The latest technology in prenatal genetic screening (NIPS)
Non-invasive: Single maternal blood draw
High accuracy: Screening for chromosomal abnormalities
Clinically endorsed: NIPS recommended by medical societies
26. SYPHILLIS AND HIV IN PREGNANCY
36. INTERNATIONAL MIDWIFERY: RAROTONGA CELEBRATES BFHI ACCREDITATION
40. TE AO MĀORI
42. BREASTFEEDING CONNECTION
46. MY MIDWIFERY PLACE DIRECTORY ISSUE 120 MARCH 2026
EDITOR
Hayley McMurtrie
E: communications@nzcom.org.nz
ADVERTISING ENQUIRIES
Hayley McMurtrie
P: (03) 372 9741
MATERIAL & BOOKING
Deadlines for June 2026
Advertising Booking: 1 May 2026
Advertising Copy: 11 May 2026
Welcome to
Issue 120 of Midwife Aotearoa New Zealand
Welcome to the 120th issue of Midwife Aotearoa. It doesn’t seem long ago we celebrated our 100th issue.
Change is constant, and as the College progresses necessary governance changes (p.5), we look ahead with optimism and a firm commitment to serve members in the best way we can. We are confident that the revised governance model will deliver strong and effective leadership for the College, ensuring members will continue to have a strong voice as we move forward.
The College is its members and we invite you to join us at one of the upcoming information sessions to ensure you have what you need to understand these changes ahead of the Special General Meeting on 31 March (p.10).
We will also shortly be inviting all members to share their views through a membership satisfaction survey. Your feedback is essential in helping us refine and improve the services we provide.
Please keep an eye out for the survey and take the time to share your thoughts. We know your time is valuable, and we appreciate your contribution as we continue to grow as an organisation and a profession.
This issue includes a range of practice related articles (p.18-27), as well as features on safe sleep (p.30), expanding options for midwifery education (p.32), and BFHI accreditation for the Cook Islands (p.36).
I hope you enjoy Issue 120. If you have ideas or suggestions for future content, we would love to hear from you.
Ngā mihi nui, Hayley Square
HAYLEY MCMURTRIE EDITOR/COMMUNICATIONS MANAGER
FROM THE CO-PRESIDENTS
BEATRICE LEATHAM
TANGATA WHENUA CO-PRESIDENT
Te Kāreti o ngā Kaiwhakawhānau o Aotearoa | New Zealand College of Midwives commenced the year by enacting the Governance restructure. This follows the culmination of kōrero from within our membership, current and past Board members, tangata whenua, Ngā Māia and tangata tiriti that all revealed a strong message of support to reset our organisation’s governance model.
Throughout 2025 the current Board meticulously discussed the change required to successfully streamline our model whilst maintaining the crucial element of membership voice. From the beginning, our approach was guided by key priorities and principles, including Te Tiriti o Waitangi and skill-based appointments to achieve the aims and objectives of the College’s strategic plan. After much consideration and expert support, we (the current Board) believe our new Board will be better equipped to support our midwives and the whānau they serve.
As exciting as this is, there is much intentional mahi ahead. The success of this change will require the continued dedication, trust and enthusiasm from our profession to ensure the new structure and Board are endorsed to fulfil their roles with confidence. The follow-through from the Cultural Review is reflected within the directives of this restructure.
Our new Board will reflect an equitable lens, reinforcing a Tiriti-led organisation. Alongside the Board, the National Forum, which will include regional chairs, consumers, students and education representatives, will
ensure a strong emphasis on maintaining the connection with the membership and stakeholders.
An integral part of the process has been taking direction from the membership and engaging with experts such as Jo Cribb and Kathie Irwin. Their work laid the foundations, confirming a move forward was essential. Paul Brown and Susan Huria from Boardworks have streamlined the next phase, supporting an efficient and equitable pathway to create an effective and sustainable Board, with a future focused perspective.
If you are motivated to influence our organisation and have fiscal, cultural, Tiriti, governance experience and attributes, we need you! I would strongly encourage you to consider a position on our Board. Square
DEBBIE FISHER
TANGATA TIRITI
CO-PRESIDENT
Kia ora koutou,
We deeply appreciate your ongoing dedication to the profession. Together, we can shape the future of midwifery in Aotearoa. We are excited to announce that we will soon be advertising for appointed positions on the new College Board of Directors. With recent governance changes, the College is transitioning to a board structure that will support effective governance, strategic planning and oversight. This change will optimise your College’s operations. (see CE's article on next page).
The regional chairpersons and representatives will now step away from board duties, enabling them to focus on local advocacy and participate actively in the newly developed National Forum. This Forum, chaired by your Co-Presidents, will have member
representation as well as input from broader partners. This Forum will address day-to-day professional and practice issues and provide valuable insights and advice to the Board. Current regional chairpersons and other current National Board members will transition into the National Forum initially.
We warmly invite members to consider putting themselves forward for a position on the College’s new Board. The Board will comprise individuals with the skills and attributes needed to ensure the College is future ready, financially sustainable, and focused on delivering the strategic plan. We welcome applications from members who are from diverse midwifery backgrounds, and have a belief and commitment to the objectives of the College, midwifery philosophy and equity. These would preferably be backed by significant clinical experience, with applicants holding some of these key skills:
• Adept at governance, with understanding of the role and legal responsibilities of the Board
• The ability to think strategically
• Knowledge of the broader health and/or midwifery education sectors
• Strong financial literacy and analytical ability
• Data literacy and appreciation of disruptive technologies
If you are looking for the next step in your midwifery career, we encourage you to apply. We will advertise these positions in April and our team is here to support you at every step. Your voice and expertise are vital. We encourage members to step forward and help lead our College into its next chapter. Please feel free to reach out with any questions, and we look forward to your involvement at this exciting stage.
Ngā mihi, Debbie Square
SHAPING THE FUTURE
FINALISING THE COLLEGE’S NEW GOVERNANCE MODEL
The College of Midwives was founded in 1989 as a grassroots organisation during a pivotal time when midwifery was reclaiming its autonomy in Aotearoa. Its governance model was built on partnership, consensus decision-making, and strong in-person connections which were essential in the pre-internet era. A defining principle from the outset was consumer participation, setting the College apart from other professional bodies.
Over the years, the College has grown significantly, now supporting and representing over 4,000 members and delivering a wide range of professional services, including indemnity insurance, quality assurance, education and workforce support programmes.
While its representative governance model has enabled inclusivity and participation, the current board structure with 26 members has become increasingly complex and unwieldy. In order to ensure the College is able to maintain progress in providing strong support and leadership for the profession, our governance structure needs to evolve to provide skilled, nimble governance for the organisation.
In late 2024, the College’s board commissioned an external review of its governance model. The context in which this review occurred included:
• Changes to the Incorporated Societies Act which sharpened the focus on organisations' governance responsibilities and board accountabilities.
• Recognition and ongoing commitment to Ngā Māia o Aotearoa as Te Tiriti partner.
• Ongoing legal action against the Ministry of Health with a High Court Class Action case (heard in August 2024).
• The evolution of health governance more broadly, with many organisations moving to more formal skillbased models.
A summary of the key themes which emerged from this independent review are set out below.
GOOD GOVERNANCE AND VALUES
Some aspects of the current College board governance model were highly valued, including:
• broad representation which brings a diversity of perspectives and skills,
• networking and relationships,
• leadership development opportunities,
• rich discussions and collaboration across regions.
ALISON EDDY CHIEF EXECUTIVE
Honouring the voices of maternity consumers and whānau was seen as critical and a core element of the midwifery philosophy. However, the review noted that the current practice of including representatives nominated by partner organisations on the board as a proxy for the consumer voice was not necessarily achieving the intent of equitable and effective consumer representation.
The philosophy of midwifery, focused on partnership, was seen as the key value that should be embedded in any future board models, along with values of inclusivity, equity, collaboration and collective action. The board was considered to have an important role in creating a strong vision and strategy for the College. There was also strong support of the Co-President model and commitment to upholding Te Tiriti o Waitangi.
REGIONAL STRUCTURES
The review identified that regional voices are a critical part of the structure of the College. However, the current mechanism of honouring regional voices through a seat at the board table was not necessarily considered an effective means of enabling this to occur. Board meeting agendas are so full of national issues that there is insufficient time for regional issues to be discussed fully. A separate forum was proposed as a possible means to enable regions to remain connected to each other and to the College nationally.
BOARD COMPOSITION
The size of the current board was deemed too large, limiting the ability to provide timely and responsive strategic direction to the organisation. The review noted that future board members collectively need to have deep and diverse midwifery experience, a commitment to protecting and supporting the profession, as well as key governance skills such as strategic thinking, political
acumen, financial and risk management and understanding of the health and midwifery education sectors.
CONSUMER INCLUSION
Honouring the voices of maternity consumers and whānau was seen as critical and a core element of the midwifery philosophy. However, the review noted that the current practice of including representatives nominated by partner organisations on the board as a proxy for the consumer voice was not necessarily achieving the intent of equitable and effective consumer representation. The possibility of a national consumer advisory group that advises the board and management was discussed as a possibility. Alternatively, a combined forum with consumer and midwifery representation could be established.
WHAT COULD BE STRENGTHENED
It was also noted that there are some aspects within the College’s current governance model which could be strengthened:
• The turnover of board membership is relatively high as regional chair roles commonly have two-year terms.
• The board’s work currently includes operational and clinical policy focuses, not just governance. Thus, a portion of the meetings is taken up with information sharing and operational matters rather than governance-related matters.
• The CE is currently a member of the board whereas best practice is to separate governance and management functions/roles.
• As well as being members of the national board, regional chairperson representatives are expected to take a leadership role in their regions.
• The opportunity to discuss regional issues, share experiences, learn about colleagues’ experiences across the country, network and socialise is highly valued. These functions are not part of governance and could be better fulfilled within an alternative, purpose-driven forum.
A dedicated “National Forum” could include broad representation, including regional chairs, whānau/consumer partners and student representatives.
• Although the board has diverse membership, it is not possible to represent all groups within the profession, so the representative model is ultimately not effective.
The board has been considering these themes and the recommendations from the review
over the past year and at its November 2025 meeting, finalised a proposed model for a future governance structure.
NEW GOVERNANCE MODEL
The new governance model agreed by the board in November 2025 is based on the following key decisions and principles:
• A board of up to 9 members in total, including 5 midwives from the College membership, 2 midwives from Ngā Māia (who will also be College members), and 2 independent members who bring necessary skills, e.g. finance and risk, digital. The chair will be elected by the board members.
• Honouring Te Tiriti o Waitangi, with the Kuia, Kaumatua and Elder advising through the transition.
• All board members will be appointed by a dedicated recruitment panel initially consisting of the two Co-Presidents and an external governance expert.
• Board members will be selected on the basis of the skills and attributes required for governance (strategic thinking, analytical ability, financial/risk management literacy, commitment to the objectives of the College, midwifery philosophy, and equity, and for midwife members, preferably backed by significant clinical and health leadership experience.
• Board member terms will be for three years and members may put themselves forward for re-appointment (with a two-term limit). Initial appointments will be staggered to enable succession planning/overlap of board members’ terms.
• Co-Presidents will continue to be elected by College members but no longer be members of the board. They will instead have a member-facing role, including leading the National Forum, AGM and other representation activities.
• A new board Charter will be developed, to set out the governance framework, including legal responsibilities, revised terms of reference, and the roles and responsibilities for governance and management.
• Evaluation processes will be embedded from the outset to ensure effective governance is being achieved, and new board members will be supported with an induction programme. Finance & Risk and Quality Assurance sub-committees will be established to advise the board.
• In addition to having two elected board representatives, Ngā Māia will have an advisory role to the board.
11 Regional Chairs: Two year term (dependent on regional constitutions) Elected by regional members - one for each region and two for Auckland
CE: TermLength of employment
Appointed by the CE employment sub-committee of the board
Up to 4 Consumers: Two year term. Selected by consumer organisations
Kuia and Elder: Two year term. Selected by board ratification
1 independent member: Finance and risk
Co-Presidents: Two year term with right to stand for second term; Elected by members – Māori and non-Māori
1 independent member: Digital
2 Pasifika Midwife Reps: Two year term with right of renewal Selected by Pasifika Midwives Aotearoa
2 Ngā Māia nominees
9 Board Members: Three year terms with right to stand for second term. Selected by appointment process. Chair selected by the board.
2 Ngā Māia Reps: Two year term with right of renewal Selected by Ngā Māia
2 Students: Two year term (dependent on regional constitutions). Selected by the schools on a rotating basis
Education Consultant (Ex-Officio, Non-Voting): Term not stated in constitution Selected by the schools
5 midwives from membership
GOVERNANCE STRUCTURE
Governance structure
Ngā Māia
Elects Co-Presidents and regional representative members of National Forum
Membership
Organised in 10 regions
National Forum (inc. Co-Presidents)
ProvidesadvicetotheBoard
• A National Forum will be established for networking and to provide advice to the board. The National Forum membership will be broad and diverse including regional consumer and midwifery representation (e.g. Pasifika midwives, students, education sector etc).
• The CE will report to the board through the Chair.
• A process of succession planning will be established for successful recruitment of future board members.
NATIONAL FORUM
Currently the board performs the vital role of being the meeting place for diverse perspectives to be considered about critical issues for the profession. A National Forum could take up this function. Held in person, representatives from across the regions, wider profession and consumer partner organisations will come together for the purpose of discussing midwifery practice issues, networking, support, and leadership development. The Co-Presidents will chair these meetings and there will be formal feedback and advisory mechanisms between the National Forum and the board to ensure there is a strong connection and accountability between governance and
membership. The National Forum will make recommendations to the Board about national and systemic issues that need to be addressed.
FINANCE & RISK AND QUALITY ASSURANCE SUB-COMMITTEES
These two formal sub-committees of the board will assist the board in fulfilling its oversight of financial and risk management responsibilities (the Finance and Risk committee) and in overseeing the College’s key portfolio areas which impact on the quality of midwifery practice (the Quality Assurance Committee).
NEXT STEPS
To enable the necessary constitutional changes to be made to establish the new model, a special general meeting (SGM) is being held in March. The supporting documentation (including a revised constitution) will be circulated prior to the meeting.
A series of member webinars will also be held in March to present and discuss the new model, offering members the opportunity to ask questions or discuss aspects of the new model. Once the changes to the constitution have been ratified, the process of selecting new board members can begin. This will
Chief Executive and National Office
be concluded by the scheduled July board meeting, where the existing board can formally hand over its responsibilities to the incoming board. It is anticipated that the National Forum will hold its first meeting during the second half of 2026.
WHAT DOES THIS MEAN FOR YOU AS A MEMBER?
These changes are about making sure your voice - and the voices of whānauremain central while creating a governance structure that is agile, strategic, and futureready. The new model will enable the board to focus on leadership and accountability, while the National Forum becomes the place for connection, collaboration, sharing ideas and bringing the voice of members to the board. Co-Presidents will have a stronger member-facing role.
This is an exciting step forward for the College and for midwifery in Aotearoa. It honours our history while setting us up to meet the challenges ahead. Your participation matters - join the upcoming webinars, read the supporting documents, and have your say at the SGM. Together, we’re shaping a governance model that reflects who we are and will provide the best guidance for the College in the future. Square
FAREWELL TO SUE MORRIS
On 5 February 2026 we said goodbye to Sue Morris, a valued longstanding MMPO staff member, as she retired after a decade and a half of service. Over those years, Sue provided dedicated support to the Lead Maternity Carer (LMC) midwifery workforce, particularly those serving rural and remote communities, and she will be missed by staff and midwives alike.
Sue joined MMPO on 16 May 2011, just months after the Christchurch earthquakes. Sue played an important role in maintaining and strengthening dependable, responsive workforce support so LMC midwives could continue providing safe, continuous midwifery care for whānau during a time of significant challenge and change.
The LMC Rural Midwifery Locum Service, established in 2009, was designed to support rural and remote LMC midwives through locum cover, mentoring, education, and practice establishment support. Sue’s contribution to this work went far beyond coordination. She brought empathy, calm, and a deep understanding of the LMC model, offering a listening ear and a steady presence when midwives were under pressure.
This was particularly evident in urgent and unplanned situations where support was needed quickly and circumstances were often complex and personal. Sue navigated these moments with discretion and care, responding to sudden illness, family emergencies, fatigue, safety concerns, and other unexpected events with professionalism and compassion. Her ability to balance swift action with genuine understanding made her a trusted point of contact for midwives across Aotearoa.
As workforce needs evolved, Sue adapted alongside them. What began as a locum-focused service grew to include mentoring, rural education workshops, and relocation and establishment grants, reflecting a stronger focus on sustainability, retention, and connection. In 2017, the introduction of the Urban Emergency Locum Contract further expanded the role, and during COVID-19 Sue remained a steady and reliable presence.
As Sue steps into retirement, we thank her for her dedication and care that she brought to her work every day. Her contribution has made a lasting difference to midwives, whānau, and the wider maternity system, and she leaves MMPO with our warmest thanks and very best wishes for the future. Square
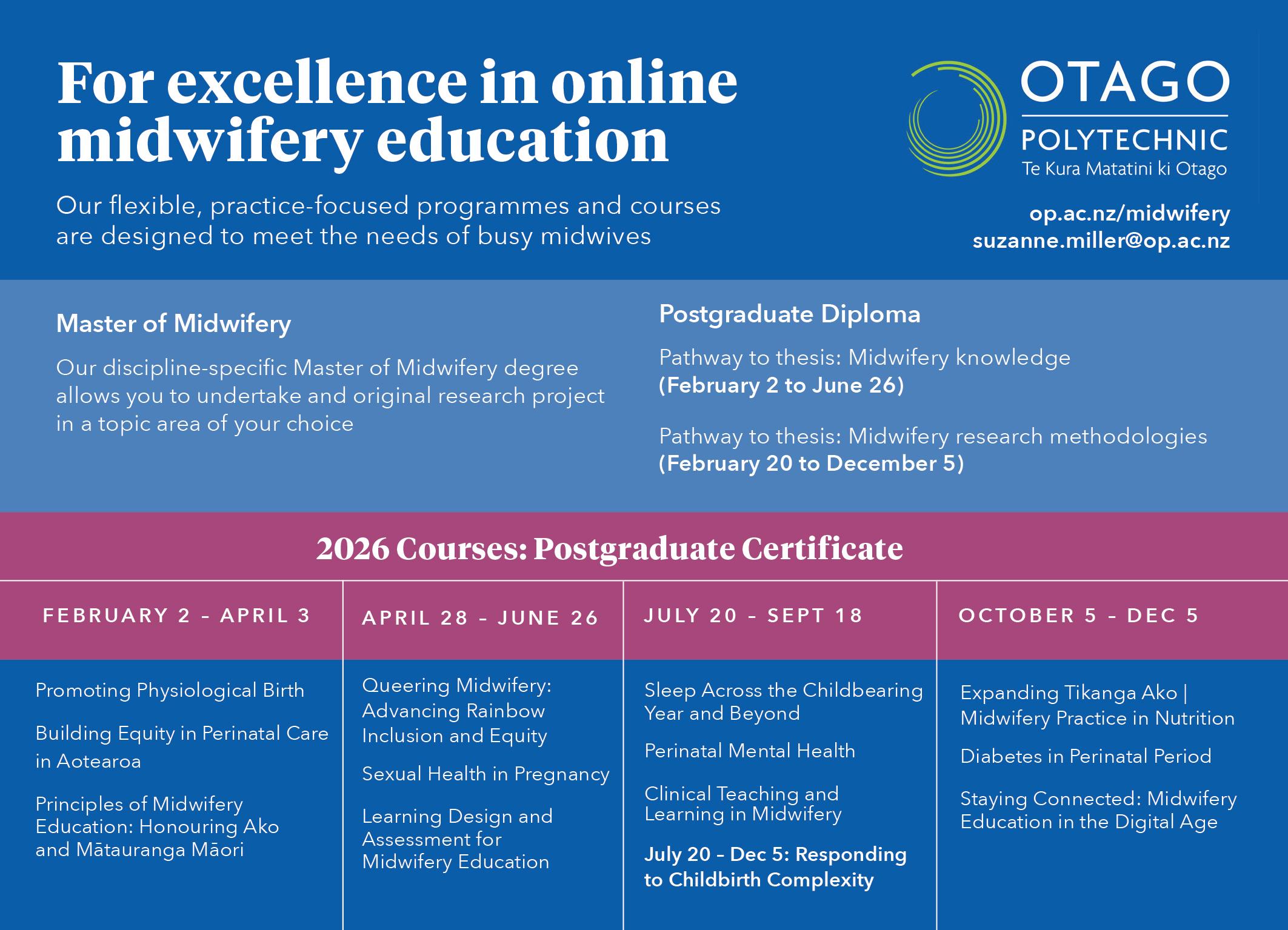
COLLEGE EDUCATION
The College's education programme includes both in-person and eLearning workshops and courses. We are currently offering the following education opportunities, with more in development and available mid-2026.
Resilient midwifery: Trauma-informed and compassionate practice
From navigating unexpected outcomes to creating psychologically safe work environments, this workshop equips midwives at all levels with the tools to thrive, not just survive, in today’s demanding maternity care landscape. This is an inperson workshop. Square
Midwifery Emergency Skills Refresher
This workshop fulfils the requirements for the mandatory full MESR day for recertification requirements for Te Tatau o te Whare Kahu | Midwifery Council. This is an in-person workshop. Square
Practicalities of mentoring
This course has been developed as a resource to explore mentoring as a professional support mechanism and is a prerequisite to become a mentor within a College programme. This is an eLearning course. Square
Te Tiriti o Waitangi
This course explores the rich story of Aotearoa, past and present. With this knowledge we gain a greater understanding and are better equipped to make informed, thoughtful decisions for the future. This is a hybrid course with eLearning and online meeting components. The complete hybrid course will take approximately six hours and may be counted towards a midwife’s compulsory cultural safety education hours under the 2024–2027 recertification cycle. Square
Syphilis and other STIs in midwifery
The primary aim of this eLearning is to equip midwives in Aotearoa with relevant and tailored information about pākewakewa | syphilis and other mate paipai | sexually transmitted infections. This is an eLearning course. Square
Midwifery care for former refugee whānau
This eLearning opportunity explores the knowledge brought by midwives and whānau from refugee backgrounds to the maternity journey in Aotearoa. Estimated to take up to 4 hours, this course may be counted towards compulsory cultural safety education hours. Square
In Person/eLearning
In Person
In Person
YOUR COLLEGE
Special General Meeting
The College invites all members to a Special General Meeting.
Date: 31 March, 6.00pm
Venue: Sudima Hotel Christchurch
In person and virtual meeting participation. Remits to update the College constitution and consensus statements for ratification will be circulated prior to the meeting. Square
LMC advisory group
In December 2025, the College established a LMC Advisory Group to help guide our engagement with Health New Zealand on Section 94 funding decisions. With the time-sensitivity of the implementation of Budget decisons, it is important to ensure LMC perspectives are represented early, clearly, and directly in the advice we provide.
The group brings together a wide range of LMC midwives, including urban, rural, Māori and homebirth practitioners, as well as midwives in their first five years of practice and those with more than a decade of experience. This breadth ensures that the realities of LMC work across Aotearoa are reflected in policy advice and funding priorities.
The group has already met to identify key priorities for any future funding uplifts and has provided this advice to Health NZ leadership ahead of Budget planning. Square
Quality Assurance framework
Following two years of dedicated mahi, including a comprehensive literature review and 17 national stakeholder focus groups, the College is ready to share the redesigned Quality Assurance framework (formerly known as MSR) with the profession. Consultation opens in March 2026. We encourage all Midwives to review the framework and have their say on the future of our quality assurance programme. Square
Joan Donley Midwifery Research Forum 2026
The Joan Donley Midwifery Research Forum will be held in Dunedin on Wednesday 9 and Thursday 10 September 2026. Call for Abstracts is now open until 20 March 2026. Square
BULLETIN
Midwifery-led immunisation
The Midwifery Council have published advice to the profession to clarify that with the appropriate education and ongoing evidence of competence, midwives may expand their practice to provide whānau immunisations that impact on the perinatal-related care of a woman or her infant up to 12 months of age. For further information see www. midwiferycouncil.health.nz.
LMC midwives who claim from the Notice (Section 94) are eligible to claim an administration fee for funded antenatal vaccination events (pertussis, influenza, and Covid-19) given from 1 July 2025, and all other funded vaccination events within their scope of practice from 1 February 2026.
This funding is managed by MMPO for all LMC midwives www.mmpo.org.nz Square
Funded treatments in the community for trauma and medical emergencies
Pharmac have announced that tranexamic acid will be added to the Practitioner Supply Order (PSO) schedule from 1 March 2026.
This decision means that the same medicines will be funded for treatment of postpartum
haemorrhage in the community enabling timely access to required treatments in emergencies.
The College has advocated strongly in support of this change and welcomes equitable access to recommended medicines for midwives.
For details visit: www.pharmac.govt.nz/ news-and-resources Square
SUDI webinar series
The National SUDI Prevention Coordination Service delivers a quarterly webinar series designed to inform, connect and upskill the SUDI Prevention workforce and kaimahi working alongside whānau.
The latest series of webinars provides context to the refreshed safe sleep messaging announced late 2025. The messaging is based on the 4 pou (pillars) that form a whānau-centric approach to SUDI prevention discussion for professionals, community and whānau. Square
Sepsis
The Sepsis Trust NZ has published a new community maternal sepsis pathway for health professionals. The College has advocated for the development of this specific pathway to
guide practice in a community setting and College representatives have worked with the Sepsis Trust during the development. The pathway can be found on the College website Practice Guidance pages or at www.sepsis.org.nz Square
Update to Guidelines for Consultation with Obstetric and Related Medical Services (Referral Guidelines)
Health NZ have advised the following changes to the codes in the maternal referral guidelines:
• Code 8048 - Maternal medication with risk to baby
• The description has been updated to remove anticonvulsants.
This code still applies to medications such as carbimazole, antipsychotics, and antidepressants.
New Code 8079 - Maternal medication with risk to baby - Anticonvulsant
This new code has been created specifically for anticonvulsant medications. Referral level: Consultation.
For the latest version of the guidelines, visit: www.tewhatuora.govt.nz Square
CELEBRATING MERAS WORKPLACE REPRESENTATIVES
CAROLINE CONROY
MERAS CO-LEADER (MIDWIFERY)
DAVID MUNRO
MERAS CO-LEADER (INDUSTRIAL)
In this edition we focus on the contribution that MERAS workplace representatives (MERAS reps) make to supporting MERAS members and the work of MERAS at a local and national level. There are over 100 MERAS reps across the maternity services of Health NZ and the maternity funded sector. These are midwife members who volunteer and are then endorsed by their colleagues. They provide a very important role in maternity workplaces as a point of contact and support for members, midwife managers and MERAS staff. They are very much the ‘eyes and ears’ of MERAS.
SUPPORT FOR MEMBERS
As workplace colleagues, MERAS reps provide a useful point of contact for MERAS members. Members can discuss a concern that affects them as an individual, such as payroll enquiries, questions about the roster or a meeting they have been requested to attend by their manager. The MERAS reps receive training when they first take on the role and, depending on how much experience they have in the role, they might support the member in addressing their concern or might seek advice from a MERAS Co-Leader.
MERAS reps have a valuable role in attending meetings with members and being a local support person. A MERAS Co-Leader or organiser will often join these meetings as well, but the workplace rep is able to offer local support and a listening ear to a MERAS member before and after the meeting.
RELATIONSHIP WITH MIDWIFE MANAGER
MERAS encourages MERAS reps to build a good working relationship with the ward or unit midwife manager and with the district chief midwife. It is much easier to have a discussion and work together to address issues for members if there is a good working relationship in place.
In most workplaces MERAS has established regular meetings between the midwife manager, district chief midwife, MERAS reps, and either Caroline Conroy, the MERAS Co-Leader (Midwifery), or MERAS organisers Karen Gray or Jess Maxwell. These meetings are an opportunity to discuss any local concerns or local and national initiatives that are likely to impact on maternity services.
LIAISON WITH MERAS STAFF
MERAS reps are a key point of contact for MERAS Co-Leaders or organisers. If MERAS staff receive a consultation document, proposal for change or concerns from members about the workplace, the reps provide a useful contact for an initial discussion. The MERAS staff are then able to work with the local reps in organising meetings with affected members or drafting feedback on consultation documents and supporting affected members through service reviews or changes within the workplace.
MERAS reps also have a key role in ensuring there is compliance with the provisions of the Collective Agreement or SECA and bringing any concerns to the attention of MERAS staff. As David Munro MERAS Co-Leader (Industrial) notes, “words
in a collective agreement are not worth the paper they are written on if they are not complied with. It will surprise many to know that non-compliance is not uncommon and frequently becomes a major talking point at Collective Agreement negotiations.”
REPRESENTING MERAS MEMBERS
MERAS reps often become involved in meetings in their workplace, local district or as part of national projects. These meetings include Maternity CCDM meetings, local bipartite meetings (BAG), working groups or SECA/Collective Agreement negotiations.
Currently MERAS reps who are working in senior midwife roles are becoming involved in the Job Evaluation project. The reps on the MERAS National Council (NRC) are selected from amongst regional reps. This ensures decisions that the MERAS NRC makes reflect the variety of workplaces and settings that members work in.
MERAS reps involved in local and national meetings and working groups bring visibility to the midwifery workforce and ensure the needs of midwifery and maternity services are to the forefront and are appropriately considered.
MERAS WORKPLACE REPRESENTATIVE CONFERENCE
MERAS has a conference for reps so that they can come together for two days for
discussions, updates and networking on key topics that impact on maternity services or work that MERAS is progressing. The conferences were initially every two years but in 2025 the conference became an annual event, as this is the one opportunity each year for reps from across the country to meet. Last year key topics discussed included:
• The establishment of the Health NZ regions and opportunities for maternity services and MERAS reps to work together. This aligns with the regional forums that MERAS is planning to establish in 2026.
• The increasing importance of digital software that supports the work of midwives, such as Badgernet and Safe Staffing (CCDM) data. There were presentations from MERAS reps who are employed in midwifery roles that support this work.
• The benefits that are being seen from acuity-based staffing (Trendcare) in maternity services.
• The sharing by MERAS reps of innovation and initiatives happening within different maternity services so that others can take these back to their own workplaces.
• The impact of the changes to pay equity legislation for some MERAS members and the challenging industrial environment for midwives and other health and public sector workers.
At some conferences there is also discussion on possible claims for Collective Agreement negotiations.
WHO ARE MERAS WORKPLACE REPS?
The members who become MERAS reps very much reflect the range of roles within the midwifery career pathway. Any MERAS member employed in a permanent midwifery role – except in midwife manager or chief/ deputy midwife roles – can volunteer to be a MERAS rep for a workplace when we are recruiting new representatives. Reps are released from clinical duties to attend meetings or are paid for that time if they are on rostered days off.
MERAS really values the contribution that our workplace reps make in bringing visibility to the needs of MERAS members, and the constructive way they work with their midwife managers and district chief midwives. If you are interested in being a MERAS rep you are welcome to indicate an interest when we are recruiting new reps for a ward or unit, or you can contact Caroline or David, as most medium or large maternity services have room for additional workplace representatives. Square
For MERAS Membership membership@meras.co.nz www.meras.co.nz
MERAS workplace representatives conference 2025.
THE IMPORTANCE OF FLEXIBLE MIDWIFERY WORKFORCE SOLUTIONS IN 2026
Access to safe, high-quality midwifery care across Aotearoa New Zealand depends on a maternity workforce that is supported, resilient and able to practise sustainably over time.
WAYNE ROBERTSON GENERAL MANAGER, MMPO
Central to the New Zealand maternity system is the integrated relationship between community-based Lead Maternity Carer (LMC) midwives and maternity facilitybased midwives. This partnership enables continuity of midwifery care for wāhine and whānau, but it also means that workforce pressures in one part of the system are often felt across the whole.
As the sector continues to navigate locational workforce dynamics, increasing complexity, geographic challenges and cumulative fatigue, flexible midwifery workforce solutions have become increasingly
important. Flexible workforce solutions, including midwifery locum support, are temporary, on-demand workforce arrangements, that help meet planned and unplanned workforce needs.
These approaches are not simply about filling gaps. They are fundamental to keeping access to midwifery care, sustaining both LMC and maternity facility midwives, and protecting the integrated model of maternity care that underpins good outcomes for mothers and babies.
ENSURING ACCESS THROUGH WORKFORCE SUSTAINABILITY
SUPPORTING THE INTEGRATED
LMC–FACILITY MODEL
The strength of Aotearoa’s maternity system lies in the close working relationship between community LMC midwives and maternity facility services. When either side of this partnership is under strain, continuity of care, clinical flow and professional relationships are affected.
Sustained access to midwifery care is only possible when midwives themselves are supported to practise safely and sustainably. For LMC midwives, extended periods on call, more limited opportunities for leave, and professional isolation can place significant strain on wellbeing.
Sustained access to midwifery care is only possible when midwives themselves are supported to practise safely and sustainably. For LMC midwives, extended periods on call, more limited opportunities for leave, and professional isolation can place significant strain on wellbeing. For maternity facility-based midwives, roster gaps, high acuity and workforce shortages contribute to fatigue, burnout and attrition.
Flexible midwifery workforce solutions support access to midwifery care by enabling planned and unplanned time off, reducing reliance on overtime, and helping safe staffing levels. By supporting midwives to remain well and engaged in practice, these approaches directly protect women’s access to care — particularly in those regions where workforce capacity is challenged.
Flexible midwifery workforce solutions help sustain this integration. Locum-supported LMC practice enables community midwives to support caseloads and continuity for women, while flexible staffing solutions within maternity facilities support prompt admissions, safe intrapartum care and effective postnatal support. By strengthening both community and facility maternity services, flexible workforce approaches reinforce collaboration, trust and continuity across the maternity system.
RESPONDING TO PERSONAL AND PROFESSIONAL
EMERGENCIES
Midwives, like all people, experience unexpected life events. Medical emergencies, bereavement, relationship breakdowns, caring responsibilities or other significant personal crises can arise suddenly and require immediate time away from practice. In these situations, flexible midwifery workforce solutions — especially locum support — are essential to keeping access to midwifery care. They allow midwives to step
away with confidence that care will continue safely and that colleagues are supported. This is particularly important in sole-charge LMC practices, small teams, and rural settings, where the absence of one midwife can significantly affect service availability.
Supporting midwives through these periods requires professional compassion and protects both continuity of care and workforce retention.
DIFFERENT ROLES, SHARED SUSTAINABILITY
Flexible workforce solutions are not one-sizefits-all; however, their purpose across roles is shared: to sustain midwives and maintain access to midwifery care.
For LMCs and self-employed midwives, flexible midwifery workforce support means midwifery locum support that enables planned leave, recovery from fatigue and continuity for women through well-managed handovers. For community and employed midwives, it means supporting safe staffing levels, managing workforce shortages and reducing burnout.
For maternity facilities — including secondary and tertiary services, rural maternity and primary birthing units — flexible workforce solutions support a wide range of situations. These include routine roster gaps, emergency and unplanned absences, annual leave, longer-term leave such as maternity or parental leave, sabbaticals, and periods of sustained workforce pressure. In many settings, this flexibility is critical to stabilising teams and supporting a culture where leave is taken rather than deferred.
STRENGTHENING RURAL AND REMOTE ACCESS
In rural, remote and geographically isolated communities, workforce pressures can have immediate and serious consequences for access to maternity care. These areas often rely on small teams with limited capacity, and are more vulnerable to transport constraints and severe weather events such as flooding, slips or prolonged isolation.
Flexible midwifery workforce solutions play a crucial role in strengthening maternity service resilience in these settings. They provide essential back-up when local midwives are unable to travel, require urgent relief or are affected by weather-related disruptions. During prolonged events, added flexible workforce capacity helps prevent fatigue and supports safe practice for resident midwives.
For wāhine and whānau, this support can prevent unsafe or distressing travel during labour or late pregnancy. For communities, it helps sustain local maternity services and supports equity of access regardless of geography.
SUPPORTING CAREER TRANSITIONS AND MIDWIFE CHOICE
Flexible midwifery workforce solutions also provide important pathways for midwives transitioning between roles or seeking different ways of working. Moving from facility-based practice to LMC work, or from LMC roles into facilities, often requires time and flexibility. For others, there are periods where stepping back from either facility or LMC work is necessary, without wanting to step away from midwifery altogether.
Flexible options allow midwives to continue practising in ways that align with their needs, circumstances and choices — whether short-term or longer-term. This may support recovery from fatigue, re-engagement with practice, skill maintenance or exploration of different models of care. By enabling choice and adaptability, flexible midwifery workforce solutions help keep experienced midwives within the profession.
A STRATEGIC, SYSTEM-WIDE APPROACH
Flexible midwifery workforce solutions are most effective when embedded within coordinated, system-wide workforce planning. This includes fair remuneration,
clear expectations, strong induction and handover processes, and recognition of the professional value flexible workforce midwives bring.
Crucially, these solutions support the sustainability of both LMC and facility midwives — not as separate workforces, but as interconnected parts of a single maternity system. By sustaining midwives, we sustain access to care.
LOOKING AHEAD
As the maternity sector moves through 2026, flexible midwifery workforce solutions — including locum support — continue to be essential to ensuring fair access to care and sustaining the integrated model that defines maternity services in Aotearoa. By investing in flexible, responsive midwifery workforce approaches, we protect midwives, strengthen collaboration between community and facility services, and ensure wāhine and whānau can continue to access safe, high-quality midwifery care, now and into the future. Square
Aotearoa New Zealand's midwife-centred support partner.
www.mmpo.org.nz
E: mmpo@mmpo.org.nz P: 03 377 2485
POOR NEONATAL ADAPTATION
FOLLOWING MATERNAL
PSYCHOTROPIC THERAPY
VIOLET CLAPHAM MIDWIFERY ADVISOR
The use of psychotropic medications during pregnancy is increasingly common in Aotearoa New Zealand, reflecting broader international trends. Primary care prescribing data show increasing administration of antidepressants and anxiolytics among women of reproductive age, meaning midwives more frequently support women taking these medicines during pregnancy (Ministry of Health, 2022). As a result, midwives are seeing more newborns who may be born with symptoms linked to in-utero exposure to psychotropic medicines, including Poor Neonatal Adaptation (PNA).
PSYCHOTROPIC MEDICINES COMMONLY USED IN PREGNANCY
The psychotropic medicines most often prescribed during pregnancy include:
These medicines are often essential for maintaining maternal mental wellbeing, preventing relapse, and supporting safe pregnancy care. Abrupt discontinuation carries significant risks, so collaborative management and informed decision-making are critical.
UNDERSTANDING POOR NEONATAL ADAPTATION
PNA refers to a cluster of symptoms occurring in newborns as they adapt to
the cessation of medication exposure after birth. While classically associated with opioids (and referred to as Neonatal Abstinence Syndrome, NAS), psychotropic medications (particularly SSRIs and SNRIs) can cause a similar PNA syndrome.
Symptoms typically emerge within hours to several days after birth. Studies suggest up to a third of infants exposed to antidepressants may develop PNA but, in the majority of infants, symptoms are mild and self-resolve, usually within 72 hours (Te Whatu Ora Waitaha, 2025).
FACTORS INFLUENCING NEONATAL EFFECTS
Across psychotropic drug classes, the likelihood and severity of neonatal effects are often influenced by maternal dose, duration of use and exposure in late pregnancy, although the relationship is not linear. SSRIs and SNRIs are most commonly associated with transient neonatal adaptation symptoms such as jitteriness, feeding difficulties and respiratory distress, while benzodiazepines (particularly at higher doses or with long-acting agents) are more
PSYCHOTROPIC MEDICINES IN PREGNANCY & NEONATAL EFFECTS
MEDICATION
SSRIS
• Sertraline
• Fluoxetine
• Citalopram
• Escitalopram
SNRIS
• Venlafaxine
• Duloxetine
TRICYCLIC ANTIDEPRESSANTS (TCAS)
BENZODIAZEPINES
ATYPICAL ANTIPSYCHOTICS
MOOD STABILISERS
• Amitriptyline
• Nortriptyline
• Diazepam
• Lorazepam
• Clonazepam
• Quetiapine
• Olanzapine
• Aripiprazole
• Risperidone
• Lithium
• Valproate
• Lamotrigine
strongly linked to hypotonia and respiratory depression. Antipsychotics may be associated with sedation or extrapyramidal features, and mood stabilisers such as lithium show a clearer dose-dependent relationship, necessitating planned hospital birth and neonatal monitoring.
MIDWIFERY CARE CONSIDERATIONS
Midwives should remain vigilant in the first 24-72 hours post-birth. Key considerations include:
• Reviewing maternal medication history and doses
• Observing baby for tremors, irritability, feeding issues, respiratory concerns or temperature instability
Observe for symptoms for 24-72 hrs; support feeding; consult paediatrics if symptoms are moderate to severe
First 72 hrs Monitor feeding, temperature, neuromuscular signs; escalate for respiratory concerns
First few days
First 48 hrs
Symptoms usually mild; review maternal dose; breastfeeding generally supported
Extended observation may be required; watch for respiratory compromise
Birth to several days Paediatric review recommended if neuromotor symptoms present; support feeding
Immediate postpartum
• Consulting paediatric or neonatal services early if symptoms of PNA develop
Maternal psychotropic use is not a contraindication to primary unit or homebirth; however, if the newborn requires observation, the midwife and woman should jointly plan for timely access to secondary services when needed.
REFERRAL AND COLLABORATIVE CARE
The Referral Guidelines state that complex maternal mental illness or diagnosed disorders requiring treatment (such as bipolar disorder) are an indication for obstetric consultation, and newborns with potential NAS/PNA may benefit from paediatric assessment (Ministry of Health, 2023). Ideally, care for women with complex mental illness should involve the woman’s GP, perinatal mental health team, obstetric
Lithium requires hospital birth and neonatal blood tests; homebirth not recommended
services and paediatric colleagues to ensure collaborative care planning across pregnancy, birth and the postpartum period.
INFORMED
CHOICE AND ONGOING COMMUNICATION
Midwives should ensure women have received balanced, evidence-informed information (from the medicine prescriber) about the risks and benefits of continuing psychotropics during pregnancy. Untreated mental illness carries significant risk for both mother and baby, therefore, medication decisions must be individualised and well documented.
Midwives should also ensure they are informed about the potential effects of any maternal medication on the baby, and discuss this with whānau. Square
References available on request
EARLY CESSATION OF THE LMC RELATIONSHIP
VIOLET CLAPHAM MIDWIFERY ADVISOR
The College continues to hear from midwives who are facing increasing complexity in their clinical work, particularly when women decline recommended care, make decisions outside guidelines, or need support that stretches midwives beyond their comfort zone. At the same time, women report difficulty finding another midwife when their LMC withdraws care, sometimes late in pregnancy. This situation creates distress for women and whānau, strain within midwifery practices, and reputational damage to the midwifery profession.
Ending a healthcare relationship in response to a consumer’s healthcare decisions is unusual in most areas of health. General practitioners, obstetricians, paramedics, core midwives and dentists rarely end a care relationship because a person declines recommended interventions. How is LMC midwifery different? And how do midwives navigate this territory while upholding professional standards and obligations, partnership and woman-centred practice?
This article explores why midwifery is unique and the frameworks that can support
midwives navigating challenging care situations.
THE MIDWIFERY RELATIONSHIP
The Lead maternity Carer model reinforces continuity of care, partnership, informed choice, and shared decision-makingfoundational principles of the College's Standards of Practice and the Primary Maternity Services Notice (2021).
Midwifery in Aotearoa is grounded in whanaungatanga, supporting relationshipbased care that is built on mutual trust and the upholding of mana. Supporting a birth journey is an intimate healthcare experience and the connections formed between midwife and whānau can be profound for both parties. The Lead Maternity Carer (LMC) model reinforces this: continuity of care, partnership, informed choice and shared decision-making are foundational principles of the College’s Standards of Practice and the Primary Maternity Services Notice (2021). The objectives of the Notice emphasise safe, evidence-informed, equitable care, with the LMC's responsibility for assessing needs, planning and providing care, and coordinating referrals when required. LMC midwifery is a publicly funded universal healthcare service in Aotearoa.
Ending an LMC relationship early disrupts continuity of care and may leave whānau without access to timely or appropriate care. This is particularly problematic in late pregnancy, when options may be very
limited. The risk of adverse outcomes or professional repercussions weighs heavily on midwives' decisions to withdraw from care. These pressures are real; however, providing ongoing care within a structured, well-documented and collaborative plan continues to offer the safest and most whānau-centred approach.
ADVICE WHEN CARE PROVISION BECOMES CHALLENGING
1. Anchor your approach in the Standards of Practice, the Midwifery Philosophy, the Code of Health and Disability Services Consumers’ Rights, and the Referral Guidelines
The College’s Standards of Practice and Midwifery Philosophy together articulate the professional responsibility of midwives to work in partnership with women, even when care becomes complex or challenging. Central to these frameworks is the expectation that midwives continue to provide care unless there are clear and negotiated reasons for transfer or cessation, and that care is grounded in respect for women’s autonomy and decisionmaking. The Midwifery Philosophy emphasises trust in women as active decision-makers in their own care, while the Standards require midwives to facilitate
informed choice through open, respectful dialogue, critical reflection and clear documentation. This includes supporting women who choose care pathways that differ from clinical recommendations, while continuing to plan, communicate and provide safe care within the scope of midwifery practice.
The College frameworks sit alongside the HDC Code of Rights, legislation that requires healthcare professionals to provide full, accurate, unbiased information to enable informed decision-making (Right 6) and to support every woman’s right to accept or decline recommendations (Right 7).
The Guidelines for Consultation with Obstetric and Related Medical Services (Referral Guidelines, Te Whatu Ora, 2023) provide a structure for consultation and transfer of clinical responsibility for care, and clearly state the importance of three-way conversations, comprehensive information sharing and documenting all discussions, including decisions that vary from the guidelines.
The process map (p.23) for when women decline recommendations is particularly useful, and was designed to protect both
women’s rights to make informed decisions and midwives in practice.
When midwives feel uncertain, these documents offer clarity on expectations: the midwife maintains responsibility for ensuring women are fully informed, for referring appropriately, for communicating with colleagues, and for planning safe care, even when recommendations are declined.
2. Support women’s right and ability to make informed decisions
Informed decision-making is not a single conversation, but an ongoing process of shared understanding. Key components include:
• Providing evidence-informed resources
• Allowing time for exploration of rationale, preferences and questions
• Explaining your professional assessment, recommendations, rationale and concerns
• Checking mutual understanding carefully
• Documenting all discussions thoroughly Supporting women’s autonomy does not mean agreeing with all decisions; it means ensuring decisions are informed, and that the midwife’s professional position is clearly articulated and documented.
Informed consent is an iterative process, and decisions made at one point in time need to be revisited if new information comes to light or the clinical situation changes.
3. Communicate your usual approach to practice early in the relationship Many challenges arise because expectations were not clearly established at the outset of the midwifery partnership.
The ideal time to discuss professional boundaries, your practice philosophy, clinical experience and practice arrangements is at the first midwifery appointment, not in the final weeks of pregnancy. It is also optimal to allow women time to discuss care options with whānau before signing a registration. Information to cover includes:
• Your usual midwifery practice (e.g. where most women birth, schedule and location of care provision, practice outcome statistics)
• Examples of situations that warrant a referral for specialist consultation or transfer of clinical responsibility for care
• Your experience and comfort level in specific clinical scenarios, particularly if they
are likely to form part of the woman’s birth plans (e.g. homebirth, breech, VBAC)
• Your availability of back-up, and how group practice arrangements work
• Your responsibility to continue providing care and to support informed decisionmaking
• The woman’s right to change midwife at any time
• The Code of Health and Disability Services Consumers’ Rights
• Options for providing feedback or making a complaint about healthcare received
This early clarity means that if differences of opinion emerge later, this occurs within a transparent and previously discussed framework, reducing conflict and protecting the relationship and the whānau experience of care.
4. Collegial support is crucial – do not leave colleagues isolated
The realities of midwifery practice often involve navigating nuanced clinical decisions. Strong collegial support is a critical safeguard, particularly for midwives in their early years of practice. Midwives can feel isolated and burdened when practice partners are uncomfortable with care plans or decline to provide back-up support. Regular, proactive communication between practice colleagues can mitigate this situation. When a woman declines recommended care, practice partners should be aware of the plan, the documentation and the supports in place.
Regular colleague-to-colleague connection, proactive discussion about caseloads, case reviews, and shared care planning enable midwives to tease out the issues they are concerned about with trusted colleagues as the issues emerge, and seek each other's experience and wisdom. This reduces anxiety, improves safety and strengthens team resilience. For a back-up midwife, these discussions are essential to understand the woman and whānau context and the reasons for her decisions, and can increase confidence in providing midwifery care if the LMC is unavailable. Back-up midwives seeing their colleagues’ clients for antenatal visits helps to build a relationship and support continuity should the LMC be unavailable for the birth. Midwives can also access wider collegial supports, including midwifery mentors, experienced colleagues and the College’s midwifery advisory service.
5. Communicate and collaborate with hospital colleagues
In many situations when women decline recommended care, there will be an indication for recommending referral for specialist consultation or transfer of clinical responsibility. The three-way conversation is an important element of consultations and transfers of clinical responsibility. In situations where women decline recommended care in advance of labour and birth, this can be discussed and supportive care arrangements can be made and documented during the three-way conversation.
When a care plan is made that differs from recommendations, or if complications emerge as pregnancy/labour progress, early communication with hospital colleagues provides preparation and support on arrival at the facility. Collaborative care planning ensures services are prepared to support the whānau choices and are able to respond safely, and LMC midwives can continue providing care for women with the knowledge that the hospital team will support them.
Core midwives can support their LMC colleagues by recognising when women have made informed decisions to decline recommended care, and responding to the current clinical situation in partnership with their LMC colleagues. Timely and effective communication is critical in ensuring all midwives feel confident and well-informed about the clinical situation. The ability to work collegially at the hospital interface to support whānau decisions is an important factor in LMC midwives’ comfort level in continuing to provide care for women who decline recommendations.
IF WITHDRAWAL OF CARE BECOMES NECESSARY
Withdrawal of care should be an exception, not a routine response to disagreement about decisions for care. This is reflected in the wording of the Primary Maternity Services Notice, which requires there to be ‘exceptional reasons’ (Clause DA7 (6)) for an LMC to cease providing care. When ending an LMC agreement becomes unavoidable, the approach must be woman and whānau centred and consistent with the Primary Maternity Services Notice, which requires midwives to advise women of alternative maternity providers and facilitate safe transition to further maternity care.
Key steps from the frameworks include:
• Explain clearly and respectfully why ongoing LMC care is no longer possible.
• Provide information on how whānau can access another LMC or the local hospital service.
• Initiate handover: if another provider has accepted care, with the woman’s consent contact them and offer a clinical handover and a copy of the clinical record.
• Document comprehensively the reasons, discussions and plan.
• Provide information on giving feedback, including the College’s Midwifery Standards Review process and Resolution Support services.
Decisions about whether to continue or withdraw from providing care must be anchored in the values of our profession. The Midwifery Philosophy calls us to protect the woman’s autonomy and nurture the midwife-whānau relationship, while the midwifery Code of Ethics requires accountability, respect and non-maleficence. These principles remind us that withdrawal of care should be rare and undertaken only when consistent with ethical practice and whānau wellbeing.
WHEN WĀHINE CHANGE MIDWIVES
Women have the right to change LMC at any time. This can be unsettling for midwives, both emotionally and professionally. Whānau may not always feel comfortable explaining why they have chosen a different caregiver.
As a midwife registering a woman who has changed LMC, it can be very useful to have a conversation with the previous midwife to get a full handover and ensure no information is lost.
Professionalism is important at all stages of a transition of care arrangements. Collegial respect and avoidance of judgement or defensiveness are essential. Midwives are encouraged to reflect on feedback when offered, maintain professional relationships with colleagues, and avoid behaviour that undermines trust or damages practice cohesion.
The College encourages midwives to send a consumer feedback link to all wāhine who have been in their care, regardless of whether the care ended early for any reason, and midwives should ensure all women receive a copy of their midwifery notes. All whānau should be informed about the Resolutions
Support service offered by the College, regardless of how the relationship has been. Providing feedback and/or participating in the Resolutions Support Service creates a supported pathway for whānau to raise concerns, seek clarity and feel heard.
KEY MESSAGES FOR MIDWIVES
• Refer to the Standards of Practice, the Referral Guidelines, and the HDC Code of Rights to guide your practice.
• The Primary Maternity Services Notice requires there to be exceptional reasons for cessation of LMC care.
• Prioritise transparent, early conversations about your usual practice.
• Support informed decision-making using evidence and sensitive dialogue.
• Ensure robust documentation to protect both the woman and the midwife.
• Engage with collegial support early; do not carry challenging situations alone.
• Remember that withdrawal of care is a significant clinical and ethical step.
• When necessary, end care in a structured, respectful and professional manner.
PROCESS MAP 6: WOMAN/PERSON (OR PARENTS) DECLINES TREATMENT
Midwifery is at its strongest when we honour partnership, uphold women’s rights and support one another.
Navigating disagreement or uncertainty is part of our work, but ending the midwifery relationship early should be an exceptional event and not become the default response to challenges or complexity which may emerge throughout the pregnancy.
With clarity, communication and collegial support, midwives can continue to provide safe, whānau-centred care, even when decisions vary from recommendations. Square
Condition warranting referral identified Options for care and evidence, risks and benefits with the woman/person (or parents)
Woman/person (or parents) declines treatment, referral to another health care practitioner, or transfer of clinical responsibilty for care
Document process, discussions, recommendations, decisions in the care plan
Consider discussing the case with another health care practitioner. Share the outcome and any advice from this conversation with the woman/person (or parents)
Consent for referral/transfer at any stage; see relevant care pathway
NO YES
Health care practitioner decides to discontinue care
Can a care arrangement satisfactory to the woman/person (or parents) and the health care practitioner be negotiated?
Clearly communicate the decision and the reason for it to the woman/person (or parents)
Assist the woman/person (or parents) to find alternative care within a reasonable timeframe
Provide a full handover to the new care provider and provide the woman/person with the provider's contact details
Health care practitioner continues to provide care
Continue to offer referral as appropriate Engage other health care practitioners as appropriate for professional support
Te Whatu Ora | Health New Zealand. (2023). Guidelines for consultation with obstetric and related medical services (Referral guidelines). https://www.tewhatuora.govt.nz/ publications/guidelines-for-consultation-with-obstetric-and-related-medical-services-referral-guidelines/
RHEUMATIC HEART DISEASE IN PREGNANCY
CLAIRE MACDONALD MIDWIFERY ADVISOR - RESEARCH
DR IAN KANDO OBSTETRIC PHYSICIAN
DEE MILES SPECIALIST MIDWIFE
The Aotearoa New Zealand Guidelines for the Prevention, Diagnosis, and Management of Acute Rheumatic Fever and Rheumatic Heart Disease were published by Health New Zealand | Te Whatu Ora in September 2025. Women and gender diverse people with rheumatic heart disease (RHD) require collaborative midwifery, physician and obstetric care, careful assessment, monitoring and care planning throughout pregnancy, birth and postpartum.
This article draws on key points from a September 2025 College webinar and the RHD guidelines. Midwives can watch the webinar and familiarise themselves with the guidelines, both of which are available on the College’s website.
Women with moderate to severe RHD are often concerned about their heart, their baby and their wellbeing during pregnancy, as are their whānau. Midwives offer comprehensive, relationship-based care for women with RHD, enabling them and their whānau to navigate pregnancy with confidence.
KEY POINTS ABOUT RHEUMATIC HEART DISEASE
• Strep A infection in the throat acts as a trigger for acute rheumatic fever (ARF) in susceptible individuals, leading to an exaggerated immune response. The immune system makes antibodies to fight Strep A infections.
• When this response becomes over-active, the immune system starts producing antibodies that may be damaging to parts of the body. This causes ARF which may cause heart damage (carditis), joint damage (arthritis), or inflammation in the brain (chorea).
• Over time, repeated Strep A infections may cause unbalanced immune responses that lead to permanent damage and scarring of the heart’s mitral valve and aortic valve,
known as RHD. Damage to these valves can affect the blood circulation on the left side of the heart, including valve regurgitation (leaky valve) and valve stenosis (narrowed valve).
• Some people with RHD require valve surgery or valve replacement. Valve replacements can be a bioprosthetic/tissue heart valve, or a metal heart valve - people with the latter require long-term medication.
• Strep A infection is spread by droplets. Household transmission is common.
• Social determinants of health associated with ARF and RHD are household crowding, poverty and lack of access to healthcare.
• 140 new ARF cases are diagnosed per year in NZ.
• RHD is an equity issue. ARF is unequally distributed by ethnicity and geography around Aotearoa. However, midwives everywhere need to be aware of the potential for RHD in all regions because people move around during their lives.
PREGNANCY, BIRTH AND POSTPARTUM CONSIDERATIONS
The heart has to cope with a lot of changes in pregnancy, labour and birth, and postpartum. When a woman has heart disease, in some cases the heart may decompensate (not cope). Maternal decompensation can
cause pulmonary oedema and heart failure; ventricular arrythmia; atrial fibrillation; thromboembolism (blood clots); and death (rarely). Cardiac disease, including RHD, remains the second leading cause of death during pregnancy and the postpartum period in Aotearoa, after suicide.
If decompensation occurs, pregnant women may need: inpatient care; transfer to specialist location; medication, intervention or surgery during pregnancy; or planned preterm birth (potentially around periviability gestation). In rare cases of severe maternal illness, pregnancy termination before periviable gestation may be advised.
During pregnancy, it is important to ask all women whether they have a history of rheumatic fever or RHD. In the Referral Guidelines, cardiac valve disease is divided into mitral/aortic regurgitation, warranting Consultation; or mitral/aortic stenosis, warranting Transfer. Cardiac valve replacement is also a transfer-level referral.
PRECONCEPTION CARE
In women who have cardiac disease, planned pregnancies and pre-conception assessments are associated with better pregnancy outcomes. Pre-conception counselling (from the medical provider who the woman sees for her heart condition) is strongly recommended for people with RHD who can become pregnant.
CARE DURING PREGNANCY
Collaborative care is essential. Routine midwifery antenatal care should be provided to women with RHD, alongside appropriate specialist referral and multidisciplinary care. Midwives should be aware of the potential for increased stress on the maternal heart from about 24 weeks of pregnancy. Warning signs of deterioration include decreased exercise tolerance, breathlessness on exertion, fainting, chest pain, pounding/fast or irregular heartbeat and oedema. Cardiac complications can also be compounded by pregnancy-related disorders like preeclampsia, and co-morbidities can further complicate pregnancy (e.g. obesity, diabetes, hypertension and renal disease).
PLANNING FOR BIRTH
A three-way discussion between the woman, midwife and specialist is important to support women in their birth planning decisions. Women with compromised heart function will need to be in a hospital setting. Women with severe heart disease may be advised to have an elective caesarean. There should be a clear plan for labour, including any medications which are recommended or contraindicated. It is common for an early epidural to be encouraged to minimise the sympathetic
drive on heart rate and blood pressure during labour. Careful fluid balance management is essential for women with RHD to prevent pulmonary overload. Active management of third stage is recommended to prevent postpartum haemorrhage. In the event of a postpartum haemorrhage, blood products may be preferable to IV fluids as treatment, in order to reduce the risk of pulmonary overload.
POSTPARTUM
Women with RHD are recommended to have at least 48 hours inpatient postnatal stay in hospital with daily medical review because the fluid shifts occurring in the first 24–48 hours can put a lot of stress on the heart. Some women may require postnatal care in a high dependency unit or cardiac ward.
Most RHD medications are suitable for use while breastfeeding. An individualised plan should be made with the woman during pregnancy to support breastfeeding, particularly if the woman may be expected to require care in a non-maternity ward.
POSTNATAL CARE
Once the woman is discharged home, routine postnatal care is appropriate, with awareness to monitor for signs of deterioration. Occasionally women have been diagnosed
with RHD for the first time in the postpartum period when they experience symptoms like difficulty breathing or chest pain.
Midwives providing postnatal care to women with RHD should check appropriate follow-up with cardiology or RF/RHD clinic has been arranged, along with a detailed discharge summary to the GP.
CONTRACEPTION
Reliable contraception is important for women with RHD, to ensure that pre-conception care can occur if another pregnancy is planned. Long-acting reversible contraception is more reliable than other forms.
Women who have RHD (or a history of acute rheumatic fever) benefit from continuity of care from pre-conception to post-birth. Midwifery care has an important role to play for women across the spectrum of disease severity, ensuring strong relationship-based care to support women’s informed choices and birth plan preferences. Specialist referral and collaborative care is indicated, and connecting these women with appropriate follow-up care (including general practice) is essential. To learn more about RHD in pregnancy, midwives can access the webinar on the College website and are encouraged to familiarise themselves with the RHD guidelines’ pregnancy section. Square
SYPHILIS AND HIV IN PREGNANCY
BRIGID BEEHAN MIDWIFERY ADVISOR
Syphilis and HIV remain significant public health issues in Aotearoa New Zealand. Despite effective pregnancy screening and treatment being available, babies are still being exposed to these infections in utero, with some newborns experiencing serious and preventable harm due to vertical transmission. Recent national surveillance data remind us that these infections have not disappeared and that gaps in access to care, testing and treatment remain. Midwives play a crucial role in offering early screening and education, and in supporting whānau to access timely treatment.
SYPHILIS
In 2024, the vast majority (88%) of infectious syphilis cases in women who have sex with men (WSM) were in those of reproductive age (defined by the Ministry of Health as aged 1544). Of the 121 infectious syphilis cases among women of reproductive age, 30 (25%) were pregnant.
There was a higher rate of congenital syphilis in liveborn babies among wāhine Māori (23 per 100,000) compared to the whole population (11 per 100,000), reflecting ongoing inequities in access to health care for Māori, including antenatal and sexual health care.
Six cases of congenital syphilis were r eported in 2024. Three of these babies were liveborn with symptoms and one was a neonatal death. Two of the mothers of these babies had incomplete treatment, two received no or late antenatal care, one was not tested despite receiving antenatal care, and one acquired a new infection in pregnancy
after a negative first-trimester test (Ministry of Health, 2025).
Midwives are uniquely positioned to support healthier futures for wāhine and pēpi through early identification, culturally safe discussion and effective management of syphilis.
HIV
HIV surveillance data from the same year reported seven infants born to women living with HIV. Of these, six mothers were diagnosed
INFECTIOUS SYPHILLIS CASES AMONGST WSM BY AGE-GROUP AND ETHINICITY: 2020-2024
in pregnancy and received antiretroviral therapy. One mother was diagnosed after pregnancy and one baby is believed to have acquired HIV (NZ Paediatric Surveillance Unit, 2024).
The context has shifted, with an outbreak of HIV in the Pacific increasing the likelihood of cases in Aotearoa. For midwives, the stories within the data are a call to action. A new joint statement by the New Zealand Microbiology Network, New Zealand Branch of the Australasian Society for Infectious Diseases, and the New Zealand Sexual Health Society (NZSHS), provides some useful advice for practice to support HIV detection, treatment and prevention.
The College was not involved in the development of this statement; however, the recommendations to strengthen first antenatal screening align with current practice and provide an important indication of risk factors to be aware of for re-screening during pregnancy.
This practice update reinforces the critical importance of first antenatal screening for all women and gender diverse people and third-trimester rescreening for syphilis and HIV for those with risk factors, alongside culturally safe conversations, timely follow up and equitable access to care for all whānau in Aotearoa.
NEW COLLEGE RESOURCES TO SUPPORT PRACTICE
In 2024, the College developed two new resources to support midwives in strengthening practice around syphilis, HIV and other STIs.
1. Syphilis and other STIs in Midwifery eLearning
The College has developed a fully funded eLearning course, Syphilis and other STIs in Midwifery, supporting midwives to refresh and strengthen knowledge in this important area of practice. The course provides up-to-date, practical guidance to support clear, tailored communication with whānau about pākewakewa | syphilis and other mate paipai | STIs, and it attracts four to six hours of elective education for Council recertification.
Expanding knowledge to support practice contributes to reducing STIrelated morbidity, decreasing rates of miscarriage and stillbirth, and supporting the elimination of congenital syphilis in neonates. Feedback from midwives highlights the impact of the course on their practice:
“This will help me to kōrero with whānau about the importance of screening for STIs during pregnancy to prevent adverse outcomes.”
“It has had a meaningful impact on my practice, particularly around equity, early recognition, and culturally safe communication.”
“I feel better informed about treatments and the discussions to have with families.”
The course is available via the College website: www.midwife.org.nz/midwives/education/elearning/ syphilis-and-other-stis-in-midwifery/
In 2024 the College also updated its Consensus Statement on STIs, strengthening the central role of Tūranga Kaupapa and Te Tiriti o Waitangi in midwifery practice. The updated statement provides guidance for midwives around communication, screening, notification and sharing results in ways that are culturally safe and whānau-centred.
Engaging with both the updated Consensus Statement and the eLearning module will support midwives to ensure they align their practice with current evidence-based guidance and provide equitable, respectful care for all whānau. Square
References available on request. Image from PHF science: PHF Science 2025. Sexually transmitted infections supplementary annual surveillance report - 2024. https://www.phfscience.nz/digital-library/sexually-transmittedinfections-supplementary-annual-surveillance-report-2024/
KEY PRACTICE POINTS FOR MIDWIVES: SYPHILIS AND HIV IN PREGNANCY
Cases of congenital syphilis and vertical transmission of HIV continue to occur in Aotearoa.
Recommend that all pregnant women and gender diverse people are screened for syphilis and HIV as part of the first antenatal screen or any time during pregnancy if not done earlier. Ensure they are able to access this screening.
- Women who received antenatal care overseas, regardless of gestation, should be retested for HIV and Syphilis as part of their first antenatal visit in Aotearoa.
Use sensitive, non-judgmental and culturally safe conversations to normalise sexual health discussions and support informed consent.
Act promptly on positive results with confirmatory testing and referral to sexual health, HIV specialist and/or obstetric services, while continuing midwifery care within the multidisciplinary team.
Syphilis and HIV are notifiable diseases. This process enables follow-up care and treatment for partners. Ensure that specialist services and/or sexual health services have completed the notification process. Midwives can also make a notification to the medical officer of health through the Notifiable Diseases page of Te Whatu Ora website.
Offer repeat screening, including:
• Third-trimester syphilis rescreening, based on local guidelines and individualised risk assessment.
• Third-trimester HIV rescreening at 28-32 weeks for those who may be at higher risk. The joint statement (mentioned above) advises that this includes those who:
- Have had a new sexual partner or more than one sexual partner during the current pregnancy
- Have a suspected or diagnosed STI during pregnancy
- Inject drugs or have sex with people who inject drugs
- Exchange sex for money or drugs
- Are sexual partners of people with HIV (acknowledging Undetectable = Untransmittable)
• HIV and Syphilis screening in labour for those not tested during pregnancy
Plan newborn care early with whānau and neonatal services, including assessment, testing, treatment and feeding plans where indicated. Breastfeeding considerations are covered in the hospital and the NZSHS STI guidelines.
Engage in ongoing education and familiarise yourself with local referral pathways and sexual health services, to ensure equitable access to timely care.
BUILDING CONFIDENCE AND RECOGNISING INEQUITY
It is time for midwifery in Aotearoa to evolve—and at the heart of progress is the Tūranga Kaupapa Education Programme 2024–2027. This programme is more than just training; it’s a pathway to becoming culturally safe, with treaty-informed care that truly monitors the needs of wāhine Māori and their whānau. But don’t just take it from us—here’s what midwives across Aotearoa have to say:
RELEVANT AND IMPACTFUL
“The course content was highly relevant to my professional needs and directly applicable to my practice.” – Manawatū
“This course provided a clear roadmap to improve my practice and integrate cultural safety.” - Mid Central
ENGAGING AND THOUGHTFULLY DELIVERED
“The facilitators brought heart and passion, creating a safe, inclusive space to learn and reflect.” - Bay of Plenty
“The mix of online learning, reflection, and live kōrero helped me deeply engage with the material.” - Canterbury
BUILDING CONFIDENCE AND ADDRESSING INEQUITY
“I have gained confidence to have meaningful conversations and provide better care for Māori women and whānau.” - Northland
“This programme sparked a real desire in me to help achieve better services for Māori in maternity.” - South Canterbury
ONGOING LEARNING AND SUPPORT
Many participants emphasise that this is just the beginning. There’s a strong call for sustained learning opportunities and resources to keep growing cultural responsiveness over time.
WHY IT MATTERS
Tūranga Kaupapa equips midwives with the tools to understand the history, context and ongoing impacts of colonisation on Māori health outcomes. It fosters self-reflection, challenges biases, and offers practical strategies to embed cultural safety in everyday care. This isn’t just professional development—it’s essential for improving health outcomes for Māori women and whānau.
JOIN THE MOVEMENT
If you’re committed to providing equitable, respectful, and culturally grounded care, the Tūranga Kaupapa Education Programme is waiting for you. Hear from your peers, see the difference it’s making, and take the next step towards transformative midwifery practice.
For more information or to register for upcoming sessions go to ngamaiatrust.org/turanga-kaupapa
Together, we can honour Te Tiriti o Waitangi and support the wellbeing of all wāhine and their whānau.
Ngā mihi nui to all midwives who shared their honest feedback and continue to lead change in our profession. Square
GROWING A PACIFIC BIRTHING VILLAGE
TISH TAIHIA
PASIFIKA MIDWIFE
O le pepe o le aiga, o le ali’i o le atunuu.
O le manutagi o le aiga, o le ali’I o le fa’alupega
The butterfly (baby) of the family, the chief of the nation. The dragonfly of the family, the lord of the village.
NGATEPAERU MARSTERS
PASIFIKA MIDWIVES AOTEAROA CO-CHAIR
Samoan poet Sia Figiel illustrates how each family member has a unique role to play within the aiga (whānau), emphasising that no one is insignificant.
South Auckland serves as the vibrant heart of Aotearoa New Zealand’s Pacific community – a diaspora so extensive it now outnumbers the populations remaining in several genealogical homelands. This demographic reality is mirrored in our maternity statistics.
Over the last decade, Pasifika births have consistently represented the largest ethnic share in Counties Manukau, accounting for 33.3% of births in 2022 and rising to 34.5% in 2023 (Tuuranga Hauora o te Mana Waahine Division of Women’s Health, 2023).
Middlemore Hospital has consistently managed high maternity volumes that often exceed its intended secondary and tertiary scope. This is largely due to Pacific mama opting for hospital births over community unit births, even for low-risk pregnancies. To alleviate this pressure, there is a critical need to expand the community-based midwifery workforce and redirect primary care back into primary settings.
Since its opening in 2019, Ngā Hau Māngere Birthing Centre (NHMBC) has served as a village hub for Māori and Pasifika families discovering the advantages of primary birthing. Founded by the late Chloe Wright, under the Wright Family Foundation, the centre was designed to provide a tailored maternity experience. NHMBC filled the gap in a landscape where primary care is typically absorbed by the over-stretched public health system. Six years on, following extensive advocacy within the evolving landscape of Te Whatu Ora and changes in government, a fixed service contract was finally secured in May 2025.
Representatives from Pasifika Midwives Aotearoa (PMWA) originally collaborated with Chloe to lead recruitment and formalise the board of the Tagata Moana Maternity Trust (TMMT). This partnership was built on a shared vision: to integrate Pacific families into NHMBC and grow the Pacific midwifery workforce. While Chloe’s passing in 2023 was a profound loss, her legacy endures.
A primary objective for TMMT remains ‘proving the case’ for expanded birthing options in underserved, high-needs communities through innovative support models. This vision is now being realised via a strategic partnership with Turuki Healthcare. This collaboration aligns our shared kaupapa with the Kahu Taurima initiative, seamlessly integrating
midwifery with broader 0-5 years services to provide holistic care beyond traditional boundaries. That it may showcase a template for the future has been voiced by many interested observers noting the direction it takes.
NHMBC has seen a significant trajectory in growth, culminating in 366 births in 2025 - a notable increase from 280 the previous year. The 2025 cohort reflects the diverse community the centre serves, with Pasifika families representing 56% of births, followed by Māori (27%), NZ European (10%), and MELAA (7%). The aim of NHMBC is its functional model: primary care delivered through dedicated LMC partnerships focused on proactive wellness.
To grow the Pacific LMC workforce, TMMT and NHMBC have focused on creating a village environment for both midwives and birthing whānau. NHMBC has become a midwifery sanctuary, where junior midwives, and some new to LMC practice, can provide primary care in a safe and supportive space. The experienced Pacific midwives who work both on the floor as well as in leadership roles within TMMT, act as aunties, mentors and role models for the next generation of Pasifika LMCs. This model reflects Pacific values and strengthens connection and relationships, which in turn increase the likelihood that the next generation of Pasifika LMCs have long and fulfilling midwifery careers. Relationships that began when they were students move fluidly into the midwifery profession.
Currently NHMBC has approximately 60 access holders - of which 25 LMCs use clinic space within the facility. There are 23 midwives who are dedicated to supporting well wāhine to birth at NHMBC and 10% identify as Pasifika.
Looking ahead in 2026, we remain committed to fostering a safe and supportive village environment where Pacific midwives can thrive, for the betterment of our entire midwifery workforce and the communities we serve. Square
FOUNDATIONS FOR SAFE SLEEP:
A NEW APPROACH TO PREVENTING SUDI IN AOTEAROA
TE PAEA BRADSHAW MĀORI MIDWIFERY ADVISOR
In December 2025, Hāpai Te Hauora launched Foundations for Safe Sleep, a national initiative designed to reduce Sudden Unexpected Death in Infancy (SUDI) rates across Aotearoa. This refreshed approach blends mātauranga Māori with evidence-based practices, creating culturally relevant and practical guidance for whānau. Fay Selby-Law, General Manager of the National SUDI Prevention Coordination Service at Hāpai Te Hauora, explains why this change matters and how midwives can lead the way in supporting safer sleep for pēpi.
WHY THE REFRESH?
Despite decades of progress, SUDI remains a significant and inequitable health issue. Current statistics show that the least deprived areas have a SUDI rate of 0.2 per 1,000 live births, while the most deprived areas face a rate of 1.5. Half of all deaths occur in the most deprived communities, with Māori babies disproportionately affected— approximately 40 Māori, 10 Pacific and 10 non-Māori/non-Pacific pēpi die each year. This equates to around 60 deaths annually. Although this rate is drastically better than nearly 200 in the 1980s and
1990s, disturbingly, the number of deaths has risen since 2017 when the rate was 48 deaths annually.
“If we keep doing what we’ve done, we’re going to keep getting the same results,” Fay says. Previous messaging, such as PEPE (Place Eliminate Position Encourage) was designed for clinicians and later adapted for whānau, but it placed responsibility solely on mothers. “That burden was unacceptable. It belongs to whānau and hapori | community. We needed to hear what was missing, and how our messaging could be strengthened.”
WHĀNAU VOICES AND MĀTAURANGA MĀORI
The refresh was informed by extensive engagement with whānau across the regions with high SUDI rates—Tairāwhiti, Bay of Plenty, Auckland and Northland. Fay and her team consulted teen parent units, young parents, tāne | men’s groups and whānau with limited support.
The refresh was informed by extensive engagement with whānau across the regions with high SUDI rates—Tairāwhiti, Bay of Plenty, Auckland and Northland. Fay and her team consulted teen parent units, young parents, tāne | men’s groups and whānau with limited support.
“They told us our resources didn’t speak to them,” Fay explains. “Images looked perfect – educated parents in beautiful settings. Nothing reflected their reality.” The new resources feature illustrations rather than staged photography, darker tones instead of bright, artificial colours and honest, clear messaging without blame.
Whānau also wanted more te reo Māori and cultural authenticity.
“Mātauranga Māori is woven throughout, drawing on atua kōrero, pūrākau, and whakataukī such as He aha te mea nui o te ao? and He taonga te mokopuna. These principles reinforce the message that every baby is a treasure, and safe sleep is a collective responsibility.”
THE FOUNDATIONS (FOUR KEY PILLARS) FOR SAFE SLEEP
1. Face Up, Face Clear Sleep pēpi on their back for every sleep, with nothing near their face like toys, loose blankets, cords or pillows.
2. Flat & Firm
Pēpi are safest in their own flat, firm bed with firm sides, like a wahakura, cot or bassinet.
3. Free
Pēpi is safest and well when they are in an environment that supports breastfeeding and is smoke, vape, alcohol, drug and harm-free; also infection-free - immunisation protects pēpi.
4. Fathers & Family
Safe sleep is not just mum’s job. It is a shared responsibility and requires everyone: pāpā, nanny, babysitter, ECE teachers –everyone must know the safe sleep plan.
HOW THIS DIFFERS FROM PREVIOUS MESSAGING
Unlike earlier campaigns, Foundations for Safe Sleep explicitly addresses bedsharing.
“Research says ‘don’t do it’, but midwives know it’s a reality,” Fay notes. The new resources provide practical guidance: if bedsharing occurs, ensure the baby is in a safe sleep space and never share a bed if smoking, vaping, drinking or using drugs. Bedsharing should also be avoided if the parents are over-tired, or if baby is preterm or unwell. Sharing statistics can help support discussions with whānau. For example, risks increase dramatically when maternal smoking and bedsharing is combined—by up to 32 times (Mitchell et al., 2017).
“The four foundations help midwives have brave conversations about bedsharing,” Fay says. “We acknowledge it happens— sometimes by choice, sometimes because of circumstances like transitional housing or extreme tiredness. Our role is to have the conversation and reduce the risk.”
SUPPORTING WHĀNAU FACING BARRIERS
Midwives often work with families experiencing housing insecurity or poverty. Fay emphasises that behaviour change starts
with relationships: “Begin the conversation at the family’s starting point, not the clinicians. Ask what they understand safe sleep is and build from there.”
But cultural safety and non-judgmental language are essential. “Know yourself first— because we all have bias,” Fay advises. “Stay tau | relaxed. Accept how it works in that household.”
BREASTFEEDING AND IMMUNISATION
Breastfeeding is a protective factor against SUDI, and is a mode of first language, offering a type of rongoā, skin-to-skin contact and nurturing. Immunisation also plays a role under the ‘Free from Harm’ foundation, reducing illness that can compromise infant safety.
RESOURCES AND TRAINING
Downloadable resources, online pamphlets, posters and magnets are available on the Hāpai te Hauora website. A “Train the Trainer” programme with eight modules will launch in 2026 to ensure champions are equipped to deliver culturally safe, evidencebased messaging. Also keep an eye out for
Pasifika-targeted resources being created by Moana Connect, these resources will align with the Four Foundations for Safe Sleep.
KEY TAKEAWAY MESSAGES FOR MIDWIVES
• Familiarise yourself with the Four Foundations and integrate them into practice.
• Engage whānau early and inclusively – pāpā and extended family matter.
• Use culturally safe, non-judgmental language.
• Be prepared to discuss bedsharing realistically and reduce associated risks.
• Support breastfeeding and immunisation as protective factors.
• “This baby is a taonga,” Fay reminds us. “Safe sleep is everyone’s responsibility.”
For more information, visit Hāpai Te Hauora website or access the latest SUDI surveillance report on the EHINZ website. Square
References available on request
EXPANDING OPTIONS FOR MIDWIFERY EDUCATION
ZAHRA SHAHTAHMASEBI JOURNALIST
The introduction of The University of Waikato’s Master of Clinical Practice (Midwifery) provides a new study pathway, enabling health practitioners registered under the Health Practitioners Competence Assurance Act to transfer their existing skills to midwifery.
The University of Waikato’s Master of Clinical Practice (Midwifery) has just seen its first cohort of students through year one. The university’s head of midwifery Liz James, who led the development of the course, says, “It is a delight to be working on the programme. It’s such a feel-good story… It is ticking so many boxes to make a difference.”
Until this programme was established, the only option for midwifery study pathways in Aotearoa was completing an undergraduate Bachelor degree at one of the five Schools of Midwifery at Waikato Institute of Technology, Auckland University of Technology (AUT), Victoria University of Wellington, Ara Institute of Canterbury and Otago Polytechnic.
Development of the graduate entry masters (GEM) midwifery programme began about three years ago, after it became clear that addressing midwifery workforce shortages required a range of responses. According to statistics from the International Confederation of Midwives, there is an international shortage of one million midwives across the globe. In Aotearoa, that translates to 680 full-time positions, or about 20% of the workforce, says University of
Waikato senior midwifery lecturer Talei Jackson.
“And if we want change, then we have to do something differently, because what we’ve been doing hasn’t been enough, despite how hard we’ve all been working for so long,” she explains.
The Master of Clinical Practice (Midwifery), which commenced in 2025, is a two-year graduate programme for registered health practitioners, and available in addition to current undergraduate degree options.
“When a health professional makes a choice to switch from an existing successful career to become a midwife, it is generally because they hold a strong passion to become a midwife, that’s what we have observed in these students,” says Liz.
The new pathway has been designed for accessibility, enabling students to study remotely from wherever they live across Aotearoa, while continuing to work part-time. In the 2025 cohort of seven students, there were two based in Waikato, and one each based in Tauranga, Gisborne, Auckland, New Plymouth and Nelson. The cohort consisted of five nurses, a pharmacist and a physiotherapist. In 2026, there will
Although midwifery has the highest percentage of practising practitioners who identify as Māori out of all of the registered health professions in Aotearoa, our increasingly culturally diverse population demands that we diversify the health professionals too.
also be new students in both Wellington and Christchurch. Liz has been thrilled to find that, as awareness of the programme grows, health facilities are encouraging interested staff to enrol.
EXPLORING THE TWO-YEAR STUDY LEARNING PATHWAY
All students undertake 1,500 hours of clinical experience and 900 theory hours. In addition to self-directed and online academic learning, throughout year one, students are required to attend seven weeks in person at the Waikato campus. This drops to five weeks in year two in addition to the online learning. Both years are interspersed with clinical placements in facilities and with LMC midwives in their hometowns. Talei says this means the students can remain immersed in their own communities and health sectors. “And now they’re just going in with a different hat - as a student midwife. Generally, they’ve been wrapped around and supported by their communities as well. I think it’s great we’ve been able to do that for them, rather than taking them outside their community for placements.”
The students are supported by clinical academics from the Waikato team, with meetings held every two to three weeks on Microsoft Teams and in-person visits once a term. Talei says she loves visiting the students in their own space: “You get a different sense
about them, you’re stepping into their space as opposed to them coming to campus and to our workplace. It’s lovely to see them in their clinical setting.”
Although midwifery has the highest percentage of practising practitioners who identify as Māori out of all of the registered health professions in Aotearoa, our increasingly culturally diverse population demands that we diversify the health professionals too, adds Liz: “Health should be available for everybody… you want the workforce to represent the population.”
This is something the Master of Clinical Practice (Midwifery) programme is aiming to rectify. Serving the Indian community in the Waikato is a big privilege for current student Ashly Mangalasseril, a registered nurse from India who has been working in the birthing suite at Waikato Hospital.
Ashly saw the graduate programme advertised and decided to apply. Her move has inspired other Indian nurses and three more have applied for the 2026 intake. “Now that I’ve done it, I can tell you how you can balance it and how it will be once you’ve done it,” she says.
Ashly is one of many nurses over the last few years who have expressed an interest in being educated to be a midwife; however, signing up to four years of study in the undergraduate programme was a major barrier for them, given the length of time, the current financial climate and lack of governmental study support available for mature students.
BUILDING THE PROGRAMME
In 2022, the University of Waikato approached Liz, who, with the support of Samantha Davenport and other colleagues, began developing the graduate entry programme. The team examined comparable graduate programmes in countries such as Australia and the United Kingdom, and consulted widely with colleagues across the sector in Aotearoa, including Talei, who was working at AUT at the time. “We were tasked with educating registered health professionals to become midwives, and we wanted to approach the teaching in a different way,” says Liz.
While there were challenges with some of the processes, the team was wellsupported by the university. This includes Pro-Vice Chancellor of Health Jo Lane, who Liz says was a key driver in getting the course established.
Final approval for the programme came in the first week of November 2024 – so they started advertising for students. While there was a lot of interest, it was too short notice for most and the programme ended up with seven enrolments.
Starting in January 2025, the teaching team of five had six weeks to get prepared before the course began on 10 February. “I want to acknowledge the support of the university to run it with only seven students because that’s been really good for us,” says Liz. She explains that it has allowed the teaching team to be flexible and troubleshoot the course as it’s being established – and the cohort has been very generous with letting them try new things.
The students have three weeks of on-campus theory learning before going out to their first fourteen-week clinical placement with a Lead Maternity Carer. This enables the students to have clinical experience to support theory, says Talei. “This means that when the 2025 cohort came back for their next campus block, we could rediscuss some topics and how they apply to practice. I love it, it’s so dynamic. No lesson is the same. It is exciting to hear what the students add into the teaching and the conversations – essentially, we are learning from them as well.”
Liz adds: “The challenge for us is to try and make the teaching as dynamic and interactive as possible. We are always considering how best to engage students in ways that are meaningful and relevant to their practice, acknowledging their lived experience as health professionals and the knowledge they bring with them. We’ve been to a conference recently and learned about gamification and learning. So we’re looking at trying various things like that and integrating simulation better into the programme.”
The first weeks of theory are “intense” –most other programmes have longer in-class time before going out to clinical placements. As with all midwifery students the Waikato students described those three weeks as “challenging” and “exhausting”. But they also acknowledged how beneficial it was to them feeling ready to go out on placement. While they’re going out earlier than other programmes, it’s helping them recognise they come with a lot of transferable skills, says Liz.
The lecturers add that enrolling for the programme is a huge challenge for these students, as they go from having a wealth of experience in their previous profession to
then going back to studying, while also working part-time and managing family commitments. “It’s courageous to step into this brand-new programme and to step down from full-time work to only being able to work two days a week, especially in the current financial climate,” says Talei. She and Liz are looking forward to what this year will bring: a new batch of students and, in December, their first graduates. They also acknowledge the resounding support of the midwifery profession for the new course and its students throughout the first year.
Similar graduate courses are also under development at AUT and Victoria University of Wellington. At AUT, Tania Fleming has been leading the charge. She says AUT is one of the country’s largest producer of midwives via its undergraduate degree, with 106 in 2024 and 86 in 2025. While the undergraduate midwifery bachelor’s programme will continue to remain as the means by which the vast majority of New Zealand midwives are educated, the graduate programme offers an alternative option, which Tania believes will be a powerful addition to the university’s current midwifery education pathway.
AUT already offers three other graduate programmes – in nursing, physiotherapy and occupational therapy – which have been great for attracting a diverse range of students with prior experiences. “We think it’s a really exciting pathway, opening up to a broader group of people who can only enhance our profession,” says Tania.
For Liz, one of the most powerful pieces of feedback from the 2025 cohort has been hearing that the students feel they have “found their place”. She says, “And for some of them, midwifery was their first love, but something got in the way and they didn’t get there… and now they’re finally able to realise their passion”.
That’s certainly the case for Nelson-based nurse Kim Caradus, who joined Ashly as one of the seven enrolments in 2025. Her journey to becoming a midwife began when she was about six. “I remember visiting a family friend who went into labour while we were at the house,” says Kim. “All of a sudden the midwife came blasting through the kitchen door, she seemed like a superhero.”
Midwifery has percolated in the back of her mind ever since, but it would be 30 years before her dream of becoming a midwife was finally realised.
She tried a couple of times to enrol for midwifery. The first time she fell pregnant herself, the second time, the intake at Ara Institute of Canterbury was full. “Obviously it wasn’t the right timing, so I shelved it again. Then we ended up moving to Melbourne,” Kim explains.
They came back to Aotearoa during the Covid-19 pandemic and she completed a nursing degree. At the end of her first year as a nurse in 2024, she had a serendipitous conversation with Nelson Hospital’s director of nurses and midwifery Sandy McLeanCooper, who told her about Waikato’s new graduate midwifery programme. The best part? She didn’t have to move her entire family to Hamilton to do it. It sounded too good to be true, admits Kim. “One thing led to another, I was all signed up and arriving in class for my first week. I was pretty amazed at how smooth and straightforward the process was. They were really supportive.”
Speaking at the end of her first year, Kim says she’s loved every second. “Obviously, there’s been some challenging moments when you’re driving home at 2.30am from a birth. But even in the midst of all that, there’s been this sense of joy of knowing I am doing the right thing, and I am at the right place at the right time.” She acknowledges the support she’s had, not just from the midwives she’s been on placement with but also her tutor, Talei. “Besides, there’s nothing quite like the moment when you catch your first baby – it’s like time stands still, despite all the checks and procedure that needs to happen next,” says Kim.
What she loves the most about midwifery is the connection between midwife and women. “I love that midwifery encourages women’s own voice and their own desires and wants, and that a midwife is supporting that to the best of their ability, while still keeping the woman and baby safe.” Square
Liz James, Head of Midwifery and Talei Jackson Senior Midwifery lecturer at the University of Waikato.
RAROTONGA CELEBRATES BFHI ACCREDITATION
HAYLEY MCMURTRIE EDITOR/COMMUNICATIONS MANAGER
Rarotonga Hospital has achieved full Baby-Friendly Hospital Initiative (BFHI) accreditation, marking a major milestone for maternal and newborn health in the Cook Islands and showing leadership in breastfeeding support across the Pacific region. The achievement follows months of dedicated work by local maternity staff, supported by New Zealand midwife Karen Palmer and the New Zealand Breastfeeding Alliance (NZBA).
BFHI, a joint initiative of WHO and UNICEF, sets out evidence-based standards that protect, promote and support breastfeeding in maternity services.
Accreditation signals that a facility is providing optimal care for mothers and babies, from education during pregnancy through to care in the postnatal period, with practices that support skin-to-skin contact, informed feeding decisions and ongoing breastfeeding success.
Karen Palmer talks to Editor Hayley McMurtrie about assisting the health team in Rarotonga achieve BFHI accreditation.
“Rarotonga is my favourite place to visit,” says Karen, whose first trip was in 1978 as a student nurse. During a 2019 visit, she visited the maternity unit and enquired whether New Zealand midwives ever volunteered on the island. That conversation quickly shifted into the unit’s desire to work toward BFHI accreditation.
The Cook Islands has a Health Visiting Specialist (HVS) programme, which brings specialist clinicians to the islands to provide clinical services and train
local staff. Although the project was delayed by two years due to Covid-19, the programme ultimately provided the pathway for Karen’s involvement.
“Cook Islanders are New Zealand citizens and are entitled to access New Zealand health services if they need to be transferred offshore. However, this process is costly, which is why there is a strong focus on upskilling local staff,” Karen explains.
Karen’s first formal visit eventually occurred in 2021 for two weeks, the standard HVS timeframe; however it soon became clear this would not be long enough, and Karen later returned for a six-month placement in 2024, and a final one-month visit in 2025.
During her extended placement, Karen worked closely with midwives and nurses to refresh breastfeeding education, update and implement policies, and strengthen consistency of care.
Her work included establishing a dedicated postnatal home visiting service, now written into policy and widely valued by local families. “I carried out this work myself for the first two months, until a midwife was available. I thoroughly enjoyed this part of the
Right: Maryann checking a baby during a postnatal visit
The Cook Islands News recently reported that WHO has praised Te Marae Ora for its leadership in improving maternal and newborn health across the region, particularly through its commitment to safe, high-quality care and breastfeeding-friendly practices.
Achieving BFHI accreditation places the Cook Islands among a small number of Pacific nations to meet these internationally recognised standards.
mahi,” says Karen. Finding homes was a challenging part of the role, she laughs as she recalls the first visits she made. “There are no letter boxes, street numbers or street names. Forget Google maps! Instructions were often...‘take the back road, turn right at the big mango tree next to water tank, go past the taro patch and it is the blue house behind the trees’.”
“I instigated guidelines of practice for home visiting, focusing on key days of assessment to ensure infant wellbeing. These were day three (if early discharge), day five, day 10, week two and so forth. Large neonatal weight losses and jaundice were common but we managed to get on top of this problem and give more support and care in the early days postpartum. This service is now going strong, and as it is written into the BFHI Policy, it will stay,” states Karen.
Karen also supported the maternity team to shift from task-focused care to more baby-led and vaine | woman-centred practice. Previously, skin-to-skin contact typically occurred for an hour once newborn procedures were completed, rather than the hour immediately after birth
that is recommended by BFHI. Through demonstration and mentoring, Karen helped staff embrace immediate skin-to-skin and facilitated the introduction of skinto-skin in theatre and recovery, a change now described as transformative for both mothers and staff. “Once the staff saw the results of babies doing the breast crawl and self-latching, they were amazed and now it is routine practice.”
“Skin-to-skin in theatre or recovery was non-existent. The baby would be born, then go back to the ward to stay with family. The māmā often didn’t see her baby for hours. With the support of the local anaesthetist, we managed to change this practice and now baby goes skin-to-skin in theatre and again in recovery.” Seeing māmā and pēpi returning from theatre together, having never been separated, was one of Karen’s highlights.
One of the many barriers Karen found, however, was a lack of warm towels for skin-to-skin. “There is barely any linen on the maternity unit, so I asked family to bring Kmart towels out when they visited. We take supplies for granted here in New Zealand,” says Karen.
Karen with Marere Smith from Hapū Wānanga Waikato who attended the Cook Islands Annual Health Conference, to share and receive insights for delivering services.
“Another challenge,” Karen adds, “was helping the staff understand when supplementation was needed and how to do it safely without compromising breastfeeding. They had practised a no formula or bottles policy for many years, no matter what the circumstances or the mother’s wishes. Now there is more understanding around feed assessment, risk factors and informed choice and consent. BFHI was never about no formula ever, just no routine or inappropriate use of formula.”
Local leadership through Te Marae Ora was vital throughout the process. Karen notes that the maternity team brought deep cultural knowledge and a strong whānau-centred approach, with staff deeply committed to better outcomes for babies and mothers.
Outside of the hospital, Karen collaborated with a group of passionate vaine to support the establishment of Nui, a communitybased antenatal education programme led by midwife Rereao Vano and supported by Karen’s Hapū Wānanga colleagues in Aotearoa. These classes continue to thrive and strengthen community understanding around breastfeeding and infant wellbeing.
In mid-2025, NZBA assessors Cara Hafner and Carmen Timu-Parata travelled to Rarotonga to conduct the formal BFHI assessment. They observed clinical practice, reviewed documentation, spoke with staff and mothers, and assessed the service against the Ten Steps to Successful Breastfeeding.
Their findings reflected a service that had worked hard, embraced new knowledge, and demonstrated strong alignment with BFHI standards. Home-based interviews with mothers gave assessors rich insight into lived experiences and reinforced the impact of recent practice changes.
NZBA’s Executive Officer, Jules Wilke, later travelled to Rarotonga for the presentation of the accreditation certificate, acknowledging the joint efforts of Te Marae Ora, local staff, Karen Palmer and NZBA in achieving this milestone.
The Cook Islands News recently reported that WHO has praised Te Marae Ora for its leadership in improving maternal and newborn health across the region, particularly through its commitment to safe, high-quality care and breastfeeding-friendly practices. Achieving BFHI accreditation places the Cook Islands among a small number of Pacific nations to meet these internationally recognised standards.
Karen notes that the shift to breastfeedingfriendly practices is already influencing
broader maternal health policy. For example, maternity leave, previously six weeks, will be expanded to three months, making continued breastfeeding more feasible for working mothers.
LOOKING AHEAD
Te Marae Ora and NZBA remain committed to ongoing collaboration to maintain BFHI standards, support refresher training, and share learnings with neighbouring Pacific nations. NZBA also continues to mentor Elina Henry, the Cook Islands’ BFHI Coordinator.
Karen’s experience in Rarotonga highlights what is possible when local leadership, cultural knowledge and external expertise come together with a shared purpose. For her, the highlights were grounded in people, the humour, the flowers worn daily, the shared meals and the deep connections formed over many months.
Rarotonga’s BFHI success stands as both an achievement and an invitation: a model of partnership and Pacific-centred maternity care that can inspire similar progress across the region. Square
The Baby-Friendly Hospital Initiative (BFHI) is a WHO/UNICEF global initiative to promote best practice for breastfeeding worldwide. This is summarised in the core principles of BFHI through the Ten Steps to Successful Breastfeeding (revised in 2018 and adapted for Aotearoa NZ). https://www.babyfriendly.org.nz/ resource/whounicef-ten-steps-tosuccessful-breastfeeding
WHY BFHI MATTERS
BFHI-accreditation has been shown to:
Increase breastfeeding initiation and duration.
Improve infant health, especially in the early months of life.
Support maternal confidence and wellbeing.
BABY-FRIENDLY HOSPITAL INITIATIVE (BFHI)
Karen, with Rereao Vano, who delivers the successful Nui Education programme in Rarotonga.
NEW GRADUATE MIDWIVES AND MANAENHANCING PRACTICE
TERINA JOSEPH MĀORI MIDWIFERY ADVISOR
Working alongside new graduate midwives in the Midwifery First Year of Practice (MFYP) programme is both a privilege and an honour. To witness their growthfrom tentative beginnings to increasing confidence in their clinical skills, decision-making, and professional identity - is deeply inspiring. Their commitment to women, pēpi and whānau, and their drive to strive for excellence in midwifery practice, reflect the strength and future of our profession.
During workshops with new graduate midwives, I often find myself reflecting on my own first year of practice. More importantly, I think back to the incredible midwives who wrapped me in their korowai of support, guidance and aroha until I grew into my confidence. Those midwives are forever etched in my midwifery heart.
REFLECTION AND CELEBRATION OF PRACTICE
Preparation for Midwifery Standards Review begins early in the new graduate year. By the final MFYP workshop, many graduate LMC midwives are engaging in meaningful reflection on their own statistics, using
them as a way to celebrate growth and development across the year.
For core midwives, reflecting on individual statistics can be challenging as they practise within a collective model of care. Instead, they often explore regional or national data, reflecting on how their own practice fits within these broader trends.
During one MFYP workshop, we explored Te Whatu Ora’s most recent national maternity data together. This activity sparked deep discussion, particularly when we examined caesarean section rates across Aotearoa. As we moved through the data, a palpable buzz filled the room, followed by concern.
CAESAREAN SECTION BIRTH: A RISING TREND
Birth remains a powerful and sacred moment: the transition of a pēpi into the world, where tinana (body), wairua (spirit), ngākau (heart/soul) and mauri (life force) converge.
The data showed that approximately 33% of babies born in Aotearoa are now born by caesarean section. This reflects a steady increase over the past 16 years, a trend mirrored internationally. The World Health Organization (WHO) reports that globally, one in five births (21%) occurs by caesarean section, compared with just 7% in 1990.
As midwives, we are compelled to reflect critically on this trend. We ask ourselves: Why is this increase occurring? Is it
influenced by lifestyle factors, diet, increasing medicalisation of birth, or a complex combination of many elements? And importantly, what is our role as midwives in responding to this shift?
The conversation soon turned to the sacredness of birth and how this is experienced within an increasingly medicalised landscape. While acknowledging that birth is birth, regardless of mode or place, we reflected on how the rising caesarean rate may impact the experience of wāhine and whānau.
Birth remains a powerful and sacred moment: the transition of a pēpi into the world, where tinana (body), wairua (spirit), ngākau (heart/soul) and mauri (life force) converge.
UPHOLDING
THE
MANA OF BIRTH
A question emerged during discussion:
As midwives, how do we uphold the mana of birth, the mana of the wahine and her whānau, within the medicalised environment of a caesarean section theatre, often characterised by white walls, bright lights, and restrictions on whānau presence?
Tūranga Kaupapa, our cultural framework guiding midwifery practice, identifies mana as a core element:
“The dignity of the wahine, her whānau, the midwife and others involved is maintained.”
When we explore this more deeply, we are invited to consider how dignity and mana can be actively upheld within the caesarean space. While many midwives already practise this intuitively, there remains scope to further support and encourage culturally safe, manaenhancing practices.
MANA OF THE WĀHINE
I recall a powerful presentation at Ngā Maia Hui-ā-Tau in Tauranga 2023, delivered by respected traditional Māori birth attendant Sarndra Mear. She described the womb as a sacred, unopened universe, capable of creating life. Following a caesarean section, the womb is physically and spiritually opened, leaving the mother vulnerable.
Sarndra spoke of offering karakia to spiritually close the womb after birth, acknowledging the profound journey undertaken to bring new life into the world. This act enhances the mana of the māmā, pēpi and whānau, honouring both the physical and spiritual dimensions of her care and birth.
MANA OF THE WHĀNAU
I have heard the piercing karanga of a newly made Nan during a caesarean birth, its sound sending chills through the room.
The karanga, likened to the instinctive vocalisations of wāhine during birth, is understood to be so powerful that it reaches the spiritual realm, calling tūpuna to witness the arrival of new life.
In that moment, the Nan welcomed her mokopuna from the darkness into the light, from the spiritual realm into the world of the living, offering pēpi their first pōwhiri, ki te ao mārama.
Karakia is another tool that can be offered or encouraged during caesarean births. It can support whakawātea and whakatau—helping māmā, pāpā and whānau to relax, to draw strength from their spiritual beliefs, and to ease anxiety so they can focus on the miracle unfolding before them.
MANA OF WHAKAPAPA
Whakapapa recitation can soothe a māmā, reminding her of the mana of the mahi she is doing, continuing ancient ancestral lines. Oriori, softly sung or spoken, can calm both māmā and pēpi, speaking of the love awaiting them, the possibilities of the world ahead, and the atua who will guide and protect them. Many midwives have witnessed pounamu or tūhua used, with karakia, to cut the umbilical cord, alongside a muka tie at the resuscitaire. These practices reflect the
weaving together of ancestral knowledge and contemporary clinical care.
More recently, I heard of a māmā who requested the return of her sacred waters and toto (blood) following a caesarean birth. With planning and obstetric support, this was approved, allowing her to return these fluids to Papatūānuku - an ancient practice honouring whakapapa and the belief that all things come from mother earth and are returned to her.
CONCLUSION
What began as an exploration of national maternity statistics during an MFYP workshop became a deeper reflection on how we, as midwives, can uphold the mana of birth within the white, sterile walls of the caesarean section theatre.
This is a merging of two worlds - a weaving of ancient whakapapa with modern medical practice. Each caesarean birth remains a birth story: one of courage, strength, and love. A story of a māmā bringing new life into the world, and the arrival of an emerging rangatira carried forward by the tides of their tūpuna.
As midwives, we have the privilege and responsibility to help create mana-enhancing spaces where culture, dignity and wairua are honoured, no matter the mode or place of birth. Tihei Mauri Ora. Square
ANKYLOGLOSSIA TONGUE TIE:
BREASTFEEDING ASSESSMENT AND SUPPORT, AND AN EVALUATION TOOL
The College consensus statement on ankyloglossia (tongue-tie) has recently been reviewed and updated, with new references added. The statement has been approved by the National Board and is now awaiting formal ratification (NZ College of Midwives, 2025).
As described in the updated consensus statement, the College supports the provision of a free, equitable and accessible service for the release of neonatal tongue-tie if this condition is impacting negatively on breastfeeding. Frenotomy is not always necessary even when a tongue-tie is diagnosed in a neonate, so accurate assessment, diagnosis, breastfeeding support and timely decisions about referral are not only key drivers of the avoidance of maternal and/ or infant pathology but also significant for breastfeeding continuation and the confidence and wellbeing of the breastfeeding mother.
Breastfeeding is an interaction between the mother and her infant, and there are many factors other than tongue-tie that need to be considered when managing breastfeeding difficulties. Midwives have a range of skills to assess and support breastfeeding, to assist with improvement of latch, positioning and breast milk supply issues, and to provide evidence-based information to parents.
Midwives can assess for and identify tongue-tie using an accredited tool, then support breastfeeding continuance accordingly. Observation of breastfeeding and subsequent evaluation requires a userfriendly, comprehensive assessment method that works well for midwives.
If a frenotomy is necessary, it should be done in a clinical setting where two practitioners are present, with a process in place in case of unexpected events such as bleeding. If parents have chosen for their infant not to receive Vitamin K after birth, frenotomy is not recommended, and
continued breastfeeding support is advised (MOH, 2020). If a later decision to give Vitamin K is made, a frenotomy needs to be delayed by at least 12 hours after the infant has received intramuscular Vitamin K.
BACKGROUND
Tongue-tie (ankyloglossia) is a congenital condition characterised by a short or tight lingual frenulum that may restrict infant tongue movements and cause breastfeeding challenges. Estimated incidence has been reported as between 4-11% of newborn infants (O’Shea et al., 2017). A meta-analysis has reported a prevalence rate of 8% in infants below one year (Hill et al., 2021). It is possible that the reported prevalence variability may be due to the variation in diagnostic criteria and different assessment tools but the rates of overdiagnosis are unknown. Mills et al. (2019a) have noted the increasing numbers of infants diagnosed with ankyloglossia, alongside a growing uncertainty about ‘normal’ lingual frenulum anatomy, resulting in the diagnosis remaining subjective. This subjective diagnosis issue presents “a major dilemma for both clinical practice and research, as well as potentially creating parental confusion” (Mills et al., 2019a, p. 825).
Social media platforms providing information about ankyloglossia were assessed by Booth et al. (2024) who found a high frequency of content misinformation. They described this misinformation as “not benign” and likely causing a substantial number of unnecessary procedures (p. 149). A crosssectional analysis on the publicly available
TikTok videos, using the term tongue tie, found the mean number of views for the top videos was 1.4 million with a mean of 88,009 ‘likes’ and 781 comments (Mozzochi et al., 2025). Frenotomy experience was the most common theme, with the next most popular being how to identify a tongue-tie. Breastfeeding was the most common secondary theme. The analysis highlights a high degree of public concern and, as explained by Mozzochi et al. (2025), while social media can create supportive communities and raise awareness, it has the potential to spread misinformation. The normal newborn finding of sucking blisters being used as a sign of tongue tie issues is an example of such misinformation (Thomas et al., 2024). Midwives can discuss, with breastfeeding mothers and their whānau, the information they may have been accessing on social media.
Nainer (2025) advocates for caution over surgical intervention, and notes that increases in surgery for ankyloglossia has led to advocacy to reduce these interventions. Addressing the issues of minimising both over- and under-treatment requires evidencebased guidance and standardised diagnostic tools (Delgadillo et al., 2025).
Degrees of ankyloglossia vary and while most infants with tongue-tie will breastfeed successfully, there may be challenges for a small number of infants. The band of tissue at the base of the tongue often contains the genioglossus muscle which may lengthen with breastfeeding, resulting in infant feeding ability improving with time (Mills et al., 2019b). Mills et al. (2019a) have conducted anatomical studies of the tongue and emphasise that ankyloglossia cannot be diagnosed purely on the appearance of the frenulum. They recommend that assessment and grading systems based solely on appearance should not be used. Mills et al. (2019b) also suggest that the term posterior tongue-tie is anatomically incorrect and should be discontinued.
MIDWIFERY ASSESSMENT
Reviewing birth events is part of a feeding assessment, particularly in situations where there are emerging breastfeeding challenges. Midwives are in a prime position to consider birth impact, observe breastfeeding and assess breastfeeding progress from birth, taking into account potential issues that can cause feeding challenges, such as a difficult birth, infant resuscitation, infant suction, maternal analgesia, token or no mother-infant skin-toskin contact, and growth restriction. Infant observation, to check face symmetry, infant
CAROL BARTLE POLICY ANALYST
muscle tone and for issues such as a chin that appears to recede more than expected, can provide some key insights for the evaluation. At the same time, maternal anatomical variability that could potentially impact latching, such as nipple size and elasticity, should be included in the assessment as they are potential compounding variables. Female breasts and nipples come in all shapes and sizes and adjustments to latch and position may need to be made to ensure the ‘fit’ between mother and infant is as optimal as possible. In the vast majority of situations, the mother will start off with the capacity to develop a full lactation but there are issues that can derail this process. When babies are not latching at the breast there is a significant risk of loss of breastfeeding exclusivity and a shortened duration of breastfeeding, so the aim is resolution of any feeding issues as soon as possible, while protecting the development and maintenance of a full lactation.
BREASTFEEDING EVALUATION AND SUPPORT
When assessing a breastfeed, the latch and how the infant ‘holds’ the latch is important to note, as is the observation of nipple appearance when the nipple is released. It is important to ask questions about pain during feeds, listen for any unusual noises made when the infant is suckling, and check milk transfer for the full duration of the breastfeed. Is it sustained for most of the feed or only when the milk is flowing, for example. The answers add more information to the broad observation. An obvious but often missed issue causing latching problems for the infant and the mother is caused by the infant being unable to instinctively tilt the head backwards to ensure the chin is against the breast – usually caused by the mother’s arm placement or a hand behind the head. This can result in a latch that is not deep enough to effectively remove milk, and that can cause nipple damage and reduced milk supply.
Working with an individual woman’s breast size and shape is important. Women with small breasts find an oblique position helpful, whereas larger breasted women may benefit from an across or underarm position. In some situations where there is anterior breast fullness, an inverted side lying position may be necessary for a few feeds until the breasts soften and the infant achieves some feeding success.
Positional instability can cause the infant to back arch, cry and fuss at the breast, and/ or refuse to breastfeed. Positional instability
KEY POINTS AND PRACTICE GUIDANCE
Breastfeeding is an interaction between the mother and her infant, and there are many factors other than tongue-tie that need to be considered when managing breastfeeding difficulties.
Infants with possible symptomatic tongue-ties need comprehensive breastfeeding observation, monitoring and continued support for breastfeeding and lactation.
Identification of a tongue-tie which is causing feeding problems can be made by a midwife during complete breastfeeding observations. An evidence-based tool such as the Bristol Tongue Tie Assessment (BTAT; Ingram et al., 2016), or Tongue Tie and Breastfed Babies (TABBY; Ingram et al., 2019) can be used in conjunction with breastfeeding assessments.
Performing limited simple lingual frenotomy using an approved assessment tool and technique is within the scope of practice for midwives who have completed specific training (Midwifery Council, 2016).
Infants who have not received Vitamin K cannot have frenotomies.
Infants with complex tongue-ties or babies with any medical or relevant physical conditions require referral to a specialist (Midwifery Council, 2016).
Conditions often referred to as posterior tie, upper lip ties, buccal ties, lower lip ties or after treatment stretches have limited or no evidence to support diagnosis or treatment (Mills et al., 2019b; New Zealand Dental Association, 2018; Shah et al., 2020).
An infant with a tongue-tie may benefit from a style of feeding that supports instinctive behaviours and feeding cues, such as mother-infant skin-to-skin contact extending into the postnatal period, and the laid-back position for breastfeeding which decreases nipple pain and trauma and supports effective latching position (Brimdyr et al., 2020; Colson, 2005; Wang et al., 2021; Widström et al., 2020).
Skilled breastfeeding support and management takes precedence over surgery and should be the first line of intervention - this includes clinical assessment, modifying the latch and the position of the infant, assessing the milk intake, monitoring infant weight gain and output, treating sore or damaged nipples, and protecting lactation as necessary (LeFort et al., 2021; Ministry of Health, 2020; Watson-Genna et al., 2017).
Shared decision making between the midwife, mother and her whānau includes discussion about the risks and benefits of all aspects of management, informed consent and decision making, assessment and documentation of care and follow-up.
Sucking blisters are a normal finding in newborn infants, and do not indicate pathology (Thomas et al., 2024).
is when the infant signals either subtle or significant discomfort, and experiences challenges with motoric postural control. This usually occurs when the infant is desperate to feed, and too distressed to stay in an optimal position (Douglas, 2016). There are modified cradle, laid back and side lying positions that can be utilised to support babies who are having difficulties with latching.
An infant needs to be well supported to adopt an instinctive posture to latch and feed well, be mostly prone and facing the mother’s body, with the head free to move. The infant’s head will instinctively tilt backwards to latch if there is no obstruction behind the head, and the body needs to be in contact with the mother – knees, chest, and chin – these are touch points that assist the infant to find the breast.
AN ASSESSMENT TOOL FOR DIAGNOSIS
It is within the scope of practice of a midwife to identify and assess for tongue-tie using an accredited tool, to provide information to parents, and to treat or appropriately refer, using an informed consent model of care. Some regions of Aotearoa have a free assessment and treatment pathway service. The specialised, multi-disciplinary pathway in Canterbury, for example, provides a consistent and expert model of care.
Identification of a tongue-tie which is causing feeding problems can be made by a midwife during full breastfeeding observations. The assessment can be made using an evidence-based tool such as the Bristol Tongue Tie Assessment (BTAT; Ingram et al., 2015a; 2015b) and Tongue Tie and Breastfed Babies (TABBY; Ingram et al., 2019), alongside skilled breastfeeding assessment and support. The TABBY Tool provides a good visual assessment guide, is generally considered to be practical and clear, and it was produced in response to requests to translate the BTAT into pictorial form (Ingram et al., 2022). The authors state:
Assessment of tongue-tie is enhanced by using structured assessment tools to evaluate breastfeeding and the severity of the tongue-tie combined with clinical judgement and a discussion with the mother about the comfort and perceived efficacy of breastfeeding. The visual assessment TABBY Tool can be found at https://link.springer.com/article/10.1186/s13006-019-0224-y.
Common pitfalls to avoid when using the BTAT score are relying solely on the BTAT without assessing breastfeeding difficulties; inconsistent technique when examining different components; failure to document baseline scores before intervention; not reassessing after frenotomy to document improvement; and overlooking other causes of feeding difficulties beyond tongue-tie.
The S position - the infant’s ears, shoulders and hips are in alignment, with the body forming an S curve.
PROBLEMS FOLLOWING A FRENECTOMY
Frenotomy is not a risk-free surgical procedure. Mills et al. (2019a) report that infant pain requiring treatment with analgesia can last for up to 13 days following a frenotomy and that the pain experience is likely to be influenced by factors such as depth and size of the wound and whether any post procedure wound interventions are used. They also highlight that pain associated with frenotomy and post frenotomy, wound treatment, such as massage/stretches, can potentially create an oral aversion in some infants. This is a serious complication as feeding aversions may lead to malnutrition, impaired growth, and long-term feeding disorders that are difficult to resolve.
An investigation of the incidence and complications arising from frenotomy using data from the NZ Paediatric Surveillance Unit over a two-year period, found 23 notifications relating to frenotomy in infants under one year old, with a mean age of procedure at 32 days (Hale et al., 2019). Complications post-frenotomy included poor feeding, apnoea and breathing difficulties, and pain and bleeding, with the majority of affected infants requiring hospital admission. One case was described as highlighting the potential complexity and importance of considering underlying causes of feeding issues: …a 4-week-old male who had an apnoea during his procedure. The subsequent admission for this complication leads to a diagnosis of congenital heart disease and associated poor weight gain.
A dentist had performed laser surgery to release lip and anterior tongue-ties, having been referred by a lactation consultant. No vitamin K had been given at birth, and the performing clinician was unaware of the risk of vitamin K deficiency bleeding” (pp.560-561).
Mills et al. (2019a) encourage a considered clinical approach that includes ruling out other potential causes of breastfeeding difficulties before proceeding to surgical intervention.
CONCLUSION
Due to concerns about over-diagnosis and unnecessary treatment, a Ministry of Health guideline was developed in 2020 to provide clear and consistent guidance to the health sector to support identification, assessment, diagnosis and treatment of tongue-tie. A statement concerning the midwifery scope of practice with regard to tongue-tie was issued by Te Tatau o te Whare Kahu Midwifery Council in 2016. However, it has been disappointing to note the limited data available on the incidence, treatment and follow-up outcomes of infants with tongue-tie in Aotearoa New Zealand, considering the concerns about over-diagnosis and over treatment. In June 2025, a NZ Herald article about the increase in frenotomy surgery contained a statement from the Ministry of Health that indicated an audit was not planned and there were no plans to mandate private providers to collect or share data on frenotomy procedures (Brown, 2025). The urgent need for good data makes these decisions inexplicable.
Midwives can provide full, ongoing breastfeeding evaluation with breastfeeding and lactation support and utilise practical and clear assessment guidance such as the BTAT/TABBY resource. If a specifically trained midwife undertakes a tongue-tie release procedure, reassessment of breastfeeding, observation of maternalinfant wellbeing and documentation, including whether there has been any improvement after frenotomy, are essential. Square
Acknowledgement: Some content in this article has been adapted from a previous Midwife Aotearoa article on tongue tie, co-written by Karen Palmer. Issue 110 September 2023. References available on request
Are you a dedicated LMC with a passion for rural care, eager to join a close-knit, small rural team based in Dannevirke?
Tararua Health Group offers a 3-bed maternity unit within the Dannevirke Community Hospital. We provide comprehensive continuity of care for women throughout antenatal, labour, birth, and rural/remote postnatal care.
About your new role:
Roster: A balanced schedule with a 24-hour roster of 4 days on/4 days off. Accommodation: The option to stay at our Maternity Cover House at no cost. Team: Be part of a supportive and welcoming team committed to exceptional rural and remote care.
Travel: If you’re from out of town and need assistance with your travel expenses, we’re happy to discuss a travel allowance.
You will have the following skills:
Experience: An experienced midwife seeking a move to a rural environment. Skills: Strong clinical skills and a compassionate approach to care.
Professional Requirements: Current APC, Indemnity and Vulnerable Children’s Check.
You will be a team player with a sense of humour, excellent bedside manner and bundles of enthusiasm. Your energy and understanding will be vital in providing exceptional care for our newest arrivals and their mothers.
Apply today and become a valued member of our team to tanya.holak@omnihealth.co.nz or call Tanya on 027 320 5616.
Comfort and safety for babies newborn-2 years
More restful, safer sleep and helps prevent flat head
• More restful, safer sleep limb and hip movement
Goes over any type of swaddling, sleeping bag or sleepwear, for a snug and more restful sleep
• Ensures swaddling, sleepwear, Sleepingbag use is safer and cosier
Natural, flexible body, limb and hip movement
• Excellent for babies requiring varied sleep positions or cot elevation est
Helps keep young babies comfortably o the tummy; older babies turn freely within the wrap Use code ‘NZCOM’ for 20%
www.safetslee
TAKU WĀHI MAHI MY MIDWIFERY PLACE -
DANNEVIRKE MATERNITY UNIT’S COMMITMENT TO COMMUNITY
In the rural North Island town of Dannevirke, a team of midwives run a maternity service that is truly embedded in the local community.
The midwives each have their own caseload, seeing a total of 170 to 200 women per year, while also running Dannevirke Community Hospital’s maternity unit and being on-call for any maternity emergencies or breastfeeding-related problems.
Their schedule is a busy one, but most importantly it allows for deep connections between midwives and whānau and for women to have continuity of care throughout their pregnancies.
“The women love it. We even have women who have birthed in Hastings who’ll come back to us for an inpatient stay and we take over their postnatal care,” says the unit’s manager Robyn McDougal.
Along with Robyn, there are three full-time midwives and one part-time midwife on the team. While they are on the hunt to recruit one more staff member, an additional team of five casual midwives provides locum support when needed.
Robyn has been a rural midwife for 35 years and started working with the Dannevirke team in 2012.
“I think Dannevirke is great, and the people, the midwives I’ve worked with over the years have been the attraction,” she adds.
With two midwives on shift each day, it’s a very supportive environment to work in.
“Dannevirke maternity services wouldn’t be where they are without having the midwives that we’ve had and their commitment to community. It’s definitely rural, it has autonomy, it has a level of midwifery that provides satisfaction and sustainability for the team,” says Robyn.
The team also provides advice on both conception and contraception, Jadelle insertions, early abortion care, ultrasound, and vaccinations for flu, whooping cough and rubella. Postnatal home visits see them travel as far as 100 kilometres away to small towns like Woodville, Pahiatua and Herbertville.
“It’s that team of two midwives [on shift] that makes all of this achievable,” says Robyn.
“It is a challenge when you’ve got someone due or even a couple of women due, but you go and if you have to get called back, everybody is so accommodating.”
Typically, about 35 to 45 women birth at the unit per year, with the remainder birthing at home or in secondary care.
In June 2025, a new road was built to replace the Manawatu Gorge Road and better connect Palmerston North to Dannevirke, Woodville and Ashhurst.
Before that, it was a “nightmare” to be transferred to Palmerston North Hospital over 50 kilometres away, says Robyn.
“So the community treasures what they've got. And we've got half a dozen health providers in our region who are totally committed to keeping services closer to home.”
The Dannevirke team often collaborate with the GPs and nurses at Tararua Medical Centre which is co-located at the community hospital.
“It definitely reduces the barriers for access for some of these women,” says Robyn.
Overall, for the enitre team, practising rural midwifery in Dannevirke is special.
“It’s that absolute team camaraderie and the relationships we have with the women and families” says Robyn. Square
The College has a range of midwiferyrelated books, leaflets, merchandise and other resources available through our website: www.midwife.org.nz/shop
ADVERTISING POLICY AND DISCLAIMER: The New Zealand College of Midwives maintains a schedule of guidelines to exclude advertisements for products or services that are not aligned with its principles and ethics. Every effort is made to ensure that advertising in the magazine falls within those guidelines. Where advertising is accepted, this does not imply endorsement by the College of the product or service being promoted
Midwife Aotearoa New Zealand is published quarterly for the New Zealand College of Midwives. The articles and reports printed in this newsletter are the views of the authors and not necessarily those of the New Zealand College of Midwives, its publishers or printers. This publication is provided on the basis that New Zealand College of Midwives is not responsible for the results of any actions taken on the basis of information in these articles and reports, nor for any error or omission from these articles and reports and that the College is not hereby engaged in rendering advice or services. New Zealand College of Midwives expressly disclaims all and any liability and responsibility to any person in respect of anything and of the consequences of anything done, or omitted to be done, by any such a person in reliance, whether wholly or partially upon the whole or any part of the contents of this publication. The College acknowledges and respects diversity of identities through the language used in this publication. Te reo Māori is prioritised, in commitment to tāngata whenua and te Tiriti o Waitangi. To maintain narrative flow, the editorial style may use a variety of terms. Direct citation of others’ work maintains the original authors’ language, and contributing writers’ language preferences are respected. All advertising content is subject to the Advertising Standards Authority Codes of Practice and is the responsibility of the advertiser. Contents Copyright 2026 by New Zealand College of Midwives. All rights reserved. No article or advertisement may be reproduced without written permission. ISSN: 2703-4546.
Abstract submissions open until Friday 20 March 2026