What is socially just lymphedema care? The roles and responsibilities of individuals and organizations
By Jennifer Brady
interact. My research explores the roles that health professionals could and should play in redressing the impact of social inequities on patients’ lives through their day-to-day practice. I also research how health professionals may work to change social inequities at a structural level (i.e. social policy) through advocacy and activism. The factors that shape Canadians’ health extend far beyond an individual’s access to healthcare services. Social inequities, including racism, sexism, classism/ poverty, homo- and trans-phobia, weightbased discrimination, and the inequitable distribution of resources across urban, rural, and remote locations cause preventable health disparities among Canadians. Since these disparities are preventable, they are also unfair and often worsen individuals’ socio-economic position.1 Social inequities rob Canadians’ capabilities2 to live healthy, dignified, and meaningful lives by making needs, such as healthy food, leisure, and safe housing, financially, physically, and/or culturally inaccessible. Through an effect known as the biochemistry or biology of discrimination,3 social inequities further harm the health of Canadians because of the physiological
and psychological impacts of the chronic stress that results from being marginalized. In other words, the health of Canadians is a matter of social justice.
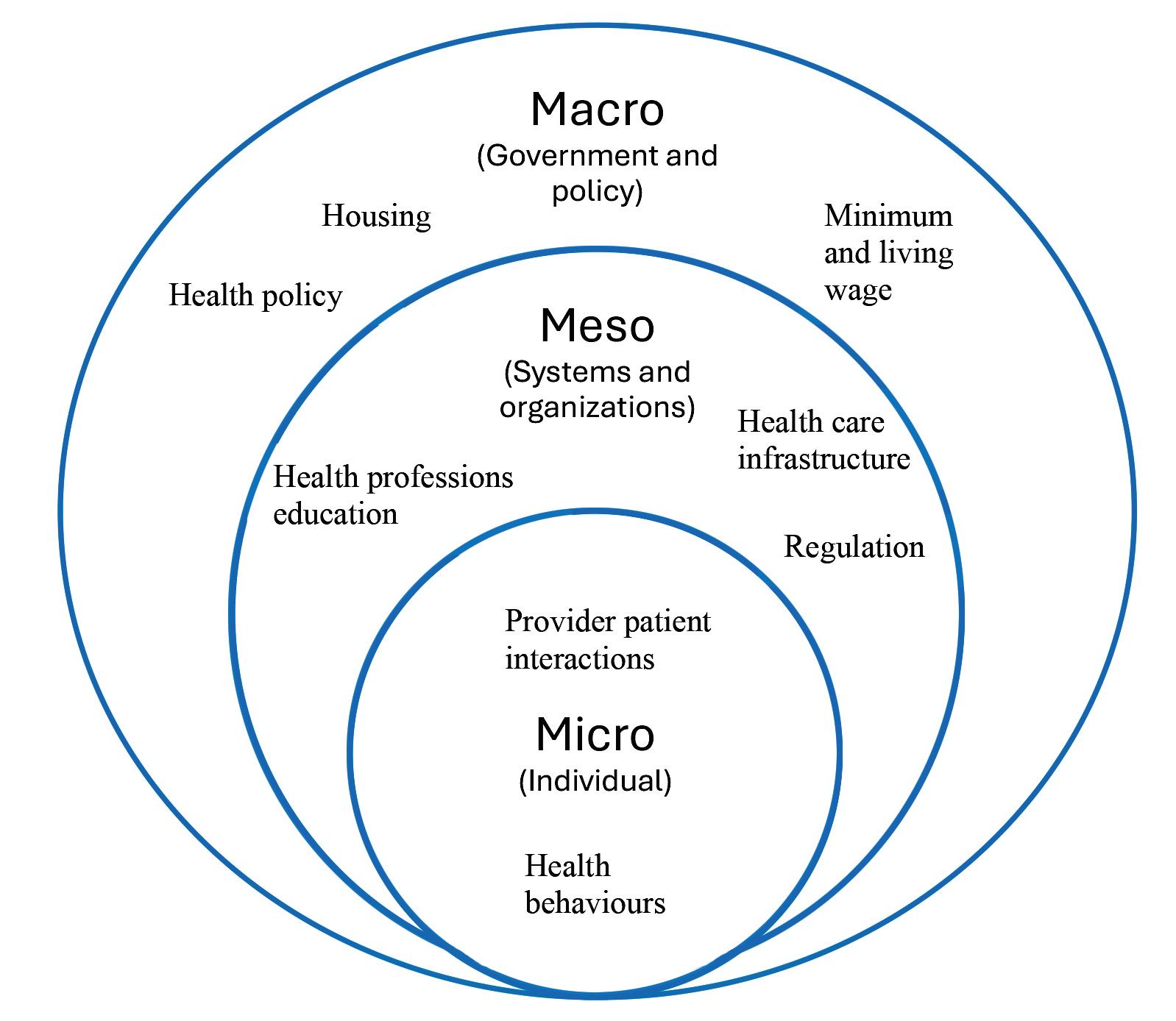
Literature on health and social justice points out that health, politics, and power interact at the micro- (i.e. individual), meso- (i.e. systems), and macro-levels (i.e. government and policy). At the micro-level, justice-enhancing healthcare requires that healthcare providers are prepared with the knowledge and skills needed to provide clinical care that is responsive to the individual-level impacts of systemic social inequities. Making justice-enhancing care possible requires that, at the meso-level, educational, regulatory, and professional organizations prepare healthcare providers and support health services that are trauma4-
Jennifer Brady PhD, RD is a Registered Dietitian and Associate Professor at Acadia University in Wolfville, Nova Scotia. She also lives with lymphedema and recently won a court battle with the Nova Scotia government for out-of-country surgery.
and harm-reduction informed5, weight-neutral6, culturally7 and structurally8 competent, accessible9, anti-racist10, gender-affirming11, and sex-positive.12 Justice-enhancing care further requires that healthcare providers and organizations advocate to redress the root causes of social inequities at the structural or macro level.13
Social inequities contribute to: a greater risk of developing lymphedema and with increased severity; delayed diagnoses and treatment; unaffordability of necessary medical supplies and therapies; and inaccessibility of quality lymphedema care. In the long term, social inequities lead to health disparities by setting some people on trajectories of worsening disease, deteriorating mental health, and socioeconomic conditions. To conceptualize what this means for lymphedema care, we must understand how social inequities shape the epidemiology, disease process, and accessibility and quality of care, as well as the lived experiences of lymphedema across diverse groups of people.
Yet, gaps in lymphedema research mean that we do not fully understand the relationship between social inequities and lymphedema. I wish to highlight some gaps in knowledge and care that have shaped my experience with lymphedema and that hinder socially just lymphedema care.
Income
Income has a profound and direct effect on health outcomes and a modulating effect on the impact of other social inequities.1 Low-income women are nearly twice as likely to develop lymphedema.14 Compression garments, bandaging, and manual lymphatic drainage are costly and often out-of-pocket expenses. Thus, income also likely modulates the social stigma of lymphedema with those of higher incomes able to afford various compression garment options and clothing that fit and/or conceal swollen areas of the body. At advanced stages, lymphedema may further mean loss of or reduced employment, which makes lymphedema care even less affordable, and increases social stigma of being un- or under-employed as a result of the disease.
Personally, I have no coverage for compression garments through my employer’s health benefits or my provincial health insurance. I was advised to try different sizes, styles, classes, and brands of compression garments to explore what worked best to manage my symptoms. Despite having a secure, well-paying job, this trial and error approach to purchasing various garments
at $420 per pair is not a realistic or equitable option. Healthcare providers involved in lymphedema care need to be more aware of and engaged in redressing income inequities that cause and are made worse by lymphedema. The lack of awareness and action among healthcare providers signals the need for changes in health professionals’
education and healthcare policy. Healthcare providers may also advocate for such changes, including: the inclusion of lymphedema care in health professionals’ education; coverage for garments and treatment by employers and provincial health insurance; and addressing inequities that impact lymphedema and health more widely (e.g., basic income guarantee15, living wage).
Attitudinal barriers, particularly those related to body weight, further hinder equitable, socially just lymphedema care.
Weight bias
Attitudinal barriers, particularly those related to body weight, further hinder equitable, socially just lymphedema care. Research shows that weight bias impairs patient-provider relationships, causes people in larger bodies to delay or avoid care for fear of body shaming from healthcare providers, results in patients being denied necessary care, increases internalized stigma and disordered eating behaviours, and overall, leads to adverse physical and mental health outcomes.16
Despite signs of lymphedema appearing soon after my cancer surgery, I was repeatedly told by my oncology team that the swelling would resolve and that I wouldn’t develop
lymphedema because I’m thin. When I later sought surgery to treat lymphedema, I was told that the worst thing I could do was gain weight. As someone with an eating disorder history and already struggling with the changes my body was undergoing as I healed from surgery and helplessly watched the swelling in my legs get worse, these experiences were devastating. While I do not face the same daily shame as those living in larger bodies, my experience is rooted in the same place, weight-based discrimination. Weight-neutral healthcare focuses on holistic and evidence-based health indicators, including diet, exercise, and stress management, rather than body weight or body mass index (BMI), which is ineffective for assessing health status,17 especially among racialized populations.18 Redressing weight bias and implementing weight neutral approaches to lymphedema care requires research, education, and advocacy on the part of healthcare providers, health professional programs, and policy makers.
Race and culture
Race and culture, or more accurately, racism and colonialism, are two additional social inequities that significantly impact racialized and Indigenous communities’ opportunities for health. Racism and colonialism are also gaps in Canadian lymphedema research. US-based research shows that Black/African Americans are nearly twice as likely19 to develop lymphedema and report a higher burden of unmet needs,20
namely lymphedema diagnosis and care, following cancer survivorship. Other research has found that Black, Hispanic, and Asian women have higher rates of lymphedema, experience worse swelling, and report lower quality of life as a result of lymphedema.21
The limited range of colour options in compression garments for diverse skin tones is emblematic of the lack of raciallyand culturally affirming care available to racialized and Indigenous people. Fewer colour options also add to the social stigma of lymphedema for racialized populations. I am acutely aware that, as difficult as living with lymphedema is for me as a white settler, it is even more challenging for racialized and Indigenous people whose dignity and needs are even more poorly served.
Gender and sexuality
Gender identity and sexuality are fundamental aspects of being human. Breast, gynecologic, and genitourinary cancer treatment are among the leading causes of secondary lymphedema. Lymphedema also has well documented negative sequalae on body image22 and gender presentation, particularly among the trans community.23 In this light, it is not surprising that research has found lymphedema to have significant deleterious impacts on sexual health.24 However, my experience suggests that this research is not being sufficiently translated to health professional practice in the context of lymphedema care. Relationships, intimacy, and sex are vitally important, but are too often overlooked by those responsible for caring for people with lymphedema.
The road ahead: what needs to change
As a volunteer-led organization, the CLF demonstrates leadership, partnership, collaboration, and innovation among its values, which guide its goals to advance awareness, access to care, and research through initiatives that center on the patient voice.25 Building on this important work, there may be opportunities to further explore principles of equity or justice as
components central to its work. Many health professionals and their respective regulatory bodies, educational institutions, and professional organizations have recognized equity and social justice as core responsibilities (e.g., in practice competencies, codes of ethics, regulatory documents, and training curricula). What could it mean if the CLF, and healthcare professionals providing lymphedema care considered power and inequity at the core of its educational and advocacy initiatives? Continued dialogue among those with lymphedema, their care providers, and organizations like the CLF can help shape a future of socially-just lymphedema care across micro-, meso-, and macro-levels. Healthcare providers are often uncomfortable taking on advocacy roles, especially when it involves speaking out
In a world where social inequities bear more heavily on health outcomes than health behaviours and services, promoting equitable access is critical.
for structural change on issues such as social inequities. Yet, improving the lives of those with lymphedema requires such change, and healthcare providers are key allies in bringing that about. I encourage readers to seek out the myriad resources available online regarding health professionals’ roles and responsibilities as advocates. Ultimately, lymphedema limits the full potential of those living with the disease— individuals who could otherwise contribute to society, given equitable, justice-enhancing
care. In a world where social inequities bear more heavily on health outcomes than health behaviours and services, promoting equitable access is critical. By working together, we can all help to remove barriers and support a socially just system that enables all with lymphedema to achieve their best possible health and well-being. LP
How to cite: Brady J. What is socially just lymphedema care? The roles and responsibilities of individuals and organizations. Pathways 2026;15(1):14-17. https://doi.org/10.70472/RAPW4552
Lymphedema
Certification coming to
Regina, SK, March 26 – April 1, 2026
Winnipeg, MB, November 8 – 14, 2026
TheKloseTrainingAdvantage
• 135-hours of lymphedema education
75-hr engaging online home study module 60-hr (6 1/2 day) classroom education
• Time-tested, effective and evidence-based curriculum
• Learn from the most experienced instructors in the field
• Fewer days away from home and work
• Greater flexibility to fit your personal schedule
• Exclusive post-graduate resources
• Special pricing for Canadian Therapists
Online Courses
• Breast Cancer Rehabilitation with Jodi Winicour, PT, CLT
• Strength After Breast Cancer with Katie Schmitz, PhD, MPH, FACSM
• Wound Management for CLTs with Jan Weiss, PT, DHS, CLT
• Head & Neck Lymphedema with Heidi Miranda-Walsh, OTR/L, CLT
• Elastic Taping for Lymphedema with Ruth Coopee, OTR/L, CLT
• Add’l courses at klosetraining.com
References can be found at https:// canadalymph.ca/pathways-references For more information: 1-303-245-0333 • info@klosetraining.com • klosetraining.com





