TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS, DENTAL TECHNICIANS AND DENTAL PROSTHETISTS
ONLY $880 FOR 2 DAYS OF EDUCATION
ONLY $220 FOR 2 DAYS OF EDUCATION (12 HOURS OF CPD) IF YOU REGISTER BEFORE 29 NOVEMBER 202
Join us again or for the first time at Digital Dentistry & Dental Technology No 6 for a fun, exciting and fully immersive learning experience with the best of the best in the new age of dentistry. This year’s program will again cover Artificial Intelligence • Digital Smile Design • Digital orthodontics • Intraoral scanning • 3D Facial Scanning • Digital implantology • Digital full arch restorations and full mouth rehabilitations • Digital Dentures • 3D Printing • Milling • CBCT • Materials and applications • Software and more with MORE Hands-on Sessions • MORE Advanced Sessions • MORE New Products • NEW Masterclasses... and more!
Join us again or for the first time at Digital Dentistry & Dental Technology No 7 for a fun, exciting and fully immersive learning experience with the best of the best in the new age of dentistry. This year’s program will again cover Digital Smile Design • Digital orthodontics • Intraoral scanning • AI • 3D Facial Scanning • Digital implantology • Digital full arch restorations and full mouth rehabilitations • Digital Dentures • 3D Printing • Milling • CBCT • Materials and applications • Software and more with MORE Hands-on Sessions • MORE Advanced Sessions • MORE New Products • NEW Masterclasses... and more!
REGISTRATION FEES
REGISTRATION FEES
INCLUSIONS
INCLUSIONS
PROGRAMME DETAILS
PROGRAMME DETAILS
$880 inc gst
$880 inc gst
ALL INCLUSIVE
EARLY BIRD PRICING
$220 before 29 nov 2025
Early bird discounts may apply
price increases $110 on the 2nd of every month
VENUE DETAILS
VENUE DETAILS
Registration fee includes participation in TWO full days of education (12 CPD hours), all catering and Friday drinks. Multiple lectures and workshops are being run concurrently to allow you to build your own program to suit your specific interests. Price is all inclusive.
Registration fee includes participation in TWO full days of education (12 CPD hours), all catering and Friday drinks. Multiple lectures and workshops are being run concurrently to allow you to build your own program to suit your specific interests. Price is all inclusive.
Novotel Sydney Brighton Beach - The Grand Parade, Brighton-Le-Sands NSW 2216 - Close to Sydney Domestic and International Airports
The Brighton Hotel Sydney - The Grand Parade, Brighton-Le-Sands NSW 2216 - Close to Sydney Domestic and International Airports
Use code 2605DDDTEC for discounted accommodation rates for the conference • Ample parking available at the hotel
Check the website for details of discounted accommodation rates for the conference • Ample parking available at the hotel
Organised by Dentevents™ a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 www.dentevents.com • info@dentist.com.au • Tel: (02) 8001-6502
Organised by Dentevents™ a division of Main Street Publishing Pty Ltd ABN 74 065 490 655 www.dentevents.com • info@dentist.com.au • Tel: (02) 8001-6502
Zir, Hybrid Ceramic
PMMA, Wax
Glass Ceramic, Custom Abutment
Titanium Disk
Co-Cr Disc
On the cover...
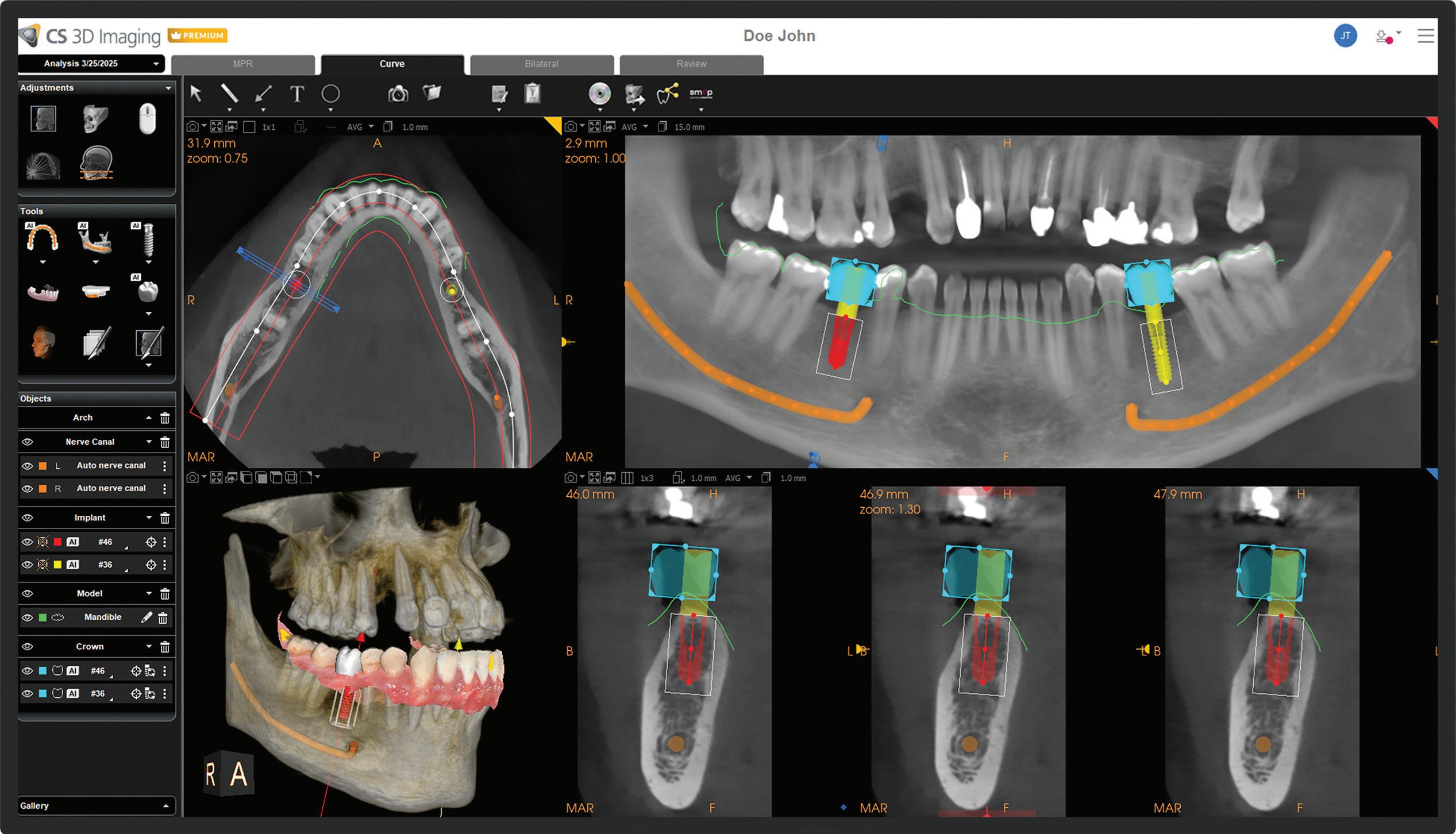
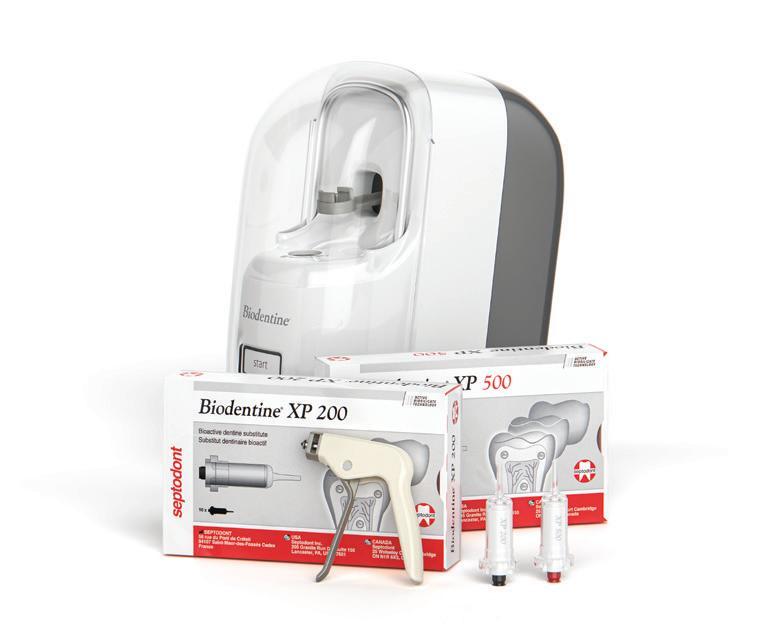
Biodentine XP is a dentine restoration system designed for daily deep cavity restorations and represents the next generation of Biodentine.
Practice seller mythbusters - Part 2 76 Put your customers first: Strategies to stay focused on their needs
78 The death of word of mouth in 2026 (For dentists who do nothing else)
and publisher will not accept responsibility for the
or for
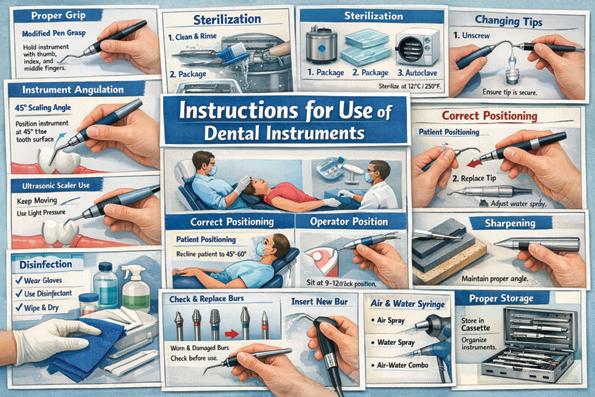
infection control
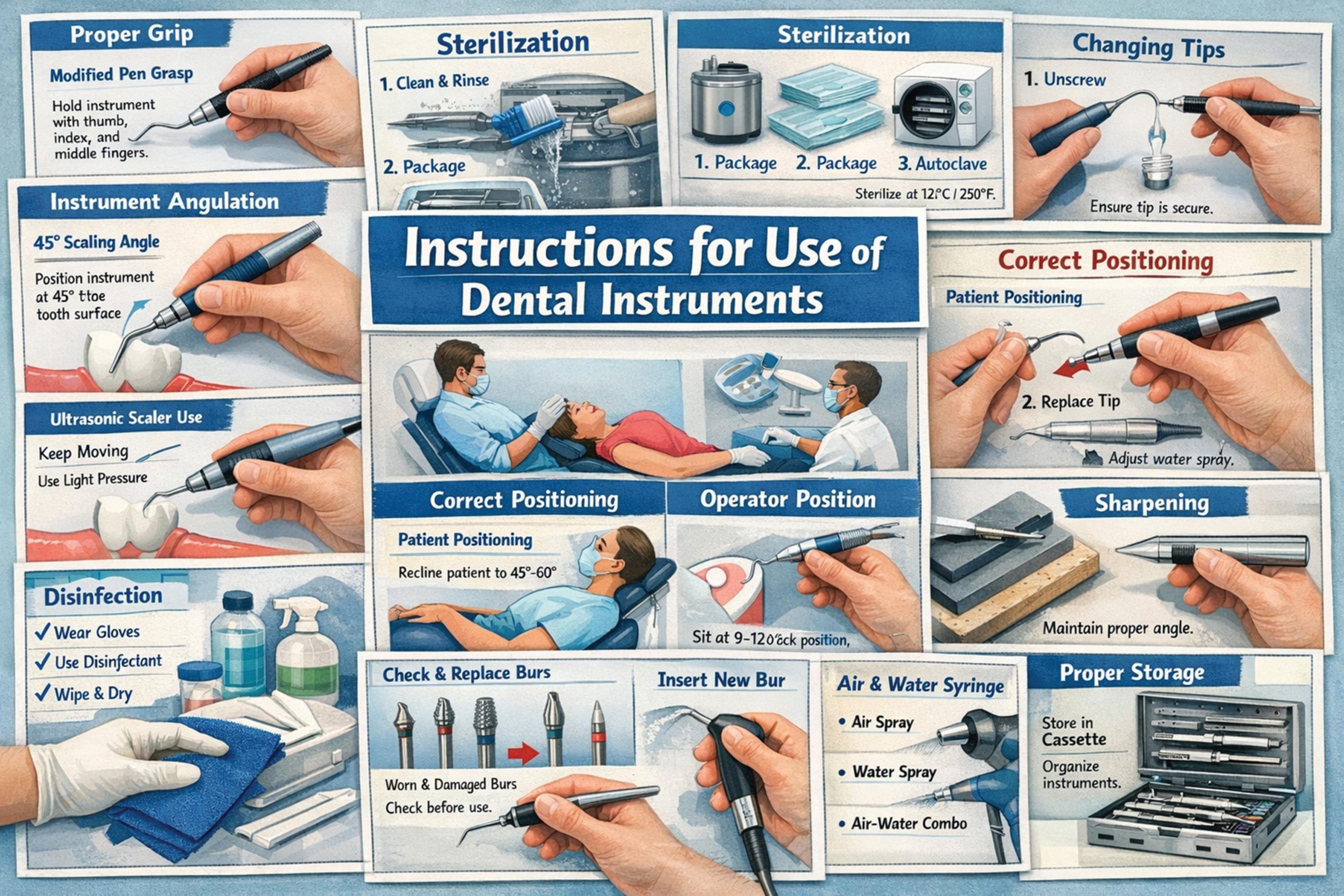
86 IFU: The most important concept in reprocessing dental instruments and handpiece
92
Peace of mind: Infection control built into A-dec equipment
surgery design
198
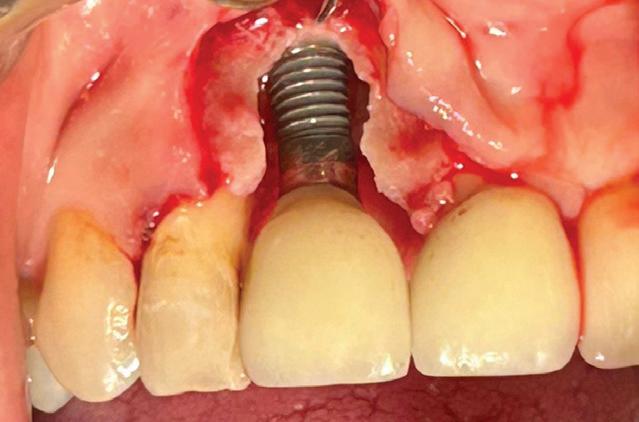
TRI matriX® Implant: A 5-year triumph in abutment-free immediate restoration
102
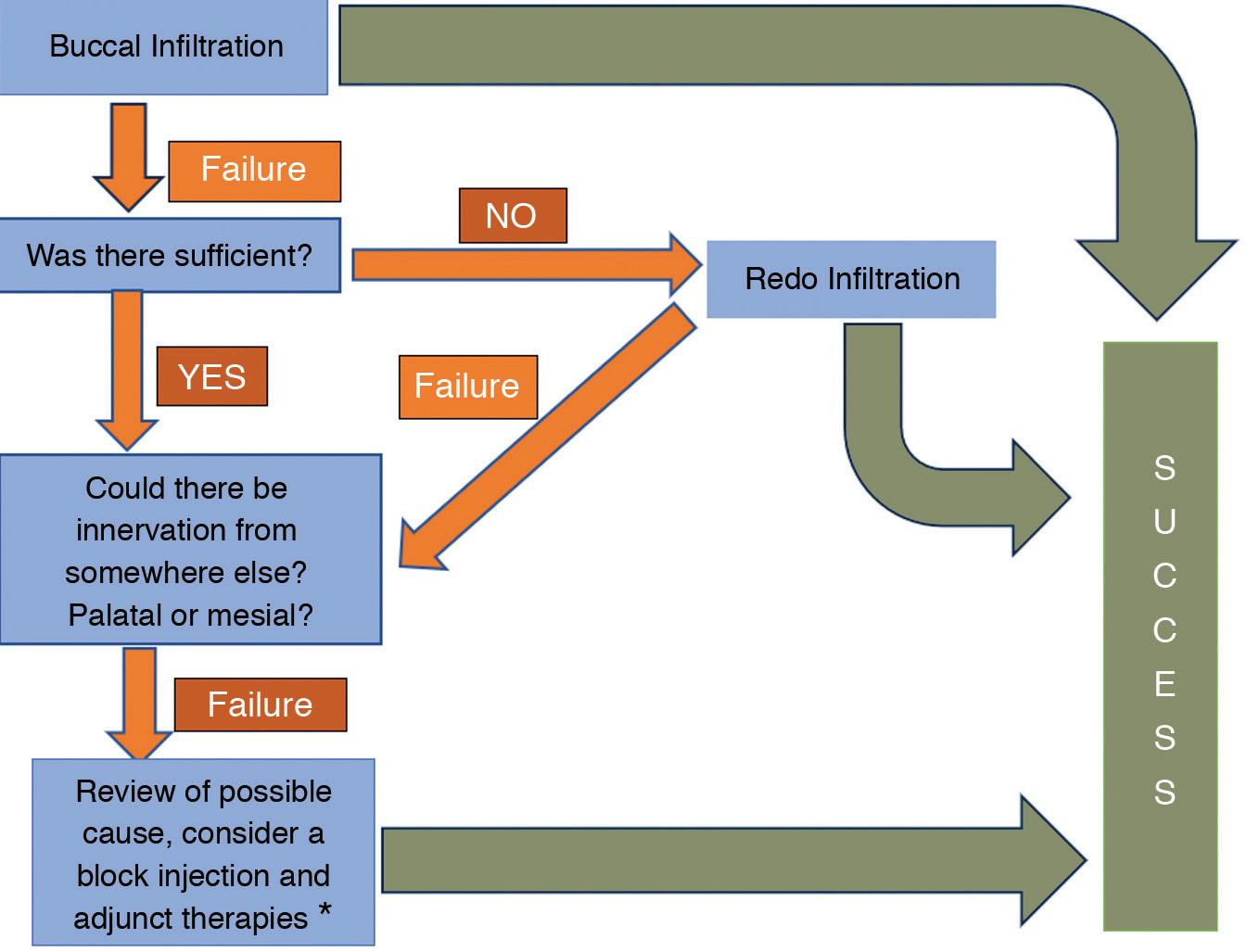
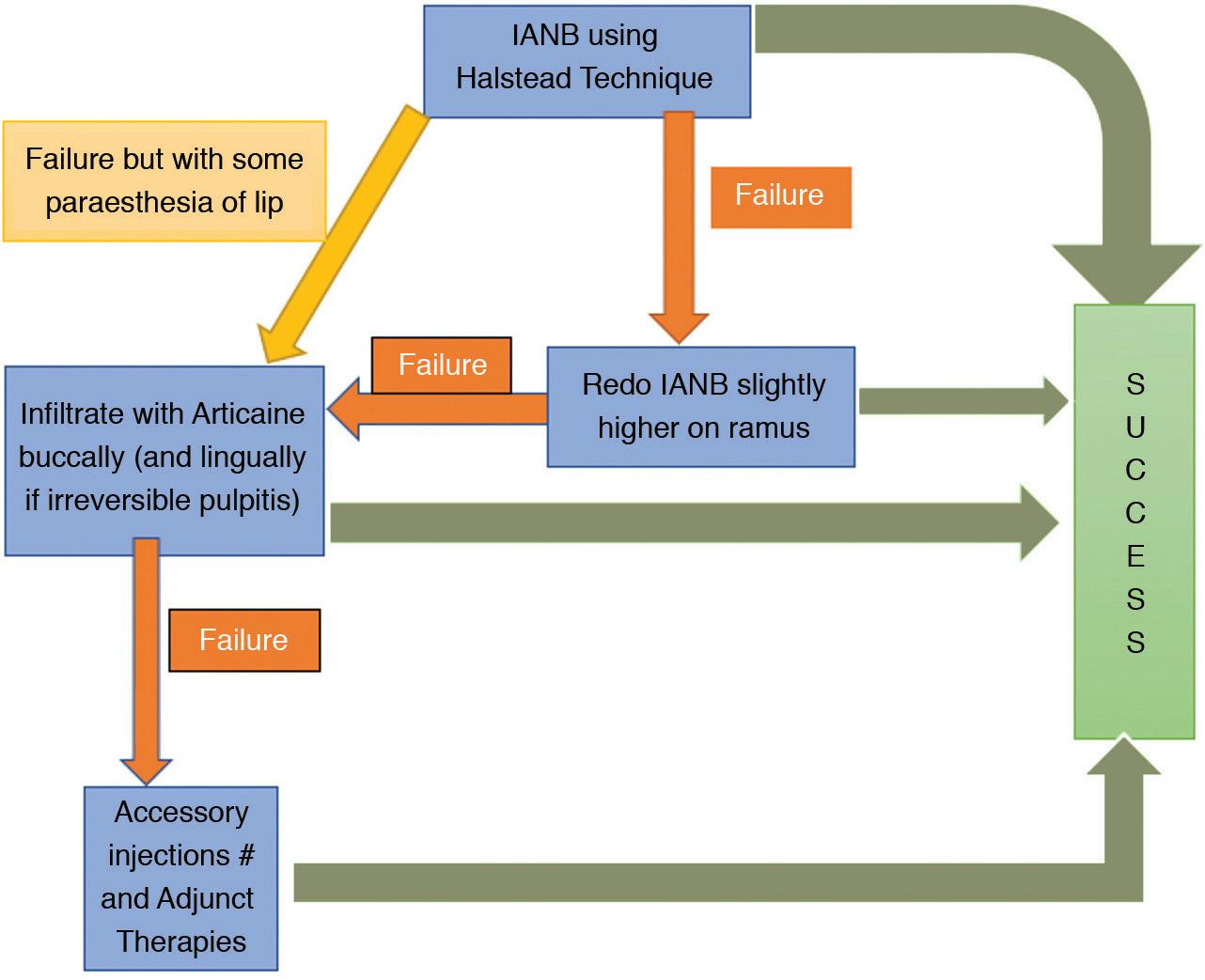
Failures with local anaesthetic - Part 2
108
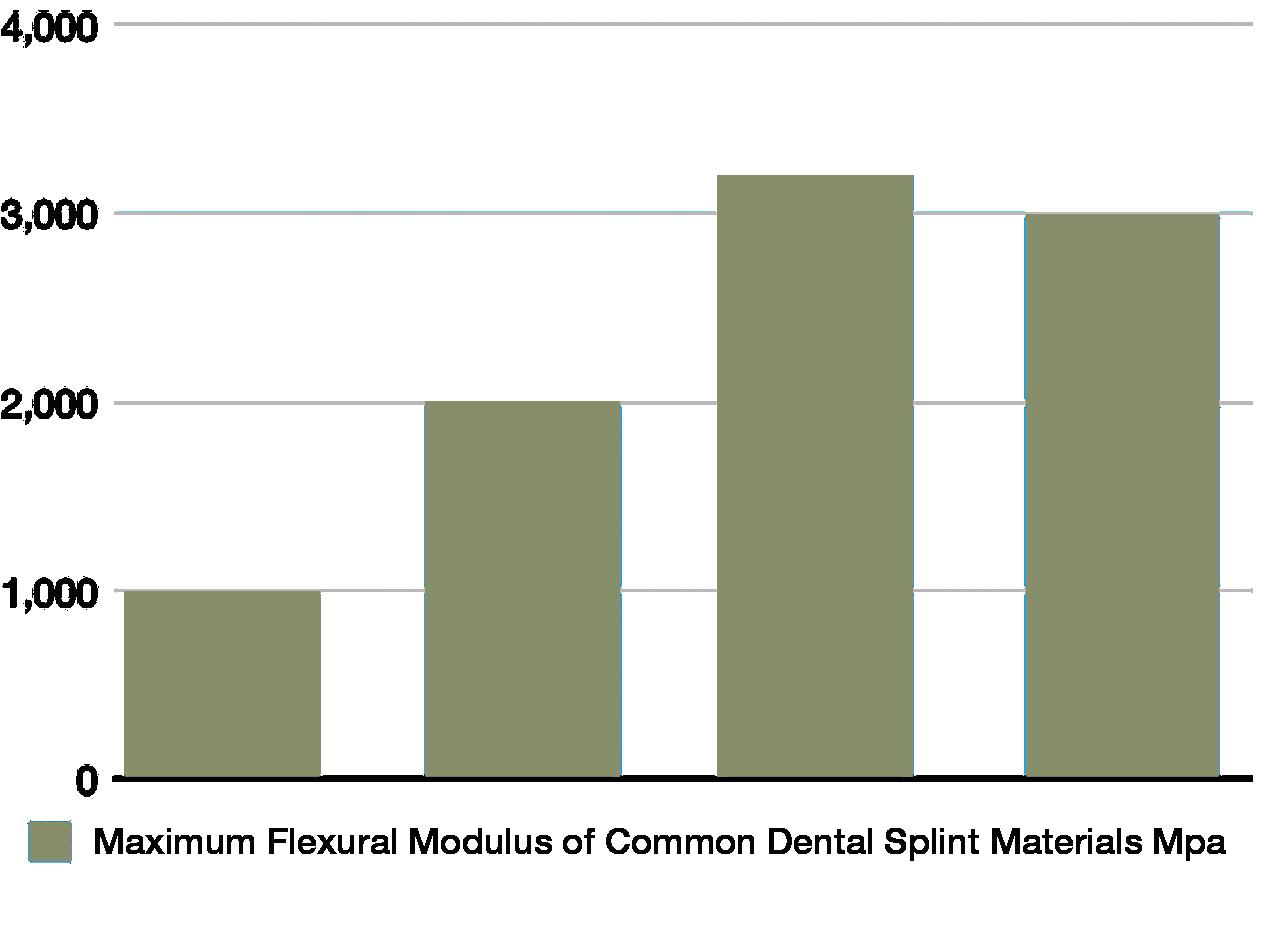
Dental splints under scrutiny: Nylon, PMMA, POM and 3D-printed resins
112
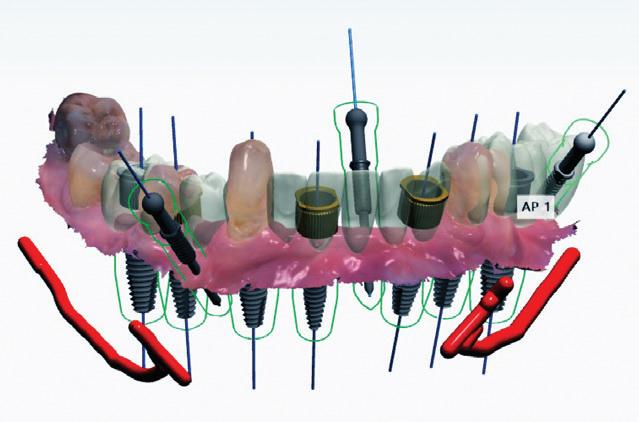
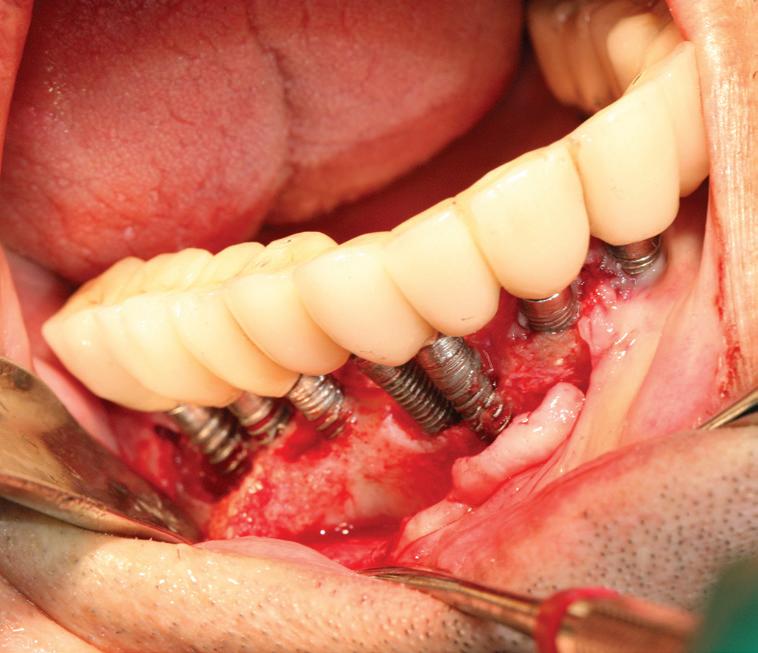
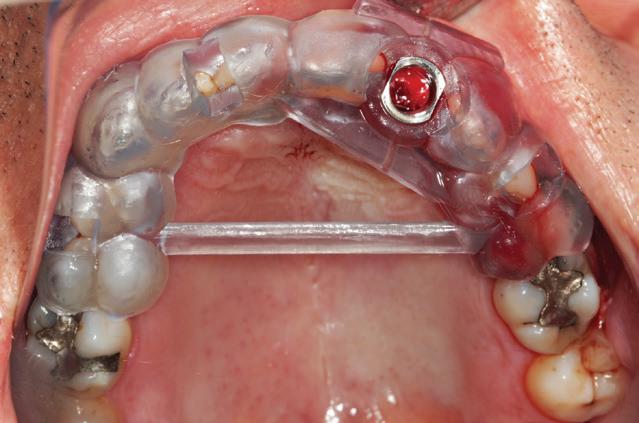
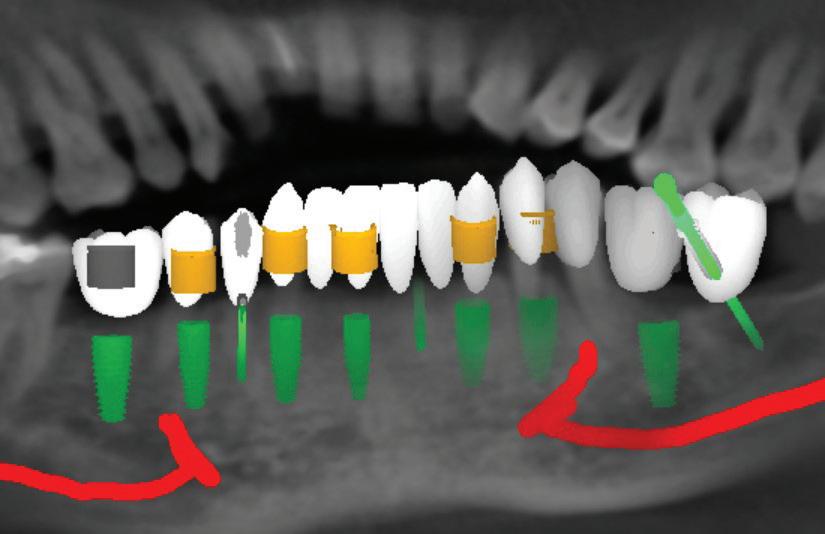
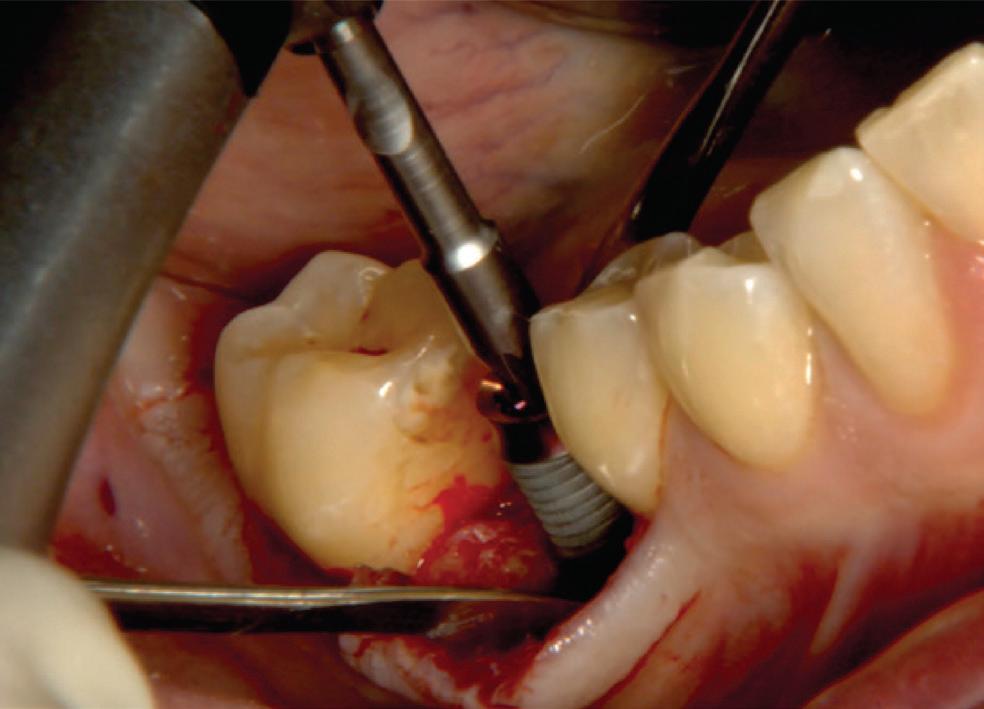
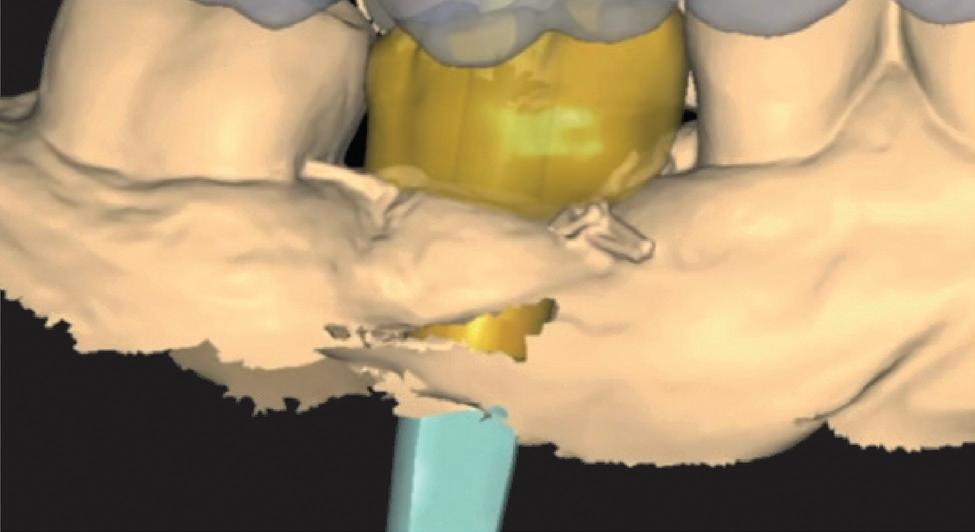
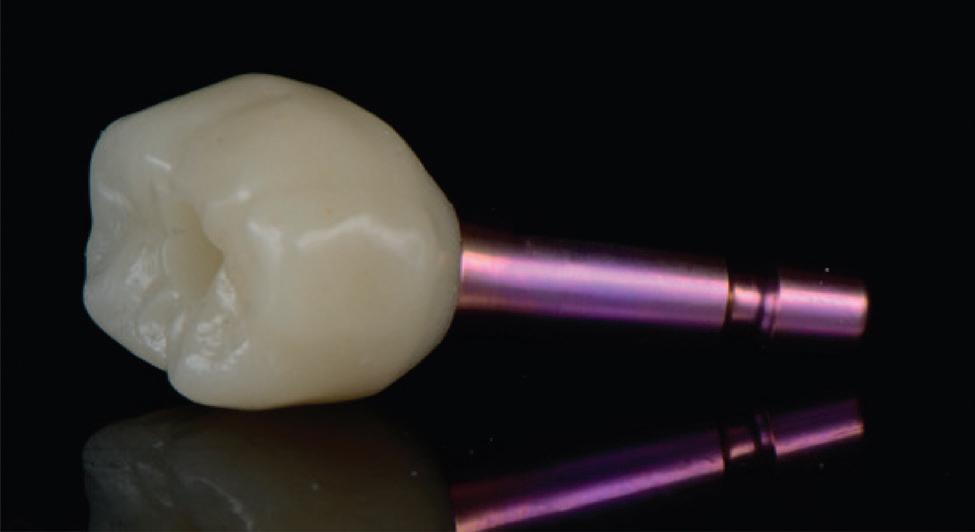
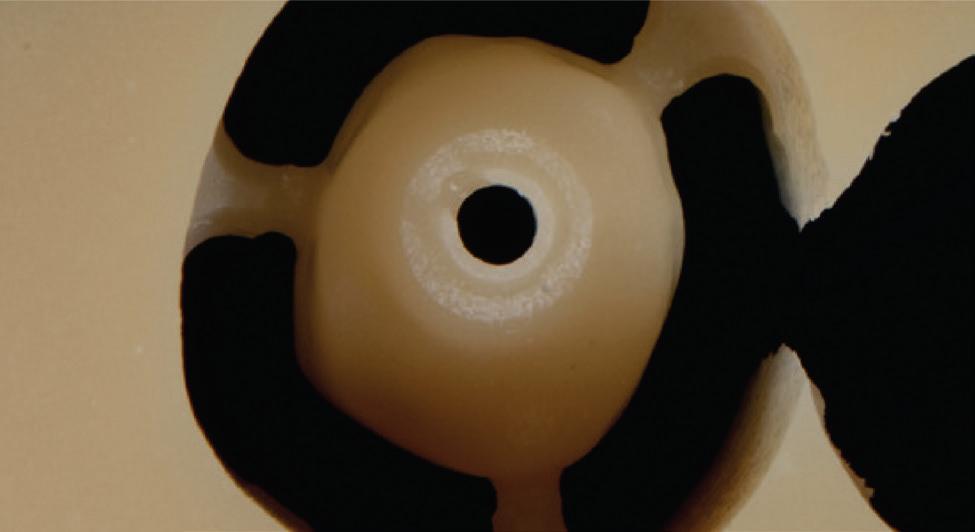
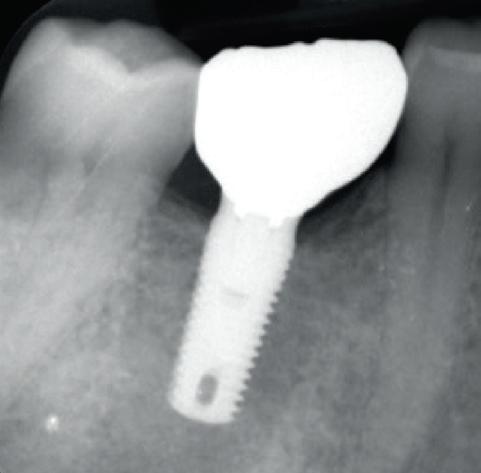
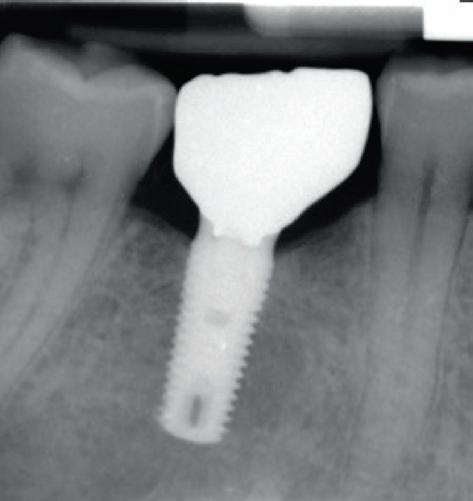
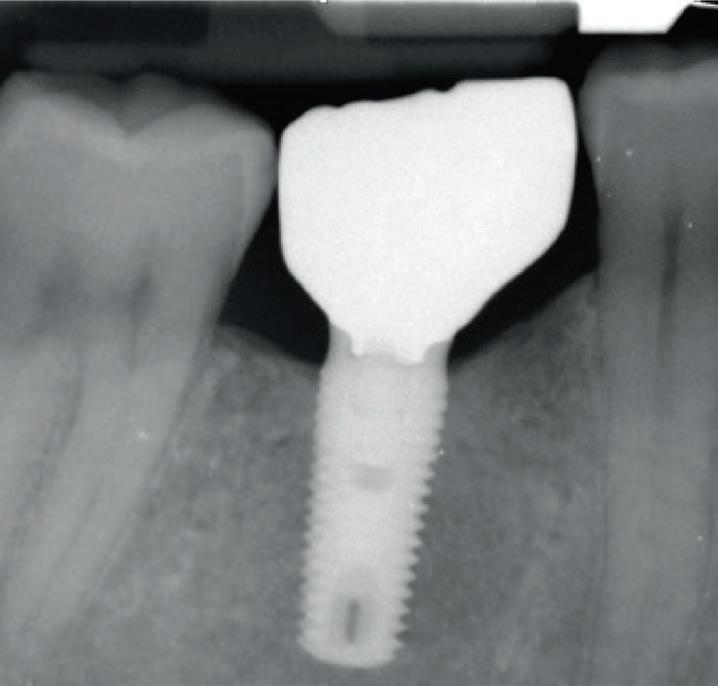
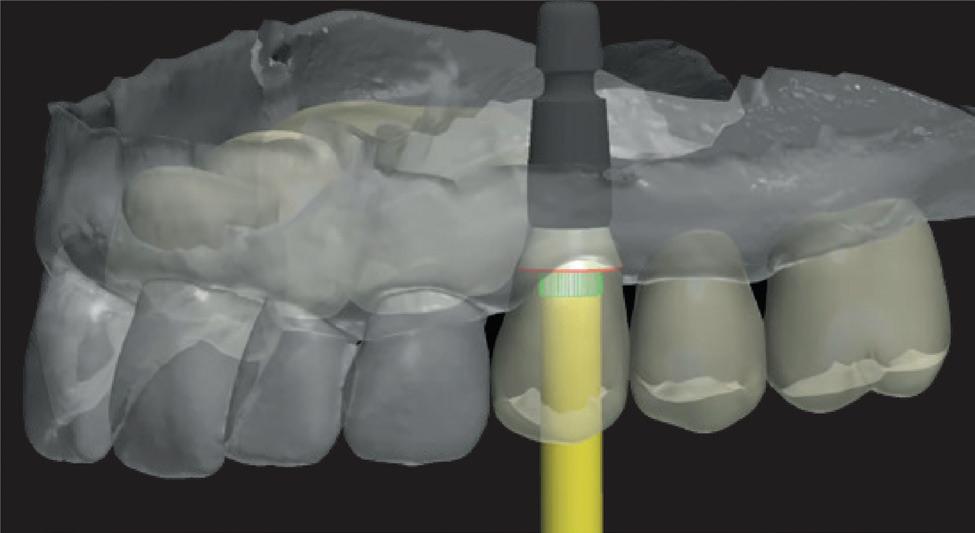
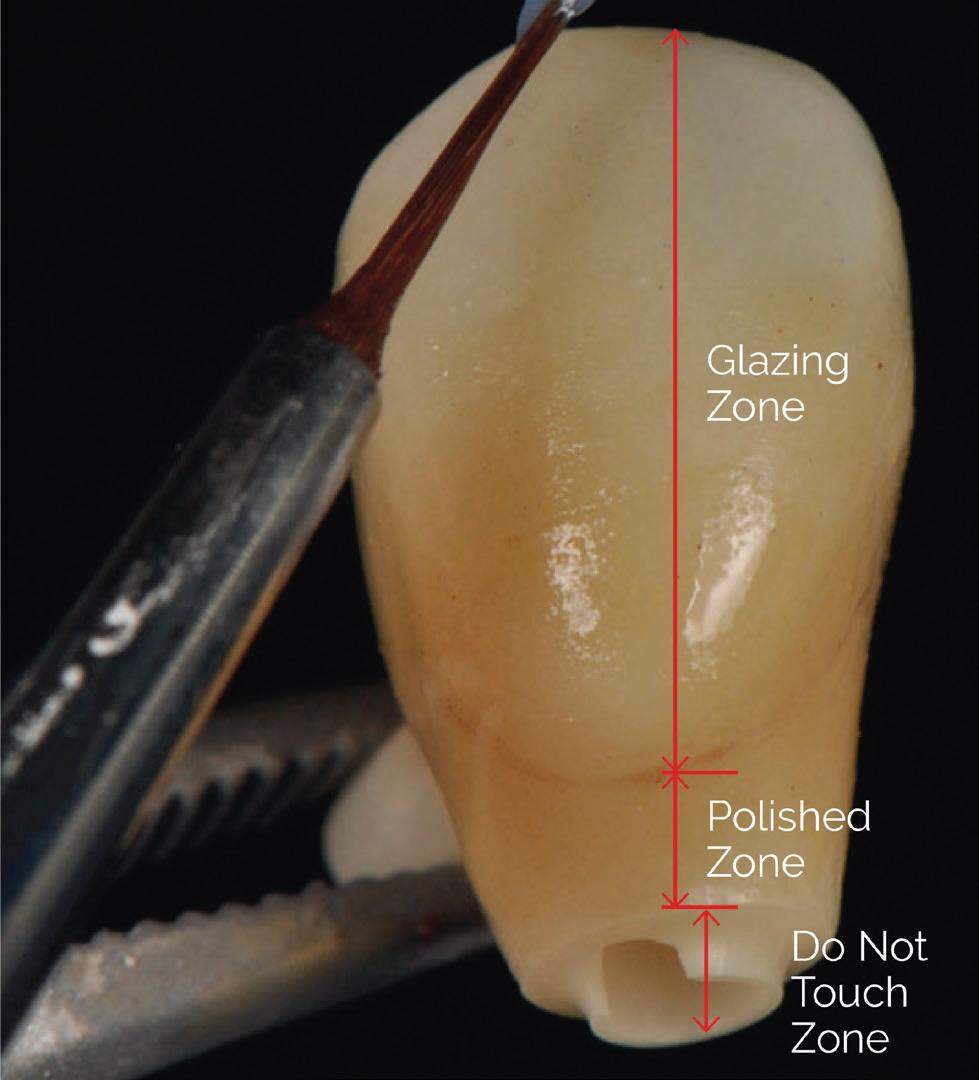
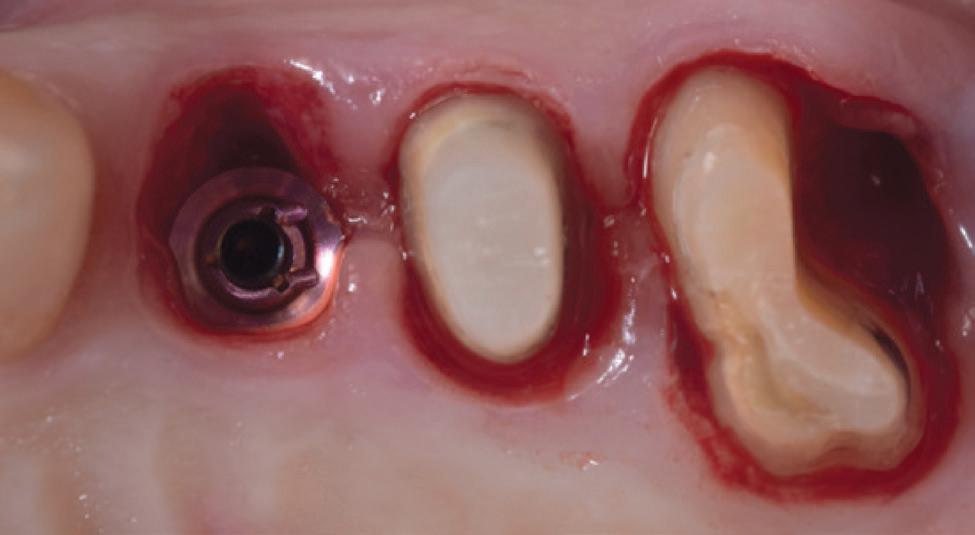
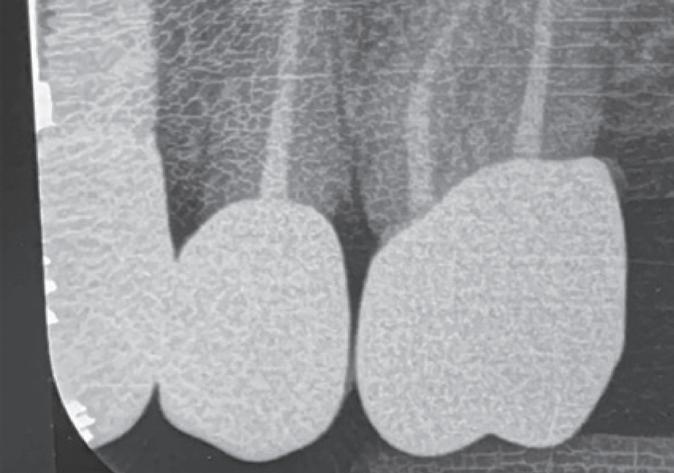
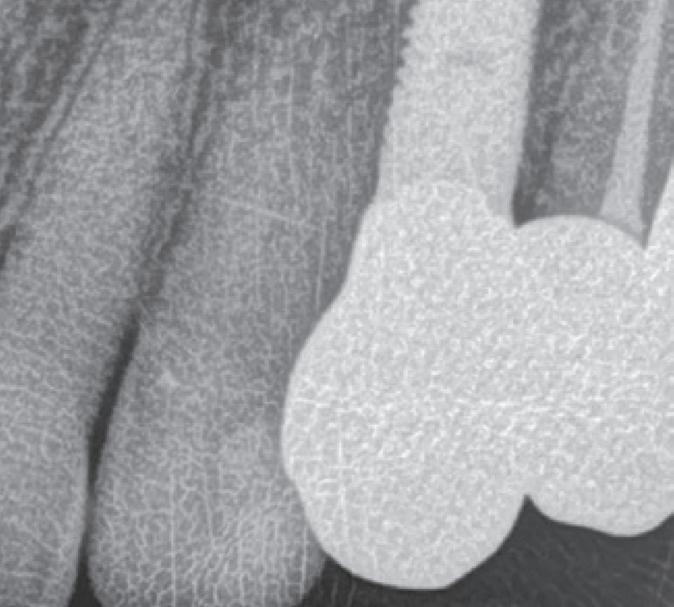
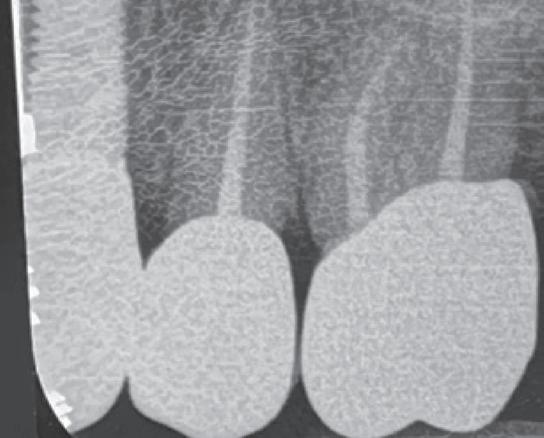
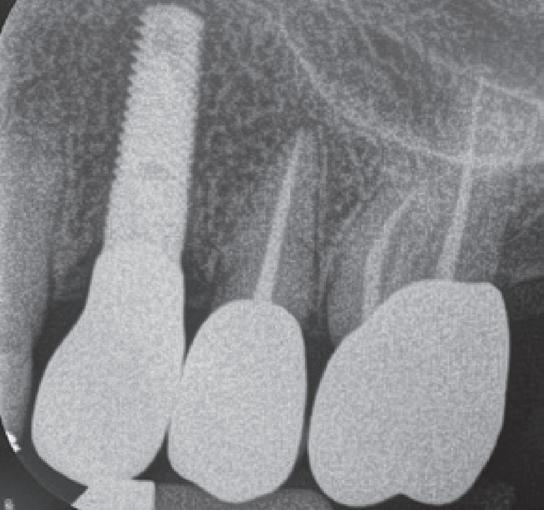
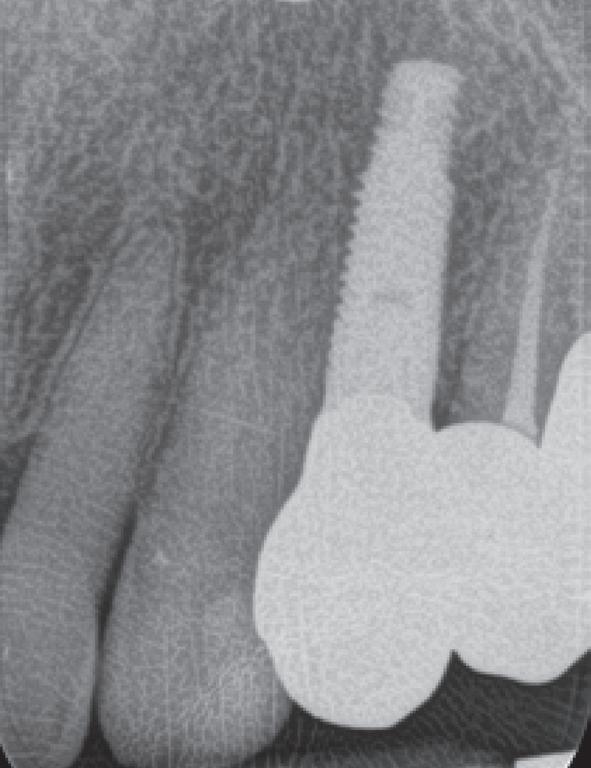
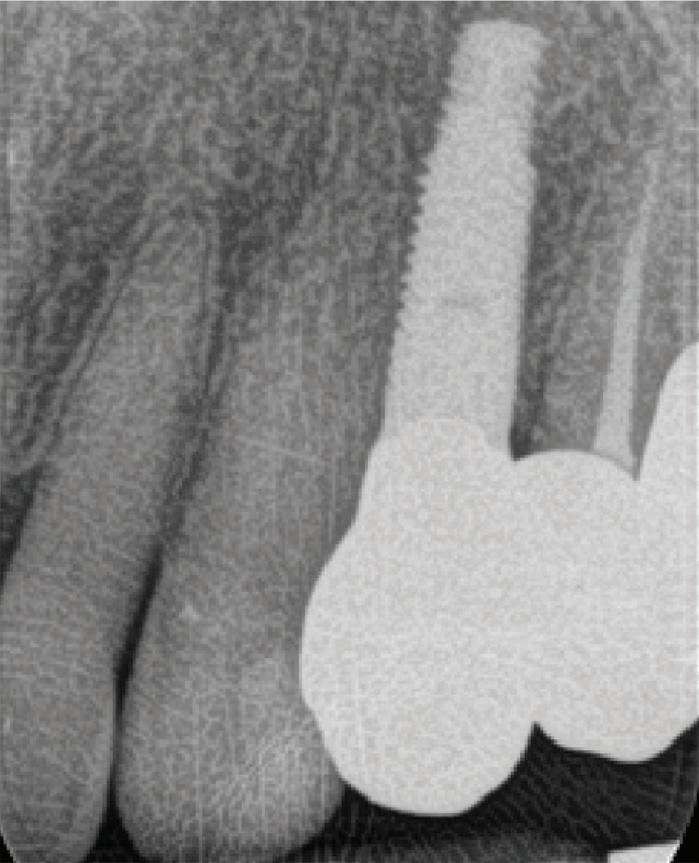
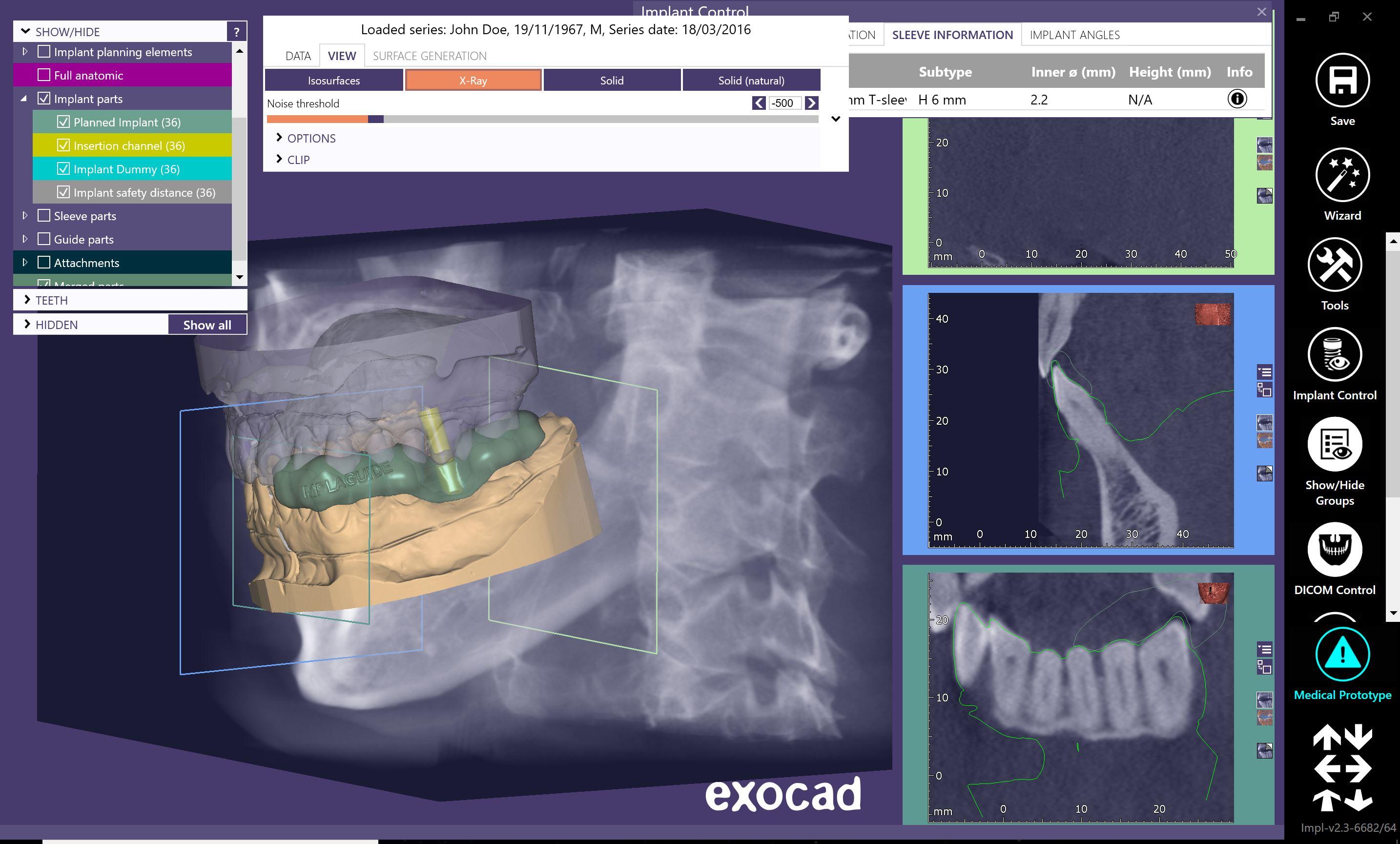
Fully digital treated aesthetic single crowns on matriX® Tissue-Level implant and root resections
124 Jannali practice puts patient health firsty
118
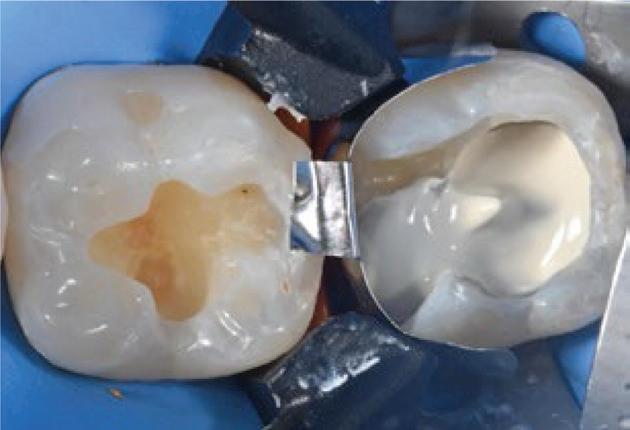
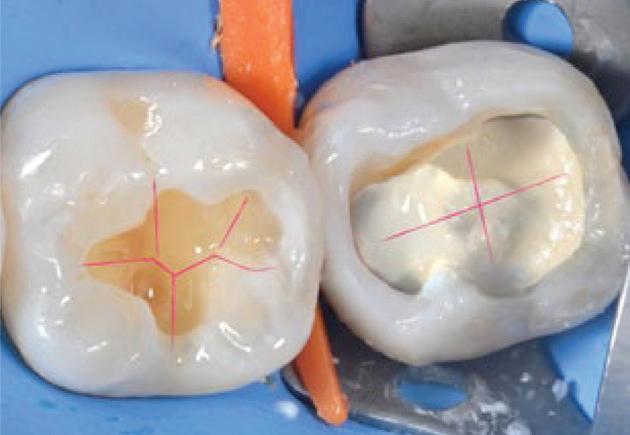
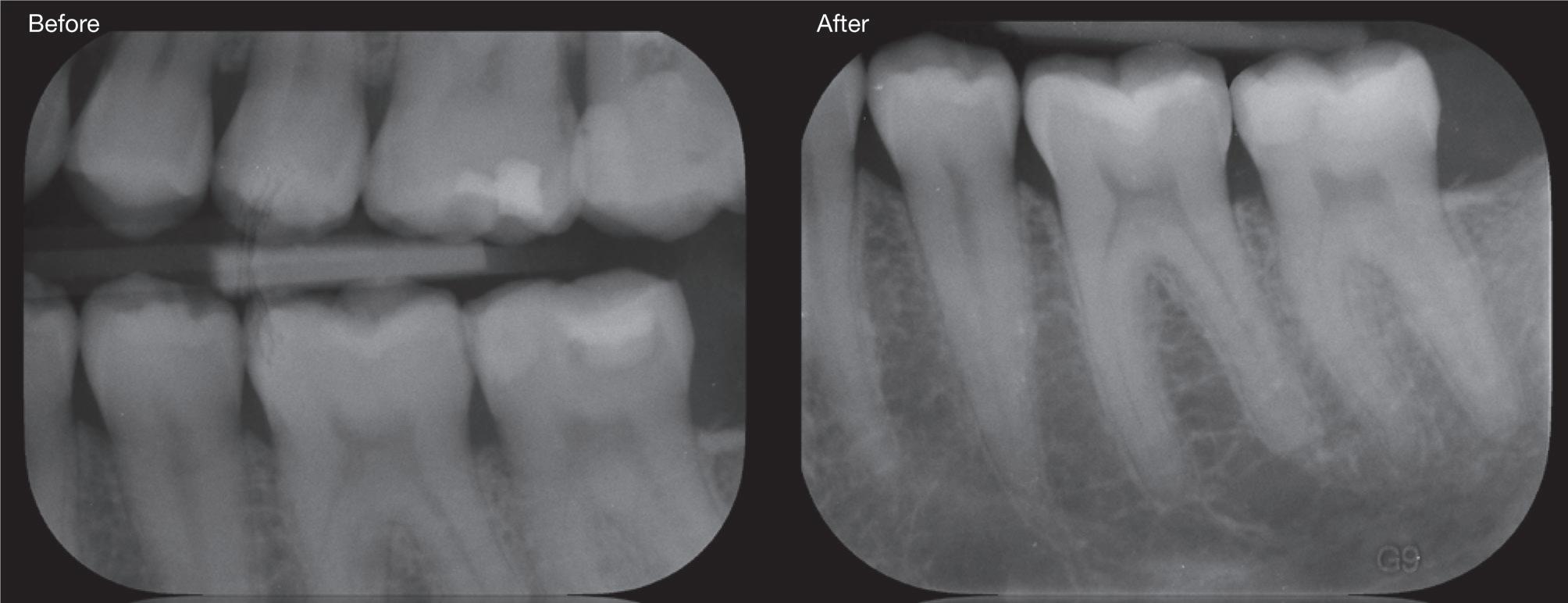
Indirect pulp capping: Bio-bulk fill technique and Bulk&Go
By Joseph Allbeury
Goodbye Graham...
An era has ended with the passing of our long-time contributor, Graham Middleton.
Over a 30-year period, he contributed close to 200 articles - the bulk of which are available to read on www.dentalcommunity.com.au - where he delivered always considered, sometimes divisive and eternally relevant advice for dentists, doctors, veterinarians and others on finance, management and life in general.
Graham’s enduring theme was the importance of getting informed advice every step of the way from professionals experienced in the machinations of dentistry, rather than just business in general. His typical method of delivery was through anonymised storytelling drawn from decades of working with dentists buying practices, selling practices, restructuring practices, getting divorced - both in life and professionally, entering and escaping partnerships, avoiding dodgy investment schemes - particularly involving apartments and pine plantations - and more.
As a final tribute, we have published typical Graham on page 68 where 20 years ago, he was delivering advice as prudent then as it is today.
I was fortunate to speak with Graham in his hospital bed a few days before his passing and he was as animated and on the ball as ever. I was sad indeed to hear a few days later that I would no longer have that privilege.
As a resident Melburnian, we were never destined to be close; but attending his funeral I learnt so much more about the man that made me wish we had been.
He loved history and was a notable world authority on the American Civil War, reading everything ever written on the subject and making many journeys to the US to explore battlefield locations, often with family and friends in tow.
He was a lifetime boxing fanatic and loved the Melbourne Storm NRL team. So much so, he would write unsolicited motivational letters to the team in their turbulent early days that had such an impact, their contents were read immediately before each game to inspire them to victory.
Most of all however, Graham was a man of integrity, heavily opinionated, always considered and never afraid to speak his mind. His legacy will be as the champion of helping professional clinicians navigate the immense noise and clutter of the business, finance and management aspects of running a successful practice and making decisions that will set them up financially for life.
He also possessed a quiet generosity, offering guidance freely and without expectation, often behind the scenes. Many who sought his counsel may never have fully realised the depth of his influence, yet their careers and lives were undeniably shaped by his wisdom and unwavering sincerity.
Graham’s passion and commitment will be greatly missed by readers of this magazine and indeed the dental profession as a whole.
Joseph Allbeury, Editor and Publisher
Vale Graham George Middleton
Our cherished long-standing columnist and industry commentator, Graham Middleton, has passed away, aged 80. He will be remembered as a man of quiet determination, generous spirit, unwavering integrity and enduring curiosity—a life defined not only by professional achievement, but by a deep commitment to people, community and craftsmanship.
Daughter Kate said “My father lived a rich life. In addition to the professional profile he developed through which he helped many in the dental, veterinary and medical professions build satisfying and rewarding practices, he brought his zest for life from the farm on which he grew up to the boarding school he attended on scholarship, from school to the army and later professional work and into his many interests. Passionate about the American Civil war, Australian military history, Meccano, boxing, rugby league and the Melbourne Storm, he was deeply involved in many communities and changed many lives for the better.”
At the heart of Graham’s professional legacy was his work with Synstrat Group, where he became a trusted advisor and advocate for dentists, vets and others across Australia. He understood that dentistry was more than a profession; it was a calling that required both clinical excellence and sound business judgment. Through his guidance, many practitioners found stability, growth, and confidence in navigating the complexities of running a practice. Graham had a rare ability to listen carefully, distill problems, and offer practical, thoughtful solutions. He took immense pride in helping dentists succeed, not for recognition, but because he genuinely cared about their futures and the communities they served.
Beyond his professional life, Graham’s generosity was perhaps most evident in his long-standing patronage of the Patrician Brothers. His support was not merely financial—it was deeply personal. He believed strongly in the value of education, mentorship, and moral guidance, and he saw in the Brothers a mission that aligned with his own principles.
His sense of duty extended to his military service, which formed an important chapter in his early life. Graham approached his service with the same integrity and discipline that would later define his career. The experience instilled in him a respect for structure, resilience, and teamwork—qualities that remained evident in everything he did.
Those who knew Graham will remember his steadiness, his thoughtful counsel, and his understated humour. He was not one to seek the spotlight, yet his influence was deeply felt by many. Whether guiding a young dentist, supporting a charitable cause, cheering on the Storm or carefully constructing a Meccano model, he brought the same care and attention to every endeavour.
Graham George Middleton’s life was one of meaningful contribution—measured not in accolades, but in the lives he touched and the communities he strengthened. He leaves behind a legacy of integrity, generosity, and quiet excellence that will endure in the many people and institutions he supported.
May he Rest In Peace.
With once or twice daily dosing1*
*Directions – First Day: Initial Dose 2 capsules. Subsequent Days: 1 capsule once or twice daily. A working day is typically 8-12 hours.
NOW AVAILABLE FROM A PHARMACIST WITHOUT A PRESCRIPTION.
SIMPLE DOSING: ONCE OR TWICE DAILY 1 STARTS WORKING IN ~30 MINUTES2†
†Examined with an initial dose of 2 capsules. SELECTIVELY TARGETS COX-2 FOR IMPROVED GI TOLERABILITY 1,3-6‡
‡Compared to non-selective NSAIDs that target COX-1 and COX-2.
FOR PAIN RELIEF FROM SOFT TISSUE INJURY INCLUDING DENTAL PAIN WITH SOFT TISSUE INJURY 1
Scan here to learn more
Indications: For the short-term treatment of acute pain in adults with musculoskeletal and/or soft tissue injury, and primary dysmenorrhea. Before recommending please review the full Product Information available from https://medsinfo.com.au/product-information/document/ Celebrex_Relief_PI
References: 1. CELEBREX RELIEF® Product Information. 2. Cheung R et al. Clin Ther 2007;29:2498–2510. 3. Tai FWD, McAlindon ME. Clin Med (Lond) 2021; 21(2):131-134. 4. Chan FKL et al. Lancet 2010; 376:173-179. 5. Australian and New Zealand College of Anaesthetists & the Faculty of Pain Medicine. PS41(G). Position statement on acute pain management 2023. Accessed October 2025. 6. Bhala N et al. Lancet 2013;382:769-79 (incl Suppl Appendix).
“We cannot admit practitioners without ensuring that their training is of the same standard as expected from Australian graduates and this is not possible without accrediting their training facilities to ensure that they are equivalent to ours and physically checking their clinical skills...”
t’s January 2026 and the health professions have been presented with another challenging proposal designed to wrest control from them over standards of health care delivery.
It would appear that in order to address perceived shortages of providers in certain geographical regions, there is a proposal to “fast track” registration of foreign trained practitioners, largely bypassing Australian assessment processes which were designed to ensure that these practitioners met the same standards as those expected from local graduates.
Australia has an enviable record of health care provision. We have pioneered many procedures and health care initiatives, starting with the Polio vaccine in the 50s to the Bionic ear right through IVF and the HPV. vaccine. If one were to speculate as to the reason for our success, one would have to give credit to the high standard of training in our institutions and rigorous supervision by the Colleges that control specialist training.
Having been in practice for over half a century and having had some involvement in dental affairs, I have witnessed many changes in our profession. Many were for the better; such things as the introduction of Fluoride into our drinking water, the emphasis on oral hygiene techniques, improved restorative materials, research-based minimal intervention procedures, implants, simplified and less invasive orthodontics, an understanding of occlusion. And yet we have allowed outside influences to have a negative impact on how dentistry as well as medicine is delivered.
It has always been in the interest of corporate entities and health funds to change the perception of health provision from a service to a product. It started with item numbers and manipulation of rebates and proceeded to the signing up of preferred-providers based on the premise that it would generate more patients. The reality was different; as profit margins were eroded it became common practice for corporates to introduce earning targets for their employee dentists and production throughput overwhelmed attention to detail.
“The overwhelming consideration must always be what’s best for the patient and part of being a ‘Professional’ was an understanding of this principle. It was always emphasised to us during our training - and I will never forget a venerable senior instructor on the first day of a postgraduate course I was undertaking at the Eastman Institute in London in 1971, starting the first lecture by stating: ‘God gave us teeth so that we are able to eat, not to make dentists richer’...”
In Australia, we have regions that have a shortage of health care providers, whilst at the same time there are areas where there is an oversupply. The solution is not to increase the number of dentists and doctors by importing them from overseas in the hope that they will fill vacancies in underserviced areas. Naturally they too will tend to gravitate to the more desirable areas and not solve the problem of regional shortages. A much neater and effective solution would mirror the “Studentship System” that existed in the past with relation to schoolteachers, whereby subsidised training and a stipend was available to those who on completion of training, contracted to work for a number of years in regions where there was a shortage. Additionally, a significant increase in the number of health care providers will not necessarily solve shortages in areas that are underserviced but is much more likely to supply employees for corporate entities as the cost of setting up independent practices has become prohibitively expensive.
Health is different and its delivery does not lend itself to commercial considerations other than possibly economies of scale.
The overwhelming consideration must always be what’s best for the patient and part of being a “Professional” was an understanding of this principle. It was always emphasised to us during our training - and I will never forget a venerable senior instructor on the first day of a postgraduate course I was undertaking at the Eastman Institute in London in 1971, starting the first lecture by stating: “God gave us teeth so that we are able to eat, not to make dentists richer”.
We cannot admit practitioners without ensuring that their training is of the same standard as expected from Australian graduates and this is not possible without accrediting their training facilities to ensure that they are equivalent to ours and physically checking their clinical skills. Furthermore, without ensuring that the candidate has kept up with continuing professional development since graduating and understands our infection control requirements, we risk registering a sub-class of practitioners who would pose a risk to the public.
At best, we would provide “factory fodder” for the corporates, at worst we would sacrifice our high standards which are the result of the hard work and commitment of generations of health care providers, that once lost would take generations to retrieve.
By David Moffet
TAre you making indelible impressions?
“How can you go above and beyond and leave an indelible impression of your value in the minds of the people you are dealing with? When you do go Above and Beyond and you [figuratively] hit the ball out of the park, you most certainly will leave an indelible impression...”
welve months ago, I had the opportunity of purchasing a very mature dwarf maple from a home in our neighbouring village.
It seemed that the fully grown tree had outgrown its place in this home and because of its maturity, the owner decided to test the market and see whether someone would be willing to dig the tree up and transplant it to their place [for a fee].
Enter Dr Dave...
At my age, this seemed like an opportunity too good to refuse.
I knew that for me to plant a younger version of one of these trees and to wait and watch it grow might take more years than the number that The Good Lord had intended for me to have remaining...
I inspected the tree.
The owner told me that he had previously [and successfully] moved the tree only a couple of metres single handedly only two years earlier.
He agreed with my suggestion that two able-bodied men should be able to dig up the tree root bulb and lift the tree onto my ute and then remove the tree from the ute at my home and plant it in a pre-dug hole.
Sometimes reality does not resemble fantasy.
On the day of transplantation...
After two and a half hours of serious digging, my friend Nick and I hadn’t even budged the tree.
The weather was cold and it was raining and it was looking like we’d messed up big time with our time estimation.
In desperation, I phoned a local excavator [whose advert I had seen in the local community news bulletin].
It was 4:30pm and it was still drizzling with rain.
To my surprise, the guy with the excavator said he’d be happy to come out and excavate the tree from its location and lift it onto the ute.
And true to his word, he did just that.
[Let’s call him Ross].
Ross appeared and in a time space that was less than the time it took for him to get the digger off his truck, Ross had the tree freed from the front yard of this house and lifted up onto the ute.
And that’s exactly what Ross said he would do.
Ross also then followed me and my ute home to Burrawang and with his excavator, lifted the tree off the ute and into the hole that had been previously prepared in waiting for the dwarf maple.
Above and beyond...
The new home for the dwarf maple had a different aspect compared to its previous home. In its previous home, the
maple received sunshine from the east and the north for most of the day, but in Burrawang, it was being planted near to the house in an area where northerly sun may not be readily available.
So we wanted to make sure that we oriented the tree in a way to take advantage of its previous growth and display it in all its glory.
Once Ross had placed the tree into its hole, Ross then helped Jayne and me position its alignment for best viewing from the two main house windows nearby, before helping to fill in the hole and secure the dwarf maple in place.
The thing was...
The thing was that Ross didn’t need to involve himself in the tree’s orientation.
It was late, and he’d already done a fair day’s work elsewhere before I phoned him.
But Ross chose to be invested in the tree’s future and because of this investment, Ross left an indelible impression of himself on my experience of buying and relocating a very expensive tree.
Ask yourself this...
How can you go above and beyond and leave an indelible impression of your value in the minds of the people you are dealing with?
When you do go Above and Beyond and you [figuratively] hit the ball out of the park, you most certainly will leave an indelible impression in the minds of those you have impacted.
The choice is yours.
You can be average and vanilla.
And nobody ever remembers vanilla.
Or you can be extraordinary.
And memorable.
Which behaviour will you pick?
In your life, in your business, in your job, which behaviour do you wish to be remembered for?
About the author
Dr David Moffet is a dentist and a #1 Amazon Bestselling author. He is the inventor of The Ultimate Patient Experience™, a simple to implement patient retention system he used to build and subsequently sell (for several million dollars) his very successful practice [of 28 years] in working class western Sydney. David has now retired from wet-fingered dentistry and spends his time lecturing and coaching private dental clients in the USA, Canada, Great Britain, Europe and Australia and New Zealand on how to improve their practices. David can be contacted at david@theUPE.com or visit www.TheUltimatePatientExperience.com
Re ge nerat io n
The Event in Ora l Regenerat io n
Three Day s Programme
90+ Ora l Re ge neratio n Experts
15+ Ha nds-o n Worksh ops
Re- li ve Sur ge ries & Interactive Formats
Lear n & Network with Peers an d much more...
The congress embraces…
the in clu si ve motto
“Beyond Regenerat io n” , promising yo u a unique le ar ning experience with hig h interact iv ity, s tr ong c li nical relevance, an d a forward-look in g perspective.
Interact iv ity
Beyon d t ra ditional learning
Scie ntific Chair
·Engaging, interactiv e ses si ons
·Sm al l grou p discussi on s & work sh ops
C li nical r el evance
Beyon d technica l exp ertis e and data overload
·Con de nsed, pr ac tica l kn owledge
·Tipp s & trick s fo r bette r pa tien t care
Fu tu re outlook
Beyon d st at e-of-the-ar t methods an d pa ra digms
·Latest adv an ceme nt s i n tec hn ol ogy an d materials
·Programme by an d fo r nex t ge neratio n profes sion als
Anton Sculean
Lisa Heitz-Mayfield
Scie ntific Chair
Biodentine™ XP - Next-generation dentine restoration system*
Biodentine is a unique dentine substitute that combines pulp therapeutic and restorative properties, in a single product. Biodentine XP is a dentine restoration system designed for daily deep cavity restorations and represents the next generation of Biodentine.
Biodentine XP is made from extra-pure tricalcium silicate using proprietary Active Biosilicate (ABS) Technology™, providing biocompatibility and bioactivity.1-7 Suitable for indirect or direct
“Biodentine XP is one material with multiple clinical applications—from emergency dentistry to endodontic repairs. The more you use it, the more you appreciate its versatility and performance.”
Dr Lan Tran, Dentist Qld
placement over the pulp, Biodentine XP stimulates the pulp’s healing capabilities and promotes the formation of reparative dentine to help maintain tooth vitality and structure.
Biodentine XP forms an interface with the dentine surface via micromechanical anchorage, providing a tight seal.8-11 Thanks to its long-lasting dimensional stability, Biodentine XP maintains this seal over time and resists microleakage.11 It reaches mechanical properties similar to sound dentine,1,12-15 making it an optimal choice for bulk-filling techniques from pulp to crown** such as the Bio-Bulk Fill procedure.***
Biodentine XP cartridges contain both powder and liquid for an easy and consistent mix with the Biodentine XP Mixer. The all-in-one cartridges are available in 2 formats (XP 200 and XP 500), depending on the procedure, the depth of the cavity and quantity needed.
Easy to use and convenient thanks to direct placement in the tooth with the Biodentine XP Gun, the Biodentine XP system is adapted to your practice with 1 or 2 sessions procedures.
1. Internal data: Biodentine™ Scientific File. 2011. p.8 to 28.
* CE for Biodentine XP was obtained on the basis of equivalence with Biodentine. ** Fill the entire cavity with only Biodentine XP from the pulp to the tooth surface. Final enamel restoration to be performed in the same session on in the second session which can be performed between 2 weeks and 6 months later.
*** Procedure extracted from international dental practitioner’s experts board (Position statement, September 2023).
References
2. Poggio C et al. In vitro cytotoxicity evaluation of different pulp capping materials: a comparative study. Archives of Industrial Hygiene and Toxicology. 2015.
3. About I, ed. Biodentine™ Properties and Clinical Applications. Springer. 2022.
4. Nowicka A et al. Tomographic Evaluation of Reparative Dentin Formation after Direct Pulp Capping with Ca(OH)2, MTA, Biodentine™, and Dentin Bonding System in Human Teeth. JOE. 2015.
5. Gong V et al. Nanoscale chemical surface characterization of four different types of dental pulp-capping materials. JOD. 2017.
6. Elbanna A et al. In vitro bioactivity of newly introduced dual-cured resin-modified calcium silicate cement. DRJ. 2022.
7. Bakhtiar H et al. Human Pulp Responses to Partial Pulpotomy Treatment with TheraCal as Compared with Biodentine and ProRoot MTA: A Clinical Trial. JOE. 2017.
8. Bakhtiar H et al. Human Pulp Responses to Partial Pulpotomy Treatment with TheraCal as Compared with Biodentine and ProRoot MTA: A Clinical Trial. JOE. 2017.
9. Atmeh et al. Dentin-cement interfacial interaction: calcium silicates and polyalkenoates. JOD. 2012.
10. Aguilar AEA, Manosalvas MSP, Valverde Haro HP. Repair of furcal perforations using different calcium silicate cements: An in vitro study. J Conserv Dent Endod. 2025 Oct;28(10):1007-1012.
11. Niranjan et al. A comparative microleakage evaluation of three different base materials in Class I cavity in deciduous molars in sandwich technique using dye penetration and dentin surface interface by scanning electron microscope. Journal of Indian Society of Pedodontics and Preventive Dentistry. 2016.
12. Biedma-Perea M., Moscoso-Sánchez M., Barra-Soto MJ et al. Survival Evaluation of Restorations in Pulpotomized Primary Teeth with MTA or Biodentine®: A Systematic Review. Journ of Clin Med. 2025, Volume 14(15):5501.
13. Aldegheishem AS., Barakat RM., AlRabiah AM et al. Fracture Resistance of Root-Canal Treated Premolars Restored with Dentin Replacement Materials: An Invitro Study. Oral health & preventive dentistry. 2022, Volume 20 : 271-278.
14. Topçuoğlu Gamze, Topçuoğlu HS. Fracture resistance of primary molars after pulpotomy procedure using mineral trioxide aggregate or Biodentine. The Journ of Clin Ped Dent. 2023, Volume 47(5): 133-137.
15. Lee SM, Song M, Kwak SW, Kim HC. Laboratory Evaluation of the Physicochemical Properties of Novel Pre-Mixed Putty-Type Bioceramic Materials. Aust Endod J. 2025 Oct 29.
IDEM 2026 ushers in the next era of smart, sustainable, digital dentistry
IDEM 2026, the International Dental Exhibition & Meeting, the Asia-Pacific’s leading dental exhibition and conference, returns to Marina Bay Sands, Singapore, from 17 to 19 April 2026, focusing on “Innovating Smart Dentistry for a Sustainable Digital Future”.
Organised by Koelnmesse in partnership with the Singapore Dental Association (SDA), IDEM 2026 will feature three days of innovation, education and international business exchange that addresses the evolving needs of modern dentistry, ranging from digital workflows and advanced clinical techniques to sustainable, patient-centric practice models.
“IDEM remains the key meeting place for the dental industry in the region,” said Mr Mathias Kuepper, Managing Director and Regional President AsiaPacific, Koelnmesse Pte Ltd. “With over 33 countries and regions represented on the exhibition floor, the event brings the global dental community together in Singapore, connecting Asia’s dental traders with international manufacturers. As organisers, we are further supporting this with programmes such as the IDEM360+ App, where visitors and exhibitors can set up meetings before the event and the IDEMclub, a buyer programme aimed at supporting key buyers to meet their future business partners.”
A dynamic exhibition with international representation
I DEM 2026 will span 17,000 square metres and host over 400 exhibitors from around the world. The exhibition will feature products and solutions in orthodontics, endodontics, prosthodontics and paediatric dentistry, presented by established industry leaders and emerging innovators.
The exhibition will showcase the global diversity of the dental industry with 12 national and regional pavilions: Brazil, China, France, Germany, Italy, Singapore, South Korea, Spain, Switzerland, Taiwan, the United Kingdom and the United
States. The United Kingdom returns as the newest pavilion, accompanied by a strong line-up of new exhibitors. More than 40 first-time exhibitors will participate this year, reinforcing IDEM’s role as a launchpad into the regional market.
Sustainable digital practices
The IDEM 2026 scientific conference will feature three parallel tracks spanning three days, comprising 42 sessions led by 36 speakers and covering a variety of topics, including Digital Dentistry, Periodontal Regenerative Therapies, CBCT for Endodontic Treatment, Pain Management, Aesthetic Dentistry and many more. Renowned speakers, including Anthony Mak, Chris Ho, Andrew Ip, Henry Kwek, Jeyavel Rajan, Leon Chen, and Taisuke Tsukiboshi, will share clinical insights and practical approaches for digital and patient-centric dentistry.
At its core, the IDEM 2026 Scientific Conference is about empowering dental professionals to run smarter, more efficient and future-ready practices,” said Dr Kelvin Chye, Chairperson of IDEM 2026 and Vice President of the Singapore Dental Association. “This year’s conference dives deep into key topics, including digital workflows and emerging innovations in clinical care, while bringing together
clinicians from key dental markets. We are proud to welcome representatives from 12 national dental associations, alongside strong participation from leading markets such as Indonesia, Australia, the Philippines and Malaysia. Together, this vibrant regional exchange will foster collaboration, strengthen professional networks and help shape the future of dentistry in Asia-Pacific.”
SDA Masterclasses and hands-on learning
IDEM 2026 will feature an immersive SDA Masterclass programme, offering delegates a chance to explore the latest innovations in digital dentistry, prosthodontics, and restorative techniques. Participants can gain hands-on experience by learning to integrate advanced digital tools into everyday practice—from veneers and crowns to implant rehabilitation, dental photography, videography, and AI-assisted smile design.
Registration for delegates is open until 19 April 2026. Dental professionals are encouraged to register early to secure their place at IDEM 2026. Visitors to the exhibition can register for free until 3 April 2026. For more information, visit www.idem-singapore.com
Get ready to...
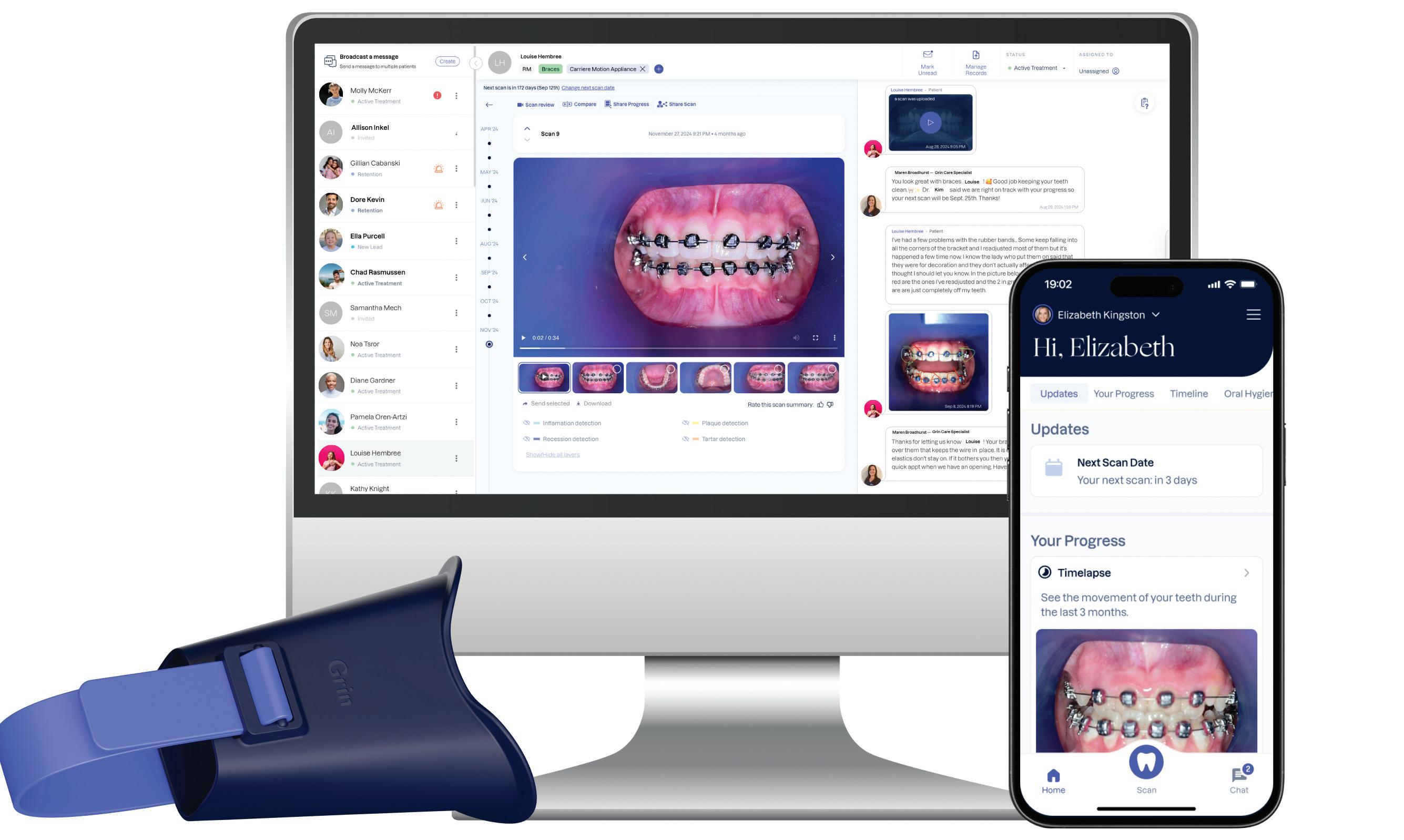
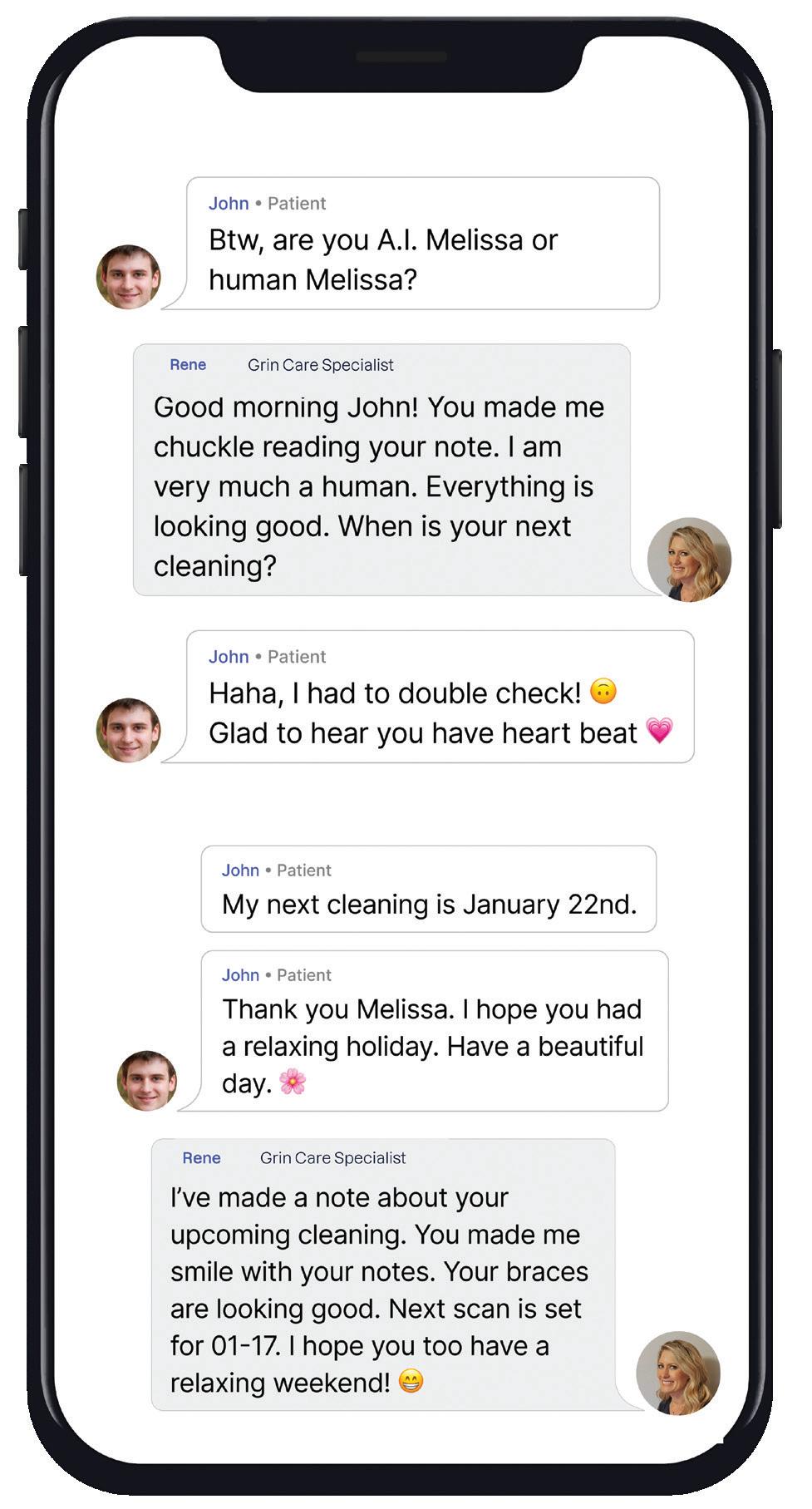
Next generation remote Orthodontic monitoring
Instantaneously receive patient scans to deliver optimal
care
Patients capture videos of their teeth at home using the Grin Scope and intuitive smartphone app
Grin Care Specialists check every scan for treatment progress and problems and communicate with patient and doctor when needed
AI treatment tracker analyses and compares actual treatment progress with digitally planned treatment
Doctors and their teams have complete control and oversight of all patients using the intuitive dashboard
Progress and milestones easily shared with referring doctors
40% to 60%
Fewer in-person visits.
240%
$266->$640
Increased revenue per visit.
16hrs per week
Time that has been saved.
$200K+
Practice ROI*
Average practice return.
*based on average practice ROI calculator
Meet the Grin Scope®
The easy way to monitor your orthodontic patients remotely
Increase your clinical excellence and enhance your patient experience without the need for unnecessary in-chair consults.
* Active treatment monitoring capped at 3 years
The Original Scope
New era in dental imaging: MyRay launches ProXIma X6 CBCT in Australia
In a major boost for Australian dental practices, premium Italian imaging brand, MyRay — distributed locally by William Green Pty Ltd — has officially launched its ProXIma X6 CBCT, ushering in a smarter, safer and more flexible diagnostic imaging solution for dentists.
Unveiled at a special Sydney launch event held against a backdrop of wellknown Italian marques including Ferrari, Lamborghini and Maserati at Scuderia Graziani in Woolloomooloo, the ProXIma X6 promises to revolutionise the way dental professionals visualise anatomy, combining ultra-high-resolution 2D panoramic imaging with powerful 3D CBCT capability — all in a compact, modular platform.
Compact design, big impact
One of the standout features of the ProXIma X6 is its space-saving, wall-mountable design, making it ideal for clinics where floor space is at a premium.
The system is also modular, allowing practices to begin with a 2D-only setup and expand later to include 3D CBCT and even a cephalometric (CEPH) arm when needed. A 7-inch full-touch control panel
guides clinicians through each scan and a virtual control panel can be used from a computer for even greater flexibility.
SMART ergonomics also come built in: a front-facing camera and microphone allow remote monitoring, while intuitive patient supports and ambient lighting promote comfort and efficient positioning.
High-quality, low radiation
MyRay emphasises that the ProXIma X6 maintains diagnostic excellence while minimising radiation dose. Its MRT (morphology-based radiation tuning) technology automatically adjusts X-ray exposure based on patient size and anatomy. QuickSCAN protocols deliver 3D volumes in seconds and QuickPAN and QuickCEPH modes reduce exposure for routine 2D imaging.
The system supports multiple fields of view (FOV) to match clinical needs — from small, focused scans (6 × 6 cm) for endodontics to larger volumes (up to 11 × 11 cm) for implant planning and maxillofacial assessment. A “Scout View” feature allows a rapid low-dose pre-scan to optimise alignment, further reducing unnecessary exposure.
DSmarter software with AI
riving the ProXIma X6’s intelligence is Neowise, MyRay’s next-generation imaging software. Neowise offers a unified interface for 2D and 3D image viewing, while automating common workflows — such as anatomical segmentation, nerve tracing for implant planning, cephalometric analysis and airway evaluation.
Under the hood, AI-powered features identify key structures like the inferior alveolar nerve, align CBCT scans with intraoral scans and even run smile-design simulations for aesthetic cases.
Designed for growth
Australian dental professionals praised the ProXIma X6’s scalability. Rather than over-investing upfront, clinics can start with a core configuration and upgrade later — adding the CEPH arm or extra scanning features as demand grows.
For more information on the MyRay X6 or to book a demo, call William Green Pty Ltd on 1300-363-830 or visit www.williamgreen.com.au
* than original XP Technology®
Easy access the thinner tip gets you where others can’t
Carestream Dental launches AI-powered software that accelerates implant planning and streamlines case sharing
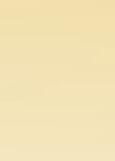
Carestream Dental continues to deliver what’s next in dentistry with the launch of CS 3D Imaging Premium, an advanced AI-powered software solution designed to streamline implant planning, improve case acceptance and simplify case sharing for dental professionals.
CS 3D Imaging Premium leverages cutting-edge artificial intelligence to automate routine tasks so practitioners can plan implants faster. Once the software has merged a CBCT scan with digital impressions, clinicians can launch the new AI Auto Implant feature, which automatically identifies and numbers teeth. After selecting an implant from the digital library featuring more than 100 manufacturers, the software calculates the crown position and the dimensions and position of the virtual implant.
In just a few clicks, clinicians are ready to present treatment options to patients so they can accept and start treatment sooner. For even more efficient planning, implant planning data can also be exported as STL files to labs or exported directly into Smop or BlueSkyBio software for surgical guide creation.
“CS 3D Imaging Premium represents our commitment to driving innovation in digital dentistry,” Andrew Malcolmson, President - Imaging Technology Solutions, Carestream Dental, said. “By integrating advanced AI into our solutions, we are enabling dental practices to work more efficiently; enhance patient engagement through clearer treatment options; and foster seamless communication between clinicians. This launch demonstrates our dedication to transforming clinical workflows and empowering dental professionals to deliver what’s next in exceptional care.”
Additionally, the new Share My Case service enables users to easily share 3D cases with other clinicians to improve communication. CBCT data and implant planning files can now be sent online with a single click, without exporting the data manually. Recipients can download the case and use a shared viewer to review the case.
These premium features available to enhance CS 3D Imaging software and are ready to be experienced through a free 30-day trial.
To learn more about CS 3D Imaging Premium or start your free trial, visit www.carestreamdental.com/cs3dpremium
Harness the power of AI
Accelerate your implant planning workflow with CS 3D Imaging
Work smarter not harder with CS 3D Imaging Premium, the AI-powered software that accelerates your implant planning workflow by automating tasks and simplifying 3D case sharing.
Try CS 3D Imaging Premium for free and unlock new features to enhance your treatment planning and boost your productivity.
Learn more at carestreamdental.com/cs3dpremium
30-day free trial
VENEERS A 2 Ω
Presented by Dr Angelo Lazaris
SYDNEY • JULY 24-25 |
• AUGUST 7-8
Dr Angelo Lazaris is renowned as the doyen of dental veneers... Celebrities, professionals, billionaires and every day Australians seek out Dr Lazaris when they want outstanding aesthetic excellence...
In the ALPHA TO OMEGA OF VENEERS, Dr Lazaris shares his unique, aesthetically-driven protocols and digital workflows as a unified system developed specifically to enhance clinical efficiency and predictability and eliminate any margin for error. Structured in a modular sequence, each topic is delivered as a step in a methodical, reverse-engineering process that maps out a logical pathway to achieving superior treatment outcomes with precision and confidence. Honed through comprehensive critical analysis and evolution, these protocols are universally applicable to every dentist, every patient and every case...
VENEERS are the #1 requested cosmetic dentistry procedure - LEARN TO DELIVER EXCELLENCE!
Dr Angelo Lazaris
BDS (Hons) (Syd), MSc (Aes) (Kings College)
Angelo has developed his own complete digital protocols from inception and design through to delivery and integrated these with biomimetic adhesive dentistry and contemporary restorative materials to create a complete clinical workflow that is equally applicable to single restorations, through to complex full mouth rehabilitations, culminating in outstanding clinical outcomes in a real-world commercial environment. His innovative approach to clinical dentistry is to start at the desired
endpoint, deconstruct complex treatments and develop solutions have made him a sought after KOL, educator and mentor. With appointments including honorary senior lecturer for Kings College London and the University of Sydney, Angelo has recently been assigned as course director for a post graduate diploma and masters degree in digital dentistry; a testament to his expertise and the influence of this discipline in dental practice.
The Ultimate Practice Makeover now playing at dentevents.tv
The Ultimate Practice Makeover, perhaps dentistry’s first reality TV show, is now streaming on dentevents.tv. The 6-episode mini series tracks the progress of Canberra dental practice, Authentic Dentistry, as it undergoes an intensive transformation under the guidance of Australia’s top experts in everything from practice management and marketing to surgery design.
“It’s exciting to finally be screening The Ultimate Practice Makeover on dentevents. tv,” said Joseph Allbeury, publisher of dentevents.tv and this magazine. “The idea of the show is to document the transformation that occurs when Australia’s top consultants and trainers apply their skills to take a practice to a new level.
“We publish articles continually about what is possible; the The Ultimate Practice Makeover now demonstrates that in the format much loved by Australiansthe reality TV show.”
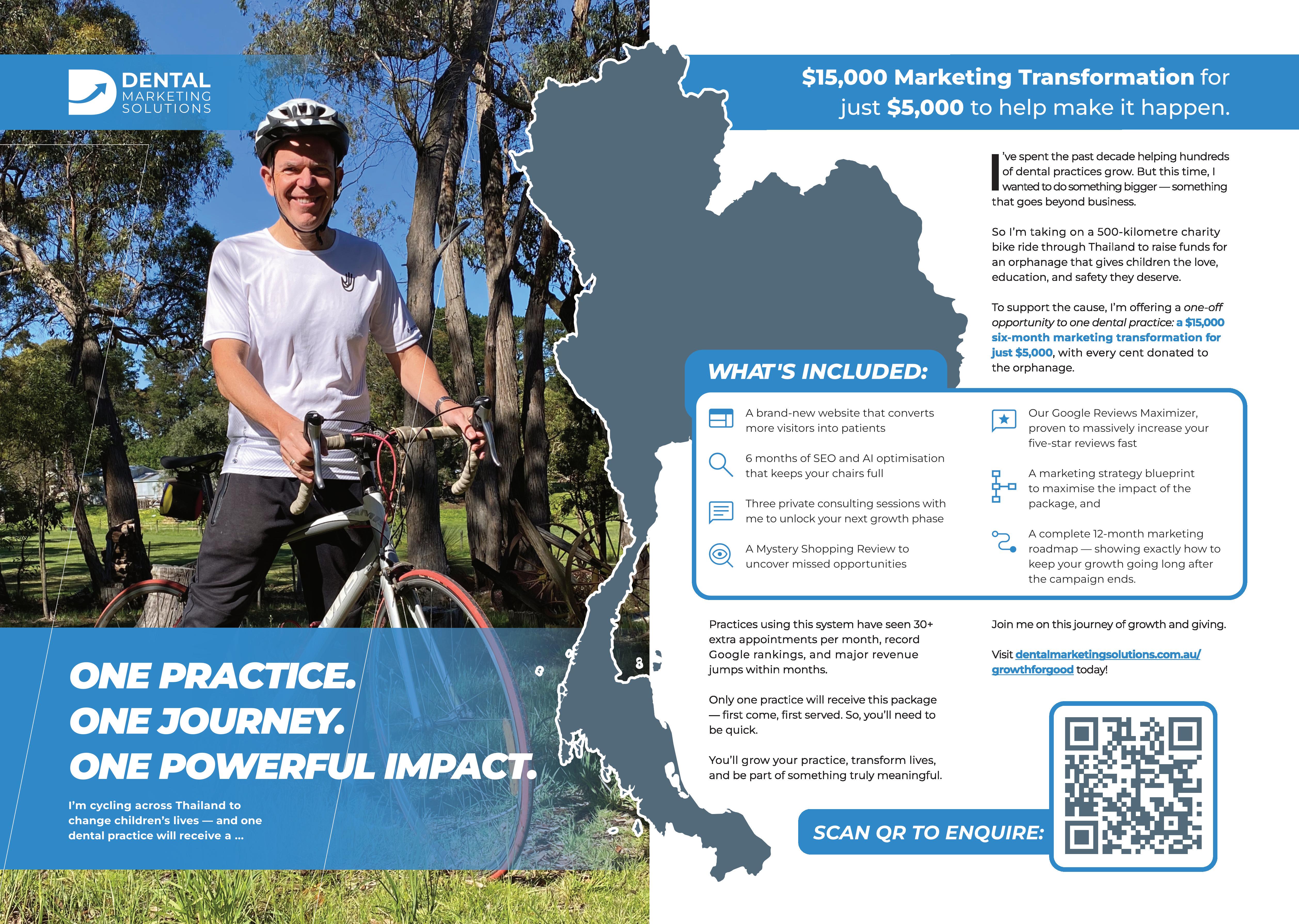
More than 100 dental practices from all around Australia applied to win The Ultimate Practice Makeover - a $100,000 makeover including a $40,000 fit out from Medifit, a comprehensive marketing makeover from Dental Marketing Solutions, high-level coaching and consulting from a hand-picked team of experts and much more.
After a rigorous selection process, the lucky winner was Dr Michael Back of Authentic Dentistry in Canberra. At the time, Michael said “when I found out that I’d won, I was really, really excited. It’s an opportunity to lean on experts who have an area of expertise where I do not... it’s a great opportunity to tap into something that I wouldn’t otherwise do.”
Dental Marketing Solution’s CEO and the show’s host, Angus Pryor, guides viewers through the makeover process presented in six episodes.
As Australia’s highest ranked dental marketer with extensive experience consulting to practices nationally, Angus was ideally placed to get to the heart of exactly what was required to elevate Authentic Dentistry to a new level, reach its overall income goals and increase the resale value of the practice.
“It was an amazing experience to host this unique, first-of-its-kind project,” Angus said. “Michael’s journey was similar to that of many of the clients that we work with whereby we look holistically at a practice and what is required to take it to a new level. It’s not just about marketing, it’s about being ready for marketing. The practice has to look welcoming, the phone has to be answered correctly and the team needs to be skilled in case presentation and conversion.
“If these key elements are not in place first, then having a great website and developing campaigns to bring in new patient traffic will be less effective.”
The Makeover included a reception and waiting area upgrade to provide patients with the best possible first impression of the practice from Australia’s leading surgery builder, Medifit Design and Construct; Full marketing review and strategy development, full business identity branding package including logo, colours, style guide; and a brand new website and Search Engine Optimisation (SEO) to maximise Google rankings in organic searches from Dental Marketing Solutions; 12 month subscription to Channel D to engage patients in the waiting area including a TV; premium listing upgrade on www.dentist.com.au to expose the practice to 1 million potential new patients a year; New uniforms from Muhan Corporate; patient welcome packs from Erskine Dental; OrthoEd Training with Dr Geoff Hall for Dr Beck; Telephone answering training from Call Tracking Excellence; and treatment presentation coaching from Dr Jesse Green.
The Ultimate Practice Makeover is now streaming on www.dentevents.tv. Sign up for free or use your Dental Community password to log in.
Model One 100 Essentials pictured starting at $28,990 inc GST
Diplomatic Immunity 6-year warranty extension option now available for $10 more on any purchase of Diplomat Dental Solutions Model One 100, Model One 200, Model Pro 500 & 700 and Model Pro 600 & 800. Warranty covers both parts and labour provided the annual fixed price service is conducted by a William Green Pty Ltd authorised representative. Terms & Conditions apply.
William Green Pty Ltd 47- 49 Mary Parade
Rydalmere NSW 2116 Ph + 61 2 8865 0300
New VITA Vionic Base Resin Flex for digital fabrication of flexible partials dentures
With VITA Vionic Base Resin Flex, VITA Zahnfabrik presents an innovative 3D printing material for the economical and efficient fabrication of flexible partial dentures in everyday digital laboratory practice. This new material solution offers stability in clinical situations with a lifespan of up to one and a half years, providing metal-free, adaptable comfort for patients and supporting optimal healing and recovery.
Efficient. Precise. Reproducible.
Flexible and removable long-term temporary restorations have proven to be a valuable prosthetic solution in the past. They help make the time until the final restoration as comfortable and aesthetic as possible and free from complications by absorbing masticatory forces in clinically uncertain situations, particularly after surgical or periodontal treatments. However, to date, their production has been labour intensive and the results have often been inconsistent and not reproducible. The digital workflow now makes it possible to cost-effectively produce this type of flexible base with integrated retaining elements, using 3D printing with VITA Vionic Base Resin Flex.
The digital production chain enables efficient, reproducible fabrication of multiple partial dentures in a single printing process, delivering significant time and cost savings in the laboratory. The flexible material is available in clear and pink translucent colours, offering patient-specific aesthetics as the natural gingival shade can show through from underneath. The recommended duration of wear for the material is stated as up to 18 months.
PMaximum flexibility in fabrication and application
artial dentures made with VITA Vionic Base Resin Flex can be repaired and extended. In addition, the material is significantly easier to process and polish than traditional injection molding processes or filament printers. VITA Vionic Base Resin Flex can also be used as a bonding material to create chemical adhesion to the precisely fitting alveoli of the base, for both printed and milled teeth.
“The digital workflow now makes it possible to cost-effectively produce flexible and removable long-term temporary restorations with integrated retaining elements using 3D printing with VITA Vionic Base Resin Flex...”
The new 3D printing material is the solution for offering customised and comfortable partial dentures with a flexible base in a cost-effective, efficient and state-of-the-art manner. Patients enjoy the benefits of a comfortable fit, metal-free aesthetics and flexible adaptability to the clinical situation.
Visit http://hs.vita-zahnfabrik.com/de/vita-vionic-base-resin-flex for more information VITA Vionic Base Resin Flex.
think x-ray. think Greens.
MyRay X6 CBCT with Ceph. pictured Multiple configurations available
MyRay ProXIma X6 5-year warranty extension offer available until 30 June 2026 on all purchases of the MyRay ProXIma X6 3D CBCT and MyRay ProXIma X6 3D CBCT with cephalometric arm models. Warranty covers both parts and labour. Terms & Conditions apply.
dentevents presents...
Go from novice to expert in dental 3D printing in your clinic or lab in this comprehenive, systematic two-day intensive
3D printing is everywhere in dentistry today, however the technology is far from plug and play. Understanding the key factors in the complex photochemical printing process that starts with optimal object design and material selection and extends through printing to washing to curing as part of a validated workflow is vital in order to achieve consistent, accurate results. This two day program delivered by industry experts is designed both for new users looking to upskill fast as well as current users who need to better understand every aspect of 3D printing.
Course overview
• Overview of 3D printing technologies (FDM, SLA, DLP and MSLA printers), their applications, benefits, ROI.
• Printer and environment setup, calibration, resin tank installation, build platform alignment.
• How to calibrate resins to the printer.
• Selecting materials, types of dental resins; handling and storage to avoid contamination and premature degredation.
• Types of software: design, mesh editing and slicers.
• File formats.
• Scanning and importing, converting intraoral and CBCT data to 3D models
• Design principles: Anatomy considerations, occlusion, margins and ensuring printability.
• Preparing for print: File import, orientation, supports generation in basic slicer software.
• Software tools for mesh repair, error detection.
• Monitoring print parameters like layer thickness, exposure time and print speed for dental accuracy.
• Washing techniques.
• Curing methods.
• Validated workflows.
• Common pitfalls.
• Printing more complex designs like surgical guides, aligners and implant models, etc.
• Optimisation for reducing material use.
• Slicer software deep dive.
• Troubleshooting common issues.
• Reasons why resin prints fail.
• Integrating 3D printing into a dental lab or clinic.
• Maintenance tips.
• Future trends: AI-assisted design, design outsourcing and new materials.
• Next steps – Advanced training, consultancy, where to get help.
And so much more...
Terry
Jeroen
Industry set for disruption as Jayne AI™ promises smarter phone reception
Artificial intelligence has rapidly entered the front offices of dental practices across Australia — but according to industry insiders, most of it is missing the mark.
“AI phone reception for dental practices is already here... but it’s all wrong,” says Dr David Moffet, who this week announced the upcoming launch of Jayne AI™, a dental-specific receptionist AI trained on the intellectual property of renowned dental phone skills coach Jayne Bandy.
Dr Moffet argues that the majority of AI reception tools currently on the market are built on generic datasets and templated scripts.
“Every AI out there is trained on generic data. Generic scripts. Generic assumptions. Generic outcomes,” he said. “None of them have been built using credible dental-specific IP — particularly the kind that actually converts enquiries into booked and kept appointments.” That, he says, is where Jayne Bandy comes in.
A recognised leader in dental phone training
Jayne Bandy is widely regarded within the Australian dental community as the country’s leading phone skills trainer. Having worked as a dental receptionist in one of Australia’s most successful practices, Jayne later transitioned into coaching and consulting, training front office teams nationwide, as well as in England, New Zealand and the USA.
Over the course of her career, she has reviewed and analysed what Dr Moffet describes as “tens of thousands — more likely hundreds of thousands — of real dental practice phone calls”.
“She knows the patterns. She knows the traps. She knows why humans fall off script,” Dr Moffet said. “Most importantly, she knows how to convert more callers into appointments that are not only made — but are also kept.”
From human coaching to AI framework
For the first time, Jayne’s proprietary frameworks, call structures and language patterns are being embedded directly into an AI platform designed specifically for dental practices.
Branded as Jayne AI™, the system is being positioned as the “world’s first dental reception AI trained on Jayne Bandy’s IP”.
According to Dr Moffet, the goal is not to replace human receptionists, but to enhance practice performance and eliminate common front-desk pain points.
“Dental practices struggle with missed calls, inconsistent scripting, staff turnover and the emotional toll that can come with front desk roles,” he said. “We’re building something that answers every call, applies proven conversion psychology and delivers consistency without staff dramas.”
The product is expected to launch publicly within three to five weeks. In the lead-up, a limited number of “Founding Dental Practices” are being invited to gain early access.
Practices selected for the initial rollout are being promised:
• Increased appointment bookings;
• Every call answered and with fewer front-desk errors;
• Reduced staff-related disruption; and
• Higher new-patient conversion rates.
Dr Moffet believes the timing is significant.
“Practices are under pressure. Competition is stronger. Patients have more choice than ever,” he said. “The practices that convert enquiries best will win. This gives them an unfair advantage.”
A sign of what’s
next?
AI adoption in healthcare administration is accelerating, particularly in areas such as appointment scheduling, patient communication and call triage. However, sector-specific training data is increasingly seen as the differentiator between generic automation and meaningful performance improvement.
Whether Jayne AI™ will reshape how dental practices handle inbound calls remains to be seen, but its creators are confident.
“If you’ve been looking at how to answer your phones better,” Dr Moffet said, “this is exactly what you’ve been waiting for.”
Try booking a dental appointment through Jayne AI by calling (02) 9000-1965 and chat with the bot. For more information, go to https://JayneAI.dental or scan the QR code above.
think handpieces. think Greens.
TORNADO
Protective Shield (PV D treatment)
More power - 30 Watt*
More quiet - 55 dB A
Head size - 12.2 mm 13.1 mm
4 asymmetrical mixed sprays
LED Light
2 years warranty
Tornado LED 1600908-001
Tornado LK 1600907- 001
William Green Pty Ltd
47- 49 Mary Parade
Rydalmere NSW 2116
Ph + 61 2 8865 0300
TORNADOS
Protective Shield (PV D treatment)
More power - 24 Watt*
More quiet - 58 dBA
Head size - 10.9 mm 12.2 mm
4 asymmetrical mixed sprays
LED Light
2 years warranty
Tornados LED 1600933-001
Tornados LK 1600932- 001
Designed for reliability and clinician comfort, Bien-Air manufactures high-precision Turbines, Straight and Contra-Angle Handpieces, Micromotors, Implant and Oral Surgery Units, Laboratory Handpieces and Maintenance Units in Switzerland. Known for smooth operation and durability, Bien-Air products support procedures from preventative and restorative dentistry to oral surgery and implantology. Bien-Air are renowned for innovative, Swiss precision engineering, high power with smooth operation, excellent ergonomics and excellent durability and longevity.
Piksters® launches new colour-coded
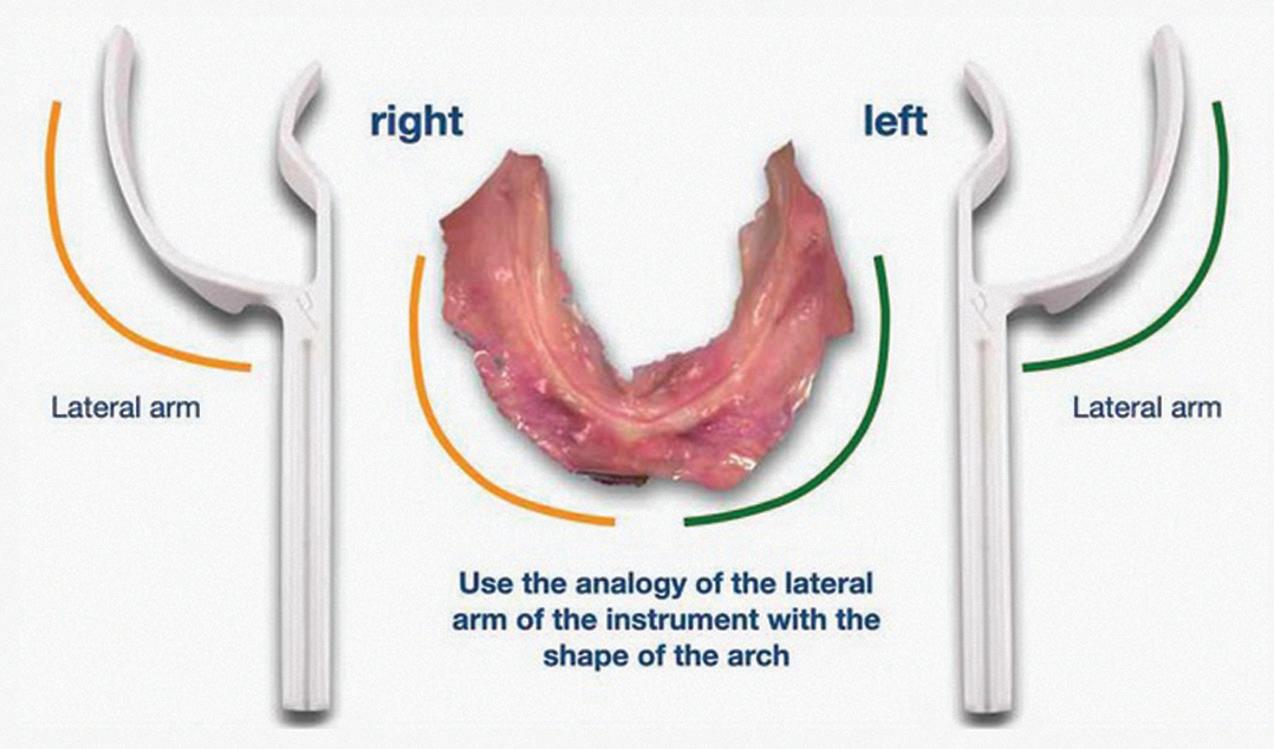
Piksters, Australia’s most used and recommended interdental brush system, has launched a new, more precise colour-coded version of its innovative Gap Sizing Probe, now covering 11 Piksters sizes including 000 and 8. This update makes it faster and easier than ever for dental professionals to prescribe the correct interdental brush size for their patients.
Originally introduced as a 9-size monochrome probe, it was a popular practical solution to eliminate guesswork, without opening packets of brushes to test sizes and wasting brushes that did not fit. It quickly became a valued clinical tool. The new, updated colour version builds on that success.
“The new probe removes the trial-and-error process, saving clinicians time,” said Piksters founder and Australian dentist, Dr Craig Erskine-Smith. “We increased the accuracy to make it more predictable. While no probe system is 100% predictive, it eliminates most of the problems in selecting a brush size.”
The updated probe is colour-coordinated to match the corresponding Piksters brush sizes. This alignment allows clinicians to instantly correlate the measured interdental space with both the colour and Pikster size number printed on the probe handle, simplifying chairside prescribing.
To use the probe, gently insert it into the interdental space and identify the band at the point it touches. This then corresponds to the same band on the handle to show the Piksters colour and size.
“For many years we have supported practices with Piksters Professional Packs for sampling,” Dr Erskine-Smith said. “The original probe helped systemise sizing; The new colour-coded probe extends the capability up to size 8 and down to the popular size 000 and is even more accurate, intuitive and consistent.”
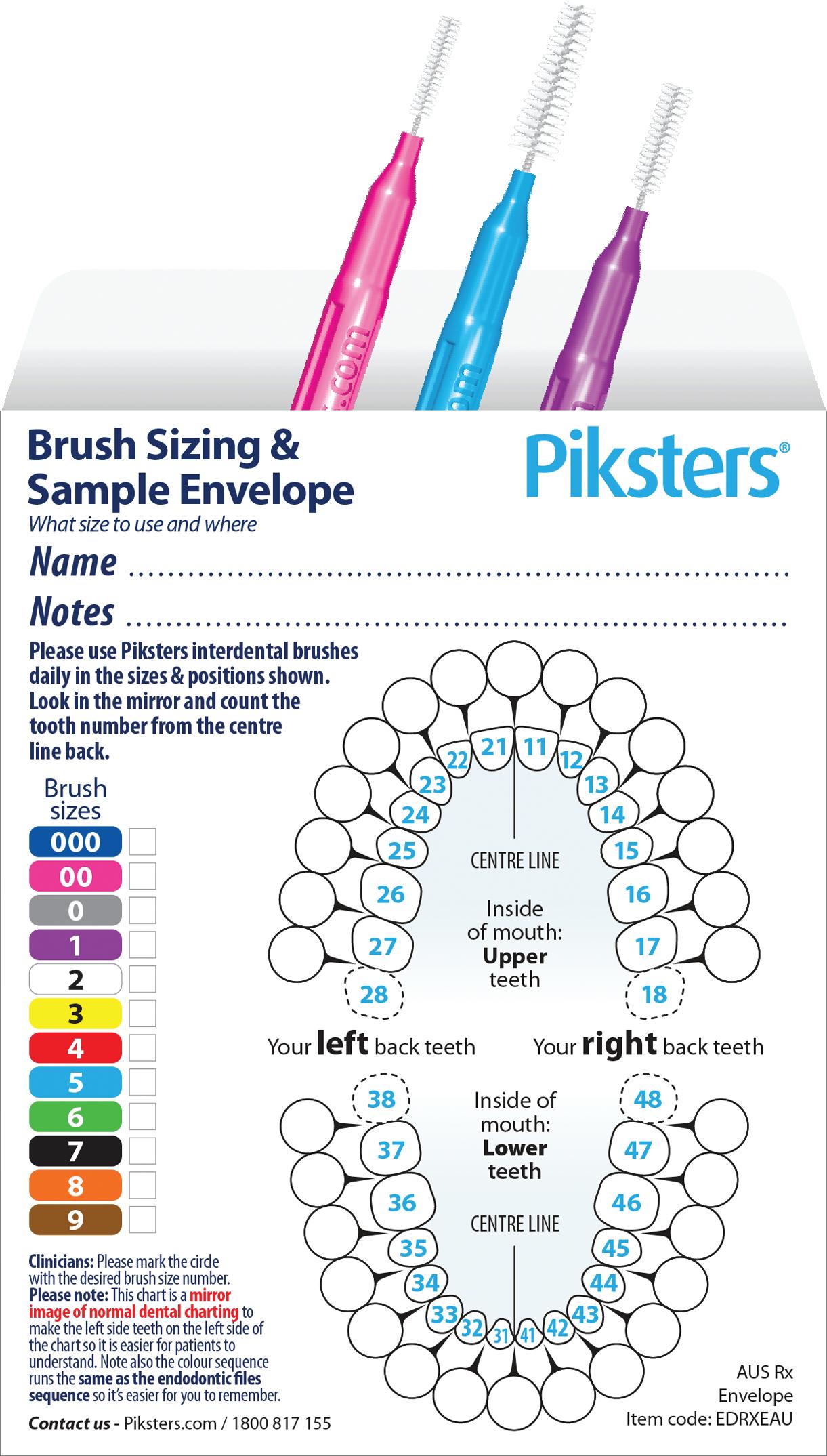
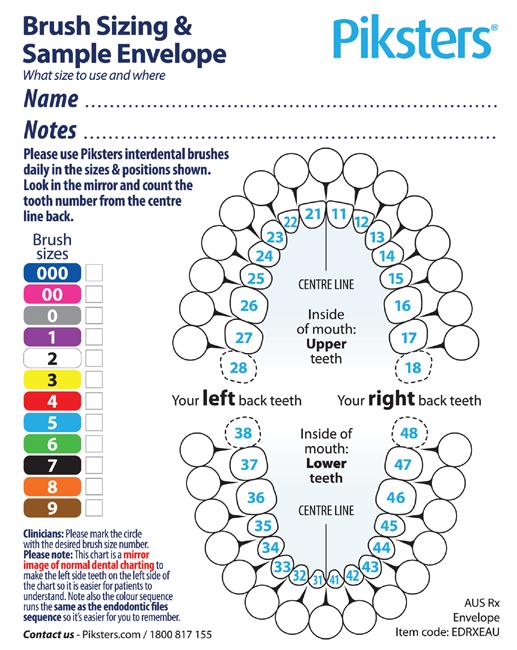
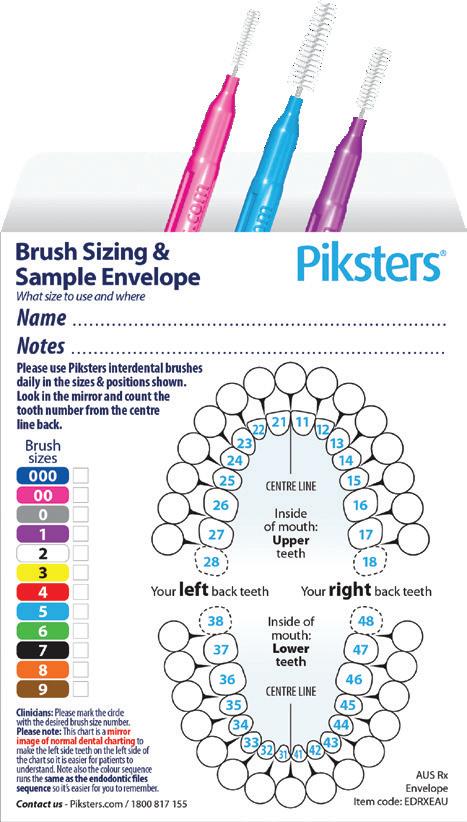
The Prescription Sampling Envelope forms part of the 3-Step Piksters Prescribing System comprising:
• SIZE: Clinicians use the Piksters Gap Sizing Probe to determine the relevant interdental brush size;
• PRESCRIBE: The tooth position and correct Pikster size are recorded on a “Mouth Map” available on Prescription Pads or the new Prescription/Sampling Envelope; and
• SAMPLE: Patients receive appropriately sized samples from a Professional Pack, ideally in the sampling envelope in a sufficient quantity to establish good habit.
Clinical evidence shows interdental brushes provide more effective interdental cleaning than dental floss, with significantly higher patient compliance when properly sized and professionally prescribed.
“The new colour probe represents a major advance in providing an affordable, accurate, time and brush saving way to provide the patient with the right size Pikster to help improve gingival, periodontal and restorative outcomes,” Dr Eskine-Smith said.
The Piksters Colour Gap Sizing Probe is autoclavable plastic and available in single and triple packs. It is also included in the latest Piksters Standard Professional Packs supplied to dental practices nationally. Modestly priced at $4.95 for single packs and $9.95 for triple packs, the Probes are available from Erskine Dental. The new A6-sized Brush Sizing and Sample Envelopes are available free to dental practices nationwide from Erskine Dental. Free A6 and A5 prescription pads are also available. Call Erskine Dental on 1800-817-155 or see erskinedental.com
Presenting the NEW 3-STEP Piksters Prescribing System
Prescription Envelopes
NEW Mouth Map & sample envelope... in one.
No need to give patients loose brushes and separate prescription pad sheets. Put it all together into a neat envelope with the prescription written on it and the brushes inside.
NEW- Both Pads & Envelopes are now in easy-to-read A6 postcard size
Implant Dentistry
The specialist perspective on common surgical and restorative quandaries
SYDNEY - JUNE 26-27 2026
BRISBANE - AUGUST 21-22 2026
Presented by Specialists Prof. Axel Spahr and Dr Tom Giblin
Professor Axel Spahr
Specialist Periodontist in Private Practice and Head of the Discipline of Periodontics and Program Director of the Doctor of Clinical DentistryPeriodontics post-graduate program at The University of Sydney Dental School.
Doctor Thomas Giblin
Specialist Prosthodontist in Private Practice
President, International Congress of Oral Implantologists, Diplomate ICOI, Board Member of Australian Society of Implant Dentistry (ASID), Member of ADA, ACP, IAG, AARD.
This advanced course is tailored for dentists with prior experience in implant surgery, aiming to further refine their expertise and clinical proficiency. The program is designed to deepen participants’ understanding and enhance their skills in both the surgical and restorative aspects of implant procedures. It emphasizes essential clinical topics to optimise outcomes and success rates, including practical insights into common challenges and solutions.
without abutment
ONE - FRIDAY
Prosthetic
Considerations
n Evaluating the digital workflow in implant dentistry: practical benefits versus technological novelty.
n Digital shade analysis and lab communication.
n Prosthetic design single / bridge /full arch / removable.
n Restorative materials.
n Impressions vs scanning.
n Optical and biomechanical properties of natural teeth and restorative materials and why it matters.
n Restoration design and preparation geometry.
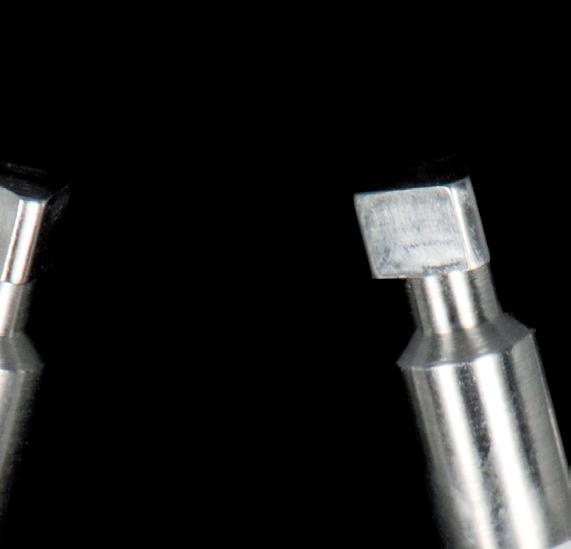
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.
n Fitting and delivery of indirect adhesive restorations.
n Verification of treatment sequences and outcome validation.
n Breaking down complex cases with novel solutions to restorative dilemmas.
n Practical clinical applications and case studies.
DAY TWO - SATURDAY Surgical Considerations
n Patient selection and comprehensive treatment planning.
n The effects of systemic diseases and medications on surgical outcomes, healing and implant success.
n Risk assessment (SAC), and the influence of implant type, material, surface characteristics and implant/abutment connections.
n The use of short and reduced-diameter implants.
n Guidelines for implant planning, key parameters and management of peri-implant tissues.
n Immediate, early and late implant placement strategies.
n One-stage versus two-stage implant surgery techniques.
n Freehand versus guided implant placement methods.
n Implant maintenance to avoid problems.
The matrix® is the first-ever specifically designed gies such as CAD/CAM allows to plan the restoration of the abutment and without full digital without
Supported by The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept
n Surgical instruments, materials, and common complications.
Discover more
Exclusively distributed by Swiss Thinking. Shared Success.
www.tri.swiss
#DIGITAL IMPLANT
Welcome to Zirkonzahn Australia
A fully equipped centre designed to support clinics and laboratories across the country
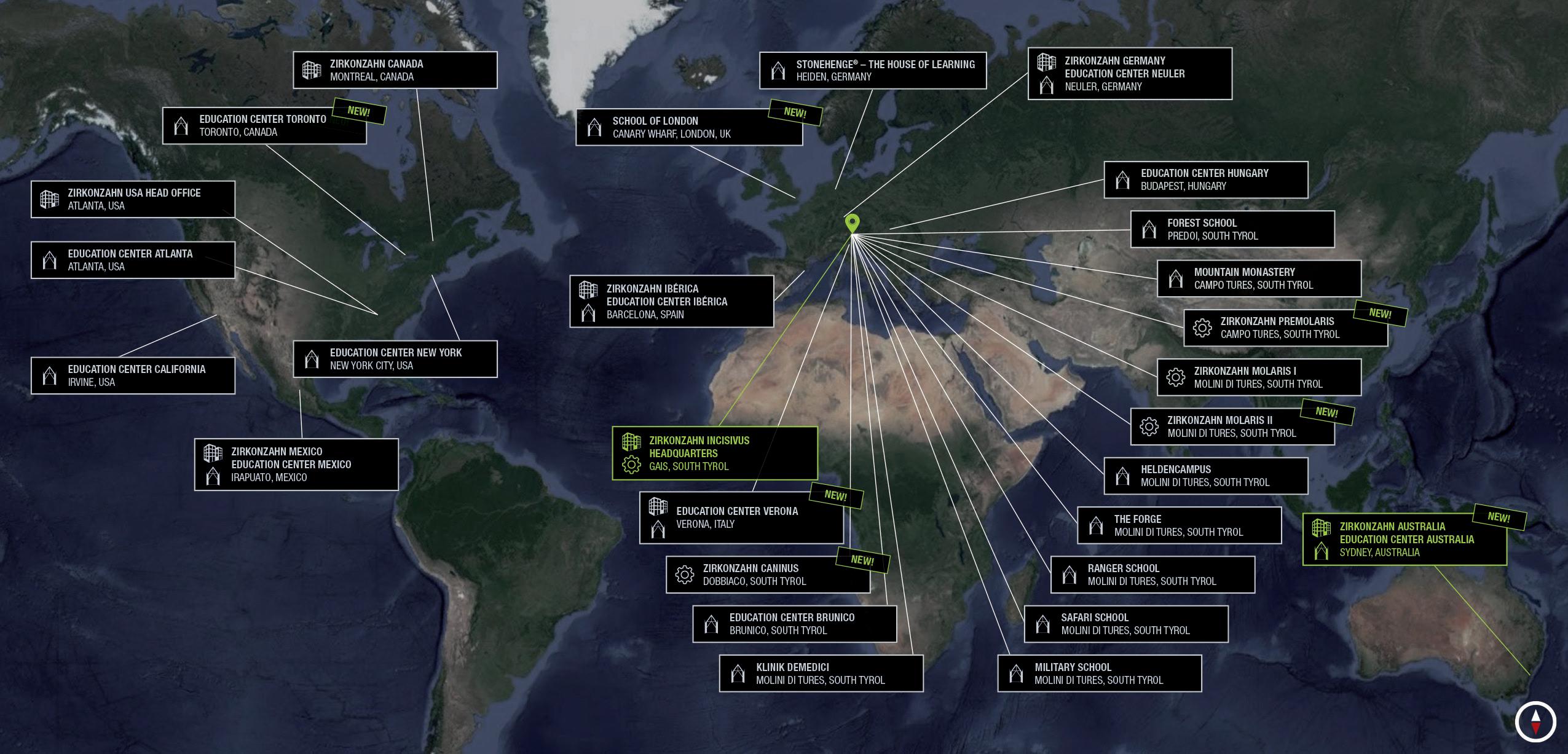
Located in the Sydney suburb of St Leonards, just minutes from the city centre, Zirkonzahn Australia becomes the company’s 13th location worldwide.
In this new facility, dentists and dental technicians can take part in on-site training courses and live demonstrations dedicated to Zirkonzahn products, equipment and digital workflows.
In addition, the educational offering also includes a wide range of webinars, accessible remotely, as part of the Zirkonzahn School – a structured and comprehensive programme designed to teach the effective use of Zirkonzahn equipment and materials without knowledge gaps.
Zirkonzahn Australia also includes a local logistics department, ensuring fast and reliable delivery of materials without waiting times. In addition, Rian Barnard, Zirkonzahn’s on-site Dental Technician and CAD/CAM expert, is also available to support customers and prospective clients in developing their workflows, showcasing the system’s various components, assisting with on-site installation and answering all related technical questions.
With the recent opening of this new dedicated service, supply and support facility, users in Australia can now explore Zirkonzahn’s innovations first-hand without having to travel to the headquarters in Italy – which, of course, always remains worth a visit. Zirkonzahn’s doors are always open to professionals interested in discovering where all products are created and in experiencing the South Tyrolean culture that has shaped the company since its foundation.
Figure 1. From a one-person business to a global company: Today Zirkonzahn counts over 350 employees, with its headquarters, main education centres and production sites in South Tyrol, plus additional facilities in seven countries worldwide.
Figure 2. From the Alps to Sydney: Zirkonzahn lands in Australia with a modern, fully equipped facility.
3 (above). One of the company’s three production halls dedicated to implant prosthetic components.
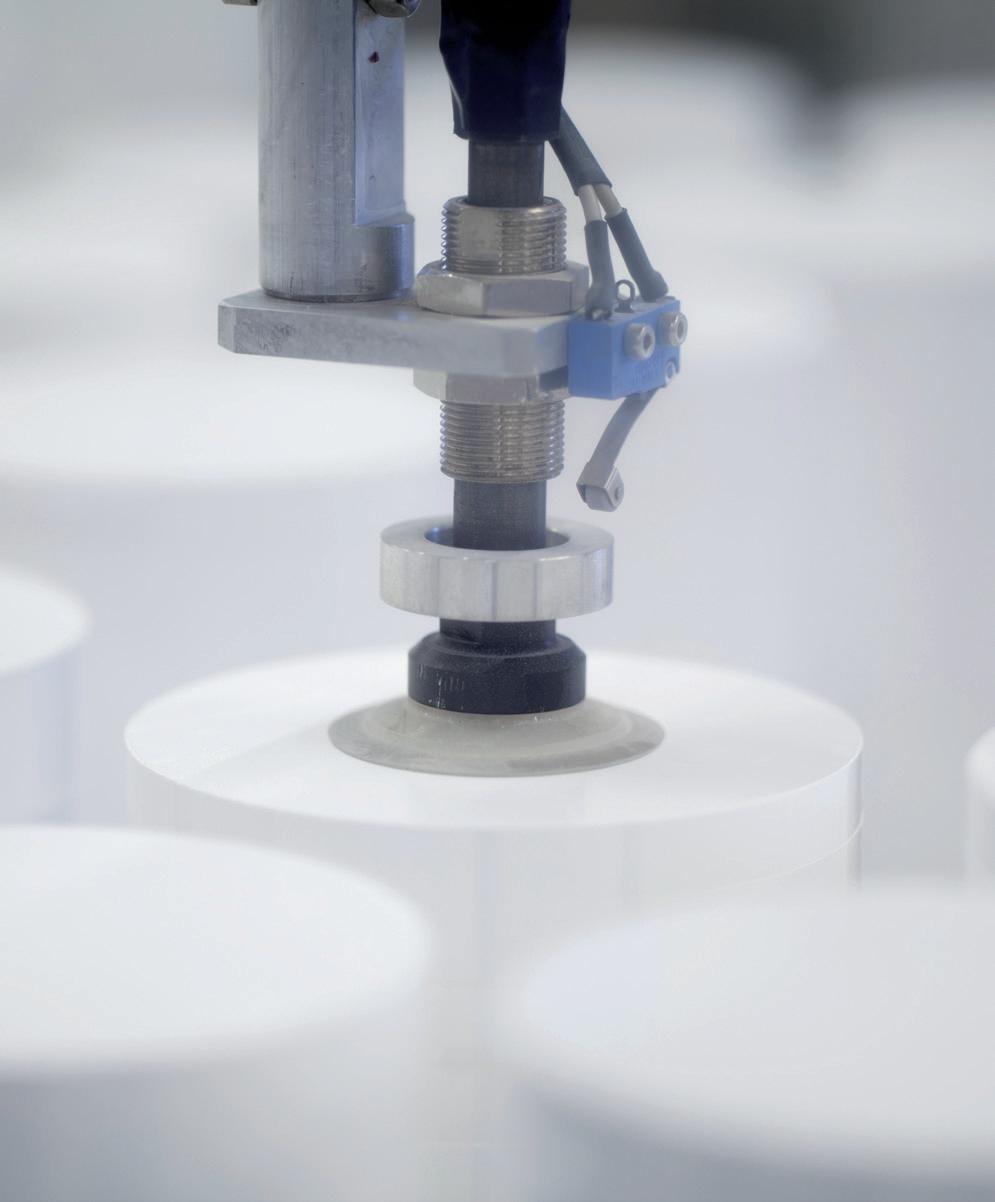
Figure 4 (right). Zirconia production. Each blank is accurately checked after every step, via specific tests and measurements to control hardness, dimensions, density, colour, translucency and materials’ shrinkage.
LSetting new standards in digital dentistry
ocated in the heart of the Italian Alps and guided by the core values of discipline, innovation, trust and responsibility, Zirkonzahn has been offering solutions and approaches for the dental sector since its founding in 2003. The expertise developed over the years is passed down from father to son – both Master Dental Technicians – ensuring continuity and creating longlasting relationships based on mutual trust.
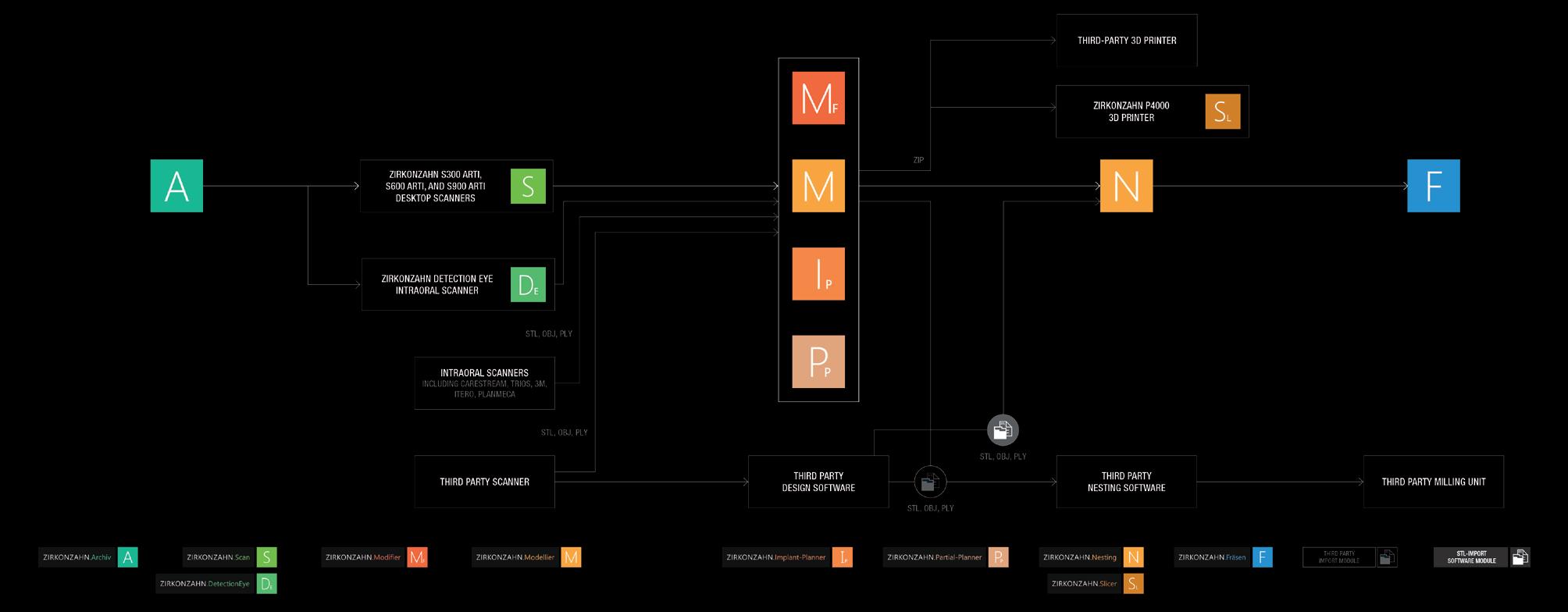
From patient diagnostics to the final restoration, Zirkonzahn’s goal is to optimise collaboration and communication between dentists and dental technicians by providing a complete workflow with perfectly coordinated tools. Under the motto “Everything from a single source”, all milling units, dental materials, equipment, software, tools and TGA-approved implant prosthetic components are conceived and developed in-house. This guarantees full control over production and compliance with the highest quality standards, ensuring seamless compatibility among all products.
With Zirkonzahn, customers do not simply purchase a product: they access an entire working philosophy that combines a wellcoordinated dental workflow (digital and/or analogue), a complete service package and reliable support.
Thanks to the multilingual helpdesk, users benefit from fast and comprehensive assistance for both technical and dental-technical issues at any stage of their workflow.
Zirkonzahn is open
Driven by continuous innovation and a search for smart, unconventional solutions, all Zirkonzahn hardware components and software modules generate open data formats (e.g., STL, OBJ). These are compatible with all open CAD systems, milling units and 3D printers. Likewise, open data from other manufacturers can be processed with Zirkonzahn’s wide range of products.
This openness allows customers to build a personalised and upgradable system, adaptable to their needs through numerous combinations. Even the design of the CAD/CAM system itself can be customised on request, in various colours and styles, to express each user’s identity.
Figure
Always at your side to face the future
In the dental market – and in the broader world of work – staying informed about the latest advancements is a sign of professionalism, competence and versatility. Professionals particularly value partners who, beyond delivering excellent results, provide valuable insight into modern and effective techniques to meet every requirement. From new materials to advanced CAD/CAM technologies, every Zirkonzahn innovation aims to enhance communication between clinic and laboratory, ensuring
the perfect balance of function, aesthetics and streamlined technical processes.
As always, Zirkonzahn stands alongside its customers—ready to walk with them through the daily challenges of work.
Discover the Zirkonzahn world! Scan the QR code or contact Valentina Sacco - valentina.sacco@zirkonzahn. com - Tel: +39-0474-066663 - or Zirkonzahn Australia – Sydney Team - Hanna Kukula – Mob: 0422-770-640 – hanna. kukula@zirkonzahn.com
Assembly of milling units, scanners and furnaces – all in-house.
ICE PLUS
ZIRCONIA UPPER AND LOWER RESTORATION ON FOUR IMPLANTS EACH
- Acquisition of implant positions using photogrammetry technology, and of soft tissue data using an intraoral scanner; smile design defi nition
- Printing of super- and substructures for a first try-in in the patient’s mouth; digital design of the upper and lower full arches in Prettau® 2 Dispersive® zirconia as well as of the substructures in ICE Plus zirconia
- After milling and sintering, bonding of the superstructures to the substructures
- Minimal layering with ICE Ceramics and characterisation with ICE Stains 3D by Enrico Steger
- High-gloss polishing of the restoration and insertion in the patient’s mouth
Dr. Anne-Maree Cole – The Littleton Cole Dental Centre, Brisbane, Australia
DT Werner Sauer – Werner Sauer Smile Design, Brisbane, Australia
Tips to stop patients choosing the practice down the road...
Patients don’t choose the “best” dentist. They choose the dentist that feels safest and easiest. Here are five practical ways to tilt that decision in your favour:
1. Win the decision before the phone rings
Patients decide long before they contact your practice.
Tip: Make your website and Google profile answer basic fears:
• What happens next?
• Will I be judged?
• Is this clinic modern and trustworthy?
2. Build familiarity, not just credentials
Patients can’t assess clinical skill, so they assume competence.
Tip: Increase recognisable presence with...
ACCOUNTING
&
• Consistent branding;
• Regular updates (photos, team, activity); and
• Clear, current online presence.
3. Choose clarity over complexity
Too much technical detail creates hesitation.
Tip: Simplify your messaging with...
• Plain English;
• Clear next steps (“Book online in 30 seconds”);
• Orient your text towards the patientless “what do you do”, more “what will you do for me”.
4. Stay visible or risk being forgotten
Silence creates doubt. Invisibility feels like risk. Tip:
• Keep your website fresh;
• Encourage current reviews; and
• Light, human content (team, community, behind-the-scenes).
5. Reduce friction everywhere
Convenience is interpreted as care. Tip:
• Easy online booking;
• Fast response to enquiries; and
• Simple directions and parking info.
The takeaway
Patients don’t compare dentists on clinical excellence – they can’t. They compare how safe, clear, and easy each option feels.
Design your online presence and patient journey to remove uncertainty before they ever call — and you’ll stop losing patients quietly to the practice down the road.
FINANCIAL SERVICES FOR DENTISTS DON’T RISK SECOND BEST
Synstrat has spent many years collecting data on dental practices. We provide you with the best available knowledge on the performance of your practice relative to others. Our proven service has assisted many dentists Australia wide to create significant wealth. We are able to provide you with business accounting, practice valuation and financial advice services tailored to the dental profession.
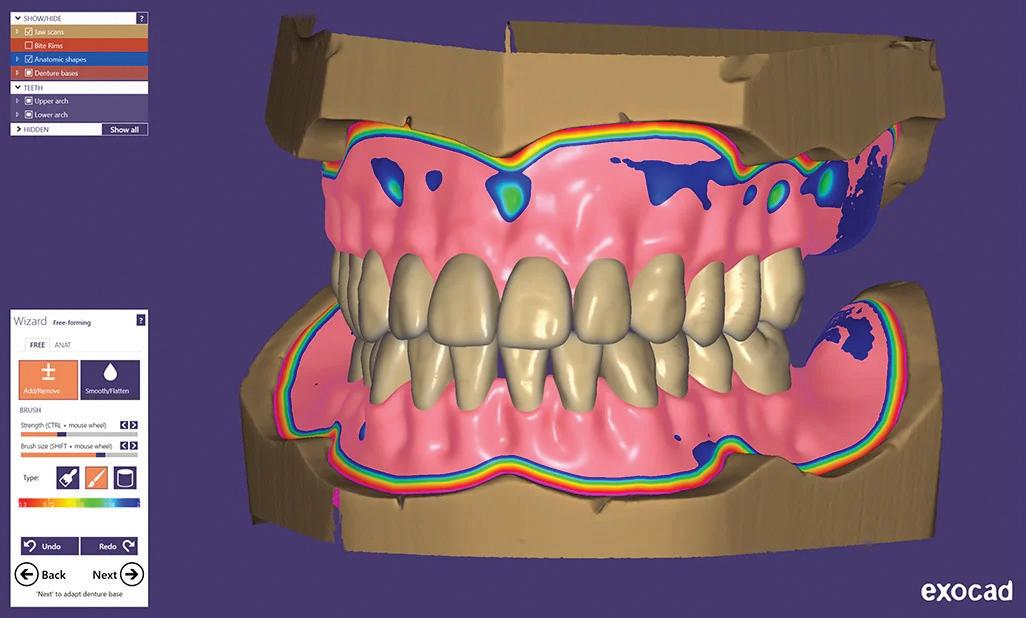
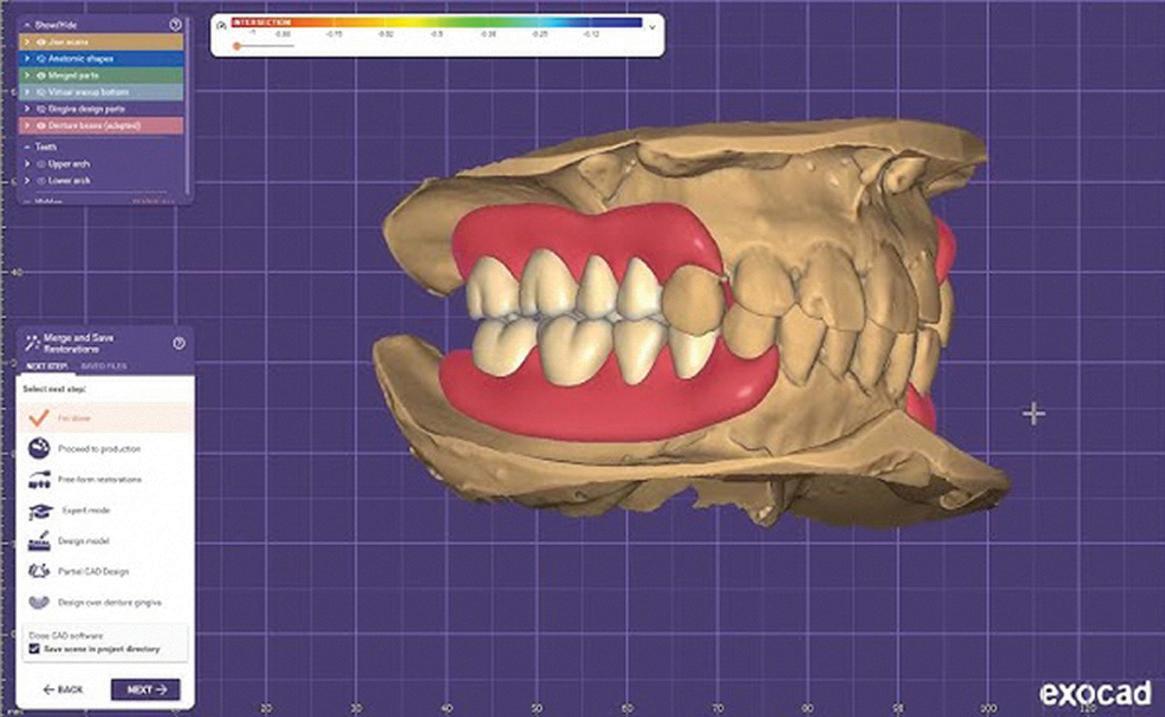
This is a structured hands-on workflow course designed to take you from setup to production-ready denture designs in just two days.
12 HOURS CPD
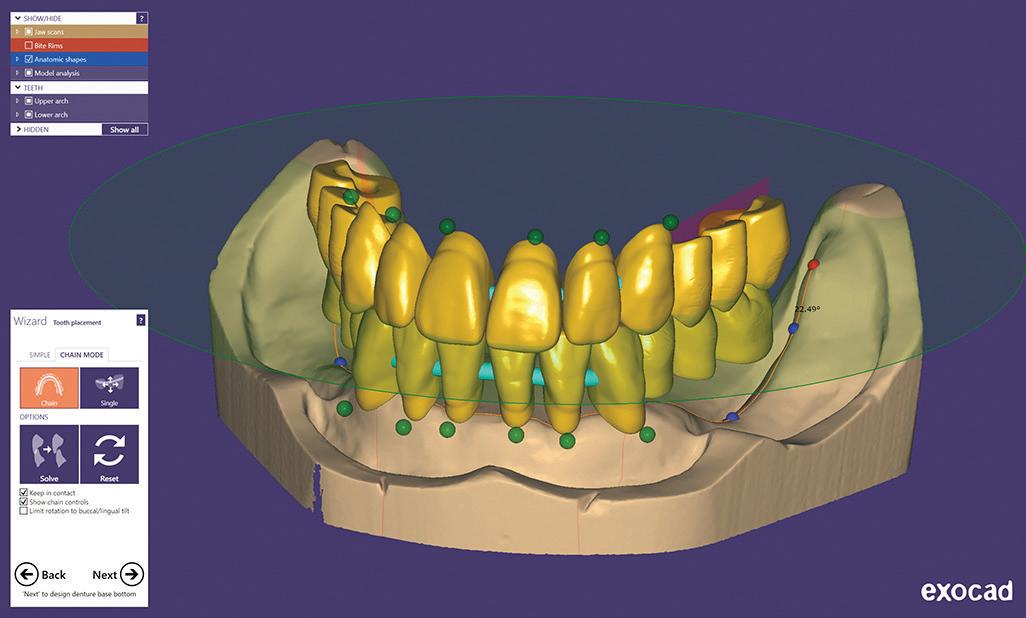
You will work through real cases, learn real workflows and deliver real outcomes — using the exocad Full Denture and Partial Denture modules.
What You Will Learn
n How to correctly set up, maintain and optimise your computer for exocad performance
n How to create clean, repeatable digital denture workflows
n Full single arch denture design from start to finish
n Complete upper and lower denture workflows
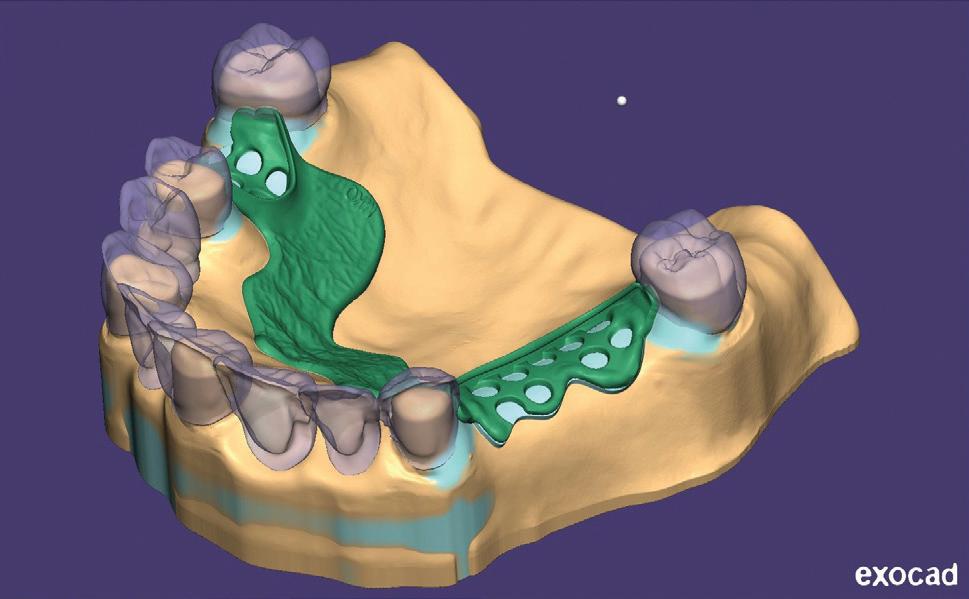
n Partial denture design, including surveying and frameworks
n Flexible denture design workflows
n How to produce accurate, production-ready files
n How to avoid the common mistakes that cause remakes and poor fit
Day 1 – Full Dentures & Foundations
You will build your understanding from the ground up:
n Computer setup and optimisation for exocad
n Case setup and scan preparation including intraoral scan acquisition and optimisation
n Single arch denture workflow (step-by-step)
n Full upper and lower denture design
n Occlusion, function and base design
n Preparing designs for digital manufacturing
You will complete both a single arch denture and a full upper & lower denture case
Day 2 – Partial Dentures & Flexible Design
Expand into more advanced workflows:
n Digital surveying and path of insertion
n Framework design (connectors, clasps, structure)
n Tooth setup for partial dentures
n Flexible denture design workflows
n Troubleshooting and design correction
n Preparing files for production
You will complete a partial or flexible denture design ready for manufacturing
Prerequisites - email terry@fabdent.com.au if you do not have the following:
n Laptop with DentalCAD 3.3 Chemnitz installed and running, fully updated (Windows updates and graphic card updates done)
n Full Denture Module and Partial Denture Module activated
n Sound knowledge of traditional denture techniques
Piksters® introduces new Right Angle interdental brushes
Piksters, Australia’s most used and recommended interdental brush system, has announced the launch of its new Right Angle Interdental Brushes.
Piksters Right Angle expands the range, providing an option for patients who require improved posterior access, greater finger leverage and hand control and improved cleaning around complex restorative and orthodontic challenges, including dental bridges and furcation tunnels.
“Piksters Right Angle is designed for use mainly on the back teeth and is excellent for cleaning around bridges,” said Piksters founder and Australian dentist, Dr Craig Erskine-Smith. “Although we already offer an extension handle for traditional Piksters brushes, the new longer Right Angle is driven by convenience. To reduce waste, we have used recycled plastic for the extra reach handle and combined this with a 90-degree pre-angled brush.”
Enhanced access for posterior cleaning
By facilitating a more direct path of insertion between teeth, the design assists in cleaning without excessive jaw opening, awkward wrist positioning or excessive bending of the wire.
The extended handle provides additional leverage and control, which may benefit individuals with reduced hand strength, finger pain, limited dexterity or difficulty managing smaller straighthandled brushes. The angled configuration also supports easier navigation along both the lingual and especially the palatal surfaces of the dental arch.
Well-suited to restorative and orthodontic care
Piksters Right Angle brushes are particularly indicated for patients with:
• Posterior implants and bridgework, where targeted plaque removal around prosthetic components is critical for the survival of the restorative work;
• Upper molars that necessitate a palatal approach, needing longer handles;
• Through-and-through furcations anywhere in mouth; or
• Fixed orthodontic appliances, where access around brackets and beneath arch wires can be challenging.
Supporting evidence-based interdental care
Research continues to demonstrate that appropriately sized interdental brushes outperform traditional flossing and are highly effective in disrupting plaque between the teeth and reducing gingival inflammation as part of a daily oral hygiene routine.
Practical and patient-friendly
Designed for daily home use, Piksters Right Angle brushes are durable and may be rinsed and reused. Many patients and dental professionals prefer using Piksters as an alternative to traditional floss and report improved compliance, convenience and comfort, particularly where larger interdental spaces are present.
Enhanced uses
T he brushes not only remove plaque, they can also be used to apply medicaments like chlorhexidine gel, GC Tooth Mousse® and stannous fluoride into periodontally compromised or caries susceptible areas, such as furcations, as part of a professionallyprescribed treatment regime.
Piksters Right Angle interdental brushes are now available in four sizes - 00, 1, 3 and 5 - in packs of six brushes. More sizes will be produced as demand dictates. Chemist Warehouse will be stocking three sizes nationally - 1, 3 and 5 - from April 2026.
Professional supply is available for Australian dental practices from www.erskinedental.com.
• 90 degree head angle saves bending the wire and reduces wire breakage.
• Long, sti handle gives better reach and control than regular handles, especially for back teeth.
• Comfortable nger-friendly handle cut-outs.
• Same size/colour coding as regular Piksters.
• 100% recycled plastic handle.
• Available from Erskine Dental in 4 popular sizes - 00, 1, 3 & 5 (6pk $4.15).
• Available from Chemist Warehouse in 3 sizes - 1,3 & 5 (6pk RRP $7.50).
Patients can buy from
Piksters launches new toothbrush
Piksters has expanded its profes sional oral care range with the launch of the new SupaGRIP Toothbrush, a dentist-designed toothbrush created to make daily oral hygiene easier, more com fortable and more effective.
“The launch of the new SupaGRIP Toothbrush is in keeping with our commitment to developing bespoke oral hygiene products that address specific challenges faced by the community,” said Piksters founder and Australian dentist, Dr Craig Erskine-Smith. “Daily brushing is essential but can be difficult if you have compromised dexterity.”
Engineered with a high-friction, rubberised handle, the SupaGRIP Toothbrush is designed to enhance control while brushing. The ergonomic, easy-grip design sits comfortably in the hand, offering improved control and stability for users seeking greater precision and comfort during everyday brushing.
Many NDIS providers and disability support groups recommend thicker toothbrush han dles for people with limited motor control, as they can improve grip while reducing the muscle and joint pressure required to brush properly—which may help with main taining oral hygiene independence.
Indeed, according to independent research utilising electromyographic studies of the forearm muscles and examining the related plaque index, an “optimal [toothbrush] handle diameter will result in increasing the subjective comfort rating which will further increase the user performance and will lower the risk of muscle fatigue.” Bhatia et al 2017
Developed by Dr Erskine-Smith, the SupaGRIP Toothbrush will enable anyone with a disability or age-related decline in manual dexterity greater ability to maintain their oral health through daily brushing. The textured handle supports a secure hold, even in wet conditions, helping users maintain consistent brushing techniques with confidence.
Available in six vibrant colours, SupaGRIP combines functionality with a simple, appealing design suited to everyday oral care routines.
Piksters is an Australian-owned oral care company, designing and manufacturing products sold globally. For more information about the Piksters SupaGRIP Toothbrush or to purchase, visit www.piksters.com.
Professional supply is available for Australian dental practices from www.erskinedental.com.
RO and maintaining water quality during boil water advisories
Many large hospitals and now smaller health care facilities utilise reverse osmosis (RO) to purify municipal water and perform periodic bacterial and endotoxin testing on the locally produced RO water to ensure these levels remain within an acceptable range. This report describes the use of RO to manage water needs in a large (746-bed) medical centre in the city of Springfield, Massachusetts, USA during a major disruption to the municipal water system in September 2023. Because of a water main break, the municipal water authority issued a boil water notice (BWN) to the entire city due to the potential of bacterial contamination of the water supply. The expectation was that the BWN would last for 48 hours. The facility needed non-sterile water for handwashing and patient bathing, scrub sinks outside of operating rooms, dilution of cleaning solutions for daily cleaning of shared patient care equipment, ice machines for patient consumption and control of swelling and eyewash stations. RO systems were used to treat the municipal water to provide the hospital’s patient care areas with purified water for hand washing, bathing and other patient care activities. RO water was transported using water jugs, providing water for handwashing and patient bathing. By providing purified water to patient care areas where non-sterile water was needed, this approach prevented interruptions in services such as elective surgeries. This approach distinguished the facility from other local hospitals, where elective surgeries were cancelled. With increasing threats from climate change, aging infrastructure and other natural disasters, a robust emergency water plan is essential for healthcare facilities and RO water could play a significant role.
Smith J, et al. A bridge over troubled water: reverse osmosis to maintain patient care in a boil water notice. Infect Control Hosp Epidemiol 2025;46:330-332.
The
world’s first implant approved for full digital restorations without abutment gies suchas CAD/CAM milling or3Dprinting.The implant concept onthe implantwithout the use of the abutment and without manual cementation.
ADVANCED HEMOSTAT WITH WOUNDHEAL
For topical applications and internal surgical use. Effective in patients using anticoagulants.
• Water soluble, oxidised-etherified regenerated nanocellulose.
• Biocompatible & pH neutral (~7.2).
• Non expanding hemostat, forming sealing clot & reducing pain.
• Tightly woven matrix of plant fibres.
• No animal derived products.
• 100% absorbable without any residue.
• Easy to use, cut, fold or layer and cost effective.
• Sterile, single use packaging. Minimum 3 years expiry.
How BloodSTOP iX Works:
• Adheres to wet/bleeding surfaces.
• Fast acting bleeding control. Actively initiates clotting cascade.
• Creates physiological environment for proliferation of tissue growth and wound healing.
• Transforms into a sticky translucent gel that adheres to and seals the wound.
• Odourless & tasteless. Can be easily removed by irrigation.
• Forms protective layer, preventing contamination.
• Enables easy monitoring of the wound.
The world’s first implant approved for full digital restorations without abutment
Indicated for: Any intraoral wound | Extraction / ridge preservation | Sutures / flap marg i ns | Do no r & re ci pient sites of gi n gi va / con n ec ti ve ti ss ue grafts | Mo uth ul ce rs
The matrix® isthe first-everdentalimplant connection thathasbeen specifically designedforthenew digitalmanufacturingtechnologies suchas CAD/CAM milling or3Dprinting.The implant concept allows to plan the restorationdirectly onthe implantwithout the use of the abutment and without manual cementation.
The matrix® isthe first-everdentalimplant connection thathasbeen specifically designedforthenew digitalmanufacturingtechnologies suchas CAD/CAM milling or3Dprinting.The implant concept allows to plan the restorationdirectly onthe implantwithout the use
connection thathasbeen
Mastering your Practice Exit Strategy
How to get the best results when selling one of
your greatest assets
A dental practice is usually one of the most valuable assets in a dentist’s life.
When it comes time to sell, many do so with little understanding of timing, the value of their practice and how to present it effectively to a buyer. By attending this seminar you will learn:
1. The pros and cons of 7 different exit strategies and which are right for you
2. 20 things you can do to get a better result in your sale without working any harder
3. How to time your exit for optimal return
4. How to avoid common pitfalls that devalue practices in the final years of ownership
6
HOURS OF CPD
5. How to identify the likely buyer profile for your practice and what will they be looking for?
6. How to value dental practices
7. How do you handle staff discretion, confidentiality and disclosure?
8. Strategies for transferring patients effectively from seller to buyer
9. Confidentiality, restraint of trade, leases, staff entitlements and other legal considerations
10. Tax implications and strategies when selling
Presented by Simon Palmer (Practice Sale Search) with expert speakers on dental finance, legal and accounting
With more than 20 years’ experience in dental practice sales, Simon Palmer has extensive knowledge of and insight into the complexities and sensitivities involved in buying and selling dental practices. Simon’s business, Practice Sale Search, sells more than 120 practices per year. He is a regular writer for dental publications and journals, and is regarded as an expert on dental practice purchases and sales in Australia and New Zealand.
BRISBANE : 27 JUNE 2026 DATES
ADELAIDE : 20 JUNE
SYDNEY : 26 SEPTEMBER
MELBOURNE : 17 OCTOBER
ONLINE CPD CENTRE
Question 1. Which ethical principle is most directly challenged when a dentist recommends unnecessary or overly expensive treatments for financial gain?
a. Confidentiality
b. Justice
c. Beneficence
d. Autonomy
Question 2. What is a key requirement for valid informed consent in dental practice?
a. The patient signs a consent form.
b. The dentist explains only the benefits of treatment.
c. The patient understands risks, benefits, alternatives and costs.
d. The procedure is completed quickly.
Question 3. A clinician continuing to perform procedures beyond their level of training instead of referring is primarily violating...
a. Autonomy
b. Non-maleficence
c. Confidentiality
d. Justice
Question 4. What is the main ethical issue when a dentist has a financial interest in a dental laboratory they recommend?
a. Breach of confidentiality.
b. Conflict of interest affecting professional judgment.
c. Lack of informed consent.
d. Inadequate sterilisation.
Question 5. If a dentist accepts large payments for treatment they do not complete, this behaviour is best described as:
a. Overtreatment
b. Professional incompetence
c. Fraudulent practice
d. Ethical misunderstanding
INSTRUCTIONS:
Question 6. What is the primary purpose of Instructions for Use (IFU) for reusable medical devices (RMDs)?
a. To advertise the product’s features.
b. To provide step-by-step guidance on use and reprocessing.
c. To outline pricing and supplier details.
d. To replace staff training.
Question 7. Why should dental clinics maintain easy access to IFUs?
a. They are required only for audits.
b. They contain legal contracts with suppliers.
c. They provide essential guidance for correct reprocessing of devices.
d. They are only useful for new staff training.
Question 8. What is a key risk of relying on third-party IFU databases?
a. They are illegal to use.
b. They may not include any manufacturer data.
c. They are often infrequently updated and may not have the latest information.
d. They are more expensive than purchasing devices.
Question 9. According to ISO 17664 standards, what must manufacturers provide in the IFU?
a. Only cleaning instructions.
b. At least one validated method for cleaning and sterilisation.
c. Instructions for disposal only.
d. Marketing comparisons with other products.
Question 10. What happens if a clinic reprocesses a single-use medical device?
a. Nothing changes legally.
b. The device becomes reusable automatically.
c. The clinic becomes the legal manufacturer and assumes full responsibility.
d. The manufacturer remains responsible.
Question 11. What is the main reason dentists are advised to avoid inserting a needle to the hub?
a. The hub is the weakest part and may break inside tissue.
b. It increases the risk of intravascular injection.
c. It causes more patient discomfort.
d. It makes aspiration less effective.
Question 12. Which type of syringe is least likely to give a false negative aspiration?
a. Manual aspirating syringe.
b. Non-aspirating syringe.
c. Reusable metal syringe.
d. Auto-aspirating syringe.
Question 13. Which of the following factors can cause failure of maxillary buccal infiltrations?
a. Incorrect syringe angle.
b. Infection, thick cortical bone, or collateral nerve supply.
c. Wrong type of aspirating syringe.
d. Overuse of computer-controlled analgesia.
Question 14. What pharmacological property of LA is most influential on the duration of its action?
a. Lipid solubility
b. pKa
c. Half life
d. Protein bounding
Question 15. What is the recommended practice when administering local anaesthetic injections?
a. Inject rapidly to reduce treatment time.
b. Aspirate only when performing blocks, not infiltrations.
c. Always inject against bone, aspirate more than once and inject slowly.
d. Use the maximum volume possible to ensure success.
Question 16. What is the main reason nylon splints are considered unsuitable for definitive occlusal therapy?
a. They are too brittle and fracture easily.
b. They lack rigidity and deform under occlusal forces.
c. They are too expensive to produce.
d. They cannot be inserted into undercuts..
Question 17. Which material is described as the “gold standard” for occlusal splints?
a. Nylon
b. POM
c. PMMA
d. 3D-printed resin
Question 18. What is a key advantage of POM over PMMA in certain clinical situations?
a. It is easier to repair chairside.
b. It offers superior aesthetics with transparency.
c. It has greater toughness and fatigue resistance.
d. It bonds easily to other materials.
Question 19. What is a major limitation of 3D-printed (VAT polymerised) splints according to the article?
a. They cannot be digitally designed.
b. They are too rigid for patient comfort.
c. They have inferior mechanical properties compared to milled PMMA.
d. They are impossible to manufacture quickly.
Question 20. According to the article, which properties are essential for effective occlusal therapy?
a. Flexibility, softness, and ease of insertion.
b. Transparency, colour stability and cost.
c. Rigidity, polishability, and dimensional stability.
d. Elasticity, thickness and opacity.
Dental splints under scrutiny: Nylon, PMMA, POM and 3D-printed
A summary of the latest research
By Emer. Prof. Laurence Walsh AO
Ceiling mounted UVC light lowers the surface bioburden in occupied clinical areas
Pathogens can persist on surfaces in clinics for prolonged periods, ranging from hours to months. Contaminated surfaces in clinics may contribute to pathogen transmission, highlighting the need for effective strategies that works between cleaning episodes. Far-UVC (200–230 nm) has gained attention due to its reduced safety risks for human skin and eyes, compared to conventional UVC light at 254 nm, which can cause significant harm to humans. This safety profile provides far-UVC with the potential to be used for pathogen inactivation in occupied clinical settings. Far UVC, with its favourable safety profile for human exposure, has the potential for continuous pathogen inactivation in occupied clinical areas. This study measured real-world bioburden reduction on surfaces in two Danish hospitals, which used lamps emitting UV light at 222 nm with a 60° dispersion angle. Efficacy assessment was done in an outpatient waiting area for respiratory disease. Bacterial sampling was performed using dipslides done daily over 6 days: 3 with far-UVC off and 3 with far-UVC on. Colonyforming units (CFUs) were quantified after 24-hour incubation at 37°C. A second part of the study involved a medical ward of another hospital, focusing on mobile workstations used by staff during rounds. A control ward with a similar layout was also evaluated. The presence and similarity of bioburden on the workstations in both wards, despite regular cleaning, were confirmed prior to the study. Weekly bacterial sampling was conducted over 14 weeks. In the waiting areas, far-UVC lamps significantly reduced mean CFU values on waiting room chair seats and backrests, from 30.8 to 8.7 and 20.7 to 6.5, respectively. Combined, the mean CFU value showed a 70.54% reduction. In the medical ward, the percentage reduction from UVC was 77.2%. Overall, ceiling-mounted far-UVC fixtures significantly reduced bioburden on surfaces in both occupied clinical settings. The farUVC light fixtures operated autonomously, providing continuous disinfection without requiring staff intervention or additional training. This allowed patient care and existing procedures to remain unaffected. Combining far-UVC with enhanced manual cleaning should offer synergistic benefits compared to manual cleaning alone. Large-scale studies are needed to determine whether far-UVC technology can significantly reduce hospitalacquired infections by continuously lowering the bioburden in clinical settings.
Mogensen EH, et al. Ceiling-mounted far-UVC fixtures reduce the surface bioburden in occupied clinical areas. Infect Control Hosp Epidemiol 2025;46:647-649.
Influenza vaccination for HCW in Victoria - effects of a government mandate
Health care workers (HCWs) have an increased risk of exposure to influenza and work in settings with an increased risk of transmitting infection to vulnerable patients. The HCW occupational risk of infection is around twice that of controls. In 2022, the Victorian government, Australia, introduced a seasonal influenza vaccination mandate for specified health care workers (HCW). This paper describes implementation of the mandate’s requirements in health care organisations by (1) Reporting 2022 and 2023 HCW vaccination coverage rates; and (2) Describing the experiences of vaccination program implementers. An analysis was undertaken of annual organisational surveillance data routinely reported by health care organisations to the coordinating centre (Victorian Healthcare-associated Infection Surveillance System (VICNISS) Coordinating Centre) from 2018 to 2023. Focus group interviews with program implementers were conducted and 27 program implementers participated in 4 focus groups, representing 12 metropolitan and 15 rural/regional health care organisations. All permanent, temporary or casual staff employed by the health care organisation were included in surveillance. Annual vaccination coverage increased from a median of 85.4% (2018-2021) to 93.6% (2022-2023). Those with “unknown status” and declinations decreased from a median of 8.2%-5.1% and 5.0%-1.1%, respectively. Implementers described increased leadership support and accountability for program delivery and a focus on educating HCWs on the mandate and how to provide evidence of vaccination. New challenges included interpreting the mandate and applying pragmatic consequences. Implementers described increased administrative burden and seeking technological solutions. Overall, the introduction of the mandate coincided with an increase in HCW influenza vaccination coverage and changes to program delivery. Investment in technological solutions can support surveillance by reducing the administrative burden and potentially increasing reporting accuracy of number of HCWs with “unknown status”. Since 2018, between 72 and 75 health care organisations annually with a combined workforce of 120,000 or more have been included in VICNISS’ surveillance, with a year-on-year increase in the number of staff captured. Vaccination coverage increased from a median of 85.4% pre-mandate (2018-2021) to 93.6% (2022-2023) with the introduction of the mandate. It is unclear whether the introduction of the mandate was directly responsible for higher vaccination coverage; other potential contributory factors include community awareness of the potential for an influenza season with high activity, improved vaccination processes in hospitals learned from delivering the COVID-19 vaccination program and heightened population awareness and vaccination acceptance. Lim L-L, et al. Vaccination coverage outcomes and health care organization program implementers’ experiences after introduction of a health care worker influenza vaccination mandate in Victoria, Australia, 2022-2023. Am J Infect Control 2025; DOI: 10.1016/j.ajic.2025.06.021 0196-6553.
tooth sensitivity
enigma no more
Building on the success of the previous webinar, Spotlight on Tooth Sensitivity is back with a NEW addition!
Dentine hypersensitivity is very common and often related conditions that can have a significant impact on patients’ daily life.
To support your professional development, Haleon invites you to view our NEW on-demand CPD webinar.
Spotlight on tooth sensitivity:
An enigma no more
Join a panel of global experts for an in-depth exploration of dentine hypersensitivity and its management. This webinar will feature a blend of insightful presentation, case studies and engaging panel discussions, providing direct scientific education on dentine hypersensitivity and related conditions.
Treatment decisions and ethical dilemmas in dentistry
By Emeritus Professor Laurence J. Walsh AO
Clinicians are constantly faced with a range of ethical dilemmas, each of which require careful consideration of professional responsibilities under the AHPRA Code of Conduct, patient rights and societal expectations. When dilemmas are mishandled or result in overtly unethical behaviour by the clinician, the accompanying coverage in the mass media and on social media can lower the reputation of the entire dental profession. This article explores some common ethical dilemmas encountered in dental practice and expands on some relevant cases as examples.
Overtreatment / Unnecessary procedures
As an example of this dilemma, during a consultation with a patient, we identify a range of potential treatments. Some of these are necessary and some are optional or less urgent. The ethical dilemma arises when, from a range of options that we can imagine, we only present and recommend the most expensive or extensive procedures primarily for financial gain rather than the patient’s optimal health outcomes. In this situation, the ethical principle at play is Beneficence (acting in the patient’s best interest) vs Non-Maleficence (doing no harm) vs Autonomy (the patient’s right to choose
treatment based on full information about options). These situations contribute to a negative perception of dental practitioners as profit-driven rather than patient-focused.
Informed consent
We are obliged to ensure that a patient fully understands the risks, benefits, alternatives (including no treatment) and costs of a proposed procedure. Challenges arise when we are running late and try to rush this; if we use overly technical jargon when the patient has a low level of health literacy; and when the patient is anxious or fixated on a particular approach. The ethical principle at play here is Autonomy (patient’s right to self-determination) vs Beneficence (dentist’s duty to provide care).
Conflict of interest
This dilemma can arise when a clinician has a financial interest in a dental lab. This can create an incentive to recommend specific work from that lab, potentially compromising objective clinical judgment. Here the ethical principle at play is Beneficence vs Professional Integrity.
Competence and referral
This dilemma arises when a clinician works outside their scope of practice, performing procedures for which they lack adequate training, experience or skill, rather than referring the patient to a suitable colleague. This often arises from a desire to retain patients or maximise income. Here the ethical principle at play is Non-Maleficence (doing no harm) vs Beneficence (providing competent are).
Confidentiality
There are many ways that clinicians can breach the Australian Privacy Principles. Discussing patient cases in public requires details to be anonymised. Problems can occur when clinicians discuss their cases on social media or with family/friends. The temptation to share interesting or challenging cases can inadvertently breach privacy. Here the ethical principle at play is Confidentiality.
Handling impaired colleagues
This dilemma arises when we suspect a dental colleague is impaired (e.g., due to substance abuse) which could endanger patients. The dilemma is between professional loyalty to a colleague and the mandatory notification responsibilities that we have as part of our ethical duty to protect the public. Here the ethical principle at play is Non-Maleficence (our duty to protect patients) vs Collegiality.
Examples of dentistry’s public reputation being impaired due to unethical behaviour
• Prioritising volume over patient care, over-servicing, providing inappropriate or unnecessary treatments to numerous patients, particularly vulnerable populations such as children or elderly patients under public health schemes. Unnecessary and fraudulent procedures include performing root canal treatments on healthy teeth, deliberately leaving decay under restorations to justify repeat visits;
• Excessive billing for simple procedures, using “up-scheduling” to bill more complex items than the procedures actually undertaken;
• Patients being charged for services not rendered;
• Patients subjected to lengthy, aggressive treatments that were not clinically justified; and
• Unhygienic practices, including the reuse of unsterilised dental instruments and inadequate hand hygiene.
Fraudulent practice
Fraud typically involves dishonest conduct causing financial gain (for the perpetrator) or financial loss (for the victim). Accepting large sums for services not delivered or making false claims about treatment items provided constitutes fraud under criminal law. Fraud in dentistry typically involves billing for services not rendered, charging for unnecessary procedures, misrepresenting services or manipulating private health insurance claims or claims to DVA or CDBS.
When such cases are exposed and prosecuted (through disciplinary tribunals or criminal courts), they inflict significant public reputational damage on the dental profession and fuel public outrage. They also add to widely held negative stereotypes that dental practitioners are profit-driven rather than patient-focussed. When there is suspicion or resentment from the public towards the dental profession as a whole, this makes it harder for ethical practitioners to build rapport and gain patient compliance.
When unethical behaviour from a dental practitioner “makes the 6 o’clock news”, there is a predictable outpouring on various social media platforms. While comments on social media may reflect profound distrust and anger of patients who are affected towards the particular clinician involved, those comments inevitably cast a shadow by extension across the whole profession. The most immediate and significant impact is an erosion of public trust. Patients become suspicious of our recommendations for treatment, because they feel vulnerable to exploitation. They start questioning our billing practices and our motives. This undermines the trust and honesty which are the foundations of the patient-clinician relationship. An important long-term impact is that patients who have now become suspicious may delay or avoid necessary dental care, due to fear of their being defrauded, leading to a decline in their oral health.
Instances of unethical behaviour by dental practitioners often gain traction in mass media and social media. This lowers public trust and diminishes the reputation of the entire dental profession. Examples include:
Fraudulent billing drains public health budgets, which has attracted attention for schemes under Medicare such as the EPC (Enhanced Primary Care) and more recently the CDBS. The poor behaviour of a few tarnish the thinking within successive governments around how to target and control dental schemes funded by taxpayers. The long-term impact of this is that schemes become very restrictive and as a consequence, vulnerable individuals have less access to appropriate care.
It is also important to mention that when considering the attention placed on the poor behaviour of a handful of clinicians, honest clinicians can feel demoralised and frustrated by the negative perception cast upon the whole profession due to the unethical actions of a few. We should not feel that we must be having to constantly defend our integrity as healthcare providers.
Accessing superannuation for extensive treatments
In March-June 2025, attention was focussed on cases where dentists accepted substantial advance payments from patients for complex dental procedures (including implants and prosthodontic work). In some cases, the treatments were not finished or poorly executed. These types of cases show a web of interconnected moral, ethical and legal issues.
There are at least 3 moral issues. The first of these is betrayal of the trust patients place in their healthcare providers. Patients entrust us not only with their health but often with significant financial resources. We must never exploit that trust for our own personal gain. The second issue relates to exploitation of vulnerable patients. Patients who present in pain, with compromised oral health, are emotionally vulnerable. Taking large advance payments from such individuals and then not delivering the promised treatment, is exploitation. This then leads to the third moral issue,
which is deception and dishonesty. When payment for services is accepted and there is no genuine intention or capacity to complete them, or to an adequate standard, that is inherently dishonest and morally reprehensible.
Using the AHPRA Code of Conduct as a point of reference, these types of cases highlight at least 4 ethical issues, including professional misconduct, lack of professional integrity, violation of patient autonomy and informed consent and a breach of beneficence and non-maleficence. Relevant elements of these issues include, respectively, fraudulent financial practices and substandard care; deceptive billing practices, misuse of funds, and failure to complete treatment; patients not being fully informed that their significant advance payments were at risk, which undermines their autonomy to make informed decisions about their healthcare and finances; and a breach of the ethical duty to act in the best interests of their patients and to do no harm. In situations like these, patients are harmed financially, physically (due to incomplete or poor treatment) and also psychologically.
Patients who access their retirement savings for dental work can potentially lose very large sums of money. Patients are left with substantial debt, unable to afford to get the necessary remedial work completed elsewhere. This financial ruin combined with physical pain causes immense stress, anxiety and depression. Affected patients feel deeply betrayed and violated. They are hesitant to seek future dental care, even from ethical practitioners, perpetuating their oral health issues.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology.
Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
• Universal – available in tube version and SingleDose
• Variety of flavours – mint, caramel, cherry and bubble gum
tribute
Soaring like an eagleperforming like a Turkey
By Graham Middleton
“Dasher simply believed that it was hard to soar like an eagle when the dentists he employed behaved like turkeys...”
Freddy was ultra ambitious early in his dental training and his classmates labelled him “Fabulous Freddy”. He liked to keep up appearances, but graduated with the largest debt of his class. He didn’t lack in confidence and he expected to become the most successful dentist in his group, even if his dedication to the course was sometimes regarded as borderline.
Harry was dissimilar to Freddy. Harry always thought through the options; even when it came down to which pub to go to for the end of term drinks with fellow students! Harry would carefully weigh up the advantage of each alternative. His classmates labelled him “Handbrake Harry”.
Fabulous Freddy and Handbrake Harry were so different that their nicknames stuck and they became known respectively as “Fabulous” and “Handbrake”.
The consensus was that Fabulous was the most likely member of the class to succeed. Most of the class thought that Handbrake was a nice enough person but that he was likely to lag behind.
Originally published Nov/Dec 2006
Starting at the top
Fabulous reasoned that there was nothing like starting at the top of what he perceived the dental ladder to be and he actively sought out leading cosmetic dentists.
Somebody reasoned that Fabulous would push hard when it came to selling, which was true, but there were going to be problems because his clinical skills did not keep pace with his desire to generate fees. Still, Fabulous quickly moved to being paid on a commission basis and within a couple of years, his share of the takings amounted to $150,000.
He continued to spend at a fast rate too and his student debts remained. He drove the “right car” with high monthly payments, joined an expensive golf club and rented an apartment at the top end of town. His credit cards had significant carry-over balances. He rationalised that he was going to increase his income further, so he could live with debt.
Handbrake’s choices
Handbrake realised that he lacked charisma and that made him work harder at studies. He knew that he had to choose which practice to work in after graduation with great care, in order that his natural lack of selling skills would not prove disadvantageous.
Handbrake approached graduation to the workforce as another exercise in choices. He had paid far more attention to the clinical subjects than had Fabulous, but he lacked the charisma. Handbrake opted to work in a busy practice in a country town about four hours’ drive from the city. He chose a practice which was heavily booked and he found that he didn’t have to hard-sell treatment plans. The practice had rigid fee protocols which were enforced strictly by the proprietor’s wife, Annie, who worked in the practice alternating as bookkeeper, relief receptionist and chairside nurse. Annie was respected, but was universally referred to by practice staff as “The Iron Lady”. Even the proprietor, Don, good naturedly referred to Annie as “His Iron Lady”. The system worked well and there was a policy of cash on the day. Those who protested were politely told “sorry - no money, no drill”. The system suited Handbrake who was prepared to work 10 full sessions per week. As Don and Handbrake were both fully booked, the situation of passing unwanted jobs from proprietor to employee dentist did not really arise. Handbrake got to do a wide range of dentistry and he gained experience rapidly. He quickly learned that the patients from the town were used to taking the dentist’s advice with regards to treatment. The Iron Lady, who seemed to know lots about the townspeople, would indicate who could afford the more expensive treatment options and those who could only afford the basics. The system worked well. By the end of Handbrake’s second year with Don, he was comfortably generating above $500,000 of fees per annum in his own surgery. After laboratory costs were deducted, Handbrake’s percentage was about $200,000 including superannuation. Tax took a significant chunk, but Handbrake was a cautious spender. He also found that living in a rural community, he was around people who valued conservatism. Handbrake’s car was a modest purchase. Away from the practice he enjoyed the simple pleasures
of belonging to the local tennis and golf clubs. Membership costs were modest and the clubs encouraged his participation. During the football season, Handbrake went to a few of the local team’s home games. That too was noticed by the locals.
Dentist in a hurry
Meanwhile, Fabulous was still a man in a hurry. After a couple of years’ experience, he approached the highest profile cosmetic dentist in the state, “Dasher Derek”. Dasher had the unfortunate habit of burning his employed dentists. Over the years, many of the city’s better dentists had worked for Dasher for a short time, but had been repelled by over the top presentation and selling and untidy administration. Dasher simply believed that it was hard to soar like an eagle when the dentists he employed behaved like turkeys. In reality, many of the turkeys were first-rate dentists who quickly discovered that they were happier leaving Dasher’s practice. There were now a number of successful practices being run by Dasher’s ex-turkeys. Still, Dasher was unlikely to change his ways.
Dasher’s meeting with Fabulous
It was a bit like the great heavyweight champion Jack Dempsey’s description of the meeting between his shifty manager, Jack “Doc” Kearns and legendary fight promoter Tex Rickard. Dempsey described it as a meeting between two terrific con artists. Dasher wanted Fabulous to see his dream of an ever-moving assembly line of patients all paying unbelievable fees to fix their smiles in between visits to cosmetic surgeons for new noses and boob jobs. Dasher wanted Fabulous badly. Fabulous wanted Dasher to know that he was just the dentist waiting to strap on his eagle wings, if only he could find a practice that wasn’t going to limit his potential. They were both so busy talking that neither listened to the other.
Needless to say, Dasher offered Fabulous the job and Fabulous accepted. It seemed that they were made for each other like a meat pie and sauce.
Fabulous congratulated himself as being way ahead of his class. He regarded many of them, Handbrake included, as fitting Dasher’s description of turkeys.
Handbrake settles into country life
Meanwhile, Handbrake was quietly enjoying country life and had acquired a girlfriend, Trish, who was a nurse at the local hospital. As with most country towns, the locals were keen to keep as many health professionals living in the town long term as possible. They approved of Handbrake’s choice and were pleased that he spent much of his time locally.
Handbrake’s contentment was matched by the routine acceptance by patients booked to his surgery. He had heard that his fellow graduate class employed in city practices were frustrated because many patients stated a preference to be booked to their boss’s surgery. They were dissatisfied with having to treat all the emergencies while the boss monopolised the best patients.
Each time Handbrake evaluated the move back to the city, the balance came down more strongly in favour of remaining where he was. There had been a couple of fee adjustments in the practice and he was better at suggesting the work that needed to be done to the right people. He began to think of settling down permanently in town and started to evaluate his long term housing options. Don was quietly pleased. He didn’t wish to push it, but he was hoping that Handbrake would stay and buy half of the practice.
Good dentists were hard to come by in the country. Don and The Iron Lady were quietly influencing Handbrake toward utilisation of his personal potential. Handbrake listened, evaluated what they had to say and implemented their advice.
Dasher’s practice from the inside
Fabulous was now experiencing Dasher’s practice from the inside and realised that it wasn’t as flawless as indicated in Dasher’s literature, nor as portrayed by the expensive marble foyer. There were too many disputes about patient fees, with some patients dissatisfied that their treatment didn’t match their expectations created at the first meeting. Although Dasher presented himself to patients as being at the forefront of the dental profession, he was occupying a small niche.
Dasher’s qualifications weren’t as impressive as people thought, with some of the Post Graduate Diplomas and Degrees being awarded by American “factories”. Dasher’s practice had unbelievable overheads. He had several hygienists working inefficient hours and lots of good looking nurses in keeping with the practice image. However, there was a high turnover of dentists and some expensive work had to be re-done. Dasher was not a good manager. However, Fabulous tended to see what he wanted to see and he remained optimistic. Behind the scenes, Dasher’s lifestyle, coupled with an expensive divorce, had left him in a precarious financial position and he began to wonder whether he could sell part of his practice to Fabulous to relieve his own financial burden. Meanwhile, Fabulous was wondering how he could buy “a piece of the action”.
Both were seeing what they wanted to see. Dasher had become so enamoured with his own propaganda that he believed the practice to be worth $2 million, whereas a hard headed financial analysis would have put the figure at about $500,000 including clear title to the equipment and fit out, much of which was on lease. Dasher’s accountant put together a financial summary from which he had removed all Dasher’s “private expenditures”. The accountant also spoke authoritatively about the unlimited “blue sky” potential of the practice. Fabulous should have sought hard headed financial advice, but he was so besotted with the practice and his own plans that he shook hands on a purchase of a 50 percent Associateship for a concessionary $900,000. Fortunately his parents owned property which they were prepared to let the bank use as security. Fabulous already thought so well of his purchase that he traded in his car for a hot European model to celebrate. It was financed on hire purchase of course. In keeping with his self-image, he had acquired a “high maintenance” girlfriend. Fabulous imagined a future of consistent success. Unfortunately, his combined practice debts, credit cards and hire purchase arrangements totalled $1.25 million, which was a tad high for a graduate of approximately three years.
Handbrake buys an associateship
Meanwhile Handbrake had approached Don concerning an associateship. He was now generating above $14,000 of fees per week. Don was realistic in recognising that it was hard to attract other dentists to the town or to sell country practices. The practice was well above average in its profitability and efficiency and well equipped. They shook hands after a little bit of negotiation and after Handbrake had had his own assessment of the practice checked by an expert in dental valuation matters. They agreed on a payment of $200,000 which represented a 50 percent share of the practice equipment and as many patients as Handbrake could treat in his own surgery. Sensibly, he borrowed the money on an interest only basis. He and Trish put their own savings towards the purchase of a home.
Two financial outcomes
Fabulous owned a 50 percent associateship in a prominent practice, but after paying interest and leasing costs and sharing the rent in an exclusive location, as well as support staff wages, his profit was less than $200,000. His cash flow was far worse because the bank considered him a risky lend and insisted upon a significant level of debt amortisation. The debt repayment had to come from his after tax income. Fabulous found that he had to work harder just to pay basic lifestyle costs and his underlying figures were affecting his presentations to potential buyers of expensive treatment plans. As a result, his success rate of patient conversion was falling. Try as he might, he couldn’t make the employed dentists and hygienists, which he shared with Dasher, make a significant profit margin. There were too many part-time chairside nurses and there was too much staff turnover. Meanwhile Handbrake was making well over $300,000 profit and this was still increasing. As his borrowings were modest, his financiers were happy to keep his business loan on an interest only basis indefinitely. He and Trish were already reducing their home mortgage at a healthy rate and they were sacrificing the maximum amount permitted into superannuation. Fabulous thought that super was something that farmers fertilised their crops with.
Five years out
Five years after graduation, Fabulous was under tremendous pressure. He was receiving phone calls about unpaid bills. He had begun to try and tighten up in the practice, but his associate, Dasher, who had overcome the worst of his financial problems, was proving difficult to rein in. As fast as Fabulous reined in part of the practice, he found that Dasher had committed them to some other expenditure. It was hard to say no to Dasher because he was the sort of person who would have been quite confident selling blocks of land below the high tide mark on a Queensland island. His arguments in favour of keeping excessive staff and of replacing already optimum furnishings were just so convincing. The $900,000 that Dasher had received from Fabulous had satisfied his most pressing needs. Dasher was also discovering that he hadn’t lost much profitability, because he had only been making a tiny margin from employing Fabulous. Most of Dasher’s profit came out of his own surgery and he was a superb salesman. Somehow Fabulous and his partner had scratched together a deposit on a house, but it was in a far more modest surrounds than Fabulous had intended.
Advice
In desperation, Fabulous cast around for advice. He went from one to another, seeking correct answers, but most wanted to sell him timber plantations or get rich quick schemes. One of the consultants wanted him to sign a contract which varied from one year at $30,000+ to three years at $90,000. All seemed vague about what it was they were going to do for him. In any case Fabulous couldn’t afford to pay them and even Dasher had cast doubts about them, saying: “They’ll take your money but nearly everything they can tell you they could tell you in a day or two. However that won’t stop them spinning it out for as long a period as you’re contracted for”.
Finally Fabulous found somebody who could benchmark his practice and tell him the truth about its true value and his financial state. What he found out shocked him to the core:
1. The practice was grossly inefficient. 2. At most his associateship was worth $300,000.
3. Taking into account the huge debt he still had on the practice purchase, his and his partner’s net worth was negative by a large sum.
4. He was told that unless he took drastic surgery to his practice, the problem was going to grow worse and he would probably end up bankrupt.
Handbrake was in a far stronger position than he had anticipated five years earlier. He and Trish had paid off their home and with appropriate tax planning were splitting a nice income. They had already graduated from managed superannuation funds to their own fund. He had the interest only long term debt on the practice, but recognised that in reality, the practice was the best investment that he was ever likely to make. Don, his ex boss and now associate, had been quietly helpful. The Iron Lady had graciously suggested that she might step aside from her role in the practice, but Handbrake had the sense to realise that she was in every sense a worker and she glued the place together because she was willing to relieve on reception and step in whenever a chairside assistant was sick. At graduation, Handbrake had never dreamed of being able to produce over $700,000 of fees per year in his own surgery. He now found himself doing it comfortably and indeed nearly matching the pace of Don up the corridor. The town and surrounding district had an insatiable demand for dentistry!
Handbrake had his practice performance benchmarked regularly and he was alert to the advice he received. His business and financial advisers also measured his net capital wealth year by year and profiled him in terms of where his capital formation stood relative to other dentists of similar age who owned their own practice or practice associateship. Since Don and The Iron Lady had compatible views on key issues, the advice that Handbrake took back to the practice was in-sync. They maintained a stable working relationship and year-by-year the practice maintained its profitability and grew a little.
At this stage of their respective dental careers, neither Handbrake nor Fabulous had knowledge of anybody else’s financial situation except their own. It probably would have come as a pleasant surprise to Handbrake to realise that he was producing a better net income than Fabulous and importantly, his net capital worth
practice | MANAGEMENT
was already far in advance. It would have shocked Fabulous to his core to realise that he had fallen so far behind one of the “turkeys” in his class.
Future projections
It is possible that Fabulous will overcome the weaknesses in his practice, discipline himself, stabilise his debt and generate sufficient income to pay off his house at a healthy rate and fund superannuation. However it is unlikely. While persons with characteristics like Fabulous tend to survive, they spend years living by their wits.
The Handbrakes of the dental world have a tendency to be very consistent and to double their net wealth approximately every five to six years.
“Wealth gained early in a dentist’s career has a dramatic impact on their long term worth due to the impact of compounding returns...”
The lessons
1. Many years of examining the actual annual financials of a multitude of dentists and benchmarking them has taught me that the best performed practices are often located in smaller cities with no dental schools, regional centres and in country towns. There are also some excellent practices in the outer suburbs of major cities.
2. While there are high performing capital city CBD practices, these are outnumbered by poor practices in similar locations.
3. Dental practice proprietors earn the lion’s share of their profit inside their personal surgeries. The busier they become personally, the less time they have to supervise a large number of staff and indeed, they spend their days with their patients and their chairside assistants. Consequently, large practices are often unprofitable at the edges.
4. While there are some very profitable cosmetic practices, the dentists who achieve this standard of profitability have usually limited the size of their practice.
5. Wealth gained early in a dentist’s career has a dramatic impact on their long term worth due to the impact of compounding returns.
6. What we all lack is time. Choosing the right practice to work in, purchasing equity on realistic terms and earning a healthy profit above personal opportunity cost early in a dentist’s careers is critical. It will enable you to educate your children comfortably and have the means to elect to retire from dentistry or slow down at a realistic time of your choosing.
7. All of the practice management consultants in the world are a poor substitute for regular benchmarking and practice performance against actual dental accounting data, as well as regular benchmarking of net wealth against dentists of similar age. These are critical in measuring progress and indicate when a dentist is in danger of underperforming.
General Advice Warning
The information contained in this article is unsolicited general information only, without regard to the reader’s individual financial objectives, financial situation or needs. The information contained in this article is general in nature and you should consider whether the information is appropriate to your needs and where appropriate, seek professional advice from an accountant or financial adviser. It is not specific advice for any particular individual and is not intended to be relied upon by any person. Before making any decision about the information provided, you should consider the appropriateness of the information in this article, having regard to your objectives, financial situation and needs and consult your professional adviser. Any indicative information and assumptions used here are summarised, are not a product illustration or quote and also may change without notice to you, particularly if based on past performance. This notice must not be removed from this article.
About the Author
After contributing almost 200 articles for Australasian Dental Practice, Graham Middleton passed away on 30 December 2025 at the age of 80. He spent the later 33 years of his working life advising health professionals on business and financial matters with dentists being the most numerous of his clients. This article was originally published in the Nov/Dec 2006 edition and 20 years later, the advice still resonates today. May he rest in peace.
How to get out of your own way as a practice owner
By Julie Parker
I’ve been thinking quite a lot lately about the invisible forces that keep dental practice owners from stepping into their full potential – I’m not just meaning as business leaders, but as human beings wanting to make a meaningful difference.
I was listening to a podcast recently about the things that stop people from being true “bad asses” in life and I couldn’t help but see how much of it applies directly to dental practice owners. Running a practice isn’t just about teeth. It’s about people. It’s about leadership, influence and creating an environment where both patients and your team feel valued, safe and inspired.
Yet so many owners stay stuck or frustrated. Not because they lack skill or passion, but because of subtle obstacles that quietly sabotage their progress. So, let’s talk about these barriers through the lens of dental practice ownership and see how we might move beyond them.
Your brain wants comfort, not growth
The human brain is wired for one main job – to keep us safe, conserve energy and seek pleasure. Fantastic if you’re running from tigers, but not so helpful when you’re running a business.
Growth requires discomfort. It demands that you challenge how you’ve always done things.
For dental practice owners, that might mean having uncomfortable conversations with team members, putting new systems in place that feel foreign at first or learning skills like financial literacy or leadership communication.
But there’s another layer to this. Sometimes we feel discomfort not just because we fear failure, but because we fear success. It sounds odd, but stepping into bigger success often challenges how we see ourselves. It stretches our confidence and pushes us beyond the limits of what we’ve achieved in the past.
Discomfort doesn’t mean danger. It just means new. The more often you lean into what feels uncomfortable, the stronger and more capable you become.
Fragility will keep you small
Something I’ve noticed over the years is how much more fragile people seem to have become. As a society, we’ve grown less tolerant of discomfort, criticism and anything that challenges how we see ourselves. And while this might feel safer in the short term, it absolutely hampers your ability to be successful as a practice owner.
Running a dental practice means facing moments when things don’t go your way. Someone might say something hurtful or challenging. A patient might complain. A team member might push back on your ideas. You might face disapproval or obstacles you didn’t anticipate.
When you’re fragile, these moments become reasons to retreat. You pull back, avoid action or keep yourself small to avoid feeling uncomfortable. But if you want to run a thriving practice, you have to build resilience – or what that podcast I listened to recently called becoming “anti-fragile”.
Anti-fragility means you don’t just survive challenges – you grow stronger because of them. Each criticism, setback or uncomfortable moment becomes fuel for growth rather than a signal to give up.
Fragility kills progress. Resilience –and ultimately anti-fragility – builds it. And it’s a critical trait for anyone who wants to create a practice that not only runs smoothly but also delivers extraordinary care and patient experiences.
Drama
Let’s talk about drama – not the type you see on reality TV, but the drama we sometimes create in our own lives.
As practice owners, we can fall into the habit of interpreting ordinary events in ways that fuel emotional reactions and create unnecessary turmoil. A patient cancels and suddenly it means “people don’t value what we do”. A team member asks a question and we decide they’re “undermining us”. Instead of allowing situations to pass through our awareness neutrally –or to prompt growth – we add layers of meaning that drain our mental energy and distract us from what really matters.
Living through the lens of drama keeps you stuck. It keeps your mind busy with stories and emotional highs and lows instead of focused on constructive action. And when you choose drama, you also tend to attract other drama-driven people into your sphere – which only compounds the problem. This doesn’t mean ignoring challenges or pretending everything is fine when it isn’t. It means choosing not to add unnecessary “mustard” to situations. Deal with problems directly, without inflating them into stories that derail your focus and your goals.
If you want to grow as a leader – and as a person – commit to observing situations as they are, not as the dramatic stories your mind might spin. Because drama might feel engaging in the moment, but it’s a huge barrier to achieving real success and fulfilment.
Self-love isn’t self-coddling
Self-care is essential. But there’s a fine line between looking after yourself and avoiding the very challenges that help you grow.
I see practice owners decide they need “balance” and then use it as a reason to avoid difficult conversations, accountability or strategic changes. But the reality is that leading a practice well sometimes requires stepping into discomfort so you can ultimately experience greater freedom and fulfilment.
The minute you find yourself retreating into self-coddling, pause and ask: how can I empower myself instead? What solutions could I seek that would ease my mind and help me grow?
Taking a break is self-love. Avoiding growth is self-coddling. It’s important to know the difference!
Negative emotions are teachers, not enemies
Many owners shy away from feelings like fear, frustration or embarrassment. But those emotions are signals. They show you where your opportunities for growth lie.
Feel defensive in a team meeting? That might be telling you that you need to work on your communication skills or boundaries. Feel anxious about finances? Maybe it’s time to face the numbers head-on and learn how to manage them.
Negative feelings don’t mean you’re failing. They mean you’re stretching.
You’re both good and bad, right and wrong
One of the most liberating truths I’ve learned as a business owner and coach is this: you can be an incredible leader and still make mistakes. You can be kind and still have moments of frustration. You can be wise and still have blind spots. Stop waiting to be perfect before you lead boldly. Your team and patients don’t need perfection. They need authenticity, vision and consistency.
Everything you do – how you manage your team, how you structure your systems, how you handle money – should serve the goal of delivering the best possible care and experience for your patients.
Be curious about working with your team
There’s something I believe is vital for practice owners and it’s curiosity –specifically, curiosity about how to work better with your team.
I’ve seen the damaging impact of the mindset that says, “I pay this person, so they must do everything I say”. It’s a trap. Yes, you’re the leader. Yes, you pay the wages. But leadership isn’t about issuing orders and expecting blind compliance.
A practice runs at its best when you create an environment where your team wants to participate. Where they’re not just doing tasks because they’re paid, but because they care, feel valued and see how they’re contributing to something meaningful.
Ask yourself regularly, “How can I collaborate better with my team? How can I make them feel respected and heard, while still maintaining accountability and standards?”
When you approach leadership with genuine curiosity – wanting to understand your people, their strengths and what motivates them – you build a team that’s more engaged, loyal and committed to the same patient-first vision you’re striving for.
Curiosity in leadership isn’t a soft skill. It’s a powerful tool for unlocking your practice’s potential and creating a culture where everyone, including you, can thrive.
The power of self-reflection
One of the strongest elements in my own personal growth has been regular self-reflection. It’s easy as a practice owner to stay busy – running from patient care to staff issues to business decisions –without ever pausing to look inward.
Putting
patients first, always
At the heart of all this is a simple idea: patients must come first. Not as a slogan, but as a lived truth.
But if you’re serious about becoming the best version of yourself, you need to make time to reflect. Not just when things go wrong, but as a regular habit.
Ask yourself questions like:
• Where am I being reactive instead of proactive?
• What patterns do I keep repeating and are they serving me?
• What situations consistently trigger discomfort or fear in me?
• Where am I avoiding growth because it feels too hard or confronting?
Self-reflection isn’t about beating yourself up. It’s about getting curious. It’s about noticing your own thoughts, habits and emotional responses so you can make conscious choices rather than running on autopilot.
Some of my biggest shifts have come from simple moments of realisation when I’ve stopped to ask, “Why am I really resisting this?” or “Is this fear talking, or is there genuinely something here I need to address?”
Growth doesn’t just happen because you read the right books or attend the right seminars. It happens when you regularly turn inward, look honestly at yourself and then choose to do something differently.
So if you take one thing away from all of this, let it be this: the obstacles that hold you back as a dental practice owner are rarely just external. More often, they’re within – in your mindset, your patterns and the stories you tell yourself. But that’s also the good news, because it means you have the power to change them.
Be willing to lean into discomfort, to become anti-fragile, to step away from drama and to reflect deeply and honestly on how you’re showing up each day. Stay curious about yourself and your team and keep your vision anchored in putting patients first.
This journey isn’t about perfection. It’s about progress. And every step you take towards growth, no matter how small, creates ripples of positive impact for your practice, your team, your patients and –most importantly – for you.
About the author
Julie Parker is a Dental Practice Management Consultant and Team Educator. At the age of 33, Julie became the first non-dentist to own a dental practice in Australia. Julie is Co-Founder of Julie Parker Practice Success and CoFounder of Dental Business Mastery. Visit julieparkerpracticesuccess.com.au and dentalbusinessmastery.com.au to find how Julie can help your dental practice be more successful through consulting programs, online courses, podcasts and more.
Practice seller mythbusters - Part 2
By Simon Palmer
“Staff that are happy with the pay, team, job description and location won’t quit and risk not getting these things at another job, just because the boss changes...”
As experienced dental practice brokers in Australia, my team and I are always amazed at the misconceptions that some dentists have about the process of selling a practice. In this second article, we thought we would address more of the most common seller misconceptions that we hear:
Seller Myth #6: A buyer will not want me work in the practice post sale because they will want ALL of my patients
While there may not be enough patients to keep 2 dentists busy full time, most buyers would still like for you to stay and work post sale in at least a reduced capacity post sale (say 1- 2 days per week) for 6-12 months.
Working alongside the purchaser:
1. Allows you to finish cases.
2. Allows you to help with the history of patient or practice issues.
3. Provides an implied endorsement to the patient base and in this way helps with patient transfer and retention.
4. Keeps patients like the vendor’s immediate family and close friends in the practice, who would be less likely to transfer easily.
Seller Myth #7: I will sell after I renovate - the practice will be more attractive and worth more then
While the aesthetics can make a practice more or less attractive to a buyer, the primary driver of what a buyer will pay (and what a bank will lend a buyer) will be the proven maintainable financial return.
The general rule that I tell vendors is that any major reinvestment that they are considering has to be reflected in the practice’s financials in increased turnover or reduced expenses before you put the practice on the market, in order for it to make an impact on the price.
Seller Myth #8: I am worried that when my staff find out that I am selling, they will start looking for another job
The truth of it is that people don’t stay at their jobs purely out of love of their boss. Most of them stay because they like some combination of:
• Their pay.
• The job description.
• The location of the job and how convenient it is in terms of where they live or where their kids go to school.
• The team, including their boss.
“Any delay can break that momentum and allow circumstances inside the practice or outside the practice to interfere with that momentum. Lawyers who can work on your matter and respond quickly are much more likely to get you to the finish line...”
Staff that are otherwise happy with the pay, team, job description and location of their job won’t quit and risk not getting these things at another job, just because the boss changes. In the vast majority of cases, when a practice sells, the staff stay and give the new owner a chance to prove themselves.
Seller Myth #9: A lawyer is a lawyer…
When you are selecting a lawyer to represent you in your transaction, please look for one who is:
1. Available and quick to respond
There is a saying that “Time kills deals”.
When you have a deal on the table and both sides are excited to accept, you want that excitement to help carry the deal to the finish line.
Any delay can break that momentum and allow circumstances inside the practice (e.g., staff quitting or a downturn in figures) or outside the practice (another offer comes in, changes in economic circumstances, etc) to interfere with that momentum. Lawyers who can work on your matter and respond quickly are much more likely to get you to the finish line.
2. Professional and polite in their approach
Alawyer who is antagonistic and combative, or rude in their correspondence, can kill a deal.
3. Experienced in dental practice sales
Most dentists would cringe to hear of someone in their profession selling themselves to patients as able to do complex clinical work that is outside of their abilities - work that should be referred to someone else. This is how I feel when a seller tells me that their lawyer for their practice sale:
• Helped them with their divorce, immigration or buying their house.
• “Does a bit of everything”.
• Is a family member who will give them a good deal.
“Selling a practice is a complex transaction, with many moving parts, that is worth hundreds of thousands (if not millions) of dollars.
To give yourself the best chance of success, you need specialised help from a commercial lawyer...”
Selling a practice is a complex transaction, with many moving parts, that is worth hundreds of thousands (if not millions) of dollars. To give yourself the best chance of success, you need specialised help from a commercial lawyer.
About the author
Simon Palmer is the Managing Director of Practice Sale Search, Australia’s largest dental practice brokerage. If you’d like more information on practice sales, or want to have a confidential discussion about your practice’s circumstances, email Simon Palmer at info@practicesalesearch.com.au or call 1300 282 042.
Simon presents Exit Planning seminars throughout Australia, providing essential information for any practice owner thinking of selling in the next 5 years. Visit www.exitacademy.com.au for more information or seminar dates.
Put your customers first: Strategies to stay focused on their needs
By Jayne Bandy
Have you ever noticed people in customer service who appear rushed and distracted?
The irony is that the people who are there to give excellent customer service to their customers, are so busy that they forget they are there to serve people and enhance their customer experience.
If you want to deliver excellent customer service, you must always keep a check to ensure you are delivering customer service no matter what.
When you’re serving your customers and delivering an excellent customer experience, you cannot afford to be distracted.
I know from time to time you can easily get caught up in the busyness of your business, but the true delivery of customer service is when you can swim gracefully like a duck on top of the water whilst your legs are paddling fiercely below.
Your customers are left unaware that you are busy because you appear calm, in control and ready to serve them.
This takes practice over time to be able to switch off from being busy, set your priority and go into delivering customer service no matter what.
In your business, you want to avoid letting your patients know you are fully booked and appear stressed about where you are going to schedule them.
Work on staying calm and confident if you do not have an earlier appointment. You can easily schedule an appointment for two weeks’ time and then let your patient know you will do everything you can to move their appointment to an earlier time.
This may not actually be possible in the end, but you give your patient hope and its great customer service.
Also avoid letting your patients know you are busy and the reason why, especially if you are short staffed. This does not help your patient and very often they don’t even care. All the patient wants to know and hear is how you are going to find them an appointment time.
Call Tracking Excellence is not a product IT’S A RESULT!
With Call Tracking Excellence your team will learn the SAME exact processes Jayne used to:
1. Dramatically improve new patient call-in conversions to booked appointments.
2. Retain existing patient appointments
3. Prevent ongoing losses from appointment cancellations. Visit the website to find out how to get started. It’s that easy!
www.calltrackingexcellence.com
I was at a restaurant recently and the waitress was clanging around, running around and trying not to make eye contact with me in case I called her over. All this commotion made me feel unimportant and stressed rather than important and relaxed. My experience was negatively affected because my waitress appeared busy, rushed and was not there to serve me and give me the positive experience I expected.
So, look at your team, are they giving off the “I’m busy, so don’t talk to me or look at me” vibe?
This is not the impression you want to give your patients at any time.
Teams must always keep in mind that their priority is the patient and how they feel and to stay calm whilst paddling like crazy under the water!
To find out how I can teach your team to know what to say and ask your patients, to help them make more kept appointments and prevent cancellations, call me on 1300-378-044 or email jayne@thedpe.com
About the author
Jayne began her career as an educator. After spending several years teaching, she made the jump to practice management, serving as a Practice Manager for a renowned dentist in Sydney for more than 25 years, giving her firsthand experience at what works when it comes to building and maintaining patient relationships, how to convert leads over the phone and most importantly - what it takes to reach your practice goals. As the CEO and Founder of Dental Phone Excellence, Jayne helps practices convert more calls into appointments, reduce cancellations and nurture effective patient communication that will result in increased profitability. Her past experience as an educator combined with her passion for practice management gives her a unique set of skills that allows your team to fully understand and take advantage of the tools she presents.
The death of word of mouth in 2026 (For dentists who do nothing else)
By Angus Pryor, MBA (Marketing)
For decades, word of mouth has been the backbone of dental practice growth. Do good dentistry, look after people, treat patients well and they tell their friends. That simple formula worked for a long time and in fairness, it still works to a point.
But here’s the uncomfortable truth: What used to be enough no longer is.
This article isn’t about dismissing referrals. It’s about understanding why relying on them alone has become risky and why many good, well-run practices are feeling more pressure despite doing “ everything right”.
Here’s what every dentist who relies on word of mouth needs to understand...
1. Word of mouth isn’t dad, but patient behaviour has changed
Word of mouth still matters. Referrals still happen. But what’s changed, and this is the critical part, is how patients act on those referrals. In 2026, a recommendation no longer leads straight to a phone call/online booking. It leads to research. Patients take your name and start checking you out online before they ever consider booking.
As a case in point, my wife recently got a recommendation from a friend at work when looking for a particular practice. But instead of simply just calling the practice and booking an appointment, she did some checking online first.
Let’s face it, a referral is one person’s opinion about a business, but by checking online and reading reviews, etc, you can get many people’s opinions.
So, what happened? As a result of the checking online, my wife decided NOT to choose the practice that had been recommended to her - even though her best buddy at work had recommended it.
This isn’t about distrust. It’s about caution. Dentistry is a high-involvement decision and patients want to feel confident they’re making the right choice. Even when a referral comes from someone they trust, they still want reassurance and that reassurance now comes from what they see online.
This shift has quietly undermined the old “we grow by referrals” approach that many practices still rely on. Referrals
haven’t disappeared, but they no longer close the deal on their own. They open the door and what patients find next determines whether they walk through it.
What’s changed:
• Referrals now start the decision-making journey, rather than finish it;
• Patients actively research before committing, even after a recommendation;
• Trust is built digitally before the first phone call;
• Social proof carries as much weight as personal endorsement; and
• Recommendation plus verification is now the norm.
If your online presence doesn’t reinforce what people are saying about you, the referral loses momentum and often disappears without you ever knowing it existed.
2. Referrals no longer equal bookings
When someone hears about your practice from a friend, they don’t ring you. They Google you. They look at your reviews, scan your website, check your socials and compare you to two or three other practices nearby. This happens even when the referral is genuine and positive. In many cases, the referring patient has already done the emotional selling for you. But the final decision is made quietly, online. If what a prospective patient finds feels outdated, inconsistent, or unclear, the referral loses momentum.
And when that happens, it doesn’t fail loudly.
No feedback.
No complaint.
No awkward conversation. Just a booking somewhere else. This is why so many dentists feel confused. They are getting referrals; they’re just not seeing them turn into bookings anymore.
What referred patients now do:
• Google your practice name;
• Check Google Reviews, focusing on recency and volume;
• Scan your website for professionalism, clarity and ease of booking;
• Check social media to see if your practice is active and current; and
• Compare you with nearby alternatives offering similar services.
A referral today is no longer a decision. It’s an introduction. And introductions only work when what follows reinforces the recommendation.
3. Silence is the new red flag in 2026
There was a time when having little or no online presence was neutral. Today, it’s a warning sign. Patients may not consciously analyse it, but they feel it instinctively. In a world where nearly every business has a digital footprint, silence creates uncertainty.
An outdated website, inactive social media or a handful of old Google reviews sends an unintended message: this practice may not be current, relevant or in demand. In the absence of any objective ability to assess your clinical skills, potential patients will make a judgment about your practice solely based on your marketing efforts.
In a crowded market, patients don’t give you the benefit of the doubt. They give it to the practice that feels safer, clearer and more visible.
Silence often looks like:
• Social media accounts with old or inconsistent posts;
• A website that hasn’t been updated in years;
• Very few reviews, or reviews that are clearly outdated;
• No visible personality or patient communication; and
• No clear reason to choose you over competitors.
“The highest-performing practices haven’t abandoned word of mouth, they’ve reinforced it. They understand that referrals work best when supported by visibility, credibility and consistency. When a patient looks them up, everything they see confirms the recommendation. Reviews are current. Messaging is clear. The practice feels active, modern and trustworthy...”
Doing nothing is no longer invisible. It’s interpreted. And more often than not, it’s interpreted negatively.
4. Word of mouth is unpredictable and unscalable
Referrals feel comfortable because they’ve worked in the past. They feel earned. They feel organic. For many dentists, they’re a point of pride. But from a business perspective, they’re also unpredictable and impossible to scale.
You can’t turn referrals up when you want to grow. You can’t reliably forecast them. You can’t optimise them or measure their performance in any meaningful way. One month the practice feels busy and humming along; the next it feels flat, with no obvious reason why. There’s no lever to pull and no clear system to fix the problem.
That isn’t strategy. It’s reliance on conditions staying favourable.
As competition increases – which it does every year - and patient behaviour continues to evolve, practices built solely on referrals find themselves constantly reacting instead of leading. Growth becomes something that happens to them, rather than something they control. Decisions around staffing, expansion or investment are made cautiously, not because the opportunity isn’t there, but because the demand feels uncertain.
Referral-based growth may feel natural, but it’s also fragile. And fragility is not a solid foundation for a modern dental practice.
What the smart practices have already worked out
The highest-performing practices haven’t abandoned word of mouth, they’ve reinforced it. They understand that referrals work best when supported by visibility, credibility and consistency. When a patient looks them up, everything they see confirms the recommendation. Reviews are current. Messaging is clear. The practice feels active, modern and trustworthy.
The real shift in 2026 is moving from accidental growth to deliberate growth. From hoping referrals continue, to building systems that support them.
Because the real question isn’t whether word of mouth still works.
It’s this: Would your practice still grow if word of mouth slowed tomorrow?
If that question makes you uncomfortable, that’s not a problem. It’s a signal. And it’s one worth listening to.
About the author
Multi-award-winning Practice Growth Specialist, Angus Pryor, is an author, marketer and international speaker. He is the #1 Google-ranked dental marketer in Australia. In 2023, Angus’ team at Dental Marketing Solutions received the ADIA’s marketing award. More details are at www.DentalMarketingSolutions.com.au. For a smarter, cheaper solution to finding great team members doing particular tasks, there is a solution. To find out how to unlock the gold in your practice from incomplete treatment plans, reactivations and more, visit www.DentalStars.com.au.
The trouble with trusts
The ATO Is taking a good hard look at dentists — what you should be doing right now
By Garry Pammer, BEc, LLB, CA, DIP.FS (FP)
“If
most of your income exists because you apply your own professional expertise , the ATO sees that income as yours, regardless of which entity invoices the patient...”
The Australian Taxation Office (ATO) has sharpened its focus on the use of trusts, income splitting and personal services income and Dentists are firmly in their sights.
If you’re a dentist with a trust, now is the time to review how you’re using it.
Trusts as well as company structures have long been part of sensible financial planning. They were established to protect assets, manage cash flow, plan for succession and yes — legitimately minimise tax.
But the ATO has made it clear: the old comfort zones are gone.
Recent guidance and public commentary from the ATO signal that longstanding comfort zones are to be looked at. This means reapplying existing law and principles with respect to income splitting and profit diversion arrangements involving professionals - including dentists - where income is primarily generated by personal skill and effort rather than by a separate, stand-alone business.
Note: This is not a change in the law. It is a major change in interpretation and enforcement.
Sure, this might mean test cases and disputes but many dentists are more exposed than they realise.
Are dentists a prime target?
Dentistry sits squarely within what the tax law calls a personal services business.
In simple terms, if most of your income exists because you apply your own professional expertise - diagnosing and treatment - the ATO fundamentally sees that income as yours, regardless of which entity invoices the patient.
The ATO has explicitly stated that its updated guidance applies to doctors, dentists, lawyers, accountants and other professionals, not just aggressive or artificial tax arrangements.
In fact, many of the structures now under scrutiny are ones that dentists have used for years —without ever being questioned.
However, just because everyone is doing it does not make it unchallengeable and that is exactly why the ATO is paying attention to this area.
finance | INVESTMENT
What has changed? (And why that change matters)
Historically, many professionals took comfort in passing the Personal Services Income (PSI) tests - such as having multiple patients or operating through a practice entity.
The ATO is now saying that passing the PSI tests does not automatically protect you from anti-avoidance rules.
So even where a structure technically complies with PSI rules, the ATO is saying it will fall back and apply the provisions of Part IVA (Income Tax Assessment Act 1936). That legislation contains complex and heavy weight general anti-avoidance provisions. That is like using a sledgehammer to crack a walnut but what the ATO is saying is that they will use Part IVA if the outcome is a lower overall tax bill that lacks sufficient commercial justification.
In plain English, the ATO will now care less about the structure — and far more about the result.
Dental arrangements the ATO now considers high risk
Based on the ATO’s published examples and commentary, several arrangements commonly seen in dental practices will now be considered higher risk.
1. Family trustsIncome splitting
Many dentists distribute trust income to a spouse or adult children.
Much of the past argument in this situation was settled by ensuring children and spouses received capped distributions and that they actually received the benefit of the trust profit distribution - in cash, university fees, a house deposit, etc.
The ATO’s current stated position is shifting focus:
• There is no “safe” percentage of income splitting; and
• The greater the diversion away from the dentist who performed the work, the higher the risk.
So the reframed issue is, if your spouse receives substantial trust distributions but performs minimal or no work in the practice, the ATO may view this as inappropriate diversion of personal services income.
2. Paying yourself a less than market salary
Another common approach is operating through a company where there are several associates or employees. This has been seen as acceptable as a practice company.
The ATO considers this structure high risk where:
• The dentist performs the bulk of the clinical work; and
• Pays themselves a deliberately modest salary; and
“The
ATO is looking at long-standing legislation and deciding to interpret and apply it differently... The ATO message is that income from your personal effort must be taxed where it truly belongs. If you haven’t reviewed your structure recently or do not fully understand how it operates, then now is the time to do so. In doing so you will not only protect your overall tax position, but also the long-term stability of your practice...”
• Retained profits represent personal services income not properly taxed to the individual.
The message here, if you do the work, you must be properly paid for it.
3. Retaining profits without clear commercial reasons
The retention of profit is not inherently a problem. The need for working capital for expansion, equipment, debt management is genuinely understood.
The ATO accepts this but they are emphasising they want to see those genuine business reasons set out. Retaining profits year after year without
documentation or clear intent, while the dentist draws a lower-than-market income, will be raising red flags.
The ATO are again reverting to their underlying mantra - if income is mainly a reward for personal effort, it should be taxed in the hands of the person who earned it.
The good news: Revise your structure and how you use it
The ATO’s publicly stated intent is that they are not seeking to ambush compliant taxpayers overnight.
The ATO does not intend to backdate enforcement action where taxpayers make a genuine effort to move arrangements into lower-risk territory by 30 June 2027.
So dentists should act before the ATO knocks at your door.
What does a low-risk dental structure look like
The ATO has outlined the features of a low risk arrangement to include:
• The dentist receives market-rate remuneration for clinical services.
• Payments to spouses or family members reflect actual work performed, at commercial rates.
• Trust distributions do not significantly divert income away from the dentist.
• Retained profits have a documented business purpose.
• Superannuation contributions are genuine retirement planning, not income diversion.
So no surprises - if the dentist has a structure whereby they ultimately pay the highest marginal rate of tax on most of the income they generate, the ATO is happy.
What you should do now
Whilst not exhaustive, you should first begin by working through this action checklist:
1. Review who is really earning the income
Strip away the entities and candidly ask, who generates this income if I cease working.
If the answer is “no one”, the ATO will expect your tax outcomes to be you as the taxable income earner.
C2. Benchmark your pay
ompare your salary and/or profit drawings to:
• Other dentists in similar roles.
• What it would cost to replace you clinically with an Associate Dentist.
• Industry benchmarks.
Not having a comparable is now a compliance risk.
3. Scrutinise payments to family members
If family members receive income:
• Are they genuinely working?
• Is the pay commercially reasonable?
• Are all of their duties and income documented?
Best of intentions are not a defence against audits.
4. Document the reasons for profit retention
If profits are retained:
• Document why;
• Document how long; and
• Document what they’re used for.
The ATO will ask these questions surrounding the commerciality of the retentions.
5. Start early and get your advice early
Being proactive in restructuring and not leaving it until the last minute is always:
• Cheaper;
• Cleaner; and
• Less stressful.
Waiting for an audit letter before you act is not a strategy.
Final words
Most dentists have absolutely not set out to avoid tax. Structures have been set up many years ago and often change at different stages of their career. The commonly accepted advice being acted upon was given during a different ATO enforcement environment.
But that enforcement environment has changed. The ATO is looking at longstanding legislation and deciding to interpret and apply it differently.
The ATO is not saying trusts are illegal or that dentists are tax avoiders. The ATO message is that income from your personal effort must be taxed where it truly belongs.
If you haven’t reviewed your structure recently or do not fully understand how it operates, then now is the time to do so. In doing so you will not only protect your overall tax position, but also the long-term stability of your practice.
About the author
Garry Pammer is a Director of Specialist Accounting & Business Advisory, specialising in providing advice to dentists. Advice not only in respect of taxation and accounting but also superannuation, practice management and the buying and selling of dental practices. For a free assessment of your position and to see how you can achieve your goals, please do not hesitate to call Garry on 1300-221-486.
dentevents presents...
Infection Control BOOT CAMP
29 VIDEOS - 8+ HOURS OF EDUCATION
Presented by Emeritus Professor Laurence Walsh AO BDSc, PhD, DDSc, GCEd, FRACDS, FFOP (RCPA), FFDT (RCS Edin)
8
Learn from Australia’s leading authority on infection prevention and control in dentistry about recent changes in infection control including from the Dental Board of Australia (July 2022), the ADA (4th edition guidelines August 2021 and the ADA Risk management principles for dentistry during the COVID-19 pandemic (October 2021)), the new guidelines from NHMRC (May 2019), Hand Hygiene Australia (Sept 2019) and the CDNA (Dec 2018) as well as recent changes in Australian Standards and TGA regulations that are relevant to infection control. The course provides a summary of how those changes interlink with one another and also covers practical implementation of the new requirements and what it means for everyday dental practice. Hear about the why and the how and keep up-to-date with the changes that are happening.
COURSE TOPICS
This one day course will cover changes in regulations and guidelines from 2018 to 2022 including:
n Risk-based precautions.
n Hand hygiene and hand care practices.
n Addressing common errors in personal protective equipment.
n Biofilm reduction strategies.
n Efficiency-based measures to improve workflow in instrument reprocessing and patient changeover.
n Correct operation of mechanical cleaners and steam sterilisers.
n Wrapping and batch control identification.
n Requirements for record keeping for instrument reprocessing.
n Correct use of chemical and biological indicators.
Laurie Walsh is a specialist in special needs dentistry who is based at the University of Queensland in Brisbane, where he is an emeritus professor. Laurie has been teaching and researching in the areas of infection control and clinical microbiology for over 25 years and was chief examiner in microbiology for the RACDS for 21 years. His recent research work includes multiple elements of infection control, such as mapping splatter and aerosols, COVID vaccines and novel antiviral and antibacterial agents. Laurie has been a member of the ADA Infection Control Committee since 1998 and has served as its chair for a total of 8 years, across 2 terms. He has contributed to various protocols, guidelines and checklists for infection control used in Australia and represented dentistry on 4 committees of Standards Australia and on panels of the Communicable Diseases Network of Australia and of the Australian Commission on Safety and Quality in Health Care.
REGISTRATION
n On-Demand access to 29 Online Learning Videos (Over 8 hours of education).
n Watch and re-watch at your leisure 24/7
n Digital Online Learning Companion.
n Digital Suggested Reading Material.
n Online Questionnaire to earn 8 Hours of CPD.
IFU: The most important concept in reprocessing dental instruments and handpieces
By Emeritus Professor Laurence J. Walsh AO
For reuseable medical devices (RMDs), such as dental instruments and handpieces, instructions for use (IFU) are defined as “the detailed, action-oriented, step-bystep written and visual instructions provided by the manufacturer of equipment to guide the user in the use of and/or reprocessing of that item”. The importance of following the IFU is highlighted by the fact that the term IFU appears 72 times in AS 5369:2023 and a further 28 times in the Australian Dental Association 2024 Guidelines for Infection Prevention and Control (Table 1).
TThe journey starts here
he Instructions For Use are the key first “go to” place for information about reprocessing an RMD. Many queries that are posted online about reprocessing particular dental devices can be answered by referring the enquirer back to the manufacturer’s IFU. The IFU will explain which parts of the device can be reprocessed and how to do that reprocessing. Hence, it is essential that all dental clinics collate their collection of hardcopy and electronic IFUs, so that they are readily available for staff working in the reprocessing area (Table 2).
infection | CONTROL
In addition to written information provided in hard copy with the device, or available electronically from the manufacturer’s website, there are now available several commercial databases which bring together the IFUs from the websites of multiple RMD manufacturers. Clinics who subscribe to such databases need to be aware that the databases are typically only updated once each year, and that these databases collate information which is otherwise publicly available for no cost from manufacturers. Hence the cost of subscribing to such databases needs to reflect the convenience and timesaving of having a simple search interface, bearing in mind that the same information could have been found by searching for it directly from the manufacturer.
Key information about reprocessing is also indelibly marked on certain devices, using the widely recognised ISO 7000 symbols for a washer-disinfector or a steam steriliser, to indicate compatibility with these processes. Both symbols will be found as laser engraved markings on some recently manufactured dental handpieces. On the other hand, the symbol for steam sterilisation will be found uniformly on the barrels of modern piezoelectric ultrasonic scalers (Figure 1).
Useful information
Awell-prepared IFU will be useful when staff are considering purchasing a new type of RMD, since it will flag the complexities of reprocessing, including the need to use specific types of cleaning processes (Table 3).
As pointed out in both AS 5369 and in the 2024 ADA Guidelines, staff should review carefully the IFU for a new RMD (e.g. by downloading it from the manufacturers website) prior to making decisions regarding purchasing.
The IFU will allow the staff member planning for the purchase to consider how the new RMD will be classified according to its product family.
For the product family of “simple solid stainless steel dental instruments”, the lack of complexity means that these can readily be cleaned in an ultrasonic cleaner or in a washer-disinfector.
On the other hand, if the new RMD is a type of complex optical device (such as an intraoral 3D scanner), reprocessing will involve multiple steps, potentially including the use of barriers and the disposal of certain parts that are then replaced after a single patient use.
There are therefore impacts on staff time as well as on the use of consumables with the new device. As well, the IFU may also point out the number of potential reuse cycles for the device.
Furthermore, the IFU will also point out particular areas of risk, such as the incompatibility of the device with certain cleaning or disinfecting chemicals, or processes. Such information is essential to prevent the item being damaged by improper reprocessing.
Obligations of suppliers of RMDs
Companies that import RMDs into Australia are the legal sponsors of these, in terms of entry of those devices into the Australian Register of Therapeutic Goods (ARTG). As part of the documentation for the approval of RMDs, the sponsor will collate a folder of information based on the “Essential Principles”, which includes information about the reprocessing of these devices. Hence, the Australian supplier should always be able to provide the current IFU for a device and they are the natural first contact point for seeking additional or more detailed information about reprocessing, should the need ever arise.
Figure 1. An example of the ISO symbol for steam sterilisation at 134° Celsius marked onto the surface of the barrel of piezoelectric ultrasonic scalers. All scaler barrels that have this marking on them need to be sterilised between each patient use.
infection | CONTROL
Obligations of manufacturers
Manufacturers of RMDs around the world are required to conform to the two ISO 17664 standards. These relate to either critical and semi-critical RMDs (Part 1) or to non-critical RMDs (Part 2).
The focus of the discussion from this point onwards will be on ISO 176641:2021 Processing of health care products - Information to be provided by the medical device manufacturer for the processing of medical devices - Part 1: Critical and semi-critical medical devices. The current 2021 version of this standard represents a significant update from the previous 2017 version.
The first part of this standard explains the risk analysis which the manufacturer must perform around reprocessing, to inform the level of documentation that they need to provide with the RMD. This risk analysis must conform to ISO 14971 (the international standard for risk assessment) and flag any foreseeable user errors and misuse and thus any necessary warnings or limitations.
The ISO 17664 standard then goes on to specify the type of information that needs to be provided to the end user regarding each of the different stages of reprocessing (Table 4). Each step needs clear and specific information for the end user, including any checks that need to be undertaken at particular points. It is common practice that manufacturers will provide information around suitability for the item to be cleaned in a washer-disinfector that meets the requirements of the ISO 15883 series, or alternatively the IFU will describe another process if the item is not able to withstand being cleaned in a washer-disinfector. The IFU must also describe lubrication and reassembly steps if these are necessary, prior to sterilisation. Information must also be given for using at least one validated method of sterilisation, typically steam sterilisation, specifying the temperature and time requirements.
This detailed procedural information will be reviewed by the expert microbiologists and other assessors within the Therapeutic Goods Administration (TGA) as part of the medical device assessment process, prior to the device being listed on the ARTG.
Table 1. Specific topics where reference
to the IFU is stressed in the 2024 ADA Guidelines
n Use of barriers where specified.
n Choosing new instruments - determining whether the practice has appropriate equipment and expertise to effectively reprocess the new RMDs.
n Silicone rubber rings for identifying instruments or instrument sets.
n Reprocessing particular RMDs (preformed crowns, implant drills, impression copings, rotary nickel-titanium endodontic files, ultrasonic scaler tips, photographic mirrors, contrasters and retractors and dental burs).
n Using pre-cleaning to remove gross debris.
n Mechanical cleaning versus manual cleaning of RMDs.
n Operation of ultrasonic cleaners, including foil testing.
n Choice and use of ultrasonic cleaning solutions.
n Proper use of air removal and steam penetration tests such as PCDs.
n Loading the chamber in steam sterilisers.
n Positioning items in the chamber in S cycles in steam sterilisers.
n Checking the chamber of a steam steriliser by daily inspection.
Table 2. Reprocessing information
n ISO symbols marked indelibly on the device itself using symbols as per ISO 7000 (e.g. washer-disinfector compatibility, steam sterilisation compatibility).
n IFU provided in hard copy with the device (user manual, wallchart, etc).
n IFU made available electronically on the manufacturer’s website.
n IFU information collated by a third party into a database.
In the document file that is submitted to the TGA, the medical device manufacturer is required to include information showing how they have validated the processes that they have described in their documentation, to demonstrate that these are in fact fit for purpose. This is done by the manufacturer providing objective evidence that the reprocessing procedures described will produce an RMD that is clean and sterilised when the processes described have been followed. This may involve them providing data from external microbiology laboratories that they have commissioned to do such validation studies.
Sufficient detail
The level of detail given in the IFU needs to be sufficient that the risks of transmission of infectious agents are minimised when the device is reprocessed according to those instructions, while at
the same time minimising degradation or other adverse effects on the device itself. This is why the IFU will often include information about servicing, inspection and any functional testing that might be necessary. A well-written IFU will highlight particular challenges with the device such as how to handle crevices, joints, serrations and lumens, so that all contaminants are removed.
The manufacturer is required to provide detailed information for at least one option for cleaning and at least one option for sterilisation. In many cases, they will provide information for more than one option, however one needs to anticipate that the instructions for use may not cover all possible available technologies that could be used. Indeed, the standards themselves acknowledge that technology is used for cleaning and sterilising have continued to evolve over time to address the challenges of devices that are difficult to clean and sterilise.
The Solution For Your Retention Issues
• Computer Designed
• Perfect Fit
• Patented Material
• Laser Cut
• Smooth edges
• 3D Printed Model
• Perfect Fit
• Upper &/or Lower
• All scans accepted
infection | CONTROL
Table 3. Important general info found in IFU
Proper use
n Intended use, including necessary warnings regarding contraindications.
n Foreseeable user errors and misuse.
n Need for user training.
Device characteristics
n Plastic or metal.
n Solid or hollow/cannulated.
n Moving parts.
n Need for disassembly and reassembly.
n Necessary maintenance or lubrication of the device.
n Life cycle of the device, including any limitations on number of reuse cycles.
Reprocessing details
n Disposable components and other consumables required.
n Equipment required for reprocessing.
n Tolerance of the device (to moisture, steam and heat) and limitations and restrictions on reprocessing methods.
n Material incompatibility with certain chemicals.
Table 4. Key components of reprocessing instructions required in ISO 17664 standards
n Initial treatment at the point of use (including pre-cleaning)
n Disassembly or other preparation before cleaning
n Cleaning methods (including the use of ultrasonic cleaning and/or washer-disinfectors)
n Inspection and maintenance
n Packaging
n Sterilisation
n Storage
n Transportation
Single use medical devices
Afinal important point is that a reuseable medical device is intended by the medical device manufacturer to be suitable for reprocessing and reuse. This is completely different from single use medical devices, which are intended by the medical device manufacturer for onetime use only, after which they are discarded, with no intention of reuse.
If a clinic attempts to reprocess a single use RMD, they then become the legal manufacturer of that item. This occurs because of the definition of a medical device manufacturer, as the “natural or legal person with responsibility for design and/or
manufacture of a medical device with the intention of making the medical device available for use, under their name, whether or not such a medical device is designed and/or manufactured by that person or on their behalf by another person(s)” (ISO 17664). Hence, the clinic now has taken on all of the responsibilities described in ISO 17664-1 to develop, validate and document a reprocessing pathway, to the same level as required for a mainstream medical instrument manufacturer.Moreover, they then become subject to a raft of quality control requirements under ISO and Australian standards for medical device manufacturers, including site inspection by the TGA.
Conclusions
Staff involved in reprocessing need to use the IFU for a device as their first “go to” place for information. The onus of responsibility lies with the device manufacturer to provide detailed information to the end user on the required steps for reprocessing. The protocols described in the IFU must have been verified by the manufacturer and subsequently approved by the TGA as the regulator. Having this base of evidence means that end users who are reprocessing devices for the clinic can have confidence in those protocols.
If an end user decides to explore using alternative techniques for reprocessing an RMD, then the responsibility for validating those alternative processes falls on their shoulders. This comes back to the requirement of the end user to validate any alternative processes that they use which are different from what is described in the IFU.
There is an inherent risk that alternative methods could cause degradation (such as corrosion), inadequate cleaning, compromised sterilisation or failure of the device during use. Failure to properly reprocess an RMD risks the transmission of infectious agents between patients. Following the IFU closely is always the simplest and most straightforward approach.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right.
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. comes to the perfect fit, Hu-Friedy is just right.
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust
Peace of mind: Infection control built into A-dec equipment
By David Petrikas
Infection control should be at the heart of every dental practice. It’s not a single process or piece of equipment, but a mindset that should govern the approach to controlling potential spread of infection throughout the practice.
That mindset is made much easier by equipment with built-in safeguards to protect both patients and staff from possible infection from contamination of equipment, instruments and airborne aerosols.
At A-dec, infection control is built into every dental unit, giving you added peace of mind.
From A-dec’s proprietary Alphasan antimicrobial tubing, together with the design of the A-dec control block which prevents
water stagnating and the A-dec self-contained dental unit waterline system which is easily and simply treated with A-dec ICX® tablets to prevent contamination.
Infection control is strongly guided by the ADA’s infection control guidelines, which cover everything from simple things like barriers and wiping down surfaces in the dental surgery, to reprocessing of dental instruments.
A-dec equipment has easy-to-clean, smooth upholstery and dental unit surfaces to make applying barriers and wiping down between patients easier. This is especially the case with the Continental design delivery system where instruments can be easily picked up to wipe down the gently contoured control head underneath.
A-dec Pro Turbines and handpieces
The new turbine “Vaporiser” feature –exclusive to the A-dec Pro delivery systems – purges the turbine with a blast of high-speed air, preventing water being drawn back into the turbine head, helping eliminate potential contamination.
It also avoids the last drop from dripping onto the patient when the handpiece is removed from the oral cavity, adding to patient comfort and safety.
A-dec’s XC-10 electric motor, suitable for contra angle and speed-increasing and speed-decreasing handpieces is also favoured by many for its quiet, powerful operation and for greatly reducing the production of aerosols compared to high-speed turbines.
New Flush Dock
The new A-dec Pro delivery systems also feature a unique “auto flush” function. Activating this operation purges all tubing to ensure there is only fresh water in the dental unit water lines.
And at the end of the day, all dental waterlines can be easily flushed using this feature and the innovative new A-dec flush dock – a hands-free solution that doesn’t require a sink, bucket, HVE or cuspidor. With specified slots to hold handpieces and A-dec syringes, you can flush, purge and consistently follow recommended waterline protocols, leaving your hands free while you get on with other important tasks.
The Flush Dock is portable, stand-alone and easy to move between rooms. At the end of the day, simply “rinse and repeat” with each chair while you get on with other things.
When an A-dec syringe is inserted into the holder, it depresses the water button, automatically triggering the syringe flush.
Hands-free instrument flushing
Handpiece lines may be started by manually holding the flush toggle – or via the timed flush feature on the latest A-dec DS7 and CP5i control pads, which allow customised, pre-set flush timers to start the process for you. With the Flush Dock in place, it’s ready to go when you need it.
The Flush Dock helps reinforce waterline maintenance protocols and can also be used for dental unit waterline purging after using A-dec ICX Renew® waterline shock treatments.
Monitor through water testing
It is good practice to test microbial levels in water from the dental unit waterline regularly (at least six-monthly or annually) as recommended by the ADA. Monitoring requirements will depend on your water quality and the clinic’s individual requirements. Initially, test water once a month, if results consistently remain below 200 CFU/mL for three consecutive months, reduce the testing frequency to once every 6 months.
A rapid waterline testing service is available from A-dec service dealers using a specialist digital test device and can be easily incorporated into your routine equipment servicing – much like periodic steriliser validation. If your test triggers an action level, treat your dental units with ICX Renew liquid shock treatment. After the prescribed time, the shock treatment is flushed out of the dental unit waterlines which are then ready to be refilled with clean water and maintained with ICX tablets.
Safe, effective and equipment-friendly
From beginning to end, the thoughtful design of A-dec delivery systems ensures the highest level of infection control for you, your team and importantly, your patients.
Contact your A-dec dealer at australia.a-dec.com or by phoning 1800-225-010 for more information on infection control products and ask about the revolutionary new A-dec Flush Dock to make waterline maintenance even easier.
Patients trust that the water you’re using is clean.
A-dec ICX® makes sure it is.
Bacteria colonise in dental unit waterlines at a rate of 200,000 colony forming units per mL within five days if left untreated. Along with a daily maintenance protocol, it’s important to monitor water quality and periodically shock the lines to clear contamination.
Bacteria colonise in dental unit waterlines at a rate of 200,000 colony forming units per mL within five days if left untreated. Along with a daily maintenance protocol, it’s important to monitor water quality and periodically shock the lines to clear contamination. A-dec ICX® waterline treatment tablets and ICX Renew® waterline shock treatment work together to deliver the highest quality water to your patients.
If CFU/mL test results are < water quality standards = continue daily maintenance with ICX.
If
If CFU/mL test results are > water quality standards = shock your dental waterlines with ICX Renew.
ULTRA SAFETY PLUS TWIST
> Protects you and your staff from needle stick injuries
> Complies with latest regulations
> Intuitive device
> Available with either sterile single use or sterilisable handle
Passive or active aspiration: security for the patient
Transparent barrel: aspiration is clearly visible
Sliding protective sheath: protection from needle stick injuries
Two different positions:
first Holding Position (reversible)
final Locking Position (irreversible)
A LONG-PROVEN EFFICACY
OF
EVERYTHING the right one with Hu-Friedy
for you. when it comes to the perfect fit, Hu-Friedy is just right.
A study demonstrated that when introduced in a dental school, Ultra Safety Plus was a the key success factor for avoiding needle stick injuries. With Ultra Safety Plus, needle stick injuries decreased from an average of 11.8 to 0 injuries per 1,000,000 hours worked(1)
STEEL PEDO CROWNS:
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust
case study
TRI matriX® Implant: A 5-year triumph in abutment-free immediate restoration
Clinical
case by Prof. Dr. med. dent. Ronald E. Jung, PhD (Switzerland)
In the fast-evolving field of implant dentistry, few innovations deliver both clinical efficiency and proven longevity as convincingly as the TRI matriX® system. A landmark clinical case by Prof. Dr. med. dent. Ronald E. Jung, PhD, demonstrates a single-crown immediate restoration achieving outstanding 5-year success without a traditional abutment. This well-documented report showcases how the Multi-Level matriX (TRI Dental Implants, Switzerland) implant simplifies workflows, accelerates healing and delivers exceptional aesthetic and functional outcomes.
The journey began at 3:00 pm with precise surgical insertion of the Multi-Level matriX implant in the maxillary right central incisor region. Just 30 minutes later, at 3:30 pm, an intraoral scan captured the site with remarkable accuracy using 3Shape® technology. A digital provisional was designed chairside and milled from PMMA as the abutment-free resin crown, allowing delivery of a perfectly fitting restoration by 4:30 pm—only 90 minutes after implant placement. This immediate abutment-free resin provisional guided soft-tissue architecture while restoring aesthetics and function from day one.
Figure 1. 3:00pm - Insertion of a Multi-Level matrix® Implant. Figure 2. 3:30pm - IO Scanning.
7. 3 months later: Copy design and exchange of temporary to final zirconia restoration without the need for a new impression.
With the matriX, TRI engineers went for a clean-sheet redesign on how to restore implants, leveraging the power of digital technology and modern techniques that didn’t exist even five years ago. This has led to a simplification of the restorative process and elimination of parts like abutments, which were always a workaround to the problem of legacy implant platforms. The result is dramatically fewer components, zero micro-movement at interfaces and a preserved biological seal. This philosophy is clearly demonstrated by the very limited prosthetic catalogue—streamlining inventory management and greatly reducing overall costs per implant for both clinics and laboratories.
Three months post-surgery, the abutment-free resin provisional served as a flawless blueprint. Its copy design was transferred directly to a final AFC – Abutment-Free Ceramic monolithic zirconia crown without new impressions or additional scans, cutting treatment visits and laboratory steps while maintaining identical emergence profiles.
Long term prognosis
Long-term follow-ups confirm the system’s durability. At 3 months, soft tissues showed healthy maturation and natural contours. One-year clinical and radiographic images revealed stable bone levels with no crestal loss.
By the 5-year mark, the AFC – Abutment-Free Ceramic restoration remained indistinguishable from adjacent natural teeth—pink and white aesthetics flawless, peri-implant bone architecture intact on radiographs and zero incidence of screw loosening, chipping or biological complications.
Patients benefit immediately: No edentulous phase, rapid return to confidence and function and significantly lower risk of peri-implantitis thanks to the cement-free, abutment-free design.
Clinicians gain a fully digital, predictable workflow compatible with 3Shape and Ivoclar® systems, reduced chair time and simplified inventory.
Figure 3. CAD Design.
Figure 5. PMMA Provisional.
Figure
Figure 4. Chairside Milling of PMMA Provisional.
Figure 6. 4:30pm - 90 minutes after surgery, perfect fit of provisional.
Figure 8. Happy team.
clinical | EXCELLENCE
11a-b.
Prof. Jung, Vice Chairman at the University of Zurich’s Clinic of Reconstructive Dentistry, ITI President and a globally recognized leader in implantology, brings unmatched credibility to these findings. His meticulous documentation, including the celebratory “happy team” photo, reflects the confidence this system inspires across the entire treatment team.
The TRI matriX implant represents a genuine paradigm shift: faster, simpler, stronger, more aesthetic—and now backed by five years of uncompromised clinical success.For modern implant practices seeking reliable immediate solutions without compromise, this case provides compelling evidence that the future of single-tooth replacement is already here.
About the clinician
Prof. Dr. med. dent. Ronald E. Jung, is Vice Chairman of the Department of Fixed & Removable Prosthodontics and Dental Material Sciences, University of Zurich, Switzerland; and Associate professor at the University of Zurich. He holds a PhD from the University of Amsterdam, ACTA dental school, Netherlands.
He has been a Visiting Associate Professor in the Department of Periodontics at the University of Texas in San Antonio, USA (2006) and at Harvard School of Dental Medicine, USA (2013). Dr Jung is currently President of the International Team for Implantology (ITI).
Figures 9a-c. Final restoration 3-month follow-up.
Figures 10a-c. 1-year follow-up.
Figures
5-year follow-up.
designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.
dental implant connection that has been new digital manufacturing technolomilling or 3D printing. The implant concept directly on the implant without the use manual cementation.
Swiss Thinking. Shared Success. NO ABUTMENT. NO CEMENT. NO LIMITS.
The world’s first implant approved for full digital restorations without abutment
The world’s first implant approved for full digital restorations without abutment
Discover more
Discover more
The matrix® is the first-ever dental implant connection that specifically designed for the new digital manufacturing gies such as CAD/CAM milling or 3D printing. The implant allows to plan the restoration directly on the implant without of the abutment and without manual cementation. full digital restorations without abutment
Swiss Thinking. Shared Success. NO ABUTMENT. NO CEMENT. NO LIMITS.
Exclusively distributed by Shared Success.
Exclusively distributed by Shared Success.
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment
The world’s first
Discover more gies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use the abutment and without manual cementation. NO ABUTMENT. NO CEMENT. NO LIMITS.
The matrix® is the first-ever dental implant connection that specifically designed for the new digital manufacturing gies such as CAD/CAM milling or 3D printing. The implant allows to plan the restoration directly on the implant without of the abutment and without manual cementation.
The world’s first implant approved for NO ABUTMENT. NO CEMENT. NO LIMITS.
dental implant connection that has been new digital manufacturing technolomilling or 3D printing. The implant concept abutment dental implant connection that has been new digital manufacturing technolomilling or 3D printing. The implant concept directly on the implant without the use manual cementation.
dental implant connection that has been new digital manufacturing technolomilling or 3D printing. The implant concept abutment
The world’s first gies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use the abutment and without manual cementation. NO ABUTMENT. NO CEMENT. NO LIMITS.
The world’s first www.tri.swiss 0297
The world’s first www.tri.swiss 0297
The world’s first implant approved for NO ABUTMENT. NO CEMENT. NO LIMITS.
Failures with local anaesthetic
Part 2 in a series on local anaesthetic
By Dr Greg Mahoney, BDSc, PhD, MSc (Dent), GradDipClinDent, FADI, FPFA
In the first of this series on local anaesthetic, we looked at what the properties of a local anaesthetic that make them fit for purpose. In this article, the author is seeking to assist the oral health practitioner in providing safe and effective local anaesthesia. All dentists have good and bad days in administering local anaesthetic and failures do occur. It is prudent, therefore, that the dentist ensures that they are using the appropriate armamentaria, protocols and dosage.
AThe needle
ll needles are not identical. An appropriate needle has a keen edge beveled to penetrate the mucosa with the minimum amount of tissue displacement. A needle 25 mm long and of 25-30 gauge is the needle of choice for infiltrations and a longer needle is required for mandibular blocks, because the depth of penetration ranges from 20-25 mm for an average adult. It is important to avoid insertion to the hub as the join is the weakest part of the needle. If the needle does break and if there is not at least 5 mm of it exposed, it could be irretrievable as patient/soft tissue movement can cover the exposed end.1
Armamentaria
Tips on needles
• Needles do get blunt, so avoid multiple injections with the same needle; n Don’t keep reloading cartridges;
• Use quality needles with large lumens;
• Remember they can get blocked or bent;
• Don’t bend your needles; and
• A larger lumen requires less force.
The syringe
It is essential for practitioners to use aspirating syringes for both blocks and infiltration as it is the inadvertent intravascular injection of local anaesthetics (LAs) that could lead to dire consequences. The false negative aspiration is less likely to occur with an auto-aspirating syringe as the back pressure is significantly less than manual aspiration. Computer controlled analgesia (CCA) syringes have an aspirating function built into the solution delivery and using CCA can result in less pain and more effective anaesthesia.2
General principles of injections
Give all injections SLOWLY! Your patients will notice the decrease in pain associated with the injection and slow injections are more likely to keep the local anaesthetic solution in the target area, improving the efficacy of your local anaesthetic. Post-operatively, because there is less trauma, there is a decreased likelihood of haematoma and site soreness.3
Always aspirate even when performing infiltrations. The oral environment is a vascular rich region and there have been a number of reported cases where infiltration for the maxillary molars has led to an unintended intravascular injection into the maxillary artery leading to convulsions, hypotension and hospitalisation.
Inject against bone, place the needle into the tissue until you hit bone, withdraw slightly, aspirate and then slowly inject.4 There is no point in emptying a whole cartridge into a patient when half a cartridge will be sufficient. The dosage given should take into account age, health and medication.
*Adjunct therapies may include pharmaceutical techniques such as sedation and nonpharmacological techniques such as behavioural modification.
# These included higher level blocks such as Gow-Gates and Akinosi - Vazirani techniques as well ipsilateral injections.
Figure 1. A protocol for maxillary infiltration failure.
Figure 2. Protocol for failed ian block.
Failures with maxillary injections
Failures with buccal infiltrations, whether on the mandible or maxilla, are not common but there could be:
• Collateral nerve supply to the pulp, usually from the palate;
• Cortical bone that is particularly thick as is the case with tori or the juxtaposition of the zygomatic buttress;
• Infection; or
• Individual anatomical variations. Maxillary blocks are particularly useful where there is localised infection or if the practitioner is working on multiple teeth.
“For most, it is the Inferior Alveolar Nerve Block (IANB) that is problematic. Variations in patient’s angle of the ramus, position of the mandibular foramen and lack of definitive landmarks, all contribute to failed analgesia...”
In case of maxillary infiltration failure, repeating your mistake won’t necessarily change the outcome and giving more to compensate would be counterproductive, although this is predicated on the fact that enough local was administered in the first place. For maxillary injection failures, it is most likely associated with the posterior molars.
Failures with mandibular injections
For most, it is the Inferior Alveolar Nerve Block (IANB) that is problematic. Variations in patient’s angle of the ramus, position of the mandibular foramen and lack of definitive landmarks, all contribute to failed analgesia.
Table 1. Maxillary and mandibular nerve blocks and dosage
Teeth/ region
Mandibular molars IANB
Mandibular premolars Mental
and incisors (unilateral)
Maxillary 2nd and 3rd Molars Posterior Superior Alveolar (PSA) Block 1ml
Maxillary Molars if PSA + mesial root infiltration 1.5ml in total includes 1st Molar
Maxillary premolars Middle Superior Alveolar (MSA) Block 1ml
Maxillary anterior teeth Anterior Superior Alveolar (ASA) Block 1ml
Palatal Greater Palatine Nerve Block (GPNB) 0.3ml or Naso-Palatine Block
References
1. Malamed S. Handbook of Local Aesthesia. 7th ed. St Louis: ELSERVIER; 2020.
2. Kwak E, Pang N, Cho J, Jung B, Kim KP. Computer-controlled local anesthetic delivery for painless anesthesia: a literature review. Journal of Dental Anesthesia and Pain Medicine. 2016;16(2):81–8.
3. Macleavy C. Gaining confidence in local anaesthesia. BDJ Team. 2018 Apr 3;5(4):18051.
4. Meechan J. Practical Dental Local Anaesthetic. London: Quintessence Publishing; 2010.
IS EVERYTHING the right one with Hu-Friedy
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. when it comes to the perfect fit, Hu-Friedy is just right. DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
EVERYTHING
right one with Hu-Friedy
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right. DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust
Table 2.
Local anaesthetics, dosage and techniques
Teeth
Lower premolars to lower premolars
Lower 1st molars (routine)
Lower molars with irreversible pulpitis
Lower 2nd and 3rd molars
Maxillary teeth
Maxillary teeth with irreversible pulpitis
Local Anaesthetic Dose Technique
Mandibular
Articaine 4% with Adrenaline 1ml Infiltration or
Lignocaine 2% with Adrenaline 1-1.5ml IANB
Articaine 4% with Adrenaline / Mepivacaine 3% / 1-1.5ml IANB
Lignocaine 2% with Adrenaline + Articaine 4% with epinephrine 1.8-2ml Infiltrations (Buccal and Lingual)
Articaine 4% with Adrenaline or 1-1.5ml IANB
Lignocaine 2% with Adrenaline
Maxilla
Articaine 4% with Adrenaline or 1ml Buccal Infiltration
Lignocaine 2% with Adrenaline
Articaine 4% with Adrenaline or 1ml Buccal Infiltration
Lignocaine 2% with Adrenaline 0.3ml Palatal Infiltration
Special Cases
Where adrenaline is contraindicated Mepivacaine 3% / Prilocaine 3% with felypressin 1-1.5ml Blocks and/or Infiltrations
Geriatrics All Teeth
Paediatrics (4-12 year old)
What nerve blocks should I use and how much should I give?
Nerve blocks are particularly useful blocks when a patient is undergoing multiple restorations or procedures. Table 1 lists nerve blocks and dose for restorations and surgery. If the patient were undergoing periodontal treatment, the infiltration doses could be halved as it often involves entire quadrants but requiring lower profoundness of analgesia.
In routine dentistry, dentists by and large give infiltrations and IAN blocks using Articaine 4% with adrenaline or Lignocaine 2% with adrenaline. Table 2 lists the local anaesthetics, dosage and techniques most likely to achieve success for the maxillary and mandibular teeth. Children, like the elderly, have less physiological reserves, poorer, less welldeveloped hepatic and renal function i.e. half-lives of LAs are longer. So, caution should always be exercised as their weight and physiology means that the toxic dose is considerably less.
Articaine 4% with Adrenaline or 0.5-1ml Blocks and Infiltration
Lignocaine 2% with Adrenaline
Articaine 4% with Adrenaline or 0.5-1ml Infiltration
Lignocaine 2% with Adrenaline
In light of this:
• Blocks should be avoided in children, if possible. The buccal bone on mandibular 1st molars is often porous enough to allow the local anaesthetic (Articaine in particular) to work;
• Extra care should be taken to avoid large doses of local anaesthetic while performing extensive work, especially during general anaesthetics. Children receiving treatment under local anaesthetic, by itself, are unlikely to have large doses given the limited clinical time that the child will tolerate; and
• Adjunct therapies are very useful e.g., distraction therapy and/or nitrous oxide/ oxygen inhalation sedation.
Tips for injecting LA
Take into account the procedure’s...
• Site;
• Duration; and
• Depth of analgesia required. Take into account the patient’s physiological and psychological health, then choose the right molecule, equipment and technique. Consider whether adjunct therapies are necessary.
• Always inject against bone;
• Always aspirate more than once;
• Give the minimum amount necessary;
• Inject slowly and withdraw slowly; and
• Avoid intravascular injections and use infiltrations where possible.
About the author
Dr Greg Mahoney was a member of the Dental Board of Australia’s Committee on Sedation (2010-2020) and, panelled member of the Australian Health Practitioner Regulatory Agency (2010-2020). Greg was the president of the Australian Society of Dental Anaesthesiology (2009-2021) and the Australasian Military Medicine Association (2009-2019). Dr Mahoney presents courses and workshops for the Australian Dental Association and the dental industry lecturing in Australia, South East Asia and Europe on Local Anaesthetic including Local Anaesthetic Systemic Toxicity (LAST).
think painless LA. think Greens.
Dentapen is a universal local anaesthetic delivery system for all techniques including intraligamentary injections. Designed for any 2.2ml dental anaesthetic carpule, it features active aspiration; two-way activation and grip (syringe or pen like); three delivery speeds (Slow 90 s/mL, Medium 60 s/mL and Fast 30 s/mL; and Ramp-up mode = anesthesia flow increases gradually for a totally painless procedure. Dentapen is battery-powered, compact and lightweight at only 50 grams.
William Green Pty Ltd
47- 49 Mary Parade
Rydalmere NSW 2116
Ph + 61 2 8865 0300
Dental splints under scrutiny: Nylon, PMMA, POM and 3D-printed resins
By Terry Whitty
Occlusal splints remain one of the simplest yet most effective tools in dentistry. Whether prescribed for bruxism, temporomandibular disorders, or as protective adjuncts in restorative therapy, splints are only as good as the materials they are made from. In an era of digital design and rapid manufacturing, clinicians now have more options than ever: flexible nylons, industrially-polymerised PMMA blanks, engineering polymers such as POM and increasingly, vat-polymerised 3D-printed resins. Each material comes with marketing promises, but not all splints are created equal.
Stability, rigidity, wear resistance, hygiene and long-term accuracy matter far more than ease of insertion or flashy comfort claims. This article examines the science behind these materials — and makes the case that nylon, in particular, is vastly oversold.
Nylon splints: Flexible but fundamentally flawed
There is a lot of noise made about nylon splints lately with manufacturers touting huge benefits, however nylon’s flexibility is its defining feature and the source of both its attraction and its undoing. For the patient, a nylon splint feels comfortable, seats easily into undercuts and is almost unbreakable. For the clinician, it could be a nightmare of instability!
Occlusal therapy usually demands rigidity. A splint must hold stable contacts, resist distortion under occlusal force and act as a platform for neuromuscular deprogramming. Nylon cannot do this. It’s low modulus of elasticity means even moderate bite forces bend and deform the appliance, undermining any precise occlusal scheme. Water sorption further compounds the problem: nylon swells, warps and loses accuracy over time (Benli et al. 2023).1
Clinically, nylon splints soon become stained, rough and malodorous. Adjustment is nearly impossible, polishing is poor - unless you use some form of solvent fuming and melting of the outer surface. This is called vapour polishing and without it, plaque accumulation is common. In effect, they are glorified sports guards: they protect teeth from direct wear but fail to provide therapeutic control. Their place is in short-term protection or for insertion into highly undercut arches — not as a definitive occlusal therapy device. And to make matters worse, it’s harder for patients to keep these types of splints clean!
PMMA: The gold standard still dominates
PMMA, especially in milled form, remains the material of choice for serious occlusal therapy. Conventional heat-cured PMMA has long been used successfully and digital workflows have elevated it further.
Now milled blanks are polymerised under industrial heat and pressure, producing dense, homogenous pucks with near-complete monomer conversion. The result is rigidity, dimensional stability and polishability. Occlusal contacts can be refined and maintained precisely. Surfaces polish to a smooth gloss, reducing plaque accumulation and improving comfort. While acrylic is more brittle than nylon or POM, fractures are predictable and repairable, unlike the gradual warpage seen in nylon. Mechanical tests repeatedly show that CAD/CAM-milled PMMA exhibits the best flexural strength, modulus of elasticity and hardness compared to other manufacturing methods (Guimaraes et al 2023).2 Most importantly, the literature consistently demonstrates that rigid acrylic appliances are more effective than soft or flexible ones in reducing muscle hyperactivity and improving temporomandibular disorder symptoms (Benli et al. 2023).1
POM: The engineering alternative
Polyoxymethylene (POM) sits between PMMA and nylon in the clinical landscape. This engineering polymer is strong, stiff, and fatigue-resistant, with very low water sorption and excellent dimensional stability. Its naturally lubricious surface resists plaque build-up and contributes to patient comfort. For bruxers who fracture acrylic splints, POM offers an appealing toughness. Thin sections are possible without chipping, and patients report smoothness and durability.
Figure 1. Nylon splint.
Figure 3. POM splint.
Figure 2. Gold standard PMMA splint.
Figure 4. 3D resin printed splint.
Table 1. Comparative science
Flexural Modulus (MPa)
n Nylon: ~500–1,000
n 3D-Printed Resins: 1,000–2,000 (variable)
n PMMA (milled): ~2,200–3,200
n POM: ~2,800–3,000
Surface Finish / Plaque Retention
n Nylon: Hard to polish, especially chair side , stains, malodour
n 3D-Printed Resins: Smooth when cured, but prone to microroughness
n PMMA: Excellent polish and gloss retention, plaque resistant
n POM: Naturally smooth, highly plaque-resistant
However, POM is difficult to adjust, cannot be bonded or repaired easily and is often available only in opaque shades. It is an excellent material for high-load cases where longevity matters, but less adaptable chairside than PMMA.
A recent review confirmed POM’s high strength, stiffness and low water sorption, highlighting its suitability in removable prosthetics and, by extension, occlusal splints (Schierz O et al 2021).3
3D-printed VAT polymerised splints: Promise and problems
VAT polymerised (resin-based 3D-printed) splints are the newest addition. Marketed as quick, economical and precise, they integrate seamlessly with digital workflows. Design in CAD, print overnight, cure and deliver the next day: the workflow it seems easy enough and chairside its very seductive, but the science is less reassuring. Mechanical testing shows that most 3D-printed resins fall short of milled PMMA in flexural strength, modulus, hardness and wear resistance (Prado Neto, Casagrande & Zanatta 2023; Gibreel et al. 2022).4 Water sorption and solubility remain higher than in PMMA or POM (Benli et al. 2023).1 Layer orientation affects strength, introducing variability. Some resins yellow or degrade under oral conditions, especially if curing is incomplete. Clinically, 3D-printed splints often feel lighter and are well-tolerated initially. But wear resistance is a concern. Occlusal contacts may erode or “mush out” faster than with milled PMMA. Longevity beyond 12–18 months is not well-documented and the literature warns against using 3D-printed splints as a long-term solution without more robust evidence (Gibreel et al. 2022).4 That said, they are valuable in short-term therapy, trial appliances or as fast, economical options in situations where speed matters more than lifespan. Their role is complementary, not yet equivalent to milled PMMA or POM.
Conclusion
Occlusal splints are simple devices with complex demands.
• Milled PMMA remains the gold standard: rigid, precise, repairable and scientifically validated.
• POM offers a strong alternative for bruxers and highload cases.
• 3D-printed resins are promising but still interim: fast and economical, but mechanically inferior and clinically under-studied.
• Nylon is comfortable but fundamentally flawed, suitable only in niche scenarios.
The science is clear: rigidity, polishability and dimensional stability are non-negotiable for true occlusal therapy. Nylon and, for now, most 3D-printed resins cannot meet that standard. PMMA and POM can.
References
1. Benli M, Al-Haj Husain N, Ozcan M. Mechanical and chemical characterization of contemporary occlusal splint materials fabricated with different methods: a systematic review. Clin Oral Investig. 2023 Dec;27(12):7115-7141. doi: 10.1007/ s00784-023-05360-0. Epub 2023 Nov 1. PMID: 37910242.
2. Guimaraes DM, Campaner M, Santos RWD, Pesqueira AA, Medeiros RA. Evaluation of the mechanical properties of different materials for manufacturing occlusal splints. Braz Oral Res. 2023 Apr 28;37:e034. doi: 10.1590/1807-3107bor-2023. vol37.0034. PMID: 37132723.
3. Schierz O, Schmohl L, Hahnel S, Rauch A. Polyoxymethylene as Material for Removable Partial Dentures-A Literature Review and Illustrating Case Report. J Clin Med. 2021 Apr 2;10(7):1458. doi: 10.3390/jcm10071458. PMID: 33918124; PMCID: PMC8038064
4. Gibreel M, Perea-Lowery L, Vallittu PK, Garoushi S, Lassila L. Two-body wear and surface hardness of occlusal splint materials. Dent Mater J. 2022 Nov 30;41(6):916-922. doi: 10.4012/dmj.2022-100. Epub 2022 Oct 27. PMID: 36288940.
About the author
Terence Whitty is a well-known dental technology key opinion leader and lectures nationally and internationally on a variety of dental technology and material science subjects. He is the founder and owner of Fabdent, a busy dental laboratory in Sydney specialising in high tech manufacturing. Using the latest advances in intra- and extra-oral scanning, CAD/CAM, milling, grinding and 3D printing, most specialties are covered including ortho, fixed and removable prosthetics, computerised implant planning and guidance, TMD, sleep appliances and paediatrics.
• Any Design
• HD PMMA Milled
• Flexion Milled
• POM Resin Milled
• 3D Print Option
• Perfect Fit
• Upper or Lower
• All scans accepted
case study
Fully digital treated aesthetic single crowns on matriX® Tissue-Level implant and root resections
By Dr Alessandro Agnini & Dr Andrea Mastrorosa Agnini (Italy) with Dental Technician Pierfrancesco Golfarelli
This case provides a perfect example on how tradional knowledge and innovative protocols are setting the stage in modern dentistry. In fact, partially edentulous patients are challenging to treat for many different reasons: an absence of an organised diagnostic criteria for example, or the effective recognition of risk factors. Infection control, strategic treatment sequencing and management of the proper occlusion are key to control during rehabilitation.
The very first step in such complex cases is conservative endodontic treatment and then positioning a first set of provisional restorations to improve aesthetics, phonetics and patient comfort. After osseous resective surgery, in combination with implant placement, which in this case was the innovative matrix Implant (TRI Dental Implants).
It is true, in fact, that the advent of new technologies has enabled the dental team to use new material and new equipment that facilitated the production of an adaptation and an accuracy of the prosthetic rehabilitation that has, up to now, been difficult to obtain.
Today, intraoral mapping technology is one of the most exciting new areas in dentistry since 3-dimensional scanning of the mouth is required in a large number of procedures such as prosthodontics, implant dentistry and orthodontics. All the existing intraoral scanners are trying to face the limitations and the disadvantages of the traditional impression procedure maintaining a high level of accuracy in order to be used as an efficacious alternative to the conventional impression technique.
Working with the innovative design, abutment and ti-base free, provided by the matrix, helped the authors in finalising this case in a timely fashion, maintaining a high level of accuracy.
Figures 1-4. Initial situation.
Figures 5-6. Insertion of matrix Tissue-Level Implant.
Figure 7. Digital impression taking after healing phase.
Figures 12-13. Final restoration in situ.
Figure 9. Design of final monolithic restoration.
Figure 11. Finalisation of monolithic crown.
Figue 10. Final design monolitic restoration ready to be milled.
Figure 8. Digitalisation of mouth situation.
Figures 14-15. X-ray 6 months follow-up.
Figures 16-18. Final restoration.
Figures 19-21. 15-month follow-up.
About Dr Alessandro Agnini
Dr Alessandro Agnini graduated in 1989 from the University of Modena and Reggio Emilia, Italy. He has private dental practices in Modena and Sassuolo, Emilia Romagna, Italy and specialises in fixed prosthetics, paradontology and implantology. He attended a two-year programme of studies with Gianfranco Carnevale and Gianfranco Di Febo and in 2002 he obtained a diploma in the Multidisciplinary Treatment of Paro-
dontal Patients from the University of Bern, Switzerland. He is a lecturer of specialist courses at the University of Foggia, Puglia, Italy. He is the author of many Italian and international scientific publications and lectures frequently at national congresses in Italy. Since 2007 he has been scientific director of an annual course in Fixed Prosthetics, Paradontology and Implantology based at his own private studios in Emilia Romagna, Italy.
The New ELITE IntraOral Scanner from Shining 3D uses patented IntraOral Photogrammetry Technology to be the most accurate scanner available.
• Small form factor
• Lightweight 124 grams!
• Ultra fast scanning
• Dual mode IPG scanner
• Complete software suite
• Scan All On X Cases accurately
• Suitable for all IntraOral Scanning
• 3-year Warranty
Figures 22-23. 5-year follow-up.
15-month follow-up. 5-year follow-up.
Dr Andrea Mastrorosa Agnini graduated in 2007 from the University of Modena and Reggio Emilia. Dr Agnini works in private practice in Modena and Sassuolo, Emilia Romagna, Italy, following his brother, Alessandro, specialised in fixed prosthodontics, periodontology and implantology. He attended the NYU Dollege of Dentistry with Dr Dennis Tarnow, Dr Christian Stappert, Dr Stephen Chu and Dr Michael Bral. He is
a Clinical Research Fellow of the Ashman Department of Periodontology and Implant Dentistry at NYU, with Dr Sang Choon Cho and is co-author of Italian and international scientific publications. Since 2007 he has been Clinical Fellow of an annual course of Fixed Prosthetics, Periodontology and Implantology based at his brother Alessandro’s, who is the scientific director, private practices in Emilia Romagna, Italy.
About Dr Andrea Mastrorosa Agnini
The Solution For Perfect Implant Position
Free Case Evaluation Send
All implant surgical guides
• Edentulous Cases
• Scan Appliances
• Free Planning Software
Indirect pulp capping: Bio-bulk fill technique and Bulk&Go
By Dr Vincenzo Tosco, DDS, PhD
This clinical case demonstrates the basic concepts of the Bio-Bulk Fill technique for indirect pulp protection, using Biodentine™ XP (Septodont) material as a dentine replacement, to perform the restoration of a deep caries lesion.
Federica, aged 37 years old, presented with mild sensitivity in her lower left molars. Clinical examination revealed a carious lesion on the first molar and an old filtered composite restoration without occlusal morphology. The tooth was positive on vitality testing and negative on percussion testing. Radiographic examination revealed no periodontal lesions.
Methods
T he two cavities were prepared with high- and low-speed burs and a vanadium excavator. The indirect pulp capping was then performed on the second molar using Biodentine XP, filling the cavity up to 1.5mm from the occlusal margin. After allowing the material to harden for 15 minutes, the class II cavity was transformed into a class I cavity and the adhesive procedures were performed. Next, a body shade composite was applied with the Essential Lines modelling technique to complete the direct restoration. Finally, the first molar restoration was performed using the Bulk&Go procedure combined with the Essential Lines technique.
Dr
Renner on Biodentine...
How long have you been using Biodentine?
In my clinical practice, I have employed Biodentine for an extended period of 6 to 7 years. With the introduction of Biodentine XP, I switched to using this new product this year.
Why do you use the Bio-Bulk Fill procedure with Biodentine? What are the main advantages for you?
This technique enables clinicians to simplify direct posterior restorations, including both direct and indirect pulp capping, through the utilisation of a bioactive material such
Discussion
Biodentine is a well-studied tricalcium silicate-based material that has demonstrated biocompatibility and bioactivity in vitro and in vivo. Pre-clinical investigations have revealed its mechanisms of interaction with dental hard tissues.
as Biodentine XP, as a dentine substitute. Indeed, the placement of a protective barrier over exposed or unexposed pulp induces the formation of a dentinal bridge and maintains its vitality and function. The combination of Biodentine XP and a resin-based composite for cavity filling ensures a safe outcome, preserving pulp vitality within a single visit.
When and in which cases do you use the Bio-Bulk Fill procedure with Biodentine XP?
I use it mainly in very deep cavities as a protective base, or for vital pulp therapy, both for indirect and direct pulp capping.
Biodentine is shown to create a protective seal that prevents bacterial infiltration, thereby safeguarding the dental pulp. It achieves this through micro-mechanical retention by infiltrating dentinal tubules and by inducing tertiary dentine synthesis, which enhances pulp protection. Biodentine also reduces the expression
and function of pain receptors, leading to the absence of postoperative pain and hypersensitivity. Additionally, when applied to odontoblastic cells, it decreases pro-inflammatory secretion, thereby reducing inflammation. These findings highlight the beneficial effects of Biodentine on dental hard and soft tissues, emphasising its potential for use in dental procedures.
Conclusion
The scientific community, supported by in vitro and in vivo clinical studies/ reports, demonstrates that Biodentine is biocompatible, has strong mechanical properties and can be safely applied in restorative dentistry. In addition, Biodentine requires no surface conditioning treatment and can be cut and reshaped like natural dentine. Because of its characteristics, it can be used as a bulk substitute for permanent dentine to replace the entire damaged or lost dentine, thus as indirect pulpal protection and not just as a direct pulp capping material. The surface of Biodentine can be bonded like natural dentine with various adhesives before the final application of composite resins.
Figure 1. Pre-operative radiograph.
Figure 3. Cavity preparation.
Figure 4. Matrix, wedge and ring placement on the second molar.
Figure 2. Isolation.
Figure 5. Verification of a proper contact point.
Introduction
Nowadays, bulk-fill composites (BFCs) are among the resin-based materials most widely used for the restoration of posterior teeth. They can be placed and cured in increments of up to 4–5mm in thickness, eliminating the need for layering, shortening the clinical procedure and simplifying handling. Furthermore, the introduction of bioceramic materials with high-performance properties as a replacement for dentine makes their application possible for the bulk-filling of deep cavities. This clinical case presents two direct restorations in the posterior sector, one based on the Bulk&Go technique proposed by Style Italiano and a second based on the Bio-Bulk Fill technique.
The Bulk&Go technique takes full advantage of the favourable chemical–physical characteristics of the high-viscosity BFCs to allow for a onestep procedure. Therefore, providing the cavity that does not exceed a depth of 4mm, its restoration can be performed in a single mass application. The Bio-Bulk Fill technique is a two-step procedure based on the positioning of a first layer of bioceramic material, which acts as a dentine substitute, instead of BFC. The second cover layer consists of an enamel-like composite, like a Body Shade composite, with low translucency.
Case report:
Clinical signs and symptoms
The young patient reported mild sensitivity in her left lower molars. Clinical examination revealed a carious lesion on the first molar and an old filtered composite restoration without occlusal morphology.
The tooth was positive on vitality testing and negative on percussion testing. Radiographic examination revealed no periodontal lesions.
Diagnosis
Dental caries was present in both molars, with a carious lesion on the first molar and secondary lesions on the second molar.
Procedure and treatement
Arubber dam was placed to isolate the two molars to be treated (Figure 2). With the cavities open, the carious lesions were first cleaned with the aid of high-speed burs and then with manual instruments such as vanadium excavators. When all the infected dentine had been removed, a class I on first molar and a class II on the second were obtained (Figure 3). For the second molar, a sectional metal
matrix was placed with wedge and ring to transform class II in class I (Figure 4).
The closure of the matrix on the preparation margin of the cavity was checked and a proper contact point verified (Figure 5).
After that, the Biodentine XP biomaterial was applied inside the cavity in a single mass up to 1.5 mm from the occlusal surface, thus leaving space for the final layer of composite enamel.
Once applied, the material was left to harden for 15 minutes before proceeding with the adhesion procedure (Figure 6). The enamel margin of the cavity preparation was kept free in order to build the mesial wall with the composite, transforming class II into class I (Figure 7).
Subsequently, the enamel was selectively etched for 20 seconds (Figure 8). The mesial wall of the second molar was built, making it possible to restore the two class I cavities (Figure 9).
The Bulk&Go technique was used in the first molar, while in the second molar, the last layer of enamel shade composite was placed using a Body Shade composite to complete the restoration. The Essential Lines technique was applied for modelling (Figure 10). After filling the cavity and condensing the composite, the essential lines were drawn to reproduce the occlusal anatomy of each posterior tooth (Figure 11). The two restorations were then finished and polished (Figure 12).
Figure 6. Biodentine XP placement.
Figure 9. Restoring the mesial wall of the second molar.
Figure 7. Enamel margin of the cavity preparation.
Figure 10. Essential lines technique.
Figure 8. Selective-etch on enamel.
Figure 11. Drawing the lines on the first and the second molars.
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy
Biodentine™ saves pulps EVEN with signs and symptoms of irreversible pulpitis*
Biodentine™ saves pulps EVEN with signs and symptoms of irreversible pulpitis*
saves pulps EVEN with signs and symptoms
saves pulps EVEN with signs and symptoms
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
Bone Grafting
For vital pulp therapy, bulk- lling the cavity with Biodentine™ makes your procedure better, easier and faster:
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
tooth
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
As the first all-in-one biocompatible and bioactive dentin substitute, Biodentine™ fully replaces dentin wherever it’s damaged.
Only one material to fill the cavity from the pulp to the top
• Immediate Pain relief for your patients’ comfort • Bio-Bulk filling procedure for an easier protocole
• Minimally Invasive treatment preserving the tooth structure
• Bio-Bulk filling procedure for an easier protocole
• Immediate Pain relief for your patients’ comfort
New Biphasic Formulations allowing you to manage the pace of your bone grafting procedures:
Similar mechanical behavior as natural dentin: ideal for bulk filling
Minimally Invasive treatment preserving the tooth structure
Immediate Pain relief for your patients’ comfort
Biodentine™ helps the remineralization of dentin, preserves the pulp vitality and promotes pulp healing. It replaces dentin with similar biological and mechanical properties.
• Bio-Bulk filling procedure for an easier protocole
(80% ß-TCP / 20% Hydroxyapatite)
The final enamel restoration will be placed within 6 months.
Improving on Biodentine the composite onto Biodentine full restoration in a single session
Bio-Bulk filling procedure for an easier protocole
Bio-Bulk filling procedure for an easier protocole
40/60 (40% ß-TCP / 60% Hydroxyapatite)
Innovative by nature
Innovative by nature
Innovative by nature
Please visit our
Please visit our website for more information
www.septodont.com
Please visit our website for more information www.septodont.com
To enjoy the clinical benefits of the first and only dentin in a capsule, ask your dental distributor for Biodentine™.
13. 9 months follow-up.
The control x-ray shows the different radiopacities of the BFC and Biodentine XP. Furthermore, the entire cavity was filled and sealed without the presence of gaps or voids within the restorations.
Follow up
At 9 months, no signs of periodontal lesions were evident and no symptoms were reported by the patient (Figure 13).
BDiscussion
iodentine has been applied as a bulk restorative material in deep dentine cavities to replace dentine. Biodentine is easy to handle, showing good marginal adaptation. When covered with resinbased composite, it is a well-tolerated permanent dentine substitute. Additionally, Biodentine can be cut and shaped like the natural dentine. Furthermore, in
References
1. About I. Biodentine: from biochemical and bioactive properties to clinical applications. Giornale Italiano di Endodonzia, 2016, Volume 30, Issue 2, Pages 81-88, https://doi.org/10.1016/j.gien.2016.09.002.
2. Falakaloğlu S, Yeniçeri Özata M, Plotino G. Microshear bond strength of different calcium silicate materials to bulk-fill composite. PeerJ. 2023 Mar 29;11:e15183. doi: 10.7717/peerj.15183. PMID:37013141; PMCID: PMC10066686.
3. Tosco V, Vitiello F, Furlani M, Gatto ML, Monterubbianesi R, Giuliani A, Orsini G, Putignano A. Microleakage Analysis of Different Bulk Filling Techniques for Class II Restorations: μ-CT, SEM and EDS Evaluations. Materials (Basel). 2020 Dec 23;14(1):31. doi: 10.3390/ma14010031. PMID: 33374708; PMCID: PMC7793523.
4. Chiodera G, Orsini G, Tosco V, Monterubbianesi R, Manauta J, Devoto W, Putignano A. Essential Lines: a simplified filling and modeling technique for direct posterior composite restorations. Int J Esthet Dent. 2021 May. 10;16(2):168-184. PMID: 33969973.
About the author
Dr Vincenzo Tosco graduated in Dentistry at the Universidad Alfonso X el Sabio, Madrid, Spain. He completed his PhD in Biomedical Sciences at the Università Politecnica delle Marche, Ancona, Italy and is currently a research fellow at the same University under the supervision of Professors Angelo Putignano and Giovanna Orsini. His main activities focus on endodontics, restorative dentistry and aesthetics.
this case, the patient reported absence of post-operative pain and post-operative sensitivity. This may be due to at least two factors:
1. The infiltration of Biodentine into the dentine tubules. The precipitation of crystals within the tubules decreases dentine tubule permeability and fluid movement, which may decrease postoperative sensitivity.
2. The reduction of odontoblast pain receptor expression and function and the reduction of the secretion of proinflammatory cytokines.
Conclusion
Biodentine has multiple applications. Considered a dentine substitute due to its similar physical mechanical characteristics, it can be used to fill the cavity up to 1.5mm from the occlusal surface in bulk mode, following the Bio-Bulk Fill technique. The combination of Biodentine for filling the cavity and the Essential Lines technique for modelling the occlusal surface simplifies and saves time in direct posterior restoration.
Figure 12. Before and after.
Figure
Jannali practice puts patient health first
By David Petrikas
Anewly built dental practice in Sydney’s Sutherland Shire is setting a new standard for accessibility and patient-centred care, offering a welcoming environment for local families, children and special care patients.
Dr Ivan Chee recently relocated Health First Dental from a smaller suite in Jannali to a purpose-designed, street-level practice that reflects his long-standing
commitment to inclusive, communityfocused dentistry. From the outset, the design brief was guided by the needs of two patient groups he is particularly passionate about — children and patients requiring special or elderly care.
“I’ve always loved working with kids, special needs patients and the elderly,”
Dr Chee said. “That’s why I deliberately chose a street-level location and designed the practice to be fully accessible for everyone, including patients with mobility challenges.”
Patient comfort was a central consideration throughout the design process, particularly for those who may feel anxious or disoriented in unfamiliar clinical environments.
“If a child is very anxious, or a patient has dementia, they may feel uneasy in a new space,” he explained. “I tried to anticipate what might help them feel calmer — from televisions and large windows to a world map that provides something familiar or engaging to focus on.”
While caring for these patient groups can present additional challenges, Dr Chee felt strongly that they should have access to high-quality dental care close to home, without the need to travel outside the “Shire”.
After attending dental expos such as ADX and seeking professional referrals, Dr Chee met with several design and fit-out companies to explore how his vision could be realised. He also worked closely with his local A-dec dealer, Tanya McRae-Klein from Dental Installations in nearby Miranda, who provided guidance on equipment selection, services placement and fit-out recommendations.
“Dental Installations have supported me for years — including helping me with a portable dental cart for use at a local nursing home,” Dr Chee said. “They’ve always been supportive, without ever trying to upsell or pressure me.”
With a clear vision in place, Dr Chee set out to create a practice that felt as “non-dental” as possible. He ultimately partnered with Andrew Mulroe, owner of surgery fit-out company Dental Fitout Projects, to deliver the project.
As the final piece of the puzzle, Teamwork Technology was selected to deliver the practice’s IT and digital infrastructure. Dr Chee said that with modern dental practices increasingly reliant on integrated technology, it was essential that IT systems were embedded from the outset rather than retrofitted later.
“Dental IT infrastructure now underpins almost everything we do, so future-proofing was essential,” he said. “Teamwork Technology were chosen because they worked closely with Dental Fitout Projects throughout the design and build process, which meant everything could be properly planned, co-ordinated and built in from day one.”
This collaborative approach ensured the practice was established with a robust, scalable IT foundation that supports current workflows while allowing flexibility as technology and clinical needs evolve.
Rather than conducting a competitive tender based solely on price, Dr Chee prioritised working with a team that understood his vision and adopted a collaborative approach. Accessibility, spatial openness and natural light were central to the design, leading to the inclusion of high ceilings and full-height glazing at the front of the building.
These features were achieved by relocating services such as air-conditioning ducting into wall cavities, allowing ceiling heights to be increased. Working closely with Andrew Mulroe and Senior Project Manager Steven Hyde, Dr Chee was involved in both major design decisions and finer details, resulting in a cohesive and carefully considered outcome.
The generously sized reception area creates a strong first impression, featuring a striking 3D carved world map that immediately invites curiosity and conversation. A curved reception counter with an LED-illuminated acrylic panel and diagonal timber detailing sits in front of Health First Dental signage and a custom tooth logo.
Throughout the practice, woodgrain flooring, upholstered chairs with timber backrests, grey cabinetry and soft white walls establish a calm, contemporary aesthetic. The central corridor has been intentionally kept wide to support disabled access while maintaining an efficient, uncluttered workflow between reception, surgeries, private office and sterilisation areas.
Each surgery features frosted glass doors, providing privacy while allowing natural light to flow through. Bespoke cabinetry with chamfered corners maximises bench space, while generous cabinets and deep drawers support efficient clinical workflows. The surgeries are fully equipped with sedation facilities, in-built X-ray units, patient monitors and overhead entertainment screens.
Family-friendly details are incorporated throughout the practice, including a built-in cabinet stocked with toys, Lego Star Wars models, figurines and books for children and visiting siblings. A large bathroom includes a baby change table stocked with wipes and tissues for added convenience. Staff amenities were also carefully considered, further enhancing the relaxed, non-clinical atmosphere for both patients and team members.
Dr Chee’s approach to equipment selection was informed by past experience. Having previously worked with European dental chairs that were prone to maintenance issues, he sought a more robust and reliable option with less electronic complexity.
surgery | DESIGN
“Repairs often required replacing entire circuit boards, which was costly and caused downtime,” he said. “That pushed me to look for something more durable and practical.”
After trialling A-dec chairs, reliability, comfort and ergonomics emerged as key decision factors. Dr Chee initially relocated A-dec 300 chairs and has since invested in an A-dec 400 chair with the latest A-dec 300 ‘Pro’ delivery system and CP5i touchpad.
“Patients really notice the comfort of the A-dec 400 chair — especially the upholstery and backrest,” he said. “They can get in and out easily, which is important.”
The modern appearance of the A-dec chairs complements the new practice environment and helps patients feel at ease during longer procedures. Dr Chee opted for a traditional delivery system with a cuspidor, recognising patient expectations and familiarity.
“Patients like having the ability to rinse — comfort matters, especially when they’re paying for care.”
Summary
The Practice
The Practice Health First Dental
The Principal Dr Ivan Chee
Practice Type General
Location Jannali, Sydney, New South Wales
Size 158 square metres
No of chairs 3 + 1
The Team
Design
Owner and Andrew Mulroe
Dental Fitout Projects Sydney
Builder Dental Fitout Projects Sydney
Project Manager Steven Hyde
Installer
IT Installer
Equipment
Dental Installations, Miranda, Sydney
Teamwork Technology
Dental Units A-dec 300 and A-dec 400 Pro traditional delivery with A-dec 572 Chair Mount LED lights
Sterilisation W&H Lisa and Melag Vacuklav 23B+
Imaging Acteon Xgenus Wall mounted x-ray unit
Intraoral Scanner Medit i700 with custom built PC
Compressor Cattani AC200
Suction Cattani Turbo Smart A
From a clinical perspective, the entire dental team is familiar with A-dec equipment, including a left-handed dentist who can easily reconfigure the delivery system. Upholstery colour options also influenced the final design palette, with Dr Chee’s wife contributing to the selection of colours and artwork to complement the latest A-dec finishes.
Lighting was another important consideration, with the practice fitted with A-dec 500 LED operatory lights. The stadium-style design delivers balanced, daylight-quality illumination with a high Colour Rendering Index, reducing shadows and supporting precision work.
“The lighting is particularly helpful when colour-matching anterior composites and when working with loupes,” Dr Chee said. “It provides a broad, even spread of light that makes a real difference clinically.”
Information contained in this section is provided by the manufacturers or distributors. Australasian Dental Practice does not assume responsibility for the accuracy of the data.
ASIGA Ultra Crown Kit
Introducing the ASIGA Ultra Crown Kit — your solution for fast, efficient, and precise crown production on the ASIGA Ultra. Designed with a compact build platform and tray, this kit minimises material usage while maximising pro-
ductivity. Achieve 3D printed crowns in under 12 minutes, streamlining your workflow without compromising accuracy or quality. Perfect for crowns, inlays, onlays, veneers, and more, the Ultra Crown Kit empowers dental professionals to deliver exceptional restorations quickly and consistently. Experience a new level of speed and efficiency — print faster, handle less material, and elevate your digital dental production with ASIGA’s advanced innovation.
Lo Russo Retractors are the essential tool for precise intraoral scanning of edentulous arches. Specifically designed to optimise visibility and access, these retractors gently and effectively displace soft tissues, ensuring a clear, unobstructed scanning field. Their ergonomic, patientfriendly design enhances comfort while improving accuracy and efficiency during digital impression procedures.
Ideal for full-arch or edentulous workflows, Lo Russo Retractors help clinicians capture data more reliably. Durable, autoclavable and easy to handle, they’re a must-have accessory for any clinician aiming to achieve consistent, highquality digital impressions.
Biodentine XP is a next-generation dentine restoration system that combines pulp therapy and restorative performance in one solution. Made from extra-pure tricalcium silicate with proprietary Active Biosilicate (ABS) Technology™, it delivers excellent biocompatibility and bioactivity. Designed for daily deep cavity restorations, it can be placed directly or indirectly over the pulp, stimulating healing and promoting reparative dentine formation to preserve tooth vitality. Biodentine XP creates a tight seal through micromechanical anchorage and maintains longterm dimensional stability to resist microleakage. With mechanical properties similar to natural dentine, it is ideal for bulk-fill techniques. Conven-
ient all-in-one cartridges and dedicated delivery tools ensure easy, consistent application in one or two visits.
Piksters®, Australia’s most used and recommended interdental brush system, has launched a new Prescription Sampling Envelope designed to make it easier for dental professionals to prescribe and sample interdental brushes to their patients.
The envelope features Piksters’ popular Mouth Map — a practical tool to record the specific interdental brush size required for each tooth gap. This personalised prescription motivates patients to use the correct size brush in the correct position, improving compliance, patient satisfaction and overall oral health outcomes. Piksters already provides Professional Packs full of interdental brushes to practices nationally for sampling and have also released a new colour gap-sizing probe. Together with the envelope, practices can now easily “Size, Prescribe and Sample” the ideal Piksters for their patients. Envelopes (and pads) are available free to dental practices.
Tru-line® Invisible Orthodontics celebrates 20 years of Australian made clear aligners with the last innovation - Tru-Line X-tra 48 hour ALIGNERS™
s Precision CAD designed and CNC manufactured, Laser Cut
s Free case evaluation
s Free online training course
s Free viewing software
s Realistic treatment setupsNo Cartoonodontics!
Mention this ad for 50% off your first case
s Free Click retainers
s 48 hour turnaround on request
s Trusted experience, Australia’s first established Aligner brand in 2004
s Satisfaction guaranteed
s 100% value
Swiss Thinking. Shared Success.
The
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.