Oxford Handbook of Clinical and Healthcare Research
Oxford Handbook of Clinical and Laboratory Investigation 4e
Oxford Handbook of Clinical Dentistry 7e
Oxford Handbook of Clinical Diagnosis 3e
Oxford Handbook of Clinical Examination and Practical Skills 2e
Oxford Handbook of Clinical Haematology 4e
Oxford Handbook of Clinical Immunology and Allergy 4e
Oxford Handbook of Clinical Medicine – Mini Edition 10e
Oxford Handbook of Clinical Medicine 10e
Oxford Handbook of Clinical Pathology
Oxford Handbook of Clinical Pharmacy 3e
Oxford Handbook of Clinical Specialties 11e
Oxford Handbook of Clinical Surgery 4e
Oxford Handbook of Complementary Medicine
Oxford Handbook of Critical Care 3e
Oxford Handbook of Dental Patient Care
Oxford Handbook of Dialysis 4e
Oxford Handbook of Emergency Medicine 5e
Oxford Handbook of Endocrinology and Diabetes 3e
Oxford Handbook of ENT and Head and Neck Surgery 3e
Oxford Handbook of Epidemiology for Clinicians
Oxford Handbook of Expedition and Wilderness Medicine 2e
Oxford Handbook of Forensic Medicine
Oxford Handbook of Gastroenterology & Hepatology 3e
Oxford Handbook of General Practice 5e
Oxford Handbook of Genetics
Oxford Handbook of Genitourinary Medicine, HIV, and Sexual Health 3e
Oxford Handbook of Geriatric Medicine 3e
Oxford Handbook of Infectious Diseases and Microbiology 2e
Oxford Handbook of Integrated Dental Biosciences 2e
Oxford Handbook of Head and Neck Anatomy
Oxford Handbook of Humanitarian Medicine
Oxford Handbook of Key Clinical Evidence 2e
Oxford Handbook of Medical Dermatology 2e
Oxford Handbook of Medical Imaging
Oxford Handbook of Medical Law and Ethics
Oxford Handbook of Medical Sciences 3e
Oxford Handbook for Medical School
Oxford Handbook of Medical Statistics 2e
Oxford Handbook of Neonatology 2e
Oxford Handbook of Nephrology and Hypertension 2e
Oxford Handbook of Neurology 2e
Oxford Handbook of Nutrition and Dietetics 3e
Oxford Handbook of Obstetrics and Gynaecology 3e
Oxford Handbook of Occupational Health 2e
Oxford Handbook of Oncology 3e
Oxford Handbook of Operative Surgery 3e
Oxford Handbook of Ophthalmology 4e
Oxford Handbook of Oral and Maxillofacial Surgery 2e
Oxford Handbook of Orthopaedics and Trauma
Oxford Handbook of Paediatrics 3e
Oxford Handbook of Pain Management
Oxford Handbook of Palliative Care 3e
Oxford Handbook of Practical Drug Therapy 2e
Oxford Handbook of Pre-Hospital Care 2e
Oxford Handbook of Psychiatry 4e
Oxford Handbook of Public Health Practice 4e
Oxford Handbook of Rehabilitation Medicine 3e
Oxford Handbook of Reproductive Medicine & Family Planning 2e
Oxford Handbook of Respiratory Medicine 4e
Oxford Handbook of Rheumatology 4e
Oxford Handbook of Sleep Medicine
Oxford Handbook of Sport and Exercise Medicine 2e
Handbook of Surgical Consent
Oxford Handbook of Tropical Medicine 4e
Oxford Handbook of Urology 4e
OXFORD HANDBOOK OF Head and Neck Anatomy
FIRST EDITION
Daniel R. van Gijn (Author)
Specialist Registrar Oral and Maxillofacial Surgery
Royal Surrey County Hospital, Guildford, UK with Jonathan Dunne (Co-author)
Consultant Plastic and Reconstructive Surgeon Charing Cross Hospital
Imperial College Healthcare NHS Trust, London, UK
consultant editors
Susan Standring
Emeritus Professor of Anatomy, Department of Anatomy King’s College London, UK
Simon Eccles
Consultant in Craniofacial Plastic and Reconstructive Surgery Chelsea and Westminster Hospital NHS Foundation Trust, London, UK
1
Great Clarendon Street, Oxford, OX2 6DP, United Kingdom
Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and in certain other countries
The moral rights of the authors have been asserted
First Edition Published in 2022
Impression: 1
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by licence or under terms agreed with the appropriate reprographics rights organization. Enquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above
You must not circulate this work in any other form and you must impose this same condition on any acquirer
Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America
British Library Cataloguing in Publication Data
Data available
Library of Congress Control Number: 2021945504
ISBN 978–0–19–876783–1
DOI: 10.1093/med/9780198767831.001.0001
Printed and bound in China by C&C Offset Printing Co., Ltd.
Oxford University Press makes no representation, express or implied, that the drug dosages in this book are correct. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulations. The authors and the publishers do not accept responsibility or legal liability for any errors in the text or for the misuse or misapplication of material in this work. Except where otherwise stated, drug dosages and recommendations are for the non-pregnant adult who is not breast-feeding
Links to third party websites are provided by Oxford in good faith and for information only. Oxford disclaims any responsibility for the materials contained in any third party website referenced in this work.
To my darling Polly and dear son, Wilfred
Foreword by Carrie Newlands
Daniel is to be commended for his combination of enthusiasm, dedication and artistic talent, which has given us this wonderful book. Anatomy is the backbone of much of a surgeon’s working day; we need to have its intricacies, vagaries, and three-dimensional complexity at our fingertips in order for us to do our jobs well and to deserve the trust our patients place in us.
Artistry and surgery go hand in hand and Daniel’s exquisite drawings in this highly practical book make anatomy easy to understand with clarity and elegance. Each picture paints a thousand words and thus, this first edition is both detailed and portable.
The etymology of anatomical terms and the historical tit-bits accompanying many anatomical eponyms serve to add another layer to the book’s readability. Likewise, the inclusion of operative considerations bridges the frequent gap between anatomical facts and surgical relevance.
A sound grounding in anatomy is still quite rightly required at undergraduate level in medicine and dentistry and often serves to kindle an early interest in many a future surgical career. I have no doubt that this addition to the bookshelf will help many students to find head and neck anatomy less of a terrifying prospect by sheer dint of its simplicity.
The Oxford Handbook of Head and Neck Anatomy will be particularly welcomed by those of us in head and neck surgical specialities at all stages of our careers, and members of many medical specialities will find the artistry and accessibility of this excellent resource to be invaluable.
Carrie Newlands Consultant Oral and Maxillofacial Surgeon Guildford, UK Chair, UK OMFS FRCS Examination Board
Foreword by Alice Roberts
If you want head and neck anatomy distilled down to its essence—this is it.
The head and neck are so densely packed with anatomical structures, it’s easy to get bogged down in unnecessary details while missing others that are more clinically relevant. Written by an experienced clinician, this book is laid out in a masterfully succinct and logical way, with clear, engineeringstyle diagrams that help the reader to conceptualize the three-dimensional jigsaw puzzle of head and neck anatomy. Along the way, there are nuggets of etymological delight that are historically fascinating—but also make the elaborate terminology more understandable and memorable. Covered as well are those much beloved TLAs—the three letter abbreviations that litter the clinical landscape of anatomy.
This book will be useful to undergraduates learning anatomy for the first time, but also for trainees specializing in those anatomical areas above the clavicle—who will look back and wish they’d had this text at medical school.
Armed with this powerful tome, the pterygopalatine fossa will never again hold such terror, the infamous infratemporal fossa will be laid bare, and the lacrimal lake of despond will dry up. And with this map in hand, a safari in tiger country will be much, much less dangerous.
Professor Alice Roberts Anatomist,
author & broadcaster Professor of Public Engagement in Science, University of Birmingham
Preface
One day I will find the right words and they will be simple.
Jack Kerouac
The idea for this book began while a medically qualified dental student, embarking (again) on the seemingly Herculean task of learning head and neck anatomy—under the watchful eye and tutelage of Professor Susan Standring. The book is aimed at medical and dental undergraduates facing similar struggles—as well as dentists, ENT, oral and maxillofacial or plastic surgeons, anaesthetists, and radiologists with a particular interest in the pathology of the head and neck.
The principle of the book is to provide a succinct yet comprehensive pocket guide to the elegant and three-dimensional anatomy of the head and neck, accompanied by simple-to-use schematic line diagrams. It intends to distil conceptually difficult regions of the head and neck into their respective ‘bare bones’—constructing a skeleton on which the flesh can be subsequently added, in a format that can be reproduced (and hopefully remembered) on the operating theatre whiteboard or in a notebook in the outpatient clinic or ward environment.
Anatomy, like medicine, has a specific language. A language monopolized by Latin. As with any language, understanding the meaning of a word helps to glean its purpose—and perhaps provide a glimpse into its etymological or eponymous past. How can regional anatomy that includes references to the winged helmet of Hermes, a goat, and a wandering vagrant not help but spark inspiration and stimulate excitatory synapses?
The science of anatomy (from ἀνατομή meaning ‘to cut up’) underpins pathology (‘the study of suffering’) which in turn provides the link to medicine and its subsequent inquiry into disease. We are all anatomists at heart: a strong foundation in anatomy promotes clinical ‘common sense’, acumen, and surgical confidence—allowing you to interpret the problem and to propose a solution on anatomical grounds.
My personal appreciation of the anatomy of the head and neck significantly improved over the course of writing, researching and illustrating this book. I have tried to balance bullet points and prose and to provide easy-tonegotiate illustrations that are intended to simplify complicated anatomical relationships. As a reader and ‘learner’, you will have your own areas of difficulty and confusion and I welcome your suggestions as to how to improve the text and figures.
Whether you are from a dental, medical, or surgical background, I hope this book gives you the enthusiasm to continue to explore the anatomy, surgery, and pathology that makes a career in a head and neck specialty so rewarding.
Daniel R. van
Gijn
Acknowledgement
Professor Patricia Collins
Chapter 15: Embryology of the head and neck
Professor of Anatomy, Anglo-European College of Chiropractic, Bournemouth, UK
Miss Lisa Pitkin
Chapter 8: The Larynx
ENT and Head and Neck surgeon, Royal Surrey County Hospital, UK
Symbols and abbreviations
% cross-reference
a. artery
AICA anterior inferior cerebellar artery
ACF anterior cranial fossa
CCA common carotid artery
CNS central nervous system
CSF cerebrospinal fluid
CT computed tomography
DCR dacrocystorhinostomy
ECA external carotid artery
EJV external jugular vein
ENT ear, nose, and throat
f. foramen
ICA internal carotid artery
ICP intercuspal position
IJV internal jugular vein
IMF intermaxillary fixation
LPS levator palpebrae superioris
m. muscle
MCF middle cranial fossa
MPL medial palpebral ligament
n. nerve
NOE naso-orbito-ethmoidal
ORIF open reduction internal fixation
PCF posterior cranial fossa
PICA posterior inferior cerebellar artery
RAPD relative afferent pupillary defect
ROOF retro-orbicularis oculi fat
RSTL relaxed skin tension line
SOOF suborbicularis oculi fat
SCC squamous cell carcinoma
SCM sternocleidomastoid
SMAS superficial muscular aponeurotic system
SOF superior orbital fissure
TMJ temporomandibular joint
v. vein
The skull
Introduction 2
Frontal view 4
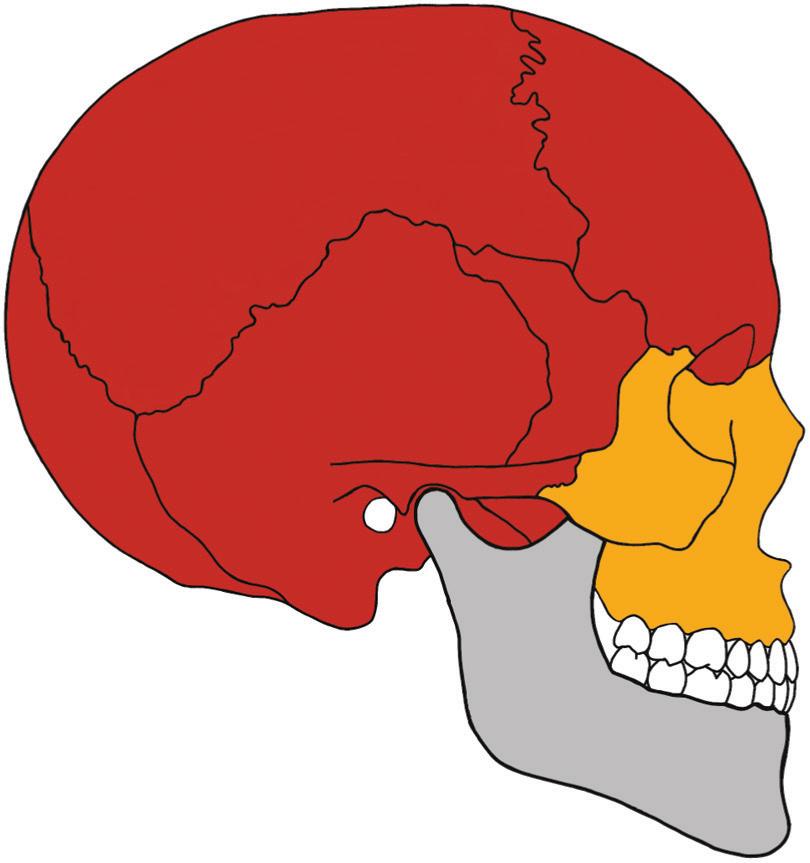
Lateral view 6
Superior view 8
Frontal bone 10
Zygomatic bone 14
Occipital bone 18
Temporal bone 22
Parietal bone 30
Maxilla 32
Sphenoid bone 40
Ethmoid bone 50
Palatine bone 54
Vomer 58
Lacrimal bone 60
Inferior nasal concha 61
Nasal bone 62
Introduction
The human skull is the skeleton of the head and is considered along with the mandible. It consists of paired bones and unpaired midline bones that contribute to the muscular attachments for mastication and facial expression, a bony foundation for the upper aerodigestive tract, and support and housing for those structures susceptible to trauma—the special sensory organs and brain.
The skull without the mandible is termed the cranium and consists of the neurocranium (skull vault) and viscerocranium (facial skeleton). The precise number of bones, rather surprisingly, varies depending on the source—with some including the hyoid and ossicles and others discounting paired bones (% Fig. 1.1b, p. 5 and Fig. 1.2b, p. 7).
The calvaria consists of the cranium without the facial skeleton and cranial base. It consists of the frontal, parietal, and occipital bones and is completed laterally by the greater wings of the sphenoid and the temporal bones. It comprises an external layer or ‘table’ and internal table with a middle cancellous, diploic bone between. Fractures may involve either in isolation or both, with varying clinical consequences.
There is significant variety in the thickness of the bones of the skull, with those areas covered by muscle thinner than those without, with obvious sequelae following trauma. The boundaries of these more vulnerable areas are the strong vertical and horizontal buttresses of the face that are the prime focus of reconstruction and restoration for the facial trauma surgeon.
The sutures found between adjoining bones of the skull are fibrous joints that allow for the growth of the developing skull and brain. The premature fusion of sutures prevents the normal expansion of the skull perpendicular to the stenosed suture and results in a multitude of craniosynostoses, classified according to the suture or sutures involved. Joints found between the bones of the skull base are cartilaginous, the most important perhaps being the synchondrosis between the sphenoid and occipital bones, which fuses at approximately 18 years of age and allow the forensic physician to attribute an age to a cadaver or isolated bones with a reasonable degree of confidence and window of accuracy.
While the base of the skull and its primary cartilaginous joints separate the neurocranium from the viscerocranium, synovial joints separate the cranium from the mandible and the skull from the cervical spine by way of the temporomandibular and atlanto-occipital joints, respectively.
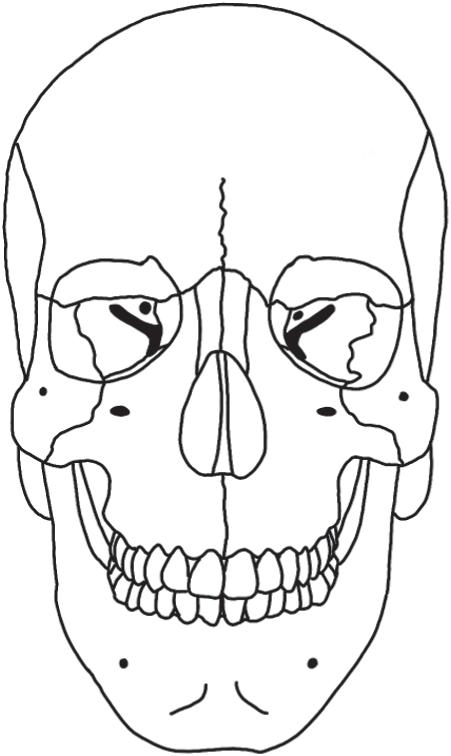
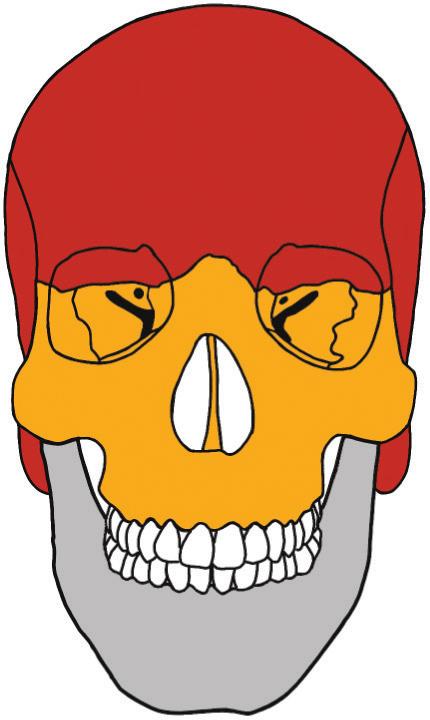
Frontal view
The upper third of the skull is principally formed by the frontal bones and exaggerated at the superciliary ridges of the superior orbit and smooth glabellar region centrally. The paired maxillary bones form the middle third, creating the circumference of the piriform aperture between them, and are separated from the frontal and temporal bones by the zygoma laterally on each side (Fig. 1.1a). They house the maxillary sinuses and meet in the midline inferiorly to form the upper jaw and most of the hard palate at the intermaxillary suture. The mandible forms the lower third of the frontal view (Fig. 1.1b).
Key features
Supraorbital foramen
• May be a notch or a foramen in the frontal bone. Lies above the orbit at the junction of the medial and lateral two-thirds of the superior orbital rim.
• Transmits the supraorbital nerve (V1) and supraorbital artery from the ophthalmic artery.
Optic canal
• Bound by the lesser wing of the sphenoid bone.
• Transmits the optic nerve and ophthalmic artery (from ICa).
Superior orbital fissure
• Between the greater and lesser wings of the sphenoid.
• Transmits the oculomotor, trochlear, and abducens nerves, the ophthalmic division of the trigeminal nerve (V1), and the superior and inferior ophthalmic veins.
Inferior orbital fissure
• Bound by the greater wing of the sphenoid, the maxilla, and the orbital process of the palatine bone.
• Transmits the maxillary division of the trigeminal nerve (V2), the infraorbital vessels, and the zygomatic nerve.
Zygomaticofacial foramen
• Malar part of the zygomatic bone (malar meaning ‘cheek’—the most prominent part).
• Transmits the zygomaticofacial nerve of V2
Infraorbital foramen
• Found 7 mm below the inferior orbital rim of the maxilla, approximately in the mid-pupillary line.
• Transmits the infraorbital (V2) nerve and vessels.
Mental foramen
• Located between the first and second premolars, midway between the upper and lower mandibular border.
• Transmits the mental nerve and vessels, which are continuations of the inferior alveolar neurovascular bundle.