
Personalized care for patients with lymphedema
Six simple questions can make a difference.
By Ad Hendrickx and Janine Dickinson-Blok
Lymphedema
(LE) is a chronic, progressive, and often debilitating condition that remains a neglected global healthcare problem, despite its significant impact on patients’ lives. Patients with LE often experience severe problems in daily life, caused not only by swelling or heaviness of the affected region, but also by reduced mobility, recurrent infections, and associated complaints such as pain, depression, and anxiety. In many cases, LE has a profound impact on patients’ quality of life.
There is no cure for LE, and its management aims to minimize and stabilize edema and to enhance both physical and mental functioning, thereby improving overall quality of life. The therapeutic approach encompasses various components, such as compression therapy, exercise therapy, skincare, and lifestyle interventions. Integral to therapeutic interventions focused on improving the clinical aspects of LE, an important part of treatment is dedicated to self-management. This involves providing patients with the knowledge and skills necessary to optimize their ability to manage their health status.
However, research shows that many patients experience difficulties in achieving optimal self-management, and adequate support from


healthcare providers is needed. In addition, there is limited knowledge about which patients benefit from which type of support, resulting in negative consequences for patient outcomes and healthcare costs. Alongside these findings, an increasing prevalence of unhealthy lifestyles is observed, often combined with denial of the need to change and an inability to change. In most cases, lifestyle-related issues involve obesity and insufficient daily physical activity.
How can supportive care be better aligned with what people actually need?
When allocating support and care, it is essential to consider how people experience their health. If care aligns with an individual’s perceptions, wishes, and needs, it is more effective and leads to greater satisfaction. The quality of diagnosis and treatment planning improves, as does individuals’ involvement in their own health. In practice, however, there is often insufficient differentiation in the supportive care provided. Despite everyone’s best efforts, supportive care is frequently based on a standard approach, or a “one size fits all” model. This needs improvement—but how can this be achieved?
Ad Hendrickx, PT, PhD works as program manager of research & development in the Dutch Center of Expertise for Lymphovascular Medicine at Nij Smellinghe Hospital in Drachten, The Netherlands. During his career as a physical therapist, he specialized in lymph- and lipedema.
Janine L. Dickinson-Blok, MD PhD is a general dermatologist with expertise in the diagnosis and treatment of lymphedema. She works at the Dutch Center of Expertise for Lymphovascular Medicine at Nij Smellinghe Hospital (Drachten, The Netherlands) and Meander Hospital (Amersfoort, The Netherlands).
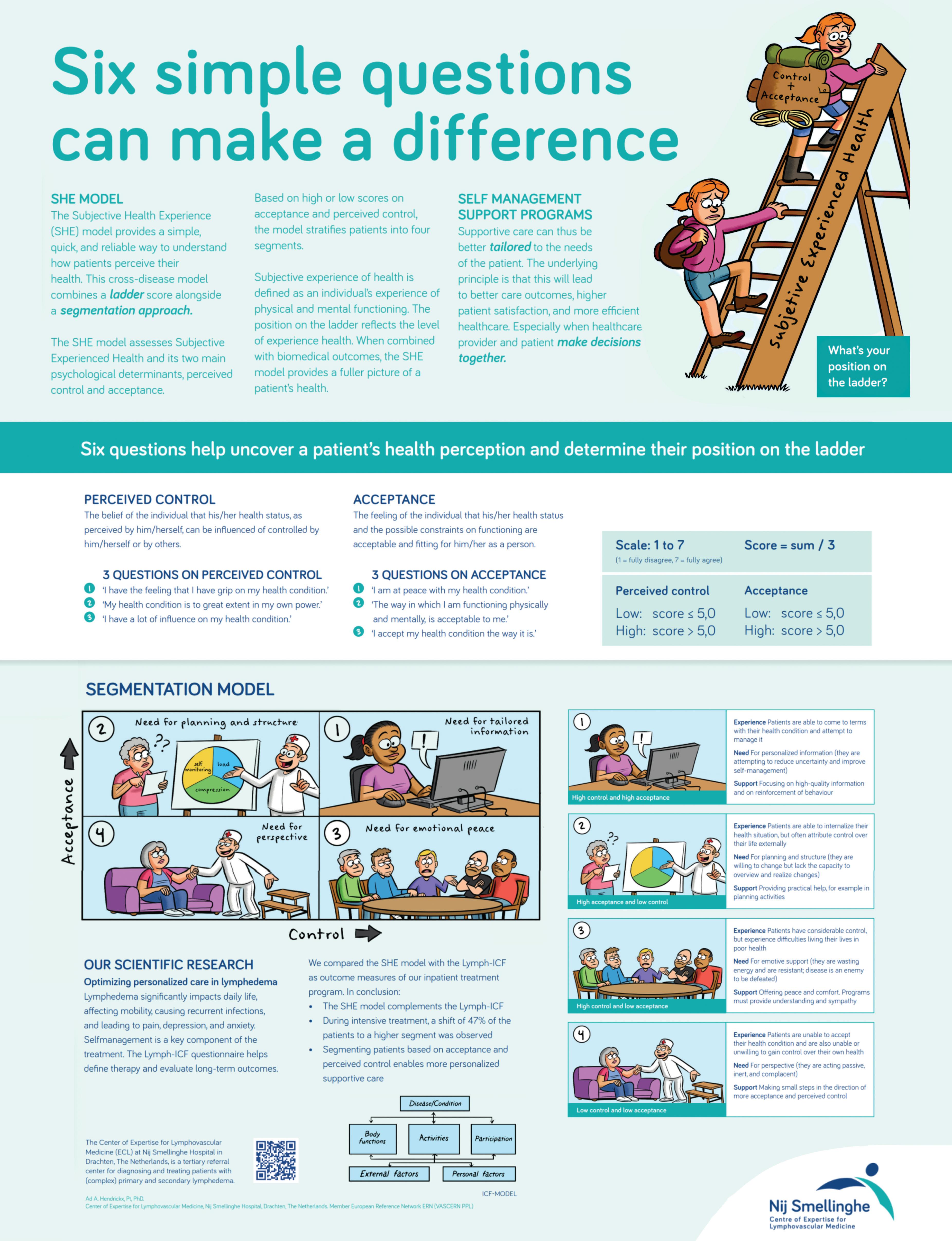
The Subjective Health Experience model (SHE model), developed by Bloem and Stalpers, provides a tool for allocating supportive care in a more personalized way. To determine which form of support is most appropriate for an individual, the individual’s experience of health must be the point of departure. In this model, health experience is the central theme within a clear, evidencebased, cross-disease framework that places experienced health at the center of care. The model is grounded in the idea that not only medical diagnoses, but especially how people experience their health, influences behavior, self-management, and the need for support.
Subjective Health Experience is defined as an individual’s experience of physical and mental functioning while living life in the way they want to, within the actual constraints and limitations of their existence. To make this experience visible and measurable, Bloem and Stalpers use a visual analogue scale (VAS 0–10), presented as a ladder. The lowest step represents the individual’s worst day in the past month (0), and the highest step represents the best day in the past month (10). Individuals are asked to indicate on which step they feel they stand today, and on which step they stood on average during the past month.
The ladder metaphor intuitively reflects changes in health experience over time. When individuals perceive themselves as functioning better, both physically and mentally, they place themselves higher on the ladder; when functioning is perceived as worse, a lower position is chosen. This approach creates a personal frame of reference and allows for meaningful discussions between healthcare
A
Disease Acceptance
• I am at peace with my health condition.
• The way I am functioning physically and mentally is acceptable to me.
• I accept my health condition the way it is.
Perceived Control
• I have the feeling that I have a grip on my health condition.
• My health condition is to great extent in my own power.
• I have a lot of influence on my health condition.
professionals, patients, and their supportive network about the most appropriate supportive care. The central question becomes: “What do you need to move higher up the ladder?”
Acceptance and perceived control: two key factors Research shows that two psychological factors are particularly important in determining where someone places themselves on the ladder: acceptance and perceived control. Acceptance refers to the extent to which a
person has been able to give their condition a place in their life. Perceived control reflects the degree to which someone feels able to influence their health and daily functioning. Acceptance is officially defined as “the feeling by the individual that their health condition and the possible constraints on functioning resulting from it are acceptable and fitting for them as a person.” Perceived control is defined as “the belief of the individual that his or her health condition can, in the individual’s perception, be influenced


or controlled by themselves or by others.”
The SHE-model makes these factors measurable using a short set of questions and translates them into a practical segmentation framework. Based on high or low levels of acceptance and perceived control, four profiles are identified, each requiring a different type of support.
From model to practice: six simple questions that can make a difference Levels of acceptance and perceived control are assessed using three questions for each construct (Figure A), rated on a 7-point Likert scale (1 = fully disagree, 7 = fully agree). Mean scores are calculated by summing the three question scores and dividing the total by three; these mean scores are then used for segmentation. High acceptance and perceived control are defined as a mean score greater than 5. Based on these determinants, patients are divided into four segments (Figure B). To make the SHE-model easily accessible in everyday practice, our organization developed a visual poster using plain language (B1 level)







Segment II
High acceptance
Low perceived control
Segment IV
Low acceptance
Low perceived control
Segment I
High acceptance
High perceived control
Segment III
Low acceptance
High perceived control
and supportive illustrations (Figure C on page 7). The core of the poster is formed by the six simple questions and the ladder. Together, they can make a meaningful difference in how care is tailored. The strength of this approach lies in its simplicity. The questions invite reflection and conversation and help make abstract concepts such as acceptance and perceived control understandable and meaningful for patients dealing with lymphedema or lipedema.
Four profiles, four types of support Based on high or low scores for acceptance and perceived control, individuals can be grouped into four segments. Patients in Segment I (high acceptance, high perceived control) seek to improve self-management skills and reduce uncertainty; professional support should focus on high-quality information and reinforcement of effective behavior. Patients in Segment II (high acceptance, low perceived control) are willing to change but lack the capacity to organize and implement plans; support should focus on practical assistance such as planning and structuring activities. Patients in Segment III (low acceptance, high perceived control) often waste energy by resisting the condition and viewing it as an enemy to be defeated. Support for this group should focus on understanding and empathy, complemented by peer support. Finally, patients in Segment IV (low acceptance, low perceived control) benefit most from gaining perspective and taking small steps toward increased acceptance and
control. The publication by Bloem et al. (2020) provides a comprehensive overview of these profiles, corresponding support strategies, and their theoretical foundations.
Cross-disease and complementary to biomedical care
An important strength of the SHE model is that it is cross-disease. It is not tied to a specific diagnosis and can be applied across a wide range of chronic conditions, including lymphedema and lipedema. Because the model starts from the individual’s subjective experience of health rather than from disease, it is broadly applicable and suitable for personalized supportive care.
The use of the SHE-model aligns closely with the new concept of health as formulated by Machteld Huber. In this vision, health is no longer defined primarily as the absence of disease, which dominated earlier definitions, but as the ability to function, adapt, and self-manage in the presence of physical, emotional, and social challenges. This perspective resonates strongly with the SHE model’s focus on experienced health and daily functioning.
The SHE model does not replace the biomedical model; rather, it complements it. While biomedical care focuses on disease mechanisms, diagnosis, and treatment, the SHE-model focuses on how individuals experience their health and manage everyday life. Together, these perspectives provide a more comprehensive understanding of health.
Application in lymphedema care
For people living with lymphedema, a condition requiring lifelong management, this combined approach is particularly valuable. Medical treatment remains essential, but the success of care is strongly influenced by how well support aligns with acceptance, perceived control, and personal context. While segmentation inevitably simplifies a complex reality, the SHE model is not intended to label individuals or prescribe fixed solutions. Instead, it serves as a guide to support a meaningful conversation.
The real value of the SHE-model lies in its ability to structure dialogue and support the process of Shared Decision-Making. By making acceptance, perceived control, and health experience visible using simple language, it creates a common starting point for discussion. The conversation tool used in our center supports this process by helping patients and healthcare professionals explore together where someone stands and what type of support may be helpful at a given moment. Finally, it is important to recognize that these constructs can change over time; therefore, repeated measurements are necessary.
The real value of the SHE-model lies in its ability to structure dialogue and support the process of Shared Decision-Making.
Conclusion
The SHE-model demonstrates that personalized care does not have to be complex. Six simple questions combined with a ladder score provide a powerful way to better align support with individual needs. In a time of increasing care demands and limited resources, this approach helps make care more human, more effective, and more sustainable. LP
Acknowledgements
Jan-Willem Spakman for his illustrations (website: wimpiecomics.nl) and Ellen de Jong, Communications and Marketing Manager of our institute, for her contributions to the poster. Professor Dr. Sjaak Bloem (Nyenrode Business University in The Netherlands) has been of great support during the introduction of the SHE mode and one of the developers of the model.
References can be found at https://www.canadalymph.ca/pathways/ all-issues/
How to cite: Hendrickx A, Dickinson-Blok J. Personalized care for patients with lymphedema. Six simple questions can make a difference. Pathways. 2026;15(2): 5-8. https://doi.org/10.70472/QCAF1202