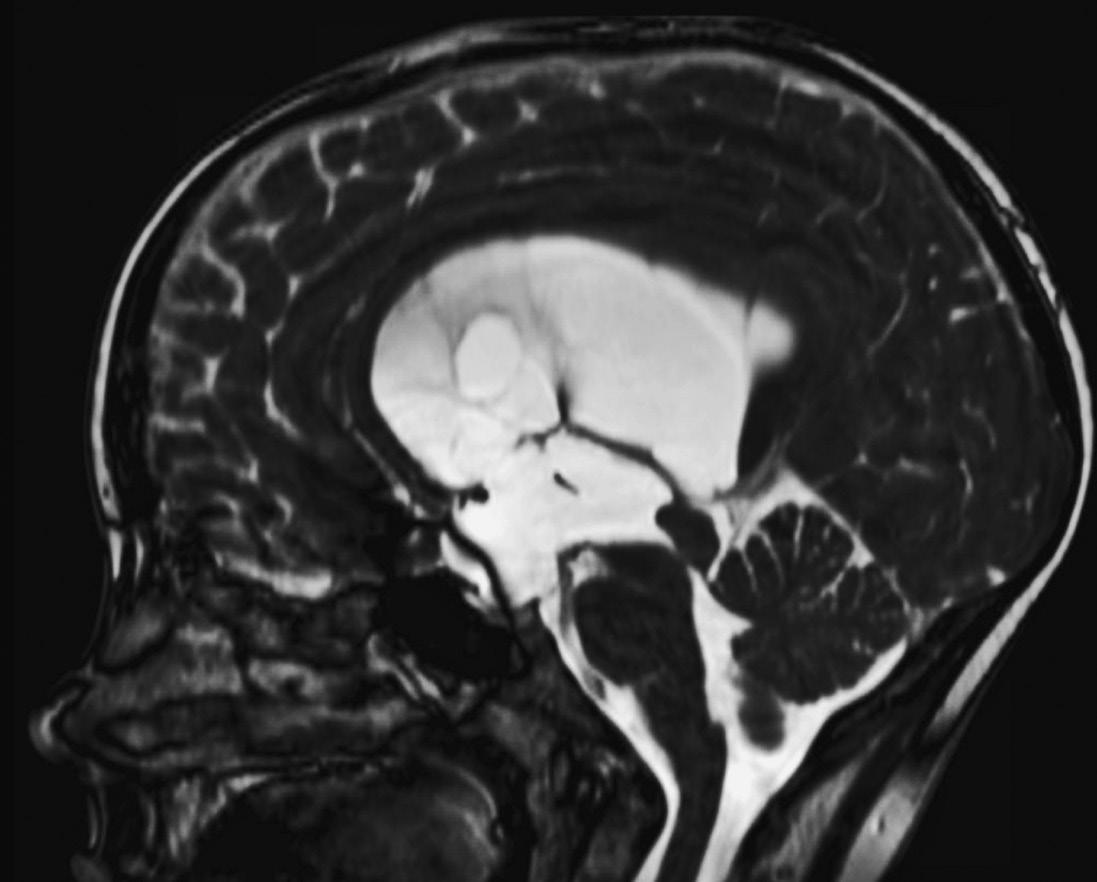
Preoperative MRI demonstrates ventriculomegaly, sulcal effacement, and transependymal flow in the periventricular white matter.
A magnetic resonance imaging (MRI) scan of the brain should be obtained to fully evaluate the ventricular anatomy and rule out the presence of a mass lesion. FIESTA (fast imaging employing steady- state acquisition), bFFE (balanced fast field echo), or CISS (constructive interference in steady state) MRI sequences should be included in order to evaluate the intracranial cisternal anatomy in detail, as this information may influence treatment options. In addition, the patient should undergo a full ophthalmological evaluation to assess for any visual compromise present pre- operatively and for post- treatment follow- up to ensure full resolution of the papilledema.
The brain MRI for this patient demonstrates dilation of the lateral and third ventricles with a normal fourth ventricle.Transependymal flow is demonstrated in the periventricular white matter, and the cortical sulci are effaced (Figure 2.1). Stenosis of the cerebral
Preoperative MRI with sagittal FIESTA sequences demonstrates aqueductal stenosis, bowing of the third ventricle, and absence of adhesions in the prepontine cistern.
(A)
(B)
Figure 2.1.
Figure 2.2.
aqueduct due to an enlarged tectum is identified. The cisternal space is open. The laminal terminalis and floor of the third ventricle are bowed (Figure 2.2). A small tectal glioma is suspected, and no other mass lesion is present. These findings are consistent with a diagnosis of obstructive hydrocephalus secondary to aqueductal stenosis.
Oral Boards Review—Diagnostic Pearls
1. The underlying etiology of newly diagnosed hydrocephalus should be established to determine the appropriate intervention and to accurately counsel the family regarding prognosis.
2. An MRI of the brain should be obtained whenever possible to rule out the presence of a mass lesion that may require alteration in the treatment plan.
3. Preoperative funduscopic evaluation should be carried out with any new diagnosis of hydrocephalus, and if papilledema or visual impairment is suspected, an urgent referral to ophthalmology should be placed.
Questions
1. Which surgical treatment options are available for the management of obstructive hydrocephalus?
2. What is the appropriate timing for intervention?
3. Which anatomic structures need to be carefully assessed in order to determine candidacy for endoscopic treatment?
Decision Making
The presence of papilledema secondary to elevated intracranial pressure can result in further visual decline, which could result in permanent deficit. Treatment should therefore be planned on an urgent basis. Therapeutic options for obstructive hydrocephalus include the surgical placement of a cerebral spinal fluid (CSF) shunt or endoscopic third ventriculostomy (ETV). While shunt placement is an effective option, it carries greater lifetime risk of morbidity, including post- operative shunt infection, need for further surgery in the setting of a shunt malfunction, and overdrainage complications. Endoscopic options for the treatment of obstructive hydrocephalus should be considered whenever the anatomy is amenable. If an obstructive lesion is found, such as with aqueductal stenosis, the likelihood of success with ETV is high. The prepontine and interpeduncular cisterns should be carefully evaluated on MRI bFFE/FIESTA/ CISS sequences in order to localize the basilar apex in relation to the floor of the third ventricle, and to determine the presence of arachnoid adhesions that may obstruct the subarachnoid cisternal space and decrease the likelihood of a successful ETV. If the preopontine cistern is occluded with adhesions, placement of a ventriculoperitoneal CSF shunt may be necessary. If the imaging workup reveals an underlying mass lesion, this should be addressed primarily and prior to any definitive hydrocephalusprocedure,asthehydrocephalusmaysubsequentlyresolvewithtreatment of the mass lesion.