Buy ebook Mesenteric principles of gastrointestinal surgery: basic and applied science coffey, john
Mesenteric Principles of Gastrointestinal Surgery: Basic and Applied Science Coffey, John Calvin, Sehgal, Rishabh, Walsh, Dara
Mesenteric Principles Of Gastrointestinal Surgery: Basic And Applied Science Coffey
Visit to download the full and correct content document: https://ebookmass.com/product/mesenteric-principles-of-gastrointestinal-surgery-basi c-and-applied-science-coffey-john-calvin-sehgal-rishabh-walsh-dara-mesenteric-princi ples-of-gastrointestinal-surgery-basic-and-applied-scie/
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Electronic materials : principles and applied science
CRC Press is an imprint of Taylor & Francis Group, an Informa business
No claim to original U.S. Government works
Printed on acid-free paper
Version Date: 20160812
International Standard Book Number-13: 978-1-4987-1122-7 (Pack - Book and Ebook)
This book contains information obtained from authentic and highly regarded sources. While all reasonable efforts have been made to publish reliable data and information, neither the author[s] nor the publisher can accept any legal responsibility or liability for any errors or omissions that may be made. The publishers wish to make clear that any views or opinions expressed in this book by individual editors, authors or contributors are personal to them and do not necessarily reflect the views/opinions of the publishers. The information or guidance contained in this book is intended for use by medical, scientific or health-care professionals and is provided strictly as a supplement to the medical or other professional’s own judgement, their knowledge of the patient’s medical history, relevant manufacturer’s instructions and the appropriate best practice guidelines. Because of the rapid advances in medical science, any information or advice on dosages, procedures or diagnoses should be independently verified. The reader is strongly urged to consult the relevant national drug formulary and the drug companies’ and device or material manufacturers’ printed instructions, and their websites, before administering or utilizing any of the drugs, devices or materials mentioned in this book. This book does not indicate whether a particular treatment is appropriate or suitable for a particular individual. Ultimately it is the sole responsibility of the medical professional to make his or her own professional judgements, so as to advise and treat patients appropriately. The authors and publishers have also attempted to trace the copyright holders of all material reproduced in this publication and apologize to copyright holders if permission to publish in this form has not been obtained. If any copyright material has not been acknowledged please write and let us know so we may rectify in any future reprint.
Except as permitted under U.S. Copyright Law, no part of this book may be reprinted, reproduced, transmitted, or utilized in any form by any electronic, mechanical, or other means, now known or hereafter invented, including photocopying, microfilming, and recording, or in any information storage or retrieval system, without written permission from the publishers.
For permission to photocopy or use material electronically from this work, please access www.copyright.com (http://www.copyright.com/) or contact the Copyright Clearance Center, Inc. (CCC), 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400. CCC is a not-for-profit organization that provides licenses and registration for a variety of users. For organizations that have been granted a photocopy license by the CCC, a separate system of payment has been arranged.
Trademark Notice: Product or corporate names may be trademarks or registered trademarks, and are used only for identification and explanation without intent to infringe.
Visit the Taylor & Francis Web site at http://www.taylorandfrancis.com
and the CRC Press Web site at http://www.crcpress.com
There is nothing new under the sun.
Ecclesiastes 1:4-11
I could be bounded in a nutshell, and count myself a king of infinite space.
Hamlet, Act II, Scene 2
To Dee and Victor Warren Fazio Master without peer
J.
J. Calvin Coffey and Jonathon Efron
J. Calvin Coffey and Steven D. Wexner
J. Calvin Coffey and Neil J. Smart
21 Mesenteric
J. Calvin Coffey and Ian Lavery
22
J. Calvin Coffey, Eoghan Condon, and David W. Waldron 23 Mesenteric considerations in ileal pouch anal anastomosis
J. Calvin Coffey and James W. Ogilvie Jr.
24 Mesenteric considerations in ostomy formation and reversal
J. Calvin Coffey, Colin Peirce, and Ann Brannigan
25 Mesenteric
J. Calvin Coffey and Feza Remzi
26
Preface
This work is intended to furnish the Student and Practitioner with an accurate view of the Anatomy of the Human Body, and more especially the application of this science to Practical Surgery.
Henry Gray (1858)
MESENTERIC-BASED SURGERY DEFINED
Mesenteric-based surgery is where the surgeon exploits mesenteric and associated structures in guiding an intestinal resection. The associated structures are the peritoneal reflction and Toldt’s fascia. Rather than indiscriminately dissecting through tissue, structures, and planes, the surgeon selects certain structures and conducts a particular activity related to that structure. For example, during sigmoid mobilization for colectomy, the surgeon divides the peritoneal reflction at the right side of the base of the mesosigmoid (via a peritonotomy), which exposes the underlying mesofascial plane. Ths plane is formed at the interface between the mesosigmoid and the underlying Toldt’s fascia. The surgeon then separates the components of this plane to mobilize the mesosigmoid.
Nonmesenteric-based surgery is one where the surgeon does not adhere to a particular anatomic roadmap. The mesentery is divided directly across and dissociated from the posterior abdominal wall. During dissociation, the retroperitoneum and contained structures are often not recognized before being damaged.
Examples of mesenteric-based surgery now abound and include complete mesocolic excision, total mesorectal excision, and total mesocolic excision. Variations are also emerging, including transanal total mesorectal excision
and modifid complete mesocolic excision. As part of these procedures, the surgeon accesses the mesofascial plane in a targeted manner (through division of the peritoneal reflection), then mobilizes an intact mesentery without its disruption. Similarly, the retroperitoneum and covering fascia are preserved. When the mesentery is su fficiently mobilized, the vessels contained within are selected, skeletonized, and divided, and the mesentery is similarly divided up to the level of the intestine.
Several terms have been used in reference to nonmesenteric-based surgery. These include “conventional” surgery, “non-CME surgery, and “non-TME surgery.” Unfortunately, the terms “CME” and “TME” have not been scienti fically defi ned in the fi rst instance, and so the related terms also lack defiition.
Mesenteric-based surgery has been practiced internationally for over a century and thus is far from new. However, it is certainly not universally practiced, and considerable variation has been demonstrated. The variation is explained by the disparity that has persisted between anatomic and surgical approaches to the intestine for the past century. While mesenteric-based surgery is far from new, it is remarkable that its anatomic basis has only recently been formally described.
Th is means that the principles can now be reproducibly taught and conducted in an entirely standardized manner. Th is book is composed of two parts. In the fi rst part, the mesentery, peritoneum, and associated fascia are characterized. In the second part, the data explained in the fi rst are applied to all aspects of resectional colorectal surgery. Surgical anatomy, activities, and operations are carefully defi ned to enable all surgeons to reproducibly conduct mesenteric-based surgery.
J. Calvin Coffy
How to access three-dimensional models using QR codes
Each figue legend in this book will direct the reader to a QR code. The QR code to be accessed is specifid in the fist number in the following annotation: “QR 2/3.” Ths directs the reader to QR code 2 and annotation 3.
The QR codes are listed below. Using the example above, the reader should identify QR 2 below and scan the QR code with a QR reader (i.e., in a smart phone, lap-top, or tablet).
1 - Over view of mesentery and intestine
The reader then will be brought to a three-dimensional model relating to the figue legend and figue in question, with a series of numbers overlaying the model. By clicking on the number 3, the reader will be brought to a particular viewpoint of the model.
QR codes and models can also be accessed directly at the website “www.mpgs.ie.”
2 - Mesentery, peritoneum and intestine
3 - QR 2d - Mesentery, peritoneum and intestine
Sectioned view of right and left mesocolon as seen from above I
QR 3d -Sectioned view of right and left mesocolon as seen from above II
QR 5 - Sectioned view of the mesosigmoid as seen from above down
QR 7 - Colon and mesocolon
QR 4 - Sectioned view of right and left mesocolon viewed from below up
QR 6 - Sectioned right and left mesocolon viewed from below up
QR 8 - Medial view of base of small intestinal mesentery
QR
QR
QR
QR 9 - Splenic flexure in isolation
QR 11 - Hepatic flexure in isolation
QR 13 - Mesorectum and fascia
QR 10 - Splenic region with flexure removed
QR 12 - Hepatic region with flexure removed
Acknowledgments
We the authors gratefully acknowledge the insight and advice offered by the following individuals:
Ann Brannigan
Consultant Colorectal Surgeon Mater Misericordiae Hospital University College Dublin Dublin, Ireland
Consultant Colorectal Surgeon Department of Surgery and Interventional Sciences University College London London, United Kingdom
Eoghan Condon
Consultant Surgeon Department of Surgery University Hospital Limerick University of Limerick Limerick, Ireland
Peter Dockery Department of Anatomy School of Medicine
National University of Ireland Galway, Ireland
Jonathon Efron Ravitch Division of GI Surgery Department of Surgery
The Mark M Ravitch Professor of Surgery and Urology Johns Hopkins University Baltimore, Maryland
Bill Heald Pelican Cancer Foundation Basingstoke Hospital Basingstoke, United Kingdom
Awad M. Jarrar Department of Cellular and Molecular Medicine Lerner Research Institute Cleveland Clinic Cleveland, Ohio
Mathew Kalady Department of Colorectal Surgery
Digestive Diseases Institute Cleveland Clinic Cleveland, Ohio
Miranda Kiernan Department of Surgery Graduate Entry Medical School University of Limerick Limerick, Ireland
Ravi Kiran Department of Surgery
Columbia University Medical Center Mailman School of Public Health Center for Innovation and Outcomes Research Division of Colorectal Surgery New York Presbyterian Hospital-Columbia New York, New York
Joep Knol Consultant General and Colorectal Surgeon Jessa Hospital Hasselt, Belgium
Ian Lavery Department of Colorectal Surgery
Digestive Diseases Institute Cleveland Clinic Cleveland, Ohio
Jeremy Lipman
Associate Professor of Surgery
Cleveland Clinic Lerner College of Medicine
Case Western Reserve University
Staff Colorectal Surgeon Cleveland Clinic Foundation Cleveland, Ohio
Deirdre McGrath
4i Centre for Interventions in Inflammation, Infection and Immunity
Graduate Entry Medical School
University of Limerick Limerick, Ireland
Manus Moloney
Department of Gastroentrology
University of Limerick Hospitals Group
University Hospital Limerick Limerick, Ireland
Brendan J. Moran
Peritoneal Malignancy Institute
Basingstoke Hospital
Basingstoke, United Kingdom
James W. Ogilvie Jr.
Department of Colorectal Surgery
Spectrum Health/Ferguson Clinic
Michigan State University Grand Rapids, Michigan
D. Peter O’Leary
Department of Surgery
University of Limerick Hospitals Group University Hospital Limerick Limerick, Ireland
James O’Riordan
Department of General and Colorectal Surgery Tallaght Hospital Dublin, Ireland
Nicola O’Riordan
Department of Surgery
University of Limerick Hospitals Group University Hospital Limerick Limerick, Ireland
Colin Peirce
Department of Surgery
University Hospitals Limerick Limerick, Ireland
Feza Remzi
Professor of Surgery
Director, Inflammatory Bowel Disease Center
NYU Langone Medical Center
New York, New York
Jonathon Roddy
Department of Surgery
University of Limerick Hospitals Group
University Hospital Limerick Limerick, Ireland
Shaheel M. Sahebally Department of Surgery
University of Limerick Hospitals Group University Hospital Limerick Limerick, Ireland
Martin Shelly Department of Radiology
University of Limerick Hospitals Group
University Hospital Limerick Limerick, Ireland
Neil J. Smart
Department of Colorectal Surgery
University of Exeter Medical School
Royal Devon & Exeter Hospital Exeter, United Kingdom
Mattias Soop
Department of Colorectal Surgery
University of Manchester
Manchester, United Kingdom
Salford Royal Hospital Salford, United Kingdom
David W. Waldron
Department of Surgery
University of Limerick Hospitals Group University Hospital Limerick Limerick, Ireland
Leon G. Walsh
University of Limerick Hospitals Group University Hospital Limerick Limerick, Ireland
Steven D. Wexner
Digestive Disease Center
Department of Colorectal Surgery
Cleveland Clinic Florida Weston, Florida
Florida Atlantic University College of Medicine
Florida International University College of Medicine Miami, Florida
History
J. CALVIN COFFEY AND NICOLA O’RIORDAN
Two roads diverged in a wood, and I— I took the one less travelled by, And that has made all the difference.
Robert Frost
INTRODUCTION
For centuries, the mesentery and associated peritoneal lining have been regarded as structurally complex. In 1885, Sir Frederick Treves provided the fist comprehensive description of both, emphasizing that while some mesenteric regions persisted in adulthood, others regressed and were lost [1]. For example, the small intestinal mesentery, transverse, and sigmoid mesocolon were consistently identifiable in adults, while the right and leftmesocolon were identifiable in a minority only. Treves’ descriptions were welcome at the time, given the apparent complexity of the topic, and were subsequently indoctrinated in virtually all anatomic, embryologic, clinical, and related literature [1–3]. To the present, the fist chapter of most reference texts on intestinal surgery focuses on anatomy and physiology and is based on Treves’ descriptions. A review of later chapters dealing with techniques in intestinal removal identifiesa remarkable disparity. The right and leftmesocolon are invariably present in the adult and must be resected like any other mesenteric region. Put simply, intestinal surgery has always relied on the persistence of all regions of the mesentery.
Numerous factors contributed to the divergence of anatomic and surgical approaches to the mesentery and peritoneum. Since the time of Treves’ anatomic-based research, surgeons focused increasingly on cellular aspects of disease. With increasing awareness of the molecular basis
of surgical disease, the emphasis of research shi fted away from the anatomic-based craftcomponent. More recently, laparoscopic and robotic surgery have increased focus on the “cra ft” component of surgery. In keeping with this, the fild of surgical anatomy has increased in relative signi ficance and led to the demonstration of continuity of the mesenteric organ from the small intestinal mesentery to the mesorectum [4,5]. The following chapter will demonstrate these shi ft ing trends and clarify the manner in which recent demonstrations allow a reconciliation of anatomic and surgical approaches to this important organ. Th is chapter fi nishes by demonstrating the opportunities that now occur across a broad array of clinical and non-clinical sciences.
CARL TOLDT (1840–1920)
Carl Florian Toldt was born on May 3, 1840, in Bruneck, Austria. A fter spending much of his childhood repairing clocks, he received his doctorate in 1864 at St. Joseph’s University in Vienna and was appointed Professor of Anatomy at the University of Vienna in 1875 (Figure 1.1). He became Professor of Anatomy at the German university in Prague. He subsequently returned to Vienna in 1884 to work with his colleague, Langer, and together they established the Anatomy Institute of Vienna. Carl Toldt’s best-known anatomic work was Anatomischer Atlas für Studierende und Aerzte (An Atlas of Human Anatomy for Students and Physicians) (Figure 1.2), which was translated into English. Despite the superb quality of this work, and its anatomic accuracy, it has been little referenced overall. Toldt died from pneumonia in Vienna in November 1920 [6–9].
Toldt’s descriptions were based on dissection of fresh cadavers that had not been exposed to corrosive preservative
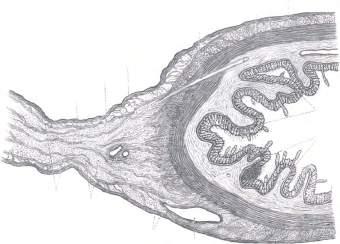
agents. He first observed that intestinal mesenteries did not simply comprise two thin layers of closely apposed cells (i.e., the mesothelia) but rather contained vessels, nerves, and fat. He called the resultant complex of structures the “lamina mesenteria propria” (Figure 1.3). While Treves described disappearance of the right and leftmesocolon as humans matured into adults, Toldt maintained they persisted and attached (i.e., flattened against) to the abdominal wall. Where they attached, Toldt identifid a thin seam of connective tissue (Toldt’s fascia) separating mesentery from abdominal wall, just as two layers of rock might be separated by a seam of rock (see Chapter 2). Toldt suggested that wherever the mesentery attached to the abdominal wall, the cellular layer lining both (i.e., the mesothelium) underwent a “gradual disappearance” to “admit contact and fusion of their connective tissue laminae.” Toldt also suggested that the outer cellular layer of the intestine, the tunica serosa, could undergo a similar process and merge with the covering mesothelium of adjacent mesentery. There is a striking similarity between current descriptions, and those of Toldt, and it is remarkable that his work should have been so infrequently referenced over the past two centuries [6–9].
SIR FREDERICK TREVES
Frederick Treves was born in Dorset, England, in 1853 (Figure 1.4). He received his medical education at the London School of Medicine and became assistant surgeon at the London hospital in 1879. In 1883 he was appointed as surgeon and head of the department of Anatomy. He famously housed Joseph Merrick, “the Elephant Man,” in his attic until Merrick died in 1890 [6,10]. Treves was awarded the Jacksonian prize for dissertations on the pathology, diagnosis, and treatment of obstruction of the intestine and numerous Hunterian lectures on the anatomy of the intestinal canal and the peritoneum. He served in the Boer war in 1899. He was knighted by King Edward VII on whom he performed an appendectomy in 1902. He was a noted travel writer and took up fi nal residence in Geneva (Switzerland) due to poor health. He died of peritonitis in 1923 [6,10,11].
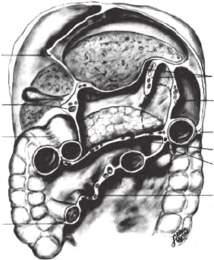
Treves described the human mesentery as fragmented. Accordingly, the right and leftmesocolic components of the mesentery are, according to Treves, mostly absent in the adult human. He described the small intestinal, transverse, and sigmoid mesentery as persisting into adulthood and attaching directly to the abdominal wall (Figure 1.5). At the time, his descriptions provided a welcome rationalization of what was, and still is, regarded as a complex anatomic topic (i.e., mesenteric and peritoneal anatomy in the adult human). Although some aspects of his descriptions of the mesentery and peritoneum are now regarded as inaccurate, he was correct in describing a “mesenteric root” at the origin of the superior mesenteric artery. He was also correct in describing the mesentery of the appendix as arising from the undersurface of the mesentery in the right iliac fossa. Treves’ stunning descriptions were made at a time when signi ficant advances were occurring in anatomic and
Figure 1.1 Carl Toldt (1840–1920).
Figure 1.2 Cover illustration of Anatomischer Atlas Fur Studierende und Aertze
Durchtr itt eines Ar terienzweiges durch die Tunica muscularis
Tela subserosa
Tunica serosa mesenterii
Epithelium
Lamina mesenterii propria Venenzweig Fettgewebe
Einstrahlung des Bindegewebes der Lamina mesenterii propria in die Darmwand
Tunica mucosa
Tela submucosa
9/1
Figure 1.3 The mesentery and adjacent intestine is demonstrated. Toldt drew submesothelial connective tissue as well as a mesenteric connective tissue lattice. He demonstrated a contiguity between these and the connective tissue of the outer layers of the intestine. (Taken from Carl Toldt’s Anatomischer Atlas Fur Studirende und Aertze.)
Figure 1.5 Mesenteric attachments and peritoneal anatomy in the adult human as per Sir Frederick Treves. The mesentery of the small intestine, transverse, and sigmoid colon are depicted by Treves as having linear attachments to the posterior abdominal wall. The attachment of the right and left colon is indicated (arrows). These correspond to the regions where a right or left mesocolon, if present, would be located.
Figure 1.4 Sir Frederick Treves (1853–1923).
Left colic attachment
Right colonic attachment
safe surgery, a factor that is likely to have aided in their indoctrination in mainstream literature. Not surprisingly, they were adopted comprehensively in most anatomic, embryologic, and surgical texts and to the present they form the basis of introductory chapters in reference textbooks. It is remarkable that even today, case reports continue to emerge describing the presence of a right or leftmesocolon (now known to be correct) as anomalous or pathologic [1,5,6].
LIMITED SUPPORT FOR TOLDT’S OBSERVATIONS
Toldt’s findings were supported by the observations of Broesike (1891), Vecchi (1910), Vogt (1926), and Congdon (1942) [12]. Gerota (1895) and Southam (1923) described an “anterior renal fascia” (also referred to as the lateroconal fascia or Gerota’s fascia) as being “fusional in nature,” thereby touching on Toldt’s concept of adhesion [13,14]. In a review of the topic in 1942, Congdon noted that only a single reference anatomic text mentioned Toldt’s fascia, that is, Poirier and Charpy’s text of anatomy [15]. Congdon also noted that at that time, several anatomic texts including that of Waterston, Last, Cunningham, and Grant omitted the fascia from contained illustrations. Toldt’s observations received little if any attention following Congdon’s corroboration of them. It is not known why this occurred. Reference in anatomic texts was, and to this day remains, scant. Although surgical texts can be credited with a little more emphasis, this has also remained limited [16]. The tide may be turning however as the most recent edition of reference anatomic texts such as Gray’s Anatomy acknowledge continuity of the mesentery, as well as the presence of Toldt’s fascia between mesentery and the retroperitoneum [4].
‘The mesocolon extends along the entire length of the colon and is continuous with the small bowel mesentery proximally and the mesorectum distally … Toldt’s fascia lies immediately posterior to the mesocolon, where it is adherent to the retroperitoneum of the posterior abdominal wall’ (Culligan et al. 2014).
In the main, Treves’ arguments supporting discontinuity were adopted in general and specialty literature [5,6]. Mesenteric discontinuity meant that the right and leftmesocolon were, in general, considered absent in the majority of adult humans. If they were present, then they were regarded as abnormal or pathologic. In an attempt to reconcile Treves’ descriptions with theories on the embryologic development of the mesentery, two theories were developed. These were attempts at explaining mesenteric regression or obliteration and were called the sliding and regression theories [17–19].
RADIOLOGY
One of the best ways of appraising living anatomy in its undisturbed format is through radiologic imaging. Radiologists continue to try reconciling the radiologic appearance of the mesentery and associated peritoneum, with Treves’ descriptions. Not surprisingly, many articles on the topic of mesenteric and peritoneal radiology open with a statement asserting the complexity of the fild in general [20,21].
As mentioned earlier, and in keeping with other disciplines, radiologic appraisals of mesenteric anatomy adhere to the descriptions of Treves. Earlier radiologic techniques relied on the injection or consumption of radiopaque contrast to outline the intestinal lumen. These provided limited information on structures outside the intestine, which, for the most part, had to be inferred. The groundbreaking development of computerized axial tomography (CT) and magnetic resonance imaging (MRI) meant that structures outside the intestinal tract could now be visualized. With this development, radiologists attempted to reconcile CT and MRI appearances of the mesentery, with classic anatomic teaching, and di fficulty was again encountered. To address this problem, Oliphant (1982) suggested that the mesentery was continuous with the retroperitoneum (Figure 1.6), leading to the concept of the “subperitoneal space of Oliphant” (Figure 1.6) [22]. In 1986, Dodd indicated that the then current theories of mesenteric anatomy could not be correlated with the shapes observed on CT imaging. He suggested that in order to reconcile both filds (i.e., radiologic and anatomic), the mesentery was best considered as being entirely extra-retroperitoneal
Figure 1.6 Schematic illustration demonstrating Oliphant’s interpretation of the subperitoneal space.
[23]. The theory of Oliphant gained acceptance, while that of Dodd went largely unnoticed until recently (see the “Anatomic continuity: a simpler principle” section).
More recently still, Charnsangavej et al. exploited vascular markings in order to identify mesenteric regions on abdominal CT [20,21,24]. Th is approach is practical and readily adopted, which likely explains its widespread use. However, the sentiment expressed by Dodd (that the CT appearance of the mesentery is di fficult to correlate with prevailing anatomic concepts) still holds.
RENAISSANCE IN FOCUS ON THE MESENTERY
Interest in the mesentery increased with the realization that when the mesentery associated with the rectum (i.e., the mesorectum) was fully excised for rectal cancer, the incidence of recurrent cancer decreased signifiantly. The concept was termed “total mesorectal excision.” Although total mesorectal excision had been conducted worldwide and for decades, the anatomic basis for its success was a recent discovery. In 1982, Heald et al. showed that a plane occurs between the mesorectum and the pelvis and that dissection in this plane, “the holy plane,” enabled a total mesorectal excision (Figure 1.7) [25,26]. Ths was a highly signifiant anatomic description as it provided surgeons with a failsafe anatomic roadmap, which, if adhered to, led to better outcomes for patients with rectal cancer. Initial uptake of the anatomic principle was begrudgingly slow, but it has now gained worldwide acceptance. Surprisingly, Heald and coworkers did not extrapolate the same anatomic basis to the remainder of the colon and mesocolon.
LAPAROSCOPIC AND ROBOTIC SURGERY: THE CRAFT OF COLORECTAL SURGERY
During the 1990s, the development of laparoscopic and minimally invasive surgery (and subsequently robotic techniques) revolutionized intestinal surgery by providing high magnifiation (greater than 20-fold) and high-resolution anatomic imagery. Just as the principles of laparoscopic and robotic intestinal surgery emerged, terminologies such as “mesocolon” and “Toldt’s fascia” were increasingly utilized. For laparoscopic and robotic colorectal surgery to be safe and repeatedly successful, the surgeon must adhere to a universally reproducible anatomic roadmap. Unfortunately, the anatomic basis for laparoscopic and robotic intestinal surgery was also sketchily developed [5,27]. Ths assertion may be considered as unexpected, given surgeons for decades practiced technically superb resections in the open context. It is not surprising, however, when one considers that descriptions of open, laparoscopic and robotic surgical techniques are hallmarked by limited reference to the mesentery, the associated peritoneum and fascia.
A brief illustration of this point is important at this juncture. The mesofascial plane is a key plane throughout colorectal surgery. Access to it is universally gained by division of the overlying peritoneal reflection. Peritonotomy (i.e., division) of the reflection and separation of plane components are core colorectal activities and are universally required for colorectal resection. Despite being centrally important, their anatomic basis has only recently been described.
Focus on the anatomic and surgical importance of the mesentery increased further when Werner Hohenberger described superb results for patients undergoing a “complete mesocolic excision” for colon cancer (Figure 1.8) [28].
Figure 1.7 Professor R.J. (Bill) Heald, OBE, MChir, FRCS(Ed)(Eng).
Figure 1.8 Professor Werner Hohenberger, MD, PhD.
In his 2009 article, he demonstrated that by applying anatomic principles, one could achieve an R0 resection (i.e., clearance of all microscopic disease) in 97% of cases. Around the same time, West et al. demonstrated the effcts of anatomic dissection on colon cancer outcomes. Their fi ndings suggested that by adopting a strictly anatomic approach, one could enhance patients’ survival following surgery for stage three colon cancer [29,30]. These fi ndings went a considerable distance in demonstrating the association between anatomic surgery and better cancer-speci fic outcomes.
Remarkably, however, a unifying anatomic principle that could reconcile anatomic with established surgical approaches to the colon, rectum, and small bowel remained elusive.
ANATOMIC CONTINUITY: A SIMPLER PRINCIPLE
In 2012, a study was performed involving collaboration between the Department of Surgery in University Hospital Limerick, Ireland, and the Department of Colorectal Surgery at the Digestive Diseases Institute at The Cleveland Clinic, in which the anatomic structure of the small and large intestinal mesentery was formally clarifid (Chapter 2) [31]. Crucially, the authors demonstrated that the small intestinal and colonic mesenteries are different regions of the same anatomic structure and that the mesentery itself spans the intestinal tract from the duodenum to the junction between the rectum and anus (Figure 1.9). Ths was a considerable departure from
the classic depictions as it meant that the mesenteric organ is a substantive and continuous structure, and not fragmented or discontinuous as was generally described [32,33]. The newer appraisal was far simpler than the classic description. Recognition of continuity led to similar observations on the peritoneal reflction and Toldt’s fascia. It is now accepted that Toldt’s fascia is continuous from the origin of the mesenteric organ (at the superior mesenteric artery) to its termination at pelvic flor. Similarly, the peritoneum is draped in a contiguous manner over intraperitoneal structures from the root region to the so-called anterior reflction in the pelvis [32,33].
FUTURE DIRECTIONS
Anatomic continuity and contiguity of mesentery, fascia, peritoneal reflection, and gastrointestinal tract has major implications at numerous levels and across multiple specialties (clinical and nonclinical). These form the basis and content of this book. For the surgeon, continuity and contiguity mean that the same anatomic technical elements can be universally used to perform a safe intestinal resection [33]. For the abdominal radiologist, they enable a clearer understanding of the type and extent of intraperitoneal disease [33]. Perhaps most importantly, identification of continuity and clarification of anatomy now permits the systematic (i.e., scientific) study of the mesentery and associated structures [33].
SUMMARY
Transverse colon
Transverse mesocolon
Figure 1.9 (See also QR 1 and 7.) The mesenteric organ. The illustration is of a model of the mesentery generated using a 3D printer. Pan-mesenteric continuity is demonstrated (from the duodenum to the anorectal junction).
There are numerous incidents in the history of medicine where an inaccurate understanding of structure was dogmatically integrated in literature. William Osler wrote that “the greater the ignorance the greater the dogma.” Recent clari fication of mesenteric structure has presented a far simpler structure than heretofore thought. The following chapters will describe the scienti fic opportunities that stem from this clari fication. In addition, it will explain the mesenteric basis of clinical practice.
REFERENCES
1. Treves, F., Lectures on the anatomy of the intestinal canal and peritoneum in man. Br Med J, 1885. 1(1264): 580–583.
2. McConnell, A.A. and T.H. Garratt, Abnormalities of fixation of the ascending colon: The relation of symptoms to anatomical findings. Br J Surg, 1923. 10: 532–557.
3. Netter, F.H., Atlas of Human Anatomy. Elsevier Health Sciences, Philadelphia, PA, 2014, pp. 263–276.
4. Standring, S., Gray’s Anatomy: The Anatomical Basis of Clinical Practice. Elsevier Health Sciences, London, U.K., 2015, Chapter 62, pp. 1098–1111, 1124–1160.
5. Coffey, J.C., Surgical anatomy and anatomic surgery—Clinical and scientific mutualism. Surgeon, 2013. 11(4): 177–182.
Right mesocolon
Right colon
Mesosigmoid
Mesorectum
Sigmoid colon
Rectum
Anorectal junction
Left mesocolon
6. Sehgal, R. and J.C. Coffey, Historical development of mesenteric anatomy provides a universally applicable anatomic paradigm for complete/total mesocolic excision. Gastroenterol Rep, 2014. 2(4): 245–250.
7. Toldt, C., Bau und wachstumsveranterungen der gekrose des menschlischen darmkanales. Denkschrdmathnaturwissensch, 1879. 41: 1–56.
8. Toldt, C., An Atlas of Human Anatomy: For Students and Physicians , Vol. 6: Primary Source Edition. BiblioBazaar, 2013.
9. Toldt, C. and A.D. Rosa, An Atlas of Human Anatomy for Students and Physicians . Macmillan, New York, 1926.
10. Cohen, M.M., Jr., Further diagnostic thoughts about the Elephant Man. Am J Med Genet, 1988. 29(4): 777–782.
11. Treves, F., Discussion on the subsequent course and later history of cases of appendicitis after operation. Med Chir Trans , 1905. 88: 429–610.
12. Congdon, E.D., R. Blumberg, and W. Henry, Fasciae of fusion and elements of the fused enteric mesenteries in the human adult. Am J Anat, 1942. 70: 251–279.
13. Chesbrough, R.M. et al., Gerota versus Zuckerkandl: The renal fascia revisited. Radiology, 1989. 173(3): 845–846.
14. Amin, M., A.T. Blandford, and H.C. Polk, Jr., Renal fascia of Gerota. Urology, 1976. 7(1): 1–3.
15. Poirier, P. and A. Charpy, Traité D’Anatomie Humaine Publié Sous la Direction de P Poirier et a Charpy BiblioBazaar, Charleston, SC, 2010.
16. Goligher, J., Surgery of the Anus Rectum and Colon. All India Traveller Book Seller, 1992.
17. Moore, K.L., T.V.N. Persaud, and M.G. Torchia, The Developing Human: Clinically Oriented Embryology Elsevier Health Sciences, Philadelphia, PA, 2015, pp. 210–239.
18. Sadler, T.W., Langman’s Medical Embryology. Wolters Kluwer Health, Philadelphia, PA, 2011, pp. 208–232.
19. Schoenwolf, G.C. et al., Larsen’s Human Embryology. Elsevier Health Sciences, Philadelphia, PA, 2014, pp. 341–374.
20. Charnsangavej, C. et al., CT of the mesocolon. Part 1. Anatomic considerations. Radiographics , 1993. 13(5): 1035–1045.
21. Charnsangavej, C. et al., CT of the mesocolon. Part 2. Pathologic considerations. Radiographics , 1993. 13(6): 1309–1322.
22. Oliphant, M. and A.S. Berne, Computed tomography of the subperitoneal space: Demonstration of direct spread of intraabdominal disease. J Comput Assist Tomogr, 1982. 6(6): 1127–1137.
23. Dodds, W.J. et al., The retroperitoneal spaces revisited. Am J Roentgenol, 1986. 147(6): 1155–1161.
24. Coffey, J.C. et al., An appraisal of the computed axial tomographic appearance of the human mesentery based on mesenteric contiguity from the duodenojejunal flexure to the mesorectal level. Eur Radiol, 2016. 26(3): 714–721.
25. Heald, R.J., The “Holy Plane” of rectal surgery. J R Soc Med, 1988. 81(9): 503–508.
26. Heald, R.J., E.M. Husband, and R.D. Ryall, The mesorectum in rectal cancer surgery—The clue to pelvic recurrence? Br J Surg , 1982. 69 (10): 613–616.
27. Coffey, J.C. et al., Terminology and nomenclature in colonic surgery: Universal application of a rule-based approach derived from updates on mesenteric anatomy. Tech Coloproctol, 2014. 18 (9): 789–794.
28. Hohenberger, W. et al., Standardized surgery for colonic cancer: Complete mesocolic excision and central ligation—Technical notes and outcome. Colorectal Dis , 2009. 11(4): 354–364; discussion 364–365.
29. West, N.P. et al., Pathology grading of colon cancer surgical resection and its association with survival: A retrospective observational study. Lancet Oncol, 2008. 9(9): 857–865.
30. Coffey, J.C. and P. Dockery, Colorectal cancer: Surgery for colorectal cancer—Standardization required. Nat Rev Gastroenterol Hepatol, 2016. 13(5): 256–257.
31. Culligan, K. et al., The mesocolon: A prospective observational study. Colorectal Dis , 2012. 14 (4): 421–428; discussion 428–430.
32. Coffey, J.C. et al., Mesenteric-based surgery exploits gastrointestinal, peritoneal, mesenteric and fascial continuity from duodenojejunal flexure to the anorectal junction—A review. Dig Surg , 2015. 32(4): 291–300.
33. Coffey, J.C. and D.P. O’Leary, The mesentery: Structure, function, and role in disease. Lancet Gastroenterol Hepatol 1(3): 238–247.
Mesenteric and peritoneal anatomy
J. CALVIN COFFEY, PETER DOCKERY, BRENDAN J. MORAN, AND BILL HEALD
There is pleasure in recognising old things from a new viewpoint.
Richard Feynman
AIM
The aim of this chapter is to summarize mesenteric and peritoneal structure in light of recent advancements in our understanding of both. A second aim is to indicate the relevance of both to current clinical practice.
INTRODUCTION
The magnification affrded by endoscopic techniques coupled with the resolution of modern displays has revolutionized our appraisal of living anatomy. Nevertheless, reference anatomic and embryologic texts continue to present classic anatomic descriptions. In keeping with this, classic descriptions of mesenteric and peritoneal anatomy continue to dominate reference texts. Sir Frederick Treves comprehensively described the human mesentery and peritoneum in a study spanning 100 cadavers in 1889 (Figure 2.1) [1].
His descriptions were first presented in a series of classic lectures and therea fter integrated in most reference anatomic, embryologic, surgical, and radiologic texts [1–11]. Treves laid down his understanding of mesenteric and peritoneal anatomy at a time when anatomic descriptions were providing a formal basis for safe and anatomic surgery (Figure 2.1) [1,9].
Treves correctly described the small intestinal mesentery as having a “mesenteric root” at the origin of the superior mesenteric artery. According to his descriptions, the small intestinal mesentery then fans out from the duodenum to terminal ileum. At the gastrointestinal margin, the mesentery elongates considerably. Th is contrasts considerably with the length of the “attachment” to the posterior abdominal wall. As per Treves, the mesenteric attachment extends across the posterior abdominal wall from duodenojejunal flexure to ileocecal level. As it does so, it obliquely traverses the aorta and inferior vena cava (Figure 2.2a and b) [1,12].
Treves described the right and leftmesocolon as being absent in the majority of cases. If an anomalous right or left mesocolon was present, then this would be seen to attach in regions corresponding closely to the attachment of the right or leftcolon (Figures 2.1 and 2.2a,b). For example, the
of the right
that
Attachment of right colon
Mesenteric attachments: classic teaching
Attachment of small intestinal mesentery
Attachment of transverse mesocolon
Attachment of left colon (i.e., left mesocolon)
Attachment of mesosigmoid
Figure 2.1 Schematic demonstrating the attachments of the mesentery as depicted by Treves. The small intestinal mesentery attaches along a diagonal line crossing the posterior abdominal wall from the fourth part of the duodenum to the ileocecal junction.
Mesentery and attachments: classic vs. current
Mesenteric attachments: classic teaching
Left mesocolon
Mesosigmoidal attachment
Mesentery: classic teaching
Transverse mesocolon
Vestigial left mesocolon
Mesosigmoid
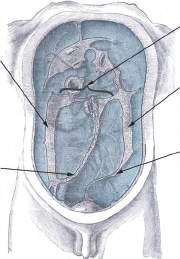
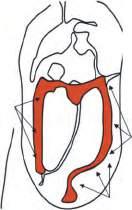
Figure 2.2 (a) Schematic summarizing Treves’ descriptions of the attachment of the mesentery and mesocolon (red region). As per Treves, when an anomalous right mesocolon is present, it attaches along a vertical trajectory from the right iliac fossa to the hepatic flexure. The transverse mesocolon attaches along a horizontal line that traverses the upper part of the abdomen. When an anomalous left mesocolon is present, it attaches along a vertically oriented region, while the mesosigmoid attaches along a v-shaped line. The attachment of the mesorectum was not defined by Treves. (b) 2.5D snapshot from a 3D digital sculpture of the mesocolon (yellow) as depicted by Treves. The small bowel and associated mesentery have been conceptually removed for clarity. The right and left mesocolon are vestigial or near absent, while the transverse and sigmoid regions are substantial. The mesorectum is absent. Overall, the mesentery is fragmented and discontinuous. (Continued )
Right mesocolon
Right mesocolic and small bowel mesenteric attachment
Mesenteric attachments: current teaching
Left mesocolic attachment
Mesosigmoidal attachment
Mesentery: current teaching
Left mesocolon
Mesosigmoid
Mesorectum
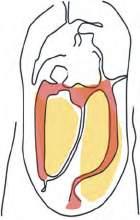
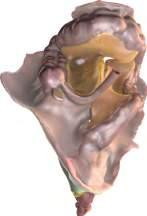
Figure 2.2 (Continued ) (c) Schematic summarizing the attachment of the mesocolon (yellow region) as described by Toldt. The right mesocolon is always present and attaches over a broad region on the right side of the posterior abdominal wall. The left mesocolon is always present and attaches over a similarly broad region on the left side of the abdomen. The mesosigmoid is a distal continuation of the left mesocolon. (d) (See also QR 1/1.) 2.5D snapshot from a 3D digital sculpture of the mesocolon (yellow) as it is currently understood. The distal small bowel and associated mesentery have been retained in the illustration. The right and left mesocolon are substantial and continuous with adjacent regions of mesentery. The right mesocolon is continuous with the small intestinal mesentery medially and with the transverse mesocolon at the hepatic flexure. On the left, the left mesocolon, mesosigmoid, and mesorectum are similarly continuous. Overall, the mesentery is continuous from root region to the mesorectum.
the right colon, extending along a vertical orientation from the right iliac fossa to the subhepatic region. The attachment of the leftmesocolon corresponds to that of the leftcolon, extending from the subsplenic region to the leftiliac fossa (Figures 2.1 and 2.2a, b) [1]. To the present, many reference texts continue to describe these regions as the attachments of the right and left olon or mesocolon [3–5,13,14].
Treves’ description of the transverse and sigmoid mesocolon was similar to that of the small intestinal mesentery. He described the transverse mesocolon as being “attached” along a horizontal trajectory to the upper part of the posterior abdominal wall (Figure 2.2a and b). He described the mesosigmoid as attaching to the posterior abdominal wall in the left iliac fossa. The attachment followed an inverted V shape, with the apex of the “V” providing an important landmark overlying the leftureter (where this crosses the bifurcation of the common iliac artery) (Figure 2.2a and b) [2,4,6,14,15].
The mesosigmoid, transverse mesocolon, and small intestinal mesentery were described as mobile, while the right and leftmesocolon were described as absent (or vestigial) [4,6,8,9,13,14]. According to this, the mesenteric organ is fragmented (present in some regions, absent in others). If this description were correct, then one would expect to identify start and end points for each mesenteric region. These were never described, a point that is explained by their absence in the fi rst place [10].
A question arises as to how Treves’ generated his fidings. His descriptions can be explained if one were to conceptually slice through the posterior region of the abdomen in a coronal plane, that is, (1) posterior to the right and leftcolon and (2) at the level where the small intestinal mesentery attaches to the posterior abdominal wall (Figures 2.1 and 2.2b). Doing this would generate the impression of a series of mesenteric insertions for the small intestine, transverse, and sigmoid mesocolon [10,16,17]. In addition, it would fail to identify the right and leftmesocolon as well as the attached region of the mesosigmoid and mesorectum.
In 2012, our group refuted the findings of Treves demonstrating mesenteric continuity from small intestinal mesentery to mesorectal level (Figure 2.2c and d) [10]. This led to a general overhaul of our understanding of mesenteric anatomy [2]. We found that the small intestinal mesentery attaches to the posterior abdominal wall and extends laterally as the right mesocolon (Figures 2.2c , d , 2.3, 2.4). Along the line of attachment, a peritoneal reflection extends from the small intestinal mesentery to the posterior abdominal wall and bridges the gap between the two. The line along which the small intestinal mesentery attaches to the posterior abdominal wall (and continues laterally as the right mesocolon) extends diagonally from the duodenojejunal junction to the ileocecal level.
Peritoneum, mesentery, fascia, and intestine
Mesentery, fascia, and intestine
Mesentery and intestine
Figure 2.3 (a) (See also QR 2/1.) 2.5D snapshot from a 3D digital sculpture of the mesentery, associated peritoneal reflection, and large bowel. Just as the mesentery is contiguous so too is the peritoneal covering and associated large bowel. (b) Same model as in (a) but with peritoneum removed. (c) Same model as in (b) but with peritoneum and fascia removed. (d) Same model as in (c) but peritoneum, fascia, and colon removed.
MESENTERIC ANATOMY
Mesenteric root region
The following is a description of mesenteric anatomy as it is currently understood. Before commencing, it is important to defi ne the terms “attachment” and “suspension.” “Attachment” refers to the flattening of the mesentery against the posterior abdominal wall so the mesentery becomes apposed to the retroperitoneum. As will be seen from the following, the mesentery does not “insert” into the posterior abdominal wall in any location. “Suspension” refers to the suspension of the mesentery to the posterior abdominal wall at vascular points of suspension.
The mesentery fans out from the “root region” where the superior mesenteric artery suspends it to the posterior abdominal wall. Th is was correctly described by Treves [1]. From this point, the mesentery expands, like a Chinese fan. In some regions, it is mobile while in others it is attached to (i.e., flattened against) the posterior abdominal wall. The continuous mesentery spans the intestine from duodenojejunal to anorectal junction.
Mesentery in the right iliac fossa
In the right iliac fossa, the mesentery tapers toward an apex at the ileocecal junction. Ths region of mesentery can be
arbitrarily called “the ileocecal mesenteric confluence,” a term that is descriptively useful (see section “Flexural anatomy”). A fatty appendage (the mesoappendix) extends from the under surface of the ileocecal mesenteric confluence (Figure 2.5a through c). Retromesenteric origin of the mesoappendix explains how the appendix often occupies a retrocecal location (the clinical relevance of this will be expanded on in Chapter 7) (Figure 2.5a through c). Treves correctly described the mesoappendix as originating from the undersurface of the mesentery in the ileocecal region [1,12].
The ileocecal mesenteric confluence is a substantive tissue mass separated from the retroperitoneum by Toldt’s fascia. When the abdomen is first entered, the confluence is obscured from direct view by a peritoneal reflection. This is an extension of the peritoneal reflection at the base of the small intestinal mesentery. Regions of the peritoneal reflection are of surgical and pathobiologic importance, as mobilization of the mesentery requires their division to permit access to surgical planes. In addition, they act as a mechanical barrier to the spread of submesenteric disease (see Chapters 6 and 7) [18].
Small intestinal mesentery
Though the base of the small intestinal mesentery (i.e., where it continues as the right mesocolon) is short, the intestinal margin of the small intestinal mesentery is approximately 4 ftin length [10,18]. As a result, the mesentery
Mesentery
(d)
(c)
(a)
(b)
Legend
Mesentery
Peritoneum
Colon Fascia
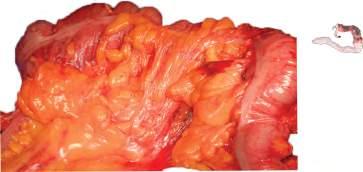
Small intestinal mesentery and right mesocolon
Small intestional mesentery
Figure 2.4 (a) (See also QR 3/1.) 2.5D snapshot of a 3D digital sculpture of the small bowel mesentery and right mesocolon. The model has been sectioned and the point of view is looking from above downward. The small intestinal mesentery is continuous with the right mesocolon. (b) (See also QR 4/1.) The model used in (a) has been sectioned through at the same level, but the point of view now is from below upward. The small intestinal mesentery is continuous with the right mesocolon. (c) Cadaveric demonstration of continuity between the small bowel mesentery and right mesocolon. (d) Intraoperative image depicting mesenteric and mesocolic continuity.