Published on behalf of the European Healthcare Investor Association by Curis Intelligence Ltd, The King’s Fund, 11-13 Cavendish, London W1G 0AN. +44 (0)20 7173 0548.
No responsibility can be taken by the publisher or contributors for action taken as a result of information provided in this publication. All rights reserved; no part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise without either the prior written permission of the publisher or a licence permitting restricted copying issued in the UK by the Copyright Licensing Agency Ltd and in the USA by the Copyright Clearance Center Inc.
Introduction
Europe has seen growing demand from investors for healthcare real assets. 2025 saw a significant flow of capital into the sector from North American as well as European investors, with M&A and large portfolio deals playing a substantial role in the reported transaction volumes across Europe. Strong operational performance and positive market sentiment, as buyers seek entry points and scale amidst vendors chasing exits, suggest a potential for an active market.
Healthcare real assets are a component of what is known as social infrastructure. Social infrastructure refers to the physical assets that support the delivery of essential public and social services such as healthcare and education. This has become increasingly important due to several factors, including ageing populations and fiscal constraints. Healthcare infrastructure forms one of the more complex elements, relating to the physical environments that enable the delivery of care across the full spectrum of healthcare. Unlike more conventional real estate asset classes, healthcare real assets encompass both the physical and operational aspects of the sector, and therefore, asset performance is driven by trading performance as well as the more traditional valuation drivers.
SOCIAL INFRASTRUCTURE
HEALTHCARE INFRASTRUCTURE
Acute and specialist hospitals. General hospitals, university hospitals and specialist surgical facilities. Primary care and outpatient facilities. GP surgeries, medical centres, diagnostics hubs and medical office buildings (MOBs).
Long‑term care and supported living. Care homes for the elderly, nursing homes, dementia care, learning disability accommodation and mental health facilities.
Rehabilitation and specialist treatment centres. Covering post-acute rehabilitation, orthopaedics, oncology and neurological care.
Ancillary healthcare infrastructure. Laboratories, pharmacies and day-case clinics.
Ryan Richards
Why Healthcare? Structural Drivers of Investment
The investment case for healthcare real assets is driven by a combination of longterm structural drivers, which are influenced primarily by short-term economic cycles. It is underpinned by key drivers, which are:
• Demographics and rising co-morbidities, creating predictable, irreversible growth in demand across care.
• Assets typically benefit from long, inflationlinked leases, which provide insulation in volatile macroeconomic conditions. This has aided the sector’s resilience, with stable occupancy and performance even during the past few years of headwinds.
• Returns have remained steady, which has been majorly driven by income rather than a pure reliance on capital growth.
• Institutional capital has, in addition to conventional returns, been chasing investments that align closely with ESG and impact objectives, which is more than covered by the social and personal nature of healthcare as a sector.
Key Investor Types in European Healthcare Real Assets
The European healthcare investment landscape attracts a broad and diverse investor base:
INSTITUTIONAL INVESTORS Including pension funds and insurance companies, attracted by long income
LISTED AND PRIVATE REITS Most active in care homes, hospitals and primary care.
INFRASTRUCTURE FUNDS Increasingly allocating to “infra-like” healthcare assets as competition for traditional infrastructure intensifies.
PRIVATE EQUITY Often pursuing platform strategies, operational consolidation
SOVEREIGN FUNDS Targeting scale portfolios and operating platforms.
FAMILY OFFICE / HIGH NET WORTH Targeting entry points to operating platforms.
Deal Structures, Capital Flows and Market Attraction
Transactions utilise a range of structures, reflecting the operational nature of the sector. These include sale-and-leaseback, PropCo/ OpCo structures, Forward funding/Forward commitments, and more recently, the trend of WholeCo and management agreementstyle structures. Whether it’s allowing operators to recycle capital, separating real estate ownership from operations or investors participating directly in operating performance alongside rental income, each of these structures has numerous benefits.
Assets typically benefit from long, inflationlinked leases, which provide insulation in volatile macroeconomic conditions.”
Capital flows into European healthcare have demonstrated cyclical sensitivity, but with strong long-term momentum, Europe consistently attracts a significant share of crossborder investment. European markets are now experiencing easing interest rates, narrowing spreads and strong operational performance. All of this has contributed to a flow of capital directed at portfolios and scalable platforms, with investors seeking reasonable entry points as well as growth opportunities.
European Transactions
Recent years have seen many standout transactions as European care markets look to be consolidating. Transactions such as Assura’s purchase of NW REIT’s uk hospital, Aedifica & Cofinimmo joining to become the 4th largest healthcare REIT in the world, the merger of PHP and Assura and a run of significant corporate care platform acquisitions by Welltower (now the largest REIT globally) have demonstrated not only the long term commitment of investors to European healthcare, but healthcare’s significance within real estate.
Investors in HealthcareHealthcare Real Assets 2026
The report expands on the themes mentioned to provide a detailed outlook of European healthcare real assets. This will include:
• Analysis across care homes, hospitals, primary care and emerging asset classes such as medical office buildings. Market dynamics, regulatory frameworks and funding models as they vary geographically.
• Operator fundamentals, labour dynamics and ESG considerations. Investment structures, risk allocation and return drivers.
While the general European economic outlook remains subdued, the view on healthcare real assets remains positive. Demand is essentially non-discretionary and driven by demographics rather than sentiment. As economic conditions stabilise, capital continues to flow decisively to the sector, and healthcare should no longer be seen as a purely defensive allocation, but also as a robust sector with proven long-term income capabilities.
Welcome
European Healthcare Investor Association (“EHIA”) is the largest association of private capital providers investing in healthcare companies in Europe. Our aim is straightforward - to facilitate deals and promote the sector.
We do this by building our community and sharing knowledge through our conferences and networking events for our members, and sector focussed market data and analysis from our strategic partners and our Official Journal, Investors in Healthcare.
Whilst we do not lobby for the sector, we do promote a better understanding of investors’ contribution to the broader healthcare economy from innovation, employment and wealth creation.
Who we are
We are a not-for-profit trade association with over 70 members including private equity, infrastructure, real estate and sovereign funds, foundations and family office investors, corporate leaders, advisors and other members of the healthcare investing community, all focussed on building successful healthcare businesses.
What we do
We help our members to invest capital and expertise into building great healthcare businesses and generating returns. Our members take a long-term approach to investing in privately-held companies, injecting not only capital but dynamism, innovation and expertise. This commitment helps create healthy and sustainable companies, securing millions of jobs and delivering strong returns for their investors such as leading pension funds and insurers, whose members depend on them for their retirements.
How we work
We have an integrated strategy combining information sharing, our two EHIA conferences (“Private Capital” and “Real Assets”), networking events, and a focussed digital offering. We actively communicate with our members on LinkedIn and email, as well as online via our Official Journal, Investors in Healthcare. This is a Google News listed digital business intelligence platform delivering news, data and analytics. This knowledge creates actionable insights for
As Executive Director I am focused on delivering for our members. Central to that mission is having an ongoing dialogue directly with as many of them as possible and my door is always open. Our strategy is for the Association to be a convener of like minded people and a source of knowledge and opportunities for healthcare investors. My remit is to deliver on that strategy by providing valuable benefits for our members.
SARAH WARD Executive Director, European Healthcare Investor Association
investors, coporate leaders and advisors in the sector. Access to the journal is included with membership, with subscriptions available for non-members.
Key to delivering for our members are our partners who not only provide valuable content, but host many of our events. EHIA works closely with a range of strategic partners in the advisory community including J P Morgan (investment banking), McDermott Will & Schulte (legal), L.E.K. Consulting (strategy consulting), Compass Carter Osborne (executive search), Marwood Group (regulatory consulting), RSM Ebner Stolz (accounting), Howden (insurance) and Virgin Money (specialist funding).
Communicating with our membership
Members are time poor, and therefore focussed, relevant content available in an easily digestible format is key. Perhaps as a result of the “virtual” start to the organisation, communication has by necessity been digital – via an active LinkedIn presence; twice monthly newsletters for members and non-members covering deals, people moves and market reports; online via the website including a Resource Hub with a growing library of member-only content; and Investors in Healthcare, the association’s online journal. Investors in Healthcare now has 11,000+ LinkedIn followers and growing as well as nearly 200,000 visitors to its website as it establishes itself as the one stop destination for investors looking for deal flow, insights and news on people, companies and sector trends.
Member feedback
Something
like this is needed in a European context –I believe in the underlying purpose of EHIA’
This isn’t an industry that organizes itself well so there are some real opportunities for EHIA in Europe’
EHIA is a great concept –it’s still early in its maturity, but it’s an idea everyone can get behind’
EHIA could do a lot just by orchestrating members to share existing knowledge’
Focusing on European Healthcare Real Estate
Ed White, Head of UK Consultants ‑ MSCI
Each year, MSCI estimate the size in value terms of the professionally managed global real estate market across all sectors and geographies. The latest iteration estimated a contraction of over 4% down from 13 Trillion (USD) to 12.5 Trillion (USD) across the world and continues a trend which has existed for the last 3 years; the real estate market by value is becoming smaller.
There are a handful of reasons; the main being the impact of currency and the re-sizing of the global office market which experienced the greatest contraction over the period due to declining values (although offices still make up the largest part of the overall global real estate market by value). However, some sectors do not correlate with this contraction and have in fact experienced growth in overall value terms; residential, logistics and industrial (including data centres) and healthcare all form part of this growing and expanding market size estimate and are slowly taking a bigger share of the overall market estimate.
Source: MSCI Real Estate Market Size Estimate
European Healthcare Real Estate
MSCI estimate the current size of the professionally managed investable healthcare real estate market in Europe to be circa £100 Billion with around 80% of this market owned by either listed entities (for example REIT’s) or via an investment vehicle such as an investment fund. This does not include assets in public ownership or the development pipeline.
Diversification of ownership and investment has become a major theme within healthcare real estate more recently. An increase in international investment, particularly from major global asset owners and asset managers has started to change the dynamic (see figure 2), with an increasing proportion of the market now owned directly. This has also become increasingly apparent within the MSCI real estate datasets where MSCI’s European healthcare coverage has nearly doubled over the past decade, with healthcare real estate one of the few sectors where institutions remain selectively active led by these types of investors. Growth in coverage has been particularly pronounced post-pandemic, reflecting a reassessment of sector allocations from retail and office to more defensive sectors and/or those sectors providing growth opportunities. This means healthcare real estate has arguably transitioned to (and can be seen as) a core sector within portfolio allocations.
This growth in coverage now means MSCI
Source: MSCI Real Assets
of Capital Value
An increase in international investment, particularly from major global asset owners and asset managers has started to change the dynamic.”
receives real estate investment data from over 100 portfolios across Europe alone covering over a third of the estimated overall market size for the European Healthcare Investable market. This is a large increase from where coverage was 5 years ago and certainly a decade ago.
The data MSCI receives on these assets is aggregated and anonymized to produce a comprehensive suite of metrics. These include investment rates of return, income fundamentals such as rental growth and yield movements, and a range of additional KPIs. All metrics are directly comparable across other real assets and the broader public and private investment universes, enabling investors and owners to gain transparency and benchmark performance effectively.
The growth in coverage and consequently transparency is due to the long term attractiveness of healthcare real estate as a thematic investment which has been well documented across the European and Global Investment Universe for many years. However, the availability of data has often meant that the investment case has been more difficult to justify particularly alongside more dominant sectors such as retail, offices, residential and logistics. But, as allocations have steadily increased, availability of good quality data has also increased which in turn has enabled MSCI to produce long-term investment metrics to sit alongside the thematic opportunity of the asset class, as described above.
The availability of data has also enabled a
Source: MSCI Real Assets
more granular analysis to be undertaken beyond simply healthcare real estate. The availability of metrics across geographies and property types provides further insight into the performance of healthcare real estate both within the sector and alongside other asset classes.
So what do the performance dynamics look like?
Over the last 10 years, healthcare real estate has delivered the highest risk-adjusted total returns of all major real estate sectors across Europe.
Volatility has been materially lower than office, retail, and hotels, while returns have remained competitive or superior across all sectors apart from industrial/logistics.
Underpinning this high risk-adjusted return profile is a continual stream of stable income which on a Total Return basis is higher than all other sectors despite negative capital growth over the last handful of years.
The differential in the income return
Source: MSCI Real Assets
between healthcare real estate and the wider real estate market is typically due to the leasing structures and operating models which sit within each asset and vehicle. This is quite different to the models which exist in other parts of the wider real estate market and very different from the healthcare sectors nearest comparators.
These structures also provide a level of value protection and appear less sensitive to changing market dynamics from both an occupancy and investment perspective. The impact of pricing and valuation movements can clearly be seen in figure 5 with Europe’s top performing sector, industrials, experiencing far greater volatility due to the external impacts of supply chain dynamics and in certain geographies restricted supply. This has led to large amount of capital squeezing yields only to be unwound as interest rates rose and consequently the risk free rate.
Retail has been the main long term underperformer as customer preferences have changed in terms of accessibility and type of product. More recently offices have suffered in terms of performance, both from return to work practices as well as regulation. But perhaps the biggest feature of this chart is the stability of healthcare real estate year on year; it simply not as volatile as the other real estate providing far more predictable total returns.
Over the long term, healthcare real estate continues to produce strong solid total returns over ten years. ”
Source: MSCI Real Assets
Placing Healthcare Real Estate in the real assets universe
Historically, changes in allocations to real estate mainly meant a variation in risk appetite along the main sectors available for investment. For example an increased allocation to offices may have meant moving in to office development or specific types of retail beyond malls and shops. As newer sectors have evolved such as logistics, hotels and indeed healthcare these have offered diversification opportunities with often very different risk and performance profiles from traditional sectors and are now well understood.
More recently, the real asset investment universe has expanded still further with investors now having access to a far wider universe of risk and return opportunities across both debt and equity. Infrastructure has been a component of many portfolios for many years and more recently debt/credit funds operating across infrastructure and real estate have also become an investment option providing access to a more nuanced risk return profile.
5
Source: MSCI Real Assets
Figure 6
Multi-asset class performance
Healthcare real estate no longer just sits alongside real estate offering real estate diversification, but also infrastructure and credit. The chart below places the performance of healthcare real estate alongside performance of the equivalent indexes for real estate debt funds, infrastructure as well as public market performance metrics. Over the long term, healthcare real estate continues to produce strong solid total returns over ten years placing between infrastructure and the wider equities market.
Note: Results shown here for direct real estate and fund-level real estate are based on separate quarterly samples with specific sources indicated below.
Sources: EQUITIES: MSCI, Mid & Large Cap, Index, Total Return, GBP BONDS/FIXED INCOME: JP Morgan. GBI Broad, Traded, Index, 7-10 Year, Total Return, GBP; PROPERTY EQUITIES: MSCI, GB/Real Estate, Gross Total Return, GBP, series#115565; DIRECT REAL ESTATE (ASSET LEVEL): MSCI, MSCI UK Quarterly Property Index (and monthly index); NET FUND LEVEL REAL ESTATE: MSCI, MSCI UK Quarterly Property Fund Index. MSCI European Fund Level Debt Index – data to Q1 2025 – Euro Variable Currency. MSCI Global Infrastructure Fund Level Index_Research Release – data to Q2 2025 – USD Fixed Currency.
Assessing the key asset classes
Thomas Atherton, Strategy & Market Intelligence Manager, Savills OCM
CARE HOMES
Care Homes remain a compelling asset class, underpinned by Europe’s ageing population and a stark supply-demand imbalance.
While the sector has faced headwinds over the last few years, including a more challenging financing environment and increasing operational costs, investment volumes began to rebound in late 2024 and are set to recover further in H2 2025 and beyond, as rates ease and investor confidence returns.
This commentary frames real estate in its global context, looks at various routes to market and their relative advantages, analyses investment volumes and trends, highlights key transactions, and discusses challenges and opportunities across seven of Europe’s core Care Home markets: the United Kingdom, Germany, France, Spain, the Netherlands, Belgium and Italy.
It assesses which markets have attracted the most investor interest in recent years, as well as evaluating those that now appear best positioned for future growth.
International Expansion Up to 2022 Cheaper Debt and Attractive Risk-Adjusted Returns
In the decade leading to 2022, strong macroeconomic performance and access to cheap capital, combined with structural demand for Care Homes (ageing populations and growing supply-demand imbalances) led to the creation of large providers that were often active in multiple geographies.
Real estate investors such as Aedifica, Cofinimmo, and Healthcare Activos, alongside Care Home operators like Clariane (formerly Korian) and Emeis (formerly Orpea), significantly expanded their global footprint, in Europe and internationally.
This expansionary phase was propelled by strong Cross-border capital flows into European Care Homes, as well as the emergence of large OpCos funding their growth with sale and leasebacks.
In larger markets, national REIT platforms such as Target, Impact (now CareREIT) and Nrep, and funds such as Octopus and Civitas, also built significant portfolios with key operator relationships.
Emeis (Dagelijks Leven) 2,000 1.5% France PLC
1,672 1.3% France PLC
(Bloezem) 1,124 0.9% France PLC De Herbergier 880 0.7% Netherlands Private De Leyhoeve 557 0.4%
Source: EAC, Savills Research
Despite COVID-19, which led to reductions in profitability, rising costs, and staffing pressures, real estate in Europe’s core Care Home markets saw decade-high capital inflows between 2020 and 2022, reaching over €5 billion in 2021, compared to a pre pandemic average of around €2.1 billion (2016–2019).
This surge was underpinned by even cheaper debt than in the years prior and an active sale-and-leaseback market, with a perception that Care Homes offered attractive risk-adjusted returns relative to other real estate asset classes.
Figure 1 Top 5 Operators in Each European Market
Geopolitical Risk, Inflation and Higher Interest Rates
As occupancy was recovering and COVID driven operational pressures were easing, a new wave of global disruption emerged from 2022 onwards, with war breaking out in Ukraine, the highest inflation and interest rates in over a decade, and growing geopolitical uncertainty as governments prepared for the possibility of conflict, both military and economic.
Central banks deployed aggressive rate hikes from the second half of 2022 through 2023 and 2024.
Investment activity slowed sharply, with capital becoming harder to access and buyers retreating as investors focused on divestments, often at discounts, in order to deleverage.
Annual investment in the core European Care Home markets addressed in this report declined for three consecutive years, dropping from €5 billion in 2021 to just €2.2 billion by 2024.
Reduced Real Estate Investment Appetite
Whilst Healthcare real estate continued to offer strong returns, the illiquidity of the underlying assets, higher cost of leverage and higher bond yields, compared to vendor expectations on PropCo yields, made real estate less attractive on a risk-adjusted basis, leading institutional investors to reallocate capital to lower risk government and corporate bonds, where deeper secondarymarket liquidity and faster settlement cycles make trading and exit more efficient.
Another group of investors that historically have been very active in Healthcare, Real Estate Investment Trusts (REITs): tax efficient vehicles that own and manage incomegenerating property while distributing most of their earnings to shareholders, also reduced their capital deployment.
UK and European REITs continued to see strong rent collection, but the public markets did not draw a distinction between real estate asset classes (such as Office, Retail and Healthcare) and many traded at significant discounts to Net Asset Value (NAV), meaning the company market capitalisation was lower than the value of its underlying assets, limiting their ability to raise fresh equity to deploy.
Being unable to raise equity meant debt was also more expensive, as the risk to lenders increased, leading to a marked slowdown in transaction activity across the sector, as REITs have historically been responsible for a large proportion of capital invested.
Despite recovering Care Home occupancy across Europe, several operators encountered financial distress due to excessive debt, rising interest rates, and increasing operational costs. Many became overleveraged after aggressive expansion during the growth phase up to 2022.
Some prioritised speed of growth and volume of assets over quality, leaving them exposed when performance fell short of expectations. The culmination of these factors led to a wave of insolvencies across the sector.
Return to Growth 2024 Onwards
Sentiment and Capital Returns Care Home investment in H1 2024 was subdued, down 39% from an already low point in 2023, but it rebounded in H2 2024, with €1.50bn deployed - 22% above the same period in the previous year. Full-year volumes reached €2.24bn, only 8% down on 2023.
Momentum from H2 2024 has carried into 2025, supported by falling interest rates and a narrowing gap in buyer and seller price expectations, which had been distorted during the earlier period of international expansion. By May 2025, cumulative investment volumes
for 2025 have reached €1.76 billion, exceeding the €1.61 billion recorded over the same period in 2021, which saw the highest full year investment volumes in over a decade.
Improving operator performance and a more favourable macroeconomic environment to last year has bolstered Care Home market sentiment. In Savills European OpRE Investor Survey 2025, the proportion of respondents looking to invest in Care Homes stood at 35%, up from just 16% in 2024.
Annualising investment volumes up to May 2025 this year makes this the second highest annual investment volume in over a decade. The rebound in total volumes during H2 2024 and through 2025 was driven by the strong performance of the UK, Spanish, German and Dutch markets, with Cross-border capital continuing to be particularly active.
US REITs Leverage WholeCo Model in the UK
In 2024, the UK saw a surge in investment, with US capital playing a prominent role. One strategic approach was the use of management contracts and RIDEA structures (for US REITs), which offer greater flexibility and allow real estate investors to participate in the operational upside of the asset, enhancing return potential.
US REITs have actively used this model when acquiring UK assets and have benefited from significant weekly fee uplifts. However, REITs are subject to regulatory differences across jurisdictions. UK REITs face tighter constraints, as at least 75% of their income must come from property rental, limiting their ability to share in operational profits and making WholeCo participation more difficult.
With bid-ask spreads too wide on PropCo transactions, this gave the American REITs an advantage in the market, especially when WholeCo’s were the main deals occurring in 2024.
In another strategic approach, US REIT Omega Healthcare Investors has targeted Tier 1 and Tier 2 stock, while other investors have focused on Prime and Super Prime. As a result, Omega has faced less competition and has secured assets at attractive pricing. As of May 2025, US Healthcare REITs were trading at a 20.6% premium to NAV, positioning them to acquire UK Care Home assets at discounted valuations and capitalise on transatlantic arbitrage as their UK-listed peers remain constrained by persistent NAV discounts and difficulties raising capital.
Figure 3
Real Estatae Care Home Ownership Models
Where is the Capital Coming From?
Both domestic and cross-border capital remains active across Europe’s Care Home markets, although investor focus varies by country.
France, Spain, Belgium, and the Netherlands all show a strong domestic focus: in each, two of the top three most active investors are domestic, with only one international player represented.
This shows a balance of interest, but with a weighting towards nationally-based investors.
By contrast, in Italy all of the most active investors are France-based, underscoring the limited role of domestic capital in that market. The UK is another geography that is seeing cross-border capital inflows, but from further afield, particularly US investors.
Cross-border investment in European Care Homes has been a consistent trend for over a decade, with the sector offering investors access to a broader range of assets while reducing reliance on any single social security system or care model.
Across Europe’s core Care Home markets, cross-border capital accounted for almost half (48%) of total investment in 2024, the highest proportion since 2020 (52%) and markedly higher than the 37% in 2023.
In 2024, notable deals included UK-based Octopus entering the Spanish market, Spanish investor Healthcare Activos expanding into Germany and deepening its presence in Belgium, and Civitas making its first investment in Germany.
As we reach the halfway point of 2025, cross-border capital is driving investment volumes, accounting for the vast majority (85%) of investment in the year up to May.
The strategic value to investors of geographic diversification has been underscored by recent challenges in the French and German markets.
Cross-border investment in European Care Homes has been a consistent trend for over a decade, with the sector offering investors access to a broader range of assets while reducing reliance on any single social security system or care model.”
PRIMARY CARE
Primary Healthcare facilities, such as General Practitioner (GP) surgeries, offer investors long-term, government-backed rental income. The UK Government is prioritising care in community settings, with plans to develop Neighbourhood Health Centres and a strategic focus on prevention over treatment.
After over a decade of limited investment, Primary Care has returned to the forefront of national policy, as highlighted by the NHS’s Fit for the Future: 10-Year Health Plan for England released this month, a national strategy aimed at driving long term system reform, with Primary Care as a central focus.
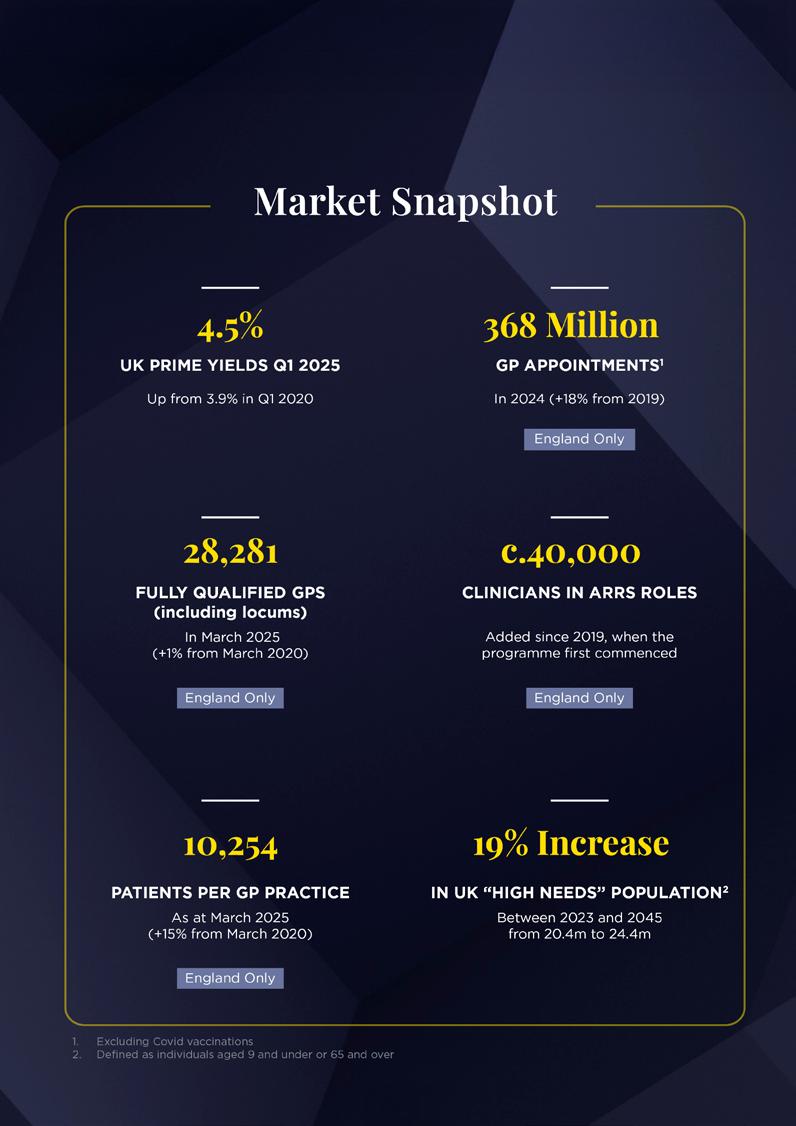
The NHS is still grappling with a major backlog of appointments following the disruption caused by Covid-19. While demand has risen, the number of fully qualified GPs has not kept pace with that demand, or with population growth.
There has, however, been the introduction of approximately 40,000 non-GP clinicians, funded through the Additional Roles Reimbursement Scheme (ARRS) by Primary Care Networks (PCNs), to support the workforce and provide more integrated, multidisciplinary care within general practice.
This includes pharmacists, physiotherapists, paramedics, and social prescribing link workers. While the introduction of these roles has helped meet rising demand, the expansion of staff and services in GP surgeries, set to accelerate through the rollout of Neighbourhood Health Centres under the NHS’s 10-Year Plan, has placed increasing pressure on an estate that is already undersized and outdated.
As the system moves towards more integrated, community-based provision, the UK’s Primary Care infrastructure will require a fundamental overhaul, with more modern, purpose-built facilities needed to support current workforce models and deliver future service ambitions.
Prime yields in the sector have been stable at 4.5%, supported by strong fundamentals and increasing investor demand, and also now driven by government backing and a renewed policy emphasis on Primary Care services across the UK
Investment is on The Road to Recovery
The past few years have been challenging for UK real estate markets. Rising interest rates have impacted investment activity across all sectors, and Primary Care has been no exception.
Stability in Primary Care
However, as the economic backdrop improves, government backing for Primary Care investment strengthens, and falling interest rates make debt more accessible, market activity is returning, and we are seeing new groups of investors enter the sector following Covid.
One of the key drivers of increased activity is the stabilisation in yields since the market shift in late 2022, with rental growth helping to offset outward movement in capital values.
The latest valuations from Primary Health Properties (PHP) and Assura provide further evidence of resilience within the sector, giving investors confidence that now is an attractive time to enter the market or expand their existing holdings, with a strong likelihood of tighter yields over the medium term.
A flight to quality and secure, long-term income property investments, which Primary Care offers, was a trend before the interest rate spike. Given the continued uncertainty in the macroeconomic environment, this trend is expected to intensify, particularly as interest rates continue to reduce.
Alongside the likes of PHP, Assura and BlackRock, who are long term investors in the market, in recent years a growing number of non-sector specialist investors have also been showing interest.
In May 2024, Assura and pension scheme USS announced that they had entered into a new £250m joint venture to support investment in essential NHS infrastructure, including GP surgeries. More recently, in May 2025, KKR and Stonepeak made an offer to acquire Assura, which was later set aside in favour of a proposed merger with PHP, subject to shareholder approval.
Figure 4
UK Prime Yields
OFFICES (LONDON CITY)
SHOPPING CENTRES HIGH STREET RETAIL
PRIMARY CARE INDUSTRIAL MULTI-LET YIELDS
Strong interest from a broadening investor base, including private equity, pension funds, institutions, REITs, infrastructure funds and private investors, highlights the renewed appeal of UK Primary Care real estate as a resilient and income-secure asset class.
Safe and Secure Government Backed Income
The asset class is particularly attractive to investors given its high degree of income security from the NHS, which provides GPs with rent reimbursement. Recently this appeal has been further strengthened by increased government health spending and a clear policy shift towards preventative care, as outlined in the NHS 10-year Plan. This is expected to drive greater reliance on Primary Care services.
Institutional lenders are seeing some, albeit limited, interest from GPs in acquiring their own real estate, which was uncommon until recently. At the same time, investors report that raising debt for large-scale acquisitions in the sector is becoming significantly easier.
There is a marked difference in the yield profile for assets depending on the remaining lease term in place. Surgeries with short dated leases, which typically include older surgeries, have yields c.75 basis points higher than those for new build investments with 20+ year leases in place.
Assets with five years or less remaining on their leases represent a relatively new segment of the market, with most properties
built between 2000 and 2010. As this market has yet to fully mature, yields remain widely spread. However, variation in yields even within similar lease profiles suggests an emerging divergence between primary and secondary assets.
Leveraging Private Sector Investment
Central to the Government’s 10-Year Plan is the creation of a national Neighbourhood Health Service, underpinned by a programme of GPled Neighbourhood Health Centres. Delivering on this vision will require substantial investment in modernising and expanding the Primary Care estate.
The plan explicitly states that it will explore new capital investment models, including greater use of private sector funding, to help unlock delivery, particularly in underserved areas.
Growing policy support for private investment in Primary Care infrastructure presents a clear opportunity for investors to contribute meaningfully to improved access and outcomes, particularly in communities facing the greatest unmet need for GP services.
Notably, while this represents a long-term strategic shift, the plan comes at a time when the NHS continues to face significant care backlogs, high demand for elective procedures, and sustained pressure on waiting lists, factors that will continue to shape service delivery in the near term.
MEDICAL OFFICE BUILDINGS
The MOB sector in Europe remains a nascent market, with adoption rates varying significantly across countries and still far less established than in the US, where outpatient healthcare real estate is long-standing and deeply institutionalised.
Within Europe, Germany represents the leading market, while the Netherlands is emerging as a key area of growth. By contrast, France and the UK remain structurally constrained by their centrally funded healthcare systems, making the development of a US-style MOB market unlikely in the near term.
These regional disparities largely reflect differences in healthcare delivery models and institutional structures within national health systems. However, in European geographies where healthcare systems make MOBs feasible, a clear shift is underway.
As healthcare provision becomes more decentralised, outpatient services are moving away from main hospital campuses and into community based settings, driving growing demand for modern, purpose-built space.
The MOB sector in Europe remains a nascent market, with adoption rates varying significantly across countries and still far less established than in the US.”
The viability of MOBs is closely tied to the degree of decentralisation within a country’s healthcare system and the balance between public, non-profit, and private providers.
A functioning MOB market relies on the separation of healthcare delivery from property ownership, where independent doctors and outpatient operators lease rather than own their premises.
This model performs best in decentralised, insurance-based systems with a strong base of independent practice, generating diverse tenant demand from clinics, diagnostic centres, and specialists seeking flexible, modern premises.
It has been most successful in Germany and the Netherlands, where insurance based frameworks and a mix of public, non-profit, and private providers enable leasing models to thrive, unlike systems that concentrate care delivery within state owned hospitals, where investor-owned MOBs are less viable.
Germany leads in both scale and maturity, supported by its mixed public–private system, a large number of self-employed physicians who prefer to rent rather than own their premises, and healthcare policies that continue to move treatments toward outpatient environments.
The Netherlands, while smaller in absolute scale, is demonstrating strong growth momentum underpinned by structural reform, insurer incentives, and an expanding base of independent treatment centres (ZBCs) and integrated health hubs.
Together, these dynamics are fostering the gradual development of the MOB market across Europe.
France is emerging as a potential future MOB market, supported by growing investment in community-based clinics and specialist outpatient centres.
However, the French healthcare system remains dominated by private clinics that are typically leased or owned by a single operator or healthcare provider, alongside publicly funded health centres, leaving few independent doctors or clinics that would lease space in an MOB format.
Similarly, the UK does not have an MOB market, reflecting the NHS’s centralised model and limited reliance on private sector outpatient services, aside from a few emerging specialties such as ophthalmology.
In the UK, independent doctors are typically contracted by private providers or, when working independently, will lease space
within private hospitals or NHS Private Patient Units (PPUs).
Key MOB Markets in Europe: Policy-Driven Demand
Germany and the Netherlands Germany’s outpatient sector has evolved from a fragmented base of small practices into a more consolidated, multi-disciplinary system. Since the 2004 introduction of Medizinische Versorgungszentren (MVZs), groups of doctors have increasingly co located within shared facilities, driving demand for larger, purposebuilt medical facilities.
The MVZ was established through the Health Modernisation Act to modernise and integrate outpatient healthcare delivery by enabling doctors from different specialties to work together within a single, jointly managed organisation.
MVZs provide a wide range of outpatient services, from general medicine and diagnostics to specialist consultations, all under one roof. Over the last two decades this has created growing demand for larger, purpose-built or refurbished premises, such as modern MOBs located near hospitals or within communities.
Germany is now undergoing another major structural transformation in healthcare delivery, shaped by two closely connected federal initiatives:
Ambulantisierung and the Krankenhausreform. Both reforms share the goal of rebalancing the healthcare system by transferring suitable medical procedures from inpatient to outpatient settings and ensuring hospitals focus on more complex, specialised treatments. Ambulantisierung refers to the ongoing shift of diagnostic, surgical, and rehabilitative procedures, traditionally performed in hospitals, into outpatient environments that do not require overnight stays.
MVZs provide a wide range of outpatient services, from general medicine and diagnostics to specialist consultations, all under one roof. Over the last two decades this has created growing demand for larger, purpose-built or refurbished premises.”
Figure 6 Germany and the Netherlands MOB
Volumes, €m, 2015 – 2025 (YTD October)
As part of this, a new reform Ambulantisierungsgesetz is expected to take effect in 2025, which expands the range of treatments eligible for outpatient reimbursement, incentivising hospitals to deliver more procedures outside inpatient settings.
Krankenhausreform, formally adopted in November 2024 and effective from 1 January 2025, restructured hospital provision by concentrating complex care in specialist centres, downsizing general hospitals, and shifting lower-acuity care into community-based settings.
The reform is expected to result in the closure of around 20% of hospitals across Germany.
As patient treatment increasingly moves out of hospitals and into outpatient environments, this reform is expected to generate sustained demand for modern MOBs and integrated health centres that can accommodate multispecialty outpatient provision.
The Netherlands represents an emerging market for MOBs in Europe, underpinned by a decentralised outpatient healthcare system and strong policy support for integrated,
community-based care. A key policy driver is the Integraal Zorgakkoord (IZA), introduced in 2022, which aims to shift appropriate hospital treatments into outpatient and independent treatment centres (ZBCs –Zelfstandige Behandelcentra) as part of a nationwide integrated-care strategy.
Dutch health insurers play a pivotal role, actively incentivising outpatient treatment to control costs and improve efficiency.
This is reinforcing the expansion of specialised clinics in areas such as ophthalmology, orthopaedics, dermatology, and diagnostics, fuelling demand for modern, flexible, and community-based medical real estate.
MOB Investment
Investor Demand Remains High but Market is Limited in Availability of High-Quality Purpose-Built Assets
Attracted by a favourable supply–demand imbalance, strong underlying growth drivers, and the emergence of modern, high-quality assets, the European MOB sector has undergone increasing institutionalisation over the past decade, supported by a growing tenant base and an influx of institutional capital.
Following the Covid period, when interest rates were at decade lows and demand for outpatient care outside hospitals accelerated sharply, investment volumes in the MOB sector reached record levels, approaching €1 billion in 2021 across Germany and the Netherlands combined.
As institutional participation in the asset class increased, a growing number of sizeable portfolios were created and brought to market. However, while portfolio activity has expanded, opportunities of scale remain limited, preventing the sector from sustaining consistent year-on-year transaction volumes.
Activity remained elevated through 2022 before declining in 2023 and 2024, largely due to rising interest rates, a higher cost of capital, broader macroeconomic uncertainty, and a shortage of high-quality portfolios being brought to market.
The slowdown in MOB investment activity reflects both the limited availability of institutional-grade portfolios and the sector’s relative immaturity as an emerging asset class in a more challenging macroeconomic environment, which constrained investor confidence and liquidity. As a result, transactional activity declined even as underlying occupational demand remained robust
Recently, the sector has attracted interest from a broad range of investors, including
pension and insurance-backed institutional capital, REITs, private equity firms, and dedicated healthcare infrastructure funds.
HIH Invest, a German institutional real estate investment manager, acquired a health centre and office building in Michendorf, Germany in September 2022. In May 2023, Cofinimmo, a Belgium-listed healthcare REIT, acquired the Baandert Medical Center in Sittard, the Netherlands at a cap rate of 6.0%. The asset was delivered as a turnkey property with a 13-year WAULT.
In June 2024, Swiss Life Asset Managers, a European insurance and pension fund manager, acquired an MOB in Wolfsburg comprising 29 rental units occupied by specialist practices and providers of medical services and products.
Additionally, TSC Real Estate is raising a €200 million fund, announced in September 2025, to invest in German outpatient medical centres, highlighting strong positive sentiment for the German outpatient real estate sector.
European VS US MOB Yields
In the United States, where the sector has long been institutionalised and benefits from an established investment track record, MSCI data indicates that MOB yields compressed steadily in the decade up to 2022, supported by entrenched structural trends in outpatient care delivery, strong fundamentals, and defensive income characteristics.
Over the last 12 months, we have advised on and transacted in excess of €5 billion of Healthcare and Senior Living real estate, in the UK and Europe.
Deals advised on range in size from €1 million to over €1.5 billion, with a broad cross-section of clients that includes institutional investors, private equity, annuity funds, banks and non-bank lenders, developers, operators, charities and NHS Trusts.
SAVILLS PAN-EUROPEAN CAPABILITIES
▪ Transaction Advisory –Disposals & Acquisitions
▪ Deal Structuring
▪ Capital AdvisoryEquity & Debt Financing
▪ Recapitalisations
▪ Valuation
▪ Consultancy
▪ Research
▪ Technical Due Diligence
▪ Planning
▪ Capital Allowances
From early 2023, US and European cap rates have experienced an expansion due to higher interest rates and tighter debt markets, increased risk premiums, and an uncertain macroeconomic outlook, with the US currently trading at c.7% and Europe trading at c.6.5%.
The long-term view shows European markets trending below the US, likely due to the lack of quality stock increasing competition for prime assets, with a convergence seen more recently.
This trend in yields, together with resilient fundamentals, a more active investment market, and a limited but increasing number of institutional-grade portfolios as investors continue to aggregate assets, should support interest from global capital and especially US capital in European MOBs going forward.
In Europe, most MOB transactions involve single assets, as the market currently lacks acquirable, institutional-scale portfolios. These smaller properties typically fall below the investment thresholds of REITs and large institutional buyers and can therefore be acquired at higher initial yields, despite offering comparable fundamentals and risk profiles to larger assets.
As a result, MOBs present an attractive entry point for smaller-scale investors seeking exposure to the healthcare sector, where the lot sizes for larger assets such as hospitals are often beyond reach.
This also offers a compelling opportunity to aggregate portfolios and ultimately exit at more attractive yields to institutional capital once scale is achieved.
MOBs
present an attractive entry point for smaller-scale investors seeking exposure to the healthcare sector, where the lot sizes for larger assets such as hospitals are often beyond reach.”
Meanwhile, consolidation in outpatient and clinic markets is gaining traction across Europe.
Many independent practices are being acquired by larger clinic chains or health service groups, particularly in segments like diagnostics and specialist outpatient care.
This trend enhances the credit quality of tenants, benefiting landlords and improving the institutional appeal of the sector over time.
MOBs represent a complementary investment opportunity for those already investing in clinics and outpatient centres, as these asset types are often sold together in portfolios across both the US and Europe and share similar investment fundamentals and tenant profiles.
Aggregating MOBs and clinics into combined portfolios can provide a route to achieving institutional scale, a strategy that has already been observed in several recent transactions.
Legal Update on Health and Social Care Investment
Candice Blackwood, Partner, Co‑Head Life Sciences & Healthcare ‑ CMS
Cameron McKenna Nabarro Olswang LLP
Investment in care assets has become an increasingly important part of institutional real estate and infrastructure portfolios across Europe. Rising life expectancy, aging demographics, declining capacity for care by families, and pressure on public healthcare systems have all resulted in more investment being needed and available for senior housing, healthcare facilities, nursing and residential care, step-down care, hospice care and home care.
CMS are an international law firm, with 10 offices covering the UK and full services provided in 45 countries worldwide including all of Europe, the Middle East, Asia, India and Africa. We have been advising investors, funders, health and social care providers for more than 30 years on all legal advice needed for significant cross border corporate, real asset and funding transactions. We advise both public and private clients, care entrepreneurs and family doctors through to public limited companies and international global Real Estate Investment Trusts (REITs) on all aspects of the sector including the acquisition and development of care assets, active portfolio management, regulatory, tax, medical malpractice claims, reputational damage, cybersecurity breaches, and capital procurement advice.
This article is focussed on Germany, France, Spain and the UK as the most developed care markets in Europe currently. We also have regard to the US and international investors. Care assets are operational real estate in all jurisdictions due to the need for active management and required regulatory oversight. These requirements might be perceived to introduce additional complexity and risk for some investors. However, care assets offer defensive characteristics for investors in turbulent markets, and support longterm demographic demand needs, while providing inflation-linked income stability.
Germany
Germany has the largest care market need by population. It is underpinned by a mandatory long-term care insurance system (Pflegeversicherung). This statutory framework Introduced in the 1990s, provides a stable and predictable funding base for care services, reducing demand risk compared with more market-driven systems.
Care assets in Germany are typically leased on long terms with conservative structures, often including inflation indexation. There are multiple care operators. Regulation is more complex than elsewhere as it is shared between federal and state (Länder) authorities. Regulations have also changed in recent years to require improved and updated facilities and service offerings and there are complex licence, staffing, and building requirements.
These increased compliance costs and timelines have challenged viability for some operators. They also create high barriers to entry that support long-term asset values and limit oversupply. This means that German care assets are being attractively priced for both domestic and international investors seeking stable, income-focused exposure. However, successful investment in Germany requires a deep understanding of regional regulatory requirements and close engagement with operators.
France
France’s care markets benefit from a highly structured regulatory and funding environment. Long-term care and healthcare facilities are regulated by regional health agencies -Agences Régionales de Santé (ARS), with quality standards monitored by the Haute Autorité de Santé (HAS). These frameworks provide regulatory clarity for investors, with consistent pricing and limited operational autonomy. Despite these
German care assets are being attractively priced for both domestic and international investors seeking stable, income-focused exposure. However, successful investment in Germany requires a deep understanding of regional regulatory requirements and close engagement with operators.”
regulations, France had some well publicised care issues in the early 2020s which affected investment and trading and from which the market is now recovering.
Investment activity is supported by the SIIC regime (the French equivalent of a REIT), which has enabled consolidation of healthcare real estate portfolios at scale. Lease structures are often closely aligned with public funding mechanisms and operator reimbursement models which reinforce income stability.
France is viewed as a lower-risk care investment market due to strong state involvement in healthcare provision. However, the highly structured regulatory and funding regimes require careful asset selection with a view to long-term investments.
Spain
Spain is now a rapidly developing market for health and social care asset investment. Historically reliant on family-based care and care provision by the Catholic church, Spain now faces increasing demand for institutional care and senior living driven by demographic ageing, urbanisation, international retirees and acceptance by the Spanish.
Regulatory responsibility for care services is decentralised to autonomous communities, resulting in fragmented standards, approval processes, and inspection regimes. This increases investor requirements for extensive due diligence and regulatory advice on the increased operational complexity. In response, lease structures in Spain increasingly include management agreements and hybrid rent models to balance risk between landlords and operators.
There is a historic structural undersupply of modern care facilities, particularly in major urban regions. Spain therefore presents higher growth potential than more mature markets, with successful investment needing careful due diligence and navigation of regional regulations and operators.
United Kingdom
The United Kingdom has followed the United States to become one of the most established markets for care asset investment, with significant participation from institutional
Poor regulatory performance can lead to occupancy decline, enforcement action, or closure, with consequential financial risk for investors and operators.”
investors, infrastructure funds, private equity and listed vehicles. In the UK, care homes, hospitals, specialist healthcare facilities, healthcare hubs for testing and vaccinations, and supported living developments are commonly structured under long leases ranging from 25 to 35 years, often with annual rent increases linked to consumer or retail price indices. These long-income structures have positioned care assets alongside other infrastructure-like investments within institutional portfolios.
The US has Healthcare REITs dominating the sector invested in senior housing, skilled nursing facilities, medical offices, and hospitals. Investors can select varying levels of operational exposure through structures such as triple-net leases or RIDEA management arrangements.
In the UK, regulatory oversight is provided by the Care Quality Commission (CQC) in England and Wales and the Care Inspectorate in Scotland. Poor regulatory performance can lead to occupancy decline, enforcement action, or closure, with consequential financial risk for investors and operators. In the US regulation is multi-layered overseen by the Centres for Medicare & Medicaid Services, and state level licences and enforcement. Despite regulatory and reimbursement risk, strong demographic demand, capital market depth, and operational innovation continue to attract investment into U.S. care.
In both jurisdictions operator business strength, structure, and regulatory records are important diligence items for transactions. Inspection ratings can materially affect operator viability and asset value.
In our experience, investors and operators in the UK liaise closely to ensure successful business operation, excellent patient care (digital wherever possible), and targeted capital expenditure and investment. The UK has also experienced strong growth in healthcare-focused REITs and social infrastructure funds. These vehicles provide
scale, liquidity, and access to capital markets while benefiting from demographic demand and policy support for private sector involvement in care delivery. Businesses are constantly evolving driven by funding and staffing requirements. Traditional residential care has moved to more intense nursing and dementia care, senior living communities are thriving, and there are more small supported living arrangements and specialist accommodation in local communities. These need to develop in parallel with the needed infrastructure support – affordable housing for care workers, good transport links, healthcare hubs for drop in attendance for vaccines, blood tests and diagnostics, eye and ear services,
Investment performance is closely linked to operator quality, regulatory compliance, and public funding stability. Care investments can also assist with institutional investors’ environmental, social and governance targets. Even the National Health Service (as one of the largest public property owners and occupiers in the UK) has ambitious Net Zero targets scheduled for delivery by the 2030s. Private capital is needed to fund, own, manage and improve care-related real estate which should result in improvements for public health and better social outcomes.
We are optimistic about the UK’s economic prospects, given the Government’s dedication to the health, social care, and living sectors, along with falling interest rates and reasonable transaction pricing. The strong influx of both global and national capital occurring from 2025 is likely to continue across these sectors, which offer sustainable, long-term value investment.
Comparative Analysis
Conclusion
Across all jurisdictions, care asset investment is shaped by demographic demand, regulatory oversight, and evolving investment structures. Care assets occupy a unique position between social policy and capital markets. While offering long-term income stability and social impact, they require sophisticated structuring, active management, and deep regulatory and regional understanding.
Care assets are a core component of social infrastructure - spaces to support shared civic life, ranging from transport, schools and healthcare to parks, libraries and community halls. These assets deliver essential services and are often supported—directly or indirectly—by public funding mechanisms. Governments increasingly rely on private capital to address funding gaps, modernise facilities, and expand capacity.
Currently the UK reflects capital markets innovation and REIT activity (particularly from the US), Germany and France offer regulatory stability and predictable funding models, while Spain is showing higher growth potential alongside greater operational complexity. Jurisdiction-specific factors and regulatory engagement and local legal advice remain important to successful investment outcomes.
We look forward to discussing these topics further at the first European Healthcare Investment Association Real Assets Conference.
Supporting clients across primary, acute, community, residential and social care including mental health, special education and children’s services. Our award winning Healthcare team provides innovative advice on transactions, claims, regulation, contracts and JVs & outsourcings between the public sector and the private sector.
So irrespective of where your real estate assets are, we can deploy specialist teams from across Europe’s largest Real Estate team to advise you immediately.
Candice Blackwood Partner, Co-Head of Life Sciences & Healthcare UK
Europe’s Healthcare Investment:
Why Ageing, Money and Technology Are Rewriting the Rules
Derek Breingan, Head of Health and Social Care Sector & Duncan Leitch, Senior Director ‑ Virgin Money
Europe’s health and social care sector is being pulled in three directions at once: people are living longer, governments are counting the pennies, and technology is changing how care, and business, is delivered. Put those together and you’ve got a most fascinating and progressive investment story.
The pressure point is elderly care and specialist services like rehab, acute care and mental health. For investors, and lenders like Virgin Money, that means steady income if you pick the right operators and keep an close eye on regulation, staffing and costs.
The Demographic Tsunami
There is no need to forecast because our ageing population is here. The elderly care market is already worth around $350 billion and growing at nearly 7% a year. Western Europe still dominates, but Central and Eastern Europe is catching up fast after decades of underinvestment. And tech such as telecare and remote monitoring is making home-based care more viable, which governments will love because it’s cheaper than institutional care.
The European Central Bank even says ageing is reshaping savings and investment patterns. This translates to more money flowing into long-term social infrastructure, and a premium on productivity tools to keep costs under control.
Investment: Back From the Brink
After the pandemic boom in 2021, the sector hit a wall when interest rates spiked and inflation and costs soared. However the rebound is here: €1.76 billion went into care homes in the first five months of 2025, outpacing even the 2021 peak. Cross-border investors are leading the charge, drawn by pricing power in the UK and supply shortages in Spain. Germany, despite recent operator distress, is back in play thanks to an insurance-backed funding model. In addition, Welltower invested £5.2 billion in UK care homes in 2025.5
Prime yields have reset to 5–5.75%, which is good news for lenders—more security cushion, less reliance on aspirational growth assumptions albeit with interest rates still comparatively high, Rent to Interest Cover is still thinner than it has been historically.
Private Equity: Slowing Down, Smarten Up
Private equity continues to love healthcare because it’s increasingly less volatile than most sectors and offers room for operational improvement. Fast roll-ups and exits are over however with borrowing costs higher, PE firms are focusing on integration, workforce investment and tech upgrades. For lenders, we believe that means more stable ‘sticky’ transactions and better-quality, longercommitted counterparties..
Private
equity continues to love healthcare because it’s increasingly less volatile than most sectors and offers room for operational improvement.”
The UK: Still the Magnet
The UK remains a principal target for international capital. This is due to pricing power, scale and investment structures that can blend property and operations. Fee increases in supply-constrained areas are continue to outpace inflation as long as operators deliver strong clinical outcomes and family satisfaction. Lender underwriting typically relies on strong, targeted diligence: CQC ratings, staffing ratios, occupancy and, in the case of new developments, building specs and local sociodemographics matter.
Spain, Germany, CEE: Opportunity With Caveats
Spain has a glaring shortage of care beds, making development attractive as long as you understand the regional nuances. Germany is stabilising after a rough patch, and CEE offers long-duration, inflation-linked assets but where political risk and regulatory maturity are still hurdles to negotiate.
Policy Tailwinds—and Watchdogs
Brussels now treats long-term care as a social priority, pushing investment in community care and digital health. That should mean more predictable reimbursement and better data integrity over time. But beware the “financialisation” backlash from general public: rapid private expansion without enough properly trained staff or insufficient governance can lead to shortcomings and scrutiny such as those seen in France in recent years. Lenders and investors then take the hit when confidence and occupancy collapses.
In terms of sustainability regulation, Jacob Hurtley, ESG Director at Elevation adds “investors and asset managers are keeping a close eye on the proposed amendments to the EU Sustainable Financial Disclosure Requirements. Following a draft proposal at the end of 2025, attention will swiftly turn to how to implement the proposed reporting requirements, as well as those for regulations being introduced or updated in other jurisdictions.
The Outpatient Shift and Digital Push
Across Europe, outpatient care is booming with day surgery, home dialysis, post operative rehab and step down care. It’s cheaper, faster and increasingly what patients want. Operational consistency is key however and lenders will seek satisfaction that outcomes are repeatable and contracts solid and sustainable.
Digitalisation isn’t a buzzword anymore because telecare, remote monitoring and AI triage are productivity tools. Give credit for proven tech, not speculative apps in infancy.
What Lenders Will Demand
Cash flow resilience: CPI-linked rent contracts, stress-tested for occupancy and wage inflation => consequent impact on earnings / rent cover
Asset standards: Dementia-friendly design, infection control, energy efficiency.
• Local expertise: Spain’s bed moratoria, Germany’s Länder rules, CEE’s political risk.
• Conservative leverage: Senior loans returned 12.5% in 2023, expected 8% in 2024—so lenders will increasingly not chase yield at the expense of discipline / safe harbour.
The UK remains a principal target for international capital. This is due to pricing power, scale and investment structures that can blend property and operations.
The Big Picture
Europe needs more elderly and specialist care capacity, delivered flexibly and built on the latest technologies and designs. The UK will stay dominant; Spain will attract development capital; Germany will grow steadily; CEE will open up slowly and selectively as the regulatory framework evolves. For lenders, the challenge is seeing beyond demographics into execution and business detail: staffing, tech readiness, governance, energy performance etc.
Jacob Hurtley, ESG Director at Elevation goes further adding, “we are seeing attention turning increasingly towards net zero targets, whether they are achievable and the route to getting there. Investors need to ensure that they have a clear and actionable plan to deliver a net zero portfolio in a given timeframe, working in partnership with operators to ensure capital is available to provide a meaningful shift in trajectory.
”The best lends will be those where money aligns with the ethics of care and dignity— buildings that maxmise and enhance wellbeing, operators that invest in people (both skills development and retention), and lenders such as Virgin Money that embed these standards in covenants. Get that right, and healthcare remains one of Europe’s most investable sectors for years to come and one which we are committed to supporting.
Footnotes
1 European elderly care market size ~USD 352.8bn (2024) with ~6.8% CAGR forecast through 2033. Source: Market research reports (2024–2025).
2 Savills European Care Home Investment Report, July 2025: €1.76bn invested Jan–May 2025, ahead of 2021 levels.
3 Cushman & Wakefield European Nursing Homes MarketBeat (2024): Prime yields stabilized at 5.0–5.75%.
4 Invesco European Credit Outlook (Jan 2024): European leveraged loans returned ~12.5% in 2023; forecast ~8% for 2024.
5 Welltower UK Care Home Investment (2025): £5.2bn committed to UK care homes. [Link](https://welltower.com/newsroom)
Getting down to business
When it comes to health and social care, we mean business – thanks to specialist products and dedicated support from our team of experienced Relationship Managers.
Here are some of the sectors we work with:
• Aged, specialist and childcare facilities
• Dentists and dental practices
• Hospitals and medical centres
For more info call:
Derek Breingan
Head of Health and Social Care
07818 454674
• Real estate and development finance
• Private equity and investment
• Doctors and medical practices
What healthcare assets are fundamental infrastructure
Ali Bahram, Associate Partner ‑ Mansfield Advisors
Why your next investor may have more experience in bridges and airports than patients
Infrastructure funds have significant capital to deploy, but a dwindling supply of traditional assets available to target. We explore what healthcare targets, including long-term care, is suitable for ‘infra-like’ investment in the current environment of a pandemic turning endemic, a major war in Eastern Europe and the return of the inflation bogeyman. The pandemic has thrust healthcare into the spotlight, and highlighted how robust and resilient the sector can be when growth in sectors like retail or travel faltered or there was suddenly no income at all.
Infrastructure investment has normally comprised two segments: economic and social. ‘Economic’ contains the core you might visualise as traditional infrastructure: transport (roads, bridges, ports and airports), energy, utilities, telecommunication and more recently, digital and cloud services. These fundamental assets are the foundation of a strong economy. These are essential services, with low risk and no real alternatives that offer strong, predictable cash flows into the longterm future. Pension funds are the typical investor example, where liabilities extend out decades into the future.
Core investments typically have effectively monopolies as they fully meet the need of the area and there’s no need for a further toll road or a power station. It would not make economic sense to build a competing asset, and there would not be backing from authorities to do so.
However, too much capital chasing these safe investments has sent prices up and encouraged fund managers to look to alternatives for their core returns, joining that smaller percentage already set-aside for higher risk/return assets.
Infrastructure investments in
Hospitals were first, then specialist care which demonstrated its predictability through the Covid pandemic
Infra-like investments
The social segment comprises services and facilities that contribute to a good quality of life, including healthcare but also housing, education, culture and recreation. There is an estimated social infrastructure funding gap in Europe of between €100bn and €150bn annually(1)(2)
Recently acute hospitals have been the busiest sector, see Exhibit 1, with specialist care seeing a number of deals. Infrastructure investors have also started to look at children’s services (special schools often with a residential element) and elderly care homes, with their property portfolios mitigating against execution risk and market growth. Mental health hospitals would also be there, but provider pricing power has been less predictable than those segments. Otherwise investors seek to own and manage the capital equipment needed in adjacent sectors such as clinical laboratories, mobile operating theatres or diagnostic imaging MRI or CT suites.
Traditional healthcare infrastructure investments would also have been in assets such as large hospitals, as part of publicprivate partnerships or what the UK called private finance initiatives. Once developed, these assets are then rented to national
Given the global uncertainty and rising inflation, healthcare is a safe option seen as an inflation hedge and has the added benefit of diversifying infrastructure funds’ portfolios.”
operators such as the NHS. This funding method has become less popular in Europe, and represents smaller investment sizes compared to most economic infrastructure investments. The most well-known example were the private finance initiatives from the nineties into the noughties, used in the UK for £13bn in new hospitals(3)
The rationale was that construction companies would build for a set price (and be accountable to their shareholders for delivering the asset on budget and in-time) and then would lease the building to the state for 30 years. Cynics argued that the state (or the UK Government in power) avoided the debt on the balance sheet but had to pay private sector interest rates for 30 years, and therefore far more in total than if construction had been funded directly by the state. The proponents would argue that without the risk being held by the construction companies, and if they were able to charge cost-plus, the original cost estimate would have always substantially exceeded and the net present value of the cost equal or greater to the taxpayer. From academic research, we can see that investors made an attractive return on capital, which we define as greater than the investors’ cost-ofcapital as calculated by those same academics. Outside some poorly negotiated early projects, we surmise the PFI hospital building program was a reasonable deal for taxpayers along with being a good opportunity for investors. Though to be sure we would need more insight into the counter-factual world where PFI had not existed, based on international or historical examples. This is only theoretical since there isn’t any apparent interest in such projects from the current UK Government. It doesn’t help that modern accounting standards (IFRS 16 to be precise) mandate that long leases be capitalised, though of course this isn’t the only factor.
Infra-like, also known as infra-adjacent or core+ investments, have a higher risk profile than traditional infrastructure investments. They must still be deemed ‘essential’, however the definition has stretched to include the operating businesses along with the physical environment and its rent.
Healthcare as infra-like Health and social (long term) care have a good story to tell the investment committee, since we are not getting any younger and until very recently at least, we were living longer with ever-growing entitlements to healthcare. Demand for healthcare is inelastic; treatments will be required regardless of economic outlook and developed countries prioritise healthcare spending.
Other sectors like care homes and retirement villages are property backed. Be warned that much UK elderly care stock is very dated and may not be suitable for a long investment period of ~20-30 years.
However there are plenty of high quality, future-proof properties, and these will remain so if maintained. Elderly care homes’ local authority and NHS payors do not default.
One Octopus Group healthcare infrastructure survey found that 60% of global healthcare infrastructure investors are focused primarily on the UK (n=100)(4)
Traditional infrastructure investments provide a rate of return between 8-15%.
Infra-like investments possess an increased risk-profile, and therefore investors demand an increased reward. Healthcare assets can achieve much higher rates of return in the realm of 20%, as targeted by private equity, however the long term goals differ.
The yields required by PE are 20%+ over a shorter investment period. The priorities of PE are to maximise the exit multiple over a 3-5 year investment period, and as such invest profits into growing businesses rapidly.
Infrastructure investments have a longer term outlook of ~10 years, but have a focus on achieving strong cash yields over that period to receive dividends payments. There is a focus on value creation over the long-term, often driven organically, which supports creating processes for maintaining high quality environments to achieve this. This long-term position, with fewer changes of ownership, can be seen as more attractive to management and other business stakeholders.
Healthcare drawbacks
There are of course some drawbacks to healthcare investment for infrastructure investors. Infrastructure investors have typically avoided taking on operational and reputational risk, and healthcare is seen as a sector which can pose both.
Operational risk can be mitigated against by choice of model. Traditionally UK private hospitals tried to offer a model which minimises clinical risk exposure; the hospital provides the physical site, equipment and
SECTOR ESSENTIAL SERVICE GROWTH IN NEED PAYOR PREDICTABILITY PHYSICAL ASSETS LOCAL BARRIERS TO ENTRY STRONG PRECEDENT FOR INFRASTRUCTURE INVESTMENT
ELDERLY CARE
ADULT SPECIALIST CARE
SOCIAL CARE
MENTAL HEALTH HOSPITALS
CHILDREN’S CARE
FOSTERING
ACUTE HOSPITALS
DIAGNOSTIC IMAGING
SPECIALIST CLINICS
DOCTORS’ PRACTICES
PHARMACEUTICAL MANUFACTURERS
CLINICAL LABS
FERTILITY
DENTISTRY
nursing staff, while patients paid surgeons separately for the procedure. This is no longer the case, as providers such as Spire Healthcare spend substantially more on clinical governance than they did a decade ago in order to lessen reliance on the clinical direction of external surgeons. They have found that necessary to maintain their public reputation, inspection ratings and avoid legal risks. Of course, the major PFI deals in state hospitals had no such clinical exposure risk, and neither should propco only investors in UK private hospitals.
In other segments, it can be safer for investors to invest directly in operators and retain direct control over service quality and avoid defensive capex falling between the opco and propco’s responsibilities.
Reputational risk is present through healthcare, but once again being selective in the quality of acquisitions can minimise this exposure. Indeed, many argue that core infrastructure investments offer similarly high levels of reputational risk as faults or failures can affect the public. Unfortunately, bridges and other concrete structures can fail and smart motorways may not that be that smart reputationally.
The rewards offered by the long-term macro trends and value creation opportunities in healthcare should warrant the performance risk.
Exhibit 2: UK sectors prioritisedMental health and elderly care are next closest to being essential and infra-like but no big block pfilike contracts are available.
Future trends
Long-term tail winds for healthcare, and value creation opportunities are sufficient mitigants against the risks posed by the sector. Coupled with limited core opportunities, infrastructure interest in healthcare is continuing to rise. Given the global uncertainty and rising inflation, healthcare is a safe option seen as an inflation hedge and has the added benefit of diversifying infrastructure funds’ portfolios.
Over the past 15 years, digital has emerged as a leading sector for infrastructure investment, who’s to say healthcare can’t follow? That Octopus Group research argued that $200bn could be invested in global healthcare infrastructure over the next five years(4)
Our analysis of factors by segment - see Exhibit 2 - helps explain why investors have prioritised different segments when aspiring for infra-like returns. Looking outside the almost traditional segments of hospitals and specialist care – and now that the Covid catastrophe has passed by – we expect more interest in the absolute highest quality mental health and elderly care assets.
1 Georg Inderst, Inderst Advisory, Social Infrastructure Finance and Institutional Investors, A Global Perspective, March 2020
2 Boosting Investment in Social Infrastructure, European Commission, January 2018
We work for public and private companies and investors, helping them understand the key commercial questions when growing, buying and selling businesses.
Executive Leadership in European Healthcare Real Assets
David Bland, Group Marketing Director ‑ Compass Carter Osborne
Across Europe’s healthcare real assets landscape, abundant capital has transformed into intense competition for quality businesses. Demographic trends such as ageing populations and chronic care demand, continue to underpin long-term investor interest, but in 2025 the decisive differentiator which emerged for value creation was executive leadership quality.
Where once capital deployment and asset selection were the dominant strategic levers, informed infrastructure funds, REITs and private equity sponsors now view senior executive recruitment as integral to investment thesis delivery. At Compass Carter Osborne (CCO), our search mandates across board, finance and commercial, and operational leadership in 2025 consistently revealed this shift as investors prioritised leaders who can navigate portfolio complexity, drive disciplined growth and translate strategic capital into sustainable operational performance.
This article explores the evolving profile of executive talent in healthcare real assets, incorporating data from CCO’s recent delivery into infrastructure fund and REIT-backed portfolio companies, and investor activities across the UK and broader European markets.
European attractiveness to US investors
The healthcare real assets sector in Europe is no longer a local or fragmented market; it is a global magnet for capital. The UK in particular has acted as a focal point for institutional investors seeking exposure to senior housing, care home portfolios and integrated healthcare infrastructure. This trend was epitomised in late 2025 by a series of transactions that underline US investor focus on scale and operational depth.
The last twelve months has seen leading healthcare REITs deploy significant capital into senior living portfolios. Welltower announced approximately $23 billion in transactions during 2025 focusing on expanding its seniors housing footprint across the UK, North America and Canada, supported by strategic asset sales and capital recycling programmes.
These high-profile investments reflect more than asset accumulation; they signal platform building at scale. Organisations like Welltower are pivoting toward operational intensity and income predictability, increasingly layering operational exposure such as RIDEA and triple-net lease structures into their real estate portfolios.
Meanwhile, private capital, exemplified by long-term investors such as Reuben Brothers, continues to deepen exposure in UK healthcare real assets, reinforcing confidence in durable demographic demand and the strategic value of owning integrated portfolios rather than passive asset stacks.
This alignment towards strategic executive leadership mirrors investor emphasis on driving scale efficiently, managing
complex operating portfolios, and aligning long-term shareholder returns with leadership incentives.”
Hiring trends and compensation packages
Drawing upon CCO’s completed mandates in the last year, there were a number of distinct patterns prevalent across hires at board, finance and executive leadership level. These trends demonstrated the specific requirements investors have been looking for, when recruiting leadership teams who can deliver strong returns on exit.
Across mandates delivered in 2025, the executive profile most consistently required combined:
Multi site operational leadership –leadership of platforms with significant geographic footprint
Property and capital markets fluency
– familiarity with real estate strategy, development cycles, CAPEX prioritisation and financing
M&A and growth execution – a track record of acquisitions, integrations and portfolio scaling
• Cross‑sector adaptability – the ability to translate best practice from adjacent healthcare or real assets disciplines
CCO supported significant board appointment – specifically CEO searches – where compensation packages reflected the premium placed on leadership depth and strategic breadth. Typical packages included base salaries in the £220k–£250k range, coupled with performance bonuses and equity components which ranged up to 5%.
Shortlist composition across these roles revealed a deliberate stretching of candidate pools, often including senior leaders from adjacent real estate or multi-site healthcare businesses who could bring fresh strategic perspective and disciplined growth experience. This alignment towards strategic executive leadership mirrors investor emphasis on driving scale efficiently, managing complex operating portfolios, and aligning long-term shareholder returns with leadership incentives – a frequently cited minimum expectations cited by investors when hiring.
Across 2025’s CFO mandates, key observations included:
• Targets with substantial multi‑site experience, not just sector familiarity
M&A deal execution experience, especially in property acquisition and portfolio integration
• Investor engagement competence, enabling CFOs to lead capital markets conversations and refine financing strategies
Typical compensation in 2025 reflected this elevated role: base salaries in the £220k–£250k band, structured bonuses reaching up to 50% of salary, and long-term incentive plans to align executives as capital stewards.
This is emblematic of a shift in comparison to previous years’ hires: CFOs are now expected to operate at the intersection of finance, strategy and execution, significantly influencing investor confidence and portfolio growth outcomes.
Operational leadership mandates such as Operational Director, or Managing Director hires were equally oriented toward candidates with:
• Regulatory and commissioning expertise, particularly in complex care segments such as mental health or learning disabilities
• Strategic oversight of large, distributed service portfolios
Capability to integrate digital and process excellence into frontline delivery
Compensation parity and incentive alignment in these roles highlighted the sector’s expectation that operational excellence directly drives asset performance metrics.
What is driving UK investment attention and what is being done to attract and retain leaders?
Despite broader regulatory and sectoral challenges, the UK continues to draw significant attention from international investors, not least because it remains one of the largest and most transparent healthcare real asset markets in Europe.
From a recruitment perspective, the UK can offer:
A deep talent pool of executives with complex multi-site leadership experience
• Regulatory clarity and a mature operator base, facilitating leadership continuity and risk navigation
• A strong pipeline of portfolios offering scale, which in turn attracts leaders comfortable with portfolio governance frameworks
For investors, this landscape has proven successful not just for asset acquisition but also for leadership deployment and capability building across finance and operational teams – demonstrated in the end of year investment activity.
Across CCO’s executive searches delivered in 2025 it became apparent that compensation structures are increasingly designed to align leadership outcomes with long-term asset value creation, which was demonstrated in three ways:
2 Multi year incentive plans: stretching beyond short financial cycles to reward strategic execution over time
3 Cross‑functional reward structures: blending operational, financial and strategic performance metrics within incentive frameworks
This reflects an investor philosophy that leadership remuneration should mirror the time horizon of real asset value realisation; a departure from traditional pure cash bonus models.
Conclusion
The evolving executive search market across healthcare real assets offers several broader insights:
• Leadership capability is a differentiator: Investors increasingly assess management strength at due diligence and portfolio review stages.
• Cross sector experience adds value: The most effective leaders bring multi-disciplinary experience, spanning operations, capital markets and regulatory experience.
• Incentive design now anchors retention: With long investment horizons and integration commitments, aligning leadership with long-term value outcomes is central to investor risk-return paradigms.
In 2025, executive recruitment in European healthcare real assets has matured from a functional exercise into a strategic imperative for value creation. Investors who recognise leadership not as an operational afterthought but as core infrastructure are better positioned to drive platform growth, integrate capital strategy with operational delivery, and navigate regulatory and market complexity.
For the real assets investment community, the emerging imperative is clear: appoint leaders who can operationalise strategy, execute growth with discipline, and deliver outcomes that resonate with both performance and purpose, and the results will follow.
Healthcare Real Estate: Navigating supply gaps and structural demand
Max Weitzmann, Octopus Healthcare Fund
The UK healthcare real estate sector closed 2025 on a paradoxical note: record levels of capital deployment and investor interest coinciding with a supply crisis that shows no signs of abating.
he underlying demographics and societal need for elderly care are firmly entrenched demand-side arguments for investment in the care sector, but despite approximately 100 new care homes being built in 2024, the net increase in available beds was just 86, according to Octopus analysis. It is a stark illustration of a sector where closures are outpacing new construction and estimates point to a 200,000-bed shortfall over the next three to four decades. The arithmetic is sobering and the sector’s challenges clear.
TYet investor confidence remains remarkably resilient. The entrance of major US REITs in 2025, particularly Welltower’s aggressive acquisition strategy culminating in the £5.2bn (US$6.9bn) acquisition of Barchester’s real estate portfolio, has validated the sector’s investment thesis and brought unprecedented levels of institutional capital drawn by the combination of defensive demographics, social impact credentials, and increasingly competitive returns.
The sector’s challenges, however, are equally evident. Planning delays have emerged as the principal bottleneck, with consent timelines stretching by six months or more compared to just a few years ago. Combined with evolving sustainability
requirements, particularly the transition to allelectric developments powered by renewable sources, developers and investors are having to factor in longer lead times and more complex approval processes.
As we head into 2026, the fundamental dynamics remain unchanged: strong structural demand, limited supply, and a planning system struggling to keep pace with societal need. Investors in Healthcare caught up with Max Weitzmann, deputy fund manager for Octopus Capital’s main care strategy (Octopus Healthcare Fund), to discuss the trends shaping investment decisions, what lies ahead for the UK care sector, and how Octopus Capital is positioning itself to address the supply/demand gap.
Nick Herbert, Editor, Investors in Healthcare
Q What defined 2025 for healthcare real estate investment in the UK?
A It was a very busy year. But even with all the good work happening across the sector, developers and contractors working hard to keep increasing the supply of quality purpose-built care homes, the number of beds across the country is expected to have remained relatively static, as older homes are still seeing persistent levels of closure. Private capital remains available and ready to further address this need.
Q There have been some major deals completed in the sector, both domestically and cross-border. Was it a surprise to see US REITs get involved?
A The scale and speed of some acquisitions were perhaps surprising. Welltower in particular has been very active and that’s a positive sign. The Barchester deal, for instance, was significant given the operation’s scale across the UK.
While the cost of capital for US REITs is relatively cheap at present, it’s not just US capital targeting the sector, we’re also seeing private equity interest from both sides of the Atlantic. This influx has been really positive for the sector because it demonstrates strong underlying demand from capital for both the real estate, as well as operational platforms.
For our investors, primarily private institutional capital, this validates the sector’s attractiveness. They’re looking for financial returns alongside social returns, and the increased mainstream attention helps confirm they’re backing the right strategy.
Q Has increased competition affected pricing?
A Yes, we’ve noticed more competition this year and we’re seeing pricing start to compress a little compared to where it was post-2022, which reflects the increased levels of demand. We’re expecting strong competition to continue from various sources, including US and European investors.
Q Which subsectors are attracting the most attention?
A Care homes remain the primary focus, driven by that persistent undersupply of elderly care beds and the quality of existing stock. We’re finding great opportunities in towns across the country that haven’t seen significant development in years, not necessarily in the well-supplied home counties, but in reasonably sized towns that haven’t had a purpose-built care home developed in 20 to 25 years.
We’re expecting strong competition to continue from various sources, including US and European investors.”
At Octopus, we’ll examine every opportunity on an undersupply basis. There aren’t many towns in the UK where you could say there’s an oversupply of purpose-built, high-quality beds. Some of the home counties have had significant development and are closer to adequate supply, but you don’t have to go far to find towns that haven’t had much new supply in the last couple of decades. We’re certainly prioritising those opportunities.
Primary healthcare properties also continue to attract strong demand.
Q What’s the biggest obstacle to delivering new supply?
A Planning. That’s the simple answer. At Octopus, we currently have double-digit numbers of homes where everything is agreed, developer, purchase price, tenant, rent, but we’re waiting for planning consent. Across those homes, that represents the best part of £150m of capital ready to deploy. We have everything in place, but we can’t proceed without consent.
Three or four years ago, you’d think from signing terms to being on site would take six months. Now we factor in an additional six months contingency for timing our equity deployment. We’ve not seen any tangible difference under the new government, despite initial planning reforms being announced.
The underlying demand for care keeps investors committed, however. Everyone understands the planning situation in the country isn’t ideal, but it’s not a reason to stop. We don’t take direct development risk ourselves as a fund, we work with experienced developer counterparties and support them as much as we can.
We keep investors informed about likely timings and maintain transparency around our pipeline so they can see the progress we’re making. But it is frustrating when you have
brilliant developers, excellent sites, and towns with material undersupply and major need, but you can’t get moving.
Q Have supply chain issues eased?
A Developers and contractors tell us that conditions have stabilised and prices have settled down over the past six to twelve months. We’re getting much more certainty now on land prices and build costs, which has helped project viability.
Q What impact have sustainability requirements had on development costs?
A
It’s interesting. Initially, some operators were reluctant to go all-electric, mainly concerned about costs and reliability compared to gas boilers. We’ve only funded all-electric homes powered by air source or ground source heat pumps for a few years now.
There’s no significant difference in funding a home with heat pumps versus a gas boiler as a percentage of overall development costs. And while our data shows there isn’t much difference in running costs right now, over our long-term investment horizon we believe the running costs of an all-electric home will become far cheaper.
We’re putting considerable effort into whole life carbon assessments as part of our target to make new developments net zero by 2030, and the entire fund by 2040. We’re targeting a maximum of 410 kilograms of carbon per square metre, and we’re seeing builds come in below that.
There is some additional cost from sustainability requirements, but not to the point where homes become uneconomic. Working with counterparties who understand the importance of sustainability, both globally and to our investors, they’re happy to work with us
At Octopus, we currently have double -digit numbers of homes where everything is agreed, developer, purchase price, tenant, rent but we’re waiting for planning consent. Across those homes, that represents the best part of £150m of capital ready to deploy.”
on this. The costs of targeting BREEAM In-Use Excellent are considerably less than four or five years ago.
You don’t really hear about green premiums for funding care homes anymore. We’re not aware of many homes being funded on a propco basis that aren’t all-electric, many have followed our lead. It’s probably more about a brown discount now for less ESG-focused homes, if they can get funding at all.
Q Is sustainability still important to investors?
A
Very much so. We get extensive questions in due diligence processes from new investors around sustainability. We’re always trying to push further each year.
This year we’ve emphasised the social side more, considering social impact across four pathways: residents, staff, supply chain, and communities. It’s not just about providing high quality care, though that’s obviously the primary responsibility. It’s about what homes are doing for their supply chain sustainability and how they’re helping communities. What additional services are they providing to the wider community? That’s what we’re pushing with our operators now.
Q What trends do you expect for 2026?
A Steady as she goes, largely. Further Bank of England interest rate cuts would help reduce costs slightly and open things up a touch. But we’re not anticipating wholesale changes. We’ll continue pushing toward our net zero target from a sustainability perspective. We work with over 30 operators now, and they’re all working hard to provide high quality care. We’ll keep doing what we’re doing, they’ll keep doing what they’re doing, and together we’ll keep working to address this societal need.
Q Any advice for investors considering the care sector?
A Investors looking at the care sector should focus on long-term fundamentals rather than short-term noise. The underlying demographic demand is well established, but outcomes are increasingly differentiated by asset quality, operator strength and governance. Modern, purpose-built homes continue to outperform, particularly where investors take a patient, partnership-led approach with experienced operators. Planning and delivery timelines need to be factored in, but long-term capital, that works with a specialist manager to minimise the perceived risks of the sector remains well placed to generate stable returns while helping address a critical societal need.
Directory - Real Estate Advisors
The Met, 24 Percy St, London W1T 2BS
Future Space UWE North Gate Filton Road Stoke Gifford Bristol BS34 8RB
Iain Lock Managing director, health
iain.lock@avisonyoung.com
+44 (0)20 7911 2603
Amanda Nurse Co Founder
amanda.nurse@carterwood.co.uk 01454 838038
Tom Hartley Managing Director tom.hartley@carterwood.co.uk 01454 838038
Henrietta House Henrietta Place, London W1G 0NB
White Friars House, 6 Carmelite St, Temple, London EC4Y 0BS
Spain
Pablo Callejo Head of Investment Banking OPRE Europe
pablo.callejo@cbre.com
+34 618 384 216 France
Adrien Prigent
Healthcare Investment adrien.prigent@cbre.fr
+33 6 98 74 64 25
Germany
Marco Schnell Head of Investment Advisory Services marco.schnell@cbre.com +49 173 2880124
Hannah Haines Head of Healthcare & Education Consultancy
Hannah.Haines@christie.com +44 7736 617 008
Michael Hodges; Managing Director Capital Markets michael.hodges@christie.com +44 7764 241 300
Frank Convery Principal
frank.convery@avisonyoung.com
+44 (0)117 988 525
Dan Madden Commercial Director
dan.madden@carterwood.co.uk 01454 838038
UK
Tom Morgan Head of Operational Real Estate tom.morgan@cbre.com
+44 7950 569 389
Sarah Livingston Head of Healthcare sarah.livingston@cbre.com +44 7764 326 129
Calum Lawrence Healthcare Investment calum.lawrence@cbre.com +44 7557 398 650
David Ketsela Alberti Head of Care France david.alberti@christie.com
+33 670 883 500
Marlon Schramm Head of Care Germany marlon.schramm@christie.com +49 172 670 9027
95 Wigmore St, London W1U 1FF
Richard Harris Director, Head of Healthcare
Richard.A.Harris@colliers.com
+44 (0) 20 7487 1864
COMPANY
HEAD OFFICE KEY CONTACTS
43-45 Portman Square London W1A 3BG United Kingdom
Peter Farnes Partner, Healthcare peter.Farnes@cushwake.com
+44 (0) 207 152 5196
Jan-Bastian Knod Head of Healthcare Advisory Capital Markets Germany jan-bastian.knod@cushwake.com +49 151 1883 0953
Max Merkel Senior Consultant Capital Markets Germany jan-bastian.knod@cushwake.com +4969506073234
30 Warwick Street, London, W1B 5NH
55 Baker St, London W1U 8AN
33 Margaret Street, London, W1G 0JD
Emily Chadwick UK & Ireland Lead –Healthcare Value & Risk Advisory Emily.Chadwick@jll.com +44 7784 037177
Julian Evans FRICS
Global Head of Healthcare julian.evans@knightfrank.com
+44 20 7861 1147
Kieren Cole MRICS Head of Commercial Valuations kieren.cole@knightfrank.com
+44 20 7861 1563
Caryn Donahue
Head of Senior Housing Transactions caryn.donahue@savills.com
+44 (0) 7800 916 955
Max Eiting Director, Head of Healthcare meiting@savills.de +49 174 4913958
Thomas Atherton Strategy & Market Intelligence tom.atherton@savills.com
+44 (0) 7812 407 724
Rick Savage Head of Healthcare Valuations rick.savage@savills.com +44 (0) 7855 772 048
Craig Woollam Head of Healthcare cwoollam@savills.com
+44 (0) 7870 555 754
Selected Investors
REITs
COMPANY
Welltower
HQ COUNTRY
United States
Aedifica Belgium
Cofinimmo Belgium
Care Property Invest Belgium
Omega Healthcare United States
Target Healthcare REIT UK
CareTrust REIT United States
Primary Health Properties PLC UK
LondonMetric Property UK
Adriano Care Spain
ReSi REIT UK
Life Science REIT UK
NorthWest Healthcare Properties Canada
Paref (Fosun) France
Parkway Life REIT Singapore
WP Carey REIT
Ventas
COMPANY
United States
United States
Altarea France
INSURANCE & PENSION FUND
HQ COUNTRY
AP3 Tredje AP-fonden Sweden
Aviva UK
Rikshem Sweden
PGIM Real Estate United States
Vacse AB Sweden
Allianz Germany
ASR Nederland Netherlands
Pensioenfonds ABP Netherlands
CNP Assurances France
Greater Manchester Pension Fund UK
Keva Finland
EfTEN Capital Estonia
USS UK
VSW Arztekammer Schleswig-Holstein Germany
Mapfre Spain
Zurich Financial Switzerland
COMPANY
BANKS
HQ COUNTRY
BNP Paribas France
UBS Switzerland
Credit Agricole France
Banca March Spain
Nordea Sweden
Edmond de Rothschild Switzerland
RBS Group UK
Raiffeisen (Switzerland) Switzerland
DekaBank Germany
Crédit Mutuel France
DNB ASA (Norway) Norway
Leumi Bank Israel
Erste Bank Austria
Hamburg Commercial Bank Germany
OakNorth Bank UK
Deutsche Bank Germany
HSBC UK
NORD/LB Germany
Societe Generale United States
ABN AMRO Netherlands
Swedbank Sweden
Danske Bank Denmark
UK
FUND MANAGERS
UK
HQ COUNTRY
Aberdeen Group Plc UK
Achmea Real Estate Netherlands
ActivumSG Jersey
Advenis France
AEW United States
AEW Patrimoine France
AIF Capital Group Germany
Alma Property Partners Sweden
Amundi France
Aroundtown Germany
Belgreen Capital Germany
BentallGreenOak Canada
BEOS AG Germany
Besqab AB Sweden
Blackbear Real Estate Germany
BlackRock United States
Bouwinvest Netherlands
BVT Group Germany
Cabinet Benedic France
Catella Sweden
Cindat Capital Management China
Civitas Investment Management UK
Cortese Capital Netherlands
Corum France
Downing LLP UK
Drees & Sommer Germany
Elevation Advisors UK
Esas Holding Turkey
Euryale AM France
Franklin Templeton Investments United States
Hamburg Team Germany
Hartelt Fund Management Netherlands
Heeneman & Partners Netherlands
Hestia Investment Management France
HIH Real Estate Germany
Holland Immo Group Netherlands
Inter Gestion (Promogere) France
InterGestion France
Iroko France
Justim Sweden
Koncenton Denmark
Kriton Immobilien Germany
HQ COUNTRY
Kryalos Italy
La Francaise France
Lantmannen Fastigheter Sweden
LaSalle United States
LeadCrest Capital Partners France
Legal & General UK
Lenferink Groep bv Netherlands
Lifento Care Pan European France
M&G Real Estate UK
M2 Asset Management Sweden
Magellim Reim France
Meijer Realty Partners Netherlands
ML Real AG Germany
MNK Partners France
NewCore Capital Management UK
NordVest Germany
Norma Capital France
Northern Horizon Finland
Octopus Real Estate UK
PASENDIA Germany
Patrizia Germany
Perial France
Praemia REIM France
Primevest Netherlands
Rabo RE Group Netherlands
REAM SGR S.p.A. Italy
Revelop Sweden
Royal London Asset Management UK
Savills IM UK
Schroders UK
Sienna Real Estate France
Silver Fir Capital Italy
Slatto Forvaltning Sweden
Swiss Life AM Switzerland
Swiss Prime Switzerland
Threestones Capital Luxembourg
Thylander Gruppen Denmark
TSC Real Estate Germany Germany
TwentyTwo RE UK
Union Investment Germany
Values Real Estate Germany
VVT Kiinteistosijoitus Finland
Key Transactions (by value)
Where Connections Create Opportunity
Joining the European Healthcare Investor Association (EHIA) connects you to a powerful network at the centre of investing in European healthcare. Membership offers exclusive access to events, insights, discounts and a vibrant community of peers shaping the sector’s future.
EVENTS & NETWORKING
Enjoy invitations to our signature gatherings, including the Investors in Healthcare Gala Dinner during Jefferies in London, Autumn Networking Drinks, Women in Healthcare Investing events in Paris and London, San Francisco Drinks during JP Morgan week, and Healthcare Investing in Düsseldorf during Medica.
Members receive complimentary tickets (worth £795 each) to key conferences such as the Investors in Healthcare Private Capital Conference, European Healthcare Real Assets Conference and McDermott’s HPE Europe Conference
Access the rooms where the conversations really happen.”
Significant discounts are available for: SuperReturn International & Europe, HLTH Europe Amsterdam, CPHI, LSX World Congress London and Abu Dhabi Global Health Week Members can also partner with EHIA on events - with full marketing support - to amplify visibility within the global healthcare investment community.
In the Diary
Healthcare investing has a regular annual rhythm of events. Depending on your market or sub-market of interest, there are a number of conferences and trade shows that any investor, advisor or company should
CONTENT & COMMUNITY
Membership includes access to exclusive webinars, from Meet Your Members to Legal Insight with McDermott Will & Schulte
Members also receive a complimentary Investors in Healthcare enterprise subscription (worth £1,495 per year).
With more than 200,000 followers across EHIA’s digital platforms, your brand and investment activities gain visibility within one of the most engaged healthcare investor communities in Europe.
Membership includes access for multiple team members per organisation, ensuring your whole team benefits from EHIA’s connections and content.
Join EHIA — where healthcare investors connect, collaborate, and lead.”
attend. EHIA offers significant discounts to many of these events for our members. A full calendar of relevant events is published on our official journal Investors in Healthcare
EHIA Conferences
Investors in Healthcare Real Assets Conference
Property & Providers Conference
4th February 2026. The King’s Fund, London
Investors in Healthcare, in association with European Healthcare Investor Association will be hosting a new one day conference to complement our pan-European healthcare real estate news and transaction coverage. The healthcare market is rapidly evolving with the emergence of pan-European healthcare infrastructure assets underpinned by its social infrastructure characteristics, as well as the increasing interplay between real estate and the need to better understand the covenant strength of the underlying operated businesses paying the rent.
Investors in Healthcare Private Capital Conference
16th June 2026. Institute of Directors, 116 Pall Mall, London.
Investors in Healthcare, in association with European Healthcare Investor Association will be hosting the 2nd edition of this innovative conference, and due to the success of the 2025 event, will be moving to a larger venue, the Institute of Directors at 116 Pall Mall. The aim of this conference is to facilitate deals and promote investment in Europe across healthcare, life sciences and pharma. Set in a private environment, investors and portfolio company corporate leaders will be able to gain insights into market and investment trends as well as network with their peers. conference.
Working with Level 20
Launched by 12 founders in 2015, Level 20 is the leading industry body for women in private equity with a mission to increase the representation of senior women, particularly in investment roles.
It works in partnership with the wider industry and more than 120 sponsors fund Level 20’s activities, including its industry-leading mentoring and event programmes, which are free for individual members.
Each year, the organisation publishes authoritative research and this data-led insight supports firms to take practical steps towards effecting change. Level 20 operates in 20 countries across 13 international chapters with over 7,250 members. Each chapter is supported by the Level 20 executive team and a committee of volunteers who bring women together to build essential relationships both in local regions, and across Europe.
Mission
To increase the representation of senior women, particularly in investment roles, to transform the leadership landscape. Level 20’s initiatives support women’s careers in partnership with the wider industry.
Gurpreet joined Level 20 as CEO in April 2023 having spent a decade at the British Private Equity and Venture Capital Association (BVCA). As Level 20’s CEO, Gurpreet is responsible for delivering across five key activities:
• mentoring
• networking & development events research & insight advocacy & sponsor support
• outreach & internships
EHIA works closely with Level 20 who empower women to succeed in private equity, and has held networking events in Paris and London supported by Apax Parters, Marwood Group, Bridgepoint and Latham & Watkins respectively. In 2025, EHIA Executive Director Sarah Ward was nominated for the "Women in Trade Associations 2025 Power List"
EHIA is also a member of the Trade Association Forum who together with CBI (Confederation of British Industry) and Federation of Small Businesses (FSB) celebrate organisations led by strong female champions who support and are supported by brilliant women at all stages of their careers to be powerful advocates for diversity and inclusion in their sectors and more widely to support and encourage female business leaders and entrepreneurs.
In 2024, Gurpreet featured on Private Equity News’ list of Twenty Trailblazing Women and under her leadership, Level 20 has welcomed new chapters and published research across Europe and the US. In her previous role as the BVCA’s Deputy Director General and Director of Policy, she led the private equity and venture capital industry’s response to a wide range of matters from a legal, regulatory and tax perspective, including on diversity and sustainability matters. Before joining the BVCA she worked at Deloitte LLP. Gurpreet studied at the LSE and is a Chartered Accountant and a fellow of the ICAEW. Outside of Level 20, Gurpreet is on the board of the UK Business Angels Association.
Investors in Healthcare is a Google News listed digital business intelligence platform delivering news, data and analytics for private capital across healthcare, life sciences and pharma in Europe with a 5,000+ article archive plus data tables on M&A, Equity, Debt and more. This knowledge creates actionable insights for investors, corporate leaders and advisors.
As the official journal of the European Healthcare Investor Association, it is the leading independent convener of knowledge for the sector using its MAP framework:
• MARKETS (overviews and deep dives including Whitechart PowerPoint slides from leading consulting firms)
• ASSETS (company profiles and Curis Intelligence asset portfolio and deal database including league tables of M&A, equity, debt and real estate deals)
COMING SOON
CURIS - THE DEFINITIVE DATABASE OF HEALTHCARE PRIVATE EQUITY
Google News listed digital business intelligence platform delivering news, data and analytics. Delivering actionable insights for investors, senior managers and advisors.