Published and forthcoming Oxford Handbooks in Nursing
Oxford Handbook of Adult Nursing 2e
Edited by Maria Flynn and Dave Mercer
Oxford Handbook of Cancer Nursing, 2e
Edited by Mike Tadman and Dave Roberts
Oxford Handbook of Cardiac Nursing, 3e
Edited by Kate Olson
Oxford Handbook of Children’s and Young People’s Nursing, 2e
Edited by Edward Alan Glasper, Gillian McEwing, and Jim Richardson
Oxford Handbook of Clinical Skills in Adult Nursing, 2e
Edited by Frank Coffey, Alison Wells, and Mark Fores
Oxford Handbook of Clinical Skills for Children’s and Young People’s Nursing
Paula Dawson, Louise Cook, Laura-Jane Holliday, and Helen Reddy
Oxford Handbook of Critical Care Nursing, 2e
Sheila Adam and Sue Osborne
Oxford Handbook of Dental Nursing
Elizabeth Boon, Rebecca Parr, Dayananda Samarawickrama, and Kevin Seymour
Oxford Handbook of Diabetes Nursing
Lorraine Avery, Joanne Buchanan, Anita Thynne
Oxford Handbook of Emergency Nursing, 2e
Edited by Robert Crouch, Alan Charters, Mary Dawood, and Paula Bennett
Oxford Handbook of Gastrointestinal Nursing, 2e
Edited by Jennie Burch and Brigitte Collins
Oxford Handbook of Learning and Intellectual Disability Nursing
Edited by Bob Gates and Owen Barr
Oxford Handbook of Mental Health Nursing, 2e
Edited by Patrick Callaghan and Catherine Gamble
Oxford Handbook of Midwifery, 3e
Janet Medforth, Susan Battersby, Maggie Evans, Beverley Marsh, and Angela Walker
Oxford Handbook of Musculoskeletal Nursing
Edited by Susan Oliver
Oxford Handbook of Neuroscience Nursing 2e
Edited by Sue Woodward and Catheryne Waterhouse
Oxford Handbook of Nursing Older People, 2e
Edited by Marie Honey, Annette Jinks, and Lauren Hanson
Oxford Handbook of Trauma and Orthopaedic Nursing 2e
Rebecca Jester, Julie Santy, and Jean Rogers
Oxford Handbook of Perioperative Practice
Suzanne Hughes and Andy Mardell
Oxford Handbook of Prescribing for Nurses and Allied Health Professionals
Sue Beckwith and Penny Franklin
Oxford Handbook of Primary Care and Community Nursing 3e
Edited by Judy Brook, Caroline McGraw, and Val Thurtle
Oxford Handbook of Renal Nursing
Edited by Althea Mahon, Karen Jenkins, and Lisa Burnapp
Oxford Handbook of Respiratory Nursing
Terry Robinson and Jane Scullion
Oxford Handbook of Surgical Nursing
Edited by Alison Smith, Maria Kisiel, and Mark Radford
Oxford Handbook of Women’s Health Nursing, 2e
Edited by Sunanda Gupta, Debra Holloway, and Ali Kubba
OXFORD HANDBOOK OF Gastrointestinal Nursing
second edition
Jennie Burch
Head of St Mark’s Nurse Education, St Mark’s Hospital, Harrow, UK
Brigitte Collins
Global Clinical Education Manager, MacGregor Healthcare Ltd, Macmerry, East Lothian, UK
1
Great Clarendon Street, Oxford, OX2 6DP, United Kingdom
Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and in certain other countries
The moral rights of the authors have been asserted
First Edition published in 2008
Second Edition published in 2021
Impression: 1
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by licence or under terms agreed with the appropriate reprographics rights organization. Enquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above
You must not circulate this work in any other form and you must impose this same condition on any acquirer
Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America
British Library Cataloguing in Publication Data
Data available
Library of Congress Control Number: 2020943967
ISBN 978–0–19–883317–8
DOI: 10.1093/med/9780198833178.001.0001
Printed and bound in China by C&C Offset Printing Co., Ltd.
Oxford University Press makes no representation, express or implied, that the drug dosages in this book are correct. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulations. The authors and the publishers do not accept responsibility or legal liability for any errors in the text or for the misuse or misapplication of material in this work. Except where otherwise stated, drug dosages and recommendations are for the non-pregnant adult who is not breast-feeding
Links to third party websites are provided by Oxford in good faith and for information only. Oxford disclaims any responsibility for the materials contained in any third party website referenced in this work.
Preface
The first edition of the Oxford Handbook of Gastrointestinal Nursing was published more than 10 years ago. The opportunity to produce a second edition has arisen. Each chapter has been updated and summarizes gut function and gives an overview of what is considered as best practice. The handbook is intended to provide a pocket-size resource allowing healthcare professionals easy access to anatomy, physiology, investigations, and common conditions and problems, regarding the gastrointestinal tract with details of further reading, including online information, where applicable.
Jennie Burch and Brigitte Collins
December 2019
Foreword to the second edition
It gives me great pleasure to see this Handbook being updated in this second edition. The nursing role in helping people with gastrointestinal disorders has continued to develop in the decade since the first edition, and this is fully reflected in the content of this new edition. This Handbook provides an excellent quick reference guide for both the specialist nurse working specifically with patients with gut disorders and the generalist nurse whose patients happen to have gastrointestinal symptoms.
This is a rapidly developing speciality, with many advances in understanding of gastrointestinal disorders and in their investigation, treatment, and management. Nurses working in both hospital and community settings need to consider the gut health of all of their patients.
A range of patients with various illnesses and disorders or taking a variety of medications will experience gut issues or side effects. These can be as bothersome as the primary disease, if not at times even more so. Additionally, many patients presenting with a variety of problems may have pre-existing gastrointestinal disorders, or will be at risk of gastrointestinal problems if their gut health is not proactively managed. The more we understand about the gut, the more we come to appreciate its central role in health. There are now strong suggestions that the gut microbiota is a major determinant of health and dysbiosis, and is a factor in many major health problems, such as depression, dementia, and diabetes. Gone are the days when we could give a broad-spectrum antibiotic without considering its effect on gut ecology, or manage a major illness such as cancer or an injury without attention to long-term gut consequences.
Nurses in all settings need the basic understanding of the gut contained in this volume. Many will want to refer to it regularly when encountering patients with gut problems as a primary or secondary health issue. The editors have done a great job of updating the text and providing links to sources of further information. I commend it to all nurses.
Christine Norton
Professor of Clinical Nursing Research, King’s College London January 2020
Anatomy and physiology of the gastrointestinal tract
Gut overview 2
Gut structure 4
Abdominal cavity and pelvic cavity 5
Gut nerves, hormones, secretions, and blood supply 6
Mouth, pharynx, oesophagus, and stomach 8
Small bowel, colon, rectum, and anus 10
Accessory organs 14
Gut overview
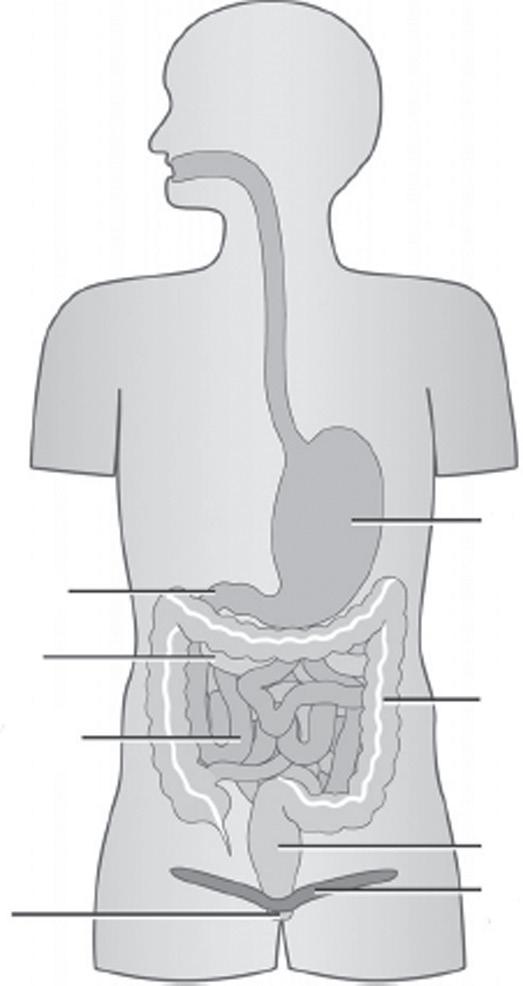
the gastrointestinal (GI) tract (Fig. 1.1) is a hollow tube passing from the mouth to the anus. there are several names for the GI tract, including the alimentary canal or gut. the GI tract is about 7–11 metres long but appears shorter due to the creases in the gut wall. there are many organs making up the GI tract:
• Mouth
• pharynx
• Oesophagus
• Stomach
• Small bowel
• Large bowel.
there are also a number of accessory organs that help breakdown ingested food:
the main function of the GI tract is to make ingested nutrients available for the body to use. there are five main processes involved in the functioning of the GI tract:
• Ingestion
• propulsion
• Digestion
• Absorption
• elimination.
Ingestion
this is another term for eating—taking food into the body.
Propulsion
Ingested food is moved through the GI tract, initially by swallowing (voluntary action) and progressing to peristalsis, an involuntary action. In peristalsis, the gut wall contracts and pushes the food bolus or waste further along the GI tract; the muscles then relax and contract again. this combination of contracting and relaxing helps to break down the food and propels it forward. peristalsis occurs in the oesophagus, stomach, small bowel, and large bowel.
Digestion
Ingested food is broken down into smaller parts in two ways: chemically and mechanically. In the mouth, the teeth chew the food, breaking it into smaller parts, and mix it with saliva (mechanical breakdown). the saliva begins to digest the food (chemical breakdown). the stomach churns the food (mechanical breakdown), and acid and digestive enzymes are secreted to breakdown it down chemically. Segmentation contractions in the small bowel mix the food with the digestive enzymes and break it down (mechanical breakdown), with peristalsis moving food further along the GI tract. there is further chemical breakdown of the food by bile, which is made in the liver (% pp. 15–6) and stored in the gall bladder (% p. 14), and pancreatic juice from the pancreas (% p. 14).
Absorption
the nutrients from the diet are taken from the GI tract into the blood or lymph. Additionally, the 7 litres of secretions (% p. 6) produced by the body and added to the GI tract are absorbed. Nutrients, electrolytes, and water are absorbed in the small bowel. electrolytes and water are absorbed in the colon.
Elimination
this is the passage of faeces, out of the body via the anus, past the anal sphincters that control defaecation (% p. 446).
Further reading
waugh A and Grant A (2018). Ross & Wilson Anatomy and Physiology in Health and Illness. 13th ed. elsevier. Cambridge.
Gut structure
there are four main layers of tissue in the GI tract, these are:
• Serosa
• Muscularis
• Submucosa
• Mucosa.
Serosa
the serosa is the outer layer of the GI tract (except the oesophagus) and the largest serous membrane of the body. In the abdominal cavity the serosa comprises:
• parietal peritoneum—lines the abdominopelvic cavity
• visceral peritoneum—covers the gut and other organs
• peritoneal cavity—space between the layers
• Folds—binds organs to each other and the abdominal wall.
Muscularis
the muscle layer that surrounds the submucosa is termed the muscularis. there are longitudinal and circular smooth muscles in the GI. this layer is responsible for peristalsis and segmentation. thicker areas of circular muscles also form the sphincters.
Submucosa
the submucosa is formed from connective tissue. the blood vessels, lymphatics, and enteric nervous system that supply the wall of the GI tract are found in this layer, and due its elasticity, organs such as the stomach (% p. 9) can stretch and regain their shape.
Mucosa
Finally, the mucosa, the inner most part of the GI tract, is lined with epithelial cells that renew every 4–7 days. this layer varies somewhat in different areas of the GI tract. Mucus is secreted into the stomach, small bowel, and large bowel to protect the GI tract from digestive enzymes and lubricate passage of food. In the stomach and small bowel, there are endocrine cells that secrete hormones into the bowel lumen. Also, in the small bowel the inner surface is covered with villi and microvilli that increase the surface area about 20-fold to vastly increase absorptive capacity from the bowel lumen. the lamina propria is part of the mucosa and is made from connective tissue; it is responsible for absorption and defence from bacteria and other pathogens.
Abdominal cavity and pelvic cavity
In the main, the GI tract is within the abdominal cavity. the thoracic cavity is separated from the abdominal cavity by the diaphragm. the abdominal cavity contains the stomach, small and large intestine, gall bladder, pancreas, and liver, and other organs such as the spleen. there is no physical separation between the abdominal cavity and the pelvic cavity. the pelvic cavity contains the rectum and other organs such as the urinary bladder. the abdominal and pelvic cavities are lined with serous membranes. the largest membrane within the abdomen and pelvis is the peritoneum. the peritoneum is formed from the parietal peritoneum and visceral peritoneum, which are joined. the parietal peritoneum lines the body walls and the visceral peritoneum covers the organs. the space between the parietal peritoneum and the visceral peritoneum is the peritoneal cavity, which contains fluid that enables the membranes to slide and allows movement within the abdominal cavity. thus mobile organs, such as the small bowel, are able to move as the body moves. Digestive organs within the peritoneal cavity are termed intraperitoneal, and those that are posterior to the peritoneum, such as the pancreas and duodenum, are termed retroperitoneal organs. within the abdominal cavity, there are parts of the peritoneum that are folded: this is called the mesentery. the mesentery holds parts of the digestive tract in place. Additionally, the mesentery is a passage for blood vessels, lymphatics, and nerves to reach the digestive viscera.
Gut nerves, hormones, secretions, and blood supply
Enteric nervous system
enteric nerves are mediators of movement and sensation in the gut. Gut motility is mostly controlled by the enteric nervous system, with stimulation or inhibition by the central autonomic nervous system. this is why the GI tract continues to work after complete spinal cord injury, albeit more slowly and often with constipation. Local reflexes are mostly in response to distension, modified by the luminal content of the gut.
Autonomic nervous system
the gut is also supplied by the autonomic (involuntary) part of the central nervous system. Sympathetic nerves slow down gut motility and close sphincters. this is useful when gut activity is not desirable, such as in relation to ‘fight or flight’. parasympathetic nerves stimulate motility and open sphincters. Digestion occurs best when the body is relatively at rest.
Hormones
Many hormones control secretions within the gut. three important examples are:
• Cholecystokinin—released in the duodenum and jejunum when fat is present. the function is to inhibit stomach activity and stimulate release of bile by the gall bladder.
• Secretin—released from the duodenum. the function is to inhibit motility in response to acid from the stomach.
• Gastric inhibitory peptide—released in the small bowel in response to the presence of fats, carbohydrate, and amino acids. the result is to inhibit the stomach and allow time for digestion and absorption in the small bowel, before the release of more gastric contents.
Secretions
there are about 7 litres of secretions that enter the GI tract every day; predominantly in the upper gut, up to and including the duodenum. this is made up from saliva (0.5–1.5 litres), gastric juices (2–3 litres), and pancreas and gall bladder (1.5–2 litres).
Blood supply
the blood supply to the GI tract is via the abdominal aorta: the splanchnic circulation. the arterial blood supply to the stomach is through the coeliac artery. the blood drains via the hepatic portal vein. the blood supply for the liver is via the portal circulation, with 70% of blood supply being carried to the liver from the small bowel. this blood contains nutrients, amongst other substances. the three hepatic veins drain into the vena cava. the other 30% of the blood supply is taken to the liver via the hepatic artery; 25% of the cardiac output goes to the liver.
Motility
In general, meals empty from the stomach within 2–3 h, with liquids emptying faster than solids. Most food residue reaches the colon within 6 h.
Mouth, pharynx, oesophagus, and stomach
Mouth
the mouth is the first part of the GI tract. external to the mouth are the lips and cheeks. within the mouth are the palate, teeth, and tongue. the palate separates the oral and nasal cavities. the teeth are used for mastication (chewing). the tongue is used for taste and speech, and is involved in mastication and swallowing. the lining of the mouth is made up of epithelial cells. the mouth produces saliva from three sets of salivary glands: the parotid glands are located between the ears and the jaw, the submandibular glands under the jaw, and the sublingual glands under the tongue. Saliva lubricates and begins digestion. the salivary glands produce ptyalin, a type of amylase, which breakdowns starch, and an antibacterial agent. the mouth receives food and drink. Digestion begins in the mouth by mechanical and chemical means: ingested food is masticated and mixed with saliva and formed into a food bolus. when the food bolus is voluntarily swallowed, it will pass into the pharynx (% p. 8).
Pharynx
the pharynx, also termed the throat, is funnel shaped and connects the mouth and oesophagus. the pharynx also joins the nasal cavity to the larynx, part of the respiratory system. these two areas are separated by the epiglottis, a flap of tissue that prevents food getting into the larynx and airway.
Oesophagus
the oesophagus is a muscular tube about 25 cm long and a little under 2 cm in diameter. It begins at the pharynx and ends at the stomach, at the cardiac sphincter, and is situated behind the trachea and close to the greater vessels and left atrium of the heart. It passes through the diaphragm as it travels to the stomach. the upper portion of the oesophagus is formed of striated muscle to aid the swallowing reflex (voluntary decision), while the lower two-thirds is formed of smooth muscle to move food towards the stomach by peristalsis (involuntary). the muscles of the oesophagus contract and relax to move food down to the stomach. peristalsis is effective and food will pass to the stomach, even if the person is lying down. the inner lining of the oesophagus is epithelial tissue, the function of which is to protect the oesophagus. protection of the oesophagus is also aided by the mucus produced from the mucous glands.
Food and fluid are swallowed from the mouth, and pass into the pharynx, the oesophagus, and to the stomach. there are sphincters at the top and bottom of the oesophagus. the upper sphincter is closed except during the swallowing, when it opens to allow food to enter the oesophagus. the lower or cardiac sphincter prevents partially digested food from re-entering the oesophagus.
If the oesophagus is involved in the vomiting reflex, the peristaltic action is reversed.
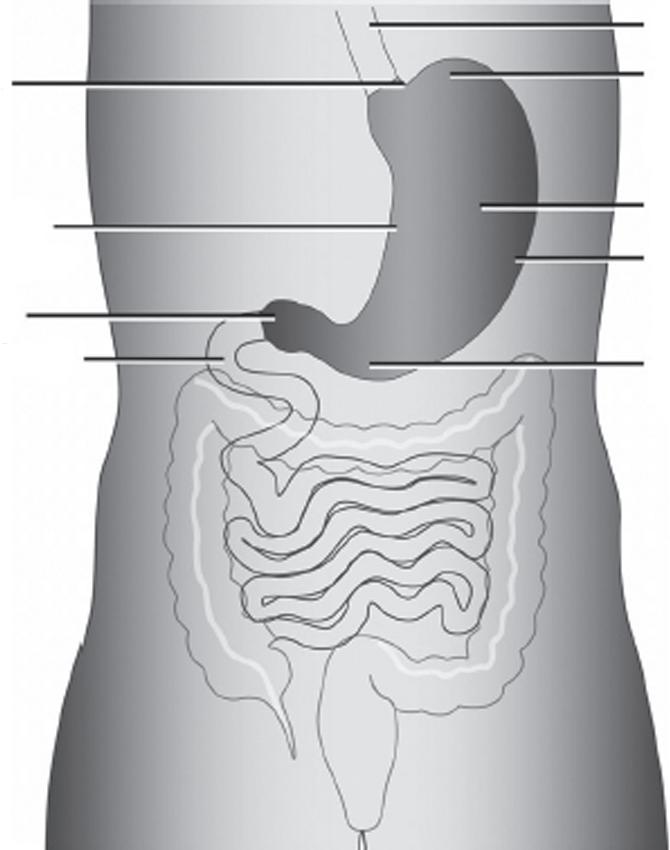
Stomach
the stomach is a hollow, J-shaped, sac-like organ that lies within the abdomen. Its function is mechanical churning, storage, and digestion of ingested food. the stomach is joined to the oesophagus % p. 8) at the top and the duodenum (% p. 10) at the bottom. the sphincters prevent unregulated flow from the stomach into the bowel (pyloric sphincter) or backflow from the stomach to the oesophagus (cardiac sphincter). the main part of the stomach is termed the body, the top is the fundus, and the lower aspect is the antrum (Fig. 1.2). the mucosa covers coarse folds (rugae) with smoother antral mucosa. the muscles of the stomach wall enable it to perform the mechanical digestion of churning and also allow for expansion. Additionally, there is chemical digestion by substances secreted into the stomach. these include hydrochloric acid (hCl) which is produced in the parietal cells, pepsin produced in the chief cells, and mucus made by the goblet cells. these gastric secretions are stimulated by either the presence of food or the anticipation of food. Once food is broken down the pyloric sphincter will allow passage of the semiliquid (chyme) into the duodenum. Liquids generally leave the stomach faster than solids, with most meals leaving the stomach within 2–3 h.
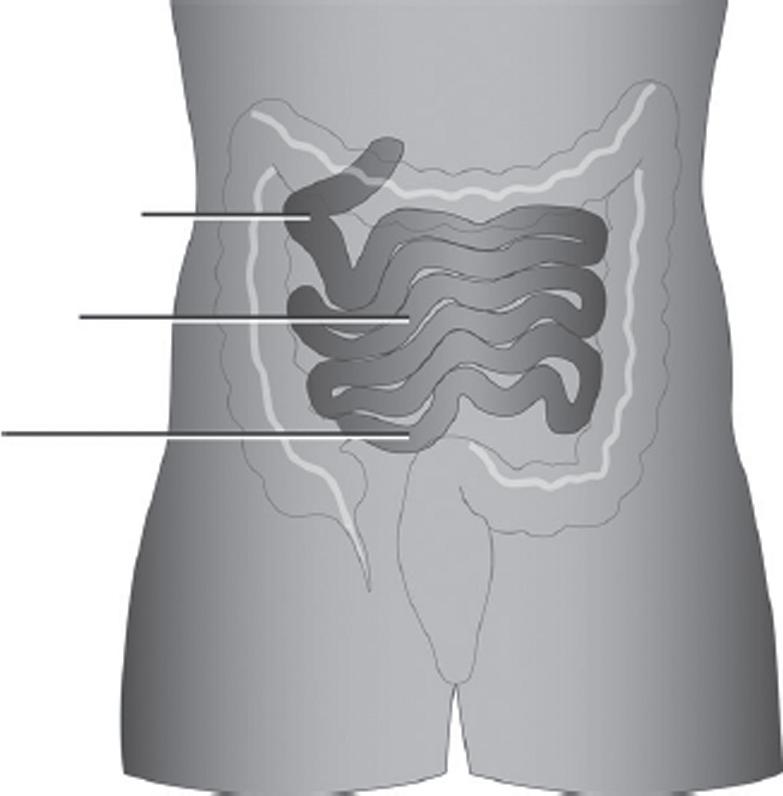
the small bowel, also termed the small intestine, is a long, hollow tube (see Fig. 1.3). the small bowel varies in length from about 3 to 9 m, and is usually longer in ♂ than ♀. the inner surface is deeply folded and covered in villi that, in turn, are covered in microvilli, to dramatically increase the surface area and increase the absorptive ability. there are three sections to the small bowel: duodenum, jejunum, and ileum.
the duodenum directly follows from the stomach (% p. 9) onto the jejunum and is a hollow tube about 20 cm long. pancreatic juice (from the pancreas) and bile (from the gall bladder) are secreted into the duodenum. within the duodenum, further breakdown of ingested food occurs by activity of pancreatic enzymes, specifically polypeptides (into peptides), polysaccharides (into monosaccharides and disaccharides), and triglycerides (into glycerol and free fatty acids). Biliary secretions (bile) make lipids soluble.
Jejunum
the jejunum follows the duodenum and precedes the ileum. At the brush border of the jejunum (formed by microvilli) simple sugars and amino acids are absorbed. Lipids are absorbed in the jejunum and ileum.
Ileum
the ileum varies in length from 2 to 4 m and follows the jejunum, although there is no definite demarcation between the two. It ends at the ileocaecal valve, which joins the small bowel to the caecum, and has a ph of neutral to alkaline. Digestion and absorption continue in the ileum. Bile salts are mainly absorbed from the last 100 cm of the ileum, and vitamin B12 from the terminal ileum (last 60 cm).
Duodenum
Jejunum
Ileum
Colon
the colon is a tubular structure about 1.5 m long in the average adult. It starts at the ileocaecal valve and ends at the anal verge. the sections of the colon are caecum (attached here is the appendix), ascending colon, transverse colon, descending colon, and sigmoid colon passing to the rectum. the area of the colon that joins the ascending and transverse colon is termed the hepatic flexure as it passes near the liver. the junction joining the transverse and descending colon is termed the splenic flexure as it passes the spleen.
the inner lining of the colon differs from the small bowel as there are no villi. the colonic mucosa consists of tightly packed crypts, lined with goblet cells. the average lifespan of the colonic cells is 3–5 days. the function of the colon is:
• to concentrate faeces by removal of water and electrolytes
• Storage and evacuation of faeces
• Fermentation of undigested sugars.
Most food residue will reach the colon within 6 h.
Rectum and anus
the rectum follows the sigmoid colon and ends at the anal canal. the rectum has three sections. the rectum accepts stools, and once a level of filling is reached, it stimulates a conscious sensation. Overfilling of the rectum can result in overdistension or inflammation.
the anus is about 3–5 cm in length, and shorter in women. proximally, the anus is similar to the colon and distally it is formed of squamous epithelium, similar to the skin. within the anus is the dentate line, the transition zone where the colonic mucosa and the anal mucosa meet. there are three blood-filled anal (haemorrhoidal) cushions.
there are two anal sphincters, internal (IAS) and external (eAS), which circle the anus.
Anal sphincters
There are two anal sphincters–sleeves of muscle, separated by a layer of longitudinal muscle–which circle the anus: the internal (IAS) and external (EAS) anal sphincters (Fig.1.4).
Internal anal sphincter
• Smooth (involuntary) muscle, which is 2–3 mm thick (thickens with age) and 2–3 cm long
• Continuous with circular smooth muscle wall of the rectum
• extends along the proximal (upper) two-thirds of the anal canal
• responsible for passive retention of stools at rest (contributes 80% of resting anal pressure)
• Subject to idiopathic degeneration with age and disruption by anal trauma (e.g. following anal surgery or abuse).