
Heart of Aotearoa
Letitia's message
Pregnancy and the risks of heart disease
COPD and your heart
TEER – open-heart surgery alternative still unfunded
How TAVI is transforming care in Aotearoa
You can also read this magazine online. Just head to issuu.com/betterbreathing
Please recycle this material after use. This material has been printed with vegetable oil-based/mineral-free inks. The paper used comes from sustainable forests.
Thank you to our sponsors for supporting this magazine.

Chief Executive
Letitia Harding
Research and Education Manager – Cardiac Health
Dr. Lina Goldstein
Individual Giving Fundraising Executive
Michaela Tahere
Grants & Fundraising Executive
Hannah Aslett
PR & Comms Marketing Manager
Chloe Bradwell
Digital Marketing Specialist
Sam Treseder
Digital Content & Marketing Advisor
Jared McOnie
Digital Content Advisor
Cat Mercer
Community Educator Manager
Sharon Pihema
Corporate Sponsorship & Engagement Advisor
Paul Aschenberger
Office Administrator
Lola Sachkova
Medical Director
Dr. Sarah Fairley
Chief Cultural Advisor – Māori
Sir John Clarke, KNZM, CNZM
Level 2, 85 The Terrace Wellington 6011 PO Box 1459, Wellington 6140
ph: 0800 100 506
kmtrust .org.nz


LETITIA'S MESSAGE
WELCOME TO THE second edition of the Heart of Aotearoa magazine.
In this edition, we provide interesting in-depth articles on cardiac procedures and medicines you may want to know a little more about.
Firstly, we take a closer look at Transcatheter Aortic Valve Implantation (TAVI) — a minimally invasive procedure that replaces a diseased, narrowed aortic valve (aortic stenosis) without open-heart surgery. You can hear more about this procedure from Dr Sanjeevan Pasupati, who is one of New Zealand's leading cardiologists in structural heart disease and has mentored many sites internationally and nationally in the development of the TAVI programme.
Then our very own Cardiology Advisory Board member, Dr Andrew Chatfield, takes a second look at the Transcatheter Edgeto-Edge Repair (TEER) technique and device. This is another type of medical procedure that can repair a heart valve without the need for open-heart surgery. Read more about this on page 6.
Both of these techniques are examples of why we should be applying value-based modelling when it comes to funding decision-making in the cardiology space.
Funding cardiac devices through value-based models aligns costs with patient outcomes, shifting away from volumedriven, fee-for-service systems toward reimbursement based on
effectiveness and quality. This approach reduces hospitalisations and better manages chronic cardiac conditions, saving millions to our healthcare system while also improving patient experiences and ultimately saving lives.
On page 12, Dr Robert Lewis, an Auckland-based respiratory specialist, talks to us about a little-known disease called Pulmonary Arterial Hypertension (or PAH). This chronic, progressive disease, which affects the heart and lungs, is characterised by high blood pressure in the lung arteries due to narrowed, stiffened vessels, forcing the heart's right side to work harder, which can lead to failure.
Finally, at the end of last year, the Trust was pleased to host a tikanga and te ao Māori introductory session for cardiac staff at Wellington Hospital. Having Dame Rangimarie Naida Glavish share her vast experience and knowledge in the health sector was a huge honour. New Zealand hospitals employ numerous international staff, and we need to take the time to teach them about health and wellbeing from
the Māori perspective. Dame Naida provided an insight into “Haki Nohi” to help understand Māori patient needs and wellbeing, whilst also noting that this representation is not exclusive to Māori but can benefit all patients. We thank Sir John Clarke — our Māori Cultural Advisor — for facilitating this insightful session. I am pleased to say that as a result of the positive feedback from this session, Sharon Pihema, our Āpiha Takawaenga Māori, alongside Sir John are currently working on a resource for cardiac staff to use with Māori patients, and we hope to host this on our website in the coming months.
Thank you all for travelling on this cardiac journey with us. We are excited to extend our expertise into the cardiac space, and we look forward to a very exciting 2026!
Noho ora mai,
Letitia Harding Kia Manawanui Trust — The Heart of Aotearoa NZ Chief Executive

RIGHT: (From left) Trust Community Educator Manager Sharon Pihema, Trust CEO Letitia Harding, and Dame Rangimārie Naida Glavish.
GAPS IN HEART HEALTHCARE PUTTING PREGNANT WOMEN AT RISK
A LEADING HEART specialist is calling for greater access to lifesaving cardiac care for pregnant women in New Zealand to prevent harm to mothers and babies.
Dr Sarah Fairley, Medical Director of Kia Manawanui Trust – The Heart of Aotearoa and Interventional Obstetric Cardiologist, says current gaps in care put many women — especially those living in rural areas — at risk of complications during pregnancy.
There is also increased risk of cardiac events later in life in those women who have experienced an adverse pregnancy outcome, including pre-eclampsia, gestational diabetes, hypertension (high blood pressure), pre-term birth, and fetal growth restriction or worse, Dr Fairley says.
"The problem we have in New Zealand is not a lack of expertise, it is less awareness of what constitutes a high-risk pregnancy, issues with access to streamlined funded services, and awareness of the importance of post-partum follow-up for women who have had cardiac issues during pregnancy."
Pregnancy places major stress on the heart.
For women with known or previously undiagnosed heart disease, this can turn into a high-risk situation without access to specialist expertise and tests, Dr Fairley says.
Globally, cardiovascular disease is the leading cause of death in women.
Typically, this risk is addressed through Pregnancy Heart Teams: dedicated multidisciplinary teams that manage women with heart disease from before pregnancy, through pregnancy, delivery, and the postpartum period.
These teams were first recommended in the 2018 European Society of Cardiology (ESC) guidelines. The 2025 ESC guidelines now state that Pregnancy Heart Teams should be established in all referral hospitals, with care spanning pre-pregnancy through to post-partum follow-up.
Trust Chief Executive Ms Letitia Harding says that while major hospitals in New Zealand have these teams, access to them remains inconsistent and often depends on where a woman lives rather than on her level of risk.
That’s why the Trust is calling for a nationally-mandated referral pathway so women with known or suspected cardiac risk can access care rapidly.
Talk to your healthcare provider about heart disease
Download and print our conversation guide by scanning the QR code below or heading to kmtrust.org.nz/pregnancy

CARDIOPULMONARY OBSTRUCTIVE PULMONARY DISEASE
LIVING WITH COPD? CHECK YOUR HEART WITH YOUR GP
If you have cardiopulmonary obstructive pulmonary disease (COPD), you’re at higher risk of heart disease.
MANY SYMPTOMS overlap between COPD and heart disease, meaning COPD could be masking signs of underlying heart problems.
COPD puts extra strain on your heart, and over time this can lead to serious cardiovascular problems like heart failure or irregular heartbeats.
People with COPD are 2–4 times more likely to die from heart disease. With COPD, your heart has to work harder to pump oxygen around your body. The risk increases even more
during COPD flare-ups, when heart problems can develop quietly and go unnoticed.
High blood pressure affects an estimated 30–50% of people with COPD. Those living with the disease also have a 28% higher risk of irregular heart rhythms, and this doubles with frequent flare ups.
Detecting heart disease early can help prevent serious complications, and it starts with talking to your doctor about your heart health.

Be aware of these symptoms:
Ǫ Shortness of breath
Ǫ Chest discomfort or tightness
Ǫ Swelling in legs, ankles, feet or abdomen
Ǫ Racing, irregular or pounding heartbeat, or an erratic pulse
Ǫ Breathlessness when lying flat or walking up incline
Talk to your doctor
This guide has been designed to help you have better conversations with your doctor about COPD and heart disease.
Download and print our conversation guide by scanning the QR code below or heading to kmtrust.org.nz/copd-day

FIXING THE HEART VALVE
THE ROLLOUT OF A LIFE-CHANGING PROCEDURE
While Transcatheter Edge-toEdge Repair (TEER) is proven to be lifesaving for high-risk patients with mitral valve disease, New Zealand’s rollout remains slow, uneven, and underfunded.
Regional disparities, workforce shortages, and lack of national coordination mean many patients — particularly elderly and Māori or Pacific populations — still face barriers to this minimally invasive treatment.
Expanding TEER access requires investment, national planning,
IN NEW ZEALAND
and equity-focused strategies to prevent unnecessary suffering and deaths.
For patients who are eligible but unable to access TEER, the consequences are immediate. Delayed or absent treatment can mean repeated hospitalisations, worsening heart failure, and, in some cases, no viable intervention at all. In practice, access is shaped by restrictive funding, workforce pressures, and where services are available.
This is the second part in a series exploring TEER in New Zealand. In the first article, we looked at how the procedure works and why it offers highrisk patients a minimally invasive, life-saving alternative to open-heart surgery. Here, we examine why access in New Zealand remains uneven, the systemic barriers at play, and what needs to change to bring TEER to all who could benefit.
A growing health challenge
Heart valve disease is increasingly common in Aotearoa.
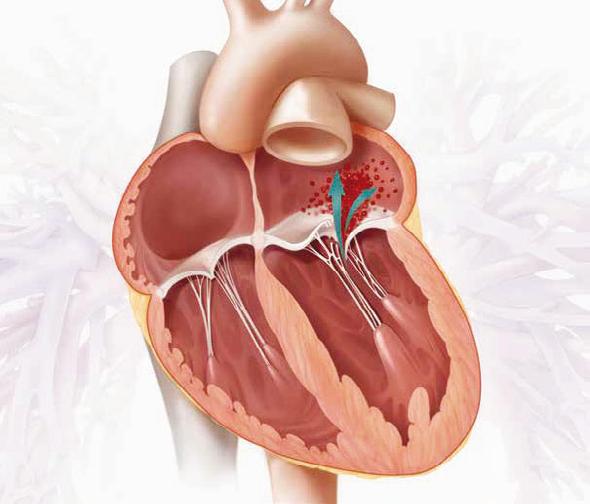
As our population ages and cardiovascular disease rates remain high, conditions such as mitral regurgitation — where the mitral valve leaks and forces the heart to work harder — pose a serious threat to patients’ health.
Left untreated, it can lead to heart failure, repeated hospitalisations, and premature death.
Traditionally, open-heart surgery has been the standard treatment, but many older or frail patients are considered too high-risk for such invasive procedures.
TEER offers a minimally invasive alternative.
By repairing the valve through a catheter rather than opening the chest, it reduces surgical risk and shortens recovery, often allowing patients to leave hospital within a day or two.
Globally, it has become a routine procedure for high-risk patients. But in New Zealand, access is still limited and inconsistent.
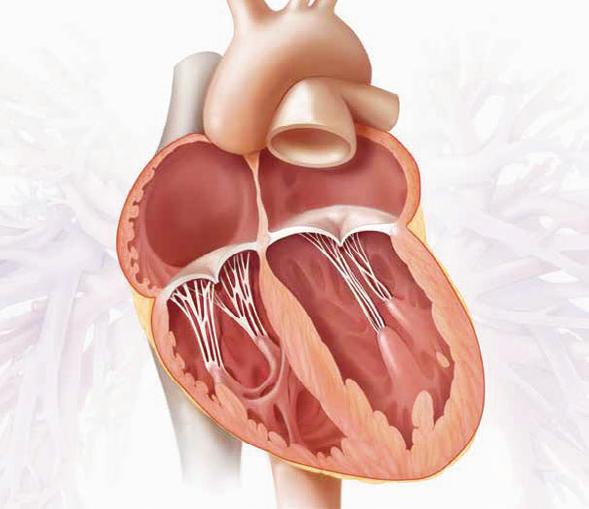
How TEER works
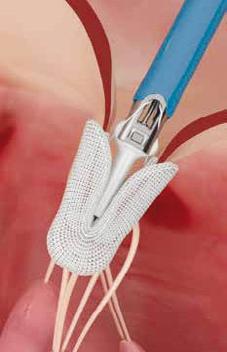
TEER is performed via a catheter inserted through the femoral vein.
A specialised clip attaches to the valve leaflets, reducing leakage and restoring more normal blood flow — all without stopping the heart. TEER preserves the patient’s native valve rather than replacing it, enabling faster rehabilitation and fewer complications.
For patients previously deemed too high-risk for open-heart surgery, TEER can be transformative.
It allows patients to maintain a higher quality of life, avoid long ICU stays, and recover more quickly than with traditional surgery.
Access remains uneven
Despite its clinical value, TEER has not been widely adopted in New Zealand’s public health system.
Dr Andrew Chatfield, Coronary and Structural Interventional Cardiologist and member of the Kia Manawanui – The Heart of Aotearoa Cardiac Advisory Board, says progress is being made, but slowly and without a clear national plan.
“Progress is happening but in fragments: it’s very slow and it’s sort of happening piecemeal rather than a big, clear national approval to treat your patients, but I'm positive about it happening — eventually — in New Zealand.”
While most major centres now offer the procedure, Wellington has yet to fully implement it.
“In the TEER space, we are lagging a long way behind — particularly Wellington, which is a shame,” Dr Chatfield says.
Currently, patients in regions without TEER must travel long distances for treatment or wait indefinitely for local services to start.
Funding is also a major barrier. TEER is approved by Health NZ Te Whatu Ora but is not yet publicly funded through PHARMAC.
“Privately, only a small number of people in New Zealand are able to pay out of pocket in full, which highlights some inequality,” Dr Chatfield says.
“Not many can afford to do this, leaving many others without that option.”
The lack of funding and regional access means that patients who could benefit most from TEER are left with either high-risk surgery or no treatment at all, he says.
“Some of these leaky valves that could be fixed with TEER,

ABOVE: Consultant in Coronary and Structural Interventional Cardiology Dr Andrew Chatfield is also a member of the Cardiac Advisory Board at Kia Manawanui Trust – The Heart of Aotearoa.
particularly in patients with other cardiovascular and noncardiovascular risks, could avoid higher-risk surgery.
“Without access, some may not be getting any treatment at all,” Dr Chatfield says.
“If TEER remains inconsistently available, existing cardiovascular inequities risk widening rather than narrowing.”
For patients previously deemed too highrisk for open-heart surgery, TEER can be transformative.
Workforce and infrastructure challenges
Access is also constrained by workforce shortages and stretched hospital resources.
New Zealand currently has only a third of the cardiologists it should have, and many hospitals operate under capacity pressures.
“We are operating within a stretched and stressed healthcare environment,” Dr Chatfield says.
“Supporting additional resources such as sonographers, nurse coordinators, extra beds, and nursing staff will help ease the workload and improve patient recovery.”
These challenges mean that even when TEER devices are available, hospitals may not have the capacity to perform procedures for all eligible patients, particularly in smaller or underresourced regions, he says.
Economic and clinical case for TEER
Experts emphasise that expanding TEER access is not only clinically important — it’s economically rational.
Delays in treatment lead to repeated hospitalisations, ambulance transfers, and extended rehabilitation, costing the healthcare system far more than the procedure itself,” Dr Chatfield says.
“Supporting TEER isn’t just a compassionate choice — it makes financial sense.
“The cost of repeated hospital stays, ambulance trips, and long
recoveries far outweighs the cost of the procedure itself.”
Investing in TEER would allow hospitals to treat high-risk patients more efficiently, reduce strain on intensive care units, and improve outcomes for patients who might otherwise be ineligible for treatment, he says.
Equity implications
Unequal access to TEER risks worsening existing health disparities.
Māori and Pacific people in New Zealand develop and die from cardiovascular disease significantly earlier than other populations.
Without equitable rollout of minimally invasive procedures like TEER, vulnerable populations may continue to miss out on treatment that could prevent high-risk surgery or death.
Moving toward national coordination
Dr Chatfield is involved in initiatives to track TEER outcomes, waitlists, and equity metrics nationwide.
He believes a national structural heart registry would help provide visibility into who is receiving

TEER, where procedures are being performed, and where gaps in access remain.
Infrastructure improvements may also help expand services in regions currently unable to provide the procedure, he says.
Wellington Hospital, for example, is expected to receive a second cardiac catheterisation laboratory later this year.
“Once the labs are fully up and operational, I don’t see a strong reason why TEER can’t be done in Wellington,” Dr Chatfield says.
Establishing national coordination, alongside investment in staffing and infrastructure, could help bring New Zealand in line with countries such as Australia and the UK, where TEER is widely available for high-risk patients.
The future of TEER in New Zealand
As the population ages, more people will require timely interventions for mitral valve and other structural heart diseases.
TEER offers a minimally invasive, life-saving option for those who would otherwise be denied treatment due to risk factors or geography.
But unless New Zealand addresses funding, workforce, and equity barriers, patients will continue to face unnecessary delays and uneven access.
“We have the technology, we have the expertise, and we have patients who desperately need it,” Dr Chatfield says.
“What’s missing is a system ready and willing to deliver it to everyone who could benefit.”
LEFT: Dr Andrew Chatfield holding a prototype of an implant system used in a TEER procedure to treat patients with conditions like mitral valve regurgitation.




HOW TAVI IS TRANSFORMING CARE IN AOTEAROA
FOR DECADES, open-heart surgery was the standard treatment for patients with severe aortic stenosis — a life-threatening narrowing of the heart’s aortic valve caused by wear and tear.
As the valve stiffens, it becomes harder for the heart to pump blood around the body. Left untreated, the condition can lead to heart failure, chest pains, loss of consciousness, or sudden death.
Today, a much less invasive treatment is transforming care.
Transcatheter Aortic Valve Implantation (TAVI) allows doctors to replace the diseased valve through a small incision, often through an artery in the groin, without opening the chest.
Many patients can undergo the procedure under conscious sedation, return home the next day, and recover far more quickly than after traditional open-heart surgery.
International guidelines increasingly support TAVI as a preferred treatment for many patients who meet the criteria. But access to the procedure — and to the diagnostic tests that identify patients who need it — is not always consistent across Aotearoa New Zealand.
Part of the challenge is workforce capacity. While New Zealand’s population has grown by around 17% since 2013, the cardiac workforce has not kept pace. In fact, in some areas it has declined.
Today, there are only half as many cardiac sonographers as there were in 2013, despite growing demand. These specialists perform echocardiograms — ultrasound scans that detect conditions such as aortic stenosis before they become emergencies. At the same time, New Zealand has only about one-third of the cardiologists it needs.
Fewer specialists can mean longer waits for diagnosis, assessment,

and treatment, potentially delaying access to procedures such as TAVI.
A treatment changing how heart valve disease is managed
Dr Sanjeevan Pasupati, one of New Zealand’s leading interventional cardiologists specialising in structural heart disease, was a pioneer of TAVI in Aotearoa.
“In Waikato, we're doing well. We perform about 200 TAVI procedures each year, but that’s not enough — we need to do more.
“There’s still more to be done for the rest of New Zealand — some regions haven’t caught up yet.”
For suitable patients, the difference between TAVI and open-heart surgery can be significant.
Because the procedure is far less invasive, recovery is usually quicker and complications are often fewer. Many patients return home the following day and resume everyday activities sooner than they could after major surgery.
In recent years, the group of patients who may benefit from TAVI has expanded.
International guidelines increasingly support the procedure for a broader range of patients, including some aged between 65 and 80. New national guidelines are expected to bring New Zealand practice more closely into line with these recommendations.
LEFT: The first TAVI being used to replace a valve in a patient, 2008.
However, introducing new treatments into a health system is rarely just about technology or clinical expertise.
“The hardest part is getting patients worked up and ready,” Dr Pasupati says.
“The investigations need to be done before and after TAVI procedures.”
Preparing patients for TAVI requires detailed imaging, including CT scans and echocardiograms.
Limited access to these services in some regions can slow the process of identifying suitable patients and preparing them for treatment. Ongoing imaging is also needed after the procedure to monitor the replacement valve.
A second chance at life
For some patients, TAVI offers a second chance.
Susan Bennett experienced this first-hand.
After being diagnosed with aortic stenosis, she initially underwent open-heart surgery to replace her valve.
However, the valve implanted during surgery turned out to be too small for her body, leaving her struggling to recover.
“I couldn’t get out of bed. I didn’t care about showering or cleaning my teeth, and that’s not like me,” she says.
Doctors later determined that TAVI might offer another option.
At the time, Susan was younger than the typical age threshold for the procedure, but her medical
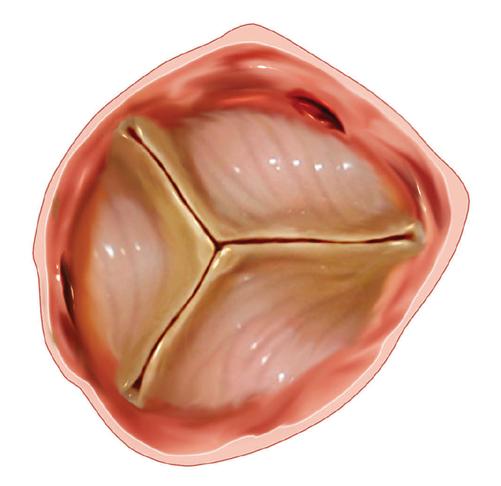

Normal valve Stenotic valve
team advocated for her to receive it following a suboptimal outcome from cardiac surgery.
“It was just so much easier on my body,” she says.
“My family couldn’t believe it when they saw me sitting up after TAVI — the difference was incredible."
“My doctors virtually saved my life because they couldn't redo me with open heart,” she says.
“There was no other way to save me other than TAVI.”
Nearly a decade later, Susan continues to live well with her implanted valve.
Uneven access across the country
Although TAVI is funded through the public health system, access can vary depending on where patients live.
Because the procedure is not mandated nationally, individual hospitals determine how many procedures they can provide.
“We’ve come a long way, but there is still more to do to make access equitable across the country,” Dr Pasupati says.
Capacity constraints play a role. In some regions, limited catheter laboratory availability and restricted access to CT imaging can delay assessment and treatment.
Growing demand for echocardiography also places pressure on a workforce that has already declined.
While the valve used in TAVI is more expensive than a surgical valve, the overall periprocedural cost is much cheaper, and focusing only on the valve cost misses the broader picture, Dr Pasupati says.
“When you look at the total cost of care, TAVI is cheaper,” he says.
TAVI represents a major advance in the treatment of severe aortic stenosis, offering many patients a safer and less invasive alternative to open-heart surgery.
But ensuring that people across New Zealand can benefit from it will require support from the top down, Dr Pasupati says.
“Without addressing the ongoing pressures facing cardiac care in New Zealand, some patients will continue to face significant delays.”
New Zealand has only one third of the cardiologists needed by international standards.
PULMONARY ARTERIAL HYPERTENSION IN AOTEAROA: A Q&A WITH DR ROBERT LEWIS
Pulmonary arterial hypertension (PAH), also known as Group 1 Pulmonary Hypertension, is a rare but serious condition in which high blood pressure develops in the arteries of the lungs, placing strain on the right side of the heart.
Over time, these arteries become narrowed and stiff, forcing the heart to work harder to pump blood through the lungs.
We spoke with Dr Robert Lewis, a respiratory physician and pulmonary hypertension specialist, about what PAH is, how it is treated in New Zealand, and where the gaps in care remain.
Q: What exactly is pulmonary arterial hypertension?
A: PAH is one of the few conditions that truly bridges cardiology and respiratory medicine. Pulmonary arterial hypertension directly affects the small blood vessels deep within the lungs. Those vessels become narrowed and tighter, which makes it harder for blood to flow through them. Over time, this increased resistance means the right side of the heart has to work much harder to pump blood through the lungs. It is like putting your finger over the end of a hosepipe — the pressure builds up, and eventually the right side of the heart can weaken or fail. Importantly, PAH is only one type of pulmonary hypertension. Pulmonary hypertension is an umbrella term
for high blood pressure in the lungs and is commonly seen in association with other conditions affecting the heart and lungs, where treatment should focus on the underlying condition.
Q: How rare is PAH in New Zealand?
A: PAH is rare. Internationally, the incidence is around six cases per million adults per year. It is unknown exactly how many New Zealanders have this condition, but probably a few hundred. To address this gap in knowledge, myself and a group of clinicians are working on being able to contribute to the Pulmonary Hypertension Society of Australia and New Zealand (PHSANZ) Registry, hopefully including data from hospitals nationwide. We don’t know our true numbers. We don’t know outcomes for Māori patients. We don’t know how our mortality compares internationally, so collecting this data is critical, not just for understanding how the disease affects patients in our country, but for advocating for better therapies.
Q: How do patients typically present?
A: Diagnosis is often delayed. People may see many doctors before they finally receive a diagnosis. The most common symptom is progressive breathlessness, which can initially be subtle but gradually becomes debilitating, even in young patients. As the condition progresses, patients may develop light-headedness, chest pain and signs of right heart failure, such as fluid build-up in the legs. PAH can affect people across the
lifespan and may be associated with other conditions, including systemic sclerosis and certain congenital heart diseases.
“PAH
is rare.
Internationally,
the incidence is around six cases per million adults per year."
Q: What is the outlook?
A: Before modern treatments, median survival was estimated at around three years, but that was around 30 years ago, before we had effective therapies. Today, prognosis has improved significantly, but outcomes vary and there are many unmet needs. Some patients respond well to oral tablet therapies, while others require more aggressive treatments, including frequent nebulised therapy (up to seven times daily), or continuous intravenous (epoprostenol) infusion, delivered via a pump 24/7. These treatments can be lifeprolonging, but they come with a significant burden. For advanced cases, lung transplantation is considered. In most cases, only a lung transplant (not heart and lungs) is required, as the right ventricle can recover once lung resistance is removed.
Q: What treatments are available?
A: There are a number of therapies that are not funded here and that we need to have access to in New Zealand. PAH
therapies have traditionally targeted three main biological pathways. In New Zealand, funded medicines are available through Special Authority, meaning strict eligibility criteria apply. However, several therapies used routinely internationally are not yet funded here. There are three medicines routinely used in other countries such as the UK for at least the last 7 years that are still not widely funded in New Zealand: Tadalafil (Adcirca), Riociguat (Adempas) and Selexipag (Uptravi). Applications for Tadalafil and Riociguat are currently under assessment by Pharmac, but no final funding decision has been announced. For medicines not listed under Special Authority, clinicians must apply via the Named Patient Pharmaceutical Assessment (NPPA) process — a timeconsuming application that must be resubmitted every few months. It’s extremely laborious and relies on clinician time and motivation. It is not sustainable long-term.
“There are a number of therapies that are not funded here and that we need to have access to in New Zealand."
Q: What about new and emerging therapies?
A: One new drug, in particular, is generating a lot of global excitement: Sotatercept (Winrevair). Sotatercept targets a newly identified fourth pathway in PAH and has shown potentially game-changing results overseas. Patients have heard about it, and there is a great sense of hope around it. However, access in New Zealand is extremely limited. Only a very small number of patients have obtained it via NPPA in
exceptional circumstances. It is not yet funded at scale here, or in Australia. International evidence suggests Sotatercept may even allow some patients to come off continuous intravenous infusion therapy, replacing it with an injection given approximately every three weeks. This drug would be transformative for so many patients living with PAH.
Q: How does New Zealand compare internationally?
A: There is a clear medicine access gap. Drugs we were using in the UK in 2019 are still not available here. Geography and service distribution also create challenges unique to Australia and New Zealand. A new Australia-New Zealand position statement is currently being finalised to address these regional realities. The lack of registry data
also weakens New Zealand’s position when advocating for funding. If we can demonstrate our numbers and our outcomes, that becomes powerful evidence — it helps show what is needed.
Q: What’s your message to patients and whānau?
A: This is a rare condition, but there are experienced clinicians who are passionate about looking after you. We are absolutely motivated to give you the best treatments we can. We will advocate on your behalf. New drugs are on the horizon, and that gives me great hope. However, regardless of what happens with funding or therapies, we will continue to support you the whole way through the journey, as well as we can.

RIGHT: Respiratory physician and pulmonary hypertension specialist Dr Robert Lewis.