ILLNESS AND MEDICAL CARE
IN PUERTO RICO
U. S. TREASURY DEPARTMENT
PUBLIC HEALTH SERVICE
WASHINGTON, D. C.

U.
U. S. TREASURY DEPARTMENT
PUBLIC HEALTH SERVICE
WASHINGTON, D. C.
U.
By
JOSEPH W. MOUNTIN, Surgeon
ELLIOTT H. PENNELL, Associate Statistician
EVELYN FLOOR, Assistant Statistical Clerk
PREPARED BY DIRECTION OF THE SURGEON GENERAL
recinto PIEDRAS
No SE PRESTA FUERA DE LA SALA-»
For many years the municipalities of Puerto Rico have operated a system of public assistance which combines medical care and certain additional elements of relief. The system carries the official designa tion "Beneficencia Municipal." A few of the municipalities contain ing large cities erected hospitals at an early date. Provisions for public medical service in other parts of the island seldom, until recent years, included much more than care of the type that might be ren dered by a physician in his office or in the home of a patient. In addition, small sums of money may have been set aside in the budget of municipalities for the payment of hospital bills.
Shortly after the American occupation of the island there began a movement for the construction of local hospitals that finally extended to the smaller municipalities, many of which are essentially rural and extremely low in taxable resources. For reasons that svill be con sidered later the municipal system of medical care, especially in the second- and third-class municipalities, failed to develop in keeping with the standards of service desired by the medical profession and the civic leaders of the island.
Late in the fall of 1934 the Governor of Puerto Rico transmitted to the Surgeon General of the United States Public Health Service a request for the assignment of personnel who would direct an inquiiy into the character of the local medical service and be responsible for preparing a report based on the findings. Actual field work was started during February 1935 and consumed a period of slightly more than 3 months.
Two of the authors (Mountin and Pennell) were in charge of the study from the initial planning through the preparation of the report. This extensive bod^'^ of data could not have been gathered, however, except for the assistance obtained on the island. The insular health department arranged the necessary entree. Health officers, public health nurses, and sanitary inspectors, normally attached to local health units, and numbering about 60 in all, were temporarily relieved from their regular duties and assigned to the field canvass. Municipal authorities most graciously placed their records at the disposal of the study staff and other agencies supported the field work in the same generous manner. Schedules were edited and coded in San Juan by the regular clerical force of the insular health department. Comple-
tion of the clerical work and the final analysis of the data were accomphshed.in Washington by the United States Public Health Service.
Pubhshed morbidity and mortahty data were used insofar as possible, but additional information was required to supplement the picture. PEspecially was this true regarding illnesses wliich did not enter the jvital statistics records of the insular health department and those C which may not have come to the attention of physicians.
In order to obtain an expression of the amoimt of illness in the general population, and especially the circumstances under which the illness occurred, it was necessary to study a sample of the population.
A total of 5,891 families, representing 31,756 individuals, were in cluded in the group used for this study. The family schedule used in the survey made provision for a description of the members and the premises, together with detailed data regarding illness, the amount and character of medical attention, and contact with public health agencies.
The director of beneficencia, or some other responsible person in each municipality, completed another schedule of information which was used in describing the facilities for medical care available in the municipality, and the services rendered through these facilities. These items were related to figures on receipts and expenditures obtained from the auditor for the insular government. More than half the municipalities were visited by one of the authors (Mountin) for the purpose of inspecting hospitals, clinics, and other facilities maintained for the care of the sick.
A more detailed description of each element of the study, together with the findings, will be presented in appropriate sections of the report. Before these data are shown, however, certain salient facts of a general character regarding the island and its people will he given to oiient the reader. Without this information, it would be impossible for any one but a technically trained person intimately acquainted with local conditions to appreciate either the influence that social and economic factors exert on the health and lives of the people, or the types of public services which would be adapted to the local needs.
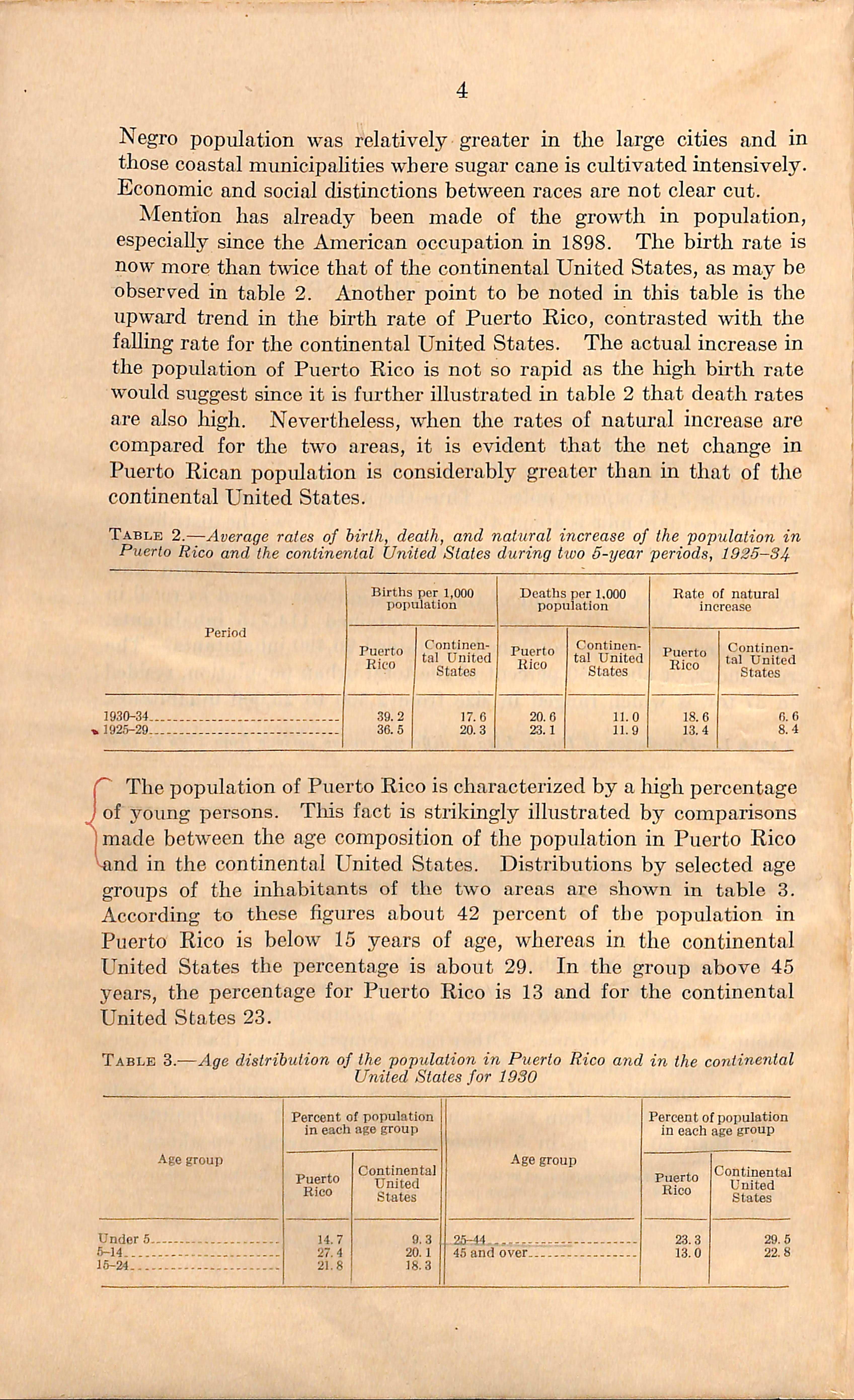
The population of Puerto Rico has increased steadily since 1765, the first year for which records were available. This may be noted in table 1. During the last intercensual period the increase amounted to nearly a quarter of a million. In 1930 the total population was 1,5^,^3. The gross area of Puerto Rico, including the adjacent islands, is 3,435 square miles. Thus the average number of inhabitants per square mile is about 450. Appendix A shows the distribution of population and the area by municipalities. The problems usually created by excess population are further intensified in Puerto Rico by the fact that 72 percent of the population was classed as rural in 1930. San Juan, the largest city, contained 114,715 inhabitants. Mayaguez and Ponce, combined, contained 90,490 inhabitants. The remainder, or about 50 percent of the total urban population, resided in 37 towns which ranged in size from 2,500 to 25,000 inhabitants.
Table 1.—Population of Puerto Rico at different census periods from 1765 to 1930'
Practically all the inliabitants of Puerto Rico are native to the island, less than 1 percent being foreign born. According to the census of 1930, about 75 percent of the inhabitants were white and about 25 percent Negroes. Other races comprised less than 1 percent of the total population. There was considerable difference in the racial composition of the municipalities, the proportion of Negro population ranging from less than 10 percent in 12 municipalities to more than 50 percent in 5 municipalities. Generally speaking, the
1 Population figuresfor Puerto Rico and for the continental United States,when used for U.S.censual years, are quoted from U. S. Census reports. When population figures are required for intercensual years, esti mate are based upon published census figures. Birth and death statistics for the continental United States are taken from annual reports of the U. S. Census Bureau and are limited to the registration area, while those for Puerto Rico are from annual reports of the commissioner of health.
(3)
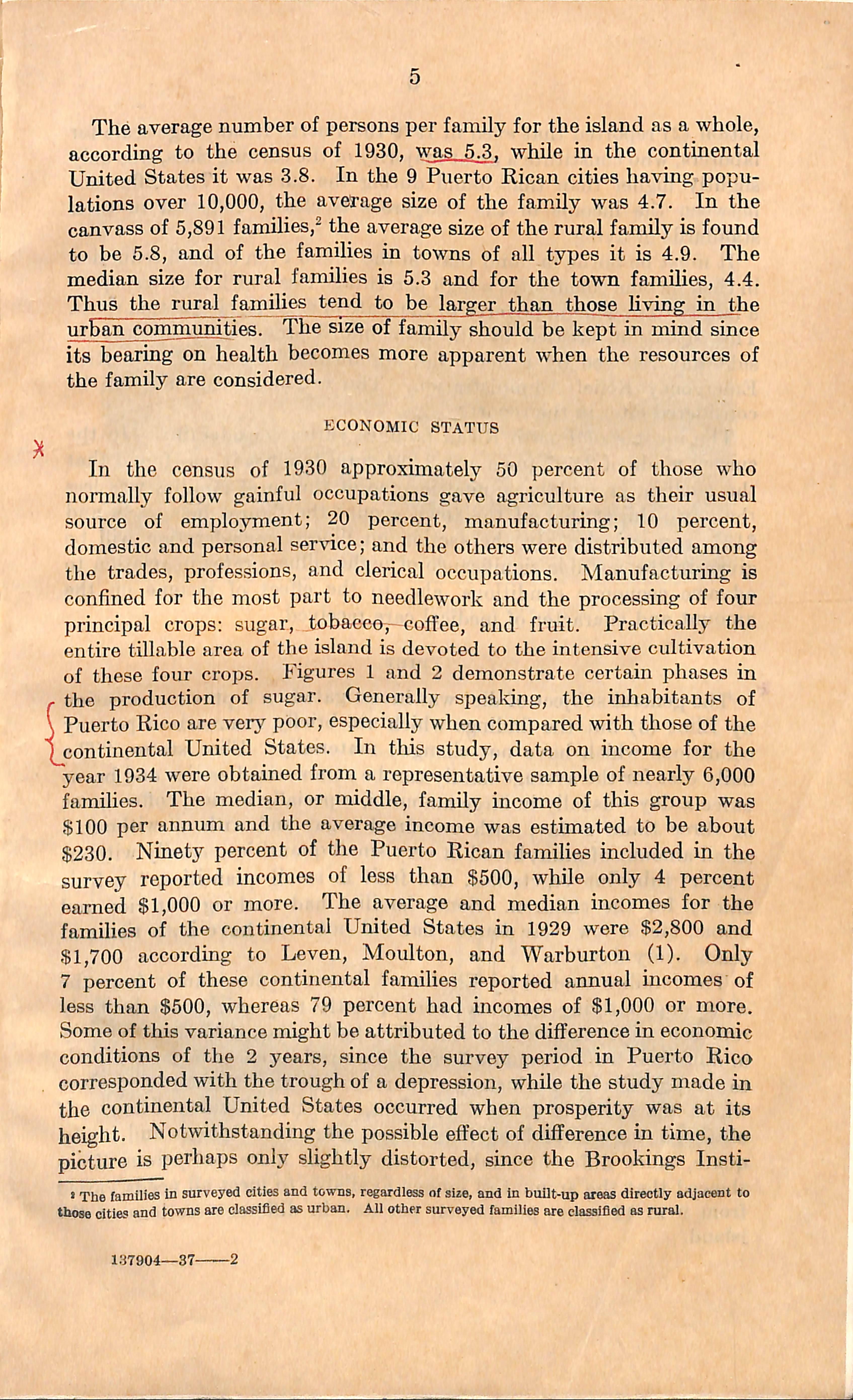
Negro population was relatively greater in the large cities and in those coastal municipahties where sugar cane is cultivated intensively. Economic and social distinctions between races are not clear cut. Mention has already been made of the growth in population, especially since the American occupation in 1898. The birth rate is now more than t%vice that of the continental United States, as may be observed in table 2. Another point to be noted in this table is the upward trend in the birth rate of Puerto Rico, contrasted with the falling rate for the continental United States. The actual increase in the population of Puerto Rico is not so rapid as the lugh birth rate would suggest since it is further illustrated in table 2 that death rates are also high. Nevertheless, when the rates of natural increase are compared for the two areas, it is evident that the net change in Puerto Rican population is considerably greater than in that of the continental United States.
Table 2.—Average rates of birth, death, and natural increase of the population in Puerto Rico and the continental United States during tivo 5-year periods, 1925-34
of young persons. This fact is strikingly illustrated by comparisons made between the age composition of the population in Puerto Rico and in the continental United States. Distributions by selected age groups of the inhabitants of the two areas are shown in table 3. According to these figures about 42 percent of the population in Puerto Rico is below 15 years of age, whereas in the continental United States the percentage is about 29. In the group above 45 years, the percentage for Puerto Rico is 13 and for the continental United States 23.
Table 3.—Age distribution of the popidation in Puerto Rico and in the continental United States for 1930
The average number of persons per family for the island as a whole, according to the census of 1930, was 5.3. while in the continental United States it was 3.8. In the 9 Puerto Rican cities having popu lations over 10,000, the average size of the family was 4.7. In the canvass of 5,891 families,^ the average size of the rural family is found to be 5.8, and of the families in towns of all types it is 4.9. The median size for rural families is 5.3 and for the town families, 4.4. Thus the rural families tend to be larger than those living in the urban comjumnities. The size of family should be kept in mind since its bearing on health becomes more apparent when the resources of the family are considered.
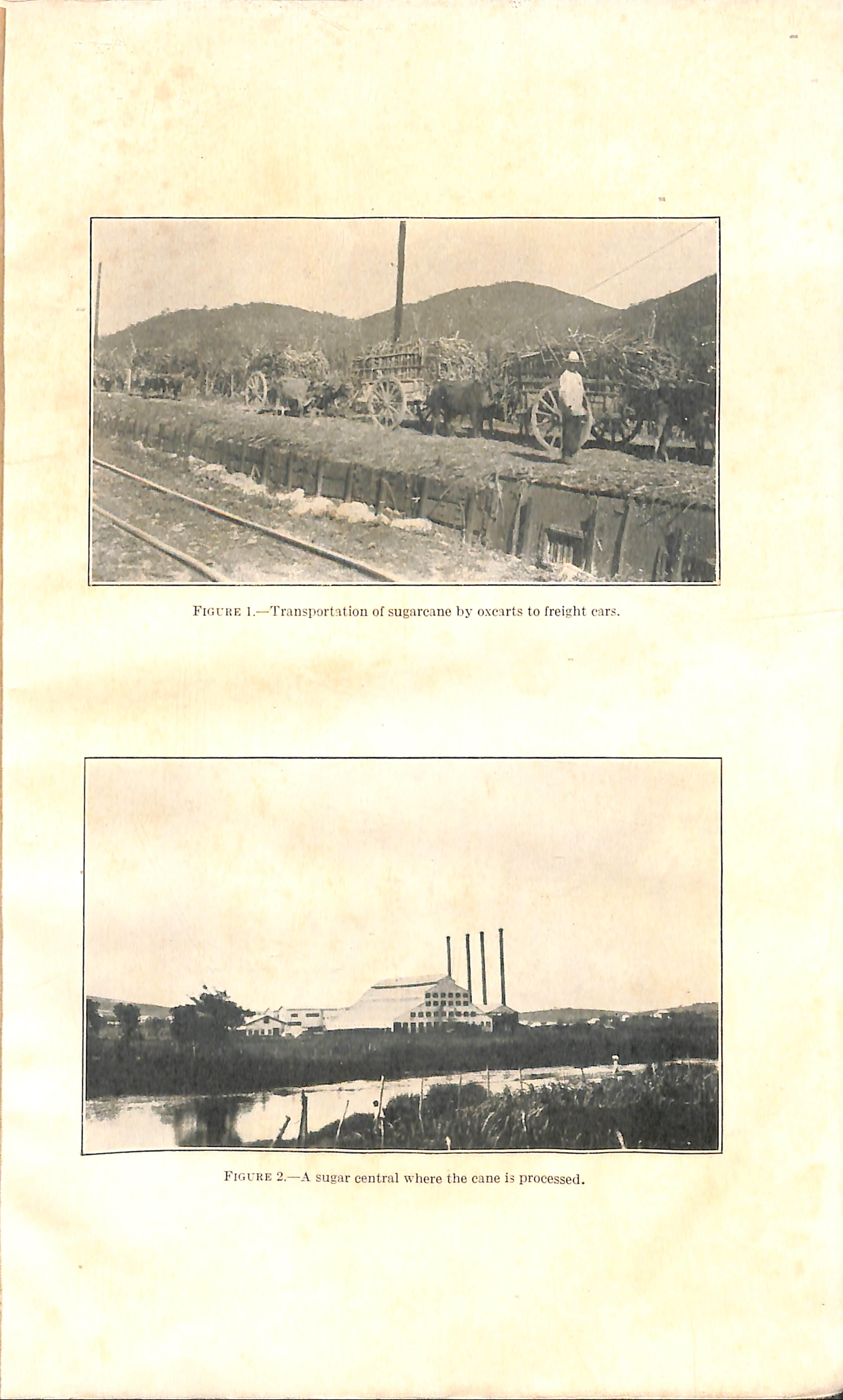
In the census of 1930 approximately 50 percent of those who normally follow gainful occupations gave agriculture as their usual source of employment; 20 percent, manufacturing; 10 percent, domestic and personal service; and the others were distributed among the trades, professions, and clerical occupations. Manufacturing is confined for the most part to needlework and the processing of four principal crops: sugar, tobaecoy-coffee, and fruit. Practically the entire tillable area of the island is devoted to the intensive cultivation of these four crops. Figures 1 and 2 demonstrate certain phases in - the production of sugar. Generally speaking, the inhabitants of \ Puerto Rico are very poor, especially when compared with those of the (continental United States. In this study, data on income for the year 1934 were obtained from a representative sample of nearly 6,000 famihes. The median, or middle, family income of this group was $100 per annum and the average income was estimated to be about $230. Ninety percent of the Puerto Rican families included in the survey reported incomes of less than $500, while only 4 percent earned $1,000 or more. The average and median incomes for the families of the continental United States in 1929 were $2,800 and $1,700 according to Leven, Moulton, and Warburton (1). Only 7 percent of these continental families reported annual incomes of less than $500, whereas 79 percent had incomes of $1,000 or more. Some of this variance might be attributed to the difference in economic conditions of the 2 years, since the survey period in Puerto Rico corresponded with the trough of a depression, while the study made in the continental United States occurred when prosperity was at its height. Notwithstanding the possible effect of difference in time, the picture is perhaps only slightly distorted, since the Brookings Insti-
'The families in surveyed cities and towns, regardless at size, and in bidlt-up areas directly adjacent to those cities and towns are classified as urban. All other surveyed families are classified as niral.
1:17904—37 2
tution (2) reported that even in 1929 the Puerto Rican wage scale for laborers, who constitute a great majority of the earning class, was only slightly higher than that found during the survey. The difference between the income of the two areas is clearly reflected in their standards of hving.
It must be borne in mind that on the island even a small reduction in cash income constitutes a high percentage loss which may transpose a family from general poverty to the state of experiencing actual want. This situation, created by the economic depression, has been con siderably relieved by Federal aid, administered by the Puerto Rico Emergency Relief Administration. The extent of this aid will he considered later in the report.
The income of Puerto Rican families varies considerably. In the survey made of 2,597 town and 3,294 rural families it was found that the median, or middle, annual income of the rural families was less than two-thirds that of the town group, the figures being $88 and $137, respectively. In the section on illness, consideration will be given to the possible significance of higher illness rates in relation to adverse economic conditions, also to the effect of income on the amount and character of medical care received.
*• The general subject of diet was investigated on a previous occasion by Eliot (3) but the findings which are briefly summarized portray conditions which have not changed materially. Eliot states, "The daily diet for the average family can be summarized as rice and beans twice a day—usually in large amounts, especially of rice; coffee twice or three times a day, with unrefined sugar and with or without a small amount of milk; bread in very small quantities, usually without butter; tuberous vegetables; and fruit in small quantities, the fruit chiefly for the cliildren. Some families had nothing but rice and beans, and a few were found that did not even have both rice and beans every day."
The families studied by Eliot were drawn predominantly from the cities and ontlying territory; consequently they might not be truly representative of the island since they had access to whatever variety in diet their income could afford. The rural dwellers raise very little to supplement that which they purchase in the neighborhood store where the stock is limited. In fact, the diet in rural districts, if observed, may have been found even more monotonous and inade quate, since different studies conducted in more prosperous times showed that the amount of money available to meet all needs varied from 9 to 12 cents per person per day in different sections of the island.
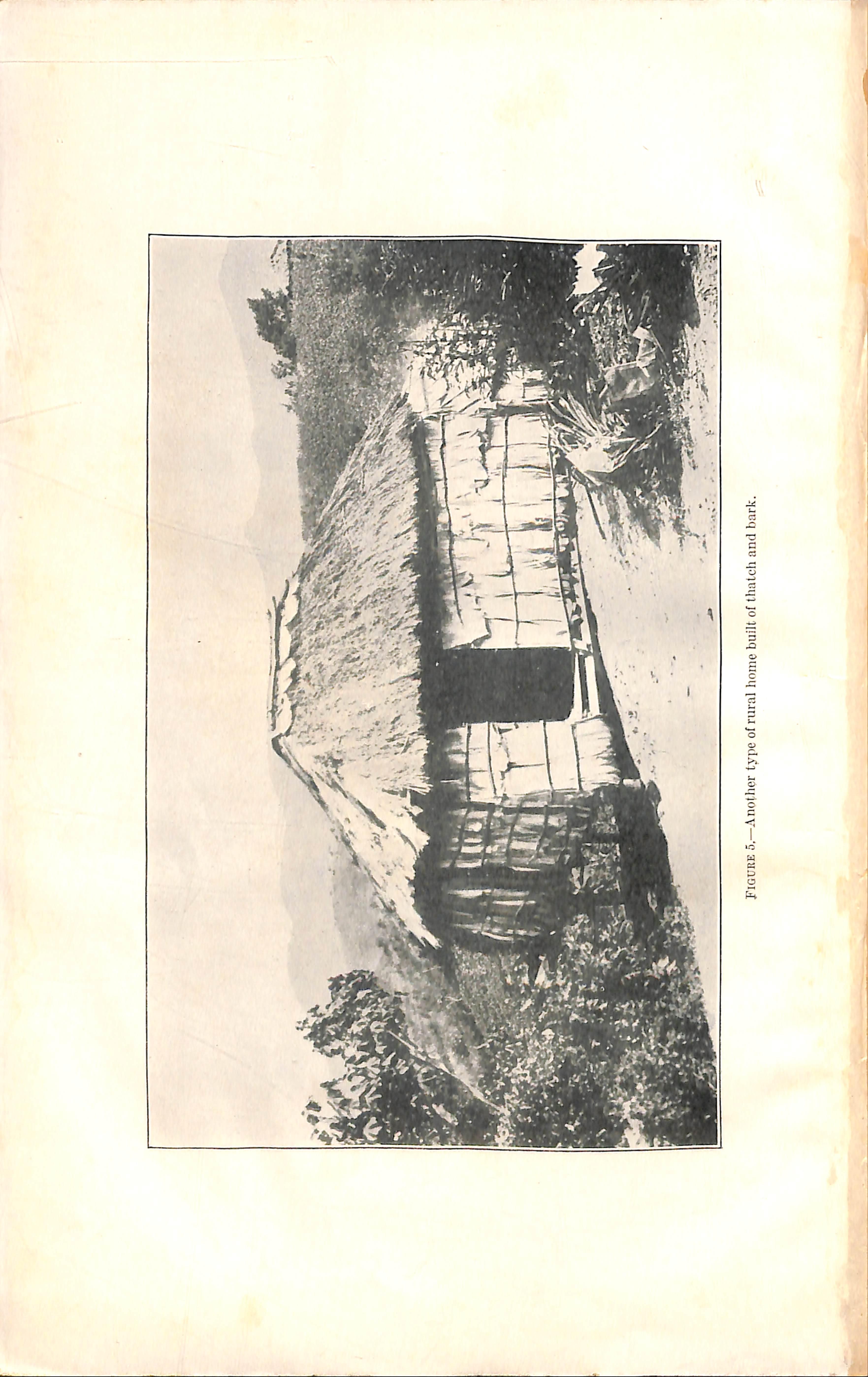
5,—Anotlier type of rural home built of thatch and bark.
The findings of Mitchell (4) -wdth regard to diet in the sample of families studied by him and coworkers accorded with those quoted from Eliot.
This dietarj*^ which is insufficient in amount, and particularly defi cient in animal proteid, results in a state of nutrition which is below that considered normal in the continental United States. Inadequate \ diet is likely to be an important factor in producing anemias of various 1types and deficiency diseases such as nutritional edema, sprue, and other related conditions which abound in Puerto Rico. Rickets, however, is not prevalent on the island.
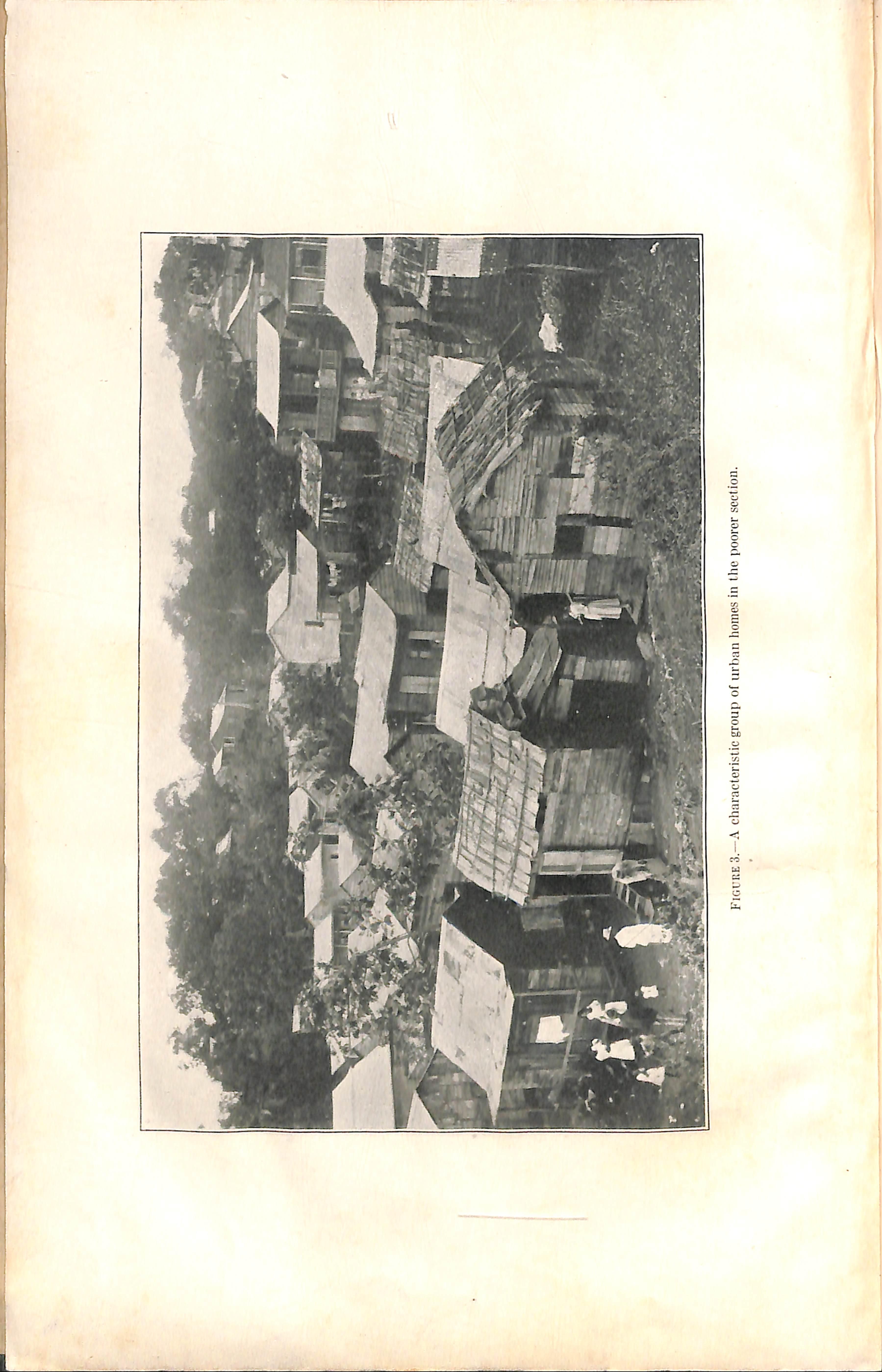
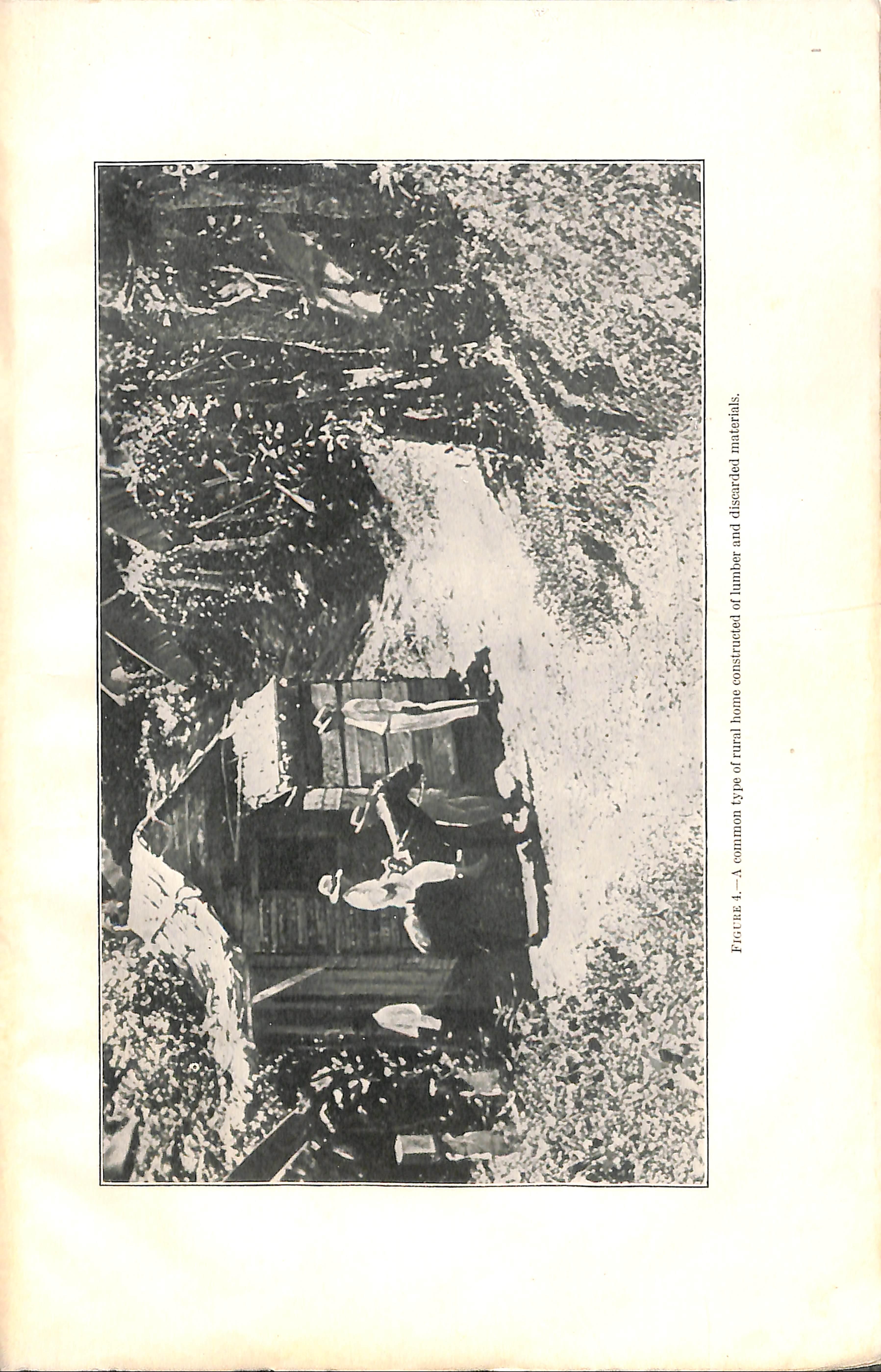
According to the data secured in the family survey, lumber is used as construction material for nearly 90 percent of the town houses and about 60 percent of those in rural areas. Of the remaining city homes, the better ones are made of stucco and the poorer ones of discarded building materials of various types. In the rural sections discarded materials are used for many domiciles and thatch is also a frequent choice. Figure 3 illustrates a group of typical urban homes, while those shown in figures 4 and 5 are representative of the dwellings in rural areas. The building law requires that the houses be elevated above the surface of the ground or that some equally effective ratproofing measure be used. Elevation is the method chosen by the poorer families. All Puerto Rican homes have floors. Screening is not practiced to any appreciable extent on the island; thus the houses afford scarcely any protection against flies and mosquitoes. Bed nets, however, are in fairly common use.
Sleeping accommodations, both from the standpoint of facilities and rooms, are markedly inadequate. Hammocks and cots are often used instead of true beds; still 2 percent of the surveyed famihes did not possess even a hammock. Under such circumstances a crude pallet is arranged upon the floor as a place to sleep. Rural families suffer more acutely than urban because of inferior sleeping facilities. Likewise, overcrowding in their homes is more evident. Wliile 26 percent of the urban families have more than two rooms used for sleeping purposes, only 8 percent of the rural group have this amoimt of sleeping space. This difference is rendered more striking when it is recalled that the average urban family has 4.9 members, whereas the average size of the rural family is 5.8. The crowded condition of rural Puerto Rican homes is further emphasized by the fact that 30 percent of 539 rural families with 9 or more individuals have only one sleeping room. Overcrowding to this extent was reported by only 16 percent of the 233 urban families of tliis size. Such a high degree of I congestion undoubtedly facilitates the spread of transmissible diseases. Obviously, in the homes described, it is not possible to establish satis-
factory conditions for the accommodation of sick persons who require bed care. This throws an added burden on the hospitals.
The sanitation status in rural areas is of particular interest since it has a direct hearing upon the prevalence of intestinal parasites. Infes tation with hookworm especially is a problem of grave importance in Puerto Rico. Some method of excreta disposal was reported as readily available to all but 4 percent of the town families. About 20 percent of the houses are connected vdth a sewer. Sixty-five percent of the urban families have latrines, three-fifths of which are classed as being in good sanitary condition, and the remainder as poor. The latrines of neighbors are used by the other 10 percent of the town families. In the rural sections, 40 percent of the families have no facilities for excreta disposal; 48 percent own latrines, one-half of which are rated sanitary, the other half being in poor condition; and 10 percent of the rural families use the latrines belonging to neighbors. Only 2 percent of the homes are cormected with a private sewer.
Inasmuch as accessibility to transportation might exert a direct influence upon the availability of medical service, this point was determined for 5,891 families. Distance from a passable road was used as the criterion of accessibility.
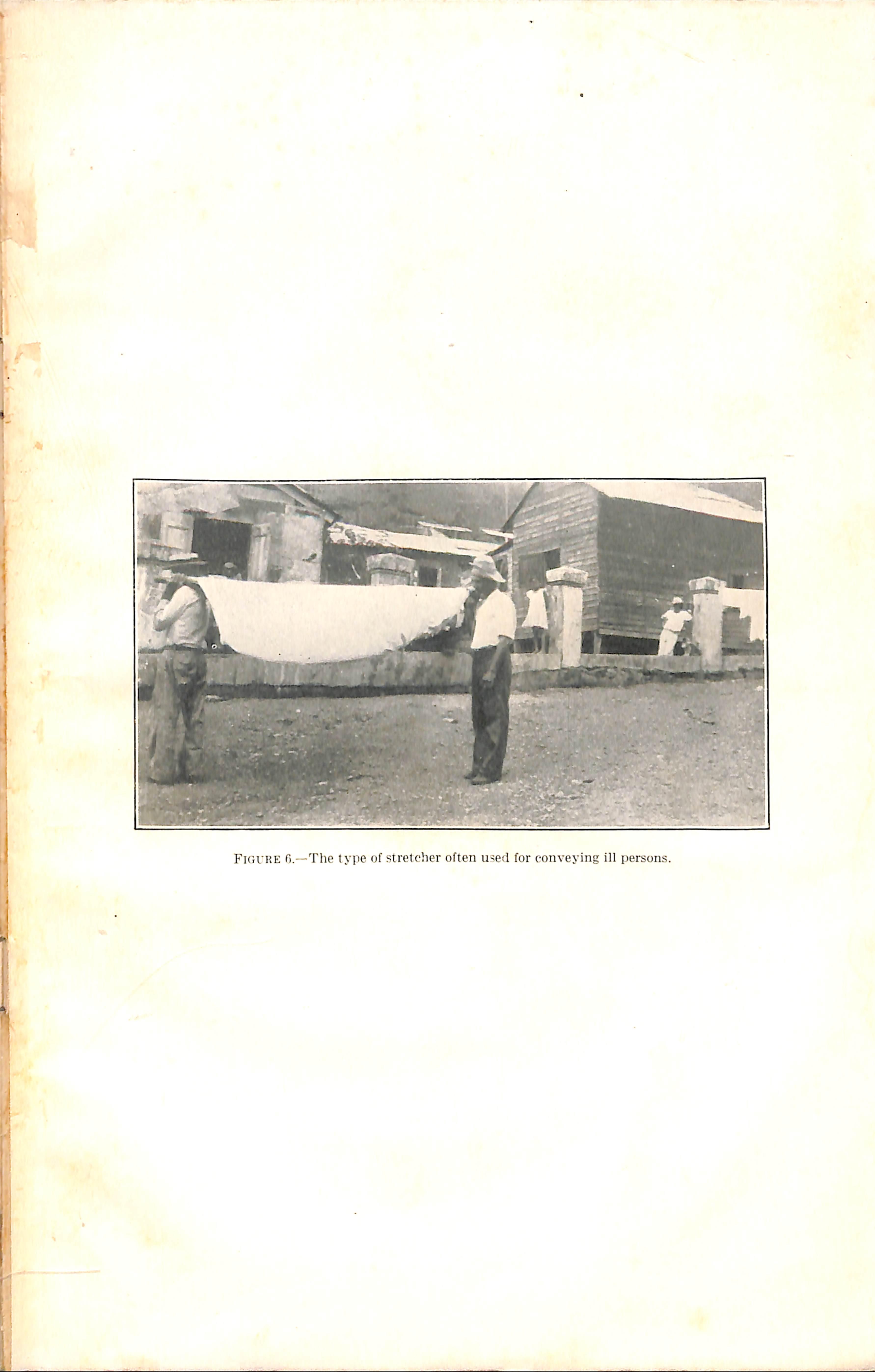
Thirty-six percent of the total number of famihes lived in towns and 8 percent were classed as suburban famihes. Both groups were re garded as accessible to transportation facihties. The rural familes were subdivided into two classes: Those living on a paved or dirt road, and those on a path more than one-half mile from the nearest road. It was found that 18 percent of the total number of families hved on a paved or other passable road. Two percent of all families visited hved in homes located on a path approximately 1 mile from the nearest road on which an automobile could travel; 22 percent were situated on paths at distances ranging from 2 to 3 miles from such a road; and about 14 percent were more than 3 miles distant from the nearest motor transportation. Since these homes located on paths can be reached only on foot or horseback, the difhculty of securing medical care when illness occurs is easily understood. Frequently the only possible means of providing a patient with medical care is to carry him,in the manner pictured in figure 6, to the nearest physician or hospital.
Coastal municipalities hold decidedly the most favorable position from the standpoint of accessibility of homes to transportation. Figure 7 illustrates a rural section of the interior. It is noted that paths constitute the only outlet from the homes shown. Nearly onehalf of the rural homes in the center of the island, as compared with 5 percent of aU others considered, are more than 3 miles from a paved or dirt road.
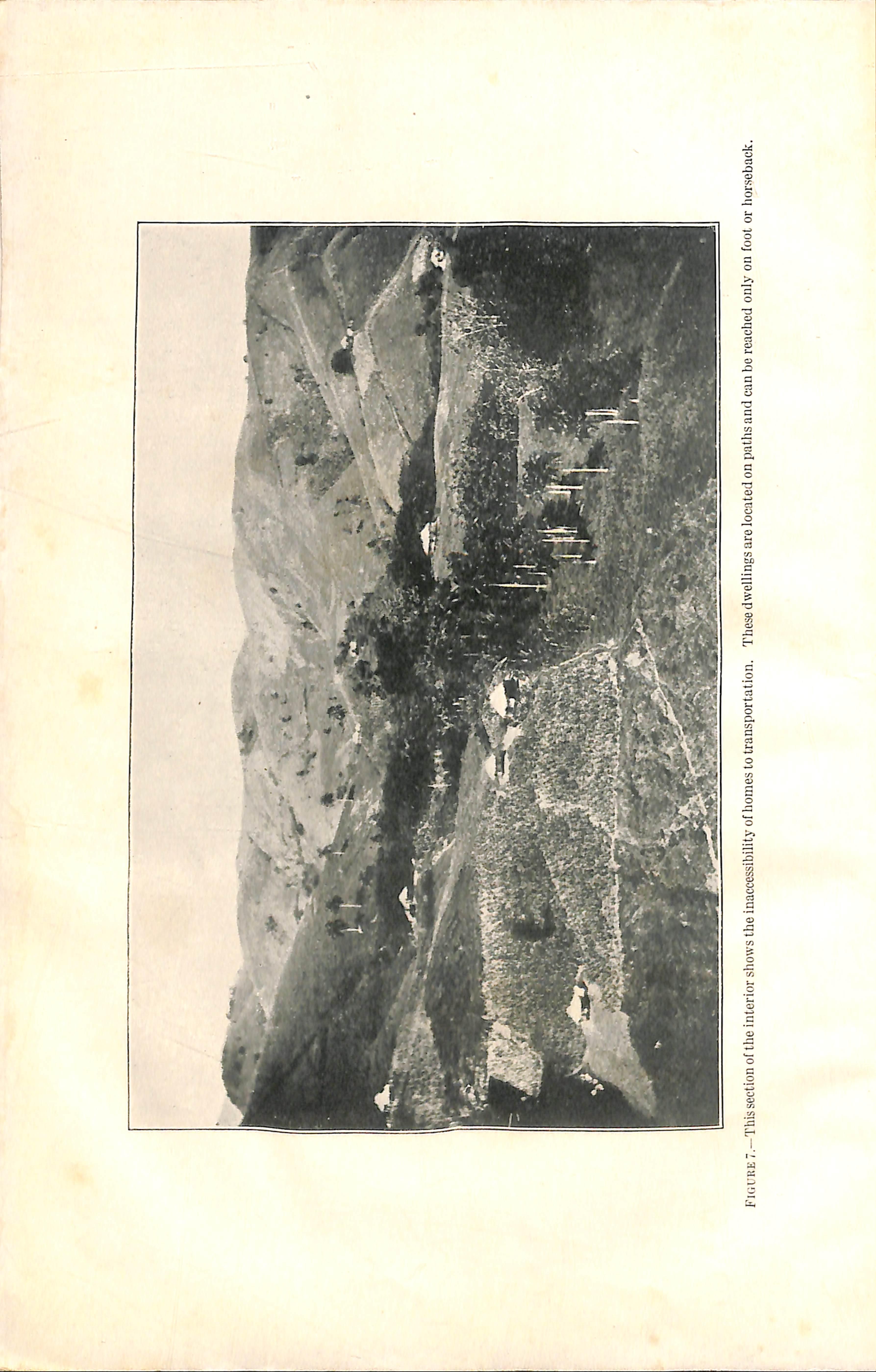
FiuURE 7—This section of the interior shows the inaccessibiiity of homes to transportation. These dweiiings are located on patiis and can bo reached only on foot or iior.seback.
Insular government.—Since government plays a prominent part in medical service, it is necessary to describe briefly the political organi zation of the island. Puerto Rico is classed as a possession of the United States, and the people of Puerto Rico, with few exceptions, are citizens of the United States. The government is modeled very much along the lines of State and local government on the continent. The central or insidar government is a counterpart of the State; and the local unit, known as the municipality, resembles a New England town, although it has certain county characteristics.
The departments of the insular government, together with the disbursements for each during the fiscal year 1934, are listed in table 4. Total disbursements of the insular government (excluding transfers) were $11,159,345.15 or about $6.85 per capita when computed on the estimated population as of January 1, 1934. Education was the largest single item and consumed 37 percent of this total. Next in order of size was health, to which was allotted $1,339,299. This amount represented 12 percent of the total, or about 80 cents per capita. The insular health department has major responsibility for public health service proper throughout the island, and it also partici pates in certain elements of medical care. Organization and func tions of the insular health department will be considered later.
Table 4.—Departments of the insular government of Puerto Rico and expenditures for each during the fiscal year 19S4
Departmenls
Municipal government.—There are 76 municipalities in Puerto Rico. Culebra, a neighboring island, has a slightly different form of local government. The municipalities are divided into three classes, broadly speaking, on the basis of population and wealth. The loca tion of municipalities in each classiflcation may be obtained from figure 8. In the first class there are 5 municipalities, in the second 23, and in the third 48. Certain data relating to area and population of each municipality can be found by referring to appendix A. The municipalities as a whole are small, since 32 have an area of less than 40 square miles each and only 3 are larger than 80 square miles. In size, the populations correspond somewhat to those of the counties of
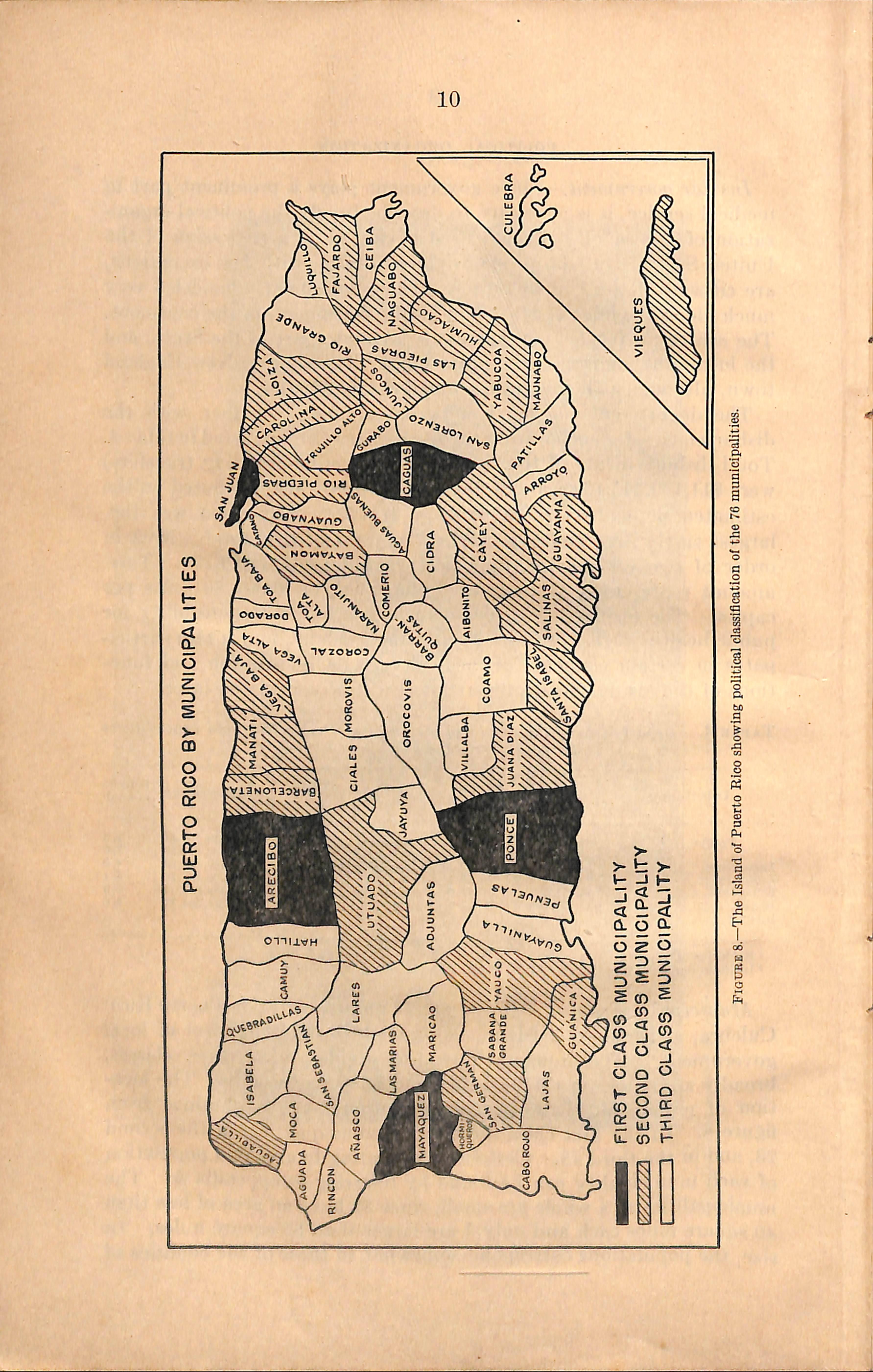
Figure 8.—The Island of Puerto Rico showing political classification of the 76 municipalities.
the continental United States; 33 'municipalities have less than 15,000 inhabitants; 36, between 15,000 and 30,000; and only 7 have more than 30,000 inhabitants. The last group contains two cities, San Juan and Ponce, and the two largest towns, Mayaguez and Arecibo.
Actual funds available in each municipahty for the conduct of local government during 1934 are listed in appendix B. Study of this table reveals that the total usable fimds for the support of all municipal functions are generally low, only nine municipahties having more than $100,000 available. Funds used during the fiscal year for the public functions of municipalities in different classes are given in table 5. While the iusular government assumes certain important responsi bilities, nevertheless, local funds__arnjmsjifficient for the__prop-CJ_discharge of municipalTimctlon^yhic^ according AoAilass^Jirslr..1asR municipnlities have some degree of responsibility for protection of personsjindjroperty, maintenance of highways,_ sanitation, cor rection, ed^ation, recreation, and charity (which includes medical care). Second- and third-class municipalities are more restricted in th^-Junctions, and even the authorized services as a rule are not well developed—^largely because of insufficiehtTeveniie: Thus the needs of the people become "secondary—to~the—availability of local resources in deterniining municipal governmental programs.
Table 5.—Total and per capita expenditures for all purposes in first-, second-, and third-class municipalities of Puerto Rico during the fiscal year 1934
Of particular interest from the standpoint of this study are the appropriations by municipalities of each class for medical care. This item appears in government reports imder the heading "Beneficencia", and will he considered later in part III, Medical Care.
Emergency reliej administration.—The rehef problem created by the economic depression current at the tune of the survey overtaxed in sular and municipal resources. The Federal Government came to the assistance of the island. A special agency Isnown as the Puerto B,ico Emergency Relief Administration, which follows very closely the pattern of State emergency rehef organizations in the continental United States, was created to meet this situation. This agency since its estahhshment has assumed almost complete responsibility for ma terial rehef. Such assistance may take the form of food orders, cash
grants, or employment. At the time of the survey approximately 60 percent of the families visited,in second- and third-class municipalities were receiving relief of some form. The percentage in the first-class mrmicipalities was reported to be somewhat less. Expenditures for relief by the Puerto Rico Emergency Relief Administration at the time of the survey were slightly in excess of $1,000,000 per month, or approximately the same as the total cost of the insular government for the same period.
Obviously it would not be possible to appraise the existing health facilities in Puerto Kico, or to make recommendations regarding changes, without an imderstanding of how illness expresses itself in the population.
Three indices were used to measure the prevalence of iUness and physical impairment: Deaths reported to the insular health depart ment, spepial studies made by other investigators, and the family canvass which was conducted as a part of the survey herein described. Reports of communicable diseases filed with the insular health department furnished some information, but they were not regarded a,s being sufficiently complete for the purpose of portraying the incidence of these diseases.
Notwithstanding the fact that only a small proportion of cases terminate in death, mortality data may be accepted as one quantita tive measure of the more serious types of Ulness. Reporting of deaths in Puerto Rico is said to be very nearly complete. On the other hand, causes of death as stated on the death certificate are not re garded by the insular health department as very reliable, since a \large percentage of the patients either have no attendant for the last lihiess or receive care under circumstances where accurate medical liagnoses are difficult to make. Under the circumstances, it is posjible to make deductions regarding illness only on the basis of gross mortality and deaths by age groups.
It has already been demonstrated in table 2 that the death rate of Puerto Rico is extremely high when compared ivith that of the continental United States. The proportionately higher birth rate in Puerto Rico, to which attention has also been directed, might be one factor in elevating the gross death rate, but the difference between the two areas is far too great to be explained on this basis alone. While ^all the underlying causes may not be understood completely, it is reasonable to suppose that the rates must be influenced adversely by a diet inadequate from the standpoint of quantity and quality, coupled with defective housing and sanitation, and the other un favorable circumstances thet usually accompany low income. Puerto Rico, in common with many tropical sections, is afflicted with tlu-ee (13) 137904—37 3
disease conditions—malaria, dysentery, and hookworm infestation— which directly an5 indirectly contribute to its excess mortality. Jji-4ulditieHr-ttii>er-culosis is extremely prevalent, and at the present time it is reported to be more malignant than it was some years ago. .The differences between Puerto Rico and the continental United States in death rates for selected age groups may be noted by referring to table 6. Attention is directed especially to the relatively high infant death rate in Puerto Rico. The rate for this age group in Puerto Rico is 159 as compared with 58 in the States. The greatest relative difference in mortality between the two areas is found when children between the ages of 1 and 4 years are considered. The death rate of this age group is six times as high in Puerto Rico as in the States. On the continent more deaths in proportion to the total occur among adults over 65 years of age when the degenerative diseases of the heart and kidneys and malignancy begin to take their toll, but even for this age group, wherein death occurs most frequently in the United States, the rate is still higher for Puerto Rico, the rates being 80 for the States and 100 for the island.
Table 6.—Death rates for certain age groups in Puerto Rico and in the continental United States during the year 1934
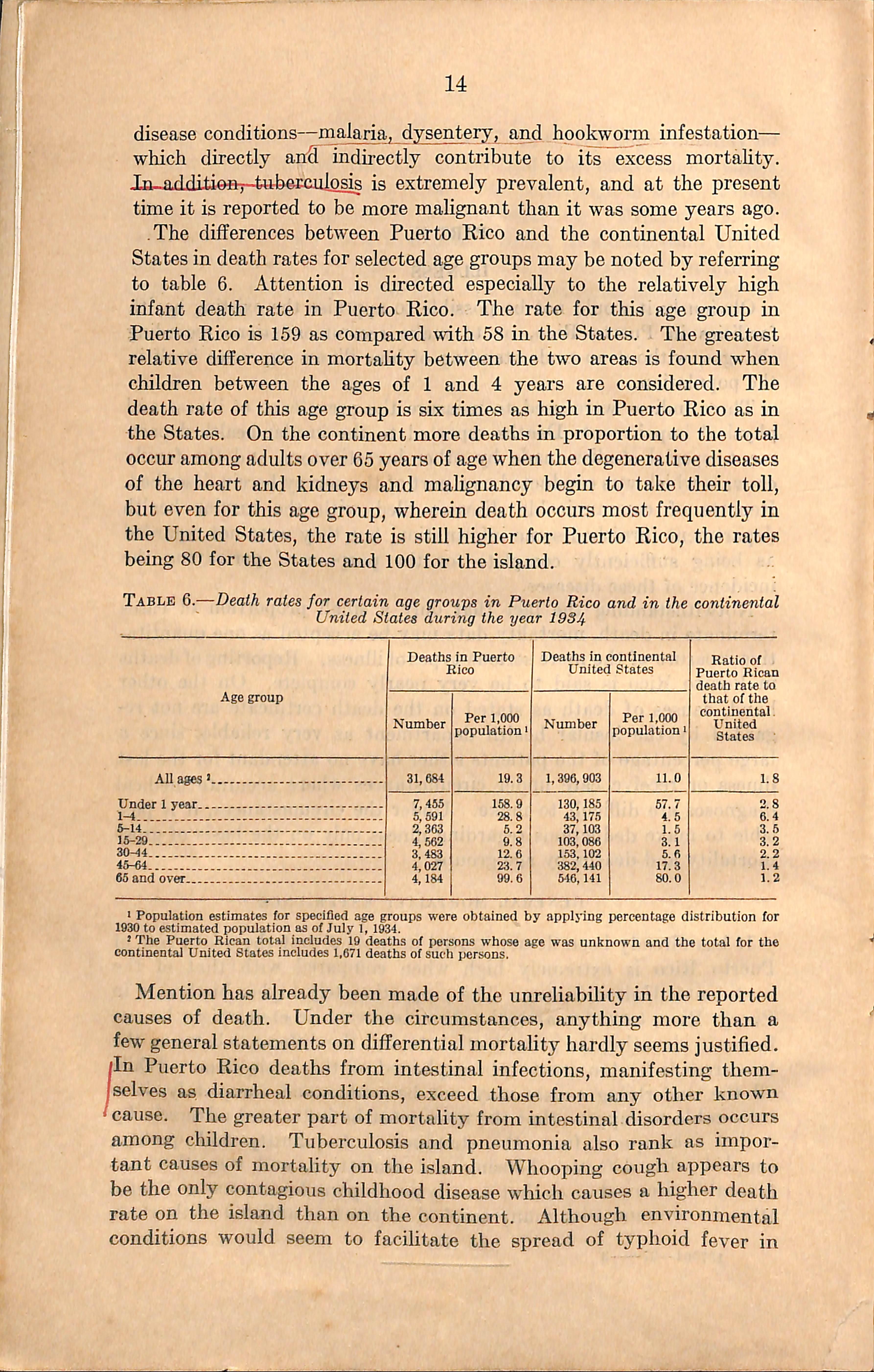
i Population estimates for specified age groups were obtained by applying percentage distribution for 1930 to estimated population as of July 1, 1934.
* The Puerto Rican total includes 19 deaths of persons whose age was unknown and the total for the continental United States includes 1,671 deaths of such persons.
Mention has already been made of the unreliability in the reported causes of death. Under the circumstances, anything more than a few general statements on differential mortality hardly seems justified. /In Puerto Rico deaths from intestinal infections, manifesting themIselves as diarrheal conditions, exceed those from any other known 'cause. The greater part of mortality from intestinal disorders occurs among children. Tuberculosis and pneumonia also rank as impor tant causes of mortality on the island. Whooping cough appears to be the only contagious childhood disease which causes a higher death rate on the island than on the continent. Although environmental conditions would seem to facihtate the spread of typhoid fever in
Puerto Rico, deatlis from this disease are not encountered as frequently as might be expected. Mortality rates for malaria and hookworm infestation do not express the serious problem which these diseases present, since deaths reported from these causes are relatively few in proportion to the cases. Indirectly, however, they constitute a grave situation, as will be disclosed in the next section.
Outstanding health problems of the island of Puerto Rico have been the subjects of intensive investigation by other workers on previous occasions. Their findings are of sufficient importance in this connec tion to warrant summarization for those who may not have access to the original publications.
Malaria.—Malaria is believed to have been endemic when Puerto Rico was first colonized by the Spaniards. Its occurrence is said to be mentioned throughout the history of the island. In recent years its incidence is believed to have increased on account of growth in popidation along the coast and extension of irrigation in connection with the cultivation of sugarcane. Malaria may be found in all parts of the island, but it is along the coast and, to a much less extent, in the nearby foothills that it constitutes the greatest problem.
In 1920 Grant (5) reported malaria parasites in the blood of only 1.3 percent of persons living in the mountains, while on the coast he found an average rate of about 30 percent. Earl (6) at a later date found essentially the same situation in the coastal area, and from 5 to 6 percent positive blood smears for individuals of the mountainous sections that were studied. Malaria is not believed by him to be a serious problem in the foothills, although occasionally localized epidemics occur, some of which are rather severe. According to Earl and his associates, the percentage of the population along the coast showing enlarged spleens varied from 11 at Guayama to 56 at Humacao, while the percentage with parasites ranged from 16 at Guanica to 55 at Humacao. These investigators believe that malaria is transmitted at all seasons of the year, but the highest prevalence occurs during September, October, November, and December.
Hookworm.—Hookworm infestation is extremely common. At the present time persons harboring the parasites may be found in all parts of the island, although infestation is much higher in certain regions. Hill (7) states that, in general, infestation increases from the coast to the interior. Conditions in the coffee-growing sections are most favorable for the propagation of the parasite. Even on the coast HiU found the average worm burden to be about 200, a condition wliich in dicates a serious problem. In the interior the infestation reached an estimated intensity of 500 worms per person. There children from 3 to 4 years of age were found harboring on the average approxi-
mately 100 worms, while children from 5 to 9 years had almost 300 worms or close to the average adult infestation.
Nutritional disorders.—Poor nutrition is a great factor in reducing efiBciency and in lowering vitality; it may also be presumed bo in fluence adversely the resistance of a large percentage of the population to specific diseases. The physical condition of a sample of approxi mately 500 children was studied by Eliot (3) who took into account such criteria as skeletal growth and body weight, amount of sub cutaneous fat, muscular development, onset of dentition, color of mucous membranes, and other physical findings. It was recognized of course that direct comparison could not be made with the children of the continental United States because of differences of racial stock, climatic conditions, and perhaps other influences on growth and body build. Eliot, however, has this to say of the nutritional status of the .children of Puerto Rico: "There is no doubt that the general nutriuional condition of the great majority of Puerto Rican children, as iseen from the clinical point of view, is far from being as satisfactory ^s that of the children in the continental United States. Many of the most poorly nourished or atrophic children are in a class entirely outside the public health experience of the physicians on the study and can be compared only with the cluldren suffering from severe marasmus or starvation who are seen elsewhere in hospital wards. Excellently nourished children, moreover, are seldom found and then only among the yoimger infants. The great mass of children belong in a group whose nutritional condition would be called fair or poor in continental United States."
After using slightly different criteria, Mitchell (4) reached essen tially the same conclusions. He states: "A definite relationship hav ing been established between the physical measurements of the chil dren and various socio-economic factors, we may safely conclude that the evidence is consistent with the claim that the Puerto Rican children suffer a considerable nutritional handicap."
Infant mortality.—It is believed by the local health authorities that the deaths among infants under 1 year of age in proportion to the live births is unduly high, but any definite statement on this point would be difficult to substantiate. Reporting of births is loiown to be far from complete,while over 90 percent of deaths are said to be registered. This difference in reporting alone would tend to elevate the death rates of infants. The average infant mortality rates for the three latest 5-year periods covered by published reports are used in table 7 to show the trend in deaths among children under 1 year of age. It will be observed that the rates for the most recent 5-year period show a precipitous drop from those which maintained during previous years. This lowering of the infant mortality rate may be due in part to the extension of the child welfare program, notably the milk stations, but it is difficult to account for changes on this basis alone.
Table 7.—Average live births, infant deaths, and infant mortality rates in Puerto Rico during three 5-year periods, 1920-34
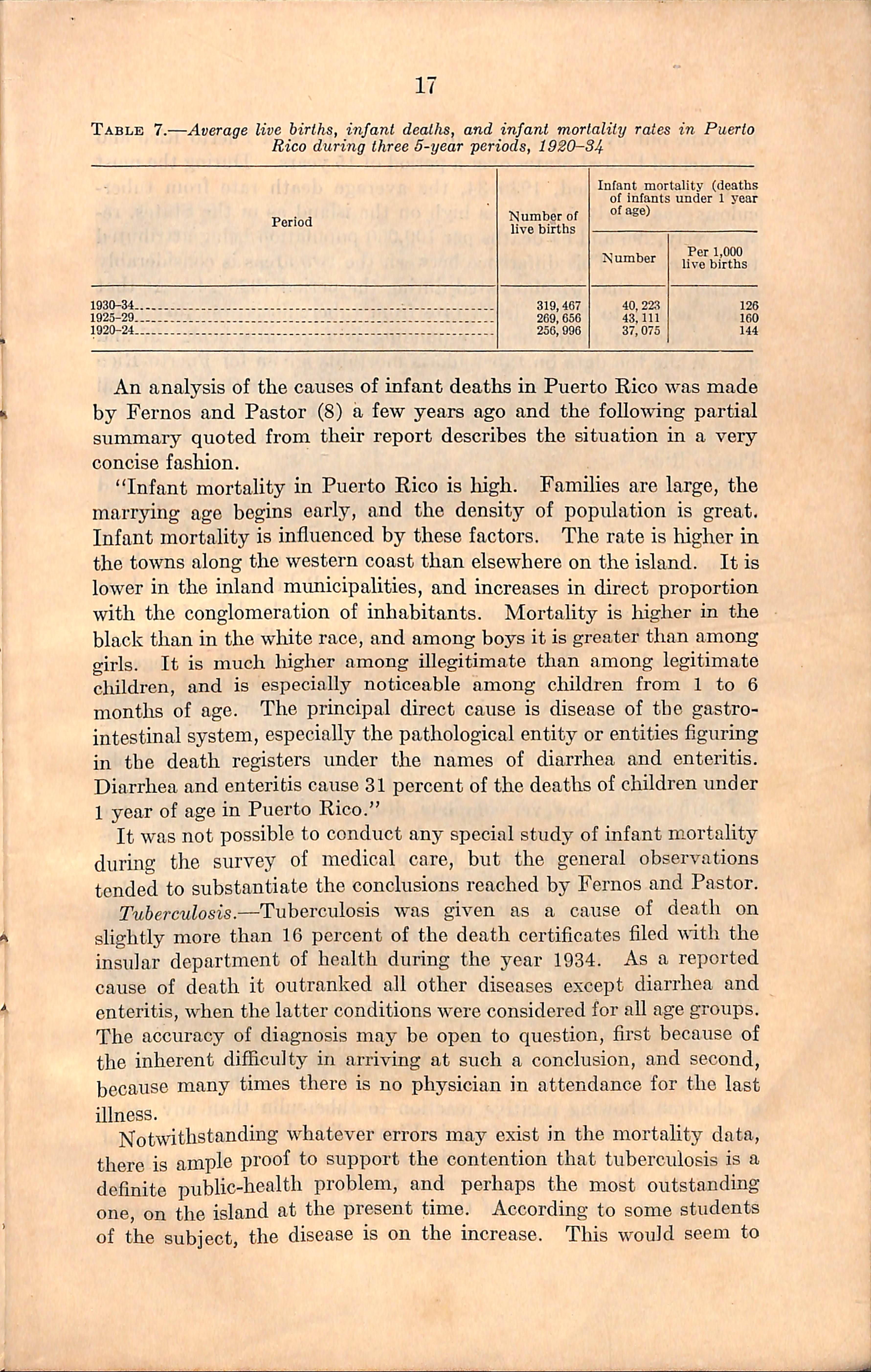
An analysis of the causes of infant deaths in Puerto Rico was made by Fernos and Pastor (8) a few years ago and the following partial summary quoted from their report describes the situation in a very concise fashion.
"Infant mortality in Puerto Rico is high. Families are large, the marrying age begins early, and the density of population is great. Infant mortality is influenced by these factors. The rate is higher in the towns along the western coast than elsewhere on the island. It is lower in the inland municipalities, and increases in direct proportion with the conglomeration of inhabitants. Mortality is higher in the black than in the white race, and among boys it is greater than among girls. It is much higher among illegitimate than among legitimate children, and is especially noticeable among children from 1 to 6 months of age. The principal direct cause is disease of the gastro intestinal system, especially the pathological entity or entities figuring in the death registers under the names of diarrhea and enteritis. Diarrhea and enteritis cause 31 percent of the deaths of children under 1 year of age in Puerto Rico."
It was not possible to conduct any special study of infant mortality during the survey of medical care, but the general observations tended to substantiate the conclusions reached by Fernos and Pastor.
Tuberculosis.—Tuberculosis was given as a cause of death on slightly more than 16 percent of the death certificates filed with the insular department of health during the year 1934. As a reported cause of death it outranked all other diseases except diarrhea and enteritis, when the latter conditions were considered for all age groups. The accuracy of diagnosis may be open to question, first because of the inherent difficulty in arriving at such a conclusion, and second, because many times there is no physician in attendance for the last illness.
Notwithstanding whatever errors may exist in the mortality data, there is ample proof to support the contention that tuberculosis is a definite public-health problem, and perhaps the most outstanding one, on the island at the present time. According to some students of the subject, the disease is on the increase. Tliis would seem to
be borne out by a comparison of the death rates of Puerto Rico and continental Uaited States over a period of 15 years. During the most recent 5-year period, 1930-34, the average death rate from tuber culosis was nearly 5 times as high on the island as in the States, re spectively,296 and 64 deaths per 100,000 population being attributed to this cause. Tliis difference between the two areas is considerably greater than that which existed during the period 1920-24. At that time the Puerto Rican death rate from tuherculosis was just twice that of the continent, the corresponding average rates being 197 and 98. While the data on tuherculosis mortality given for Puerto Rico may not be comparable in all respects with those for the continental United States, yet the gross picture presented is that of a declining rate for the continental United States and a gradual upward trend in Puerto Rico.
After an exhaustive study of tuberculosis on the island, Townsend (9) became convinced that the alleged prevalence of tuberculosis is perhaps an understatement of the true condition. His findings may be summarized as follows; "The death rate from tuberculosis is about twice that of the continental United States. Pulmonary tuherculosis overshadows aU other forms—bone, joint, and glandular types are very rare. Rates are highest in cities.and especially among tobacco factoi-y workers. The disease is less frequent among those engaged in growing sugarcane than among those in other agricultural pursuits and it is comparatively rare in rural mountain dwellers. Milk is not a factor in disseminating the disease. Low income, overcrowding, inadequate diet, and chronic disease—especially malaria and hook worm, are beheved to be predisposing factors."
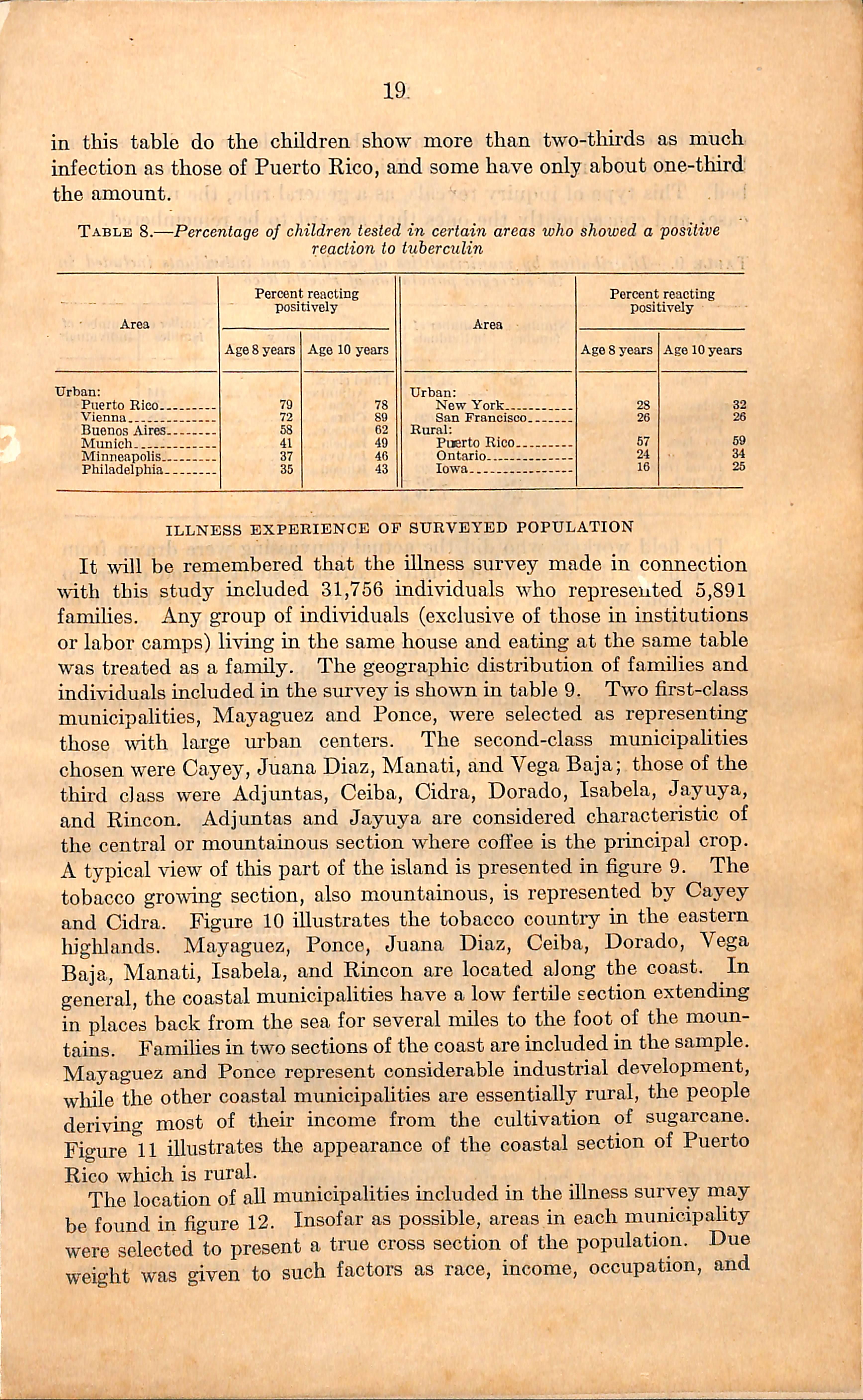
Death reports, however complete, disclose only a small part of the infection present in a population. A common procedure for determin ing the amount of infection is the application of the tuhercuhn test to a sample of the population. This plan was followed by Pastor (10) as part of a comprehensive study into the health of Puerto Rican children which was made by the American Child Health Association in 1930. The group tested included 189 urban and 335 rural children 8 years of age, and 691 urban and 348 rural cliildren of 10 years, or in all 1,563. The percentages of children in Puerto Rico showing positive reaction are contrasted in table 8 with the findings of other Workers using a similar method. According to the data presented in this table, Puerto Rico, with one exception, has a higher percentage of children showing positive reaction to tuberculin than any other area under consideration. Only in Vienna did a higher percentage of 10-year old children show positive reactions than in Puerto Rico; 8-year old cliildren there, however, merely approached the Puerto Rican record. In no part of the continental United States reported
sr'.iw-r.
19, in this table do the children show more than two-tliu'ds as much infection as those of Puerto Rico, and some have only about one-third the amount.
Table 8.—Percentage of children tested in certain areas who showed a positive reaction to tuberculin
Area
Urban: Puerto Rico.. Vienna Buenos Aires, Munich Minneapolis. Philadelphia.
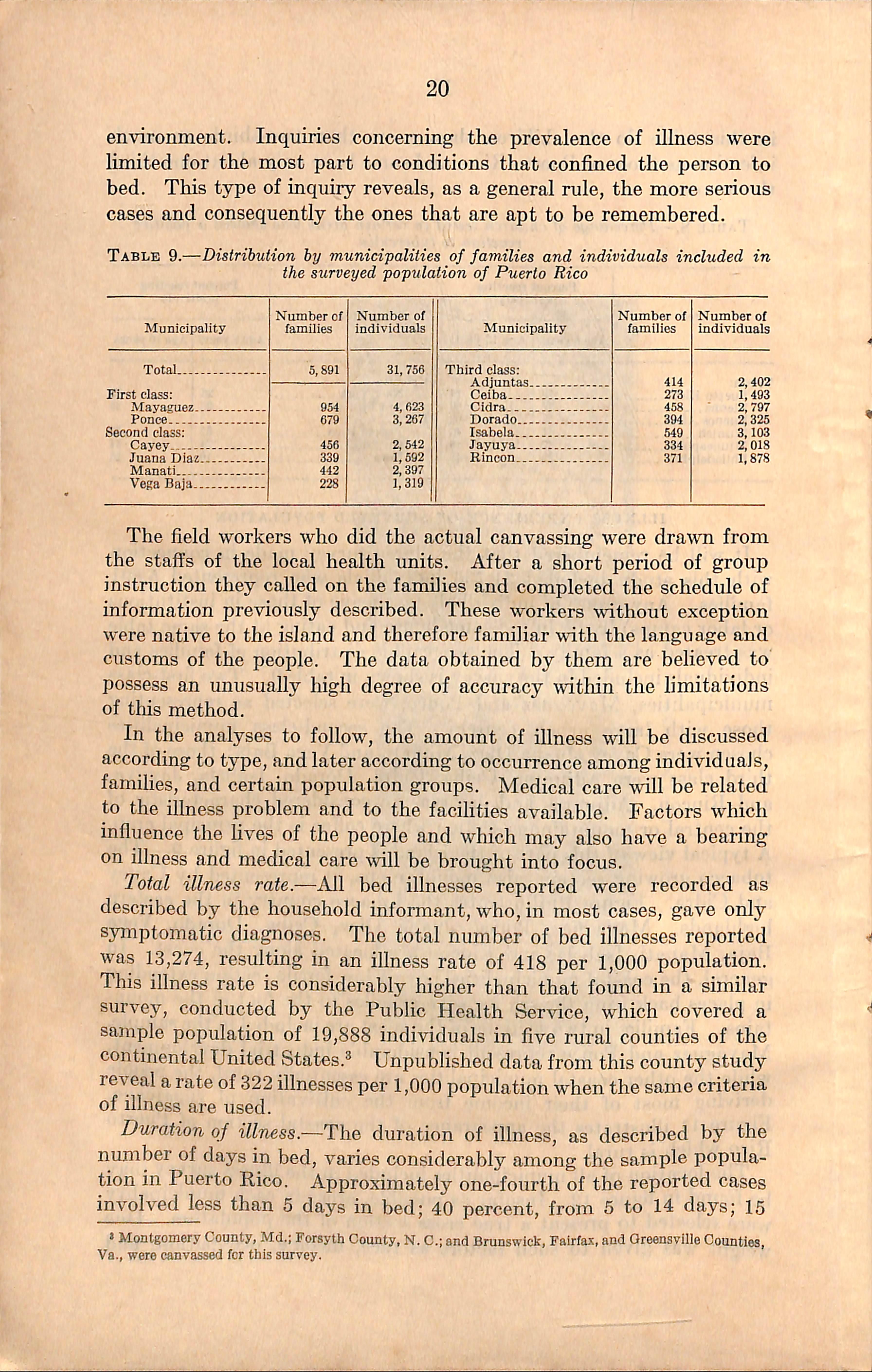
It whl be remembered that the Ulness survey made in connection wth this study included 31,756 individuals who represented 5,891 families. Any group of individuals (exclusive of those in institutions or labor camps)living in the same house and eating at the same table was treated as a family. The geographic distribution of families and individuals included in the survey is shown in table 9. Two first-class municipalities, Mayaguez and Ponce, were selected as representing those wdth large urban centers. The second-class municipalities chosen were Cayey, Juana Diaz, Manati, and Vega Baja; those of the third class were Adjuntas, Ceiba, Cidra, Dorado, Isabela, Jayuya, and Rincon. Adjuntas and Jayuya are considered characteristic of the central or mountainous section where coffee is the principal crop. A typical view of tliis part of the island is presented in figure 9. The tobacco growing section, also mountainous, is represented by Cayey and Cidra. Figure 10 illustrates the tobacco country in the eastern higlilands. Mayaguez, Ponce, Juana Diaz, Ceiba, Dorado, Yega Baja, Manati, Isabela, and Rincon are located along the coast. In general, the coastal municipalities have a low fertile section extending in places back from the sea for several miles to the foot of the moun tains. Families in two sections of the coast are included in the sample. Mayaguez and Ponce represent considerable industrial development, wliile the other coastal municipalities are essentially rural, the people deriving most of their income from the cultivation of sugarcane. Figure 11 illustrates the appearance of the coastal section of Puerto Rico which is rural.
The location of aU municipalities included in the illness survey may be found in figure 12. Insofar as possible, areas in each municipality were selected to present a true cross section of the population. Due weight was given to such factors as race, income, occupation, and
environment. Inquiries concerning the prevalence of Ulness were limited for the most part to conditions that confined the person to bed. This type of inquiry reveals, as a general rule, the more serious cases and consequently the ones that are apt to be remembered.
Table 9.—Distribution by municipalities of families and individuals included in the surveyed 'population 0/ Puerto Rico
The field workers who did the actual canvassing were drawn from the staffs of the local health units. After a short period of group instruction they called on the families and completed the schedule of information previously described. These w-orkers without exception were native to the island and therefore familiar with the language and customs of the people. The data obtained by them are believed to possess an unusually liigh degree of accuracy within the h'mitations of this method.
In the analyses to follow, the amount of illness wiU be discussed according to type,and later according to occurrence among individuals, famihes, and certain population groups. Medical care will be related to the illness problem and to the facilities available. Factors which influence the hves of the people and which may also have a bearing on illness and medical care Avill be brought into focus.
Total illness rate.-—All bed illnesses reported were recorded as described by the household informant, who,in most cases, gave only symptomatic diagnoses. The total number of bed illnesses reported was 13,274, resulting in an illness rate of 418 per 1,000 population. This illness rate is considerably higher than that foimd in a similar survey, conducted by the Public Health Service, which covered a sample population of 19,888 individuals in five rural counties of the continental United States.^ Unpublished data from this county study reveal a rate of 322illnesses per 1,000 population when the same criteria of illness are used.
Duration of illness.-—The duration of illness, as described by the number of days in bed, varies considerably among the sample popula tion in Puerto Rico. Approximately one-fourth of the reported cases involved less than 5 days in bed; 40 percent, from 5 to 14 days; 15 > Montgomery County, Md.;Forsyth County. N.C.;and Brunswick,Falrfa.x, and Greensville Counties, Va., were canvassed fcr tliis survey.
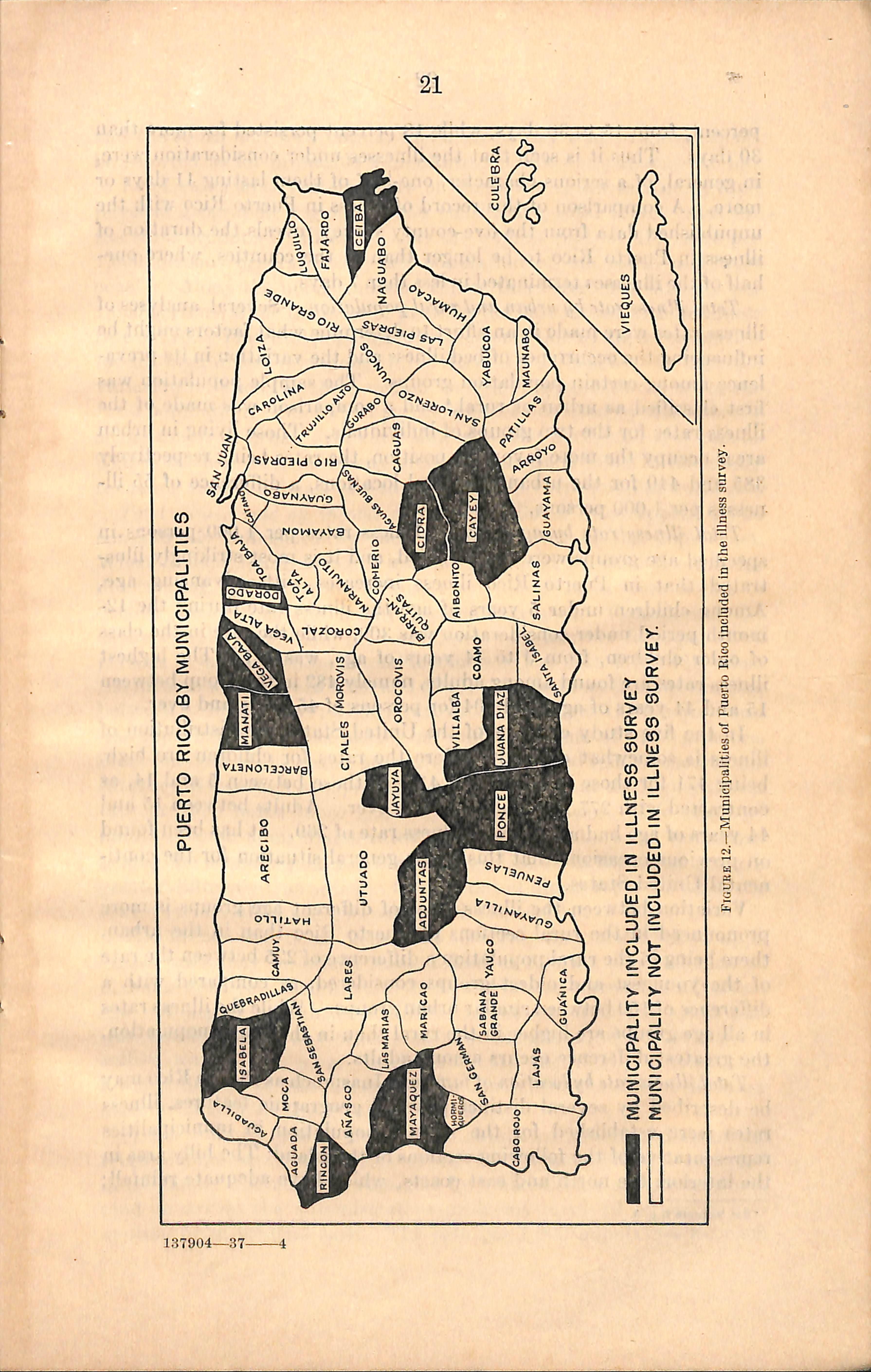
MUNICIPALITY INCLUDED IN ILLNESS SURVEY
MUNICIPALITY NOT INCLUDED IN ILLNESS SURVEY.
Figure 12.—Municipalities of Puerto Rico included in the illness survey.
percent, from 15 to 30 days, while 18 percent persisted for more than 30 days. Thus it is seen that the illnesses under consideration were, in general, of a serious character, one-half of them lasting 11 days or more. A comparison of this record of illness in Puerto Rico with the unpublished data from the five-county survey reveals the duration of illness in Puerto Rico to be longer than in the counties, where onehalf of the illnesses terminated in less than 7 days.
Total illness rate by urban and rural population.—Several analyses of illness rates were made in an effort to determine what factors might be mfluencing the occurrence of bed illness and the variation in its preva lence among certain population groups. The sample population was &st classified as tirban or rural,^ and a comparison was made of the illness rates for the two groups of individuals. Those living in urban areas occupy the more favorable position, the rates being respectively 385 and 440 for the urban and rural locations, a difference of 55 ill nesses per 1,000 persons.
Total illness rate by age group.—Illness rates per 1,000 persons in specified age groups were next studied, and it is most strikingly illus trated that in Puerto Rico illness increases with advancing age. Among children under 5 years of age the illness rate during the 12month period under consideration was 309, while the rate in the class of older children, from 5 to 14 years of age, was 327. The highest illness rates are found among adults, namely 482 in the group between 15 and 44 years of age, and 504 for persons of 45 years and over.
In the five study counties of the United States the distribution of illness is somewhat different. Here the rates for children are high, being 471 for those under 5, and 412 for those between 5 and 14, as contrasted with 277 for adults of 45 or over. Adults between 15 and 44 years of age had a still lower illness rate of 269. It has been found on previous occasions that this is the general situation for the conti nental United States.
Variation between the illness rates of different age groups is more pronounced in the rural sections of Puerto Rico than in the urban, there being in the rural population a difference of 225 between the rate of the youngest and oldest groups considered, as compared with a difference of 159 between similar urban groups. While the illness rates in all age groups are higher in the rural than in the urban population, the greatest difference occurs among adults.
Total illness rate by location offamily.—Inasmuch as Puerto Rico may be described by several distinct physical geograpliic features, illness rates were established for the sample population in municipalities representative of the following sections of the island: The hilly area in the interior, the north and east coasts, which have adequate rainfallj
'See footnote 2, p. 6.
and the south and west coasts, which are so dry that irrigation must be resorted to for profitable agriculture. These comparisons are felt to be of value since certain types of illness are characteristic of each physical geographic region. Upon considering total illness rates for the three sections it is learned that the highest rate, or 477 cases per 1,000 persons occurs among the population of the south and west coasts. Along the north and east coasts there were 399 illnesses per 1,000 persons, while the interior presents the best record with an illness rate of 370. The rural population,rather than the urban,is responsible for the high illness rate along the south and west coasts. In fact, the variation between the three regions is, in all cases, accentuated in the rural population. One rather surprising fact disclosed by this analysis is the excess of urban over rural illness on the north and east coasts. This is the first instance of any investigation made so far in this study revealing an urban illness rate that exceeds the corresponding rural one.
Toted illness rede by income of family. Illness rates appear to be considerably influenced by the economic status of the population. When annual family money income was used as the criterion for determinmg the economic status, total illness rates were noted to decline steadily as the family income increased. Considering the entire sample population, the total illness rate was 444 cases per 1,000 persons in families whose annual income was less than $100;436, when the income was between $10P and $249; 363,for those families earning between $250 and $749; while a rate of 297 cases per 1,000 individuals was reported in families having an annual income of $750 or more. Since one-half of the entire population of the island falls in the income category of less than $100,it will be appreciated that the higher illness rate prevails much more generally than the lower. The effect of family income upon illness rates would seem to be more important among the urban population than the rural, since in the urban group a greater difference was noted in the amount of illness reported when the lowest income class was compared with the highest.
The influence of such factors as location, age, and income upon illness rates may be briefly summarized as follows: The amount of illness is relatively liigh in rural areas and among persons of advanced age. A higher prevalence of illness maintains upon the south and west coasts than in any other section of the island, while the interior suffers least. The more nearly adequate the family income, the lower is the illness rate; or, stated conversely, the occurrence of illness becomes higher as the income level drops.
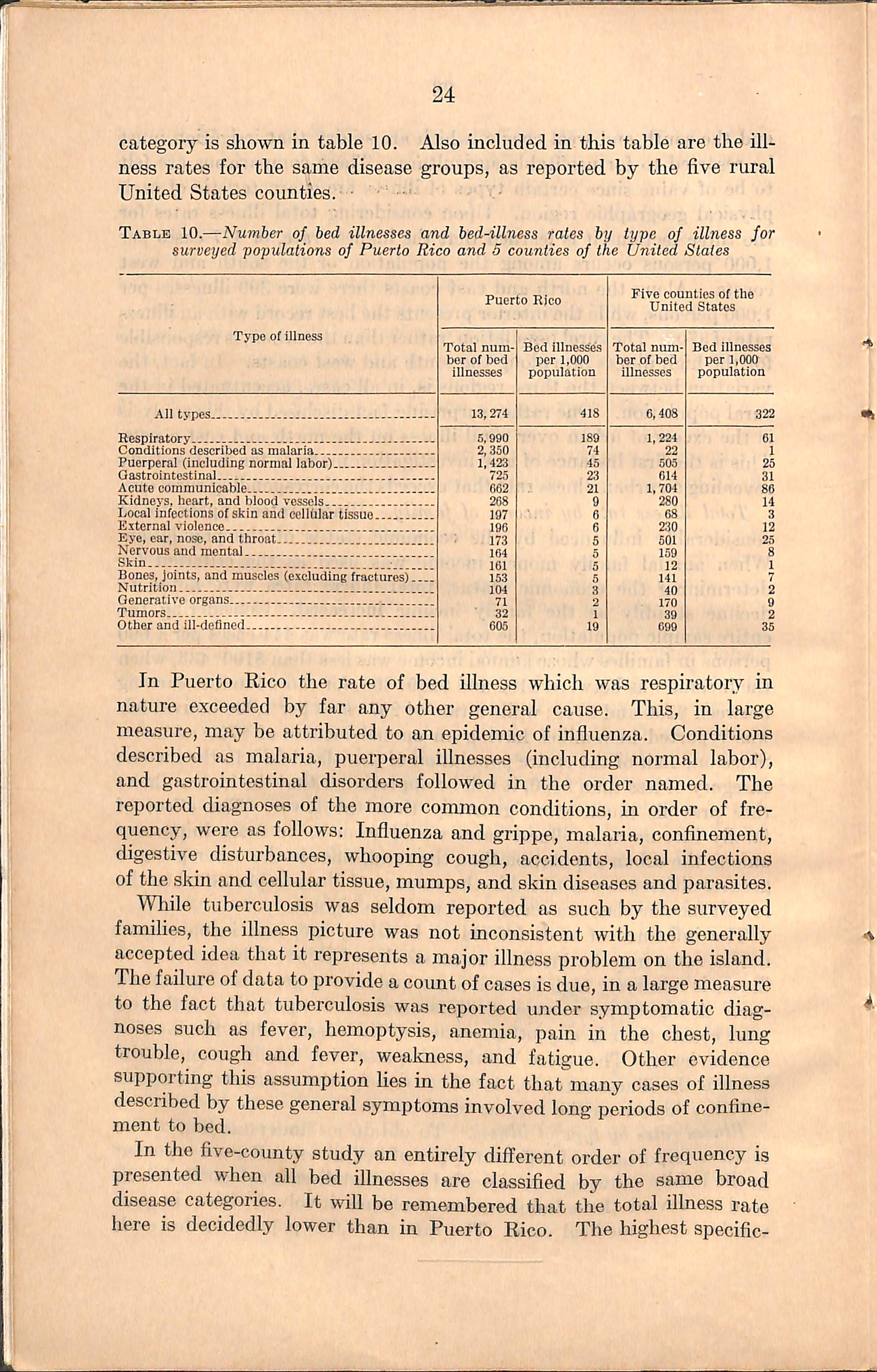
Illness rates by type of illness.—To obtain an understanding of the relative importance of different types of bed illness, all cases reported in the family canvass were classified by broad disease categories which tend to reveal the administrative problems involved either in pre vention or in medical care. The rate per 1,000 population for each
category is shown in table 10. Also included in this table are the ill ness rates for the same disease groups, as reported by the five rural United States counties. ■ ■ '
Table 10.—Number of bed illnesses and bed-illness rales by type of illness for surveyed populations of Puerto Rico and 5 counties of the United Stales
described as malaria
(including normal labor)
Kidneys, heart, and blood vessels
Local infections of skin and cellular tissue
External violence
Eye, car, nose, and throat
Nervous and mental II
Skin j
Bones, joints, and muscles (excluding fractur^)
Nutrition
Generative organs
Tumors
and ill-defined
In Puerto Rico the rate of bed illness which was respiratory in nature exceeded by far any other general cause. This, in large measure, may be attributed to an epidemic of influenza. Conditions described as malaria, puerperal illnesses (including normal labor), and gastrointestinal disorders followed in the order named. The reported diagnoses of the more common conditions, in order of fre quency, were as follows: Influenza and grippe, malaria, confinement, digestive disturbances, whooping cough, accidents, local infections of the sldn and cellular tissue, mumps,and skin diseases and parasites. While tuberculosis was seldom reported as such by the surveyed families, the illness picture was not inconsistent with the generally accepted idea that it represents a major illness problem on the island. The failure of data to provide a coimt of cases is due,in a large measure to the fact that tuberculosis was reported under symptomatic diag noses such as fever, hemoptysis, anemia, pain in the chest, lung trouble, cough and fever, wealaiess, and fatigue. Other evidence supporting this assumption hes in the fact that many cases of illness described by these general symptoms involved long periods of confine ment to bed.
In the five-county study an entirely different order of frequency is presented when all bed illnesses are classified by the same broad disease categories. It will be remembered that the total illness rate here is decidedly lower than in Puerto Rico. The highest specific-
illness rate in the counties was caused by acute communicable dis eases. The epidemic of measles, previously referred to, was partly responsible for the fact that this rate was four times as high as the corresponding one in Puerto Rico. Wliile the rate of gastrointestinal disturbances reported in the counties exceeded that of Puerto Rico, this, no doubt, was due to the fact that indefinite diagnoses, such as indigestion and stomach trouble unqualified, swelled the total for the counties. Such Ulnesses as diseases of the kidneys, heart, and blood vessels; disorders of the eyes, ears, nose, and throat; diseases of the bones, joints, and muscles; and tumors probably attained higher rates in the counties than in Puerto Rico because of the greater tend ency on the continent to obtain medical diagnosis and thus assign symptoms to the organs or parts of the body involved. Moreover, the people of Puerto Rico are not likely to rest in bed imless the illness has a large element of disability. The illness picture of Puerto Rico becomes most unfavorable when rates of respiratory and malarial conditions are compared with corresponding ones in the counties. Puerto Rico also showed an excess of puerperal conditions. This is to be expected in view of the facts that the birth rate for the island as a whole is relatively Irigh, and that the majority of the puerperal con ditions listed constitute cases of normal labor. While childbirth may not be considered a true illness in every sense of the word, yet it represents a definite need for medical care and so is included as a type of iUness for the purposes of this report.
To determine which types of ULness were more prevalent in the country than in cities or to\vns, all reported illnesses were classified according to broad disease categories, and the urban and rural rates were computed for each. Rural rates significantly exceeded urban for the following types of illness: Respiratory, conditions described as malaria, and acute communicable diseases. Some excess of puer peral illnesses was also noted in the rural population. No essential difference was found between the urban and rural groups for any other iUness category.
An analysis was made of illness rates in broad disease categories by geographic regions of the island. The purpose of this study was to ascertain which types of illness were responsible for the high illness rates in different sections. The most important difference between the rates of the south and west coasts and those of the north and east coastal regions lay in the amount of respiratory illness in the two areas. A rate of 236 was recorded in the municipalities of the south and west coasts, as compared with 172 for the interior, and 154 for the municipalities along the north and east shores. The area in the center of the island had less than one-half the rate of illness from conditions described as malaria as was reported by either coastal area. Gastrointestinal disorders also maintain a considerably lower rate in the interior.
The rate of acute communicable diseases, however, was higher in the interior than in cither area along the coast.
Deaths in sample population.—From the total sample population of 31,756 individuals, 550 deaths were reported by the family informant as having occurred during the 12-month period preceding the canvass. Of this number, 145 deaths, or more than one-fourth of the total number, were attributed to respiratory illnesses. This is not surpris ing, however, when one recalls that data on the prevalence of illness revealed that 45 percent of the cases of sicloiess confining the patient to bed were of a respiratory nature. Other conditions given as fre quent causes of death were: Gastrointestinal disorders, malaria, malnutrition of young cliildren, and diseases of the kidneys, heart, and blood vessels.
All deaths reported to the canvassers resulted in a death rate of 17 per 1,000 sample popxilation. This rate is somewhat lower than the 19.2 deaths per 1,000 population for the entire island as published by the Census Bureau for 1934, but failure to get a record of all deaths which occur during a study period is a recognized discrepancy in sm^vey methods. In the five study counties of the United States already referred to, the death rate among the sample population was found to be 7.5 per 1,000 individuals, or less than half that of the sample population in Puerto Rico.
An analysis of the Puerto Rican deaths occiirring within the study year revealed that 38 percent of the persons who died were less than 5 years of age. When deaths of infants under 1 year were related to the total number of live births for the year, it was found that the infant mortality rate for the sample population under consideration was 81 infant deaths per 1,000 live births. This rate of infant mor tality, as well as the total death rate, was lower than that of the entire island for 1934. According to published reports there were, in aU Puerto Rico, 113 infant deaths per 1,000 five births. Since the differ ence between the survey and published figures for infant mortality is even greater than for total death rates, one might assume that many of the deaths not reported to the canvassers were those of infants.
Illness as expressed by experience oj individuals and jamilies.—-All findings of the survey which have already been presented in this report have dealt with the incidence and nature of illness as expressed by actual cases reported. In other words, the condition has been the unit of consideration. Attention is now directed to the illness experi ence of the individual and of the family. It was found that relatively few persons reported more than 1 illness. Considering the entire sample population of 31,756 individuals, 63 percent had no illness, 33 percent had 1 illness, and 4 percent had more than 1. When the experience of the family as a whole was studied, it developed that 22 percent of all families were entirely free from bed illness during the
study year;45 percent suffered 1 or 2 illnesses, and 33 percent reported 3 or more. Upon comparing the illness record of urban famihes with that of the families of rural areas, the latter group appeared at a dis tinct disadvantage. Twelve percent of these families, and only half that proportion of the urban, had 6 or more illnesses during the year.
From data presented in foregoing sections it is apparent that the siclaiess hurden of the people of Puerto Rico is a heavy drain on their limited financial resources. It will also he recalled that the average number of persons per family for the island as a whole was 5.3 and that the average annual family income for a representative study group was $229. About 90 percent of the families included in the survey reported incomes of less than $500. Under such ch'cumstances only a very small percentage of families, those comprising the economically privileged group, could be expected to meet the costs of medical care through their private resources. The great majority do not have sufficient income to provide food, shelter, and clothing in amounts necessary to afford health and a reasonable degree of comfort. There is no large group vdth moderate income that might purchase medical service if the costs were distributed over time and through the popula tion by some prepaj'ment or insurance scheme. Because of these economic considerations medical care in Puerto Rico, for most of the population, must be a public service supported through taxation.
While the municipal governments constitute the primary agencies for providing medical care, it would be misleading if one were to exclude from consideration those facilities that are represented by private physicians, voluntary hospitals, local health units, and the institutions of the insular health department.
Physicians.—The total number of physicians in Puerto Rico is 436. Of this number 228 are located in the 5 first-class municipalities, 145 being in San Juan alone. In the 23 second-class municipalities, there are 131 physicians, and the remaining 77 physicians are divided among 43 of the third-class municipalities. Five third-class munici palities have no resident physician. A large percentage of the 41 physicians residing in Rio Piedras and Bayamon—both suburbs of San Juan, but rated as second-class municipalities—have offices in San Juan. Thus, in effect, the number of physicians practicing in the San Juan area is increased to 186, and the number available to the entire group of second-class municipalities is reduced to 90. From these fio'ures it is evident that the smaller and more rural municipalities suffer most from the lack of medical personnel. Table 11 shows the 137004—37 -•')
distribution of ali physicians on the island by connection as well as by class of municipality.
Table 11.—-Number of first-, second-,and third-class municipalities of Puerto Rico having resident physicians, and total nwnher of physicians according to connection residing in each class
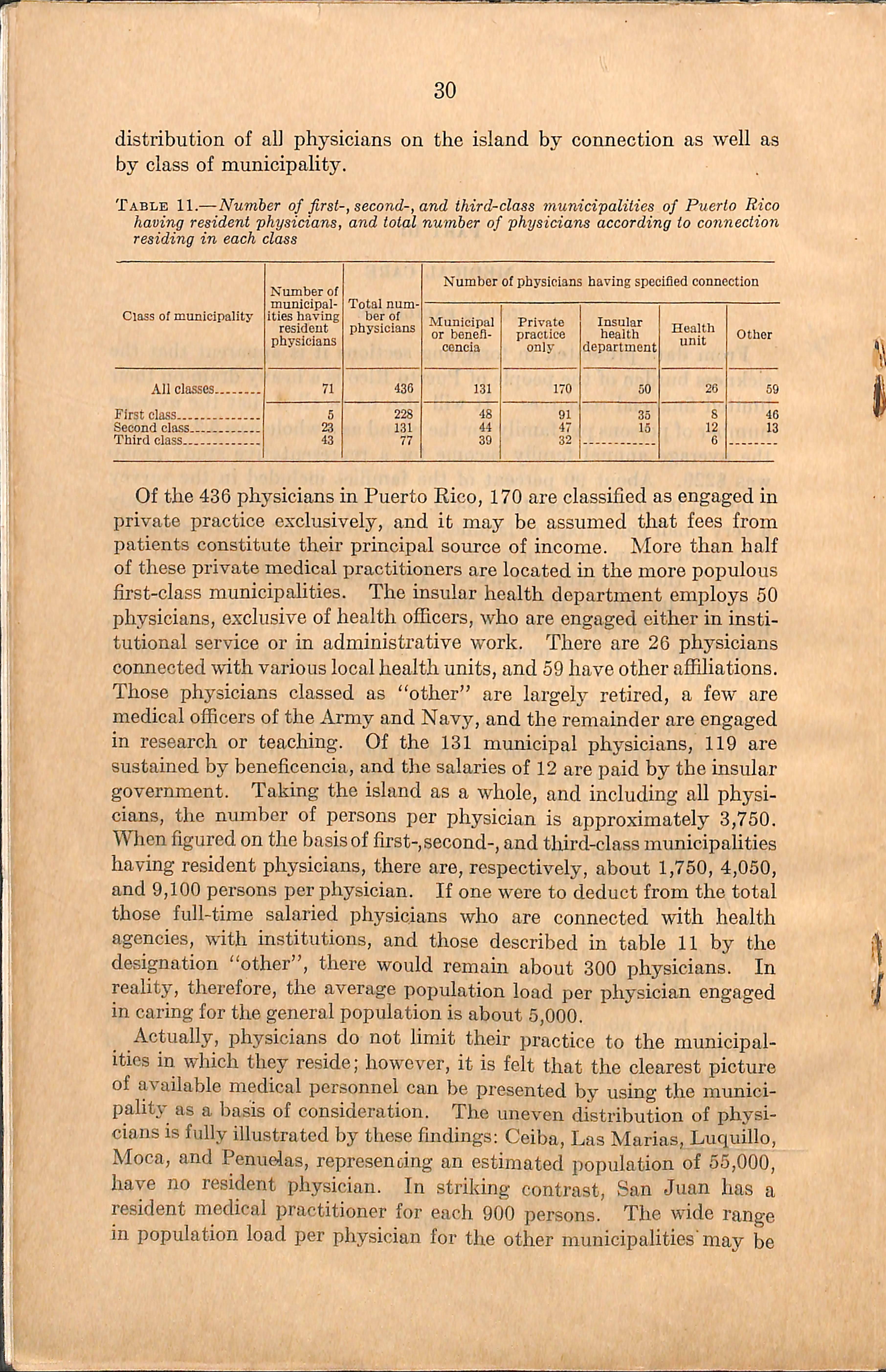
Of the 436 physicians in Puerto Eico, 170 are classified as engaged in private practice exclusively, and it may be assumed that fees from patients constitute their principal source of income. More than half of these private medical practitioners are located in the more populous first-class municipalities. The insular health department employs 50 physicians, exclusive of health officers, who are engaged either in insti tutional service or in administrative work. There are 26 physicians connected with various local health units,and 59 have other affiliations. Those physicians classed as "other" are largely retired, a few are medical officers of the Army and Navy,and the remainder are engaged in research or teaching. Of the 131 municipal physicians, 119 are sustained by beneficencia, and the salaries of 12 are paid by the insular government. Taking the island as a whole, and including all physi cians, the number of persons per physician is approximately 3,750. When figured on the basis of first-,second-,and third-class municipahties having resident physicians, there are, respectively, about 1,750, 4,050, and 9,100 persons per physician. If one were to deduct from the total those full-time salaried physicians who are connected with health agencies, with institutions, and those described in table 11 by the designation "other", there would remain about 300 physicians. In reality, therefore, the average population load per physician engaged in caring for the general population is about 5,000.
Actually, physicians do not limit their practice to the municipal ities in which they reside; however, it is felt that the clearest picture of available medical personnel can be presented by using the munici pality as a basis of consideration. The uneven distribution of physi cians is fully illustrated by these findings; Ceiba, Las Marias, Luquillo, Moca, and Penuelas, represencing an estimated population of 55,000, have no resident physician. In striking contrast, San Juan has a resident medical practitioner for each 900 persons. The wide range in population load per physician for the other municipalities'may be
appreciated when one finds that in 17 municipalities a single physician is responsible for the care of 1,000 to 5,000 inhabitants; in 33 municipaUties the corresponding ratio is between 5,000 and 10,000 persons per physician;in 13, between 10,000 and 15,000; and in 7, over 15,000. The responsibility resting upon municipal physicians only will he discussed in the section treating municipal facilities.
Dentists.—The people of Puerto Rico are served by 143 dentists. Dentists as well as physicians have, congregated in the larger cities. In the 5 first-class municipalities there are 88 dentists; 46 are located in 19 of the 23 second-class municipalities; and only 9 are found in 6 of the 48 third-class municipalities. The need for additional dental service can well be appreciated when one considers that there are 42 third-class municipalities, representing a population of 572,775, and 4 second-class municipalities, representing 56,250 persons, without a single practicing dentist. When only the municipalities which have 1 or more practicing dentists are considered, the number of persons per dentist is about 4,500 for the first-, 10,500 for the second-, and 14,000 for the third-class group of municipalities. Eight of the dentists in the first-class municipalities and 6 in the second class are employed by beneficencia, usually for part-time service. The distribution of den tists, even more than that of phj'^sicians,is determined by the economic position of people in the several sections of the island.
General hospitals.—The island of Puerto Rico has 97 general hospital buildings, though 7, belonging to municipalities, are not used for care of patients. Of the total number, 61 belong to the municipalities; 34 are privately owned; and 2 district general hospitals are operated by the insular health department. Table 12 shows the distribution of these general hospitals according to class of municipality, and the number of hospital beds represented by each.
Table 12.—Total number of general hospitals and their bed capacities in first-, second-, and third-class municipalities of Puerto Rico according to ownership of hospitals
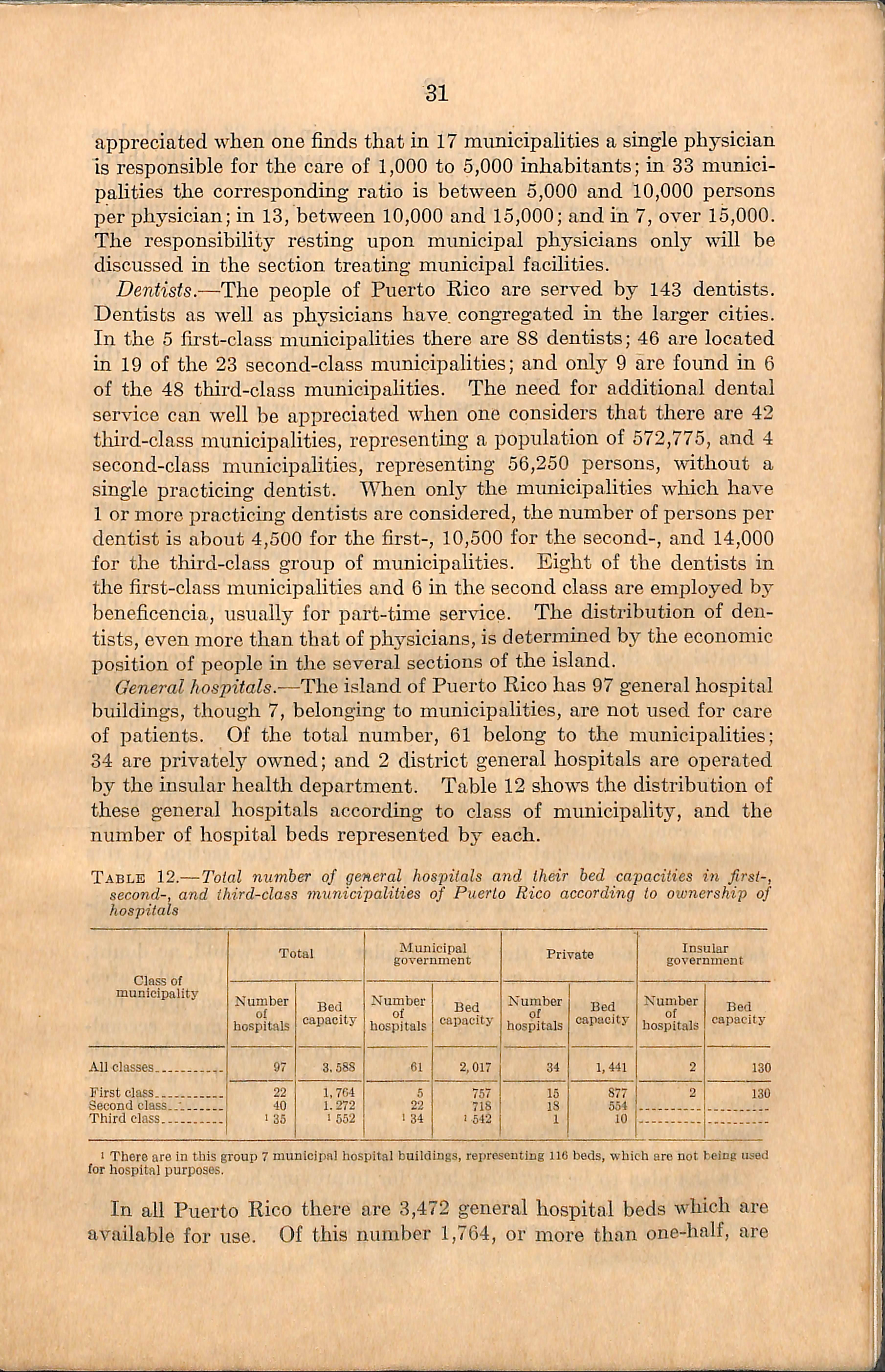
I There are in this group 7 municipel hospital buiidings, representing 116 beds, which are not being used tor hospitai purposes.
In all Puerto Rico there are 3,472 general hospital beds which are available for use. Of this number 1,764, or more than one-half, are
in the 5 first-class municipalities; 1,272 are in the 23 second-class municipahties; and 436 are in 27 of the 48 municipalities of the thirdclass group. Considering the island as a whole, there is 1 available hospital bed for every 470 persons. In the first-class municipalities the ratio is 225 persons per hospital bed; in the second-class group, about 425 persons per bed; and in the tliird, where hospitals are in use, there is only 1 available hospital bed for each 945 persons. No hospital beds are available in 21 of the tliird-class municipalities which have a total population of approximately 287,500.
With one exception, privately owned hospitals are located in the first- and second-class municipalities. Lares is the only third-class municipality having a privately owned general hospital. The capacity of this institution is 10 beds. The 7 private hospitals in San Juan have a total capacity of 425 beds and the 3 in Ponce have 288 beds. Two of those in San Juan and 2 in Ponce have between 100 and 130 beds each. The only other private hospital vnth more than 100 beds is located in Rio Piedras, a second-class municipahty, but really a suburb of San Juan. There are 150 beds in tliis hospital. Each of the 5 first-class municipalities and aU but 1 of the secondclass group have a municipal general hospital. San German is the exception. This municipality, however, contracts with a private hospital for the use of 25 beds by patients admitted through the beneficencia office. In the third-class group 34 of the 48 munici palities have a municipal hospital, although 7 of these buUdings are not in use for hospital purposes. Generally speaking, the capacity of municipal hospitals varies with the class of municipality. The average number of beds in hospitals owned by first-class municipalities is about 150, as contrasted with an average of 33 beds in the hospitals of the second, and 16 beds in those of the third class. A more detailed discussion of municipal hospitals will appear in the section of this report devoted exclusively to municipal facilities.
It must be recognized, of course, that, while the first class munici palities have a striking advantage over the other two groups in all facilities for the care of the sick, a similar situation would, no doubt, be found in the study of many areas of the continental United States, since the larger cities generally have more and better equipped hos pitals than are found in rural sections. In reality, many secondand third-class municipalities are unable to support the hospitals they now have. The presence or absence of a hospital in a munici pahty should not be interpreted as expressing the availability of hospital facilities, since service can be obtained on a contractual basis from hospitals located in neighboring municipalities.
In the plan to be suggested later for improving hospital service in rural municipalities, the insular health department is to play a promi nent role. For this reason, and because the insular health department
is a participant in several fields of health service, a brief discussion of its organization and facilities is in order.
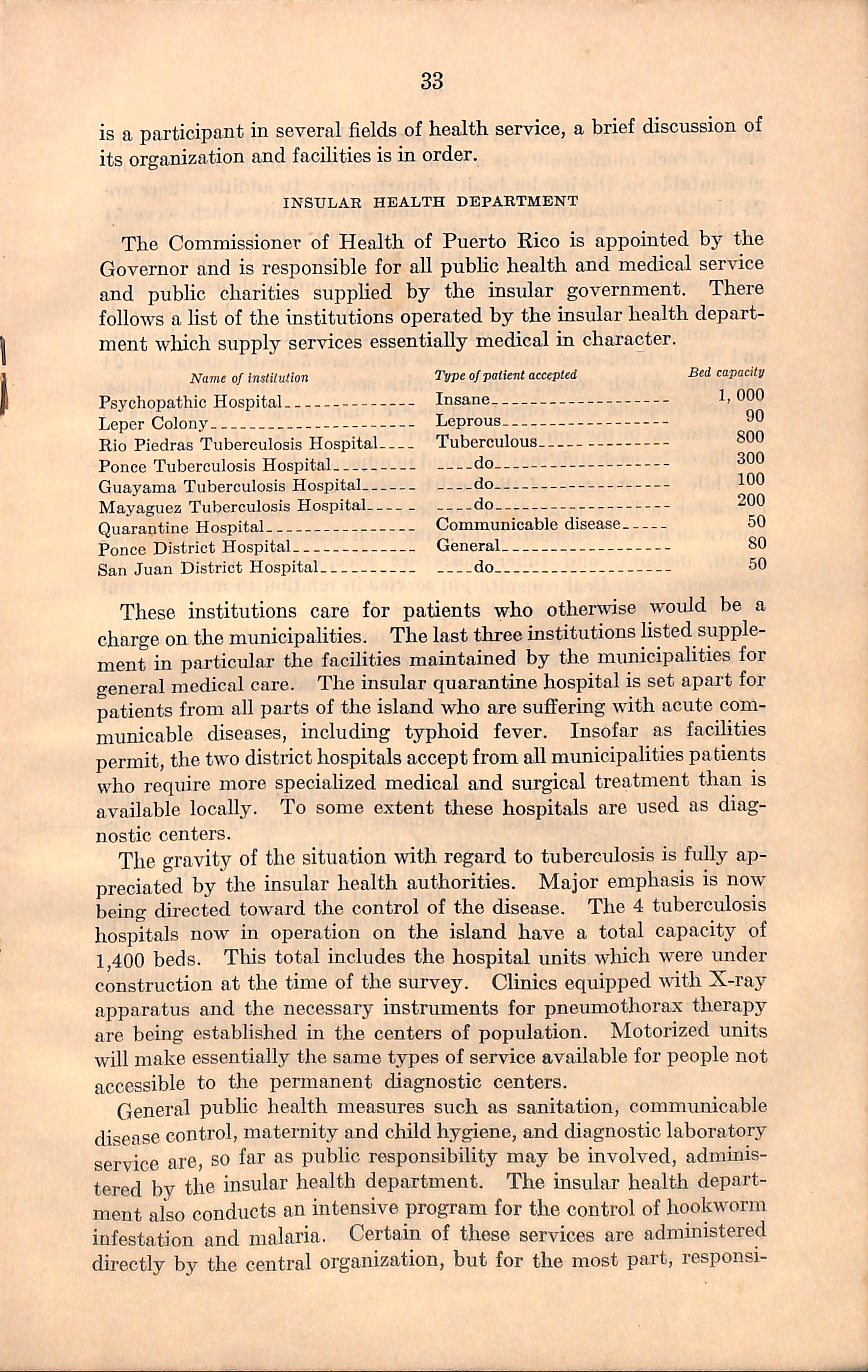
The Commissioner of Health of Puerto Rico is appointed by the Governor and is responsible for all public health and medical service and public charities supplied by the insular government. There follows a list of the institutions operated by the insular health depart ment which supply services essentially medical in character.
Name of instilution
Psychopathic Hospital
Leper Colony
Rio Piedras Tuberculosis Hospital
Type ofpatient accepted
90
Ponce Tuberculosis Hospital do 000
Guayama Tuberculosis Hospital do Mayaguez Tuberculosis Hospital do
Hospital
These institutions care for patients who otherwise would be a charge on the municipalities. The last three institutions listed supple ment in particular the facilities maintained by the municipalities for general medical care. The insular quarantine hospital is set apart for patients from all parts of the island who are suffering with acute com municable diseases, including typhoid fever. Insofar as facilities permit,the two district hospitals acceptfrom all municipalities patients who require more specialized medical and surgical treatment than is available locally. To some extent these hospitals are used as diag nostic centers.
The gravity of the situation with regard to tuberculosis is fully ap preciated by the insular health authorities. Major emphasis is now being directed toward the control of the disease. The 4 tuberculosis hospitals now in operation on the island have a total capacity of 1,400 beds. This total includes the hospital units which were under construction at the time of the survey. Chnics equipped with X-ray apparatus and the necessary instruments for pneumothorax therapy are being established in the centers of population. Motorized units will make essentially the same types of service available for people not accessible to the permanent diagnostic centers.
General public health measures such as sanitation, communicable disease control, maternity and child hygiene, and diagnostic laboratory service are, so far as public responsibility may be involved, adminis tered by the insular health department. The insular health depart ment also conducts an intensive program for the control of hookworm infestation and malaria. Certain of these services are administered directly by the central organization, but for the most part, responsi-
bility is discharged through local personnel. The minimum health staff of each municipahty is a sanitation officer who is paid by, and accountable to, the insular health department. In addition there are 24 health organizations known as public health units which serve 54 municipalities. The insular health department accepts major admin istrative and financial responsibility for these organizations, but in most cases there is some participation by the municipalities. Each of the 5 first-class municipahties has a health unit; 20 of the 23 secondclass municipahties are served by 14 health units and 6 sub-units; and in the third-class municipalities there are 5 health units and 24 sub-imits which render public health service to 29 municipalities. In most respects these organizations are comparable to county health departments of the continental United States. A list of the personnel employed by each unit may be found in appendix D.
While the program of the health units is primarily preventive in character, a large amount of medical service is rendered. Patients known to have or suspected of having such diseases as syphilis, hook worm, malaria, and tuberculosis are accepted for diagnosis and treatment. Medical consultation service in relation to maternal and child health may be obtained at special clinics.
From the foregoing discussion, it may be seen that the insular health department has certain clear-cut responsibilities in the broad field of medical care and that it has already taken definite steps to aid the municipals ties in the handling of particular problems relating to care of the sick.
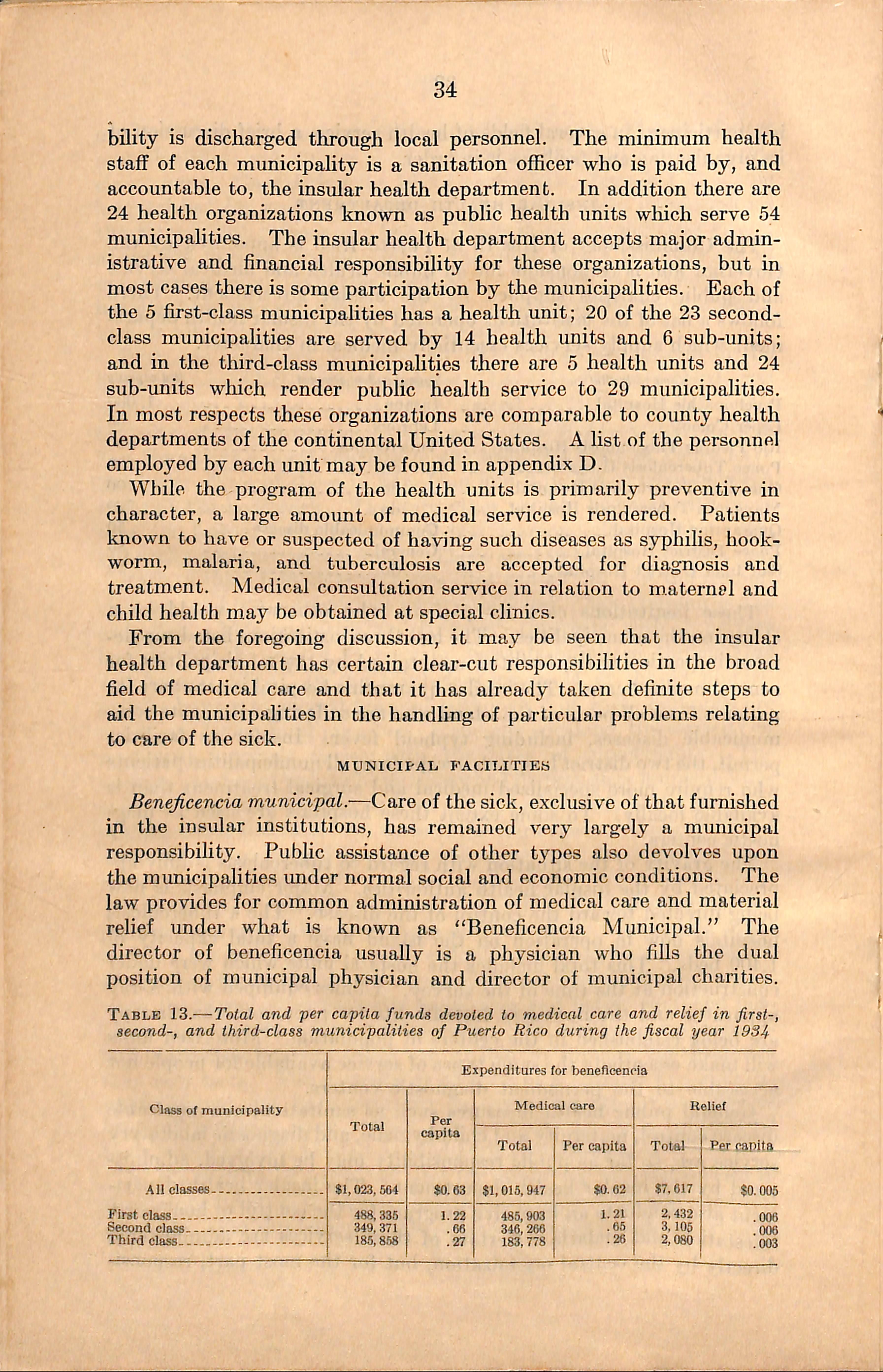
Benejicencia municipal.—Care of the sick, exclusive of that furnished in the insular institutions, has remained very largely a municipal responsibihty. Public assistance of other types also devolves upon the municipalities under normal social and economic conditions. The law provides for common administration of medical care and material relief under what is known as "Beneficencia Municipal." The director of beneficencia usually is a physician who fills the dual position of municipal physician and director of municipal charities.
Table 13.—Total and per capita funds devoted to medical care and relief in first-, second-, and third-class municipalities of Puerto Rico during the fiscal year 1934
Expenditures for benedceneia
Table 13 presents data shomng expenditures for beneficencia by the three classes of municipalities. Those funds reported for medical care include amounts expended for the employment of mumcipal physi cians, operation of municipal hospitals, and the purchase of medical and surgical supphes used in the care of the indigent sick.
At the time of the survey it was reported by persons familiar with medical problems of the island that approximately 80 percent of the population was dependent, in part at least, on the municipalities for medical services. This estimate is not inconsistent with the survey findings on approximately 13,000 cases of illness which will be pre sented later. While the funds assigned to medical care obviously are not sufficient for providing adequate service to those in need, it may he said in extenuation that the mimicipalities allocate a reasonable share of their total revenue to this purpose. First-class municipalities devote approximately 18 percent of their total budget to medical care, while those of the second class contribute 20 percent, and third class municipalities use about 16 percent of all budgetary receipts for this purpose. In a number of individual municipalities the amount devoted to medical care is about 30 percent of the total governmental costs. Beneficencia,in commoii with other piibhc services,is seriously crippled since most municipahties are not able to meet ordinary financial obligations. Of the 69 municipalities that filed reports, all but 8 had unpaid accounts for operating expenses incurred during the previous fiscal year. Twenty-one reported between 1 and 29 percent delinquency; 26 were from 30 to 59 percent delinquent; and 14 were in arrears for more than 60 percent of their operating expenses of the year before. According to data obtained directly from bene ficencia employees, no essential difference was noted between the classes of municipalities as to the length of time for which salaries had not been paid. Considering all municipalities whicli reported this item, salaries in 18 were paid to date; in 9, payment of part salary, at least, was from 1 to 6 months in arrears;in 16, the delinquency ranged from 7 months to 1 year; in 12 it was from 13 months to 2 years; and in 18 municipalities the unpaid period for either part or all of the salary was from 25 months to 5 years.
Beneficencia personnel engaged in medical service.—The entire per sonnel of aU municipalities whose salaries are paid from beneficencia funds, and whose duties are concerned with care of the sick, number 864. They are listed by types of training in table 14. The number of beneficencia physicians and their distribution by class of municipality have already been presented in the section devoted to all Puerto Rican physicians. In 5 second- and 18 tliird-class municipalities, having a combined population of 322,260, the municipal doctors constitute the only resident physicians and are the chief source of medical service. Considering municipal physicians only, the popula-
tion load per physician is nearly twice as great in the third-class municipalities employing physicians as in the first-class group, while the ratio of population to municipal physicians is one and one-half times as great in second-class municipalities as in the first. The respective population loads for municipal physicians in first-, second-, and third-class municipalities are approximately 8,350, 12,000, and 15,400. No tliird-class municipality employs more than 1 municipal physician, while in 9, there is no resident municipal doctor. Quite different is the record of first-class municipalities where the number of physicians maintained hy heneficencia ranges from 4 to 24.
Table 14.—Beneficencia 'personnel engaged in medical service in first-t second-, and third-class municipalities of Puerto Rico
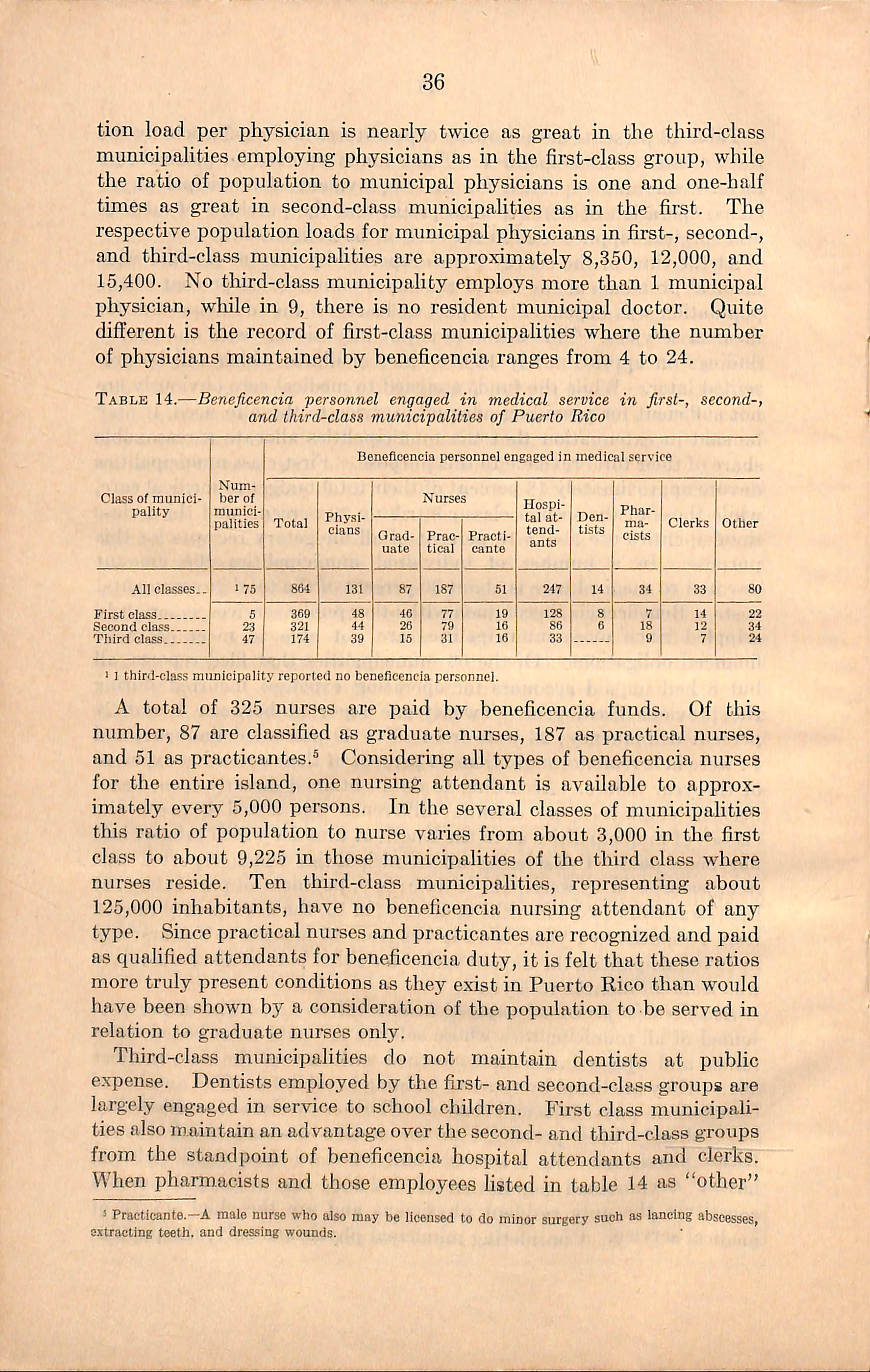
1 J third-class municipality reported no beneficencia personnel.
A total of 325 nurses are paid hy heneficencia funds. Of this number, 87 are classified as graduate nurses, 187 as practical nurses, and 51 as practicantes.® Considei-ing all types of heneficencia nurses for the entire island, one nursing attendant is available to approx imately every 5,000 persons. In the several classes of municipalities this ratio of population to nurse varies from about 3,000 in the first class to about 9,225 in those municipalities of the tliird class where nurses reside. Ten third-class municipalities, representing about 125,000 inhabitants, have no beneficencia nursing attendant of any type. Since practical nurses and practicantes are recognized and paid as qualified attendants for beneficencia duty,it is felt that these ratios more truly present conditions as they exist in Puerto Rico than would have been shown by a consideration of the population to be served in relation to graduate nurses only.
Third-class municipalities do not maintain dentists at public expense. Dentists employed by the first- and second-class groups are largely engaged in service to school children. First class municipali ties also maintain an advantage over the second- and third-class groups from the standpoint of beneficencia hospital attendants and clerks. When pharmacists and those employees listed in table 14 as "other"
^ Practicante.—A male nurse who also may be licensed to do minor surgery such as lancing abscesses, extracting teeth, and dressing wounds.
are considered, however, municipalities of the second class outrank those of the first.
From the foregoing data it is seen that the size of the beneficencia medical staff of the first-class municipahties is more nearly in keeping with the service needs than that of either the second or third class and that the second-class group is better in this respect than the third. Maricao is the only municipality without a single beneficencia em ployee. The entire system of beneficencia has been practically abandoned there.
During the last 10 years each of the 3 groups of municipalities has had an average of 4 different directors of beneficencia. In the first class gi'oup the nmnber of directors dming this period varied from 2 to 6. In the second-class municipalities the range in the number of directors of beneficencia for the 10-year period has been from 1 to 9. The third-class group reported 1 director for the entire time in each of 4 mimicipalities, while 20 mimicipahties,in strildng contrast, had from 5 to 7 directors. The figiues quoted show the extremes in behavior for mimicipalities of each class. The most frequent experience in munic ipalities of all classes was from 2 to 4 directors. Thus it may be appreciated how unstable the position of director, commonly known as mvmicipal physician, actually is.
Besides being used to employ the personnel just described for the care of the sick, beneficencia funds are also devoted to the purchase of medical supplies. About $160,000 was spent by beneficencia of the entire island for medicines dming the fiscal year 1934. The first-class municipalities spent approximately $67,000, the second, $53,000, and the third, $40,000.
Some mimicipalities have a pharmacy for fiUing prescriptions of beneficencia patients; other municipalities have a contract vith some private drug store whereby the poor can secure medicines upon pre senting an order from the municipal physician; while still other municipalities use a combination of these two plans. Generally speaking, the first-class municipalities favor the plan of supplying medicines from the municipal pharmacy; the third class tend to con tract with private firms more frequently than any other class; and a higher percentage of second-class municipalities than any other obtain some of their drugs by the combined methods.
Funds available for drugs and other medical supplies seldom are adequate; consequently, patients often are expected to make pur chases with personal funds. This, in many cases, they are unable to do.
Municipal hospitals.—The number of mimicipal hospitals in Puerto Rico, their location by class of municipality, and their average size were shown in table 12. It was also stated that seven mimicipal
hospitals of the third-class municipalities are not used lor the care of patients. Municipal hospitals not in use for care of patients are located in Adjuntas, Camuy, Jayuya, Maricao, Morovis, Penuelas, and Toa Baja. These hospital buildings are generally used for the office of beneficencia, the housing of the health imit, or the municipal pharmacy. The Morovis hospital, however, is closed. Figure 13 shows the municipalities having mimicipal hospitals which are used for the care of patients, as well as those whose mimicipal hospital build ings are not in use as such. It woidd appear from the diagram that Puerto Rico is well provided with municipal hospitals. Unfortunately the number of hospital buildings in no way indicates the actual facilities available for service. Several of the hospitals have a rated capacity of less than five beds each and are equipped for little more than first-aid work, while in other instances only a small proportion of the available space is furnished and used for hospital service. In fact, the large number of poorly maintained hospitals represents a problem rather than a solution in the field of medical care. Reference has already been maae to the limited resoinces of the individual munic ipalities. The state into which many of the hospitals have deterior ated is a reflection of this low income and of the misguided policy which encouraged indiscriminate hospital building without regard to the ability of the municipalities to maintain them properly.
The 5 tax-supported hospitals in the first-class municipalities are used for the care of patients. Patients are admitted to all 22 municipal hospitals of the second-class municipalities. Twenty-seven out of 34 municipal hospitals in the third-class municipalities are used for the care of patients. However, several of these hospitals may more accurately be rated as first-aid stations. In one hospital no overnight patients are accepted. No municipal hospital facilities are available in the municipalities of: Adjuntas, Camuy, Catano, Ceiba, Cidra, Corozal, Guaynabo, Isabela, Jayuya, Las Marias, Maricao, Moca, Morovis, Naranjito, Orocovis, Penuelas, Rtncon, Rio Grande, Toa Baja, Trujillo Alto, and Villalba. San German also is without a municipally owned hospital, but has a contract with a private hospital under which 25 beds are set apart for beneficencia patients.
The relative utilization of available municipal hospital beds by the several classes of municipalities is shown in table 15. Only municipal hospitals which admit patients are considered. Therefore,those seven hospitals which are not used for care of the sick are omitted. It has already been brought out that the first class municipalities have more nearly adequate hospital faciities than either of the other gi-oups, and that the second class municipalities have more available beds in pro portion to the population than the third. One would assume, there fore, that the hospitals of the third-class municipalities would be the most crowded of any group. However, when a count was made of
PUERTO RICO BY MUIMICIPALITIES MUNICIPALITY HAVING MUNICIPAL HOSPITAL IN USE FOR CARE OF PATIENTS.
MUNICIPALITY HAVING MUNICIPAL HOSPITAL NOT IN USE FOR CARE OF PATIENTS.'' viEquEs_ I I MUNICIPALITY HAVING NO MUNICIPAL HOSPITAL.>i^
•ySAM GERMAN CONTRACTS WITH A PRIVATE HOSPITAL FOR CARE OF INDIGENT PATIENTS AT MUNICIPAL EXPENSE.
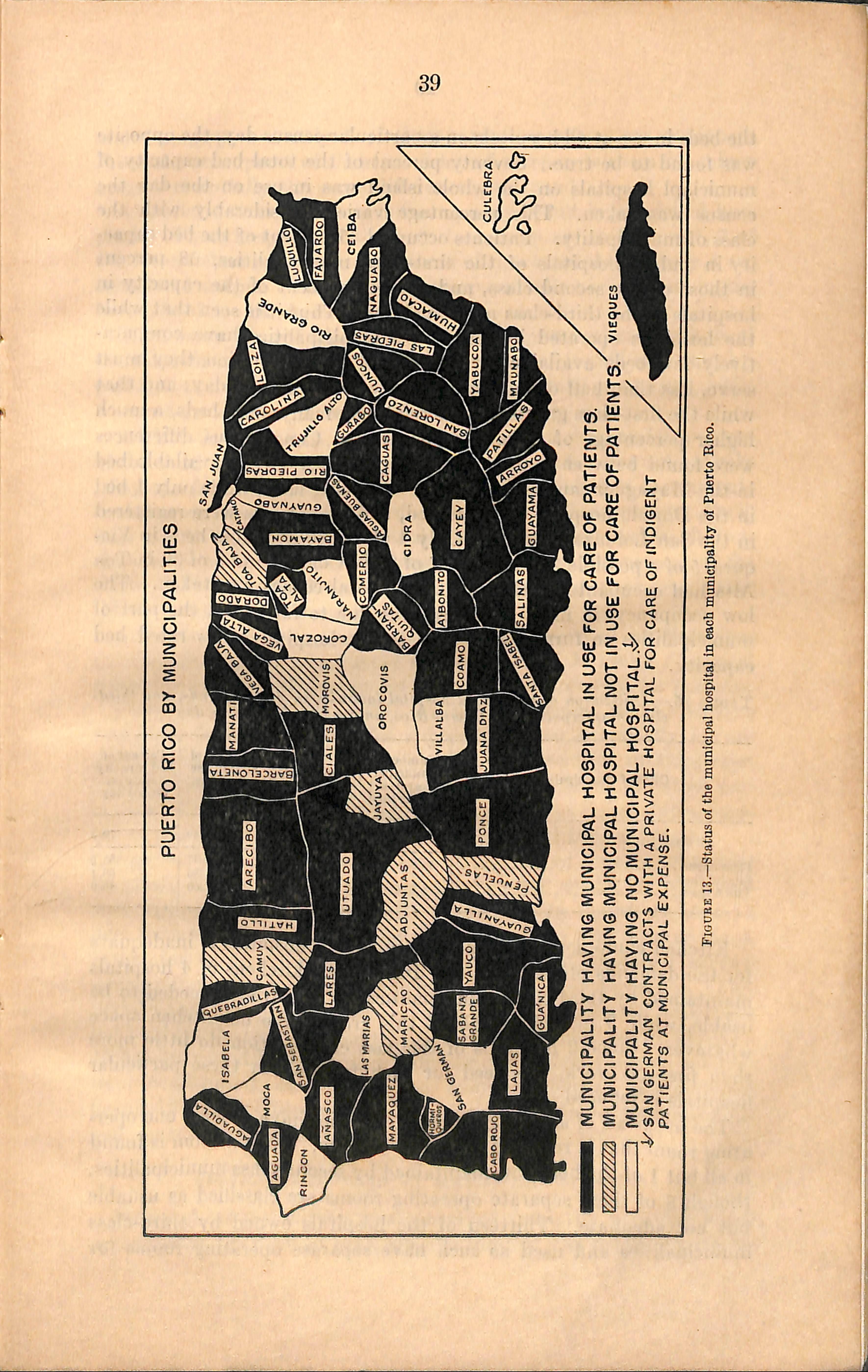
Fiocbe 13.—Status of the municipal hospital in each municipality of Puerto Rico.
the beds in use at all hospitals on a particular census day, the opposite was found to be true. Seventy percent of the total bed capacity of municiapl hospitals on the whole island was in use on the day the census was taken. This percentage varied considerably with the class of municipahty. Patients occupied 85 percent of the bed capac ity in public hospitals of the first-class municipalities, 68 percent in those of the second class, and only 47 percent of the capacity in hospitals of the third-class municipalities. Thus it is seen that while the hospitals operated by third-class municipalities have compara tively few beds available for the size of the population they must serve, less than half of those were in use on the census day; and that while the first-class group provide relatively many more beds, a much higher percentage of them were occupied. Conspicuous differences were found between individual municipalities. Every available bed in the Mayaguez mimicipal hospital was being used, while only 1 bed in the Dorado hospital was occupied, and no patients were registered in the San Lorenzo hospital. Only 4 of the 30 available beds in Vie ques, 5 of a possible 22 in Ciales,7 of 25 in Coamo, and 3 of 30 in Toa Alta had occupants on the day the hospital census was taken. The low occupancy, in most instances, was due to failure on the part of municipalities to furnish and operate the hospital at its rated bed capacity.
Table 16.— Ulilizaiion of municipal hospital faciliiies in first-, second-, and thirdclass municipalities of Puerto Rico, on a particular census day
Kitchen equipment in almost aU municipal hospitals is inadequate for the demands placed upon it. Indeed, the kitchens of 4 hospitals maintained by third-class municipalities are not even conceded to be usable, while 3 more hospitals of this group have no kitchen space whatever. Since 2 hospitals of this last classification do little more than first-aid work, the need for such facilities in these particular hospitals is reduced.
The hospitals of all first-class municipalities have at least one opei*ating room that is reserved for major surgery. Such a room is found in all but 1 of the hospitals maintained by second-class municipalities, though 8 of these separate operating rooms are classified as usuable but not adequate. Thirteen of the hospitals owned by third-class municipalities and used as such have separate operating rooms for
major surgery, but only 5 of these operating rooms are equipped. From the standpoint of their provision of a separate room fdr minor surgery essentially the same differences are found.
A special delivery room is not commonly found in municipal hos pitals. Three hospitals of the first-class group are so equipped; 7 of the second class have a separate room of this type, though only 4 are considered usable. Such facUities are practically nonexistent in the hospitals of the third-class municipahties.
There is no clinical laboratory or X-ray equipment in hospitals of the third-class municipalities. Four hospitals of second-class munici pahties and 3 of the first-class have some laboratory equipment, while 1 second-, and 4 first-class hospitals own an X-ray unit.
All first-class hospitals,64 percent of the second class, and 22 percent of the third describe their surgery instruments as fair but not entirely adequate for their needs. At the remaining hospitals instruments could scarcely be considered satisfactory even for minor surgery. Facilities for sterilizing instruments and dressings are provided in aU firstclass hospitals, 55 percent of the second class, and 37 percent of the third. This equipment, as a general rule, is in such poor repair that effective sterilization cannot be insured.
An ambulance is o^vned by all hospitals provided by first-class municipalities and 6 hospitals of the second-class, but only 1 hospital belonging to the tliird-class group can offer transportation for patients.
From this description of the equipment present in the various municipal hospitals, it \vill be appreciated that practically aU are deficient in most respects but that hospital facilities in third-class municipalities are far below those in municipalities of the other two classes. Very few of the hospitals woidd be rated as acceptable accord ing to standards which prevail in the continental United States.
Figures 14 and 15 represent two of the better type of municipal hospitals. Both of these buildings are in good repair, are relatively well equipped, and are efficiently operated. In figures 16 and 17 one recognizes municipal hospitals wliich have deteriorated to a rather low state. First-aid work constitutes the principal service which either of these institutions is now in position to render. Fig ures 18 and 19 represent that group of municipal hospitals which are not used for the care of patients. In fact, the hospital shown in figure 19 has been used for tliis purpose during only 1 year since its comple tion, emphasizing once more the overdevelopment of municipal hospital building where resources are insufficient to insure continuous and satisfactory operation.
SERVICES EENnERED BY MUNICIPAL FACILITIES
Inasmuch as this survey was concerned primarily with municipal organization for medical care, specific inquiiy was made relative to
the service rendered through facihties supported by the municipal governments. For purposes of description, the services provided by municipal governments, commonly known as beneficencia, are con sidered under two headings: Ambulatory and domicihary care by municipal physicians, and service by municipal hospitals. In reality, the two services operate as one. The beneficencia physician always is employed for home and office care, but he treats patients in the municipal hospital should one be maintained.
Service reported hy beneficencia physicians.—OSicq calls constitute the major part of all service required of municipal physicians. Under the system of medical practice that prevails in most beneficencia offices, one physician often will see 50 or more patients in the average office period which occupies, as a rule, between 3 and 4 hours. A single patient is seldom allotted more than 5 minutes of the physician's time. Remedies are prescribed as a rule after a cursory review of the symptoms, and only occasionally is a physical examination made. Many patients do not even see the physician; instead, medicines and supplies are given to a neighbor or member of the family who describes the symptoms to the physician. In some beneficencia offices minor surgery is performed by the practicante, and surgical dressings are applied by him or by some other attendant who may be a practical or graduate nurse. It was not possible to secure satisfactory data with which to describe the total service of all municipal phj^sicians .In a later section of the report an account will be given of that part which was reported by families included in the special illness survey.
Service reported hy municipal hospitals.—^Most municipal hospitals render service which is general in character. In some, however, the service is seldom more than first aid. Table 16 presents the number of admissions reported by municipal hospitals and the admission rate per 1,000 population. The patients, with very few exceptions, were residents of the municipalities where the hospitals are located. In the first-class group 38 cases per 1,000 population were hospitalized through beneficencia during the year. The admission rate was 24 in the 21 second-class municipalities for which records were available, and 10 in those 22 third-class municipalities which had hospitals, and for which a record of patients was kept. Thus it is seen that the rate of admission is almost four times as high in the first class as in the third having municipal hospitals. Considering all municipalities wliich recorded hospital admissions, 25 cases per 1,000 population received hospital care during the fiscal year 1934. When the total number of admissions reported by municipal hospitals is related to the population of the entire island, the admission rate becomes 19 per 1,000 population. Based upon the amount of bed illness reported by the surveyed popidation,it is estimated that an average of 4.5 percent of all bed illnesses are hospitaUzed in municipal institutions.
Figure 14.—A well-maintained municipal hospital of moderate size.
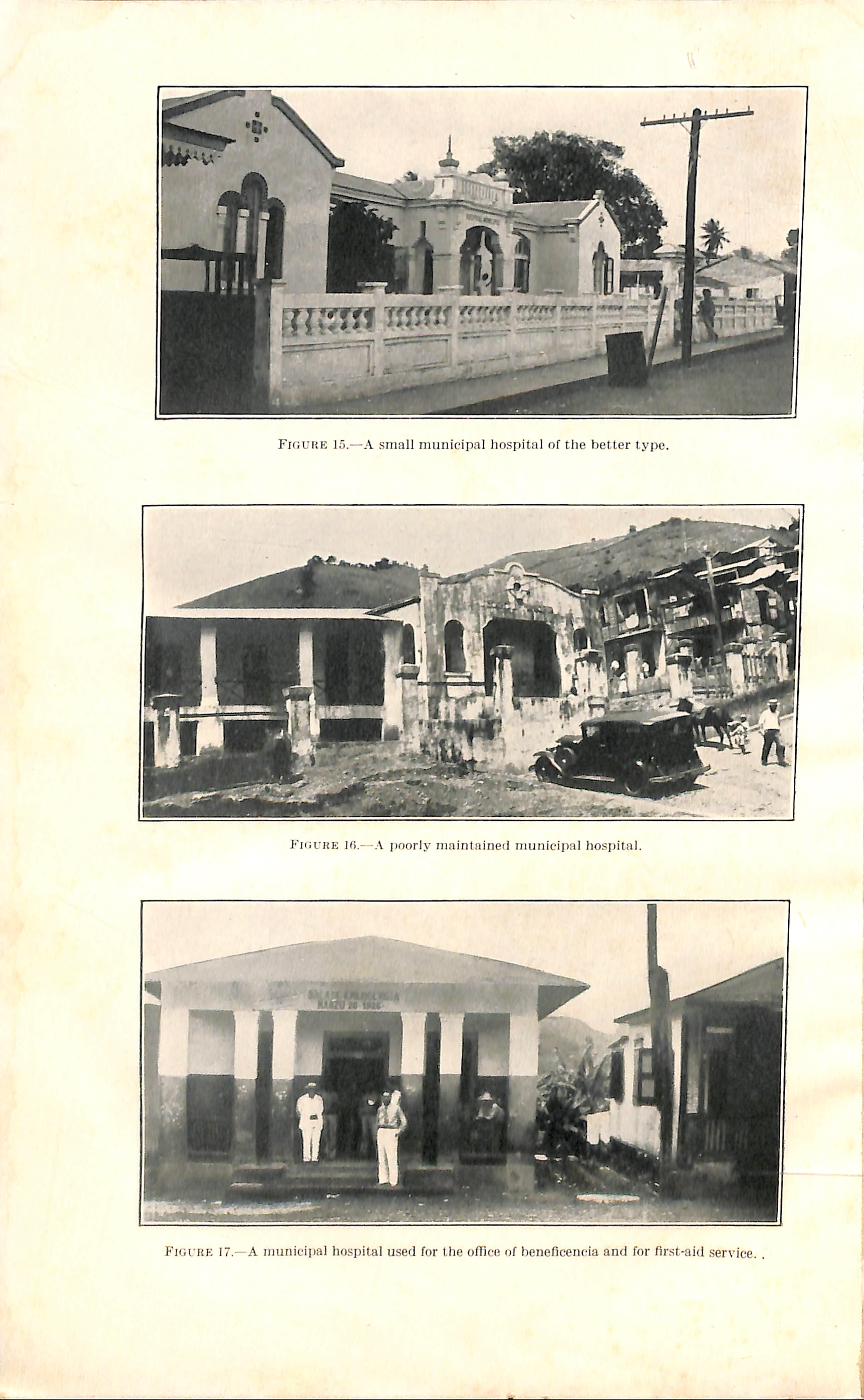
Table 16.—Number of first-, second-, and third-class municipalities of Puerto Rico supplying count of patients admitted to municipal hospitals, and the hospital ad missions for these municipalities during the fiscal year 1934
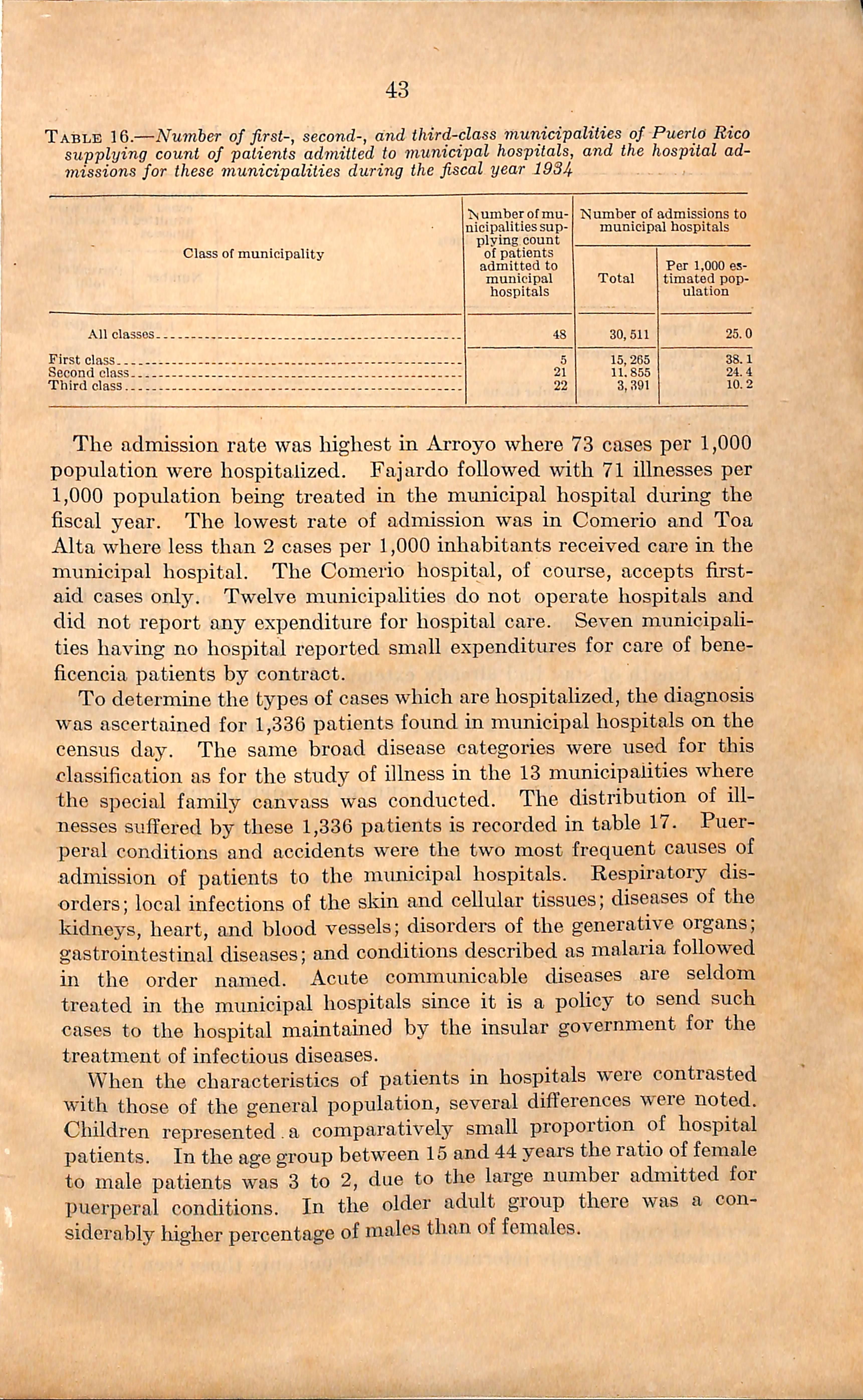
The admission rate was liighest in Arroyo where 73 cases per 1,000 population were hospitalized. Fajardo followed with 71 illnesses per 1,000 population being treated in the municipal hospital during the fiscal year. The lowest rate of admission was in Comerio and Toa Alta where less than 2 cases per 1,000 inhabitants received care in the municipal hospital. The Comerio hospital, of course, accepts firstaid cases only. Twelve municipalities do not operate hospitals and did not report any expenditure for hospital care. Seven municipali ties having no hospital reported small expenditures for care of heneficencia patients by contract.
To determine the types of cases which are hospitalized, the diagnosis was ascertained for 1,336 patients found in municipal hospitals on the census day. The same broad disease categories were used for this classification as for the study of illness in the 13 municipalities where the special family canvass was conducted. The distribution of ill nesses suifered by these 1,336 patients is recorded in table 17. Puer peral conditions and accidents were the two most frequent causes of admission of patients to the municipal hospitals. Respiratory dis orders; local infections of the skin and cellular tissues; diseases of the kidneys, heart, and blood vessels; disorders of the generative organs; gastrointestinal diseases; and conditions described as malaria followed in the order named. Acute communicable diseases are seldom treated in the municipal hospitals since it is a policy to send such cases to the hospital maintauied by the insular government for the treatment of infectious diseases.
When the characteristics of patients in hospitals were contrasted with those of the general population, several differences were noted. Children represented.a comparatively small proportion of hospital patients. In the age group between 15 and 44 years the ratio of female to male patients was 3 to 2, due to the large number admitted for puerperal conditions. In the older adult group there was a con siderably higher percentage of males tlnm of females.
Table 17.—Number and percentage of patients in all municipal hospitals on census day according to type of illness
Patients in hospitals on census day who were admitted for specified illnesses
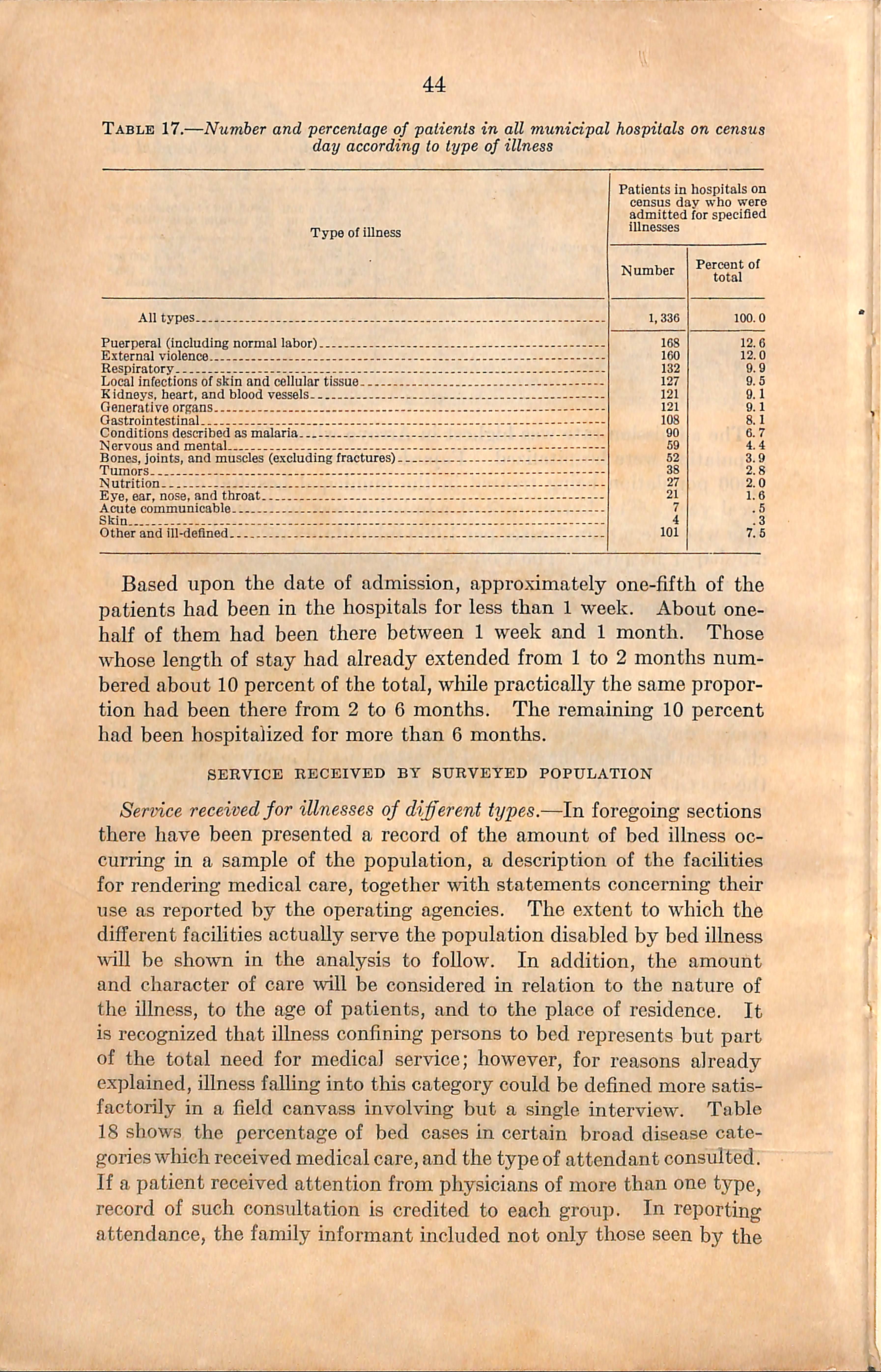
Type of illness
All types
Puerperal (including normal labor)
External violence
Respiratory
Local infections of skin and cellular tissue
K idneys, heart, and blood vessels
Generative organs
Gastrointestinal
Conditions described as malaria
Nervous and mental
Bones,joints, and muscles (excluding fractures)
Tumors
Nutrition--
Eye,ear, nose, and throat
Acute communicable
Skin - -
Other and ill-defined
Based upon the date of admission, approximately one-fifth of the patients had been in the hospitals for less than 1 week. About onehalf of them had been there between 1 week and 1 month. Those whose length of stay had already extended from 1 to 2 months num bered about 10 percent of the total, wliile practically the same propor tion had been there from 2 to 6 months. The remaining 10 percent had been hospitalized for more than 6 months.
SERVICE RECEIVED BY SURVEYED POPULATION
Service receivedfor illnesses of different types.—In foregoing sections there have been presented a record of the amount of bed illness oc curring in a sample of the population, a description of the facilities for rendering medical care, together with statements concerning their use as reported by the operating agencies. The extent to which the different facilities actually serve the population disabled by bed illness \viU be shown in the analysis to follow. In addition, the amount and character of care will he considered in relation to the nature of the illness, to the age of patients, and to the place of residence. It is recognized that illness confining persons to bed represents but part of the total need for medical service; however, for reasons already explained, illness falhng into this category could be defined more satis factorily in a field canvass involving but a single interview. Table 18 shows the percentage of bed cases in certain broad disease cate gories winch received medical care,and the type of attendant consulted. If a patient received attention from physicians of more than one type, record of such consultation is credited to each group. In reporting attendance, the family informant mcluded not only those seen by the
Figure IS.—-This numicipal hospital i.s no lonser used for the care of palienis.
19 —A municipal hospital building about 20 years old which was used only 1 year for the care of l)atients.
physician but also instances where a member of the family, or a neighbor, sought medical consultation on behalf of the patient. Hospital care will be treated separately later.
A physician attended 53 percent of the bed illness resulting from any cause. This record of care is considerably lower than that of the fivecovmty snrvey on the continent, where 66 percent of all such illnesses were brought to the attention of a physician.
In Puerto Rico the municipal physician cared for a higher per centage of bed illness than did any other type of medical attendant. This mil be seen in table IS. When considering illness in relation to medical care, it was found that between 75 and 80 percent of eye, ear, nose, and throat conditions, nutritional disorders, local infections of the slvin and cellular tissue, tumors, and accidents received some at tention from a physician. A physician was consulted for a smaller percentage of puerperal conditions than for illness of any other cause. This is explained by the custom in Puerto Rico of most deliveries being attended by licensed niidwives who are classed as nonmedical atten dants. Only 35 percent of the bed cases of acute communicable diseases, and 50 percent of the respiratory illnesses were attended by a physician.
Table 18. Percentage of illnesses of different types, as reported by surveyed families 'of Puerto Rico, which received some attention from a physician
Type of illness
All types- -
Hespiratory

In table 19 one finds that, except for puerperal conditions, the percentage of all bed illnesses receiving the care of a nonmedical attendant was much smaller than the percentage treated by a physi cian. As previously suggested, the licensed midwife was the non medical attendant who cared for this high percentage (68) of puerperal cases. The nonmedical attendant classed as "other" in table 19 is
largely represented by the unlicensed midwife who attended 16 percent of the maternity cases. A curandero ® was consulted,for about 9 per cent of the sldn diseases and parasites and for the same proportion of nervous and mental conditions. This type of attendant also was occasionally consulted for illnesses falling in the ill-defined group andfor intestinal infections and parasites. Not more than 6 percent of illness of any type was treated by a druggist. Nursing care only was reported for 5 to 10 percent of all accidents, local infections of skin and cellular tissue, and acute communicable diseases. Lower percentages were reported for illnesses of other types.
Table 19.—Percentage of illnesses of different iypes^ as reported by surveyed families of Puerto Ricoj which received some attention from a nonmedical attendant
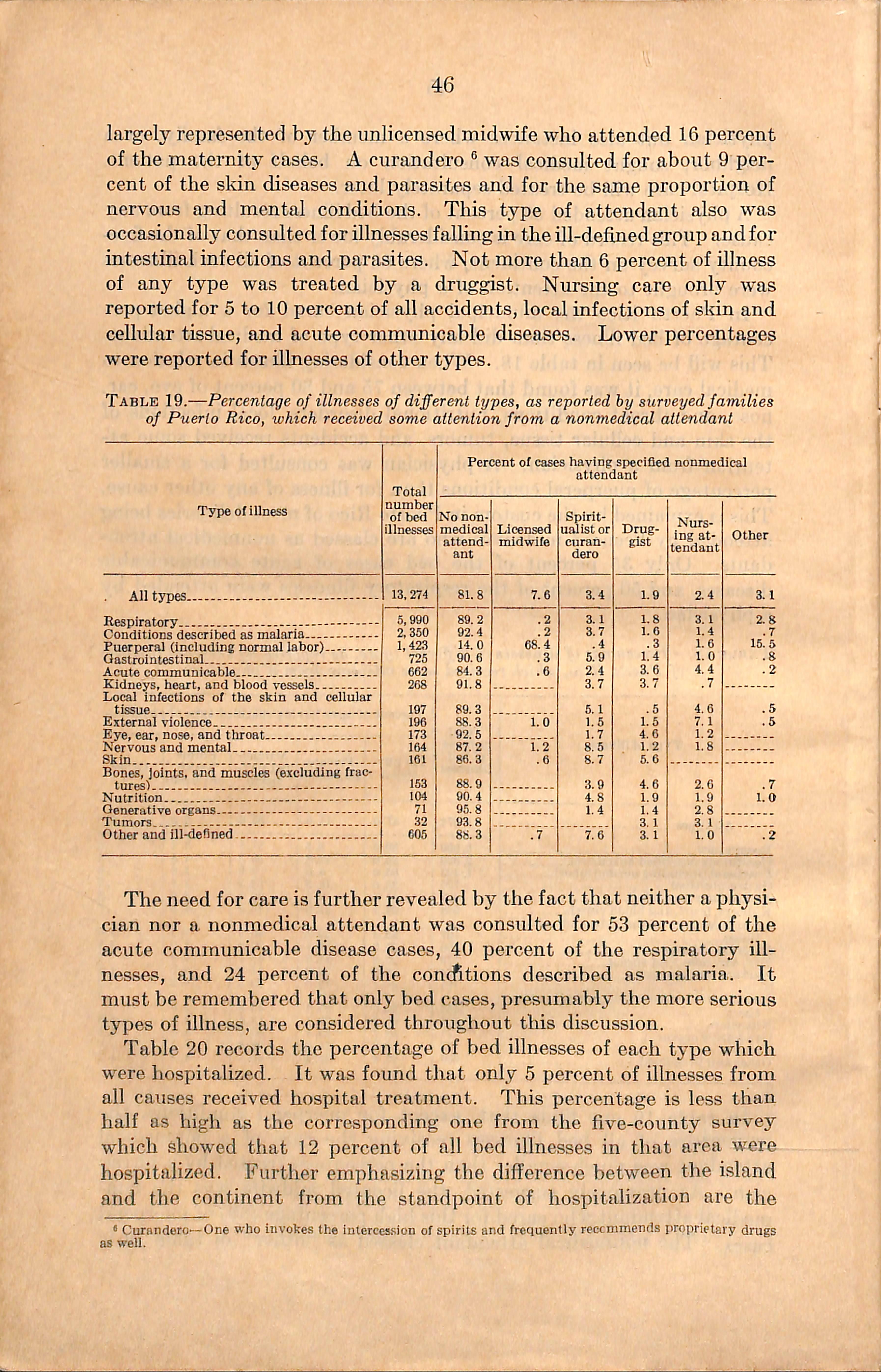
The need for care is further revealed by the fact that neither a physi cian nor a nonmedical attendant was consulted for 53 percent of the acute communicable disease cases, 40 percent of the respiratory ill nesses, and 24 percent of the concfttions described as malaria. It must be remembered that only bed cases, presumably the more serious types of illness, are considered throughout tliis discussion.
Table 20 records the percentage of bed illnesses of each type which were hospitalized. It was found that only 5 percent of illnesses from all causes received hospital treatment. This pei'centage is less than half as high as the corresponding one from the five-county survey which showed that 12 percent of all bed illnesses in that area were hospitalized. Further emphasizing the difference between the island and the continent from the standpoint of hospitalization are the
® CuTflndero—One who invokes the iiilercession of spirits and frequently rcccmmends proprietary drugs as well.
relative admission rates per 1,000 population in the two areas. In the 5 study counties there were 38 hospital admissions per 1,000 sample population during the study year. Data secured by the Committee on the Costs of Medical Care (11)in a survey of 38,688 white persons reveal the rate of hospitalized cases to be 59 per 1,000 persons. The corresponding rate found in the Puerto Rican illness survey is 20 per 1,000 population. The difference becomes more significant when it is recalled that the illness rate is much higher on the island than in the States and that the average home in Puerto Rico is less suited to the needs of bed patients than is true for the continental United States. In reahty, therefore, proportionately more hospital care is needed in Puerto Rico.
By referring to table 20, one finds that more than 20 percent of the Puerto Rican illnesses resulting from accidents; eye, ear, nose, and throat conditions; and disorders of the generative organs were treated in a hospital. Less than 5 percent of respiratory conditions, acute communicable diseases, conditions described as malaria, sldn diseases and parasites, and diseases of the bones, joints, and muscles entered a hospital. Thirty or more days were spent in the hospital by a larger percentage of patients suffering from accidents than for any other cause, while disorders of the generative organs ranked second among the group remaining for this period of time.
Table 20.—Percentage of illnesses of different types, as reported by surveyed families of Puerto Rico, whick received hospitalization
Bones,joints, and muscles (excluding fractures)
Tumors
Other and ill-defined
Service received by individuals andfamilies.—When all illnesses were arranged according to age of the patient, and percentage of illness in each age group receiving care from a medical or nonmedical attendant was computed, the findings revealed that age had no apparent effect upon the proportion of illness receiving care from a medical attendant.
On the other hand, young adults, those between the ages of 15 and 44, more frequently received care from a nonmedieal attendant than did any other specified age group. This is attributed to the number of puerperal conditions attended by a midwife occurring within this group.
Of all surveyed families having bed iUness, 24 percent reported no medical attendant; 23 percent, a private physician; 54 percent, a municipal physician; 6 percent, the health officer from the local health unit; and 2 percent, some other physician. In general, a higher percentage of families with bed iUness in the first- and secondclass municipalities reported medical care than did those in the third class, while fewer families from the mountainous municipalities of the interior reported medical care than did those from the remainder of the island.
The significant effect of location upon domiciliary medical care is further indicated by the fact that while 45 percent of all families with bed illness who live on a road reported a physician's visit to the home, attention in the home by a physician was reported by 15 percent of such famihes living on a path approximately 1 mile from the nearest road, and only 5 percent of those on paths that were more than 1 mile from a road. One may conclude, therefore, that physicians more frequently visited homes which were accessible to transportation than those which were removed from passable roads.
From the 13 municipalities surveyed to reveal the prevalence of illness,6 were chosen for a special study of expenditures on all items of medical care. The municipalities selected in this study were: Cayey, Dorado, Jayuya, Juana Diaz, Manati, and the urban section of Mayaguez. The field worker obtained from the family a report of the total amonnt of money expended for medicines and paid to medical and nonmedieal attendants, as well as tliat spent for bandages and other essentially "medicine chest" supplies.
When all families from which information was obtained were con sidered, the average annual expenditure for medical care was found to ■ be $10 per family. The average per capita expenditure for medical care was $2 per annum. These data present a marked contrast to those secured by the Committee on the Costs of Medical Care (11)in a survey of 8,758 representative white famihes of the continental United States. In this group of families the average annual expenditure for medical care was $108 per family. Even the lowest income group (below $1,200) reported an average expenditure of $50 per family per year, or five times the amount spent by the average Puerto Rican family. Average per capita figures obtained by the committee were $23 for all individuals included in the study and $9 for those in the
lowest income group (family income below $1,200). Thus, again, it is seen that expenditures for medical care are about five tunes as high for individuals of the lowest income strata on the continent as for the average Puerto Rican. However, the difference between the fee schedules of the two areas makes it impossible to translate directly these figures into absolute differences in the amount of medical care.
Tlie family income on the island, as well as on the continent, appears to exert a definite influence upon the money which was paid for medi cal care. No consistent difference was found between the municipal ities when expenditures for medical care were analyzed according to location of the families. Finally, it should be emphasized that a far greater proportion of the expenditures made in Puerto Rico were de voted to medical supplies than to actual care by an attendant.
The incidence of illness in Puerto Rico is considerably higher than that found in selected county populations of the continental United States studied by similar methods. Low incomes, crowded and in sanitary homes,inadequate diet, and the prevalence of certain endemic diseases are factors which contribute to the high rate of illness in Puerto Rico. The total death rate is appro.ximately twice as high on the island as on tlie continent.
Previous studies bj'^ other investigators cite malaria, hookworm, nutritional disorders,infant mortality, and tuberculosis as outstanding public health problems on the island. The observations made during the study herein reported tend to confirm the work of others, although direct comparisons are not jjossible since the survey data cover bed illness only. It became apparent, however, that a large part of the illness in Puerto Rico is susceptible to control by recognized preventive methods. Programs now in operation need to be amplified. How ever, it is recognized that these, diseases in Puerto Rico have pecidiar social and economic implications which render control measures extremely complex.
The family survey in Puerto Rico revealed tliat the median duration of bed illness in Puerto Rico was 11 days, while the median duration in a particular surveyed section of the United States was 7 daj's. It •was also brought out in this smwey that bed illness rates are higher in rural areas of the island than in urban, along the south and west coasts than in other geographic diUsions considered, among adults than among children, and in families with lower incomes than in those with higher.
When bed illnesses are classified according to broad categories,respir atory diseases and conditions described as malaria are the two most
7 In appendix E will be foundar§siin:§oflegislation relative to public medical care which enacted since the completion of this survey.
frequent causes. Puerperal conditions (including normal labor) rank third in order of frequency as a cause of bed illness in the surveyed population of the island. In a large measure the Ulness experience attributed to maternity may be explained by a birth rate which is more than twice that of the continental United States.
Four percent of the bed illnesses revealed by the survey in Puerto Rico, as compared with 2 percent of those in five counties of the United States studied by a similar method, resulted in death. The leading causes of death in Puerto Rico are intestinal infections, respiratory conditions(including tuberculosis), malaria,and nutritional disorders of young children.
Each of the 76 municipalities, except Maricao, has made some pro vision for public medical care. The facilities and service, however, vary greatly among the mimicipalities principally on account of the differences in public revenue. In general, a larger percentage of the population is served through beneficencia in first-class municipalities than is the case for either of the other classes, while the second-class municipahties provdde a larger measure of service than the third. This is only what may be expected in view of the fact that wealth is one of the factors which was taken into accormt when establishing the basis for classifying municipalities.
When aU physicians on the island as a whole are considered, the ratio of persons per physician is approximately 4,000. MTien computed on the basis of first-, second-, and third-class municipalities having resident physicians, the approximate ratios are respectively 2,000, 4,000, and 9,000 persons per physician. If the 131 municipal physicians only are considered and related to the total population, the corresponding ratios become approximately 8,350, 12,000, and 15,400 individuals per physician. Five mrmicipahties, representing a combined population of 55,000, have no resident physician. In 23 municipalities the municipal physician is the only resident medical practitioner.
Fifty-five percent of the available general hospital beds, or 1,901, are located in municipal hospitals. Every fu'st-class municipality and all but one in the second class operate a hospital. San German, the exception, has a contract under which 25 beds in a private hospital are reserved for the exclusive use of patients referred by the municipal authorities. Thirty-four of the 48 third-class mimicipalities have municipal hospitals but only 27 are now in use for care of patients. Practically all municipal hospitals are in need of repair, and only half of them possess equiimient which might be used for major sm-gery. X-ray facilities, laboratory equipment, and an ambulance are found in relatively few municipal hospitals. Equipment in most clinics is not sufficient for ordinary diagnostic and treatment purposes.
The first-class and a few of the wealthier second-class municipahties might develop their present hospitals if funds for this purpose could be secured through local taxation. As a general principle, however, the budding of additional pubhc hospital facihties in second and third class municipalities should be discouraged. Eventually most of the smaller hospitals should be abandoned as hospitals, but the buddings could stdl be used as quarters for the municipal physician, the dentist, and the pharmacy, and for the public health unit. A few beds and minimum equipment for first-aid work of a minor character would fdl a definite need. . .
The insular government already has the major responsibdity for the institutional care of the insane, the tuberculous, and the leprous, and it operates the only hospital on the island for the care of persons ■with acute communicable disease.
The hospital for the insane is fdled to capacity. About 150 vio lently insane are detained in municipal hospitals and jads. At least an equal number of persons with mental disorders which warrant institutional care are said to be in homes of relatives or in asylums other than mental. The capacity of the insular hospital for the insane should be increased by approximately 500 beds so as to relieve the municipahties and relatives of caring for the insane.
TuberciJosis hospitals under construction at the time of the survey should bring facdities up to the point of being reasonably adequate. It is believed by the local health authorities that through the use of chest surgery, supplemented by field diagnostic and treat ment service, each hospital bed can accommodate on the average about 3 patients per year, thus affording some measure of hospital care to about 4,500 patients. The projected field and institutional program, which is designed to reheve the municipalities entirely of responsibdity for care of the tubercidous, should be given a fair trial before any alteration or enlargement is considered.
It is beheved that practically all Imo^vn lepers (except those on parole) are segregated in the leper hospital. No enlargement of these buildings is being contemplated, but extensive repairs are needed.
Several years ago a system of insular district hospitals was con ceived, but up to the present time only two small units have been constructed: One at San Juan has a capacity of 50 beds and the other at Ponce can accommodate about 80 patients. The San Juan District Hospital serves in part as a research hospital for the School of Tropical Medicine. Its greatest field of usefulness perhaps lies in tliis direc tion. Another hospital of not less than 250 beds for rendering clinical service to a part of the island should be built in close proximity to tbe School of Tropical Medicine. Such a unit would be in a position to draw on the professional resources of San Juan and offer post-
graduate instruction to physicians of the island, thus filling a most fundamental need.
The Ponce District Hospital, while in excellent condition, is too small for efficient operation. Its capacity should be increased to at least 250 beds, and a diagnostic service similar to that now operating in the district hospital of San Juan should be established for the beneficcncia physicians of neighboring municipalities. After the San Juan and the Ponce district hospitals have been developed, consideration might be given to the construction of a third and later on perhaps a fourth district hospital in other centers of population.
On the census day a total of 1,336 patients occupied beds in munici pal hospitals, thus showing that 70 percent of the rated bed capac ity was in use. As a rule, hospitals of the first- and larger secondclass municipalities were being utilized to a high percentage of the rated capacity, while in the smaller and poorer municipalities the percentage of utilization was extremely low. During the fiscal year 1934, 38 persons per 1,000 population received public hospital care in the first-class municipalities; in those of the second class the rate was 24; and in the third class 10 persons per 1,000 inhabitants were accommodated through municipal facilities.
Of those bed illnesses, excluding puerperal conditions, reported in the family canvass 47 percent had no attendant, 39 percent received the attention of municipal physicians, and 11 percent of private physicians. In addition, a small amount of medical attention was given by physicians not falling in these categories. Births, with few exceptions, were attended by midwives. According to local opinion, at least 80 percent of the total population is unable to pur chase private medical service. This estimate perhaps does not exaggerate the situation since it will be remembered that about 60 per cent of the families studied in the second and third classes of munici palities were receiving material relief in some form at the time of the canvass.
Professional and lay persons encountered on the island are in sub stantial agreement that public medical service furnished by the municipalities has not kept pace with the standards which obtain in private practice. Data gathered and observations made during the survey indicate that there is a foundation for the growing dissatis faction with the public service. The excessive patient load on muni cipal physicians has enforced a pernicious practice of prescribing remedies without physical examination or the xise of other diagnostic procedures. Frequentreplacementofphysicians has, to a great extent, destroyed confidence of patient in physician and interest ofphj^sician in patient. The remedy, however, is perhaps not so simple as it may appear to many who see only certain aspects of the problem.
While funds assigned to medical care are manifestly inadequate for providing satisfactory ser^^ce to those in need, it is recognized that the municipalities allot a reasonable share of their total revenue to this purpose. However, not all of the budgeted funds actually become available, since most of the municipalities are delinquent in the payment of their obhgations for salaries and operation costs. Insufficient budget, frequent turnover in personnel, and lack of pro fessional supervision are the more important factors which have brought about a quality of service wliich is not at all in keeping with medical standards of the present time. Hospitals, particularly, have deteriorated to the extent that only a few are in a position to give more than a custodial type of care.
It must he understood that a complete medical service will cost several times what is now being spent. But if it is conceded that stationary or only slightly increasing budgets are to be expected, then there is no other recourse except to do what may be possible toward decreasing the burden of illness by applying preventive measures, and by providing the type of medical organization, freed of present local restrictions, which will function at the highest possible level of efficiency. A very marked reduction in the present sickness burden could be efi'ected by bringing under control such preventable conditions as malaria, hoolvworm, dysentery, and tuberculosis and by improving tlie nutritional status of the population. Greater efficiency should result from a scheme of organization, professional in character, which would be permitted to develop at least certain elements of the service on a district basis. Above all, some method must be devised for selecting physicians on the basis of merit and for retaining them so long as their worit is satisfactory. The physician must be given greater latitude in planning the program and in select ing for attention those patients who are most m need of his services.
Grave doubt exists in the minds of many civic and professional leaders as to whether the municipality should be retained as the basis of organization in any scheme for medical care. While there is very little in the present plan of service that would recommend administra tion of medical care by the municipality, yet, the people probably will choose to exercise some local control over services of this character through their municipal government. As a general principle, however, only that part of the service should be administered by the munic ipality which is paid for through municipal taxation. But in any event the quality of service could be improved if the insular govern ment were to determine standards of care and participate financially in support of the program.
There does not seem to be any necessity of establishing a new governmental agency for the administration of public medical care even though some plan different from the present is agreed upon.
it is decided that a more highly centrahzed system offers the greatest promise of improvement in the service, change may he accomplished through the agency of the insular health department. It clearly appears to have heen the intent of the organic act to place the commissioner of health in charge of all insular activities pertaining to health and charities. Health in Puerto Rico very properly should be interpreted to include medical care. The insular health department has demonstrated its capacity for successful administration, including the ahdity to cooperate mth local units of government. Both insular and municipal governments have ample authority for participating in any reasonable scheme of medical service, and the existing structure is sufficiently flexible to accommodate itself to such changes in program as may be indicated in the light of further experience.
(1) Leven, Maurice; Moulton, Harold G.; and Warburton, Clark, America's Capacity to Consume, The Brookings Institution, Washington, D. C., 1934.
(2) Puerto Rico and Its Problems, The Brookings Institution, Washington, D. C., 1930.
(3) Eliot, Martha M., The Effect of Tropical Sunlight on the Development of Bones of Children in Puerto Rico, U. S. Children's Bureau, Publication 217, Pages 76-97. Government Printing Office, Washington, D. C., 1933.
(4) Crumbine, S. J.; Mitchell, H. H.; and Tapping, A. P., Puerto Rico, An Inquiry as to the Health of Children, American Child Health Association, New York, 1930.
(5) Grant, John B., Report on Hookworm Infection Survey and Malaria Survey of Puerto Rico, December 1919 to January 1930 (Unpublished Report of Rockefeller Foundation).
(6) Earl, Walter C., Malaria in Puerto Rico, American Journal of Tropical Medicine, May 1930.
(7) Hill, Rolla B., The Amount and Distribution of Hookworm Infestation in Puerto Rico, Health Review, Vol. II, No. 3, September 1926.
(8) Eernos, Isern A. and Pastor, R. J., A Survey of Infant Mortality in Puerto Rico, The Puerto Rico Journal of Public Health and Tropical Medicine, Vol. VI, No. 2, December 1930.
(9) Townsend, J. G., Tuberculosis Survey of the Island of Puerto Rico. Public Health Bulletin No. 138, December 1923, Government Printing Office, Washington, D. C.
(10) Pastor, J. Rodriguez, Tuberculosis Infection in Puerto Rico School Children, Puerto Rico, An Inquiry as to the Health of the Children, American Child Health Association, New York City, 1930.
(11) Falk, I. S.; Klem, Margaret C.; Sinai, Nathan, The Incidence of lUness and the Receipt and Costs of Medical Care Among Representative Families, Pubhcations of the Committee on the Costs of Medical Care; No. 26. The University of Cliicago Press, Chicago, Illinois.
APPENDIX A.—AREA AND POPULATION IN FIRST-, SECOND-, AND THIRD-CLASS MUNICIPALITIES OP PUERTO RICO
Municipality
All classes.. First class.. Arecibo Caguas Mayaguez. ponce San Juan...
Second class.. Aguadilla Barceloneta.. Bayarnon Carolina Cayey FajardoOuanica—.. Guayama Huinacao Juana Diaz.. juncos Loiza Manati Naguabo Rio Piedras— Salinas. San German. Santa Isabel.. Utuado Vega Baja Vieques Ynbucoa Yauco... Third
Adjuntas Aguada-Aguas Buenas.. Aibonito-Anasco Arroyo-------Barranqnitas... Cabo Rojo Camuy.Catano Ceiba dales Cldra CoamoComerio corozal Culebra porado. Guayanilla Ouaynabo Gurabo Hatillo Hormlgueros... Isabeln...
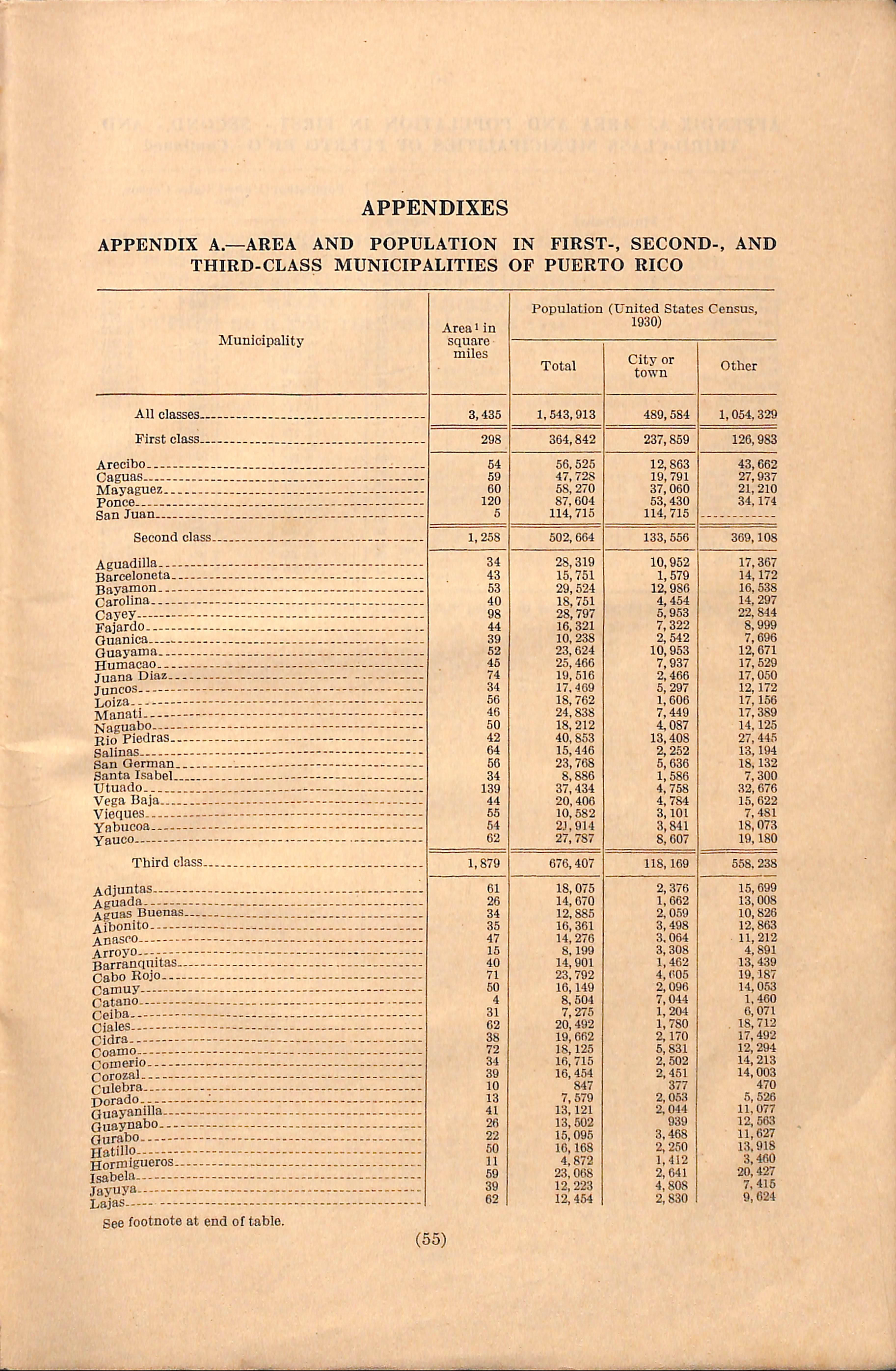
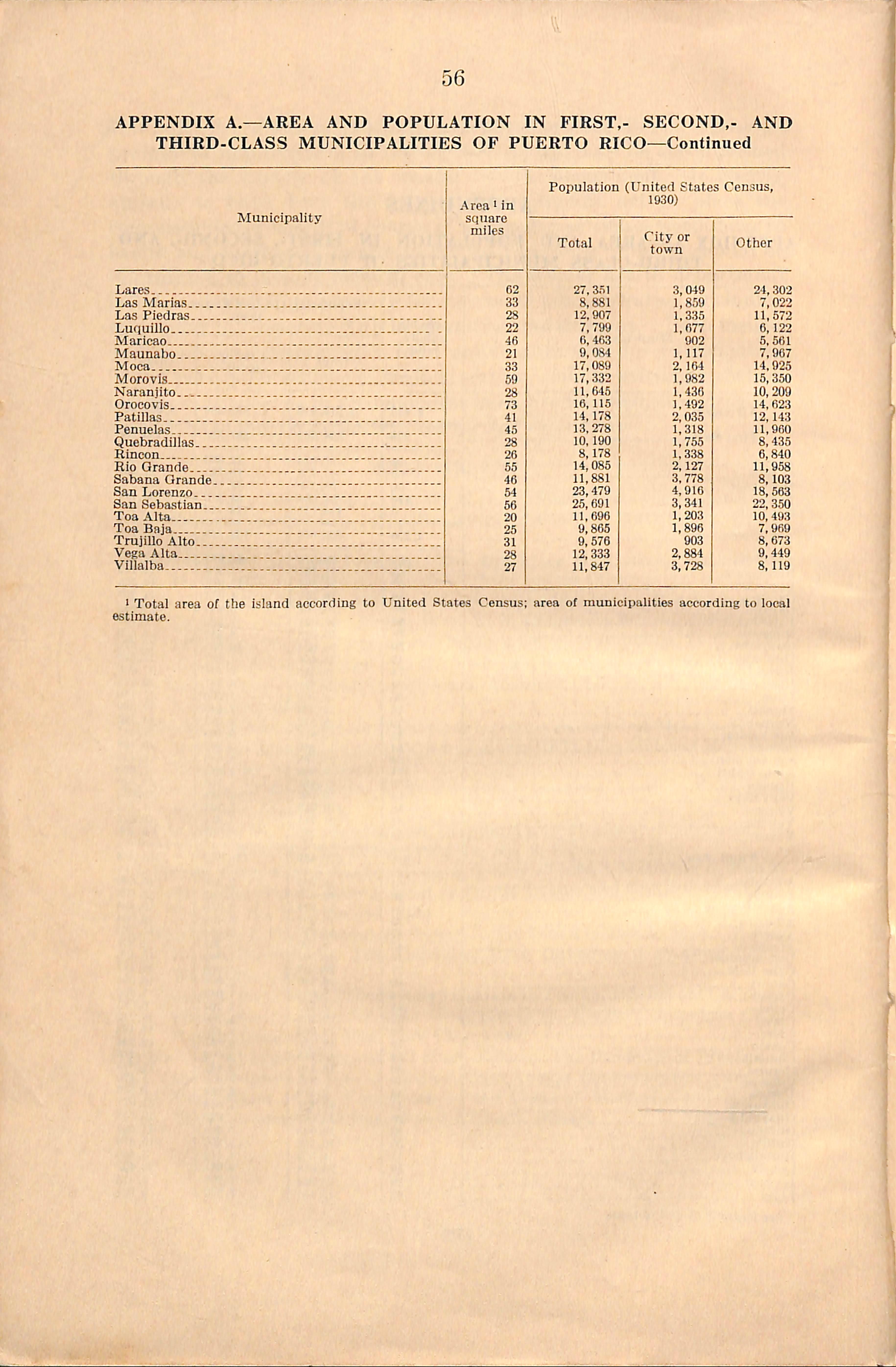
7,022 11,572 6,122 5,561 7,967 14,925 15,350 10, 209 14,623 12,143 11,960 8.435 6,840 11,958 8.103 18,563 22, 350 10,493 7,969 8,673 9,449 8.119
1 Total area of the island according to United States Census; area of municipalities according to local estimate.
APPENDIX B.—DISTRIBUTION OF TOTAL AND PER CAPITA EXPENDI TURES FOR ALL PURPOSES AND FOR BENEFICENCIA, AND PER CENTAGE OF TOTAL EXPENDITURES DEVOTED TO BENEFICENCIA IN FIRST-, SECOND-, AND THIRD-CLASS MUNICIPALITIES OF PUERTO RICO FOR THE FISCAL YEAR 1934
Expenditures for all purposes
Municipality
All classes-
First class., Arecibo Caguas Mayaguez.. Ponce San Juan...
Second class.
Aguadilla... Barceioneta.. Bayamon Carolina Cayey
Fajardo Guanica Guayama Huinacao
Juana Diaz... Juncos Loizft
Manati Naguabo Rio Piedras.. Salinas San German. Santa Isabel.. Utuado Vega Baja— Vieques Yabucoa Yauco
Third class.
Adjuntas Aguada Aguas Buenas. Aibonito Anasco
Arroyo Barranquitas... Cabo Rojo
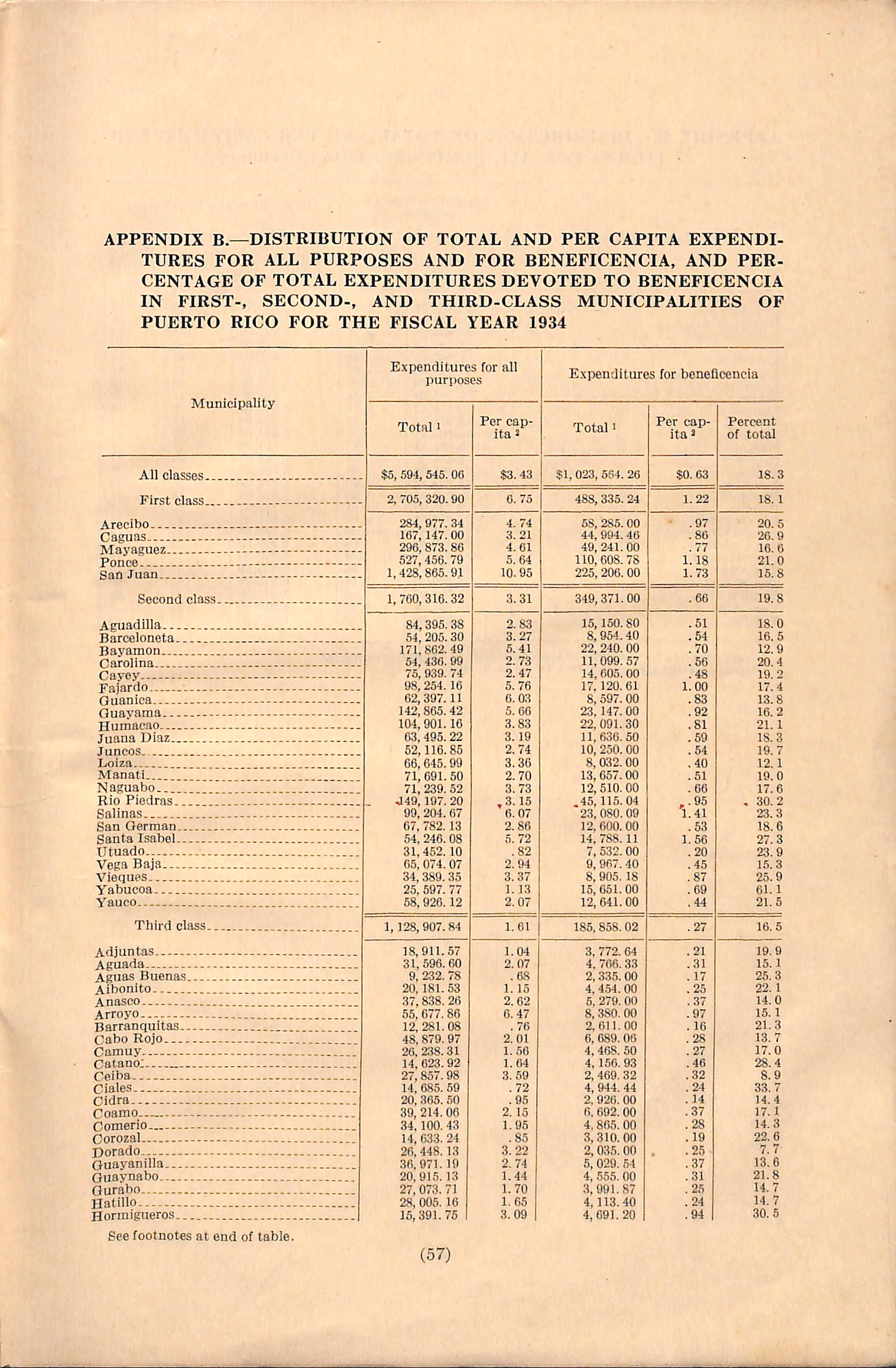
Total 1
$5,594,545.06
2, 705, 320.90 284,977. 34 167,147.00 296,873.86 527,456. 79 1,428,865.91
1, 760,316.32 84, 54, 171, 54. 75, 98, 02, 142, 104, 63, 52,
Expenditures for beneficencia
Total 1 $1,023,564.26 488,335.24 58, 285.00 44,994.40 49,241.00 110,608.78 225,
20
452.10 074.07 389.35 597. 77 926.12 1,128,907.84 18, 31, 9, 20. 37, 55, 12, 48. 26, 14, 27, 14, 20, 39, 34. 14. 20. 36. 20, 27, 28, 15, 911.57 596.60 232. 78
Camuy Catano: Ceiba Ciales Cidra Coamo Comerio. Corozal Dorado Guaynnilla Guaynabo Gurabo Hatillo Horrnigueros... 71, 71, J49, 99, 67, 54. 31. 05, 34, 25, 58, 395. 38 205.30 862.49 436.99 939. 74 254.10 397.11 865.42 901.16 495.22 116.85 045.99 691.50
1.70 1.65 3.09 15,150.80 8,954.40 22, 240.00 11,099. 57 14,605.00 17,120.61 8,597.00 23. 147.00 22.091.30 11,636. 50 10, 250.00 8,032. GO 13,657.00 12,510.00 .45,115.04 23. 080.09 12,600.00 14. 788.11 7,532.00 9,967.40 8,905.18 15,051.00 12,641.00 185,858.02 3. 772.64 4. 766. 33 2,335.00 4,454.00 5. 279.00 8,380.00 2,011.00 6. 689.06 4,468. 50 4, 156.93 2, 469.32 4, 944. 44 2. 926.00 fi 692. GO 4.865.00 3,310.00 2.035.00 5,029. 54 4,555.00 3. 991.87 4,113.40 4. 691.20
Municipality
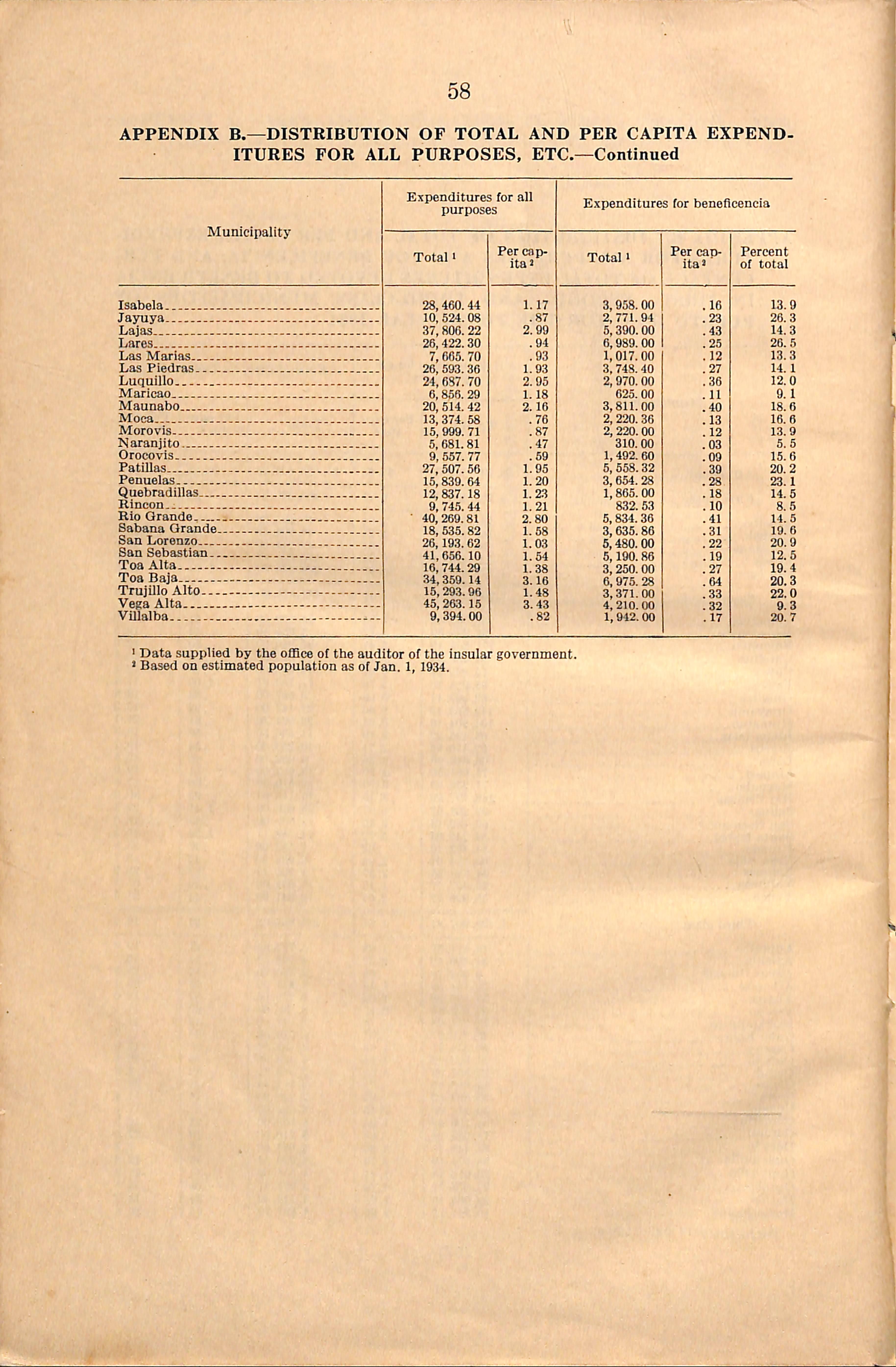
'Data supplied by the olBce of the auditor of the insular government. * Based on estimated population as of Jan. 1, 1934.
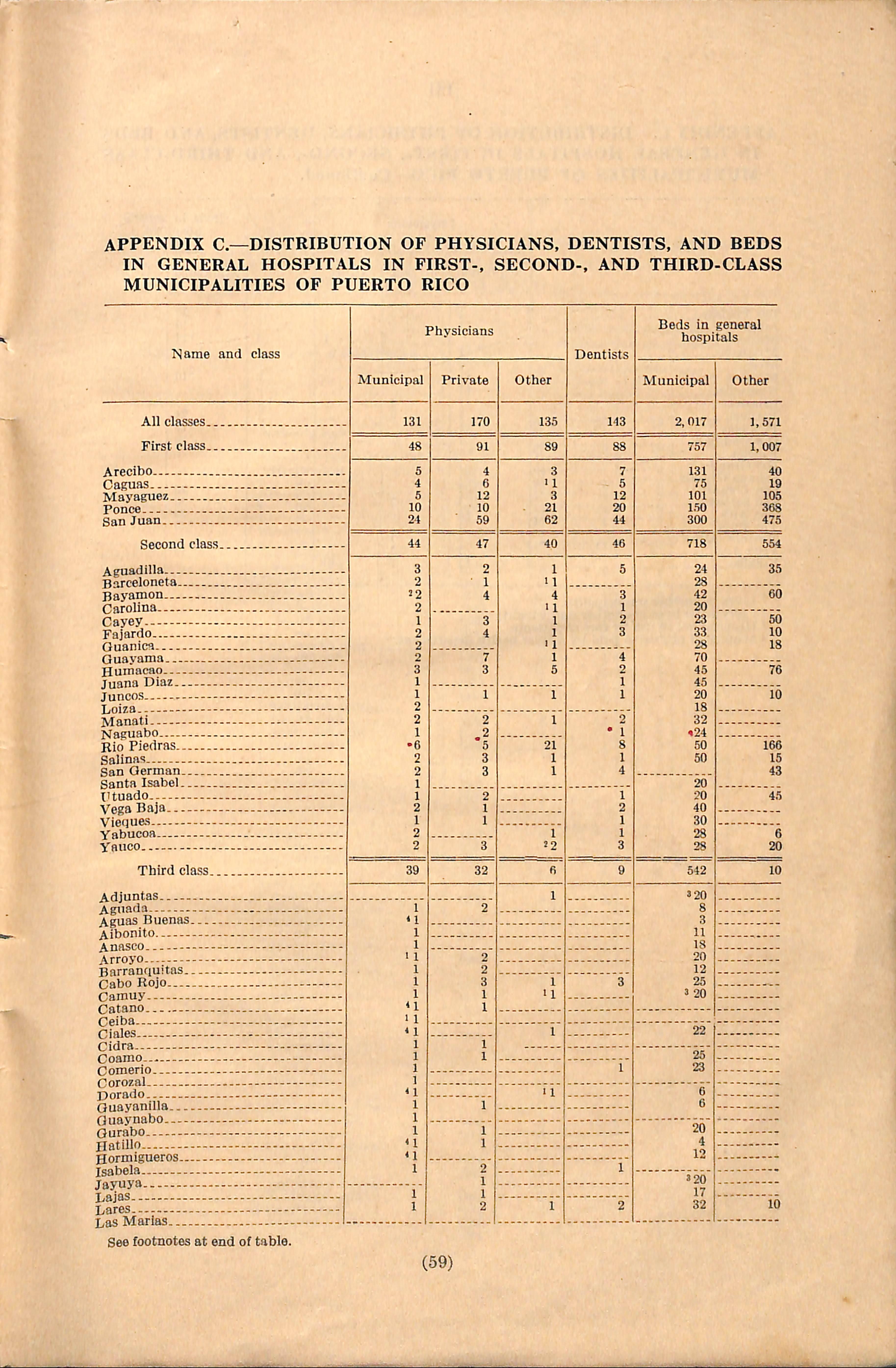
appendix c.—distribution of physicians, dentists, and beds IN GENERAL HOSPITALS IN FIRST-, SECOND-, AND THIRD-CLASS MUNICIPALITIES OF PUERTO RICO
APPENDIX C.—DISTRIBUTION OF PHYSICIANS, DENTISTS, AND BEDS IN GENERAL HOSPITALS IN FIRST-, SECOND-, AND THIRD-CLASS MUNICIPALITIES OF PUERTO RICO—Continued.
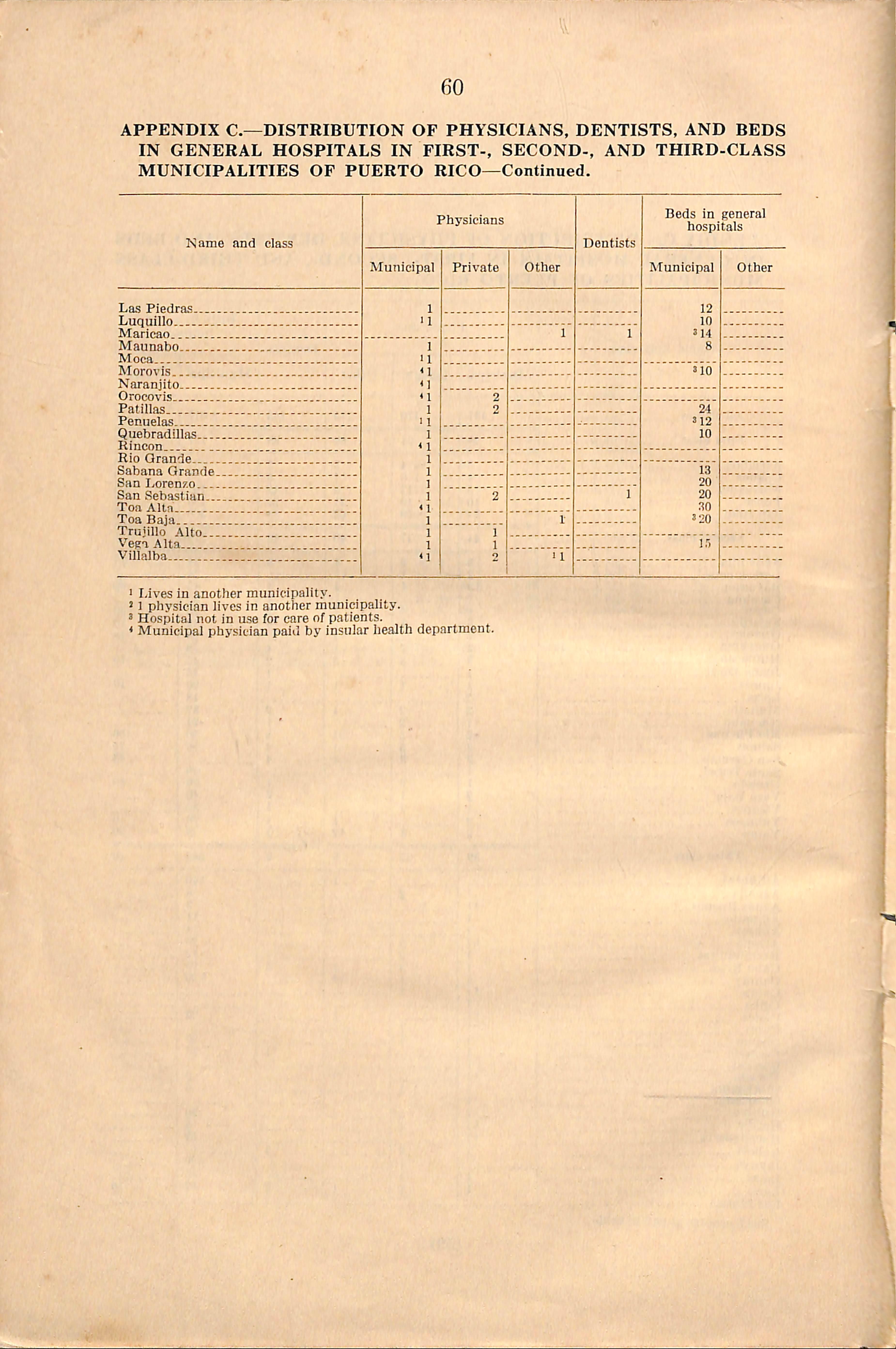
■ I/i%'es in another municipality.
' 1 physician lives in another municipality.
3 Hospital not in u.se for care of patients.
* Municipal physician paiil by insular health department.
APPENDIX D.—DISTRIBUTION OF LOCAL OFFICIAL HEALTH AGENCIES, AND FULL-TIME PERSONNEL IN FIRST-,SECOND-, AND THIRDCLASS MUNICIPALITIES OF PUERTO RICO
Municipality
All classes..
First class.. Arecibo— Capuas Mayapuez.. Ponce San Juan...
Second class..
Aguadilla Barceloneta.. Bayamon Carolina Csyey. Fajardo
Guanica Guayama Humacao
Juana Diaz... Juncos Loiza Manati Naguabo Rio Piedras.. Salinas San German. Santa Isabel.. Utuado. Vega Baja— Vieques Yabucoa Yauco -
Third class..
Adjuntas Aguada Aguas BuenasAibonito Anasco.. Arroyo Barranquitas... Cabo Rojo
Camuy Catano. Ceiba
Ciales
Cidra Coamo...--
Comerio
Corozal Dorado
Guayanilla Ouyanabo Gurabo
Hatillo Hormigueros... Isabela Jayuya
Lajas
Pares. Las Marias Las Piedras—
Health

Sanitation service. Health unit
Subhealth unit Health unit do do
Subhealth unit do
Sanitation service. do Health unit do.
Health unit
Sanitation service. Subhealth unit do
Sanitation service. Subhealth unit
Sanitation service. Health unit
Subhealth unit do
Sanitation service. Health unit
Sanitation service. do.. do
Subhealth unit do
Sanitation service
Subhealth unit do
Sanitation service.. Subhealth unit do
Sanitation service.. Subhealth unit
APPENDIX D.—DISTRIBUTION OF LOCAL OFFICIAL HEALTH AGENCIES,AND FULL-TIME PERSONNEL IN FIRST-,SECOND-,AND THIRDCLASS MUNICIPALITIES OF PUERTO RICO—Continued.
Municipality
Luquillo Maricao Maunabo Moca Morovis Naranjito Orocovis Patillas PenuelasQuobradillas Itincon Rio Grande Sabana Grande
San Lorenzo San Sebastian
Tea Alta
Toa Baja
Trujillo Alto Vega Alta Villalba
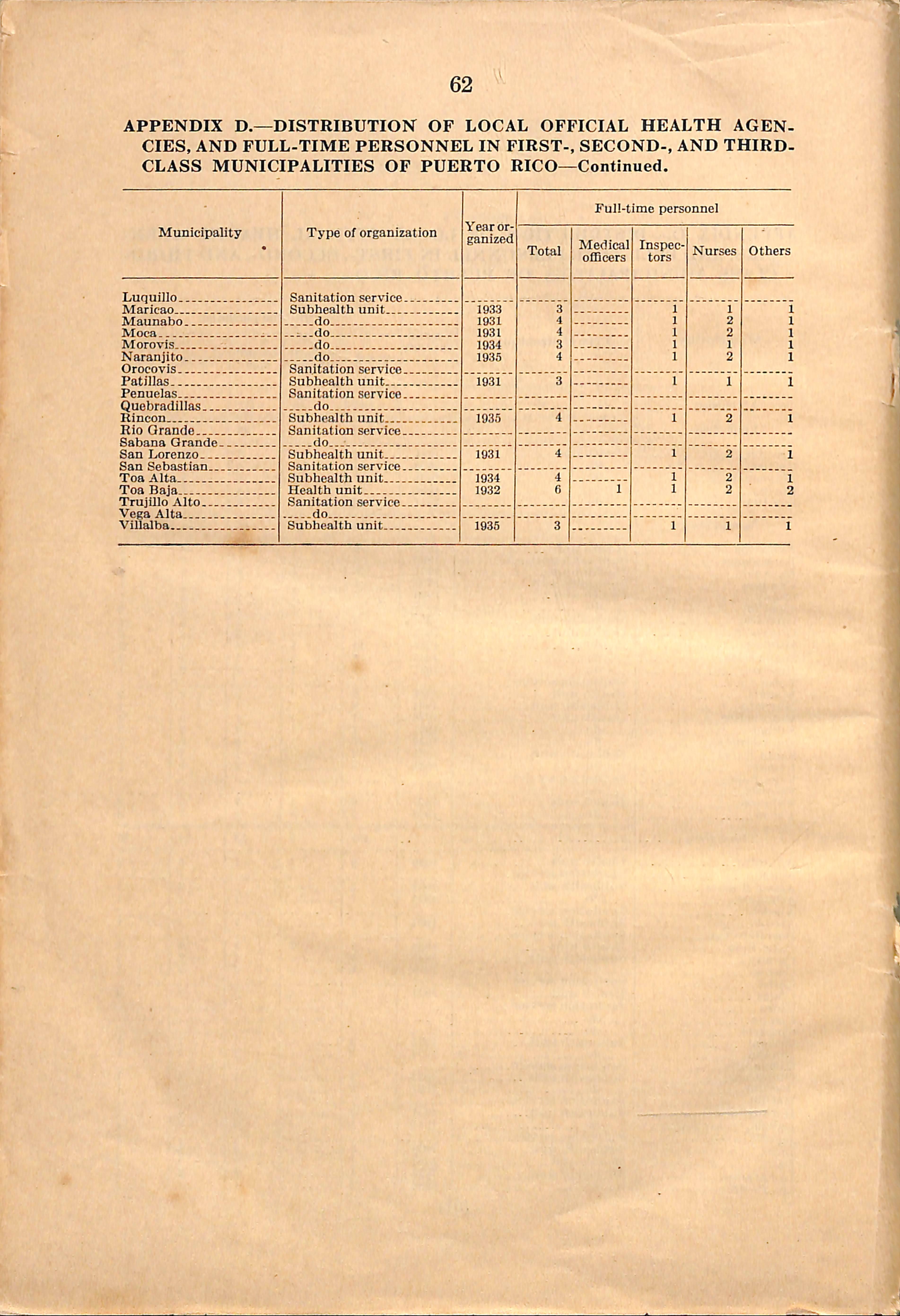
Sanitation service.
Subhealth unit do ..i..do do .do..
Sanitation service.
Subhealth unit
Sanitation service. do
Subhealth unit
Sanitation service.
Subheaitii unit
Sanitation service..
Subhealth unit
Health unit
Sanitation service.. do
Subhealth unit
The Public Hospital Charities Act (Act 29) passed by the Legislature of Puerto Rico, July 1935, provides as follows;
1. Creation of a Territorial Charities Board.
2. Division of the island into four zones to be known as charities districts.
3. Authority for borrowing $500,000 to be used for the construction of four district charity hospitals.
4. Creation of the "Charity Hospital Trust Fund" which provides for their operation and maintenance.
5. Authorization for construction of the 4 district hospital units, each of which shall consist of 300 beds and shall include the services of medicine, surgery, obstet rics, and pediatrics, and a dispensary service as well as an ambulance service. (63)
COLECCION PUERTORRlQUEf^A.
NO SE PRESTA FUERA DE LA SALAL
614.0972 M928i C.I Illness and medical care In Pu crM
0 20 110154647 5
UPR - Rio Piedras - SIstema Bibliotecas
614.0972 M928I C.I Illness and medical care In Pu cr'-