
Empowering patients and professionals

Empowering patients and professionals

What I enjoy most about conferences is the opportunity to network with the vibrant lymphedema community, reconnecting with old friends and colleagues, and meeting new people who share a common purpose. For example, when I listened to Ad Hendrickx from the Netherlands present at the 2025 International Lymphoedema Conference, his approach to personalized patient care closely aligned with our shared aims. I knew it would make a valuable article for Pathways readers. Each person’s experience of their health issues is subjective and unique. This influences how patients participate in their treatment and care, emphasizing the value of self-management.
self-lymphatic massage when needed, the new recommendations also emphasize the benefits of exercise, movement, and mobility, as well as maintaining overall health.
This new model aligns well with the published paper on the Essential components of the maintenance phase of decongestive therapy. In an interview with Margie McNeely (the lead author of this published paper), she relayed that one of the guiding principles of establishing this new consensus document was to empower individuals to self-manage their lymphedema. In addition to selfmanagement strategies, which may include
Lymphedema care often reveals a disconnect between clinical understanding and the day-to-day reality of living with lymphedema. Moving toward individualized and patient-led care, reinforces the need for collaboration between health professionals and their patients. A patient-centred workshop at last fall’s conference and facilitated by Juliana Conte, Lori Radke, and Catharine Bowman, intentionally positioned patients and professionals as equal partners to share their experiences and help bridge the gap between research, care and patient experiences.
So, how do we continue to build the future of lymphedema care and ensure that new clinicians, therapists, and researchers have the benefit of the acquired wisdom of the experienced members of our community? Mentorship is vital. It shapes careers, strengthens teamwork, and builds collaboration. The International Lymphoedema Framework, Canadian Lymphedema Framework, and other community organizations help to connect us. Margie McNeely, Anna Towers, and Jane Armer reflect on
Each
person’s experience of their health issues is subjective and unique. This influences how patients participate in their treatment and care, emphasizing the value of self-management.
the mentorship workshop that was held at the 2025 conference and share tips for both mentors and mentees.
To share more highlights from the 2025 International Lymphedema Conference, we expanded the “Did You Know” section with condensed abstracts from our conference presenters. We encourage you to click on the links to read the unabridged versions. With the 2025 conference now behind us, plans are already underway for an even more impactful biennial event in 2027. Bonnie Baker gives us a sneak peek at what to expect, encouraging us all to stay engaged and continue shaping the future of lymphedema care together. LP

Anna Kennedy
Spring 2026 n Volume 15 Issue 2
Publisher
Pathways is published four times per year by BCS Communications Ltd. on behalf of the Canadian Lymphedema Framework.

Editorial Board
Mei Fu PhD RN FAAN
David Keast MD FCFP
Lori Radke PT CLT
Margie McNeely PhD PT Anna Towers MD FCFP
Editor-in-Chief Anna Kennedy
Executive Director Bonnie Baker
Marketing Manager Grace Neumayer
Advertising and Submissions
We welcome your ideas, contributions, letters and ad copy. While all material is subject to Editorial Board approval, inclusion does not constitute an endorsement or reflection of the views and opinions of the CLF and its Editorial Board. Contents may not be reproduced without written permission of the Canadian Lymphedema Framework.
Subscription Rates (1 year)
Canada - $30. United States - $60. International - $75. Single copies and back issues - $8.
Subscriptions/return mail to Canadian Lymphedema Framework / Partenariat Canadien du lymphoedème PO Box 35062 RPO Hartzel St. Catharines ON L2P 0C5 Telephone: 647-693-1083
Email: pathways@canadalymph.ca www.canadalymph.ca
Photo credits: Canva. Wimpiecomics.nl. Dissolve Stock Photos. Fin Dunford (Adelaide Hills Courier).
Canadian Publications Mail Agreement 40065546
ISSN 1929-1418 (Print) • Printed in Canada ISSN 2818-5714 (Online)
We acknowledge the financial support of the Government of Canada.
Personalized care for patients with lymphedema
Questions that can make a difference.
........................................
Essential maintenance phase of decongestive therapy
An interview with Margie McNeely. Fifth in a series of transcribed interviews from the LANA/ACS Summit. .......................................................................

Building bridges between science and lived experience
How patient voices can shape global priorities in lymphedema care and research. ...........................................
Lymphedema Advocacy
Shaping the future of lymphedema care in Canada. Your voice can help. ...........................................
Moving forward together

Building the future through mentorship and collaboration.
.......................................................................
Keeping the train on track
An illustrated overview of the lymphatic system. .......................................................................










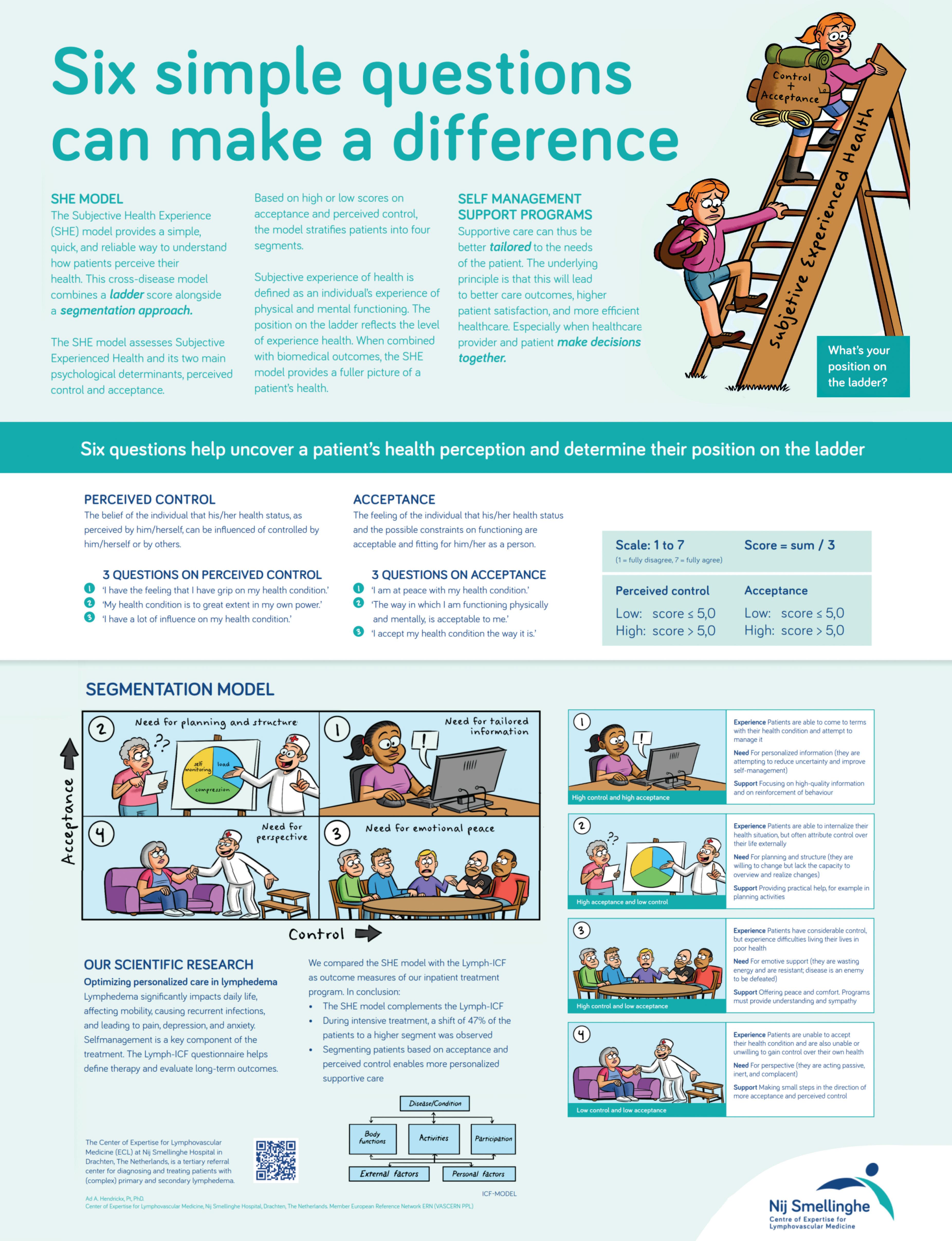
Six simple questions can make a difference.
By Ad Hendrickx and Janine Dickinson-Blok
(LE) is a chronic, progressive, and often debilitating condition that remains a neglected global healthcare problem, despite its significant impact on patients’ lives. Patients with LE often experience severe problems in daily life, caused not only by swelling or heaviness of the affected region, but also by reduced mobility, recurrent infections, and associated complaints such as pain, depression, and anxiety. In many cases, LE has a profound impact on patients’ quality of life.
There is no cure for LE, and its management aims to minimize and stabilize edema and to enhance both physical and mental functioning, thereby improving overall quality of life. The therapeutic approach encompasses various components, such as compression therapy, exercise therapy, skincare, and lifestyle interventions. Integral to therapeutic interventions focused on improving the clinical aspects of LE, an important part of treatment is dedicated to self-management. This involves providing patients with the knowledge and skills necessary to optimize their ability to manage their health status.
However, research shows that many patients experience difficulties in achieving optimal self-management, and adequate support from


healthcare providers is needed. In addition, there is limited knowledge about which patients benefit from which type of support, resulting in negative consequences for patient outcomes and healthcare costs. Alongside these findings, an increasing prevalence of unhealthy lifestyles is observed, often combined with denial of the need to change and an inability to change. In most cases, lifestyle-related issues involve obesity and insufficient daily physical activity.
How can supportive care be better aligned with what people actually need?
When allocating support and care, it is essential to consider how people experience their health. If care aligns with an individual’s perceptions, wishes, and needs, it is more effective and leads to greater satisfaction. The quality of diagnosis and treatment planning improves, as does individuals’ involvement in their own health. In practice, however, there is often insufficient differentiation in the supportive care provided. Despite everyone’s best efforts, supportive care is frequently based on a standard approach, or a “one size fits all” model. This needs improvement—but how can this be achieved?
Ad Hendrickx, PT, PhD works as program manager of research & development in the Dutch Center of Expertise for Lymphovascular Medicine at Nij Smellinghe Hospital in Drachten, The Netherlands. During his career as a physical therapist, he specialized in lymph- and lipedema.
Janine L. Dickinson-Blok, MD PhD is a general dermatologist with expertise in the diagnosis and treatment of lymphedema. She works at the Dutch Center of Expertise for Lymphovascular Medicine at Nij Smellinghe Hospital (Drachten, The Netherlands) and Meander Hospital (Amersfoort, The Netherlands).
The Subjective Health Experience model (SHE model), developed by Bloem and Stalpers, provides a tool for allocating supportive care in a more personalized way. To determine which form of support is most appropriate for an individual, the individual’s experience of health must be the point of departure. In this model, health experience is the central theme within a clear, evidencebased, cross-disease framework that places experienced health at the center of care. The model is grounded in the idea that not only medical diagnoses, but especially how people experience their health, influences behavior, self-management, and the need for support.
Subjective Health Experience is defined as an individual’s experience of physical and mental functioning while living life in the way they want to, within the actual constraints and limitations of their existence. To make this experience visible and measurable, Bloem and Stalpers use a visual analogue scale (VAS 0–10), presented as a ladder. The lowest step represents the individual’s worst day in the past month (0), and the highest step represents the best day in the past month (10). Individuals are asked to indicate on which step they feel they stand today, and on which step they stood on average during the past month.
The ladder metaphor intuitively reflects changes in health experience over time. When individuals perceive themselves as functioning better, both physically and mentally, they place themselves higher on the ladder; when functioning is perceived as worse, a lower position is chosen. This approach creates a personal frame of reference and allows for meaningful discussions between healthcare
A
Disease Acceptance
• I am at peace with my health condition.
• The way I am functioning physically and mentally is acceptable to me.
• I accept my health condition the way it is.
Perceived Control
• I have the feeling that I have a grip on my health condition.
• My health condition is to great extent in my own power.
• I have a lot of influence on my health condition.
professionals, patients, and their supportive network about the most appropriate supportive care. The central question becomes: “What do you need to move higher up the ladder?”
Acceptance and perceived control: two key factors Research shows that two psychological factors are particularly important in determining where someone places themselves on the ladder: acceptance and perceived control. Acceptance refers to the extent to which a
person has been able to give their condition a place in their life. Perceived control reflects the degree to which someone feels able to influence their health and daily functioning. Acceptance is officially defined as “the feeling by the individual that their health condition and the possible constraints on functioning resulting from it are acceptable and fitting for them as a person.” Perceived control is defined as “the belief of the individual that his or her health condition can, in the individual’s perception, be influenced


or controlled by themselves or by others.”
The SHE-model makes these factors measurable using a short set of questions and translates them into a practical segmentation framework. Based on high or low levels of acceptance and perceived control, four profiles are identified, each requiring a different type of support.
From model to practice: six simple questions that can make a difference Levels of acceptance and perceived control are assessed using three questions for each construct (Figure A), rated on a 7-point Likert scale (1 = fully disagree, 7 = fully agree). Mean scores are calculated by summing the three question scores and dividing the total by three; these mean scores are then used for segmentation. High acceptance and perceived control are defined as a mean score greater than 5. Based on these determinants, patients are divided into four segments (Figure B). To make the SHE-model easily accessible in everyday practice, our organization developed a visual poster using plain language (B1 level)






Segment II
High acceptance
Low perceived control
Segment IV
Low acceptance
Low perceived control
Segment I
High acceptance
High perceived control
Segment III
Low acceptance
High perceived control
and supportive illustrations (Figure C on page 7). The core of the poster is formed by the six simple questions and the ladder. Together, they can make a meaningful difference in how care is tailored. The strength of this approach lies in its simplicity. The questions invite reflection and conversation and help make abstract concepts such as acceptance and perceived control understandable and meaningful for patients dealing with lymphedema or lipedema.
Four profiles, four types of support Based on high or low scores for acceptance and perceived control, individuals can be grouped into four segments. Patients in Segment I (high acceptance, high perceived control) seek to improve self-management skills and reduce uncertainty; professional support should focus on high-quality information and reinforcement of effective behavior. Patients in Segment II (high acceptance, low perceived control) are willing to change but lack the capacity to organize and implement plans; support should focus on practical assistance such as planning and structuring activities. Patients in Segment III (low acceptance, high perceived control) often waste energy by resisting the condition and viewing it as an enemy to be defeated. Support for this group should focus on understanding and empathy, complemented by peer support. Finally, patients in Segment IV (low acceptance, low perceived control) benefit most from gaining perspective and taking small steps toward increased acceptance and
control. The publication by Bloem et al. (2020) provides a comprehensive overview of these profiles, corresponding support strategies, and their theoretical foundations.
An important strength of the SHE model is that it is cross-disease. It is not tied to a specific diagnosis and can be applied across a wide range of chronic conditions, including lymphedema and lipedema. Because the model starts from the individual’s subjective experience of health rather than from disease, it is broadly applicable and suitable for personalized supportive care.
The use of the SHE-model aligns closely with the new concept of health as formulated by Machteld Huber. In this vision, health is no longer defined primarily as the absence of disease, which dominated earlier definitions, but as the ability to function, adapt, and self-manage in the presence of physical, emotional, and social challenges. This perspective resonates strongly with the SHE model’s focus on experienced health and daily functioning.
The SHE model does not replace the biomedical model; rather, it complements it. While biomedical care focuses on disease mechanisms, diagnosis, and treatment, the SHE-model focuses on how individuals experience their health and manage everyday life. Together, these perspectives provide a more comprehensive understanding of health.
For people living with lymphedema, a condition requiring lifelong management, this combined approach is particularly valuable. Medical treatment remains essential, but the success of care is strongly influenced by how well support aligns with acceptance, perceived control, and personal context. While segmentation inevitably simplifies a complex reality, the SHE model is not intended to label individuals or prescribe fixed solutions. Instead, it serves as a guide to support a meaningful conversation.
The real value of the SHE-model lies in its ability to structure dialogue and support the process of Shared Decision-Making. By making acceptance, perceived control, and health experience visible using simple language, it creates a common starting point for discussion. The conversation tool used in our center supports this process by helping patients and healthcare professionals explore together where someone stands and what type of support may be helpful at a given moment. Finally, it is important to recognize that these constructs can change over time; therefore, repeated measurements are necessary.
The real value of the SHE-model lies in its ability to structure dialogue and support the process of Shared Decision-Making.
The SHE-model demonstrates that personalized care does not have to be complex. Six simple questions combined with a ladder score provide a powerful way to better align support with individual needs. In a time of increasing care demands and limited resources, this approach helps make care more human, more effective, and more sustainable. LP
Jan-Willem Spakman for his illustrations (website: wimpiecomics.nl) and Ellen de Jong, Communications and Marketing Manager of our institute, for her contributions to the poster. Professor Dr. Sjaak Bloem (Nyenrode Business University in The Netherlands) has been of great support during the introduction of the SHE mode and one of the developers of the model.
References can be found at https://www.canadalymph.ca/pathways/ all-issues/
How to cite: Hendrickx A, Dickinson-Blok J. Personalized care for patients with lymphedema. Six simple questions can make a difference. Pathways. 2026;15(2): 5-8. https://doi.org/10.70472/QCAF1202
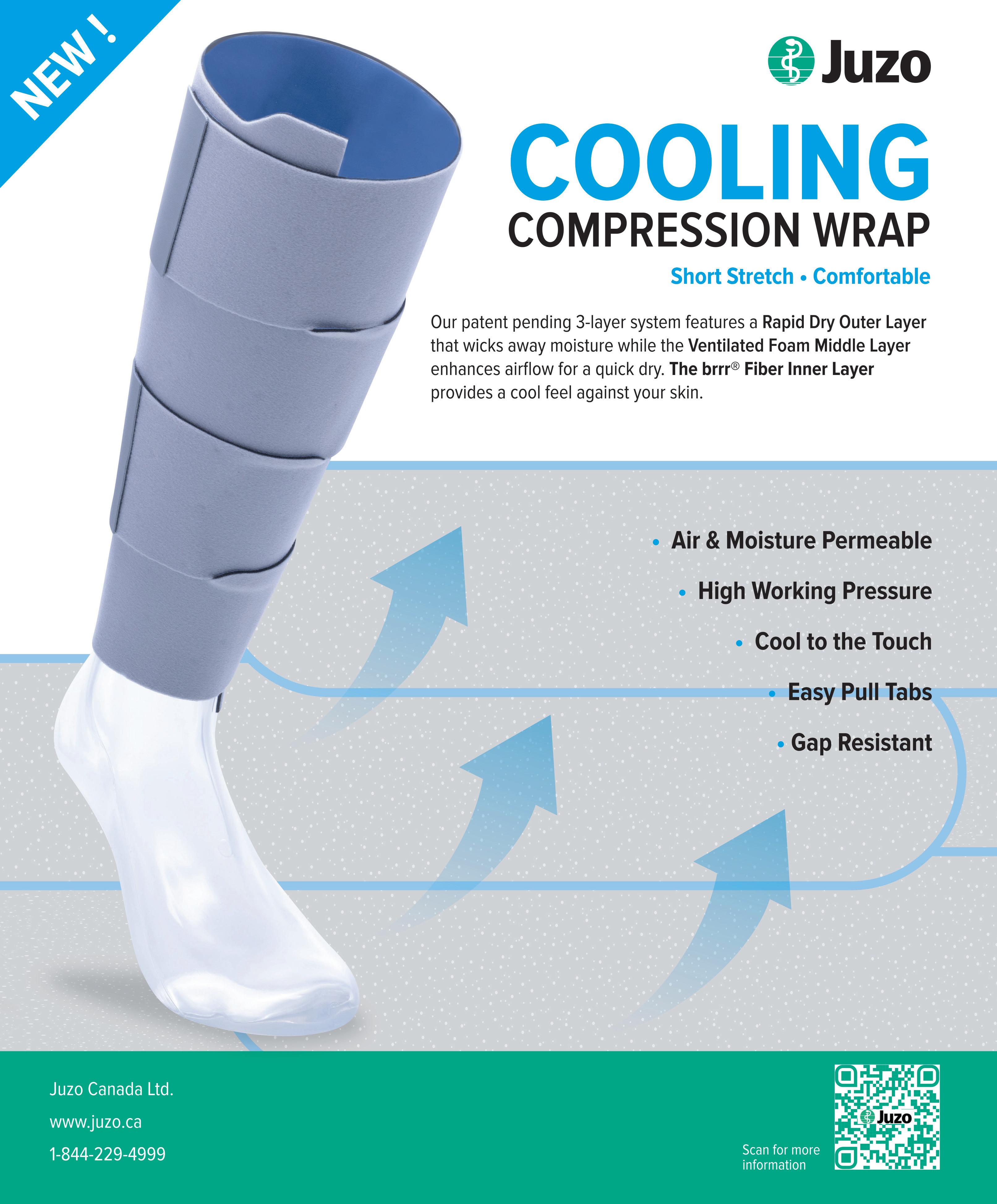
Product features
• Comfortable feeling in the sensitive back of the knee
• Seamless sitting and walking surface
• Ideal for high activity levels
• Sporty look with proven medical effectiveness

An interview with Margie McNeely
• Options for self-management to inform shared decision-making
• Signs and symptoms of cellulitis
• Identification of, and mitigation strategies to address barriers to self-management
• Counseling to support healthy lifestyle behaviors
• Assessment of limb volume and body weight
• Evaluation of garment wear and fit
• Review of selfmanagement plan
• Further reduction treatment as needed
• Management of cellulitis and other lymphedema complications
This is the fifth in a series of transcribed interviews highlighting the published body of work resulting from the LANA/ACS Summit. By highlighting these research papers and consensus statements, we hope to promote the concepts and facilitate moving them into daily practice. Readers are encouraged to access the reference links at the end of the article to read the research papers and some supporting evidence in their entirety.
AK - Were any of the six recommendations your group came up with more difficult to reach consensus on among the working group members? How was the group able to overcome those challenges?
MM - The working group process was very collegial, and, for me, it was a very positive experience coming out of the Summit. There was strong agreement on the essential components of maintenance-phase care from the outset, so we did not have any difficulty reaching consensus. Most of our discussion focused not on what should be included, but on how best to describe the recommendations in a way that stayed true to our three guiding principles— that best care is interdisciplinary, tailored to individual needs, and focused on empowering the individual to self-manage their lymphedema. The process itself was very collaborative.


• Skin and nail care
• Compression garment application and care
• Self-lymphatic massage
• Decongestive exercise
• As needed: selfapplication multicomponent compression bandaging/ night-time garment
• Day-time compression garments:
3 sets per affected body part every
6 months
• Night-time compression garments:
2 garments per affected body part every 2 years
• Compression bandaging systems and supplies
• Gradient compression wraps with adjustable straps
• Necessary accessories for gradient compression garments and wraps, including: aids for donning and doffing items, fillers, lining, padding, zippers
The working group included people from different care settings and with different scopes of practice, so everyone brought a unique perspective to the discussion. The different viewpoints really strengthened the recommendations and helped ensure they were relevant to clinical practice. As a group, we would draft sections, come together to review them, discuss and debate the wording, and then revise the recommendations based on those discussions. It was exciting to see the recommendations evolve, become clearer and more fine-tuned over time. We were mindful that wording matters. We wanted the recommendations to also align with the U.S. Lymphedema Treatment Act, so that they reflect current policy and help support access to appropriate coverage for people living with lymphedema. Considering an insurance and coverage lens, we had to be careful though not to be overly prescriptive
in how the recommendations were written. For example, we avoided setting exact time frames and treatment schedules as we know that lymphedema management needs can be different from person to person and may change over time. Some individuals need more support at certain points, while others need less. One thing I learned through this process is that recommendations can be interpreted very narrowly, with insurance funding aligned to the exact prescription rather than to individual needs. Keeping the wording flexible was important to ensure the recommendations reflect real-world care and can be applied across different healthcare systems and coverage models.
AK - What is the evidence for your group’s recommendation to include nighttime compression as well as daytime compression for effectiveness?
Margaret (Margie) McNeely is a Professor in the Departments of Physical Therapy and Oncology at the University of Alberta, in a jointly funded position with Cancer Care Alberta. She is the Director of the Cancer Rehabilitation Research Clinic at the University of Alberta. Anna Kennedy is a founding member of the Canadian Lymphedema Framework and Editor-in-Chief of the Pathways magazine. In 2012 she was awarded the Queen Elizabeth Diamond Jubilee Medal.
MM - We know that compression remains the foundation of the lymphedema maintenance phase, but the amount and type of compression needed can vary across individuals. For many, daytime compression alone is enough to keep the swelling stable. However, others may find that swelling returns overnight or that their lymphedema is difficult to control despite consistent daytime garment use.
In these situations, night-time compression may be needed to help stabilize lymphedema and prevent symptom relapse. This can include the use of night-time garments or short-stretch bandaging. The recommendation is not meant to suggest that everyone needs nighttime compression, but rather that it is an option to consider when daytime compression alone is not sufficient. I think it is important to mention that ongoing reassessment is key, allowing compression strategies to be adjusted over time based on symptoms, comfort, function, and the person’s ability to manage their own care.

L y m p h A c t i v a t i o n
Most of our discussion focused not on what should be included, but on how best to describe the recommendations in a way that stayed true to our three guiding principles— that best care is interdisciplinary, tailored to individual needs, and focused on empowering the individual to self-manage their lymphedema.
AK - The only recommendation for manual lymphatic drainage in the maintenance phase is self-lymphatic


In the maintenance phase, we felt it was important to shift away from routine, therapist-applied manual lymphatic drainage (MLD) and toward self-management strategies, which may include self-lymphatic
practical realities of long-term management.

( M L A ) C o u r s e
G o l d s t a n d a r d f o r

While therapist-applied MLD may be beneficial for some individuals in the maintenance phase, it can be time-intensive, costly, and difficult to access on an ongoing basis, particularly over the long term. For this reason, the recommendations place greater emphasis on exercise and regular movement, which have stronger and broader benefits for managing lymphedema symptoms, maintaining strength and mobility, and supporting overall health. Exercise is also easier to incorporate into daily life and sustain over time. Self-lymphatic massage or self-bandaging may still be useful tools for

e d e m a m a n a g e m e n t
G o l d s t a n a r o r e d e m a m a n a g e m e n t
L A N A R e v i e w e d & e x a m p r e - q u a l i f i e d
L A N A R e i e e d & e x a m p r e - q u a i f i e d
B l e n d e d L e a r n i n g : O n l i n e T h e o r y + I n P e r s o
I n c l u d e s C o m p r e s s i o n , Ta p i n g & M a n u a l Te c h n i q u e s I c u d e s C o r e s s o n , Ta p i n g & M a n l Te c h n i q u e s


some individuals, particularly when the swelling flares or symptoms change.
AK - What recommendations do you have to help transition this knowledge into everyday practice?
MM - Moving recommendations into everyday care requires practical, easy-to-use knowledge tools. There is a real opportunity for clinicians, researchers, and advocacy groups to develop clear written and electronic resources that explain lymphedema maintenance care in plain language that can be used consistently by patients, caregivers, and healthcare providers. Importantly, we know that these tools can also support advocacy, especially given the variation in services and coverage across provinces. Patient-friendly summaries, checklists, and short evidence-based documents may be helpful to explain what resources are needed for effective lymphedema care such as access to compression garments, supplies, education, and follow-up care. I think that having consistent, evidence-
informed materials strengthens conversations with healthcare teams, administrators, and policymakers, and can help support more equitable access to lymphedema care.
AK - Is there anything you would like to leave readers with?
MM - One of the most important messages I want to leave with readers is that our working group felt strongly that lymphedema is best managed with the support of a knowledgeable and supportive interdisciplinary lymphedema care team. At the same time, we know that access to specialized lymphedema expertise is lacking for many individuals across Canada, which can make long-term management more challenging. This is where establishing lymphedema networks of excellence can play an important role. Networks bring together clinical expertise, education, research, and referral pathways, and help guide individuals and providers toward appropriate care. One example in Canada is the LE&RN Network of Excellence Centre at
the McGill University Health Centre in Montreal, led by Dr. Anna Towers, which integrates care, education, and research to support people living with lymphedema. We need more of these centres of excellence in Canada.
I also hope that these maintenance recommendations help guide conversations, support advocacy, and improve care over time. I think that when people with lymphedema have the right support and access to shared knowledge, they feel more confident in performing selfmanagement and are more successful in controlling their lymphedema long term. LP
Essential components of the maintenance phase of decongestive therapy. Margaret L. McNeely, Mona M. Al Onazi, Mike Bond, Andrea Brennan, Heather Ferguson, Deborah A. Gross, Fedor Lurie, Linda Menzies, Steven Norton, Yuanlu Sun, Alaina Newell. Medical Oncology (2024) 41:289 https:// doi.org/10.1007/s12032-024-02442-1. https://link.springer.com/article/10.1007/ s12032-024-02442-1.






























By Juliana Conte, Lori Radke and Catharine Bowman
At the 2025 International Lymphoedema Framework Conference, delegates gathered not only to exchange knowledge, but to build meaningful and lasting connections. The conference theme—Building Bridges: Connecting Global Perspectives—was brought to life through a featured patient-centred workshop that intentionally positioned patients and professionals as equal partners.
The session created space for patients to share lived experience and collective wisdom, offering insight that cannot be captured through clinical data alone. While many people living with lymphedema feel unheard or marginalized within healthcare systems, those in attendance spoke openly about unmet needs, systemic gaps, and emerging priorities. Their contributions illuminated where current models fall short—and how meaningful, patient-informed progress can be made.
The roundtable was collaboratively facilitated by members of the lymphedema community, including a researcher, a clinician, and a patient-advocate-researcher. Areas of uncertainty related to lymphedema care and research were gathered in advance and used to formulate discussion questions. Following the session, notes generated from roundtable discussions were reviewed to develop a patient-informed prioritization list intended to support future care development, education, and research initiatives. What follows is a glimpse into what happens

when patients are handed the microphone—and discussion is centered on their perspectives.
Why this workshop mattered
Living with lymphedema often reveals a persistent gap between clinical understanding and day-to-day reality. This workshop was designed to bridge that gap by creating a safe, inclusive environment where patients and professionals could engage in honest, meaningful dialogue. The primary objective was to identify gaps in current care and research through patient-defined priorities. By centering lived experience as a form of expertise, the session reinforced the value of collaboration in shaping systems that genuinely meet patient needs and reflect the realities of living with a chronic lymphatic condition.
design
The session followed the World Caf é methodology (https://theworldcafe.com), a structured conversational approach developed to foster meaningful dialogue through shared etiquette and guiding principles.1 Participants were divided into four tables and rotated through six predetermined questions. Key points were documented on poster-sized notes displayed beneath corresponding domain labels on the wall of the room. All contributions were kept anonymous. Three tables were composed of patient experts, while one table consisted of lymphedema therapists and garment fitters.

Their presence added valuable clinical and practical perspective, reinforcing the importance of multidisciplinary collaboration.
Two disclaimers were shared at the outset:
1 Recommendations that could be harmful or contraindicated would not be included
2 Participants were told to consult healthcare providers before adopting any strategies discussed.
Domains that guided the conversation
Discussions focused on five key areas of uncertainty:
– Disease progression, causes, and diagnosis
– Non-surgical management
– Surgical management
– Psychosocial impact and access to resources
– Prevention
Responses generated during the workshop were synthesized using reflexive thematic analysis.2 Notes recorded at each table were reviewed collectively, with recurring ideas grouped into shared themes across domains. This approach allowed patient-identified priorities to emerge organically while respecting individual experiences within broader community-level insights.
What participants shared
Diagnosis, education, and ongoing care
Across all domains, one message was clear:
Juliana Conte MSc, PhD, CPT, is a biochemist and certified personal trainer. Diagnosed with lymphedema in 2011, she is a former dual-sport NCAA athlete who promotes a holistic, science-informed approach to lymphedema care. Lori Radke BScPT, CLT, is a physiotherapist and certified lymphedema therapist. She coordinated the Rehabilitation Oncology program in Calgary, AB from 2009-2021, and continues to actively treat patients with Cancer Care Alberta. Catherine Bowman BHSc, is a PhD Candidate in the Department of Epidemiology and Population Health at Stanford University and MD Student at the University of Calgary. She is one of Forbes Magazine’s 30 Under 30.
earlier diagnosis, better education, and consistent ongoing care are urgently needed. Participants emphasized that many gaps in care stem from limited education among healthcare professionals regarding the lymphatic system, early signs of lymphatic dysfunction, and evidence-based management strategies.
Standardized protocols for diagnosis and care were repeatedly identified as a priority, along with their consistent implementation, and an expressed interest in genetic precursors and early identification of lymphedema.
One recommendation made was that individuals diagnosed with lymphedema receive an “at risk of cellulitis” medical alert bracelet, ensuring that healthcare professionals are aware of the infection risk in emergency situations.
Living with lymphedema:
What patients are already doing
A recurring theme was the disconnect between how patients manage lymphedema in daily life and what many clinicians recognize or routinely address. Participants discussed multiple management strategies
that they have adopted through the use of innovative modalities and products. This emphasized the need for further research on these novel interventions to ensure evidencebased information is available to patients and providers. Personal autonomy and independence were emphasized as central to effective management of lymphedema.
The breadth and complexity of these approaches underscored the reality that lymphedema management is costly in both time and money. It is also dynamic, individualized, and often patient-led— reinforcing the need for clinicians with advanced, condition-specific expertise, but also a collaborative approach with their patients.
Recognizing the complexity of patient-led management highlighted the need for greater access to specialized lymphatic care providers. While Certified Lymphedema Therapists play an essential role, participants expressed a desire
for expanded training pathways and multidisciplinary teams capable of supporting long-term, complex care. Remote access and language barriers were also identified as issues.
Furthermore, a strong demand emerged for well-equipped lymphatic disease centres in major cities to improve access to correct diagnoses and specialized care to reduce reliance on self-navigation through online resources and peer support alone. Disparities between public and private services and services for primary versus secondary lymphedema patients were discussed. In particular, the question was posed as to whether differences in cost and access influence outcomes and quality of care.
Surgical management: A call for transparency
Surgical intervention remains one of the most complex and emotionally charged areas of lymphedema care. Experiences varied widely, and for some, surgical complications had profound and lasting effects on quality of life. Participants voiced concerns related to financial barriers, limited access, surgeon


expertise, and variability in outcomes, as well as difficulty accessing clear, unbiased information to support decision-making.
To address these concerns, participants identified several priorities: pre-operative lymphatic imaging and mapping; honest discussions of risks and limitations; transparency regarding surgeon experience and outcomes; improved collaboration and communication among surgeons; and the development of globally accessible guidelines. Questions were raised as to whether surgery can reduce dependence on compression, whether new lymphatic vessels form postoperatively, and how timing, body composition, and disease stage influence outcomes.
Beyond physical symptoms, lymphedema profoundly affects mental health, identity, relationships, employment, and financial stability. Participants spoke openly about isolation, stigma, and inequities in access,
as well as the dearth of support for elderly patients, different cultures, and languages. The cost of treatment and required supplies places significant strain on many patients, often compounded by reduced work capacity. Adequate financial support, education, and communication were identified as essential components of living well with lymphedema. Disability tax credits were cited as one example of support that many patients struggle to access despite clear need. Clearly, more psychosocial professionals are essential on lymphedema care teams.
Therapists and garment fitters bring a unique and informed perspective, often walking alongside patients as educators, advocates, and sources of continuity. Their insights reinforced the value of professionals who engage closely with patients’ lived experiences and build strong therapeutic partnerships.
The insights gathered during this workshop offer clear direction for future care delivery, research priorities, education, and advocacy. Patient-led prioritization highlights where resources should be focused and underscores why inclusive, collaborative spaces must become the norm rather than the exception. Expanding and repeating patient-centred forums across regions and disciplines offers an opportunity to align global efforts with realworld needs.
As the workshop concluded, the room held more than just notes on the wall. There was a shared sense of validation, connection, and momentum. When patients are invited to contribute as partners—and truly heard—bridges are built not only between people, but between science and lived reality. LP
References can be found at https://www. canadalymph.ca/pathways/all-issues/
How to cite: Conte, J, Radke, Bowman, C. Building bridges between science and lived experience. How patient voices can shape global priorities in lymphedema care and research. Pathways. 2026;15(2): 14-17. https://doi.org/10.70472/RTPC7220
Specialist Clinic for Lymphology EuropeanCenterforLymphology
Do you suffer from Lymphedema?
The Foeldi Clinic, European Center for Lymphology, in the Black Forest, Germany offers a special treatment.
4 WEEKS of intensive lymphological decongestive therapy includes:
• Specialist medical care by experienced MD‘s
• Daily decongestive therapy by our specialised lymphedema therapists (expert manual lymph drainage and bandaging) and many different decongestive movement therapies as part of group therapy
What we offer: www.foeldiklinik.de/en/
• Wound treatment if necessary by our certified wound experts and psychological support if necessary by our psychotherapists
• Accommodation and meals at the Foeldi Clinic
Contact: Dr. Tobias Bertsch, Senior Consultant tobias.bertsch@foeldiklinik.de
By Bonnie Baker
In the spring of 2027, the Canadian lymphedema community will come together for something truly special: a national gathering designed not just to share knowledge, but to build the future of lymphedema care in Canada—together.
As part of our March Lymphedema Awareness Month celebrations and in anticipation of World Lymphedema Day on March 6, I’m delighted to offer Pathways readers a first look at our 2027 Canadian Lymphedema Conference. Planning is underway for this 3-day event to take place in May 2027 in Halifax, Nova Scotia. It will be unlike anything we’ve done since 2009. Our approach—and the collaborative spirit behind it—come directly from our history.
The Canadian Lymphedema Framework (CLF) was formed in 2009 through a remarkable, open, community-driven conversation using a meeting format called Open Space Technology (OST). People from across the country—patients, therapists, researchers, physicians, industry partners, and advocates— gathered into one room with a shared purpose: to imagine what lymphedema care in Canada could become. Their ideas, questions, frustrations, and hopes laid the foundation for the CLF itself.
So much has changed since then. Our community has grown—not because lymphedema is new, but because awareness, recognition,


Unlike traditional conferences where sessions are preselected, OST empowers participants to create the agenda themselves. The conversations are shaped by what matters most to those in the room. It’s a space where clarity emerges, priorities take shape, and real collaboration begins.
and connection have steadily increased through our collective efforts. More health professionals now understand how to recognize, diagnose, and manage lymphedema. More researchers are directing their attention to it. And more Canadians who have long lived with swelling and related symptoms are finally being diagnosed, giving them language for their condition and better access to information, care, and support.
At the same time, the individuals who make up this community—patients, clinicians, researchers, advocates, and partners, including many who were present at the very beginning— are far more visible and connected than ever before. Yet despite this progress, the core challenge remains unchanged: how do we create a future where every person in Canada can rely on timely access to knowledgeable care, reliable information, and supportive resources for lymphedema and related conditions? Fittingly, our 2027 conference will begin by returning to the collaborative method that first brought us together.
Why Open Space Technology?
OST is a participant-driven meeting format designed for tackling complex issues—exactly the kind of challenges our community faces. It works when a diverse group of people care deeply, want to move forward, and understand that no single person or organization has all the answers. One of my favourite descriptions of OST comes from openspaceworld.org: “Open Space works best when the work to be done is complex, the people and ideas involved are diverse, the passion for resolution (and potential for conflict) are high, and the time to get it done was yesterday. It’s been called passion bounded by responsibility, the energy of a good coffee break, intentional self-organization, spirit at work, chaos and creativity, evolution in organization, and a simple, powerful way to get people and organizations moving — when and where it’s needed most.”
Unlike traditional conferences where sessions are pre-selected, OST empowers participants to create the agenda themselves. The conversations are shaped by what matters most to those in the room. It’s a space where clarity emerges, priorities take shape, and real collaboration begins. For our community—diverse, passionate, growing, and united by shared urgency—this approach feels not only fitting, but essential.
Because this meeting will help define the CLF’s next 10-year strategic plan, it is extremely important that the room reflects the full scope of Canada’s lymphedema landscape. We are working closely with every provincial lymphedema association to ensure that participants represent many perspectives, including:
4 People living with lymphedema and related disorders, and their caregivers
4 Therapists, nurses, physicians, and other clinicians
4 Researchers and educators
4 Compression garment fitters and suppliers
4 Industry partners developing products, technologies, and solutions
4 Policy makers, funders, insurers, and health-system leaders
4 Professionals in intersecting areas: oncology, skin and wound care, vascular disease, obesity medicine, dermatology, palliative care, and more
4 Community advocates, volunteers, and emerging leaders

We hope to welcome people from every province and territory and from all walks of life. There is no required experience or educational background—just a genuine connection to lymphedema and a desire to make a difference. Because space may be limited, we anticipate capping participation at approximately 300 attendees for the OST portion of the event. However, our intention is clear: if you want to be there, we want to find a way to include you.
This Spring special issue of Pathways reaches a wide audience—including many people who may be exploring our community for the first time. Whether you are newly diagnosed, a longtime clinician, a caregiver, a student, or someone whose work intersects with chronic edema in any form—your voice matters.
To help us plan responsibly and to ensure strong representation across Canada, we invite you to pre-register your interest in participating. Pre-registration is free, has no commitment, and simply lets us keep you informed as plans take shape.
We ask that participants be 18 years or older. If we receive significant interest from young people under 18, we will explore options to accommodate them with an adult chaperone.
The outcomes of this collaborative meeting will guide our work for the next decade. They will help determine priorities, shape research directions, strengthen advocacy, and ultimately
improve access to care across Canada.
In the months ahead, we will share more details about the event, registration, and travel information. For now, I hope you will mark your calendars for May 13 – 15, 2027 and consider joining us in Halifax, where we’ll gather with purpose, energy, and optimism. This is your chance to help chart the course for the next chapter of lymphedema care in Canada. We look forward to taking those steps with you. LP

By Margie McNeely, Anna Towers and Jane Armer
Introduction
Drawing on ancient writings, Isaac Newton is credited with writing to a colleague: “If I have seen further, it is by standing on the shoulders of giants.” This metaphor acknowledges that one’s current achievements emerge from a foundation of past intellectual and scientific work by predecessors, leading to greater insight, understanding, and innovation in moving a given field forward. Crucial to this cycle of forward movement is the process of mentorship (and, ideally, eventual collaboration). The complexity of lymphology, combined with the dynamic interaction between experienced professionals and those new to the field, makes mentorship by expert clinicians, educators, and researchers especially valuable and essential. The mentorship panel at the October 2025 International Framework Conference explored key elements of effective mentorship through shared reflections from mentors and mentees, along with audience discussion.
Membership Panel
•Mona Al Onazi
•Elizabeth Anderson
•Naomi Dolgoy
•Marie-Eve Letellier

What makes a strong mentor?
Panel members agreed that strong, effective mentors demonstrate integrity, honesty, and genuine care in their behaviours when providing care for people living with lymphedema.
“Mentors combine integrity with a passion for supporting people affected by lymphedema.”
•Nike Odemuyiwa
•Shirin Shallwani
•Dorit Tidhar
Mentorship Panel summary
Objective: To reflect on how mentorship helps shape careers, strengthens teamwork, and builds the future of lymphedema care globally.



The best mentors model these values, while also creating a supportive environment that provides opportunities for different team members to contribute ideas and participate in decision-making.
A panel member reflected on the importance of communication in strong mentorship: “Strong mentorship is grounded in effective communication, including mentor-mentee relationships, engagement
with the community, collaboration with other healthcare professionals and most importantly, communication with the patients.”
Panelists emphasized that mentorship in lymphedema can take many forms and is not strictly limited to academia or research. There are mentors who guide practice and policy, community mentors who share lived experience, and industry mentors who help connect innovation to patient care.
One panel member noted that mentorship can often come full circle, reciprocal mentorship. She described how a clinical mentor guided her early career in professional practice, and now years later, she is supporting this clinical mentor in research and implementation areas.
Margaret (Margie) McNeely is a Professor in the Departments of Physical Therapy and Oncology at the University of Alberta, in a jointly funded position with Cancer Care Alberta. She is the Director of the Cancer Rehabilitation Research Clinic at the University of Alberta. Dr. Anna Towers MD is the Director, Lymphedema Support Centre of the Breast Cancer Foundation of Quebec at the MUHC, McGill University Health Centre, Montreal. Jane M. Armer, RN, PhD, FAAN is Professor Emerita, University of Missouri Sinclair School of Nursing and Director, American Lymphedema Framework Project.
What does a positive mentorship environment look like?
A panel member highlighted that the importance of interdisciplinary collaboration in lymphedema mentorship, involving physicians, surgeons, nurses, wound care specialists, physiotherapists, kinesiologists, massage therapists, and patient partners. However, true inclusivity in mentorship extends beyond professional roles, encompassing diversity in culture, ethnicity, language, and lived experiences. By including individuals of varied backgrounds that reflect the diversity of the lymphedema community, the field gains broader perspectives and a deeper understanding of the issues it faces.
“Effective mentorship goes beyond professional expertise to include diverse voices and perspectives – all valued as equal contributors. Mentors play a key role in fostering supportive, inclusive environments and modeling what good team functioning looks like.”
One panel member shared the importance of understanding how practice may differ from country to country, and how understanding
local approaches can inform and help in the mentorship process.
How does a mentor provide support?
Mentors often identify a trainee’s strengths early on and provide opportunities for them to showcase their learning and skills.
“A mentor sees leadership potential in a trainee and will express that, often years before the mentee realizes that they can be a leader.”
Good mentors recognize potential and facilitate pathways for growth, helping mentees expand their knowledge, confidence and capabilities. One panel member shared that after giving a presentation in her own area of research, she was invited to expand her work to the area of lymphedema, while another, working clinically as a nurse educator, was encouraged to pursue graduate studies focusing on lymphedema self-management. As a nurse researcher, the panel member was encouraged to share her knowledge with other students by mentoring undergraduate and doctoral students and in classroom teaching work.
coming to Winnipeg, MB, November 8 – 14, 2026
• 135-hours of lymphedema education
75-hr engaging online home study module 60-hr (6 1/2 day) classroom education
• Time-tested, effective and evidence-based curriculum
• Learn from the most experienced instructors in the field
• Fewer days away from home and work
• Greater flexibility to fit your personal schedule
• Exclusive post-graduate resources
• Special pricing for Canadian Therapists
Online Courses
• Breast Cancer Rehabilitation with Jodi Winicour, PT, CLT
• Strength After Breast Cancer with Katie Schmitz, PhD, MPH, FACSM
• Wound Management for CLTs with Jan Weiss, PT, DHS, CLT
• Head & Neck Lymphedema with Heidi Miranda-Walsh, OTR/L, CLT
• Elastic Taping for Lymphedema with Ruth Coopee, OTR/L, CLT
• Add’l courses at klosetraining.com
more information: 1-303-245-0333 • info@klosetraining.com
“Strong
One panel member shared how a mentor encouraged her to pursue training and certification in lymphedema, something not typically within her scope of practice. This opportunity allowed her to integrate her professional and research expertise (epidemiology) into the lymphedema clinic setting and ultimately take on a leadership role.

“Effective mentorship goes beyond professional expertise to include diverse voices and perspectives – all valued as equal contributors. Mentors play a key role in fostering supportive, inclusive environments and modeling what good team functioning looks like.”
are actively included in mentorship and leadership development opportunities.
Another audience member raised a practical question: “How do you find a mentor?” Panelists reflected that sometimes mentors emerge naturally through shared interests or informal conversations, while other times they are sought out intentionally. They agreed that mentorship often begins with curiosity and by reaching out, even informally.
Why is mentorship important?
Panel members also noted that mentorship often happens outside of formal programs.
“Much mentorship happens in informal settings – over coffee or a hallway conversation.”
These simple, everyday interactions can have a lasting impact and help generate new ideas, initiatives and strategies.
What perspectives did the audience share?
An audience member comment during the session provided an “aha moment” for many: “Academic clinicians and researchers must not forget that there are experienced lymphedema professionals in the community who need to be included, to be seen and heard. They have a lot to contribute.”
This comment resonated strongly with the panel members as it emphasized the importance of recognizing and valuing the expertise that exists beyond academic settings and ensuring that community-based professionals (who provide much of the direct care for people living with lymphedema)
Panel members also spoke about the importance of strategic mentorship to ensure the field remains strong and continues to grow for years to come. With many longtime leaders in the field of lymphedema nearing retirement, there is a need to support and encourage others to step forward.
What happens next?
The International Lymphoedema Framework (ILF) and its national framework partners (like the Canadian Lymphedema Framework) are organizations that can help mentor new leaders in the field. Panelists suggested that the Frameworks can support mentorship by connecting new and experienced professionals, creating mentorship programs, and providing opportunities for emerging leaders to share their ideas and adopt new roles.
such as communities of practice and fireside chats, editorial publications and case studies.
4 Educational initiatives - formal and informal learning opportunities, such as short courses and practical workshops.
4 Leadership opportunities - expert and novice board and committee positions, and representative opportunities within organizations like the ILF and CLF. Scientific committee positions and opportunities to co-chair a conference committee.
4 Conference opportunities - attending, participating through volunteering and planning committees, and knowledge sharing of clinical experiences.

4 Relationship and community building - establish structured opportunities (e.g., introductions, joint meetings, or co-led initiatives) for mentees to engage with leaders and decision makers. Senior mentors can leverage their networks to connect emerging clinicians, researchers and educators, supporting continuity, legacy planning and smooth transitions within organizations and communities.
There is an African proverb which seems an appropriate closing here: “If you want to go fast, go alone. If you want to go far, go together.”
Suggestions for how this may be carried out include:
4 Communications - opportunities for knowledge sharing and dissemination,

To move our field forward, moving together through mentorship and collaboration is crucial. LP
For additional tips on Finding a Mentor see “Hints and Tips” on page 23. How to cite: McNeely M, Towers A, Armer, J. Moving forward together. Building the future through mentorship and collaboration. . 2026;15(2): 20-22. https://doi.org/10.70472/RUCN6419
www.canadalymph.ca/getinvolved



Finding a Mentor: The importance of mentorship and its benefits are detailed on pages 20-22. However, the mentor-mentee relationship expands beyond the clinical and research roles.
Examples of types of mentees
4 a lymphedema therapist seeking guidance on a challenging case from a more experienced clinician
4 a researcher or educator wanting to tap into the knowledge of a seasoned individual interested in the same topic
4 a lymphedema community advocate just getting started and looking to explore work previously done by others
4 a newly diagnosed lymphedema patient connecting with a peer mentor who is already successfully self-managing.
Resources
Resources for finding a mentor
4 Take advantage of networking opportunities. Many (if not most) relationships are formed at conferences, presentations, rounds, professional social events, hallway conversations, and so on.
4 Join professional organizations in your field to connect with experienced peers.
4 Consult the websites of lymphedema community organizations such as the Canadian Lymphedema Framework (CLF), Provincial Associations, the National Lymphedema Network (NLN),

Lymphology Association of North America (LANA) and Lymphatic Education & Research Network (LE&RN) for listings of local experts, certified lymphedema therapists and patient support networks.
4 The NLN Start Strong Program is for new Certified Lymphedema Therapists (CLTs) and offers mentorship from clinicians, virtual roundtables, and a community forum.
4 Explore online communities such as LinkedIn or specialized forums. LP
Source: Canadian Lymphedema Framework
Reviewed by Lori Radke BScPT, CLT, a physiotherapist and certified lymphedema therapist in Alberta who sits on the Editorial Board of Pathways
Thiscollaborative resource from Dr. Dhruv Singhal, and Megan Belanger provides an informative, illustrated overview of the lymphatic system, explaining what happens when it is disrupted to create lymphedema.
The “train on the tracks” analogy is a clever way to represent the vascular system and the causes of lymphedema. The creative illustrations, with colour coding and the train passengers, reinforce how veins, arteries, and lymphatics work together as a whole system.
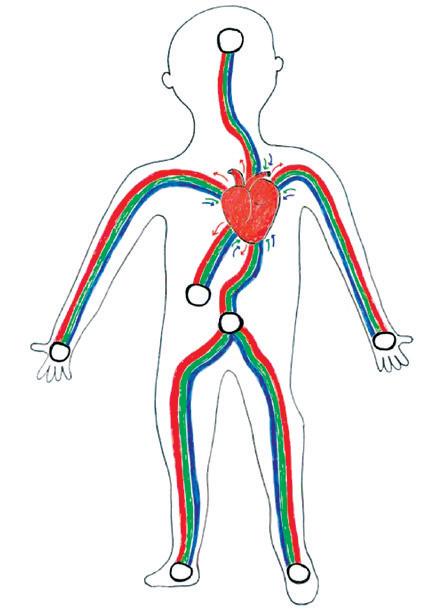
It is often a challenging concept for patients and healthcare professionals to understand the interactions between these three parts. The explanations provide a basic understanding, but not the complexities of the whole system that occur to produce the high protein swelling of lymphedema. In section #2, the authors refer to cancer-related lymphedema as the most common cause of secondary lymphedema in the
USA. However, prevalence studies now show that chronic venous insufficiency from obesity is the leading cause in developed countries.
The physical therapy treatments for lymphedema described in section #3 could have been expanded. The authors infer that manual lymphatic drainage is the only physical therapy treatment technique based on the description they use and the accompanying illustration. Compression is not mentioned and is only included in their surgical description of liposuction, emphasizing the need for lifelong compression. The book could be improved with more detail on the components of Complete Decongestive Therapy including exercise, skin care and the various types of compression that are used to manage lymphedema. The chronicity of lymphedema necessitates the inclusion of more information for patients about these self- management techniques.
The treatment section also focuses primarily on surgical options. It explains the different procedures available, and the illustrations of the
train tracks are helpful in showing what each procedure entails and how they differ. The last section then suggests that the immediate lymphovenous anastomoses after a lymph node dissection can prevent lymphedema from developing. However, this may be misleading as it is not always 100% successful.
The book concludes with an excellent paragraph highlighting the benefits of multidisciplinary care and the need for individualized treatment. This is vitally important in lymphedema management. This resource is a good starting point for education about the lymphatic system and lymphedema treatments for all patients and healthcare professionals, in particular pediatric patients, to help them “stay on the tracks” of managing their lymphedema. LP
The booklet is available free online through the LE&RN website in the Resource Downloads: https://tinyurl.com/LERN-KTTOTT




The following selection of condensed abstracts are from some presenters at the 2025 International Lymphedema Conference. We encourage you to refer to www.ilf2025.com to browse all of the unabridged published abstracts from the conference program.
Accurate classification of breast cancer–related lymphedema (BCRL) is essential for effective treatment planning. This study evaluated the relationship between physiotherapists’ clinical classifications and objective volume-based measurements and examined how diagnostic accuracy affects treatment outcomes. Upper-limb assessment data were analyzed by comparing therapist-assigned severity levels with classifications derived from segmental limb volume calculations. Correlation analyses assessed agreement across mild, moderate, and severe categories, and regression models explored the impact of diagnostic accuracy on therapeutic efficacy.
Segment-based volume analysis demonstrated stronger alignment with physiotherapist assessments than whole-limb measurements. High agreement was observed for mild (r = 0.79) and severe (r = 0.76) lymphedema, while moderate classifications showed weaker correspondence (r = 0.58), with frequent misclassification occurring between mild and moderate cases. Regression findings indicated that inaccurate diagnosis— particularly when based solely on the most swollen segment—was significantly associated with less effective treatment outcomes. This relationship did not appear when whole-limb criteria were used, suggesting that segment-level precision captures clinically meaningful differences more effectively.
Overall, physiotherapist classifications corresponded more accurately with segmental measurements than with whole-limb assessments. Diagnostic misclassification, especially from overreliance on localized swelling, was linked to suboptimal treatment results.
These findings support adopting segmental measurement strategies to enhance diagnostic accuracy and improve outcomes in BCRL management.
Source: Correlation between therapist measurements and classification decision in BCRL and their impact on treatment outcomes. D.Tidhar, W.Baskett, J.Armer and Chi-Ren Shyu. Presented at the ILF/CLF conference Niagara Falls, Canada October 2025.
Introduction: In children, nearly all cases of lymphedema are primary. Pediatric lymphedema is rare and shows significant phenotypic variability. Typically, one or two limbs are affected, but other body regions, including nails (ski-jump nails), can also be involved. Compression therapy and physical exercise are essential for management. Multiple compression therapy options exist, but their application and timing differ by country. Monitoring treatment outcomes in children is challenging due to natural growth in height and weight. At our center, we initiate compression therapy within the first two years of life to prevent irreversible changes. Aims: This retrospective observational study evaluates the diagnosis, timing, types of compression therapy, follow-up time, and outcomes, as well as any complications associated with treatment. Methods: We assessed approximately 40 children with primary lymphedema affecting the legs/feet. We assessed the diagnosis the type and timing of compression therapy, therapeutic effects, and complications. Results: Most children began therapy within their first year. Initial bandaging was followed by therapeutic elastic stockings, leading to reduced edema and no hinder on foot/toe growth. Ski-jump nails also flattened. Conclusions: Compression therapy, when started early, is well tolerated in children under 2, with significant edema reduction and normalization of nail growth.
Source: Compression therapy in children with lymphedema. K.F.van Duinen. Presented at the ILF/CLF conference Niagara Falls, Canada October 2025
Background: Resistance exercise has been shown to improve symptoms and quality of life in individuals with breast cancer related lymphedema (BCRL). However, the effects of combining therapeutic resistance exercise with compression on lymphedema volume remain unexplored. Purpose: To determine the efficacy of a 12-week decongestive resistance exercise (DRE) programme with compression garments compared with standard care. Methods: In a three-arm RCT, individuals with BCRL were allocated to standard care, DRE with a daytime compression garment (CG), or DRE with an adjustable compression wrap (CW). The primary outcome was percentage change in excess arm lymphedema volume. Secondary outcomes included tissue composition, shoulder range of motion, muscle strength, physical activity, body image, and health-related quality of life (HRQoL). Results: Sixty participants were enrolled, and 59 (98%) completed the intervention. Excess arm volume significantly decreased in the DRE+CG (47.5% ±50.9; p<.001) and DRE+CW by (28.9% ±29.2; p=.02) compared to the standard care. MRI analyses (n=29) showed significant reductions in subcutaneous fat and water in the affected arm, favouring DRE group. Secondary outcomes showed improvements in shoulder abduction, muscle strength, physical activity leisure score index, body image, and HRQoL. Conclusion: A combined DRE with compression is a promising, clinically applicable approach for managing BCRL.
Source: Combined Therapeutic Approach for Managing Breast Cancer-Related Lymphedema: A Randomized Controlled Trial. M.Al Onazi. Presented at the ILF/CLF conference Niagara Falls, Canada October 2025
Introduction: Lymphedema is associated with obesity, yet while guidelines advocate weight loss, randomised trials indicate weight management is not an effective lymphoedema treatment. This study explores this discrepancy,
providing new insights into current UK practice. Methods: A mixed-methods design included an audit of lymphoedema records from four UK Health Boards (n=120), practitioner questionnaires (Scotland: 27/53; Wales: 24/59) and a focus group (n=6).
A UK-wide questionnaire of people living with lymphoedema (n=358) and follow -up interviews (n=11) explored lived experience. Reflexive thematic analysis and triangulation identified key determinants of practice, informed by the Tailored Implementation for Chronic Diseases Framework and theories of self-determination and self-management.
Results: Practitioners widely believed high body weight worsens lymphoedema outcomes, shaping treatment goals. Barriers and enablers to addressing weight were consistent across nations, though confidence and frequency of weight-related discussions varied. Weight stigma and systemic barriers linked to guidance were evident. People with lived experience commonly lived with overweight or obesity but reported that weight was rarely discussed in consultations, and
weight change had limited impact on lymphoedema. Autonomy, competence, and connection influenced successful self-management. Conclusion: A clear disconnect exists between evidence, guidance, and practice. Holistic, person-centred, multidisciplinary approaches are needed to improve care and reduce frustration.
Source: Mixed methods research: Building a composite picture of lymphoedema with obesity. Debbie J Provan. Presented at the ILF/CLF conference Niagara Falls, Canada October 2025
Introduction: The lymphoedema-specific Patient Reported Outcome Measure (LYMPROM©) was developed to support Value-Based Healthcare.
Aims: LYMPROM© was assessed following the Consensus-based Standards for the selection of health Measurement Instruments guidelines.
Method: Face and content validity were examined by anonymous survey with key stakeholders. LYMPROM© Cymraeg (Welsh) included two forward and one backward translation. A longitudinal study used anonymized routinely collected data to examine internal consistency; structural validity; construct validity;

measurement error; test-retest reliability and responsiveness. Results: LYMPROM© was relevant, clear, and comprehensive (content validity index 0.83-1.00; average 0.94, n=32) and translations were reviewed to be appropriate. LYMPROM© item and domain (physical, social and emotional) scores were positively correlated (domain correlations: 0.595 to 0.812). LYMPROM© total and domain scores showed moderate, negative correlations (-0.577 to -0.435) with EQ5D-5L scores. LYMPROM© total and domain scores showed good test-retest properties, with little or no change in scores, and strong positive correlations (total: 0.919; physical domain: 0.922; social domain: 0.889; emotional domain: 0.820). LYMPROM© showed good responsiveness, with strong, positive correlations between scores, with a slight reduction in scores (-3.8 to -2.0 units).
Conclusion: Evidence shows that LYMPROM© is valid, reliable and is feasible as part of routine lymphedema care.
Source: The reliability and validity of a new Lymphoedema-specific Patient Reported Outcome Measure (LYMPROM©) for adults. M.Thomas. Presented at the ILF/CLF conference Niagara Falls, Canada October 2025

Mar 6, 2026 World Lymphedema Day (WLD). An annual celebratory Worldwide event to educate the world about lymphatic diseases. Contact your provincial association to learn about local events. n www.canadalymph.ca/WLD
Apr 10-12, 2026 11th World Symposium for Lymphedema Surgery Columbus, OH USA n tinyURL.com/WSLS-2026
Apr 25-26, 2026 LymphyCON 2026 Calgary, AB Canada n tinyURL.com/LymphyCON-2026
Apr 30-May 3 16th Australasian Lymphology Conference Cairns, Australia n https://www.alaconference2026.com.au/
May 13-15, 2026 Mayo Clinic Lymphatic Disorders Symposium 2026 Rochester, MN USA n tinyURL.com/MC-LDS-2026
Oct 22-24, 2026 2026 Wounds Canada National Conference Niagara Falls, (in-person and online) ON Canada n www.woundscanada.ca/
Nov 6-8, 2026 National Lymphedema Network 2026 Summit Mesa, AZ USA n https://lymphnet.org/page/2026-summit


Lymphedema and Chronic Edema Management Learn more: tinyurl.com/uabmicrocourse

Congratulations to Professor Neil Piller, who was recently appointed a Member of the Order of Australia (AM) for his significant service in the area of lymphology/lymphedema. Neil is an Australian Professor in the area of lymphology and Director of the Lymphedema Clinical Research Unit in the College of Medicine and Public Health, Flinders University.
As a dedicated and enthusiastic professor, clinician and academic, his contributions to the world of lymphology/lymphedema include authoring more than 200 academic papers, supervision of PhD and MD students in the area of lymphedemas and editing multiple worldwide publications, as well as serving as a board member or patron of various national and international associations.
Read about all Professor Piller’s honours, awards and accomplishments at https://www.flinders.edu.au/people/neil.piller



















May 13-15, 2027
Halifax, Nova Scotia







Bauerfeind’s flat-knit Curaflow garments are custom-made and perfectly adapted to the lymphedema and lipedema patients. Made with breathable and moisture-regulating knitted fabric, it was specifically made to move with you.


• SUPPORTING DOCUMENTS • OUTSERTS
A full set of references can be found at: https://www.canadalymph.ca/pathways-references/

Personalized care for patients with lymphedema
Six simple questions can make a difference
By Ad Hendrickx and Janine Dickson-Blok
1. Bloem S, Stalpers J. Subjective Experienced Health as a Driver of Health Care Behavior. SSRN. Electron J. 2012;(12).
2. Bloem S, Stalpers J, Groenland EAG, Van Montfort K, Van Raaij WF, De Rooij K. Segmentation of health-care consumers: Psychological determinants of subjective health and other person-related variables. BMC Health Serv Res. 2020;20(1):1–12.
3. Houtum L Van. Self-management and support needs of chronically ill people. 2016.
4. Huber M, Knottnerus JA, Green L, van der Horst H, Jadad AR, Kromhout D, et al. How should we define health? BMJ [Internet]. 2011;343(9666):d4163.
5. Trappenburg J, Jonkman N, Jaarsma T, van Os-Medendorp H, Kort H, de Wit N, et al. Self-management: One size does not fit all Patient Educ Couns 2013;92(1):134–7
An interview with Margie McNeely
1 Essential components of the maintenance phase of decongestive therapy Margaret L McNeely, Mona M Al Onazi, Mike Bond, Andrea Brennan, Heather Ferguson, Deborah A Gross, Fedor Lurie, Linda Menzies, Steven Norton, Yuanlu Sun, Alaina Newell Medical Oncology (2024) 41:289 https://doi org/10 1007/s12032-024-02442-1 https://link springercom/article/10 1007/s12032-024-02442-1
By: Juliana Conte, Lori Radke, and Catharine Bowman
1 World Cafe Community Foundation (2026, January) The World Cafe, theworldcafe com/ Used under creative commons license: https://creativecommons org/licenses/by/4 0/deed en
2 Braun, V, & Clarke, V (2019) Reflecting on reflexive thematic analysis Qualitative Research in Sport, Exercise and Health, 11(4), 589–597