The Australian Nursing and Midwifery Federation WA (ANMF WA) is the brand name that represents two entities: the Australian Nursing Federation Industrial Union of Workers Perth and the Australian Nursing and Midwifery Federation WA Branch. Romina Raschilla (RN MBA) is State Secretary of both entities.
Acknowledgement
The Australian Nursing and Midwifery Federation Western Australia acknowledges the Traditional Custodians of the Lands on which our services operate throughout WA. We pay our respects to Elders past, present and emerging. We are committed to walking alongside all First Nations Peoples on our journey of reconciliation.
The beginning of a new year offers a natural opportunity to reflect on the past and look ahead to the priorities that will shape our future, and I think you’ll find this edition strikes a good balance between reflection and forward focus.
It’s our first issue since introducing our new brand name and I’m so happy to see the word ‘midwife’ featured heavily throughout these pages. I encourage you to take time to read about two particularly special midwives –our former president Margaret Baird and Australian Midwife of the Year Carli Beange. I wasn’t lucky enough to meet Margaret personally but it’s clear she was a remarkable woman and the work of today’s midwives, like Carli, is immeasurably shaped by her contribution. I know many of you are feeling her loss.
You can also read recaps from two significant events of last year –our AGM and the ANMF national conference, as well as take a deep dive into what it means to be a workplace delegate, a role that will have a huge influence on our work this year.
2026 is shaping up to be a big year. Our Council is in the process of developing a strategic plan that will clarify our union’s purpose
(why we exist), our vision of where we’re heading and the values that will drive our behaviour and actions along the way. It’s important for us to have a clear strategy in place to guide our decisions and ensure we’re focused on the right priorities, and I look forward to sharing more about this in the months ahead.
In the meantime, there’s plenty of hard work continuing to improve member experiences, expand risk management capabilities and ensure we’re meeting our regulatory obligations. This involves developing new policies, processes and systems (including a much-needed upgrade to our membership management system!) to modernise our union. While this might not be the most headline-grabbing work, it’s setting vital foundations for our future and will have a ripple effect on what we can achieve together.
We’re also recruiting more industrial advisors so we can continue improving the speed and quality of support you receive when contacting us about individual issues or navigating the bargaining process. At the same time, we’re going to be more active out in the workplace so we can help to stop issues in their tracks and build greater connections with you.
In 2026, we will continue to strengthen our collaboration with peers from the federal team and other ANMF branches on important issues, such as aged care reforms. We will also play an active role on government working groups focused on key initiatives, including the continued rollout of ratios. We won’t stop focusing on ratios until they are extended to every part of the WA health system, with all compliance and reporting obligations being met.
I look forward to working with as many of you as possible this year as we continue to advocate for important changes that will improve your working lives in all sorts of ways, while ensuring decisions are always made with patient care at the heart.
Romina Raschilla, RN MBA ANMF WA State Secretary
A name that reflects who we are
For several years, members have been telling us that our name no longer reflects who we are. In response to that feedback, we’ve now changed our brand name to the Australian Nursing and Midwifery Federation WA (ANMF WA).
The addition of “midwifery” and “Western Australia” signals our commitment to inclusion, modernising our union and aligning to the national federation to amplify our collective voice.
3 THINGS TO KNOW ABOUT OUR NEW BRAND NAME
1. This change was driven by members
Over the past year, feedback came through workplace conversations, social media comments and responses to the frontline feedback survey. In response, members were invited to take part in a formal survey to choose between two name options, both of which included midwifery. The outcome was clear, with 83% of participating members supporting Australian Nursing and Midwifery Federation WA (ANMF WA).
2. We are still two entities
We will continue to be two separate entities –the state-registered union and the WA branch of the national federation. ANMF WA is the name we will use to brand ourselves, reflecting who we are and how members recognise their union. This change will not otherwise affect your experience as a member.
3. The change will be gradual
The transition to the new name will be gradual and cost-conscious. Digital platforms such as our website and social media will be updated first. Printed materials, merchandise and other items will be updated over time as they are ready to be restocked, helping minimise waste and unnecessary expense. This change will not otherwise affect your experience as a member.
Quick explainer
Australian Nursing Federation Industrial Union of Workers Perth
State registered union
Australian Nursing & Midwifery Federation WA Branch.
State branch of the federal union
The name we use to brand ourselves
Become an ANMF WA WORKPLACE DELEGATE
A workplace delegate is someone who steps forward to make sure no one stands alone.
We are looking for members who want to take an active role in supporting their colleagues and strengthening the union at work. You will be essential in keeping members connected and informed.
As a workplace delegate, you will:
Unite your colleagues and keep everyone connected to their union.
Share updates and campaign actions that strengthen our collective voice.
Support campaigns to improve pay, conditions and workplace safety. Help identify and resolve workplace issues quickly.
Ready to lead?
Scan the QR code today and register your interest in becoming a workplace delegate.
Francesca Tantino, ANMF WA Lead Organiser
2025 AGM wrap-up
On 20 November, members came together for our 2025 Annual General Meeting (AGM), marking the first time since 2008 that a quorum was achieved. The night highlighted the progress made over the past year and the strong foundations being built for the future.
The meeting opened with a moving Welcome to Country from Nyoongar Elder Theo Kearing and his nephew. From there, members were taken through a summary of key activities, covering improvements to the overall member experience, governance, union operations and strategic planning.
A central achievement this year has been opening our members helpline from 9am to 5pm weekdays, with no booking required, to make it easier for members to reach industrial, legal and professional support when they need it. The changes made throughout the 24/ 25 financial year have already resulted in stronger advocacy, faster response times and improved advice for members facing workplace issues.
Members were also presented with a preliminary annual financial report, which showed modest revenue growth, decreased expenditure and a strong operating surplus, leaving the union in a strong financial position. The reports presented on the night were formally accepted and members also voted to appoint HLB Mann Judd as the auditor for the next financial period.
A highlight of the evening was the presentation by Lori-Anne Sharp, CEO of the Nurse Midwife Health Program Australia (NMHPA). Lori-Anne spoke about how important it is to have accessible wellbeing support available for nurses and midwives across the country and she explained how the NMHPA’s free, independent peer-to-peer counselling support service works.
State Secretary Romina Raschilla also shared some priorities for the coming year, including continued collaboration with other ANMF state branches and WA health unions, advancing the union’s strategic planning, refreshing the workplace delegate program and advocating for minimum nurse-topatient ratios to be extended across WA. Following the member survey, our new brand name was also announced at the AGM and it will be gradually rolled out in the months ahead.
Nyoongar Elder Theo Kearing and his nephew.
Senior Vice President Terry Jongen and State Secretary Romina Raschilla introducing the new name.
Lori-Anne Sharp, CEO of the Nurse Midwife Health Program Australia
36,886 Full member
4,154 Enrolled
8
42,675
Total number of members
6,091
Total number of helpline calls
3,866 Queries answered immediately
357
431 Student nurse
1,196 Honorary member
926
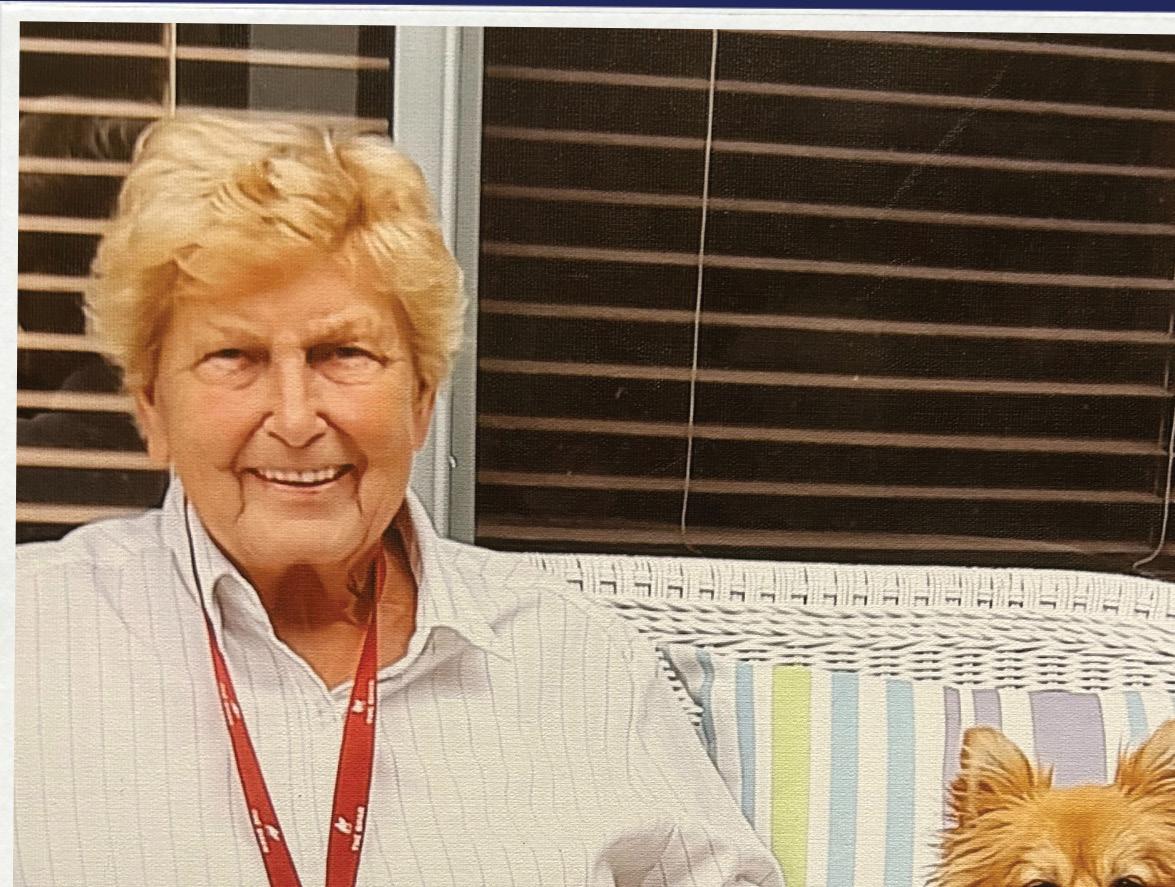
Honouring the legacy of Margaret Baird
Throughout the 100-year history of our union, there have been few people who have made as much of an impact on the WA nursing and midwifery professions as Margaret Baird.
A former president of our union, Margaret’s leadership was instrumental in many areas, including the transition from hospital-based training to university education. Margaret died peacefully in November and we pay tribute to her legacy and thank her for her contribution.
“She was a fierce advocate for safety, dignity, and professional excellence, insisting that unqualified student nurses should never again be given unsafe clinical responsibilities. Many of today’s core national standards reflect principles she fought to establish,”
- Nathan Joy, Margaret’s grandson
During her time at the union, Margaret contributed to a series of major reforms, including improvements to staffing and safety standards, and the modernisation of clinical supervision and competency frameworks.
Those who worked with her recall her strong advocacy of student nurses and her conviction about the importance of advanced education.
Margaret’s impact extended far beyond her years with the union. In 1984, she established WA’s first university-based School of Nursing, helping to design science-based curriculum that shifted nurse education into a new era. She was known for mentoring educators and emerging leaders, encouraging them to think critically and confidently about the future of the profession.
In the 90s, Margaret led an innovative and forward-thinking maternity service at Peel Regional Birthing Centre, which became a template for midwife-led, woman-centred care and remains influential to this day.
Margaret’s expertise was also sought in the United Arab Emirates and Scotland, where she helped to strengthen nursing education within rapidly developing systems.
Lorrie Gray, a close friend and long-time colleague met Margaret in 1975 at the Western Australian School of Nursing and later worked with her as part of a team responsible for those major curriculum reforms. She remembers Margaret as a leader who inspired enthusiasm in everyone around her. “Margaret was a great ideas person and she needed a team to help her implement those ideas,” Lorrie recalls. “She was great to work for, she would support you all the way. However, there were times when we joked that we didn’t want to walk past her door, as we would be sure to get another job.”
“That advocacy role was definitely a legacy that a lot of us tried to live up to,”
-Lorrie Gray, close friend and long-time colleague
Lorrie describes Margaret as someone who always thought outside the box, a strong-minded leader who expressed her ideas clearly and brought people along with her through collaboration and genuine positivity. Margaret was also known for looking out for others. One example that stayed with Lorrie involved a nurse who was being bullied. Margaret stepped in and took her under her wing, making sure she was not alone in facing the situation. “That advocacy role was definitely a legacy that a lot of us tried to live up to,” Lorrie says.
State Secretary Romina Raschilla attended Margaret’s service, representing ANMF WA. She reflected afterwards on how Margaret inspired her as a pioneer and strong advocate for the profession.
‘“On behalf of everyone at the ANMF WA, we offer our deepest condolences to Margaret’s family and pay tribute to this remarkable woman who has influenced so many people through her training, mentoring and friendship,”
-Romina Raschilla, ANMF WA State Secretary
‘Margaret and her dog Angel, who continued to visit her throughout her final days.
Stepping up to get more involved
Our refreshed workplace delegate program
Workplaces delegates help ensure that nurses and midwives have a voice where it matters most, in their own workplaces. You may have heard the terms job representatives (or reps), workplace leaders or delegates before. These are all referring to members who step up to represent their colleagues in the workplace.
Workplace delegates act as a first point of contact for issues, support and advocating for rights and better conditions. They represent all members in the workplace regardless of their role, provide education about your rights, can support members in meetings and actively participate in negotiations for enterprise agreements.
Delegates are not expected to have all the answers. What they bring is empathy, commitment and firsthand understanding of what it means to deliver care in today’s health system. With the backing of ANMF WA staff (particularly our team of organisers), delegates can lead positive change in every workplace.
Through training and ongoing support, delegates will develop skills in communication, negotiation and problem-solving. They will also learn how to turn conversation into action, helping colleagues stand together to achieve safer, fairer conditions.
THE RIGHT SUPPORT
Behind every workplace delegate is our small but mighty team of organisers and other ANMF staff who will work directly with them to build strength, develop leadership and ensure there’s a strong union presence in their workplace.
Our organisers will be closely connected to delegates and other members, regularly visiting workplaces, listening to member’s stories and helping to identify what matters most. Organisers are great at finding opportunities for growth and understanding the local challenges that affect different workplaces. Organisers empower delegates and members to build the confidence to speak up and take action together, turning everyday workplace issues into opportunities for change.
Once in place, organisers and delegates will work together with members to build stronger, and fairer workplaces.
For example, when a group of nurses raises concerns about staffing levels or unsafe workloads, an organiser can help them to “map” the issue, gather evidence and discuss solutions. Workplace delegates can then lead those conversations with management, supported by the union’s knowledge and resources.
Through this approach, members gain confidence in their ability to act collectively, not just to respond to problems but to prevent them and build better workplaces for everyone.
OUR FOCUS
Our refreshed workplace delegate program will focus on:
OUR VISION FOR THE FUTURE
Our vision is to see every workplace represented by active delegates who are connected, informed and confident in their role. We want nurses and midwives across WA to feel supported, respected and part of something bigger.
Refreshing our delegate program will help us reach more workplaces, connect with more members and grow the next generation of union leaders.
Recruitment and engagement
Growing membership and ensuring every nurse and midwife knows the value of collective strength.
Leadership development
Supporting members who want to become delegates by providing training and mentoring opportunities.
Campaigns and advocacy
Identifying workplaces issues and developing plans that members can act on.
Representation and connection
Ensuring every workplace has a clear link to the ANMF WA and a strong network of support.
By investing in these foundations, we aim to build workplaces where nurses and midwives feel supported and equipped to speak up, take part in campaigns and support one another.
Meaningful change doesn’t happen all at once, it starts with small, deliberate steps – a conversation, a connection, a decision to stand up and be heard. Together, these moments create momentum that drive lasting change across our health system.
HOW TO GET INVOLVED
If you’ve ever spoken up about workloads, fairness, or patient safety, you already have the qualities of a workplace delegate. Consider taking the next step and express your interest in becoming a delegate and acting as a voice for your colleagues.
Whether you’ve been a member for years or just joined, there is a place for you in this vision. The union is not something separate to members. Every member, in every ward, on every shift and in every conversation forms the heart of our union.
TOGETHER WE’RE STRONGER
The work ahead will take time, collaboration and commitment. But with each step, we are building something powerful – a union that truly reflects the voices of members across the state.
As we refresh our workplace delegates program, we’re setting the stage for a stronger ANMF WA that can stand up for the profession, protect members’ rights and make sure every member feels represented and supported.
The union is all of us. And together, we will make it stronger than ever.
We need to talk about productivity
Highlights from the ANMF’s 17th Biennial National Conference
The Australian Nursing and Midwifery Federation’s (ANMF) 17th Biennial National Conference was held on the Gold Coast in October, bringing together more than 100 delegates from across Australia to consider the theme, ‘Productivity with purpose: empowering nurses, midwives and care workers.’
The event provided an invaluable opportunity for delegates to share experiences, debate policy and set priorities for the federation’s work over the next two years. Delegates from every state and territory came together to discuss how the union can continue to strengthen the professions, protect members’ rights and ensure that nurses, midwives and care workers remain at the centre of Australia’s healthcare system.
ANMF WA State Secretary Romina Raschilla said the conference was a fantastic opportunity to collaborate with other branches and hear directly from members about the shared challenges being faced across the country and what people are doing to tackle those.
“It was particularly rewarding to see our delegation of WA members doing such a wonderful job of representing our state and contributing to the discussion. I’m already looking forward to the next national conference, which we will be hosting here in Perth for the first time in 30 years,”
Redefining productivity
With the federal government naming productivity a national priority, the conference was an opportunity to examine what this means in the context of nursing, midwifery and care work.
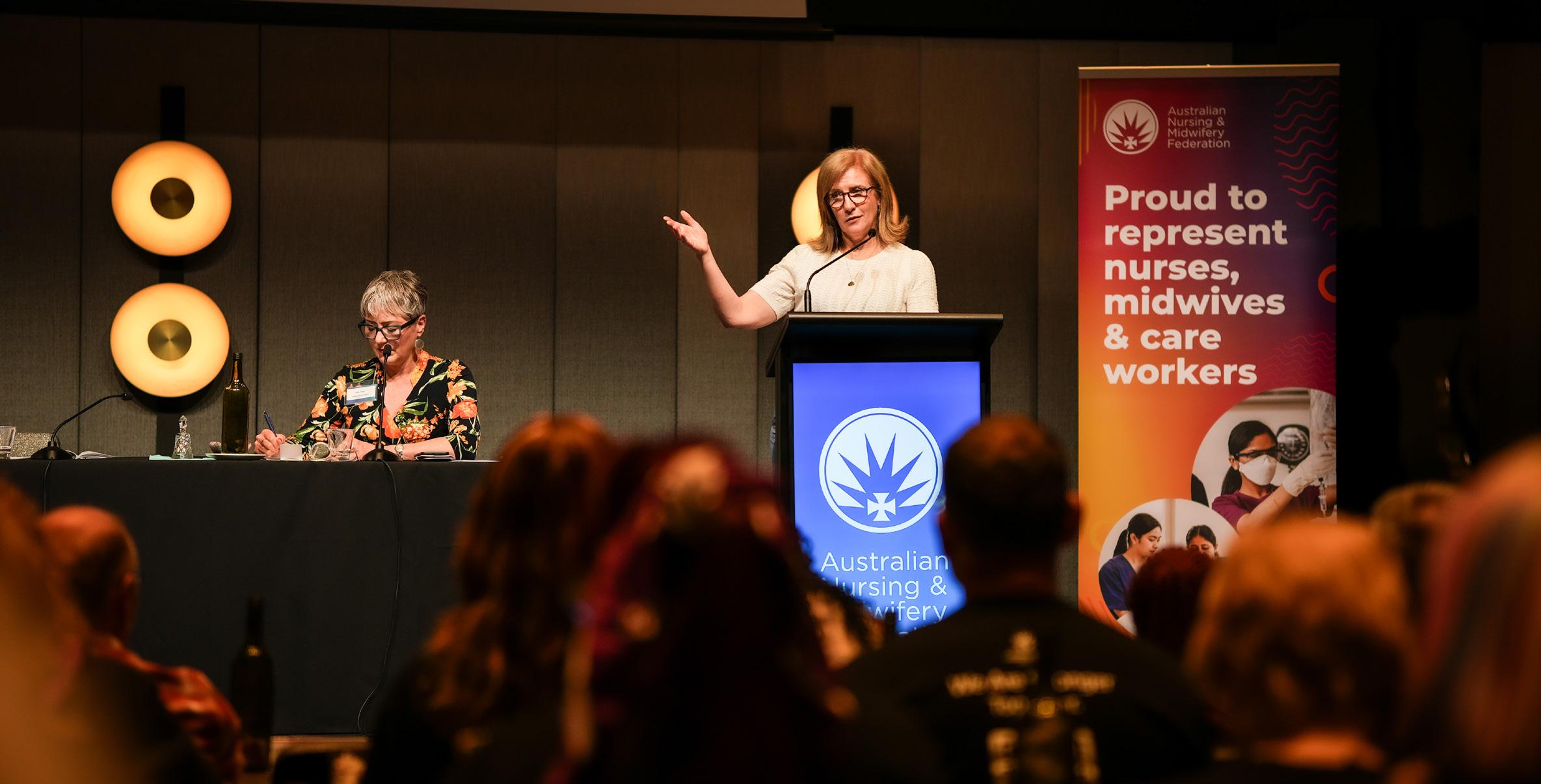
ANMF Federal President
Sally-Anne Jones opened the discussion by highlighting the disconnect between traditional economic measures
of productivity and the human-centered nature of health professions.
ANMF WA State Secretary Romina Raschilla speaking at the conference
“Service roles like ours involve emotional labour, critical thinking and interpersonal care” she told delegates. “These elements are difficult to capture in metrics like throughput or time for task. When productivity is framed very narrowly, it can add pressures to do more with less,” she said.
Federal Secretary Annie Butler echoed this message, noting that while the union has achieved major wins such as 24/7 registered nurse coverage in aged care, wage rises and financial support for students, the work is far from done.
‘“If we invest in the motions you’ve put forward,” she said. “They wouldn’t only help empower nurses, midwives and care workers, they will also actually increase productivity. This is why we need to talk about productivity.”
‘Policy, debate and solidarity
Over two days, delegates debated more than 40 motions covering workforce issues, aged care, industrial rights, gender equality, sustainability and social justice. Each motion reflected the grassroots experiences of members in their workplaces and communities. Key motions included calls for the ANMF to:
Lobby for legislation protecting nurses and midwives from unacceptably high levels of occupational violence.
End placement poverty by campaigning for paid placements and financial support for students.
Mandate national minimum staffing levels across all healthcare settings to ensure safe workloads.
Ensure compliance with direct care minutes in residential aged care to prevent data manipulation by providers.
Establish a national registration scheme for all aged care workers and mandate specific Enrolled Nurse care minutes in nursing homes, including an EN 24/7 requirement.
Coordinate a National Nurses and Midwives Day of Action to demand that governments prioritise healthcare funding over discretionary spending such as fossil fuel subsidies.
Investigate with the ACTU a 32-hour/4 day working week for all nurses and midwives to improve retention, wellbeing and work-life balance.
Advocate for fairer industrial action rights, by amending the Fair Work Act 2009 so nurses and midwives in private facilities can take action outside enterprise bargaining periods.
Lobby for tax deductibility of workrelated transport costs, acknowledging the long commutes and shift patterns many nurses and midwives face.
Each of these motions will now be reviewed for endorsement by the ANMF Federal Executive.
ANMF WA at the conference, including State Secretary Romina Raschilla, executive delegates and staff.
MEMBER SPOTLIGHT
Carli Beange - Australian Midwife of the Year.
When Carli Beange first began her career as a nurse more than 20 years ago, she couldn’t have imagined that one day she would be recognised as the Australian Midwife of the Year.
Awarded by the Australian College of Midwifes, the honour celebrates Carli’s leadership, advocacy and lifelong commitment to empowering both midwives and those they care for.
As the Midwifery Manager at the Bentley Midwifery Birth Centre (WA’s first and only standalone, publicly funded, midwife-led birth centre), Carli has championed a model of care that puts women and midwives at the centre. She leads what she proudly calls a “small but excellent” team and together, they provide continuity of care from conception to six weeks postpartum, an approach she describes as “the gold standard of midwifery.”
Carli’s journey into midwifery began early. “I come from a long line of nurses and midwives,” she said. “It’s in the blood.” After completing her graduate nursing year at Fremantle Hospital, she quickly transitioned into midwifery, working across several Perth hospitals and in private practice. A brief stint in London early in her career broadened her horizons, but her heart and passion remained in supporting women and families through birth.
Over the years, Carli has seen how structural barriers can make midwifery more challenging than it needs to be. She believes hospital systems often limit midwives’ ability to work to their full scope of practice, creating stress and burnout for midwives and inequity in care for women. Her vision is for a future where midwifery-led care is recognised as an essential profession, supported by statewide guidelines that embed it as the primary model of maternity care.
She hopes to see antenatal clinics that accept self-referrals from women and policies that allow midwives to practise without unnecessary restrictions. “We need systems that trust and value the expertise of midwives,” she said. “That’s how we’ll achieve better outcomes for women, babies and families.”
Carli also believes advocacy is intertwined with midwifery itself. “As midwives, we support people through one of the most transformative experiences of their lives. As a unionist, I see it as an extension of that same advocacy, only this time for my colleagues and the profession itself,” she said.
“It means fighting for fair conditions, safe staffing and recognition of the vital role midwives play in the health system. It’s about solidarity, making sure our voices are heard so we can deliver the best care without compromising our wellbeing. When we act collectively, we can achieve real change. The progress may seem slow some days but when we are together, improvements come faster.”
It’s this mix of compassion and determination that has earned Carli the respect of colleagues across WA. Her leadership has been instrumental in building the Bentley Midwifery Birth Centre into a place where midwives feel empowered and women feel supported to make informed choices about their birth experience.
Even on difficult days, Carli finds motivation in her colleagues and the families she has supported. “I keep all the thank you cards from the women I’ve cared for. Reading their words reminds me why I do this work,” she said.
On behalf of everyone at the ANMF WA, congratulations to Carli for being recognised as the Australian Midwife of the Year!
‘
“As midwives, we support people through one of the most transformative experiences of their lives. As a unionist, I see it as an extension of that same advocacy.”
‘
We can’t have another
winter like this
The five-point plan to tackle
one
ramping
After one of the most difficult winters on record for Western Australia’s health system, the message from the workforce was clear – it cannot happen again. Nurses, midwives, doctors, allied health professionals and ambulance staff are standing together and calling for urgent action to fix the root causes of ramping.
The ANMF WA, alongside the Health Services Union, United Workers Union and the Australian Medical Association, has presented the WA Government with a five-point plan to relieve pressure on the health system before next winter.
For nurses and other healthcare workers, the statistics on ramping are not just numbers. They represent the daily reality of patients left waiting for the care they need. This winter saw record numbers of Western Australians stuck in ambulances outside emergency departments while staff inside worked through unrelenting pressure. Beds that could have been used for emergency admissions were filled by patients with nowhere else to go.
care left others with no choice but to seek help in already full emergency departments. Nurses and midwives are doing everything they can for their patients, yet the system continues to place them in impossible situations.
ANMF WA State Secretary Romina Raschilla said the strain on nurses and midwives is unsustainable.
‘“Nurses and midwives across the health system have shown incredible resilience through one of the toughest winters on record. We need to ensure we have enough staff available and every bed open,” she said.
A shortage of aged-care beds meant older patients could not be discharged safely. Gaps in mental health and community
‘
The five-point plan reflects the insights of the state’s frontline health workers who know the system best and keep it running every day. The plan focuses on prevention, resourcing and consistency, offering practical measures that can be implemented quickly with government support.
Terry Jongen, Senior Vice President of the union and President of the state branch.
The plan’s first point is to add 400 aged-care beds across the state, properly staffed and resourced. At the peak of winter, more than 300 hospital beds were occupied by patients who no longer needed acute care but had nowhere else to go. Freeing those beds would ease hospital congestion, reduce ambulance delays and help patients move safely into the right kind of care.
The second point focuses on stronger community health and better pathways of care. That includes improved access to primary care, telehealth assessments, virtual emergency departments, sexual assault and domestic violence services, extendedcare paramedics and acute mental health supports. Preventive measures such as immunisation must remain a high priority to reduce hospital admissions during winter peaks.
The third call is to staff every bed. Too many hospital beds remain closed because there are not enough staff to operate them safely.
The unions are asking the government to clearly outline how many beds exist, how many staff are needed to run them and ensure those positions are filled. Safe care depends on safe staffing, with every bed open, every shift covered and every nurse supported to do their job properly.
The plan also calls for hospitals to provide continuous, seven-day care. Services such as radiology, pharmacy, pathology and allied health need to be fully staffed across weekends to ensure timely discharges and reduce the Monday surge that currently leaves emergency departments overcrowded. A genuine seven-day system would improve continuity of care and keep patients moving safely through the system.
Finally, the plan calls for one rulebook for healthcare. Different hospitals currently use different procedures for admission, escalation and discharge, creating inconsistency and unnecessary delays. A unified system-wide approach would ensure
patients receive consistent and timely treatment no matter where they present. It would also give staff greater clarity and the confidence to focus on what matters most, caring for patients.
Along with the other health unions, we’ve made it clear we’re prepared to work constructively with the government to put these solutions in place. We’ve called for a detailed winter surge plan to be presented by March 2026, outlining how each element of the plan will be implemented and reported.
Nurses and midwives know what it takes to keep patients safe. We see the consequences of an under-resourced system every day. The five-point plan offers a practical, coordinated way forward.
Ramping is not inevitable. With proper planning, staffing and investment, it can be reduced and eventually prevented.
HSUWA Secretary Naomi McCrae, UWU WA Secretary Carolyn Smith, AMA WA Vice President Dr. Kyle Hoath and ANMF WA State Secretary Romina Raschilla
members CAREER COMPASS
Mapping your next move with workshops exclusive to
Finding direction in your career can be challenging, especially in professions as demanding and dynamic as nursing and midwifery. Whether you’re at the beginning of your journey or ready to move into a new role, having the right guidance can make all the di erence.
That’s exactly what the Career Compass workshops offer a practical, supportive space to clarify goals, build confidence and take charge of your professional future.
Exclusively available to current ANMF WA members, these half-day workshops encourage you to step back from the day-to-day pressures of work and invest time in reflecting, refocusing and planning ahead.
Led by experienced career coach Gerry Gulla, the workshops are filled with interactive discussions, practical exercises and valuable insights drawn from Gerry’s decades of experience in employment and human resources across both public and private sectors, in WA and internationally.
Her approach is supportive and empowering, she guides participants to explore key areas that influence career growth and satisfaction, including:
Understanding personal values and beliefs.
Taking ownership of career direction.
Setting meaningful professional and life goals.
Practicing self-care to sustain motivation and wellbeing.
Identifying strengths and transferable skills.
Learning effective job application and interview techniques.
Crafting strong, personalised cover letters and CVs.
Building confidence to pursue new opportunities.
Creating a practical plan to stay on track.
By combining self-reflection with practical skill-building, the workshops provide a clear framework to identify where you are now and where you want to be. It’s not just about finding a new job, it’s about gaining the clarity and confidence to shape a career that aligns with your personal values, skills and aspirations. Participants can expect to leave the session with renewed motivation, practical strategies for achieving goals and a deeper understanding of how to leverage strengths in a competitive job market.
For ANMF WA members, this is a rare opportunity to connect with peers and access expert coaching, tailored to the realities of the nursing and midwifery professions.
Gerry
Gulla, Career Compass coach
Career Compass workshop dates
Out & about
Members at the Australian College of Midwifery Conference.
ANMF WA Professional Officer Donna Brooking and ANMF WA State Secretary Romina Raschilla at the Australian College of Midwifery (ACM) Conference.
Donna Brooking, Jill Ritchie and Romina Raschilla at the Australian College of Midwifery Conference.
Romina Raschilla and a member at the ACM Conference.
Senior Vice President Terry Jongen, Councillor Amanda de Feularde and ANMF WA Executive Director Jon Phillips at the AGM.
Union members attending the AGM.
ANMF WA Lead organiser Francesca Tantino and union members Candace and Felicity at the AGM.
Organiser Hanita Bhana and nurses and midwives from the Royal Perth Bentley Group at the Nursing and Midwifery Awards 2025.
Union members and Romina at the AGM.
Nurses and midwives from the Royal Perth Bentley Group at the Nursing and Midwifery Awards 2025.
5 (less obvious) benefits of health cover
Nurses & Midwives Health has shared some of the ways they support ANMF WA members that you may not have thought of.
In an ideal world you wouldn’t hesitate to prioritise your health and wellbeing over expenses, work and other commitments. But when your vocation is all about caring for others, the reality is rarely that simple.
Cost-of-living concerns, shiftwork, and caring for loved ones may be just a few of the blockers to you taking care of you.
As insurance for nursing and midwifery union members, Nurses & Midwives Health can help. Let’s skip the standard spiel and explore how private health insurance can benefit you.
Already with us? You may gain fresh insights. And anything that helps you get the most from your cover is a plus.
Not a member? Find out how Nurses & Midwives Health cover can support you. No hard sell, just facts to inform key decisions.
Hospital treatment - on your schedule
cover doesn’t just enable you to skip public waitlists and choose a specialist doctor. You can also schedule elective treatment at the least disruptive time.
This can be a game-changer for the nursing and midwifery community, and their families.
Mental health support- on your terms
Challenging days are a given, but ongoing distress warrants attention. Again, flexibility may equal accessibility. Eligible Nurses & Midwives Health members can receive valuable support online, via telehealth (phone or video) or in person.
Extras - for thriving (or at least surviving) at work
While not technically lifesaving, services like dental and physio can sure feel like it in the moment. As you’ll know all too well if you’ve been tormented by toothache or felt the exquisite pain of your ‘back going’. When working from home isn’t an option, these may provide much-needed relief and keep you off the injury list.
Less tax - who wants to pay more?
The Medicare Levy Surcharge (extra tax for higher earners without hospital cover) is based on your income. Your living expenses don’t come into it. And key workers can find themselves on the wrong side of the threshold while still feeling the pinch. Any level of hospital cover equals no surcharge for you.
Cashback - who wants less?
Okay, this one isn’t industryspecific. If easy money isn’t your thing, feel free to look away! Otherwise, know that it takes seconds to join the canny consumers earning cashback via Nurses & Midwives Health Member Rewards. Register your payment details, shop at selected retailers and the money drops into your bank account. Money in your pocket to offset the cost of your cover.
Find out more at nmhealth.com.au
About Nurses & Midwives Health: Nurses & Midwives Health supports the health and wellbeing of nurses, midwives, care workers, assistants in nursing and their families. So, while the ANMF WA has your back on the work front, we support you with great value health cover.
Demystifying workers compensaton
Eureka Lawyers works closely with the ANMF WA and is WA’s largest trade union legal practice providing expert advice, support and representation to members on a variety of workplace issues, including workers compensation.
The Eureka team has prepared this handy guide to demystify workers compensation - a maligned and misunderstood area of law. Often, workers are reluctant to make a claim, and those who do, can become frustrated with the process once it’s initiated.
This article is designed to help you feel more confident if you ever need to lodge a claim, navigate the system, and ultimately get the compensation you’re entitled to.
What is workers compensation?
Workers compensation is a statutory system that enables workers who have become injured or ill because of work to access compensation for lost income, permanent incapacity, and medical expenses. It also prescribes processes for claims, injury management, and the worker’s return to work.
When would you need to access it?
Common causes of serious illnesses and injuries for nurses and midwives include handling or moving a patient, exposure to biological materials, and stressrelated depression and anxiety. Whatever the cause, you may be eligible for workers compensation any time you miss work or incur expenses because of a workplace
illness or injury. In some cases, permanent physical injuries can be compensated by a lump sum payment.
How do you start the process?
After reporting the injury or illness to your employer, you should contact the ANMF WA for advice and ask a doctor of your choice to complete a ‘First Certificate of Capacity’. Your doctor will record details of your injury and other information, like your diagnosis, your capacity for work, treatment, and injury management.
You then give the ‘First Certificate of Capacity’ to your employer, along with a workers compensation claim form. The employer must complete their part of the form and give it to their insurer, who will make a decision about whether to accept or decline your claim, or defer to gather more information.
When is legal support needed? Whether your claim is accepted, denied or deferred, contact the ANMF WA for guidance. They will advise if legal support is needed.
A lawyer can help you to:
• understand the insurer’s decision and explore your options;
• obtain medical evidence to support your claim;
• achieve an outcome by settlement, conciliation, or arbitration; and
• ensure you are treated fairly by the insurer and your employer.
Important things to remember
It’s best to report your injury as soon as you can. Putting it off may create difficulties further down the line.
You should look after your own interests and health needs throughout the claim process. Don’t expect your employer or the insurer to progress your claim for you, or manage your medical treatment.
You are entitled to maintain confidentiality over parts of your medical history that are irrelevant to your claim.
You are entitled to choose your own medical practitioners, medical treatment, and rehabilitation providers.
Make sure you seek out support and care from personal networks and qualified professionals.
For a referral to Eureka Lawyers, call the ANMF WA Helpline on 6218 9459 or email anfindustrial@anmfwa.org.au
Principles of safe vaccine storagecold chain management: a clinical update
Vaccines are delicate biological substances and must be continuously stored in a limited temperature range. Vaccines can be destroyed or become less effective if they get too warm or too cold, or if are exposed to direct sunlight or ultraviolet light.¹
Vaccines have varying degrees of temperature sensitivity. The safe temperature range for most vaccines is +2°C to +8°C, and the optimal storage temperature is +5°C.¹ While most vaccines are destroyed by freezing, some vaccines, such as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines based on messenger RNA, must be stored frozen.1,2
Exposure to temperatures outside the safe temperature range diminishes vaccine potency which cannot be reversed. Repeated exposure to unsafe temperatures has a cumulative effect on vaccine viability.¹
Healthcare professionals have a professional obligation to ensure patients receive effective vaccines that have been stored appropriately.³
COLD CHAIN
and handling of vaccines.1,3 The cold chain starts when the vaccine is manufactured, continues through its transportation and storage, and ends when the vaccine is administered.¹
A vaccine management protocol is essential to effective vaccine cold chain management. The protocol should include:1,3
• Written policies and procedures for vaccine management.
• Appropriate equipment for vaccine storage and temperature monitoring.
• A designated trained person responsible for vaccine storage and protocol implementation.
• A trained back-up person to relieve the designated person when required.
• Training of all staff to effectively manage the cold chain.
A vaccine storage self-audit must be performed by vaccine service providers at least every 12 months.¹
COLD CHAIN BREACH
If a cold chain breach occurs the effected vaccines should be immediately isolated from other vaccines and labelled ‘do not use’. They may need to be moved to an alternative vaccine refrigerator or cooler.
The effected vaccines should be kept within the safe temperature range for the vaccine.¹
If the vaccines are governmentfunded, the breach should be reported to the Western Australia Department of Health as soon as possible. For vaccines with a safe temperature range of +2°C to +8°C, a cold chain breach does not need to be reported if the vaccine is exposed to a maximum temperature of +12°C for 15 minutes or less.1,4
Information required when reporting a cold chain breach includes:1,4
• Vaccine type and dose quantities.
• Date, time, and duration of the breach and the temperate range of the breach.
• Reason for breach (if known) and whether it has been rectified.
• Whether the involved vaccines have previously been exposed to temperatures outside the safe range. Read this article and complete the quiz to earn 1 iFolio CPD hour
The ‘cold chain’ is the system of maintaining a safe temperature range for the transport, storage,
A ‘cold chain breach’ occurs when vaccines are stored at temperatures outside the recommended range (+2 to +8°C for most vaccines).¹
• Whether involved vaccines have been administered to any patients.
• Data logger information for the breach period.
• Information about the relevant vaccine refrigerator including service dates and any maintenance issues.
• Visible damage to vaccines.
The vaccines must not be discarded until advised to do so by the Western Australia Department of Health.1,4
If the vaccines are privately purchased, the manufacturer should be contacted for advice.¹
After a cold chain breach, steps must be taken to correct the problem (if known) and prevent any recurrence.¹
EQUIPMENT
Vaccine refrigerators
• Vaccines with a safe temperature range of +2°C to +8°C should be stored in purpose-built vaccine refrigerators.¹ Purpose-built vaccine refrigerators have a range of features that make them the only suitable storage option, including:¹
• A uniform, stable, and controlled temperature of +2°C to +8°C.
• Effective temperature recovery after the door is opened.
• Inbuilt digital temperature monitoring and/or digital temperature indicators.
• Standard alarm and safety features that alert to or prevent irregular temperature fluctuations.
The following principles should be followed for vaccine refrigerators:1,3
• Refrigerator should be placed in a secure room where only appropriate staff have access.
• Refrigerators should be serviced every 12 months and following any malfunction.
• Refrigerators should be plugged into an uninterruptible power supply (an emergency generator should be used where an uninterruptible power supply is not available).
• The electricity connection must be clearly labelled ‘do no turn off power or disconnect’.
• Refrigerator should be equipped with a basic data logger and thermometer to maintain continuous temperature monitoring.
Coolers
A cooler is a solid-walled, or a vaccine-specific soft-walled, insulated container used for portable vaccine storage or transport. Coolers have a limited cold life and are only adequate for short-term vaccine storage of up to 8 hours.¹
The temperature inside a cooler is usually maintained by using ice packs or gel packs. The number of packs required depends on a range of factors, such as the cooler size and type, the number of vaccines, and the ambient temperature.¹
One of the greatest risks for cold chain breaches is vaccines freezing in a cooler during transport. To avoid freezing, care should be taken to correctly pack the cooler. The cooler temperature should be monitored every 15 minutes for the first two hours, when freezing usually occurs, and then at least hourly.¹
Vaccine temperature monitoring
To ensure vaccines are stored within the safe temperature range, the temperatures that vaccines are exposed to must be monitored, recorded, and reported throughout the cold chain. Temperature monitoring procedures help to ensure vaccine quality is maintained and any temperature deviations that may impact on vaccine potency are identified early.¹
Minimum and maximum temperatures must be monitored and manually recorded twice daily, and as soon as possible after any power outage.1,3
A variety of vaccine temperaturemonitoring devices are available including data loggers, thermometers, disposable cold chain monitors, automated temperature-monitoring systems, and back-to-base systems.¹
Data loggers
A data logger is a small electronic device that measures temperatures at preset intervals and records the results. All vaccine refrigerators should have a data logger (portable or built-in) set to continuously measure
the temperature at 5-minute intervals.¹ The data logger should be co-located with the minimum/ maximum thermometer in the refrigerator.1,3
Data logging reports should be downloaded and reviewed at least weekly, and as soon as possible after an alarm is activatted.¹
The data logger should be regularly checked for accuracy.¹
Thermometers
A minimum/maximum thermometer with a sensor probe should be placed in an empty vaccine box to monitor the temperature of the refrigerator under the same conditions as the vaccines.1,3
Minimum and maximum temperatures must be monitored and manually recorded twice daily. The thermometer should be reset each time a temperature is recorded.1
The thermometer should be regularly checked for accuracy. A check is recommended at least every 12 months and if there are cold chain breaches. The thermometer battery should be changed every 6-12 months.¹
Disposable cold chain monitors
Disposable cold chain monitors are used to detect cold chain breaches during vaccine transport. The disposable cold chain monitor should be checked, and the temperature recorded, when the vaccines arrive at their destination.1,3
Disposable cold chain monitors must be discarded following receipt of vaccine deliveries and must not be stored with the vaccines or used to monitor vaccine temperature after delivery.1,3
Automated temperaturemonitoring systems
An automated temperaturemonitoring system uses wireless monitoring to transmit continuous data to a web server, providing real-time access to temperature-monitoring data from a connected device, such as a mobile phone. In the event of a temperature deviation outside the safe temperature range, an alert is sent to the designated user.¹
Back-to-base alarm system
A back-to-base alarm system is a computer-based control system that alerts the nominated person when a temperature deviation occurs outside the safe temperature range. Back-to-base alarm systems support the timely identification of any breach in the cold chain.¹
POWER FAILURES
Healthcare services should have a back-up plan and alternative vaccine storage available to allow vaccines to be stored at a safe temperature if a power failure occurs.1,3
This may include a back-up power supply, such as a generator or battery, an off-site vaccine refrigerator, or appropriate coolers.
The back-up plan should be clearly documented and trialled to ensure its effectiveness.¹
Battery-operated minimum/ maximum thermometers or data loggers should be available to monitor vaccine temperature during a power failure.¹
REFERENCES
1. Australian Government Department of Health. National vaccine storage guidelines: Strive for 5 [Internet]. Canberra (Australia): Australian Government Department of Health; 2019 [cited 2023 Sep 10]. Available from: https://www.health.gov.au/sites/default/ files/documents/2020/04/nationalvaccine-storage-guidelines-strive-for-5. pdf
3. NSW Health. Policy Directive: Vaccine Storage and Cold Chain Management [Internet]. Sydney (Australia): NSW Government; 2020 [cited 2023 Sep 10]. Available from: https://www1.health. nsw.gov.au/pds/ActivePDSDocuments/ PD2020_028.pdf
4. Government of Western Australia Department of Health. Articles [Internet]. Cold chain management; 2023 [cited 2023 Sep 10]. Available from: https://www. health.wa.gov.au/articles/a_e/cold-chainmanagement#:~:text=Cold%20chain%20 management%20protocols%20are,freeze
Hypermesis gravidarum: a clinical update
Read this article and complete the quiz to earn 1 iFolio CPD hour
Nausea and vomiting are common during pregnancy, with pregnancy related nausea and vomiting affecting up to 90% of pregnant women.1,2 Nausea and vomiting typically occur during the first trimester, between four and seven weeks, peaking in severity around nine weeks, and resolving by 20 weeks gestation.3 Approximately 10% of women will experience nausea and vomiting during pregnancy.4
Hyperemesis gravidarum is a severe and persistent form of pregnancy related nausea and vomiting characterised by maternal weight loss, dehydration, and electrolyte imbalance.3,4 It is the most common cause of hospitalisation of pregnant women in the first trimester.5,6
In addition to physical effects, hyperemesis gravidarum also has significant psychological, social, and economic implications for pregnant women.5
The onset of hyperemesis gravidarum typically occurs in the first trimester before 10 weeks and peaks in severity around 12 weeks gestation.3 For most pregnant women hyperemesis gravidarum resolves by 20 weeks gestation, however some women may experience hyperemesis gravidarum for the entire pregnancy.3,4
Hyperemesis gravidarum is relatively rare, affecting 0.3-2% of pregnant women.⁴
1. In the last 24
for how long have you felt nauseated or sick to your stomach?
2. In the last 24 hours, have you vomited or thrown up?
3. In the last 24 hours, how many times have you had retching or dry heaves without throwing up?
Causes and risk factors
The aetiology of hyperemesis gravidarum remains unknown and is thought to be complex and multifactorial.2,6
Factors that may increase the risk of developing hyperemesis gravidarum include:2,4,7
• Young maternal age.
• Multiple pregnancy.
• Hyperemesis gravidarum in a previous pregnancy.
• Gestational trophoblastic disease.
• History of migraines.
• History of motion sickness.
• Family history of hyperemesis gravidarum.
SIGNS AND SYMPTOMS
Signs and symptoms of hyperemesis gravidarum include:7,8
• Severe nausea and vomiting.
• Difficulty eating and drinking.
• Weight loss.
• Excessive saliva production.
• Dehydration.
• Decreased urine output.
• Headache.
• Fatigue.
• Dizziness.
SCREENING
AND ASSESSMENT
All pregnant women should be asked about nausea and vomiting at each antenatal visit between four and 16 weeks gestation as a routine part of antenatal care.5,6
Nausea and vomiting assessment
If the pregnant woman is experiencing nausea or vomiting, the severity should be assessed using the Pregnancy-Unique Quantification of Emesis (PUQE24) scoring system.5,6 The PUQE24 system assesses the severity of nausea and vomiting over a 24hour period with three questions about the duration of nausea, and frequency of vomiting and dry retching (see Table 1).3,5
The severity of nausea and vomiting is classified based on the PUQE-24 score:3,5
hours,
Table 1: PUQE-24 scoring system6
• Mild – a score of 4-6.
• Moderate – a score of 7-12.
• Severe – a score of 13 or more. A comprehensive physical examination, including measuring the patient’s weight and hydration status, is also required to identify the severity of nausea and vomiting.3,5
Psychosocial screening
Due to the potentially significant psychological and social implications of hyperemesis gravidarum, psychosocial screening with the Edinburgh Postnatal Depression Scale is recommended for pregnant women with hyperemesis gravidarum or suspected hyperemesis gravidarum.⁵
Psychosocial screening should be repeated as necessary.⁵
DIAGNOSIS
There is no universally accepted definition of hyperemesis gravidarum.2,6 The most common criteria for diagnosing hyperemesis gravidarum are:2,6
• Severe nausea and/or vomiting.
• Weight loss of at least 5% of the pregnant woman’s prepregnancy weight.
• Dehydration.
• Electrolyte abnormalities.
Clinical assessment of patients with suspected hyperemesis gravidarum should be undertaken by healthcare professionals with experience recognising the signs and symptoms of hyperemesis gravidarum.⁶
Hyperemesis gravidarum is a diagnosis of exclusion; a diagnosis is only made after the exclusion of other pathology. As there are a large number of differential
diagnoses, a full examination is necessary including:3,4
• Obtaining a detailed patient history including any maternal conditions related to nausea and vomiting, past history of hyperemesis gravidarum or nausea and vomiting during pregnancy, and history to exclude other causes of nausea and vomiting.
• Performing a clinical assessment for signs of dehydration, such as weight and signs of muscle wasting.
• Excluding molar pregnancy.
• Calculating the PUQE-24 score.
Pregnant women with suspected hyperemesis gravidarum should have the following investigations to determine the degree of physiological disturbance and exclude significant pathology:3,4,6
• Urinalysis.
• Full blood counts.
• Blood glucose.
• Electrolytes (sodium, potassium, chloride, bicarbonate), urea, and creatinine.
• Serum magnesium, phosphate, and calcium.
• Liver function tests - bilirubin, alanine transaminase, aspartate aminotransferase, and albumin.
• Thyroid function tests.
• Obstetric ultrasound.
Any additional tests to exclude other causes of nausea and vomiting should be performed as indicated by the patient history and physical examination.3,6
TREATMENT
It is important for healthcare professionals to acknowledge both the physical symptoms of hyperemesis gravidarum and the psychological distress.⁵
Principles for the holistic management of hyperemesis gravidarum include:5,6
• Reducing nausea, retching, and vomiting.
• Managing associated gastric dysmotility, gastroesophageal reflux, and constipation.
• Maintaining hydration and fluid, and electrolyte replacement.
• Maintaining adequate nutrition, including through vitamin supplements where required.
• Psychosocial support.
• Monitoring and preventing side effects and adverse pregnancy and fetal outcomes.
Pregnant women with hyperemesis gravidarum should be referred to a consultant obstetrician or general practitioner with experience managing severe nausea and vomiting or hyperemesis gravidarum.5,6
Non-pharmacological interventions
Non-pharmacological interventions for hyperemesis gravidarum include dietary and lifestyle changes, such as:1,4-6
• Herbal remedies, such as ginger, chamomile, and peppermint.
• Eating small frequent meals of well-tolerated food.
• Avoiding fatty and spicy foods.
• Drinking small amounts often.
• Wearing acupressure bands.
• Minimising tiredness and gaining more rest, such as by modifying working patterns, going to be earlier, and daytime sleeps. The success of nonpharmacological interventions depend on the patient’s symptoms and the severity of the condition.⁵
Pharmacological treatments
Pharmacological treatment may require a combination of agents including:5,6
• Antiemetics to alleviate nausea and vomiting, and corticosteroids for severe cases.
• Gastric acid suppression to treat symptoms of gastroesophageal reflux.
• Laxatives and stool softeners to improve constipation.
• Vitamin and mineral supplements.
• The selection and timing of pharmacological treatments should be made on a caseby-case basis, taking into account the patient’s symptoms and medical history.5
Intravenous hydration
Intravenous fluids and electrolyte replacement are effective in treating dehydration and electrolyte abnormalities.3,6
Enteral and total parenteral nutrition
In severe cases, where other treatments have failed, nutritional support through enteral or parenteral nutrition may be required to adequately restore hydration, correct electrolyte abnormalities, and maintain nutrition.6
COMPLICATIONS
Maternal complications of severe hyperemesis gravidarum include:2,5,6
• Electrolyte disturbances, such as hyponatraemia and hypokalaemia
• Venous thromboembolism
• Oesophageal rupture or ulcerative oesophagitis
• Mallory-Weiss tear
• Abnormal thyroid and liver function
• Dental enamel erosion.
Pregnant women with hyperemesis gravidarum may also experience adverse mental health effects, such as anxiety and depression.2,5
Placental dysfunction associated with hyperemesis gravidarum may also cause fetal complications, such as preterm birth, placental abruption, intrauterine growth restriction, low birth weight, neonates that are small for gestational age, and a low Apgar (appearance, pulse, grimace, activity and respiration) score.2-6
REFERENCES
1. Safer Care Victoria. Maternity ehandbook [Internet]. Hyperemesis gravidarum (HG) – assessment and management; c2023 [cited 2023 Oct 2]. Available from: https://www. safercare.vic.gov.au/clinical-guidance/ maternity/hyperemesis-gravidarum-hgassessment-and-management
2. Jennings LK, Mahdy H. Hypermesis Gravidarum. 2023 [cited 2023 Oct 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing LLC. Available from: https://www.ncbi.nlm.nih.gov/books/ NBK532917
3. Government of South Australia. Clinical Guidelines [Internet]. South Australian Perinatal Practic eGuideline: Nausea and Vomiting in Pregnancy and Hyperemesis gravidarum; 2020 [cited 2023 Oct 2]. Available from: https://www. sahealth.sa.gov.au/wps/wcm/connect/ a814a7004ee49c07836f8fd150ce4f37/6. Lowe SA, Bowyer L, Beech A, Robinson H, Armstrong G, Marnoch C, Grzeskowiak L. Guideline for the Management of Nausea and Vomiting in Pregnancy and Hyperemesis Gravidarum [Internet]. Sydney (Australia): Society of Obstetric Medicine of Australian and New Zealand; 2019 [cited 2023 Oct 2]. Available from: https://www.somanz. org/content/uploads/2020/07/NVPGUIDELINE-1.2.20-1.pdf
7. Australian Government Department of Health and Aged Care. pregnancybirth&baby [Internet]. Severe vomiting during pregnancy (hyperemesis gravidarum); 2022 [cited 2023 Oct 2]. Available from: https:// www.pregnancybirthbaby.org.au/ severe-vomiting-during-pregnancyhyperemesis-gravidarum
8. Cleaveland Clinic. Health Library [Internet]. Hyperemesis gravidarum; 2023 [cited 2023 Oct 2]. Available from: https://my.clevelandclinic.org/health/ diseases/12232-hyperemesis-gravidarum
Shigella: a microorganism
Read this article and complete the quiz to earn 0.5 iFolio CPD hour
Shigella are a genus of rodshaped, nonmotile, gram-negative, facultatively anaerobic bacteria.1,2 There are four species of Shigella: Shigella flexneri, Shigella boydii, Shigella dysenteriae, and Shigella sonnei.2,3
Shigellosis is an acute infection of the intestine caused by Shigella.2,5,7
Shigella are the major cause of bacillary dysentery worldwide.3 Globally, it is estimated that Shigella cause 80-165 million cases of diarrhoea and 600,000 deaths each year.4
Shigella flexneri is the most prevalent species of Shigella and accounts for most cases of endemic shigellosis in low and middle income countries. Shigella dysenteriae, while less prevalent, causes the most severe form infection and is responsible for epidemic disease outbreaks.⁴
The prevalence of shigellosis in Australia is increasing and prolonged outbreaks have been reported in remote First Nations communities and among men who have sex with men in major cities.⁵
TRANSMISSION AND INFECTION
Shigella bacteria are primarily transmitted by the faecal-oral route.⁵ The bacteria may also be transmitted through the ingestion of contaminated food or water, person-to-person contact, contact with a contaminated surface,
recreational contact with contaminated waters, and during oral or anal sex.5,8
Shigella are highly infectious and require a low infectious dose of only 10-100 organisms.3,5
After ingestion, Shigella bacteria establish an infection by invading the intestinal epithelium and spreading from cell to cell, causing the death and sloughing of contiguously invaded epithelial cells and inducing a severe inflammatory response.3,4
Shigella are adept at surviving and replicating in the gastrointestinal tract and incorporating exogenous genetic material from other Gram-negative bacteria. Shigella gain antimicrobial resistance by interacting with and acquiring the antimicrobial resistance genes of other bacteria. As a result, the prevalence of antimicrobial resistant Shigella is increasing.2
SIGNS AND SYMPTOMS
The incubation period of Shigella is usually one to three days.6
Common signs and symptoms of shigellosis include:7,8
• Diarrhoea, which may contain mucous or blood.
• Fever.
• Nausea and vomiting.
• Abdominal cramps.
Signs and symptoms of shigellosis usually last for four to seven days, however bacteria can be shed in
the faeces for up to four weeks.6 The prolonged shedding of bacteria after a person is asymptomatic poses a high risk for ongoing transmission.⁵
While patients usually recover from shigellosis, severe complications, such as dehydration, electrolyte imbalance, fever, seizures, and haemolytic uraemic syndrome, may develop in some cases. Complications are more common and severe in young children, elderly people, people who are malnourished, and people who are immunocompromised.2,5,7
DIAGNOSIS
Shigellosis is diagnosed using a combination of preliminary clinical assessment and supportive laboratory tests.7 Faecal culture to detect and identify Shigella is the goldstandard for diagnosing shigellosis. Culture allows for the identification of the species of Shigella and antibiotic sensitivities.5 Shigellosis may be diagnosed from a stool specimen or rectal swab.⁹
TREATMENT
Most cases of shigellosis are self-limiting, and people recover from the infection within seven days without medication.5,8 In these cases, treatment generally focuses on preventing and treating dehydration caused by diarrhoea.7,8
Patients with a severe Shigella infection or who are immunocompromised may require treatment with antibiotics. Antibiotics can alleviate and
shorten the duration of symptoms associated with shigellosis.⁵
Treatment with antibiotics can also prevent prolonged bacterial shedding and reduce the risk of transmission.5,8 Antibiotics are recommended to reduce transmission in key risk groups, such as children under the age of six, healthcare workers, and people living or working in residential aged-care facilities and prisons.⁵
In Australia, shigellosis is a nationally notifiable disease; both confirmed and probable cases are notifiable. Notification allows the geographic spread of infections to be monitored and informs disease.6,9
PREVENTION
The most important preventive measure is good hygiene. Washing hands thoroughly, especially after going to the toilet or changing nappies, and before preparing or handling food will significantly reduce the risk of transmission.7,8
Other preventive measures include thoroughly cooking foods and thoroughly washing or peeling raw fruits and vegetables before eating.⁷
To prevent further transmission, people with shigellosis should not:6,7,8
• Prepare food for others.
• Share linen or towels with others while they have any symptoms.
• Have sex for at least seven days after diarrhoea has completely stopped.
• Use swimming pools for at least two weeks after diarrhoea has completely stopped.
• Go to childcare, pre-school, school, or work until they are asymptomatic for at least 24 hours (at least 48 hours if they work in a high-risk occupation, such as a handling food or caring for children, older people, or people who are immunocompromised).
For shigellosis caused by Shigella dysenteriae, people who work handling food or in healthcare, aged-care, or childcare, and children who attend childcare require two consecutive negative faecal specimens collected at least 24 hours apart before returning to work or childcare.⁶
REFERENCES
1. Aslam A, Okafor CN. Shigella. 2022 [cited 2023 Sep 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing LLC. Available from: https://www.ncbi. nlm.nih.gov/books/NBK482337
2. Baker S, Scott TA. Antimicrobialresistant Shigella: where do we go next? Nat Rev Microbiol [Internet]. 2023 [cited 2023 Sep 19];21:409-410. doi: 10.1038/ s41579-023-00906-1
3. Mattock E, Blocker AJ. How Do the Virulence Factors of Shigella Work Together to Cause Disease? Front Cell Infect Microbiol [Internet]. 2017 [cited 2023 Sep 19];7. doi: 10.3389/ fcimb.2017.00064.
4. Meza-Segura M, Birtley JR, MaldonadoContreras A, Mueller C, Simin KJ, Stern LJ, et al. SepA Enhances Shigella Invasion of Epithelial Cells by Degrading Alpha-1 Antitrypsin and Producing a Neutrophil Chemoattractant. mBio [Internet]. 2021 [cited 2023 Sep 19];12(6). doi: 10.1128/ mbio.02833-21
5. Ibrahim AF, Glass K, Williamson DA, Polkinghorne BG, Ingle DJ, Wright R, et al. The changing epidemiology of shigellosis in Australia, 2001–2019. PLoS Negl Trop Dis [Internet]. 2023 [cited 2023 Sep 19];17(3). doi: 10.1371/journal.pntd.0010450
6. Government of Western Australia Department of Health. Notification of infectious diseases and related conditions [Internet]. Shigellosis; c2023 [cited 2023 Sep 19]. Available from: https://www. health.wa.gov.au/Articles/S_T/Shigellosis
7. State Government of Victoria. Better health channel [Internet]. Gastroenteritis - shigellosis; 2022 [cited 2023 Sep 19]. Available from: https://www.betterhealth.vic.gov.au/ health/conditionsandtreatments/ gastroenteritis-shigella
9. Australian Government Department of Health and Aged Care. Diseases [Internet]. Shigellosis; 2022 [cited 2023 Sep 19]. Available from: https://www.health.gov. au/diseases/shigellosis
Zoster vaccine: a medication update
Read this article and complete the quiz to earn 0.5 iFolio CPD hour
Brand name: Shingrix¹
Drug class: vaccine1
The zoster vaccine Zostavax has been discontinued in Australia.¹ Shingrix has replaced Zostavax on the National Immunisation Program on 1 November 2023.²
Herpes zoster, also known as shingles, is caused by the reactivation of the varicellazoster virus (chickenpox).³ It presents as a painful, self-limiting vesicular skin rash and can lead to complications, such as postherpetic neuralgia.³
MECHANISM OF ACTION
Shingrix is a subunit vaccine.³ It contains recombinant varicella-zoster virus glycoprotein E with AS01B adjuvant to strengthen and lengthen the immune response.3,4 As a subunit vaccine, Shingrix, stimulates a different immune response to that induced by a natural infection, and multiple doses of the vaccine are required to stimulate and maintain a protective response.4,5 Shingrix provides protection against herpes zoster for immunocompetent patients for at least 10 years, and for up to two years for severely immunosuppressed patients.¹
ADMINISTRATION
Shingrix is administered by intramuscular injection.1,3,5 The preferred injection site is the deltoid muscle.5 A slow steady injection into the muscle minimises discomfort.1
INDICATIONS
Shingrix is indicated for the prevention of herpes zoster and postherpetic neuralgia in patients aged 50 and over, or patients aged 18 and over who are at an increased risk of herpes zoster.1,5
CONTRAINDICATIONS
Shingrix is contraindicated in patients with a hypersensitivity to any component of the vaccine, or who have had an anaphylactic reaction to a previous dose of Shingrix.3,5
INTERACTIONS
Shingrix Shingrix is not known to have any clinically meaningful drug interactions.5
Shingrix may be administered with the unadjuvanted seasonal influenza vaccine, 23-valent pneumococcal polysaccharide vaccine (PPV23) or reduced antigen diphtheriatetanusacellular pertussis vaccine (dTpa). However, the vaccines should be administered at different injection sites.⁵
Dosage
Shingrix is administered as two doses of 0.5mL each.⁵ For immunocompetent adults the initial dose is followed by a second dose after 2-6 months. For immunocompromised adults, a shorter vaccination schedule is recommended with the initial dose is followed by a second dose after 1-2 months.⁵
PRECAUTIONS
As bleeding may occur following intramuscular injections in patients with thrombocytopenia or any coagulation disorder, Shingrix should be used with caution these patients.⁵
Pregnancy and breastfeeding Shingrix is not recommended for use during pregnancy; it has not been established as safe for use.⁵ Shingrix should be used with caution while breastfeeding as its effects on the infant are unknown.1,5
ADVERSE EFFECTS
Common adverse effects associated with Shingrix include headache, fatigue, shivering, myalgia, nausea, vomiting, diarrhoea, and abdominal pain.¹ Injection site reactions, such as redness, pain, itching, swelling, burning, or a small hard lump, occur infrequently and may persist for some weeks.¹ Rarely, Shingrix is associated with hypersensitivity reactions, such a s rash, urticaria, angioedema, and anaphylaxis.1,5
REFERENCES
1. Zoster vaccine. 2024 [cited 2024 Mar 2]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https://amhonline-amh-netau/chapters/vaccines-chap/ vaccines/zoster-vaccine
2.Australian Government Department of Health and Aged Care. Immunisation [Internet]. Shingles (herpes zoster vaccine); 2023 [cited 2024 Mar 2]. Available from: https://www.health. gov.au/topics/immunisation/ vaccines/shingles-herpes-zoster-immunisation-service
3.Zoster (herpes zoster). 2023 [cited 2024 Mar 2]. In: Australian Immunisation Handbook
[Internet]. Canberra (Australia): Australian Technical Advisory Group on Immunisation. Available from: https://immunisationhandbook.health.gov.au/ vaccine-preventable-diseases/ zoster-herpes-zoster
4.Vetter V, Denizer G, Friedland LR, Krishnan J, Shapiro M. Understanding modern-day vaccines: what you need to know. Ann Med [Internet]. 2017 [cited 2024 Mar 2];50(2):110-120. Available from: https://doi.org/ 10.1080/07853890.2017.1407035
5.Therapeutic Goods Administration. Australian Product Information: Shingrix (recombinant Varicella Zoster Virus glycoprotein E antigen) [Internet]. Woden (Australia): Therapeutic Goods Administration; 2022 [cited 2024 Mar 2]. Available from: https://www. ebs.tga.gov.au/ebs/picmi/picmirepository.nsf/pdf?OpenAgent&id=CP-2018-PI-02062-1
Moved house? Changed jobs?
New email?
If your workplace has changed or you have a new personal email address, please let us know. Without up-to-date details, we may not be able to reach you about important information relating your workplace.
NEWS bites
Work begins on new women and babies hospital
The WA Government has started site works for the new women and babies hospital at the Fiona Stanley Hospital precinct, unveiling the design for the 12-storey, 274-bed facility.
The $1.8 billion project will replace the centuryold King Edward Memorial Hospital and expand services for women, newborns and families across WA. Considered one of the state’s most complex health infrastructure projects, the hospital will include inpatient facilities for gynaecology and maternity patients, a neonatology unit, operating theatres, a family birth centre and outpatient clinics.
Health news from across WA
New clinical guidelines to support abortion care in WA
The Department of Health WA has released the first Abortion Care Clinical Guidelines, supporting health professionals providing abortion services across the state.
Developed following the Abortion Legislation Reform Act 2023 (WA), which came into effect in March 2024, the guidelines replace interim advice and aim to ensure safe, consistent and equitable care.
Adapted from Queensland’s Health’s framework, the guidelines were developed in consultation with abortion care providers and include cultural consideration statements for Aboriginal people, and for those who identify as culturally and linguistically diverse.
Needle-free flu vaccine coming for WA children
From 2026, children in WA aged from two to under 12 will be eligible for FluMist, a needle-free nasal spray influenza vaccine.
Over 130,000 doses are planned for delivery across the state.
The vaccine offers the same protection as the injectable version and aims to improve uptake in children, especially those with needle anxiety, after a notably severe flu season and low child vaccination rates.
ANMF WA HELPLINE
Allegations at work
AHPRA notifications
Workers compensation
Wages & entitlement queries
Rosters and more! Our Helpline team is ready to provide you with advice over the phone and escalate your matter furhter if necessary. Call us on 08 6218 9459 Monday to Friday 9am to 5pm or email anfindustrial@anmfwa.org.au