AMERICAN ASSOCIATION of PHYSICISTS IN MEDICINE


Mammography | Image-Guided Breast Biopsy: ACR QC Manual Update and Clinical Overview
Radiotherapy | A pathway away from measurement-based patient-specific QA: A review of contemporary quality assurance for external-beam radiotherapy sub-systems
General Medical Physics | AAPM report 438: A white paper on cybersecurity management for business continuity in radiology and radiation therapy
Artificial Intelligence | AAPM task group report 273: Recommendations on best practices for AI and machine learning for computer-aided diagnosis in medical imaging
Brachytherapy | Attention 3D UNET for dose distribution prediction of high-dose-rate brachytherapy of cervical cancer: Intracavitary applicators
External Beam | Dosimetric consequences of adapting the craniocaudal isocenter distance to daily patient position in craniospinal irradiation
Brachytherapy | Practical experience in commissioning ring applicators using ring applicator component type with bravos control software v1.2
Brachytherapy | AAPM task group 317 report: A joint AAPM and ESTRO report on brachytherapy catheter, needle, and applicator tracking technology
General Medical Physics | Navigating Conflicts of Interest in Medical Physics
Diagnostic Radiology | Current progress of digital twin construction using medical imaging
AAPM Annual Meeting - 2024
AAPM Summer School - 2024
AAPM Spring Clinical Meeting - 2024
QUESTIONS OR CONCERNS?
Contact Us: Online Learning Services Subcommittee
INTERESTED IN SUBSCRIBING TO THE ONLINE CONTINUING EDUCATION PROGRAM?
Contact Jennifer Hudson or Jackie Ogburn to purchase a subscription
Inside the AAPM Summer School Subcommittee: History, Purpose, and Impact
Adaptive Rediotherapy: Transforming Technology, Modern Practice, and Clinical Impact — Why the 56th AAPM Summer School should be on Your 2026 Calenddar
Jennifer Pursley, PhD, Editor Assistant Professor
Mayo Clinic Radiation Oncology
200 First St SW Rochester, MN 55905
507-284-2511
newsletter@aapm.org
SUBMISSION INFORMATION
To keep all reports uniform, we kindly request that submissions be made through a QuestionPro portal
Questions? Contact Nancy Vazquez
PUBLISHING SCHEDULE
The AAPM Newsletter is produced bi-monthly.
Next issue: May/June 2026
Submission deadline: March 27, 2026
Posted online: week of May 4, 2026
CORPORATE AFFILIATE ADVERTISING
Advertising Rates & Deadlines
CONNECT WITH US!

EDITOR’S NOTE
I welcome all readers to send me any suggestions or comments on any of the articles or features to assist me in making the AAPM Newsletter a more effective and engaging publication and to enhance the overall readership experience. Thank you.
All articles appearing in this newsletter are expressions of the authors' own personal views and are not a reflection of the views of their places of employment or of AAPM.

Registration

Registration Opens March 9, 2026
Registration Opens March 3, 2026
Registration Opens August 5, 2026
Welcome to the March/April edition of the 2026 AAPM Newsletter. As the first day of spring approaches and the days grow longer, we are looking forward to the summer! This edition’s Special Interest Group feature is from the Summer School Subcommittee. They provide a fascinating look back at the history of the Summer School and a preview of this year’s Summer School on Adaptive Radiotherapy. Check it out and consider adding the summer school to your schedule! Registration opens on March 9.
Also in this Newsletter, you’ll find a report from President-Elect Andrew Maidment with many updates on this year’s upcoming AAPM activities. There are some timely updates on government affairs, 2026 CPT code updates, and an analysis of NIH funding trends for AAPM members. This issue also contains interesting articles on topics as diverse as medical physicist onboarding checklists available through ASTRO’s quality and safety resources, a summary of the recent EXCOM Summit, and reports from the Southern California and Upstate New York Chapters. Please enjoy these articles and many more within this edition of the Newsletter.
Whether you read the Newsletter cover-to-cover or only have time to read a few articles that catch your eye, we hope that you find the infor mation in the Newsletter to be relevant and interesting. All AAPM members are encouraged to submit feedback, content, and ideas for the Newsletter through the submission link on the Newsletter page. And as always, please share with your social media network; the Newsletter is available for all to read.
Happy spring! ¢

Jennifer Pursley, PhD Mayo Clinic


With their automated setup, rapid scanning and AI-powered data processing, BEAMSCAN® water phantoms save signifi cant time and deliver results you can trust, time and time again. Which BEAMSCAN solution best fits your needs? All-in-one or flexible? One for all or a perfect fit? On-site or mobile? No matter your clinical environment, there is a BEAMSCAN that is just right for you.
Ready to meet your new techmate?
PRESIDENT-ELECT'S REPORT
As we spring towards spring, I want to start by expressing my gratitude to our incredible volunteers, council chairs, and AAPM staff. Reflecting on the momentum from 2025 — the success of our Annual Meeting and Advocacy Day in Washington, DC — I am energized by what lies ahead in 2026. AAPM is a diverse and dynamic community of over 10,000 members spanning radiation oncology, diagnostic imaging, nuclear medicine, MR physics, and emerging specialties. Your dedication strengthens our organization and advances the field of medical physics. Our strength lies in collaboration, making this year’s theme of “Medical Physics Community” more relevant than ever.
Spring Clinical Meeting and Beyond
I look forward to seeing many of you at the Spring Clinical Meeting (SCM) which will be held March 21–24, 2026 in Orlando, Florida, at the Hyatt Regency Orlando. The SCM delivers clinic-ready knowledge through interactive sessions, case-based learning, and expert panels spanning therapy, imaging, mammography, and professional development. With more than 400 attendees expected, the SCM creates an intimate environment ideal for hands-on learning and collaborative discussion.
The program emphasizes timely topics such as regulatory updates, accreditation challenges, and strategies for quality improvement in everyday practice; areas that are increasingly important as clinical workflows evolve. There will be detailed coverage of recent AAPM task group reports including TG299 – Quality Control for Multi-Energy CT, TG330 – EPID-based Quality Assurance of Linear Accelerators, and MPPGs both current and future. Attendees will learn about The Power of Influence, The Math behind Your Staffing Requests, how to Elevate Your Career, and Patient Expectations in the AI Era.
While the SCM is already upon us, there is still time to register and attend both the Summer School and the Annual Meeting. The AAPM Summer School will take place June 16–20, 2026, at the University of Michigan in Ann Arbor, focusing on Adaptive Radiotherapy (ART). Driven by advances in imaging, AI, motion management, and data-driven planning, ART is helping to transform cancer care. The four-day immersive program provides an opportunity to deeply engage with real time treatment adaptation and the growing integration of personalized radiotherapy. Through interactive lectures, discussions and debate, attendees will gain practical skills and confidence to implement or optimize ART across diverse clinical settings. Guided by a distinguished roster of expert faculty, the Summer School is one of AAPM’s most valuable educational experiences.

Andrew D. Maidment, PhD
University of Pennsylvania
Finally, the 2026 AAPM Annual Meeting & Exhibition will take place July 19–22, 2026, at the Vancouver Convention Centre in beautiful Vancouver, British Columbia, in coordination with the Canadian Organization of Medical Physicists. As the flagship event for the medical physics community, the Annual Meeting presents the latest advances in imaging, therapy, radiological sciences, and professional development through scientific sessions, workshops, student and trainee events, and a vibrant exhibit hall. I hope to see you there.
Our Advocacy Day on July 31, 2025, was the largest advocacy event in the association’s history, an important milestone for the AAPM. Training sessions and resources developed by the government relations team strengthened our ability to advocate effectively for research funding, workforce sustainability, and patientcentered care.
Building on that success, we have plans for increased and more coordinated advocacy. In 2026, AAPM will be actively engaged at the federal level to ensure that the perspectives of medical physicists are reflected in national science and health policy. AAPM has already provided input to the National Science Foundation’s FY 2026–2030 strategic plan and is advocating for strong and predictable funding for the NIH. We continue to advocate for H.R. 3489, the Department of Veterans Affairs Medical Physicist Pay Cap Relief Act, which would formally recognize medical physicists within the VA system and address longstanding pay limitations. AAPM members and staff continue to meet with representatives on Capitol Hill to educate members of Congress on the critical role medical physicists play in delivering safe, high-quality care for veterans.
Locally, our State Champions (CHAMPS) have established a grassroots network ensuring medical physicists have a voice in state policy and regulatory discussions. There are ongoing efforts by CHAMPS in Illinois, California, Washington and elsewhere to ensure that radiation in the healing arts is used safely and efficaciously. In Washington state, for example, state CHAMPS engaged with the Washington Department of Health (DOH) on proposed requirements related to aftermarket shielding devices and fluoroscopy equipment modifications, emphasizing
evidence-based approaches that protect both patient and staff safety. Please consider joining CHAMPS to strengthen our collective voice as medical physicists.
There are a number of advocacy events that you can participate in to help advocate for medical physics. At AAPM’s Spring Clinical Meeting happening in Orlando on Tuesday, March 24, AAPM Advocacy will be holding a panel, “Turning Challenges into Action: Medical Physics Advocacy in a Changing Policy Environment.” The session will provide updates on current federal and state policy developments affecting medical physics, share lessons learned from AAPM’s 2025 Advocacy Day, and highlight ongoing state-level engagement efforts. The discussion will focus on practical strategies for member involvement and include time for questions and dialogue. In addition, ASTRO is holding its annual Advocacy Day in Washington DC. AAPM members who are also ASTRO members are encouraged to participate.
This progress reflects the dedication of many volunteers and staff. A special thank you to AAPM’s Government Relations Committee (GRAC) led by its chair Sébastien Gros for their leadership and strategic guidance, as well as to AAPM staff, including Lauren DePutter, Emily Townley, and others.
The recently published AAPM Task Group 234 (TG 234) report, Virtual tools for the evaluation of new 3D/4D breast imaging systems, represents an important contribution to the maturation of simulation-based methods in medical imaging. The report provides a comprehensive review of virtual clinical trials (VCTs) as a framework for the preclinical evaluation of emerging breast imaging technologies, covering topics ranging from anatomically realistic digital phantoms and imaging-chain simulation to the use of model observers for task-based assessment. By articulating best practices and consensus recommendations, TG 234 laid essential groundwork for improving reproducibility, reducing dependence on largescale clinical trials, and accelerating the safe translation of new imaging systems into clinical use, while also acknowledging the perspectives of industry and regulatory stakeholders who increasingly rely on computational evidence.
The relevance of TG 234 was underscored by the recently concluded AAPM Summit, Empowering Medicine Through Physics, which brought together leaders from across medical physics, medicine, industry, and regulatory science to examine how the field should position itself for the coming decades. The purpose of the Summit was to identify areas where physics-enabled innovation can have the greatest impact on medicine over the next 10-30 years and to catalyze concrete action. Among the themes that featured prominently were virtual clinical trials and digital twins, concepts that were discussed not as distant possibilities but as emerging tools for evidence generation, personalization of medicine, and regulatory science. Notably, these same ideas had already been highlighted in the earlier report of the AAPM Ad Hoc Advisory Committee on New Science, which identified computation-driven medicine, including in silico trials and digital twins, as a primary strategic area for the future of our profession.
Taken together, TG 234, the AHNS report, and the Summit discussions point toward a future in which medical physics increasingly operates in hybrid physical-digital environments. Digital twins and VCTs are poised to become integral to how technologies are designed, evaluated, regulated, and ultimately deployed in personalized patient care. This trajectory should feel familiar — medical physicists have long been at the forefront of modeling, simulation, and quantitative validation in medicine. As these tools become more central to clinical and regulatory decision-making, there is both an opportunity and a responsibility for medical physicists to deepen their engagement, build shared expertise, and help shape how digital representations of patients and systems are used responsibly and effectively. The work captured in TG 234 serves as both a marker of how far the field has come and a signal of where it is headed next.
I also want to take a moment to address an important aspect of how we communicate as an Association — surveys. Surveys are a valuable tool — whether we
are gathering clinical practice data, seeking member feedback on professional issues, or improving AAPM’s own operations. At the same time, we also hear consistently that members are mindful of the number of emails they receive, and they appreciate when communications are coordinated, purposeful, and clearly authorized. We take that feedback seriously.
AAPM has a well established framework for this: Policy AP104C, which guides how surveys related to the practice of the profession (those initiated by councils, committees, task groups, etc.) are proposed, reviewed, approved, and distributed. In parallel, AAPM staff may distribute operational surveys (e.g., those related to member services, website improvements, or meeting experiences). These help us refine how the Association functions. This process helps ensure that surveys carrying AAPM’s name are timely, relevant, and respectful of members’ inboxes.
Recently, we’ve noticed that a few surveys have been conducted informally to gather information quickly. In some cases, these surveys looked “official,” even though they did not go through the formal AP-104C process. These actions highlight an opportunity. Moving forward, we are asking all groups and all members to follow the existing survey approval process.
Thank you to everyone who has raised questions and offered thoughtful suggestions.
As we navigate an era of rapid change — AI integration, evolving reimbursement models, and global collaboration — AAPM’s mission of advancing human health through physics remains clear. I invite you to join us in shaping the future: submit an abstract, volunteer for a committee, participate in Advocacy Day, or mentor a student, resident or junior colleague.
Thank you for your commitment to AAPM and to the patients we serve. I look forward to seeing many of you at the Spring Clinical Meeting and beyond. ¢
Did you know AAPM has TWO powerful resources to support you in your volunteer and leadership roles?
Created by AAPM Headquarters, this guide provides essential information for volunteers during their service to the Association. Key features include:
HQ Staff Support: Get the help you
Governance & Policies: Links to AAPM Policies, Position Statements, By-Laws, and Rules.
Budget Process: Guidance on accessing committee-specific financial details.
Scheduling Meetings: Tools for Zoom, F2F meetings, templates, and minutes.
Committee Rosters: Tips for filling positions with the "Committee Classifieds" system.
New Group Creation: Includes the New Group Creation Form
Sunsetting policies and progress reporting tools.
Step-by-step guidance on how to get started and navigate the reporting
Volunteer Handbook today to make the most of your volunteer experience!
Brought to you by the Medical Physics Leadership Academy (MPLA), this handbook is designed to equip medical physicists stepping into leadership roles. It offers:
• Practical Tools: Set up AAPM Zoom calls, manage committee tasks, and more.
• Professional Guidance: Learn how to review applications and fulfill leadership responsibilities.
• Personal Development: Assess and refine your leadership style.
View the Leadership Handbook to take your leadership to the next level!
Medical Physics Leadership Academy
Overthe past year, I’ve shared updates in this column on AAPM’s technology transformation — the work of migrating away from legacy systems, strengthening our security posture, and building a modern digital foundation. Much of that work has been behind the scenes. Now, with our new website scheduled to launch in the second quarter of this year, it’s time to talk about what you will actually see and experience when that happens.
The short version: our new website will look, feel, and operate differently than what you are used to. That is intentional, and I want to explain why.
Our current site has accumulated more than a decade of content — thousands of pages, tools, and resources built up over time by dozens of groups across the organization. Some of that content is actively used and essential. Some of it is outdated, duplicative, or no longer relevant. Carrying all of it forward onto a new platform would undermine the very goals of this project: clarity, usability, and sustainability.
So we are making a deliberate choice. The new site will launch with a smaller, more focused set of content, organized around what members need most. Rather than migrating everything and hoping for the best, we are curating what goes forward based on usage data, member input, and strategic priorities. The result will be a site that is easier to navigate and far more useful day to day.
I know that any time you reduce content, there’s a concern that something important will be lost. We share that concern. That’s why we are maintaining a complete archive of all retired content. If something we didn’t initially carry over turns out to be critical, we will be able to access it and bring it back in a new form on the updated platform. This isn’t a one-way door — it’s a thoughtful reset with a safety net.
The new site is designed from the ground up to work well on phones, tablets, and desktops. Our current site was built in an era when most professional web traffic came from desktop computers. That’s no longer the case. Members check schedules, look up resources, and connect with colleagues from a range of devices, and the new design reflects that reality. Whether you’re at your workstation or on your phone between patients, the experience should be clean and functional.

C. David Gammel, FASAE, CAE Executive Director, AAPM HQ
EXECUTIVE DIRECTOR'S REPORT , Cont.
The design itself is cleaner and more modern, with improved navigation, stronger accessibility, and a more consistent look across AAPM’s programs and services. If you’ve visited any of our recent meeting websites, you’ve already seen the design framework in action. The broader AAPM website will build on that same foundation.
Alongside the website, we are continuing to roll out AAPM ECHO — Engage, Connect, Help, Organize — our new volunteer and member community built on the Forj platform. ECHO provides modern tools for collaboration and engagement, and early volunteer groups have been testing it since January. We are expanding access as we move through the year.
ECHO will give our committees, councils, and working groups a modern space to share documents, coordinate projects, and communicate — replacing a set of aging custom tools that had become increasingly difficult to maintain. It will also open up new ways for the broader membership to connect around shared interests, across institutions and specialties. This is a meaningful upgrade in how AAPM supports the collaborative work that drives our mission.
I want to be straightforward: when the new site launches, it will not be a cosmetic refresh of what you’re used to. It will be a different experience. Some features and content will have moved. Some workflows will have changed. The organization of the site will be different. That can be disorienting, even when the changes are improvements.
We will provide guidance and support to help members find what they need as they get oriented. And your feedback after launch will be essential. A focused initial release gives us the ability to respond to what members tell us matters most and build from there, rather than trying to anticipate every need in advance.
I’m pleased to share that Liz Kohlway, MPH, PMP, is joining AAPM in early March as our new Director of Digital Experience and Engagement. This is a role I mentioned in my last column as one we were actively recruiting for, and I’m glad to have it filled by someone with Liz’s background. She brings extensive experience building and managing large, global, online communities in the biomedical space — exactly the kind of expertise we need as our new platforms come online. Liz will play a central role in shaping how our website, content, and digital tools evolve to serve our members and support our mission. I look forward to introducing her more fully as she settles in.
The infrastructure work of the past two years — migrating data, retiring custom applications, strengthening security — was necessary to get us here. It was not always visible, and I appreciate the patience our members have shown throughout that process. What comes next should be much more tangible: a website that serves you better, tools that support your volunteer work and professional connections, and a platform we can continue to build on as the needs of the profession evolve.
I look forward to sharing the new experience with you soon, and to hearing what you think once it’s live. ¢
Whenmany people think about advocacy, they picture legislation moving through Congress or regulations being proposed for public comment. Those are essential stages of policymaking, alongside earlier phases when agencies are defining problems, gathering evidence, and considering different approaches, phases in which technical expertise can be especially valuable.
For AAPM, engagement across all stages of the policy process is a deliberate and strategic approach. Through responses to requests for information, participation in listening sessions and stakeholder discussions, and ongoing dialogue with federal and state agencies, the Association works to ensure that policies affecting research, technology adoption, and clinical practice are informed by scientific evidence and real-world experience. These activities are not about advancing political positions. They are about contributing technical insight so that policy decisions are grounded in sound science and clinical reality.
Requests for information, or RFIs, play an important role in this process. When agencies seek input, they are often testing assumptions, identifying gaps in knowledge, and exploring different policy options before committing to a specific direction. For example, in January, the National Science Foundation issued a public request for input on its FY 2026–2030 Strategic Plan, and AAPM provided formal comments emphasizing the importance of sustained investment in shared research infrastructure, interdisciplinary research pathways, workforce development, and evaluation metrics that extend beyond publication counts. AAPM also submitted detailed comments to the White House Office of Science and Technology Policy (OSTP) in response to its RFI on Accelerating the American Scientific Enterprise, highlighting the need for risk-based regulatory approaches, public–private collaboration, and equitable pathways for research translation. These early engagements help agencies think through policy design before moving to formal rulemaking or guidance.
In technical fields, absence at this stage can lead to policies that are difficult to implement, misaligned with clinical practice, or insufficiently responsive to patient and staff safety considerations. Timely, evidence-based input helps agencies frame issues accurately and consider practical implications early in the process.
Written comments frequently lead to follow-on conversations or invitations to participate in stakeholder sessions. For instance, AAPM’s prior engagement on artificial intelligence policy contributed to an invitation from the Small Business Administration Office of Advocacy to participate in a listening session convened in connection with a Department of Health and Human

Lauren DePutter Director of Government Affairs and External Relations, AAPM HQ
For questions related to Government Affairs and advocacy, please contact Lauren DePutter.

Services RFI. Over time, this type of engagement builds credibility and trust. It allows medical physicists to explain how complex technologies are evaluated, how safety is ensured, and how innovation is translated into patient care. It also reinforces the essential role of qualified medical physicists in overseeing advanced technologies and supporting high-quality clinical practice.
As policy discussions expand beyond traditional areas such as research funding into domains like artificial intelligence, data governance, and evolving radiation protection frameworks, engagement across multiple stages becomes even more important. These issues often develop through guidance, pilot programs, and rulemaking rather than through high-profile legislation. Early and sustained engagement helps ensure that emerging policies recognize technical complexity, support innovation, and remain grounded in evidence-based, risk-informed approaches.
At the same time, not all policies develop with sufficient technical input from the outset. In those cases, responsive advocacy remains essential. Whether through formal comments, direct communication with policymakers, or efforts to clarify or mitigate impacts during implementation,
AAPM works to ensure that finalized policies are interpreted and applied in ways that remain consistent with scientific evidence, clinical realities, and patient safety.
Taken together, proactive and responsive advocacy form a comprehensive strategy. Early engagement helps shape policy direction, while later-stage engagement helps ensure appropriate interpretation and implementation. Both rely on the same foundation of expertise, credibility, and sustained involvement.
For AAPM members, the effects of this work may not always be visible as discrete policy outcomes, but they are reflected in how research is supported, how technologies are evaluated and adopted, and how clinical practice evolves over time. When medical physics expertise is consistently part of policy discussions, decisions are more likely to support innovation while maintaining high standards of care.
Advocacy is most effective when it is deliberate, sustained, and grounded in expertise. By engaging across the policy lifecycle, AAPM helps ensure that medical physicists are contributing to policy decisions at every stage, from early problem definition through implementation, in ways that benefit the profession and the patients we serve. ¢


Volunteers are essential to furthering the AAPM mission of advancing medicine through excellence in the science, education, and professional practice of medical physics. Become a part of this dynamic community via the AAPM Commi ee Classifieds. Exciting new opportunities are posted regularly; bookmark or check back o en to explore the latest possibilities to get involved!
Written on behalf of the Work Group on
A more detailed analysis of NIH funding trends for AAPM members is available at https://arxiv.org/abs/2601.07187
The Research Funding Database
Advances in medical physics have been largely driven by decades of federally funded research. In the United States, the National Institutes of Health (NIH) is the primary source of federal research funding for our field. To better understand the relationship between federal investment and research activity in medical physics, the Working Group for the Development of a Research Database (WGDRD) previously established a database of NIH awards to AAPM members.
This database has been updated annually and provides a valuable foundation for analyzing NIH funding trends and the role AAPM members have played in federally supported research. In 2022, WGDRD merged with the Working Group for Funding and Grantsmanship (WGFG). The combined group continues to track NIH funding received by AAPM members, guide the selection of timely and relevant topics for the association’s annual grant symposia, and address key questions related to the AAPM workforce.
Over the past year, federal funding for scientific research experienced significant and unprecedented disruptions, including grant cancellations, delays in peer review, and new administrative requirements. Using the AAPM NIH Funding Database, we compared funding patterns between the last two fiscal years (FY24 and FY25), seeking to better understand the impact on our field.
The database is built by cross-referencing public data from NIH RePORTER with AAPM membership records. Each entry includes detailed information on award timing, type, and funding amount. Importantly, multi-year projects are typically supported in annual increments, leading to a distinction between competing and noncompeting awards. Competing awards undergo full peer review and generally reflect the initiation of new research projects, whereas noncompeting awards support the continuation of already-approved work.
Overall, total NIH funding for research projects led by AAPM members was comparable in FY24 and FY25 when both competing and noncompeting awards are included. Despite a slight slowdown during the second half of

Guillem Pratx, PhD Stanford University
University of California, San Francisco

Purdue University
FY25, funding accelerated in September, resulting in similar total funding levels across the two fiscal years ($95.9M vs $97.3M).
NIH operated under a continuing resolution in FY25, and its overall budget remained flat relative to FY24. Despite unprecedented disruptions, extramural grantmaking remained stable, reflecting NIH’s legal obligation to distribute funds appropriated by Congress.
In FY25, NCI remained the largest funder of medical physics research (61%), followed by NIBIB (24%), NHLBI (9%), and NINDS (6%), a distribution that closely mirrored the previous fiscal year.
To understand how medical physics research was impacted by last year’s changes at NIH, a closer look at the composition of awards is necessary. When tallied separately, funding for competing awards declined by 51%, whereas, for noncompeting awards, it increased by 10%. In practical terms, fewer new projects were funded, while more resources were funneled toward ongoing work.
Cumulative funding curves provide additional insight. For noncompeting awards, funding trajectories were nearly identical for most of the fiscal year (Figure 1A). However, a notable uptick occurred in the final month of FY25 due to a small number of projects receiving multiyear extensions. Although these extensions do not increase total lifetime funding, they result in larger single-year award amounts since future project years are funded upfront.
In sharp contrast, competing awards displayed a widening gap throughout FY25, culminating in a $14.7M shortfall relative to FY24 (Figure 1B). Pauses in award activity around February and again in June/July likely reflect disruptions in NIH peer-review and grant decision making. Larger competing awards (R01 and U01) were disproportionately affected, compared to smaller R21 and R03 mechanisms (Figure 1C).
Figure 1D further underscores a historic realignment in institute-level support. After years as the dominant funder of medical physics research, NCI support declined 64% in FY25, placing it on roughly equal footing with NIBIB. This
shift coincided with severe budget constraints, historically low NCI paylines (reduced to the 4th percentile), and an apparent shift toward biologically and clinically oriented priorities over technology-focused research.
Figure 1. Noncompeting and competing awards to AAPM members. (a) Cumulative funding of noncompeting awards (type 3,4 and 5). (b) Cumulative funding of competing awards (type 1 and 2). (c) Competing awards by activity code, including small research grants (R03), exploratory grants (R21), research project grants (R01), cooperative agreements (U01), program project grants (P01) and specialized centers (U54). (d) Funding of competing awards by NCI, NIBIB, NHLBI, and NINDS.
NCI has long been a major supporter of medical physics research, reflecting the central role of imaging and radiation therapy in the continuum of cancer care. In FY25, however, new R01 awards to medical physicists fell by 80% compared with the prior year (Figure 2A). Overall funding levels were maintained only because noncompeting funding increased by 10%, largely due to multiyear extensions issued late in the fiscal year. The number of new R01 awards dropped sharply, from 17 in FY24 to just 4 in FY25, an unprecedented decline confirmed by historical data from FY22 and FY23 (Figure 2B).
For context, we examined NCI’s broader portfolio of competing R01s across all disciplines (Figures 2C and 2D). While FY25 showed irregular funding patterns compared with FY24, total funding levels by year’s end were similar ($372M vs $387M).
To better understand this disparity, we analyzed a subset of 25 study sections responsible for roughly 60% of funded NCI R01s. Grouping these sections by focus revealed a clear trend: funding declined by approximately 18% in clinically or biologically oriented panels, compared with a 34% decline in technology-focused panels. As much of the research conducted by AAPM members falls within the latter category, it is likely to have been disproportionately affected by this change in direction.
Medical physics delivers substantial benefits to patients with relatively modest NIH investment. Radiation therapy, enabled by medical physicists, is used in approximately half of all cancer patients and contributes to roughly 40% of cures. Life-saving technologies such as low-dose mammography, image-guided radiation therapy, and advanced magnetic resonance imaging account for only a small fraction of NIH’s extramural portfolio, yet they have an outsized impact on patient outcomes.
FY25 marked the sharpest year-over-year decline in new competing awards since 2000. While the impact of these cuts was felt across medical physics programs nationwide, much of the damage can still be reversed. If FY25 proves to be an aberration driven by temporary upheaval at NIH, recovery remains possible. However, a sustained loss of support would severely limit the field’s ability to innovate and train the next generation of medical physicists.
Although we are still early in FY26, a quick look at RePORTER reveals that NIH has issued only ~100 awards thus far in the fiscal year, compared to over 2000 at the same time last year. The WGFG will continue to monitor NIH funding trends and will present an updated analysis of FY26 data at the AAPM annual meeting in Vancouver. ¢
Figure 2. NCI funding of competing R01s. (a) Cumulative funding curve for AAPM principal investigators (PIs). (b) Number of competing R01 awarded to AAPM members over the past four years. (c) Cumulative funding allocated by NCI to competing R01s for all investigators. (d) Total number of competing R01s awarded by NCI in the past 4 years..
2026 CPT Radiation Therapy Delivery Update: Effective January 1, 2026, radiation oncology delivery coding shifts to a technique-agnostic, three-level hierarchy (Levels 1–3) that better reflects modern clinical practice. Technical IGRT and active motion management are now bundled into delivery codes, leading to the deletion of IMRT delivery codes 77385/77386 and CT guidance code 77014, while SBRT/SRS remain unchanged. Level selection is based on setup complexity and isocenters, with Level 3 reserved for cases requiring medically necessary active motion management and increased complexity, supported by appropriate documentation. CMS has adopted these CPT changes under both HOPPS and MPFS and has deleted the temporary Medicare G-codes, fully aligning Medicare reporting with the new CPT framework.
The 2026 CPT code updates for radiation oncology represent a significant restructuring of how treatment delivery is reported and reimbursed. Effective January 1, 2026, the American Medical Association (AMA) has moved away from technique-specific descriptors in favor of a technique-agnostic model. This change is designed to streamline the coding process, reduce administrative burden, and better reflect modern clinical workflows where advanced technology is the standard of care.
The core of this transition involves the transformation of three existing codes (77402, 77407, and 77412) into a three-level hierarchy. Rather than being defined by specific megavoltage energy or the "simple, intermediate, or complex" labels used in previous years, these codes now represent "Level 1," "Level 2," and "Level 3" delivery. A critical feature of this restructuring is the "bundling" of services: the technical component of image guidance (IGRT) and active motion management are now included within these delivery codes rather than being billed as separate line items.
As part of this consolidation, several high-volume codes have been deleted for 2026. Most notably, the Intensity Modulated Radiation Therapy (IMRT) delivery codes 77385 and 77386 have been retired, as IMRT services are now captured within the new three-level framework (typically Levels 2 or 3). Additionally, 77014 (CT guidance for field placement) has been deleted, reflecting that guidance is no longer a distinct add-on but an inherent part of the daily treatment process. It is important to note that SBRT and SRS codes are not impacted by these specific delivery changes.
The levels are distinguished by setup complexity and the number of isocenters. Level 1 (77402) typically covers basic treatments. Level 2 (77407) encompasses single-isocenter 3D-CRT and IMRT treatments. Level 3 (77412) is reserved for the most complex scenarios, including treatments involving multiple isocenters

Blake M. Dirksen, MS University

or those requiring active motion management for a single isocenter. Active motion management includes intrafraction localization and tracking of targets or patient motion to optimize beam delivery. Notably, the Level 3 (77412) valuation accounts for medical physics resources, reflecting the necessity of medical physics support for these complex deliveries.
Active motion management refers to techniques used to monitor and manage target or patient motion during radiation delivery, rather than relying solely on pretreatment imaging or passive margins. This includes intra-fraction localization and tracking methods such as respiratory gating, breath-hold techniques, real-time tumor tracking, surface-guided radiation therapy (SGRT), and other technologies that actively adapt beam delivery in response to patient or organ motion. These approaches are increasingly used to improve target accuracy, reduce normal tissue exposure, and enable tighter treatment margins.
Importantly, the use of active motion management must be medically necessary and supported by clinical documentation. Selection of Level 3 delivery should be based on patient-specific factors such as tumor location, magnitude and unpredictability of motion, proximity to critical structures, or inability to adequately manage motion through simpler techniques. Routine or default use of active motion management, in the absence of a documented clinical need, may not meet payer expectations for medical necessity.
The inclusion of active motion management as a defining criterion for Level 3 delivery reflects the additional clinical, technical, and operational complexity associated with these treatments. Such workflows often require extended
treatment times, specialized equipment, enhanced quality assurance, and direct medical physics involvement for system commissioning, validation, and ongoing support. Accordingly, the valuation of Level 3 delivery accounts for the increased medical physics resources and expertise necessary to safely and effectively deliver these advanced treatments.
Although the technical component of IGRT is now bundled into the delivery codes and is no longer separately reportable, the professional component remains distinct. Providers should continue to report CPT code 77387 for the physician’s review and interpretation of image guidance.
From a reimbursement perspective, the Centers for Medicare & Medicaid Services (CMS) have adopted these revised CPT delivery codes under both the Hospital Outpatient Prospective Payment System (HOPPS) and the Medicare Physician Fee Schedule (MPFS) for 2026. In conjunction with this adoption, CMS has deleted the temporary G-codes that had previously been used to describe radiation therapy delivery under Medicare. With the retirement of these G-codes, CMS has fully aligned Medicare reporting with the new CPT-based delivery framework, eliminating parallel coding structures and further simplifying billing across care settings.
Overall, the 2026 CPT updates modernize radiation oncology coding by aligning reimbursement more closely with contemporary clinical practice, while reinforcing the importance of appropriate use and documentation of advanced technologies such as active motion management.
For further guidance, please contact the AAPM Professional Economics Committee ¢
UPDATES FROM ACR HQ
Lookback Period for Non-Mammography Modality Submission Extended to Accommodate Previous Annual Survey
I am pleased to share that for all ACR diagnostic accreditation modalities except mammography, the lookback period for phantom submission images has been extended to allow images acquired during the previous annual medical physicist’s survey, effective immediately. The following updated paragraph can now be found in the four accreditation support articles pasted below it:
• All phantom examinations submitted must have been performed within 14 months of the date on the testing package that was released to the facility. Phantom images from the most recent annual medical physicist’s survey may be used, provided they meet all other submission requirements. No images will be accepted for review that predate the testing package date by more than 14 months.
Testing Overview: MRI
Testing Overview: CT
Testing Overview: Nuclear Medicine and PET
Testing Overview: Stereotactic Breast Biopsy
Please note that no change has been made for clinical images, i.e., the lookback period for clinical images remains six months.
The ACR Medical Image Quality Assessment System (MIQAS) establishes a unified, task based framework for assessing diagnostic image quality, defining it as the degree to which an image approximates the true representation of patient anatomy in ways that matter for the intended clinical task. MIQAS introduces a reproducible 5 point scoring system (0–4), differentiating between bounded factors, where quality requires balancing risks or costs, from unbounded factors like positioning or labeling, for which excellence is always the target. MIQAS emphasizes descriptive (not prescriptive) evaluation, composite scoring with weighted quality elements, and reproducible measurement characteristics (trueness, precision, stability, comprehensiveness). As specific modality and clinical task scoring systems are developed, diagnostic medical physicists will be able to evaluate and optimize image quality more consistently and effectively across modalities. Opportunities should materialize for benchmarking performance, contributing to AI readiness, and participating in clinical quality improvement projects. You can read the paper in JACR here.

Dustin A. Gress, MS Senior Advisor for Medical Physics ACR Quality and Safety, Reston, VA
In each issue of this newsletter, I present information of particular importance or relevance for medical physicists. You may also check out the ACR’s accreditation support page for more accreditation information and QC forms. Thank You to all the other staff that keep ACR programs running and assist with creating the content in this column. This page has forms and quick links for all ACR accreditation programs.
UPDATES FROM ACR HQ , Cont.
As most of you know, ACR’s Diagnostic Centers of Excellence program, DICOE, allows facilities to demonstrate the infrastructure, policies and procedures required to assure consistently high-quality care and service. New in November of 2025, ACR now offers two additional tiers of DICOE:
• DICOE With Distinction facilities meet DICOE requirements and demonstrate elements of outstanding performance in some advanced DICOE domains.
• DICOE Pinnacle facilities meet DICOE with Distinction criteria and demonstrate excellence in many advanced DICOE domains.
You can read a Q&A with Ben Wandtke, MD, MS, Vice Chair for the ACR Quality and Safety Commission and Chair of the DICOE Committee online here. Learn more on the DICOE landing page and see the comprehensive list of criteria here.
Breast imaging practices have reported occasionally experiencing payment problems with the CMS for FFDM
and/or DBT services. The FDA does not provide MQSA certificates that specifically state that a facility is certified to perform FFDM or DBT. Instead, they send CMS a weekly file containing the most recent approval information. Your payer must look at the current MQSA file to see whether your facility is certified to perform digital mammography or tomosynthesis.
See CMS Transmittal 913 on the handling of these files and provide a copy to your local payer. You may contact the appropriate CMS headquarter representatives.
Please provide them with your facility’s 6-digit FDA ID number from your MQSA certificate and your MQSA expiration date.
If you continue to have problems after contacting the individuals below, please contact the ACR Economics Department for assistance at (800) 227-5463. Other updates on MQSA Regulations and Small Entity Compliance Guide have been posted to this Accreditation Support article. ¢
CHANGES TO NIST AIR-KERMA STANDARDS AND ADCL CALIBRATION COEFFICIENTS FOLLOWING ADOPTION OF ICRU 90 RECOMMENDATIONS
The National Institute of Standards and Technology (NIST) maintains and disseminates standards for ionizing radiation dose through the work of the Dosimetry Group. The AAPM Accredited Dosimetry Calibration Laboratories (ADCLs) provide NIST-traceable calibrations of ionization chambers and radioactive sources to customers, including clinical medical physicists.
As a National Measurement Institute (NMI), NIST follows recommendations of the Consultative Committee for Ionizing Radiation (CCRI) to maintain consistency with standards at other NMIs around the world. The International Commission on Radiation Units and Measurements published Report No. 90, “Key Data for Ionizing-Radiation Dosimetry: Measurement Standards and Applications” (ICRU 90), includes updates to various parameters used in radiation dosimetry[1]. NIST has adopted these updates, resulting in changes to air-kerma and air-kerma strength standards realized using free-air and cavity ionization chambers. There are no changes to NIST absorbed dose to water standards, as they are realized using water calorimetry.
The changes to NIST standards are as follows:
Co-60 air kerma (Kair): Kair decreased by 0.8 % effective May 1, 2023
Cs-137 air kerma (Kair): Kair decreased by 0.6 % effective May 1, 2023
Diagnostic x ray and electronic brachytherapy air kerma (Kair): Kair decreased by 0.06 % to 0.46 %, depending on beam code, effective June 1, 2022
Low Dose Rate (LDR) brachytherapy source air-kerma strength (SK): SK decreased by 0.24 % for Pd-103, 0.20 % for I-125, and 0.19 % for Cs-131 effective January 1, 2025
Calibration reports issued by NIST include an attachment explaining the ICRU 90 related changes.
The AAPM ADCLs will begin applying these changes to their calibrations effective May 1, 2026. Users should expect slight decreases in reported airkerma and air-kerma strength values due to these updates. For air-kerma calibrated ionization chambers, this corresponds to a small decrease in the reported calibration coefficients (e.g., NK), reflecting the decreased NIST standard values. ¢
Reference
1. ICRU Report No. 90 Volume 14 (2016), “Key Data for Ionizing-Radiation Dosimetry: Measurement Standards and Applications”.


National Institute of Standards and Technology

University of Wisconsin-Madison

MD Anderson Cancer Center

Jeffrey Siebers, PhD
University of Virginia Health System

Jucilene Stabin, PhD
K&S Associates, Inc.

• ASTRO has created role-specific sample orientation/onboarding checklists for radiation oncologists, nurses, therapists, and dosimetrists.
• A new physicist onboarding checklist spans infrastructure, process-ofcare responsibilities, quality and safety training, treatment techniques and equipment, disease-site–specific considerations, documentation expectations, and team integration to provide a comprehensive starting point that practices can tailor to their clinical environment.
• Download the checklists from ASTRO's website
• Patient Safety Awareness Week (March 8-14) is an opportunity to celebrate the numerous quality and safety initiatives already in place and to identify what more can be done to improve patient safety
Standardization is a cornerstone of high-quality and safe radiation oncology practice, and medical physicists play a central role in establishing and maintaining standards. To ensure that consistent practices are followed by all staff, especially new hires, a standard onboarding process is required. Whether a new hire is just out of training or a seasoned expert joining from another practice, a comprehensive orientation to an unfamiliar facility is essential. Clear expectations and consistent training support a smoother transition and faster integration into the clinical team. In an era of increasing technical complexity, evolving regulatory requirements, and workforce constraints, standardized onboarding also supports operational resilience by reducing reliance on informal knowledge transfer and minimizing variability during staff transitions. For therapy medical physicists in particular, effective onboarding is critical to maintaining continuity in technical oversight, regulatory compliance, and patient safety.
To help practices meet this need, especially during staffing challenges, ASTRO’s Multidisciplinary Quality Assurance Subcommittee developed a set of sample orientation/onboarding checklists. These tools are designed as practical resources rather than formal recommendations or prescriptive guidelines. Available in Word format on ASTRO’s website, the checklists are easy to customize to reflect each practice’s unique infrastructure, workflows, and technologies. While role-specific checklists for radiation oncologists, nurses, therapists, and dosimetrists were released previously, the Medical Physicist Onboarding Checklist is a newly developed addition to this resource set, addressing the unique technical, clinical, and safety responsibilities of physicists.
For physicists to be effective in the clinic, onboarding must address their role throughout the full process of care. A well-designed orientation clarifies

UC San Diego

Stanford University
expectations for troubleshooting at every stage, from simulation through treatment delivery. Familiarity with technique-specific support for procedures such as motion management, adaptive treatments or SRS, to name a few, is essential.
A structured and standardized onboarding process also helps new medical physicists become familiar with each practice’s unique configuration, including equipment management procedures, equipment operation, and knowledge of critical hardware and software features. Additionally, understanding who to contact for machine service, breakdowns, IT support, etc., and how responsibilities are divided among facilities, engineering, and IT teams allows physicists to respond efficiently when issues arise.
Quality assurance (QA) is a major focus of the physicist’s role and should be a key area for standardized onboarding. New physicists must be oriented to patient-specific QA processes, including pre-treatment chart checks, and any special physics consultations. Understanding clear communication pathways with the radiation oncology team is critical for timely care. Equipment QA expectations — ranging from commissioning new systems to daily, monthly, and annual checks, as well as QA equipment calibration and documentation — should be clearly outlined.
ASTRO’s sample physicist onboarding checklist spans infrastructure, process-of-care responsibilities, quality and safety training, treatment techniques and equipment, disease-site-specific considerations, documentation expectations, and team integration to provide a comprehensive starting point that practices can tailor to their clinical environment. The document offers a comprehensive framework to support standardized and resilient onboarding.
Regularly reviewing the onboarding process supports both safety and quality. Additional resources, such as the RO-ILS themed report on training and education, provide data and examples illustrating the impact of comprehensive onboarding. Likewise, APEx Accreditation Standard 5 emphasizes staff qualifications and ongoing training including onboarding processes. Standardized onboarding also reinforces expectations related to quality and safety
programs, including incident learning participation, emergency response procedures, and the application of risk analysis methods to clinical workflows. Introducing these elements early helps foster a shared culture of safety and continuous improvement.
The 2026 national Patient Safety Awareness Week (March 8–14) offers an important opportunity to highlight critical needs, showcase ongoing projects, and celebrate meaningful achievements in patient safety. This provides an ideal occasion for the radiation oncology team and practice leaders to reassess onboarding practices, incorporate ASTRO’s sample checklists, and strengthen a culture of standardization and patient safety.
The abbreviated outline below presents a high-level view of the “Process of Care” section of the Therapy Medical Physicist Onboarding Checklist, showing only the top two levels of the checklist hierarchy. This summary is intended to illustrate the scope and organization of physicist responsibilities across the clinical workflow, from commissioning and simulation through treatment delivery and ongoing quality management.
While some items are intentionally presented at a higher level, the full checklist provides additional detail and context where appropriate, allowing practices to tailor onboarding to their local workflows, technologies, and clinical responsibilities.
Equipment (hardware and software)
o Commissioning of new equipment using practicespecific workflows and processes
o Design and implementation of daily, monthly, annual equipment QA
o QA equipment calibration and documentation (user manual)
Imaging import/export
o Importing diagnostic and simulation images
o Importing outside records
o Exporting treatment plan data to external practices
Manipulation and registration procedures for available imaging modalities
Simulation
o Expectations and roles of physicists during patient simulation
o Available immobilization devices
o Support for creation and placement of treatment devices (e.g., bolus, gazing fixation, compression belt)
o Motion management
o Policies and workflow for patients with implanted electronic devices
o Technique-specific support (e.g., total body irradiation (TBI) measurements, clinical setup simulations)
o Special imaging protocols (e.g., dual-energy CT, extended Hounsfield Units CT image)
Treatment planning
o Physicist roles and support expectations for treatment planning
o Details of the treatment planning process
o Planning considerations and tradeoffs related to implanted electronic devices (e.g., AAPM TG 2031, Heart Rhythm Society Consensus guidelines2)
o Communication process when a plan is ready for review, including anticipated or unanticipated expedited or delayed planning scenarios
o Plan revision workflows (e.g., add/remove fractions, complete treatment early)
Quality assurance
o Details of the patient-specific QA
o Special medical physics consultations (e.g., stereotactic treatment, TBI, in vivo dosimetry, reirradiation, implanted electronic devices)
o Performing end-to-end testing
Treatment delivery
o Physicist roles and expectations during treatment delivery
o Management of patient in vivo dosimetry and typical situations requiring measurements
o Treatment interruption workflow
o Procedures for patient transfer between machines
o Linear accelerator and ancillary system support
o Special procedure set-ups (e.g., TBI, prone and decubitus position)
o Management of specialized equipment (e.g., respiratory gating systems, surface guided radiation therapy)
Common areas of troubleshooting at any step in the process of care (e.g., working with the dosimetrist to improve plan quality, working with therapists to improve patient set up)
Coverage plans
o How to contact the covering “physicist/dosimetrist of the day”
o Who to contact in an emergency
o Point person for specific procedures
Research and clinical innovation
o Existing research programs and infrastructure
o Available resources and contacts
o Available clinicals trials and credentialling requirements to open new trials
o Clinical trial QA and data export
Supervising responsibilities (e.g., residents, physics assistants) as applicable ¢
References
1. Miften M, Mihailidis D, Kry SF, et al. Management of radiotherapy patients with implanted cardiac pacemakers and defibrillators: A Report of the AAPM TG-203. Med Phys. 2019 Dec;46(12):e757-e788. doi: 10.1002/mp.13838. Epub 2019 Nov 1.
2. Indik JH, Gimbel JR, Abe H, et al. 2017 HRS expert consensus statement on magnetic resonance imaging and radiation exposure in patients with cardiovascular implantable electronic devices. Heart Rhythm. 2017 Jul;14(7):e97-e153. doi: 10.1016/j.hrthm.2017.04.025.








Vrinda Narayana, PhD | University of Michigan, Henry Ford Providence
Colleen J. Fox, PhD | Dartmouth Health, Dartmouth College


Vrinda Narayana, PhD Colleen J. Fox, PhD
Written on behalf of the Summer School Subcommittee
The Beginning
In the summer of 1969, just after the 2nd International Organization of Medical Physics (IOMP) Congress in Boston, a quieter but equally important event took place a few hours north in Burlington, Vermont. On a college campus, AAPM launched its first-ever Summer School.
Peter Almond envisioned the program. Bob Gorson organized the local arrangements. Janey Clint created a welcoming social program for spouses and families. Carrie Borrás quietly documented the early discussions, which focused on a rapidly evolving theme: dosimetry.
The faculty roster was impressive. Harold Rossi spoke on microdosimetry, Professor Stevenson represented the Manchester system, and André Deutrix joined from Paris. It was an international, immersive, and transformative week. It became the model for what was to follow.
The AAPM Summer School Subcommittee — At a Glance
• Established: 1969 • First Summer School: Dosimetry, Burlington, Vermont • Committee Placement: Meeting Coordination Committee (Administrative Council) • Educational Model: In person, immersive, single topic deep dive • Formats: 2.5 day and 4.5 day schools • Faculty Model: On campus, full week participation • Participants: Strong repeat attendance • Materials: Peer reviewed monogram + on demand access (registrants only) • Financial Model: Self-sustaining with a 3-year rolling average
More than 50 years later, the AAPM Summer School remains one of the organization’s most unique and enduring educational experiences.
Its success is sustained by the Summer School Subcommittee (SS), which operates under the Meetings Coordination Committee (MCC) in the Administrative Council.

Standing first from the left in the top row is Dr. Peter Almond, widely recognized as the founding force behind the AAPM Summer School. His vision for a week-long, topic-focused learning experience laid the foundation for what has become one of the most enduring and impactful educational traditions in medical physics.
While always centered on education, the school’s connection to the Education Council is more
philosophical than structural. The Summer School is not just a meeting. It's a learning environment. A deep
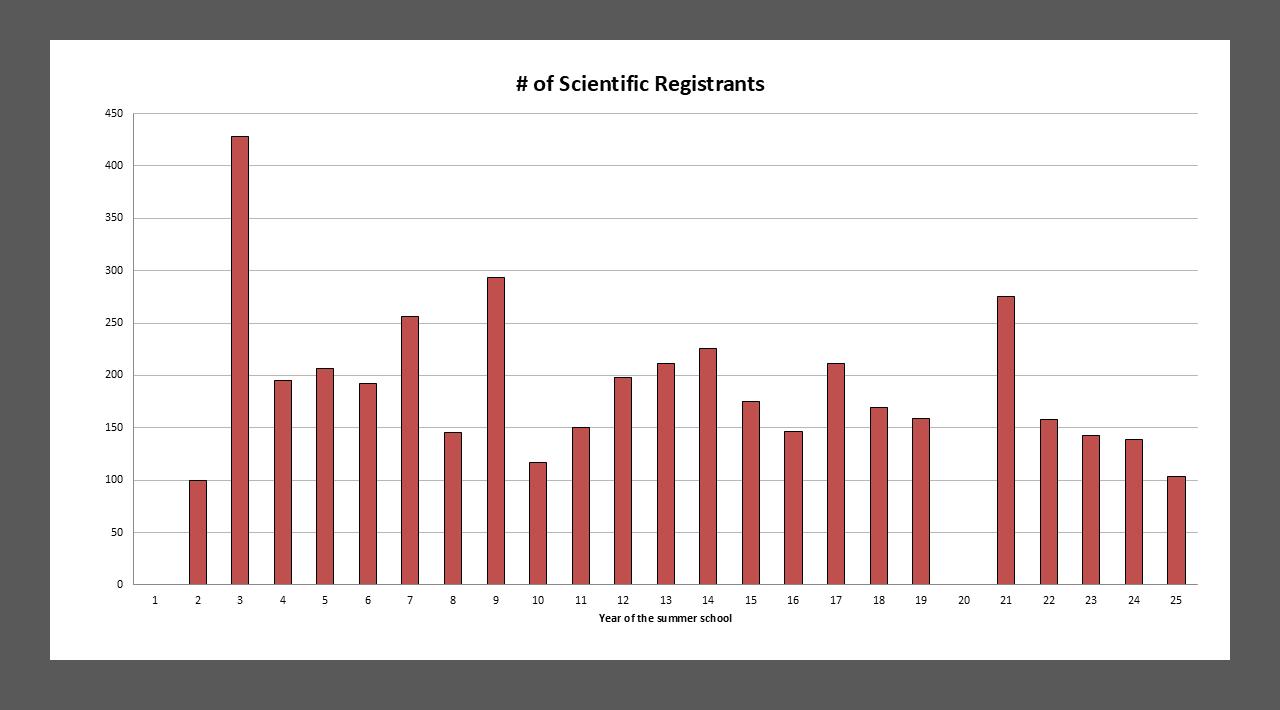
Scientific registrant numbers have remained remarkably steady over the past two decades, reflecting the enduring value of the in-person Summer School model. Attendance tends to be strongest for therapy-focused topics, though all schools consistently attract a robust and engaged audience.
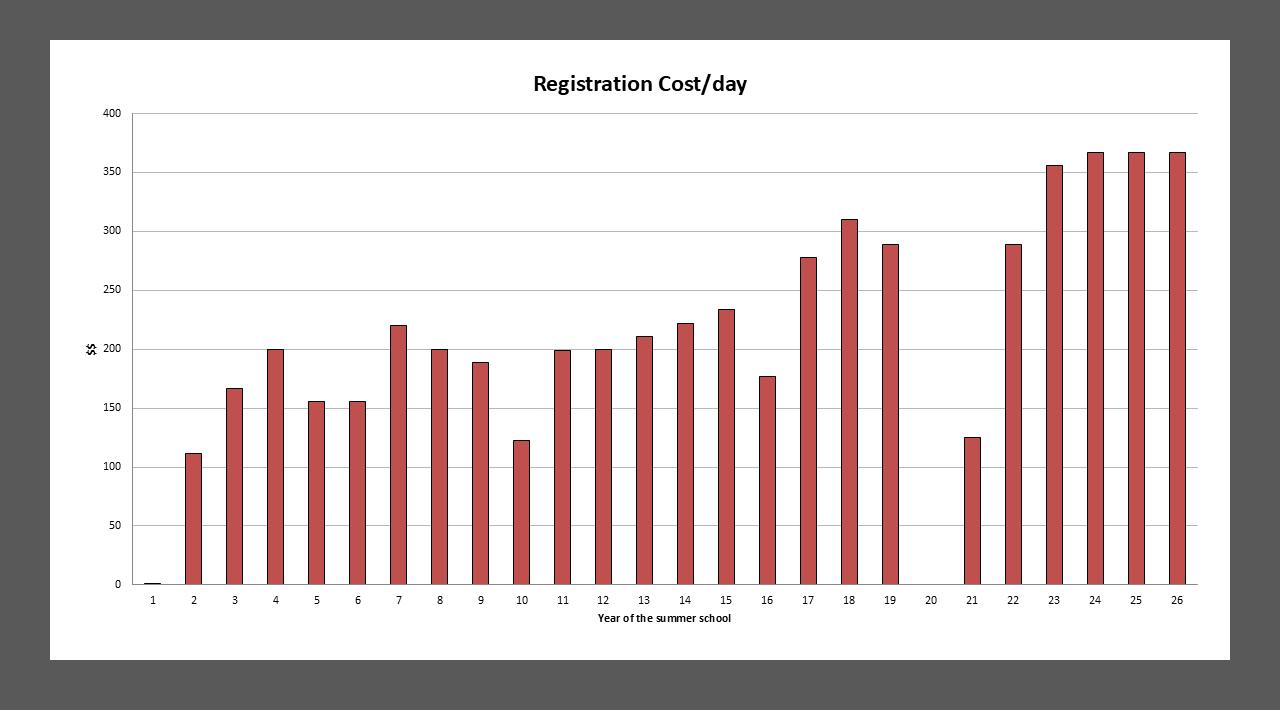
Despite rising costs, daily registration fees have increased only gradually. Recent efforts have held costs flat, preserving access while maintaining quality. Registration continues to include meals, housing, a printed monogram, evening events, and on-demand content, offering strong educational value.
dive. A temporary academic village built around a single topic.
The subcommittee’s charge is broad. It guides the educational and logistical structure of each Summer School, reviews proposals, recommends topics, and approves sites and dates. It works with publishing partners on the monogram and collaborates with the Finance Committee to review budgets and fees.
What began as a purely volunteer-led initiative remained so for decades. Since 2005, the program has become a close partnership with AAPM Headquarters. Karen MacFarland, and now Linda Minor, have played key roles in helping the program grow while preserving its academic integrity.
Ask any repeat attendee, and they’ll tell you: the Summer School doesn’t feel like a conference. It feels like something more immersive, more connected, and more personal.
The program focuses on a single clinical topic and takes place in a residential setting. Participants live on campus, eat in the cafeteria, and interact informally with faculty and peers from breakfast through bedtime. Faculty stay onsite all week, creating opportunities for mentoring and indepth discussion.
The educational design is intentional. In-person sessions focus on interactivity, while longer lectures are offered online. A peer-reviewed monogram supports deeper reading. Hands-on workshops reinforce concepts and allow for practical engagement. The design supports multiple learning
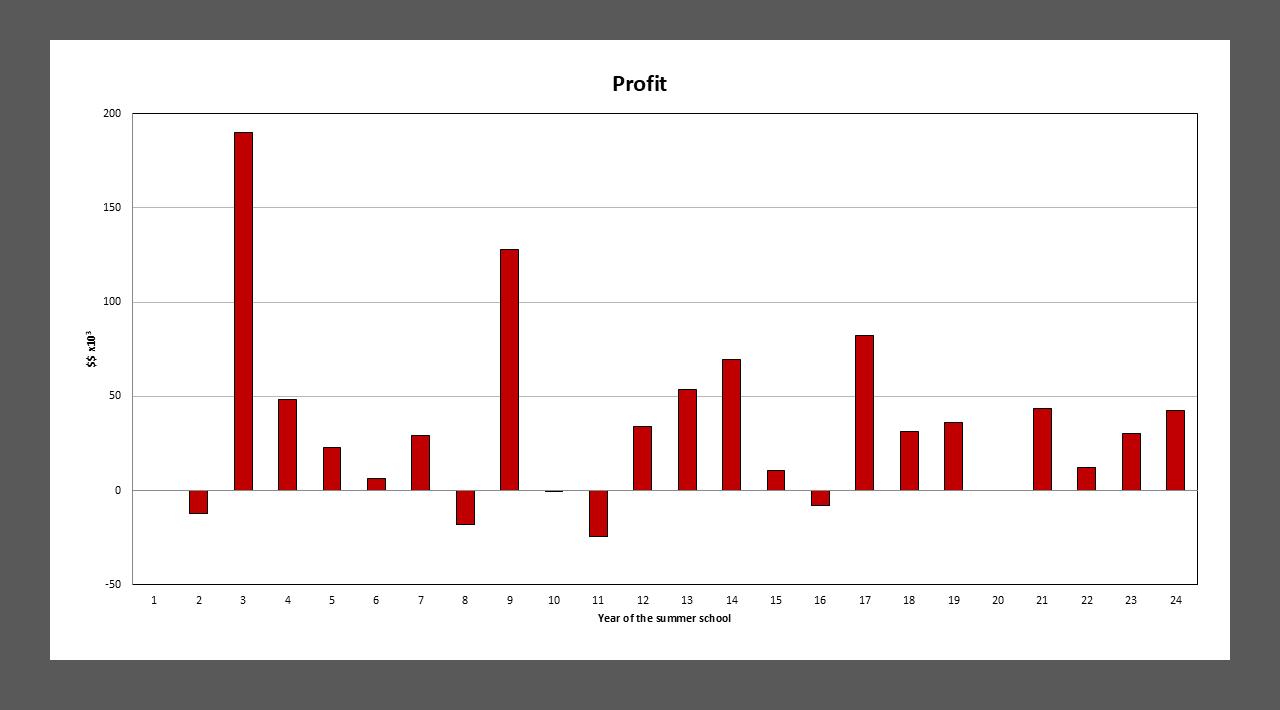
Profit from AAPM Summer School (2002–2024) Summer School profits have varied year to year, reflecting differences in topic appeal and format. Therapy-focused schools tend to generate higher returns, while others prioritize essential education despite lower margins. In recent years, the program has maintained sustainable profitability, supporting AAPM’s broader mission. This consistency allows the Summer School to meet its goal of delivering a $60K rolling three-year average, contributing reliably to the organization’s financial health.
styles, from visual to kinesthetic to collaborative.
Evenings are not unstructured. They are reserved for informal, high-value sessions - without CAMPEP credit, but full of educational depth. Over beer and wine, participants and faculty tackle medical event scenarios, artifact troubleshooting, “Good Plan, Bad Plan” case studies, ethical dilemmas, and even trivia. These events build professional community in ways that slides and lectures alone cannot.
The Long Road to Each Summer School
Planning a Summer School typically takes two years. It starts with a Request for Proposal (RFP) from members. Proposals outline the structure, clinical significance, proposed faculty, and
ideas for engagement. Many are detailed enough to serve as full course outlines.
The SS Subcommittee evaluates proposals based on diversity, relevance, interactivity, and feasibility. Selected schools run in either a 2.5-day or 4.5-day format.
Program Directors then work with the SS Subcommittee and AAPM HQ to build the schedule, finalize faculty, and coordinate the monogram. Headquarters handles the logistics, including housing, dining, breakout rooms, and classroom setups.
The choice of location is strategic. Most schools are held on academic campuses that can support workshops and, when needed, clinical equipment like linear accelerators or CT simulators. Lecture spaces
must have clear sightlines, good acoustics, and reliable A/V. Dorms must be clean, comfortable, and within walking distance. Dining services must accommodate dietary restrictions and serve meals on a fixed schedule. Access to outdoor spaces and activities for the afternoon off is a bonus. Cost is a constant consideration.
Despite rising costs in higher education and hospitality, the AAPM Summer School remains remarkably affordable. Registration includes:
• Three full meals per day
• Two refreshment breaks
• All academic sessions and the monogram (produced only for this AAPM meeting)
• Evening receptions and events
• The traditional afternoon off with swag (T shirt)
• One-year access to recorded content (for registrants only)
Few national programs offer this level of immersion at this price point.
Attendance remains strong. Therapyfocused topics draw the largest crowds. The 2003 IMRT Summer School set records in both attendance and profit. The 2009 Clinical Dosimetry school, led by Dave Rogers and Joanna Cygler, followed closely. Most recent schools return $30,000 to $40,000 in profit. This supports a rolling three-year average of $60,000, helping offset lower-profit but clinically essential topics.
The Summer School was the first AAPM meeting to offer on-demand access to registrants. This has been standard
for years. But the in-person experience remains irreplaceable. You can watch the content later. But if you miss the school, you miss the magic.
The impact of the Summer School extends beyond the campus. Each year, select sessions are featured at RSNA under the Best of AAPM Summer School banner, with a focus on imaging content for a diagnostic audience. Regional AAPM chapters have also hosted highlights from
recent schools. The SS Subcommittee welcomes opportunities to collaborate with local groups who want to bring the content home.
In 2026, the Summer School will focus on Adaptive Radiation Therapy June 16-20, and is hosted in Ann Arbor, Michigan.
In 2027, the focus will shift to ReIrradiation in the Clinic. Tentative dates are June 24–28, with plans to return to

The 2025 Summer School cohort poses with their monograms at the University of Denver, host of the 55th AAPM Summer School focused on Clinical MR Physics: State-of-the-Art Practice. Each participant received a copy of the monogram, a hallmark of the Summer School experience and a lasting reference that reflects the depth of the program.
the Boston area, bringing the Summer School full circle to its roots.
Mark your calendars. Pack your walking shoes. Bring your questions.
Because if the AAPM Summer School Subcommittee has shown anything over the last 50 years, it's that inperson, interactive education is here to stay. ¢

Planning for an AAPM Summer School begins years in advance, with site visits playing a key role. On the left, Karen MacFarland and Vrinda Narayana visit Southern Methodist University while scouting locations for the 52nd Summer School on Small Field Dosimetry. On the right, Linda Minor and Vrinda tour the University of Denver in preparation for the 55th Summer School on Clinical MR Physics
The 2024 AAPM Summer School began with a lively icebreaker reception on the campus of Dartmouth College, setting the tone for a week of learning and connection. Pictured here is C. David Gammel, AAPM Executive Director, joining attendees in welcoming participants to the 54th Summer School on Workflow Optimization in Radiation Oncology

Learning Through Real Cases: A defining feature of the AAPM Summer School is its commitment to interactive, real-world learning. In this session, Dr. Robert Timmerman, MD, Chair of the Department of Radiation Oncology at UT Southwestern, leads an in-depth discussion on actual patient treatment plans. Participants examine clinical cases in small groups, weighing the pros and cons of different planning approaches, and discussing compromises made in real-world scenarios. Sessions like this bring faculty and attendees together to tackle the complexities of clinical decision-making — beyond what textbooks can teach.

Modern Learning in Action: 53rd Summer School at the University of Minnesota This photo captures a modern, tech-enabled classroom during the 53rd AAPM Summer School, held at the University of Minnesota in 2023. The focus that year was on Radiopharmaceutical Therapy and Dosimetry. Designed for interactive learning, the tiered classroom layout supported dynamic discussions between attendees and faculty, reinforcing the Summer School’s commitment to real-time engagement and hands-on education.

Making QA & QC Memorable: At the 54th AAPM Summer School, a creative workshop used bracelet-making to illustrate key concepts in QA, QC, workflow, and bottlenecks. Handson activities like this helped turn complex ideas into something tangible and fun. When moving from theory to clinical implementation, learning sticks better when it’s tied to something creative — and wearable!

ADAPTIVE RADIOTHERAPY: TRANSFORMING TECHNOLOGY, MODERN PRACTICE, AND CLINICAL IMPACT — WHY THE 56 TH AAPM SUMMER SCHOOL SHOULD BE ON YOUR 2026 CALENDAR
Vrinda Narayana,
PhD | University of Michigan, Henry Ford Providence
Bring your team. ART is multidisciplinary, and this Summer School is built for physicists, physicians, dosimetrists, and therapists to learn together—through discussion, debate, and hands-on workshops that translate directly to clinical practice. Register here.
Adaptive Radiotherapy (ART) has moved fast. It’s no longer a “future state” idea limited to a few flagship centers. With better imaging, smarter automation, improved motion management, and more datadriven planning, ART is becoming an everyday expectation in modern radiation oncology. The mindset shift is real: we’re moving from delivering a single plan to delivering a course of treatment that can respond to a patient’s anatomy, physiology, and biology as they change.
Why ART? And Why Now?
ART is exciting. It’s also hard. ART adds new technical challenges, workflow bottlenecks, safety risks, and team communication demands. Clinics everywhere are asking the same question: how do we implement and/ or refine ART in a way that is clinically meaningful, efficient, and safe, across real-world constraints?
The 2026 AAPM Summer School on Adaptive Radiotherapy: Transforming Technology, Modern Practice and

Clinical Impact (June 16–20, 2026) is built to answer exactly that. This year’s Summer School is an immersive experience for medical physicists, radiation oncologists, dosimetrists, and therapists who want to integrate or optimize ART in their practice. The point isn’t just understanding ART as a concept. It’s leaving with the confidence to lead adaptive workflows in diverse clinical settings.
Since 1969, AAPM Summer School has become a defining educational tradition. It has evolved with the field, moving from primarily didactic sessions to a more interactive, applicationdriven experience. ART is the perfect
topic for that format. Learn the principles. Then pressure-test them against implementation reality.
Interactivity isn’t an add-on. It’s the design. The week goes beyond lecture-only learning. Expect repeated opportunities for discussion, debate, and engagement, the kind of learning that turns “interesting” into “actionable.”
If ART is on your roadmap or already part of your clinic’s day-to-day planning, timing matters. Registration opens March 9, 2026. Early Bird ends May 18. Register early. Stay in the dorms. Eat in the cafeteria. Go
home with a Summer School t-shirt, a proceedings book, on-demand session recordings, and the ability to earn continuing education credits, all for under $2000 for four days. Scholarships are also available for early-career medical physicists, helping broaden access at a key stage of professional growth.
The 2026 Summer School is led by Program Directors with deep expertise in adaptive radiotherapy physics and clinical implementation: Laura I. Cerviño, PhD (Memorial Sloan Kettering Cancer Center), Dandan Zheng, PhD (University of Rochester), and Heng Li, PhD (Johns Hopkins Medicine). Claire Park and Xiuxiu He, as part of the AAPM Science Council Associates Mentorship Program (SCAMP), also played an instrumental role in organizing the 2026 Summer School and serve as faculty as well, bringing an important early-career perspective.
Together with an invited faculty slate spanning academic and clinical institutions, the program reflects the full breadth of ART, from core imaging and workflow design to advanced and emerging directions.
What does it feel like as an attendee? Like moving through the full arc of ART, from the “why” to the “how,” and into the decisions that determine whether a program succeeds or stalls. You’ll dig into adaptive workflows across modalities and clinical approaches, including CBCT-based online adaptive workflows, MR-guided ART, and other paradigms reshaping practice. You’ll
also explore the expanding ART universe, including proton adaptation, PET-guided adaptation, and biologically informed strategies aimed at aligning treatment with patientspecific response.
The value isn’t just seeing the options. It’s understanding what each approach demands in real life, including complexity, staffing implications, and safety considerations.
Implementation is treated as the main event because ART succeeds, or fails, between the big idea and the treated patient. The program focuses on the essentials: registration and segmentation strategy, dose accumulation and reporting, image quality, motion management, and margins. It also includes forwardlooking topics like AI and synthetic images, with an emphasis on responsible use.
Safety and quality are woven throughout, including QA, risk analysis, and adaptive safety frameworks, plus the people-and-process realities that make programs sustainable: training, role clarity, workflow design, and ethics. The energy comes from how it’s taught, through iterative problemsolving, candid peer discussion, and direct conversations about what worked and what didn’t. The week culminates in a dedicated day of Adaptive Workshops, giving attendees a chance to pressure-test workflows under realistic constraints and leave feeling ready to make ART work.
Ann Arbor Adds to the Experience
The setting adds to the experience.
Hosted at the University of Michigan in Ann Arbor, the 2026 Summer School benefits from an environment built for immersive learning. Ann Arbor is walkable, welcoming, and easy to explore. It’s the kind of place where conversations keep going after sessions, over meals, coffee, and evening walks. Summer School has always been about more than a syllabus. It’s community learning, and a campus-centered environment helps that happen.
Summer School is also about community. The 2026 program brings together clinicians, physicists, dosimetrists and therapists who share a deep interest in adaptive radiotherapy, creating opportunities to learn from peers at different stages of ART adoption. Conversations during sessions, workshops, meals, and informal gatherings often become as valuable as the lectures themselves, helping participants exchange practical insights, compare approaches, and build professional relationships that support ongoing learning and collaboration.
Ultimately, the promise of the 2026 AAPM Summer School is simple: you don’t just leave with information. You leave with clarity. A good course teaches you what something is; a great course changes what you do. By design, this year’s Summer School aims to help participants return home ready to speak confidently about ART workflows, evaluate implementation risks and bottlenecks, strengthen safety and QA thinking for adaptive practice,
and participate more effectively in decision-making around adaptive care.
Save the Date
The dates to remember are June 16–20, 2026 Registration and housing open March 9, 2026 Early
Bird registration ends May 18 The Tuition Scholarship portal has been open since Jan 14, 2026. If adaptive radiotherapy is part of your clinic’s present, or its near future, the 56th AAPM Summer School offers a practical opportunity to accelerate implementation maturity, connect
with peers solving the same problems, and learn directly from faculty shaping adaptive radiotherapy practice today.
For additional questions about the Summer School, please contact vnaraya1@hfhs.org ¢

These experiences are designed to support your learning, career development, and connection with peers and professionals across the field.
We’re building a dynamic lineup at the 2026 Joint AAPM | COMP Annual Meeting & Exhibition created specifically for you.
STUDENT NIGHT OUT



Greetings from the AMSC! With 4,335 participants, our 2025 Annual Meeting & Exhibition in Washington, DC was a tremendous success. We are grateful to everyone who attended and contributed to the meeting’s outstanding quality. The overwhelmingly positive feedback reflects the dedication and engagement of our society’s members; each year’s success is truly made possible by your participation.
Looking ahead, the 68th Annual Meeting & Exhibition, titled “Medical Physics Community: Inspiration, Innovation, Impact,” will be a Joint AAPM | COMP Annual Meeting & Exhibition held in Vancouver, British Columbia. The meeting will run from Sunday, July 18 through Wednesday, July 22, 2026, continuing the successful Sunday–Wednesday format introduced last year.
Keynote Speakers
Building on the success of last year’s first ever keynote sessions, we are pleased to announce our 2026 keynote speakers.
Our first keynote speaker is Dr. Douglas Boreham of the Northern Ontario School of Medicine University (NOSM U). Dr. Boreham is Professor and Division Head of Medical Sciences at NOSM U and Professor in the Department of Biology at McMaster University. He is a board member of the Radiation Research Foundation and was the 2024-2025 President of the Radiation Research Society. His research focuses on radiation biology, and he supervises undergraduate, graduate, and postdoctoral trainees. Dr. Boreham has published more than 160 peer-reviewed manuscripts and has secured over $18 million in research funding. His work spans low-dose medical radiation health effects (CT and PET), radioprotective dietary supplements to prevent age-related cognitive decline, predictive assays for radiosensitivity in radiation therapy, and cytogenetic assays for DNA damage detection and emergency biological dosimetry.
Our second keynote speaker is Dr. Simon Cherry, Professor of Radiology and Biomedical Engineering at the University of California, Davis, and Professor of Total Body Imaging at King’s College London. Dr. Cherry’s research centers on biomedical imaging, with major contributions to positron emission tomography (PET). He is a co-leader of the EXPLORER consortium, which developed the world’s first total-body PET scanner. His work also includes innovations in PET detector technology, early biomedical applications of Cerenkov luminescence, and the first proof-of-concept hybrid PET/MRI systems. Dr. Cherry is an elected Fellow of six professional societies, a member of the U.S. National Academy of Engineering and the National Academy of Inventors, and served as Editor-in-Chief of Physics in Medicine and Biology from 2011–2020. He has authored more than 300 peer-reviewed publications and is

Cincinnati Children's Hospital Medical Center

University of Maryland
The 68th Annual Meeting, titled “Medical Physics Community: Inspiration, Innovation, Impact,” will be a Joint AAPM | COMP Annual Meeting & Exhibition held in Vancouver, British Columbia. The meeting will run from Sunday, July 18 through Wednesday, July 22, 2026
FROM THE ANNUAL MEETING SUBCOMMITTEE , Cont.
lead author of the widely used textbook Physics in Nuclear Medicine
The 2026 Joint AAPM/COMP Annual Meeting & Exhibition will continue the successful structure introduced in 2024 and 2025, with sessions organized by specialization: (1) Professional, (2) Diagnostic and Interventional Radiology Imaging, (3) Radiopharmaceuticals, Theranostics, and Nuclear Medicine, (4) Therapy, (5) Exhibit Hall and Vendor Showcase, and (6) SNAP Orals. In addition to these 6 session tracks, an all-day Clinical Trials Program will be held on Monday, July 20
This program will bring together global experts involved in the development, implementation, and management of clinical trials. Topics will include artificial intelligence in clinical trials, expanding the role of medical physicists in trial support, combined external beam radiation therapy and radiopharmaceutical trials, diagnostic and screening trials, and two joint sessions with ESTRO and ASTRO.
Each evening will feature opportunities for members to connect and celebrate. Events will include an opening party on Sunday evening, the Awards and Honors Ceremony and Reception on Monday, and the Leadership Reception on Tuesday. As always, we will continue to offer, and expand upon, the amenities our members value at the Annual Meeting.
We look forward to an exciting and enriching Joint AAPM/ COMP Annual Meeting & Exhibition and are confident that the program will enhance your experience. Together, we will continue to advance the field of medical physics and foster collaboration across diverse specialties. We invite you to join us in Vancouver, BC, and contribute to the success of this important event. Thank you for your continued support of AAPM and COMP; we look forward to seeing you in July. ¢


Thanks to the generous support of the Southwest Chapter (SWAAPM), the AAPM DREAM (Driving Recruitment through Education and Mentoring) Program was able to o er an additional undergraduate summer fellowship this year.
The Upstate New York Association of Physicists in Medicine (UNYAPM) presented its 2025 Lifetime Achievement Award to Stanley Benedict, PhD, during its fall meeting held on December 6, 2025 at the Zebro Family Conference Center on the campus of Roswell Park Comprehensive Cancer Center in Buffalo, NY. Dr. Benedict is the 24th recipient of this annual award; previous winners can be found on the Chapter’s website: https://unyapm.org/ hall-of-fame.
Dr. Benedict is Professor and Chair of Medical Physics in the Department of Radiation Oncology at the Massey Cancer Center at Virginia Commonwealth University in Richmond, VA. He received this award in recognition of his many contributions to the field of medical physics throughout his career. During the award ceremony, Dr. Benedict presented a talk titled “Overview of the preparation, submission, and review of manuscripts to the AAPM journal, Medical Physics”, which was of special interest to the student members who attended the meeting. Dr. Benedict, who currently serves as Editor — Therapy for Medical Physics, gave some important pointers on manuscript preparation for the AAPM’s two journals: Medical Physics and the Journal of Applied Clinical Medical Physics


James Steinman, MS Roswell Park Comprehensive Cancer Center

Alexander Podgorsak, PhD University of Rochester

Islam,
Roswell Park Comprehensive Cancer Center

Matthew Podgorsak, PhD Roswell Park Comprehensive Cancer Center
The Chapter also hosted its annual Young Investigator Symposium. This year there were competitors from medical physics graduate programs at the University at Buffalo and the University of Rochester. The 3rd place winner was Edward Opalko, MS who spoke on the ‘Dosimetric evaluation of interfractional shift corrections in Gamma Knife radiosurgery using a 3D printed phantom’. In 2nd place was Sudeeptha Liyanage, MS, who presented ‘Digital twin approach to PET/CT image-driven Monte Carlo precision dosimetry in theranostics’. And the 1st place prize was awarded to Ricardo Garcia Santiago, MS for his presentation on the ‘Effect of matrix size on accuracy and calculation time for a deep-learning VMAT dose engine’. All seven competitors gave great talks; it was difficult to select the top three.

The Young Investigator Symposium was followed by a scientific session during which Siddarth Mehta, BS and Avantika Guleria, BS presented their results on ‘Indexing projection angular sampling completeness and multiplexing to enable multiplexed SPECT imaging’. This talk
The AAPM Physics Plan Review Toolkit Specialty Meeting is a virtual, interactive experience designed to support high-quality physics plan review through practical learning, real-world scenarios, and peer collaboration. Stay tuned for details.
was followed by Nicholas Becerra-Espinosa, MS who spoke on the ‘Effects of CT table displacement and pitch on respiratory gating for scanners’.
The next semi-annual meeting of the Chapter will be held in Rochester, NY in spring 2026. More information can be found at the Chapter’s website: https://unyapm.org. ¢
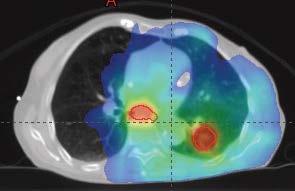
Resources & Contacts:
• CDPH Radiologic Health Branch
• For technical and regulatory questions, contact the RHB-RMT inbox or your regional office.
President’s Welcome
Julie Shen, President of the AAPM-SCC, opened our Fall 2025 meeting with a warm welcome to members and guests. We were honored to host two distinguished CDPH officers who provided essential updates for our chapter’s medical physicist community.
Meeting Highlights
Radiologic Health Branch Updates
• Sean Tierney (Radiation Machine Inspection, Compliance & Enforcement Section Chief) presented updates on regulatory changes, inspection programs, and resources for facilities.
• The CDPH website remains the key resource — visit the “New and Important” section for all recent notices and changes.
Medical Physicist Registration & Facility Certification
• Manasa Pinisetty (Senior Health Physicist) reviewed updated procedures for medical physicist applications, renewals, and training requirements.
• The online registration portal now makes it easier to maintain compliance for all X-ray and mammography facilities.
Mammography: New Technology & Compliance
• The CDPH has certified the novel Coning Vera CDT 1000 breast CT unit; ensure all new mammography/CT units meet dual state and federal requirements.
• Facilities must keep both their registration and equipment certificates current.
Therapy Equipment: Authorization Steps
• Outlined the three-stage process for therapy equipment approval.
• Authorization for physical measurement must be initiated at least 60 days before installation or construction.


Southern California




Reminders:
• Frequently review the CDPH RHB website for updates.
• For inspection/compliance questions: reach out to your RHB regional contact.
• Physicists: submit 8-hour CT/DBT training proof with renewals or via the RHB-RMT inbox.
• Apply early for all therapy equipment authorizations. ¢
Medical physicists seeking certification by the ABR complete three computer-based qualifying exams: two Part 1 exams — General and Clinical — and one Part 2 exam in either diagnostic medical physics (DMP), nuclear medicine physics (NMP), or therapeutic medical physics (TMP). These are followed by a final oral certifying exam in the chosen specialty. Part 1 General and Clinical exams are based on the expected knowledge of a second-year graduate student and can be taken by the candidate at a single administration or separately. The General Exam focuses on medical physics at the level of common graduate courses. The Clinical Exam focuses on anatomy, medical terminology, and physiology at the level of an introductory course taught in a college of health sciences.
The questions that make up the ABR exams are written by medical physics volunteers who are board certified in one or more of the three specialties and are clinically active in their professional roles. Volunteers serve on either the general or clinical committee based on their specialty and professional focus.
The Part 1 General Qualifying Exam is administered to all candidates, regardless of which specialty they choose for their certification. As such, the Part 1 General Qualifying Exam Committee consists of volunteer subject matter experts from all three specialties. The committee has seven to eight members, including a chair and an associate chair. The associate chair is chosen during the chair's last year on the committee. All committees are overseen by a Trustee.
Sameer Tipnis, PhD, served as committee chair until this past October, when he became the ABR Trustee responsible for diagnostic medical physics. The committee is now chaired by Justin Zenn and includes Mandar Bhagwat, PhD; Courtney Buckey, PhD; Jian-Feng Chen, PhD; Jonathan Nye, PhD; Alek Rapchak, MS; and Yifang Zhou, PhD. The committee has been assigned one permanent ABR staff exam developer and one rotating exam developer as needed. Staff provide administrative assistance in the management of the meetings, keep track of questions reviewed, and manage behind-the-scenes issues that are critical in producing a fair and well-balanced exam within the proper time frame.
Committee members are typically selected by the committee chair and the Trustee and are appointed initially for a three-year term, with the possibility of reappointment for another three-year term. Committee members participate actively in the exam question-writing process, which runs from January to June in the year prior to the year the exam is expected to be administered. The committee members submit their questions and meet frequently during the cycle to review, edit, and ultimately approve questions that are used for the Part 1 Qualifying Exam. They are encouraged to participate in the discussions


ABR Trustee
Medical University of South Carolina

ABR Trustee
Colorado Associates in Medical

ABR
Chair, ABR Board of
Roswell Park Cancer Institute
ABR exams are written by experienced medical physicist volunteers. ABR staff edit grammar and ensure exam items meet the ABR guidelines for multiplechoice questions.
during the regularly scheduled committee meetings.
Volunteer engagement throughout a question-writing cycle is typically many hours of independent work, followed by committee meetings, and finally a 1.5day in-person annual meeting in June. An exam is constructed using both new and previously used questions and is reviewed during the annual meeting, which is attended by several committee members and a Trustee. After the committee approves an exam, the Trustee provides final approval.
UPDATE , Cont.

The ABR works hard to maintain exam quality. To this end, the Exam Development staff conduct annual assessments to evaluate both committee productivity and individual contributions. When selecting committee members from the pool of approved volunteers, the committee chair and a Trustee prioritize subject matter experts with deep, hands-on knowledge of the material that forms the foundation of the exams. To the extent possible, committees are constructed to maintain diversity in clinical practice and geographic location.
Part 1 General Qualifying Exam Committee at the annual meeting in April 2025. From left to right, and with the titles they held at the time of the photo: Rachel Alm (Exam Developer), Dr. Mandar Bhagwat, Dr. Kalpana Kanal (Trustee), Dr. Christina Brunquell, Dr. Sameer Tipnis (Chair), Mr. Justin Zenn (incoming Chair), Ashley Robles (Exam Developer), Dr. Yifang Zhou, and Dr. Jian-Feng Chen.
The ABR’s mission could not be fulfilled without the dedication and expertise of the medical physicists who
generously volunteer countless hours to develop, review, and approve the exam questions that the ABR uses to certify that all their diplomates demonstrate the requisite knowledge, skill, and understanding of their disciplines to the benefit of patients. We express our sincere gratitude to the members of this committee as well as to all the medical physics exam development committees. ¢
Our deepest sympathies go out to the families. We will all feel the loss in the Medical Physics community
If you have information on the passing of members, please inform HQ ASAP so that these members can be remembered appropriately. We respectfully request the notification via email to: 2026.aapm@aapm.org (Please include supporting information so that we can take appropriate steps.)
Entering its fifth year of support, the Medical Imaging and Data Resource Center (MIDRC) remains a central force in advancing the responsible application of artificial intelligence (AI) in medical imaging. By prioritizing wellcurated, high-quality, and diverse datasets, MIDRC supports the development and validation of innovative imaging algorithms grounded in real-world clinical needs.
MIDRC has strengthened its data infrastructure by establishing a closed citation loop using persistent digital object identifiers (DOIs), making it easier for R01 and other NIH-funded investigators to comply with the NIH Data Management and Sharing (DMS) Policy. By enabling standardized, trackable citation of datasets, MIDRC reduces administrative burden for grantees while ensuring transparency, reuse, and long-term stewardship of shared data. This approach also makes MIDRC a more attractive and citable alternative to ad hoc repositories, reinforcing its role as a trusted, high-quality resource for the medical imaging research community.
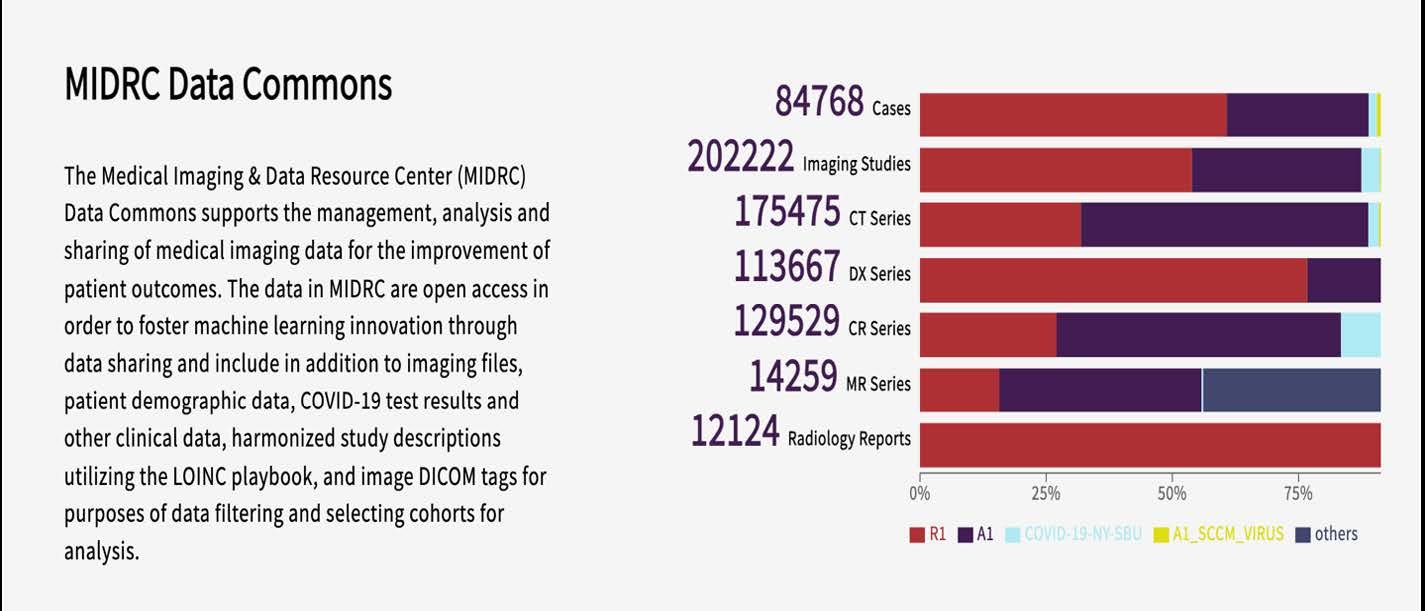
(MIDRC data publication numbers, as of January 2026. The Medical Imaging and Data Resource Center (MIDRC) is funded by the National Institute of Biomedical Imaging and Bioengineering (NIBIB) of the National Institutes of Health under contract 75N92020D00021 and through The Advanced Research Projects Agency for Health (ARPA-H))
MIDRC was invited to present at the NIH Data Science Town Hall, on Thursday, January 22. Data Science Town Halls are monthly meetings hosted by the Office of Data Science Strategy (ODSS) to share updates on the data science activities happening across NIH in support of the NIH Strategic Plan for Data Science, and are open to just NIH employees. The talk, entitled Collaboration at Scale: The MIDRC Approach to Image Data Sharing was presented by MIDRC PIs Dr. Maryellen Giger, Dr. Adam Flanders, Dr. Robert Grossman,


Maryellen Giger, PhD
University of Chicago Paul Kinahan, PhD
University of Washington
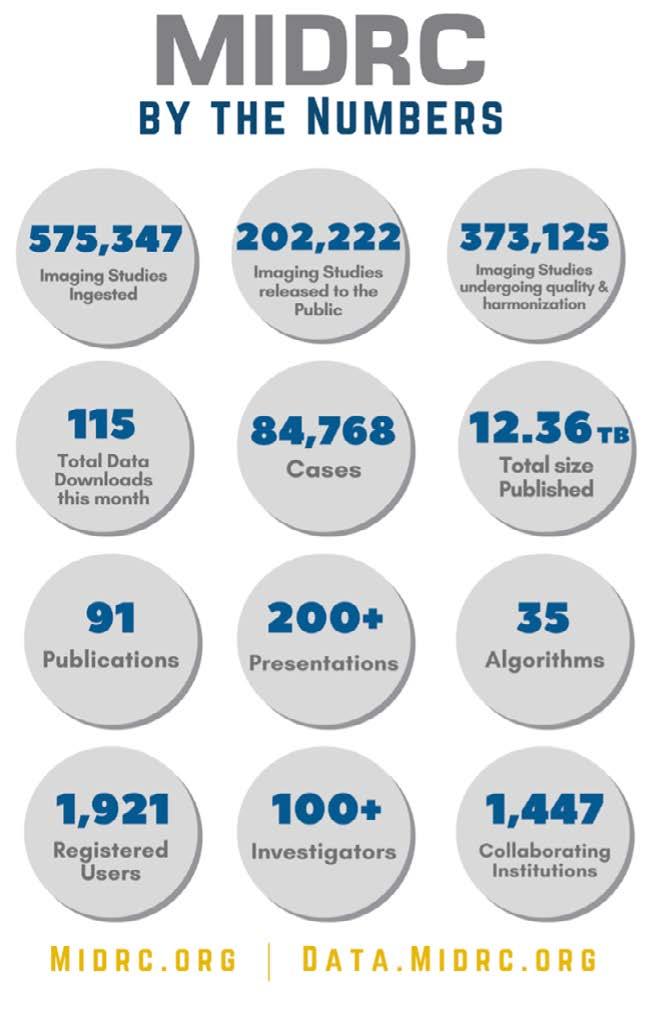
Please direct inquiries to:
Maryellen Giger, PhD, FAAPM, Paul Kinahan, PhD, FAAPM, or Emily Townley, AAPM MIDRC Program Manager

AAPM-MIDRC SUBCOMMITTEE REPORT , Cont.
Dr. Paul Kinahan, Dr. Curtis Langlotz, and Mr. Mike Tilkin. It provided a detailed overview of MIDRC, including its growth since its inception in 2020 as a flexible, efficient, and scalable imaging data solution, including its ingestion, curation and harmonization processes, its state-of-the-art infrastructure, interoperability and security, and tools and resources, as well as its impact and plans for sustainability and the future.
MIDRC had a strong presence at RSNA2025 again this past year with its well-visited booth in the Lakeside Learning Center at McCormick Place, featuring prominently across several high-impact sessions highlighting the infrastructure, governance, and clinical relevance of large-scale imaging data resources for AI research.
MIDRC leaders contributed to the advanced session Nuts and Bolts: Building a Multi-Site Data Repository for Imaging Studies & AI Validation Tools, which focused on the practical realities of creating and sustaining multisite imaging repositories. MIDRC PIs also shared MIDRC’s origin story, mission and growing impact on AI development and biomedical research during the MIDRC: Innovation in Imaging AI and Interoperability presentation held in the AI Theater. And the MIDRC: Engaging the Cancer Imaging

Research Community session introduced attendees to MIDRC’s open tools and datasets through practical examples. These talks covered MIDRC’s cancer imaging toolbox, the use of large language models to help patients better understand radiology reports, and the central role of high-quality data in translating AI into routine clinical care. Together, these sessions reinforced MIDRC’s role as a national, cross-society resource advancing responsible imaging AI and data-driven innovation.
MIDRC Investigator and AAPM-WGGC Chair Dr. Karen Drukker recently received The Academy for Radiology & Biomedical Imaging Research 2025 Distinguished Investigator (DI) Award, a prestigious honor recognizing sustained, high-impact contributions to medical imaging research.
We also congratulate MIDRC PI Dr. Maryellen Giger, the recipient of SPIE's 2026 Gold Medal for her pioneering role in computer-aided detection and diagnosis, quantitative imaging, radiomics, and imaging-based AI. Her foundational work helped establish the field of computer-aided diagnostics in medical imaging and has

been successfully translated into clinical practice, including co-founding QuantX, the first FDA-cleared machinelearning system for cancer diagnosis. Maryellen is a strong advocate for broad, responsible access to imaging AI and has spearheaded MIDRC into becoming one of the nation’s largest public imaging data resources.
There are many ways you can get involved in MIDRC’s work:
• Contribute data — MIDRC continues to welcome diverse datasets spanning diseases and imaging modalities
• Index your datasets through the BDF Imaging Hub (BIH)
• Access and test algorithms via MIDRC’s open-source GitHub repository
• Connect with the AAPM MIDRC Subcommittee — we welcome questions, ideas, and opportunities for collaboration!
We are grateful for the continued support of AAPM members and leadership, as well as our strong partnerships with RSNA, ACR, academic institutions, and government agencies across the country. Thank you for your ongoing engagement with MIDRC. ¢


Do you know an important, unsolved medical physics scientific issue?
Let AAPM's Working Group on Grand Challenges (WGGC) help you organize a Grand Challenge, an engaging way to address scientific dilemmas while connecting with the AAPM membership and the broader medical physics research community!
WGGC is dedicated to promoting Grand Challenges focused on enhancing medical imaging in diagnostic and therapeutic applications. We're currently welcoming proposals from groups interested in hosting a Challenge ahead of the 2027 Annual Meeting. Selected proposals will receive sponsorship, including some financial support, and guidance from WGGC to facilitate successful execution.
Don't miss this opportunity to make an impact! Learn more and download the proposal application form HERE.
Please e-mail proposals to Emily Townley (emily@aapm.org) by 5:00 PM EDT on Friday, July 10, 2026.
MRI SAFETY: THE INVISIBLE FORCE PODCAST
I
t wasn’t unforeseeable or a "freak accident." The July 2025 fatal MRI accident that occurred on Long Island, New York is the subject of a new multi-part podcast, the Invisible Force Podcast, available through Spotify and Apple Podcasts. The co-hosts, Tobias Gilk and John Posh, tell the story of how the accident happened, and the responses and reactions (both expected and surprising) in the wake of this preventable tragedy.
MRI gets labeled as “the safe imaging option,” but history has shown us — many times — that there are risks that are peculiar to MRI… risks that often aren’t effectively managed. When your odds of getting an MRI in the next year are around 1-in-10, MRI safety will be of interest to you.
The podcast is built around telling the story of the accident and those involved. If you’re interested in medical dramas like The Pitt, or true-crime mysteries, you’ll enjoy the narrative-propelled story that makes you feel like you’re in the room while it’s happening.
“MRI accidents are almost 100% anticipatable and preventable,” says cohost Tobias Gilk. “This means that they’re especially tragic when we let one happen.”
Season one of the Invisible Force podcast will detail what happened that allowed Mr. Keith McAllister to be ‘sucked up’ into an MRI scanner by a heavyduty chain around his neck, what structures are supposed to be in place to keep us all safe during MRI, and how this accident -or ones like it- could be prevented.
The Invisible Force podcast is also relying on crowd-sourcing to help with the end of the story, between their website and a tip-line specific to MRI incidents (631-MRI TIPS or 631-674-8477), the hosts are gathering details on what happens in response to this tragedy.
The podcast is available for subscription and download through both Apple Podcasts and Spotify: Apple Podcasts: https://podcasts.apple.com/us/podcast/invisible-force/ id1860117430
Spotify: https://open.spotify.com/show/1KDYV8Z4Md5x9mW8pFccsw
The first season of the Invisible Force podcast has been underwritten by CAIREreporting.org, an online and enterprise MRI adverse event reporting platform. ¢

Tobias Gilk, MRSO, MRSE Gilk Radiology Consultants
Throughout the medical world we heard about the fatal MRI accident that happened in New York in the summer of 2025. The initial reporting, however, was somewhat slapdash, and corrupted with spin from the interested parties. What *actually* happened... and how do we help make sure that accidents like this don't happen again?
Contact:
Tobias Gilk, MRSO, MRSE Invisible Force Co-host and Producer 913-515-8449
TGilk@MRIpatientsafety.com
https://invisibleforcepodcast.com
Tuesday, July 21, 2026
5:10 PM–6:00 PM
Vancouver, Convention Center, Room 301
As a new member of AAPM, it is easy to feel overwhelmed by the size and complexity of the association and to be unaware of the benefits and opportunities available to members. At this year’s AAPM Annual Meeting in Vancouver, BC, we will host a New Professional Symposium where you can learn more about the organization, member resources, opportunities to get involved, and about topics of particular interest to new professionals. We encourage you to take advantage of this great opportunity to learn valuable information and to grow your professional network.
Registered attendees will receive a raffle ticket. Enter to win a complimentaryregistration for the 2027 Annual Meeting & Exhibition in Columbus, OH!
In addition, all new members who register for the Symposium will receive a drink ticket, good for one complimentary soda or beer served after the Professional Symposium during the social with committee chairs from five AAPM Councils: Science, Education, Professional, Administrative, and International.

A Headshot Lounge will be available in the Exhibit Hall to have a professional photo taken for your AAPM Member Directory profile. Get Your Picture Taken.
Written on behalf of the RTSEC membership
Radiation therapy (RT) clinics rely on a complex ecosystem of information systems to support clinical care. While communication protocols and data standards are addressed by established standards organizations such as DICOM and HL7, and interoperability frameworks are developed within groups such as IHE-RO, there remain important areas of system interaction that fall between these efforts or lack concrete, implementation-focused guidance.
Recognizing this gap between standards, the leadership of the DICOM WG07 (DICOM-RT) and IHE-RO committees encouraged the formation of the RT Systems Engineering Council to focus on these cross-cutting challenges. The council’s membership spanning vendors, clinical medical physicists, and physicians brings practical experience at the intersection of system design and clinical use.
Informed by current academic and professional literature, the group applies this expertise to evaluate the current landscape, build consensus, and develop pragmatic position statements for the radiation therapy community, with the goal of establishing a sound technical foundation for future guidance and collaboration.
As an initial focus, the council is examining the current state of security across networked components in radiation oncology, including existing practices, limitations, and candidate-engineered solutions that may be realistically deployed within clinical environments. Experience across the radiation oncology community has underscored the practical challenges of securing and integrating clinical systems in increasingly networked environments.
In day-to-day practice, radiation therapy departments operate collections of tightly coupled yet independently designed systems, many of which are legacy platforms with limited ability to adopt modern security architectures. As connectivity increases, these constraints complicate the application of recommended cybersecurity controls and can create mismatches between theoretical best practices and what can be safely and reliably deployed in clinical workflows.
The RT Systems Engineering Council aims to bridge these gaps by taking a systems engineering view of how radiation oncology technologies are actually used and interconnected in the clinic. By considering existing standards, cybersecurity guidance, and real-world clinical workflows together, the council works to identify areas where failures, misuse, or unexpected interactions are most likely to occur and to understand the relative impact

Stuart Swerdoff, PhD
RT Systems Engineering Council
Co-Chair

Rex Cardan, PhD
UAB | RT Systems Engineering Council Co-Chair
Modern radiation therapy depends on tightly interconnected systems that were often designed independently and deployed incrementally over decades. As clinics integrate treatment planning systems, oncology information systems, imaging platforms, and hospital IT infrastructure, risks increasingly emerge not from individual components, but from how those systems interact in real clinical workflows. The RT Systems Engineering Council was formed to address this gap by bringing vendors, physicists, and physicians together to examine system integration from an engineering perspective grounded in clinical reality. By focusing on how technologies are actually used, constrained, and interconnected in practice, the Council aims to develop pragmatic guidance that improves safety, security, and reliability across the radiation therapy ecosystem.
of those risks. This approach supports the development of practical prototypes and shared recommendations that vendors can realistically implement, and clinicians can meaningfully apply.
Cybersecurity has emerged as a paramount priority for the healthcare industry, necessitating a rigorous, pragmatic analysis of its implications for radiation therapy departments and their integration within broader hospital ecosystems. While DICOM specifies protocols for secure communication, vendors within DICOM WG-07 and IHE-RO have encountered significant difficulties in implementation, deployment, and interoperability of these security protocols.
There are a variety of excellent recommendations regarding cybersecurity processes, including those specific to radiation therapy departments. However, there is currently a lack of agreed-upon, implementation-specific guidance that vendors and clinics can reliably follow.
To address this, the RT Systems Engineering Council has initiated STRIDE-based threat modeling of selected workflows between systems within the radiation therapy department. STRIDE is a widely used industry framework for identifying security risks such as spoofing, tampering, and information disclosure and provides a structured yet adaptable method for analyzing complex technical environments.
By applying this framework to radiation therapy data flows, the council aims to ensure that proposed mitigations are aligned with the most consequential cybersecurity risks. Building on this modeling work, the council’s approach is to design practical solutions and, where appropriate, develop open-source reference implementations that vendors and clinical users can adopt or adapt. In parallel, the council plans to produce white papers and other guidance materials to document the underlying problems, design considerations, and implementation tradeoffs.
Together, these outputs are intended to support informed decision-making by vendors regarding development effort, and by clinical institutions when evaluating cost, benefit, and operational impact.
The council’s near-term goal is to present STRIDE models centered on treatment planning related workflows at the 2026 Joint AAPM | COMP Annual Meeting & Exhibition. The models characterize vulnerabilities and plausible worst-case outcomes of system compromise, organized according to relative risk priority. This framing is intended to clarify where engineering effort is most impactful and to provide a shared starting point for developing solutions that improve the safety and deployability of interconnected radiation therapy systems. ¢
Artificial Intelligence T heranostic s Frontiers
yourself: What do you think you’ll be doing in ten years? What would your day-to-day work life look like?
The purpose of this Summit was to push participants to imagine — and articulate — true breakthrough challenges. That’s no small feat, especially in an intense 48-hour sprint. But the stakes are real. Medical physics, medical physicists, have the opportunity to not only survive in the future — but to thrive. We must remain relevant. So the question becomes, “How do we get there?” What does a thriving future for medical physics look like? What bold steps are required to make it real?
The Summit was a small invitation-only gathering that brought together a select group of AAPM members and external stakeholders from industry, science, medicine, and government. Together, they engaged in a deep and focused dialogue about where the field could be in ten years, the breakthrough initiatives required to get there, and ways that we can direct our profession to anticipate these changes.
I must share that the willingness of our external stakeholders to participate and partner with us was truly inspirational. Many of these attendees came from adjacent fields and had only a limited awareness of medical physics and the breadth of our expertise. Yet they generously gave their time, rolled up their sleeves, and engaged deeply in the work — helping us expand our thinking and shape what may be possible for the future.
The conversation was directed through three forward-looking lenses. First, artificial intelligence (AI) — already here and increasingly embedded in our daily lives. Second, theranostics — also present today, yet poised for significant expansion and transformation. And third, the broader frontiers of science — a space for emerging ideas and innovations that defy traditional categories but will shape what comes next.

Robin A. Miller, MS AAPM President
In an open, rapid-fire discussion the group voted to explore 6 areas for in-depth reflection; there is no implied priority in the list order.
• Education, Workforce and Incentives
• Precision Guided therapeutics (includes theranostics)
• Patient centered trust and ethical care (includes the ethics of AI)
• Professional and Scientific Frontiers/ Medical Physics Outreach
• Regulatory Science/ Synthetic Data
• AI: QA/QC, Integrated Intelligence, End-to-end data custody/provenance, AI agents (and Robots)
Each category is only a starting point — beneath each lies a far wider landscape of emerging challenges and opportunities.
More information will be shared in the coming weeks and months as we digest the output of the six groups, combined with the many pre-Summit interviews. There will be many opportunities for members to engage.
The Councils will draw upon the Summit outcomes, the many conversations that preceded it, and the
foundational work of the Ad Hoc Committee on New Science envisioned by Ehsan Samei and chaired by Jim Dobbins, to curate and distill these insights into clear recommendations for where our field should explore next. These ideas will help shape the next AAPM Strategic Plan and guide the Board of Directors as it determines where to focus the Association’s efforts, where to invest resources, and how best to allocate funding.
I am indebted to the entire Excom team (M. Mahesh, Andrew Maidment, Sam Armato, Sonja Deterich, and David Gammel) including our past chairman of the Board, Todd Pawlicki as well as the prior officers and board of directors who understood this need and chose to make this a priority. I have immense gratitude to our AAPM HQ staff and especially Emily Townley, whose effort made this Summit possible.
This is an exciting time to be a medical physicist. There will be many more newsletter articles forthcoming. If you will be joining me at our 2026 Joint AAPM | COMP Annual Meeting & Exhibition in Vancouver, we will be having a special session on The Summit to provide more information. ¢ EXCOM SUMMIT REPORT , Cont.





The AAPM Awards and Honors Committee is happy to announce that AAPM member Thomas G. Ruckdeschel has been selected by the Conference of Radiation Control Program Directors to deliver the prestigious 2026 Villforth Lecture. Mr. Ruckdeschel was nominated by the American College of Radiology with support from AAPM. He will deliver his lecture “Radiation Exposure Monitoring in Medical Imaging: Evolution of Methods, Effectiveness and Potential Pitfalls” in May at the annual meeting of the CRCPD. He joins a distinguished group of AAPM members who have received this honor over the last 20 years. ¢