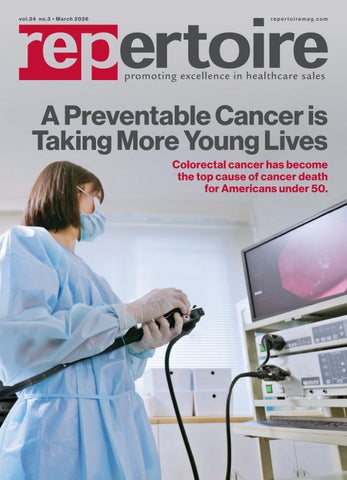

A Preventable Cancer is Taking More Young Lives
Colorectal cancer has become the top cause of cancer death for Americans under 50.



A Preventable Cancer is Taking More Young Lives
Clear,
How
Mark Van Sumeren’s latest book examines how business leaders can harness AI without surrendering professional judgment, ethics, or accountability.
The AMA launches new Center for Digital Health and AI. 42 Amazon’s One Medical Launches AI Health Assistant for Members
New tool aims to help patients navigate symptoms, appointments, and routine care through the One Medical platform.
Responding to Change APIC and SHEA create HIPAG to guide infection prevention priorities and dialogue within the industry.
As emergency department utilization grows, Vizient and Sg2 forecasts suggest hospitals must shift how patients access care
– using better metrics, smarter staffing and expanded ambulatory options to relieve ER congestion. 50 Supply Chain Leader Profile Jane Torzewski, RN, MAN, MBA, Director of Medical Device Contracting at Mayo Clinic.
Maintaining overall health helps protect the kidneys.
The State of Respiratory Season
While overall respiratory illness levels have dropped since January’s peak, flu-related emergency visits among school-aged children are rising, RSV remains elevated in many states, and COVID-19 activity is ticking up.
Turning Good Products Into Trusted Ones
Clear, consistent storytelling supports the reps who bring products to market and ensures a brand’s message is working even when its team isn’t in the room.
In a relationship driven industry like ours, success isn’t built in a single meeting or sales call. It’s built over time through familiarity, trust and ongoing communication.
As distributor reps, you sit at the center of that process. You’re managing multiple product lines, maintaining long-standing relationships, and helping customers make confident decisions every day. In the middle of all that, the information you consume, often quickly and between office visits, plays a bigger role than it may seem.

By Aili Casey
Good content builds familiarity long before a sales conversation happens. It answers questions before they’re asked. It gives reps something to reference, forward or lean on when explaining why one product stands out over another.
At its best, content marketing doesn’t feel like advertising. It feels useful. It makes products easier to understand, easier to remember, and easier to represent. For reps, that means confidence in the products and manufacturers you choose to bring into the conversation. For manufacturers, it means their message is present and working even when they aren’t in the room.
At Repertoire , we spend our days helping manufacturers connect and socialize with the distribution community. What we consistently see is that brands who invest in thoughtful, relevant content become easier to work with. Their story is clearer. Their value is easier to communicate. And their presence extends beyond a single touchpoint.
As our industry continues to evolve, understanding what content and advertising actually resonate with distributor reps matters more than ever. That’s why in our April issue, we’ll run our annual ad survey focused on how this audience engages with industry media. When you receive the survey, I hope you’ll take a few minutes to participate. Your feedback directly shapes the content you see and as a thank you, we’ll be giving away $100 to five respondents.
At the end of the day, even the best products don’t become great on their own. They become great when their story is told clearly, consistently, and in a way that supports the reps who bring them into the market. Marketing is what turns a strong product into a trusted one because a product can’t make an impact until people understand why it matters.
editorial staff
editor Graham Garrison ggarrison@sharemovingmedia.com
editor-in-chief, Dail-eNews Jenna Hughes jhughes@sharemovingmedia.com
content creator Pete Mercer pmercer@sharemovingmedia.com
art director Brent Cashman bcashman@sharemovingmedia.com
circulation Laura Gantert lgantert@sharemovingmedia.com
sales executive Aili Casey acasey@sharemovingmedia.com (404) 625-9156
publisher Scott Adams sadams@sharemovingmedia.com (800) 536.5312 x5256
founder Brian Taylor btaylor@sharemovingmedia.com
Subscriptions www.repertoiremag.com/subscribe or (800) 536-5312 x5259
Repertoire is published monthly by Share Moving Media 350 Town Center Ave, Ste 201 Suwanee, GA 30024-6914 Phone: (800) 536-5312, FAX: (770) 709-5432; e-mail: info@sharemovingmedia.com; www.sharemovingmedia.com

Every heartbeat matters. Every result counts.
From the lab to the bedside, QuidelOrtho delivers comprehensive cardiac testing solutions when time is critical.















QUIDEL™ TRIAGE™ System cardiac testing menu
QUIDEL cardiac


VITROS™ Systems cardiac testing menu
• NT-proBNP
• Myoglobin
• D-dimer*
• Homocysteine
• Wide-range CRP*
• Apolipoprotein A
• Apolipoprotein B


• Cholesterol
• CK
• CK-MB
• Direct HDL
• Direct LDL
• Lipoprotein(a)*
• Triglycerides









Owning the “Oops”
Why admitting mistakes fast, asking better questions and knowing your limits are essential skills for every consultant.
 This month I plan to take us down a dark road that most of us are uncomfortable experiencing or talking about. I plan to explore what happens when consulting goes “oops.”
As consultants to our customers and trusted members of our communities, we are often called upon to provide guidance on CLIA, reimbursement, test mix selection, legislation affecting the laboratory business, and many other areas.
For the most part, we take our time, consider the situation, the source and how much information is needed, then come up with a thoughtful answer that fits the need. To be thorough, we often seek confirmation from our trusted manufacturing partners.

By Jim Poggi

We need to be mindful to provide the right amount and balance of information. Is it accurate? Does it fully answer the question? Is it explained so the person asking the question can understand it? Does it need and have supporting data? Is it actionable?
Why actionable? This may be the most important element. Most people do not ask us questions out of boredom. They ask because they need information to take action. Therefore, we also need to understand that when consulting goes “oops,” the person asking the question may take inappropriate action.
Admitting a mistake
This leads to my first rule of admitting we have screwed up: admit the mistake as soon as possible. While painful, this can eliminate or minimize more painful downstream consequences. If you are lucky, the person who asked for help did not take action yet.
If they have already taken action, there may still be time to minimize or blunt the damage of inaccurate advice by quickly helping the person who asked for information to retract it if possible. “Upon further reflection” and “after consulting other sources” are usually acceptable

ways to honestly admit an error without falling on your sword more than necessary.
If possible, offer to help the questioner correct the error. They may ask you to discuss it with their staff, the person who asked them for advice, etc. There are a lot of permutations, but your offer to directly address the issue should be helpful in most situations.
Know thyself
Now let’s step back and remember something we have heard many times before: “an ounce of prevention is better than a pound of cure.”
How do we apply that advice here? By knowing ourselves. When are we most likely to offer off-hand information without thinking or doing the right amount of research? I know my weaknesses. There are two times I am likely to fall into this trap. First, when I am on a roll and at my most confident, I sometimes confuse myself with some omniscient being. Offering bad advice at that time has had the effect of helping me to become more appropriately humble. Like it or not, overconfidence should be self-correcting. It is in my case.
The second scenario where I sometimes make unforced errors is when I am tired, distracted or not at the top of my game. For me, fortunately at these times I am more likely to respond “let me get back to you.”
The message here is not necessarily to share more about when I am liable to screw up, but to offer you the opportunity for self-reflection so you can honestly ask yourself when you are likely to make the same
sorts of errors. Knowing when you should pause and offer a little time before you answer the question saves a lot of heartache and a lot of apologies. For every active consultant, it is a secret weapon we should use daily.
An “oops” example
Now that most of us can admit we are not infallible and that people who ask us for consultation deserve the best possible solution, let’s play out an “oops” in this
column, where we can actually do no harm to ourselves or others.
In this scenario, we are asked for the best variety of tests a new lab should have. Without reflecting or asking questions for clarity (because we need to screw up here), we offer a variety of waived respiratory and basic metabolic tests. We know these meet most new or small lab needs and serve as building blocks to future testing. What we did not know and failed to ask was that this is a
Forgive yourself. It may sound self-evident, but it is not. Obsessing over a screw up is not a useful way to spend your time and does nothing for your overall sense of well-being. Take the lesson you have learned, incorporate it into your daily life and move on.

urology practice, and the practice manager is new and does not yet know enough to realize our error. Clearly, our advice does not suit a urology practice.
Once we learn the type of practice, we will realize we have offered inappropriate advice. Now comes the opportunity to fix the problem before it gets out of hand rather than delay and make the situation worse. Speed is your friend here. As soon as you realize your error, immediately contact the person who asked you the question and admit: “I did not ask the right questions about the medical practice you manage to provide you with the proper advice. Can we set up some time to sit down together and for me to learn from you more about the medical practice you manage?”
If you are very lucky, they have not already shared your first thoughts with the clinical team. If they have shared this information, it is likely they were told the information is wrong and been embarrassed. In that latter case, while an apology to the questioner is mandatory, offer to share your apology with the clinical team.
In my experience, when this sort of bad information gets back to the clinical team, they have already written you off (at least temporarily) as a source of useful information. Relationship building typically needs to start back at ground zero. In this case, take a step back and ask the practice manager for a new introductory meeting to start over. If possible, contact as many of the clinical team members you can, admit the error, apologize and offer a new, proper list of tests.
PHASE respiratory diagnostics
Built for high-pressure seasons
This respiratory season is shaping up to be one of the most severe in recent years. As patient volumes rise and symptoms overlap, clinicians need tools that support fast, confident decision-making—without adding complexity to care delivery.
PHASE delivers a respiratory diagnostics portfolio built for real-world pressure across today’s care settings.

Rapid respiratory detection at the point of care
CLIA-waived
Why it matters
→ Supports timely identification of respiratory infections
→ Helps clinicians evaluate symptomatic patients during high seasonal demand
→ Designed for use across a variety of care settings
INDICAID enables rapid respiratory assessment when speed and efficiency are critical.
Built for today’s season—and what comes next
From rapid respiratory detection to tools that support treatment decision-making, PHASE respiratory diagnostics are built to support confident care when it matters most.

Rapid clinical insight at the point of care
Moderate Complexity
When respiratory symptoms overlap, understanding whether an infection is bacterial or non-bacterial is critical to patient management.
Why it matters
→ Supports differentiation of bacterial versus non-bacterial acute respiratory infections
→ Helps guide appropriate treatment decisions
→ Reinforces antimicrobial stewardship during peak respiratory burden
Key highlights:
→ Supports appropriate antibiotic use
→ Results after 10 minutes
→ Designed for moderate complexity settings
→ Ideal for Urgent Care and Emergency Departments
In partnership with Lumos Diagnostics
Yes, you are in a deep hole, but remember that errors are unavoidable and your job is to recover from this one as quickly as possible. If the bad information has not gotten to the clinical team, set up the meeting with your practice manager and offer one of your trusted lab manufacturers as support.
In either case, you should have observed a few things:
` Avoid offering information without asking the right questions
` Be reflective of answers you may have already given (search your memory to make sure you have given proper advice),
` Correct errors immediately
` Offer apologies to any folks who may have been impacted by your advice.
I will offer a few tips that work for me. First, if you have a good coach, give them a call. Let them know what happened and how you tried to rectify the situation. Ask for their advice on any further steps you need to take. Consider any actions you may have missed. They are your coach for a reason.
At this point, the best coaches will know you are feeling a little down and will offer suggestions about how to get back in good order. If they don’t, ask them for ways to get out of your funk. Just having that discussion usually makes me feel better, and my coach usually offers some quality discussion topics to distract me and get my mind off of the mess up. Spending quality time with our family, friends and colleagues
Just like “no” is the pathway to “yes” once you learn how to respond to a “no” from a customer, “oops” is a way to make us stronger. No one ever plans to make a mistake, but when you do, learn from it and carry on.
How to reset after a mistake OK, so now our fictitious “oops” example is over. Whew. If you are like me, you may have remembered a similar situation and have cringed a bit. We have discussed how to get the person who asked the question back in good order, but what about ourselves? We have given bad advice, needed to apologize to one or more customers, provided new advice (if possible) and have put a customer at risk.
Most of us need to take care of ourselves a bit to regain our equilibrium. How do we do so?
is also a time proven way to cheer up. We all know we feel energized after a sales meeting. Catch up with some of your favorite fellow account managers and feel their energy. It’s sure to help. Forgive yourself. It may sound self-evident, but it is not. Obsessing over a screw up is not a useful way to spend your time and does nothing for your overall sense of well-being. Take the lesson you have learned, incorporate it into your daily life and move on.
Another way I get my good spirits back is to engage in
activities I enjoy and know I am good at. Writing this column is always a day brightener. So is researching new lab technology or taking a break to read the latest lab journals. Each of these activities helps me to get my positive energy back. Your list may be different, but be sure to engage in activities you enjoy.
Finally, allow a little time to create distance from your “oops.” It’s funny how time creates a sense of perspective. Don’t obsess over your mistake and, when the time is right, re-engage with the person who asked for your advice and let them know you are prepared to set things right and move on if they are.
Sometimes a thoughtful note (not an email) helps to set the tone for rebuilding your relationship. Maybe you can ask a mutual contact to step in and smooth the path. We are all creative or we would be in a different business.
There are a number of ways of putting positive energy back into a damaged relationship. Add your thoughts to those I have offered and you will build back as many as possible. Just like “no” is the pathway to “yes” once you learn how to respond to a “no” from a customer, “oops” is a way to make us stronger. No one ever plans to make a mistake, but when you do, learn from it and carry on.
“Oops” may feel bad for a while, but if we carry the lesson forward, we will become better at our consulting activities and better friends and family members. Here’s hoping it is a rare experience for you, but that you extract all the value you can from each “oops” in your life.
1 CBC/Day or

10,000 CBC/Day

Sysmex has the most reliable hematology solution for any lab.

3,000+
XN-L placements in the U.S.
26 years Sysmex has rated highest for System Reliability.*
1 hematology solution for all your customers.
XN-330™ Automated Hematology Analyzer
XN-9100™ Automated Hematology System
The Sales Professional’s Creed: If I Were a Pro Athlete, Would I
Be Cut?
Reps say they want to earn like professionals. But do they train, recover and review like one?
By Brian Sullivan
 Let’s be honest – if your sales career were a tryout, would you make the team?
Not “the team” as in “you have a territory and a line card.” The team – as in the starting lineup. First call on the new facility. The rep they trust when the contract is on the line.
Every salesperson loves to say they’re a “sales professional.” But here’s the question most won’t ask: Would your habits – your preparation, training and mindset – actually earn you a spot? Or would you be riding the bench, waiting to get cut when a competitor outhustles you at the hospital, the surgery center, or the long-term care facility down the road?
Here’s the thing: pros don’t just show up and play. They prepare.
They watch film. They condition. They recover. They rehearse. And they do it every damn day – without someone begging them to.
Let’s call it what it is: most reps aren’t professionals. They’re recreational players with a quota.
Want the money?
Match the mindset.
A pro athlete gets paid based on production. So do you. They wake up thinking about how to get 1%
better – faster, sharper and more durable. You should too.
I don’t have a study for this, but after two decades in sales rooms, here’s my gut: if we judged medical distribution reps the way we judge athletes, 80% would be cut by the second week of camp. Another 10% would get called up on “potential.” And the top 10%? They’d dominate – because they act like professionals before they earn like professionals.

It’s not about talent. It’s about how you train between calls and contract cycles.
Want to raise your game? Steal these habits from the pros
1 Practice more than you perform In sports, the ratio is obvious: 90% training, 10% game time. In medical distribution? Most reps barely practice at all.
What would a closer have done differently?
Here’s the uncomfortable truth: reps who avoid watching themselves usually have the most to learn.
3 Recover like it matters Ever notice how your voice flattens after a day of running between hospitals, physician offices, and surgery centers? That’s not burnout – that’s
In medical distribution, it’s easy to hide behind relationships and legacy contracts.
“They love me over there” becomes an excuse to stop sharpening the blade.
Audit yourself: When was the last time you rehearsed your opener for a new account? Dry-ran a pitch before a value-analysis meeting? Roleplayed your toughest conversion objection until you owned it?
If you’re winging it in front of directors and materials managers, you’re not a pro. You’re hoping. And hope is not a strategy –it’s a prayer with a quota attached.
2 Watch the tape. Every week. Pro athletes watch film – a lot of it. Why? Because growth doesn’t come from experience alone. It comes from studied experience. Review one recorded call per week. With a peer or manager. No skipping. Ask yourself: Where did I lose energy? Where did I take a shortcut?
depletion. Athletes call it “leaving it on the field.” You’re doing it every Tuesday by 2 p.m. Groggy reps skip questions and miss buying signals. Stress from a tough call at the longterm care facility bleeds into your next stop – and customers hear it.
You want more share? Fix your fuel tank first.
4 Have a pre-game routine Athletes don’t jog into the stadium and start scoring. They warm up. Stretch. Lock in mentally before the whistle.
Your version: Review your call plan before you walk in. Set one learning goal. Visualize the objection you fear most – whether it’s from a CNO, a materials director or a practice manager.
Write down a question you haven’t asked yet this week. No more “let’s see how it goes.” That’s amateur hour.
5 Train with people who push you
Ask any athlete – your environment shapes your output. Sit next to lazy reps, you become one. Train with closers, you get better. Find one training partner –someone who’ll roleplay and debrief calls with you weekly. Spend more time with reps who make you feel behind, not comfortable.
In medical distribution, it’s easy to hide behind relationships and legacy contracts. “They love me over there” becomes an excuse to stop sharpening the blade. But that friction – competing with sharper reps, getting called out – that’s where breakthroughs live.
Start acting like you’re under contract
Professional athletes don’t wait to be told to train. They do it because not training means losing the job, the income, the dream. Medical distribution is no different.
If you’re going to call yourself a sales professional, back it up. Show me your calendar. Show me your pre-call plans. Show me how you recover from losses and prep for wins.
You might not wear a jersey. But the minute you decide to train like you’re under contract, you’ll start performing like you deserve the big one.
Brian Sullivan, CSP, is the founder of PRECISE Selling, where he helps companies train, coach, and develop top-tier sales talent in medical and healthcare distribution. Learn more at preciseselling.com.


Managing Resistance
How shifting language away from the customer and toward the issue helps sales leaders defuse negativity and build alignment.
By Patrick T. Malone
 No matter how skillful your sales presentation is, distribution reps are likely to encounter negative reactions. When dealing with negative attitudes, reps must stay focused on their goal and realize the customers with negative attitudes are not rejecting the rep or their goal. The customer’s negativity is mostly directed at the plan and/or the strategy for achieving the goal.
In other words, they are resisting “it” (the plan/strategy) and not “you” (the rep). If you look at negative attitudes in this manner, you can maintain the confidence necessary to acknowledge the customer’s point of view and align with even the most emotional negative attitudes, When responding to negative customers, avoid saying “I know how you feel,” “You sound frustrated,” or “You seem skeptical.” Instead, take the “you” out of the response and focus on the issue by using “it.” For example: “that appears to be a problem,” “it can be frustrating,” or “skepticism is perfectly understandable.”
Switching pronouns from you to it may seem like a small thing now, but in a sales leadership interaction, this simple act is extremely powerful in helping your customers separate themselves from the problem at hand. Utilizing terms such as I and you often create a competitive win/lose battle by causing problems to become internalized. “If I can prove my
point, will you drop yours” is a terrible sales strategy and a game no customer wants to play.
“It” problems, not people
Using “it” puts the focus on the issues and concerns. Instead of problems becoming people problems, you turn all issues and problems into it. By removing you from the discussion and triangulating from you and me to “it”, all issues and problems become an “it” and aligning begins – you and me versus it.
Consider these triangulated examples: Customer: “Why bother? At my age I’m not interested in increasing my workload or adding staff.”
Rep: Sounds like that isn’t a priority. What are the priorities at this moment in time?
Customer: “AI is not beneficial in a primary care practice. It doesn’t work.”
Rep: It is disappointing when a plan doesn’t work. So, let’s look at some of the more proven effective and less expensive ways to lighten the workload in practice.
Customer: “I’d be uncomfortable investing a lot of money in disaster preparedness for a 100-year event that may or may not occur. Rep: It appears that could be a risky situation so let’s explore some ways to mitigate the risk.
Customer: “I’m not cutting my margin just to keep a few price shoppers. Let them go to Drug Mart.”
Key points
1. Negative reactions are about the plan – not the rep
Customers with negative attitudes are usually resisting the strategy or proposal, not the salesperson personally. Viewing resistance as “it” rather than “you” helps reps stay confident, objective, and aligned.
Your personal and professional success hinges on your ability to align a full range of negative and positive attitudes.
Rep: Got it. Margins are important so let’s stop here and explore the options for protecting the pharmacy business without drastically impacting margins.
Customer: “You are going to have to prove to me that investing more in primary care will ease the burden on emergency rooms”
Rep: Looks like more proof is needed before proceeding and that is fine. Let’s review the performance of some of the hospitals that have implemented the program then determine if it would work in this practice.
Working all the angles
Effective sales leaders are skillful at working with all the
possible negative attitudes and it is certainly easier to do business with customers who are open or positively inclined. However, the most successful sales leaders can influence conversations even when they turn negative.
Your personal and professional success hinges on your ability to align a full range of negative and positive attitudes. Depersonalization is a key component of that competency. Try it and find out for yourself.
If you’re still having difficulty managing a specific point of resistance, send me your customer’s actual negative response plus background on the situation and I will send you some recommended responses for your consideration.
2. Shift language from “you” to “it” to reduce defensiveness
Removing “you” from responses and focusing on the issue (“it can be frustrating,” “that appears to be a problem”) helps depersonalize the conversation and prevents a win/lose dynamic.
3. Triangulation creates alignment, not confrontation
Reframing objections as you and me versus it turns tension into collaboration. This approach keeps discussions focused on solving the problem rather than proving a point.
Patrick Malone is a leadership mentor and independent business advisor with over 40 years of experience. Malone started in customer service with American Greetings in Cleveland, Ohio, where he worked his way up to the role of vice president for the Southeast region. In the last 20 years, he’s worked with a company called The PAR Group, focusing on sales leadership development. Most recently, he’s hosted several live talk radio shows in a two-hour block every weekday morning. To contact Pat, email ptm4936@gmail.com.
Strategic Leadership in the Age of AI
Mark Van Sumeren’s latest book examines how business leaders can harness AI without surrendering professional judgment, ethics or accountability
By Pete Mercer
 Artificial intelligence (AI) is here. Over the last few years, we have seen it explode from a conceptual idea to a widely used and applicated tool, with varying degrees of success. Sure, it’s not perfect – but it is prevalent, and people are using it to make important decisions, often at an alarming rate. The ability to make strategic decisions is integral to being a leader, and it’s even more important to discern the best way to build a strategy in today’s market.
Leaders are at a crossroads where they must decide whether or not they’re going to adopt artificial intelligence, and then they must decide where artificial intelligence is going to be implemented and how much the team is expected to rely on it. Setting those parameters from the outset of this journey is critical, giving your team a very clear understanding of how it’s going to be used and why.
Repertoire Magazine sat down with Mark Van Sumeren to discuss his newest book, “A Return to Strategic Leadership: Judgment in the Age of AI”, how the growth of artificial intelligence is
Diagnostics that deliver, wherever care happens






























































From large hospitals to non-acute care settings, Siemens Healthineers delivers a comprehensive portfolio of laboratory diagnostics solutions — from cutting-edge analyzers to a broad menu of high-quality assays. Wherever care happens, our diagnostics deliver trusted results that empower clinical decisions and improve patient outcomes. siemens-healthineers.us





Atellica CI Analyzer Integrated Chemistry and Immunoassay
Immulite 2000 XPi Immunoassay and Allergy
CA-660 Coagulation
Connect with a representative from Siemens Healthineers to learn more.
going to impact business leadership and what strategy looks like in the face of AI.
Creating fiction from fact
“A Return to Strategic Leadership” is a fictional business novel that looks at the all-too-real world scenarios that business leaders are facing with artificial intelligence today. It follows retired Bill Ellis, a former executive in the medical device manufacturing business, as he grapples with business decisions where artificial intelligence points one way, while his years of experience and sense of ethical responsibility point another.
second book. Once artificial intelligence started to become widely accepted and applied in business settings, though, he began to develop the next steps in Bill Ellis’ journey.
He said, “Just from watching how artificial intelligence went from hype and conceptual to reality this year, bringing with it a lot of anxiety, consternation and uncertainty, I began to develop an idea. I thought that now was the time to write about it, so I had a topic for my second book.”
With this book, Van Sumeren is hoping to give business leaders a roadmap on how to navigate
For those who are looking to fold artificial intelligence into their decision-making and strategy building processes, it’s important to take it slow at first. Van Sumeren said, “I see a lot of people getting their toes in the water, trying to understand it and getting familiar with it first. From there, they can do some lower-level tactical things with it, as opposed to bigger picture stuff.”
This book is the second in a series of business novels where Van Sumeren is using his lived experience to craft narratives around real-life business challenges and what it looks like to navigate those as a business leader.
After writing the first book, “A ‘Trip’ to Strategic Leadership”, wherein Bill Ellis goes on a selfawakening journey to learn about his shortcomings as a leader and how that ultimately impacts his business and employees, Van Sumeren didn’t immediately have a topic he wanted to cover in the
and even use artificial intelligence to build business strategies. While the use of artificial intelligence is pretty divisive, there are ways to apply it to business decisions without compromising any ethical boundaries or replacing the human element.
It’s all about challenging and checking the information that the artificial intelligence provides. Van Sumeren said, “Think of the algorithm as a very smart analyst that has several years of experience –despite that experience, you’re not going to just accept what it has to say on face value. You have to test
it, probe it, challenge it, rework it, send them back to do it again because of things that they’ve missed, and then come back with the right answer. It’s no different than what you’ve been doing; it’s just faster.”
Leveraging AI as a strategic tool
Building a strategy is a crucial part of the business leader’s journey – it’s rarely easy to get it right, but a good strategy can make a significant difference for how an organization operates. When it comes to artificial intelligence, it’s important to remember that while it can be used as a tool to improve efficiency and productivity, it also carries a certain amount of risk. Certain people are afraid of losing their livelihoods to artificial intelligence, while others, Van Sumeren included, are concerned about how artificial intelligence is being used ethically.
“My biggest fear is not that it’s taking people’s jobs, because I think it can do some things to save time,” he said. “But to get real value out of it, there’s a higher order of activity that needs to be applied to it that can actually increase the skill demands for the people that are using it right. If you’re using it to accomplish a task, but you’re not applying professional judgement to it, it’s going to take you down a path that is wrong and inappropriate.”
One of the ideas he uses in the book is that “technology amplifies everything, including the character of the people using it.” This idea that technology can positively or negatively impact people is compelling, especially for a novel. Van Sumeren said, “In the wrong hands, AI can
really do damage. If we apply filters of human morality and ethics it can be effective, but if we leave that filter off, it can do a lot of damage.”
For those who are looking to fold artificial intelligence into their decision-making and strategy building processes, it’s important to take it slow at first. Van Sumeren said, “I see a lot of people getting their toes in the water, trying to understand it and getting
familiar with it first. From there, they can do some lower-level tactical things with it, as opposed to bigger picture stuff.”
For those already well into their journey, Van Sumeren advocates four key pillars to successful AI adoption:
` Curated data – building the AI on information of the highest quality, rather than internet scrapping of questionable data
About Mark Van Sumeren
Mark Van Sumeren has devoted his nearly forty-year career to listening to and advising healthcare leaders, as they tackle the challenges of an ever-changing industry. His work has helped senior leadership teams make sense of market dynamics; define and strengthen competitive advantages; secure organic and inorganic growth; and, shape corporate strategy. Mark’s clients have included executives and directors of hospitals, health systems, medical device manufacturers and service providers, ranging from $1M to $9B in annual sales.
Mark currently serves in retained advisory and governance roles with selective, growth-oriented health care services companies. His passion is to bring a broad industry perspective and strong strategic insights, to enhance organizational performance. Mark’s mission is to encourage profitable growth for those companies that he serves.
When not addressing business issues, Mark spends his time following his favorite teams - University of Michigan football, Detriot Tigers baseball, Green Bay Packers, as well as in joining his wife of 34 years, Kate, in spoiling their three grandchildren.
` Probing questions – precise questions that sharpen the inquiry
` Ethical oversight – values that put guardrails on its use and application
` Professional judgment – the expertise needed to turn the output into meaningful decisions.
In his book, Van Sumeren wrote: “Machines accelerate thought; only humans ensure that thought means something.”

A Preventable Cancer is Taking More Young Lives
Colorectal cancer has become the top cause of cancer death for Americans under 50, even as deaths from lung, breast and other cancers decline, raising the stakes for screening, advocacy and health equity.
Anew study from the American Cancer Society (ACS) reveals that cancer mortality among Americans under age 50 has dropped sharply overall, but one disease bucks the trend.
According to research published Jan. 22 in the Journal of the American Medical Association, the U.S. cancer death rate for people younger than 50 fell by 44% from 25.5 per 100,000 in 1990 to 14.2 per 100,000 in 2023 – largely due to significant decreases in deaths from lung, breast, brain cancers, and leukemia.
However, colorectal cancer was the lone exception, rising steadily and becoming the leading cause of cancer death in this age group in 2023 after increasing 1.1% per year since 2005.
Rebecca Siegel, MPH, senior scientific director of surveillance research at the ACS and lead author of the report, said: “The steady rise in colorectal deaths under 50 is even more alarming compared to the dramatic declines for lung and breast, even as breast cancer incidence is climbing.”
Siegel added that while the reasons for the rising numbers remain unclear, “lives can be saved now through symptom awareness and destigmatization, and more screening uptake, as three in four people under 50 are diagnosed with advanced disease.”


Preventable Cancer
For the study, scientists analyzed trends in the annual numbers of cancer deaths and agestandardized rates per 100,000 men and women aged 0-49 years for the top 5 cancer-related deaths during 1990-2023 in the U.S. They used data from the National Center for Health Statistics as provided by the Surveillance, Epidemiology, and End Results (SEER) program at the National Cancer Institute.
The ACS said results showed that 1,267,520 people died from cancer in the U.S. before age 50 from 1990 through 2023, and the overall death rate decreased by 44%. Four of the five leading causes of cancer death decreased, with the average annual decline during 2014-2023 ranging from 0.3% for brain cancer and 1.4% for breast cancer to 2.3% for leukemia and 5.7% for lung cancer.
men mirrored the overall pattern, with breast cancer replaced by non-Hodgkin lymphoma (4th) in 1990 and pancreatic cancer (5th) in 2023.
“We weren’t expecting colorectal cancer to rise to this level so quickly, but now it is clear that this can no longer be called an old person’s disease. We must double down on research to pinpoint what is driving this tsunami of cancer in generations born since 1950,” said Dr. Ahmedin Jemal, senior vice president, surveillance, prevention, and health services research at the ACS and senior author of the study. “In the meantime, people 45-49 years make up 50% of diagnoses under 50, so increased screening uptake will prevent disease as well as death.”
Catching it early
CRC is one of the most preventable and treatable cancers when
“Fight CRC pushes systemic solutions such as mailed outreach, patient navigation, no cost follow up for diagnostic colonoscopy and state level quality measures so that noninvasive testing translates into timely diagnosis and care.”
Only CRC mortality increased annually for people under 50. Lung cancer and leukemia dropped from ranking first to fourth and third to fifth, respectively, whereas breast cancer remained the second leading cancer death overall and first in women. Cervical cancer ranked third in women in 1990 and 2023, despite a continuous decline throughout the study period. The cancer distribution in
found early, according to the Centers for Disease Control and Prevention (CDC). That’s in part because CRC grows slowly, often starting as a small, noncancerous polyp. Over time, some polyps can turn into cancer.
Another reason why early screening is so essential: Colorectal cancer often produces no early warning signs, especially for adults age 45 and older, the CDC says.
When symptoms do occur, they may include persistent changes in bowel habits, such as diarrhea or constipation; blood in or on the stool; a feeling that the bowel does not empty completely; ongoing abdominal pain, cramps or aches; and unexplained weight loss. Because these signs can also stem from non-cancer causes, health officials urge individuals experiencing any of them to consult a clinician promptly.
Health experts stress that multiple colorectal cancer screening options are available, allowing patients and providers to choose an approach that fits individual risk, preferences, and access to care. Screening tests generally fall into two categories: stool-based tests and visual exams of the colon and rectum.
Stool-based tests are noninvasive and can be completed at home. These include the fecal immunochemical test (FIT) and guaiac-based fecal occult blood test (gFOBT), which look for hidden blood in the stool, as well as FIT-DNA tests, which detect both blood and abnormal DNA linked to cancer or polyps. These tests are typically repeated every one to three years, depending on the method used. A positive result requires follow-up with a diagnostic colonoscopy.
Visual exams allow clinicians to directly examine the colon. Colonoscopy, considered the most comprehensive option, enables providers to detect and remove precancerous polyps during the same procedure and is usually performed every 10 years for average-risk adults. Other options include flexible sigmoidoscopy and CT colonography, also known as virtual colonoscopy, which are performed at shorter intervals.
Advocacy efforts
The increase in colorectal cancer among younger adults is shifting public health toward earlier screening, better symptom recognition and risk-based approaches, said Anjee Davis, CEO of Fight Colorectal Cancer, an organization that works to empower individuals, influence policy, and accelerate breakthroughs that improve prevention, care and outcomes.
Fight CRC’s efforts include educating providers and the public, expanding digital navigation tools, and advocating for coverage reforms so people ages 45 to 49 and symptomatic younger patients are identified and tested promptly.
Fight CRC’s advocacy program mobilizes patients, caregivers and supporters to influence public policy at both the federal and state levels. Through initiatives such as Call-on Congress and the State Catalyst Program, advocates receive training and tools to engage lawmakers on issues including access to screening, affordability of care and research funding. These efforts ensure that colorectal cancer remains a visible priority in health policy discussions.
Fight CRC also plays a significant role in advancing research and innovation. The organization supports research focused on prevention, early detection and treatment, while emphasizing patient involvement in the scientific process. Its Research Advocacy Training and Support (RATS) program equips advocates to participate in clinical trial design, advisory panels and funding decisions, helping ensure that research reflects real-world patient needs.
In addition, Fight CRC offers a range of education and support resources for patients and caregivers navigating a colorectal cancer diagnosis. These include medically reviewed educational materials, community connections, and digital tools such as ChatCRC, an AI-powered chatbot designed to provide personalized
guidance on screening, treatment options, and survivorship.
Community engagement and awareness are further strengthened through national campaigns and events, including United in Blue during Colorectal Cancer Awareness Month and signature fundraising initiatives like Climb for a Cure.

An AI-enabled patient chat for colorectal cancer patients and caregivers
Davis said technology will make screening and diagnosis more accurate, less invasive, and more personalized. Even initial outreach efforts can be boosted by the latest advances in communication tools.
Fight Colorectal Cancer’s AI-enabled patient chat, ChatCRC, is an artificial intelligence–powered chatbot created to support people affected by colorectal cancer – including patients, caregivers and clinicians – by providing accurate, accessible information and personalized responses related to colorectal cancer prevention, screening, diagnosis, treatment and care management. ChatCRC delivers 24/7 interactive support, helping users ask questions and receive immediate answers about topics like risk factors, screening options, treatment side effects, wellness strategies and available resources. It’s designed to remove complex medical jargon so information is easier to understand, and it can even be accessed by SMS text message for users without internet access.
While the tool provides tailored information and connects users with educational resources, clinical trial info and support groups, it does not offer medical advice or replace consultation with a healthcare provider.
Together, these programs reflect Fight CRC’s comprehensive approach: driving policy change, accelerating research, and supporting patients at every stage of their journey. As colorectal cancer rates continue to rise, particularly among younger adults, the organization’s multifaceted strategy aims to ensure that progress keeps pace with the growing need.
Addressing disparities and gaps
Disparities in colorectal cancer risk and outcomes across different populations or regions are both large and avoidable, said Fight CRC’s Davis. Black, Hispanic, rural, low income and uninsured communities shoulder a disproportionate burden.
patient navigation, no cost follow up for diagnostic colonoscopy and state level quality measures so that noninvasive testing translates into timely diagnosis and care,” she said. “These barriers are most acute where Medicaid expansion and coverage policies vary.”
At the national level, the CDC’s Colorectal Cancer Control Program (CRCCP) is driving measurable increases in colorectal cancer screening by partnering with clinics, hospitals and other health care organizations to implement proven strategies that help detect cancer early and save lives.
The CRCCP targets adults aged 45 to 75, particularly in clinics where fewer than 60% of patients are up to date on screening –often in lower-income or medically underserved communities.
With effective screening tools, proven public health strategies and growing advocacy to expand access and awareness, experts say the means to reverse this trend already exist.
“Fight CRC advances health equity by targeting resources and culturally appropriate education to clinics and communities that need them most and by pushing state and federal policy to close coverage and access gaps,” she said. “This is evident in places with constrained or limited access to endoscopy.”
Davis said barriers to care for younger patients are practical and solvable: cost, access, awareness, provider recommendation and follow up after abnormal tests.
“Fight CRC pushes systemic solutions such as mailed outreach,
At the heart of the program are evidence-based interventions recommended by the Guide to Community Preventive Services. These include regular assessment and feedback to healthcare providers on their screening recommendations, electronic or written provider reminders for due or overdue tests, and targeted patient reminders via mail, email or phone.
The CRCCP also works to remove structural barriers that can hinder screening access. Efforts range from extending clinic hours and offering stool
tests in nonclinical settings like vaccination sites to providing patient navigation services, transportation, childcare and simplified paperwork, all aimed at making screening more accessible and less burdensome. By collecting and analyzing clinic data, the CDC says it can identify where screening gaps remain and adjust strategies to maximize impact. Public health evaluations indicate that these interventions have increased screening rates, particularly in clinics serving underserved populations, though challenges remain in closing gaps across all regions.
Health officials emphasize that increasing colorectal cancer screening not only saves lives by detecting precancerous conditions early but also reduces long-term health care costs, lost wages and the burden on patients, employers and insurers.
In a compelling example of the CRCCP’s real-world impact, a free clinic in West Virginia dramatically increased its screening rate through tailored interventions supported by CDC funding. At Wheeling Health Right, only 9% of eligible patients were screened initially, largely because the clinic relied on an older fecal occult blood test that many patients found inconvenient. By switching to the easier fecal immunochemical test (FIT), training staff on screening guidelines, updating electronic records, and implementing follow-up phone reminders, the clinic saw its screening rate jump first to 53% in 2017 and then to more than 67% in 2018 – a 58% overall increase over two years. Staff calls alone boosted FIT return rates by nearly 40%,

NDC Exhibition 2026
April 6–8 | Grand Hyatt Nashville
The NDC Exhibition returns to Nashville, Tennessee — uniting healthcare distributors and manufacturers for the conversations that help guide our industry forward.
New This Year
An expanded program designed to bring what’s ahead into sharper focus — alongside the Manufacturer Hall meetings and networking experiences that define the NDC Exhibition.
Fireside Chats
Candid conversations with industry executives exploring the forces shaping our future
Educational Sessions with Brian Sullivan
Focused, practical insight from one of the industry’s most respected thought leaders
Keynote Speaker: Nick Pericle
A grounded, actionable look at how AI is transforming manufacturing and distribution, and how to move from hype to execution



underscoring the power of patient engagement and simple systemic changes in improving health outcomes. Despite progress, about one-third of patients still need screening, and clinic leaders plan to continue adapting strategies to raise rates even further.
In another example of the CRCCP’s influence, a public health clinic in St. Petersburg, Florida, more than doubled its colorectal cancer screening rate by adopting a series of targeted outreach and follow-up strategies. Before partnering with the Florida Department of Health’s Colorectal Cancer Control Program, only about one-third of eligible patients were being screened.
With CDC support, the clinic hired a full-time patient navigator, developed daily electronic reports of screening needs, and implemented a robust reminder system that combines pre-visit and follow-up calls and letters.
One especially effective innovation allowed clinic staff to collect stool samples while patients were already visiting for other services, escorting them to the restroom and providing results the same day. These combined efforts helped boost screening from 34% to over 75%.
80% in Every Community
Another major health equity campaign is gaining momentum
Polyps in the colon or rectum
Most colorectal cancers start as a growth on the inner lining of the colon or rectum. These growths are called polyps. Polyps are quite common, especially as you get older. Most polyps are benign, or noncancerous. Some types of polyps can change into cancer over time (usually over many years). The chance of a polyp turning into cancer depends on the type of polyp it is. There are different types of polyps.
` Adenomatous polyps (adenomas): These polyps sometimes change into cancer. Because of this, adenomas are called a precancerous condition. The 3 types of adenomas are tubular, villous, and tubulovillous. Tubular adenomas are the most common type of adenomatous polyps. Villous adenomas are the least common type of adenomatous polyps, but are more likely to change into cancer.
` Hyperplastic polyps and inflammatory polyps: These polyps are more common, but in general they are not precancerous. Some people with large (more than 1cm) hyperplastic polyps might need colorectal cancer screening with colonoscopy more often.
` Sessile serrated polyps (SSP) and traditional serrated adenomas (TSA): These polyps are often treated like adenomas because they have a higher risk of changing into cancer.
Source: American Cancer Society
across the United States with a shared aim: get at least 80% of eligible adults screened for colorectal cancer in every community nationwide. The initiative, 80% in Every Community, is led by the American Cancer Society National Colorectal Cancer Roundtable (ACS NCCRT) – a coalition of health systems, community organizations, employers, health plans and other partners committed to reducing colorectal cancer deaths through increased early detection.
The 80% in Every Community campaign builds on earlier national efforts – including the original 80% by 2018 pledge –by focusing not just on overall national targets but on ensuring that every community, regardless of location, income or racial and ethnic makeup, reaches screening rates of at least 80%. This expanded focus on health equity aims to close persistent gaps in access to lifesaving colorectal cancer tests.
What counts as a “community” under the initiative is intentionally flexible: it can be a city, county, state, a patient population served by a particular health system, a workforce group, or a racial or ethnic community striving together toward higher screening rates.
ACS NCCRT encourages organizations to commit to the goal, adopt screening improvement strategies, share best practices and use a suite of available tools and resources to support their outreach work. There is also a social engagement aspect: partners and supporters share progress and stories using #80inEveryCommunity to help raise awareness and inspire action.
Success stories from participating organizations show that reaching 80% is achievable with coordinated effort, tailored outreach and systematic follow-up. A core part of the initiative’s strategy includes addressing barriers to care, particularly in underserved populations, and investing in data tracking to monitor progress.
As the campaign moves forward, its leaders emphasize collaboration and shared responsibility in eliminating colorectal cancer disparities and ensuring that everyone – regardless of where they live – can benefit from timely, life-saving screening.
Reversing the trend
Taken together, the data point to a clear and urgent message: while cancer outcomes for younger Americans have improved dramatically overall, colorectal cancer is moving in the opposite direction– and it does not have to. With effective screening tools, proven public health strategies and growing advocacy to expand access and awareness, experts say the means to reverse this trend already exist.
The challenge now is turning knowledge into action, ensuring that age, income, geography or insurance status no longer stand
between patients and early detection. As researchers, clinicians, advocates and communities align around that goal, the hope is that colorectal cancer will soon follow the same downward trajectory as other cancers – and that fewer lives will be lost to a largely preventable disease.
Whether at the national or local level, Fight CRC’s Davis said simplicity is key to effective screening strategies. “Simple, well-designed systems work: mailed noninvasive tests, patient navigation, and programs that remove cost and logistical barriers,” she said.
When Budgets Shift, Accessibility Cannot
The Exam Chair helps facilities deliver ADA-compliant care while keeping long-term costs under control:
` 17-inch low seat height for safe, independent transfers
` TruComfort™ Support Rails that help patients independently transfer onto the exam chairs and reduce fall risks
` Durable, American-made construction that helps reduce lifetime replacement costs


See more at umfmedical.com/freedom or scan the QR





The Rise of Value-Based Care in Ambulatory Surgery Centers
By Pete Mercer
 As value-based care gains momentum across the healthcare system, ambulatory surgery centers are increasingly at the forefront of the shift. Long valued for their efficiency and lower costs, these outpatient facilities are now being measured by a broader standard – one that emphasizes patient outcomes, care coordination, and accountability over volume. The continued rise of value-based care models in ambulatory surgery centers is beginning to reshape how procedures are delivered, financed, and evaluated, signaling a broader transformation in outpatient care.
Repertoire Magazine spoke to Blake Peart, managing director for Vertess, about the rise of value-based care in the ambulatory surgery space, how it’s going to impact patients and providers, and some emerging trends for the industry.
What is value-based care?
Value-based care is a payment model in healthcare designed to pay providers for the quality of patient outcomes, as opposed to the quantity of services rendered. This incentivizes providers to put a greater emphasis on the quality of care and patient wellness, moving towards a patient-centered approach to providing care.
While patients benefit significantly from an increased focus on better health outcomes, payers and providers also benefit from this model. Payers benefit from greater cost predictability and lower total spending, as valuebased models reward efficiency and prevention rather than volume. For providers, while the shift requires new workflows and accountability, it offers opportunities to improve care quality, reduce waste, and share financial gains when outcomes and patient satisfaction improve.
Peart said, “A big part of the shift toward value-based care in ambulatory settings is all about performance. You have to provide

good care, cut the cost, shorten the length of stay – you’re cutting costs from hospitals and clearing out the bottleneck in those systems. It’s an efficient system that works quickly. If it meets all the proper metrics for quality markers that need to be tracked, then you’ve got the right system.”
Value-based care is only one of the newer developments for ambulatory surgery centers, including things like expanded specialty services. As technology and care processes continue to improve, new services are added that would usually only be offered in the traditional hospital setting.
“It’s interesting how the eligibility criteria for surgery

For ambulatory surgery centers operating within a value-based care model, the future will likely demand a broader role and a higher level of accountability.
centers have evolved over the last 15 to 20 years,” Peart said. “You wouldn’t have seen things like total hips and knees in an ASC 25 years ago, but we’re seeing them now because the data supports it. This shows that we’re getting better quality markers, we’re saving money, and it’s obviously friendly to the patient, so we’re getting higher satisfaction levels. Plus, you’re not bogging down hospitals, allowing them
to focus on what they need to be focused on.”
The role of convenience
Part of what makes value-based care a perfect fit for ambulatory surgery centers is the fact they already offer more convenience than the traditional hospital setting, Peart noted. Value-based care strengthens this advantage by encouraging care models that reduce unnecessary steps,
improve coordination, and anticipate patient needs before and after surgery.
“I think it’s more convenient than going through the hospital system, with all the delays, loops, and hoops that people have to go through. Most patients don’t want to be in a hospital – they’d rather be in the surgery center environment and go home the same day.”
By aligning incentives around outcomes rather than volume, value-based approaches support smoother care journeys – making it easier for patients to access timely, high-quality surgical care without the friction and inefficiencies often associated with traditional hospital settings.
Peart also believes that ambulatory surgery centers can do things as effectively as hospitals can, without putting patients in jeopardy. “We keep seeing the bar go higher and higher. ASCs are doing ablations and other procedures in cardiac care that they never would have thought about 30 years ago.”
Now that there’s data to support the viability of these procedures in this setting, it opens the doors to a whole new wave of patients. These new procedures allow for new ways to implement value-based care, especially in post-op. Peart said that ambulatory surgery centers are now making referrals to rehab facilities, which is helping to build more continuity of care in this setting.
The future of value-based care and ASCs
How will value-based care models impact the future of ambulatory surgery centers? One
of the bigger opportunities for this shift is that it places ambulatory surgery centers as a central part of the future of the healthcare industry.
For ambulatory surgery centers operating within a valuebased care model, the future will likely demand a broader role and a higher level of accountability. These ASCs will move beyond focusing solely on procedural efficiency to managing outcomes across the full episode of care, from preoperative planning through recovery. Success will hinge on robust data capabilities, closer collaboration with physicians and payers, and a willingness to take on financial risk.
In the current political climate, it’s hard to determine exactly where the healthcare industry is headed. Peart argues that we are about to see a complete revamp of healthcare, but no one is sure what the tea leaves are indicating. As for value-based care, he explained that insurance companies and providers will always be looking for ways to justify a better rate, which usually falls back to a value-based care model.
“I think everyone is going to be challenged with some type of value-based care model moving forward,” Peart said. “I think insurance companies have been paid a lot of taxpayer dollars to supplement them, which might be coming to an end. I tell a lot of our customers to take advantage of the system now, before the policies change. It always happens.”
According to Peart, insurance carriers have received significant taxpayer-funded support
Key points
ASCs align naturally with value-based care. Their efficiency, lower costs, and strong patient satisfaction make ambulatory surgery centers well suited for payment models that reward outcomes over volume.
Expanded procedures are reshaping outpatient care.
Advances in data, technology, and care coordination now allow ASCs to safely perform more complex procedures – relieving hospitals while maintaining high quality and convenience.
Greater accountability is coming. As value-based care expands, ASCs will face increased financial risk and responsibility for outcomes across the full episode of care, favoring centers with strong data capabilities and care coordination.
“ I think insurance companies have been paid a lot of taxpayer dollars to supplement them, which might be coming to an end. I tell a lot of our customers to take advantage of the system now, before the policies change. It always happens.”
in recent years through subsidies and stabilization programs, which are likely to be reduced as policy priorities shift. For the ambulatory surgery space, this creates predictable pressure on case rates, contract escalators, and authorizations. He said, “We are advising clients to act within the current reimbursement environment while it remains favorable, ahead of expected policy-driven adjustments.”
From Peart’s perspective, ambulatory surgery centers got an elevated influx of patients at the height of COVID, especially when hospitals were overrun with COVID patients. For patients that needed a
procedure done and wanted to avoid COVID, ambulatory surgery centers became a great option. That surge in patients helped to raise the bar for ambulatory surgery centers, providing data to show that they could handle the increased workloads just like a hospital would.
“As far as 2026, value-based care will more directly shift financial risk onto ASCs through mandatory bundles and qualitybased reimbursement, accelerating consolidation and favoring scaled operators that can manage outcomes, data reporting, and post-acute coordination across full episodes of care,” Peart said.
open
or closed patients are covered.
Whichever they choose, our masks go with their flow.
Monitoring patient’s EtCO2 can help physicians reduce adverse events from sedation. Now we’re making it even easier with open and closed mask options that go with the flow — helping physicians better measure patient’s airflow and better manage their team’s workflow.

Oxy2Mask™* EtCO2 with Microstream™ connector

An all-new open design with an improved diffuser to help monitor and better manage oxygenation and ventilation for patients before, during, and after sedation procedures.
• Ideal for medical-surgical suites, the ER, and other patient care areas where procedural sedation is performed
• Flexible oxygen titration from 1 LPM to 15+ LPM
• FiO2 delivery from 24% to 83% FiO2

with
Pro
™*
Microstream

An all-new closed design with an improved diffuser to help better manage oxygenation and ventilation during sedation procedures with higher O2 needs.
• Ideal for patients with in upper endoscopy, bronchoscopy, and other sedation procedures
• Flexible oxygen titration from a closed mask minimum of 5 LPM to 15+ LPM†,1
• Best-in-class FiO2 delivery from 48% to 95% FiO22 Oxy2
Helping physicians better measure their patient’s airflow.
References:
Closed masks require minimum 5 LPM O2 flow. 1. Kallstrom TJ; American Association for Respiratory Care (AARC). AARC Clinical Practice Guideline: oxygen therapy for adults in the acute care facility--2002 revision & update. Respir Care. 2002;47(6):717-720. 2. Burke R, Puddicombe C. SMI First in Human analysis of Oxy2Pro™* FiO2 performance report. 2324-01; 2022.
ASC News
NueHealth announces expansion with four new ASC partnerships
NueHealth, an ambulatory surgery center (ASC) management and value-based care solutions company, recently announced it has accelerated its growth plans for 2026 by entering into four new ASC management and development partnerships across Missouri and New Jersey.
The agreements include established facilities and upcoming projects: Hackensack Musculoskeletal Surgery Center in Hackensack, New Jersey; St. Joseph Center for Outpatient Surgery in St. Joseph, Missouri; The Surgical Center at Columbia Orthopaedic Group in Columbia, Missouri; and the Surgery Center of the Northland in Platte City, Missouri, which is slated to open in spring 2026.
“Our ability to maintain local independence while accessing the tools and support to advance our center is invaluable,” said J. Michael Smith, M.D., orthopedic surgeon and physician partner at St. Joseph Center for Outpatient Surgery. “Working with NueHealth gives us the operational depth we need to evolve, without compromising the autonomy and culture that define our practice.”
In contrast, Hackensack Musculoskeletal Surgery Center and NueHealth entered a minority-equity joint venture,
establishing a shared ownership structure supported by an integrated management approach.
“We want to make it more convenient and affordable for our patients to get the care they need and return to their lives sooner.
That’s why we’re expanding our same-day surgery options, especially for bone, joint, and spine procedures,” said Mark Sparta, COO of Hackensack Meridian Health.
“For our new Hackensack Musculoskeletal Surgery Center, providing the best and safest possible experience is our top priority. We chose to partner with NueHealth because their expertise will help us deliver the exceptional, highquality care our patients deserve.”
Symmetry Anesthesia
onboards five hospitals in five months
Dallas, Texas-based Symmetry
Anesthesia, a clinician-led anesthesia organization, announced it has kicked off 2026 with strong momentum after onboarding five hospitals within its first five months of operation. Launched in mid-2025, the group now partners with eight hospitals and has hired more than 250 anesthesia clinicians across its expanding network.
“Our model puts decisionmaking back where it belongs – in the hands of clinicians – and the results speak for themselves,” said Symmetry CEO Phil Eichenholz, MD. Chief Anesthetist Officer
Andi Damron, MS, CRNA, APRN, added that the organization’s early success reflects broad enthusiasm among anesthesia professionals and hospital partners for an approach focused on alignment and quality care.
Symmetry plans to continue its expansion throughout 2026, adding operational resources and creating additional opportunities for clinicians seeking a practice environment centered on professional respect and high-quality anesthesia care.
CMS final rule on ASC payments for 2026
The Centers for Medicare & Medicaid Services (CMS) finalized the 2026 Hospital Outpatient Prospective Payment System (OPPS) and ASC Payment System Final Rule, which includes a 2.6% payment increase for ASCs in 2026. This change reflects adjustments for cost updates and productivity and is expected to help support ASC operational costs in an inflationary environment.
Sutter Health breaks ground on Advanced Cancer Center in Modesto
Sutter Health has officially broken ground on a state-ofthe-art Advanced Cancer Center and Care Complex in Modesto, signaling a major expansion of cancer and specialty care in California’s Central Valley. The
$380 million, 165,000-squarefoot facility is expected to open in 2029 and will serve as a comprehensive hub for cancer treatment and outpatient services.
The new complex will consolidate cancer screenings, infusion and radiation therapy, imaging, lab and pharmacy services, surgical care, and outpatient clinics under one roof. Patients will also have access to clinical trials and specialists from the wider Sutter Health network, reducing the need for long-distance travel for advanced care.
Sutter Health plans to staff the center with approximately 120 physicians and 400 team members, serving tens of thousands of patients each year. The project reflects the organization’s ongoing commitment to improving access to high-quality care and addressing healthcare gaps in the Central Valley.
“This center represents our dedication to providing advanced, coordinated care close to home for the communities we serve,” said a Sutter Health representative.
Proliance expands access to workplace injury care in
Seattle suburb
Renton, Washington-based Proliance Orthopedic Associates is expanding workplace injury care in South King County with a new occupational medicine clinic opening in Renton in February 2026. The Renton location
will complement existing sites in Renton, Covington, and Auburn, offering same-day treatment for sprains, strains, fractures, lacerations, and repetitive-use injuries, plus on-site imaging and claim support. The expanded services also
include fit-for-duty and return-towork exams and employer health initiatives. Proliance’s integrated care model aims to reduce barriers to occupational healthcare and support healthier, more productive local workforces.
Mass General Brigham and Tampa General Hospital launch Ambulatory Care Network in Florida
Boston-based Mass General Brigham and Tampa General Hospital have announced a new joint ambulatory care network aimed at expanding outpatient services along Florida’s growing East Coast. The partnership will deliver coordinated primary care, specialty services, advanced imaging, oncology, and outpatient surgical care to communities in Martin, St. Lucie, and Palm Beach counties, a region home to more than 2 million residents.
“As one of the state’s leading academic health systems, Tampa General is committed to meeting the needs of Floridians by expanding access to world-class care,” said John Couris, president and CEO of Florida Health Sciences Center | Tampa General Hospital. “With this new ambulatory network, we are building on our strong foundation in Florida to ensure patients along the East Coast have seamless access to the highest-quality outpatient services. This partnership with one of the nation’s top academic health systems reflects our vision to lead in delivering innovative, patient-centered care across the state, while strengthening the health of our communities today and for generations to come.”
“This collaboration brings together two leading academic health systems with a shared commitment to clinical excellence and innovation,” said Anne Klibanski, MD, CEO of Mass General Brigham. “By creating a unified ambulatory network, we can broaden access to trusted physicians and advanced outpatient services, improve health outcomes, and deliver care that is more coordinated and patient-focused.”
Integrating Value-Based Care Models
How a newly formed organization assists providers in navigating the shift to value-based care.
By Jenna Hughes
 Value-based care (VBC) is a very highly sought after goal for health systems today, as many providers have shifted focus to ensuring improved patient outcomes as opposed to delivering volume of healthcare services.
By aligning incentives and payment, according to the American Medical Association (AMA), value-based care models promote better coordination among healthcare professionals, reduce the need for unnecessary healthcare services, lower the risk of medical errors and expand access to care.
As the industry transitions to value-based patient care, healthcare organizations are increasingly seeking clarity as to what exactly it means to operationalize these models and deliver quality, patient-first care.
The American Academy of Value-Based Care (AAVBC), a clinician-led nonprofit organization, provides a central resource for evidence-based practices in the transition to value-based care by advancing patient-centered and value-oriented care.
“AAVBC was specifically created to address gaps in early and accurate diagnosis, appropriate utilization of healthcare services and consistent performance on quality measures,” said Eric Haas, MD, Chief Medical Officer, AAVBC.

Until the formation of AAVBC, providers lacked an authoritative source for best practices, treatment plans and guidelines regarding clinical care and documentation for VBC. Now, through comprehensive educational resources, clinical pathways and vendor information, the organization helps providers navigate the shift from traditional fee-for-service to patient-centered models of care.
Origins of value-based care
In the early 2000s, research increasingly showed that fee-for service reimbursement models were contributing to rising healthcare costs and inconsistent quality outcomes for providers and healthcare organizations. As a result, the National Academy of Medicine called for a “STEEP” approach to healthcare: safe, timely, efficient, equitable, patient-centered care – which
ultimately became the framework for today’s VBC.
Value-based care models are now a significant component of both public and private payer structures across the healthcare industry.
AAVBC defines value-based care as a healthcare model rewarding providers based on patient outcomes, quality of care and cost efficiency rather than volume of services delivered.
“This definition directly informs AAVBC’s strategy – our quick-reference guidelines, tools and educational resources are designed to help physicians and healthcare organizations succeed in outcome-driven payment models by delivering higher-quality, more efficient care,” said Dr. Haas.
Value-based care places a growing emphasis on interoperability, risk adjustment and health equity – AAVBC’s framework for high-value healthcare today includes the right care, to the right patient, at the right time, in the right setting, for the right reasons.
Evidence-focused, quality patient care
A value-based care approach, according to AAVBC, prioritizes adherence to evidence-based guidelines, understanding patient goals, promoting cost-effectiveness, improving population health, enhancing patient experiences and providing equitable access to care.
“Many organizations struggle to operationalize these concepts –including consistent performance on quality measures such as Stars and HEDIS – in day-to-day care delivery, and AAVBC focuses on turning complex requirements into clear, usable guidance for clinicians and care teams,” said Dr. Haas.
AAVBC’s STAR Measures Overview (governing quality performance for more than 33 million Medicare Advantage beneficiaries) provides a concise, evidence-informed framework to help organizations understand Centers for Medicare & Medicaid Services (CMS) requirements, improve quality scores and strengthen performance across value-based programs. HEDIS is also a widely used performance improvement tool, and nearly 235 million people are enrolled in health plans that report HEDIS results.
“By centralizing high-quality, evidence-based resources in one place, the platform enables clinicians and organizations to move from theory to execution more efficiently and consistently,” said Dr. Haas.
A centralized resource
Early engagement from providers and value-based care organizations has validated a need in the healthcare industry for a centralized resource and educational material informing value-based care processes.
“While AAVBC is still early in its growth, feedback consistently
One of the most common barriers is the shift from a reactive, fee-for-service care model to an outcomes-based approach that prioritizes prevention and long-term health.
AAVBC additionally launched the nation’s first centralized hub for value-based care education in early 2026 as a resource for providers and other key healthcare groups to be able to access a wide range of resources designed to improve care quality.
“The AAVBC platform serves as a single source of truth for curated diagnostics, care pathways and operational tools that support valuebased care delivery,” said Dr. Haas.
The educational platform provides physicians with a clear understanding of value-based care principles, practices and regulatory standards by offering access to resources such as evidence syntheses, guidelines on STAR Measures, coding practices and utilization benchmarks as well as independent vendor rankings and price guides to clarify true cost and quality of digital health tools.
highlights the value of having clear, evidence-based guidance that bridges clinical care, documentation and quality performance – areas that are often fragmented today,” said Dr. Haas.
Guidance from healthcare organizations in the platform’s early stages is a critical part of AAVBC improving on its educational resources, strategy and offerings.
“Frontline clinician feedback is a core part of AAVBC’s development process,” said Dr. Haas. “Our platform allows users to directly submit feedback, which we use to improve our guidelines, tools and educational content. This ensures our resources remain practical, relevant and grounded in real-world clinical experiences.”
As the organization continues to grow, AAVBC aims to drive and assist in the system-wide adoption of value-based care over
the next three to five years by simplifying complex requirements for providers, health plans and healthcare organizations.
“Our key priorities include increasing transparency in the digital health ecosystem through independent vendor rankings and pricing guides, expanding CME offerings as well as developing educational resources for resident physicians and medical students,” said Dr. Haas. “Success going forward will be measured by adoption of our tools, earlier diagnosis of diseases, increased use of preventive services and measurable reductions in avoidable utilization and total cost of care.”
The future of value-based patient care
AAVBC was formed to address the ongoing gaps in value-based care, such as early and accurate diagnosis and appropriate utilization of healthcare services to emphasize early prevention, intervention and avoidance of unnecessary downstream utilization; which includes helping providers
overcome common obstacles to adopting value-based care.
One of the most common barriers is the shift from a reactive, fee-for-service care model to an outcomes-based approach that prioritizes prevention and long-term health.
“This transition requires new workflows, new metrics and a deeper understanding of how early intervention and appropriate utilization improve both outcomes and cost performance,” said Dr. Haas. “AAVBC helps organizations overcome these challenges by providing clear guidance, practical tools, and education that make preventive, value-based care operationally achievable.”
Making value-based care achievable requires a focus on data analytics, care coordination and empowering patients with tools to keep improving.
The increasing role of data, technology and analytics is also addressing some of these challenges by rapidly promoting the adoption of value-based care.
What is value-based care?
Value-based care (VBC) is a healthcare delivery structure where providers are graded and reimbursed for safe, efficient, highquality care rather than the volume and complexity of services performed. A value-based approach prioritizes:
` Adherence to evidence-based guidelines
` Understanding patient goals
` Promoting cost-effectiveness
` Improving population health
` Enhancing patient experiences
` Providing equitable access to care
Source: www.aavbc.org
Technology is foundational to advancing value-based care, said Dr. Haas, because it enables prevention on a larger scale.
“Technological advancements and tools allow organizations to identify high-risk patient populations early, track chronic conditions proactively and deploy targeted interventions before health issues escalate,” said Dr. Haas. “When used effectively, analytics shift care from reactive treatment to proactive, evidence-based population health management that improves outcomes and lowers costs.”
Aligning financial incentives with patient outcomes is one of the most powerful levers for driving meaningful, lasting adoption of value-based care going forward, says Dr. Haas. AAVBC promotes the acceleration of the shift to value-based care through health insurers and government payers transitioning from feefor-service reimbursement to compensation models that reward outcomes and quality.
“Several converging trends give us confidence in the future of value-based care in the U.S., including advances in healthcare technology and analytics, a growing emphasis on preventive care and patient engagement, continued payment reform focused on outcomes and quality as well as the expansion of Accountable Care Organizations (ACOs) and Management Service Organizations (MSOs) that improve care coordination and reduce fragmentation,” said Dr. Haas. “With chronic disease driving the majority of healthcare costs, prevention is no longer optional – it is essential to the sustainability of the healthcare system.”
Most of the healthcare facilities you work with will need an ADA Compliant examination chair and transfer support that meet ADA Standards by Summer 2026.
MTI has 10 ADA compliant exam chairs to meet the needs of every customer.



Regulating AI Implementation
The AMA launches new Center for Digital Health and AI.
 Artificial Intelligence (AI) is rapidly transforming the way that healthcare professionals use technology to diagnose and treat patients in clinical settings.
As a result, physicians are increasingly seeking involvement in the implementation and use of artificial intelligence (AI) in hospitals and outpatient settings to ensure that these new, automatous technologies assist – rather than complicate –healthcare workflows.
In October 2025, the American Medical Association (AMA) announced the launch of its Center for Digital Health and AI, an initiative created to put physicians at the center of implementing new technologies, such as AI, that are transforming medicine.
According to the AMA, AI and other digital health tools are continuing to advance, but without physician leadership and input, they risk creating unintended burdens and failing to reach their full potential.
Clinical insight through physician involvement is therefore key
to making digital health tools truly effective and to reduce their burdens, per the AMA.
Workflow integration, education and collaboration
The new Center aims to reach the full potential of AI and digital health by engaging physicians throughout the lifecycle of technology development and deployment. This entails placing physicians at the forefront of AI implementation to ensure that the technology fits well into clinical workflows and that healthcare staff know how to properly utilize it.
“Augmented Intelligence will be a defining force in the future of health care, but right now we are barely scratching the surface of its potential,” said AMA CEO and Executive Vice President John Whyte, MD, MPH in a press release. “Digital health tools are everywhere, and the technology has limitless opportunity, but if you don’t understand clinical practice or clinical workflow, even the best tools will never be fully implemented.”
The Center for Digital Health and AI endeavor outlines four strategic guiding pillars for the rollout of AI technology in health, including policy and regulatory leadership, clinical workflow integration, education/ training and collaboration.
The Center will take advantage of the full potential of AI by focusing on working with regulators, policymakers and technology leaders to shape benchmarks for the safe and effective use of AI in medicine; create opportunities for healthcare professionals to influence AI so they enhance the patient experience and integrate
“Digital health tools are everywhere, and the technology has limitless opportunity, but if you don’t understand clinical practice or clinical workflow, even the best tools will never be fully implemented.”
into existing workflows to building partnerships across tech, research, government and healthcare sectors to drive innovation.
Building enthusiasm for AI
Many physicians across healthcare are, in fact, excited about the future of AI – with 68% seeing at least some advantage to the use of AI in their practice, up from 65% in 2023, per the AMA –however, some concerns remain about how AI tools will impact practices going forward.
Nearly a quarter of physicians remain more worried than excited about AI technology, according to the AMA, citing risks to data privacy, reliability and safety concerns.
Nevertheless, the AMA reported an increase in AI use in healthcare from 38% in 2023 to 66% of physicians reporting they use some type of AI tool in practice in 2024.
According to the AMA, the new Center for Digital Health and AI has the potential to address these concerns, grow enthusiasm around AI and help incorporate the technology into clinical workflows.
“By launching this Center, the AMA is leading in this space, so physicians have a say in the technology and clinical care of the future,” said Dr. Whyte. “Our goal is to harness innovation responsibly and effectively, so it improves patient care and reduces unnecessary burdens on physicians.”
` Policy and regulatory leadership: Working with regulators, policymakers, and technology leaders to shape benchmarks for safe and effective use of AI in medicine and digital health tools.
` Clinical Workflow Integration: Creating opportunities for doctors to shape AI and digital tools so they work within clinical workflows and enhance patient and clinician experience.
` Education & training: Equipping physicians and health systems with knowledge and tools to integrate AI efficiently and effectively into practice.
` Collaboration: Building partnerships across the tech, research, government, and health care sectors to drive innovation aligned with patient needs.
The Center for Digital Health and AI will focus on:
Amazon’s One Medical Launches AI Health Assistant for Members
New tool aims to help patients navigate symptoms, appointments, and routine care through the One Medical platform.
 Amazon’s primary care company One Medical has launched a new AI-powered Health Assistant, expanding the role of artificial intelligence in how patients access and manage care. The tool is now available to One Medical members through the company’s mobile app and website.
The Health AI assistant is designed to help patients navigate routine health questions, understand medical information, and take next steps in their care. According to Amazon, the assistant can answer questions about symptoms, medications, lab results, and preventive care, as well as help members determine whether they should schedule a virtual visit, an in-office appointment, or seek urgent care. Unlike general consumer health chatbots, the One Medical assistant is integrated into members’ existing medical records. With patient permission, it can draw on information such as diagnoses, medications, test results, and vaccination history to deliver more personalized responses. Amazon said the assistant was developed in collaboration with One Medical clinicians and operates within HIPAA-compliant privacy and security safeguards.
The AI tool can also handle certain administrative tasks, including booking appointments and supporting prescription renewals, with prescriptions able to be filled through Amazon Pharmacy when appropriate. Company leaders said these features are intended to
reduce friction for patients while allowing clinicians to spend more time on direct patient care.
“The U.S. health care experience is fragmented, with each provider seeing only parts of your health puzzle,” said Neil Lindsay, senior vice president of Amazon Health Services. “Health AI in the One Medical app brings together all the pieces of your personal health information to give you a more complete picture – helping you understand your health, and supporting you in getting the care you need to get and stay well. Health AI makes getting health care easier and more convenient, so patients can focus on what matters most: their health.”
Amazon emphasized that the assistant does not replace physicians or provide emergency medical care. When a situation requires clinical judgment or urgent attention, the tool is designed to escalate the issue by connecting patients with One Medical’s care teams or directing them to appropriate in-person services.
The Health AI assistant follows a beta testing phase in which select One Medical members used the tool and provided feedback. Amazon said it will continue to refine the assistant based on realworld use, with clinicians involved in ongoing oversight to ensure safety and accuracy.
The launch comes as health systems, insurers, and technology companies increasingly turn to artificial intelligence to improve access, efficiency, and patient engagement. Since Amazon acquired One Medical in 2023, the company has steadily integrated its technology and logistics capabilities into the primary care platform.
Commercial Health News
Kroger Health hits major prescription safety milestone
Kroger Health announced it has surpassed 250,000 students completing its Prescription Drug Safety: Know the Truth education program for high school students, marking a significant milestone in its drug safety efforts. The free program, offered in partnership with Everfi, teaches safe use, storage and disposal of medications and aims to reduce misuse among young people. Since partnering with Everfi in 2018, participation has grown dramatically, helping equip students with critical knowledge to support healthier decisions and stronger communities.
Walmart launches new health services
Walmart is kicking off 2026 with a major push into health and wellness, unveiling a new digital health platform and cutting prices on more than 1,000 wellness products in a move aimed at boosting access, affordability and everyday healthy living.
The retailer’s Better Care Services platform gives customers instant access to a curated network of third-party urgent care and behavioral health providers, plus connections to LillyDirect for chronic care support. Consultations can be completed same day, with flexible pickup and delivery of prescriptions and over-the-counter items – and a limited-time $15 discount on select telehealth services beginning January 15.

CVS Health announces progress to “simplify” health insurance
CVS Health announced new progress in efforts to simplify and reduce costs in U.S. health insurance, focusing on smoother prior authorizations, lower hospital readmissions, and cheaper prescription drugs. Aetna, part of CVS Health, now approves most prior authorization requests within 24 hours and is improving interoperability across systems to reduce administrative friction. The company is expanding low-cost primary care, no-cost preventive services, and free virtual care to help lower overall expenses for its roughly 185 million members. CVS Health also promotes biosimilars and shares negotiated drug rebate savings directly with consumers at the pharmacy counter.
Walmart is also rolling back prices on wellness essentials, spanning healthy foods, supplements, fitness products and other health staples. Nearly 60% of Walmart shoppers say saving money is a top priority, and the price cuts are designed to meet that need while encouraging healthier routines.
To support broader wellbeing, the company’s Nutrition Hub uses AI-driven recommendations for personalized food and
recipe suggestions, and more than 400 budget-friendly “New Year reset” recipes are available online. Walmart’s wellness assortment continues to grow with new products across vitamins, snacks, beverages and tech-enabled health gear.
The retailer will extend its commitment into communities with nearly 4,600 pharmacy wellness events nationwide on January 24 offering free screenings, low-cost immunizations and health consultations.
Responding to Change
APIC and SHEA create HIPAG to guide infection prevention priorities and dialogue within the industry.
 Two leading infection prevention organizations announced in late 2025 the formation of a new collaborative body aimed at bolstering national infection control efforts.
The Association for Professionals in Infection Control and Epidemiology (APIC) and the Society for Healthcare Epidemiology of America (SHEA) unveiled the Healthcare Infection Prevention Advisory Group (HIPAG) this past December, a multidisciplinary initiative designed to address infection prevention priorities of national importance.
The move comes after the Centers for Disease Control and Prevention’s (CDC) decision to eliminate the Healthcare Infection Control Practices Advisory Committee (HICPAC) – a longstanding source of coordinated, evidence-based guidance on infection prevention, control, and antimicrobial stewardship. With HICPAC no longer in operation, public health leaders expressed concern about potential inconsistency in clinical practice and policy at a time when emerging infectious threats continue to challenge healthcare systems.
In a joint statement, APIC and SHEA emphasized that HIPAG is intended to “help fill these gaps and ensure continuity” by offering timely, evidenceinformed advisory expertise to healthcare organizations and the broader community. The group will bring together invited experts

from medical societies, healthcare organizations, public health entities, and patient advocacy groups to promote unity and prevent fragmented efforts across sectors.
“HIPAG must reflect the full breadth of expertise and experience in infection prevention and epidemiology,” said Dr. David Weber, president of SHEA. He underscored the importance of broad, inclusive engagement across disciplines to ensure infection prevention policies remain grounded in scientific evidence.
APIC President Dr. Carol McLay echoed the sentiment, noting that the collaboration aims to keep infection
prevention “science-driven, practical, and grounded in realworld expertise.” McLay added that the initiative is “critical to the safety of healthcare delivery” and essential for restoring confidence among patients, families, and health professionals.
APIC and SHEA said they are “proceeding thoughtfully and at a measured pace to intentionally build the group” A call for applications had been distributed to APIC and SHEA members in late January. HIPAG organizers hope that a transparent application process, combined with intentional engagement of core stakeholders, will ensure that all voices in this space have a seat at the table.
“This is still a work in progress,” organizers said. “We are leaning more towards a structure to provide rapid guidance during emerging threats as well as one that reviews and assesses processes that are currently in practice. Based on our resources, we are leaning on our current process within each organization for rigorous, evidence-based recommendations, with an evaluation or input from HIPAG during our established process. We feel this gets to the best of what this group can convene to provide –expert opinion and expertise.”



Don’t let symptoms get in the way of a clear picture.
In sexual health, symptoms often overlap, making it difficult to diagnose. That’s why comprehensive PCR testing isn’t just helpful — it’s essential.
At Cepheid, we deliver cutting-edge PCR diagnostics that look beyond the obvious, identifying infections at once with speed and accuracy. Because in sexual health, seeing the full picture means getting patients the right treatment, fast. Clear answers start here. Learn More about Cepheid’s Women’s & Sexual Health Portfolio.
Dukal Expands Access to Comprehensive Wound Care Portfolio Through New Provista Contract
Today’s non-acute healthcare providers are navigating an ever-complex operating environment. Workforce shortages, shifting care settings, and unpredictable supply chains are rewriting the norms for clinical teams and distributor partners alike. Sales representatives are now expected to provide not only products but also consistency, reliability, and innovative solutions that drive real results.

In response to these challenges, Dukal has established a new agreement with Provista, one of the nation’s leading group purchasing organizations (GPOs). Significantly expanding access to Dukal’s comprehensive portfolio of traditional and advanced wound care solutions – empowering Provista’s non-acute customer network.
For distributors, this partnership offers a strategic opportunity to enhance product alignment, improve standardization, and expand access to a contract-backed portfolio that is both clinically effective and operationally efficient.
Expanding High Value Solutions Across Non Acute Care
Through the new agreement, Provista members gain streamlined access to Dukal’s comprehensive traditional wound care offering:
` Gauze pads and sponges
` Adhesive bandages
` Elastic and cohesive bandages
` Medical tapes
` Primary and secondary dressings
` A complete range of cotton products
Foundational products are essential in physician offices, postacute care settings, long-term care facilities, and home health organizations. Settings where product consistency and reliable supply directly impact staff efficiency and the quality of patient care. As budgets become more constrained and patient volumes fluctuate, sourcing a wide range of highquality wound care essentials from a single, trusted manufacturer provides significant operational value.
For distributor sales teams, the contract streamlines discussions
regarding standardization, alignment, and long-term planning, strengthening customer confidence in both product performance and supply continuity.
Advancing Care Through Innovative Wound Management Solutions
The agreement further extends Provista member access to Dukal’s advanced wound care solutions with the inclusion of RENCURA™ Silicone Bordered Foam Dressings. The RENCURA™ line is designed to support healing across the continuum of care by integrating clinical performance focused on promoting healing and reducing recovery time.
by diversified sourcing strategies, expanded inventory, and proactive communication practices – core elements of Dukal’s InSight Supply Chain Solutions.
“We’re proud to contract with Provista to expand access to Dukal’s trusted wound care solutions,” said Charles Abbinanti, President of Dukal. “This agreement reflects our shared commitment to supporting healthcare professionals and strengthening family and community health.”
For distributors, this commitment provides more than contract eligibility. It instills confidence in continuity, stability, and the support of a partner dedicated to long-term performance.
“ This agreement reflects our shared commitment to supporting healthcare professionals and strengthening family and community health.”
With the increasing use of advanced wound care in outpatient, long-term care, and homebased care settings, distributor representatives can now present RENCURA™ as a contractsupported solution. This offering aligns with provider priorities for improved outcomes, streamlined workflows, and standardized clinical protocols.
Building Supply Chain Confidence Through Stability and Scale
Supply reliability remains a primary concern for healthcare organizations amid ongoing volatility. A distinguishing feature of the Provista contract is Dukal’s ongoing commitment to supply chain resilience, supported
Enabling Distributor Growth and Customer Success
With the Provista contract in place, Dukal is positioned to accelerate distributor growth strategies through:
` A broader portfolio spanning both traditional and advanced wound care
` Reliable supply chain backed by a resilient infrastructure
` Dedicated sales team committed to developing long-term partnerships
Establishing a robust platform for distributor sales teams to expand their wound care presence, enhance customer support, and assist providers in addressing the daily operational and clinical challenges we face today.
Rethinking the Front Door to Care
As emergency department utilization grows, Vizient and Sg2 forecasts suggest hospitals must shift how patients access care – using better metrics, smarter staffing and expanded ambulatory options to relieve ER congestion.
By Pete Mercer

 According to a recent study conducted by Vizient and Sg2, a Vizient company, emergency departments across the country are facing an increase in patient visits. The Centers for Disease Control and Prevention (CDC) found that patients in America made approximately 139.8 million visits to the emergency department in 2024. Sg2’s 2025 Impact of Change Forecast projects that emergency department volumes will grow 5% over the next decade.
This increase in demand is a significant challenge for the structural and operational infrastructure of hospitals, threatening safety, efficiency, and financial stability. Repertoire Magazine recently spoke to Brianna Motley, the vice president of intelligence strategy and delivery for Vizient, about overcrowding in the emergency department, protecting vulnerable patient groups and what the future for the emergency department looks like.
The dual bottleneck
It’s not news that hospitals are under tremendous strain and pressure – the healthcare industry is constantly in a state of flux and is in many ways still recovering from COVID-19. Now, hospitals are facing what the forecast calls a “dual bottleneck”, where critically ill patients are waiting too long for beds, while low-acuity patients flood the emergency department for conditions that could be
addressed in other care settings. The distinction that needs to be made in these scenarios is whether the condition is urgent or emergent.
Motley said, “The biggest difference between urgent and emergent visits is really the acuity level. With urgent visits that are lower acuity, you typically have other care settings that you can get those needs addressed. That would include an urgent care center or primary care clinic. With emergent visits that are higher acuity, there typically aren’t too many other places that you can go to get those needs taken care of outside of the emergency department.”
This dual bottleneck is exacerbating other problems as well, like staffing and supply shortages, creating an unsustainable environment across the board. If hospitals want to meaningfully address these pressures, they have to rethink their entire care delivery system.
Staffing is an important component of the bigger picture. Motley offered a practical solution to meeting patient volume demand, by looking at how schedules are built in comparison to the typical incoming patient surge windows. “One of the classic analyses to compare is, what is the arrival pattern for patients? Do you have the right staff to effectively meet those demands at certain inflection points within a given day?”
Understanding the metrics to build better strategies
Building a better plan for the future requires a deeper understanding of the current challenges, which can be accessed through performance metrics and benchmarks. One of the key metrics found in the Sg2 forecast is the average
length of stay, which shows how long patients wait for care in an emergency department setting. This is a key operational metric for hospital systems to understand to develop a better strategy in the future.
The best way to build a strategy that will help the emergency department with metrics like a verage length of stay is to look at how it compares to other benchmarks or emergency departments of similar sizes.
“Understanding how far out of sync you are with other emergency departments of a similar size, or what we would expect to see, lets you know how acute the problem is,” Motley said. “From there, you need to assess the conditions that are frequently presenting to your emergency department and what strategies you need to get better in line.”
According to Motley, hospitals that are looking to reduce the average length of stay need to look at the metric across the whole continuum. First, hospitals have to make sure that they have the capacity for incoming patients – the open space to be able to move people from the waiting room to an open bed to receive the care they need. Once they are out of the emergency room, hospitals need the right diagnostics to quickly triage and determine the clinical issues. From there, the team can determine whether the patient needs to be admitted and what that admission process looks like.
Having a strategy in place can help hospitals reduce the overall average length of stay, while also improving the workflow and productivity of the emergency department. This will impact the quality of care and the speed with which
it’s delivered is one of the most important parts of the hospital.
The next decade of emergency department utility These projections from Vizient and Sg2 are expecting emergency department utilization to increase over the next decade. This includes more volume and a higher average length of stay for patients, driven by an aging population that has multiple comorbid conditions and access limitations across the rest of the system of care.
How can health systems successfully navigate the next decade of this trend? Motley said, “It really comes down to understanding, at the local level, what the demand is, the type of patients that frequent the hospital, and developing strategies to meet that demand in the appropriate care setting.”
Implementing technology is a great way to streamline the workflow inside the emergency department, especially when triaging patients. Patients can also leverage
technology to better understand the resources and care touchpoints that are available in their area, which could help them to decide if the emergency department at the hospital is really the best option for their care needs. If it isn’t, they can find a better option to fit what they need at the moment.
If health systems want to effectively reduce the strain within the emergency department over the next 10 years, there are some adjustments that can be made to make this possible. According to Motley, in a perfect world, the emergency department would no longer be the front door, or the primary access point, to the hospital. Improved access to ambulatory care locations and lower acuity care locations could help to reduce the need for the emergency department. While the emergency department will always be a necessary touchpoint for health systems, there are ways to decrease dependence on the ER and increase utilization across the rest of the care continuum.
ED utilization numbers
New data from Vizient’s Sg2 “Data on the EDGE» report reveals a critical shift in ED utilization, forcing health systems to fundamentally rethink how they allocate resources across the entire hospital. As patient acuity continues to rise, health systems will need to look for ways to expand care capacity to address the inpatient/ED interplay, deploy AI for surge prediction and staffing optimization, and redefine the ED within their broader ambulatory portfolios, a recent study conducted by Vizient and Sg2, a Vizient company.
Key findings from the report include:
` ED length of stay for emergent cases: 5.3 hours (vs. 2.4 for urgent cases)
` 67% of inpatient admissions now originate from the ED
` Medicare patients represent 29% of ED visits but 50% of inpatient admissions
` Facilities seeing 25K+ annual visits face significantly longer patient stays ` Behavioral health is driving growth making EmPATH units and behavioral health urgent care critical investments.
Supply Chain Leader Profile
Jane Torzewski, RN, MAN, MBA, Director of Medical Device Contracting at Mayo Clinic
 Jane Torzewski, RN, MAN, MBA, serves as the Director of Medical Device Contracting at Mayo Clinic, leading a team responsible for managing contracts that support both Mayo and Captis, a supply aggregation service provider, in the physician preference space. With nine years in this leadership role, Torzewski’s career path reflects a unique combination of clinical experience and business acumen, providing her with a distinctive perspective on healthcare supply chain management.
“My role is really to meet the needs of our practice,” Torzewski said. “Our primary value at Mayo Clinic, which we’ve had since inception more than 150 years ago, is that the needs of the patient come first. I listen to the
practice and meet those needs across our contracting areas, particularly in medical device implants.” Her approach emphasizes that, even in supply chain management, patient-centered care remains the guiding principle.

Torzewski’s career began far from the corporate boardroom. After earning a business degree, she worked in retail management before transitioning into nursing, where she spent 15 years at the bedside. “Nursing was honestly my second career,” she recalls. Her dual background in business and clinical practice eventually led her to pursue an MBA rather than an advanced practice nursing degree, driven by an interest in healthcare economics. This combination of experiences positioned her to join Mayo Clinic’s Value Analysis department, where she merged clinical knowledge with financial strategy – a foundation that naturally led to her current role in contracting.
Even as her daily work shifted from direct patient care to managing physician relationships and contracts, Torzewski remains motivated by her ability to impact patient outcomes indirectly. “I’m less close to the patient today in contracting, but the needs are no less felt in managing and working with physicians to meet those needs,” she notes. She draws energy from Mayo Clinic’s
Jane Torzewski
broader initiatives, including the transformative Unbound Project, aimed at shaping the hospital of the future and advancing the organization’s mission to cure, connect, and transform care.
Torzewski credits several mentors for shaping her leadership philosophy. Early in her career, a nurse manager modeled advocacy, demonstrating how to support staff with internal and external stakeholders. Later, a supply chain leader taught her the importance of relationship building, transparency, and empathy. “Those moments crystallized some of my core beliefs and behaviors and created the leadership style I have today,” she reflects.
For women aspiring to leadership roles in healthcare supply chain, Torzewski offers clear guidance: embrace opportunities, take risks, and consciously build your personal brand. “Women leaders bring their own unique viewpoint and dimension. You should take advantage to lead if there’s an opportunity. It builds confidence, elevates your reputation, and helps you create your personal brand,” she advises. “Seek out opportunities when they’re given to you, don’t shy away, and find excuses to lean in rather than lean out.”
Building a strong, diverse team is equally central to Torzewski’s philosophy. She emphasizes the deliberate cultivation of multiple viewpoints and experiences to complement existing team strengths. “Retention is about creating a culture of excellence,” she says. “Within your team, that culture is really about a group that gets together, maintains humbleness, grace,
and support for one another to grow each other, which helps elevate the whole team.” This approach fosters cohesion and stability, ensuring team members are empowered and motivated to stay.
Innovation and problemsolving, Torzewski believes, emerge naturally when team members feel empowered and supported. By providing leadership opportunities and encouraging skill growth, team members contribute to both their own development and the collective strength of the group. “All boats rise as the team individually gets better and matures,” she observes, underscoring the symbiotic relationship between individual growth and team success.
would do is ensure we always have something to meet the needs of our patients. Unfortunately, almost daily, you run into situations where products are unavailable, and when it’s critical, you just try to figure out what you can do.” Her perspective highlights the tangible impact of leadership in supply chain operations on patient care and outcomes.
Ultimately, Jane Torzewski’s leadership is defined by a balance of clinical insight, business strategy, and human-centered values. Her journey – from retail management to bedside nursing to healthcare supply chain leadership – illustrates the power of diverse experiences, thoughtful mentorship, and the courage to take risks. By prioritizing patient needs, fostering team cohesion,
Innovation and problem-solving, Torzewski believes, emerge naturally when team members feel empowered and supported.
Reflecting on her early career, Torzewski wishes she had taken more risks and focused earlier on networking. “I wish I could have been bolder about the choices I made and concentrated on honing my networking skills. That skill nourishes you for years to come,” she says. This advice extends to younger professionals: seize challenges, expand your horizons, and actively cultivate relationships that will serve you throughout your career.
When asked about an industry problem she would solve overnight, Torzewski identifies business continuity in healthcare supply chain. “The one thing I
and advocating for women in leadership, Torzewski exemplifies a holistic approach to leading complex healthcare operations.
For professionals aspiring to make an impact in healthcare, her guidance is clear: take calculated risks, invest in relationships, and lead with empathy. By doing so, future leaders can shape not only their careers but also the systems and teams that directly impact patient care. In an era of rapid healthcare transformation, Jane Torzewski’s leadership insights serve as a roadmap for success, demonstrating how vision, values, and adaptability converge to drive meaningful outcomes.
Cleveland Clinic pursuing a Level I Trauma Center at main campus
Cleveland Clinic is pursuing the establishment of a Level I trauma center for adults and children at its Main Campus.
Level I trauma centers provide the highest level of care for severely injured patients, offering access to specialized surgeons, physicians and critical care specialists at all times. Cleveland Clinic currently operates a Level I trauma center at Akron General Hospital and Level II trauma centers at Hillcrest, Fairview and Mercy hospitals for adult patients.
“Cleveland Clinic is committed to providing the highest quality care to all patients and expanding our capacity to care for critically ill and injured patients,” said Tom Mihaljevic, MD, CEO and President and Morton L. Mandel CEO Chair of Cleveland Clinic. “Adding a Level I trauma center to our Main Campus will extend our world-class care to patients in need of trauma care, provide continuity of care for our patients, and help us better meet the needs of our community.”
Premier, Inc. announces transition of Michael J. Alkire as President and Chief Executive Officer
Premier, Inc. announced that President and Chief Executive Officer, Michael J. Alkire, plans to transition as the company’s leader
IDN News
upon the successful selection of an appropriate successor by the Board of Directors. Alkire will remain in his current role during a targeted search process for a new CEO to support future growth as a private company.
Alkire, who joined Premier in 2003, is a seasoned healthcare executive with more than 30 years of operational, technology and business leadership experience. He has held numerous leadership roles at the company, including serving as Chief Operating Officer starting in 2013, becoming President in 2019 and CEO in 2021.
Geisinger recognized nationally for advancing health and worker well-being
Geisinger has been nationally recognized for its continued efforts to support the mental health and well-being of its healthcare workforce, earning designation as a WellBeing First Champion for the second consecutive year. The recognition comes from ALL IN: WellBeing First for Healthcare, a coalition focused on removing systemic barriers that prevent clinicians from seeking mental health care.
The designation reflects Geisinger’s commitment to creating a culture in which healthcare professionals can prioritize their mental health without fear of stigma or professional consequences. As part of this effort, Geisinger has removed invasive and outdated
mental health questions from its licensure and credentialing applications – an important step toward ensuring clinicians can access care confidentially and without risking their careers.
Gartner releases 2025 Healthcare Supply Chain Rankings
Gartner has released its 2025 Healthcare Supply Chain Top 25, highlighting the organizations leading the way in operational excellence, cost management, and innovation. AdventHealth retains the No. 1 spot, demonstrating sustained leadership in supply chain strategy, while other health systems show strong gains through technology adoption and clinical collaboration.
AdventHealth’s consecutive top ranking underscores the organization’s commitment to comprehensive supply chain management. Stanford Medicine, Bon Secours Mercy Health, Rush University System, and Corewell round out the top five.
New entrants such as NewYorkPresbyterian and Mass General Brigham signal the evolving competitiveness of the healthcare supply chain landscape.
Meanwhile, long-standing leaders like Intermountain Health, Mayo Clinic, and Cleveland Clinic maintain their positions in Gartner’s “Masters” category, reflecting years of consistent excellence.


Invest in Leadership. Strengthen Your Team. Accelerate Results.



The Professional Women in Healthcare® (PWH) Leadership Summit is the only event in the industry dedicated to inclusive leadership development—open to women and men of all career levels. By sending a team member, you’re not just supporting professional growth—you’re investing in stronger leadership, higher engagement, and measurable team performance gains that directly benefit your organization.
Actionable Leadership Development
• Proven frameworks from TED-style talks, keynotes, and workshops led by healthcare’s top executives.
• Topics include empathy, resilience, communication, and multi generational leadership.
• All sessions include on-demand access, presentations, and toolkits designed for immediate implementation. 1 2 3 4 5
Scalable Learning & On-Demand Resources
• Every session provides tangible takeaways and materials—including:
• Step-by-step guides for recreating workshops internally to build other leaders.
• Printable worksheets and templates for post-event use across teams.
• Access to on-demand leadership resources for continued development long after the summit.
• This structure ensures your investment extends beyond one attendee—amplifying impact across our entire organization.
Strategic Relationship Building
• High-impact networking with supply chain leaders, manufacturers, distributors, and innovators.
• Builds pipelines for future partnerships, vendor collaborations, and competitive market insights.
Immediate Knowledge Transfer
• Key takeaways and best practices are provided to attendees in a post-summit debrief.
• Topics include AI in healthcare, team building, and communication, ensuring learnings are applied organization-wide.
Stronger Teams & Elevated Culture
• Attendees will learn how to systematically build high-performing, empowered teams and strengthen executive presence.
• Gain exposure to cutting-edge leadership trends and solutions from respected industry partners.
PWH® 2026 Summit Leadership Panel







Register today to attend the industry’s only conference completely dedicated to inclusive leadership development. Registration at mypwh.org/summit

Julie Berry
Michelle Clouse
Maria Amoedo
Kidney Health: Protecting the Body’s Filters
Maintaining overall health helps protect the kidneys.
 The kidneys act as the one of the body’s primary filters of waste, performing crucial functions to maintain internal balance – yet, more than one in seven adults in the U.S. has chronic kidney disease (CKD), according to the Centers for Disease Control and Prevention (CDC).
Kidney disease is a major public health concern. There are usually no noticeable symptoms in early kidney disease, and the illness often goes undetected until it is very advanced. In fact, about 90% of adults with CKD do not know they have it, according to the National Kidney Foundation.
For this reason, understanding the measures that can be taken to prevent kidney disease is essential to keeping the kidneys functioning properly and to avoid kidney disease.
“No matter what clinical environment you’re in, physicians and healthcare professionals must also recognize and understand good kidney medicine,” said Suzanne Watnick, MD, FASN, ASN Health Policy Scholar and Chair of Policy and Advocacy Committee. “Health systems in general must also have access to proper kidney care so that patients can have access to the treatment that they deserve.”
Dr. Watnick is a Professor of Medicine in the Division of Nephrology at the University of Washington and currently practices in the VA Puget Sound Health Care System in Seattle. She serves on the Quality Committee and Chairs the
Policy and Advocacy Committee of the American Society of Nephrology and is a member of its Home Dialysis Task Force.
“The American Society of Nephrology’s mission is to create a world without kidney diseases, as well as to educate the medical community, drive breakthroughs and innovation and advocate for policies that create changes in kidney medicine and kidney care throughout the world,” said Dr. Watnick.

Prioritizing kidney health
Most people are born with two kidneys, located in the body on either side of the spine, just below the rib cage.
Inside the kidneys are many small components called nephrons which help filter and clean the blood. Once the kidneys filter the blood, it is sent back into the body, and any waste material is moved to the bladder as urine. About every 30 minutes, the kidneys filter all the blood in the body.
For the rest of the population, maintaining healthy kidneys starts with making healthy food choices, introducing physical activity, aiming for a healthy weight, getting enough sleep, stopping smoking, limiting alcohol intake, reducing stress and managing diabetes, high blood pressure and heart disease, according to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
The typical way to diagnose kidney disease is through both blood and urine tests. Physicians can help high risk patients determine the recommended tests and screenings for their specific condition.
Healthy kidneys, according to NKF, automatically remove waste products and extra water from the body, help maintain blood pressure, keep the bones healthy, help make red blood cells and balance important minerals.
Possible signs and symptoms of kidney disease, however, include fatigue, difficult urination, dark or foamy urine, decreased concentration, swollen abdomen, ankles and feet and more.
“There are various stages of chronic kidney diseases. You can have early disease through stages 1 through 5, where you are at the point where you need dialysis or a kidney transplant to survive.”
Patients diagnosed with kidney disease should focus on lowering their blood pressure, managing blood sugar levels, reducing salt intake, avoiding NSAID painkillers and moderating protein consumption.
“Good kidney health is part of overall good health – to maintain good kidney health you need to have a healthy diet, exercise, drinking enough water (follow your thirst) and lead a generally healthy lifestyle,” said Dr. Watnick.
Research and innovation
When kidney disease enters its advanced stages, patients may require intensive treatments such as dialysis or a kidney transplant. Since kidney disease may not have symptoms early on, regular testing – at least once per year for people with known risk factors or symptoms, such as high blood pressure or diabetes – can detect changes in kidney function early on.
The two most common causes of advanced kidney disease are diabetes and hypertension, says Dr. Watnick. Patients are also more likely to develop kidney disease if they have heart disease or a family history of heart failure, according to NIDDK.
“Half of all people starting dialysis are starting because of diabetic kidney disease, and then another quarter are starting because of high blood pressure related kidney disease,” said Dr. Watnick. “Other causes include rarer kidney diseases, genetic abnormalities and anatomic abnormalities, which account for another 20 percent of kidney diseases.”
for general screening of the population at large, but there is recommended screening for certain subgroups of people,” said Dr. Watnick. “Patients with high blood pressure or type 1 or 2 diabetes should be screened regularly for kidney disease.”
Advancements in medication have helped patients manage kidney disease by controlling blood pressure, reducing swelling, balancing minerals, lowering cholesterol and addressing other related issues.
medications, such as SGLT-2 inhibitors and GLP-1 agonists, have been shown to slow down the progression of kidney disease and improve survival in people with kidney disease. There has also been a lot of traction in our field in research on some of the rarer kidney diseases and diseases of the kidney filters.”
Prioritizing one’s overall health is ultimately the best way to manage kidney disease and address kidney health.
Prioritizing one’s overall health is ultimately the best way to manage kidney disease and address kidney health.
The typical way to diagnose kidney disease is through both blood and urine tests. Physicians can help high risk patients determine the recommended tests and screenings for their specific condition.
“There is no current United States Preventative Services Task Force (USPSTF) recommendation
“In the last several years there has been innovation in nephrology where there has been a lot of stagnation in the past,” said Dr. Watnick. “For the earlier stages of kidney disease, prior to dialysis, we now know that certain
“It is important to focus on a heart healthy lifestyle and to get screened by your primary care provider for regular diseases,” said Dr. Watnick. “If you are one of the one in seven U.S. adults with kidney disease, make sure to follow up regularly with your primary care provider or kidney doctor – we now have new therapies that can slow down the progression of kidney diseases and there are a lot of new things coming down the pipeline to potentially result in cures.”
Celebrating transformative work in kidney health
This year marks 75 years of the National Kidney Foundation’s (NKF) transformative work in kidney health, advocacy, research, education, and patient support. Founded in 1950 by a determined mother who challenged the status quo to help her son, NKF has grown into a leading voice in kidney care nationwide.
Over the decades, NKF has driven major advancements, including contributing to the Medicare End-Stage Renal Disease Benefit, which expanded federal coverage for Americans with kidney failure, and helping establish standards like the KDOQI® Clinical Practice Guidelines that have shaped care. The Foundation also played key roles in organ donation awareness and advancing more equitable diagnostic tools, such as the race-free
eGFR equation developed with the American Society of Nephrology.
Now through its “75+You” campaign, NKF aims to impact 75 million lives by 2030 across three strategic pillars: preventing the preventable, enabling patients to live the life they want, and ensuring access to transplants for all. Initiatives include doubling awareness and early testing, expanding home dialysis access, and increasing both living and deceased kidney donations.
During National Kidney Month, NKF encourages people to take the Kidney Risk Quiz, become advocates, or support efforts to revolutionize kidney care and improve outcomes for millions.
For more information, visit: www.kidney.org.

The State of Respiratory Season
While overall respiratory illness levels have dropped since January’s peak, flu-related emergency visits among school-aged children are rising, RSV remains elevated in many states, and COVID-19 activity is ticking up.
 The beginning of 2026 saw an active respiratory season – with the nation battling record cases of influenza virus among increases in cases of respiratory syncytial virus (RSV) and COVID-19.
Visits to a physician for flu-like symptoms – fevers, sore throat, extreme fatigue and body aches – hit the highest level in nearly 30 years in early January, according to the Centers for Disease Control and Prevention (CDC). At least 19 million Americans had come down with the flu by late January – and 10,000, including 44 children, have died from the illness – during the 2025-26 flu season so far.
As of late January 2026, however, the amount of acute
respiratory illness causing people to seek health care is now considered at a “low” level, according to the CDC.
While seasonal influenza activity has remained elevated across the country as of late January, rates had decreased for three consecutive weeks, according to newly released CDC data. Despite flu activity being on the decline overall, flu-related emergency department visits for school-aged children between ages five and 17 increased since
the week of January 19-23, while hospitalizations remained stable, according to ABC News. Flu activity as of late January was increasing or stable in the Midwest, Central and West Coast regions.
Influenza A(H3N2) viruses are the most frequently reported influenza viruses so far this season, per the CDC. A new subclade of influenza A(H3N2) viruses, subclade K, emerged and is the predominant virus among influenza A(H3N2) viruses this year. The CDC reports that national vaccination coverage for influenza, as well as for COVID-19 and RSV vaccines, remains suboptimal for children and adults.
RSV activity is also elevated in many areas of the country, including emergency department visits among infants less than 1 year and children 1-4 years old and hospitalizations among infants less than 1 year old. RSV activity has been increasing in the Southeastern, Southern and MidAtlantic areas of the country – as of December 16, RSV infections are growing or likely growing in 32 states.
Additionally, COVID-19 activity is elevated in some areas of the country. COVID activity remains low at a national level, but activity is increasing as of late January, as indicated by the CDC’s National Wastewater Surveillance System.
The CDC continues to expect that the winter respiratory disease season in the United States will likely have a similar number of combined peak hospitalizations due to COVID-19, influenza and RSV compared to last season.
HIDA Emerging Leaders Class Of 2026: In Their Own Words
 HIDA’s Emerging Leaders program recognizes college students pursuing degrees in supply chain management and public health who have a demonstrated interest in working in healthcare distribution. These students are provided with scholarships to attend HIDA’s annual MedSupplyChain conference. Now in its third year, this class of Emerging Leaders offers an impressive array of credentials and experience.
` This year’s Emerging Leaders were chosen from the most competitive selection process yet, with more than 30 students applying for just 10 spots.
` Students come from eight colleges, the largest cohort of schools ever represented.
` For the first time ever, three graduate students are joining seven undergraduates in the class of Emerging Leaders.
The depth and breadth of this class of Emerging Leaders extends beyond these statistics. We wanted to hear from these students in their own words, asking them to share their interest in the medical supply chain and their motivations to participate in HIDA’s programming. From their responses, several key themes repeatedly emerged:
Advancing operational excellence in medical supply chains
The 2026 cohort draws from a variety of work experience across the continuum of care – with internships and part-time jobs at hospitals, pharmacies and drug manufacturers. These students have contributed to initiatives to improve vaccine access, boost HIV/AIDS research, and promote exercise as a form of preventative medicine. They have global perspectives, with experience spanning the globe from Canada to Nigeria.
Damilola Bolanle from Johns Hopkins University shared that “Before graduate school, I oversaw the movement of investigational medicinal products from manufacturers to over 35 clinical trial sites across
eight countries. This experience deepened my understanding of how operational precision and collaboration underpin supply chain reliability in healthcare.”
Improving patient care through better systems and processes

By Wyeth Ruthven, Director of Congressional and Public Relations, Health Industry Distributors Association
HIDA’s Emerging Leaders possess a deep commitment to improving patient care. They understand that supply chain performance directly affects patients and clinicians. Many describe how operational inefficiency impacts care, and how thoughtful system design can empower healthcare teams and improve outcomes.
According to Shayan Siddiqui from Arizona State, “Healthcare especially motivates me because the stakes are human.” Jadazay Ledbetter at Western Michigan added that: “I was only one class away from applying to nursing school when I realized that what truly interested me wasn’t just patient care itself, but the system that made it possible.”
A passion for innovation, problemsolving, and continuous improvement
Students in the 2026 Class expressed enthusiasm for tackling complex challenges. They are drawn to opportunities to optimize processes, strengthen partnerships, and build more agile, data-driven systems.
Aleeza Rana from Michigan State University commented: “What excites me most about supply chain management is its problem-solving nature. The impacts of COVID-19 and a strained supply chain hit close to home. Seeing how end-toend supply chain processes directly affected families like mine inspired my passion for creating resilient systems.”
Running through all of this year’s Emerging Leaders is a shared dedication to enhancing healthcare access and outcomes through innovative supply chain practices. With such driven and talented individuals entering the profession, the outlook for healthcare distribution is more optimistic than ever.
Henry Schein Names Frederick M. Lowery as CEO
 Henry Schein, Inc. announced the appointment of Frederick M. Lowery as its new Chief Executive Officer, effective March 2, 2026, at which time he will join the Board of Directors.
Lowery succeeds Stanley M. Bergman, who will step down as CEO after 35 years and continue to serve as Chairman of the Board to ensure a smooth and effective leadership transition.
Lowery brings more than two decades of healthcare expertise to Henry Schein, with a strong track record of scaling complex businesses to drive significant growth and sustained value creation. Most recently, he served as Executive Vice President and President, Laboratory Products and BioProduction at Thermo Fisher Scientific, leading the Fisher Scientific distribution channel’s above-market performance. “His experience growing distribution and owned product businesses – including manufacturing, R&D, marketing, and sales functions – closely aligns with Henry Schein’s business model, positioning him well to guide the Company’s next phase of growth and continued execution of its BOLD+1 strategic plan,” Henry Schein said in a release.
“I am honored to join Henry Schein at such a pivotal moment. This is an organization with immense potential to impact clinicians and patients, given its remarkable reputation for innovation, customer service, and partnership,” said Lowery. “I look

forward to working with Team Schein to build on the strong foundation established by Stan while accelerating value creation.”
Prior to joining Thermo Fisher, Lowery worked in leadership roles for Maytag Corporation and General Motors. He holds a master’s degree in manufacturing management from Kettering University (formerly General Motors Institute of Engineering and Management) and a bachelor’s degree in mechanical engineering from Tennessee Technological University.
“I am very pleased to welcome Fred to Henry Schein. Beyond his extensive operational experience, he brings a leadership philosophy that reflects the values that have long defined our Company,” said Bergman. “Fred understands the critical role we play in supporting dental and medical practitioners, and he is exceptionally well
equipped to lead Henry Schein into its next phase of growth.”
“On behalf of the Board, I would like to thank Stan for his exceptional leadership and invaluable contributions over more than three decades,” said Phil Laskawy, Lead Director and Chair of the Nominating and Governance Committee at Henry Schein. “After a comprehensive search process, we are confident that Fred is the right successor to honor Henry Schein’s proud heritage. With extensive commercial, logistics, and manufacturing expertise, and a focus on customer satisfaction, he has the combination of experience and capabilities necessary to accelerate growth and value creation.”
“We are excited about our strategic partnership with Henry Schein and look forward to supporting the next chapter of the Company’s journey under Fred’s leadership,” said Max Lin, Board Member and Vice Chair of the Nominating and Governance Committee at Henry Schein and Partner at KKR. “We believe Fred brings a unique combination of healthcare distribution experience, operational best practices, and accountable leadership that will accelerate our strategic initiatives and further differentiate Henry Schein as a world-class business.”
Frederick M. Lowery
Industry News
Estimates show U.S. health spending grew 7.2% in 2024
U.S. health care spending reached $5.3 trillion in 2024 – growing 7.2% from 2023 – the Centers for Medicare & Medicaid Services reported Jan. 14 in Health Affairs. CMS cited non-price factors, including use and intensity of services, as the primary drivers of increased spending. Spending on hospital care increased 8.9% due to continued postpandemic rebounds in service use.
Clorox to acquire GOJO industries
The Clorox Company announced it has entered into a definitive agreement to acquire GOJO Industries, the Akron, Ohio–based maker of Purell and other skin health and hygiene products, in a cash transaction valued at $2.25 billion. Including anticipated tax benefits of roughly $330 million, the net purchase price totals about $1.92 billion.
The move significantly expands Clorox’s presence in the health and hygiene sector by bringing the market-leading Purell brand into its portfolio, spanning consumer and institutional channels. GOJO, founded in 1946 and generating nearly $800 million in annual sales with strong business-to-business reach, will remain based in Ohio following the acquisition’s completion.
Clorox expects the acquisition to accelerate growth for the Purell brand through its distribution capabilities and to deliver strategic benefits, including cost synergies and earnings accretion by the second year. The transaction is subject to regulatory approval and customary closing conditions and is anticipated to close before the end of Clorox’s fiscal year 2026.
Midmark promotes Sailesh Tangirala to VP of Corporate Strategy

Midmark Corp. announced the promotion of Sailesh Tangirala to Vice President of Corporate Strategy, reinforcing its commitment to innovation and strategic growth.
Tangirala joined Midmark in January 2025 as senior director of corporate strategy. In his new role, Tangirala will lead the development and execution of Midmark’s five-year strategic plan, driving innovation and alignment across all business units.
“Sailesh’s strategic insight and collaborative leadership have already made a significant impact at Midmark,” said Jon Wells, president and CEO of Midmark. “In this expanded role, Sailesh will be
instrumental in shaping our future and delivering on our promise to improve patient-caregiver experiences. His leadership will accelerate the launch of new products and solutions, ensuring Midmark remains at the forefront of healthcare innovation.”
Prior to joining Midmark, Tangirala held senior roles at Mammotome, where he led global product management and strategic marketing. Tangirala earned a Master of Science degree in mechanical engineering from the University of Kentucky and a Master of Business Administration degree from Xavier University.
ZOLL LifeVest® WCD saved 143 lives over the holiday season
ZOLL®, an Asahi Kasei company that manufactures medical devices and related software solutions, announced that the LifeVest® wearable cardioverter defibrillator (WCD) saved 143 patients between Thanksgiving Day (U.S.) and New Year’s Day, an average of four patients per day. LifeVest is a wearable cardioverter defibrillator (WCD) that is prescribed to heart patients who are at temporary risk of sudden cardiac death due to certain rapid life-threatening heart rhythms. When needed, the device can deliver a lifesaving treatment shock.
Sailesh Tangirala

Improving Patient Health Better BP®
Heart disease is the leading cause of death for Americans today and hypertension is a contributing and modifiable risk factor for heart disease and stroke. 1 Proper patient positioning alone can lower resting blood pressure (BP) measurements by 7 mmHg systolic and 4.5 mmHg diastolic. 2 That’s why, Midmark designed the first and only fully integrated point of care ecosystem that has been clinically validated to achieve improved accuracy for a resting BP.
01 Low-height exam chair helps patients keep their back supported and feet flat on the floor
Articulating arm rail supports the patient’s arm with cuff at heart height
02 Automated vital signs promote consistency and data accuracy
03 EMR connectivity improves workflow efficiency and reduces errors
midmark.com/improve-bp
Scan to explore the latest study reporting the cumulative effect of poor positioning that occurs when BP is taken with the patient sitting on a typical clinical exam room table. 1 2 3
1 https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
2 https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(23)00396-6/fulltext
© 2026 Midmark Corporation, Versailles, Ohio USA

Check-up on Device Health During Your Next Off ice Visit
Connect with us and review the latest Baxter and Welch Allyn technology empowering patient exams. ON SPOTLIGHT THIS MONTH:

Welch Allyn Diagnostic Cardiology Suite

















Welch Allyn Integrated Wall Systems

Welch Allyn RetinaVue 700









Welch Allyn Spot 4400 Vital Signs Device
< Scan To View Our Current Promotions
Rx Only. For safe and proper use of the product mentioned here, please refer to the appropriate Operator’s Manual or Instructions for Use.
Baxter, Hillrom and Welch Allyn are trademarks of Baxter International Inc. or its subsidiaries.
US-FLC45-260004 (v1.0) 02/2026