I had seen Ms. Johnson before for a visit or two, though it had been several years. In the years since, she had apparently come to the clinic numerous times for a variety of problems, but always just to see her primary care physician. Today she was returning to me, at the urging of the physician, after just completing a visit with him. Stress was affecting how she was managing her diabetes; she had gained some weight and was depressed. She started our visit by apologizing for not having returned sooner to see me, stating she had often considered it, but never followed through. I reassured her that this happens for many people, and the important thing was that she was here now. We made our way through the visit, catching up on her life and devising a plan for improving her current situation. At the end of this seemingly routine visit, she suddenly broke into tears. “I just want to tell you,” she said, “that I appreciate you being here.” She continued, “Even though I haven’t had a visit with you in many years, I’ve been practicing what we talked about before and it has helped me. When I come in here, I often see you around. It always reminds me of what we talked about and makes me feel so comfortable here. I just want you to know you are making a difference.”
In that simple human interaction, Ms. Johnson managed to capture so much of what this book is about. This book is about making a difference. We can talk about policy, models, cost-offsets, core competencies, quality outcomes, and all the rest, but in the end our goal is to improve people’s lives. And the potential for that to happen in primary care is enormous, if we do it right.
Since the first edition of this book was published in 2007, a lot has changed in the primary care behavioral health integration landscape. Integration has spread, and so has the model described in this book. Whereas the notion of a behavioral health provider seeing a patient for 20 or 30 minutes (or less) was often greeted with a fair dose of skepticism (or even hostility) in 2007, today it is common within integrated practices. Thousands of clinicians around the country now refer to themselves as “behavioral health consultants,” a title that in earlier years was greeted mostly with quizzical looks. Integration is happening, it is happening quickly, and it is moving inexorably toward the model outlined here.
The Primary Care Behavioral Health (PCBH) model has received most of its support from grassroots efforts. This is a model developed by and for clinicians. At the frontlines of the nation’s healthcare system, the clinicians in primary care understand what the system needs, and they also understand what it doesn’t need. It was their collective wisdom that created this model, and the same collective wisdom has continued to refine it. Thus, while outcome studies of this model have been done, this is not what drives its success. While the billing and financial climate for PCBH has improved, no organization has adopted this model to get rich. The model has spread because it makes a difference. It makes a difference for primary care providers, who are the true heroes of the healthcare system, and it makes a difference for patients, who so desperately need something better.
The PCBH model has evolved some over the years. We have learned how to do even more with even less time. We have discovered new ways that a behavioral health provider may contribute to the primary care team. We have refined what it means to practice this model, and how to spread it throughout organizations large and small. And the language of PCBH, with terms like warm-handoffs, consultants, pathways, and others, has been clarified and more standardized.
As the model has evolved, so have the two of us authors. Both of us have enjoyed diversifying our professional lives, through involvement in a variety of new activities. We both work at the “macro-level” world of policy, training, consulting, writing, and speaking, yet we still enjoy the “micro-level” world of direct patient care. One of us (PR) has focused her work on the macro-level, helping large healthcare organizations to build a workforce for the delivery of PCBH care. The other (JR) has focused more on the micro-level, refining the delivery of the PCBH model in the same community health organization where he runs the integrated care service and still sees patients for 70% of his time. For both of us, our work is a real-world “laboratory” for understanding, testing, and improving the PCBH model.
As time has gone by, the need for a revised edition of this book became apparent. As noted above, the PCBH model has been refined, clarified, and applied in a variety of new ways. Outcome studies have been done and the need has emerged to focus more on certain topics and less on others. Primary care itself is also in flux. The content of this book reflects the current state of these changes. To help primary care physicians and nurses learn the PCBH model, we include a new chapter on competencies for them. Additionally, we include an entire chapter devoted to the problem of prescription drug abuse in primary care. We also detail new developments in primary care, such as the Patient Centered Medical Home. We have refined the tools used for training behavioral health consultants and offer a number of new practice support tools as well. We also present new strategies for making the PCBH model even more of an influence on the efficiency and effectiveness of primary care, and we update the literature on many different topics. In short, there is a lot of new material in this book; more than we imagined there would be when we began. Throughout the book, we reference resources available on the book website, and the URL for the book website is www.behavioralconsultationandprimarycare.com.
As was the case with the first edition of this book, we have many people to thank for helping with this one. Many colleagues reviewed parts of this book and offered
feedback that was invaluable. This list includes, in no particular order: David Bauman, Psy.D., Bridget Beachy, Psy.D., Chris Krumm, N.D., Kim McDermott, M.D., Melissa Baker, Ph.D., Kirk Strosahl, Ph.D., Debra Gould, M.D., and Joanna Robinson, B.A. Sharon Panulla at Springer has believed in us since the 2005 lunchtime meeting where we first pitched the book proposal, and her continued support has helped us publish this book as well. We also thank all of the pioneers and innovators who have taken the first edition of this book and run with it. There are too many of you to mention, but your comments, feedback, ideas, and support for the model over the years have all influenced the writing of this book. This model and this book are truly built on the shoulders of giants.
I (JR) wish to thank the many friends and family who brought me lunch, texted words of encouragement, and just generally tolerated my inaccessibility while hunkered down over the keyboard. I also wish to thank my colleagues at HealthPoint, which simply must be the best community health organization ever. From the executive team to the primary care providers to the behavioral health team to the frontline staff, my colleagues never cease to amaze me with their passion, kindness, and skills. What I have gained professionally, and personally, from working with these people simply cannot be measured. I also wish to thank Ms. Johnson and the thousands of patients like her, whom I have seen over the years at HealthPoint. Thank you for humbling and amazing me everyday by your resilience, and for all that you have taught me about courage and acceptance. This book is for you.
I (PR) wish to thank Jeff for saying, “Yes,” to my request to write a second edition of this book and for the countless hours of discussion, writing, and editing that went into completing this work. I can truly say that I’ve learned a lot from Jeff in writing the second edition and I have become a better consultant and trainer. I also want to thank two people who supported this work in a very fundamental way: Joanna Robinson, BA, an amazing editor who brings a sense of wonder and extraordinary attention to detail to her work, and Pamela Rieger, a loving sister who was a daily cheerleader for me. I also want to thank the brilliant and caring people I have worked with in the United States Air Force, the San Francisco Department of Public Health, the Calgary Health District, the University of Texas San Antonio Health Sciences Department, Psychology Partners in Sweden, the Oregon Patient Centered Primary Care Institute, the Saint Louis County Department of Health, the Louisiana Public Health Institute, the University of Arkansas Medical Science Clinics, Trillium Coordinated Care Organization, Multnomah County Public Health Department, Community Health of Central Washington (my home clinic), and other Federally Qualified Health Centers and Family Medicine residency training programs with whom I’ve worked large and small. Watching you help others and seeing your willingness to experiment and evaluate how you do that is my inspiration. This book is for you.
Patricia J. Robinson Portland, OR Jeffrey T. Reiter Seattle, WA
In this 2nd edition, Robinson and Reiter give us an updated blueprint for full integration of behavioral health and primary care in practice. They review the compelling rationale, but their real contribution is telling us exactly HOW to think about it and how to do it. This latest book is a must for anyone interested in population health and the nuts and bolts of full integration through using the Primary Care Behavioral Health consultation model.
Susan H
McDaniel
Ph.D.
2016 President, American Psychological Association (APA) Dr Laurie Sands Distinguished Professor of Families and Health Associate Chair, Department of Family Medicine Director, Institute for the Family, Department of Psychiatry University of Rochester Medical Center
We highly recommend this book as a resource for clinicians, educators, and administrators involved in advancing integration at the practice level. Robinson and Reiter go well beyond the basic rationale and foundational concepts of integration of behavioral health and primary care; they provide practical tips and strategies, honed from decades of experience in the field, for implementation of the PCBH model in an easy-to-use format. Packed with practice support tools, updated clinical protocols, and current literature reviews, this second edition of Behavioral Consultation and Primary Care is an excellent resource for healthcare professionals committed to strengthening primary care.
Dennis Freeman, Ph.D. CEO, Cherokee Health Systems
Parinda Khatri, Ph.D. Chief Clinical Officer, Cherokee Health Systems
The 2007 edition of Behavioral Consultation and Primary Care, A Guide to Integrating Services has been a must-read for anyone interested in implementing Primary Care Behavioral Health. The second edition will have an even wider impact in today’s healthcare environment when the spread of integrated care is gaining momentum by the moment. The updated volume has new content and benefits from seven additional years of practice experience, emerging research, and new opportunities (or imperatives) created by healthcare reform. What is not new is the approach that we have come to expect from these authors—one that is entirely accessible, practical, and immediately applicable.
Natalie Levkovich, CEO
Health
Federation
of Philadelphia
2015 President-Elect, Collaborative Family Healthcare Association (CFHA)
As we planned integration for Healthcare for the Homeless—Houston FQHC, we identified the most compelling resource available, Behavioral Consultation and Primary Care: A Guide to Integrating Services. With the model described in this book, we were able to transform our system quickly in uncharted waters, with immediate gains in capacity and willingness to address complex behavioral health issues among our primary care providers. Perhaps most significantly, using the model in this book we are seeing enhanced capacity to address the behavioral health needs inherent to all patients. The ability of this model to help us adapt our complex setting of homelessness and comorbid health problems, including severe mental illness, means this book is an indispensable resource for primary care.
David S. Buck, M.D., MPH Winner,
2013 AAFP Public
Health Award
Founder, Healthcare for the Homeless—Houston
Robinson and Reiter have done it again! They characteristically produced another seminal book on integrated care—filled with theory, evidence, expert opinion, and practical resources for novice to proficient behavioral health clinicians working in primary care. There is something for everyone! This book will be equally valuable for administrators, practice managers, support staff, and primary care providers who want to better understand the rationale, challenges, and opportunities of integrated primary care. Their passion for this work and the patients they have cared for leaps off the pages, while the foundational elements and evidence are eloquently and expertly weaved throughout the book. From beginning to end, this rich, well-written, cogently organized academic resource reads like the kind of story you have to know and share with others.
Tina Runyan, Ph.D., ABPP Clinical Associate Professor University of Massachusetts Medical School Dept of Family Medicine and Community Health
These two nationally recognized behavioral health consultants offer the Primary Care Behavioral Health model of service delivery as a framework that any primary care team can use to effectively integrate behavioral health services into practice. Combining their vast experience with the latest science, they have created practical service delivery support tools and detailed guidance on improving team-based competencies that produce effective outcomes. Behavioral Consultation and Primary Care is a “have-to-have” text for any graduate or medical school student and a necessary desktop reference for primary care providers, administrators, nurses, and behavioral health consultants looking to achieve the Triple Aim of simultaneously enhancing the experience and outcomes of the patient, reducing per capita cost of care, and improving the health of the population they serve.
Christopher
L. Hunter, Ph.D., ABPP
Lead author of Integrated Behavioral Health in Primary Care: Step-By-Step Guidance for Assessment and Intervention
Like many behavioral health professionals in primary care, I often went back and forth among the many available book and resource options to find what I needed for practice or programs. When the first edition of this book came out, however, I found that it was a priceless foundation and a “go-to” resource for the beginner or seasoned veteran. In this 2nd edition, Drs. Robinson and Reiter have found a way to extend beyond their first offering to provide us with an engaging presentation of all of the resources a behavioral health consultant, program developer, or trainer needs AND with the essential human side seamlessly woven throughout. You will enjoy hours in one sitting or use as an easy quick reference with this very readable and informative primary care compendium. Bravo!
Abbie O. Beacham, Ph.D. Associate Professor PsyD Program—Director of Clinical Training School of Psychology, Xavier University
“Integrated Behavioral Health is not a fad or buzzword that will fade. It is a crucial, evidence-based tool of practice transformation in primary care. How do you get there from where you are, especially when the workforce is not equipped for this role? The authors’ previous works and tools have been essential to the implementation of the model, and to sustaining it with fidelity. This second edition of Behavioral Consultation and Primary Care builds upon their prior work and will serve as an invaluable tool to all who aspire to this important change.
Mike Maples, M.D., CEO Community Health of Central Washington, Yakima, WA
This text is a quintessential component of our training program for both new and established Behavioral Health Consultants. In an era where Patient Centered Medical Homes are standard practice, Patti and Jeff not only do a fantastic job of covering the rationale for integrated behavioral health, but they also deliver on practice tools that are easy to grasp and apply to daily practice. The core competencies in this version have been incorporated seamlessly into our workflows and have provided increased structure and uniformity in our program. Whether you are just beginning your integration efforts or have a well-established Primary Care Behavioral Health program, this book is an invaluable resource that will guide your program toward excellence on many levels.
Brian E. Sandoval, Psy.D. Program Manager, Primary Care Behavioral Health Yakima Valley Farm Workers Clinic
When the first edition of Behavioral Consultation and Primary Care was published, the idea of primary care behavioral health was largely ignored, marginalized, or even ridiculed. My, how times have changed. Integrated behavioral health is now the hot topic in healthcare reform, and suddenly new “experts” are jumping on the bandwagon. What a welcome relief to have two maestros update their classic with a practical, how-to guide for the Behavioral Health Consultant in primary care. This new edition is completely updated with clear guidelines, practice tools, and a precise roadmap for transforming primary care. Primary care behavioral health is not for the weak of heart, tradition-bound, or chaos adverse clinician. However, for those ready to take the plunge into the future of behavioral health, this book will prove invaluable.
Ronald R. O’Donnell, Ph.D., Clinical Professor Arizona State University, College of Health Solutions Doctor of Behavioral Health
Whether you are reading Robinson and Reiter’s book for a general understanding of PCBH or for the implementation of the PCBH model in a primary care clinic, this is a must-read. This book presents a practical, evidence-based approach to integrating behavioral health into a primary care setting. The material presented offers a structured approach and speaks to all levels of readers, with information for the advanced BHC or the beginner BHC.
Michael D. Fitts, Psy.D. University of Arkansas Medical Systems Regional Programs Instructor
If you want to improve health care, start in primary care and start with this book. In this second edition, Robinson and Reiter provide up-to-date evidence and practical guidance for implementing the Primary Care Behavioral Health model, an optimal method for integrating behavioral health into medical homes. Resources include core competency tools that promote model fidelity, clinical practice support materials, and guidance for difficult problems, such as the prescription drug abuse epidemic—a great resource for practicing providers, administrators, and graduate students.
Maria X Martinez Deputy Director of Community Programs
San Francisco Department of Public Health
Drs. Robinson and Reiter are genuine authorities in the area of integrated primary care practice. I am thrilled with their Second Edition, which incorporates the very latest innovations and research findings in this rapidly evolving field. It is at once comprehensive and pragmatic. I believe it will serve a wide range of audiences— medical providers, behavioral health consultants, and administrators. It will most certainly be assigned as the primary required text for our doctoral students in clinical psychology.
Jodi Polaha, Ph.D. Associate Professor
Department of Psychology East Tennessee State University
This is the “go-to” for “how-to” for developing a fully integrated primary care behavioral health (PCBH) service in your clinical setting. Excellent resource based on the authors’ many years of experience in PCBH design and implementation. Since their 2007 edition, the authors have updated the content in addressing real-life micro- and macro-system issues in delivering PCBH services. I especially liked the attention to training medical clinicians and other staff to maximize services, as it is a paradigm shift for all of us!”
Debra A. Gould MD, MPH
Associate Clinical Professor, University of Washington Central Washington Family Medicine Residency Program Yakima, WA
List of Figures
Example of poster announcing BHC
10.3 GATHER: An example of a BHC educational handout
10.4 Educational handout providing information on connecting patients with the BHC .................................................
10.5 Example of a BHC shadowing note
10.6 Example of a PCP/RN survey concerning patients PCPs/RNs would like BHCs to see
10.7 Example of a BHC “Request of the Week” communication to PCPs and RNs .................................................................................
10.8 Example of an educational handout for BHCs to use to teach PCPs and RNs strategies for talking with the patient about BHC services.............................................................................
10.9 An example of an educational handout to encourage PCPs and RNs to refer a broad range of patients to the BHC
10.12 Example of a relapse prevention plan that BHCs can use as an educational tool for PCPs and RNs and an intervention for
List of Abbreviations
ARNP Nurse Practitioner
BH Behavioral Health
BHA Behavioral Health Assistant
BHC Behavioral Health Consultant
EHR Electronic Health Record
ER Emergency Room
LPN Licensed Practical Nurse
MA Medical Assistant
MH Mental Health
NA Nursing Assistant
PA Physician Assistant
PC Primary Care
PCBH Primary Care Behavioral Health (model)
PCMH Patient Centered Medical Home
PCP Primary Care Provider
RN Registered Nurse
The Perfect Storm of Primary Care
The forces pressuring primary care and behavioral health services are like a series of interconnected weather conditions transforming the landscape of healthcare service delivery. Escalating rates of physical and mental health problems nationwide are combining with high healthcare costs to create a vortex of problems. Lifestyle and behavior issues are at the heart of the vortex, playing a major role in the escalation of health problems. Yet, while the influence of the pharmaceutical industry has grown, attention to basic behavior change approaches has strayed. Our shelter, the mental health system, is collapsing, leaving many patients out in the cold and forcing many others into primary care for help. They join the growing ranks of patients seeking help in primary care for chronic medical problems, most of which have a significant behavioral component. As more people live with poor health, primary care providers are pressured to work faster and harder, and, not surprisingly, patient–provider relationships have suffered. In addition, provider job satisfaction has declined and burnout has become a common concern. The shortage of physicians trained to provide primary care services is growing at a time when more and more patients are able to access healthcare services. Patients have become frustrated as they wrestle with the behavioral challenges of managing chronic diseases while fighting for access to healthcare providers. We are no doubt in the midst of a violent storm and its epicenter is in primary care. However, there are emerging strategies for getting through it. Continued evolution, expansion, and evaluation of primary care behavioral health services that align with the Patient Centered Medical Home model will help see us through. In Part I of this book, we provide an overview of the Primary Care Behavioral Health (PCBH) model as a foundation for this effort. We also introduce the reader to the structure, players, and milieu of the primary care world. Finally, we describe a new role for behavioral health providers in primary care—the role of behavioral consultation—that we believe holds particular promise for decades to come.
Chapter 1
Behavioral Consultation and Primary Care: The “Why Now?” and “How?”
“There are those who look at things the way they are, and ask why. . .I dream of things that never were and ask why not.”
Robert Kennedy
Before beginning our careers in primary care (PC), both of us authors worked in traditional specialty mental health (MH) settings. Like most MH providers, we worked hard, kept up on clinical innovations and had the best interests of our clients at heart. Of course we had clients who progressed and many who appreciated our assistance. However, we could not help but wonder what happened to clients who failed to show. On a typical day, we might have seven clients scheduled, of which two or three would not show. What happened to them? Why didn’t our follow-ups return? If first time clients failed to show, we rationalized that the client was not ready for change; but was that really the case? Further, we felt frustrated that, by the end of the day, we might have only seen a handful of clients, many of whom were weekly regulars. This begged the question: How many people were we really helping?
As we have since learned, our experiences and questions were not unique. Further, we have learned that our PC colleagues also had some nagging questions: Why do so few patients referred to MH care follow through on the referral? Why are so many “psych patients” coming here when a system already exists to tend to their needs? How can we get patients with chronic conditions like diabetes to manage their condition better? How can a primary care provider (PCP) be expected to meet the needs of every patient with a 15-minute visit?
What we have learned is that the MH system in this country simply does not meet the needs of the population, and the PC system has been left to pick up the slack. Unfortunately, though, PC historically has not been the best place for treating
Electronic supplementary material: The online version of this chapter (doi:10.1007/978-3319-13954-8_1) contains supplementary material, which is available to authorized users.
P. Robinson, J. Reiter, Behavioral Consultation and Primary Care, DOI 10.1007/978-3-319-13954-8_1
behavioral issues. Overwhelmed by the demand for care, underprepared for many of the problems seen, and often unable to access timely specialty help, PC is a busy and stressed system. All of this has led to the question: Is there a better way?
This book aims to help provide a better way. The chapters that follow are a guide for reinventing PC, by improving the quality and accessibility of care for patients whose health is compromised by behavioral issues. We hope to reshape ideas about how to help patients change problem behaviors by restructuring the way that care services are delivered. The Primary Care Behavioral Health (PCBH) model, as outlined here, provides a framework for integrating MH providers into PC settings. It changes how MH providers practice in that setting, how PCPs practice, and how they work together for the health of the population. As noted by Strosahl (1998), an early developer and proponent of PCBH care, this model is best considered a form of health care rather than mental health care.
The general rationale for integrating PC and MH has been discussed thoroughly in other texts (e.g., Belar & Deardorff, 2009; Blount, 1998; DiTomasso, Golden & Morris, 2009; Frank, McDaniel, Bray & Heldring, 2004; James & Folen, 2005; James & O’Donohue, 2009; Patterson, Peek, Heinrich, Bischoff & Scherger, 2002). Rather than rehashing those writings, this book will focus on how to implement, evaluate, and sustain integration. Specifically, this book explains how to integrate using the PCBH model. This is first and foremost a pragmatic book. We begin by outlining the problems that our healthcare system faces in both the PC and specialty care sectors. Understanding the problems with the current system is essential when considering the importance of taking a fundamentally different approach. One by one, these problems help us not only understand the need for integration but also the need for the particular type of integration the PCBH model provides. We then introduce the PCBH model.
Primary Care and the Epidemic of Behavioral Health Problems
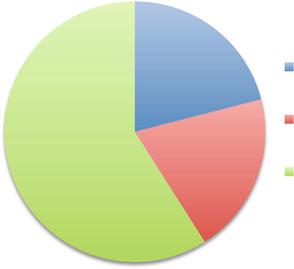
At the time of this writing, the population of the United States is 313.9 million. Remarkably, around 30% of these Americans have a diagnosable psychiatric disorder at a given point in time (Kessler, Berglund, et al., 2005). Around 50% will experience a diagnosable disorder at some point in life (Kessler, Demler, et al., 2005). Reflect for a moment on this point—That is a lot of people! So what happens to all of these people? Figure 1.1 offers some clues.
As shown in Figure 1.1, only about 20% of those with a diagnosable problem receive care from a specialty MH or substance abuse clinic, while 21% are treated in PC. The majority, around 59%, receive no care at all (Wang et al., 2005). These basic statistics upend the notion many have about where and how MH problems are treated in this country. Most people with problems seek no care, and many who do seek care simply go to the family doctor; few will ever see a therapist’s couch. Primary care providers see the full spectrum of psychiatric disorders, from depression to substance abuse to psychosis. They prescribe around 60% of psychotropic medications (Mark, Levit & Buck, 2009; Mojtabai, 2008). They regularly handle chronic psychiatric problems as well as acute flare-ups (e.g., a suicidal 1 The “Why Now?” and “How?”
Distribution of Mental Health, Substance Abuse and Primary Care in the U.S.
Primary
Care
Specialty MH/Substance Abuse Care
No Care
patient). Because they provide care across the life span, PCPs also treat child behavior problems (e.g., ADHD) in addition to the problems of adults and older adults. Of course, they must do all of this while also tending to the medical needs of their patients. A PCP must truly be a generalist! For all of these reasons, PC has earned the label of the country’s “de facto mental healthcare system” (Regier et al., 1993).
Thus, one reason to integrate MH services into PC is to help meet the demand for care there. Another reason lies with the 59% of people who seek no care. An interesting point is that approximately 80% of adult Americans will visit PC in the course of a year (National Center for Health Statistics 2012b). Among American children, the number is about 93% (National Center for Health Statistics 2012c). Thus, many if not most of these undiagnosed people will most certainly enter the PC system. They might only seek help for a sore throat or a work physical, rather than for psychiatric or substance abuse problems. However, the point is that they do enter PC.
Most of the time, these patients pass in and out of the clinic without the psychiatric problem being detected. For example, patients with alcohol dependence receive appropriate assessment and referral in PC only about 10% of the time (McGlynn et al., 2003), and depression goes undetected 30–50% of the time (Simon, Von Korff & Barlow, 1995). However, a PC clinic with good screening protocols, behaviorally savvy clinicians, and a robust behavioral health staff might be able to detect and treat problems that may otherwise go unnoticed. Thus, a second reason to integrate is to increase a clinic’s ability to identify and provide MH care to patients who would otherwise slip through the cracks of a broken system.
Takeaway: Integration must improve identification of undiagnosed problems.
Figure 1.1 Distribution of mental health and substance abuse care in the United States
Yet, improving care for psychiatric problems is not the only reason to integrate a clinic. Behavior interferes with health in many ways, and the consequences show up in PC patients in many ways. To illustrate this, we often have new behavioral health consultants (BHC; we explain this term later in the chapter) trainees review the daily patient schedule of a PCP, with the goal of finding possible behavioral components to the problems patients are presenting with that day. For example, the patient seeing the PCP for headaches might be stressed or skipping meals; the patient presenting with stomach pain might be drinking alcohol to excess; the patient complaining of dizziness might be having panic attacks. There is even a behavioral component to the common cold, in that frequent hand washing helps prevent it! The point is that health and behavior are so intertwined that it can be difficult to find any medical problem that does not involve behavior in some way. A behavioral influence is most notable in four types of patient concerns: (1) lifestyle-based somatic complaints, (2) subthreshold syndromes, (3) preventive care, and (4) chronic disease management. We describe these concerns in detail below.
Irritable bowel syndrome, tension headaches, insomnia, and chronic pain are a few examples of lifestyle-based somatic complaints. In a classic study of these complaints, researchers demonstrated that, of the 14 most common complaints in a PC clinic, 84% had no clear organic etiology over a 3-year follow-up period (Kroenke & Mangelsdorff, 1989). In other words, these symptoms were likely the result of stress and/or lifestyle. Because these conditions are experienced as physical symptoms, patients often view them as medical problems and thus seek help from a PCP rather than a MH provider (Bray et al., 2004; Patterson et al., 2002). Obesity is another lifestyle-based somatic issue that PCPs confront almost hourly. On rare occasions, patients seek help specifically for obesity, but much of the time it is a problem that never even gets discussed (Greiner, Born, Hall, Hou & Kimminau, 2008).
The second category of subthreshold syndromes includes marital conflict, domestic violence, bereavement, and other life stressors. These are problems that do not meet the “threshold” of a DSM diagnosis, but are nonetheless problems that may take a significant expenditure of PCP time and energy. For example, conservative estimates indicate 12–23% of patients in family medicine have experienced intimate partner violence in the last year (Cronholm, Fogarty, Ambuel & Harrison, 2011), and such patients utilize 1.3–2.6 times as much health care (Ulrich et al., 2003).
Preventive care is another area where PCPs spend a lot of time and energy, and mostly this involves counseling patients on healthy behavior change. Risk factors for heart disease, cancer, stroke, diabetes, and respiratory diseases go far beyond genetics and social inequalities. To prevent these problems, patients must modify tobacco use, unhealthy diets, sedentary lifestyles, and problematic alcohol and drug use, and PCPs help them with this. They also teach patients to use seat belts, bike helmets, and contraceptives and help them avoid high-risk sexual behavior. Most MH providers in a traditional MH setting would be surprised and perplexed if asked to help a client with one of these behavioral issues. However, PCPs counsel patients regarding these issues every day.
Behavioral issues also arise in patients with chronic diseases, the major causes of morbidity and mortality in the world in both developed and developing countries 1 The “Why Now?” and “How?”
Primary Care and the Epidemic of
(Heron, 2010). Primary care systems have historically focused mostly on treating acute problems, but chronic conditions are the fastest growing part of PC (Patterson et al., 2002). More than 75% of healthcare costs are now attributable to chronic conditions (see Web Link 1). This rise is due to several factors, including an aging population; an increase in conditions such as diabetes, lipid disorders, and obesity; and medical advances that allow people to live longer with diseases that would have been fatal in earlier years. The trend toward more chronic disease means that PCPs must more often help patients learn to manage them. They must counsel patients on how to cope with a chronic condition, educate family members, motivate patients to make changes, and teach them skills for managing it. Unfortunately, estimates suggest that up to 60% of patients with chronic disorders adhere poorly to treatment (Dunbar-Jacob & Mortimer-Stephens, 2001).
Takeaway: Integration must help with ALL behaviorally influenced conditions.
The challenge of responding to all of these behavioral issues in PC may be reason enough to integrate services. Yet, there is another reason why integration is so crucial: PCPs simply cannot do it alone. Primary care is a very busy place and a very stressed system.
Primary Care: Overworked and Underpaid
Imagine you are a PCP seeing a patient who is brand new to your clinic. The patient reports having diabetes, hypertension, high cholesterol, depression, sleep apnea, and chronic pain. The patient also tells you he has been off all of his medications for a few months and can’t recall the names of most nor the dosages. He is coming in now because he has not been feeling “right” and thinks his blood sugar is “off.” You call an endocrinologist the patient recently saw (the patient recalled the name, but you had to find the phone number), but after 20 minutes, the endocrinologist still has not called you back. You were 45 minutes behind at the start of the visit and need to see four more patients in the next hour before lunchtime. If this scenario sounds unrealistic, it is not; if it sounds unworkable, it very nearly is. The reality is that scenarios like this play out every day on the schedule of most any PCP. The typical PCP sees 20–25 patients in a day, many with complex problems. The average length of a PCP visit is 16–18 minutes, during which time the average patient will bring up three health concerns (more than three concerns in 37% of visits; Beasley et al., 2004; Mechanic, McAlpine & Rosenthal, 2001). Obviously, this means PCPs have little time to treat behavioral and medical issues that may be complex. In addition to patient visits, a recent study in The New England Journal of Medicine documented that in a typical day, a PCP has over 36 urgent but unpaid
1 The “Why Now?” and “How?”
tasks to tend to. Such tasks include reviewing labs, refilling medications, returning phone calls to patients or other providers, reading consult reports, and many others (Baron, 2010). Similarly, a PCP would need 7.3 hours per day, in addition to patient visits, to implement all of the preventive screening and counseling that is recommended (Yarnall et al., 2003), as well as ten additional hours a day to implement all of the clinical guidelines for chronic problems like diabetes (Yarnall et al., 2005). Primary care is a very busy place, and all too often there is little time for anything but acute concerns.
The entire PC team often experiences the same high stress level of the PCP. Medical assistants (MAs), RNs, and lab technicians also operate under a time crunch and are likely no more prepared to deal with behavioral problems than PCPs. In some cases, they bear the brunt of complaints from disgruntled patients who may be reluctant to complain to the PCP. Similarly, receptionists and other administrative staff must often interact with psychotic, depressed, or otherwise challenging patients, and referral coordinators must try, often in vain, to locate accessible specialty services. When training a new BHC, we often have her spend 30 minutes in the waiting room of the clinic, observing the patients and patient interactions with staff. Almost inevitably, there will be a disagreement over a bill, frustration with a lengthy wait, and questions beyond the realm of what front desk staff are able to answer. Observing the waiting room can provide valuable insight into the challenges faced by staff, all of which place additional strain on a PC system that is already taking on more than it can handle.
If patients with complicated problems reliably accessed the specialty care system, perhaps the situation would be improved. PC is supposed to be the entry point for treatment of any nonurgent problem, with the specialty care system standing by to accept those who fail to improve in PC. This is the case for all manner of health issues, including MH problems. Unfortunately, PCPs in the United States report being “unable” to access specialty MH services for two-thirds of their patients (Cunningham, 2009)! Thus, in the majority of cases where PCPs need specialty help, they simply cannot get it.
Adding insult to injury, PCPs have also not been compensated as well as their specialist colleagues. They are consistently the lowest paid of all physicians. In 2012, the median salary for a PCP was $220,000, whereas the median for the other physician specialties was $396,000 (Bureau of Labor Statistics & U.S. Department of Labor, 2014). In comparison to their peers, PCPs are a classic example of “overworked and underpaid.” Perhaps not surprisingly, all of this has resulted in a shortage of PCPs nationwide. Medical students have been shunning PC, and seasoned PCPs are retraining or retiring early. Healthcare reform, with its emphasis on strengthening PC, may help PCP salaries some. However, it is also expected to bring about 30 million newly insured people into the already stressed PC system.
The important point from this discussion is that any attempt at integration must aim to reduce the burden on the PC system. Integration efforts that add more work to the overflowing plates of PCPs and other team members are doomed to fail. Behavioral health providers who practice in PC without understanding the system’s stresses, or who choose to ignore them, risk being viewed as irrelevant at best
and a nuisance at worst. Integration must help not only patients but also the PC system to function better.
Takeaway: Integration must subtract from, not add to, the workload of PCPs.
In addition to a lack of time, PCPs also report feeling underprepared for managing many behaviorally influenced problems. In a typical 3-year family medicine residency, the “psychiatry” rotation lasts just 1 month (and it is during this month that, as Strosahl (2013) likes to joke, most residents take a vacation). Indeed, many residents assume they will rarely need to manage complex behavioral issues and that they will be able to reliably refer to psychiatrists and psychologists, only to learn after residency that much of what they must help patients with involves behavior.
Not only is the quantity of training insufficient, the quality often is as well. Residency programs are rather notorious for not equipping PCPs with the behavioral tools they really need. In the real world of 15-minute visits, treating patients with multiple behavioral issues can be quite a jolt for new clinicians. Almost every PCP has at some point uttered, “My training never prepared me for this!” While diagnosing and prescribing are often a heavy focus of residency training, much less attention is typically given to teaching basic behavior change strategies, especially strategies for very brief encounters. Surveys of physicians and residents show that only around 25% feel effective when counseling patients on smoking cessation, diet, exercise, and weight management Foster et al., 2003. And while the majority of PCPs say they feel comfortable treating anxiety and depression, many struggle with treating other types of psychiatric and substance abuse issues.
Takeaway: Integration must help PCPs improve behavior change skills.
The Effects on Patients
At the risk of stating the obvious, we must note that patients also suffer under the current system. As indicated earlier, many if not most psychiatric problems go undetected in PC. When one is detected, the treatment is likely to be medication focused, and the outcome is likely to be subpar. This is true not only for psychiatric problems but for a host of behaviorally influenced problems including obesity, diabetes, and other chronic conditions. Numerous studies have shown that care for psychiatric disorders in PC is inadequate. Common problems include poor followup and tracking of care, inappropriate prescribing, over reliance on medica tion