IMPLEMENTATION GUIDE



HOW TO USE THE TIMM TRAINING PROGRAM
Phase 1: Readiness and Planning
2: Training and Capacity Building
Suggested Training Task/Timeline List
Sample Welcome Letter for Participants
Face/Demographic Sheet
Opening Minds Survey
National Child Traumatic Stress Network (NCTSN) 12 Core Concepts
Community/Referral Resource Guide
E L C O M E

WestCare is a global family of nonprofit organizations providing treatment and rehabilitation, mental health and wellness services, emergency support, housing opportunities, education and prevention, criminal justice services, domestic violence support, and Veteran services. We empower everyone we encounter to engage in a process of healing, growth, and change, benefiting themselves, their families, co-workers, and communities. We achieve this through our efforts toward “Uplifting the Human Spirit” by consistently improving and strengthening everything we do to build for the future.
We are proud to provide you with the Trauma-Informed Ministry Model (TIMM) Training Program Implementation Guide, a framework designed to support faith-based organizations in their mission to foster mental wellness within their communities. At WestCare, we are dedicated to eradicating stigma and empowering community leaders to become wellness ambassadors.
This TIMM Training Program Implementation Guide will equip faith-based organizations with resources, evidence-based materials, and support systems to develop an effective trauma-informed ministry. Our intention is to encourage understanding and acceptance. With passion and creativity, every community can benefit from this framework.
We are excited that you have decided to join us in this important work and make a lasting impact on your community. Together, we are “Uplifting the Human Spirit.”

INTRODUCTION OF THE IMPLEMENTATION GUIDE
This implementation guide is a comprehensive resource designed to help organizations establish Trauma-Informed Wellness Ambassadors, empowering them to foster holistic wellness within their communities. By providing evidence-based materials, support systems, and essential resources, the TraumaInformed Ministry Model (TIMM) Training Program equips ambassadors to make a meaningful impact on community wellbeing. At the heart of this approach is the belief that every community has the potential to benefit from trauma-informed practices, especially when applied with creativity, passion, and purpose.
The TIMM Training Program is designed for faith-based organizations (FBOs) seeking to develop a robust wellness ministry or program that promotes healing, resilience, and spiritual well-being. We believe this should be embraced with passion and creativity, honoring the unique culture and needs of each faith-based community.

KEY TERMS & ROLES
As you review this guide, note the important terms and roles essential to the TIMM Training Program. Below are definitions of the terms and roles used in the TIMM Training Program.
TERMS
Curriculum: An evidence-based training course to be provided to Wellness Ambassadors. Based on the programming, some curricula may be adjusted for the target audience (e.g., youth, adults, teens, etc.).
Faith-Based Organization (FBO): A faith-based organization is an entity whose values are founded on faith and beliefs, with a mission rooted in the social values of the faith, and which typically draws its activists (leaders, staff, volunteers) from a particular faith group.
The National Child Traumatic Stress Network (NCTSN) has identified 12 Core Concepts that are essential for understanding the impact of trauma on children and adolescents. These concepts help frame how trauma affects development, behavior, and relationships (See Resource Section)
One-on-one Meetings: Sometimes, due to the nature and severity of discussions, a participant may need to have a “one-on-one” discussion to ensure they are still in a good place to complete the training/discussions.
Evidence-Based Program/Practice (EBP): These are programs/practices that are an integration of scientific evidence, patients' values, and one's own judgment to make the best possible decision.
Psychological First Aid (PFA): An evidence-informed modular approach to help children, adolescents, adults, and families in the immediate aftermath of disaster and trauma events Whether survivors, witnesses, or responders to such events, individuals may struggle with or face new challenges in the aftermath of the event. PFA was developed by the National Child Traumatic Stress Network and the National Center for PTSD, with contributions from individuals involved in disaster research and response. This is an online self-paced course.
Verbal Intervention (VI): Prepares individuals to identify, respond to, and prevent low-risk crisis behavior with verbal intervention techniques This can be taught with trauma or mental health-specific information. Crisis Prevention Institute-certified instructors provide this course.
Skills for Psychological Recovery (SPR): Aims to help survivors gain skills to manage distress and cope with post-disaster stress and adversity. This course utilizes skills-building components from mental health treatment that have been found helpful in a variety of posttraumatic situations Research suggests that a skills-building approach is more effective than supportive counseling. SPR is appropriate for developmental levels across the lifespan and is culturally informed This is an online self-paced course
Mental Health First Aid (MHFA): Teaches participants how to identify, understand, and respond to signs of mental health and substance use challenges among youth or adults Participants build the skills and confidence they need to reach out and provide initial support to those who are struggling. They also learn how to help connect them to appropriate support Adult or Youth MHFA can be taught depending on the FBO's focus This course is provided by National Council for Mental Wellbeing-certified MHFA instructors.
ROLES
Partners: Programming is more successful with partnerships that provide the support that brings additional assistance to those in need These relationships can also be leveraged for referrals that provide valuable resources. These can include, but are not limited to: other FBOs business associations nonprofit organizations sponsors
Presenter/Trainer (PTs): This role serves as the primary guide and instructor for the TIMM program or cohort These individuals need to be trained as trainers of the curriculum that is to be implemented.
TIMM Trauma-informed Wellness Ambassador: This is a compassionate individual trained to provide immediate support and guidance in times of crisis, with specialized training in Faith-Based Psychological First Aid (PFA), Crisis Prevention Institute’s (CPI) Verbal Intervention, and Mental Health First Aid (MHFA) Ambassadors are equipped to recognize signs of trauma, respond empathetically, and help individuals feel safe, valued, and heard With skills in de-escalation techniques, ambassadors will be able to help diffuse tense situations and promote respectful, empathic communication. They are skilled at assessing the needs of individuals and providing supportive interventions to connect them with the appropriate resources
HOW TO USE THE TIMM TRAINING PROGRAM
We encourage you to adopt the TIMM Training Program with passion and creativity, tailoring it to the unique needs and characteristics of your community. Participants can use the TIMM Training Program to support the development of their leadership as trauma-informed Wellness Ambassadors.
The target audiences for the TIMM Training Program include, but are not limited to, faithbased organization leadership, youth group leaders, educators, parents, and volunteers.
The TIMM Training Program aligns with the values, mission, and community role of faith organizations in several key areas of strength by fostering compassion, care, and community building. It enables leaders to effectively respond to and refer individuals with mental health needs in a Community-Centered Approach. The program encourages breaking stigma through conversations and education around mental health. It provides skills for responding to crises with calm and compassion. It helps to empower leaders and


Central to the TIMM program are the Substance Abuse and Mental Health Services Administration’s (SAMHSA) Eight Dimensions of Wellness, which collectively contribute to an individual’s overall wellness and life balance. These dimensions include emotional, environmental, financial, intellectual, occupational, physical, social, and spiritual wellness.
1 Emotional: Coping effectively with life and creating satisfying relationships.
2 Environmental: Good health by occupying pleasant, stimulating environments that support well-being.
3.Financial: Satisfaction with current and future financial situations.
4.Intellectual: Recognizing creative abilities and finding ways to expand knowledge and skills.
5 Occupational: Personal satisfaction and enrichment from one’s work.
6 Physical: Recognizing the need for physical activity, diet, sleep, and nutrition.
7.Social: Developing a sense of connection, belonging, and a well-developed support system.
8.Spiritual: Expanding a sense of purpose and meaning in life.
Each dimension highlights a specific area of life that, when nurtured, enhances an individual’s resilience, stability, and capacity to thrive. By addressing these interconnected facets, the TIMM Training Program Implementation Guide helps ambassadors guide communities towards greater wellness, allowing individuals to build a more fulfilled and balanced life.
RECOMMENDED SOLUTIONS FOR EFFECTIVE IMPLEMENTATION
To facilitate a seamless and impactful implementation of the TIMM Training Program, we offer a series of recommended solutions grounded in data-driven insights and lessons learned from past experiences. Each recommendation has been carefully crafted to address common challenges and support the successful adoption and integration of TIMM practices. These solutions are designed to be flexible and scalable, allowing for customization to meet the unique needs of diverse communities and organizational structures.
Establish Clear Program Objectives and Goals. Define specific, measurable, and achievable goals for your TIMM Program to ensure that everyone involved has a shared understanding of its purpose and expected outcomes. This will foster alignment and provide a clear framework for measuring progress.
Invest in Comprehensive Training and Education. Offer comprehensive, ongoing training for all stakeholders, focusing on trauma-informed principles, resilience-building practices, and culturally sensitive approaches. This training should be revisited periodically to reinforce core concepts and integrate new insights as the program evolves.
Build a Supportive Community Network. Engage a wide network of participants, including community leaders, educators, mental health professionals, and peer mentors, to create a collaborative support system. This community-based approach will encourage knowledgesharing, foster peer support, and provide a stable network for both staff and participants.
Leverage Data Collection and Feedback Mechanisms. Implement data collection methods to regularly monitor program outcomes, participant satisfaction, and areas for improvement. These insights can then be analyzed and used to adapt and refine program strategies, ensuring the TIMM Training Program remains responsive to community needs.
Encourage Flexibility and Adaptability in Implementation. Recognize that different communities may have unique cultural, social, and logistical needs. The TIMM Training Program should be adapted to fit these specific contexts, allowing it to be more effective and inclusive in diverse settings.
Prioritize Self-Care for Program Facilitators. Since the TIMM Training Program facilitators often work directly with individuals affected by trauma, it is crucial to promote a culture of self-care among staff. This includes access to mental health resources, regular debriefing sessions, and structured support for managing compassion fatigue.
Implementing Ongoing Fidelity Monitoring and Assessment. Develop a system for regularly monitoring fidelity through periodic assessments, such as facilitator selfassessments, peer reviews, and external evaluations. This process should involve spotchecks, recorded sessions (if possible and ethical), and feedback forms to gauge consistency across all program delivery points.
By incorporating these solutions, the TIMM Training Program can be implemented more effectively, creating a resilient, trauma-informed environment that is adaptable to varying contexts and continually improved based on feedback and data-driven insights.

RECOMMENDED MARKETING
This section offers practical guidance on marketing the Trauma-Informed Ministry Model (TIMM) Training Program to faith-based organizations and a broader general audience. Effective marketing ensures that the TIMM Training Program reaches faith-based organizations and community partners who are positioned to apply trauma-informed principles in meaningful and sustainable ways.
Marketing Principles
Marketing the TIMM Training Program is grounded in the same trauma-informed values that shape the program itself. All outreach efforts should reflect:
Consistency and Trust: Use consistent branding, tone, and messaging across all platforms to establish credibility and recognition.
Cultural and Spiritual Sensitivity: Honor the language, values, and structure of faithbased communities while remaining inclusive and respectful of diverse traditions.
Mission Alignment: Clearly connect the TIMM Training Program to each organization’s mission and to the shared goals of faith communities—healing, compassion, and service.
Clarity and Accessibility: Communicate the purpose, benefits, and outcomes of the TIMM Training Program in clear, approachable language.
Target Audiences
Marketing efforts should be tailored for the following primary audiences:
1.Faith-Based Organizations and Leadership
Pastors, ministry leaders, and any other faith-based staff
Churches, ministries, and faith-affiliated nonprofits
2 Organizational Internal and External Audiences
Organization staff and leadership
Community partners, referral sources, and stakeholders
Individuals already engaged with the organization’s services
Each audience may require slightly different messaging while maintaining consistent visual branding and core themes.
Core Messaging
All TIMM Training Program marketing materials should consistently communicate: What TIMM is: A trauma informed training model designed specifically for faith-based organizations
Why it matters: Trauma impacts individuals, families, and congregations, and faithbased organizations are often on the front lines of response
Who it is for: Faith-based organizations and community-facing organizations
The outcome: Stronger, safer, more compassionate leadership equipped to respond to trauma
Messaging should emphasize empowerment, hope, and practical application rather than clinical language.
Branding and Visual Consistency
To build recognition and trust, all marketing materials should maintain consistent branding, including:
Logos, colors, fonts, and design elements aligned with the organization’s brand standards
Unified look and feel across digital and print materials
Repeated use of recognizable phrases and taglines connected to the TIMM Training Program and the presenting organization
Consistency across social media graphics, paper flyers, event invitations, email communications, and presentations reinforces program legitimacy and professionalism.
Marketing Channels and Tools
A multi channel approach allows the TIMM Training Program to reach audiences where they are most engaged:
Digital Marketing
Branded social media posts highlighting training benefits, upcoming sessions, and testimonials
Email invitations and newsletters to faith leaders and partners
Event pages or registration links shared across platforms
Print and In‑Person Outreach
Paper flyers distributed to churches, faith networks, and community spaces
Branded invitations for training, informational sessions, and speaking engagements
Presence at faith-based events, meetings, and conferences
All materials should clearly direct audiences to the next steps, such as registration, contact information, or informational sessions.
Messaging Tone and Voice
The tone of the TIMM Training Program marketing should be:
Hope centered and encouraging
Strength based rather than deficit-focused
Accessible to both faith leaders and community partners
Reflective of trauma-informed principles (safety, trust, empowerment)
IMPLEMENTATION PHASES
PHASE 1: READINESS AND PLANNING
The Phase 1 planning process ensures that leadership is aligned and ready for implementation The staff and congregants will be engaged Participants are prepared for a meaningful learning experience. The community is equipped to sustain trauma-informed ministry practices long term
To ensure a productive and impactful TIMM Training Program, the following structure and best practices are recommended as part of Phase 1 This phase is to prepare leadership and participants to implement the TIMM program successfully and to foster a traumainformed, healing-centered community.
1. Leadership Commitment
Secure leadership buy-in from faith-based organization leadership, board, and other key participants.
Identify a TIMM Champion or Coordinator to serve as the primary point of contact for the initiative and support its sustainability
2. Readiness Assessment
Conduct a trauma-informed self-assessment of current FBO practices (use the TIMM Self-Assessment Tool, see Appendix).
Survey staff and congregants to assess training needs and interest
Identify opportunities and barriers to integrating trauma-informed practices.
3. Implementation Team Formation
Form an interdisciplinary implementation team (staff, congregants, mental health professionals).
Clearly define roles and responsibilities for team members
Schedule regular team planning meetings during the implementation period.
4. Participant Recruitment & Intake
Application/Intake Process
Utilize an application or intake process to gauge participants' readiness and baseline mental health knowledge.
Intake forms (i.e., FACE Sheet) help trainers understand participants’ needs and determine appropriate group size
Intake can also help limit class size if necessary and promote cohort cohesion.
Orientation / “Session Zero”
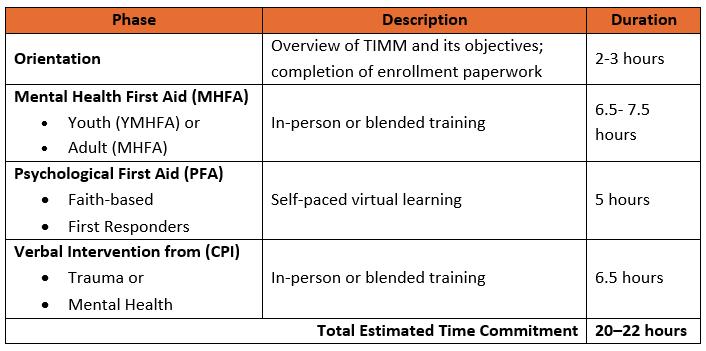
You can start the model by hosting an Orientation session (2-3 hours) to introduce the TIMM Training Program objectives and components.
Use this session to:
Set clear expectations for Trainers and Participants
Address sensitive topics in person
Complete enrollment paperwork
Distribute participant materials
Build initial cohort connections
Optional: hold an information session in advance for interested participants.
PHASE 2: TRAINING & CAPACITY BUILDING
Phase 2 focuses on building the knowledge, skills, and capacity of clergy, ministry leaders, staff, and volunteers to implement trauma-informed ministry practices and to support healing within their congregations and communities.
This phase provides practical trauma-response tools (PFA). Give participants crisis prevention and de-escalation skills (Verbal Intervention). Enhance mental health literacy and early intervention skills (YMHFA).
Training
Psychological First Aid (PFA): Provides practical tools to support congregants in the aftermath of trauma. Teach participants to utilize core PFA actions in real-time posttrauma responses, promoting safety, stabilization, and connection, while also enhancing coping and resilience.
Delivery - Self-paced online (5 hours), 8 interactive modules, and certification Skills for Psychological Recovery (SPR) may be offered as supplemental training following PFA. It teaches coping skills and long-term recovery strategies for traumaimpacted individuals and families.
Verbal Intervention from CPI (CPI) Trauma Version: Trains everyone in de-escalation techniques grounded in trauma-informed care, safety-centered interventions that prioritize Care, Welfare, Safety, and Security℠. Helps to manage escalating behaviors while preserving dignity and reducing harm. It will equip TIMM teams with protocols for managing crisis situations compassionately, post-crisis reflection, and restorative practices.
In-person or blended/virtual (6.5 hours), Scenario-based learning, and practice of verbal de-escalation skills and safety interventions
Mental Health First Aid (MHFA) or Youth Mental Health First Aid (YMHFA): Equips participants to identify signs of mental health challenges in youth, respond effectively to youth experiencing mental health and substance use challenges, and provide initial help and connect individuals to appropriate supports. The youth curriculum has a special focus on trauma, self-care, bullying, and the impact of social media.
Delivery - In-person (6.5 hours) OR Blended (2-hour self-paced + 4.5–5.5-hour instructor-led)
Session Planning & Implementation Considerations
Schedule sessions to accommodate participant availability. Cohort-based (singleorganization) sessions should be scheduled with the organization's designated representative in a flexible manner. Community-based cohorts can be scheduled with set dates and times in advance for broader community participation. When scheduling, ensure to plan to provide breaks and create space for processing sensitive discussions and scenarios.
Session components should include clearly outlined session goals, learning outcomes, and key questions that align with the objectives. The activities will be interactive exercises and real-life scenarios for skill practice. Conduct pre- and post-assessments for each training component to measure learning and gather feedback.
TIMM Training Program Model & Structure
MHFA
10 participants max per instructor, (blended/virtual) / 30 max (in-person)
2 instructors max
5 participants minimum required
PFA
Self-paced virtual training
CPI
15 participants max per instructor, (blended/virtual) / 40 max (in-person)
2 instructors max
5 participants minimum required
Flexible Scheduling
The TIMM Trainer should collaborate with the organization to customize a schedule that accommodates participants’ needs and availability.
Conclude Phase 2 with a celebration ceremony or an informal gathering that recognizes participant accomplishments, including a certificate presentation, group reflection, and a storytelling session. This will reinforce a sense of community and ongoing commitment to trauma-informed ministry.
By completing Phase 2, your organization will have established a core team of trained, confident leaders who are now Wellness Ambassadors, equipped to recognize and respond to trauma, support resilience and healing within the congregation, and foster safe and compassionate faith communities.
This capacity-building phase lays the foundation for the ongoing integration of traumainformed practices into every aspect of the faith-based organization.
After completing the initial TIMM Training programming, you can offer additional sessions on topics such as advanced trauma-informed care, resilience-building, self-care for faith leaders, and grief and loss.
PHASES 3 & 4: EVALUATION & SUSTAINABILITY
Phase 3 is to help TIMM Training Program-certified organizations measure impact and guide continuous improvement. Program evaluation is the systematic collection and analysis of data to assess the effectiveness of the program, guide improvements, and demonstrate value to stakeholders.
Evaluation Goals should include ensuring accountability and transparency to funders and community partners, continuous program quality and improvement, and contributing to the evidence base for trauma-informed ministry. The evaluation should monitor changes in knowledge, attitudes, behaviors, and resilience among participants and the broader community.
Key Evaluation Components:
Process Evaluation - Examine program delivery: participation rates, session completion, adherence to protocols. Key question: Is the program being delivered as intended?
Outcome Evaluation - Measure participant change: knowledge, attitudes, behaviors, and skill application. Key question: Is the program achieving its intended effects?
Impact Evaluation - Assess long-term outcomes: organizational culture shifts, stigma reduction, strengthened community supports. Key question: What lasting changes occur because of program participation?
TIMM Recommended evaluation tools:
Pre- and post-assessments for the entire program to measure stigma reduction, such as the Opening Minds Survey for Health Care Providers (OMS-HC).
Pre- and post-surveys for in-person/virtually delivered curriculum.
Track certifications in YMHFA, PFA, and VI.
Conduct 6-month post-program follow-up surveys to assess application of skills and program impact in congregational settings.
Based on the project design, the following is a simplified version of the program logic model, which utilizes evidence-based practices/programs (EBPs) as its theory of change and a validated tool to measure outcomes. The logic model constructs flow chronologically from left to right.
Trainers certified in EBP facilitation
EBP curriculum materials
Zoom/Teams
subscription
Survey Monkey subscription
Program Director
Evaluator Program plan
Community outreach and recruitment
Orientation/Assessm
ent
PFA training
CPI training
YMHFA training
Post Assessment
Graduation
Follow-up
Creating partnerships with local providers and developing referral pathways
Clergy and congregants registering for TIMM
Training Program
Baseline OMS-HC scores
PFA certifications
CPI certifications
YMHFA certifications
Follow-up OMS-HC
scores
TIMM Training Program
graduates
Qualitative data on TIMM impact
Localized referrals pare pathway resource guides
Lowered stigma towards serving people experiencing mental health challenges
Clergy, congregants, and community members are receiving support and timely hand-offs to professional help
Often found in the project budget, but also includes in-kind resources
Often found in a project timeline and detailed in the project narrative
Often relates to the project goals and objectives that produce physical deliverables
Often relates to the project goals and objectives that produce abstract deliverables
Often relates to the impact or intended vision for the project
For data collection, we recommend integrating evaluations into the program’s flow, including pre-assessments at orientation and post-assessments at the final session. Be sure to use both quantitative (survey scores) and qualitative (participant feedback, success stories) data. Assign a dedicated staff member to manage data collection and ensure fidelity. This could be the trainer, the point person for an FBO, or, if available, an individual specializing in data and research.
Some common challenges you may face include survey fatigue, follow-up attrition, and the trade-off between technology and paper-based access. To address survey fatigue, we recommend limiting data collection to essential items and focusing on the “meaningful use” of participant information. For follow-up attrition, consider maintaining ongoing engagement with participants and alumni through newsletters, support groups, continuing education opportunities, and attending community events. If you have access, consider incentives to encourage follow-up participation. When considering technology versus paper, ensure that you select an assessment modality that aligns with your program delivery (virtual or inperson) and staff capacity. Clearly document processes to ensure consistency.
For continuous quality improvement, adopt CQI practices (Lean, Six Sigma, Root Cause Analysis) to identify and resolve operational issues. Ensure the use of EBP fidelity checklists to ensure consistent delivery of core components. Always involve program staff and participants in ongoing feedback loops to drive iterative improvements.
It is vital to celebrate and share successes, as this helps sustain momentum and fosters a trauma-informed community. You can do so through documenting and sharing stories. Collect and showcase testimonials, success stories, and case studies of hope, healing, and resilience. Use multimedia (videos, newsletters, social media, congregational reports) to amplify these stories.
Host recognition events to celebrate program graduates with ceremonies or informal gatherings. Have ways to recognize leaders and volunteers who embody trauma-informed faith values. Share key outcomes and lessons learned with broader faith and community networks to inspire ongoing engagement and support.
APPENDIX
The TIMM Training Program appendix has been created to provide you with the tools used in implementing the TIMM Training Program, as well as a rich collection of supplemental resources. Together, these appendices are your companion for embedding the TIMM Training Program’s Service, Encouragement, Passion, and Transformation in real-world contexts.
Included, you'll find:
Suggested Training Task/Timeline List
Sample Welcome Letter for Participants
Face/Demographic sheet
Opening Minds Survey
The National Child Traumatic Stress Network (NCTSN) 12 Core Concepts
Sample Community/Referral Resource Guide
Sample TIMM Interest Meet-Up Flyer
Name:
TRAINING TASK/TIMELINE LIST
Date of Training:
6 WEEKS OR MORE PIOR DATE
Interest meetup - pre-scheduled or scheduled separately – PowerPoint
Consultation with MPC and scheduling (Time, Virtual or in person, Participants)
Confirm the date, time, and location
Create an Eventbrite collection with all dates and training specified.
Virtual Cohorts: create Zoom links for each day of training and attach to Eventbrite pages.
Send the Eventbrite link to marketing to WestCare Brand and to generate a registration flyer
Acquire emails/contact information for each participant
Send out the registration flyer to all participants
3 TO 4 WEEKS PRIOR
On an ongoing basis, monitor Eventbrite registration
Get an update/ re-confirm the location and time for the 0 module (orientation)
In Person, check for: seating arrangement spacing technology requirements
Virtual: Arrange for pick-up or shipment of physical training materials. Face sheets, opening minds, and consent forms are completed via a survey link.
In-person: Host Zero Module: ensure all registration is complete hand out training materials explain CPI/YMHFA pre-work have participants complete the following: face sheet open mind pre media consent informed consent
In-person: Scan the paperwork and submit it to the research team.
Register participants for CPI pre-work (if needed for blended course)
Register participants for YMHFA pre-work
Send a reminder email to complete CPI & YMHFA pre-work
Purchase snacks, prizes, and any other materials needed for class
On an ongoing basis, monitor email and CPI/YMHFA progress - assist with CPI/YMHFA prework when necessary
Pre-type printed awards with participants the day before, in case of changes
1 DAY PRIOR
Set up for training, try to have everything in place and assessed i.e., technology, spacing, seating, snacks
Confirm participants
Pre-type printed awards with participants
If Virtual: Re-send Zoom link to participants
If Blended: Confirm completion of CPI Pre-work
THE MORNING OF – TRAINING DAY 1
Be on site for training 60 to 45 minutes prior to the start of class.
If the facility is not available prior, Set up for training, try to have everything in place, and assess
Place the book at the seats (CPI)
Provide name tags and a sign-in sheet at the entry if possible
Complete CPI Training
Document Blue Cards in CPI portal
THE MORNING OF – TRAINING DAY 2
Be on site for training 60 to 45 minutes prior to the start of class.
If the facility is not available prior: Set up for training, try to have everything in place, and assess
Place the book at the seats (YMHFA manual and participant log)
Provide name tags and a sign-in sheet at the entry if possible
Complete YMHFATraining
Have participants complete the post work: open minds post, YMHFA post
Award the participants with certificates upon completion. If Virtual: Arrange certificates for pick up or delivery
Document completed training in MHFA Connect
SAMPLE WELCOME EMAIL/LETTER
Dear [Participant Name],
Welcome to the Trauma-Informed Ministry Model (TIMM) Training Program! We are a few short days away! We are thrilled that you have chosen to join us on this journey towards mental health awareness. This program aims to inform and educate the faith-based community with a comprehensive curriculum that includes Psychological First Aid, Youth Mental Health First Aid, and Verbal Intervention Training. By participating in this program, you will receive certification in each of these platforms and gain valuable tools to help combat the stigma surrounding mental health, while also bridging the gap between faith and mental well-being.
The plan is as follows:
1. Attend in-person class, please try to arrive on time. Make sure to mark your calendars for the in-person classes, which will be conducted on the following dates:
Insert Date here, from Insert Time here (Orientation/Zero Model)
Insert Date here, from Insert Time here (Verbal Intervention Session)
Insert Date here, from Insert Time here (Mental Health First Aid Day 1)
Insert Date here, from Insert Time here (Mental Health First Aid Day 2)
2. Log into the National Child Traumatic Stress Network’s website (NTSN) and create an account: Visit https://learn.nctsn.org/login/signup.php to create your account on NTSN. This platform will be used for course materials and resources.
3. Begin Psychological First Aid. Once you have created your NTSN account, please start the course "Psychological First Aid (PFA) Online" under the topic "Access the Curriculum" on the NTSN website: https://www.nctsn.org/.
I would welcome any inquiries or feedback you may have. Please do not hesitate to contact me via the phone number or email address provided. We are genuinely eager to offer this valuable training opportunity and encourage you to share it with your peers. Together, we can create a positive and lasting difference in our community.
Thank you for your participation!
Best,
FACE/DEMOGRAPHIC SHEET



Name:
OPENING MINDS SURVEY
ParticipantId: CompletionDate:
OpeningMindsSurvey(Pre-Test)
Thequestionsbelowaskyoutoagreeordisagreewithaseriesofstatements.Thereisno correctanswertoeachquestion.Pleaseplacean“X”intheboxthatbestfitsyouropinion.
Iammorecomfortablehelpinga personwhohasaphysicalillnessthanI amhelpingapersonwhohasamental illness.
Ifapersonwithamentalillness complainsofphysicalsymptoms(e.g. nausea,backpainorheadache),I wouldlikelyattributethistotheir mentalillness.
IfacolleaguewithwhomIworktold metheyhadamanagedmentalillness, Iwouldbeaswillingtoworkwith him/her.
IfIwereundertreatmentforamental illnessIwouldnotdisclosethistoany ofmycolleagues.
Iwouldbemoreinclinedtoseekhelp foramentalillnessifmytreating healthcareproviderwasnotassociated withmyworkplace.
IwouldseemyselfasweakifIhada mentalillnessandcouldnotfixit myself.
IwouldbereluctanttoseekhelpifI hadamentalillness.
Employersshouldhireapersonwitha managedmentalillnessifhe/sheisthe bestpersonforthejob.
IwouldstillgotoaphysicianifIknew thatthephysicianhadbeentreatedfor amentalillness.
Name:
OPENING MINDS SURVEY
ParticipantId: CompletionDate:
IfIhadamentalillness,Iwouldtellmy friends.
Itistheresponsibilityofhealthcare providerstoinspirehopeinpeople withmentalillness.
Despitemyprofessionalbeliefs,Ihave negativereactionstowardspeoplewho havementalillness.
ThereislittleIcandotohelppeople withmentalillness.
Morethanhalfofpeoplewithmental illnessdon’ttryhardenoughtoget better.
Peoplewithmentalillnessseldompose arisktothepublic.
Thebesttreatmentformentalillnessis medication.
Iwouldnotwantapersonwitha mentalillness,evenifitwere appropriatelymanaged,toworkwith children.
Healthcareprovidersdonotneedtobe advocatesforpeoplewithmental illness.
18. 19. Istruggletofeelcompassionfora personwithamentalillness.
Iwouldnotmindifapersonwitha mentalillnesslivednextdoortome.
THE NATIONAL CHILD TRAUMATIC STRESS NETWORK (NCTSN) 12
CORE CONCEPTS
The National Child Traumatic Stress Network (NCTSN) has identified 12 Core Concepts that are essential for understanding the impact of trauma on children and adolescents. These concepts help frame how trauma affects development, behavior, and relationships and provide a framework for understanding and responding to the complexities of childhood trauma. Here’s a brief overview of the 12 Core Concepts:
1.Trauma: The experience of trauma can disrupt a child's sense of safety and well-being, impacting their emotional and physical health.
2.Development: Trauma can affect a child's development, altering their emotional, cognitive, and social growth.
3.Individual Differences: Each child's response to trauma is influenced by factors such as age, gender, culture, and prior experiences.
4.The Importance of Relationships: Supportive relationships can help mitigate the effects of trauma, while negative or disrupted relationships can exacerbate its impact.
5.Impact on Family: Trauma affects not just the child but also the family dynamics and functioning, which can influence recovery.
6.Cultural Considerations: Cultural background plays a significant role in how trauma is perceived and addressed, influencing coping strategies and support systems.
7.Systems of Care: Effective responses to trauma involve collaboration across multiple systems, including schools, healthcare, and social services.
8.Resilience: Children can demonstrate resilience in the face of trauma, with protective factors that promote recovery and positive adaptation.
9.Trauma-Informed Care: Approaches that recognize the impact of trauma are essential in supporting children and families.
10. Signs and Symptoms: Understanding the varied signs and symptoms of trauma is crucial for identifying and addressing children's needs.
11. The Role of Environment: A child’s environment, including their home, community, and school, can influence their experience of trauma and their recovery process.
12. Treatment and Recovery: Effective interventions and support can foster healing and recovery for children affected by trauma.
SAMPLE COMMUNITY/REFERRAL RESOURCE GUIDE
SAMPLE TIMM INTEREST MEET-UP FLYER

NATIONAL CHILD ABUSE HOTLINE
1-800-4-A-CHILD (1-800-422-4453)
RESOURCES
NATIONAL SEXUAL ASSAULT HOTLINE
1-800-656-HOPE (4673)
NATIONAL DOMESTIC VIOLENCE HOTLINE RAINN (RAPE, ABUSE & INCEST NATIONAL NETWORK)
1-800-799-SAFE (7233) 1-800-787-3224 (hearing impaired line)
NATIONAL RUNAWAY SAFELINE
1-800-621-4000
LGBT NATIONAL TALKLINE
1-800-246-7743 https://lgbthotline.org/chat/
ALCOHOLICS ANONYMOUS
1-800-656-HOPE (4673) www.rainn.org
LGBT NATIONAL HELP CENTER
1-888-843-4564
TREVOR PROJECT CRISIS LINE – LGBTQ YOUTH
1-866-4-U-TREVOR (488-7386) www.theTrevorProject.org
NARCOTICS ANONYMOUS www.aa.org/pages/en_US/find-aa-resources
NATIONAL DOMESTIC VIOLENCE HOTLINE
1-800-799-7233 thehotline.org
HOUSING/FOOD/EMPLOYMENT
WWW.FINDLAW.COM
COUNCIL FOR MENTAL
(CLICK ON “FIND A PROVIDER”)
1-888-GET-HOPE (438-4673) (Hopeline) www.na.org/meetingsearch
NAR-ANON FAMILY GROUPS
WWW.NAR-ANON.ORG/FIND-A-GROUP
HOPE™ HOTLINE
1-888-995-HOPE (4673)
1-800-662-HELP (4357) HTTP://FINDTREATMENT.SAMHSA.GOV
HTTPS://WWW.WESTCARE.COM
LIVINGWORKS
1-800-4-A-CHILD (1-800-422-4453) https://livingworks.net/
REFERENCES
NATIONAL SEXUAL ASSAULT HOTLINE
1-800-656-HOPE (4673)
NATIONAL COUNCIL FOR MENTAL WELLBEING RAINN (RAPE, ABUSE & INCEST NATIONAL NETWORK)
TheNationalCouncil.org (click on “Find a Provider”)
1-800-656-HOPE (4673) www.rainn.org
THE NATIONAL CHILD TRAUMATIC STRESS NETWORK (NCTSN) www.nctsn.org
ACKNOWLEDGEMENTS
We would like to take this opportunity to express our sincere appreciation to everyone who has contributed to the authoring of this implementation guide We extend our gratitude to WestCare’s Training, Research, and Evaluation, and Marketing teams for their invaluable insights, collaboration, and dedication Special thanks to the main authors of this guide for their expertise and support in gathering the necessary data and information
We are grateful for the collective effort that has made this report a valuable tool for decision-making and future planning.
IMPLEMENTATION GUIDE AUTHORS (In alphabetical order)
Rev. Jermine Alberty, BSB/M, M. Div., Founder/ Principal, Salt Initiative LLC www jerminealberty com
William Baldwin, MPH, CPH, Director of Research and Evaluation, WestCare william.baldwin@westcare.com
Lisa Compton, Marketing Manager, WestCare lisa.compton@westcare.com
Jennifer Hilton, BA Psy, Director of Training and Technology Transfer, WestCare jennifer hilton@westcare com
Clifford Taylor, D. Min, TIMM Project Director, WestCare clifford taylor@westcarwe com
