Respiratory Symptoms
What Do I Do Now?: Palliative Care
SERIES EDITOR
Margaret L. Campbell, PhD, RN, FPCN
Professor Emeritus, Wayne University College of Nursing, Detroit, MI
OTHER VOLUMES IN THE SERIES
Pediatric Palliative Care, Edited by Lindsay B. Ragsdale & Elissa G. Miller
Pain, Edited by Christopher M. Herndon
Respiratory Symptoms
Edited by Margaret L. Campbell, PhD, RN, FPCN
Professor Emeritus, Wayne University College of Nursing, Detroit, Michigan
Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and certain other countries.
Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America.
© Oxford University Press 2023
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by license, or under terms agreed with the appropriate reproduction rights organization. Inquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above.
You must not circulate this work in any other form and you must impose this same condition on any acquirer.
CIP data is on file at the Library of Congress
ISBN 978–0–19–009889–6
eISBN 978–0–19–009891–9
DOI: 10.1093/med/9780190098896.001.0001
This material is not intended to be, and should not be considered, a substitute for medical or other professional advice. Treatment for the conditions described in this material is highly dependent on the individual circumstances. And, while this material is designed to offer accurate information with respect to the subject matter covered and to be current as of the time it was written, research and knowledge about medical and health issues is constantly evolving and dose schedules for medications are being revised continually, with new side effects recognized and accounted for regularly. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulation. The publisher and the authors make no representations or warranties to readers, express or implied, as to the accuracy or completeness of this material. Without limiting the foregoing, the
publisher and the authors make no representations or warranties as to the accuracy or efficacy of the drug dosages mentioned in the material. The authors and the publisher do not accept, and expressly disclaim, any responsibility for any liability, loss, or risk that may be claimed or incurred as a consequence of the use and/or application of any of the contents of this material.
List of Contributors
Introduction
Dyspnea Assessment
Margaret L. Campbell
Reducing Dyspnea by Optimizing Treatment of Chronic Obstructive Pulmonary Disease
Miranda Wilhelm and Jennifer Arnoldi
Treating Chronic Breathlessness in Severe Chronic Obstructive Pulmonary Disease
Lynn F. Reinke, Mary M. Roberts, and Tracy A. Smith
Dyspnea, Chronic Obstructive Pulmonary Disease, and Pulmonary Rehabilitation
DorAnne Donesky and Julie Howard
Treating Episodic Breathlessness
Yvonne Eisenmann and Steffen Simon
Reducing Episodic Dyspnea in Heart Failure
Beth B. Fahlberg and Ann S. Laramee
Dyspnea in Pediatric Congenital Heart Disease
Jennifer Wright and Jessica L. Spruit
Treating Chronic Dyspnea in Patients with Lung Cancer
Elizabeth A. Higgins, Susan Ezemenari, and Julia Arana West
Treating Dyspnea Through Reducing Malignant Pleural Effusion
Christine A. Crader
Treating Dyspnea in Lung Cancer with Noninvasive Ventilation
Vittoria Comellini and Stefano Nava
Palliative Care for Infants with Bronchopulmonary Dysplasia
Christine A. Fortney and Jodi A. Ulloa
Reducing Dyspnea by Treating Ascites
Habib A. Khan
Panting for Breath in End-Stage Dementia
Hermien W. Goderie-Plomp, Carole Parsons, David R. Mehr, and Jenny T. van der Steen
Last Days with Chronic Obstructive Pulmonary Disease
Margaret L. Campbell
Withdrawal of Invasive Mechanical Ventilation
Margaret L. Campbell
Palliative Sedation for Intractable Dyspnea
Patricia Bramati and Eduardo Bruera
Sialorrhea in Amyotrophic Lateral Sclerosis
Mark B. Bromberg
Death Rattle
Margaret L. Campbell
Index
Contributors
Jennifer Arnoldi, PharmD, BCPS
Clinical Associate Professor
Southern Illinois University
Edwardsville (SIUE) School of Pharmacy
Edwardsville, IL, USA
Patricia Bramati, MD
The University of Texas MD
Anderson Cancer Center
Houston, TX, USA
Mark B. Bromberg, MD, PhD
Department of Neurology
University of Utah
Salt Lake City, UT, USA
Eduardo Bruera, MD
The University of Texas MD
Anderson Cancer Center
Houston, TX, USA
Margaret L. Campbell, PhD, RN, FPCN
Wayne State University, College of Nursing
Detroit, MI, USA
Vittoria Comellini, MD
Respiratory and Critical Care Unit
University Hospital St. Orsola-Malpighi
Bologna, Italy
Christine A. Crader, MD
Ascension Medical Group
Internal Medicine
Detroit, MI, USA
DorAnne Donesky, PhD, ANP-BC, ACHPN, ATSF
Professor, School of Nursing
Touro University of California
Vallejo, CA, USA
Yvonne Eisenmann, MD
University of Cologne
Faculty of Medicine and University Hospital
Department of Palliative Medicine
Cologne, Germany
Susan Ezemenari, MD
Fellow, Palliative Medicine
Division of Internal Medicine, Palliative Medicine and Geriatrics
Medical University of South Carolina
Charleston, SC, USA
Beth B. Fahlberg, PhD, MN, RN
University of Wisconsin
Madison, WI, USA
Christine A. Fortney, PhD, RN
Assistant Professor
The Ohio State University College of Nursing
Martha S. Pitzer Center for Women, Children and Youth
Columbus, OH, USA
Hermien W. Goderie-Plomp, MD, MSc, MSc
Elderly Care and Palliative Care Physician
De Zellingen, Rotterdam, The Netherlands
Lecturer in Palliative Care
Leiden University Medical Center
Leiden, The Netherlands
Elizabeth A. Higgins, MD
Associate Professor of Internal Medicine
Division of Internal Medicine, Palliative Medicine and Geriatrics
Medical University of South Carolina
Charleston, SC, USA
Julie Howard, RRT, TTS, CCM
COPD Case Manager
Adventist Health Rideout
Marysville, CA, USA
Habib A. Khan, MD
Johns Hopkins Medicine
Department of Palliative Medicine
Wayne State University
Baltimore, MD, USA
Ann S. Laramee, MS, ANP-BC, ACNS-BC, CHFN, ACHPN, FHFSA
University of Vermont Medical Center
Burlington, VT, USA
David R. Mehr, MD, MS
Professor Emeritus
Department of Family and Community Medicine
University of Missouri
Columbia, MO, USA
Stefano Nava, MD
Department of Specialistic, Diagnostic and Experimental Medicine (DIMES), Alma Mater Studiorum University of Bologna Bologna, Italy
Carole Parsons, PhD, MPharm, MPSNI
Lecturer in Pharmacy Practice
School of Pharmacy
Queen’s University Belfast Belfast, UK
Lynn F. Reinke, PhD, RN
Claire Dumke Ryberg, RN
Presidential Endowed Chair in End-of-Life/Palliative CareUniversity of Utah College of Nursing
Salt Lake City, UT, USA
Mary M. Roberts, MSN, RN
Department of Respiratory and Sleep Medicine, Westmead Hospital
Ludwig Engel Centre for Respiratory Research, Westmead Institute for Medical Research
The University of Sydney at Westmead Hospital
Westmead, New South Wales, Australia
Steffen Simon, MD
Department of Palliative Medicine
University of Cologne
Faculty of Medicine and University Hospital Cologne, Germany
Tracy A. Smith, MD
Department of Respiratory and Sleep Medicine, Westmead Hospital
The University of Sydney at Westmead Hospital
Westmead, New South Wales, Australia
Jessica L. Spruit, DNP, CPNP-AC
Pediatric Nurse Practitioner
Stepping Stones Pediatric Palliative Care Program
University of Michigan Health System
Ann Arbor, MI, USA
Jodi A. Ulloa, DNP, APRN-CNP, NNP-BC
Assistant Professor of Clinical Practice
The Ohio State University College of Nursing
Martha S. Pitzer Center for Women, Children and Youth
Columbus, OH, USA
Jenny T. van der Steen, MSc, PhD, FGSA
Associate Professor
Leiden University Medical Center, Department of Public Health and Primary Care
Leiden, The Netherlands
Senior Researcher
Radboud University Medical Center, Department of Primary and Community Care
Nijmegen, The Netherlands
Julia Arana West, MD
Fellow, Palliative Medicine
Division of Internal Medicine, Palliative Medicine and Geriatrics
Attending Physician, Department of Emergency Medicine
Medical University of South Carolina
Charleston, SC, USA
Miranda Wilhelm, PharmD
Clinical Associate Professor
Southern Illinois University Edwardsville (SIUE) School of Pharmacy
Edwardsville, IL, USA
Jennifer Wright, MS, CPNP
Stepping Stones Pediatric Palliative Care
Michigan Medicine
Ann Arbor, MI, USA
Introduction
Margaret L. Campbell
In this volume, nearly all the chapters relate to the complex symptom dyspnea across diagnoses, lifespan, and care settings. Other chapters relate to oral and pharyngeal secretions. These topics are addressed from a palliative care context.
Dyspnea, also known as breathlessness, has been defined as a person’s awareness of uncomfortable or distressing breathing. As this can only be known by the person, the term “respiratory distress” is used as the observed corollary relying on patient signs when the person is unable to report dyspnea, such as infants, young children, and adults with cognitive impairments, which may be acute or chronic.
Dyspnea develops when inspiratory effort, hypoxemia, and/or hypercarbia develops, which activates three redundant brain areas. In the cerebral cortex, the dyspneic person has an awareness of the change in breathing efficiency. The amygdala in the subcortical temporal lobe is activated when there is a threat to survival and produces a fear response. The pons in the brainstem reacts by activating compensatory accelerations of heart and respiratory rates and recruiting accessory muscles.
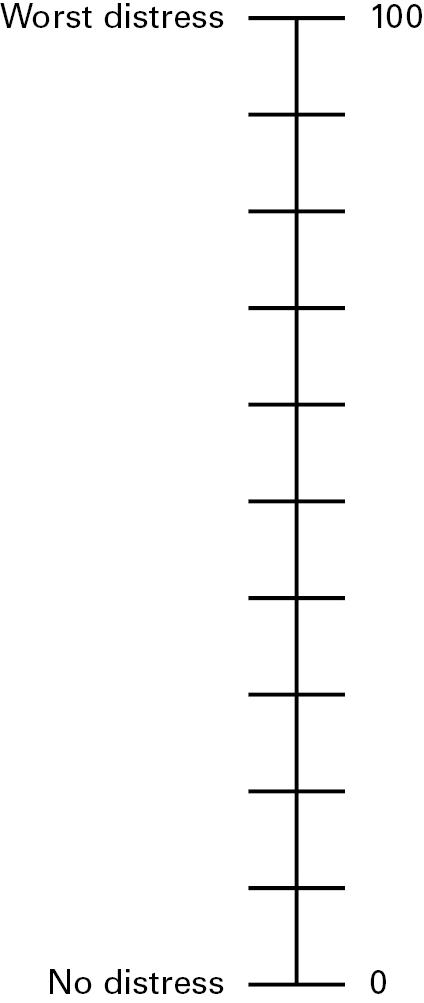
Assessment of dyspnea relies on self-report from as simple as a yes-or-no response to the query “Are you short of breath?” to more complex numeric scales (0–10) or categorical scales (none, mild, moderate, or severe). For patients unable to report dyspnea, observation scales such as the Respiratory Distress Observation
Scale may be used. High-risk patients should be assessed at every clinical encounter.
Dyspnea is one of the most difficult symptoms to experience and is also one of the most difficult to treat, as the evidence base for this symptom lags behind other prevalent symptoms such as pain or nausea, to name two. Dyspnea is prevalent in patients with cardiopulmonary disorders and cancer, and it escalates as death approaches. The development of dyspnea in chronic disease is a predictor of mortality.
Dyspnea may be acute when a reversible etiology presents such as pneumonia, pleural effusion, or ascites. It is chronic in an irreversible condition such as chronic obstructive pulmonary disease (COPD), advanced heart failure, or congenital cardiac conditions. Episodic dyspnea may typify acute exacerbations in chronic conditions such as heart failure.
Treating dyspnea relies on a hierarchy of responses, beginning with treating underlying, reversible conditions such as infections, pleural effusions, volume overload, or ascites. Nonpharmacological treatments include pulmonary rehabilitation, noninvasive ventilation, balancing rest with activity, and optimal positioning. Pharmacological treatments include oxygen, bronchodilators, and opioids. In cases of refractory dyspnea, palliative sedation may be indicated.
Patients receiving invasive mechanical ventilation for respiratory failure may undergo ventilator withdrawal to afford a natural death. These patients are at very high risk for developing respiratory distress, which warrants careful attention to the processes to minimize distress.
Salivary secretions pose a significant problem for patients with bulbar-onset amyotrophic lateral sclerosis characterized by difficulties swallowing. Treatment begins with anticholinergic medications and may include botulinum toxin injections or irradiation of salivary glands.
Pharyngeal secretions, also known as death rattle, develops in about half of dying patients in the last days of life. Controversies about whether medications are indicated or effective make up the
evidence base. Ethical concerns about medicating the patient to assuage the listener have been raised.
The contributors to this volume have addressed all the treatments currently known for dyspnea, respiratory distress, and secretions with a case study approach.
TABLE 1.2. Respiratory Distress Observation Scale
Variable 0 points 1 point 2 points Total
Heart rate per minute <90 beats 90–109 beats ≥110 beats
Respiratory rate per minute ≤18 breaths 19–30 breaths >30 breaths
Restlessness: nonpurposeful movements
Accessory muscle use: rise in clavicle during inspiration
Paradoxical breathing pattern
Grunting at endexpiration: guttural sound
Nasal flaring: involuntary movement of nares
Look of fear
None Occasional, slight movements Frequent movements
None Slight rise Pronounced rise
None
None
Present
Present
None
Present
None
Eyes wide open, facial muscles tense, brow furrowed, mouth open
Source: m.campbell@wayne.edu
SUMMARY
Several unidimensional and multidimensional scales and an observation scale were described as suitable for assessment in patients receiving palliative care. Selection of the optimal tool will
depend on the patient’s cognitive abilities, which are influenced by disease trajectory, fatigue, sedation, mechanical ventilation, and underlying conditions such as dementia.
Stella has a heart rate of 108 and respiratory rate of 22. She has slight restlessness and a slight rise in the clavicle, signifying accessory muscle use. There is no apparent paradoxical breathing, nor grunting, nor nasal flaring or a fearful facial expression. Thus, her RDOS score is 4, signifying moderate distress. The nurses elevated the head of her bed, placed a fan blowing on her cheek, and began immediate-release morphine elixir at 5 mg every 4 hours.
Subsequent RDOS scores decreased to 2 or 3 with this regimen.
KEY POINTS TO REMEMBER
Assessment is critical to optimizing treatment. Patient abilities will inform selection of an assessment tool or scale. Self-reported dyspnea presence and intensity is the gold standard. Respiratory distress signs are indicated for those who cannot report their experience.
References
1. Gift A. Validation of a vertical visual analogue scale as a measure of clinical dyspnea. RehabNurs. 1989;14:323–325.
2. Yorke J, Moosavi SH, Shuldham C, Jones PW. Quantification of dyspnoea using descriptors: development and initial testing of the Dyspnoea-12. Thorax. 2010;65(1):21–26.
3. Banzett RB, O’Donnell CR, Guilfoyle TE, et al. Multidimensional Dyspnea Profile: an instrument for clinical and laboratory research. Eur Respir J. 2015;45(6):1681–1691.
4. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93(3):580–586.
5. Campbell ML, Templin T, Walch J. A Respiratory Distress Observation Scale for patients unable to self-report dyspnea. J Palliat Med. 2010;13(3):285–290.
6. Campbell ML. Psychometric testing of a respiratory distress observation scale. JPalliat Med. 2008;11(1):44–50.
7. Campbell ML, Kero KK, Templin TN. Mild, moderate, and severe intensity cutpoints for the Respiratory Distress Observation Scale. Heart Lung. 2017;46(1):14–17.