Humanizing Hospice
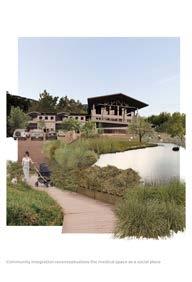
Reclaiming Medicalized Space for Community Well-Being
In dedication to my faithful community of support in family and friends—thank you for teaching me how to enjoy doing my best work for God every day.
With special appreciation to my dear grandmother for her time cultivating my love of caring for others.
This thesis is submitted in partial fulfillment of the requirements for the Bachelor of Architecture Degree in the Auburn University College of Architecture, Design, and Construction.
Professor David Shanks, Spring 2026
Architectural Thesis
1.0
Thesis Research
Hospice as Typology
Paradigms of Public Health
Care in Crisis
Reclaiming Hospice
3.0 2.0
Design Proposal
Site Selection
Humanizing Hospice
Synthesis
Notes
Bibliography
Images Cited
1.1
1.2
1.3
1.4
Thesis Research
Examination of existing literature and architectural precedents
Reclaiming Hospice Hospice as Typology
Paradigms of Public Health Care in Crisis
1 2 Worpole, 51. Adams, 252.
Hospice as Typology
An overview of hospice care terminology
Palliative care encompasses the physical, emotional, psychological, and spiritual support of terminally ill patients at the end of their lives. The goal insists on maintaining patient quality of life to provide meaningful life closure with their community. This community often witnesses their loved one transitioning from independent residency to assisted living, nursing homes, and finally the hospice facility for an estimated last ten days of life.1 The design of the hospice building must therefore cultivate an environment attuned to these final moments. Hospice creates
“a place where ordinary people face up to extraordinary challenges, and with the help of skilled and dedicated health professionals, triumph in the face of progressive physical deterioration and sequential losses. People live until they die and it is the job of the hospice to support and enable each patient to live their life as fully as possible.”2
Reimagining a hospice facility to address embedded flaws in community support necessitates an examination of the existing model to provide practical solutions for care and closure through design.
Typical progression for elderly patients
Typical progression for children and young adults
1 2 3 4 Verderber, 10. Wang et al, 2. Goldin, 387. NIV.
Paradigms in Public Health
Evolution from social construct to public policy
Hospice care extends from a tradition more than two thousand years old as a social construct to care for the broad community; the hospice facility exists only within the last fifty-eight years. Examining this new architectural typology through its historical development explores a shift in the view of public health.
Pilgrimage
The word hospice originates from the Latin hospitum, meaning “guesthouse.” 1 It shares linguistic roots with hospes, the source of modern terms such as hospital, hospitality, hostel, and hotel.2 These connections emphasize the connotation of a welcoming and comforting space, a safe shelter for those in need. Historically, the term referred to homes that hosted weary travelers on pilgrimage routes, offering rest to those whose provisions waned or whose feet hurt. Medical architecture historian Grace Goldin traces the foundation of this social structure to the religious ethos of the time, identifying the Christian text Matthew 25:35-26 as “the key text for the construction of merciful shelters for the poor.”3 This passage reads:
“For I was hungry and you gave me something to eat, I was thirsty and you gave me something to drink, I was a stranger and you invited me in, I needed clothes and you clothed me, I was sick and you looked after me....”4
In a time of limited public health infrastructure, this guiding principle set the foundation for modern hospice care. The use of this charitable term integrated into the modern vernacular as a metaphor for doors opening to travelers on a journey from one life to the next. It symbolized the spiritual connection to the human body in medieval times, and it continues to evoke a holistic understanding of care.
5 6 7 Verderber, 13. Ibid, 12. Schwarz, 349.
Almshouses
As rural pilgrimage traditions faded and urban populations grew in the eighteenth century, almshouses emerged as a solution to hospitals and asylums overcrowded with the infirm and elderly.5 This new typology rescued the destitute elderly by providing communal care. Residents, referred to as “pensioners,” lacked family and monetary support, relying on the almshouse for refuge.6 These institutions were typically adapted houses or similarly styled buildings arranged around courtyards. Supervisions within these facilities required linear wings with long corridors and open rooms. Although conditions for the physical building varied widely, the intentional space for the elderly portrays the first attempt of acknowledging the aging population. This model for community housing continued until after World War II when the rise of the architectural International Style and medical standardization laws shaped these institutions into the modern nursing home.7
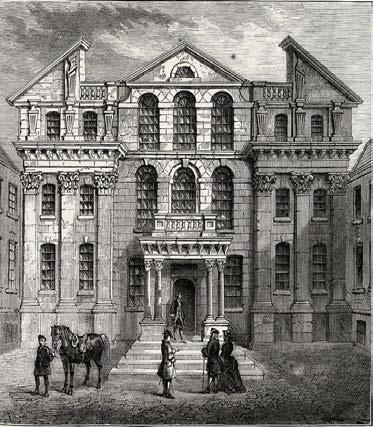
Figure 1—Pilgrimage as the first example of hospice care
Figure 2—Drawing of an eighteenth-century almshouse
Verderber, 13. Goldin, 403. Verderber, 13. Goldin, 402.
St. Luke’s Home
In response to the poor conditions of the almshouse, St. Luke’s Home for the Dying and Poor provided specific care for the terminally ill in London. Founded by Dr. Howard Barrett in 1893, the philosophy of care differed greatly from the custodial approach of the typical almshouse.8 Barrett sought to emphasize the individuality of his patients, writing that “each one is a human microcosm, with their own characteristics, their own aggregate of joys and sorrow, hopes and fears, their own life history.”9 This core value introduced one of the first documented ward layouts intentionally arranged for patient-centered care. As nurses admitted new patients, an “undetected rotation” moved the sickest patients closest to the nursing station and entrance, reducing distress at time of death.10 The home occupied several different locations across London from 1893 through 1903 as Barrett sought to find a building matching these ward ideals, retrofitting a variety of housing types. He es-
tablished a series of public ward layouts for men and semi-private rooms for women. With these distinctions, he sought to specialize care and provide a comfortable place for all hurting. He explained this shift in layout by stating:
“We aim at giving to all those who are brought to us a Home of peace, comfort, and even pleasure… Thus we do not need to put in force the rigid discipline of a hospital nor expend ourselves in striving after asepticism with the beneficent but bare and barrack-like results.” 11
While the architectural significance of the building remained uncodified due to these relocations between adapted buildings, his intentional approach to care marked St. Luke’s Home as the first “protohospice” by establishing the values later embedded in design.
Claire Hardin
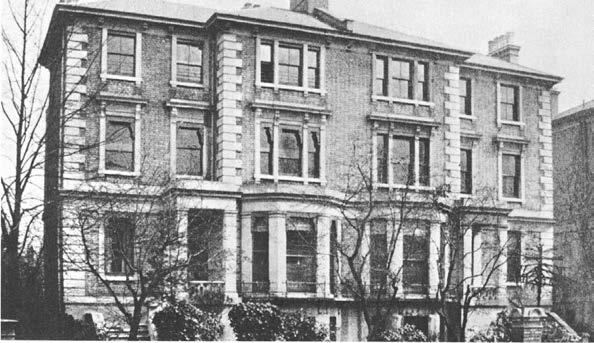
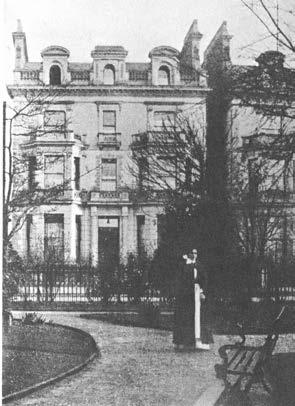
Figure 3–6—Timeline of St. Luke’s Home locations
Osnaburgh Street, 1894
Lawn Road, 1901
Pembroke Square, 1903
12 13 Worpole, 28. Ibid, 11.
Building
Location
Architect
Firm
Client
Size
Completed
St. Christopher’s Hospice
Sydenham, London
Justin Smith
Steward, Hendry and Smith
Cicely Saunders
5 stories
1967
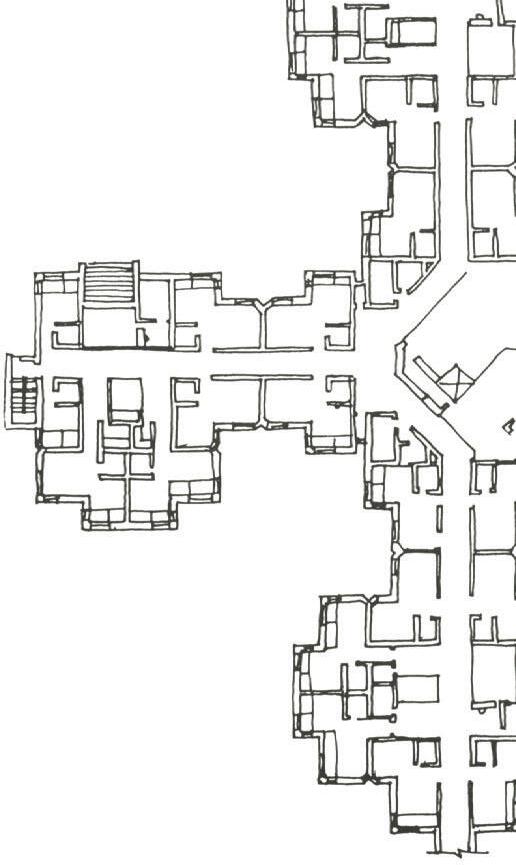
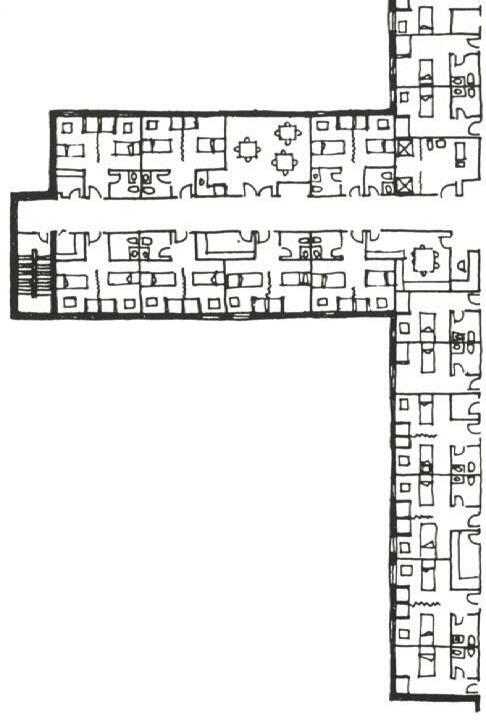
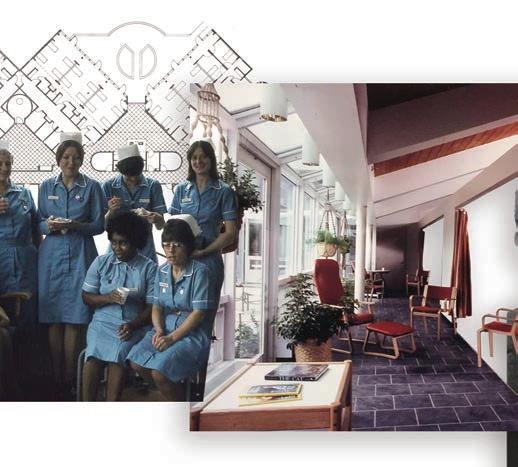
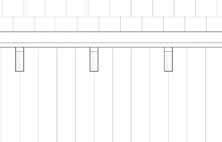
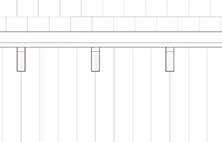
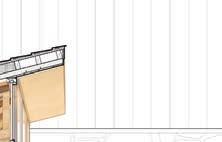
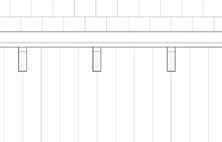
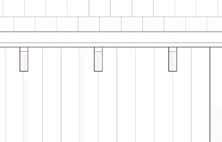
The design of St. Christopher’s Hospice prioritizes patient orientation within the space.12 Patient rooms line the western façade, with offset windows capturing the extreme light. This feature provides a natural sense of passing time and mitigates symptoms of confusion at night. The layout further encourages patient engagement in communal activities through easily accessible rooms, oversized to accommodate multiple beds. A dedicated staff wing supports the main building by offering respite to workers and counseling for families. This holistic approach established a pioneering model for hospice architecture that extended to new facilities worldwide by the late 1970s.
Today, the organization continues to serve the community from this original building. Small renovations reconfigured patient rooms and added sustainability strategies.13 While outreach programs expand, Saunder’s intention to create a meaning space for end-of-life care continues to attract patients from around London.
Figure 7—Western window orientation providing maximum light for patient bedrooms
Figure 8—Gathering space for chapel services
Form responds to light access 1/256” = 1’
Goldin, 384. Ibid, 385. Worpole, 28. Zadeh, 1019. Worpole, 28.
St. Christopher’s Hospice
St. Christopher’s Hospice established the modern architectural typology as a patient-centered care system developed through evidence-based design. As historian Goldin describes, founder Cicely Saunders practiced nursing during World War II where she witnessed the distress inflicted on elderly patients during hospitalization.14 Saunders began to practice medical social work to advocate for their quality of life before being encouraged to study as a doctor. During her studies at St. Luke’s Hospital, the result of St. Luke’s Home, Saunders encountered the emerging philosophy of pain management for terminal cancer patients, in which patients received regimented analgesics every four hours rather than PRN, or “as needed.” She then completed her residency at St. Joseph’s Hospital under the guidance of nuns who practiced the traditional hospice method: caring for each patient physically as if they were on a spiritual pilgrimage.15 It was during this time
that Saunders converted to Christianity and dedicated her work towards serving the elderly. She credited this decision to her patient David Tasma, a Polish refugee who shared her vision of creating “homely places where people could die in greater tranquility.” 16 Saunders related this to her philosophy of caring for the “total pain” of a patient: the physical, emotional, social, and spiritual aspects of distress at terminal decline.17 Together, they imagined “a house where people could find relief from pain, where they could meet with encouragement for self-awareness and socialization, and where the setting would be uplifting, not depressing,” where people could die peacefully without the distress of the public palliative unit.18 At his death, Tasma left Saunders with the sentiment “let me be a window in your home” and £500 to start a hospice home. In his honor, Saunders opened St. Christopher’s Hospice in 1967 in Sydenham, London, redefining hospice in the modern era.
Figure 9—Original staff working with Cicely Saunders at St. Christopher’s Hospice in 1967
19 20 21 Jennings, 290. Verderber, 16. Chan, 44.
Connecticut Hospice
Modern hospice care in the U.S. began with the establishment of the Connecticut Hospice in New Haven in 1974.19 Deriving principles from St. Christopher’s Hospice, nurse and founder Florence Wald sought to implement this philosophy of care into the American healthcare standard. She partnered with architect Lo-Li Chan who, at the time, had no healthcare experience. Instead, they sought to create a series of principles from eye-witness testimonies to design a residential hospice environment instilled with patient-specific features.20 The success of this project led Chan to writing his article “Hospice: A New Building Type to Comfort the Dying” in the 1976 edition of the American Institute of Architects Journal, introducing concepts and constraints of hospice architecture to the U.S. Ahead of its time, the article remained obsolete for thirty years until evidence-based design became a leading design principle. The article outlined five principles for residential hospice design:
1. Designing for a community of patients, family, and staff
2. Creating transitions to acknowledge and support grief
3. Encouraging mobility or the perception of mobility
4. Illuminating the passage of time through carefully positioned windows
5. Confronting the meaning of death and the means to die well21
Innovations such as viewing alcoves, dedicated grieving spaces, and staff retreats reflected the understanding that care extends beyond the patient. This architecture modeled fundamental design concepts for hospice care for the following fifteen years, and the philosophy of care-centered hospice became integral in the development of private hospices.
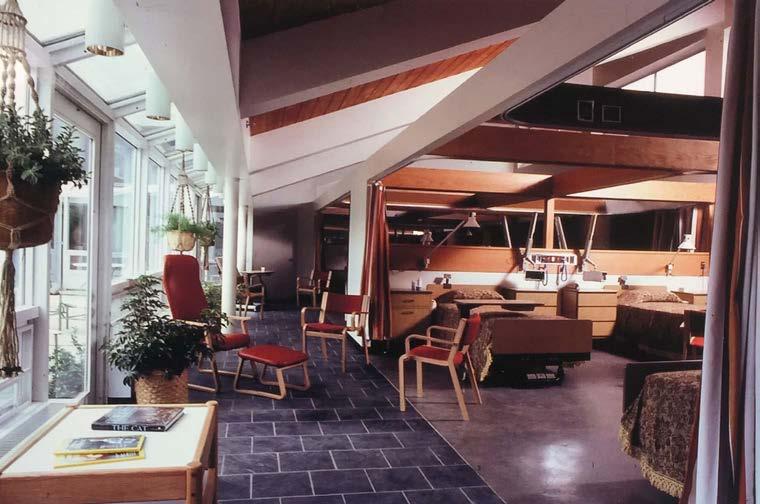
Figure 10—Interior conditions in designing with the pillars of hospice
Private corridor protects patient utility spaces
Four-bed rooms encourage community
Social corridor acts as a threshold
Terrace allows views of all times of day and season changes
Institutional spine maintains entry and staff spaces for offices, lockers, kitchen, and pharmacy
Family room accesses natural light through a clerestory
Main corridor connects institutional and residential portions
Common room provides mobility opportunities
Figure 12—Diagram of Chan’s principles for hospice
Figure 11—Modulated floor plan at Connecticut Hospice
22 23 24 Schwartz, 346. Jennings, 287. Ibid, 295.
Reducing floor plate inconsistencies for envelope control
Regulating corridors for efficiency rather than privacy
Establishing standard rooms for patient quality control
Providing minimum space requirements for patient rooms
Figure 13—Standardizing patient rooms and resulting building forms
System Standardization
The development of the hospice system changed with the implementation of public health policy and the rise of invasive medicine. The 1954 Hill-Burton Act funded hospital construction and included hospice in the standardization, effectively shifting terminal healthcare from a domestic-style approach to a regulated system.22 As health policy advocate Benjamin Schwartz noted, this incorporation “made them part of health policy rather than an extension of the welfare system,” diminishing the individualism of care. The 1965 Social Security Act Amendments further regulated hospices with the establishment of Medicare and Medicaid. Funding concerns challenged the typology of the hospice philosophy as these programs instigated the Certificate of Need qualification for new healthcare building funding, requiring the design and construction of hospice facilities within an eighteen month deadline before funding cuts. This ruling determined the public healthcare

system as an institutionalized business managed for the population rather than the individual.
Concurrently, the advancement of intensive care medicine questioned the relevance of end-of-life facilities. The technological revolution of the 1960s introduced ventilators, enteral nutrition, and coronary stents as solutions to terminal diagnoses. Jennings described this shift as “half-way technologies [that] could stave off death and prolong biological functions of life, but could not necessarily restore the patient to a meaningful mode of being alive.”23 While life-saving for thousands, these interventions redefined death as a medical failure, and hospice came to be viewed “not as a model for end-of-life care generally, but rather as a kind of last resort alternative, after life-extending medical treatments had become futile.”24 Standardized buildings and standardized deaths overtook the care aspects of healthcare.
26 27 Jennings, 290. Verderber, 18. Jennings, 301.

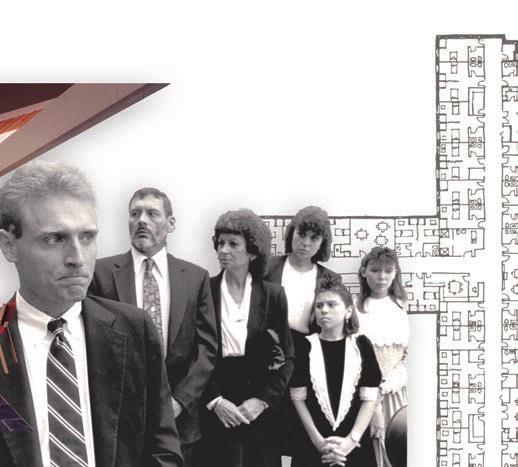
In reaction to this new public healthcare, patient rights increasingly sought individual autonomy in treatment decisions. The seminal 1990 Supreme Court case Cruzan v. Director affirmed “the right of the individual patient to refuse any and all forms of medical treatment, including life sustaining treatment.”25 This ultimately elevated palliative care to national recognition, exemplified by the 1999 postal stamp titled “Hospice Care.”26 Reformed Medicare policies began prioritizing the patient and their families rather than a standardized procedure, creating one of the “only programs in the entire American healthcare system that allows patients and families to forget about financial worries and to concentrate instead on the hard work of grieving and living in the face of dying.”27 While the standardization of systems continued to invade the hospice model for efficiency and cost purposes, the care instilled within the design provided an alternate view of mechanized death.

Figure 14—Cruzan v. Director case trial
Figure 15—1999 stamp
28 29 AtkinsRéalis. Adams, 259.
Building
Location
Firm
Client Size
Cost Completed
McGill University Health Centre
Montreal, Canada
AtkinsRéalis
McGill University
2,691,000 sq ft total, 11 stories
$1,579,000,000
2015
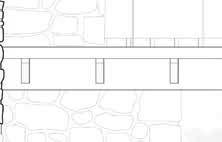
Recognized as one of the most technologically advanced healthcare centers in the world, the megahospital promotes its “patient-centered design focused on creating the healthiest environment for healthcare workers and patients.”28 The 517-bed facility incorporates zen gardens, an interfaith chapel, and an expansive parking deck for maximum visitors. Planned for over 20 years, the LEED Gold design demonstrates rigorous sustainability features for the care of every inhabitant. However, even with these resources, the specific development of the palliative care unit remains inadequate. Located on the ninth floor and directly connected to the oncology center, the 12 patient rooms occupy the entirety of the layout, allowing no dedicated space for family consultation or grieving away from the bedside.29 Adams critiques these failures as a cancer-focused, technologically indoctrinated model that discourages exterior access. Integrating palliative care units into megahospitals requires a intense reconsideration of the patient and family experience within these rooms.
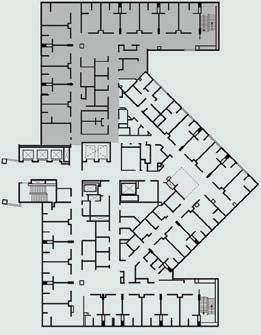










Figure 16—Megahospital in-situ
Figure 17—Palliative care unit within oncology
Massive form dominating site 1/512” = 1’
Jiang, 56. Adams, 261. Ibid, 259. Worpole, 12.
Megahospital
The introduction of the megahospital as the current architectural typology for palliative care reconfigures hospice towards an institutionalized identity. Designed to normalize illness and medicine, the megahopsital blends healthcare with mall, park, spa, and commercial spaces to present the complex as a “healing machine.”30 The technological advancement of these specialized wards provides consistent care; yet, in examining the palliative aspect of these buildings, all advancement in the philosophy of end-of-life care is lost. Adams describes this as a “culture of silence” surrounding death.31 He continues on to write that palliative units “often occupy the uppermost levels or most distant areas, perhaps as an effort to either safeguard it; ensure peace and quiet; or to minimize the visual impact of death.”32 Unlike the domestic environment of St. Luke’s Home, hospitals rely on custodial hardened surfaces. As St. Christopher’s Hospice taught the care of total pain within communi-
ty, current designs reduce palliative care units to the most distant areas. The standardization era categorizes hospices as institutions for the dying, a mindset that can be detrimental to the philosophy of palliative care. The institutionalization of healthcare building design, while successful in maintaining order, ultimately results in the dehumanization of the spaces and loss of socialization.33 When patients become numbers in a building, the very people we seek to care for cease to exist.
With this understanding of the hospice model progression throughout history, it becomes clear that the transition from a domestic environment to an institutional system directly correlates to a change in the philosophy of palliative care. The apparent need to shift the architectural expression back towards the community sphere of the domestic model requires examining the current medical programs shaping hospice care.
Institutional
Domestic
Timeline correlating domestic and institutional trends with development periods
13th c.
18th c. 1893 1954
Pilgrimages
Almshouses
St. Luke’s Home
Hill-Burton Act
St. Christopher’s Hospice
National hospice support
Connecticut Hospice
Cruzan v. Director
Megahospital
1 2 3 4 Silvers et al, 1. NHPCO. Brent and Schwarz, 278. Utz, 320.
Care in Crisis
Exponential need for hospice facilities in modern medicine
The relevance of palliative care as a core component of the healthcare system continues to grow as populations age and people live longer. In 2024, the Center to Advance Palliative Care (CAPA) reported 13 million adults and 700,000 children in the U.S. need palliative services, yet only 14% receive care.1 Among these patients, geriatric admissions account for 73.4% of licensed hospice beds, with terminal illnesses such as certain cancers, dementia, and circulatory diseases creating complex care needs.2 The healthcare system for this elderly community cannot be ignored, and there is no doubt that
“humankind is witnessing the unfolding of a potential human tragedy, that of a society not yet equipped emotionally, spiritually, and certainly not financially to absorb the latest influx of a new culture—its aging citizens.”3
Current projections indicate that by 2050, one in five Americans will be over 65 years old, increasing the elderly population from 35 million in 2000 to 88 million.4 People are living longer, and existing care systems for the dependent and debilitated will be insufficient. Reconceptualizing the current hospice facility model remains crucial to successful care of the community.
5 6 7 Hakola, 32. Jennings, 287. Worpole, 110.
Of Americans will be admitted to a hospice facility at end-of-life
Of hospice admissions are geriatric patients with multiple chronic illnesses
Americans will be over the age of 65 by 2050
Adults serve as full-time caregivers
Age of Medicalization
In recognition of these statistics, the medicalization of terminal patients questions the extent of intervention. Following the medical technology revolution of the 1960s, the rescue-oriented healthcare system insists on performing to cure disease rather than care for the patient. This medicalization often diminishes the quality of life and even exacerbates the dying process.5 Jennings claims that “there is a growing recognition of the suffering and cost…that high-technology medicine has created for critically and terminally ill persons.” Societal expectations insist on the preservation of life at all costs, often to the detriment of the psychological, relational, and spiritual aspects of well-being. When treatment ultimately fails due to chronic illness, the death itself becomes perceived as a medical failure rather than a natural progression of life. Americans are dying poor deaths, deaths with “inadequate palliative support, inadequate compassion, inadequate human presence and witness;
deaths preceded by a dying marked by fear, anxiety, loneliness, and isolation; and deaths that effaced dignity and denied individual self-control and choice.”6 This especially affects the elderly population who often suffer from multiple chronic illnesses. The prevalence of these diseases continue to increase as the population ages and treatments extend life without extending the quality of life. Rounds of hospitalizations result in a depletion of funds and a removal from the care for loved ones. The effect of this isolation on the modern patient suggests a social death long before physical decline. Of this isolation, Worpole writes, “Never before have people died as noiselessly and hygienically as today in these ‘more developed’ societies, and never in social conditions so much fostering solitude.” 7 Patients must be treated as autonomous individuals in need of a supportive community, not as passive participants in the institutionalization of death.
8 9 10 11 Jennings, 289. Verderber, 15. Jennings, 294. Chan, 42.
Demedicalization
The countervailing hospice philosophy establishes a patient-centered system designed to preserve the quality of life. This approach emphasizes dignity, comfort, security, relationships, and rest.8 As life-prolonging treatments become inviable, the terminal diagnosis prescription shifts towards providing autonomy and fostering engagement with family, friends, and community. Hospice thus rejects “the medical profession’s standard cliche ‘There is nothing more we can do’” to instead create opportunities for social presence in the final moments.9 Jennings writes of these moments and the ability to achieve meaningful closure by stating,
“to live well while dying is to navigate those relationships and meanings intact through the shoals of crisis; to die well is to preserve, and perhaps repair, those relationships right up until the end, and even beyond in the memory of those who survive.” 10
The opportunity, and truthfully, the responsibility, for medical facilities to support a good death provides a role for architecture to partake in caring for the patient. With the intent to demedicalize the last few days of life, the hospice unit shifts from a vessel for medical devices to a threshold space enabling patients to experience the passage of time in a safe and clean home. This setting welcomes family and friends to grieve well within the space, and it supports staff by providing efficient systems for the most personal care. The right to a good death continues to infiltrate public policy as a demand for ethical practices in all aspects of care.11
Gawande, 72. McLaughlan, 150. Jiang, 1. Craven, 1820. Worpole, 52.
the central focus uniting everyone in loving and grieving well revolving motions of giving and receiving, coming together, and letting go
neighborhood community patient family staff
a passerby, a visual stimulant through landscape interaction, a participant in remembering
the active and motivated group selflessly caring and dedicated to providing respite
Community-Centered Care
Designing a hospice building insists on redefining the social goals to achieve a demedicalized death. Gawande writes of the current architectural hospice model by saying, “it was never truly made for us.” 12 The model exists as a generalization of the typical patient to establish a standard and institutionalize those qualities; the hospice program exists to individualize every patient and establish meaningful connections to the community. The hospice model must therefore be reenvisioned as a new paradigm of social healthcare. Void of isolation and overmedicalization, the reconceptualized model will recall the original intent for hospice to be community-centered care. While the hospice facility will not cure patients of their terminal illnesses, it is possible for them to die healed through the fostering of “a secure environment grounded in a sense of connectedness.” 13 This new approach in establishing the hospice facility as a social architecture demands the right to a dignified death.
A social care model relies on four groups of occupants to successfully foster relationships in the last days of life:
1. Patient
2. Family
3. Staff 4. Neighborhood
The architecture must support patient well-being by allowing the most autonomy within the room. The opportunity to interact visually and physically with surroundings can stimulate the desire for social interaction.14 Families, often caregivers years prior to hospice, must be provided spaces to grieve together or individually.15 Staff members similarly need areas of gathering and respite in order to facilitate difficult discussions well.16 The neighborhood responds by interacting with the landscape, providing volunteer support, or returning to the facility for counseling after the passing of a loved one.
Building Location
Firm
Client Size
Completed
17 18 Verderber, 202. Worpole, 92.
Robin House Children’s Hospice
Balloch, Scotland
Gareth Hoskins Architects
Children’s Hospice Association of Scotland
29,060 sq ft on 6 acres 2005
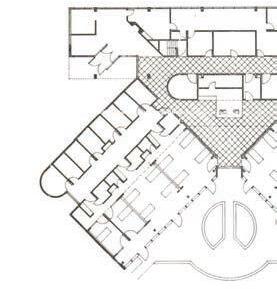
Located just outside Balloch, the children’s hospice offers families a place of respite while remaining integrated in the community. Two linear bars and a bisecting axis designate patient rooms and social spaces.17 The bars contain nine patient rooms with adjacent overnight accommodations. The surrounding mixed activity areas, pools, bereavement suites, chapel, and quiet rooms instigate an interior community of continual support.
The exterior landscape extends this concept by inviting visitors to explore orchards, therapeutic gardens, and livestock pastures. The roof form mimics this rolling terrain through syncopated waves, compressing over contemplative spaces and lifting over the children’s rooms. This form “exudes a sense of quirkiness and playfulness.” 18 Curvilinear steel beams support these single-story spaces, allowing clerestories to intersect play and gathering spaces. Through these playful design decisions, the building seeks to encourage respite and activation for interactions.
Figure 18—Patient room connection to community
Figure 19—Undulating roof interior condition
Linear form within the landscape
19 20 Willis, “Interview.” Gawande, 15.
Designing for Every Inhabitant
While patient and family spaces define the hospice building, the staff spaces often reside within central cores with no natural light. These spaces rely on efficiency, minimizing socialization and containing only medicalized spaces. The research suggests that these work environments for staff occupying the building every day can lead to low retention rates. Providing respite for staff to communicate well with each other, take a moment to recover from a traumatic interaction, or step away from an emotional moment, encourages the staff to continue to serve well.
To credibly discuss staff spaces within a hospice environment, Whitnie Willis, Assistant Clinical Professor at Auburn University College of Nursing, consulted during the research process. Her background as a registered nurse and educator encourages evidence-based practice, teaching a class specifically for Wellness in Aging. This human-centered care ori-
entation provides a unique perspective to staff spaces within a hospice building. A large portion of her research focuses on gerontology and ADRD, or Alzheimer’s Disease and Related Dementia. While the proposed design innovates for all, the majority would be within these groups.
In discussion with Willis, she asserts that loss of independence often becomes one of the greatest strifes for patients during the last few days of life.19 She cites the “Activities of Daily Living” to explain this concept, a model that defines parameters for autonomous living:
1. Using the toilet
2. Eating
3. Dressing
4. Bathing
5. Grooming
6. Getting out of bed
7. Getting out of a chair
8. Walking without assistance20
21 22 Willis, “Interview.” Verderber, 100.
As these functions decrease, the need for staff availability increases. These staff include both nurses and CNAs, or Certified Nursing Assistants. Hospice nurses undergo careful training for tempered closure, aiding families through the grief process and managing expectations for the ultimate passing of their loved one. Of this hospice experience, Willis says, “It doesn’t have to be negative,” commenting on how communities surrounding each other in shared grief provides closure for families long awaiting a painless time.21 Designing for “dignified death in private spaces” can be a moment of healing for the family.
A significant clarification within this discussion distinguishes a freestanding hospice facility from at-home hospice care. Outreach programs for at-home hospice allow nurses and CNAs to care for patients within their own home, a luxury requiring significant financial compensation and access to resources. The reality of palliative care necessitates that the majority of families choose facility residency
because of finances, centralized care, or supportive services, among other criteria. This requires available hospice facilities in every community, a need only increasing in reference to the statistics. As patients move between assisted living and nursing homes to the hospice facility, the staff spaces should intentionally invite nurses from these facilities to visit the patient cared for years previously. By designing a hospice facility with resources for outreach programs and visiting nurses, the building can support staff through a community of expertise.
The role of the hospice building should be to facilitate conversations between the nurses and families well, providing a variety of spaces for both gatherings and intimate meetings. Such spaces require “theraserialization,” or the therapeutic sequence of spaces for moments of respite before entering another room.22 Designing with these critical moments in mind can cultivate an appreciation for these staff members.
23 24 Silvers et al, 4. Verderber, 15.
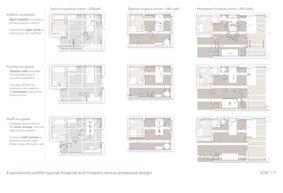
Reconceptualizing Hospice
Through the examination of hospice philosophy and the call for a demedicalized end-of-life, the advancement of hospice design depends on reconceptualizing medicalized spaces into places of social connection. Typical hospital rooms reserve an additional 6.45% of their square footage solely for storing medical equipment, devices essential in acute care but largely irrelevant in hospice settings.23 As these machines disappear, the current hospice model reduces this requirement to 2%, effectively limiting the overall square footage by creating strict corridors and generalized rooms. Reclaiming and restructuring these lost spaces to facilitate social interaction can become a form of healing within the end-of-life care environment. In hospice, healing does not emerge from technological intervention aimed at prolonging life; healing emerges from opportunities for community, moments of shared grief, and intentionally designed environments to support every inhabi-
tant.24 When the goal of hospice remains true to its founding philosophy, a goal intent on enabling the patient and family to live effectively even at death, the hospice building can facilitate a good death.
By reclaiming medicalized spaces, the hospice building can create site-specific domesticity through familiar environments and materials to form theraserialized spaces for community-centered care.
The heart of the thesis advocates for the demedicalized death—the right to die well in a space personally designed for its inhabitants.
Diagrams for reclaiming medical storage spaces within circulation areas
25 26 27 Mitchell, 98. Ibid, 101. Maggie’s.
Building Location
Firm
Client Size
Completed
Maggie’s Centre—Glasgow Glasgow, Scotland
Rem Koolhaas of OMA
Maggie’s 2,650 sq ft 2011
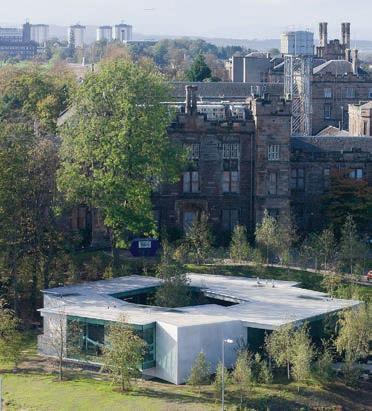
Maggie’s Centres display the foremost example for non-institutional care focusing on the total healing of its inhabitants. Founded by Maggie and Charles Jencks following a terminal diagnosis, the twenty-seven worldwide facilities provide respite for visitors dealing with cancer.25 A “non-type” structure, each building seeks “to elevate the human spirit through the integration of architecture and landscape design.”26 The hybrid form addresses palliative care as a social endeavor to care for the whole being.
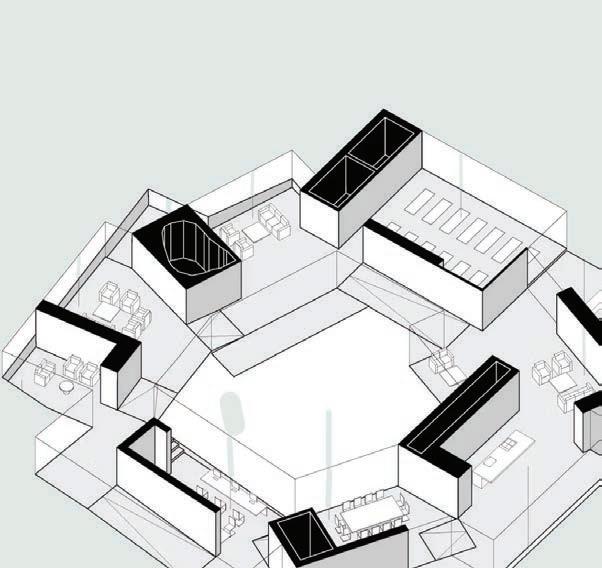
A specific case study of the Glasgow location reveals a sequence of interlocking rooms “like a series of scenes of domesticity.”27 The internal courtyard form concentrates visitors through a welcoming circulation path. A completely demedicalized space, the building seeks to instill “enthusiasm for life” by welcoming, encouraging, and cultivating interaction. This environment directly contrasts with the adjacent Gartnavel General Hospital, revealing the need for a reconceptualized palliative care.
Figure 20—Wandering circulation around courtyard and through domestic scenes
Courtyard form adjacent to hospital
Figure 21—Scales of interaction
1/512” = 1’
City and hospital surroundings
Emphasis on landscape, designed by founder’s daughter Lily Jencks
Courtyard form shelters and comforts visitors
37 Claire Hardin
Figure 24—Domestic scenes circulating courtyard
Figure 22–23—Building relationships to foster interior community
1 2 3 4 Worpole, 14. Chan, 45. Ulrich, 402. Chan, 45.
Reclaiming Hospice
Applying research to the design proposal
In developing a program that reconceptualizes hospice as a communal architecture, an evaluation of patient interaction within the last few days of care informs the spatial qualities. By applying site-specific domestic elements to familiar spaces serialized for respite, the overall building returns to the intent of hospice care. To help a patient live well until their death requires considering these aspects of their built environment.
Patient Interaction
In discussion of medicalization and the subsequent “social death” long before the physical death, patients must be allowed mobility or the appearance of mobility in order to sustain relationships.1 At the smallest level, the requirement for mobility begins at patient rotation, or the systematic turning of patients in the bed to avoid bed sores.2 Bedridden patients should have the opportunity to move around their room, to larger gathering spaces, and outside by wheeling the bed through enlarged doorways and corridors. For patients that can walk or use a wheelchair, circulation to their privatized and attached restroom greatly increases their autonomy. A small number of patients can even enjoy the community spaces and explore the facili-
ty. The opportunity for mobility enhances their feeling of independence, and it can ease family anxieties.3 Chan writes of this phenomenon in saying:
“Patients are trapped in their dying bodies; they must not also be trapped in their rooms.”4
By facilitating social interaction through the built design, patients and families can receive closure within the last few days of life. The design proposes that site-specific domesticity and theraserialized spaces can accomplish this goal.
5 6 7 8 Chan, 42. Worpole, 33. Marquardt, 147. McLaughlan, 150.
Reclaiming spaces to nurture instead of standardize
Site-Specific Domesticity
Acknowledging the pursuit of a reformed social environment, the hospice building can follow an institutional, neutral, or domestic design model. The institutional model, well-established in the austerity of the megahospital, rejects the social policy for personal interaction that hospice seeks to cultivate. In search for necessary efficiency and in legitimate fear of infection, the hospital often facilitates a culture of isolation.5 Examining a neutral environment, Worpole argues that there is no evidence for its effectiveness as it does not “offer an opportunity to make a thoughtful response as to how we best find a place and home for our frail but inviolable human condition.”6 By contrast, the domestic environment fosters a personal connection and provides therapeutic responses for both the patient and family. Marquardt asserts that “offering residents an environment that does not have an institutional design but has a homelike appearance and allows for individual transformations
has positive effects on behavior, well-being, social abilities, and care outcomes.”7 When hospice provides familiar, comforting cues through the domestic environment, patients and families can rest in the physical environment.8 Designing spaces that estrange community from familiar environments, especially in such times of emotional vulnerability, contradicts the core philosophy of hospice care.
To evaluate domesticity within a specific site, the design process must catalog the historical vernacular, the modern design forms, the architecturally significant landmarks within the city, and the materials often used. Construction methods, especially for any locally-sourced materials, supports these efforts. Motifs from these precedents and palettes originating from the materials guide the design towards a familiar environment.
Theraserialization from corridor to bedroom
Theraserialized Spaces 9 10 11 12 Verderber, 100. Chan, 44. Ibid, 43. Cama, 7.
Developing a program that reconsiders the conventional layout of hospice requires a systematic study of “theraserialization.” Coined by Verderber, the term hybridizes “therapeutic” and “serialization” to describe how the philosophy of hospice care can be integrated into the entire sequence of spatial experiences.9 This serialized progression from entry to exit positions individualized spaces as active contributors to the healing environment. An examination of these spaces categorizes them into areas for the collective, the personal, the intimate, and the isolated grief. The need for layered spaces with different degrees of public and private qualities, as well as corresponding scale, allows a personal approach to a social building.
The sequence further allows patients and families to move around the hospice facility through a series of “relief valves” where they can “confront the unknown gradually” and be allowed to withdraw.10 A careful
progression acknowledging the difficulty of transitions, the sequence drastically contradicts the typical assembly line in hospitals as patients move from waiting rooms to prep, operating, post-op, recovery, and out-patient rooms. Instead, the sequence provides thresholds for visitors to grasp the situation, and it allows patients the opportunity for socialization or withdrawal at given times.11 By allowing patients to personalize their environment by offering scales of interaction, some resemblance of autonomy can be restored.
An essential aspect for the success of these serialized rooms requires generous and well-lit spaces. While efficiency must be retained, allowing extra spaces for occupation within the room enhances the feelings of choice and independence. Additionally, evidence-based design supports the requirement for natural light within spaces to maintain helpful environments for healing.12
Public
Private bedroom
15 16 Cama, 7. Adams, 254. McLaughlan, 150. Ibid, 159.
Evidence-Based Design
Discussing the effects of daylighting on these user groups requires this evidence-based design approach, a study of environmental effects through an interactive and iterative analysis.13 By applying this method in the programmatic design phase, the building seeks to facilitate specific behavior and care outcomes otherwise lost in the expression of room layout or technical forms of healing. Designing for the “vanishing user group” acknowledges that the few days must provide a sense of the passing time.14 The sunrise, daylight, sunset, and night sequence becomes one of the last rituals experienced, and the building must reveal these qualities to the patients, families, and staff.
Hospice centers care for patients differently, not seeking to heal the body to full recover, but rather to cultivate a healing of relationships. McLaughlan emphasizes this distinction by saying, “the very measure of healing within palliative care is
different from other inpatient settings.” 15 He further insists that designers “have a responsibility, therefore, to advocate well-being” for every building inhabitant.16 The grieving family fundamentally understands the passing of time during the last few days of life, and the building design can reinforce this fact to provide a sense of closure. Window placement, glazing length, and views outward greatly affect this environment. Evidence-based design teaches that seeing the sky and ground in the same window, whether viewed by a patient or family member, enhances the overall processing of the stressful environment and increases the opportunity to grieve well. This method of study further suggests that well-designed views of landscape verses paved solids improves the overall comfort of the interior space. The communal hospice building must respond to these personal facts to emphasize the care experience.
Building Location
Firm
Client Size
Completed
Wilson Hospice House
Albany, Georgia
Perkins + Will
Phoebe Putney Memorial Health System
34,000 sq ft on 205 acres
2010
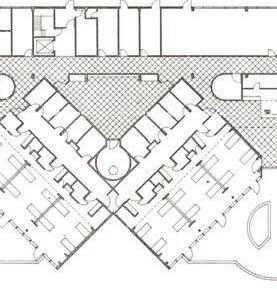
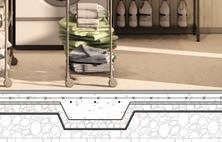
The domestic environment of the Wilson Hospice House cultivates spaces intent on maintaining human dignity. Located adjacent to wetlands, the expansive site supports a biodiverse exterior environment.17 Formed as a series of pods arranged in a semi-radial progression along the circulation spine, the facility “appears as a series of independent residences,” a quality accentuated by skylights, clerestories, and large windows providing views outward. Each pod holds six private bedrooms and a shared living room. These spaces cultivate a sustainable practice by pairing the non-institutional imagery with exposed wooden structure. Perkins+Will emphasizes the physical building caring for the inhabitants by designing the building with this mission:
“The building conveys a commitment to help terminally-ill patients live as fully as possible and encourages families at their most difficult moments.” 18
17 18 Verderber, 265. Perkins+Will.
Staff respite
Staff
Patient rooms
Living rooms
Figure 25–28—Domestic environment cultivated through evidence-based design
Programmatic layout
Branching form within landscape 1/512” = 1’ 1/256” = 1’
Verderber, 265.
Patient
Privatized rooms extend the mission of the hospice through layout and daylighting. The bed rests as the central component, allowing the social atmosphere of visitors to surround the patient.19 This spatial feature allows entry from the corridor, into the compressed vestibule, and to the larger gathering area next to the bedside. The wooden bed and headboard reveal this non-institutionalized approach and further support mobility as the bed can be wheeled through the double-doors to the patio. These doors and large windows allow patients to experience the outdoors through physical and visual connection.
Family
Adjacent to the patient rooms, the shared living room provides a place of respite and gathering. Carpeted floors, wooden structure, and lifted ceilings facilitate community in the residential space. Perkins + Will writes of these finishes, “In a world of stainless steel and technology, the building is intentionally different, warmer and more inviting.”20 One essential component in designing this space is the acknowledgment of the variety of visitors: parents, children, siblings, friends, coworkers, previous caregivers, and interdisciplinary staff. By providing a living room, the unfamiliar context of the hospice facility can ease anxieties for the visit.
Staff
Discussing the domestic versus institutional design of the hospice facility, creating ease and respite for staff greatly enhances the quality of care. Staff spaces in the circulation spine and staff wing offer immediate support to patients. These zones offer places for “focused headsdown work, staff and collaboration, as well as places of respite for staff to recharge.”21 Within the patient rooms, the headboard disguises medical outlets and technology while still providing ergonomic access.22 This pairing of the necessary medical devices within the domestic atmosphere creates the modernized hospice.
Claire Hardin
McLaughlan, 155. Wang et al, 1. McLaughlan, 160. Verderber, 99. Kaimal, 58.
Program Intent
Through theraserialization and evidence-based design practices to create a domestic environment, designing a social hospice lends itself to specific qualities per space.
Entry
Entering from a porch environment, the vestibule welcomes everyone into a collective environment of a well-lit, warm toned domestic atmosphere.23 Clear wayfinding to patient rooms, medical care zones, and auxiliary functional spaces eases discomfort.24
Living room
A counterpart to the residential space, the living room redefines the medicalized waiting room into a place of comfort and socialization. A variety of seating options provide a familiar setting to reduce distress.25 Identifying key aspects of the home living room to incorporate into this space will enhance the ideals.25
Office
A specifically designed staff environment welcomes camaraderie between facility nurses and outreach nurses. This place for respite seeks to aid in staff retention.
Hallway
Redefining the equipment alcoves along institutionalized corridors, hallways can provide a variety of seating and viewing opportunities. Intersecting the medicalized corridor with gathering spaces can reimagine the hallway as a personal entry into the room of a loved one.26
Bedroom
The bedroom serves every inhabitant in one space, functioning as the succinct moment for every kind of care. The room can empower the patient to seek meaningful connection, the family to grieve well, and the staff to care intimately.27 By increasing the size of the space and decreasing the visibility of clinical aspects
of care, the domestic environment of the bedroom centers around the scale of the bed itself. Lighting controls and exterior views of the sky and ground allow control of the space.28 The bedroom is the place of last goodbyes, and it should be treated with such reverence. Death requires grieving and oftentimes an evaluation of spiritual beliefs. As Worpole insists, “secularism in design and the provision of care and treatment does not require people to disengage with the deeper issues of ritual and occasion.”29 These rooms can thus maintain a personal connection.
Bathrooms
As resident agency declines, the bathroom should be designed to accommodate a variety of physical abilities. Devising a system for custodial ease with domestic attributes allows opportunities for familiarity. The family and visitors will most often occupy this space, requiring accommodations for their needs.
Yard
Therapeutic landscapes provide retreat, meditation, and all levels of communal interaction. Residents can interact with these environments through visual or physical connection to improve their psychological, emotional, and spiritual well-being.30 The evidence-based design research considers “the quality of the landscape [as] a vital element in the success of any hospice.”31 Significantly, these landscaped elements should pull from the logic of the surrounding site conditions, utilizing sidewalks and walking trails, water features, and a variety of gardens. These features all connect back to the building with simple exterior access and lookout points designed within the architecture for successful landscapes. 28 29 30 31 Kaimal, 58. Worpole, 143. Murphy, 53. Jiang, 3.
Building Location
Firm
Client Size
Completed
Urban Hospice
Copenhagen, Denmark
NORD Architects
Deaconess Foundation
25,000 sq ft
2016
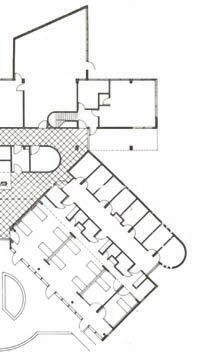
The layout of the Urban Hospice provides precedent for the spatial dimensions used to create an initial program concept. Surrounding by a residential neighborhood, the “quiet building” utilizes rectangular alignments with penetrating courtyards.32 These three semi-circular courtyards curve to “foster a greater overall sense of internal community” throughout the two-story building. Level One houses staff and services; Level Two houses patient rooms and overnight guest rooms. These adjacencies facilitate long-term stays and suggest a respite care model.
Patient care
Shared space Roof terrace
Figure 29—Massing in context
Figure 30—Shared interior spaces
Form within urban fabric
= 1’ Figure 31–32—Programmatic layout Staff care
32 Verderber, 235.
Program Proposal
Visitor Floor
Entry
Living room
Dining room
Kitchenette and storage
Family consultation
Restrooms (2)
Janitorial
Respite patient rooms (6)
Terminal patient rooms (8)
Wing living rooms (7)
Staff station (2)
Yard
Visitor parking
Staff and service parking
Hard walking trails
Soft walking trails
Water feature
Staff Floor
Staff station (2)
Facility nurse offices (4)
Outreach nurse offices (6)
Living room
Dining room
Kitchenette
Conference
Pharmacy
Linens
Kitchen
Private restrooms (2)
Public restrooms (2)
Janitorial
On-call room
Storage
Mechanical
Electrical
Riser
Net interior square footage
x 1.4 inpatient grossing factor
Total interior square footage
17,095
23,933
2.1
2.2
Design Proposal
Testing research theories through design
Site Selection
2.3 Humanizing Hospice Synthesis
Site Selection
Columbus, in Polk County, North Carolina
To reclaim medicalized spaces, the hospice building must instill community-centered care into every condition by considering programmatic adjacencies for social interaction. In selecting a specific site to test the design proposal, the following criteria determined the success of the environment:
Site Requirements
Location within U.S.
Distance to hospital
Hospital resources
Support facilities
Community services
Program requirements
Accessibility needs
Landscape qualities
Southeast U.S. to respond to an available site
Located within a 20 minute drive to local hospital
Serving an oncology unit with no in-house hospice
In relationship to assisted living or nursing home
Integration with existing public infrastructure
Opportunity for multiple site entries
Ability for on-grade entry to patient floor
Visual interest for exterior access
1 2 U.S. Census, 2020. NHPCO.
Respite care—Short-term care provided while caregivers travel or rest
Terminal care—Predicated 0-10 day period before passing, expected high visitor frequency and consultation for medical decisions
Qualifications for Need
After identifying these criteria, the next selection process cross-references two key statistics: (1) the percentage of senior citizens relative to gross population per county in southeast U.S. and (2) the serving hospitals with oncology units and no associated hospice.
The publicly available U.S. 2020 Census ranks the highest populations of senior citizens per county.1 In referencing this list, researching the highest ranks within the region for the serving hospital provided information for critical access versus acute care facilities. The selection of a hospital with an oncology unit recognizes that over 42% of hospice patients have been diagnosed with cancer and are no longer receiving treatment; notably, most other hospice patients have a variety of chronic diseases with no discernible common illness.2 To design within a county specifically with this need creates a level of feasibility for the project.
Locating a hospital with no in-house hospice further ensures the need of adding a freestanding facility to serve the area. This aligns with the real process of starting a hospice with a Certificate of Need, a lengthly process that involves government approval for funding and state registered beds. The proposed design qualifies as a private, freestanding hospice with government funded services, such as Medicare and Medicaid, and state registered beds with licensed nurses and CNAs. The facility also houses outreach offices for at-home hospice nurses, another layer of community within the staff. With separated respite and terminal wings, patients and families receive specific care with similar turnover rates. The design seeks to serve the area personally, using a repeatable model of domestic design in a site-specific study for site conditions, materials, and residential style.
National Rank of Counties with Most
Serving
Oncology
Site selection in Polk County
Site Selection
State County City
Parcel
Zoning
Conditions Serving
Infrastructure
North Carolina
Polk County
Columbus
4.3 acres owned by AdventHealth Hospital
Multiple Use Commercial, to be rezoned as Municipal Public Service
Available road access from multiple points, existing fitness trail from community spaces, large topography slope, some water on-site requiring water management system, opportunity for exterior gardens and paths
Adjacent to AdventHealth Hospital, in proximity to LaurelWoods Assisted Living and LaurelHurst Nursing Home
Located between the residential and business district, existing out-patient facilities and private medical offices offer services to the proposed freestanding hospice
Downtown retains historic storefront façades across one and two-story massings
Existing healthcare facilities ignore this county character
Polk County architecture centers around an equestrian and mountain-cabin style
The
55 Claire Hardin
prized architecture of the county is Tryon Presbyterian Church, constructed of local stone and timber
LaurelHurst and LaurelWoods Assisted living and nursing home facilities serving Polk County
Business District—Offices serving into downtown Columbus
H-108—Offices serving downtown Columbus
Isothermal Community College Satellite medical training and lecture facilities
Polk County Community Library Newly built community space for recreation and classes
AdventHealth Hospital—Formerly St. Luke’s Hospital, the one-story facility serves three cities
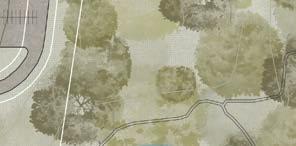
Selected site—4.3 acres currently owned by AdventHealth, holds existing walking trails along steep topography slope on densely wooded land
Private medical practices—Offices surrounding hospital core
Selected site connects to the community through program proximity and activation
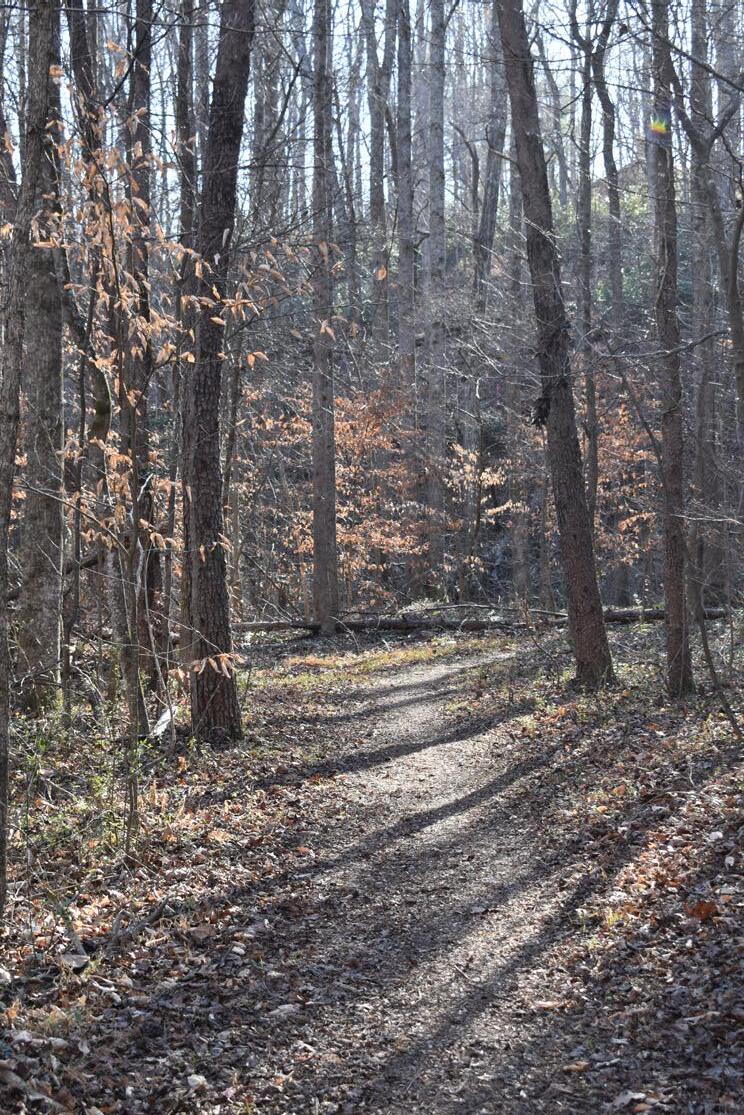
Claire Hardin
Densely wooded conditions of walking trail through site
3 4 Alan et al, “Interview.” Amanda, “Interview.”
Documentation
In visiting Polk County, documenting the site conditions and surrounding architecture allowed an understanding for the vernacular style of the specific area. A large portion of the visit was devoted to learning the history of the three towns of Columbus, Saluda, and Tryon. Through the expertise of librarians Dawn, Eli, and Wanangwa at the Polk County Community Library, public records revealed the historical significance of the mountain-style housing as a combination of motifs from the railroad industry and equestrian influence. Further conversation discussed the recent purchase of the local St. Luke’s Hospital and conversion to AdventHealth. Of this transition, Dawn says that the “fastfood medical [is] so industrialized, it’s the last place you’d become comfortable.”3 Locals Michael and Alan agreed with this statement, arguing that the neighborhood hospital had become a financial institution for profit rather than focused on community well-being.
Visiting LaurelWoods Nursing Home provided further reference for the need of a hospice facility with the city of Columbus. Interviewing business director Amanda and nurse Kathy, they explained the crisis for registered beds in the area. The expected wait time for entry into the assisted living or nursing home stays at about two years.4 After the nursing home no longer meets the needs of the patient, wherein the patient requires more than a two-person assist to lift, many residents move over state lines to a facility in South Carolina due to inadequate facilities within the county. The design proposal seeks to address this need while also integrating into the community, serving the existing facilities while also remaining personal to the surrounding area.
Site
LaurelWoods domestic exteriorLocal stone at college Surrounding mountains at site
Polk County, NC
25,380 sq ft
Architectural Thesis
Humanizing Hospice
Reclaiming Medicalized Space for Community Well-Being
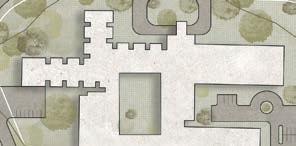
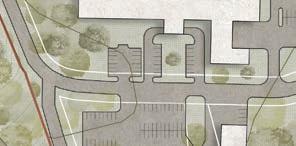
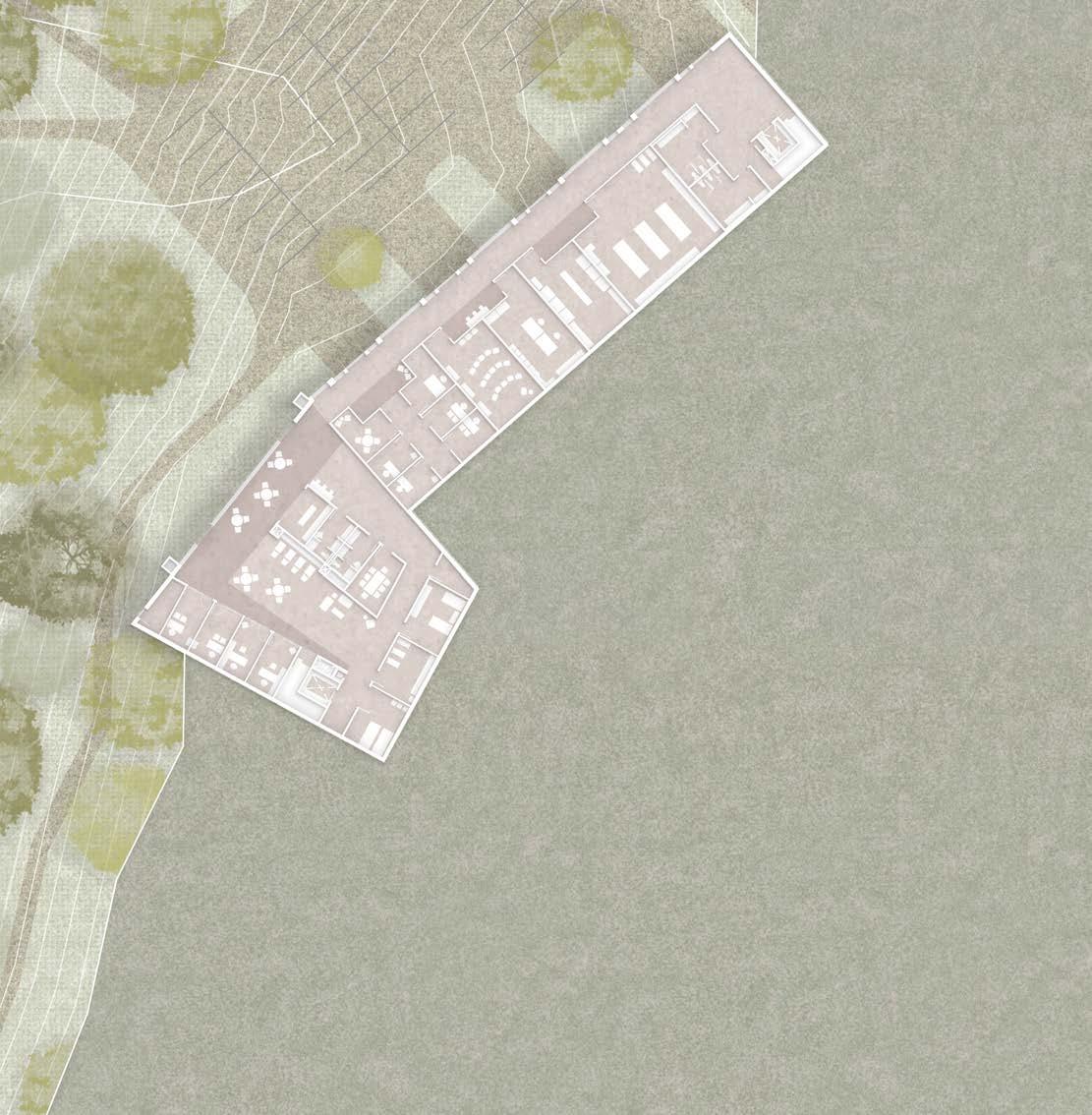
As prescribed by the research for healthy hospice architecture, the proposed design seeks to provide site-specific domesticity through familiar environments and materials to create theraserialized spaces for community care. The site documentation reveals significant program proximities the building must engage. Additionally, the steep topography of the wooded area demands a two-story response. Through an efficient layout, the additional square footage gained in repurposing medicalized spaces for social interaction allows a domestic environment intent on caring for all inhabitants.
Entry to the site delineates visitors from staff and services. The visitor entrance loops around the front lawn to provide an appropriate procession into the sacred space. The covered entry offers a simple wayfinding technique for the main doors. A welcoming space, the design intends to elicit emotions of walking into the neighbor’s living room, not walking into a medical facility. The two-story open room pulls
from the site vernacular of the mountain cabin, utilizing mass timber trusses and slanted roofs. The living room directs visitors from the hearth of the building into the dining area and back porch. The porch overlooks the landscape, offering views of the existing walking trails connecting to community programs and the retention pond for water management.
From this main gathering space, two wings extend to support respite and terminal care. The circulation creates a spine connecting patient rooms, but the typical medicalized corridor intersects living rooms every 16 feet. These shared living rooms offer families moments to have a conversation, receive a phone call, or take a moment to collect themselves. These rooms lead into semi-private alcoves as a theraserialized space for relief before entering the patient room.
The patient room further pulls from the site-specific domestic elements. Trusses lead from the window wall to a cleresto-
Collage during initial design for site documentation
ry, providing a view of the passing of time from the patient bed in support from evidence-based design techniques. In moments of deepest vulnerability, the stability in experiencing these aspects can ease difficult emotions. To further demedicalize the space, all necessary outlets, medical gas connections, and suction connections shift onto an inset wall perpendicular to the patient headwall, hiding the elements within easy access. This allows the family to fully focus on their loved one. Family accommodations intend to facilitate personal occupation. These designs include a sleeper sofa, an additional window seat daybed, and abundant storage in shelving units, drawers, cabinetry, and closets. Simple measures, such as providing a vanity in the bathroom, allow the family to fully occupy the space. These qualities continue to the private porch where families can move their loved one outside.
Even as these design choices hide medical intervention, the staff space must remain easily accessible. Discreet doors at
the entry to each wing allow nurses and CNAs to travel easily between the domestic visitor floor and the efficient staff floor. This subfloor opens out into the landscape, providing natural light and simple access from the staff parking. Instead of allocating enclosed cores for central staff collection, the floor houses both facility nurses and outreach nurses, as well as consultation rooms, a conference room for lectures, and services for the building. The staff occupy the building every day, and it is important to care for them as an inhabitant of the design.
The following drawings depict these moments with intention selection of materials and textures, all drawn from site-specific domestic studies. The heart of the thesis advocates for this demedicalized death—the right to die well in a space personally designed for its inhabitants.
01 Site Conditions
Adjacent facilities support community activation in site
Topography encourages two-level design strategies
02 Layout Design
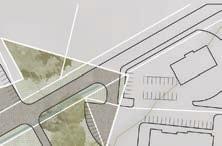
Site integration informs regulating lines along existing topography
Separate parking for visitors and services protects the domestic design intent
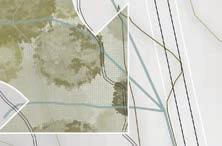
03 Hospice Home Form
Programmatic studies form a central entry with a respite and terminal wing
Entry reinforces views out into the wooded site
04 Proposed Design
Domestic forms and materials encourage a demedicalized outlook
Lighting conditions through clerestories and picture windows pull views out to the wooded site
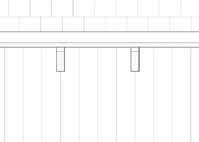
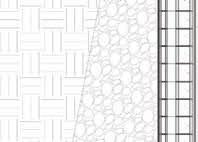
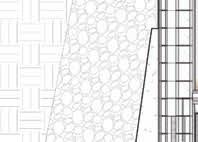
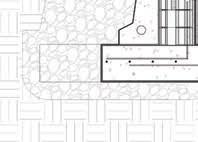
Detail section perspective provides information of building systems and materials specific to site
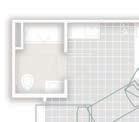
Visitor Floor
By separating domestic spaces from the necessary medicalized staff spaces, family living rooms and porches cultivate thresholds of respite. These alcoves, or reallocated spaces from a medicalized model to a demedicalized environment, provide respite to families to transition into caring for their loved one personally.
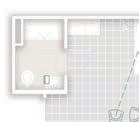
Staff Floor
All staff functions maintain simple circulation to the visitor floor while still having access to natural light. This intentionally facilitates a community of staff and nurses to aid in retention and care for the people caring for families every day.
Staff parking Living room
Dining room Kitchen
Consultation
On-call rooms
Outreach offices
Facility offices Conference
Pharmacy
Linens
Staff station
Patient parking
Entry
Respite wing
Terminal wing
Patient room
Porch
67 Claire Hardin
Staff level allows generous and efficient spaces for facility and outreach nurses
Staff parking Living room Dining room
Kitchen
Consultation
On-call rooms
Outreach offices
Facility offices Conference
Pharmacy
Linens
Staff station
Patient parking
Entry
Respite wing
Terminal wing
Patient room
Porch
Locally-sourced materials support the domestic environment specific to the Polk County vernacular
Entering the home welcomes visitors into their neighbor’s living room
Oak hardwood flooring in visitor areas
Speckled terrazzo flooring in staff areas
Pine CLT roof structural panels
Scraped plaster for textured walls
Travertine tiles in transitional spaces
Local quarried stone on exterior walls
Variety of fabric swatches
Quilted and tiled patterns throughout
71 Claire Hardin
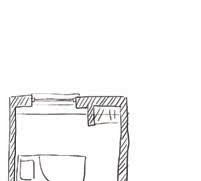
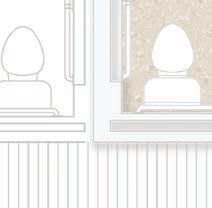
Patient occupied
As most hospice patients are bedridden, the typical mobility opportunities only allow the bed to be moved through the room door. The proposed design allows the bed to move outside to the patient porch. Additionally, sightlines from the bed position allow the patient to immediate know who entered the room, avoiding confusion.
Family occupied
Typical family accommodations include a countertop for bags and a reclining chair. The proposed design seeks to encourage family visitation by providing a sleeper sofa, several seating options, and an additional daybed in the window seat. Storage for suitcases and bags also allows personalization to maintain community.
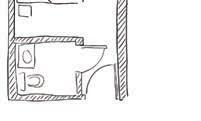
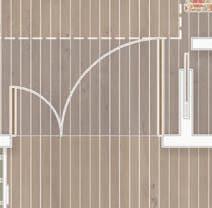
Staff occupied
In examining a specific staff function within the room as a case study, the removal of soiled linens involves bringing in a cart or carrying out the linens by hand. Building a closet specifically for this function allows nurses to dispose of the linens and collect them all at once from the hallway, without disturbing the patient or family in the process.
Typical
Typical hospice room Proposed design solution
Diagrams of innovations for specific modes of occupation by users
Accessible landscape
Semi-private alcove Service
Claire Hardin
Shared living room
Patient bedroom
Private porch
Transitional window seat
Patient room uses a consistent material palette and natural light access
Family accommodation encourages community support and interaction
75 Claire Hardin
Patient room model allows viewers to experience the lighting conditions
3’x4’ model contextualizes the surrounding mountain and densely wooded site
77 Claire Hardin
AdventHealth
Outpatient facilities
LaurelHurst and LaurelWoods Site
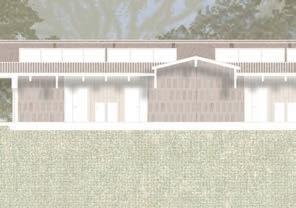
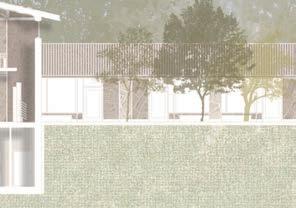
Living rooms intersect typical medicalized corridor to cultivate community
79 Claire Hardin
Staff floor retains domesticity while providing efficiency in industrial layout
81 Claire Hardin
Alcoves—Living rooms transition to quiet alcoves for private conversations and phone calls
Corridor—Moments of transition provide theraserialization between room pairings
Levels of interaction within section offer public and private moments in design
Mezzanine—Separated space allows reflection
Roof—Pitched roofs provide domestic motifs and clerestory views from patient rooms
Porches—Individualized exterior spaces allow ownership
Entry accommodates simple wayfinding and sequencing through the home
85 Claire Hardin
Synthesis
Research and Design Proposal
After researching the hospice typology in critique of modern medicalized precedents, the design begins a conversation of reconceptualizing the model through a domestic lens specific to a site. The resulting project questions typical standardization and pushes innovation in program layout, space utilization, family and staff interactions, and inclusion in surrounding community. A careful topic, the interdisciplinary study requires expertise from design professors, healthcare professionals, site locals, historians, and consultations for structural and material selection. The success of the thesis relies heavily on the reaction from the presentation, a reaction that suggests the innovations provoke thought and consideration of the sacred topic.
Research Analysis
The research follows a chronological progression from the origin of hospice as a social construct to the introduction as a public healthcare system, the inclusion as an architectural typology, a shift into public policy and standardization, and finally to the modern era of healthcare. This sequence distinguishes the idea of hospice away from the medicalized system and towards the right to die well. The culmination of research extends from only two design books for hospice; the majority of the research stems from medical journals discussing the demedicalization of care.
In beginning the design phase, the completed research remained sufficient for the proposal needs. Elements pulled from precedents, or designed in reaction to precedents, provided credible resources. Additionally, interviews conducted with local nurses and historians at the site further supported the design work.
To continue the research, more information for evidence-based design across healthcare facilities could support the design further. The research was not questioned within the design review.
Design Proposal
The proposal also follows a sequential documentation of the site and through the design process, from diagrams of regulating conditions to sectional decisions, plan layout, room innovations, and perspectives for material palettes. The proposal seeks to cultivate community within several scales:
1. County scale through program adjacencies and proposed services
2. Site scale by incorporation of existing infrastructures and topography
3. Building scale in the use of domestic motifs from the region
4. Room scale through intentional decisions for light access, personalization, and storage opportunities
5. Detail scale by the locally-sourced materials and proposed construction methods of the systems
The completed drawings follow the logic of the research by providing these scales
in layout, occupation, and texture. The composition of the physical review corresponded to the main ideas by tiling images on individual textured plates. This intentional layout focuses attention across the scales of the drawings.
Feedback from the review suggested the drawings showcased the research fully. The review focused on the innovations in the design, a successful discussion to provoke thought and consideration of the demedicalized hospice home.
Pinup for final design proposal presentation
3.1
Notes
Comprehensive list of sources
3.2 Images Cited Bibliography
Bibliography
Adams, Annmarie. “Home and/or Hospital: The Architectures of End-of-Life Care.” In Change Over Time, Volume 6, No. 2, 248–263. University of Pennsylvania Press, 2016.
Amanda and Kathy. “Interview with business director and nurse at LaurelWoods in Columbus, NC.” In-person interview. December 16, 2025.
AtkinsRéalis. “McGill University Health Centre.” AtkinsRéalis. Accessed November 2, 2025. atkinsrealis.com/en/projects/mc-gill-university-health-centre.
Brent, Ruth and Benyamin Schwarz. Aging, Autonomy, and Architecture: Advances in Assisted Living. Baltimore: John Hopkins University Press. 1999.
Cama, Rosalyn. Evidence-Based Healthcare Design. New Jersey: John Wiley & Sons, Inc., 2009.
Chan, Lo-Li. “Hospice: A New Building Type to Comfort the Dying.” The American Institute of Architects (AIA) Journal (1976): 42–45.
Craven, Joan and Florence S. Wald. “Hospice Care for Dying Patients.” The American Journal of Nursing 75, no. 10 (1975): 1816–1822. doi.org/10.2307/3423575.
Alan, Dawn, Eli, Michael and Wanangwa. “Interview with librarians and locals at Polk County Community Library NC.” In-person interview. December 16, 2025.
Gawande, Atul. Being Mortal. New York: Macmillan Publishing Group, 2014.
Grace, Goldin. “A Protohospice at the Turn of the Century: St. Luke’s House, London, from 1893 to 1921.” Journal of the History of Medicine and Allied Sciences 36, no. 4 (1981): 383–415. jstor.org/stable/24625460.
Hakola, Outi. “Medical Documentaries: Demedicalisation of Death.” In Filming Death: Endof-Life Documentary Cinema, 29–51. Edinburgh University Press, 2024.
Jennings, Bruce. “Design for Dying: New Directions for Hospice and End-of-life Care.” In Hospice Ethics: Policy and Practice in Palliative Care, edited by Timothy W. Kirk and Bruce Jennings, 285–308. New York: Oxford University Press, 2014.
Jiang, Shan. Nature Through a Hospital Window: The Therapeutic Benefits of Landscape in Architectural Design. New York: Routledge, 2022.
Kaimal, Girija, Janell L. Mensinger and Katrina Carroll-Haskins. “Outcomes of Collage ArtBased and Narrative Self-Expression Among Home Hospice Caregivers.” International Journal of Art Therapy 25, no. 2 (2020): 52–63. doi.org/10.1080/174548 32.2020.1752756.
Maggie’s. “Glasgow.” Maggie’s—Architecture & Design. Accessed August 21. maggies.org about-us/buildings-architecture/glasgow/.
Marquardt, Gesine, Kathrin Bueter and Tom Motzek. “Impact of the Design of the Built Environment on People with Dementia.” In HERD: Health Environments Research and Design Journal, Volume 8, no. 1, 127–157. Vendome Group: 2014.
McLaughlan, Rebecca, Richards, Kieran, Lipson-Smith, Ruby, Collins, Anna, and Jennifer Philip. “Designing Palliative Care Facilities to Better Support Patient and Family Care: A Staff Perspective.” The Center for Health Design 15, no. 2 (2022) 149–162. 10.1177/19375867211059078.
Mitchell, Jamie. “Renewing the Human Spirit Through Design: Celebrating Maggie’s Centres.” In Architecture and Health: Guiding Principles for Practice, edited by Dina Battisto and Jacob J. Wilhelm, 98–112. New York: Routledge, 2020.
Murphy, Michael, Jeffrey Mansfield and MASS Design Group. The Architecture of Health: Hospital Design and the Construction of Dignity. New York: Cooper Hewitt Smithsonian Design Museum, 2021.
“National Coalition for Hospice and Palliative Care (NCHPC). Accessed November 8, 2025. nationalcoalitionhpc.com.
New International Version (NIV) Bible. Grand Rapids, MI: Zondervan, 2011.
Perkins+Will. “Wilson Hospice House: A New Way to Deliver Care.” 2010.
Schwarz, Benyamin. “Nursing Home Design: A Misguided Architectural Model.” Journal of Architectural and Planning Research 14, no. 4 (1997): 343–359. jstor.org/ stable/43030436.
Silvers, Allison, Stacie Sinclair, Rachael Heitner, and Brynn Bowman. “America’s Readiness to Meet the Needs of People with Serious Illness: A State-by-State Look at Palliative Care Capacity.” Center to Advance Palliative Care (CAPC), edited by Melissa Scholl and Kirby Leadle, New York: CAPC, 2024.
Ulrich, Roger. “View through Window May Influence Recovery from Surgery.” American Association for the Advancement of Science 224, no. 4647 (1984): 420–421.
United States Census Bureau. 2020 Census of Population and Housing. Washington, DC: U.S. Department of Commerce, 2020.
Utz, Rebecca. “Caregiver Respite: An Essential Component of Home and Community Based Long-Term Care.” Health and Human Services 23, no. 2 (2022): 320–321.
Verderber, Stephen and Ben J. Refuerzo. Innovations in Hospice Architecture, 2nd ed. New York: Routledge, 2020.
Wang, Hongyi, Ling Zhang, and Yifei Shou. “Rest in Peace: Research on the Architectural Types and Design Ideas to Guide Design of Hospice Care Building.” Journal of Health Care Organization, Provision, and Financing 61, no. 12 (2024): 342–359. 10.1177/00469580241249435.
Willis, Whitnie. “Interview with nurse and educator concerning staff spaces in hospice design.” In-person interview. October 28, 2025.
Worpole, Ken. Modern Hospice Design, ed. 2. New York: Routledge, 2024.
Zadeh, Rana Sagha, Paul Eshelman, Judith Setla, Laura Kennedy, Emily Hon, Aleksa Basara. “Environmental Design for End-of-Life Care: An Integrative Review on Improving Quality of Life and Managing Symptoms for Patients in Institutional Settings.” Department of Health and Human Services 55, no. 3 (2018): 1018–1034.
Images Cited
Images not listed as figures within work were created or photographed by author.
Figure 1: Pilgrimage Group. Painting. Parishable Items. parishableitems.com/wp-content uploads/2010/01/sassetta-giovanni-journey-of-the-magi1.jpg.
Figure 2: An early example of Philadelphia almshouses, the Friends Almshouse was built in 1713. Drawing. The Encyclopedia of Greater Philadelphia. philadelphiaencyclopedia.org/essays/almshouses-poorhouses/.
Figure 3: Grace, Goldin. Interiors of the first St. Luke’s House at 50 Osnaburgh Street, London. Annual Report, 1894. Photograph. “A Protohospice at the Turn of the Century: St. Luke’s House, London, from 1893 to 1921.” Journal of the History of Medicine and Allied Sciences 36, no. 4 (1981): 397. jstor.org/stable/24625460.
Figure 4: Grace, Goldin. Exterior, Lawn Road. 1901. Photograph. “A Protohospice at the Turn of the Century: St. Luke’s House, London, from 1893 to 1921.” Journal of the History of Medicine and Allied Sciences 36, no. 4 (1981): 397. jstor.org/stable/24625460.
Figure 5–6: Grace, Goldin. Exterior, 14 Pembroke Square. 1903. Photograph. “A Protohospice at the Turn of the Century: St. Luke’s House, London, from 1893 to 1921.” Journal of the History of Medicine and Allied Sciences 36, no. 4 (1981): 397. jstor.org stable/24625460.
Figure 7–8: The Voices that Shaped Us: Modern Hospice in the Making. Photograph. St. Christopher’s. stchristophers.org.uk/voices/work/.
Figure 9: Our History. Photograph. St. Christopher’s. stchristophers.org.uk/voices/work/.
Figure 10: Fentress, Clare. View of a four-patient bedroom from the greenhouse hallway, ca 1980. Photograph by Norman McGrath. Courtesy of Lo-Li Chan. Photograph. “The Avery Review: Staff Needs: The Spaces of Hospice.” averyreview.com/issues/62 staff-needs.
Figure 11: Chan, Lo-Li. Plan. Drawing. “Hospice: A New Building Type to Comfort the Dying.” The American Institute of Architects (AIA) Journal (1976): 44.
Figure 12: Fentress, Clare. Robert Conrad and Lo-Li Chan, cutaway axon of southern half of the Connecticut Hospice, 1976. Courtesy of Lo-Li Chan. Drawing. “The Avery Review: Staff Needs: The Spaces of Hospice.” averyreview.com/issues/62/staffneeds.
Figure 13: Schwarz, Benyamin. Detail of a floor plan and a typical cluster unit plan in the original design. Drawing. “Nursing Home Design: A Misguided Architectural Model.” Journal of Architectural and Planning Research 14, no. 4 (1997): 352. jstor.org/stable/43030436.
Figure 14: U.S. Supreme Court Cruzan vs. Director Missouri Department of Health, 1990 407 U.S. 261, 110 S. Ct. 2841, 111 L. Ed. 2d 224. Photograph. Center for Practical Bioethics. https://practicalbioethics.org/shared-decision-making-and-advance-care planning/end-of-life-ethics/the-case-of-nancy-cruzan/.
Figure 15: 1999 33c Hospice Care. Photograph. Mystic Stamp. mysticstamp.com/3276-1999 33c-hospice-care/.
Figure 16: McGill University Health Center (MUHC) Redeployment Project, Montreal, Quebec. Photograph. AXOR. axor.com/en/projects/mcgill-university-health-centermuhc-redeployment-project/.
Figure 17: Adams, Annmarie. Floor plan of the McGill University Health Centre, Montreal, showing how palliative care is embedded in oncology. (Redrawn from the original plan by Adriana Mogosanu). Drawing. “Home and/or Hospital: The Architectures of End-of-Life Care.” In Change Over Time, Volume 6, No. 2, 248–263. University of Pennsylvania Press, 2016.
Figure 18–19: Robin House Children’s Hospice. Photograph. Hoskin Architects. hoskinsarchitects.com/en/projects/healthcare/robin-house-childrens-hospice.
Figure 20–23: Maggie’s. Glasgow. Photograph. Maggie’s—Architecture & Design. maggies. org/about-us/buildings-architecture/glasgow/.
Figure 24: Maggie’s Center Glasgow. Photograph. OMA. hicarquitectura.com/2021/10/omamaggies-centre/.
Figure 25–29: Perkins+Will. “Wilson Hospice House: A New Way to Deliver Care.” 2010.
Figure 30–32: Urban Hospice: A New Typology in a Historic Setting. NORD. nordarchitects. dkprojects/first-urban-hospice-in-denmark/.
8 inches by 10 inches
Montserrat designed by Julieta Ulanovsky, 2011.
Printed by Blurb