The moral rights of the authors have been asserted
First Edition published in 2010
Second Edition published in 2023
Impression: 1
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by licence or under terms agreed with the appropriate reprographics rights organization. Enquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above
You must not circulate this work in any other form and you must impose this same condition on any acquirer
Every effort has been made to contact copyright holders of material reproduced in this work. We would be pleased to rectify any omissions in subsequent editions of this work should they be drawn to our attention.
Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America
British Library Cataloguing in Publication Data Data available
Library of Congress Control Number: 2022942555
ISBN 978–0–19–879072–3
DOI: 10.1093/med/9780198790723.001.0001
Printed in the UK by Bell & Bain Ltd., Glasgow
Oxford University Press makes no representation, express or implied, that the drug dosages in this book are correct. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulations. The authors and the publishers do not accept responsibility or legal liability for any errors in the text or for the misuse or misapplication of material in this work. Except where otherwise stated, drug dosages and recommendations are for the non-pregnant adult who is not breast-feeding
Links to third party websites are provided by Oxford in good faith and for information only. Oxford disclaims any responsibility for the materials contained in any third party website referenced in this work.
Melissa, Florence, and Freddy Ward. May, Ross, Kyle, Alice, Olivia, and Rachel Irwin.
Preface from first edition
Oral and maxillofacial surgery is the surgical specialty concerned with the diagnosis and treatment of diseases affecting the teeth, mouth, jaws, face, and neck and represents one of the commonest indications for anaesthesia worldwide. The anaesthetic care of oral and maxillofacial patients requires specific knowledge and skills on the part of the anaesthetist. An understanding of the subject matter is fundamental to the safe practice of anaesthesia.
This textbook is intended to go some way to address this need. The anaesthetist can be called upon to provide anaesthesia for patients presenting with impacted or carious teeth, infections of the mucosa and adjacent structures, complex facial injuries, head and neck cancers, salivary gland disease, facial disproportion, temporomandibular joint disorders, cysts, and tumours of the jaws.
Anaesthetists may also be involved in managing patients experiencing chronic and intractable facial pain and provide anaesthesia for multiple trauma involving the face.
Although primarily written for anaesthetists, this textbook will also be of interest to maxillofacial surgeons, anaesthetic practitioners, anaesthetic nurses, and Operating Department Practitioners involved in providing anaesthesia for dental, oral, and max-illofacial surgery. We would also expect the work to be of interest to those anaesthetists currently in training and studying for their professional examinations.
Ian Shaw Chandra Kumar Chris Dodds
Preface
Anaesthesia for oral and maxillofacial surgery encompasses a wide range of procedures, treatments, and interventions for an array of pathologies affecting the teeth, mouth, and jaw. There is frequently overlap with other related surgical specialties such as otorhinolaryngology, neurosurgery, plastic surgery, and reconstructive surgery. Since the publication of the first edition of the Oxford Textbook of Anaesthesia for Oral and Maxillofacial Surgery in 2010, this subspecialty has continued to develop, with procedures and techniques evolving, new guidelines and standards being introduced, and new research evidence becoming available. This second edition has been completely updated by a new group of authors, adding an original, contemporary, and fresh
perspective on existing topics, with the addition of new chapters on human factors in anaesthesia and surgical complications, written from the surgeon’s perspective.
The safe perioperative care of patients undergoing oral and maxillofacial surgery necessitates a comprehensive knowledge and understanding of the specific challenges posed by this cohort, and their underlying pathologies and comorbidities, including a full appreciation of the implications of a ‘shared airway’. This textbook is primarily intended as a reference tool for anaesthetists of all grades, but will also be of interest to maxillofacial surgeons, anaesthetic practitioners, anaesthetic nurses, recovery and intensive care nurses, and operating department practitioners.
Abbreviations xv
Contributors xvii
1. Preoperative assessment 1
Roger H. Y. Ho and David M. H. Lam
Introduction 1
Range of procedures 1
Airway evaluation and planning 1
Pathology-specific considerations 2
Environmental considerations 4
Evaluation of comorbidities 4
Preoperative risk stratification 10
Perioperative management of medications 12
Conclusion 15
2. Difficult airway 19
Craig Lyons and Ellen P. O’Sullivan
Introduction 19
Airway assessment 19
The airway plan 20
Positioning 20
Preoxygenation 20
Neuromuscular blockade 20
Apnoeic oxygenation 21
Bag mask ventilation 21
Supraglottic airway devices 21
Direct laryngoscopy 21
Videolaryngoscopy 22
Awake tracheal intubation 22
Fibreoptic intubation 22
Awake videolaryngoscopy 24
Awake tracheostomy 24
Retrograde intubation 24
Blind nasal intubation 25
Cricothyroidotomy 25
Intubation for maxillomandibular fixation 25
Tracheal extubation 26
Human factors 27
Conclusion 27
3. Surgical airway 29
William P. L. Bradley and Gordon A. Chapman
Introduction 29
Anatomy 29
Elective tracheostomy 30
Percutaneous dilatational tracheostomy 30
Surgical tracheostomy 31
Complications of surgical and percutaneous tracheostomy 33
Submental tracheal intubation 33
Emergency front of neck airway 34
Use of ultrasound 36
Conversion techniques 37
Retrograde intubation 38
Jet oxygenation 39
Conclusion 40
Acknowledgements 40
4. Regional anaesthesia 43
Shona Love and Ian Bailes
Introduction 43
The face 43
Anaesthetizing the face 46
The scalp 47
Anaesthetizing the scalp 47
The nasal cavity 47
Anaesthetizing the nasal cavity 48
The mouth 49
Anaesthetizing the mouth 49
The pharynx 50
Anaesthetizing the pharynx 51
The larynx 51
Anaesthetizing the larynx 52
Awake tracheal intubation 52
Complications of regional anaesthesia 53
Conclusion 54
5. Imaging 57
Indu Mitra
Introduction 57
Imaging modalities 57
Trauma imaging 58
Dentition 59
Craniofacial anatomy 60
Craniofacial fractures 60
Infection 63
Tumours 63
Conclusion 64
6. Sedation 65
James W. D. Mann and Vivian Yuen
Introduction 65
Aims of sedation 65
Advantages of sedation 66
Potential complications of sedation 66
The ideal sedative agent 67
Pharmacology of sedative agents 67
Synergy of agents 70
Conduct of sedation 71
Conduct of surgery 72
Safety and guidelines 72
Preoperative assessment and preparation 73
Monitoring 74
Equipment availability 74
Training and personnel 74
Recovery and discharge 75
Conclusion 75
7. Hypotensive anaesthesia 77
Kimberley Hodge, Patrick A. Ward, and Michael G. Irwin
Introduction 77
Background 77
Physiology 77
Indications 78
Contraindications 78
Conduct of deliberate hypotensive anaesthesia 79
Pharmacological techniques for hypotensive anaesthesia 79
Non-pharmacological techniques to minimize blood loss 82
Conclusion 82
8. Dental anaesthesia 83
Jennifer Gosling and John Myatt
Introduction 83
Background and history 83
Preoperative assessment 84
Consent 84
Anaesthesia 86
Postoperative complications and follow-up 89
Sedation 89
Conclusion 90
9. Aesthetic surgery 93
Corina Lee
Introduction 93
Orofacial aesthetic surgery 93
Preoperative assessment 93
Anaesthesia for orofacial aesthetic procedures 94
Surgical requirements for orofacial aesthetic procedures 96
Postoperative priorities for orofacial aesthetic surgery 97
Considerations for specific orofacial surgical procedures 97
Considerations for non-surgical facial aesthetic procedures 102
Revision surgery 104
Acknowledgements 104
10. Orthognathic surgery 107
Patrick A. Ward and Michael G. Irwin
Introduction 107
Preoperative assessment, preparation, and planning 107
Preoperative consent and premedication 110
Intraoperative management 110
Tracheal extubation and emergence 117
Postoperative management 118
Specific orthognathic procedures 121
Conclusion 121
11. Paediatric surgery 123
Silky Wong and Theresa Wan- Chun Hui
Introduction 123
Preoperative evaluation 123
Premedication 123
Fasting 124
Identification of the difficult airway and its management 124
Induction of anaesthesia 125
Tracheal tube selection 125
Fluid management 126
Analgesia 126
Postoperative nausea and vomiting 126
The compromised airway in the postoperative period 126
Oromaxillofacial procedures 127
Craniofacial procedures 128
Orthognathic procedures 129
Anaesthesia for craniofacial and orthognathic procedures 130
Surgery for trauma 131
Minor oromaxillofacial procedures 131
Conclusion 132
12. Infection 135
Adam R. Duffen and David J. A. Vaughan
Introduction 135
Epidemiology 135
Pathophysiology 135
Microbiology 136
Antimicrobials 137
Antibiotic prophylaxis 138
Clinical assessment 138
Management of the uncomplicated patient 139
Management of the patient with serious complications 139
Tracheal extubation and postoperative management 142
Secondary infections 142
Conclusion 143
13. Trauma 145
Rebecca Thurairatnam and Fauzia Mir
Introduction 145
Epidemiology and aetiology 145
Classification of fractures 145
Associated injuries 147
Emergency airway management 147
Airway guidelines and maxillofacial trauma 149
Anaesthetic management of maxillofacial trauma 150
Conclusion 153
14. Burns and inhalational injury 155
Caroline A. R. Nicholas and Tim N. Vorster
Introduction 155
Epidemiology 155
The emergency department acute major burn admission 155
Resuscitation 156
Secondary survey 157
Inhalation injury 158
Systemic gaseous toxins 158
Thermal injury to the airway 159
Smoke injury to the lungs 160
Chemical burns 161
Other considerations in patients with airway burns 161
Prognosis in the airway burns patient 162
Critical care therapy 162
Immediate major burn debridement 162
General considerations in burns anaesthesia 162
Burns pharmacology 163
Long-term considerations 164
Conclusion 164
15. Malignancy 167
Michelle Gerstman, Orla J. Lacey, and Cyrus Kerawala
Introduction 167
Anatomical distribution of malignancy 167
Risk factors for malignancy 167
Types of surgical procedures 167
Treatment options 167
Anaesthetic assessment 169
Fourth National Audit Project 170
Difficult Airway Society 2015 guidelines 170
Awake airway management techniques 170
Oxygenation techniques 172
Airway devices 173
Anaesthesia and perioperative care 173
Tracheal extubation techniques 174
Range of procedures 175
Conclusion 177
16. Postoperative care and planning 179
Joshua H. Atkins, Christopher H. Rassekh, and Andrew Herlich
Joshua H. Atkins, MD, PhD, CPE Associate Professor of Anesthesiology & Critical Care, Associate Professor of Otorhinolaryngology: Head and Neck Surgery (Secondary), Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA
Ian Bailes, BMBCh MA (Oxon), FRCA Consultant Anaesthetist, Imperial College NHS Trust, London, UK
William P. L. Bradley, MBChB, FANZCA, MAICD Adjunct Clinical Associate Professor, Monash University, TAS & VIC State Airway Lead, Specialist Anaesthetist, Department of Anaesthesia and Perioperative Medicine, The Alfred, Melbourne, Victoria, Australia
Gordon A. Chapman, MBChB, FRCA, FANZCA, MD Consultant Anaesthetist, Royal Perth Hospital, Perth, Western Australia, Clinical Senior Lecturer, University of Western Australia, Australia
Chi Wai Cheung, MBBS (HK), MD (HKU), FHKCA, FHKAM (Anaesthesiology), FHKCA (Pain Med), Dip Pain Mgt (HKCA) Clinical Professor, Department of Anaesthesiology, University of Hong Kong; Honorary Consultant, Department of Anaesthesiology, Queen Mary Hospital and Grantham Hospital and Duchess of Kent Children’s Hospital, Chair of Specialty for Anaesthesiology and Adult Intensive Care Services Gleneagles Hospital, Chief of Service Department of Anaesthesiology HKU-Shenzhen Hospital, Hong Kong
Justin P. Curtin, FRACDS (OMS), FRCSEd Associate Professor in Oral and Maxillofacial Surgery, College of Medicine and Dentistry, James Cook University, Australia
Adam R. Duffen, MBBS, BSc, FRCA Consultant Anaesthetist, University Hospitals Bristol and Weston, UK
Michelle Gerstman, MBBS, FANZCA, MD Consultant Anaesthetist, Peter MacCallum Cancer Centre, Melbourne, Australia
Jennifer Gosling, MBBS, BSc, MA, FRCA, FFICM Senior Registrar in Anaesthesia, St. Mary’s Hospital Department of Anaesthesia, Imperial College Healthcare NHS Trust, London, UK
Andrew Herlich, DMD, MD, FAAP, FASA, FAAOMS (H) Professor Emeritus, Department of Anaesthesiology and Perioperative Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA
Roger H. Y. Ho, MBBS, BSc, MRCP, FRCA, FHKCA, FHKAM (Anaesthesiology) Associate Consultant, Department of Anaesthesiology, Queen Mary Hospital and University of Hong Kong, Hong Kong
Kimberley Hodge, MBChB, FRCA, PGDip Med Ed Senior Registrar in Anaesthesia, St. Mary’s Hospital Department of Anaesthesia, Imperial College Healthcare NHS Trust, London, Squadron Leader, Royal Air Force, UK
Theresa Wan-Chun Hui, MBBS, FANZCA, FHKAM Consultant Anaesthetist, Department of Anaesthesiology, The Duchess of Kent Children’s Hospital, Hong Kong
Michael G. Irwin, MBChB, MD, FRCA, FCAI, FANZCA, FHKAM Daniel CK Yu Professor, Department of Anaesthesiology, University of Hong Kong, Hong Kong
Cyrus Kerawala, BDS (Hons), FDSRCS (Eng), MBBS (Hons), FRCS, FRCS (OMFS) Professor, Consultant Maxillofacial/Head & Neck Surgery, Royal Marsden Foundation Trust, London, UK
Orla J. Lacey, MBChB FRCA Consultant Anaesthetist, The Royal Marsden NHS Foundation Trust, London, UK
David M. H. Lam, MBChB, FHKCA, FHKAM (Anaesthesiology) Honorary Clinical Assistant Professor, Department of Anaesthesiology, University of Hong Kong, Hong Kong
Corina Lee, MBChB, FRCA, MRCP Consultant Anaesthetist, Chelsea & Westminster Hospital, London, UK
Gene Lee, MBBS, FRCA, FANZCA Consultant Anaesthetist, Department of Anaesthesia and Pain Management, Royal North Shore Hospital and St Vincent’s Hospital, Sydney, Australia
Shona Love, BSc (Med Sci), MBChB, MRCS, FRCA Consultant Anaesthetist, Imperial College NHS Trust, London, UK
Frances Lui, MBChB, FHKCA, FHKAM (Anaesthesiology), FANZCA Consultant Anaesthetist, Department of Anaesthesiology, Queen Mary Hospital, Honorary Clinical Associate Professor, University of Hong Kong, Hong Kong
Craig Lyons, MBBCh, BAO, FCAI Senior Registrar, Department of Anaesthesia and Intensive Care Medicine, Galway University Hospitals, Galway, Ireland
James W. D. Mann, MBChB, FRCA Consultant Anaesthetist, Great Western Hospital, Swindon, Wiltshire, UK
Fauzia Mir, MBBS, FRCA, EDICM, PGCert Med Ed Consultant Anaesthetist, St George’s Hospital, London, UK
Indu Mitra, MRCS, FRCR Consultant Radiologist, Department of Imaging, Chelsea & Westminster Hospital, London, UK
John Myatt, BSc, MBBS, FRCA Consultant Anaesthetist, Imperial College NHS Trust, London, UK
Caroline A. R. Nicholas, BSc (Hons Lon), MB BS, FRCA Consultant Anaesthetist, University Hospitals Sussex NHS Foundation Trust, UK
Ellen P. O’Sullivan, MBBCh, BAO, FRCA, FCAI Professor and Consultant in Anaesthesia, Department of Anaesthesiology and Intensive Care, St James’s Hospital, Dublin, Ireland
Christopher H. Rassekh, MD Professor of Otorhinolaryngology: Head and Neck Surgery, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA
Rebecca Thurairatnam, MBBS, BSc, FRCA Consultant Anaesthetist, Croydon University Hospital, London, UK
David J. A. Vaughan, MBBS, FRCA Consultant Anaesthetist, Northwick Park Hospital, Harrow, UK
Tim N. Vorster, BSc (Hons Lon), MBBS, FRCA Consultant Anaesthetist and Clinical Director Anaesthetics, Perioperative and Clinical Support Services, Queen Victoria Hospital, East Grinstead, UK
Patrick A. Ward, MBChB, BSc, FRCA Consultant Anaesthetist, St John’s Hospital, NHS Lothian, Scotland, UK
Silky Wong, MBBS, FHKCA, FHKAM (Anaesthesiology), FANZCA Associate Consultant in Anaesthesia, The Duchess of Kent Children’s Hospital, Hong Kong
Stanley Sau Ching Wong, MBBS (HK), MD (HKU), FHKCA, FHKAM (Anaesthesiology), FANZCA, FHKCA (Pain Med) Clinical Assistant Professor, University of Hong Kong, Hong Kong
Vivian Yuen, MD, MBBS, FANZCA, FHKCA, FHKAM Consultant Anaesthetist, Queen Mary Hospital, Honorary Assistant Clinical Professor, Department of
1
Preoperative assessment
Roger H. Y. Ho and David M. H. Lam
Introduction
Preoperative assessment for oromaxillofacial surgery (OMFS) can be particularly challenging. OMFS encompasses a wide range of procedures, some of which may overlap with ear, nose, and throat surgery; head & neck surgery; neurosurgery; and/or plastic surgery. The anaesthetist must have a good understanding of the extent and complexities of the surgery being undertaken in order to make an appropriate assessment and formulate an effective plan for anaesthesia and postoperative care. The setting in which these procedures are undertaken may be variable, ranging from the hospital operating theatre to the less familiar environment of the outpatient dental clinic, placing emphasis on the preoperative assessment in determining the most appropriate pathway. The indications for OMFS procedures frequently have anaesthetic implications, where concomitant injuries or associated syndromes/diseases must be considered in the anaesthetist’s preoperative evaluation—in particular, the potential for difficult airway management. As with all shared-airway surgery, sound preoperative assessment and planning is essential in ensuring patient safety, while optimizing surgical access and operating conditions.
Range of procedures
OMFS encompasses dentoalveolar procedures (such as general dentistry and wisdom teeth extraction), intraoral surgery, orthognathic surgery, facial cosmetic surgery, major reconstructive surgery with implants or local/distant microvascular free flaps, temporomandibular joint (TMJ) surgery, and craniofacial surgery. The goals of surgery can be broadly classified as functional restorative, structural support, and aesthetic reconstruction.
Airway evaluation and planning
Preoperative assessment of the airway for OMFS should include screening patients for the following:
• Predictors of difficulty in tracheal intubation (oral or nasal).
• Predictors of difficulty in ventilation/rescue oxygenation (via face mask or supraglottic airway device).
• Potential requirement for an awake airway management technique (and ability of patient to cooperate/consent for this approach).
• Ease of a front of neck airway.
In the elective setting, a detailed review of previous anaesthetic records, past medical history, and surgical history should be undertaken. In addition to routine examination of the airway, which includes assessment of mouth opening, dentition, thyromental distance, jaw protrusion, and neck mobility, the OMFS airway examination often necessitates assessment for nasotracheal intubation—screening for potential contraindications, such as nasopharyngeal carcinoma or previous cleft palate repair, and risk factors for epistaxis, such as altered coagulation or nasal polyps. The findings of recent imaging, such as computed tomography or magnetic resonance imaging, may provide additional information (including the specific location of any lesion and degree of airway compression, distortion, or obstruction). Other technologies, including virtual airway endoscopy and three-dimensional printed models, have also been described in the assessment and planning of complex airway management, though are less commonly utilized at present. Should the findings of bedside assessments and routine investigations remain inconclusive, awake nasendoscopy can often provide invaluable information. These assessments and investigations assist the anaesthetist in formulating an airway management strategy, which should comprise a primary airway plan, as well as airway rescue plan(s), in accordance with the UK National Audit Project 4 (NAP4).1 (Assessment and management of the difficult airway is discussed in greater detail in Chapter 2.)
In the emergency setting (e.g. oromaxillofacial trauma or infection), it is crucial to identify any signs or symptoms indicative of impending airway obstruction—stridor, dyspnoea, hoarseness, drooling, and/or lack of tongue protrusion, requiring urgent airway intervention. Management of the airway may be further complicated by limited mouth opening due to trismus, difficult front of neck access due to previous surgery/radiotherapy, infection, obesity, or the presence of a rigid cervical spinal collar, and/or an uncooperative/ combative patient.
A crucial aspect in formulating any airway management strategy is the involvement of the multidisciplinary team—prior discussion with the surgical team (in advance of anaesthesia) is essential to
ensure the respective requirements/priorities of each team are met. The anaesthetist may wish the surgeon to be present at induction of anaesthesia if there are concerns that a rescue surgical airway may be required. The position of the airway device/breathing circuit should be specifically discussed, so as not to obscure the surgical field or prevent assessment of bite occlusion (if required). Where significant movement of the head and neck is expected (particularly TMJ surgery), this should be emphasized by the surgical team to the anaesthetist, thus ensuring the airway device is secured appropriately to prevent accidental tracheal extubation. In some procedures, patency of the airway may be compromised postoperatively by bleeding or oedema, therefore a plan for tracheal extubation (technique, timing, and setting) must be agreed preoperatively (and modified as necessary). Clearly, if a tracheostomy, intermaxillary fixation device, or other significant intervention is planned, the anaesthetist and surgeon must have discussed them with each other, and with the patient.
Pathology-specific considerations
Trauma
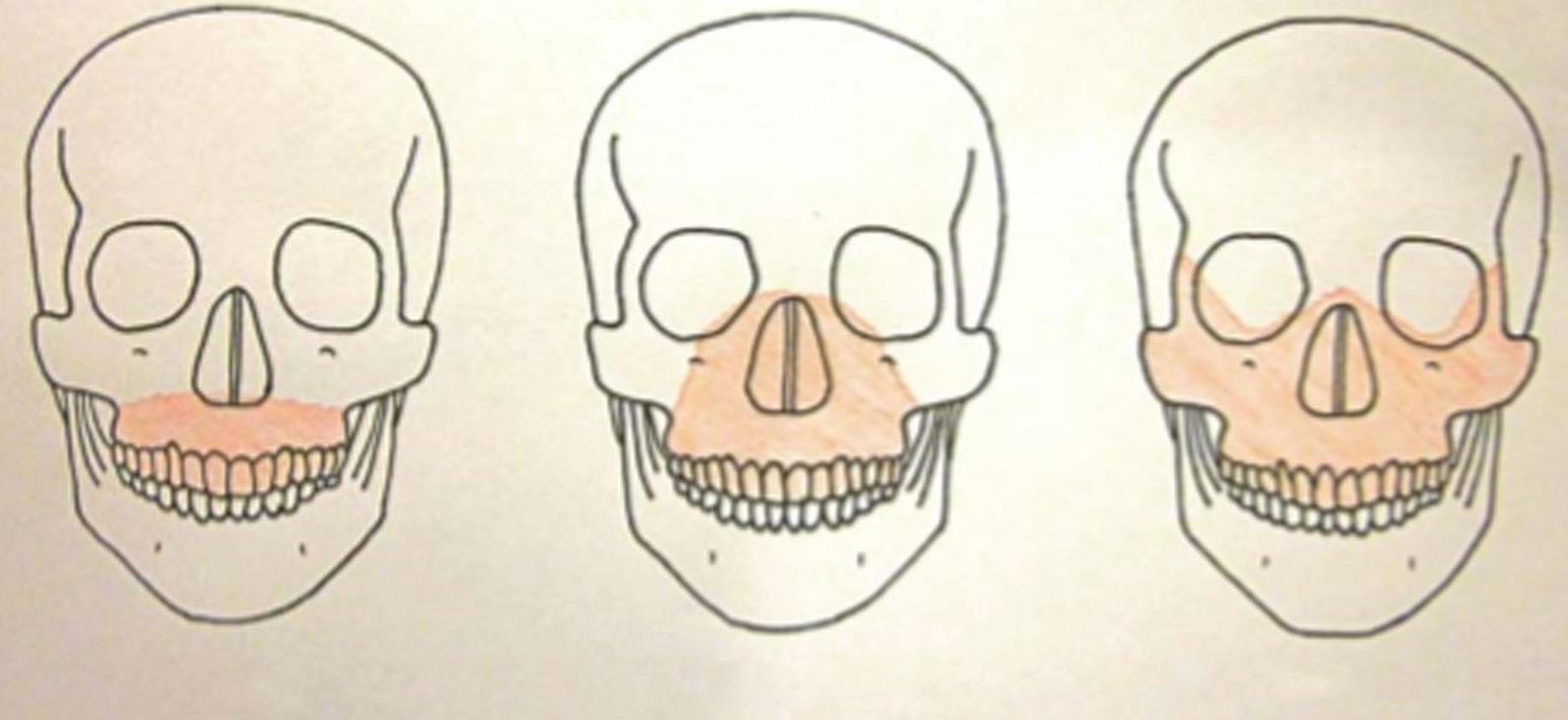
While the appearance of facial injuries can be distracting, it is critical to prioritize management of trauma patients according to clinical importance, following a systematic approach (as per Advanced Trauma Life Support principles). The goal of the airway assessment in the primary survey is to establish any immediate threat to patency, identifying any signs and symptoms of potential airway obstruction (e.g. tracheal deviation, subcutaneous emphysema, and/or marked soft tissue swelling). Traumatic injuries classically associated with airway obstruction include bilateral anterior mandibular fractures and the Le Fort III fracture (Fig. 1.1).
Airway management in the trauma setting should always be presumed to be difficult. Cervical spine movements are often restricted due to the application of a rigid cervical spine collar and/ or manual in-line stabilization. Mouth opening may be restricted by pain, muscle spasm, or mechanical obstruction (e.g. a tripod fracture of the zygomatic complex may interfere with movement of the coronoid process of the mandible). The patient may be combative/ unable to cooperate with an awake tracheal intubation technique,
and there may be the additional risk of aspiration of blood or broken teeth fragments. Having undertaken initial assessment and stabilization of the patient, the secondary survey should include an ‘AMPLE’ (Allergy, Medication, Past medical history, Last food and drink, Event) history, full body examination, and relevant investigations. In particular, the mechanism of injury and magnitude of energy transfer are important factors in guiding identification and assessment of injuries. Classification of facial fractures as lower, middle, and/or upper third may also be helpful in identifying concomitant injuries commonly associated at each level. (Management of the oromaxillofacial trauma patient is discussed in detail in Chapter 13.)
Infection
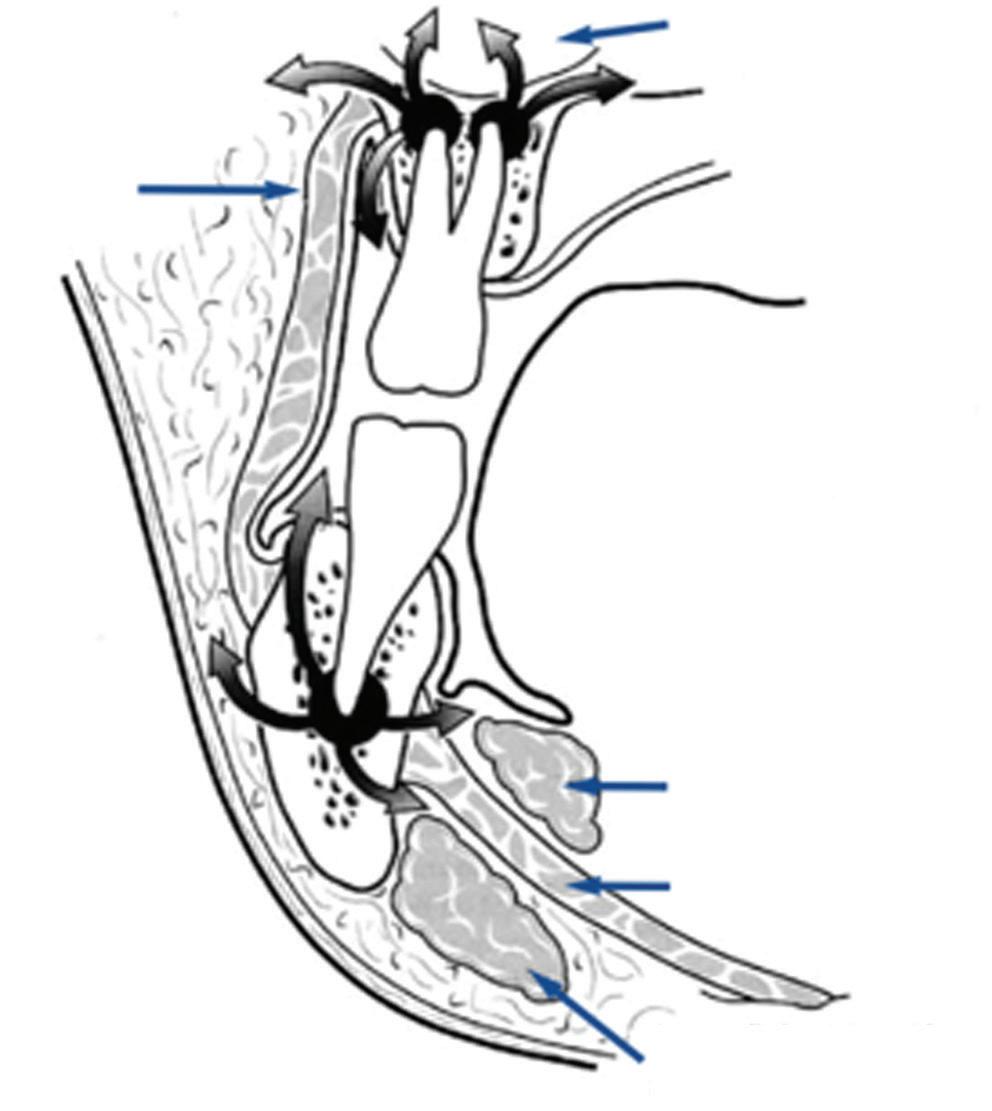
The most common cause of oromaxillofacial infection is impacted teeth, and the resulting dental abscess may cause significant facial swelling and trismus, affecting airway management (rarer causes of infection include tuberculosis, syphilis, and fungal or viral infection in immunocompromised states). Infection usually begins with dental decay and pulpitis, leading to perforation of the bone cortex, allowing the infection to spread to the subperiosteal region. In more severe cases, infection may spread along the fascial planes into the infratemporal fossa, subtemporalis, or even the cervical fascial plane (Fig. 1.2), forming a parapharyngeal abscess and even mediastinitis. The classic example of this is Ludwig’s angina, in which cellulitis extends over the entire floor of mouth, including both the submandibular and sublingual spaces. Preoperative evaluation of the airway reveals difficulty in swallowing secretions and an inability to protrude the tongue. Neck and/or pretracheal fascial involvement complicates the option of tracheostomy formation. In addition to assessing the extent of local spread, the systemic effects of bacteraemia/sepsis via haematogenous spread must be actively sought and promptly managed according to the Surviving Sepsis Campaign.3 (Management of oromaxillofacial infection is discussed in greater detail in Chapter 12.)
Congenital anomalies
Cleft lip and palate are among the most common congenital defects requiring surgery. In addition to the primary repair, patients often require subsequent procedures for lip aesthetics, closure of residual palatal defects, bone grafts, alignment of alveolar and dental defects,
Le Fort ILe Fort IILe Fort III
Fig. 1.1 The Le Fort classification of facial fractures.2
Maxillary sinus
Deep lobe of submandibular gland
Mylohyoid muscle
Superficial lobe of submandibular gland
jaw realignment, and correction of nasal deformity. Although cleft defects per se do not lead to upper airway obstruction and/or difficult airway management, coexisting structural or neuromuscular dysfunction may result in either/both. For example, in Pierre Robin sequence, the combination of micrognathia, glossoptosis, and cleft palate may cause airway obstruction relieved only by prone positioning or insertion of a nasopharyngeal airway, and in some cases necessitating tracheostomy formation. Crucially, beyond the airway examination, the anaesthetist must be aware of the multisystem nature of many of the syndromes associated with cleft anomalies, and make appropriate assessment of cardiac, renal, and skeletal systems as required (Table 1.1).
Malignancy
Airway management may be complicated by distortion, invasion, or compression of tissues by the tumour and/or progressive airway obstruction by the lesion itself. Previous cancer treatments/surgery may also contribute to airway management difficulties (Table 1.2).
Consideration should be given to the specific risk factors associated with head and neck cancer, including human papilloma virus, smoking, and alcohol use, and their associated comorbidities—in particular, chronic obstructive lung disease, ischaemic heart disease, alcoholic cardiomyopathy, liver cirrhosis, and alcohol dependence. There is a 10% risk of a synchronous primary cancer elsewhere within the aerodigestive tract, which should be sought through appropriate imaging. Malnutrition is common due to poor appetite, dysphagia, or side effects of chemotherapy and/or radiation mucositis, and dietician input is advocated to optimize nutritional support preoperatively in order to minimize the reduced wound healing, and increased risk of infection/other postoperative complications associated with it. (Management of the oromaxillofacial patient with malignancy is discussed in detail in Chapter 15.)
Table 1.1 Congenital syndromes associated with cleft lip and palate
Down syndrome
Pierre Robin sequence
Hemifacial microsomia
Treacher Collins syndrome
Velocardiofacial syndrome
Microstomia and macroglossia
Atlantoaxial subluxation and instability
Congenital cardiac disease
Micrognathia
Glossoptosis
Usually easier to intubate with age
Hemifacial and mandibular hypoplasia
Cervical spine abnormalities
Eye and ear malformations
Usually more difficult to intubate with age
Micrognathia and maxillary hypoplasia
Choanal atresia
Eye and ear malformations
Usually more difficult to intubate with age
Microcephaly
Microstomia, flat nasal bridge, velopharyngeal incompetence, tracheal and laryngeal anomalies
Congenital cardiac disease
Small ears, short stature
Stickler syndrome
Klippel–Feil syndrome
Free flap transfer
Micrognathia and flat face
Eye, ear, and joint abnormalities
Congenital cardiac disease
Webbed neck and fused cervical vertebrae
Congenital cardiac disease
Short stature
This surgical technique may be employed to provide tissue for reconstruction. Successful flap perfusion (and surgical outcome) relies upon optimization of perioperative haemodynamics (a relative hyperdynamic circulation with high cardiac output and vasodilation is desirable), thus preoperative assessment of cardiorespiratory reserve is crucial in establishing the appropriateness of the planned procedure. Contraindications might include sickle cell disease and untreated polycythaemia rubra vera due to their hypercoagulable states, and flap survival may be compromised in patients with active vasculitis or peripheral vascular disease. Prolonged preoperative fasting should be avoided in order to minimize any fluid deficits.
Table 1.2 Sequelae of oromaxillofacial and head and neck cancer treatments
Maxillectomy and craniofacial resection
Tongue, floor of mouth surgery
Laryngeal surgery
Neck dissection
Radiotherapy
Difficult facemask seal
Difficult nasotracheal intubation
TMJ pseudoankylosis
Trismus
Limited mandibular space
Fixed tongue
Laryngeal stenosis
Impaired swallowing
Aspiration risk
Damage to cranial nerves IX, X, XII
Vocal cord palsy
Impaired swallowing
Aspiration risk
Limited neck extension
TMJ ankylosis
Osteoradionecrosis of mandible
Carotid artery stenosis
Poor wound healing
Buccinator muscle
Fig. 1.2 Spread of odontogenic infection through the fascial planes.
(Management of OMFS patients for free flap reconstruction is discussed in greater detail in Chapter 15.)
Environmental considerations
Minor dental procedures are commonly performed under sedation or general anaesthesia in short-stay ambulatory care centres, and sometimes dental clinics. Accessibility to drugs and equipment, availability of postoperative recovery facilities, staff numbers, and staff training in airway management, resuscitation, and sedation may vary significantly between the settings. Appropriate patient selection through thorough preoperative assessment is crucial in ensuring patient safety in the remote site/day surgical environment. Patient suitability should be based upon assessment of comorbidities and fitness for day surgery, as well as determining the availability of an appropriate escort, geographical proximity, and access to emergency services if required (as described by the Society of Day Surgery4). The guidelines for the management of children referred for dental extraction under general anesthesia5 state that sedation or general anaesthesia is best delivered in the inpatient setting for patients considered to be of high anaesthetic risk, with significant comorbidities or complex dental problems (Table 1.3), where high dependency unit/intensive care is immediately available or may be arranged in advance. (Dental anaesthesia and sedation are covered in greater detail in Chapters 8 and 6, respectively.)
Evaluation of comorbidities
Obesity and obstructive sleep apnoea syndrome
Obesity is defined as a body mass index (BMI) ≥30 kg/m2; morbid obesity ≥35 kg/m2; and supermorbid obesity ≥50 kg/m2. There is an increasing number of patients with raised BMI presenting for OMFS, and the pathophysiological consequences of obesity pose significant challenges to the anaesthetist.
Obstructive sleep apnoea syndrome (OSAS) arises from periodic partial or complete collapse of the upper airway during sleep,
Table 1.3 Conditions for dental extraction in the inpatient (hospital) setting
High anaesthetic risk
Anatomically or functionally abnormal airway
Significant learning disabilities or behavioural abnormalities
Severe anxiety
Congenital syndromes associated with increased anaesthetic risk
History of adverse reaction to anaesthetic agents
History of complications occurring under general anaesthesia
Family history of significant problems occurring under general anaesthesia
Table 1.4 Classification of the severity of OSAS according to the American Academy of Sleeping Medicine Task Force
Apnoea–hypopnoea index
<5
5–15
15–30
>30
Significant comorbidities
Severe or poorly controlled asthma
Symptomatic cardiac disease, requiring treatment
Coagulopathy, anticoagulant therapy, or antiplatelet therapy
Impaired renal or hepatic function
Unstable metabolic or endocrine disorders
Significant neurological or neuromuscular disorders
Active systemic infection
Haemoglobinopathies
Abnormal BMI (<18.5 kg/m2 or >30 kg/m2)
Severity classification
Normal
Mild
Moderate
Severe
Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep. 1999;22(5):667–89.
resulting in decreased (hypopnoea) or complete cessation (apnoea) of airflow. The severity of OSAS is defined by the apnoea–hypopnoea index (the number of apnoea or hypopnoea events per hour) (Table 1.4).6 These recurrent episodes of hypoxia can lead to significant cardiopulmonary morbidity, such as pulmonary hypertension and cor pulmonale. Patients often have poor sleep quality due to the frequent arousal that occurs during their sleep cycle to restore airway patency,7 resulting in behavioural disturbances, such as daytime hypersomnolence and sexual dysfunction.
Patients with OSAS presenting for surgery are at increased risk of perioperative airway, respiratory, and cardiovascular complications,8 and these risks are further increased if the condition remains undiagnosed (and untreated) at the time of surgery.9 Respiratory complications (e.g. oxygen desaturation, acute respiratory failure, respiratory arrest, and aspiration pneumonia) are the most common, as the underlying pathophysiology of OSAS may be exacerbated by the depressant effects of anaesthetic medications upon respiratory drive, airway protective reflexes, and arousal responses.8 These problems may be further compounded in patients undergoing major OMFS procedures due to significant alterations in airway anatomy and postoperative oedema.
Obesity per se is not always associated with difficult tracheal intubation; however, many aspects of airway management may be more challenging. Thorough preoperative airway examination should be undertaken, seeking features suggestive of difficult airway management—in particular, a Mallampati score ≥3, a high Wilson score, and increased neck circumference. Often, a standard asleep tracheal intubation is both practical and safe (especially following the advent of videolaryngoscopy); however, a robust strategy for airway management must always be in place prior to induction of anaesthesia.
Obese patients are more prone to both restrictive and obstructive respiratory insufficiency—decreased chest wall and lung compliance results in a restrictive defect, while increased adipose tissue within the pharyngeal walls predisposes to airway collapse during normal breathing and contributes to the development of OSAS. Obese patients should therefore be routinely screened for OSAS preoperatively—including identification of any risk factors (Box 1.1),10 thorough physical examination, use of the STOP-BANG questionnaire (Table 1.5),8 and appropriate investigations such as electrocardiography, pulse oximetry, pulmonary function tests,11 and polysomnography.12 Abnormal spirometry is associated with increased postoperative complications.13 The STOP-BANG questionnaire is currently the most sensitive, specific, and best-validated screening questionnaire for OSAS. A score of 0–2 indicates ‘low risk’, 3–4 indicates ‘intermediate risk’, and a score of ≥5 indicates ‘high
Box 1.1 Predisposing conditions for obstructive sleep apnoea
• Obesity
• Age 40–70 yr
• Male gender
• Excess alcohol intake
• Smoking
• Pregnancy
• Low Physical activity
• Unemployment
• Neck circumference >40 cm
• Surgical patient
• Tonsillar and adenoidal hypertrophy
• Craniofacial abnormalities (e.g. Pierre Robin, Down’s syndrome)
• Neuromuscular disease
Source: Martinez G, Faber P. Obstructive Sleep apnoea. Continuing Education in Anaesthesia Critical Care & Pain. 2011; 11(1): 5–8.
risk’ for OSAS. Patients who have an intermediate-to-high risk score are at greater risk of perioperative complications14 and referral to a sleep specialist for formal evaluation and optimization is recommended. Strategies that may be considered include weight loss, the use of mandibular advancement devices, and non-invasive positive pressure ventilation.6 Utilization of continuous positive airway pressure/bi-level positive airway pressure devices may reduce the incidence of perioperative hypoxic events in obese patients, regardless of whether OSAS has been formally diagnosed.11
Early preoperative identification of OSAS allows initiation of non-invasive ventilation therapy (as indicated) prior to surgery, reducing the overall risk of perioperative complications. Prompt diagnosis also enables the appropriate preoperative planning to occur, influencing the conduct of all aspects of anaesthetic care, including the choice of anaesthetic medications, airway management, and nature of the postoperative care facility. Many patients with OSAS will also suffer from concomitant comorbidities that should be optimized preoperatively.
Obesity is associated with cardiovascular comorbidities such as hypertension, ischaemic heart disease, and arrhythmias. Patients with these conditions should be managed in accordance with the European Society of Cardiology (ESC)/European Society of Anaesthesiology (ESA) guidelines11 or American College of Cardiology (ACC)/American Heart Association (AHA) guidelines15 to achieve satisfactory control prior to any elective surgery.
Table 1.5 STOP-BANG questionnaire, utilized as a screening tool for
Snoring: do you snore loudly (louder than talking or loud enough to be heard through closed doors)?
Yes/No
Tired: do you often feel tired, fatigued, or sleepy during the daytime? Yes/No
Observed: has anyone observed you stopping breathing during your sleep? Yes/No
Blood Pressure: do you have high blood pressure or are you on treatment for high blood pressure? Yes/No
BMI: is your body mass index greater than 35 kg/m2? Yes/No
Age: are you over 50 years old? Yes/No
Neck circumference: is your neck circumference greater than 40 cm (16 inches)? Yes/No
Gender: are you male?
Yes/No
Hall A. Sleep physiology and the perioperative care of patients with sleep disorders. BJA Education. 2014;15(4):167–72.
Obesity is an independent risk factor for perioperative renal dysfunction,16 and although there is no evidence that any particular preoperative optimization strategy is effective in minimizing postoperative renal impairment, general protective strategies such as correcting preoperative anaemia, avoiding nephrotoxic medications, and maintaining adequate volume status should be employed.17
Obesity is also commonly associated with metabolic disorders such as diabetes, hyperlipidaemia, and fatty liver disease. Perioperative hyperglycaemia is associated with increased morbidity and mortality in patients undergoing non-cardiac surgery.18 The 2018 ESA guidelines recommend that laboratory testing to screen for diabetes should be carried out in obese patients prior to elective non-cardiac surgery (if the condition has not already been diagnosed).11 Glycaemic control should be optimized, with elective surgery delayed in order to achieve this.19
Obesity is also associated with anaemia, and deficiencies in various micronutrients such as vitamin D, ascorbic acid, and betacarotene.20 These deficits should be identified during preoperative assessment and corrected before elective surgery is undertaken (anaemia is discussed in detail later in this chapter).
Patients with OSAS should have their condition thoroughly reviewed at preassessment, and, if compliant with existing therapy, asymptomatic, and without significant cardiopulmonary sequelae, can be considered appropriate to proceed with surgery as planned without further investigation and/or treatment. The non-invasive ventilation device used by the patient should be brought into hospital on admission and its use continued throughout the perioperative period,11 unless specifically contraindicated (e.g. if there are surgical concerns following craniofacial surgery). However, patients who have poorly controlled OSAS (or who have developed secondary cardiopulmonary complications) should be referred for further assessment and optimization before elective surgery. In semi-elective/expedited surgery (e.g. cancer surgery), the decision to defer surgery for further investigation and/or treatment for OSAS should take an individualized approach, taking into consideration the urgency and risk of surgery, the severity of OSAS and other comorbidities, and the relative accessibility of proposed investigations/treatments. In urgent or emergency surgery, where preoperative optimization may be precluded, patients considered to be at high risk of OSAS should be presumed to have the condition and managed as such, with measures taken to minimize perioperative complications, including postoperative care in an appropriately staffed and monitored facility.
OSAS is not an absolute contraindication for day surgery, although patient selection is key—taking into consideration the extent of planned surgery, severity of OSAS, comorbidities, anaesthetic technique, postoperative analgesic requirements, and necessity for advanced postoperative monitoring and non-invasive ventilation.
Coronary artery disease and revascularization
Coronary artery disease is a risk factor for perioperative major adverse cardiovascular events.15 For elective surgery, perioperative cardiac assessment should proceed according to the stepwise approaches described in the ‘ESC/ESA guidelines on non-cardiac surgery: cardiovascular assessment and management’11 or the ‘ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing non-
OSAS
Patient scheduled for surgery with known or risk factors for CAD* (Step 1)
Emergency
No
ACS† (Step 2)
No
Yes
Clinical risk stratification and proceed to surgery
*See Sections 2.2, 2.4, and 2.5 in the full-text CPG for recommendations for patients with symptomatic HP, VHD, or arrhythmias.
†See UA/NSTEMI and STEMI CPGs (Table 2).
Yes
Estimated perioperative risk of MACE based on combined clinical/surgical risk (Step 3)
Low risk (<1%) (Step 4)
No further testing (Class III: NB)
Proceed to surgery
Elevated risk (Step 5)
Evaluate and treat according to GDMT†
Excellent (>10 METs)
Moderate or greater (≥4 METs) functional capacity
Moderate/Good (≥4–10 METs)
No further testing (Class Ila)
Proceed to surgery
No or unknown
Poor OR unknown functional capacity (<4 METs): Will further testing impact decision making OR perioperative care? (Step 6)
Yes
No further testing (Class Ilb)
Pharmacologic stress testing (Class Ila)
If normal
No If abnormal
Proceed to surgery according to GDMT OR alternate strategies (noninvasive treatment, palliation) (Step 7)
Coronary revascularization according to existing CPGs (Class I)
Fig. 1.3 Step-wise approach to assessment of patients with pre-existing coronary artery disease (CAD) undergoing surgery.15 ACS, acute coronary syndrome; CABG, coronary artery bypass graft; CPG, clinical practice guideline; DASI, Duke Activity Status Index; GDMT, guideline-directed medical therapy; HF, heart failure; MACE, major adverse cardiac event; MET, metabolic equivalent; NB, no benefit; NSQIP, National Surgical Quality Improvement Program; PCI, percutaneous coronary intervention; RCRI, Revised Cardiac Risk Index; STEMI, ST-elevation myocardial infarction; UA/ NSTEMI, unstable angina/non-ST-elevation myocardial infarction; VHD, valvular heart disease.
Reproduced with permissions from Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130(24):e278–333.
a low combined clinical and surgical risk (<1% risk of a major adverse cardiovascular event) can safely proceed to surgery without additional testing. Many OMFS procedures are considered to be of low surgical risk (e.g. superficial oral and periodontal surgery); however, the presence of ischaemic heart disease alone may elevate the overall risk of major adverse cardiovascular events to ≥1%.21 In such cases, assessment
of patients’ functional capacity is essential, and pharmacological stress testing (and subsequent coronary revascularization) may be indicated (Figs 1.3 and 1.4). Routine preoperative coronary angiography or prophylactic revascularization is not recommended to exclusively reduce perioperative cardiac events22 an approach supported by the recent Coronary-Artery Revascularisation Prophylaxis (CARP) trial,
One of active or unstable cardiac conditions (table 9)
Determine the risk of the surgical procedure (table 3)
Intermediate or high
Consider the functional capacity of the patient
In patients with a poor functional capacity consider the risk of the surgical procedure
High-risk surgery
Cardiac risk factors (table 4)
Consider non-invasive testing. Noninvasive testing can also be considered prior to any surgical procedure for patient counselling, change of peri-operative management in relation to type of surgery and anaesthesia technique.
Interpretation of non-invasive stress test results
risk surgery
Patient or surgical specific factors dictate the strategy, and do not allow further cardiac testing or treatment. The consultant provides recommendations on peri-operative medical management, surveillance for cardiac events and continuation of chronic cardiovascular medical therapy.
Treatment options should be discussed in a multidisciplinary team, involving all peri-operative care physicians as interventions might have implication on anaesthesiological and surgical care. For instance in the presence of unstable angina, depending on the outcome of this discussion, patients can proceed for coronary artery intervention, with the initiation of dual-anti platelet therapy if the index surgical procedure can be delayed, or directly for operation if delay is impossible with optimal medical therapy.
The consultant can identify risk factors and provide recommendations on lifestyle and medical therapy, according to the ESC Guidelines.
In patients with one or more clinical risk factors, preoperative baseline ECG may be considered to monitor changes during the peri-operative period.
In patients with known IHD or myocardial ischaemia, initiation of a titrated low-dose beta-blocker regimen may be considered before surgery .
In patients with heart failure and systolic dysfunction, ACEI should be considered before surgery.
In patients undergoing vascular surgery, initiation of statin therapy should be considered.
In addition to suggestions above:
In patients with one or more clinical risk factors, non-invasive stress testing may be considered.
In addition to suggestions above: Rest echocardiography and biomarkers may be considered for evaluation of LV function and obtaining prognostic information for peri-operative and late cardiac events
No/mild/ moderate stress-induced ischaemia
Bare-metal stent:
Balloon angioplasty:
Surgery can be performed >2 weeks after intervention with continuation of aspirin treatment
Surgery can be performed >4 weeks after intervention.
Dual antiplatelet therapy should be continued for at least 4 weeks.
An individualized peri-operative management is recommended considering the potential benefit of the proposed surgical procedure compared with the predicted adverse outcome, and the effect of medical therapy and/or coronary revascularization.
Surgery can be performed within 12 months after intervention for old-generation DES and within 6 months for new-generation DES.
Continuation or discontinuation of aspirin in patients previously treated with aspirin may be considered in the peri-operative period, and should be based on an individual decision that depends on the peri-operative bleeding risk weighed against the risk of thrombotic complications (see also Table 8).
Surgery
aTreatment should be initiated optimally between 30 days and at least 2 days before surgery and should be continued postoperatively aiming at target resting heart rate of 60–70 beats per minute and systolic blood pressure >100 mmHg. bFor strategy of anaesthesia and perioperative monitoring see appropriate sections.
Fig. 1.4 Assessment and treatment strategies in the management of patients with cardiac risk factors undergoing surgery.11
Kristensen SD, Knuuti J, Saraste A, Anker S, Botker HE, Hert SD, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J. 2014;35(35):2383–431. 2014;35(35):2383–431