Juzo Sensation is a medical compression garment specifically designed for managing lipedema.
• Micro Massage Technology
• High Rise Waistband
• Therapeutic Medical Compression
• Available in 3 styles
• Black or Beige
Capri
Shorts
Pantyhose
Managing any chronic disease is hard work
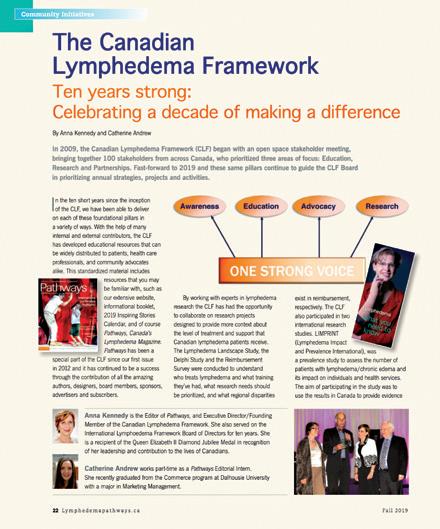
Dr.Céline Koryzma presented a keynote address at the National Lymphedema Conference in Toronto in November 2023. Her article validates the feelings that many people face while struggling with lymphedema. Managing lymphedema or any chronic disease is definitely hard work. It’s also human nature for us to be hard on ourselves when we fall short of our good intentions to change health behaviours. Practising self-compassion can help us deal with the negative emotions and setbacks.
The International Consensus for Best Practice for Managing Lymphoedema states that the arterial vascular status of the legs of all patients with lower limb lymphedema should be assessed before choosing the appropriate compression level. Maryse Baumier has been involved in the development of wound care for more than 20 years. She presents the three principal non-invasive instruments for assessing the arterial vascular status. Health professionals treating lower leg lymphedema should pay extra attention when reading this article.
Distributive justice is a term Dr. Anna Towers uses to describe the challenges of funding for lymphedema care that faces the McGill
Lymphedema Clinic and all lymphedema centres across Canada. She believes we need to advocate for our share of the cancer budget. Getting even just one percent of cancer care budgets dedicated to rehabilitation would allow better post-operative care, including lymphedema, for cancer patients. It’s a start.
Someone who was posting all the details of her cancer treatment on social media received a frank comment from someone on her account: “Cancer is the least interesting thing about you.” This statement stopped her in her tracks and made her realize that cancer shouldn’t define her. She had so much more interesting components of her life to share with her followers. I think we can all take this to heart for any diseases we are facing.
great photo of Jill on the cover of this issue. The Canadian Lymphedema Framework’s first stakeholder meeting was held in February 2009. Bonnie Baker, the CLF’s Executive Director, recounts the incredible journey of the organization and shares some of the goals and aspirations for the future. One of those is another collaborative conference with the International Lymphoedema Framework (ILF) in Canada. Some of you may remember the incredibly successful ILF/CLF conference
https://www.canadalymph.ca/columns/
Photo: NLNet
Fall 2024 n Volume 13 Issue 4
Publisher
Pathways is published four times per year by BCS Communications Ltd. on behalf of the Canadian Lymphedema Framework.
Editorial Board
Mei Fu PhD RN FAAN
David Keast MD FCFP
Lori Radke PT CLT
Anna Towers MD FCFP
Editor-in-Chief
Anna Kennedy
Executive Director
Bonnie Baker
Marketing Manager
Grace Neumayer
Advertising and Submissions
We welcome your ideas, contributions, letters and ad copy. While all material is subject to Editorial Board approval, inclusion does not constitute an endorsement or reflection of the views and opinions of the CLF and its Editorial Board. Contents may not be reproduced without written permission of the Canadian Lymphedema Framework.
Subscription Rates (1 year) Canada - $30. United States - $60. International - $75. Single copies and back issues - $8.
Subscriptions/return mail to Canadian Lymphedema Framework 4800 Dundas Street West, Suite 204 Toronto, Ontario M9A 1B1 Telephone: 647-693-1083
Email: pathways@canadalymph.ca www.canadalymph.ca
Photos:
NLNet, B.Baker, M.Beaumier, J.Edmondson, C.Koryzma All stock images are CanStock Canadian Publications Mail Agreement 40065546
ISSN 1929-1418 • Printed in Canada
We acknowledge the financial support of the Government of Canada.
Healthier lives through self-compassion
Dealing with the negative feelings that come with managing a chronic health challenge.
Peripheral arterial disease
Best practice assessment for lower limbs with lymphedema.
case for distributive justice The challenge of lymphedema treatment funding in Canada.
Celebrating 15 years of progress and impact A message from the CLF Executive Director.
Your print subscriptio complimentary digita
REQUEST ACCESS ONLINE OR BY EMAIL www tinyURL com/yes-digital pathways@canadalymph ca
Healthier lives through self-compassion
Dealing with the negative feelings that come with managing a chronic health challenge
By Céline Koryzma
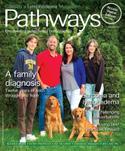
Haveyou ever tried to make a healthy behaviour change and failed? When I present to healthcare professionals on how to motivate patients to make healthy lifestyle changes and ask the audience members this question, almost everyone raises their hand. Even though I’m an expert in health behaviour change, I raise my hand too! Engaging in healthy behaviour over the long term is hard. It’s not about if we are going to “fall off the wagon” but when. Lymphedema management is hard work (Figure 1). If you are coping with a chronic condition like lymphedema, you understand that there will be good days and bad days, both in terms of your symptoms and your ability to manage them. It is extremely common for people managing chronic health conditions to fall back into old habits or stray from their self-management routine.
Popular culture, the media, influencers and salespeople want us to think that change can happen quickly and easily, and when it does not, we mistakenly believe there is something wrong with us, not with whatever they are selling. However, when people change their behaviour to become healthier, this change usually happens slowly, over a long period, with lots of bumps in the road and stops and starts along the way. Thousands of years of evolution have primed humans to prioritize short-term pleasure and to live for today rather than worry about health complications that may or may not happen years down the road. It is normal for people to avoid engaging in
1
Factors that make lymphedema management difficult.
behaviours that they find difficult, like managing a chronic health condition.
It is also normal for people to be hard on themselves—blaming or criticizing themselves when they do not meet their health goals. Even though this may be many people’s first reaction, unfortunately this does not work very well to motivate individuals to get back on track. This article will highlight how people living with chronic health challenges like lymphedema could use the practice of self-compassion to help manage the negative emotions and setbacks that come with this condition.
What is self-compassion?
Because we know change is hard, we don’t need to be so hard on ourselves. Studies demonstrate that being kind to ourselves, not being hard on ourselves, is most strongly linked to sustained behaviour change (Neff, 2003). Self-compassion is simply compassion directed inward, where a person is aware of their pain
Céline Koryzma PhD, R.Psych is a registered psychologist with Alberta Health Services in Calgary who specializes in chronic disease management. She also teaches communication and mental health counselling skills in her role as Clinical Assistant Professor with the Department of Family Medicine at the University of Calgary.
and has a deep desire to alleviate their suffering without blaming and placing negative value judgements on themselves. It is a kind and understanding attitude towards oneself that recognizes that making mistakes and getting off track is part of being human. Dr. Kristen Neff, a psychologist with the University of Texas at Austin and an expert in this field, defines self-compassion as consisting of three elements:
1 Self-kindness: Rather than engaging in harsh self-judgment, treating yourself with the same kindness, care and understanding that you would treat someone you care about. What would you say to a friend or your child if they made a mistake?
2 Sense of common humanity: Recognizing that suffering is part of the shared human experience. We all have areas of difficulty and imperfect lives. We can feel connected in our struggles rather than isolated and like we’re going through difficulties alone.
3 Mindfulness: Mindfully becoming aware and acknowledging our struggles rather than trying to make our feelings go away by moving into problem-solving or avoidance. Recognizing we’re struggling without being judgmental.
FIGURE
Self-compassionate people are more likely to face their health challenges headon. This means that they behave in ways to maintain or improve health.
Sometimes, people think being selfcompassionate means avoiding or ignoring difficult situations or letting oneself off the hook and doing whatever feels good at the moment, but self-compassion is something quite different. With self-compassion, we mindfully accept that the moment is painful and embrace
ourselves with kindness and care in response, remembering that imperfection is part of the shared human experience. Self-compassion is very different from self-indulgence. Many people say they are reluctant to be selfcompassionate because they are afraid they would let themselves get away with anything: “I’m stressed out today, so I’m going to stay in bed all day and not wear my compression garments.” This, however, is self-indulgence rather than self-compassion. Remember that being compassionate to oneself means that you want to be happy and healthy in the long term. In this case, showing yourself compassion may mean being understanding with yourself if you have stayed in bed longer than usual on a rough day, but also taking responsibility for your health and deciding to go for a short walk so you do not feel even worse later on.
A growing body of research has demonstrated the benefits of self-compassion across a wide range of domains. People who are more selfcompassionate tend to have lower levels of depression and anxiety and higher levels of life satisfaction (Neff, 2003). Self-compassion has also been associated with positive outcomes and coping skills in people living with chronic disease (Semenchuk et al., 2022).
When coping with a chronic condition like lymphedema, it is crucial for individuals to see themselves with some degree of kindness and compassion. Self-compassion can help individuals living with a chronic disease in several specific ways:
Self-compassion helps people deal with the negative feelings that come with managing a chronic health challenge.
Many chronic physical health conditions, especially those that require a lot of selfmanagement, have an impact on a person’s
mental health. Living with lymphedema can be emotionally frustrating. Challenging feelings like disappointment, sadness, anger and anxiety can understandably arise from the burden of time-consuming self-care, the unpredictability of the disease, and the impact of the condition on day-to-day activities, among other obstacles. Self-compassionate people show greater emotional resilience, which is the ability to adapt to stressful situations and cope with adversity (Semenchuk et al., 2022.) They tend to respond to challenges with more calmness and composure, which allows them to direct their attention towards healthier behaviours and coping strategies. In other words, they are able to respond thoughtfully to challenges rather than react hastily in ways that are not helpful in the long run. Practicing self-compassion helps people become more aware and mindful of their feelings and, therefore, less likely to become overwhelmed by them. Feeling better emotionally makes you more likely to engage in healthy behaviours.
Self-compassionate individuals take a more proactive approach to their health.
Self-compassion is a proactive coping strategy that helps people approach, rather than avoid, the difficult feelings, thoughts and actions that come with adverse life events like facing a chronic health condition. While it is normal to want to avoid thinking about and acting on a difficult challenge, avoidance often only makes the problem worse. Self-compassionate people are more likely to face their health challenges head-on. This means that they behave in ways to maintain or improve health, seek out medical attention more quickly, and are more likely to follow their healthcare provider’s recommendations (Terry, Leary, Mehta, & Henderson, 2013).
Practicing self-compassion helps people re-engage in healthy behaviours when they’ve encountered a setback. Providing comfort and validation to oneself is motivating and helps people move forward. Self-compassionate people are less likely to allow health setbacks to derail them entirely. They can better acknowledge and accept mistakes without dwelling on them (Zhang & Chen, 2015). Self-compassionate people may also feel less embarrassed or ashamed about their health condition because they keep in mind that many people suffer from chronic conditions and struggle to meet their health-related goals. The kindness and understanding they show themselves help them take responsibility for their missteps and be more honest with themselves and their healthcare providers about what needs to change to help get them back on track.
How to practice self-compassion
Although some individuals may be naturally more self-compassionate, it is a skill that can be learned. Like any new skill, becoming more compassionate with yourself can seem strange or be difficult at first. If you’re used to beating yourself up when you don’t accomplish your health-relat-
ed goals, it may feel uncomfortable or even silly to show yourself kindness and understanding. As a health psychologist, patients often share with me the harsh and self-critical thoughts they have when they get off track. The point is not that you will never be self-critical again. Those “I’m not good enough” or “I got off track this time; I guess I’m a lazy person” thoughts might always be with you. The idea is to mindfully acknowledge them, “Wow, I’m being really hard on myself; I would never talk to a friend the way I talk to myself!” and to offer yourself compassion instead, “I know I didn’t incorporate as much movement as I planned to this week. I had a lot going on. It is hard balancing all my roles while also managing a chronic disease. A lot of people struggle with the same things that I do.”
It may take some time to engage in compassionate self-talk in a way that feels authentic to you. There are guided practices you can find on Dr. Neff’s website that you may find helpful (www.self-compassion.org).
Below are some basic steps for practicing self-compassion.
– Explore which words and phrases feel right for you.
Specialist Clinic for Lymphology European Center for Lymphology
Do you suffer from lymphedema?
Because we know change is hard, we don’t need to be so hard on ourselves. Self-compassion helps us get back on track faster. This is a photo of my son when he was about 18 months old. He grabbed the maple syrup without me noticing, and safe to say he overdid it!
– Mindfully notice what you’re saying to yourself and if it’s unkind.
– Try not to judge yourself for having these thoughts; we are all hard on ourselves.
– Remind yourself that you are not alone and that many people experience health challenges.
– Generate compassionate images and phrases by picturing what you would say to a dear friend or a child if they made a mistake or did not follow through.
close proximity to Switzerland and France
Price for a 4-week treatment: $15,000 USD
(with accompanying person in the same room $20,000 USD)
4 WEEKS of intensive lymphological decongestive therapy includes:
• Specialist medical care by experienced MD‘s
• Daily decongestive therapy by our specialised lymphedema therapists (expert manual lymph drainage and bandaging) and many different decongestive movement therapies as part of group therapy
• Wound treatment if necessary by our certified wound experts and
• Accommodation and meals at the Foeldi Clinic psychological support if necessary by our psychotherapists
Price for a 4-week outpatient treatment: $13,000 USD
Contact:
Dr. Tobias Bertsch Senior Consultant tobias.bertsch@foeldiklinik.de
Transfer to and from Zurich or Frankfurt airport to the Foeldi Clinic
Picturesque Black Forest mountain range in
Some examples of selfcompassionate phrases include:
“I am having a hard time because this is hard, not because something is wrong with me. There will be good days and bad days.”
“If I’ve gotten off track, I can begin again. I forgive myself for my mistakes while I take responsibility for moving forward.”
“I am having a difficult time accepting these changes in my body. I know other people with lymphedema are also struggling with this.”
Self-compassion is a skill that can be started today and honed over time with practice that can help you keep up healthy habits that positively impact your lymphedema. Along with the self-compassion.org website, I recommend the following two resources for learning more about self-compassion and healthy behaviour change:
• Neff, K., & Germer, C. (2018). The mindful self-compassion workbook: A proven way
to accept yourself, build inner strength, and thrive—the Guilford Press.
• Lee-Baggley, D. (2019). Healthy habits suck: How to get off the couch and live a healthy life…even if you don’t want to. New Harbinger Publications. LP
References
• Breines, J.G., & Chen, S. (2012). Selfcompassion increases self-improvement motivation. Personality and Social Psychology Bulletin, 38(9), 1133-1143. https://doi.org /10.1177/0146167212445599.
• Fu, M.R., Ridner, S.H., Hu, S.H., Stewart, B.R., Cormier, J.N., & Armer, J.M. (2013). Psychosocial impact of lymphedema: A systematic review of literature from 20042011. Psychooncology, 22(7), 1466-1484. https://doi.org/10.1002/pon.3201.
• Gilbert, P. (2009). Introducing compassionfocused therapy. Advances in Psychiatric Treatment, 15(3), 199-208. https://doi. org/10.1192/apt.bp.107.005264.
• Neff, K.D. (2003). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity,
• Neff, K., & Germer, C. (2018). The mindful self-compassion workbook: A proven way to accept yourself, build inner strength, and thrive. The Guilford Press.
• Semenchuk, B.N., Kullman, S.M., Neilson, C.J., Ceccarelli, L., Boreskie, K., Kehler, D.S., Tutkaluke, T., Duhamel, T.A., & Strachan, S.M. (2022). Self-compassion, health behaviors, self-regulation, and affective states among individuals at risk of or diagnosed with a chronic disease: A scoping review. Mindfulness, 13, 1085-1111. https: //doi. org/10.1007/s12671-021-01821-3.
• Terry, M.L., Leary, M. R., Mehta, S., & Henderson, K. (2013). Self-compassionate reactions to health threats. Personality and Social Psychology Bulletin, 39(7), 911-926. https://doi.org/10.1177/0146167213488213
• Zhang, J.W. & Chen, S. (2015). Selfcompassion promotes personal improvement from regret experiences via acceptance. Personality and Social Psychology Bulletin, 42(2), 244-258. https://doi. org/10.1177/014616721562327.
~ Easy learning modules with small class sizes
~ Interactive, live classroom instruction with physicians
~ Learn precise manual skills with expert, accredited instructors
~ ISO 29990: 2010 certified training
~ CE credit available
• Decreases edema post-mastectomy
• Decreasing graduated compression from wrist to shoulder
• Revolutionary 3-dimensional fabric. Exceptional softness and elasticity
• Available in “Pro” open-toe format. Avoids chafing at the ankles
Be You Tonic Curvy Leggings
Pro Open-Toe Leggings
Micromassage Wave Fabric
Arm Care Arm Bands CCL1 & CCL2
Peripheral arterial disease
Best practice assessment for lower limbs with lymphedema
By Maryse Beaumier
Introduction
Lymphedema affects an estimated 35 million people in the United States and more than a staggering 140 million people worldwide, yet lymphedema is the forgotten vascular disease.1 Lymphatic, arterial and venous are the three vascular systems in the lower limb.1 All of them work together. The weakness of one can disturb the others, so it is essential to evaluate all of them before deciding on a treatment plan.
Each vascular problem in a lower limb has its unique treatment. Still, all the lower limbs require an assessment of the underlying arterial vascular condition before deciding on any compression or wound treatment.2,3 For example, compression of 40-45 mmHg
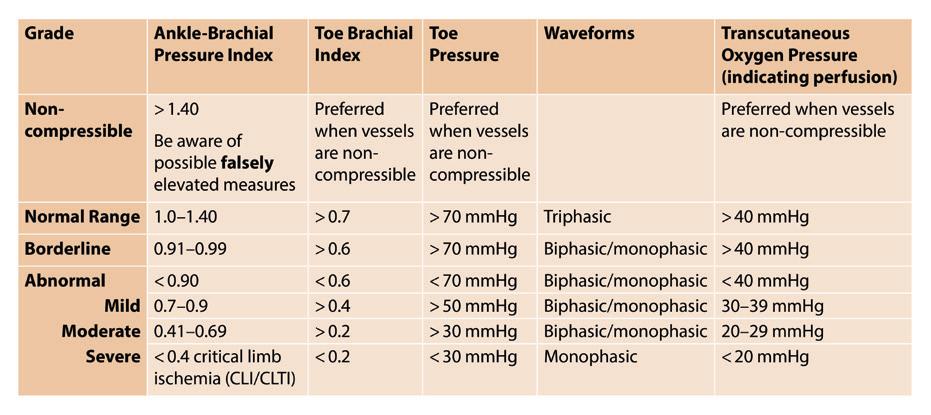
TABLE 1
Assessing Arterial Flow and Perfusion
is necessary to treat a wound when a venous deficiency is present. For lower limb lymphedema, a higher compression of up to 60-90 mmHg may be required.34 Finally, with severe arterial insufficiency (chronic limbthreatening ischemia), compression may not be safe. Chronic limb-threatening ischemia (CLTI) is a condition characterized by chronic ischemic rest pain presenting for >2 weeks, non-healing ulcers and/or gangrene in one or both lower extremities in conjunction with a clear diagnosis of peripheral arterial disease (PAD).19 Thus, persons with CLTI should always be assessed for the level of risk for amputation.35 The arterial status is the most critical step to assess a lower limb before deciding on treatment for a lymphatic or venous leg.
Complication of bandaging applied too tightly.
Source: M.Beaumier
As per the International Consensus for Best Practice for the Management of Lymphoedema, the arterial vascular status of the legs of all patients with lower limb lymphedema should be assessed before choosing the appropriate compression level.4,5 This article will present three non-invasive ways to assess the arterial status of the legs: the Ankle-Brachial Index (ABI), toe pressure measurement, and waveform interpretation.
Assessment
Source: Beaumier, M., Murray, B. A., Despatis, M.-A., Patry, J., Murphy, C., Jin, S., & O’Sullivan-Drombolis, D. (2020). Best Practice Recommendations for the Prevention and Management of Peripheral Arterial Ulcers. In: Foundations of Best Practice for Skin and Wound Management. A supplement of Wound Care Canada.
Maryse Beaumier BScN, MSc, PhD is a Professor in the Department of Health at the Université du Québec, Board Member of the Canadian Lymphedema Framework, Scientific Director and Researcher at the CISSS ChaudièreAppalaches Research Center, and author of Best Practice Recommendations for the Prevention and Management of Peripheral Arterial Ulcers.
Assessment of the arterial vascular condition means detecting the presence of peripheral arterial disease in the lower limbs. Peripheral arterial disease (PAD) is a chronic disease that can affect the upper and lower extremities but occurs more frequently in the lower extremities. The presence of PAD may contraindicate compression therapy or require a reduced level of compression.6 PAD causes decreased blood and oxygen supply to the skin, constituting ischemia that can affect any healing process. PAD leading to stenosis or occlusion of arteries supplying the lower limbs is caused by atherosclerosis in approximately 95% of cases.7 Clinical assessment is a central component of evaluation.8 About 200 million people worldwide are estimated to experience lower extremity peripheral artery disease.9 Peripheral artery disease is becoming an increasingly serious public health problem.10 A meta-analysis reported a 23.5% increase in PAD prevalence during the first decade of the new millennium.11 With the demographic trend towards aging and the projected rise in important risk factors, a more significant burden of peripheral artery disease is to be expected in the foreseeable future.10 The clinical presentation of patients
with objectively confirmed PAD can be categorized into four clinical subsets: asymptomatic PAD, chronic symptomatic PAD, chronic limb-threatening ischemia (CLTI),
smoking, dyslipidemia, hypertension, sedentarity, obesity and alcohol excess.3 The history story and physical examination are essential to identify patients with PAD or at increased risk of PAD; to assess for lower extremity symptoms, assess for pulse deficits, and other signs of PAD, including lower
Ankle-brachial pressure index
The ankle-brachial pressure index (ABPI) is also commonly known as ankle-brachial index (ABI).
It is a simple, non-invasive physiological test that remains the cornerstone for the initial diagnosis of PAD. Peripheral artery disease, defined as an ankle-brachial index lower than or equal to 0.90, is a major cardiovascular disease worldwide10 The values are well described in Table 1. However, this measure has multiple limitations, particularly in the setting of diabetes and chronic kidney disease (CKD), which are associated with noncompressible vessels, and for the assessment of CLTI.12,13 The validity
FIGURE 1
Ankle-brachial Pressure Index
Source: M.Beaumier
Toe pressure assessment
of this test is known to be suboptimal in the presence of medial wall calcification of the main arteries, especially in the diabetic population, where it has been reported to be prevalent close to 19%.14,15 A literature review recognized a high specificity level for PAD (83.3-99.00%) for an ABPI ≤ 0.90 but sensitivity levels of 15 to 79% for ABPI > 0.90, with lower sensitivity in the elderly and people with diabetes.18 ABPI must be minimally accompanied by waveform sounds and/or toe pressure assessment. According to global vascular guidelines on the management of chronic limb-threatening ischemia, noncompressible arteries may lead to falsely elevated or false normal ABPI values in patients with diabetes, chronic renal insufficiency, or advanced age, thus leading to inconclusive, distorted results or potentially
The arterial vascular status assessment: an essential part of lower limb lymphedema treatment.
overestimating the actual vascular flow.16 Ankle-brachial pressure index (ABPI) objectively measures the patency of the large arteries supplying blood to the foot. It is calculated from the ratio of the highest ankle systolic pressure for each limb to the highest systolic pressure in the arm. There are limitations to the test, particularly in the presence of lymphedema. Tissue thickening, hyperkeratosis or edema may make it difficult to detect blood flow using the standard 8MHz probe. Using a 4MHz probe and a larger blood pressure cuff may overcome these problems.17
Clinical guidelines recommendations, such as Trans-Atlantic Inter-Society Consensus (TASCII), recommend using toe pressure measurement in addition to the ABPI and transcutaneous oximetry for diagnosing PAD and CLTI.19 However, anecdotal evidence exists that lymphedema practitioners do not use doppler in assessing lymphedema patients because there is doubt over the sensitivity and accuracy of results in edematous limbs. However, there is no empirical evidence relating to the sensitivity and accuracy of doppler on oedematous limbs.20,21 Researchers and practitioners have an opportunity to collaborate on this important missing piece of clinical evidence. The arteries of the big toes are less prone to calcification. Hence, measuring pressure
vascularization.19 Their psychometric properties show a sensitivity of 50.0% specificity of 73.1% for the pedal artery and sensitivity of 72.5%, and specificity of 91.3% for the posterior tibial artery. The posterior tibial pulse is known to be the best predictor of arterial status, but in more recent studies, the pedal pulse was two times the best predictor of arterial status. Three waveforms are possible: triphasic for healthy arteries, biphasic for the presence of light or moderate PAD, and monophasic for severe PAD.
Table 1 from Best Practice Recommendations for the Prevention and Management of Peripheral Arterial Ulcers (Best Practice— Wounds Canada) summarizes the results from ABPI, toe pressure, and waveforms for the arterial status assessment for PAD detection in the lower limbs.
Best Practice Recommendations for the Prevention and Management of Peripheral Arterial Ulcers. In: Foundations of Best Practice for Skin and Wound Management. A supplement of Wound Care Canada.
at the toe gives more accurate results with fewer false-positive values.7,22-25 Toe pressure is considered more sensitive than ABPI in diagnosing PAD.16,25-29 A sensitivity varying from 90 to 100% and a specificity ranging from 65 to 100% for detecting arterial stenosis have been reported.30 Toe pressure can be measured either by a manual procedure using plethysmography or with a laser doppler device. A correlation of 0.92 has been calculated about their results, so a manual device at the clinic is enough for the measure.31 Normal toe blood pressure values were between 70 - 100 mmHg, and values considered insufficient arterial blood supply were <30 mmHg or ≥ 100 mmHg.32,33
Waveforms interpretation
The waveforms (noise and graphic) of arterial waves detected when measuring systolic pressures in the pedal and posterior tibial arteries also make it possible to qualify the health of the arteries and help evaluate arterial
Conclusion
As mentioned in the International Consensus for Best Practice for Managing Lymphoedema, the arterial vascular status of the legs of all patients with lower limb lymphoedema should be assessed before choosing the appropriate compression level.
This article presents three principal non-invasive methods to assess the arterial status of the legs: the ankle-brachial pressure index (ABPI), the toe pressure measurement, and waveform interpretation. This step is mandatory before applying any compression of the lower limb of patients with lymphedema. LP
References can be found at https:// canadalymph.ca/pathways-references
FIGURE 3 Waveforms
Source: Beaumier, M., Murray, B. A., Despatis, M.-A., Patry, J., Murphy, C., Jin, S., & O’Sullivan-Drombolis, D. (2020).
FIGURE 2
Toe Pressure
Source: M. Beaumier
Towers
One way to start our conversation is to imagine what an adequate healthcare system for lymphedema would look like in a highly developed country like Canada. We can then work backwards and examine the deficiencies, which vary depending on local community factors.
Since cancer is the best known, let’s start there. There’s prevention of cancer because if you don’t have cancer in the first place, you’re not going to develop all the complications of cancer treatment. Ideally, there would be more of a government focus on the prevention of smoking, excessive alcohol, obesity, lifestyle issues, chemicals and toxins.
Once cancer develops, it would be diagnosed early. After treatment, oncologists would be aware of the risk of lymphedema, and patients would have access to lymphedema information. For breast cancer, for example, one would have limb measurements before surgery and a couple of times post axillary node dissection. Then, afterwards, there would be educational information sessions about lymphedema, and there would be enough therapists to diagnose these patients early.
We know from a recent review that will be published shortly that cancer-related lymphedema is still a prevalent problem despite the use of more conservative surgeries, such as sentinel node biopsy. In our center right now, we are screening women who have had four or more axillary
A case for distributive justice
The challenge of lymphedema treatment funding in Canada
Transcribed from a conversation with Dr. Anna Towers regarding the challenge of adequate funding for lymphedema care in Canada.
nodes removed for breast cancer. We see them in our clinic one year later, and the lymphedema rate is 25%. So, it’s still a significant issue. Assessment and treatments need to be government-funded. If they need compression garments, orthotics, or more intensive treatment, Medicare would cover all that. Then, in the community, primary care physicians would be aware of lymphedema and chronic edema, so once patients stabilize, there would be physicians in the community who could take over with compression prescriptions, or a multi-disciplinary team at wound, lymphedema or Home Care clinics. For non-cancer lymphedema patients, again, the same prevention strategy: prevention of obesity and encouragement of exercise, more community programs would be in place to promote exercise in children, subsidized sports, and nutrition classes for young people.
Kennedy
Making highly processed food less available or taxed and fresh produce less expensive would also help. Obesity is so complex and the accessibility of psychological services for these patients is dismal.
Towers
Then, there would be multidisciplinary teams who are aware that any edema over three months needs an assessment of the cause.
Anna Towers, MD is the Director, Lymphedema Support Centre of the Breast Cancer Foundation of Quebec at the MUHC, McGill University Health Centre, Montreal.
Anna Kennedy is a Founding Member of the Canadian Lymphedema Framework, Editor of Pathways magazine and lives with lymphedema in Toronto, Ontario.
If the patient is obese and/or has chronic venous insufficiency, there’s a likely diagnosis of lymphedema. Then, the team should be aware of how to steer the patient towards proper compression garments and would advise them on the prevention of cellulitis. Wound care nurses would be called wound prevention nurses or chronic edema nurses. They would work with their colleagues to help
We know from a recent review that will be published shortly that cancerrelated lymphedema is still a prevalent problem despite the use of more conservative surgeries.
with the early detection of chronic swelling, get those patients diagnosed as contributing factors, and treat them before they develop wounds. All of that, of course, would be funded by the healthcare system.
I’m unaware of any community in Canada where that works the way it should. The system is in place for any other chronic condition, like diabetes, hypertension, or heart disease, and they’re aware of what to do at the primary care, secondary, and tertiary care levels and what everyone’s role is. But not for lymphedema.
Kennedy
So how do we change that? Is it primarily the lack of awareness among healthcare providers and policymakers? I remember the letter the Canadian Lymphedema Framework wrote 14
years ago to our Prime Minister, outlining the deficiencies in lymphedema care in Canada. The reply message from the Health Minister at the time was basically that for both cancer care and research dollars, lymphedema was adequately covered. Why are politicians and policy makers naïve about what we do and don’t have?
Towers
I think it will take a lot of advocacy and resources. We must insist that the health care system invest resources to save money in the long term, reducing morbidity and mortality. You’re saving money with people getting less cellulitis; you’re saving costs to society in general because people are more functional. And especially for non-cancer-related lymphedema, you’re actually saving lives because those people who are now neglected tend to have wounds, recurrent cellulitis in the lower extremities, and a significant rate of septicemia that can be life-threatening. They have reduced mobility. Your life expectancy will be reduced if you can’t walk and function normally. Non-cancer-related lymphedema, when combined with obesity, is as bad as having cancer in terms of shortening life expectancy.
care practice that some palliative regimens, costing six figures, continue to be provided to patients with very advanced cancer who get neither life prolongation nor a better quality of life from those treatments. And yet, these treatments are available and are provided because there seems to be a bias towards drug treatment and new technologies.
disease requiring dialysis, you get people who go blind, who require amputations, who die prematurely from heart disease. And that’s what used to happen before the 1940s and 1950s, before these diabetes services were properly implemented at all levels: primary, secondary and tertiary care.
Kennedy
Let’s go back to the issue of distributive justice that was brought up in the Spring issue of Pathways. For chronic diseases other than lymphedema, we have pharmaceutical products to treat those conditions. The pharmaceutical industry partners with clinicians and is there to advocate and lobby the government to have medications approved and subsidized. For lymphedema, we have good partners in the form of garment manufacturers and garment providers. However, compared to the large pharmaceutical firms, they are small companies. Therefore, we don’t have the same lobbying power in lymphedema as we do with other chronic conditions.
So, for conditions that are treated with medication, such as chemotherapy for cancer, you have the latest drugs; you have the latest palliative chemotherapies, immunotherapies, and stem cell transfers. Some of these technologies cost hundreds of thousands of dollars per patient. I know from my palliative
One way to make this more equitable would be, for example, to advocate for a certain percentage of the cancer care budget to be set aside for rehabilitation for problems caused by cancer treatment. What about even just one percent? And I think if people inquire as to what the cancer care budget is in their cancer centers, they would be surprised at how high it is. You will be surprised at how little it takes to provide rehabilitation for those who need it. In our institution in Montreal, just one percent of the cancer care budget would cover not only lymphedema care but also other cancer rehabilitation issues like fatigue, weight loss, lack of appetite, psychological issues and chronic pain. It might even cover some palliative care programs like music therapy, art therapy, and volunteer coordinators for palliative care. There’s a lot you can do with 1% of the total cancer care budget because an enormous amount is spent in cancer centers to treat the disease.
Kennedy
Comparatively, as an example, what disease covers all aspects of care from start to finish? Diabetes?
Towers
Diabetes is a good example. There is early diagnosis with blood tests administered to check if the glucose level is high, especially in those at risk, if they’re obese, or if they have a family history of diabetes. Then, it is treated early with medication. If that doesn’t work, you get insulin. The aim is to prevent kidney disease, heart disease, peripheral vascular disease, eye problems. And if you don’t provide proper care to diabetics, then you get people in emergency rooms with hyperglycemia, you get kidney
Could it be that other diseases have complete care because they involve essential internal organs (kidney, heart) and lymphedema, in the minds of many physicians, is considered just a swelling problem?
Towers
You are right. I don’t think there’s the awareness of the functional problems that lymphedema can lead to if it’s not treated properly, along with the cellulitis rate, especially with lower extremities. There isn’t an awareness that lymphedema is not just a cosmetic issue but that it can shorten life if it is not properly managed.
Kennedy
So, in regards to advocacy, it’s starting at the root cause and ensuring that physicians and policymakers are aware.
Towers
Yes. We have some help from garment manufacturers who are promoting education. Of course, the lymphedema associations are a big help.
Kennedy
They do an excellent job of raising awareness with the general public. Still, many cater to their members and people who already know about lymphedema and are living with it. The people we need to reach are healthcare providers to perform prospective surveillance and educate those at risk about what to look for and what to be aware of once they’ve had cancer treatment.
Towers
Yes. For non-cancer lymphedema, one target that could lead to rapid multiplication of efforts would be for wound care nurses to be trained to treat chronic edema early. They could have a significant role in educating the primary care providers they interface with. They could teach nursing colleagues and primary care physicians that any chronic swelling lasting more than three months needs to be looked at. Is it a lymphatic failure from venous disease or obesity, or is there another underlying cause that needs to
be investigated? And then, if not, should that person be in proper compression? Proper compression requires education on adequate flat knit compression for chronic edema.
Kennedy
The six-week modular micro-course that the Canadian Lymphedema Framework offers with the University of Alberta is an excellent start. It provides a general overview for health professionals interested in learning about lymphedema. However, it is not a certification course. I would love to see a collaborative effort with Wounds Canada to integrate education about lymphedema into certification courses for their nurses.
So, specifically at the McGill lymphedema clinic, what has changed since the spring?
Towers
We have interim funding and, I believe, an understanding of the situation from the Ministry of Health in Quebec -- in particular, the agency that deals with cancer care. I believe and hope that it’s just a matter of working out the details over the next six to 12 months.
Kennedy
Was that progress due to the excellent advocacy support, including the number of petitions received?
Towers
I believe so. The patients went to the media. We received dozens of letters of support from colleagues, academics, and patients from across the country, the US, Europe, and internationally. To date we have 14,795 signatures on the petition. People can still sign here: https://www. change.org/p/sauvez-le-programme-dulymphoed%C3%A8me-du-cusm-save-thelymphedema-program-of-the-muhc. If we encounter any more roadblocks, we will present that petition to the hospital and
One Wish Awards
the Ministry of Health. We know that the healthcare system is overstretched. But we need to advocate for the essentials. We need to demand distributive justice.
Kennedy
I love the term distributive justice and fighting for 1% of the cancer budget to gain equitable access for lymphedema care. Another example of equitable funding would be advocating for the same comprehensive care that diseases like diabetes have. Everything from start to finish. So why are there these gaps? Why is lymphedema treated like a poor cousin?
Towers
In contrast with Europe, where rehabilitation and physical treatments are more respected, I believe that North America has a cultural bias towards providing new high-tech, expensive treatments that might not benefit the population relative to what these products or technologies cost. So, without absolutely impeding technological progress, administrators will have to make important decisions as to how to distribute funds.
close December 31, 2024.
Kennedy
In Canada, those decisions are made at the provincial level. But at the Canadian level, there’s a lot of education that can be done. We could be sharing strategies among advocates about what has worked elsewhere. But I think an explanation of distributive justice is important because you will have some patient advocates insisting on access to private MLD therapy sessions every four weeks. And that’s not what we’re saying.
Towers
That’s an important point. Something that we stress with our administration is the need to provide evidence-based care that is cognizant of limited resources. In other words, we need to do as much as possible with the limited resources we have. For example, we could maximize online presence, provide group education sessions. We need to really look at what’s the evidence for the various therapy techniques that are being used. I think we need to focus on patient education on self-management.
Kennedy
The update of the Canadian Breast Cancer Lymphedema Guidelines, that Margie McNeely
and her team are leading will also better support evidence-based care. We talked about the role that advocates, provincial lymphedema associations and the Canadian Lymphedema Framework can have. In conclusion, what can organizations do, and what can our readers do?
Towers
We need to advocate for more academic clinical lymphedema programs to create the knowledge base and treatment guidelines – those certified therapists based in a university teaching hospital that see complex cases, do research and provide teaching. They would then need to partner with their provincial lymphedema association to create educational programs and to inform health professionals and patients about the latest research.
So how do we get there? Well, it’s heartening to know that we’re slowly getting more lymphedema therapists who have PhDs, and we’re slowly getting more physicians involved. We need more academic nurses who might have expertise in wound care. So, nursing professors involved for the noncancer population. All this would need to be
built up over the next 10 to 20 years.
In summary, we know that resources are limited in the health care system. The bias towards increased access to expensive technological solutions makes things worse rather than better. Lymphedema and chronic edema lead to increased morbidity and reduced life expectancy. Lymphedema patients deserve care and distributive justice demands that they receive it. LP
Editor’s Note:
Dr. Towers, Anna Kennedy and several other Canadians participated last fall in the LANA Summit in collaboration with the American Cancer Society. The working groups were tasked with providing updated reviews of lymphedema treatments, prospective surveillance, surgery etc. Their reports will be published as open access later this year or early 2025 in the Medical Oncology Journal. We encourage readers to look out for the publication and update their educational programs on the latest reviews of the literature and the scientific evidence for lymphedema treatments.
TheKloseTrainingAdvantage
• 135-hours of lymphedema education
75-hr engaging online home study module
60-hr (6 1/2 day) classroom education
• Time-tested, effective and evidence-based curriculum
• Learn from the most experienced instructors in the field
• Fewer days away from home and work
• Greater flexibility to fit your personal schedule
• Exclusive post-graduate resources
• Special pricing for Canadian Therapists
Online Courses
• Breast Cancer Rehabilitation with Jodi Winicour, PT, CLT
• Strength After Breast Cancer with Katie Schmitz, PhD, MPH, FACSM
• Wound Management for CLTs with Jan Weiss, PT, DHS, CLT
• Head & Neck Lymphedema with Heidi Miranda-Walsh, OTR/L, CLT
• Elastic Taping for Lymphedema with Ruth Coopee, OTR/L, CLT
• Add’l courses at klosetraining.com
Celebrating 15 years of progress and impact A message from the Executive Director
By Bonnie Baker
By reflecting on our achievements and setting our sights on future goals, we reaffirm our commitment to the lymphedema community and continue to strive for a brighter, healthier future for all.
Aswe mark the 15th anniversary of the 2009 inception of the Canadian Lymphedema Framework (CLF), I am filled with immense pride and gratitude. Over the past decade and a half, we have grown from a fledgling organization to a formidable force in the field of lymphedema education, research, and advocacy. This milestone serves as a testament to the dedication of our Board of Directors, the efforts of our founders, past directors and staff, the support of our partners, and the resilience of the Canadian lymphedema community.
Introducing our Board of Directors
Our current Board of Directors is a diverse group of passionate individuals who bring a wealth of expertise and a shared commitment to our mission. It is my pleasure to introduce them, below. The Board’s leadership and vision have been instrumental in steering the
CLF towards new horizons, and I am profoundly grateful for their service.
Honouring
our founders and past directors
We owe a debt of gratitude to our founders and past directors. Their vision and efforts laid the groundwork for our current successes. Their pioneering spirit and relentless pursuit of excellence have been the bedrock upon which we have built our current initiatives. These contributions have created a lasting impact that continues to inspire. Read about the CLF’s first 10 years in our anniversary article from 2019 at: tinyurl.com/CLF-10Years.
A pathway of achievement
The CLF has achieved many milestones that have contributed to advances in the field of lymphedema:
Education initiatives:
We have developed comprehensive educational resources which have empowered healthcare professionals and patients with essential
Bonnie Baker is Executive Director of the Canadian Lymphedema Framework (CLF) and represents the CLF on the International Lymphoedema Framework’s Framework Committee. She works closely with the CLF’s Board of Directors to align the organization’s strategic direction and day-to-day operations with its vision, mission, and charitable purposes.
knowledge and skills. These include the University of Alberta Lymphedema and Chronic Edema Management microcourse, our web-based and print educational materials, and our Lymphedema Learning Library Online. Of course, we are incredibly proud of our Pathways magazine, and grateful to our editor and her editorial board members, past and present, for their passion and hard work to produce this quarterly magazine which celebrated 50 issues this past summer.
Research and clinical advancements:
Our participation in international studies like LIMPRINT (lympho.org/limprint) has contributed valuable data on the prevalence and impact of lymphedema, helping to shape the future of treatment and care in Canada.
Our biennial, national conferences bring the lymphedema community together to network and learn and aim to inspire new research and collaboration to improve the lives of those living with lymphedema.
Advocacy and awareness:
Through initiatives like World Lymphedema Day and March Lymphedema Awareness Month, we have raised the profile of lymphedema, advocating for better recognition, diagnosis, and treatment.
Collaborative partnerships:
Our partnerships with provincial and international lymphedema organizations and other stakeholders have been pivotal in advancing our mission and expanding our reach.
These achievements are a collective victory, made possible by the unwavering support and collaboration of our stakeholders. We invite you to learn more about our work by reading our 2023-24 Impact Report at tinyurl.com/2024CLFImpactReport.
Reaffirming our vision and mission
The Canadian Lymphedema Framework remains steadfast in its dedication to our vision and mission:
Vision: comprehensive treatment for lymphedema and related disorders will be accessible to all persons across Canada.
Mission: To improve the management of lymphedema and related disorders in Canada through collaboration, innovation, and evidence-based practices.
medi Therapy Concept Lymphology
Effective lymphedema solutions for all stages of treatment.
Decongestion
•circaid reduction kit
Great reduction results during the decongestion phase.
Transition
• circaid juxtafit • circaid� profile (new)
Maintenance
• mediven flat knit
• circaid juxtafit
• circaid� profile (new)
Effective compression device throughout the transition phase. Compression devices for maintaining best therapy results.
The 15th anniversary of the Canadian Lymphedema Framework is not just a celebration of our past but a beacon lighting the way forward. Together we have achieved remarkable things and together we will continue to make a difference.
We continue to strive for a future where lymphedema is universally recognized, effectively treated, and no longer a silent burden.
Gratitude to our supporters
None of our accomplishments would be possible without the generous support of our readers, volunteers, sponsors, advertisers, exhibitors, and partner organizations. Your contributions, whether through financial support, advocacy, or collaboration, have been the lifeblood of our organization. We are deeply grateful for your unwavering support and commitment to our purpose.
Looking ahead: The 2025 International Lymphoedema Conference
As we celebrate our past achievements, we also look forward to the future with excitement and anticipation. The CLF is incredibly proud to co-host the 2025 International Lymphoedema Conference in Niagara Falls, Canada in October 2025. This event promises to be a landmark gathering of experts, practitioners, patients, and advocates from around the world, fostering knowledge exchange and collaboration on a global scale. We invite you to join us at this prestigious event, to share in the latest advancements in lymphedema research and treatment, and to contribute to the ongoing dialogue that shapes our field. To stay informed about the conference and other CLF activities, we encourage you to sign up for our eNews at tinyurl.com/CLFeNews.
Inspiring future leaders
We invite passionate and dedicated individuals to consider joining us to contribute to our mission. Whether as a conference attendee, a contributor to our Pathways magazine, a volunteer supporting our special projects and events, or by joining our staff or Board of Directors, your unique perspective and expertise can help drive forward our initiatives and ensure the continued success of the CLF.
In conclusion, the 15th anniversary of the Canadian Lymphedema Framework is not just a celebration of our past but a beacon lighting the way forward. Together we have achieved remarkable things and together we will continue to make a difference in the lives of those affected by lymphedema. By reflecting on our achievements and setting our sights on future goals, we reaffirm our commitment to the lymphedema community and continue to strive for a brighter, healthier future for all. With heartfelt gratitude, thank you for being part of this journey. Here’s to many more years of progress, innovation, and impact. LP
Humour and creativity
My lymphedema management strategies
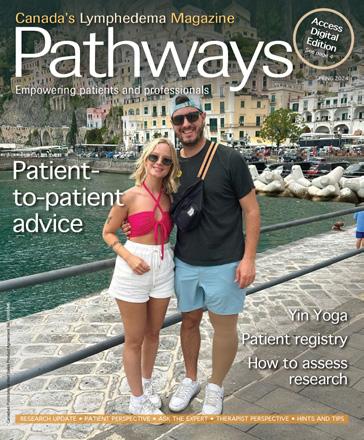
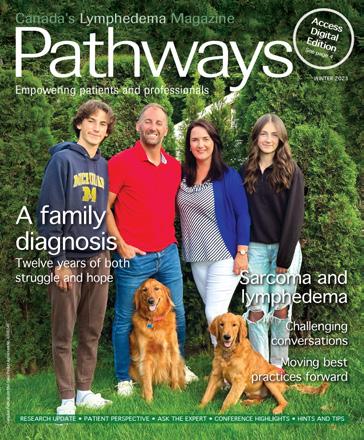
By Jill Edmondson
I was utterly dismayed when I suddenly developed secondary lymphedema in my left arm just after Christmas in 2017. I had a single mastectomy in October 2015. The breast cancer had migrated to the lymph nodes in my armpit; thus, a cluster of nodes was removed. Following the surgery, I slogged through a vigorous course of chemotherapy and radiation.
Through it all, a contingent of doctors, nurses, and other healthcare professionals warned me about lymphedema. I was educated about prevention strategies, knew the warning signs, and became aware of the risks it could present.
Accordingly, I was vigilant in my efforts to stave off lymphedema. I regularly did
preventative physiotherapy and decongestive massage. I kept the area clean and well moisturized. I avoided temperature extremes. I didn’t lean on my left arm. I slung my knapsack over my right shoulder. I wore loose clothing. I forfeited wearing bracelets, rings, and watches.
Nevertheless, lymphedema ambushed me 26 months after my mastectomy. Accepting that I had lymphedema was very difficult. I had done all the right things, and yet… After developing it, I learned as much as possible about managing and arresting lymphedema. I continued with physiotherapy and massage. I exercised regularly. I bought every type of compression garment in existence, including several that were custom-made. I also tried interferential current therapy, dry brushing, cold laser therapy, hyperbaric chamber, selenium, essential oils, vibration, compression wrapping, shock wave, hydrotherapy, pneumatic pump, K-tape, taro-diclofenac liquid, iLipo, and cupping. I’ve even had lymphaticovenous anastomosis (LVA) surgery – twice. Everything works… for five minutes. I can reduce the swelling, but almost instantly, the fluid starts building up again.
“There
is no healthier drug than creativity.”
- Nayyirah Waheed
Eventually, I decided to try a technique that helped me get through the worst days of cancer: comedy.
I have dabbled in stand-up comedy off and on for years. As the saying goes, laughter is the best medicine. But for me, it’s much more than that. Being able to laugh at something is a way of taking control. For instance, making jokes about my baldness during chemo was my way of saying: “Hey, cancer! You’re not the boss of me!” I decided to apply that mindset to lymphedema.
I’m not rich enough to afford daily massages, so I bought a portable massager for home use. It was somewhat helpful but awkward. I would try to hold the massager against the side of my upper arm or the back of my forearm.
Jill Edmondson is a “Jill of All Trades” in Toronto. She teaches law, fuses glass, and produces and performs stand-up and improv comedy. Jill is also the author of four mystery novels, including “Blood and Groom” and “Dead Light District.”
Comedy is not my only creative passion. I’m also an avid glass fuser, which is glass art formed in a kiln.
It was cumbersome, and I could never get consistent, appropriate pressure. I started thinking about the massager’s shape and size and wished I could find something long and narrow to strap onto my arm. Meanwhile, I was trying to develop a comedy routine about my lymphedema experience. And here’s how lymphedema and stand-up merged one night in front of a packed house at a pub in downtown Toronto:
n I bought two pink vibrators, pink because… run for the cure!
n First of all, what happened to good old-fashioned batteries? Modern vibrators have to be plugged in and charged. So, I save money on batteries, but spontaneity is killed. And what do I do if there’s a power failure?
n I keep the vibrators in the kitchen, not because a sink full of dirty dishes turns me on, but because that’s where there’s a plug I can reach.
n Convenient or not, it’s weird to see pink vibrators on my kitchen counter, right between the soda stream and the waffle iron.
n I get the vibrators all charged up and then light a few candles to set the mood.
n Then I Velcro the two vibrators onto my left arm to try and get the fluid moving.
n I listen to Barry White while my swollen arm tries to achieve sweet release.
n My left arm gets hot and tingly, while my right arm looks on with envy.
n After about an hour, my left arm is basking in the afterglow, while my right arm starts sulking.
n Then I take a shower and wonder what will happen decades from now when I die, and someone has to go through my stuff. When they find a vibrator in my kitchen, I hope they’ll think it’s a meat tenderizer, which, in a way, it is.
The crowd loved my set! They laughed the whole way through, particularly when I mimed strapping the vibrators onto my arm. That night was a victory for me: Jill-1, lymphedema-0.
Comedy is not my only creative passion. I’m also an avid glass fuser, which is glass art formed in a kiln. In my early days with lymphedema, I avoided glasswork. I was paranoid about cuts and the risk of infection. Then COVID came along, and everything shut down. When the post-pandemic world eventually started dawdling towards normalcy, I recognized that something was missing from my life.
In May of 2023, I decided to stop being afraid. By this time, I had been living with lymphedema for over five years. It was time to let lymphedema know who was in charge. I became a member at Glasstronomy Glass Studio in Markham, and I’ve been smiling ever since! I find true joy in the beauty of glass. I love the sound glass makes when I cut it. I love playing with textures. I love how the colours flow after being kilned.
As excited as I am to do glass fusing again, I’m not cavalier about lymphedema.
I engage my left hand as little as possible. I constantly check for scratches and nicks. I repeatedly wash my arm and hands. Additionally, I made a deliberate decision not to wear a sleeve the few hours a week that I’m at the studio. If a sliver of glass became embedded in my sleeve, that could be disastrous, especially since I might not even notice, given that lymphedema diminishes sensation in my left arm. But the compression garment goes back on when I put down my tools.
In the year since I re-embraced glass fusing, I’ve made almost one hundred pieces: bowls, vases, platters, sculptures, wall hangings, and jewellery. Every piece brings me pleasure, but also reminds me that even though glass is breakable, I am not. LP
Size matters
3M™ Coban™ 2 Two-Layer Compression System and 3M™ Coban™ 2 Lite Two-Layer Compression System
Coban 2 Compression System has advanced the science of compression therapy by designing materials engineered with Intelligent Compression Dynamics. These materials, which comprise the Coban 2 Compression System and Coban 2 Lite Compression System, create a conformable, inelastic sleeve that supports the patient’s muscle movements for e ective venous return and reduction of edema.
E ective compression Simple application
3M Health Care is now Solventum
At Solventum, we enable better, smarter, safer healthcare to improve lives. We’re a new company with a long legacy of creating breakthrough solutions for our customers’ toughest challenges. Because at Solventum, we never stop solving for you.
Coban 2 Lite Compression System does not have an extra long sizing option.
Hints and Tips
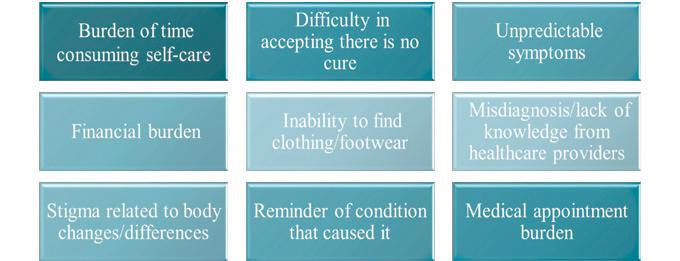
Taking charge: Being active
Being active and regular exercise is a key part of lymphedema self-care. By moving your muscles and breathing more deeply, you stimulate your lymphatic system and help your lymph flow. What it means to be active is varied and can include organized sporting activities, working out at a gym or in your home, a brisk walk with friends or running errands, running around with your children or grandchildren, or working in your house or garden. Exercise safely, ideally with the advice of your self-care team: your family doctor or nurse, lymphedema therapist and fitness specialist. Be aware that many fitness specialists or personal trainers are unfamiliar with lymphedema. You’ll need to educate them about the condition, what helps you and what you need to avoid.
Guidelines for exercise
4 Measure your affected area before starting a new activity and monitor it over time.
4 Wear a well-fitting compression garment while you exercise.
4 Start slowly, progressing at your own pace, build your strength and stamina slowly.
4 Make time for deep breathing, and water breaks to stay hydrated.
Types of activities
The key is finding activities that fit into your life and that you enjoy. Here are some safe exercises and ways to be active:
4 Pay attention to any signs of pain or discomfort during/after exercise and modify as needed.
4 Monitor for changes in swelling and keep a record of regular measurements.
4 Pool exercises like aqua fit, aqua lymphatic therapy, or just walking in water
4 Walking, gentle cycling, dancing and light aerobics
4 Gentle stretching and rest after any cardiovascular exercise or strength training
4 Yoga and Pilates; however, if you have upper body lymphedema, ask your instructor for alternatives to poses that require static weight-bearing of the arms (e.g. downward dog). LP
Source: Canadian Lymphedema Framework website: https://www.canadalymph.ca/taking-charge-of-your-health/
Did You Know?
Immediate
lymphatic reconstruction effective?
Background: Immediate lymphatic reconstruction (ILR) has been proposed to decrease lymphedema rates. The primary aim of our study was to determine whether ILR decreased the incidence of lymphedema in patients undergoing axillary lymph node dissection (ALND). Methods: We conducted a two-site pragmatic study of ALND with or without ILR, employing surgeon-level cohort assignment, based on breast surgeons’ preferred standard practice. Lymphedema was assessed by limb volume measurements, patient self-reporting, provider documentation, and International Classification of Diseases, Tenth Revision (ICD-10) codes. Results: Overall, 230 patients with breast cancer were enrolled; on an intention-to-treat basis, 99 underwent ALND and 131 underwent ALND with ILR. Of the 131 patients preoperatively planned for ILR, 115 (87.8%) underwent ILR; 72 (62.6%) were performed by one breast surgical oncologist and 43 (37.4%) by fellowship-trained microvascular plastic surgeons. ILR was associated with an increased risk of lymphedema when defined as ≥10% limb volume change on univariable analysis, but not on multivariable analysis, after propensity score adjustment. We did not find a statistically significant difference in limb volume measurements between the two cohorts when including subclinical lymphedema (≥5% inter-limb volume change), nor did we see a difference in grade between the two cohorts on an intent-to-treat or treatment received basis. For all patients, considering ascertainment strategies of patient self-reporting, provider documentation, and ICD-10 codes, as a single binary outcome measure, there was no significant difference in lymphedema rates between those undergoing ILR or not. Conclusion: We found no significant difference in lymphedema rates between patients undergoing ALND with or without ILR.
Source: Lymphedema Rates Following Axillary Lymph Node Dissection With and Without Immediate Lymphatic Reconstruction: A Prospective Trial. Ann Surg Oncol. 2024 Jul 2: 10.1245.
Minimum three-year follow-up post-surgery
Background: The PREVENT randomized control trial monitored progression to chronic breast cancer-related lymphedema (cBCRL) following intervention for subclinical breast cancer-related lymphedema (sBCRL) assessed by bioimpedance spectroscopy (BIS) versus tape-measure (TM). This multi-institutional
trial demonstrated a 92% risk reduction of developing cBCRL. This secondary analysis reviews the timing of sBCRL and cBCRL following breast cancer (BC) treatment. Patients and Methods: Women at risk of cBCRL (n = 919) were screened regularly up to 36 months after BC treatment using either BIS or TM. Following diagnosis of sBCRL, patients underwent a 4-week compression sleeve intervention. The time in months from BC treatment to detection was reviewed at 3-month intervals. Results: In total 209 patients developed sBCRL (BIS: n = 89, TM: n = 120) and were eligible for intervention. 30 progressed to cBCRL postintervention (BIS: 7, TM: 23).
More than half of patients had measurements consistent with sBCRL within 9 months of BC treatment. Patients continued to have initial detections of sBCRL, regardless of screening method, with rates remaining consistent in years two and three (p > 0.242) postsurgery. Additionally, 39 patients progressed to cBCRL without developing sBCRL or receiving intervention across the 3-year period. Conclusions: The timing of sBCRL detection demonstrates that patients continue to be at risk years after treatment and may continue to progress to cBCRL years after surgery. Early detection of sBCRL allows for early intervention decreasing the likelihood of decreasing the likelihood of progression to cBCRL. Patients should continue to be monitored for a minimum of 3 years following completion of cancer treatment. Specifically, careful targeted monitoring over the initial 9-month period is important.
Source: Timing of Breast Cancer Related Lymphedema Development Over 3 Years: Observations from a Large, Prospective Randomized Screening Trial Comparing Bioimpedance Spectroscopy (BIS) Versus Tape Measure. Ann Surg Oncol. 2024 Jul 4. :10.1245.
Assessing measurement tools
Purpose: To investigate reliability, concurrent validity, and clinical feasibility of measurements assessing volume in patients with lower limb lymphedema (LLL) and healthy controls.
Materials and Methods: To investigate intra- and interrater reliability, 47 patients with LLL and 30 healthy controls were assessed three times by two assessors. To investigate between session reliability, 50 participants were reassessed two weeks later. Each assessment included measurements of the midline region (hip circumference; suprapubic volume), leg volume (perimeter every 4 cm; Perometer®), and foot volume (water displacement; figure-of-eight method). Concurrent validity was assessed with correlation coefficients. Measurements
were timed and practical limitations were reviewed. Clinical trial registration number: NCT: 05269264. Results: Measurements of the total volume of different regions showed weak to very high intraclass correlation coefficients (ICCs) (0.131-998). Absolute and relative volume differences had lower ICC values (0.360-0.976). A strong correlation was found between the total volumes of the same region. The Perometer® and figure-of-eight method were the fastest method for leg and foot volume, respectively. Conclusions: The assessed total volumes might be more valuable in assessing the evolution of volume in bilateral LLL than the calculated absolute and relative differences between both limbs. The Perometer® and figure-of-eight method were the most time efficient for leg and foot volume, respectively. Implications for rehabilitation. Lymphedema is a chronic condition for which a reliable and clinically feasible assessment of volume is essential for the diagnosis, treatment decisions, and the evaluation of the treatment. This study shows that the total leg/foot volumes were more reliable than the calculated absolute and relative differences between both limbs and could therefore more valuable to evaluate bilateral lower limb lymphedema. For the assessment of leg volume, the Perometer® was the most reliable and fastest method. For the evaluation of the foot volume, the figure-of-eight method was overall the best method.
Source: Reliability, concurrent validity, and clinical feasibility of measurement methods determining volume in patients with lower limb lymphedema and healthy controls. Disabil Rehabil. 2024 Jul 8:1-15. :10.1080/09638288.2024.2374482.
Source: Demonstrating the benefit of a cellulitis-specific patient reported outcome measure (CELLUPROM()) as part of the National Cellulitis Improvement Programme in Wales. J Patient Rep Outcomes. 2024 Jul 10. :10.1186.
YouTube BCRL exercises
This descriptive study aimed to determine the content, quality, and reliability of YouTube videos on breast cancer-related lymphedema exercises. A total of 127 videos were independently assessed, with 103 of them categorized as either informative or misleading content groups. The content (mean score: 4.07 ± 2.29) and quality (mean score: 3.15 ±
1.46) of videos concerning lymphedema exercises were moderate, while reliability (mean score: 2.27 ± 1.64) was low. Among the 103 videos categorized using the content checklist, Global Quality Scale, and DISCERN reliability instrument, 57.3% (n = 59) were informative, and 42.7% (n = 44) had misleading information. The mean scores of the content, quality, and reliability of the informative content videos were substantially higher than the misleading content videos, and of videos uploaded by universities/professional organizations/health care professionals/ medical advertisements were higher than the videos uploaded by other sources. Through this study, the researchers have unveiled that the content and quality levels of YouTube videos in lymphedema exercises were moderate, and the reliability level was low.
Source: YouTube as a source of information on breast cancer-related lymphedema exercises: A content, quality and reliability analysis Health Care Women Int. 2024 Jun 27.-15:10.1080/07399332.2024.2368499.
Skin barrier dysfunction in lymphedema
Breast cancer-related lymphedema (BCRL) is characterized by skin changes, swelling, fibrosis, and recurrent skin infections. Clinical studies have suggested that lymphedema results in skin barrier
defects; however, the underlying cellular mechanisms and the effects of bacterial contamination on skin barrier function remain unknown. In matched biopsies from patients with unilateral BCRL, we observed decreased expression of filaggrin and the tight junction protein zona occludens-1 (ZO-1) in skin affected by moderate lymphedema, or by subclinical lymphedema in which dermal backflow of lymph was identified by indocyanine green lymphography, relative to controls (areas without backflow and from the unaffected arm). In vitro stimulation of keratinocytes with lymph fluid obtained from patients undergoing lymphedema surgery led to the same changes, as well as increased expression of keratin 14, a marker of immature keratinocytes. Finally, using mouse models of lymphedema, we showed that like the clinical scenario, the expression of skin barrier proteins was decreased relative to normal skin and that colonization with S. epidermidis bacteria amplified this effect, as well as lymphedema severity. Taken together, our findings suggest that lymphatic fluid stasis contributes to skin barrier dysfunction in lymphedema.
Complete Lymphedema Certification
135-hour certification training in the management of lymphedema Hybrid option
Advanced Lymphedema Management Expand your skill set in the management of lymphedema
Lymphedema Management Seminar Introduction to the management of upper & lower extremity lymphedema
Manual Lymph Drainage Certification 40-hour certification training in the management of edema; as well as other indicated conditions Hybrid option
Oncology Considerations for Manual Lymph Drainage
Safely use MLD when working on those with cancer or history of cancer treatments
A hybrid course
Advanced MLD: Post Plastic Surgery Procedures
Sequences & protocols specific to plastic surgery & contraindications Hybrid option
Online
Work at your own pace in an array of topics
Source: Breast cancer-related lymphedema results in impaired epidermal differentiation and tight junction dysfunction. J Invest Dermatol. 2024 Jun.
Canadian and International Events
Sep 14-15, 2024 2024 National Lymphedema Network Conference
VIRTUAL Evolving Lymphatic Concepts (Part 1). n https://lymphnet.org/
Oct 5-6, 2024 2024 National Lymphedema Kansas City, MO Network Conference
Evolving Lymphatic Concepts (Part 2). n https://lymphnet.org/
Oct 10-13, 2024 American Vein & Lymphatic Society’s Chicago, IL 38th Annual Congress n Register at www.myavls.org
Oct 17-19, 2024 Wounds Canada National Hybrid Conference London, ON n Learn more at: https://lymphnet.org/
Apr 12-15, 2025 POWER Lymphatics 2025 Denver, CO n https://thepowersymposium.com/power-lymphatics/
Oct 23-25, 2025 12th International Niagara Falls, CAN Lymphoedema Conference
Building Bridges: Connecting Global Perspectives International Lymphoedema Framework, with Canadian Lymphedema Framework and International Lipoedema Association. n Register: www.lympho.org
Congratulations on the 50th issue of Pathways - hands down the best lymphedema magazine in the world!
Guenter Klose, Klose Training Lafayette, Colorado
I was wondering if I could get a PDF of the Lymphedema Research Update from the Fall 2023 Pathways written by Dr Spencer Gibson. I’d like to use it in my MLD classes to show how far-reaching the lymphatic system is. Thanks.
Sandra MacDonald Halifax, Nova Scotia Letters to the
Discover ProLymph SCAN TO LEARN MORE
Canadian Lymphedema Framework (CLF) wishes to thank these partners for their support in making this magazine a reality.
CRAFTED FOR CONFIDENCE
At JOBST, we want to help your patients with lipedema or lymphedema find their inner confidence. We’ve added new design features to JOBST Confidence, so your patients can benefit from more comfort and style. With these new design features, you can help your patients manage their condition and inspire them to feel good about themselves, giving them the confidence to live life to the fullest.
New colours Comfort waistband Decorative seams Motivational prints